prevalence of causes of primary caesarean section ...utq.edu.iq/magazines/pdfmed2017/1.pdf ·...
TRANSCRIPT

Ministry of Higher Education and Scientific Research
University of Thi-Qar
College of Medicine
Department of Obstetrics and Gynecology
Prevalence of Causes of Primary
Caesarean Section Operation which
did in Al-Habubi Hospital From
January to March at 2017
By
Haider Issa Ahmed Madhi Hasaneen Faisal
Supervised By
Dr. Nadia Al-Asady
2016 – 2017

Abstract
Background : Caesarean section is surgery to deliver a baby. The
baby is taken out through the mother's abdomen , may be is emergency
or elective procedure according to state of mother and her fetus.
Cesarean delivery has become a commonly used measure for delivery of
the fetus. In the recent years incidence of Cesarean section (CS) has
increased dramatically with massive pubic interest. It is called "Primary
Cesarean section" when it is performed for the first time on a pregnant
woman.
Aim : to estimate the causes of 1st C-section in Al-Nasiriyah in Al-
Habubi hospital in 1st 3 months of 2017
Methods : this was across sectional study. The data was taken
from recorded files of patients who were made the operation in
Habubi hospital in Al-Nasiriyah city in the (January , February ,
march ) of 2017
Result : A total of 606 cases the major findings of the study were as
follows: Overall cesarean section rate was 46 per cent and among
them 31 per cent were primary cesarean section. The median age
group of patients being operated was 20 to 25 years. The main
indications were malpresentation fetal distress , pre-eclampsia and
other.
Introduction
History:
There are three theories about the origin of the name.
The name is said to derive from a Roman legal code called Lex
Caesarea, which allegedly contained a law prescribing that the
baby be cut out of its mother’s womb in the case that she dies
before giving birth.
The derivation of the name is also often attributed to an ancient
story, told in the first century AD by Pliny the Elder, who claimed
that an ancestor of Caesar was
delivered in this manner.
An alternative etymology suggests that the procedure’s name
derives from the Latin verb caedere, to cut, in which case the term
‘Caesarean section’ is redundant.
The 1st recorded incidence of a woman surviving a C-section was in
1500, in Switzerland: Jakob Nufer, a pig gelder, is supposed to have
performed the operation on his wife after a prolonged labour.
For most of the time since the 16th century, the procedure had a high
mortality. A C-section was considered an extreme measure, performed
only when the mother was already dead or considered to be beyond
help. In Great Britain and Ireland, the mortality
rate in 1865 was 85 per cent.
Key steps in reducing mortality were:
adherence to principles of asepsis;
• the introduction of uterine suturing by Max Sänger in 1882;
• extraperitoneal C-section and then moving to low transverse incision
(Pfannenstiel)
• anaesthesia advances
• blood transfusion
• antibiotics.

Definition
A Caesarean section, also known as C-section or Caesar, is a surgical
procedure in which incisions are made through a mother’s abdomen
(laparotomy) and uterus (hysterotomy) to deliver one or more babies.
Prevalence
In 2010, there were a total of 128 million births in the world, and of
those 18.5 million (14.45%) were delivered by C-section.
In England, rates of C-section have increased from 9% of births in 1980
to 24.8% in 2010.
In 2014, 32.2% of women who gave birth in the US did so by cesarean
delivery
The incidence of CS varies between 10% and 25% in most developed
countries.
The principal aims must be to ensure that those women and babies who
need delivery by C-section are so delivered and that those who do not
are saved from unnecessary intervention.
Types of Caesarean section
The type of CS is based on the type of incision of the uterus.
Lower uterine segment incision
is used in over 95 per cent of Caesarean deliveries due to ease of repair,
reduced blood loss and low incidence of dehiscence or rupture in
subsequent pregnancies. The loose reflection of vesico-uterine serosa
overlying the uterus is divided laterally, the underlying lower uterine
segment is refl ected with blunt dissection, the developed bladder fl ap
is retracted and the lower uterine segment is opened in a transverse
plane for a distance of 1–2 cm; the incision is extended laterally to allow
delivery of the fetus without extension into the broad ligament or
uterine vessels.
Midline vertical incision
The midline vertical incision could be in the lower or upper segment of
the uterus. Commonly, it starts in the lower segment as a small
buttonhole incision until the uterine cavity is reached and is extended

upwards. The midline incision is reserved for specific indications because
of the difficulty in making the incision, increased blood loss, inadequate
approximation at closure, increased postoperative morbidity, and
inability to offer a trial of vaginal delivery in the next pregnancy due to
possible higher incidence of scar rupture. A midline approach is used
when the lower segment approach is difficult because of fibroids or
anterior placenta praevia with large vessels in the lower segment. Other
indications include preterm breech with poorly formed lower segment,
impacted transverse lie with ruptured membranes or transverse lie with
congenital anomaly of the uterus. An extreme example is peri-mortem
CS.
Factors that may contribute to an increase in the rates
of C-section
1- Inaccurate dating of the pregnancy particularly when the
date of the last menstrual period is uncertain. Such accurate
dating reduces the anxiety experienced by many women when
they pass their ‘expected date of delivery’ and also reduces the
requests for ‘early’ induction of labour.
2- Fetal monitoring. electronic fetal monitoring (EFM) was
universally implemented without the appropriate trials. This has
resulted in an increase
in the incidence of C-section without demonstrable
improvement in perinatal outcome. Current recommendations
are for intermittent auscultation to be performed in all ‘low
risk pregnancies’, with continuous EFM in those pregnancies
deemed to be ‘high risk’.
3- Macrosomia Although there is evidence to suggest that
birthweights are rising in developed countries, the amount (30 g
over 12 years) is unlikely to be of any biological significance.
Unfortunately, both clinical and ultrasonographic estimations of
fetal size are prone to inaccuracy (especially in large term
infants), and unnecessary inductions of labour and Caesarean
deliveries are performed as a consequence.

4- Maternal request. Controversy exists regarding elective
cesarean delivery on maternal request (CDMR). The 2013
American College of Obstetricians and Gynecologists (ACOG)
Committee on Obstetric Practice and 2006 National Institutes of
Health (NIH) consensus committee determined that the
evidence supporting this concept was not conclusive and that
more research is needed.
Both committees provided the following recommendations
regarding CDMR :
Unless there are maternal or fetal indications for cesarean
delivery, vaginal delivery should be recommended
CDMR should not be performed before 39 weeks’ gestation
without verifying fetal lung maturity (due to a potential risk
of respiratory problems for the baby)
CDMR is not recommended for women who want more
children (due to the increased risk for placenta previa/accreta
and gravid hysterectomy with each cesarean delivery)
The inavailability of effective analgesia should not be a
determinant for CDMR
The NIH consensus panel on CDMR also noted the following [10] :
CDMR has a potential benefit of decreased risk of
hemorrhage for the mother and decreased risk of birth
injuries for the baby
CDMR requires individualized counseling by the
practitioner of the potential risks and benefits of both vaginal
and cesarean delivery
Indications
There are many different reasons for performing a delivery by C-section.
The four major indications accounting for greater than 70 per cent of
operations are:
1. Previous C-section
2. Dystocia
3. Malpresentation
4. Suspected acute fetal compromise.
Other indications, such as( multifetal pregnancy, abruptio placenta,
placenta praevia, fetal disease and maternal disease) are less common.
No list can be truly comprehensive and whatever the indication, the
overriding principle is that whenever the risk to the mother and/or the
fetus from vaginal delivery exceeds that from operative intervention, a
C-section should be undertaken
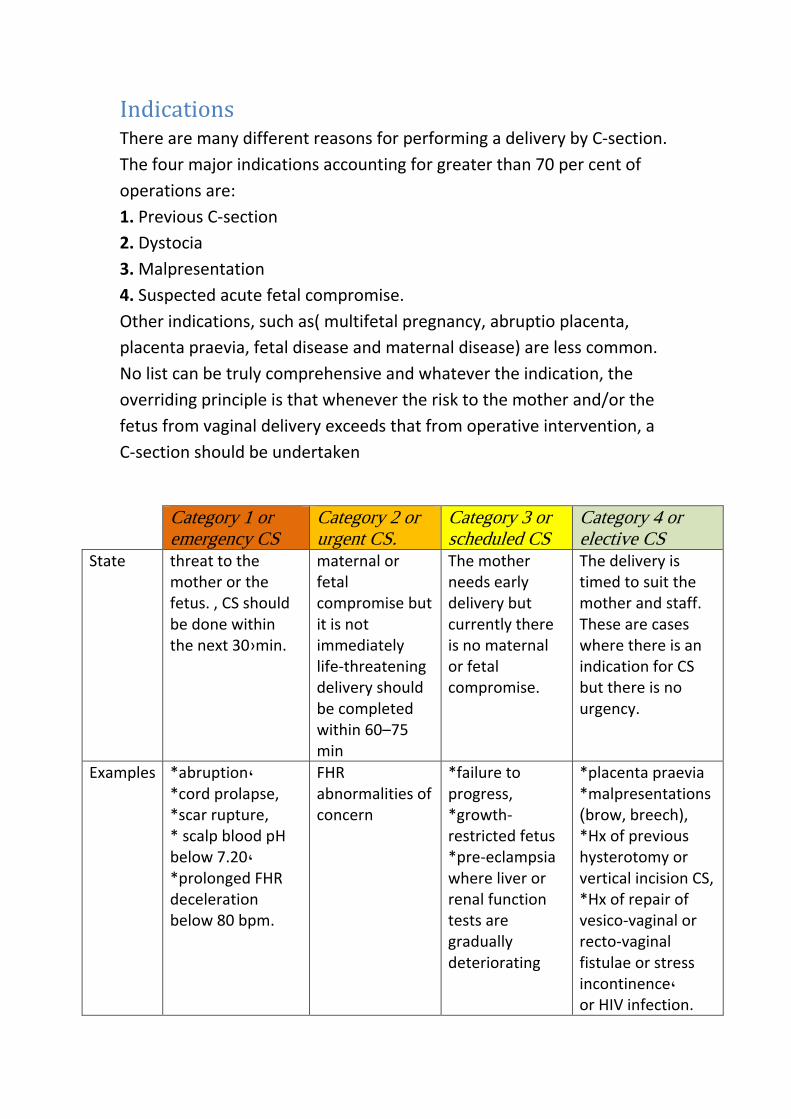
Category 1 or emergency CS
Category 2 or urgent CS.
Category 3 or scheduled CS
Category 4 or elective CS
State threat to the mother or the fetus. , CS should be done within the next 30›min.
maternal or fetal compromise but it is not immediately life-threatening delivery should be completed within 60–75 min
The mother needs early delivery but currently there is no maternal or fetal compromise.
The delivery is timed to suit the mother and staff. These are cases where there is an indication for CS but there is no urgency.
Examples *abruption, *cord prolapse, *scar rupture, * scalp blood pH below 7.20, *prolonged FHR deceleration below 80 bpm.
FHR abnormalities of concern
*failure to progress, *growth-restricted fetus *pre-eclampsia where liver or renal function tests are gradually deteriorating
*placenta praevia *malpresentations )brow, breech), *Hx of previous hysterotomy or vertical incision CS, *Hx of repair of vesico-vaginal or recto-vaginal fistulae or stress incontinence, or HIV infection.
Morbidity and mortality
Confidential Enquiries into Maternal Deaths have enabled the risks
associated with different methods of delivery to be analyzed; case
fatality rate for all Caesarean sections is five times that for vaginal
delivery, although for elective Caesarean section the difference does not
reach statistical significance. Some maternal deaths following Caesarean
section are not attributable to the procedure itself, but rather to medical
or obstetric disorders that lead to the decision to deliver using this
approach. Many women who deliver vaginally encounter the same
problems.
Complications
C-section is a major abdominal surgical procedure and carries significant
risks.
Intraoperative complications
1- Bowel damage may occur during a repeat procedure or if adhesions
are present from previous surgery.
2-Caesarean hysterectomy The most common indication for Caesarean
hysterectomy is uncontrollable maternal haemorrhage; The most
important risk factor for emergency postpartum hysterectomy is a
previous C-section – especially when the placenta overlies the old scar,
increasing the risks of placenta
accrete.
Other indications for hysterectomy are( atony, uterine rupture,
extension of a transverse uterine incision and fibroids preventing uterine
closure and haemostasis).
3-Haemorrhage may be a consequence of damage to the uterine
vessels, or may be incidental as a consequence of uterine atony or
placenta praevia. In patients with an anticipated high risk of
haemorrhage.
4-Placenta praevia The proportion of patients with a placenta praevia
increases almost linearly after each previous C-section, and as the risks
of such a complication increases with increasing parity, future

reproductive intentions are very relevant to any individual decision for
operative delivery.
5-Urinary tract damage The risk of bladder injury is increased after
prolonged labours where the bladder is displaced caudally, after
previous C-section where scarring obliterates the vesicouterine space, or
where a vertical extension to the uterine incision has occurred
Post-operative complications
1-Infection and endometritis
Women undergoing C-section have a 5–20-fold greater risk of an
infectious complication when compared with a vaginal delivery.
Complications include fever, wound infection, endometritis,
bacteraemia and urinary tract infection. Other common causes of
postoperative fever include haematoma, atelectasis and deep vein
thrombosis.
2-Psychological
All difficult deliveries carry increased maternal psychological and
physical morbidity. The compromised postpartum psychological
functioning in women
delivered by C-section may be secondary to delayed contact with the
baby; a factor that in most cases should be amenable to remedy.

Methodology
Data from Habubi hospital in Al-Nasiriyah city Survey were analyzed for
pregnant females did operation in this hospital .
Site and Study Design: A cross-sectional descriptive study was
conducted on a conveniently selected 1st C-section.
Data sources: The data was taken from Habubi hospital in Al-Nasiriyah
city for all patients who did her 1st C-section in this hospital from
(January to march ) of 2017.
The information was taken from files of patients which documented and
recorded in the statistic unite.
Sample size: All cases was taken during these 3 months was 189 case of
1st C-section from 606 case of all type of C-section was do it.
Result From (January to march ) of 2017 , about 1923 case of delivery.
About 1317 case was normal vaginal delivery (68.48 per
cent).
And about 606 case was C-section (31.51 per cent).
The number cases of 1st C-section was 189 case ( 31.18 per
cent from case of C-section , and 9.82 from total delivery) .
Table 1 : Number percentage of each type of delivery in this study.
Normal vaginal delivery Cesearian section 1st C-section Total No.
Count percent Count percent Count percent 1923
1317 68.48% 417 21.68% 189 9.82%

Fig. 1 percentage of each type of delivery.
The causes of primary C-section were variable and contribute between
many reason ; ex. (were malpresentation fetal distress , pre-eclampsia
and other)
Table 2 : percentage of each case from the total number of primary C-
section in this study.
S Cause Count Percentage 1 Malpresentation 39 20.6 %
2 Failure to progress 34 17.9 % 3 cephalopelvic disproportion 33 17.4 %
4 Fetal distress 21 11.11 %
5 Post date 12 6.3 % 6 Sever Oligohydramnios 12 6.3 %
7 Prolong rupture membrane 9 4.7 % 8 Premature labor 9 4.7 %
9 Pre-eclampsia 7 3.7 %
10 Patient preference 4 2.1 % 11 Placenta previa 4 2.1 %
12 Polyhydramnios 3 1.58 % 13 Precious baby 2 1.05 %
Normal vaginal delivery
68%
C-section not 1st
22%
1st C-section 10%
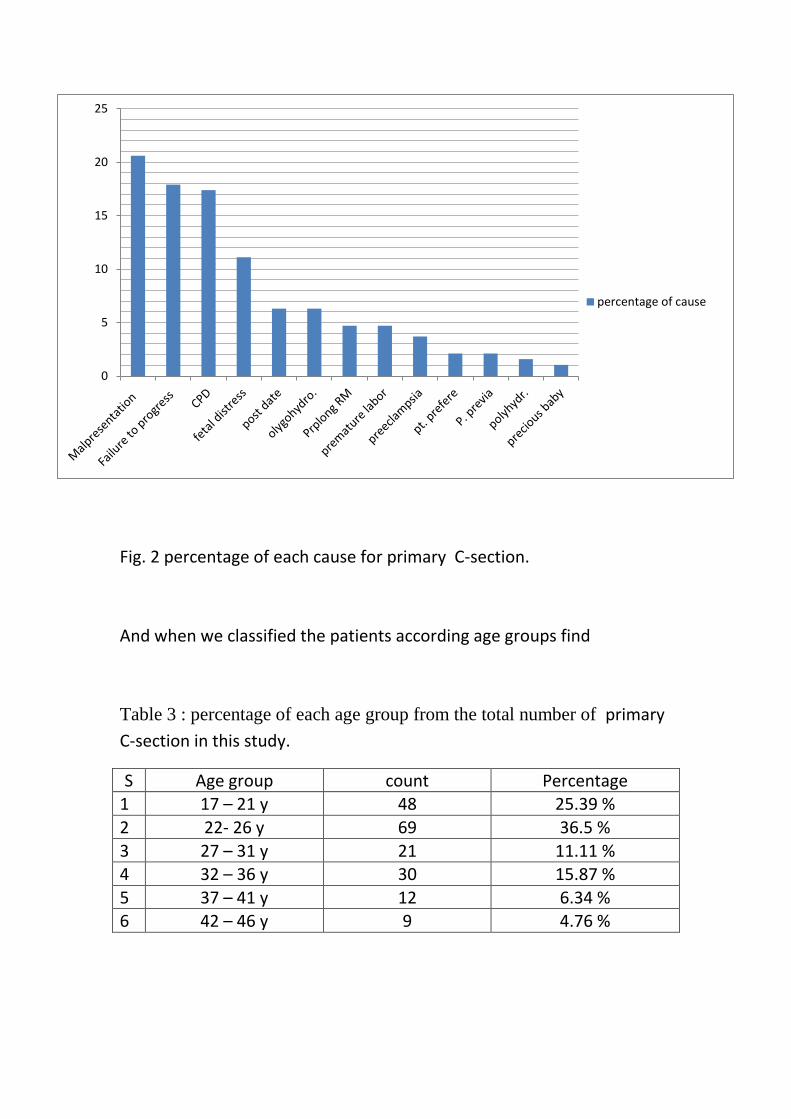
Fig. 2 percentage of each cause for primary C-section.
And when we classified the patients according age groups find
Table 3 : percentage of each age group from the total number of primary
C-section in this study.
S Age group count Percentage 1 17 – 21 y 48 25.39 %
2 22- 26 y 69 36.5 %
3 27 – 31 y 21 11.11 % 4 32 – 36 y 30 15.87 %
5 37 – 41 y 12 6.34 % 6 42 – 46 y 9 4.76 %
0
5
10
15
20
25
percentage of cause

Fig. 3 : percentage of each age group from the total number of primary
C-section in this study.
Discussion The results of this study that do to estimate the percentage of each cause
for the patient did a primary C-section in from Habubi hospital in Al-
Nasiriyah city for all patients who did her 1st C-section in this hospital
from (January to march ) of 2017.
We found the common causes for the primary C-section are
(malpresentation , failure to progress and CPD) and the most age group
of this patients are teenage and 3rd decade reproductive women.
The study compare with same study made in Iran ( A survey on causes of
cesarean sections performed at theuniversity hospitals of Niknafs and
Ali-Ibn Abi Talib of Rafsanjan, Iran, in the second trimester of 2014)
But the percentage of C-section in our study less than it , because the
difference in the economic state and education level.
17-21 y 22-26 y 27-31 y 32-36 y 37-41 y 42-46 y
25.39 1سلسلة 36.5 11.11 15.87 6.34 4.76
0
5
10
15
20
25
30
35
40
per
cen
t o
f gr
ou
ps
Limitation We find many limitation and difficulties in the preparation this stydy
some of these :
1- In adequate information in the files of patients which did operation.
2- The study depend on the diagnosis find it in the file of patients.
3- Difficulty in obtaining information and routine administrative
procedures
4- The cost of financial fees for the purpose of the license in the
preparation of the study
Recommendation 1- Health awareness and education about the advantage of normal vaginal
delivery.
2- Health awareness about the risk and suspected complication of the C-section.
3- Encourage visit to pregnant care centers(antenatal care program).
4- Taxation of Caesarean deliveries without indication for caesarean.
5- Encourage the female and pregnant women to do sport and decrease obesity.
Conclusion Considering drastic causes of caesarean in our country and its upward
procedure on one hand, and its side effects on mothers, infants,
treatment-health system and generally social health, health system
managers, planners and other qualified members of this field, should
design and administrate effective interferes and plans in reducing
caesarean amount and promoting normal vaginal delivery. Considering
the key reasons for caesarean prevalence including: previous caesarean,
fear of pain in normal vaginal delivery and doctors recommendation,
Providing psychological interventions and education, Increase the quality
of vaginal delivery services, appropriate culture, providing solutions and
legislation which are preventing doctors from personal

Reference 1- OBSTETRICS by Ten Teachers 19
th edition
2- Dewhurst’s Textbook of Obstetrics & Gynaecology 8th
edition
3- Open Journal of Obstetrics and Gynecology
Vol.3 No.7(2013), Article ID:37028,9
4- Medscape website
5- BMJ (British medicine journal) website
6- Study: A survey on causes of cesarean sections performed at
theuniversity hospitals of Niknafs and Ali-Ibn Abi Talib of Rafsanjan, Iran, in the second trimester of 2014