presentazione standard di powerpoint - acute medicine€¦ · •interventional radiology...
TRANSCRIPT


VENOUS THROMBOEMBOLISM:
THE PRESENT
P.M. Mannucci
IRCCS Ca’ Granda Maggiore Policlinico
Hospital Foundation and University of Milano
DISCLOSURES
Honoraria for lectures as speaker or chair at
symposia organized by Bayer, Biotest, Grifols,
Kedrion, LFB, Novo Nordisk and Pfizer.
He also acted as scientific consultant for Bayer
and Kedrion

BACKGROUND
• Venous thromboembolism (VTE) is the third most
common cardiovascular disease (2-3/1000 each year)
• There is a markedly positive age gradient for its main
clinical manifestations: deep vein thrombosis (DVT)
and pulmonary embolism (PE)
• More patients die from PE than from breast and
prostate cancer, AIDS and traffic accidents combined
• Anticoagulant drugs have been extensively employed
as the mainstay of VTE treatment
PRINCIPLES OF ACUTE AND EXTENDED
VTE TREATMENT
TO
TOTO

THE BIG ISSUE OF VTE RECURRENCE
• After cessation of anticoagulants, 10% of
patients experience recurrent VTE within 12
months
• Up to 30% of patients experience recurrence
within 10 years
Prandoni et al. Haematologica 2007; 92: 199

Pharmacological
• Unfractionated heparin (UFH)
• Low molecular weight heparins (LMWHs)
• Fondaparinux
• Vitamin K antagonists (VKAs)
• Direct oral anticoagulants (DOACs) (dabigatran, rivaroxaban,
apixaban, edoxaban)
• Thrombolysis (only for hemodynamically severe PE)
Non pharmacological
• Surgery (embolectomy, thrombectomy)
• Interventional radiology (mechanical fragmentation,
thrombosuction)
• Vena cava filters (IVCFs)
VTE TREATMENT WEAPONS
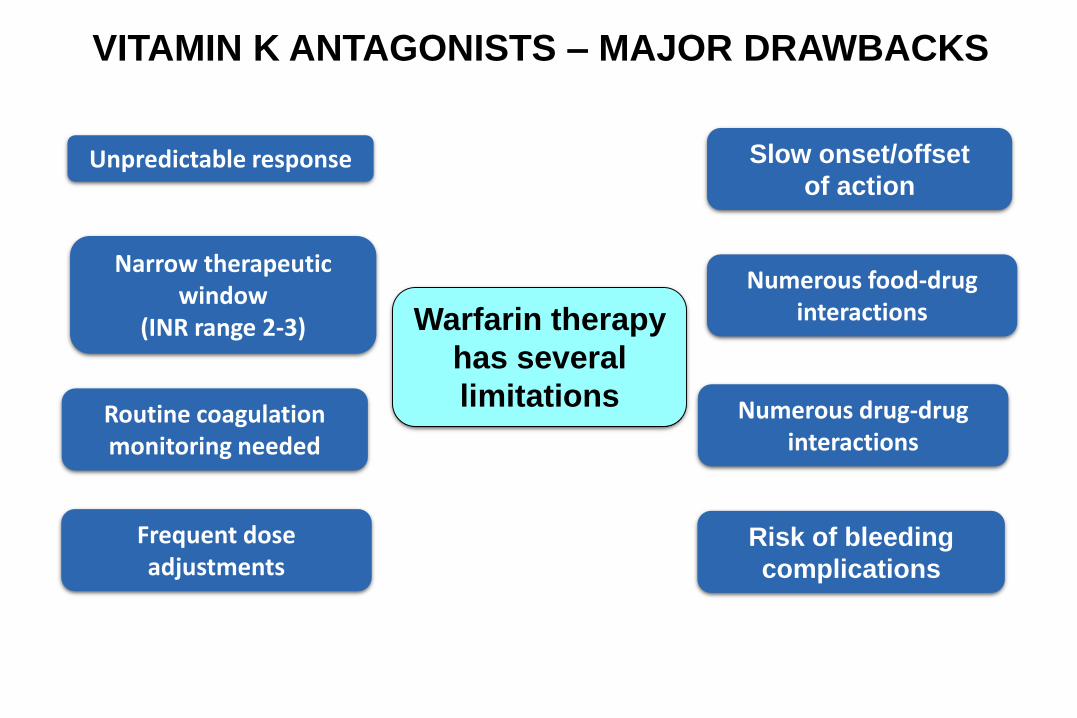
Unpredictable response
Routine coagulation monitoring needed
Slow onset/offset
of action
Risk of bleeding
complications
Warfarin therapy
has several
limitations Numerous drug-drug interactions
Numerous food-drug interactions
Frequent dose adjustments
Narrow therapeutic window
(INR range 2-3)
VITAMIN K ANTAGONISTS – MAJOR DRAWBACKS
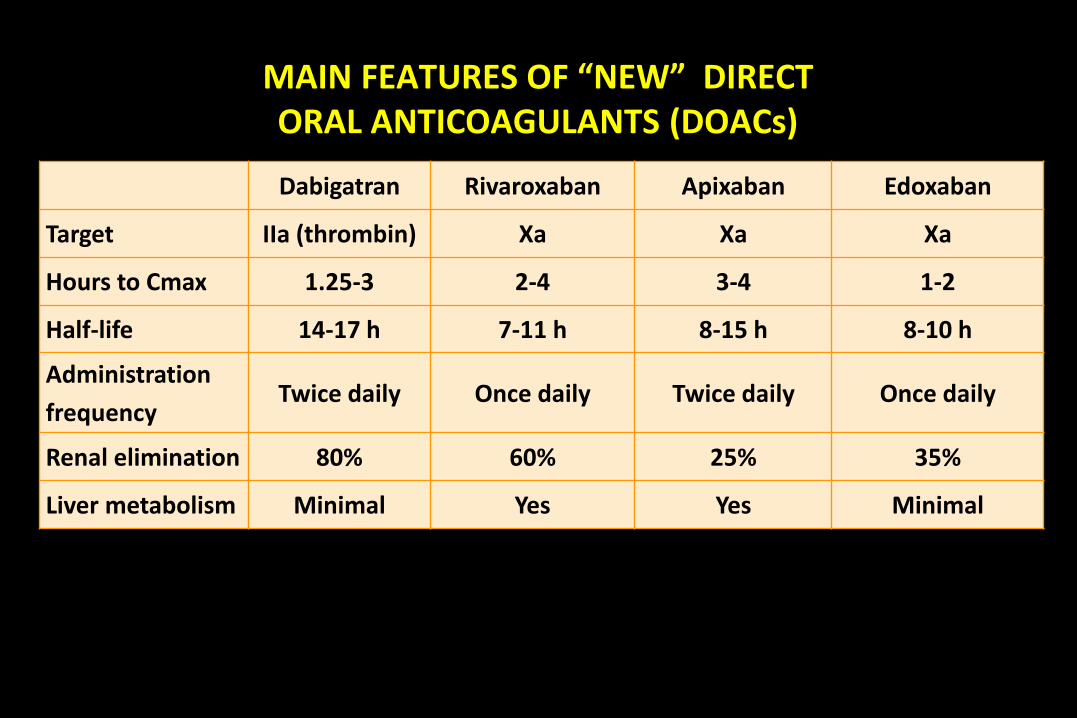
MAIN FEATURES OF “NEW” DIRECT ORAL ANTICOAGULANTS (DOACs)
Dabigatran Rivaroxaban Apixaban Edoxaban
Target IIa (thrombin) Xa Xa Xa
Hours to Cmax 1.25-3 2-4 3-4 1-2
Half-life 14-17 h 7-11 h 8-15 h 8-10 h
Administration
frequencyTwice daily Once daily Twice daily Once daily
Renal elimination 80% 60% 25% 35%
Liver metabolism Minimal Yes Yes Minimal
TREATMENT OF ACUTE VTE WITH DIRECT ORAL
ANTICOAGULANTS: POSSIBLE OPTIONS
• Initiation of therapy with standard parenteral
drugs (i.e. LMWHs) before the subsequent oral
use of VKAs or DOACs
• Initiation with an intensive regimen of DOACs
for the first few weeks (“single drug oral
approach”), followed by lower maintenance
doses of DOACs

EXTENDED TREATMENT OF VTE
• In some instances, anticoagulant therapy
is prolonged for more than the 3-6 months
of acute management
• This is named extended VTE treatment

SUMMARY OF THE MAIN PHASE III NON-INFERIORITY TRIALS REGARDING
ACUTE AND EXTENDED TREATMENT OF VENOUS THROMBO-EMBOLISM
Low-molecular-weight heparin has to be given upfront for the initiation of the treatment with dabigatran and edoxaban (A), while a
single-drug approach drives the treatment with rivaroxaban and apixaban both in the initiation and the early maintenance phases
(B).
Fontana P , EHJ 2014
+ LMWH
or
or

Main results (summarized by a meta-
analysis) of non-inferiority trials comparingVKA and DOACs for acute VTE treatment

PRIMARY EFFICACY END POINTS:
EARLY RECURRENT VTE OR VTE-RELATED DEATH
Van Es N, et al. Blood 2014
0.2
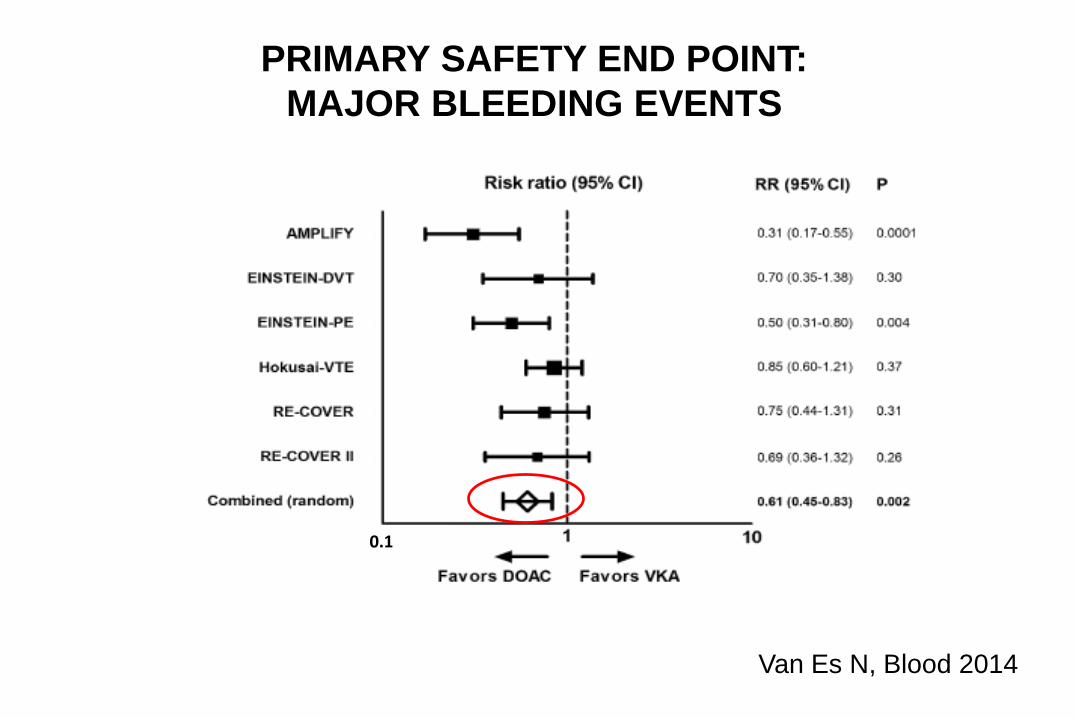
PRIMARY SAFETY END POINT:
MAJOR BLEEDING EVENTS
Van Es N, Blood 2014
0.1

INTRACRANIAL, MAJOR GASTROINTESTINAL, FATAL, AND
CLINICALLY RELEVANT NON MAJOR (CRNM) BLEEDING
Van Es N, Blood 2014
0.1
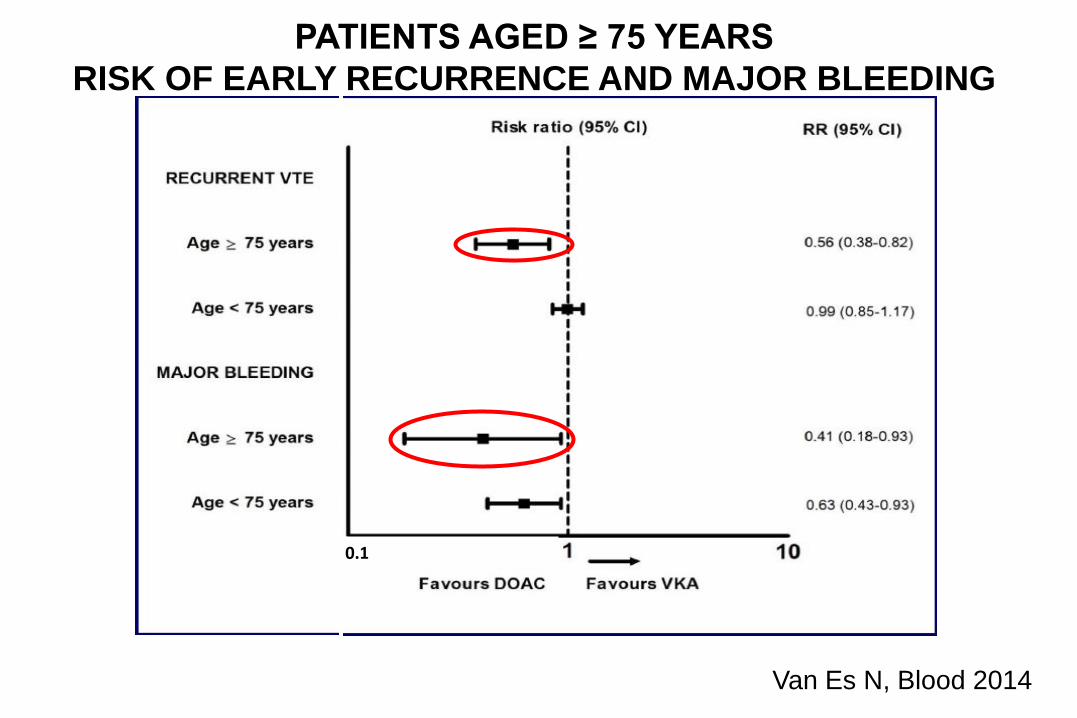
PATIENTS AGED ≥ 75 YEARS
RISK OF EARLY RECURRENCE AND MAJOR BLEEDING
Van Es N, Blood 2014
0.1
VTE RECURRENCE
• After cessation of anticoagulants, 10% of
patients experience recurrent VTE within
12 months
• Up to 30% of them experience recurrent
VTE within 10 years
• Hence, evaluation of extension therapies
is warranted after the acute phase
Prandoni et al. Haematologica 2007; 92: 199

Schulman S, et al. N Engl J Med 2009; Agnelli G, et al. N Engl J Med, 2013; Prins M, et al.
Thromb J, 2013; Hokusai VTE, N Engl J Med, 2013
EXTENSION STUDIES: RECURRENT VTE AND
RECURRENCE RELATED MORTALITY
1.750.50 0.75 1.00 1.25 1.50
Dabigatran
HR
(95% CI)
Rivaroxaban
Apixaban
P-value
(non-inferiority)
<0.001
<0.001
<0.001
Edoxaban <0.001
Favors NOAC Favors Warfarin

ACCP RECOMMENDATIONS
Kearon C, Chest 2016
• In patients with proximal DVT or pulmonary
embolism (PE), we recommend long-term (>3
months) anticoagulant therapy over no such
therapy (Grade 1B)
• In patients with DVT of the leg or PE and no cancer,
as long-term anticoagulant therapy we suggest
dabigatran, rivaroxaban, apixaban or edoxaban
over vitamin K antagonist (VKA) therapy (all Grade
2B)
Efficacy in PE patients?
DVT AND PE ARE THE SAME DISEASE
• Share the same risk factors
• Diagnostic approach similar (D dimer +
imaging)
• Prognosis comparable
• Treatment strategy identical (except for
massive PE with hemodynamic impairment)

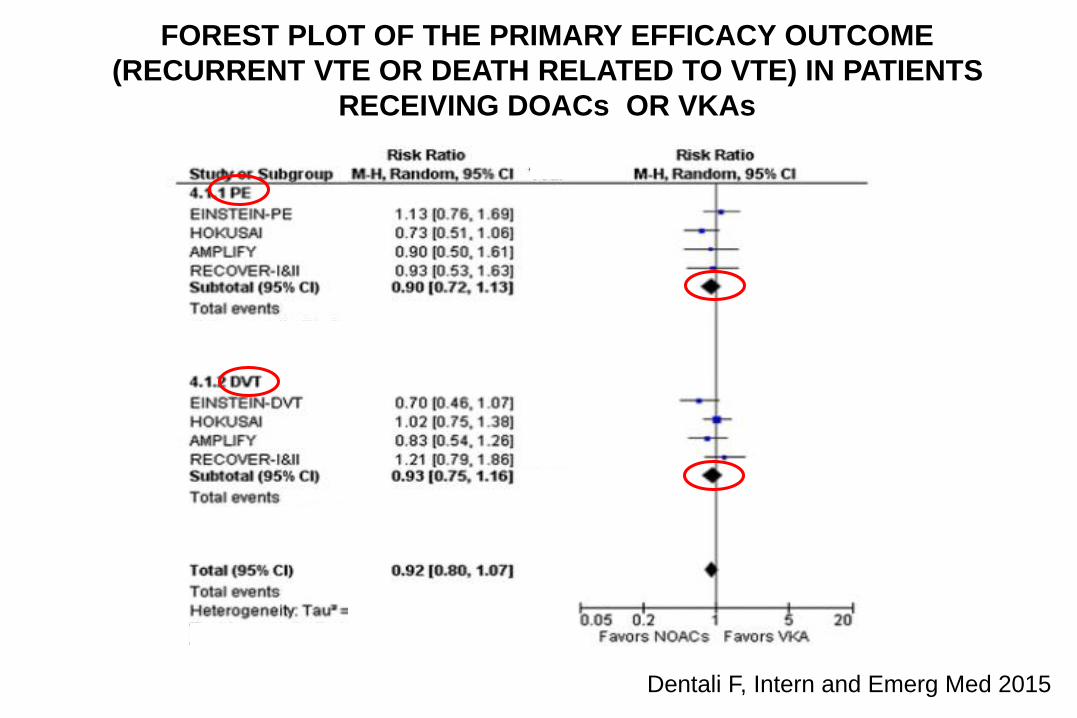
Dentali F, Intern and Emerg Med 2015
Dentali F, Intern and Emerg Med 2015
FOREST PLOT OF THE PRIMARY EFFICACY OUTCOME
(RECURRENT VTE OR DEATH RELATED TO VTE) IN PATIENTS
RECEIVING DOACs OR VKAs

DOAC UNCERTAINTIES
• Cancer
• Antiphospholipid syndrome
• Heparin induced thrombocytopenia
• Atypical sites
ACCP RECOMMENDATIONS FOR
CANCER-ASSOCIATED VTE
Kearon C, Chest 2016
• In patients with DVT of the leg or PE and
cancer, as long-term anticoagulant therapy we
suggest LMWH over VKA therapy (Grade 2B),
dabigatran (Grade 2C), rivaroxaban (Grade 2C),
apixaban (Grade 2C),or edoxaban (Grade 2C)

VTE TREATMENT:
TWO DECISION POINTS

Schulman S, Seminar TH 2015
The treatment of VTE can formally be divided
into two decision points, at which a choice
must be made regarding treatment regimen:
- at the time of diagnosis
- at 3 to 6 months from index event

Schulman S, TH 2015
AT THE TIME OF DIAGNOSIS
• Low-risk patients can be offered outpatient
treatment
• Today, this can be done with one of the
DOACs, but
• with a few exceptions for certain patient
subsets:
• UFH (severe renal failure)
• LMWH (active cancer)

Schulman S, TH 2015
THREE TO SIX MONTHS FROM ACUTE EVENT
Does one limit the anticoagulant treatment duration or continues
it indefinitely?
Extended treatment should be considered for:
- males (and females) with unprovoked VTE even after the first
event
- patients with recurrent VTE or severe forms of thrombophilia
(antithrombin deficiency, homozygosity for factor V Leiden,
or combined defects)
- patients with massive PE
This choice has become more attractive with the increased safety
and convenience of the direct oral anticoagulants

Conclusions

• All the DOACs are at least as efficacious of
warfarin
• They can be used with no laboratory
monitoring
• All the DOACs have a smaller risk of severe
bleeding (particularly intracranial) than
warfarin

• DOACs simplify anticoagulant therapy in
VTE and cause less bleeding than warfarin
• The personalized choice of each DOAC for
each patient should aim to maximize
advantages and minimize risks

MAIN FEATURES OF “NEW” DIRECT ORAL ANTICOAGULANTS (DOACs)
Dabigatran Rivaroxaban Apixaban Edoxaban
Target IIa (thrombin) Xa Xa Xa
Hours to Cmax 1.25-3 2-4 3-4 1-2
Half-life 14-17 h 7-11 h 8-15 h 8-10 h
Administration
frequencyTwice daily Once daily Twice daily Once daily
Renal elimination 80% 60% 25% 35%
Liver metabolism Minimal Yes Yes Minimal

ANTIDOTES
• Antidotes are seldom needed (except for life
threatening bleeding episodes), owing to the
very short half-life of all DOACs
• A monoclonal antibody (idarucizumab) is
licensed as a specific reversal agent for
dabigatran
• An antidote for all the factor Xa inhibitors
(rivaroxaban, apixaban, edoxaban) will be soon
available (Andexanet)

Thank you for listening


DIFFERENCES AND SIMILARITIES
• Hokusai/Recover I/II used initially low
molecular weight heparins before edoxaban or
dabigatran
• Mostly DVT and PE combined
• Duration of treatment/follow-up variable, but:
• Comparable definition of efficacy and safety
outcomes

REAL-LIFE POST-MARKETING
OBSERVATIONAL STUDIES
• XALIA compared in 5142 patients the efficacy
and safety of rivaroxaban compared with VKA
• No difference between rivaroxaban and VKA in
the acute and extension phase of treatment
Lancet Hematology. 2016; 3:e12-21

Caratteristiche Scelta del farmaco Razionale
Interferenza con altrifarmaci
Dabigatran(edoxaban)
Minore interferenza con altri farmaci
Terapia a lungo terminein pazienti ad alto rischio
Dabigatran Studio di confronto con warfarina
CrCl 30-50 ml/min Inibitori del XaMeno condizionati dall’IR neiconfronti di dabigatran
Dispepsia o disordinidelle prime vie digestive
Inibitori del XaDispepsia con dabigatran fino al 10% dei pazienti
Significativa CHD Inibitori del Xa Debole segnale con dabigatran
Terapia tutta orale Apixaban o rivaroxabanNon richiedono iniziale terapia parenterale
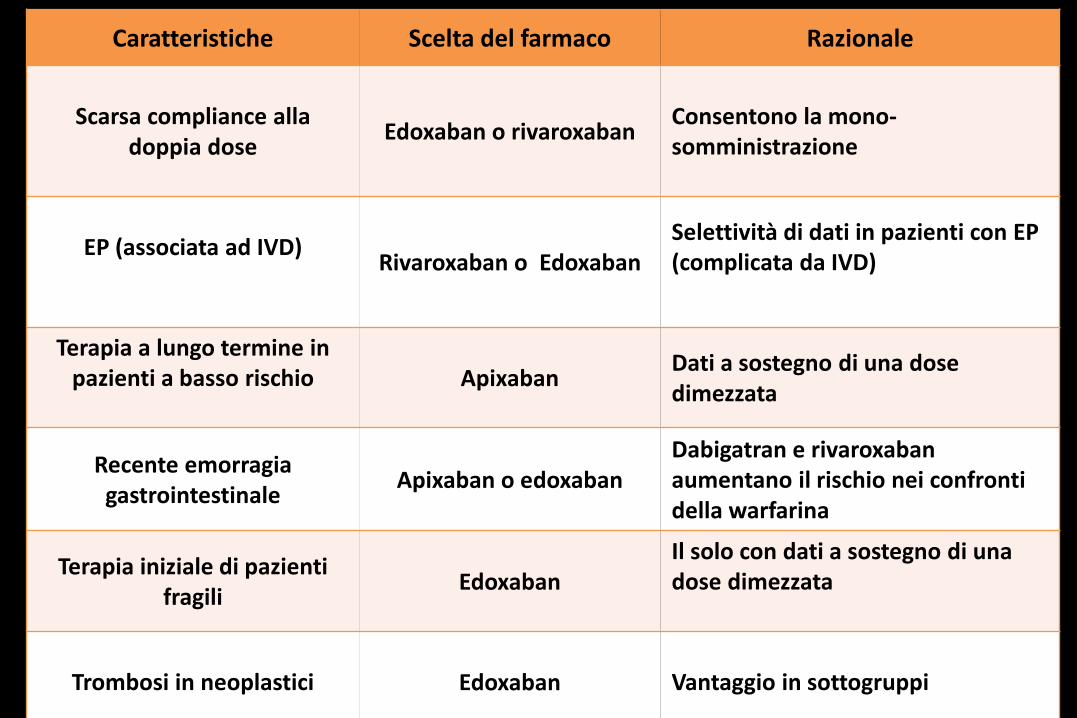
Caratteristiche Scelta del farmaco Razionale
Scarsa compliance alladoppia dose
Edoxaban o rivaroxabanConsentono la mono-somministrazione
EP (associata ad IVD)Rivaroxaban o Edoxaban
Selettività di dati in pazienti con EP (complicata da IVD)
Terapia a lungo termine in pazienti a basso rischio Apixaban
Dati a sostegno di una dose dimezzata
Recente emorragiagastrointestinale
Apixaban o edoxabanDabigatran e rivaroxaban aumentano il rischio nei confrontidella warfarina
Terapia iniziale di pazientifragili
EdoxabanIl solo con dati a sostegno di unadose dimezzata
Trombosi in neoplastici Edoxaban Vantaggio in sottogruppi

EINSTEIN_
EXT1
AMPLIFY_EXT2 RE-MEDY*3 RE-SONATE3
Study drug Rivaroxaban Apixaban Dabigatran Dabigatran
Study design Double-blind Double-blind Double-blind Double-blind
Comparator
drug
Placebo Placebo Warfarin Placebo
Dose 20 mg OD 2,5 mg BID
5 mg BID
150 mg BID 150 mg BID
Randomized
population
1,197 2,482 2,866 1,353
Treatment
duration
6 or 12 months 12 months 6-36 months 6 months
VTE: DESIGN OF DOAC EXTENSION STUDIES
1. Einstein Investigators N Engl J Med 2010;363:2499-510; 2. Agnelli et al. N Engl J Med 2013;368:699-708;
3. Schulman et al. N Engl J Med 2013;368:709-18.

43
Kaplan–Meier: Non-fatal and fatal VTE
100
80
60
40
20
0
0 1 2 3 4 5 6 7 8 9 10 11 12
Cum
ula
tive e
vent
rate
(%
)
Months
1211109876543210
0
1
2
3
4
5
6
7
8
9
10
Baseline
840
813
826
Month 3
836
807
796
Month 6
825
799
768
Month 9
818
791
743
Month 12
533
513
471
No. at risk
Apixaban 2.5 mg
Apixaban 5 mg
Placebo
Placebo
Apixaban 2.5 mg
Apixaban 5 mg
Cum
ula
tive e
vent
rate
(%
)

Benefits of DOACs vs warfarin in patients with PE have been demonstrated across Phase III studies
Study Primary endpointHR*/RR†
(95%CI)
RECOVER 1+2 (Index PE)Recurrent symptomatic VTE or fatal VTE
1.09 (0.76–
1.57)
EINSTEIN-PE Recurrent VTE1.12*
(0.75–1.68)
AMPLIFY (Index PE)Recurrent VTE / VTE-related death
0.90†
(0.50–1.61)
HOKUSAI (Index PE) Recurrent VTE0.73*
(0.50–1.06)
HOKUSAI (Severe PE)(ProBNP ≥500 pg/mL)
Recurrent VTE0.52*
(0.28–0.98)
EINSTEIN-PE Investigators N Engl J Med 2012;366:1287–97; Agnelli G et al. N Engl J Med 2013;369:799–808;Hokusai-VTE Investigators N Engl J Med 2013;369:1406–15

TREATMENT RECOMMENDATIONS FOR PE PATIENTS WITHOUT SHOCK OR HYPOTENSION (INTERMEDIATE OR LOW-RISK)
Recommendations Class Level
Anticoagulation: direct oral anticoagulants
As an alternative to the combination of parenteral anticoagulation and a VKA, anticoagulation with rivaroxaban (15 mg twice daily for 3 weeks, followed by 20 mg once daily) is recommended
I B
As an alternative to the combination of parenteral anticoagulation and a VKA, anticoagulation with apixaban (10 mg twice daily for 7 days, followed by 5 mg twice daily) is recommended
I B
As an alternative to VKA treatment, administration of dabigatran (150 mg twice daily, or 110 mg twice daily for patients >80 years of age or those under concomitant verapamil treatment) is recommended following acute phase parenteral anticoagulation
I B
As an alternative to VKA treatment, administration of edoxaban* is recommended following acute-phase parenteral anticoagulation I B
New oral anticoagulants (rivaroxaban, apixaban, dabigatran, edoxaban) are not recommended in patients with severe renal impairment III A
*Edoxaban is currently subject to regulatory review for the treatment of venous thromboembolism in the European Union
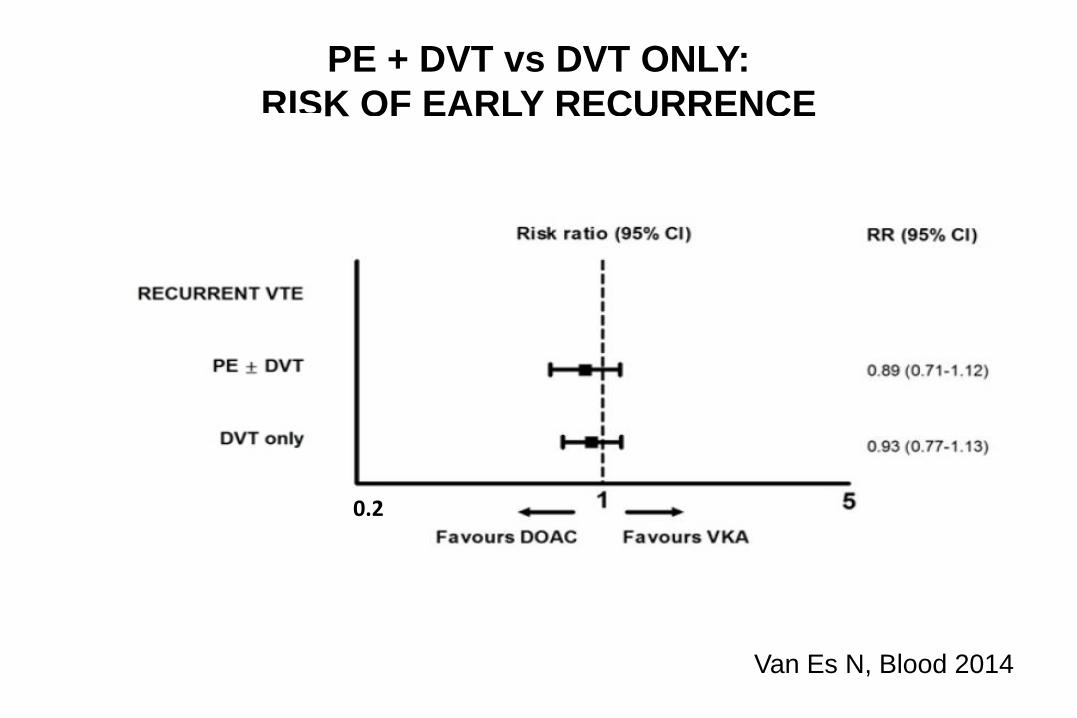
PE + DVT vs DVT ONLY:
RISK OF EARLY RECURRENCE
Van Es N, Blood 2014
0.2