preoperative management of hyperthyroidism in a goiterous patient
TRANSCRIPT

BY
KANZA KHALID
BUSHRA KHAN

1866……
– “If a surgeon should be so
foolhardy as to undertake it
[thyroidectomy] … every step of
the way will be environed with
difficulty, every stroke of his knife
will be followed by a torrent of
blood, and lucky will it be for him
if his victim lives long enough to
enable him to finish his horrid
butchery.” Samuel David Gross Samuel
1920…. “feat which today can be
accomplished by any
competent operator
without danger of mishap”
(William Halsted)

The thyroid gland secretes two principal hormones –
THYROXINE (T3) AND TRIIODOTHYROXINE (3).
These major metabolic hormone are required for homeostasis of
all cell and influences cell differentiation ,growth , and
metabolism

HYPERTHYROIDISM Hyperthyroidism is the overproduction of thyroid
hormones by an overactive thyroid.
THYROTOXICOSISThyrotoxicosis is defined as the clinical syndrome of hypermetabolism resulting from increased free thyroxine (T4) and/or free triiodothyronine (T3) serum levels

CLINICAL FEATURES OF HYPERTHYROIDISMSudden weight loss
Rapid heartbeat (tachycardia) — commonly more than 100 beats a minute — irregular heartbeat (arrhythmia) or pounding of your heart (palpitations)
Increased appetite
Nervousness, anxiety and irritability
Tremor — usually a fine trembling in your hands and fingers
Sweating
Changes in menstrual patterns
Increased sensitivity to heat
Changes in bowel patterns, especially more frequent bowel movements
An enlarged thyroid gland (goiter)
Fatigue, muscle weakness
Difficulty sleeping
Skin thinning . Fine, brittle hair

WHAT IS GOITER?? A goitre is a swelling of
the neck or larynx resulting from enlargement of the thyroid gland (thyromegaly), associated with a thyroid gland that is not functioning properly.


INDICATIONS FORTHYROIDECTOMY
Thyroid cancer
Toxic thyroid nodule (produces too much thyroid hormone)
Multinodular goiter (enlarged thyroid gland with many nodules), especially if there is compression of nearby structures
Graves' disease, especially if there is exophthalmos (bulging eyes)
Thyroid nodule, if fine needle aspirate (FNA) results are unclear[

TYPES OF THYROID SURGERIES Thyroid lobectomy to remove a nodule (solitary hot or
cold nodules) and goitres that occur in one lobe. Partial thyroid lobectomy to remove a solitary nodule in
one specific part of the thyroid. Thyroid lobectomy with isthmectomy for benign
Hürthle cell tumours and for non-aggressive thyroid cancers.
Subtotal thyroidectomy (leaving enough of the gland to produce some hormones) is now little used and has been replaced by total thyroidectomy or thyroid lobectomy alone.
Total thyroidectomy for thyroid cancers, Hürthle cell tumours and also increasingly for multinodular goitres and patients with Graves' disease.

HISTORY History of onset, duration, rate of growth
History suggestive of primary or secondary thyroid toxicity
History of pain
History of palpitation, precordial pain, exhaustion
History of pressure effects- like dyspnoea, dysphagia, hoarseness of voice.
Past history/family history.
Personal history-diet, menstrual, mental attitude, sleep

PHYSICAL EXAMINATION General appearance
Vital signs
Respiratory system
CVS system
Abdomen
Extremities and spine
Neurologic system
GENERAL PHYSICAL EXAMINATION Built, nourishment
Fullness of thyroid region, pallor, icterus, cyanosis,
clubbing, oedema
Temperature, Sleeping pulse rate, blood pressure
Skin- hot and moist palm
Tremors
Mental status-anxiety, nervousness.
Airway assessment
Local examination Inspection :
Whether diffuse/ nodular swelling
Pizzillo's method : in obese and short necked patient hands are placed behind head and patient is asked to push head backwards against her clasped hand. Ask the patient to swallow, thyroid slowly moves upwards on deglutition.
Pemberton's sign : Patient is asked to raise both the arm over his head until they touch the ears. This is maintained for a while, congestion of face and distress becomes evident because of obstruction of great veins at thoracic inlet.

Palpation:
Percussion : Over manubrium sterni to exclude
presence of a retrosternal goiter.
Auscultation : A systolic bruit may be heard over
goiter due to increased vascularity in primary toxic
goiter.
Systemic examination CVS :
Enlarged heart
Atrial fibrillation
Signs of CCF.
Systolic murmurs
CNS :
Myopathy and tremors
Reflexes- hyperreflexia
INVESTIGATIONS Complete Blood Count, BT, CT to rule out
anemia, thrombocytopenia and agranulocytosis.
Urine Albumin, Sugar, Microscopy
RBS, B. Urea, Serum creatinine
ECG- Sinus tachycardia, ST elevation, QT shortening, atrial fibrillation/flutter, ventricular ectopics
INVESTIGATIONSTHYROID FUNCTION TESTS:
TSH Assay : single best test of Thyroid Hormone action at cellular level.
Normal level : 0.4-5.0 mU/L.
Subclinical hyperthyroidism : TSH level is 0.1-0.4mU/L with normal FT3 & FT4.
Overt hyperthyroidism : TSH level is <0.03mU/L with increased T3 & T4.
Thyroid Storm : TSH level is <0.01mU/L.
Free T4 (FT4) : approx 0.02% of total T4.
Elevated in 90% of patients with hyperthyroidism.
Decreased in 85% of patients with hypothyroidism
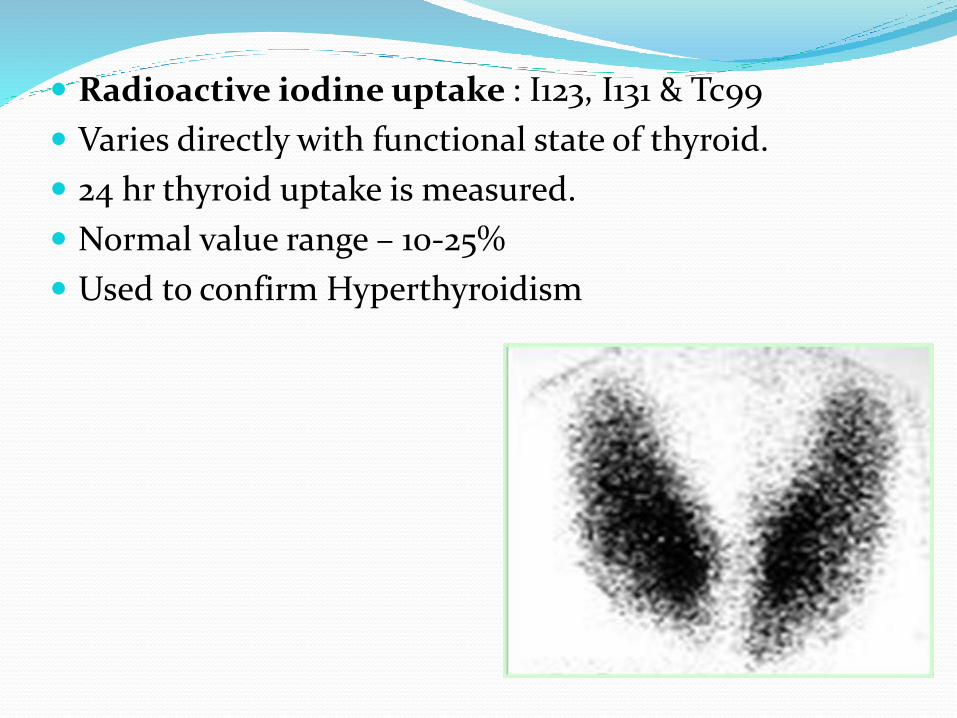
Radioactive iodine uptake : I123, I131 & Tc99
Varies directly with functional state of thyroid.
24 hr thyroid uptake is measured.
Normal value range – 10-25%
Used to confirm Hyperthyroidism

Ultrasonography: to differentiate between cystic, mixed or solid lesion in gland.
Thyroid scan using I123 or Tc99 evaluate nodules as
Warm/ Normal
Hot/ Hyperfunctioning.
Cold/ Hypofunctioning.
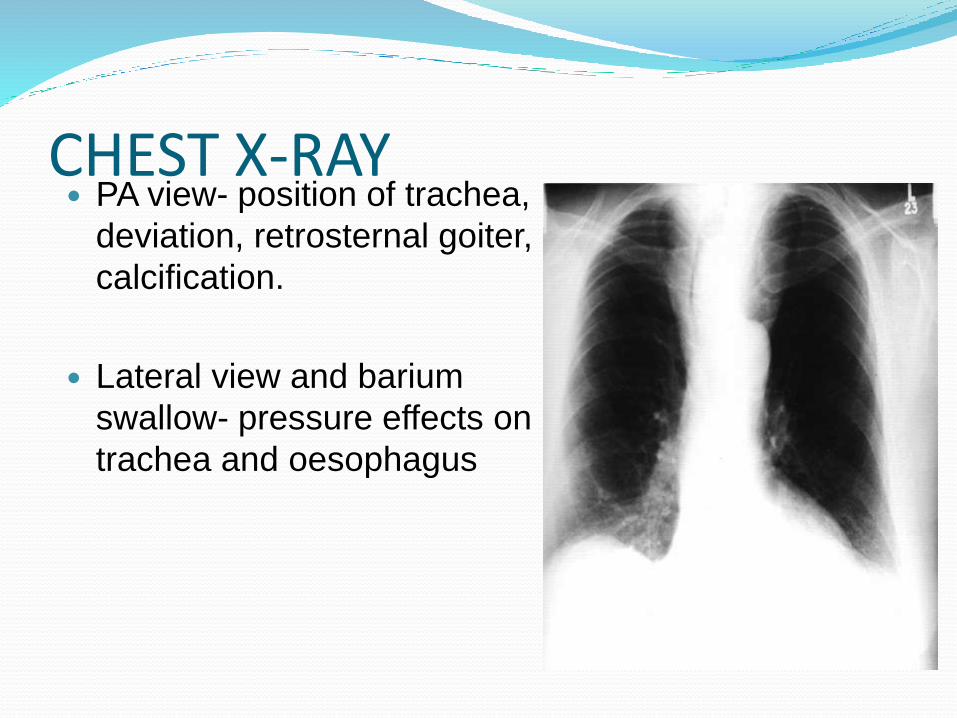
CHEST X-RAY PA view- position of trachea,
deviation, retrosternal goiter,
calcification.
Lateral view and barium
swallow- pressure effects on
trachea and oesophagus

CT scan and MRI scan-for airway evaluation and extension of thyroid.

Difficult tracheal intubation in thyroid surgery 6% of tracheal intubations for
thyroid surgery will be difficult.
When conventional methods of laryngoscopy and endotracheal intubation do not provide airway management. The best choice is
Fiberoptic intubation. If fiberoptic bronchoscope
is not available, mask ventilation, laryngeal mask, combitube, nasotrachealintubation, rigid bronchoscope intubation.
MEDICAL TREATMENT OBJECTIVES
Making the patient asymptomatic
Making a thyrotoxic patient euthyroid before surgery
WHAT IS EUTHYROIDISM?? Euthyroid is clinically assessed by-
◦ Sleeping pulse rate < 90/min
Progressive weight gain
◦ Disappearance of toxic symptoms like tremors, nervousness, anxiety etc .
◦ No requirement of sedation for sleep.
◦ Normal pulse pressure, sinus rhythm, disappearance of cardiac murmurs

Making the patient Euthyroid
• Anti thyroid drugs : Carbimazole vs. PTU
• Start Carbimazole 10-30 mg/day based on severity of symptoms and time left for surgery
• Call back after 6 weeks and reassess
MAKING THE PATIENT ASYPMTOMATIC
Beta blockers
• Reduces myocardial oxygen consumption, reduces heart rate, improves myocardial efficiency
• Used to prepare patients for surgery• Used with caution in patients with
congestive heart failure, bronchial asthma• Useful in thyrotoxic crisis

ANTITHYROID DRUGS CARBIMAZOLE: commonest drug used.
Dose: 5-10mg, 8hrly.
Maintenance Dose: 5mg 6-24 months.
Blocks the synthesis of thyroid hormones.
Suppresses the autoimmune process in Grave’s disease.
METHIMAZOLE: Alike carbimazole. Dose is 5-20mg daily.

ANTI THYROID DRUGS PROPYLTHIOURACIL:
Blocks thyroid hormone synthesis.
Blocks peripheral conversion of T4 to T3.
Decreases thyroid autoantibody levels.
Safe to be given in children and pregnancy.
Dose: 200mg 8hrly.
Side Effects: agranulocytosis and aplastic anemia

BETA BLOCKERS β-Blockers reduces the cardiac symptoms .
Blocks peripheral conversion of T4 to T3.
Propranolol 80 -160 mg once daily
Atenolol 25-100 mg once or twice daily
Metoprolol 50 - 200 mg divided 2 or 3 times per day
IODIDES Saturated solution of potassium iodide: 1-3 drops 3
times per day
Lugol’s solution (5%Iodine +10%KI) : 5 drops 3 times per day dissolve in a full glass of water
Iodide therapy added 1 wk before surgery and continued through the day of surgery
Involution of the gland
Decreases its vascularity, (decreased rate of
intraoperative blood loss)
• Contraindicated in toxic multinodular goiter and AFTN
BLOCK AND REPLACEMENT TREATMENT
It is giving high dose of carbimazole to inhibit T3 and T4 production completely with a maintainence dose of 0.1 mg of L Thyroxine .It reduces iatrogenic thyroid insufficiency.
For Emergency Surgery
Esmolol 100-300 mcg/kg/min IV until heart rate <100/min
Why should a toxic patient beEuthyroid before surgery ?To Prevent
Thyrotoxic crisis
Cardiac arrhythmias and tachycardia
Worsening of co existent medical conditions:
Cardiovascular
Diabetes mellitus
Blood pressure
Hemodynamic compromise
Anesthetic drug interactions

Thyroid Storm Is a life threatening emergency
Characterized by sudden appearance of clinical signs of hyperthyroidism due to the abrupt release of T4 and T3 into circulation.
Mortality is as high as 25% to 30%.
Commonly associated with Grave's disease.

Triggers Trauma
Infection
Surgery

THYROID STORMCLINCAL PRESENTATION 2 most important defining features :
High fever (usually over 40 degrees C)
Significantly abnormal mental status
Agitation, confusion, psychosis, coma
May also exhibit :
Marked tachycardia
Vomiting, diarrhea
Jaundice (in 20 %)
Associated signs of Graves' disease
TREATMENT OF THYROID STORM High flow O2
Rapid cooling if markedly hyperthermic
Ice packs, cooling blanket, mist / fans, nasogastric tube lavage, acetominophen (Salicylates contraindicated because cause peripheral deiodinationto T3)
IV fluid bolus if dehydrated
May need inotropes instead if in CHF
Propranolol 1 mg doses or labetolol 10 to 20 mg doses IV & repeat doses as needed
IV diltiazem +/- digoxin for rate control for atrial fib
IV diuretics if in CHF
IV hydrocortisone (or equivalent) 100 mg
Propylthiouracil (PTU) 600 to 1200 mg PO or by NG
Sodium iodide 1 gram IV one hour after the PTU
Find and treat the precipitating cause

PRE OP ORDERS………. Informed consent
Keep NPO.
Absolute bed rest.
Sedation : Diazepam 2mg-5mg
Resting pulse chart
Patient must be made euthyroid or near euthyroid at operation.
Sleeping pulse rate < 90/min
Progressive weight gain
THANK YOU!!
