pre-operative heparin reduces pulmonary microvascular fibrin deposition following cardiac surgery
TRANSCRIPT

Thrombosis Research 127 (2011) e27–e30
Contents lists available at ScienceDirect
Thrombosis Research
j ourna l homepage: www.e lsev ie r.com/ locate / th romres
Letter to the Editors-in-Chief
Pre-operative heparin reduces pulmonary microvascular fibrindeposition following cardiac surgery
Background
Cardiac surgery triggers a pulmonary inflammatory response due tolung ischemia and the release of inflammatory mediators throughcontact of bloodwith the foreign surface of the cardiopulmonary bypasscircuit. There is indirect evidence that this inflammatory response maycause lung injury through the developmentof pulmonarymicrovascularfibrin deposition. Animal models of cardiopulmonary bypass orpulmonary ischemia demonstrated the development of pulmonarymicrovascular fibrin deposition. Furthermore, of important clinicalrelevance, administration of anti-coagulants limited both pulmonarymicrovascular fibrin deposition and the extent of lung injury [1–4].Similar results have been demonstrated in clinical studies. Cardiacsurgerywas associatedwith an increase in the pulmonary dead space (afinding consistentwith pulmonarymicrovascularfibrin deposition) andevidence of coagulation activation in the pulmonary circulation,providing strong but indirect evidence of pulmonary microvascularfibrin deposition [5]. Moreover, a pre-operative heparin infusionattenuated the increase in pulmonary dead space and the extent ofcoagulation activation in the pulmonary circulation [5]. In the currentstudy we sought to establish direct evidence of pulmonary microvas-cular fibrin deposition in patients undergoing routine cardiac surgerythrough histological examination of a lung biopsy. In addition, weassessed if prophylactic anti-coagulation with heparin limited theextent of pulmonary microvascular fibrin deposition.
Materials and methods
We undertook a double blind randomised placebo controlled trialof a pre-operative heparin infusion or placebo in patients undergoingelective coronary artery bypass graftingwith cardiopulmonary bypass.Patients were excluded if they were having re-do cardiac surgery, anyplanned surgical intervention in addition to coronary artery bypassgrafting, plasma creatinine greater than 250 μmol/L, age greater than85, or current heparin administration. The study was approved by theSt. Vincent's Hospital Human Research Ethics Committee and allpatients gave written informed consent before participation.
Patients were randomised (computer generated blocks of four) toeither a continuous pre-operative infusion of heparin or placebo. Theinfusion bags (500 ml of 5% Glucose) and rates of infusion wereidentical in both groups. The pre-operative heparin group had 25,000Units (U) of heparin (Porcine Heparin Sodium, Pharmacia, MelbourneAustralia) added to the bag. The infusion commenced with a bolus of100 ml of fluid (5000 U of heparin) over 30 minutes, and wascontinued at 0.36 ml/kg/hr (18 U of heparin/kg/hr). The infusioncommenced on average 10 hours before surgery and was continueduntil cardiopulmonary bypass, at which time 300 U/kg of heparin wasadministered to maintain an activated clotting time above 480 sec-
0049-3848/$ – see front matter © 2010 Elsevier Ltd. All rights reserved.doi:10.1016/j.thromres.2010.08.022
onds. Protamine (~ 300 mg) was administered after discontinuationof cardiopulmonary bypass. All patients were administered aprotinin2 million U intravenously following anesthetic induction, followed byan infusion at 0.5 million U/hr for the duration of the operation. Anadditional 2 million U was added to the pump prime. This study wasundertaken prior to the withdrawal of aprotinin by the manufacturer.No fresh frozen plasma, cryoprecipitate or platelets were adminis-tered prior to the lung biopsy.
An open wedge biopsy of the lung was undertaken followingprotamine administration and immunostaining for fibrin undertaken(refer to the Supplement for further details of histological and statisticalanalysis). To assess the temporal changes of coagulation activation inthe pulmonary circulation the ratio or prothrombin fragments in radialand pulmonary artery blood was measured (pulmonary prothrombinfragmentproduction). At inductionof anesthesia, following sternotomy,and at 0, 1 and 2 hours following cardiopulmonary bypass, blood wasaspirated from the distal port of the pulmonary artery catheter and thenimmediately from the radial arterial line. Prothrombin fragments 1+2were assayed by enzyme-linked immunoassay (Enzygnost F1+2Monoclonal assays, Behring, Marburg, Germany).
Results
Thegroupswere similarwith respect to baseline, operative andpost-operative characteristics (Supplement, Table 1). The activated partialthromboplastin time at induction of anesthesia was higher in patientsrandomised to pre-operative heparin (121±34 vs. 36±4 seconds,p=0.02). Pulmonary microvascular fibrin deposition was presentfollowing cardiopulmonary bypass. A pre-operative heparin infusionreduced the extent of pulmonarymicrovascular fibrin deposition (20±11 vs. 44±12 microvascular deposits/mm2 alveolar tissue, p=0.03,Fig. 1). Fibrin deposits typically did not totally occlude the lumen butwere layered on the endothelium forming a circumferential rim. Thefibrin commonly appeared to extend into the blood vessel wall (Fig. 2).Fibrin deposition was also present in small pulmonary arteries andveins. The fibrin deposits were also associated with the endotheliumand were generally small relative to the diameter of the lumen andrarely totally occluded the lumen. Fibrin deposits were particularlymarked at sites of leucocyte margination (Fig. 3A, B). Leucocytesappeared tethered to each other and the endothelium by fibrin strands(Figs. 3C,D). Occasionally, afibrinweb spread across the lumen (Fig. 3E).Within the alveolar space fibrin was also associated with alveolarmacrophages forming early hyaline membranes (Fig. 3F).
The ratio of radial to pulmonary artery blood prothrombin fragmentlevelswas less than1atboth inductionand following sternotomy.At theend of cardiopulmonary bypass the ratio was above 1 (indicatingcoagulation activation in the pulmonary circulation). In the placebogroup this ratio remained above 1 at 1 hour following cardiopulmonarybypass, but fell below1 in the heparin group. Pre-operative heparinwasassociated with a trend to over all lower levels following cardiopulmo-nary bypass (p=0.08, Supplement, Fig. 1).

Fig. 1. A pre-operative heparin infusion reduced pulmonary microvascular fibrindeposition following cardiac surgery. Data shown as mean and standard error.
e28 Letter to the Editors-in-Chief
Discussion
We found pulmonary microvascular fibrin deposition was presentfollowing cardiac surgery. The extent of microvascular fibrin deposi-
Fig. 2. Immunohistochemical staining of fibrin (brown) in lung tissue. Panel A (x 10 magnifiPanel C (x 40magnification) shows thrombi occluding alveolar capillary beds (arrow). Panelforming a circumferential rim (arrow head). Fibrin commonly appeared to extend into the
tion was reduced by additional anti-coagulation with a pre-operativeheparin infusion.
A number of our findings high-light that an inflammatory processunder-lied the development of pulmonary microvascular fibrin deposi-tion. Firstly, the fibrin deposits, typically, formed a layer on theendothelium. This is consistent with activation of the endotheliumgiving rise to tissue factor expression and fibrin deposition. There isdebate regarding which surface of the endothelial cell expresses tissuefactor [6,7]. Our finding that fibrin sometimes extended into themicrovascular wall, suggests the basal surface of the endothelial cellmay be responsible. Secondly, fibrin deposition was not confined to themicrovasculature but was also present on the endothelium of smallpulmonary arteries and veins. In these larger vessels other acuteinflammatory changes were also evident with strands of fibrin formingwhich appeared to tether leucocytes to the endothelium and to otherleucocytes. These features suggest fibrin played a role in leucocyteadhesion to an activated endothelium. Thirdly, the temporal changes inpulmonary prothrombin fragment production indicated that pulmonarycoagulation activation developed following cardiopulmonary bypassandcontinued after theendof surgery. Thisfinding is in keepingwith thedevelopment of an acute inflammatory response. Finally, pre-operativeanti-coagulation with heparin limited the development of pulmonarymicrovascular fibrin deposition. This is consistent with the knownactions of heparin on the endothelium. These actions include increasedendothelial expression of heparan-sulfate, inhibition of tissue factor
cation) and Panel B (x 20 magnification) show fibrin deposition in alveolar capillaries.D (x 40magnification) showsmicrovascular fibrin layered on the capillary endotheliumcapillary wall (black arrow).
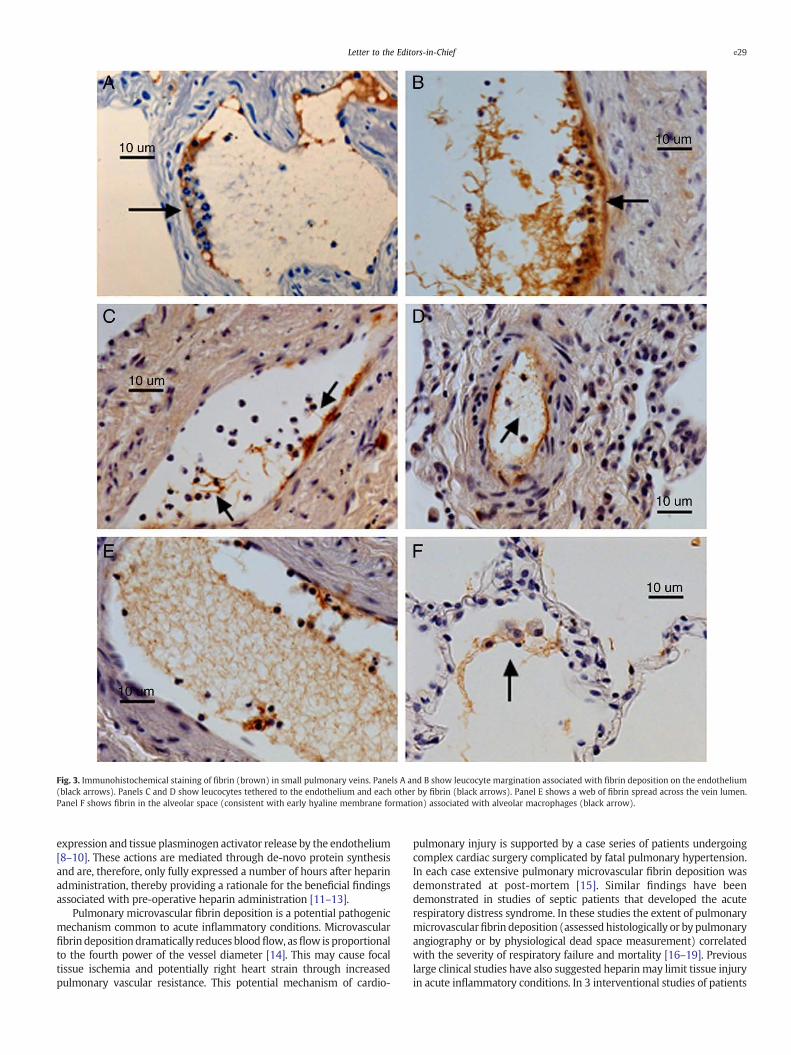
Fig. 3. Immunohistochemical staining of fibrin (brown) in small pulmonary veins. Panels A and B show leucocyte margination associated with fibrin deposition on the endothelium(black arrows). Panels C and D show leucocytes tethered to the endothelium and each other by fibrin (black arrows). Panel E shows a web of fibrin spread across the vein lumen.Panel F shows fibrin in the alveolar space (consistent with early hyaline membrane formation) associated with alveolar macrophages (black arrow).
e29Letter to the Editors-in-Chief
expression and tissue plasminogen activator release by the endothelium[8–10]. These actions are mediated through de-novo protein synthesisand are, therefore, only fully expressed a number of hours after heparinadministration, thereby providing a rationale for the beneficial findingsassociated with pre-operative heparin administration [11–13].
Pulmonary microvascular fibrin deposition is a potential pathogenicmechanism common to acute inflammatory conditions. Microvascularfibrin depositiondramatically reduces bloodflow, asflow is proportionalto the fourth power of the vessel diameter [14]. This may cause focaltissue ischemia and potentially right heart strain through increasedpulmonary vascular resistance. This potential mechanism of cardio-
pulmonary injury is supported by a case series of patients undergoingcomplex cardiac surgery complicated by fatal pulmonary hypertension.In each case extensive pulmonary microvascular fibrin deposition wasdemonstrated at post-mortem [15]. Similar findings have beendemonstrated in studies of septic patients that developed the acuterespiratory distress syndrome. In these studies the extent of pulmonarymicrovascularfibrin deposition (assessedhistologically or by pulmonaryangiography or by physiological dead space measurement) correlatedwith the severity of respiratory failure and mortality [16–19]. Previouslarge clinical studies have also suggested heparinmay limit tissue injuryin acute inflammatory conditions. In 3 interventional studies of patients

e30 Letter to the Editors-in-Chief
with severe sepsis (which assessed activated protein C, tissue factorpathway inhibitor and antithrombin) post-hoc analysis of the placeboarms demonstrated prophylactic heparin administrationwas associatedwith reduced mortality [20–23]. A subsequent prospective randomisedstudy of prophylactic heparin in patients treatedwith activatedprotein Cfor severe sepsis also demonstrated a trend to reducedmortality (28.3 vs.31.9%; p=0.08) [24]. We speculate that reducing microvascular fibrindeposition may be one mechanism by which heparin could limit tissueinjury in these acute inflammatory conditions.
Limitations
All patients were administered aprotinin and thismay have played arole in ourfindings. Aprotinin is a uniqueanti-fibrinolytic agent, becauseit also promotes coagulation activation through inhibition of activatedprotein C and could, therefore, promote more extensive pulmonarymicrovascular fibrin deposition [25–28]. A potential criticism of thisstudy is the small number of patients enrolled. The number enrolledwas, however, based on a priory analysis of previous published data [5].In addition, the potential risks associated with a lung biopsy, takensolely for research purposes, dictated a conservative approach. Finally,the statistical analysis, demonstrated the study had adequate power todemonstrate a significant difference between groups.
Conflict of interest statement
There were no conflicts of interest.
Acknowledgements
We would like to acknowledge and thank the patients whovolunteered to participate in this study. Supported by a grant from theSt.Vincent's Hospital Research Endowment Fund.
Appendix A. Supplementary data
Supplementarydata to this article can be foundonline at doi:10.1016/j.thromres.2010.08.022.
References
[1] Tanaka K. Specific inhibition of thrombin activity during cardiopulmonary bypassreduces ischemia-reperfusion injury of the lung. Hukuoka acta medica Jan2001;92(1):7–20.
[2] Okada K, Fujita T, Minamoto K, et al. Potentiation of endogenous fibrinolysis andrescue from lung ischemia/reperfusion injury in interleukin (IL)-10-reconstitutedIL-10 null mice. J Biol Chem 2000;275(28):21468–76.
[3] Pinsky DJ, Liao H, Lawson CA, et al. Coordinated induction of plasminogen activatorinhibitor-1 (PAI-1) and inhibition of plasminogen activator gene expression byhypoxia promotes pulmonary vascular fibrin deposition. J Clin Invest 1998;102(5):919–28.
[4] Lawson CA, Yan SD, Yan SF, et al. Monocytes and tissue factor promote thrombosisin a murine model of oxygen deprivation. J Clin Invest 1997;99(7):1729–38.
[5] Dixon B, Campbell DJ, Santamaria JD. Elevated pulmonary dead space andcoagulation abnormalities suggest lung microvascular thrombosis in patientsundergoing cardiac surgery. Intensive Care Med Jul 1 2008;34(7):1216–23.
[6] Mulder AB, Hegge-Paping KS, Magielse CP, et al. Tumor necrosis factor alpha-induced endothelial tissue factor is located on the cell surface rather than in thesubendothelial matrix. Blood 1994;84(5):1559–66.
[7] Ryan J, Brett J, Tijburg P, et al. Tumor necrosis factor-induced endothelial tissuefactor is associated with subendothelial matrix vesicles but is not expressed on theapical surface. Blood Aug 15 1992;80(4):966–74.
[8] Olivotti L, Spallarossa P, Piana A, et al. Maximal endothelial tissue plasminogenactivator release is not impaired in patients with acute coronary syndromes beforeheparin treatment. Blood Coagul Fibrinolysis Jun 2001;12(4):261–7.
[9] Cadroy Y, Gaspin D, Dupouy D, et al. Heparin reverses the procoagulant propertiesof stimulated endothelial cells. Thromb Haemost Jan 1996;75(1):190–5.
[10] Gori AM, Pepe G, Attanasio M, et al. Tissue factor reduction and tissue factorpathway inhibitor release after heparin administration. Thromb Haemost 1999;81(4):589–93.
[11] Pepe G, Giusti B, Attanasio M, et al. Tissue factor and plasminogen activatorinhibitor type 2 expression in human stimulated monocytes is inhibited byheparin. Semin Thromb Hemost 1997;23(2):135–41.
[12] Grulich-Henn J, Preissner KT, Muller-Berghaus G. Heparin stimulates fibrinolysisin mesothelial cells by selective induction of tissue-plasminogen activator but notplasminogen activator inhibitor-1 synthesis. Thromb Haemost Dec 30 1990;64(3):420–5.
[13] Marsh NA, Minter AJ, Chesterman CN. The effect of heparin and otherglycosaminoglycans on levels of tissue plasminogen activator and plasminogenactivator inhibitor in cultured human umbilical vein endothelial cells. BloodCoagul Fibrinolysis Jun 1990;1(2):133–8.
[14] Guyton AC, Hall JE. Textbook of Medical Physiology. Ninth ed. Philadelphia: W. B.Saunders; 1996.
[15] Cooper Jr JR, Abrams J, Frazier OH, et al. Fatal pulmonary microthrombi duringsurgical therapy for end-stage heart failure: possible association with antifibri-nolytic therapy. J Thorac Cardiovasc Surg May 2006;131(5):963–8.
[16] Blaisdell FW. Pathophysiology of the respiratory distress syndrome. Arch Surg1974;108(1):44–9.
[17] Greene R, Zapol WM, Snider MT, et al. Early bedside detection of pulmonaryvascular occlusion during acute respiratory failure. Am Rev Respir Dis 1981;124(5):593–601.
[18] Jantsch H. Incidence and prognostic significance of pulmonary artery thromboses inpatientswith acute respiratory failure.WienKlinWochenschr Suppl 1989;179:3–15.
[19] Nuckton TJ, Alonso JA, Kallet RH, et al. Pulmonary dead-space fraction as a riskfactor for death in the acute respiratory distress syndrome. N Engl J Med Apr 252002;346(17):1281–6.
[20] Dixon B. The role of microvascular thrombosis in sepsis. Anaesth Intensive CareOct 2004;32(5):619–29.
[21] Warren BL, Eid A, Singer P, et al. Caring for the critically ill patient. High-doseantithrombin III in severe sepsis: a randomized controlled trial. Jama Oct 172001;286(15):1869–78.
[22] Abraham E, Reinhart K, Opal S, et al. Efficacy and safety of tifacogin (recombinanttissue factor pathway inhibitor) in severe sepsis: a randomized controlled trial.Jama Jul 9 2003;290(2):238–47.
[23] Bernard GR, Vincent JL, Laterre PF, et al. Efficacy and safety of recombinant humanactivated protein C for severe sepsis. N Engl J Med Mar 8 2001;344(10):699–709.
[24] Levi M, Levy M, Williams MD, et al. Prophylactic heparin in patients with severesepsis treated with drotrecogin alfa (activated). Am J Respir Crit Care Med Sep 12007;176(5):483–90.
[25] Taby O, Chabbat J, Steinbuch M. Inhibition of activated protein C by aprotinin andthe use of the insolubilized inhibitor for its purification. Thromb Res Jul 1 1990;59(1):27–35.
[26] Sweeney JD, Blair AJ, Dupuis MP, King TC, Moulton AL. Aprotinin, cardiac surgery,and factor V Leiden. Transfusion Nov-Dec 1997;37(11-12):1173–8.
[27] Alston TA. Procoagulant action of aprotinin. Anesth Analg Jun 1996;82(6):1305–6.[28] Linden MD, Schneider M, Erber WN. Factor V(LEIDEN) and cardiopulmonary
bypass: investigation of haemostatic parameters and the effect of aprotinin usingan ex vivo model. Perfusion Nov 2001;16(6):476–84.
Barry DixonDepartment of Intensive Care, St.Vincent's Hospital,
Melbourne, AustraliaCorresponding author. Intensive Care, St. Vincent's Hospital,Melbourne, Victoria, 3065, Australia. Tel.: +61 3 9288 4488;
fax: +61 3 9288 4487.E-mail address: [email protected].
Kenneth OpeskinGeorgia Stamaratis
Department of Pathology, St.Vincent's Hospital, Melbourne, Australia
Ian NixonMichael Yi
Andrew E. NewcombAlexander Rosalion
Department of Cardiac Surgery, St.Vincent's Hospital,Melbourne, Australia
Yuan ZhangThe University of Melbourne Department of Medicine,
St.Vincent's Hospital, Melbourne, Australia
John D. SantamariaDepartment of Intensive Care, St.Vincent's Hospital,
Melbourne, AustraliaDuncan J. Campbell
St.Vincent's Institute of Medical Research, Melbourne, Australia
5 July 2010