pregnancy and lung dr shital patil
DESCRIPTION
Pregnancy has undergo physiological adaptations in mother to meet the requirements of growing fetus. Bronchial Asthma, Pulmonary Tuberculosis, Bacterial and Viral Pneumonias, Sleep disorders, DVT, LAM and other disorders are adequately covered.TRANSCRIPT
Pregnancy and Lung
Dr. Patil Shital, MD Resp.Med. DCH Asst. Prof & HeadDept. of Pulmonary MedicineMIMSR Medical College Latur India
Introduction
The respiratory system undergoes a number of changes during pregnancy to meet the metabolic needs of both the mother and the fetus.
Many acute and chronic pulmonary disorders are encountered during pregnancy ,most common being asthma, which affects up to 4 percent of women.
Physiologic adaptations to pregnancy
Anatomic changes- upper airway-hyperemia and
glandular hyperactivity are observed in pregnancy and are associated with edema and friability.
These changes are result of the expansion of plasma volume and indirect effect of the elevated levels of estrogens.
Up to 30% of pregnant women suffer from nasal congestion and epistaxis.
This condition is known as “gestational rhinitis” and usually resolves very quickly after delivery.
The higher propensity to snoring in pregnancy as compared to the non-pregnant population is related to these changes.
Mucosal edema of the upper airway associated with difficulties in airway management and failed or difficult endotracheal intubations.
Small endotracheal tubes, such as 6.0 mm or less, may be advised for nasotracheal intubations.
Changes in the chest wall
The lower ribcage widens, leading to an increase in the anteroposterior and transverse diameters of the chest by 2 cm each , resulting in an overall increase of 5–7 cm in the chest wall circumference.
Subcostal angle widening from 68.50 to 103.50 (about 30% change)
Gravid uterus causes upward displacement of diaphragm by 4 cm but this is compensated by increased diameter of chest.
Improved diaphragm mechanics in pregnancy is explained by increased area of opposition of diaphragm to the rib cage.
Relaxin hormone responsible for relaxation of pelvic ligaments also causes relaxation of lower rib cage ligaments.
Impaired chest wall compliance related
to the enlarging uterus can occur late in
pregnancy, causing decreased total
lung compliance.
Respiratory muscles-
No significant respiratory muscle change during pregnancy despite upward displacement of diaphragm and changes in chest wall configuration.
Diaphragm excursion increased by 2 cm as compared with non-pregnant state.
Preserved muscle strength with increased excursion of diaphragm are important adaptations for increase in tidal volume (TV) and minute ventilation (MV) that occurs in pregnancy
Physiologic measurements in pregnancy
The major effect of pregnancy on lung physiology occurs on volumes.
There is an increase in tidal volume (TV) and a reduction in functional residual capacity (FRC) 10 to 25% secondary to a decreased residual volume 7 to 22% and expiratory reserve volume 8 to 40% .
FRC is further reduced in the supine position late in gestation.
The inspiratory capacity is increased so that total lung capacity remains the same in the pregnant and nonpregnant state
Ventilation
Minute ventilation, a product of tidal volume and respiratory rate, is increased by about 40% in pregnancy which is proportional to increase in tidal volume from 500 mLto700 mL (about 40%).
Minimal change in the respiratory rate in pregnancy and any change should be interpreted as pathologic rather than physiologic.
This increase in ventilation leads to a reduction in PaCO2 levels from 35–40 mmHg in the pre-pregnant state to an average of 30 mmHg during pregnancy.
The drop in PaCO2 is matched by an increased renal excretion of bicarbonate, leading to lower plasma bicarbonate levels.
Plasma pH that is not significantly changed but there may be less buffering capacity in the face of an acidosis.
Oxygenation
Maternal PaO2 increases in pregnancy to 100–105 mmHg at sea level.
This increase is in part secondary to an increment in cardiac output leading to an improvement in ventilation/ perfusion matching in the upper lobes.
Oxygen consumption is increased in pregnancy by about 20% and increases further during labor and delivery
The alveolar–arterial gradient (the difference between PO2 in the alveoli and that measured in the arterial blood) has been reported to increase slightly in the late stages of pregnancy from 15 to about 20.
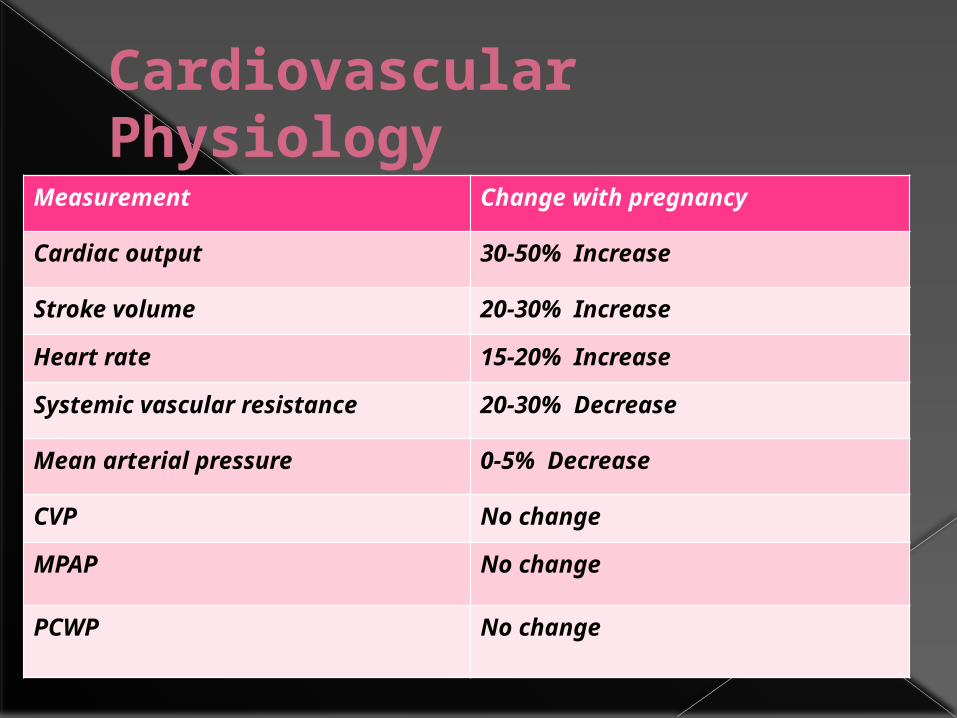
Cardiovascular Physiology
Measurement Change with pregnancy
Cardiac output 30-50% Increase
Stroke volume 20-30% Increase
Heart rate 15-20% Increase
Systemic vascular resistance 20-30% Decrease
Mean arterial pressure 0-5% Decrease
CVP No change
MPAP No change
PCWP No change
Total blood and plasma volume increases up to 35 to 50% of normal, peaking in the mid-third trimester with a lesser increase in RBC volume (approximately 20 to 40%).
This result in hemodilution with a relative decrease in hemoglobin, hematocrit (approximately a 12% decrease), and relative RBC volume “the anemia of pregnancy.”
Breathlessness in pregnancy
Approximately 50% of normal pregnant women will note dyspnea before 19 weeks gestation and 76% by 31 weeks.
Reasons for experiencing the sensation -The effect of progesterone on the
respiratory center -Mechanical changes associated with
weight gain or decreased venous return -and/or the demands of the fetus.
Progesterone lowers the threshold and increases the sensitivity of the respiratory center to CO2.
It is also possible that progesterone acts as a primary stimulant to the respiratory center independently of any change in CO2 sensitivity or threshold.
Women often describe their symptoms as “needing to take a deep breath.”
Physical exam is normal and oxygen saturation is normal at rest and with exertion.
The presence of an anemia should be sought as this is common in pregnancy.
If there is no underlying disease as a cause of dyspnea, the patient can be reassured that there is no increased risk for complications during pregnancy or labor and delivery.
Asthma in Pregnancy
Asthma is common in young women and therefore is seen frequently during pregnancy.
Kwon and associates (2006) estimated asthma prevalence during pregnancy to range between 4 and 8 percent.
Moreover, Namazy and Schatz (2005) reported that the prevalence in pregnant women appears to be increasing.
Effects of Pregnancy on Asthma
The course of asthma is usually unpredictable in pregnancy and numerous studies have suggested that one-third of patients improve, one-third remain the same and the last third worsen.
Factors contributing to improvement may be the pregnancy associated
-rise in serum cortisol, an anti-inflammatory hormone, or
-the increase in progesterone which acts as a potent smooth muscle relaxant
Epidemiologic studies suggest that asthma
exacerbations are most common between
gestation weeks 17–24 and symptoms worsen mostly between 29 and 32
weeks.
There is usually an improvement in symptoms after 36 weeks. It is possible that this improvement late in the pregnancy is related to cortisol levels at term reaching four times pre-pregnancy levels.
factors that predispose to worsening of asthma during pregnancy
clear evidence linking upper airway and nasal symptoms and asthma control.
The course of asthma seems to parallel that of gestational rhinitis and those patients who have an improvement in their symptoms of rhinitis during pregnancy also have improvements in their asthma symptoms
The rate of bacterial sinusitis is 5–6 times higher in pregnant women and may contribute to worsening of asthma symptoms.
Gastroesophageal reflux disease (GERD), common in pregnancy, may also play a role in worsening asthma control during pregnancy
premenstrual asthma
Many studies of premenstrual asthma that suggest changes in beta-agonist receptor density in the airways that occur during the menstrual cycle.
Declines in FEV1 have been shown to occur in the luteal phase in women with premenstrual exacerbations of their symptoms.
Emergency room visits are more frequent in the premenstrual period than in the pre-, peri- or postovulatory periods of the menstrual cycle.
presence of premenstrual asthma does not necessarily suggest that asthma will worsen during pregnancy.
Effect of asthma on pregnancy
well-controlled pregnant asthmatics do not have a significantly higher rate of adverse outcomes than women without asthma.
Suboptimal control appears to be associated with low birth weight, preterm delivery, intrauterine growth restriction, and cesarean section.
Pre-eclampsia has also been associated with severe asthma in some studies, but it is unclear whether it is the underlying disease or the concomitant use of systemic steroids may have a confounding effect.
Case–control studies have shown that Of
37,000 women with asthma and 2495
exacerbations, those with exacerbations were more likely to have miscarriage or therapeutic abortions than those without.
Clinical Evaluation
The subjective severity of asthma frequently does not correlate with objective measures of airway function or ventilation.
Useful clinical signs include labored breathing, tachycardia, pulsus paradoxus, prolonged expiration, and use of accessory muscles.
Signs of a potentially fatal attack include central cyanosis and altered consciousness.
Pulmonary function testing should be routine in the management of chronic and acute asthma.
Sequential measurement of the FEV1 or the peak expiratory flow rate,PEFR are the best measures of severity.
An FEV1 less than 1 L, or less than 20 percent of predicted value, correlates with severe disease defined by hypoxia, poor response to therapy, and a high relapse rate.
The PEFR measured reliably with inexpensive portable meters.
Each woman determines her own baseline when asymptomatic—personal best—to compare with values when symptomatic.
Brancazio and associates showed that the PEFR did not change during the course of pregnancy in normal women.
In general, women with moderate to severe asthma should measure and record either their FEV1 or PEFR twice daily.
The FEV1 ideally is >80 percent of predicted.
For PEFR, predicted values range from 380 to 550 L/min.
Each woman has her own baseline value, and therapeutic adjustments can be made using this.
Management
The first step in management is establishing the diagnosis of asthma
Pregnant asthmatic patients should be asked about food allergy, aspirin sensitivity, rhinitis and sinusitis, GERD, exercise- or cold-induced asthma, and nocturnal asthma.
Many patients are misdiagnosed with asthma for many years before they are correctly diagnosed with asthma mimics such as chronic obstructive lung disease, sinus disease or vocal cord dysfunction.
management guidelines
Patient education—general asthma management and its effect on pregnancy.
Environmental precipitating factors—avoidance or control.
Objective assessment of pulmonary function and fetal well-being—monitor with PEFR or FEV1.
Pharmacological therapy— appropriate combinations and doses to provide baseline control and treat exacerbations
Compliance and proper use of medications is another major issue in patients with asthma as poor asthma control results in many cases from inadequate use of the drugs.
US Food and Drug Administration DrugClassification
category A drug – controlled studies show no risk
category B drug – no evidence of risk in humans
but controlled drug studies have not been performed in pregnant women in first trimester and in later months show no risk to fetus.
category C – risk can not be ruled out. studies in animals have
revealed adverse effects on the fetus, including teratogenicity, and there are no controlled studies in women.
These drugs can be used if the potential benefit of the drug outweighs the potential risk to the fetus
category D – positive evidence of risk. studies have shown positive
evidence of human fetal risks, but in certain situations, these drugs may be of benefit if the risk is outweighed by potential gain.
Category X agents –contraindicated in pregnancy
studies in animals or humans have demonstrated fetal abnormalities and/or there is evidence of fetal risks based on human experience and clearly the risk outweighs the benefit of the drug (eg, thalidomide).
Other than budesonide (category B), all other inhaled corticosteroids are category C agents.
Systemic corticosteroids (category C) can also be used for control of severe and acute exacerbations of asthma.
Salmeterol has not been well studied in pregnancy and is listed as category C.
Short-acting selective β2-agonists are indicated for intermittent (well-controlled) asthma are category C.
Montelukast and zafirlukast can be used in patients demonstrating a previous response to these agents. Both are listed as category B agents.
Zileuton (category C) has been associated with teratogenicity in animals and should be avoided.
Theophylline (category C) has been used safely in pregnancy
Omalizumab, an IgE inhibitor,category B and can be considered for improved control of poorly controlled asthma.
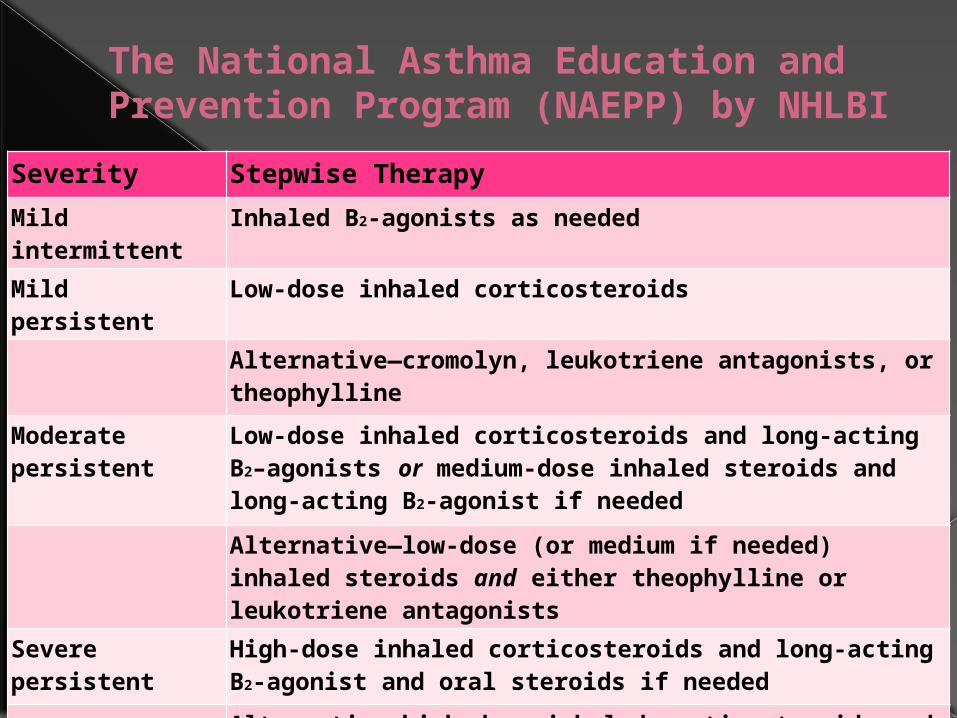
The National Asthma Education and Prevention Program (NAEPP) by NHLBI
Severity Stepwise Therapy
Mild intermittent
Inhaled B2-agonists as needed
Mild persistent Low-dose inhaled corticosteroids
Alternative—cromolyn, leukotriene antagonists, or theophylline
Moderate persistent
Low-dose inhaled corticosteroids and long-acting B2–agonists or medium-dose inhaled steroids and long-acting B2-agonist if needed
Alternative—low-dose (or medium if needed) inhaled steroids and either theophylline or leukotriene antagonists
Severe persistent
High-dose inhaled corticosteroids and long-acting B2-agonist and oral steroids if needed
Alternative—high-dose inhaled corticosteroids and theophylline and oral steroids
GINA 2011 guidelines-
For most medications used to treat asthma there is little evidence to suggest an increased risk to fetus.
Appropriately monitored use of theophylline, ICS, B2-agonist and leucotriene modifier is not associated with increased incidence of fetal abnormalities.
ICS have been shown to prevent exacerbation of asthma during pregnancy.
Focus of asthma t/t must remain on control of asthma symptoms and lung function.
Acute exacerbations should be treated aggressively in order to avoid fetal hypoxia . Treatment should include nebulised rapid acting B2 agonist, Oxygen and systemic corticosteroids .
Labor and Delivery
Maintenance medications are continued through delivery.
Stress-dose corticosteroids are administered to any woman given systemic steroid therapy within the preceding 4 weeks.
The usual dose is 100 mg of hydrocortisone given intravenously every 8 hours during labor and for 24 hours after delivery.
Tuberculosis in pregnancy
Of all the TB deaths in women, 80% occur during the childbearing years.
Because of its significant impact on pregnant women and their children, TB is targeted in Millennium Development Goals 4 and 5 to reduce childhood mortality and improve maternal health.
The prognosis of TB in pregnant women has been debated. At one time, it was thought that TB had an increased incidence of dissemination in the pregnant woman.
Most data support that there is no difference
in the susceptibility to infection, course of disease, obstetrical outcome, prognosis, and
incidence of TB in nonpregnant or pregnant women unless immunosuppression coexists.
Active pulmonary tuberculosis was associated with increased incidences of preterm delivery, low-birth weight and growth-restricted infants, and perinatal mortality.
Twofold increased rates of low-birth weight and preterm infants as well as preeclampsia.
The perinatal mortality rate was increased almost tenfold.
Adverse outcomes correlate with late diagnosis, incomplete or irregular treatment, and advanced pulmonary lesions.
TREATMENT-
Treatment of active TB in pregnancy is similar to that of treatment in the nonpregnant individual.
Drugs approved in pregnant patients include isoniazid (INH), rifampin, and ethambutol.
These drugs all cross the placenta but have not been shown to have teratogenic effects.
In general, pyrazinamide, streptomycin, and ethionamide should be avoided in pregnancy.
Pyrazinamide has been avoided traditionally in the United States , but it is used routinely by the World Health Organization and the International Union Against Tuberculosis and Lung Disease.
standard treatment for active TB should include INH, rifampin, and ethambutol for 9 months because the regimen does not contain pyrazinamide.
(BTS Guidelines for TB
in ANC)
WHO guidelines 2010- TB treatment in pregnancy
With the exception of streptomycin, the first line anti-TB drugs are safe for use in pregnancy: streptomycin is ototoxic to the fetus and should not be used during pregnancy.
The 6-month regimen based upon isoniazid, rifampicin ,ethambutol and pyrazinamide should be used
Although detailed teratogenicity data are not available, pyrazinamide can probably be used safely during pregnancy
Pyridoxine supplementation is recommended for all pregnant or breastfeeding women taking isoniazid
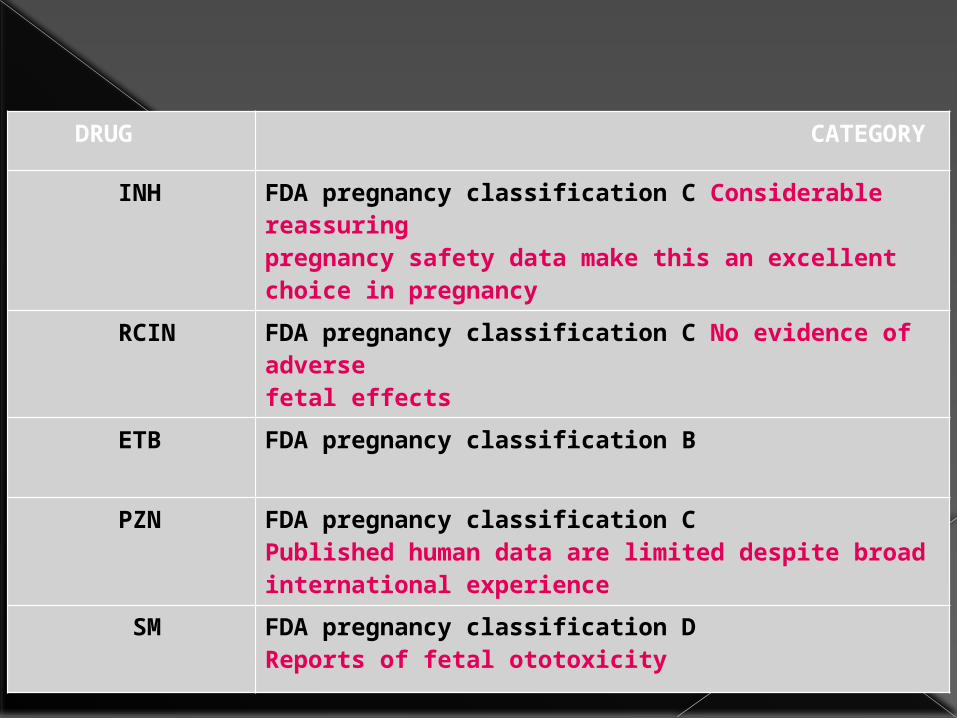
DRUG CATEGORY
INH FDA pregnancy classification C Considerable reassuringpregnancy safety data make this an excellent choice in pregnancy
RCIN FDA pregnancy classification C No evidence of adversefetal effects
ETB FDA pregnancy classification B
PZN FDA pregnancy classification CPublished human data are limited despite broadinternational experience
SM FDA pregnancy classification DReports of fetal ototoxicity
ATT during Lactation
AAP considers use of all First Line and Second Line drugs like Kanamycin, Cycloseriene compatible with breastfeeding.
MDR TB during Pregnancy
All women of childbearing age who are receiving MDR-TB therapy should be advised to use birth control measures because of the potential risk to both mother and foetus.
Evaluation-
Risks and benefits of MDR-TB treatment Severity of the MDR-TB Gestational age Potential risk to the foetus
Management of MDR-TB patients who are pregnant prior to initiation of Cat IV treatment or whilst on Cat IV treatment are based on the duration of pregnancy.
Duration of pregnancy is <20 weeks
Advised to opt for a Medical Termination of Pregnancy (MTP) in view of the potential severe risk to both the mother and foetus
Unwilling for MTP- Start modified Cat IV
modified Cat IV
≤ 12 weeks – Omit Kanamycin and Ethionamide; add PAS
>12 wks – Omit Kanamycin only ; add PAS
Replace PAS with Kanamycin after delivery and continue till end of IP
Pregnancy of >20 weeks
Start modified Cat IV Omit Kanamycin; Add PAS till
delivery Replace PAS with Kanamycin after
delivery and continue till the end of IP
Pregnant MDR-TB patients need to be monitored carefully both in relation to the Cat IV treatment and the progress of the pregnancy
Breast-feeding should be encouraged as long as the patient is sputum negative.
ACUTE RESPIRATORY DISTRESS INPREGNANCY
Preexistent cardiac and pulmonary disorders may be aggravated by pregnancy.
Several conditions that develop during or are specific for pregnancy need to be considered in evaluating acute respiratory distress during pregnancy.
Differential Diagnosis of Acute Respiratory Distress in Pregnancy
Venous thromboembolism Amniotic fluid embolism Pulmonary edema secondary to preeclampsia Tocolytic pulmonary edema Aspiration pneumonitis Peripartum cardiomyopathy Pneumomediastinum Air embolism Other: asthma, pneumonia, cardiac disease,
ARDS
clinical evaluation of acute respiratory distress in pregnancy is to r/o preexistent heart and/or lung disease
Detailed history to characterize precipitating and associated events
Knowledge of infectious complications commonly encountered in pregnancy
Meticulous examination of the patient and chest radiograph for findings consistent with cardiogenic cause.
Pneumonia
Pneumonia and influenza combined are the seventh leading cause of mortality in the United States and the most common cause of death from an infectious disease.
Pregnancy is associated with reduction in cell-mediated immunity and this may explain the increased risk of severe pneumonia and disseminated disease from atypical pathogens.
Other anatomic and physiologic changes of pregnancy that may add to the vulnerability of the lung to injury during infection.
Physiological and Immunological alterations leading to increased risk of pneumonia are-
Immunological- -decreased CD4 T-Helper cell count -decreased cytotoxic T-cell mediated cytotoxicity -decreased lymphocyte proliferation
responce
Physiological changes-
-Elevation of diaphragm -Increased Lung water -Increase in Oxygen consumption -Aspiration more likely during labor and
delivery
Bacterial and atypical pneumonia
Etiology is similar to the nonpregnant population.
Streptococcus pneumoniae is the most commonly isolated organism.
Other causes of pneumonia - Staph. aureus, H.influenzae,
Legionella spp, Mycoplasma pneumoniae, Chlamydia and viruses.
Signs and symptoms of pneumonia in pregnancy are similar to those in nonpregnant individuals.
Symptoms -cough, sputum production, chills, rigors, dyspnea and pleuritic chest pain, & nonrespiratory symptoms such as vomiting, abdominal pain and fever may also occur.
Mothers who develop pneumonia are more likely to have co-existing medical problems including asthma, drug abuse, anemia and HIV infection.
The use of corticosteroids for enhancement of fetal lung maturity and tocolytic agents has also been associated with antepartum pneumonia
Diagnosis
To confirm the diagnosis, assess severity of illness and presence of complications such as pleural effusion or multilobar disease, a chest radiograph should be performed with abdominal shield in all patients suspected to have pneumonia.
Radiation risk during pregnancy
Diagnostic radiological studies rarely exceeds 10-rads (0.1Gy) exposure as of abdomen and pelvis, & threshold for congenital malformations or miscarriage is more than 20-rads(0.2Gy)
Additional risk of 10-rads exposure for pregnancy loss , major congenital malformations, mental retardation, ,stillbirth , infertility is Zero percent.
(0.1 rad-1.0 mGy or 1 rad-0.01Gy)
A chest X-ray gives a fetal dose of 0.01 mGy & CT chest-0.1to1.0 mGy.
It is estimated that fetal exposure to X-rays increases the risk of fatal cancer in childhood by 1 in 33,00,000 .
A pelvic CT scan gives an approximate fetal radiation dose of 25 mGy, which increases the risk of fatal childhood cancer to 1 in 1320.
IN CAP- However, even with extensive diagnostic testing, the etiologic agent cannot be identified in at least 50% of cases.
The American Thoracic Society (ATS) does not recommend routine performance of sputum culture and gram stain.
Blood cultures may be positive only 7–15% of the time.
Criteria for Severe Community-Acquired Pneumonia
Respiratory rate 30/min PaO2/FiO2 ratio 250 Multilobar infiltrates Confusion/disorientation Uremia Leukopenia—WBC <4000/L Thrombocytopenia—platelets
<100,000/L Hypothermia—core temperature <36°C Hypotension requiring aggressive fluid
resuscitation
IDSA/ATS guidelines
Beta Lactum Abts. Or Cephalosporins are safe and preferred DOC.
Moderate cases of CAP are treated with
Beta Lactum plus Macrolides or Respiratory FQ
The teratogenicity risk of FQ is low, and these should be given if indicated.
If community-acquired methicillin -resistant S. aureus is suspected, then vancomycin is added.
Prevention Pneumococcal vaccine is 60 to 70
percent protective against its 23 included serotypes. Its use has been shown to decrease emergence of drug-resistant pneumococci.
The vaccine is not recommended for otherwise healthy pregnant women
RECOMMANDATIONS
Persons >65 years of age Persons aged 2–64 years with chronic
illnesses (e.g., diabetes, pulmonary or cardiovascular disease, alcoholism, hepatic dysfunction, chronic cerebrospinal fluid leak, or sickle cell disease)
Immunocompromised persons (e.g. HIV, malignancy, chronic renal failure, or asplenia; patients on long-term immunosuppressive therapy; and transplant recipients)
Persons aged 2–64 years who reside in chronic care facilities
Pregnancy Outcome with Pneumonia
During the pre-antimicrobial era, as many as a third of pregnant women with pneumonia died (Finland and Dublin, 1939).
In five studies published after 1990, the maternal mortality rate was 0.8 percent of 632 women. Importantly, almost 7 percent of the women required intubation and mechanical ventilation.
Influenza Pneumonia
caused by RNA viruses of which influenza A and B form one genus.
The virus is spread by aerosolized droplets and quickly infects ciliated columnar epithelium, alveolar cells, mucus gland cells, and macrophages.
Disease onset is 1 to 4 days following exposure
Pneumonia is the most common complication, and it is difficult to distinguish from bacterial pneumonia
Primary influenza pneumonitis is the most severe and is characterized by sparse sputum production and radiographic interstitial infiltrates
More commonly, secondary pneumonia develops from bacterial superinfection by streptococci or staphylococci after 2 to 3 days of initial clinical improvement.
The Centers for Disease Control and Prevention (2009) reported a number of cases in which community-acquired methicillin-resistant staphylococci caused influenza-associated pneumonitis with a case-fatality rate of 25 percent.
Management
The management of pregnant women with influenza rests primarily on supportive care and aggressive treatment of superinfection.
Cases should be followed closely for any deterioration as those with worsening shortness of breath, hypoxia requiring mechanical ventilation
Drugs- Oseltamivir is given orally, 75 mg
twice daily, or zanamivir is given by inhalation, 10 mg twice daily.
The drugs interfere with the release of progeny virus from infected host cells and thus prevent infection of new host cells.
The drugs shorten the course of illness by 1 to 2 days, and they may reduce the risk for pneumonitis.
Use of these agents requires careful consideration of the potential benefits against their unknown risks.
Prevention Vaccination against influenza
throughout the influenza season is recommended by the Centers for Disease Control and Prevention (2007) for all women who will be pregnant during the influenza season.
This is especially important for those affected by chronic medical disorders such as diabetes, heart disease, asthma, or human immunodeficiency virus (HIV) infection.
Inactivated vaccine prevents clinical illness in 70 to 90 percent of healthy adults, and importantly, there is no evidence of teratogenicity.
Zaman and associates (2008) found decreased rates of influenza in infants up to 6 months of age whose mothers were vaccinated during pregnancy
Smoking cessation in pregnancy
For the smoking pregnant woman and her fetus, the risks are more immediate and include
- low birth weight -spontaneous pregnancy loss -stillbirth -premature rupture of membranes -placental abruption -placenta previa and -preterm delivery.
In the postpartum period, cigarette smoking is associated with further risks for babies-
-increased risk of neonatal death -sudden infant death
syndrome(SIDS) -respiratory infections, otitis
media -asthma -childhood obesity, and -possibly type 2 diabetes mellitus
Mechanisms by which these adverse outcomes occur-
Impaired oxygen delivery to the feto-placental unit
Exposure to carboxy-hemoglobin Direct fetal genetic damage Other toxicities from the multiple
substances present in cigarettes and cigarette smoke.
Specific benefits of smoking cessation to tell pregnant patients
After you stop smoking more nutrition will go to your baby to help him/her grow.
After you stop smoking, your chances of having a healthy baby increase, and the baby is more
likely to have a healthy childhood. After you stop smoking you will have more
energy and may feel less stressed. After you stop smoking you’ll breathe
easier and you will be better able to keep up with your active, healthy baby.
After you stop smoking, you’ll reduce your risk for cancer, cardiovascular, and other diseases so you can be around a long time to be a good mother.
Sleep-Disordered Breathing
Snoring is increased in pregnancy, and sleep-disordered breathing may worsen during pregnancy
The incidence and prevalence of sleep-disordered breathing during pregnancy are unknown.
Hormonal changes -increased estrogen resulting in
hyperemia and upper airway narrowing
- increased progesterone resulting in increased respiratory drive AND
-other physiologic changes of sleep (decreased FRC and respiratory system compliance) predispose to alterations in sleep during pregnancy.
Factors protects against SDB in pregnancy
Increased Minute ventilation Preference for lateral sleeping
position during late gestation Decrease in REM sleep.
Symptoms of sleep-disordered breathing should be reviewed with women who develop pregnancy-induced hypertension or preeclampsia.
All pregnant women with symptoms of sleep-disordered breathing should be evaluated with a polysomnogram and treated with nasal continuous positive airway pressure as indicated.
Effect of SDB on maternal health
Gestational hypertension Gestational Diabets and
worsening of established case (by increasing insulin resistance)
Increased risk of Cesarean deliveries
Foetal outcomes
Preterm Birth Growth restriction Foetal Heart rate responce
Treatment Guidelines-
AASP recommends therapy for patients
with RDI of 5 to 15 and a/w witnessed apneas or awakenings caused by gasping or chocking, daytime hyper somnolence , loud snoring or
RDI > 15 or more events per hour with or without symptoms.
Behavior modification – weight reduction avoid weight reduction surgeries avoid smoking, alcohol, sedatives and
sleeping pills Medical options to treat underlying
endocrinal disorders like hypothyroidism
CPAP-
CPAP in pregnancy is efficacious , with positive hemodynamic effects in women with preeclampsia
Pressure requirement may increase slightly during the course of pregnancy and repeat titration should be considered as pregnancy progresses
Auto titrating positive airway pressure is best alternative to conventional CPAP
THE SEVERITY OF SBD AND ITS EFFECTS IMPROVES AFTER DELIVERY.
In summary Pregnancy may either protect against or predispose to the development of SBD.
Studies evaluating predictors of SBD in pregnancy are limited.
Some factors such as Pre pregnancy BMI, Weight gain during pregnancy, age and neck circumference associated with loud snoring , gasping and witnessed apneas.
Venous Thromboembolism
The risk of venous thrombosis during pregnancy ranges from 0.5 to 3.0 per 1000 pregnancies in those without a history of thromboembolism.
Prior thromboembolic disease, smoking, prior venous thrombosis, and thrombophilias are risk factors for deep venous thrombosis or pulmonary embolism (PE) during pregnancy
The risk of venous thromboembolism is greatest in the postpartum period.
Heparin prophylaxis for women with increased risk of thromboembolism during pregnancy and in the immediate postpartum period remains controversial.
Evaluation of the pregnant woman with suspected venous thromboembolism should begin with lower extremity venous ultrasound.
If negative, a ventilation-perfusion (V-P) scan or helical computed tomography (CT) scan should be performed next.
While helical CT is more sensitive for the diagnosis of PE, and the average fetal radiation dose appears to be less with helical CT when compared with V-P scanning, helical CT delivers about a 40 times greater radiation dose to the breast at a time when it is proliferating.
Confirmed cases of venous thromboembolism during pregnancy should be managed with unfractionated or low molecular weight heparins. Coumarin should be avoided due to the risk of embryopathy.
LAM IN Pregnancy
LAM is a rare disease (prevalence 1 to 2/million) affecting premenopausal women with a mean age of 35 years.
The disorder is characterized by proliferation of atypical smooth muscle in the broncho-vasculature, lymphatics, and interstitium of the lung, as well as the abdomen and pelvis.
Complications of LAM include recurrent pneumothoraces in 50% of patients, chylous effusions in approximately one third of patients, chylous ascites, and renal angiomyolipomas in up to 50% of patients.
High-resolution CT can reveal diffuse, homogenous cystic disease with cysts ranging from a few millimeters to ≥ 1 cm in size (6-cm cysts have been reported); characteristically, nodularity, as seen in eosinophilic granuloma, is absent.
Pulmonary function testing most commonly shows mixed obstructive and restrictive physiology with an elevated total lung capacity and residual volume and a reduced diffusion capacity, but up to one third of patients can have normal pulmonary function.
Treatment for LAM - hormonal manipulation with the
use of antiestrogen agents (such as
tamoxifen), progesterone agents, luteinizing hormonereleasing
hormone analogs, and/or oophorectomy with variable
results.
Lung transplantation has been performed for LAM, although disease recurrence has been documented.
Recently, sirolimus, acting via suppression of mammalian target of rapamycin signaling, has been studied with a primary end point of decreasing angiomyolipoma volume at 12 months.
Patients should avoid estrogens and pregnancy.
The prognosis with LAM is variable, but median survival is often reported to be 8 to 10 years. The cause of death is usually respiratory failure.
THANK YOU !!!