preconception health in nc think tank meeting #3 august 16, 2007
DESCRIPTION
Preconception Health in NC Think Tank Meeting #3 August 16, 2007. What’s UP?. NC Women’s Health Report Card Released National Preconception Clinical Curriculum to be housed on mombaby.org NC Featured on National Webcast – National Association of City and County Health Officials - PowerPoint PPT PresentationTRANSCRIPT
Preconception Health in NC
Think Tank Meeting #3
August 16, 2007

What’s UP?
NC Women’s Health Report Card Released
National Preconception Clinical Curriculum to be housed on mombaby.org
NC Featured on National Webcast – National Association of City and County Health Officials
National Summit on Preconception Health October 29-31 in Oakland, CA 5 presentations/posters from NC

Planning Steps
March 2007 Think Tank Meeting #1• To initiate a focused, collaborative,
comprehensive process to create a state Preconception Action Plan
May 2007 Think Tank Meeting #2• To collect diverse ideas and understand
how preconception fits into existing work
August 2007 Think Tank Meeting #3• To develop the components of the plan
Guiding Principles
• Focus on the whole woman – not only her reproductive capacity.
• Consider the woman’s health needs and related wellness recommendations within the context of her family and community.
• Be careful that messages don’t imply that certain groups of women should not become mothers.
• Be cognizant of health disparities and prioritize programs with potential to close the gaps.
Work should address…
• Clinical practice – continuity of care• Evaluation & research• Integrating new messages into
current campaigns• Policy & advocacy• Holistic view of health• Social marketing• Interconception health
Themes
• Include men & families
• Start early / young• Use existing programs
to carry messages• Build on public health
outreach into worksites, private practice, and communities
• Master tool kit – clear and consistent messages

Potential Target Audiences
• Age (teens, 20s, 30s, 40s)
• Contemplators / Non- Contemplators
• Race/Ethnicity• Gender• Income• Education• Mothers • Geography (13 counties
have most of the excess infant death)
• Families / Couples• Women w/health
conditions• Communities• Health care providers
(OBs, Pediatrics, Family Medicine, Internal Medicine, etc)
• Public health leaders• State opinion leaders• Media• Insurers / Funders• Researchers

The chasm
There is a gap between knowing and doing.
We need to use education and resources – knowledge and mechanisms to narrow that gap and enable women to make positive changes.

Qualitative Data
Data SourcesWhat New Mothers Say: Personal Comments from the North
Carolina PRAMS Survey, NC DHHS SCHS, May 2007
Latina Infant Mortality Awareness Project,NC Healthy Start Foundation, April 2007
Women’s Health: Attitudes and Practices in North Carolina – Focus
Group Research, NC SIM Collaborative/NC Healthy Start Foundation, June 2005
Uncovering Community Voices: A Catalog of Qualitative DataRegarding Women’s Health in North Carolina 1995 – 2005, UNC MCH 315 Spring 2005 Class with Supervision from UNC
ShepsCenter and UNC Center for Maternal and Infant Health

What women say…
• Behavior Change: Awareness not enough to change behaviors. Knowledge of family history, family support and healthcare options can lead to change.
• Stress: Emotional, physical and financial stress negatively influence health. Need more social support and networking.
What women say…
• Mental health issues, especially depression, are significant. Lack of resources in communities.
• Barriers to Health Care: Cost. Racism. Lack of – insurance, access, trust/respect, childcare, and transportation.

What women say…
• Approach to Healthcare: Prefer holistic approach.
• Substance Use: Many women reported
they knew someone struggling with drug addiction. Reported as coping mechanism for extreme stress.
• Most pregnancies are unplanned. Women are concerned about becoming pregnant but don’t use contraception. Inconvenient clinic hours and quality of care problems with family planning services.

Quantitative Data
Obesity and Related Conditions
• 25% of NC Women aged 18 – 44 y.o. are obese BRFSS 2005
• Obesity increases risk for hypertension (13%) and diabetes (2%) BRFSS 2005
• 62% of NC women do not meet minimum recommendations for physical activity
NC Women’s Health Report Card, 2007
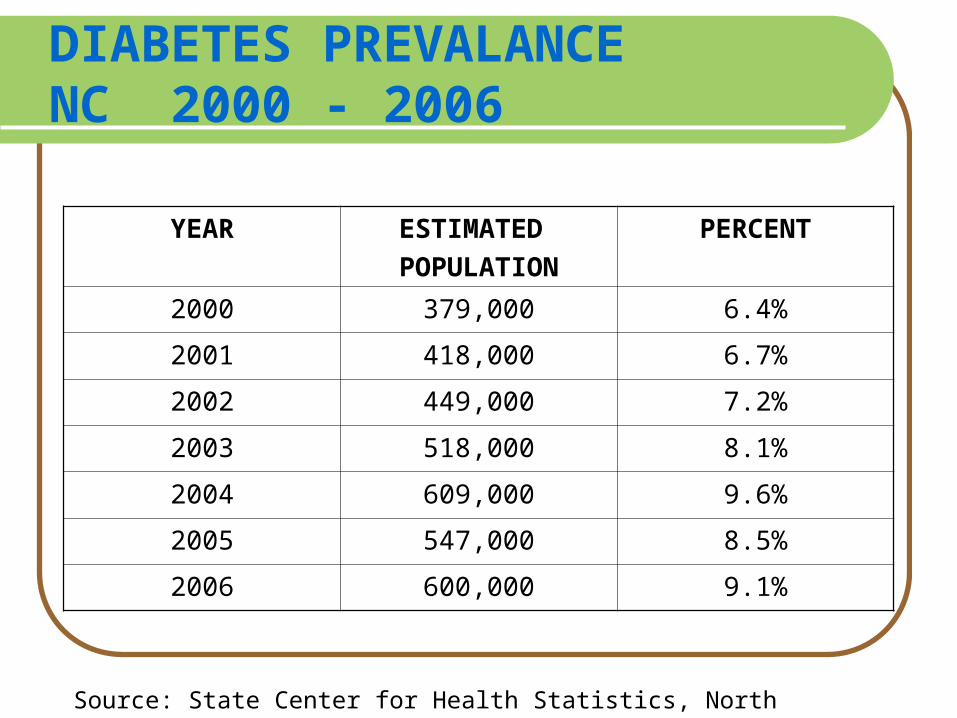
DIABETES PREVALANCE NC 2000 - 2006
YEAR ESTIMATED POPULATION
PERCENT
2000 379,000 6.4%
2001 418,000 6.7%
2002 449,000 7.2%
2003 518,000 8.1%
2004 609,000 9.6%
2005 547,000 8.5%
2006 600,000 9.1%
Source: State Center for Health Statistics, North Carolina
Gestational Diabetes
Occurs only during pregnancy and affects 2-4% of all pregnant women.
Obesity is a risk factor for the development of gestational diabetes.
Women who develop gestational diabetes are at higher risk of developing type 2 diabetes.
Source: ADA. Clinical Practice Recommendations 2005. Diabetes Care 28 (Sup 1): S38. (17)

Complications Associated with Obesity
Obesity is a risk factor in the higher perinatal mortality and morbidity rate found in type 2 diabetes, including congenital malformation and macrosomia. Complications include: Hypertension Obstructive sleep apnea Preeclampsia Increased urinary tract infections Higher rates of cesarean and difficult deliveries
in the mother
Source: Diabetes Care. 1992; 15:1640-57
Impact on Infants
Major congenital malformations remain the leading cause of mortality and serious morbidity in infants of mothers with type 1 and type 2 diabetes.
Observational studies indicate that the risk of malformations increases continuously with maternal glycemia during the first 6-8 weeks of gestation (1st trimester).
Source: ADA. Clinical Practice Recommendations 2005. Diabetes Care 28 (Sup 1): S38. (17)
Substance Use NC Women Aged 18 – 44 years old
24% Use Tobacco
8% Engage in Binge Drinking
7% Engage in Illicit Drug Use*
NC BRFSS 2005*NC Adults aged 12 and older, SAMHSA, National Survey on Drug Abuse and Health, 2005
Substance Use
• Lack of outpatient and inpatient services
• Need for provider training and screening tools
• Need for more NC-specific research

NC Women & Factors Affecting Pregnancy Outcomes
45% of pregnancies are unintended
NC PRAMS 1997 - 2000
62% do not take folic acid daily NC BRFSS 2006
19% may not be rubella immune NC State Lab, prenatal clients, 2006

NC Women and Sickle Cell
• Nationally one in every 12 African Americans has sickle cell trait NIH NHLBI, 2007
• 3,908 newborns born in NC with sickle cell trait in 2006 NC State
Lab

STIs/HIV Case RateNC Women Aged 18 – 44 years old
1320.3/100,000 Chlamydia Case Rate
432.5/100,000 Gonorrhea Case Rate
312.4/100,000 living with HIV/AIDS
8.1/100,000 Syphilis Case Rate (PSEL)
NC DPH, HIV/STD Prevention and Care Branch 2006
Mental Health NC Women Aged 18 – 44 years old
23% Report 1- 8 days of poor mental health
during the past month NC BRFSS, 2005
20% Report being moderately or very depressed in the months after delivery NC PRAMS 2000, 2003
Barriers to Healthcare NC Women - Aged 18 – 44 years old
24% Uninsured
27% No dental visit in the past year
NC BRFSS 2005
Criteria for Areas of Focus
Impact women’s and/or infant health Consistent with CDC Recommendations Based on best available scientific evidence,
including NC data highlighting disparities and needs/gaps
Reflect issues that women have highlighted as important to them
Reflect priorities of participants in previous meetings
Offer concrete opportunities for action BONUS: Impact chronic disease in the future
What Bubbles to the Top?
1) Pregnancy Intendedness2) Substance Use3) Obesity and Related Conditions
4) Mental Health5) Barriers to Healthcare
Questions?
Structure• Leadership Team• Topic Area Groups (Workgroups)
• Collaborate around agreed-upon areas of focus• Will have Chairperson and develop agenda• Collaborate on existing programs, funding
opportunities, develop new programs/advocacy plans, measurement of progress
• Use expertise of researchers and messaging experts as needed
• Preconception Collaborators (project-specific)
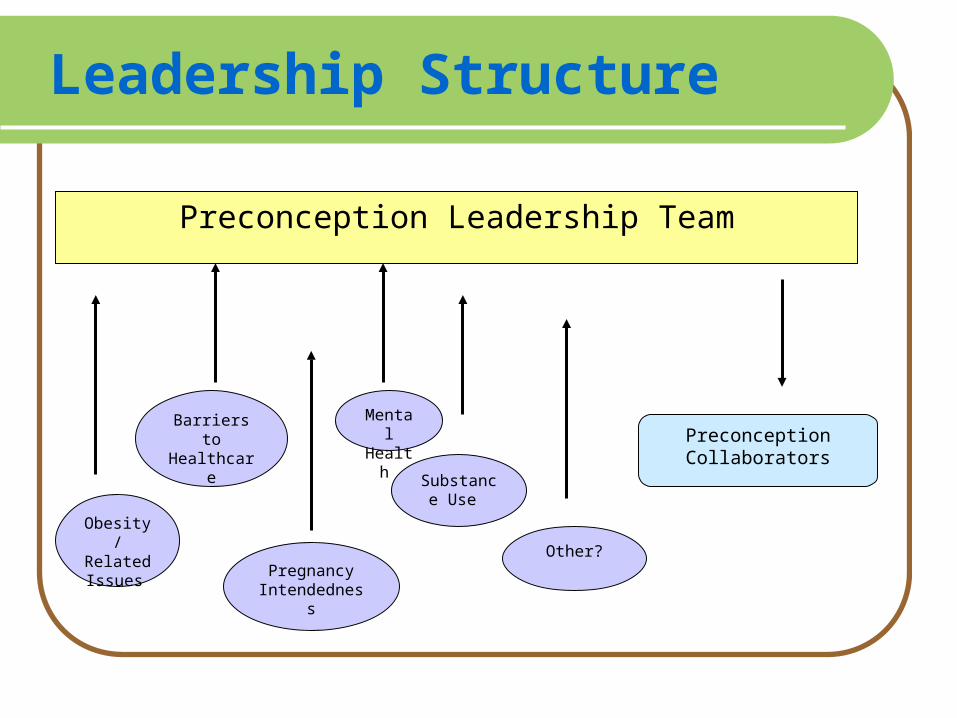
Leadership Structure
Preconception Leadership Team
PreconceptionCollaborators
PregnancyIntendednes
s
Barriers to Healthcare
Obesity /
Related Issues
Mental Health
Substance Use
Other?

The Website
www.mombaby.org• Resources• National News• Minutes• Feedback

Please join us!
• Sign up for the Leadership Team, a workgroup(s), or to provide other support
• Workgroups will meet in Fall 2007• Progress reports from workgroups
to be given at next large-group meeting on December 4 (save the date!)
• NC Preconception Conference: January 23, 2008 (Greenville)