presentation of acute wernicke's encephalopathy and treatment with thiamine
TRANSCRIPT

Metabolic Brain Disease, Vol. 10 No. 1 1995
Presentation of Acute Wemicke's Encephalopathy andTreatment with Thiamine
Beverley Woodll3 and Jon Currie2
Received 14 August, 1994; Accepted 3 October, 1994
Thirty two cases of acute Wernicke's encephalopathy were observed in a period of 33months, and prior to the mandatory thiamine enrichment of Australian bread-making flourin 1991 . These cases were carefully assessed by multiple tests at specified intervals priorto, and following thiamine administration until discharge from hospital . Structuredscoring of neurological signs and symptoms, CT scans, psychometry, nutritionalmeasurements, and liver biopsies were performed. There was variation in the presentationand severity of clinical signs and symptoms and in response to treatment . All patientshad alcohol-related liver disease, and the results indicated that fatty liver was important inpresentation and in response to treatment with thiamine . Other forms of alcohol relatedbrain damage were present in these patients, most of whom were in the 4th or 5th decadeof life and had been drinking beer to excess for more than 20 years .
Key words : Wernicke's encephalopathy, thiamine, alcoholism, nutritional status
INTRODUCTION
Thirty two cases of acute Wernicke's encephalopathy were observed at St . Vincent'sHospital Melbourne over a period of 33 months (Wood et al, 1986) . These cases presentedagainst a background of alcoholism, and although heavy recent drinking may have ceased,the person had often had little or no food for the past two weeks .
This report provides further details of the presentation of these clinical cases of acuteWernicke's encephalopathy and their response to treatment with thiamine .
1 Senior Research Fellow, University of Melbourne, Department of Community Medicine andPublic Health
2 Director, Alcohol and Drug Services, Westmead Hospital, Sydney, Australia3 To whom correspondence should be addressed at Department of Community Medicine and
Public Health, University of Melbourne, Parkville, Victoria 3052, Australia
570885-7490/95/0300-0057$07 .50/0 © 1995 Plenum Publishing Corporation

58
Wood and Currie
MATERIALS AND METHODS
Neurological AssessmentA diagnosis of acute Wernicke's encephalopathy was recorded if ophthalmoplegia was
present together with at least two of the three other features, namely nystagmus, ataxia anda global confusional state (Victor et al, 1971) . To assist description of the severity of thesediagnostic features, the Neurologist (J.C .) assigned the subjects to one of five differentdiagnostic classes of Wernicke's encephalopathy (see Table VII), on admission and at eachinterval of assessment .
Prior to the administration of thiamine, and at each subsequent time interval, carefulstructured clinical assessment was conducted . Mathematical scores (wherein normal wasscored zero) were assigned to each neurological observation, including ophthalmoplegia,nystagmus and global confusion . These procedures were carefully standardized and appliedat each time interval by one trained observer (J.C .) ; the detailed scoring system is availableon request.
Laboratory TestsPrior to administration of thiamine and at each time interval thereafter, blood was drawn
for the assessment of thiamine status by the erythrocyte transketolase assay (Wood andPenington, 1973), and a random urine specimen obtained for determination of urinarythiamine (Interdepartmental Committee on Nutrition for National Defence, 1963) andcreatinine excretion (Bosnes and Taussky, 1945) .
Biochemical tests were also used to assess riboflavin status (by a WHO modification ofBeutler 1969a,1969b), pyridoxine status (by a WHO modification of Karmen et al ., 1955 ;Stanulovic et al., 1967), and Vitamin C (Denson and Bowers, 1961) .
The patients height and weight were measured on day one after admission to hospital andpercent reference weight calculated and used for the diagnosis of overweight (Garrow, 1974)and protein-energy malnutrition (International Classification of Diseases, 1979) .
Other general biochemical and haematological tests were performed by the hospitalBiochemistry and Haematology Departments using standard methods .
TreatmentFollowing initial assessment, each subject was treated with a therapeutic dose of
thiamine hydrochloride intravenously, followed by daily parenteral thiamine .Multivitamins were witheld for the first week then given at day seven. Assessment
was repeated in an identical manner at intervals of within 12 hours, and at 24 hours, 48hours, 7 days and 14 days .
Liver BiopsyA liver biopsy was performed within one week of admission, and the presence of fatty
liver, alcoholic hepatitis, fibrosis and cirrhosis determined. Biopsies were independentlyread by a pathologist and the clinical hepatologist, and assigned to a grade of severity ofliver disease (0 to 4) and of fatty liver (0 to 3) (Tables III).

Wernicke's encephalopathy : response to thiamine
59
Table I. Severity grade of liver disease in 32 subjects .
Other Alcohol Related Brain DamageAt 14 days or just prior to discharge, whichever came first, the presence of alcoholic
cerebellar dysfunction was noted if there was ataxia of stance and gait (truncal ataxia) andlimb movements (Dreyfus, 1979) .
Computerized tomographic (CT) brain scans were performed on the majority of subjectswithin 10 days of admission to hospital . A clinical diagnosis of Korsakoffs psychosis wasalso assigned then if the pa ' showed defective short term memory and/or confabulation(WHO, 1975) .
In the last 10 subjects to enter the study, psychological tests were applied 7 - 10 daysafter admission and treatment; these tests comprised the Adult Intelligence Scale (Wechsler,1958) and the Wechsler Memory Scale (Wechsler and Stone, 1945) ; the results were used toform a psychometric diagnosis of Korsakoffs Psychosis and/or Dementia .
StatisticsThe nature of the change in a number of variables with time was investigated by
regression analysis with hierarchical and stepwise procedures to establish the least squaresline of best fit to the data; the resultant models have been shown as graphs. Statisticalanalysis was facilitated by the Statistical Package for the Social Sciences (SPSS) (Nie et al,1970) .
Grade Liver disease N (%)0 Normal 01 Fatty liver only 02 Alcoholic hepatitis (+/- fatty liver) 15 (56)3 Fibrosis (+/- alcoholic hepatitis +/- fatty liver) 8 (30)4 Cirrhosis (+/- fibrosis+/- alcoholic hepatitis+/- fatty liver) 4 (15)(a)
(a) One of these subjects had cirrhosis on liver scan . N = Number of subjects .
Table II. Severity grade of fatty liver in 26 subjects .
Grade Fatty liver N (%)0 Normal 4 (15)1 Mild 11 (42)2 Moderate 7 (27)3 Severe 4 (15)
N = Number of subjects .

60
Wood and Currie
RESULTS
Liver DiseaseLiver biopsies were performed in 26 of 32 subjects, and in one additional patient the
presence of cirrhosis was diagnosed from liver scan ; all patients had some form of liverdisease (Tables I,11) .
On admission, there was a high frequency in abnormality of liver function tests (TableIII), and at discharge many subjects still had abnormal values .
Table III . Liver function tests (a) in patients with acute Wernicke's encephalopathy
(a) For actual results, refer to Wood et al, 1983 ; N = Number; A = Admission ; D = Discharge ;Admission/ Discharge : ** p<0.01 .
Thiamine StatusWhen thiamine status was assessed on the basis of both an elevated TPP effect and low
urinary thiamine excretion, it was considered to be deficient, borderline and normal in 21(66%), 5 (16%) and 6 (19%) subjects respectively (Table IV) . Normal thiamine status intwo subjects was not explained by recent vitamin supplementation as their urinary thiamineexcretion was in the normal range . In four other subjects with normal thiamine status(normal TPP effects), urinary thiamine excretion was high and closer investigation revealedthat two patients had received intravenous thiamine in the Emergency Department afterdiagnosis but prior to blood sampling, one patient had received vitamin B groupsupplements prior to diagnosis in hospital and the other patient had been prescribed them athome .
The alternative classification of thiamine status based on low erythrocyte transketolaseactivity (ETKA) alone revealed 29 of 32 subjects on admission (Table IV). Two subjectswith normal ETKA had no evidence of recent vitamin supplementation (see above) but theother subject was found to have received vitamin treatment in the Emergency Department .
The ETKA level was low (median 44 .3 IU, range 22 .7 - 150.9 IU) on admission . Aftertreatment with thiamine, it rose to normal within hours (F=128 .66, p<0.001), andcontinued to increase within the normal range thereafter (F=19 .35, p<0 .001) (Figure 1) .The administration of multivitamins at day seven appeared to have no effect and bydischarge ETKA was still low in 13 subjects (42%) (Table IV) .
Frequency of abnormalityReferencevalues
N
A/D
N (%)
A
N (%)
DSerum albumin (g/l) 35-55 32/29 3(9) 9(31)Serum aspartate amino-transferase (U/I) 7-30 32/28 27(84) 20(71)Serum alkaline phosphatase (U/I) 2-80 32/28 26(81) 21(75)Total serum bilirubin (mmol/1) <17 32/28 20(63) 5 (18)**

N = Number; A = Admission ; D = Discharge; ETKA = Erythrocyte transketolase activity .a) Recent vitamin medication in 4 subjects ; b) Recent vitamin medication in one subject ;c) 28 subjects on admission only; d) 26 subjects on discharge only .Reference range : Refer Wood et al, 1980 & ICNND, 1963 . Admission/ Discharge : *** p<0.001 .
On admission the TPP effect was elevated (median = 49 .8%, range 0 - 89%). Aftertreatment with thiamine the TPP effect returned to normal within hours (F=334.65,p<0.001), and no further change was observed (Figure 2) .
Prior to treatment, ETKA was independent of the severity of liver disease (on liverhistology) and unrelated to the results of liver function tests . The percent TPP effect at thistime was higher in subjects with Grade 4 liver disease (n=3, mean TPP effect=70 .2%,SD=11 .72) than in those with Grade 3 (n=8, mean TPP effect=57 .8%, SD= 18.48) or Grade2 liver disease (n=15, mean TPP effect=36 .6%, SD=27.12) (F=3 .7044, p<0 .05) . Onadmission, there was a complete association between the presence of fatty liver andabnormal thiamine status (reflected by ETKA and the TPP effect). No subjects with normalthiamine status had evidence of fatty liver .
Prior to treatment, ETKA was lower in patients with fatty liver (Figure 3), all of whomshowed dramatic improvement within hours of thiamine administration (F=268 .09,p<0.001) and then slow improvement with time (F=15 .47, p<0.001) . Prior to treatment,ETKA was normal in subjects without fatty liver, and during treatment showed the samelinear improvement with time (F=15 .47, p<0.001) .
Wernicke's encephalopathy : response to thiamine
Table IV . Thiamine status in 32 subjects
61
Frequency of abnormality
Reference rangeN (%)A
N (%)D
TPP effect (%)(a) Deficient (>35 .4) 21(66) 0Borderline (14.2-35 .3) 5(16) 0Normal (<14.2) 6(19) 31 (100)***
ETKA (IM (b) Low (<99 .2) 29(91) 13 (42)***Normal (99 .2-158.3) 3(9) 17(55)High (>158 .3) 0 1 ( 3)
Urine thiamine excretion (c,d) 'Low (0-26 .9) 18(64) 0(µg thiamine/g creatinine) Borderline (27-65 .9) 3(11) 0
Normal (66-999.9) 3(11) 0High (1000+) 4(14) 26(100)

a
62
120
100
40
20
0
Figure 1 . Change in ETKA with treatment(Prior to treatment - 1: Subjects with normalTPP effect, II : All subjects, III : Subjects witha high TPP effect)
0 91 2
Time (days)
2
1
014
0 4 1 2
i
Time (days)
Time (days)
Time (days)
Figure 3. The effect of the presence or absence
Figure 4 . Change in severity of theof fatty liver on change in ETKA with treatment .
ophthalmoplegia with treatment .The heavy line represents all subjects .
Anthropometric DataOn the basis of percent reference weight for age 25 years, one subject (3% s obese,
three (10%) were overweight, 12 (41%) were of normal weight and 13 (44% edegree of protein-energy malnutrition (PEM) . Mild, moderate and severe forms of PEMwere found in seven (24%), five (17%), and one (3%) of 29 subjects respectively .
Wood and Currie
Figure 2. Change in the TPP effectwith treatment . (Prior to treatmentI: Subjects with normal TPP effect,II : All subjects, III : Subjects with a highTPP effect).
14
90
0
O20 Cm
N
0
1
. ..
00 41 2
7
19
0 4 1
2
1
14

Wernicke's encephalopathy : response to thiamine
63
Other Measures of Nutritional StatusThe frequency of abnormality in other measures of nutritional status are shown in Table
V. Multiple vitamin deficiencies were observed on admission in some patients .
Ocular Signsa) Ophthalmoplegia
Prior to treatment, ophthalmoplegia was present in 30 of 32 subjects, predominantly aslateral rectus palsy (6th cranial nerve palsy) and less often as conjugate horizontal gazepalsy (Table VI) . Ptosis was observed in one subject only . Of the two subjects withoutophthalmoplegia, one was subsequently found to have normal thiamine status due to recentvitamin supplementation, while the other had clear evidence of biochemical thiaminedeficiency . Three of the subjects had ophthalmoplegia in the face of normal thiamine statusassociated with recent vitamin supplementation .
Table V. Frequency of abnormality(a) in other biochemical and haematologicalmeasurements
F 11 .5-16.5(a) For actual results, refer to Wood et al, 1988 ; N = Number ; A = Admission ;D = Discharge; B = Borderline; DF = Deficient ; H = High ; L = Low; M = Male; F = Female .Admission/Discharge : * p<0 .05, *** p<0.001 .
A dramatic and significant improvement in the severity of ophthalmoplegia was noticedimmediately after treatment with thiamine (F = 99 .9, p<0 .001) (Figure 4), and continuedtowards normal (F = 33 .1, p,<0 .001). Scores for individual ocular movements all showed asimilar pattern of improvement (all p<0 .01). By discharge there was a significantimprovement in the frequency of abnormality and only four subjects showed slight tomoderate evidence of ophthalmoplegia (Table VI) .
Frequency of abnormalityReference values N
A/DN (%)A
N (%)D
Serum albumin (g/1) 35-55 32/29 3(9) 9(31)Riboflavin status (FAD ratio) <1 .34 29/27 21(72) 4 (15)***Pyridoxine status (PP ratio) <1 .80 28/27 0 0Serum folate (µg/ml) >5 27/24 6 (22)B 4 (17)B
5 (19)DF 2 (8)DFSerum Vitamin B12 (pg/ml) 150-900 29/18 1 (3)H 2 (11)LLeucocyte ascorbate 20-50 8/10 3(38) 1(10)(µg/10 leucocytes)Serum magnesium (mmol/1) 0.76-0.90 26/24 10 (38)L 12 (50)L
7 (27)HSerum zinc (p.mol/1) 12.0-16.5 10/11 10(100) 7(64)Haemoglobin (g/100 ml) M 13-18 21/28 2(10) 15 (54)*

64
Wood and Currie
On admission, a trend was observed towards greater severity of ophthalmoplegia withincreased severity of liver disease (Figure 5) or fatty liver (Figure 6) but neither reachedsignificance. Following withdrawal of alcohol, and with thiamine treatment, thee severity ofophthalmoplegia reached approximately the same end point, regardless of the severity ofliver disease or fatty liver . However, the rate of improvement (over and above the effect oftime itself) was affected by the severity of liver disease (F=20 .2275, p<0.001) (Figure 5)and alternatively by the severity of fatty liver (F=18 .2869, p<0 .001) (Figure 6) .
The statistical significance of the effect of severity of fatty liver on improvement in theseverity of ophthalmoplegia with treatment was over and above that of the severity of liverdisease (F=9.4403, p<0.01) and when the effect of fatty liver was fitted in the regressionmodel, the effect of severity of liver disease almost vanished (F=0 .6238,p>0.04) . The finalmodel (Figure 6) shows that subjects with no fatty liver had the fastest improvement inophthalmoplegia to treatment, but all subjects reached the same level by the end of 14 days .
Table VI. Frequency of abnormalities in ocular signs and the global confusional state in32 patients with Wernicke's encephalopathy
N = Number ; A = Admission; D = Discharge; R = Right; L = Left ; V = Vertical .For actual scores, refer to Wood et al, 1983 . Admission/discharge : *p<0.05, **p<0.01,***p<0.001 . 31 patients only at A (a) and D (b) .
Frequency of abnormalityN (%)A
N (%)D
Ophthalmoplegia 30(94) 4 (13) ***R/lateral rectus 18(56) 2(6) ***L/lateral rectus 16(50) 2(6) ***R/medial rectus 9(25) 1 (3) *L/medial rectus 10(21) 1 (3) **
V/upwards gaze 15(47) 2(6) ***
V/downwards gaze 6(19) 0 *R/conjugate gaze palsy 12(37) 2(6) **L/conjugate gaze palsy 13(41) 2(6) ***Nystagmus 29(91) 26 (81) ***R/lateral 22(69) 23 (72) **L/lateral 22(69) 25 (78) **V/upwards 15(47) 1 ( 3) ***V/downwards 11(34) 1 ( 3) **
State of consciousness (a,b) 24(77) 5 (16) ***Disorientation in time (a) 31(100) 25 (78) ***Day unknown 31(97) 18 (56) ***
Disorientation in place 27(84) 18 (56) *Country unknown 6(19) 0*

Wernicke's encephalopathy : response to thiamine
i 2
Time (days)
U
Time (days)
Figure 5. The effect of severity of liver disease
Figure 6. The effect of severity of(grade) on change in the severity of ophthalmoplegia fatty liver on change in the severitywith treatment. See Table I for description of
of ophthalmoplegia with treatment .grades 0-4 .
See Table II for description of grades0-3 .
b) NystagmusNystagmus on lateral gaze was the predominant abnormality prior to treatment but
nystagmus on vertical gaze was also common (Table VI) . Nystagmus was not evident inthree of the 32 subjects because of total ophthalmoplegia .
A slow but significant improvement in the severity of nystagmus was observed withtime (F = 51.0, p<0 .001) (Figure 7). This improvement plateaued (F = 6 .2, p<0 .002) andafter administration of multivitamins at day seven, the rate of improvement increased againbut normality was not achieved .
Scores for individual tests of nystagmus all showed improvement (all p<0 .01), and atdischarge, only six subjects were completely free of nystagmus (Table VI) .
Global Confusional StatePrior to treatment, 7 of 31 (23%) subjects were alert and co-operative (Table VI) . Seven
subjects were vague and clouded, nine subjects were withdrawn and had poorcomprehension, none were semicomatose or comatose .
The state of consciousness improved rapidly within hours of thiamine treatment (F =79.24, p<0 .001) and continued to improve slowly (F = 6 .07, p<0.02) (Figure 8) . By
65

Q
8 2rn0EL
Tzm 10FemdI
6 6
Wood and Currie
discharge a significant improvement was observed, when only five subjects (16%) were stillvague and clouded.
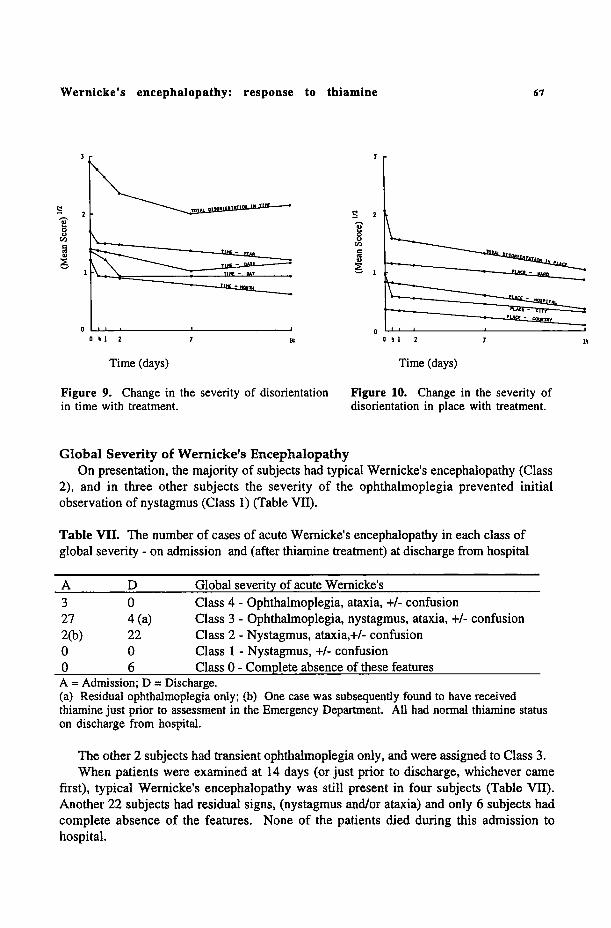
All subjects were severely disorientated in time on admission (Table VI) . The severityof disorientation in time improved over time (F= 13 .20, p<0.001) but improvement hadslowed by seven days (F=4 .97, p<0.05) and thereafter (F = 9 .60, p<0.01) (Figure 9). Eachtest of disorientation in time showed slow improvement (all p<0 .05). By discharge, mostsubjects were still disorientated in time and 18 subjects still did not know the day of theweek .
2
3
0 00 51
2
7
14
0 S1
2
7
to
Time (days)
Time (days)
Figure 7. Change in the severity of nystagmus
Figure 8 . Change in severity of thewith treatment.
state of consciousness (abnormality)with treatment .
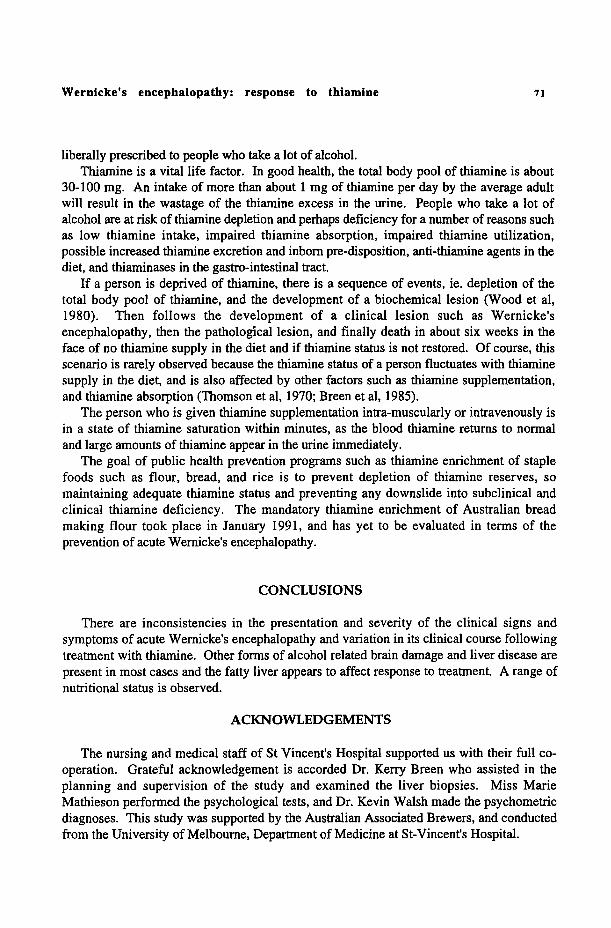
Twenty-seven of 32 subjects (34%) were severely disorientated in place on admission(Table VI).
Immediate improvement was observed within hours of treatment (F = 6 .14, p<0.02),and continued only slowly (F = 6.96, p<0.01) (Figure 10). The individual tests all showed
ement with time (all p<0 .02) .At discharge, 56% of subjects were still disorientated in place, but all knew which
country they were living in .
Wernicke's encephalopathy: response to thiamine
c
0U
UN
0 51
2
Time (days)
7 10
Time (days)
67
Figure 9 . Change in the severity of disorientation
Figure 10. Change in the severity ofin time with treatment .
disorientation in place with treatment .
Global Severity of Wernicke's EncephalopathyOn presentation, the majority of subjects had typical Wernicke's encephalopathy (Class
2), and in three other subjects the severity of the ophthalmoplegia prevented initialobservation of nystagmus (Class 1) (Table VII) .
Table VII . The number of cases of acute Wernicke's encephalopathy in each class ofglobal severity - on admission and (after thiamine treatment) at discharge from hospital
A = Admission ; D = Discharge .(a) Residual ophthalmoplegia only ; (b) One case was subsequently found to have receivedthiamine just prior to assessment in the Emergency Department . All had normal thiamine statuson discharge from hospital .
The other 2 subjects had transient ophthalmoplegia only, and were assigned to Class 3 .When patients were examined at 14 days (or just prior to discharge, whichever came
first), typical Wernicke's encephalopathy was still present in four subjects (Table VII) .Another 22 subjects had residual signs, (nystagmus and/or ataxia) and only 6 subjects hadcomplete absence of the features . None of the patients died during this admission tohospital .
A D Global severity of acute Wernicke's3 0 Class 4 - Ophthalmoplegia, ataxia, +/- confusion27 4 (a) Class 3 - Ophthalmoplegia, nystagmus, ataxia, +/- confusion2(b) 22 Class 2 - Nystagmus, ataxia,+/- confusion0 0 Class 1 - Nystagmus, +/- confusion0 6 Class 0 - Complete absence of these features

6 8
Wood and Currie
In the group, the global severity of Wernicke's encephalopathy showed mostimprovement in the first 12 hours following thiamine treatment, and then slowcontinuation of improvement (Figure 11). This improvement was most marked in patientswith lower levels of percent-relative body weight .
3
7
14
Time (days)0 %1
2
1205
1105
1002
755
602
Figure 11. Change in global severity (class) of Wernicke's encephalopathy in time withtreatment, effect of weight (percent relative body weight) . The heavy line represents all subjects .
Other Forms of Brain Damagea) Korsakoff's psychosis.
A diagnosis of Korsakoffs psychosis was shown on clinical examination in 56% (18 of32 subjects) (Table VIII) . The results of psychometric testing in 10 of these 32 subjectsrevealed the characteristic pattern of Korsakoffs psychosis in all 10 subjects, with alterationin all aspects of new learning (Memory Passage, Visual Reproduction and AssociatedLearning), preservation of immediate memory (in the form of both forwards and backwardsdigit repetition) and also long established stereotyped operations reflected by the MentalControl subtest. Three of 10 subjects also showed a characteristic pattern of dementia withpoor performance on all intellectual tests . For detailed results of the psychometric tests,refer to Wood et al, 1983 .
b) Brain atrophy and cerebellar dysfunctionIn all 23 subjects (100%) tested by CT scan, 21 (91%) showed evidence of cerebral
atrophy (Table VIII).Six subjects showed evidence of cerebellar atrophy on CT scan and cerebellar
dysfunction on clinical assessment was present in 12 of 23 subjects (52%) who could beassessed.

Wernicke's encephalopathy : response to thiamine
69
Table VIII. Frequency of abnormality in other manifestations of alcohol-related braindamage
DISCUSSION
In Australia, clinical thiamine deficiency has occurred mostly in people who drinkalcohol excessively, where thiamine deficiency has usually taken the form of Wernicke'sencephalopathy . Epidemiologically, it was estimated that there were about 500 cases ofWernicke's encephalopathy a year (based on the study of 662 000 people in Sydney) (Goldet al, 1985) . The most striking evidence of Wernicke's encephalopathy was pathological -2.8% of 4677 autopsies examined in Perth, and 2 .1% in Sydney (Harper and Kril, 1990) .
The diagnosis of Wernicke's is difficult (Wood et al, 1986), depending as it does on theskilled assessment of the eye signs - opthalmoplegia and nystagmus, also ataxia, and aglobal confusional state which varies in intensity . Neurologists have considered that adiagnosis of Wernicke's encephalopathy can only be made with the appearance of thespecific sign of opthalmoplegia which is unique and specific to the condition . Others nowdisagree, and consider that less rigid criterion should apply (Bowden, 1992; Price, 1991).
The evidence for thiamine deficiency being responsible for Wernicke's encephalopathy isbased on the associated thiamine deficiency observed (which is an incomplete association ina few cases) and on the rapid responsiveness of the ophthalmoplegia and some aspects of theglobal confusional state to massive doses of thiamine (Victor and Adams, 1953 ; Victor etal, 1971). There are inconsistencies in this theory, and there is variation in the presentationand severity of clinical signs and symptoms . Pathological brain lesions are also observedin the absence of a past history of clinical Wernicke's encephalopathy (also possiblyexplained by the difficulty of making the diagnosis) .
Number examined N (%)Brain CT 23Normal 0Cerebral atrophy 17(74)Cerebellar atrophy 2(9)Cerebral and cerebellar atrophy 4(17)
Clinical cerebellar dysfunction 23 12(53)Korsakoffs psychosisClinical diagnosis 32 18(56)Psychometric diagnosis last 10 10(100)
DementiaPsychometric diagnosis last 10 3(30)
Past history of neurological disordersEpilepsy 32 3(9)Head injury 32 1(3)Stroke 32 1(3)
CT = computerized tomography .

70
Wood and Currie
Many physicians and psychiatrists consider that the mental conditio
asKorsakoff's psychosis is due to thiamine deficiency, because it may follow an eWernicke's encephalopathy . Korsakoff's psychosis iusually associated with alcoholism, and may require institutiona i
To date, the aetiology of Korsakoffs psychosis is controversial, and there i onlyindirect evidence that thiamine deficiency is involved - particularly with respect to themental disturbance. The issue is very complex and includes the difficulty of diagnosing thedisorder, circumstantial evidence only for its link with Wernicke's encephalopathy, its rareoccurrence in the absence of alcoholism, its failure to correct with thiamine medication, itsvariable occurrence following reversal of Wernicke's encephalopathy, and its observationwithout preceding Wernicke's encephalopathy . These problems lead to uncertainty aboutthe role of thiamine deficiency in the aetiology of Korsakoff's psychosis, and uncertainty asto the efficacy of preventive methods .
In addition to the well recognised syndromes (Wernicke's encephalopathy and Korsakoffspsychosis) associated with high alcohol consumption, it has been increasingly recognisedthat heavy drinkers develop milder forms of brain damage (cognitive defects, short termmemory lapses, difficulty with planning) . Whether these relate to alcohol alone, previoushead injury, trauma, thiamine deficiency, or ageing is debated by researchers .
Nutrition is only one of multiple factors responsible for alcohol related brain damage .The only definite types of alcohol related brain damage known to be due to specificnutritional problems are acute Wernicke's encephalopathy (thiamine deficiency), and pellagra(niacin deficiency) . The most constant factor associated with alcohol related brain damageis excessive alcohol intake.
Variation in the clinical course of acute Wernicke's encephalopathy is observed . Oneprevious report utilized a simple scoring system (0 to 4) for the severity ofophthalmoplegia, nystagmus, ataxia and confusion (Phillips et ad., 1952). In this presentstudy, a more complex scoring system was devised to facilitate review of progress in theclinical signs and symptoms during treatment . Urgent treatment of patients with thiamineprevented external validation of this scoring system, but internal validation was performed .
This variation in the clinical course may be explained by the varying degrees ofpermanent brain damage, by different rates of regeneration of nervous tissue, by the processof withdrawal from alcohol, by the presence of multiple nutrient deficits, by the effect ofrecurrent episodes increasing the severity of the presenting signs and symptoms, and by
nknown aetiology, by age, and previous hypoxic episodes .In this present study, all patients had alcoholic liver disease and fatty liver appeared to be
important in response to treatment with thiamine . Other alcohol related brain damage waspresent, most were in the fourth/ fifth decade of life and had had an excessive consumptionof beer for more than 20 years (Wood et al, 1986) .
In Australian alcoholics, it is not appropriate to assume that they are all malnourished .This and other studies in this laboratory (Wood et al, 1992) indicate that people who abusealcohol have a range of nutritional status from overnutrition, through normal nutrition toprotein-energy malnutrition . Global malnutrition and micronutrient deficiencies are notinevitable, the latter particularly since multivitamin and trace element supplements are now
Wernicke's encephalopathy : response to thiamine
71
liberally prescribed to people who take a lot of alcohol .Thiamine is a vital life factor . In good health, the total body pool of thiamine is about
30-100 mg. An intake of more than about 1 mg of thiamine per day by the average adultwill result in the wastage of the thiamine excess in the urine . People who take a lot ofalcohol are at risk of thiamine depletion and perhaps deficiency for a number of reasons suchas low thiamine intake, impaired thiamine absorption, impaired thiamine utilization,possible increased thiamine excretion and inborn pre-disposition, anti-thiamine agents in thediet, and thiaminases in the gastro-intestinal tract .
If a person is deprived of thiamine, there is a sequence of events, ie . depletion of thetotal body pool of thiamine, and the development of a biochemical lesion (Wood et al,1980). Then follows the development of a clinical lesion such as Wernicke'sencephalopathy, then the pathological lesion, and finally death in about six weeks in theface of no thiamine supply in the diet and if thiamine status is not restored. Of course, thisscenario is rarely observed because the thiamine status of a person fluctuates with thiaminesupply in the diet, and is also affected by other factors such as thiamine supplementation,and thiamine absorption (Thomson et al, 1970 ; Breen et al, 1985) .
The person who is given thiamine supplementation intra-muscularly or intravenously isin a state of thiamine saturation within minutes, as the blood thiamine returns to normaland large amounts of thiamine appear in the urine immediately .
The goal of public health prevention programs such as thiamine enrichment of staplefoods such as flour, bread, and rice is to prevent depletion of thiamine reserves, somaintaining adequate thiamine status and preventing any downslide into subclinical andclinical thiamine deficiency . The mandatory thiamine enrichment of Australian breadmaking flour took place in January 1991, and has yet to be evaluated in terms of theprevention of acute Wernicke's encephalopathy .
CONCLUSIONS
There are inconsistencies in the presentation and severity of the clinical signs andsymptoms of acute Wernicke's encephalopathy and variation in its clinical course followingtreatment with thiamine. Other forms of alcohol related brain damage and liver disease arepresent in most cases and the fatty liver appears to affect response to treatment . A range ofnutritional status is observed .
ACKNOWLEDGEMENTS
The nursing and medical staff of St Vincent's Hospital supported us with their full co-operation. Grateful acknowledgement is accorded Dr . Kerry Breen who assisted in theplanning and supervision of the study and examined the liver biopsies. Miss MarieMathieson performed the psychological tests, and Dr . Kevin Walsh made the psychometricdiagnoses . This study was supported by the Australian Associated Brewers, and conductedfrom the University of Melbourne, Department of Medicine at St-Vincent's Hospital .

72
Wood and Currie
REFERENCES
Beutler, E . (1969a) . Effect of flavin compounds on glutathione reductase activity. In vivo and in vitro studies .J. Clin . Invest. 48:1957 .
Bender, E. (1969b) . Glutathione reductase : Stimulation in normal subjects by riboflavin supplementation .Science 165:613 .
Bosnes R .W. and Taussky H .H . (1945) . On the colorimetric determination of creatinine by the Jaffe reaction .J. Biol. Chem. 158:581 .
Bowden, S . (1992). Is there more than one neuropsychological disorder commonly associated with alcoholdependence. Drug & Alcohol Rev . 11 :299-304 .
Breen, K . Buttigieg, R. lossifidis, S. Lourensz, C, Wood, B . (1985) . Jejunal uptake of thiamin hydrochloride inmananfluence of alcoholism and alcohol . Amer. J. Clin. Nutr. 42:121-126.
Denson, K.W. and Bowers, E.F. (1961) . The determination of ascorbic acid in white blood cells . Clin. Sci.21:157 .
Dreyfus, P.M. (1979). The effects of alcohol on the nervous system . In Gastineau, C.F ., Darby, W.J ., Turner,T.B . (eds.) Fermented food beverages in nutrition, New York :Academic Press ., Ch . 22, p . 341 .
Garrow, J.S . (1974). Energy balance and obesity in man . London: Elsevier North Holland .Gold, J., Perdices, M ., Lardner, K et at. (1985) . The Wernicke-Korsakoff Project - the final report . Sydney :
School of Public Health and Tropical Medicine .Harper, C . and Kril, J. (1990) . The nature and progress of alcohol related brain injury . Proc of the 1990
Autumn School of Studies on Alcohol & Drugs, May 1990.Godding, R ., Rankin D, & Whelan G (eds .) .Melbourne: Dept. Comm. Med ., St Vincent's Hospital .
International Classification of Diseases (9th Revision) (1979) . Clinical modification, Volume 1 . Ann Arbor(Michigan): 1978 Commission on Professional and Hospital Activities .
Interdepartmental Committee on Nutrition for National Defence (1963) . Manual for Nutrition Surveys . 2ndedn. Bethesda, Maryland: National Institutes of Health, p.117, p .136.
Karmen, A., Wroblewski, F., and La Due, J.S . (1955). Transaminase activity in human blood. J. Clin. Invest.34 :126 .
Nie, N.H., Hadlai-Hull, C ., Jenkins, J.G . et at. (1970) . SPSS. Statistical Package for the Social Sciences . NewYork: McGraw - Hill .
Phillips, G .B ., Victor, M ., and Adams, R .D. (1952) . A study of the nutritional defect in Wernicke's syndrome :Effect of purified diet, thiamine and other vitamins on clinical manifestations . J. Clin. Invest . 31 :859-871 .
Price, J . (1991) . Neurological complications of alcohol usage . Drug & Alcohol Rev . 10:233-246.Stanulovic, M ., Miletic, D„ & Stock, A. (1967) . Die diagnostik des Vitamin B6-mangels auf grand der
bestimmung von erythrocytarer 1-aspartat :2-oxoglutarat amino transpherase (glutamat-oxalacetate-transaminase) and ihrer stimulation in vitro mit pyridoxal-5'-phosphate . Clin. Chim. Acta 17:353 .
Thomson, A .D ., Baker, H ., Leevy, C.M. (1970) . S-thiamin hydrochloride absorption in the malnourishedalcoholic patient. J. Lab. Clin. Med. 76: 34-44.
Victor, M., and Adams, R .D . (1953). The effect of alcohol on the nervous system . In Merritt, H . H. & Hare, C.C . (eds .) Metabolic and toxic diseases of the nervous system . Res . Publ. Ass . : nerv. ment. Dis ., Baltimore :The Williams & Wilkins Co ., Vol . 32, p.526.
Victor, M ., Adams, R.D., Collins, G .H. (1971) . The Wernicke-Korsakoff Syndrome . Oxford: BlackwellScientific Publications.
Wechsler, D. (1958) . The measurement and appraisal of adult intelligence . Baltimore, Maryland :Williams &Wilkins,
Wechsler D, Stone CP. (1945). Wechsler Memory Scale . New York, NY:The Psychological Corporation .WHO. (1975) . Manual of the international classification of diseases, '
d cause of death. Geneva,Switzerland, Vol. 1 ., p .156 .
Wood, B. and Penington, D.G. (1973). Biochemical assessment of thiamine st
adult Australians . Int . J.Vtt. Nutr. Res. 43 :12-19.
Wood, B., Currie, J ., Breen, K. (1986) . Wernicke's encephalopathy in a metropolitan hospital : A prospectivestudy of incidence, characteristics and outcome. Med. J. Aust. 1 :12-16 .
Wood, B., Goode, A., and Breen, K . (1988) . Biochemical studies of riboflavin, pyridoxine and Vitamin C statusin apparent health and in alcoholism. J. Food & Nutr. 45:9-12 .
Wood, B ., Nicholls, K.M ., Breen, K .J. (1992) . Nutritional status in alcoholism . J. Hum. Nutr. & Dieter. 5 :275-285 .
Wood, B., Breen, K., Walsh, K ., and Santamaria, J . (1983). Wernicke's encephalopathy in alcoholism :Towards a better perspective by comparison with a defined population group . Aust. Alcohol/ Drug Rev.2:74-80.
Wood, B ., Gijsbers, A ., Goode, A ., Davis, S ., Mulholland, J ., Breen, K. (1980) . Partial thiamin restriction inhuman volunteers . Am. J. Clin. Nutr. 33 : 848-861 .