predictors of self- management of type 2 diabetes in first generation u.s.-based mexican americans...
TRANSCRIPT

PREDICTORS OF SELF-MANAGEMENT OF TYPE 2 DIABETES IN FIRST GENERATIONU.S.-BASED MEXICAN AMERICANS AS COMPARED TO RESIDENTS OF MEXICO
PREDICTORS OF SELF-MANAGEMENT OF TYPE 2 DIABETES IN FIRST GENERATIONU.S.-BASED MEXICAN AMERICANS AS COMPARED TO RESIDENTS OF MEXICO
Dr. Chris Latham California State University, Fullerton: LA County-USC Medical Center & Universidad Autónoma de Tlaxcala
PurposePurpose
The aim of both studies was to determine predictors of successful Type 2 diabetes management in a newly diagnosed adult population in the U.S. and Tlaxcala, Mexico using a research-based Hispanic Health Protection Model.

Hispanic Health Protection Theoretical Framework Hispanic Health Protection Theoretical Framework
U.S. and Tlaxcala, MexicoU.S. and Tlaxcala, Mexico
• NINR-funded study of US group of new immigrants from Mexico: Minimal health coverage; 51% female; n =240, Low-acculturation – Bi-cultural approach to health care
• US TIES-funded study of residents in Mexico: 80% female, n = 109, Moderate use of traditional healing
Methodology: SampleMethodology: Sample
Convenience sample of participants from clinics who had newly confirmed diagnoses of Type 2 diabetes
Exclusion criteria included chronic infection(s), diagnosed psychiatric disease or personality disorders, and known substance abuse.

Data Collection ProceduresData Collection ProceduresInformed consent process over three sets of
interviews
Clinic- based questionnaires were conducted in three points in time over 4-6 months
Private interviews in clinic
• Interview #1: At time of diagnosis
• Interview #2: Following education classes
• Interview #3: After 4-6 months after diagnosis
(at home setting in Tlaxcala)
L.A. SettingL.A. Setting
City of Los Angeles: East L.A.
Over 8,200,000
One medical clinic devoted to care of diabetic clients: 2-5 new clients
per
day
Tlaxcala SettingTlaxcala Setting City of Tlaxcala is capital in smallest State
45 miles southeast of Mexico City
1,200,000, with only 7.62% living in Tlaxcala
Tlaxcala has a diverse economic base
163 “Health Centers”: 4 used in this study
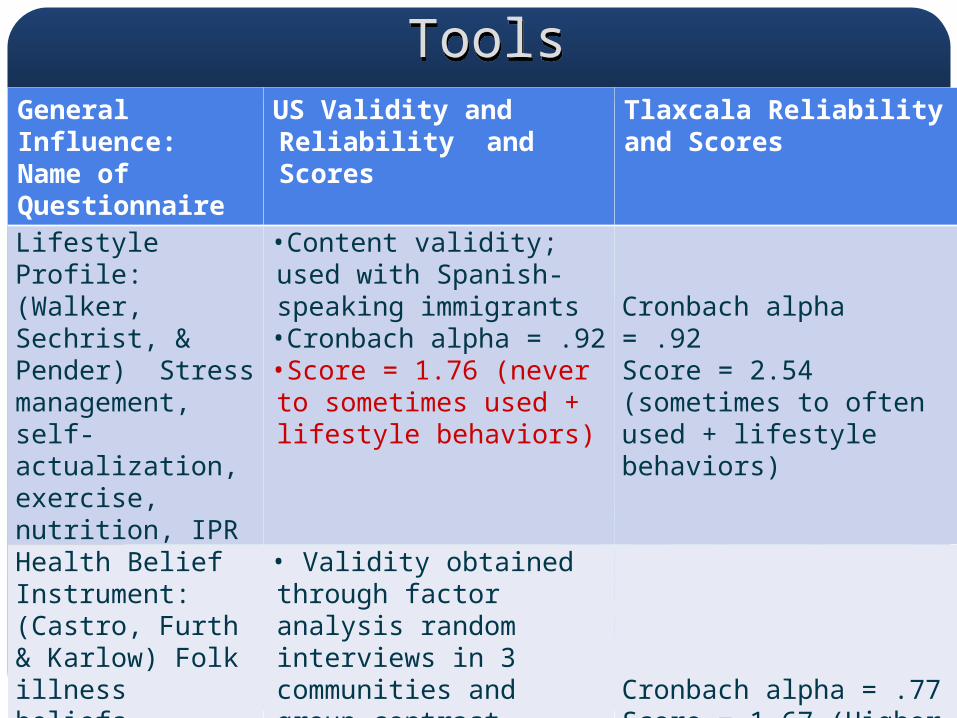
ToolsToolsGeneral Influence:Name of Questionnaire
US Validity and Reliability and Scores
Tlaxcala Reliability and Scores
Lifestyle Profile: (Walker, Sechrist, & Pender) Stress management, self-actualization, exercise, nutrition, IPR
•Content validity; used with Spanish-speaking immigrants•Cronbach alpha = .92•Score = 1.76 (never to sometimes used + lifestyle behaviors)
Cronbach alpha = .92Score = 2.54 (sometimes to often used + lifestyle behaviors)
Health Belief Instrument: (Castro, Furth & Karlow) Folk illness beliefs, personal responsibility for health and control over health
• Validity obtained through factor analysis random interviews in 3 communities and group contrast techniques; •Cronbach alpha = .70•Folk Belief and Lower Control over Health Score = 2.08
Cronbach alpha = .77Score = 1.67 (Higher belief in folk healing & control over health)

Enabling Factors: US Validity and Reliability and Scores
Tlaxcala Reliability and Scores
Patient Satisfaction Instrument (Hinshaw & Atwood) quality of technical, educational, and support by nurses
•Convergent and discriminant validity established across two previous studies; total score Cronbach alpha of .94•Total Score = 3.95 (higher satisfaction with care)
Cronbach alpha = .86Total Score = 3.23 (lower satis)
Perceived Social Support (Prociando & Hiller) (from Family (Fa) and Friends (Fr))
•Discriminant and convergent validity was determined by significant relationships over three studies•Cronbach (Fr)= .87; (Fa)= .91•Friend= 14.14; Family= 15.90; Total Score = 15.02
Cronbach alphas:(Fr) = .90; (Fa) = .81Friend =11.06;Family = 15.06Total Score = 13.06 (lower social support)
Diabetes Self-Efficacy Scale (Crabtree) Ability to carry out DM regimen
•Content validity and factor analysis • Cronbach alpha = .89•Total Score = 4.32 (problems with DM)
Cronbach alpha = .88Total Score = 2.74 (able to handle DM)

HHPM Outcomes: US Validity and Reliability and Scores
Tlaxcala Reliability and Scores
BMI T1 and T2
1st interview 33.47Range = 19.00- 41.02
3rd interview 31.85Range = 19.59-39.20
1st interview 26.67, Range= 19.53 - 38.29 3rd interview 26.36, Range = 19.53 -38.31
HbA1c T1 and T2
1st interview 12.04 (s.d.= 4.32)Range = 5.2-22.3
3rd interview 9.21 (s.d.=3.06)Range 4.9 – 20.2
1st interview 7.74 (s.d.=0.171) Range =4.40 –16.363rd interview 7.33 (s.d=1.43) Range = 4.80-10.60
Diabetes Knowledge Test (Baker, Vallborn & Pavlik)
•Content validity •Cronbach alpha of .94•Total Score = 42.4
Cronbach alpha = .83
Total Score = 30.55Diabetes Quality of Life Measure: Self-Satisfaction and Impact of Diabetes (Jacobson, Barofsky, Cleary & Rand)
•Previous content validity & field testing with 192 patients with Type 1 diabetes•Cronbach alphas = .89 -.79
Self-satisfaction Score = 1.86Impact of DM Score = 1.92
Cronbach alphas: Self-satisfaction = .83; Impact of Diabetes = .78Self-satisfaction Score = 2.42Impact of Diabetes Score = 2.68
Findings: Description of SampleFindings: Description of SampleResidence: 56% of participants lived in the City of
Tlaxcala; others in surrounding areas;100% of L.A. participants lived in an urban
area
Education:Tlaxcala: 30.3% had 1-6 years of formal
education; 95.4% had up to 9 years; 51% of U.S. sample had 1-6 yrs of formal
education with an additional 49% between 7-12 years.
Findings: Description of SampleFindings: Description of SampleHealth Care Coverage: Tlaxcala: Most had Seguro Popular and
Secretary of Health coverageU.S. only 1.3% (n=3) private/HMO health care
coverage. 10.8% (n=26) indicated having either Medi-cal or Medicare coverage.
Other Characteristics:
Similar in age(41.3 yrs)
Findings: Description of SampleFindings: Description of Sample
Employment: Tlaxcala: 32% work full-time; 22% work
part-time; 6% unemployed; 36.7% either retired or disabled. 13.8% (n=15) were enrolled as students
U.S.: 35.8% full-time, 28.3% part-time and 29.6% unemployed.Of the unemployed, some reported being retired (15.8%), disabled (15.4%), or attending school (30.4%).

Findings: Description of SampleFindings: Description of Sample
Alternative Health Care:
Tlaxcala: 24.8% used a herbalist folk
healer/masseuse; 59% used medical doctors, 27% used dentists; 12% used a nutritionist (37% believed that herbal teas could cure illness)
U.S.: Low Acculturation Levels: Almost two-thirds reported reading or speaking only Spanish, while 74.6% reported thinking in Spanish; many used herbs and teas to treat illness
Findings: Description of Sample(s)Findings: Description of Sample(s)
Rating of health: Tlaxcala: 92% of respondents indicated a
“fair-good” rating of their health as compared to others.
U.S.: 89% of respondents rated their health as “fair-good.”
Statistical AnalysesStatistical Analyses
Correlation matrices, confirmed the absence of multicollinearity between the final model variables
Durbin-Watson (2.44) and VIF stats (1.045 – 1.209)
Goodness of Fit and the Comparative Fit Index = .95-1.0

Statistical Analyses (continued)Statistical Analyses (continued)
Path analyses and structural models using AMOS 16.0 with most likelihood estimation was completed
Parsimonious, best-fitting models were completed by deletion of non-significant paths (p<.05) and without significantly increasing Chi Square
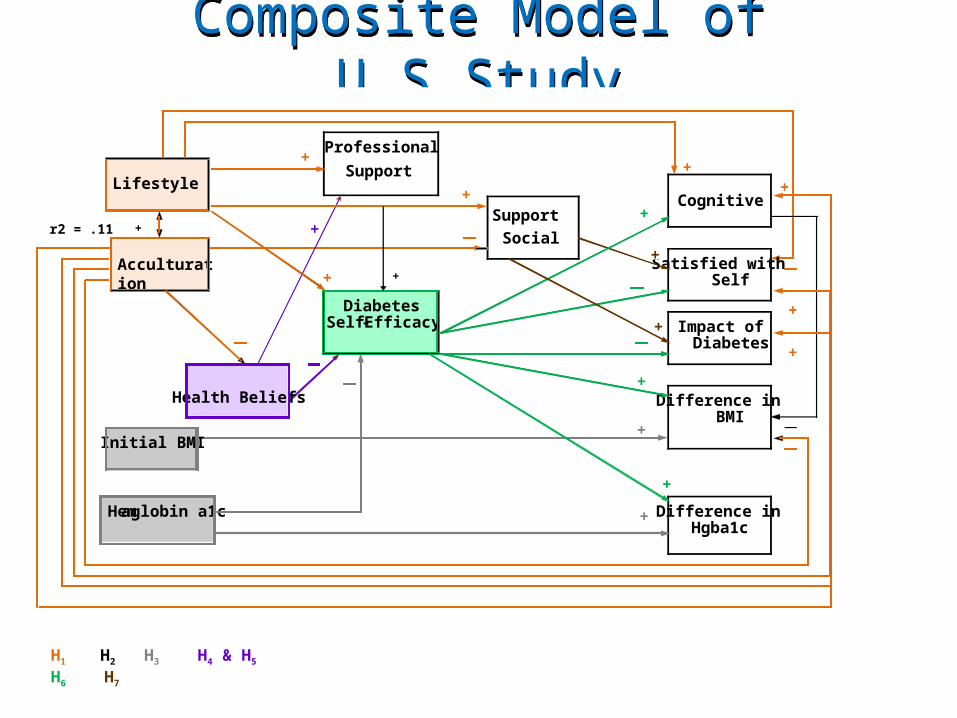
Composite Model of U.S.StudyComposite Model of U.S.Study
Professional
Support
Cognitive
+
Diabetes Self - Efficacy
Satisfied with Self
Impact of Diabetes
Difference in BMI
Difference in Hgba1c
Lifestyle
Acculturation
Initial BMI
Hemaglobin a1c
Health Beliefs
Support
Social
+ +
+
r2 = .11
+
+
+ +
+
+
+
+
+
+
+
+
+
H1 H2 H3 H4 & H5 H6 H7
Figure 1. Composite U.S. Hispanic Health Protection Model (© Latham & Calvillo, 2008)
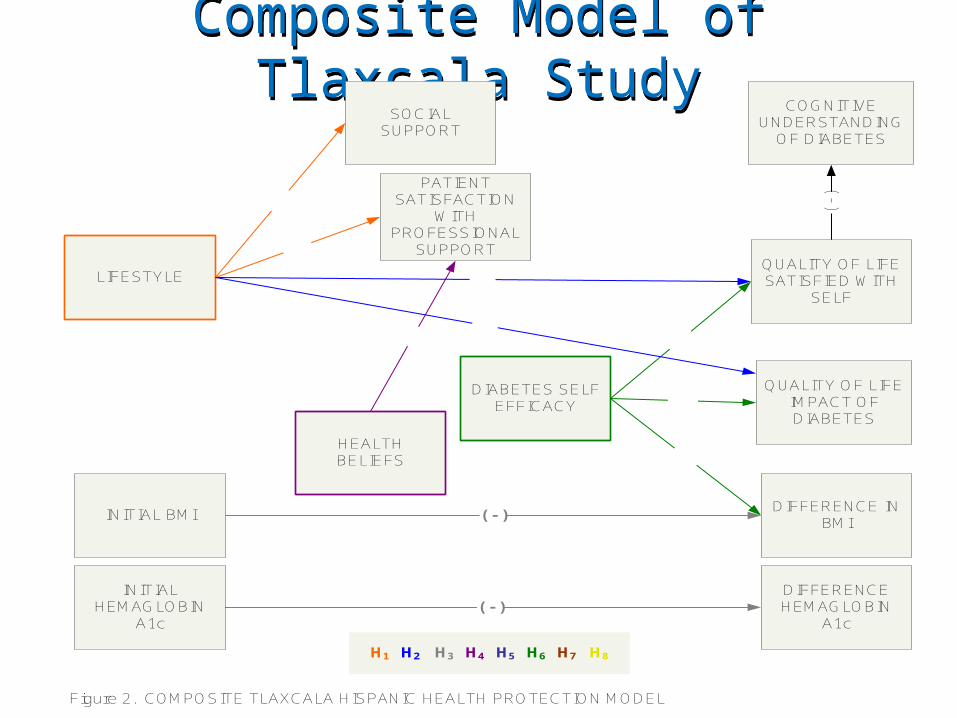
Composite Model of Tlaxcala StudyComposite Model of Tlaxcala Study
LIFESTYLE
PATIENT SATISFACTION
WITH PROFESSIONAL
SUPPORT
SOCIAL SUPPORT
DIABETES SELF EFFICACY
HEALTH BELIEFS
COGNITIVEUNDERSTANDING
OF DIABETES
INITIAL BMIDIFFERENCE IN
BMI( - )
( - )
QUALITY OF LIFESATISFIED WITH
SELF
QUALITY OF LIFEIMPACT OF DIABETES
( - )INITIAL
HEMAGLOBIN A1c
DIFFERENCE HEMAGLOBIN
A1c
Figure 2. COMPOSITE TLAXCALA HISPANIC HEALTH PROTECTION MODEL
H1 H2 H3 H4 H5 H6 H7 H8

DiscussionDiscussion
Pre-morbid lifestyles and self efficacy about performing diabetes self-care are important determinants of outcomes.
Pre-morbid lifestyles slightly affect perceptions of professional and social support and have a negative influence on subsequent psychological effects of diabetes (QOL).
Other research: Changing lifestyle is not a priority and cultural beliefs about family needs over individual needs decreases emphasis of D.M. regimen. (Lopez-Amador and Ocampo-Barrio, 2007)
Discussion (continued)Discussion (continued)Following nurse-provided classes on
diabetes, satisfaction with health care providers had high scores in US and low scores in Mexico
Social support received low scores with both groups
Diabetes knowledge tests had extremely low scores in both the U.S. and Tlaxcala
Discussion (continued)Discussion (continued)Health beliefs based in culture, including use
of folklore and alternative medicines and an internal locus of control over health seem to negatively influence perceptions of health care providers in Mexico and positively influenced perceptions in the U.S.
Other research: D.M. patients report “lack of a voice” in shared decision making with health care providers, even when patients seek professional help. (Garcia et al., 2007)

Discussion (continued)Discussion (continued)Low social support from friends and family
lacked influence on subsequent outcome variables
Other research:Family difficulties with communication or
knowing how to help has been reported. (Castillo-Sanchez, Castaneda-Sanchez, & Marua-Ramirez, 2008)
Family non-acceptance of diabetic needs isolates diabetics and creates feelings of loneliness and being different. (Garcia et al., 2007)
Discussion (continued)Discussion (continued)Role of health beliefs, folklore, and
misconceptions about diabetes
Other research: (Garcia et al., 2007; Munoz-Regna, Ocampo-Barrio, & Quiroz-Perez, 2007)
Psychological support to accept diabetesIncremental information about diabetes and
recommended changesRigid vs. flexible diabetic lifestyle adherence
Practice ImplicationsPractice Implications
Public health focus on prevention related to chronic disease decompensation
Improve clarity of role of professional and friend/family involvement with diabetic family members
Evaluate psychological status and provide support
Assess lifestyle and self efficacy

Practice Implications (continued)Practice Implications (continued)
Inclusion of culturally relevant health education
Evaluate the breadth and depth of diabetes education and provide follow-up
Monitoring diabetes control – how is it accomplished?
Education ImplicationsEducation ImplicationsPublicize health implications of lifestyleImprove focus on health promotion &
disease prevention Public health: Media and policyCommunity and Neighborhood planningSchool and Workplace targets for
educationTrain the trainerNutrition: Influence school and work Increase time of formal education/support

Research ImplicationsResearch ImplicationsTheoretical model emphasizes a
comprehensive outcome approach:oquality of lifeounderstanding of diabetes and self-
care Utilize social supportPatient satisfaction with health care
providers needs additional workInfluence of health beliefs in relation to
the provision of health care & outcomes

Tlaxcala Faculty ParticipantsTlaxcala Faculty Participants

Company
LOGO
California State University, [email protected]
California State University, [email protected]
PREDICTORS OF SELF-MANAGEMENT OF TYPE 2
DIABETES IN FIRST GENERATION
U.S.-BASED MEXICAN AMERICANS AS COMPARED TO RESIDENTS OF MEXICO