pregnancy outcome after preconception progesterone in...
TRANSCRIPT

Pregnancy Pregnancy outcomeoutcome after after preconception progesterone preconception progesterone in recurrent pregnancy lossin recurrent pregnancy loss
Manuela RussuManuela Russu(1)(1),,
RuxandraRuxandra Stănculescu Stănculescu(3), ŞŞ. Nastasia. Nastasia(1) (1) ,
Maria PăunMaria Păun(2) (2) , J.A MarinJ.A Marin(1) (1) , I. LachanasI. Lachanas(1) (1) ,
JaninaJanina ArseneArsene(3)(3)
““Dr. I. Dr. I. CantacuzinoCantacuzino”” Clinic of Obstetrics & Gynecology Clinic of Obstetrics & Gynecology (1)(1),, andand
Department of Neonatology Department of Neonatology (2)(2);;
““St. St. PantelimonPantelimon”” Emergency Clinic of Obstetrics & Gynecology Emergency Clinic of Obstetrics & Gynecology (3) (3)
““Carol DavilaCarol Davila”” University of Medicine & PharmacyUniversity of Medicine & Pharmacy
Bucharest, ROMANIABucharest, ROMANIA1st Central Eastern European Summit on Preconception Health,
Health Care, and the Prevention of Birth Defects
Budapest, HUNGARY, August 27-30, 2008

ObjectivesObjectives
The assessment of The assessment of
pregnancy outcomes after pregnancy outcomes after
preconception to 36 wks gestation preconception to 36 wks gestation
treatment with treatment with
1mg/d folic acid & 1mg/d folic acid &
200mg/d vaginal 200mg/d vaginal micronizedmicronized progesteroneprogesterone
in recurrent pregnancy lossin recurrent pregnancy loss

Material and methodsMaterial and methods (1)(1)
Patients are diagnosed and enrolled in two university Patients are diagnosed and enrolled in two university
clinics of obstetrics from clinics of obstetrics from ““Carol DavilaCarol Davila”” University of University of
Medicine and Pharmacy, Bucharest, if they accomplished Medicine and Pharmacy, Bucharest, if they accomplished
inclusion & exclusion criteriainclusion & exclusion criteria
Inclusion CriteriaInclusion Criteria:: 2 pregnancy loss (first or third 2 pregnancy loss (first or third
trimester)trimester)
Subjects: Subjects: different by moment of 2 previous different by moment of 2 previous
pregnancies loss: first trimester pregnancies loss: first trimester -- group A and third and third
trimester trimester –– early pretermearly preterm birth with neonatal death or birth with neonatal death or
stillbirthstillbirth,, -- group B

Material and methodsMaterial and methods (2)(2)
Exclusion CriteriaExclusion Criteria::�� major uterine malformations, major uterine malformations,
�� subtle subtle ovulatoryovulatory dysfunction, as that related to dysfunction, as that related to hyperprolactinemiahyperprolactinemia, ,
�� positivitypositivity for infections as: toxoplasmosis, for infections as: toxoplasmosis, listeriosislisteriosis, CMV, , CMV,
syphilis,syphilis,
�� major chronic medical diseases (e.g.: insulinmajor chronic medical diseases (e.g.: insulin--requiring diabetes requiring diabetes
mellitus or pharmacologically treated hypertension), treatment wmellitus or pharmacologically treated hypertension), treatment with ith
10,000 or more units of 10,000 or more units of unfractionatedunfractionated heparin per day, treatment heparin per day, treatment
with lowwith low--molecularmolecular--weight heparin at any dose or other diagnosed weight heparin at any dose or other diagnosed
blood coagulation protein or platelet defects, blood coagulation protein or platelet defects,
�� previous pregnancies with chromosomal abnormalities as numeric previous pregnancies with chromosomal abnormalities as numeric
abnormalities (abnormalities (aneuploidiesaneuploidies) and structural anomalies (defects in the ) and structural anomalies (defects in the
structure of 1 or more chromosomes),structure of 1 or more chromosomes),
�� previous gestation over 42 weeks with fetal wastageprevious gestation over 42 weeks with fetal wastage

Material and methodsMaterial and methods (3)(3)
�� An ultrasonic examination was required An ultrasonic examination was required between between 12 and 20 weeks 6 days of 12 and 20 weeks 6 days of gestationgestation: :
-- to confirm the duration of gestation,to confirm the duration of gestation,
-- to screen for major fetal abnormalities, to screen for major fetal abnormalities,
-- for the diagnosis of an ultrasonic large or for the diagnosis of an ultrasonic large or restricted fetus, andrestricted fetus, and
�� repeated at 32 to 34 weeksrepeated at 32 to 34 weeks to evaluate to evaluate fetal growthfetal growth

�� PrimaryPrimary: : birthweightbirthweight, , ApgarApgar scores, congenital scores, congenital
malformations, GA of preterm birth,malformations, GA of preterm birth, composite neonatal composite neonatal
morbidity rate, containing severe respiratory distress morbidity rate, containing severe respiratory distress
syndrome (RDS), syndrome (RDS), bronchopulmonarybronchopulmonary dysplasiadysplasia (BPD), (BPD),
intraventricularintraventricular haemorrhagehaemorrhage (IVH), (IVH), necrozitingnecroziting enterocolitisenterocolitis
(NEC), need of oxygen supplementation, & of mechanic (NEC), need of oxygen supplementation, & of mechanic
ventilation, length of admission in NICU ventilation, length of admission in NICU
�� SecondarySecondary: time to conceive, moment of miscarriage, time : time to conceive, moment of miscarriage, time
until delivery: preterm birth before 32 and 37 weeks, until delivery: preterm birth before 32 and 37 weeks,
maternal morbidity (gestational diabetes, gestational maternal morbidity (gestational diabetes, gestational
hypertension), maternal hospitalization for threatened of hypertension), maternal hospitalization for threatened of
miscarriage/ preterm birth.miscarriage/ preterm birth.
Outcome measuresOutcome measures
Material and methodsMaterial and methods (4)(4)
Statistical AnalysisStatistical Analysis
Student testStudent test for comparison of each group for comparison of each group
of treated patients to controlsof treated patients to controls ((P valueP value),), by by
ANOVA methodANOVA method
P < 0.01 = statistical significantP < 0.01 = statistical significant

� Treated groups: 32 (group A) + 6 (group B)
6 months preconception treatment with folic acid
1mg/d & vaginal micronized progesterone 200mg/d
(14 days/month, each night, from the 14th day of
menstrual cycle), continued immediately after a positive
pregnancy test (the 7th – 10th days of amenorrhea) and
prolonged till the 36th week gestation
� Control group: 58
treated during pregnancy with non a specific
antispastic muscle-relaxant mixture, when necessary.
ResultsResults (1)(1)
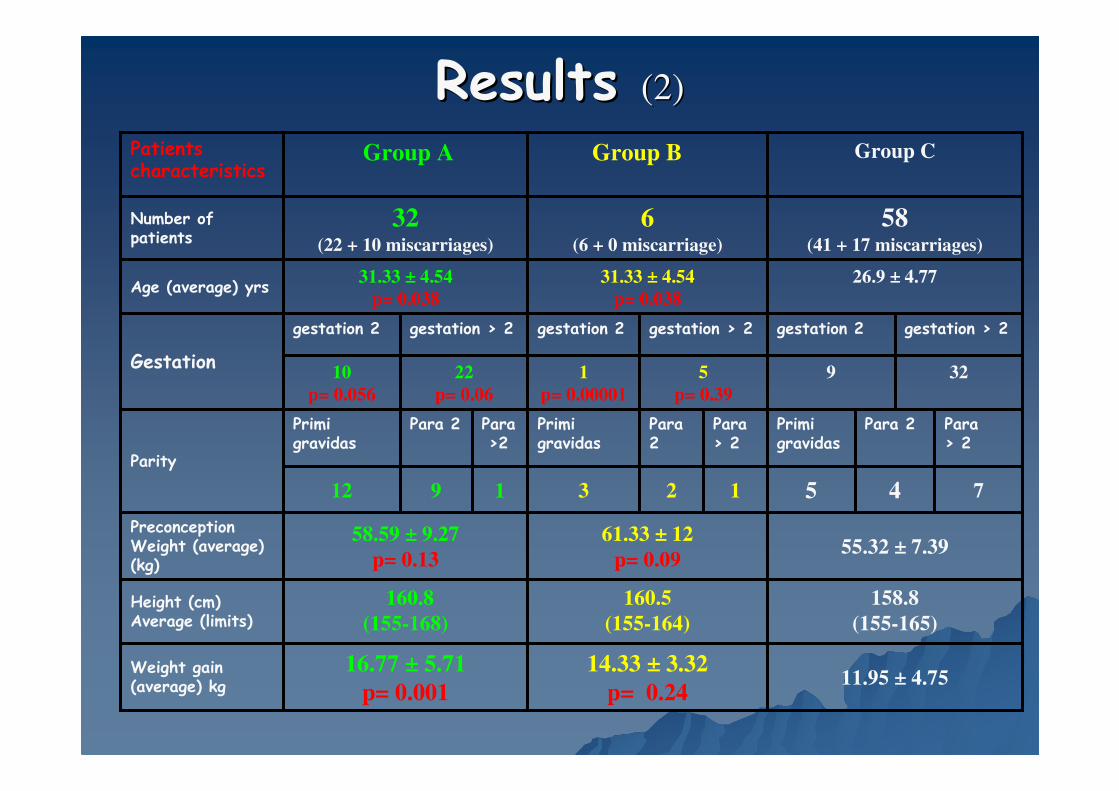
Results Results (2)(2)
11.95 ± 4.7514.33 ± 3.32
p= 0.24
16.77 ± 5.71
p= 0.001
Weight gain (average) kg
158.8
(155-165)
160.5
(155-164)
160.8
(155-168)Height (cm)Average (limits)
55.32 ± 7.3961.33 ± 12
p= 0.09
58.59 ± 9.27
p= 0.13
PreconceptionWeight (average) (kg)
7451231912
Para > 2
Para 2Primigravidas
Para > 2
Para 2
Primigravidas
Para>2
Para 2Primigravidas
Parity
3295
p= 0.39
1
p= 0.00001
22
p= 0.06
10
p= 0.056
gestation > 2 gestation 2 gestation > 2 gestation 2 gestation > 2 gestation 2
Gestation
26.9 ± 4.7731.33 ± 4.54
p= 0.038
31.33 ± 4.54
p= 0.038Age (average) yrs
58(41 + 17 miscarriages)
6(6 + 0 miscarriage)
32(22 + 10 miscarriages)
Number of patients
Group CGroup BGroup APatients characteristics
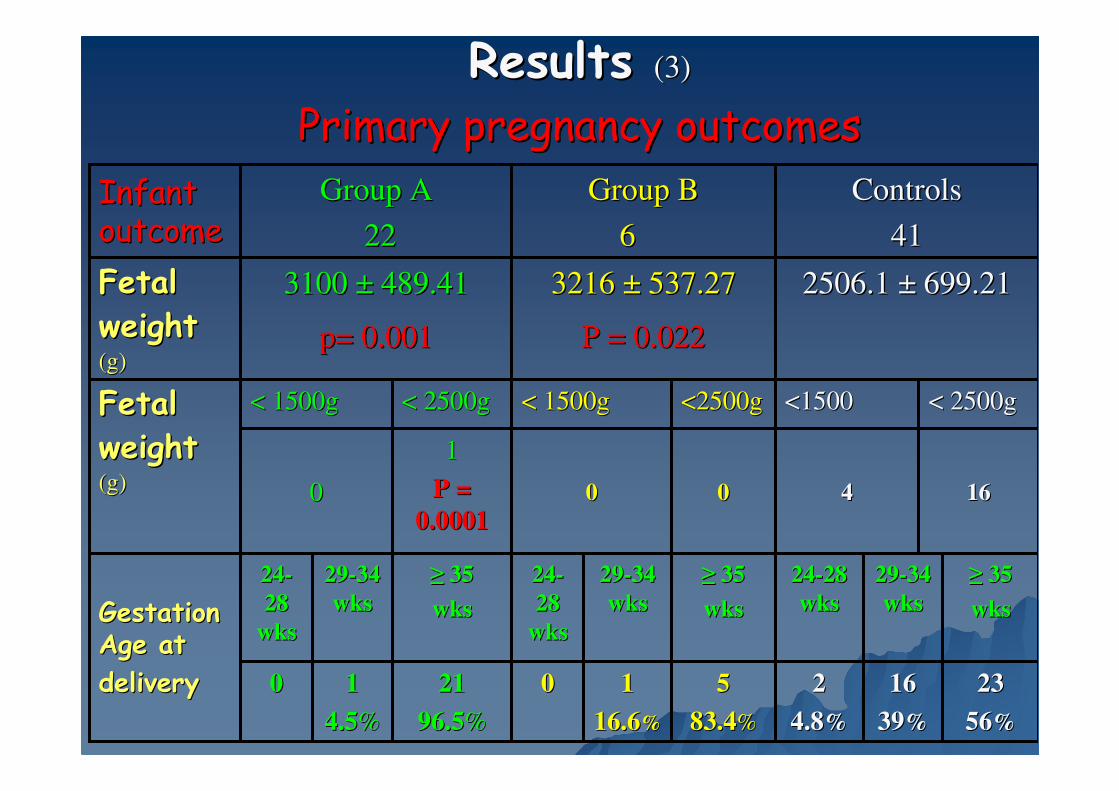
Results Results (3)(3)
Primary pregnancy outcomesPrimary pregnancy outcomes
2323
5656%%
≥≥ 3535
wkswks
2929--34 34
wkswks
55
83.483.4%%
≥≥ 3535
wkswks
2929--34 34
wkswks
2121
96.596.5%%
≥≥ 3535
wkswks
2929--34 34
wkswks
2424--28 28
wkswks
2424--
28 28
wkswks
2424--
28 28
wkswksGestation Gestation Age atAge at
deliverydelivery 1616
3939%%
22
4.84.8%%
11
16.616.6%%
0011
4.54.5%%
00
1616440000
11
P = P =
0.00010.000100
< 2500g< 2500g<2500g<2500g< 2500g< 2500g <1500<1500< 1500g< 1500g< 1500g< 1500gFetal Fetal
weightweight(g)(g)
2506.1 2506.1 ±± 699.21 699.21 3216 3216 ±± 537.27537.27
P = 0.022P = 0.022
3100 3100 ±± 489.41489.41
p= 0.001p= 0.001
Fetal Fetal
weightweight(g)(g)
ControlsControls
4141
Group BGroup B
66
Group AGroup A
22 22
Infant Infant outcomeoutcome

Results Results (4)(4)
Primary pregnancy outcomesPrimary pregnancy outcomes
665544000022220033
>7.25>7.257.21 7.21 --
7.247.24
>7.25>7.257.217.21--
7.247.24
>>7.257.257.217.21--
7.247.24
< <
7.207.20
< <
7.207.20
< <
7.207.20
15 cases 15 cases
ApgarApgar score <7score <7
2 cases 2 cases
ApgarApgar score <7score <7
5 cases5 cases
ApgarApgar score < 7score < 7
pH blood cord pH blood cord
whenwhen
ApgarApgar < 7/5< 7/5’’
8.05 8.05 ±± 1.981.98
8.2 8.2 ±± 1.991.99
4.83 4.83 ±± 4.574.57
p= 0.14p= 0.14
4.83 4.83 ±± 4.624.62
p= 0.13p= 0.13
8.45 8.45 ±± 1.531.53
p= 0.40p= 0.40
8.77 8.77 ±± 1.111.11
p= 0.21p= 0.21
ApgarApgar ScoreScore-- 1 min1 min
-- 5 min5 min
ControlsControls
4141
Group BGroup B
66
Group AGroup A
2222
Infant Infant outcomeoutcome

Results Results (5)(5)
Primary pregnancy outcomesPrimary pregnancy outcomes
000000000000000000551122
CCBBCCBBCCBBCCBB AAAAAAAA
Composite Neonatal MorbidityComposite Neonatal Morbidity
1 Umbilical hernia: control1 Umbilical hernia: control
1 1 HydroceleHydrocele: control : control
1 1 CriptorhydiaCriptorhydia: control : control
NECNECIVHIVHBPDBPDRDSRDS
2 2 HypospadiasHypospadias: : group Agroup A, control, control
MalformationsMalformations
ControlsControls
4141
Group BGroup B
66
Group AGroup A
22 22
Infant Infant outcomeoutcome
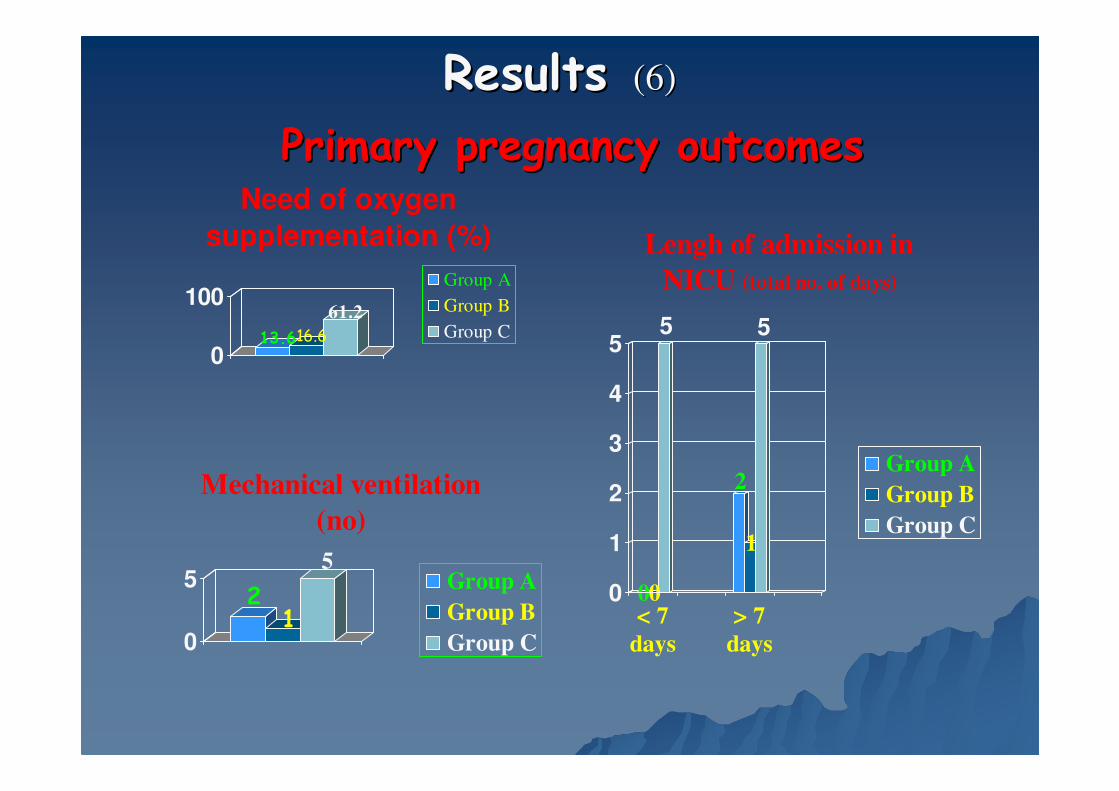
ResultsResults (6)(6)
Primary pregnancy outcomesPrimary pregnancy outcomes
13.616.6
61.2
0
100
Need of oxygen
supplementation (%)
Group A
Group B
Group C
21
5
0
5
Mechanical ventilation
(no)
Group A
Group B
Group C
00
5
2
1
5
0
1
2
3
4
5
< 7
days
> 7
days
Lengh of admission in
NICU (total no. of days)
Group A
Group B
Group C
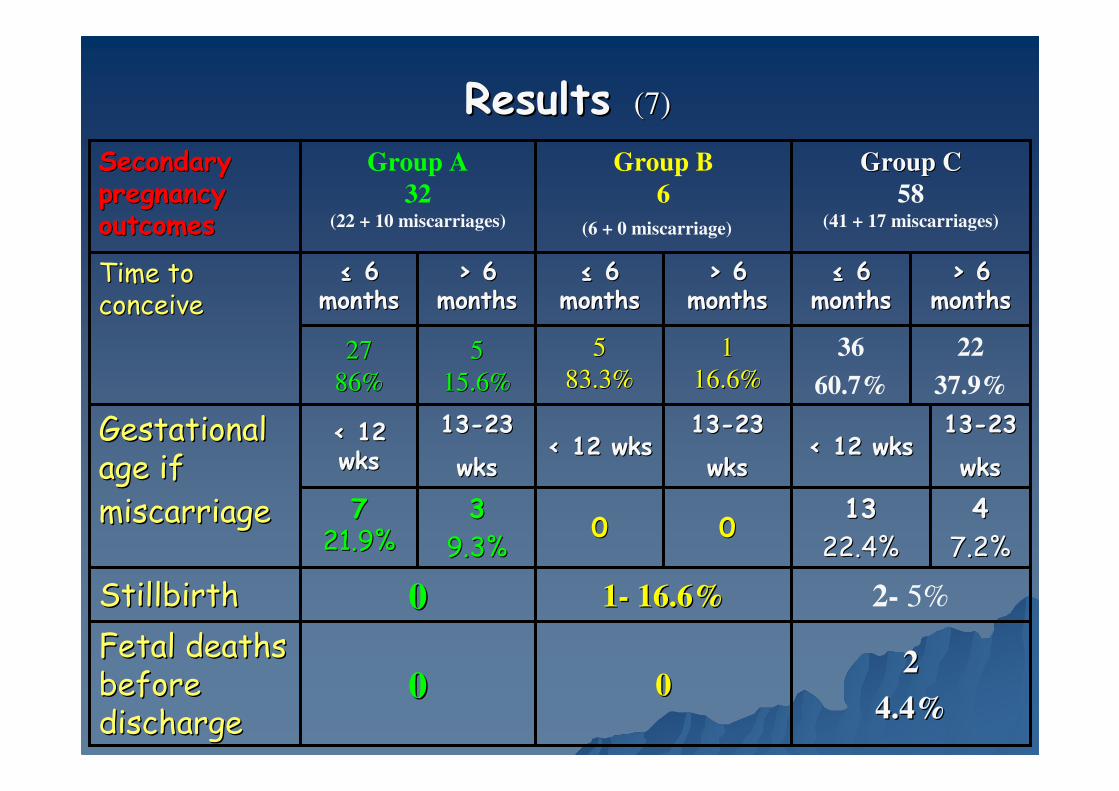
ResultsResults (7)(7)
22
37.9%
36
60.7%
11
16.6%16.6%
5 5
83.3%83.3%55
15.6%15.6%
27 27
86%86%
> 6 > 6 monthsmonths
> 6 > 6 monthsmonths
> 6 > 6 monthsmonths
≤≤ 6 6 monthsmonths
≤≤ 6 6 monthsmonths
≤≤ 6 6 monthsmonths
Time to Time to conceiveconceive
2- 5%00 11-- 16.6%16.6%
44
7.2%7.2%
1313--23 23
wkswks
00
1313--23 23
wkswks
33
9.3%9.3%
1313--23 23
wkswks
7 7 21.9%21.9%
Stillbirth Stillbirth
1313
22.4%22.4%00
2 2
4.4%4.4%0000
Fetal deaths Fetal deaths before before discharge discharge
< 12 wks< 12 wks< 12 wks< 12 wks< 12 < 12 wkswks
Gestational Gestational age if age if
miscarriagemiscarriage
Group CGroup C
58(41 + 17 miscarriages)
Group B
6
(6 + 0 miscarriage)
Group A
32(22 + 10 miscarriages)
Secondary Secondary pregnancy pregnancy outcomesoutcomes

ResultsResults (8)(8)
Secondary pregnancy outcomesSecondary pregnancy outcomes
9
0
26.8
45
0
48.7
9
16.6
19.5
0
5
10
15
20
25
3035
40
45
50
25-28
wks
29- 34
wks
35- 37
wks
Hospitalization for threatened preterm birth
(%)
Group A
Group B
Group C
31.2
16.6
41.4
37.5
33
62
0
10
20
30
40
50
60
70
< 12 wks 13- 24 wks
Hospitalization for threatened miscarriage (%)
Group A
Group B
Group C
00
3 3
19%19%
GroupGroup
CC
n= 41
0000GestationalGestational
DiabetesDiabetes
2 2
33%33%00
Gestational Gestational hypertensionhypertension
Group
B
n= 6
Group
A
n= 22

DiscussionsDiscussions (1)(1)
In the last 40In the last 40-- 50 years 50 years progestinsprogestins and progesterone and progesterone
derivates have been administered during reproductive derivates have been administered during reproductive
years for several reasons: years for several reasons:
�� lutealluteal phase support when phase support when lutealluteal phase defect phase defect or inadequate corpus or inadequate corpus luteumluteum, ,
�� spontaneous pregnancy achievement or IVF spontaneous pregnancy achievement or IVF treatment, treatment,
�� threatening miscarriage, recurrent miscarriage, threatening miscarriage, recurrent miscarriage,
�� prevention of preterm laborprevention of preterm labor. .

DiscussionsDiscussions (2)(2)
Only two formulations are considered safe: Only two formulations are considered safe:
�� natural progesteronenatural progesterone administered vaginally (as administered vaginally (as either a either a pessarypessary or a cream), or a cream),
�� a synthetic a synthetic caproatecaproate esterester of naturally 17 alphaof naturally 17 alpha--hydroxyprogesteronehydroxyprogesterone*, given as a long*, given as a long--acting acting intramuscular injection.intramuscular injection.
*17 alpha*17 alpha--hydroxyprogesteronehydroxyprogesterone is produced by the placenta itselfis produced by the placenta itself
DiscussionsDiscussions (3)(3)
��micronizedmicronized progesteroneprogesterone: the only natural progesterone : the only natural progesterone
available in Romania, and available in Romania, and
�� vaginal route of administrationvaginal route of administration: better bioavailability : better bioavailability
of Progesterone in the uterus (of Progesterone in the uterus (10 fold higher to that of 10 fold higher to that of i.mi.m. . administrationadministration) & ) & minimal systemic undesirable effectsminimal systemic undesirable effects
CicinelliCicinelli E, de Ziegler D, 1999E, de Ziegler D, 1999
TavaniotouTavaniotou A, A, SmitzSmitz J, J, BourgainBourgain C, C, DevroeyDevroey P, 2000P, 2000
�� because of a because of a first uterine pass effectfirst uterine pass effect, explained by: , explained by:
�� direct diffusion through tissuedirect diffusion through tissue, , �� intracervicalintracervical aspirationaspiration,,�� absorption into the venousabsorption into the venous or or lymphatic circulatory lymphatic circulatory systems,systems, andand
�� countercurrent vascular exchange with diffusion from countercurrent vascular exchange with diffusion from uteroutero-- vaginal veins/lymph vessels vaginal veins/lymph vessels toto arteriesarteries

DiscussionsDiscussions (4)(4)
�� In this study: maternal age in studied > controlsIn this study: maternal age in studied > controls
31.33 31.33 ±± 4.54 4.54 vsvs 26.9 26.9 ±± 4.77: 4.77:
P = 0.038P = 0.038
DevotoDevoto L, Vega M, L, Vega M, KohenKohen P, et al, 2002P, et al, 2002
↓↓
�� with aging the molecules (prowith aging the molecules (pro--inflammatory cytokines, inflammatory cytokines,
reactive oxygen species, steroids and inducible nitric oxide reactive oxygen species, steroids and inducible nitric oxide
synthethase) linked to apoptosis of corpus luteum synthethase) linked to apoptosis of corpus luteum
�� are increasing, and are increasing, and
�� are inducing a preferentially diminish of progesterone are inducing a preferentially diminish of progesterone
biosynthesis in mid and late luteal cells in culturebiosynthesis in mid and late luteal cells in culture
DiscussionsDiscussions (5)(5)
•• Preconception Progesterone supplementation by Preconception Progesterone supplementation by binding to the nuclear/membrane receptors: binding to the nuclear/membrane receptors:
�� modulates the contractility of fallopian tubes & modulates the contractility of fallopian tubes & myometrium for gamete/embryo transportation myometrium for gamete/embryo transportation throughout the uterotubal cavities and successful throughout the uterotubal cavities and successful embryo implantation in spontaneous and/or assisted embryo implantation in spontaneous and/or assisted reproduction,reproduction,
Goldenberg RL, Iams JD, et al, 1998Goldenberg RL, Iams JD, et al, 1998
Ayoubi JM, Fanchin R, de Ziegler D, et al, 2001Ayoubi JM, Fanchin R, de Ziegler D, et al, 2001
Bulletti C, De Ziegler D, Bulletti C, De Ziegler D, CicinelliCicinelli E, et al, 2004E, et al, 2004
PalagianoPalagiano A, A, BullettiBulletti C, de Ziegler D, C, de Ziegler D, CiccinelliCiccinelli E, et al, 2004 E, et al, 2004

DiscussionsDiscussions (6)(6)
�� maintains maintains deciduadecidua viabilityviability ((LanLan KKG, KKG, DeMetsDeMets DL, DL,
19831983), together to estrogens ), together to estrogens lower the vascular resistance lower the vascular resistance
in the uterine circulationin the uterine circulation, ,
�� increases the rate of embryo implantationincreases the rate of embryo implantation by effect by effect
on endometrial on endometrial stromastroma cells, cells, acting on different cytokine acting on different cytokine
profilesprofiles which are present as response of the female which are present as response of the female
reproductive tract to the different paternal MHC reproductive tract to the different paternal MHC
histocompatibilityhistocompatibility antigens (the uterus = antigens (the uterus = immunoprivilegedimmunoprivileged
site during pregnancy). site during pregnancy).
Preconception Progesterone supplementation by binding Preconception Progesterone supplementation by binding to the nuclear or membrane receptorsto the nuclear or membrane receptors

DiscussionsDiscussions (7)(7)
�� Th1Th1-- type cytokines are detrimental to pregnancy by type cytokines are detrimental to pregnancy by
stimulating NKstimulating NK-- macrophage system that is involved in macrophage system that is involved in
abortion, whereas abortion, whereas
�� Th2Th2-- type cytokines (and CD81 T cells) prevent type cytokines (and CD81 T cells) prevent
abortions by suppressing of the NKabortions by suppressing of the NK--macrophage macrophage
system, and inhibiting Th1 responses may allow system, and inhibiting Th1 responses may allow
allograft tolerance allograft tolerance
ChaouatChaouat G, G, 1994 1994
Progesterone enhances local production of Th2 Progesterone enhances local production of Th2 and/or LIF cytokines which may contribute to and/or LIF cytokines which may contribute to
the maintenance of pregnancythe maintenance of pregnancy

�� Leukemia inhibitory factorLeukemia inhibitory factor -- produced locally by produced locally by
deciduas, & deciduas, & macrophagemacrophage--stimulating factorstimulating factor (M(M--CSF) are CSF) are
essential for embryo implantation, being associated with essential for embryo implantation, being associated with ThTh--22cells, cells,
•• upup--regulatedregulated by by ILIL--4 4 andand progesteroneprogesterone and and
•• downdown--regulatedregulated by by ThTh--1 1 type cytokines, and by type cytokines, and by ILIL--1212, ,
IFNIFN--γγγγγγγγ,, and and IFNIFN--αααααααα (produced by Th(produced by Th--1)1)
PiccinniPiccinni M, M, BeloniBeloni L, L, LiviLivi C, et al, 1998 C, et al, 1998
PiccinniPiccinni M, M, MaggiMaggi E, E, RomagnaniRomagnani S, 2000S, 2000
DiscussionsDiscussions (8)(8)
Progesterone enhances local production of Th2 Progesterone enhances local production of Th2 and/or LIF cytokines which contribute to the and/or LIF cytokines which contribute to the
maintenance of pregnancymaintenance of pregnancy

�� Our studyOur study: Preconception progesterone supplementation : Preconception progesterone supplementation
during luteal phase was associated to a rate of immediate during luteal phase was associated to a rate of immediate
gestation (in less than 6 months) in gestation (in less than 6 months) in 86%86% respectively respectively 83.3%83.3%in groups in groups AA and and BB vsvs 60.7%60.7% in controls; the supplementation in controls; the supplementation
was continued as soon as was continued as soon as ββ HCG pregnancy test was positive HCG pregnancy test was positive (after 7 to 10 days from fertilization) (after 7 to 10 days from fertilization)
�� The defective The defective decidualdecidual production of LIF, Mproduction of LIF, M--CSF, Il CSF, Il --4, 4, ILIL--10 (which is not found in peripheral10 (which is not found in peripheral--blood Tblood T--cells) and/or cells) and/or Th2 type cytokines may contribute to the development of Th2 type cytokines may contribute to the development of
unexplained recurrent abortionsunexplained recurrent abortions
PiccinniPiccinni M, M, ScalettiScaletti C, C, VultaggioVultaggio A, et al, 2001A, et al, 2001
SzekeresSzekeres--BarthoBartho J, J, BarakonyiBarakonyi A, A, MikoMiko E, et al, 2001E, et al, 2001
DiscussionsDiscussions (9)(9)

DiscussionsDiscussions (10)(10)
�� Our protocol: sustaining corpus Our protocol: sustaining corpus luteumluteum, and both , and both
early & late pregnancy by early & late pregnancy by vaginal vaginal micronizedmicronized
progesteroneprogesterone supplementation, in cases with high risk supplementation, in cases with high risk
for recurrent pregnancy loss. for recurrent pregnancy loss.
�� Proctor A, Hurst BS, Proctor A, Hurst BS, MarshburnMarshburn PB, et al, 2006: PB, et al, 2006:
have used either have used either lutealluteal protocol or first trimester protocol or first trimester
protocol in IVF pregnancies, showing that in the protocol in IVF pregnancies, showing that in the
lutealluteal protocol the rate of miscarriage was higher than protocol the rate of miscarriage was higher than
the first trimester protocol, but the rate of the first trimester protocol, but the rate of lifebirthlifebirth
was better was better (76.8% luteal protocol vs. 75.0% first (76.8% luteal protocol vs. 75.0% first
trimester protocol; P = 0.80)trimester protocol; P = 0.80)
DiscussionsDiscussions (11)(11)
Progesterone supplementation was advocated for Progesterone supplementation was advocated for preterm preventionpreterm prevention
Dodd JM, Dodd JM, FlenadyFlenady V, V, CincottaCincotta R et al, for R et al, for
Cochrane Database Cochrane Database SystSyst RevRev. 2006. 2006
ILIL--1111 is a cytokine with is a cytokine with pleiotropicpleiotropic biological effects, biological effects,
including induction of including induction of ThTh--2 2 type, and inhibition of type, and inhibition of ThTh--11
type cytokine responses, paradoxically, it enhances the type cytokine responses, paradoxically, it enhances the
synthesis of prostaglandins, which induce labor. synthesis of prostaglandins, which induce labor.
ProgestinsProgestins/Progesterone derivates are suppressing /Progesterone derivates are suppressing ThrombinThrombin-- and Iland Il--1{beta}1{beta}--Induced Il Induced Il --1111, which , which are related to preterm delivery, abruption are related to preterm delivery, abruption placentaeplacentae, and , and chorioamnionitischorioamnionitis..
CakmakCakmak H, Schatz F, Huang SH, Schatz F, Huang S--TJ, et al, 2005TJ, et al, 2005

Our protocol:Our protocol: Preconception Preconception –– 36 wks36 wks: the rate of delivery : the rate of delivery
after 35 wks increased from 56% to 96.5%after 35 wks increased from 56% to 96.5%
DiscussionsDiscussions (12)(12)
Natural ProgesteroneNatural Progesterone/ / 17 alpha17 alpha--hydroxyprogesteronehydroxyprogesterone are are administered for miscarriage & preterm birth prevention at administered for miscarriage & preterm birth prevention at different pregnancydifferent pregnancy’’s ages:s ages:
�� from from 1616--20 wks to 36 wks20 wks to 36 wks:: MeisMeis PJ, PJ, KlebanoffKlebanoff M, Thom M, Thom
E, et al (2003) for E, et al (2003) for National Institute for Child Health and National Institute for Child Health and
Human Development: Human Development: reduced the rate of delivery before 32 reduced the rate of delivery before 32
wks from wks from 18.6%18.6% to to 11.4%11.4% ((P: 0.0180P: 0.0180), and before 35 wks ), and before 35 wks
from from 30.6%30.6% to to 20.6 %20.6 % ((P: 0.0165P: 0.0165) )
�� 2424--34 wks34 wks: : dada Fonseca EB, Fonseca EB, BittarBittar RE, RE, CarvalhoCarvalho MH, MH,
ZugaibZugaib M, 2003M, 2003: reduced the rate of delivery before 34 wks : reduced the rate of delivery before 34 wks
from 34% to 19%from 34% to 19%

ConclusionConclusion (1)(1)
Vaginal Vaginal micronizedmicronized progesterone & Folic acid progesterone & Folic acid
preconception, in early and late pregnancy in preconception, in early and late pregnancy in
recurrent pregnancy loss are followed byrecurrent pregnancy loss are followed by::
�� A significant reduction of preterm birth before 34 A significant reduction of preterm birth before 34
wks (13.6% treated wks (13.6% treated vsvs 36.6%controls), 36.6%controls),
�� A reduction of miscarriages (A reduction of miscarriages (23.7%23.7% treated treated vsvs 27,7% 27,7%
controls),controls),
�� An increase of An increase of birthweightbirthweight ((P=.001, group AP=.001, group A; ; P=.022 P=.022
group Bgroup B), less cases with reduced blood cord pH ), less cases with reduced blood cord pH
((P=.0001P=.0001--groupBgroupB) when ) when ApgarApgar score <7/5 minutes, score <7/5 minutes,
ConclusionConclusion (2)(2)
Folic acid & vaginal Folic acid & vaginal micronizedmicronized progesterone progesterone
preconception, in early and late pregnancy in preconception, in early and late pregnancy in
recurrent pregnancy loss are followed byrecurrent pregnancy loss are followed by::
�� Less number of cases who Less number of cases who need oxygen need oxygen
supplementation (supplementation (10.5%10.5% vsvs 61.2%),61.2%), and mechanical and mechanical
ventilationventilation ((7.6% 7.6% studiedstudied vsvs 12.1% 12.1% controlcontrol))
�� Less number of days of admission in the NICU Less number of days of admission in the NICU
(> 7 days: (> 7 days: 7.6% 7.6% studiedstudied vsvs 12.1% 12.1% control)control)
ConclusionConclusion (3)(3)
Vaginal Vaginal micronizedmicronized progesterone & Folic acid progesterone & Folic acid
preconception, in early and late pregnancy in preconception, in early and late pregnancy in
recurrent pregnancy loss are followed byrecurrent pregnancy loss are followed by::
�� less neonatal morbidity (only RDS: less neonatal morbidity (only RDS: 10.3% 10.3% treated treated
vsvs 12.2%controls), 12.2%controls),
�� a a nonsignifiantnonsignifiant difference in difference in perinatalperinatal mortality; mortality;
�� 22 cases with cases with hypospadiashypospadias ((group Agroup A, controls), more , controls), more
other abnormalities in controls.other abnormalities in controls.
ConclusionConclusion (4)(4)
Vaginal Vaginal micronizedmicronized progesterone & Folic acid progesterone & Folic acid preconception, in early and late pregnancy in recurrent preconception, in early and late pregnancy in recurrent
pregnancy loss are followed bypregnancy loss are followed by::
�� Less time to conceive (< 6 months: Less time to conceive (< 6 months: 81.3 %81.3 % studied studied vsvs
60.7%60.7% control)control)
�� Lower incidence of gestational hypertension in treated Lower incidence of gestational hypertension in treated ((5.2%)5.2%) vsvs controls (19%), no gestational diabetes, controls (19%), no gestational diabetes,
�� Less hospitalization for miscarriage threaten (Less hospitalization for miscarriage threaten (28.6%28.6%treated treated vsvs 48.8% control), 48.8% control),
�� Less hospitalization for preterm birth threaten (Less hospitalization for preterm birth threaten (35.1%35.1%studied studied vsvs 43.8% control)43.8% control)
