prevention, diagnosis and management of … · 2016-03-08 · this latest iipp booklet on the...
TRANSCRIPT

PREVENTION DIAGNOSIS ANDMANAGEMENT OF COLORECTAL
ANASTOMOTIC LEAKAGE
March 2016
wwwasgbiorguk wwwacpgbiorguk
1
ISSUES INPROFESSIONAL PRACTICE
PREVENTION DIAGNOSIS ANDMANAGEMENT OF COLORECTAL
ANASTOMOTIC LEAKAGE
AUTHORSF D McDermott S Arora J Smith R J C Steele
G L Carlson and D C Winter(on behalf of the joint ASGBIACPGBIAnastomotic Leakage Working Group)
PUBLICATION DATEMarch 2016
PUBLISHED BYAssociation of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
SPONSORED BYAN EDUCATIONAL GRANT FROM
No part of this publication may be reproduced stored or transmitted in any form or by any means withoutthe prior written permission of the publisher or in the case of reprographic reproduction in accordancewith the terms of licenses issued by the Copyright Licensing Agency in the UK [wwwclacouk] Enquiriesconcerning reproduction outside the terms stated here should be sent to the publisher at the above addressThe use of registered names trademarks etc in this publication does not imply even in the absence of a specificstatement that such names are exempt from the relevant laws and regulations and therefore for general use
Association of Surgeonsof Great Britain and Ireland
The Association of Coloproctologyof Great Britain and Ireland
2
FOREWORDIssues in Professional Practice (IIPP) is an occasional series ofbooklets published by the Association of Surgeons of Great Britainand Ireland to offer guidance on a wide range of areas whichimpact on the daily professional lives of surgeons Some topicsfocus on clinical issues some cover management and servicedelivery whilst others feature broader aspects of surgical workinglife such as education leadership and the law
This latest IIPP booklet on the Prevention Diagnosis andManagement of Anastomotic Leakage has been produced inpartnership with the Association of Coloproctology of Great Britainand Ireland and it is hoped that this joint collaboration will be ofsignificant clinical benefit to members of both societies
The Association intends that this publication and others in theseries (all of which are accessible atwwwasgbiorgukpublications) will provide concise advice andguidance on major current issues and prove to be a helpful andaccessible resource to support your professional practice Wewelcome feedback on this and other booklets in the Issues inProfessional Practice series and proposals and contributions forfuture issues in the series
Mr John MooreheadPresident
3
CONTENTS
Introduction 5
Patient Perspective 6
Acknowledgements 7
Abbreviations 7
Introduction 8
Development of Methodology and Delphi Meeting 8
Definitions and Epidemiology of AL 8
Definition 8
Epidemiology 8
Avoidance of Anastomotic Leakage 9
Preoperative considerations 9
Modifiable risk factors 9
Non-modifiable risk factors 11
Intraoperative considerations 13
Operative technique 13
Goal directed fluid therapy 13
Interventions 14
Postoperative considerations 15
(NSAIDS) 15
Diagnosis of Anastomotic Leakage 16
Scoring systems 17
Treatment of AL 17
Initial management 17
Subsequent and Definitive Management 18
1 General principles 18
2 Source control 18
Management of Specific Patterns of Anastomotic Leakage 20
1 Intraperitoneal Anastomotic Leakage 20
2 Extra-peritoneal Anastomotic Leaks 21
4
Appendix 23
Summary of findings from Delphi process for colorectalanastomotic leaks 23
Demographics and Format of Delphi Process 23
Regions 24
Delphi Process 25
Definition of anastomotic leaks 25
Non-modifiable risk factors 25
Modifiable risk factors 25
Periintraoperative risk factors 25
Reduce risk of anastomotic leaks 25
Risk factors required to consider defunctioning 27
Air Leak Testing 27
Intraoperative endoscopy 27
Useful indicators for anastomotic leaks 27
Investigation of anastomotic leak 28
Factors to determine whether to resect an anastomosis 28
References 29
5
INTRODUCTIONAn anastomotic leak as all colorectal surgeons are aware is adevastating complication that may not only result in severemorbidity but can also unfortunately lead to the demise of thepatient We all fear it and will do all we can to prevent it Howeverno matter how skilled the surgeon may be there are times when thiscomplication will occur despite best efforts
These guidelines which have been developed by an exhaustivereview of the literature and meticulous scientific process provideextremely valuable advice as how to prevent diagnose treat and -very importantly - counsel patients about the possibility of thisdreaded complication The group have worked diligently to sift andinterpret the information and are to be commended on producing adocument that is clear concise and balanced If teams follow theiradvice there is no doubt in my mind that the incidence ofanastomotic leakage will be reduced but also when it occurs liveswill be saved
I do hope that all practicing surgeons will heed the current thinkingthat is embodied in the document and apply it appropriately
Professor Sir Norman WilliamsMS FRCS FMed Sci FRCP FRCP (Edin) FRCA FDS (Hon)FACS (Hon) FRCSI (Hon) FRCSEd (Hon)
Past President The Royal College of Surgeons of EnglandDirector National Centre for Bowel Research and SurgicalInnovation Barts amp The London School of Medicine amp Dentistry
6
Patient PerspectiveWhilst this document is intended to review the clinical evidence onthe prevention diagnosis and management of anastomotic leakage itis essential that the impact of anastomotic leakage on the patient andtheir family is also considered Good communication remains animportant aspect of care
Careful history taking may elicit important risk factors foranastomotic leakage (eg a history of smoking or alcohol abuse)which may not otherwise be evident and about which some patientsmay be reticent
It is important to prepare patients and their families for surgerywhere an anastomosis is being considered by giving a balancedassessment of the risk of anastomotic leakage This will allow better-informed decision-making regarding whether the risk of ananastomosis (in particular a higher risk anastomosis) is acceptableor whether a stoma may be preferable This may enable patients tomake a better-informed choice and to be better prepared to deal withthe consequences of an anastomotic leak should this occur
Good quality timely information before and after surgery is part ofthis process and should include input from an enterostomal therapistwhich may help allay the patientrsquos fears with regard to a stoma andits impact on future quality of life
Patients who have suffered from anastomotic leakage should notonly be offered prompt and appropriate medical attention but afrank open and honest discussion about the complication as soon astheir condition permits They should have access to psychologicalsupport to help them deal with associated anger grief and stress
Jo ChurchPatient Representative
7
AcknowledgementsThe authors wish to thank the following members of theASGBIACPGBI joint anastomotic leak working group for generouslygiving their time and effort in assessing the clinical evidence andproviding expert opinion
Austin Acheson Tan Arulampalam Arnie Bhowmick Cat BoereboomKen Campbell Jo Church (Patient Liaison) Mark Coleman JustinDavies Michael Davies Peter Dawson Nicola Fearnhead NaderFrancis Richard Guy Nigel Hall Athur Harikrishnan Deena HarjiCharles Hendrickse Stephen Holtham Kourosh Khosraviani RobinKennedy Anil Lala Gerald Langman Charles Maxwell-ArmstrongBrendan Moran Neil Smart Henry Tilney Jared Torkington JanindraWarusavitarne
Thank you to Louise Hull for her assistance with the DelphiMethodology
AbbreviationsAL Anastomotic leak
ASA American Society of Anaesthesiologists Physical StatusClassification
BMI Body mass index
CI Confidence intervals
CRP C-reactive protein
DFS Disease free survival
IR Interventional radiology
NSAID Non-steroidal anti-inflammatory drug
OS Overall Survival
OR Odd Ratio
RCT Randomised Control Trial
SDD Selective decontamination of the digestive tract
TNF Tumour necrosis factor
WHR Waist hip ratio
8
IntroductionAnastomotic leaks (AL) are potentially catastrophic complicationsof colorectal surgery The spectrum of clinical severity associatedwith AL is broad however ranging from a small-contained leakwithout sepsis in a patient with a defunctioning stoma to a patientwith four-quadrant peritonitis and septic shock ALs increase theneed for reoperation the risk of local recurrence1 and reduce bothoverall (OS) and disease free survival (DFS)2-4 Despite the gravityof the complication and potential sequelae data regarding riskfactors and optimal perioperative management of ALs are relativelypoor and few attempts have been made to bring together the datawhich are available in order to provide clinical guidance Thisdocument aims to present the current best evidence and utilisedDelphi methodology to provide expert colorectal opinion
Development Of Methodology amp Delphi Meeting A systematic review of the literature searching for colorectalanastomotic leaks was performed5 Due to low quality evidenceacross multiple domains of risk factors assessment and managementof ALs a Delphi methodology was proposed Following the reviewand Delphi process it was agreed that formal gradingstrength ofrecommendation would be inappropriate due to the lack of highquality evidence A formal cut-off for consensus was not used ratherthe evidence was discussed and the percentage consensus after 3rounds of discussion is presented in brackets
A steering group of colorectal consultants and trainees was formedand met at the Tripartite meeting in Birmingham in July 2014Current evidence was presented and on the basis of this it wasagreed that a Delphi format would be beneficial to help developguidelines A questionnaire was developed using Survey Monkey6
and distributed to ACPGBI members covering all ACPGBI regionalchapters The initial round was completed on-line by participantsprior to a meeting with a further 2 rounds (See Table 7 Appendix)
Definitions and epidemiology of ALDefinitionThe preferred definition for anastomotic leaks was lsquoA leak ofluminal contents from a surgical join between two hollow viscerarsquo7
EpidemiologyThe prevalence of AL varies from 1 to 19 depending uponanatomical site pre intra and postoperative factors5 These arediscussed below
9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

wwwasgbiorguk wwwacpgbiorguk
1
ISSUES INPROFESSIONAL PRACTICE
PREVENTION DIAGNOSIS ANDMANAGEMENT OF COLORECTAL
ANASTOMOTIC LEAKAGE
AUTHORSF D McDermott S Arora J Smith R J C Steele
G L Carlson and D C Winter(on behalf of the joint ASGBIACPGBIAnastomotic Leakage Working Group)
PUBLICATION DATEMarch 2016
PUBLISHED BYAssociation of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
SPONSORED BYAN EDUCATIONAL GRANT FROM
No part of this publication may be reproduced stored or transmitted in any form or by any means withoutthe prior written permission of the publisher or in the case of reprographic reproduction in accordancewith the terms of licenses issued by the Copyright Licensing Agency in the UK [wwwclacouk] Enquiriesconcerning reproduction outside the terms stated here should be sent to the publisher at the above addressThe use of registered names trademarks etc in this publication does not imply even in the absence of a specificstatement that such names are exempt from the relevant laws and regulations and therefore for general use
Association of Surgeonsof Great Britain and Ireland
The Association of Coloproctologyof Great Britain and Ireland
2
FOREWORDIssues in Professional Practice (IIPP) is an occasional series ofbooklets published by the Association of Surgeons of Great Britainand Ireland to offer guidance on a wide range of areas whichimpact on the daily professional lives of surgeons Some topicsfocus on clinical issues some cover management and servicedelivery whilst others feature broader aspects of surgical workinglife such as education leadership and the law
This latest IIPP booklet on the Prevention Diagnosis andManagement of Anastomotic Leakage has been produced inpartnership with the Association of Coloproctology of Great Britainand Ireland and it is hoped that this joint collaboration will be ofsignificant clinical benefit to members of both societies
The Association intends that this publication and others in theseries (all of which are accessible atwwwasgbiorgukpublications) will provide concise advice andguidance on major current issues and prove to be a helpful andaccessible resource to support your professional practice Wewelcome feedback on this and other booklets in the Issues inProfessional Practice series and proposals and contributions forfuture issues in the series
Mr John MooreheadPresident
3
CONTENTS
Introduction 5
Patient Perspective 6
Acknowledgements 7
Abbreviations 7
Introduction 8
Development of Methodology and Delphi Meeting 8
Definitions and Epidemiology of AL 8
Definition 8
Epidemiology 8
Avoidance of Anastomotic Leakage 9
Preoperative considerations 9
Modifiable risk factors 9
Non-modifiable risk factors 11
Intraoperative considerations 13
Operative technique 13
Goal directed fluid therapy 13
Interventions 14
Postoperative considerations 15
(NSAIDS) 15
Diagnosis of Anastomotic Leakage 16
Scoring systems 17
Treatment of AL 17
Initial management 17
Subsequent and Definitive Management 18
1 General principles 18
2 Source control 18
Management of Specific Patterns of Anastomotic Leakage 20
1 Intraperitoneal Anastomotic Leakage 20
2 Extra-peritoneal Anastomotic Leaks 21
4
Appendix 23
Summary of findings from Delphi process for colorectalanastomotic leaks 23
Demographics and Format of Delphi Process 23
Regions 24
Delphi Process 25
Definition of anastomotic leaks 25
Non-modifiable risk factors 25
Modifiable risk factors 25
Periintraoperative risk factors 25
Reduce risk of anastomotic leaks 25
Risk factors required to consider defunctioning 27
Air Leak Testing 27
Intraoperative endoscopy 27
Useful indicators for anastomotic leaks 27
Investigation of anastomotic leak 28
Factors to determine whether to resect an anastomosis 28
References 29
5
INTRODUCTIONAn anastomotic leak as all colorectal surgeons are aware is adevastating complication that may not only result in severemorbidity but can also unfortunately lead to the demise of thepatient We all fear it and will do all we can to prevent it Howeverno matter how skilled the surgeon may be there are times when thiscomplication will occur despite best efforts
These guidelines which have been developed by an exhaustivereview of the literature and meticulous scientific process provideextremely valuable advice as how to prevent diagnose treat and -very importantly - counsel patients about the possibility of thisdreaded complication The group have worked diligently to sift andinterpret the information and are to be commended on producing adocument that is clear concise and balanced If teams follow theiradvice there is no doubt in my mind that the incidence ofanastomotic leakage will be reduced but also when it occurs liveswill be saved
I do hope that all practicing surgeons will heed the current thinkingthat is embodied in the document and apply it appropriately
Professor Sir Norman WilliamsMS FRCS FMed Sci FRCP FRCP (Edin) FRCA FDS (Hon)FACS (Hon) FRCSI (Hon) FRCSEd (Hon)
Past President The Royal College of Surgeons of EnglandDirector National Centre for Bowel Research and SurgicalInnovation Barts amp The London School of Medicine amp Dentistry
6
Patient PerspectiveWhilst this document is intended to review the clinical evidence onthe prevention diagnosis and management of anastomotic leakage itis essential that the impact of anastomotic leakage on the patient andtheir family is also considered Good communication remains animportant aspect of care
Careful history taking may elicit important risk factors foranastomotic leakage (eg a history of smoking or alcohol abuse)which may not otherwise be evident and about which some patientsmay be reticent
It is important to prepare patients and their families for surgerywhere an anastomosis is being considered by giving a balancedassessment of the risk of anastomotic leakage This will allow better-informed decision-making regarding whether the risk of ananastomosis (in particular a higher risk anastomosis) is acceptableor whether a stoma may be preferable This may enable patients tomake a better-informed choice and to be better prepared to deal withthe consequences of an anastomotic leak should this occur
Good quality timely information before and after surgery is part ofthis process and should include input from an enterostomal therapistwhich may help allay the patientrsquos fears with regard to a stoma andits impact on future quality of life
Patients who have suffered from anastomotic leakage should notonly be offered prompt and appropriate medical attention but afrank open and honest discussion about the complication as soon astheir condition permits They should have access to psychologicalsupport to help them deal with associated anger grief and stress
Jo ChurchPatient Representative
7
AcknowledgementsThe authors wish to thank the following members of theASGBIACPGBI joint anastomotic leak working group for generouslygiving their time and effort in assessing the clinical evidence andproviding expert opinion
Austin Acheson Tan Arulampalam Arnie Bhowmick Cat BoereboomKen Campbell Jo Church (Patient Liaison) Mark Coleman JustinDavies Michael Davies Peter Dawson Nicola Fearnhead NaderFrancis Richard Guy Nigel Hall Athur Harikrishnan Deena HarjiCharles Hendrickse Stephen Holtham Kourosh Khosraviani RobinKennedy Anil Lala Gerald Langman Charles Maxwell-ArmstrongBrendan Moran Neil Smart Henry Tilney Jared Torkington JanindraWarusavitarne
Thank you to Louise Hull for her assistance with the DelphiMethodology
AbbreviationsAL Anastomotic leak
ASA American Society of Anaesthesiologists Physical StatusClassification
BMI Body mass index
CI Confidence intervals
CRP C-reactive protein
DFS Disease free survival
IR Interventional radiology
NSAID Non-steroidal anti-inflammatory drug
OS Overall Survival
OR Odd Ratio
RCT Randomised Control Trial
SDD Selective decontamination of the digestive tract
TNF Tumour necrosis factor
WHR Waist hip ratio
8
IntroductionAnastomotic leaks (AL) are potentially catastrophic complicationsof colorectal surgery The spectrum of clinical severity associatedwith AL is broad however ranging from a small-contained leakwithout sepsis in a patient with a defunctioning stoma to a patientwith four-quadrant peritonitis and septic shock ALs increase theneed for reoperation the risk of local recurrence1 and reduce bothoverall (OS) and disease free survival (DFS)2-4 Despite the gravityof the complication and potential sequelae data regarding riskfactors and optimal perioperative management of ALs are relativelypoor and few attempts have been made to bring together the datawhich are available in order to provide clinical guidance Thisdocument aims to present the current best evidence and utilisedDelphi methodology to provide expert colorectal opinion
Development Of Methodology amp Delphi Meeting A systematic review of the literature searching for colorectalanastomotic leaks was performed5 Due to low quality evidenceacross multiple domains of risk factors assessment and managementof ALs a Delphi methodology was proposed Following the reviewand Delphi process it was agreed that formal gradingstrength ofrecommendation would be inappropriate due to the lack of highquality evidence A formal cut-off for consensus was not used ratherthe evidence was discussed and the percentage consensus after 3rounds of discussion is presented in brackets
A steering group of colorectal consultants and trainees was formedand met at the Tripartite meeting in Birmingham in July 2014Current evidence was presented and on the basis of this it wasagreed that a Delphi format would be beneficial to help developguidelines A questionnaire was developed using Survey Monkey6
and distributed to ACPGBI members covering all ACPGBI regionalchapters The initial round was completed on-line by participantsprior to a meeting with a further 2 rounds (See Table 7 Appendix)
Definitions and epidemiology of ALDefinitionThe preferred definition for anastomotic leaks was lsquoA leak ofluminal contents from a surgical join between two hollow viscerarsquo7
EpidemiologyThe prevalence of AL varies from 1 to 19 depending uponanatomical site pre intra and postoperative factors5 These arediscussed below
9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk
1
ISSUES INPROFESSIONAL PRACTICE
PREVENTION DIAGNOSIS ANDMANAGEMENT OF COLORECTAL
ANASTOMOTIC LEAKAGE
AUTHORSF D McDermott S Arora J Smith R J C Steele
G L Carlson and D C Winter(on behalf of the joint ASGBIACPGBIAnastomotic Leakage Working Group)
PUBLICATION DATEMarch 2016
PUBLISHED BYAssociation of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
SPONSORED BYAN EDUCATIONAL GRANT FROM
No part of this publication may be reproduced stored or transmitted in any form or by any means withoutthe prior written permission of the publisher or in the case of reprographic reproduction in accordancewith the terms of licenses issued by the Copyright Licensing Agency in the UK [wwwclacouk] Enquiriesconcerning reproduction outside the terms stated here should be sent to the publisher at the above addressThe use of registered names trademarks etc in this publication does not imply even in the absence of a specificstatement that such names are exempt from the relevant laws and regulations and therefore for general use
Association of Surgeonsof Great Britain and Ireland
The Association of Coloproctologyof Great Britain and Ireland
2
FOREWORDIssues in Professional Practice (IIPP) is an occasional series ofbooklets published by the Association of Surgeons of Great Britainand Ireland to offer guidance on a wide range of areas whichimpact on the daily professional lives of surgeons Some topicsfocus on clinical issues some cover management and servicedelivery whilst others feature broader aspects of surgical workinglife such as education leadership and the law
This latest IIPP booklet on the Prevention Diagnosis andManagement of Anastomotic Leakage has been produced inpartnership with the Association of Coloproctology of Great Britainand Ireland and it is hoped that this joint collaboration will be ofsignificant clinical benefit to members of both societies
The Association intends that this publication and others in theseries (all of which are accessible atwwwasgbiorgukpublications) will provide concise advice andguidance on major current issues and prove to be a helpful andaccessible resource to support your professional practice Wewelcome feedback on this and other booklets in the Issues inProfessional Practice series and proposals and contributions forfuture issues in the series
Mr John MooreheadPresident
3
CONTENTS
Introduction 5
Patient Perspective 6
Acknowledgements 7
Abbreviations 7
Introduction 8
Development of Methodology and Delphi Meeting 8
Definitions and Epidemiology of AL 8
Definition 8
Epidemiology 8
Avoidance of Anastomotic Leakage 9
Preoperative considerations 9
Modifiable risk factors 9
Non-modifiable risk factors 11
Intraoperative considerations 13
Operative technique 13
Goal directed fluid therapy 13
Interventions 14
Postoperative considerations 15
(NSAIDS) 15
Diagnosis of Anastomotic Leakage 16
Scoring systems 17
Treatment of AL 17
Initial management 17
Subsequent and Definitive Management 18
1 General principles 18
2 Source control 18
Management of Specific Patterns of Anastomotic Leakage 20
1 Intraperitoneal Anastomotic Leakage 20
2 Extra-peritoneal Anastomotic Leaks 21
4
Appendix 23
Summary of findings from Delphi process for colorectalanastomotic leaks 23
Demographics and Format of Delphi Process 23
Regions 24
Delphi Process 25
Definition of anastomotic leaks 25
Non-modifiable risk factors 25
Modifiable risk factors 25
Periintraoperative risk factors 25
Reduce risk of anastomotic leaks 25
Risk factors required to consider defunctioning 27
Air Leak Testing 27
Intraoperative endoscopy 27
Useful indicators for anastomotic leaks 27
Investigation of anastomotic leak 28
Factors to determine whether to resect an anastomosis 28
References 29
5
INTRODUCTIONAn anastomotic leak as all colorectal surgeons are aware is adevastating complication that may not only result in severemorbidity but can also unfortunately lead to the demise of thepatient We all fear it and will do all we can to prevent it Howeverno matter how skilled the surgeon may be there are times when thiscomplication will occur despite best efforts
These guidelines which have been developed by an exhaustivereview of the literature and meticulous scientific process provideextremely valuable advice as how to prevent diagnose treat and -very importantly - counsel patients about the possibility of thisdreaded complication The group have worked diligently to sift andinterpret the information and are to be commended on producing adocument that is clear concise and balanced If teams follow theiradvice there is no doubt in my mind that the incidence ofanastomotic leakage will be reduced but also when it occurs liveswill be saved
I do hope that all practicing surgeons will heed the current thinkingthat is embodied in the document and apply it appropriately
Professor Sir Norman WilliamsMS FRCS FMed Sci FRCP FRCP (Edin) FRCA FDS (Hon)FACS (Hon) FRCSI (Hon) FRCSEd (Hon)
Past President The Royal College of Surgeons of EnglandDirector National Centre for Bowel Research and SurgicalInnovation Barts amp The London School of Medicine amp Dentistry
6
Patient PerspectiveWhilst this document is intended to review the clinical evidence onthe prevention diagnosis and management of anastomotic leakage itis essential that the impact of anastomotic leakage on the patient andtheir family is also considered Good communication remains animportant aspect of care
Careful history taking may elicit important risk factors foranastomotic leakage (eg a history of smoking or alcohol abuse)which may not otherwise be evident and about which some patientsmay be reticent
It is important to prepare patients and their families for surgerywhere an anastomosis is being considered by giving a balancedassessment of the risk of anastomotic leakage This will allow better-informed decision-making regarding whether the risk of ananastomosis (in particular a higher risk anastomosis) is acceptableor whether a stoma may be preferable This may enable patients tomake a better-informed choice and to be better prepared to deal withthe consequences of an anastomotic leak should this occur
Good quality timely information before and after surgery is part ofthis process and should include input from an enterostomal therapistwhich may help allay the patientrsquos fears with regard to a stoma andits impact on future quality of life
Patients who have suffered from anastomotic leakage should notonly be offered prompt and appropriate medical attention but afrank open and honest discussion about the complication as soon astheir condition permits They should have access to psychologicalsupport to help them deal with associated anger grief and stress
Jo ChurchPatient Representative
7
AcknowledgementsThe authors wish to thank the following members of theASGBIACPGBI joint anastomotic leak working group for generouslygiving their time and effort in assessing the clinical evidence andproviding expert opinion
Austin Acheson Tan Arulampalam Arnie Bhowmick Cat BoereboomKen Campbell Jo Church (Patient Liaison) Mark Coleman JustinDavies Michael Davies Peter Dawson Nicola Fearnhead NaderFrancis Richard Guy Nigel Hall Athur Harikrishnan Deena HarjiCharles Hendrickse Stephen Holtham Kourosh Khosraviani RobinKennedy Anil Lala Gerald Langman Charles Maxwell-ArmstrongBrendan Moran Neil Smart Henry Tilney Jared Torkington JanindraWarusavitarne
Thank you to Louise Hull for her assistance with the DelphiMethodology
AbbreviationsAL Anastomotic leak
ASA American Society of Anaesthesiologists Physical StatusClassification
BMI Body mass index
CI Confidence intervals
CRP C-reactive protein
DFS Disease free survival
IR Interventional radiology
NSAID Non-steroidal anti-inflammatory drug
OS Overall Survival
OR Odd Ratio
RCT Randomised Control Trial
SDD Selective decontamination of the digestive tract
TNF Tumour necrosis factor
WHR Waist hip ratio
8
IntroductionAnastomotic leaks (AL) are potentially catastrophic complicationsof colorectal surgery The spectrum of clinical severity associatedwith AL is broad however ranging from a small-contained leakwithout sepsis in a patient with a defunctioning stoma to a patientwith four-quadrant peritonitis and septic shock ALs increase theneed for reoperation the risk of local recurrence1 and reduce bothoverall (OS) and disease free survival (DFS)2-4 Despite the gravityof the complication and potential sequelae data regarding riskfactors and optimal perioperative management of ALs are relativelypoor and few attempts have been made to bring together the datawhich are available in order to provide clinical guidance Thisdocument aims to present the current best evidence and utilisedDelphi methodology to provide expert colorectal opinion
Development Of Methodology amp Delphi Meeting A systematic review of the literature searching for colorectalanastomotic leaks was performed5 Due to low quality evidenceacross multiple domains of risk factors assessment and managementof ALs a Delphi methodology was proposed Following the reviewand Delphi process it was agreed that formal gradingstrength ofrecommendation would be inappropriate due to the lack of highquality evidence A formal cut-off for consensus was not used ratherthe evidence was discussed and the percentage consensus after 3rounds of discussion is presented in brackets
A steering group of colorectal consultants and trainees was formedand met at the Tripartite meeting in Birmingham in July 2014Current evidence was presented and on the basis of this it wasagreed that a Delphi format would be beneficial to help developguidelines A questionnaire was developed using Survey Monkey6
and distributed to ACPGBI members covering all ACPGBI regionalchapters The initial round was completed on-line by participantsprior to a meeting with a further 2 rounds (See Table 7 Appendix)
Definitions and epidemiology of ALDefinitionThe preferred definition for anastomotic leaks was lsquoA leak ofluminal contents from a surgical join between two hollow viscerarsquo7
EpidemiologyThe prevalence of AL varies from 1 to 19 depending uponanatomical site pre intra and postoperative factors5 These arediscussed below
9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

2
FOREWORDIssues in Professional Practice (IIPP) is an occasional series ofbooklets published by the Association of Surgeons of Great Britainand Ireland to offer guidance on a wide range of areas whichimpact on the daily professional lives of surgeons Some topicsfocus on clinical issues some cover management and servicedelivery whilst others feature broader aspects of surgical workinglife such as education leadership and the law
This latest IIPP booklet on the Prevention Diagnosis andManagement of Anastomotic Leakage has been produced inpartnership with the Association of Coloproctology of Great Britainand Ireland and it is hoped that this joint collaboration will be ofsignificant clinical benefit to members of both societies
The Association intends that this publication and others in theseries (all of which are accessible atwwwasgbiorgukpublications) will provide concise advice andguidance on major current issues and prove to be a helpful andaccessible resource to support your professional practice Wewelcome feedback on this and other booklets in the Issues inProfessional Practice series and proposals and contributions forfuture issues in the series
Mr John MooreheadPresident
3
CONTENTS
Introduction 5
Patient Perspective 6
Acknowledgements 7
Abbreviations 7
Introduction 8
Development of Methodology and Delphi Meeting 8
Definitions and Epidemiology of AL 8
Definition 8
Epidemiology 8
Avoidance of Anastomotic Leakage 9
Preoperative considerations 9
Modifiable risk factors 9
Non-modifiable risk factors 11
Intraoperative considerations 13
Operative technique 13
Goal directed fluid therapy 13
Interventions 14
Postoperative considerations 15
(NSAIDS) 15
Diagnosis of Anastomotic Leakage 16
Scoring systems 17
Treatment of AL 17
Initial management 17
Subsequent and Definitive Management 18
1 General principles 18
2 Source control 18
Management of Specific Patterns of Anastomotic Leakage 20
1 Intraperitoneal Anastomotic Leakage 20
2 Extra-peritoneal Anastomotic Leaks 21
4
Appendix 23
Summary of findings from Delphi process for colorectalanastomotic leaks 23
Demographics and Format of Delphi Process 23
Regions 24
Delphi Process 25
Definition of anastomotic leaks 25
Non-modifiable risk factors 25
Modifiable risk factors 25
Periintraoperative risk factors 25
Reduce risk of anastomotic leaks 25
Risk factors required to consider defunctioning 27
Air Leak Testing 27
Intraoperative endoscopy 27
Useful indicators for anastomotic leaks 27
Investigation of anastomotic leak 28
Factors to determine whether to resect an anastomosis 28
References 29
5
INTRODUCTIONAn anastomotic leak as all colorectal surgeons are aware is adevastating complication that may not only result in severemorbidity but can also unfortunately lead to the demise of thepatient We all fear it and will do all we can to prevent it Howeverno matter how skilled the surgeon may be there are times when thiscomplication will occur despite best efforts
These guidelines which have been developed by an exhaustivereview of the literature and meticulous scientific process provideextremely valuable advice as how to prevent diagnose treat and -very importantly - counsel patients about the possibility of thisdreaded complication The group have worked diligently to sift andinterpret the information and are to be commended on producing adocument that is clear concise and balanced If teams follow theiradvice there is no doubt in my mind that the incidence ofanastomotic leakage will be reduced but also when it occurs liveswill be saved
I do hope that all practicing surgeons will heed the current thinkingthat is embodied in the document and apply it appropriately
Professor Sir Norman WilliamsMS FRCS FMed Sci FRCP FRCP (Edin) FRCA FDS (Hon)FACS (Hon) FRCSI (Hon) FRCSEd (Hon)
Past President The Royal College of Surgeons of EnglandDirector National Centre for Bowel Research and SurgicalInnovation Barts amp The London School of Medicine amp Dentistry
6
Patient PerspectiveWhilst this document is intended to review the clinical evidence onthe prevention diagnosis and management of anastomotic leakage itis essential that the impact of anastomotic leakage on the patient andtheir family is also considered Good communication remains animportant aspect of care
Careful history taking may elicit important risk factors foranastomotic leakage (eg a history of smoking or alcohol abuse)which may not otherwise be evident and about which some patientsmay be reticent
It is important to prepare patients and their families for surgerywhere an anastomosis is being considered by giving a balancedassessment of the risk of anastomotic leakage This will allow better-informed decision-making regarding whether the risk of ananastomosis (in particular a higher risk anastomosis) is acceptableor whether a stoma may be preferable This may enable patients tomake a better-informed choice and to be better prepared to deal withthe consequences of an anastomotic leak should this occur
Good quality timely information before and after surgery is part ofthis process and should include input from an enterostomal therapistwhich may help allay the patientrsquos fears with regard to a stoma andits impact on future quality of life
Patients who have suffered from anastomotic leakage should notonly be offered prompt and appropriate medical attention but afrank open and honest discussion about the complication as soon astheir condition permits They should have access to psychologicalsupport to help them deal with associated anger grief and stress
Jo ChurchPatient Representative
7
AcknowledgementsThe authors wish to thank the following members of theASGBIACPGBI joint anastomotic leak working group for generouslygiving their time and effort in assessing the clinical evidence andproviding expert opinion
Austin Acheson Tan Arulampalam Arnie Bhowmick Cat BoereboomKen Campbell Jo Church (Patient Liaison) Mark Coleman JustinDavies Michael Davies Peter Dawson Nicola Fearnhead NaderFrancis Richard Guy Nigel Hall Athur Harikrishnan Deena HarjiCharles Hendrickse Stephen Holtham Kourosh Khosraviani RobinKennedy Anil Lala Gerald Langman Charles Maxwell-ArmstrongBrendan Moran Neil Smart Henry Tilney Jared Torkington JanindraWarusavitarne
Thank you to Louise Hull for her assistance with the DelphiMethodology
AbbreviationsAL Anastomotic leak
ASA American Society of Anaesthesiologists Physical StatusClassification
BMI Body mass index
CI Confidence intervals
CRP C-reactive protein
DFS Disease free survival
IR Interventional radiology
NSAID Non-steroidal anti-inflammatory drug
OS Overall Survival
OR Odd Ratio
RCT Randomised Control Trial
SDD Selective decontamination of the digestive tract
TNF Tumour necrosis factor
WHR Waist hip ratio
8
IntroductionAnastomotic leaks (AL) are potentially catastrophic complicationsof colorectal surgery The spectrum of clinical severity associatedwith AL is broad however ranging from a small-contained leakwithout sepsis in a patient with a defunctioning stoma to a patientwith four-quadrant peritonitis and septic shock ALs increase theneed for reoperation the risk of local recurrence1 and reduce bothoverall (OS) and disease free survival (DFS)2-4 Despite the gravityof the complication and potential sequelae data regarding riskfactors and optimal perioperative management of ALs are relativelypoor and few attempts have been made to bring together the datawhich are available in order to provide clinical guidance Thisdocument aims to present the current best evidence and utilisedDelphi methodology to provide expert colorectal opinion
Development Of Methodology amp Delphi Meeting A systematic review of the literature searching for colorectalanastomotic leaks was performed5 Due to low quality evidenceacross multiple domains of risk factors assessment and managementof ALs a Delphi methodology was proposed Following the reviewand Delphi process it was agreed that formal gradingstrength ofrecommendation would be inappropriate due to the lack of highquality evidence A formal cut-off for consensus was not used ratherthe evidence was discussed and the percentage consensus after 3rounds of discussion is presented in brackets
A steering group of colorectal consultants and trainees was formedand met at the Tripartite meeting in Birmingham in July 2014Current evidence was presented and on the basis of this it wasagreed that a Delphi format would be beneficial to help developguidelines A questionnaire was developed using Survey Monkey6
and distributed to ACPGBI members covering all ACPGBI regionalchapters The initial round was completed on-line by participantsprior to a meeting with a further 2 rounds (See Table 7 Appendix)
Definitions and epidemiology of ALDefinitionThe preferred definition for anastomotic leaks was lsquoA leak ofluminal contents from a surgical join between two hollow viscerarsquo7
EpidemiologyThe prevalence of AL varies from 1 to 19 depending uponanatomical site pre intra and postoperative factors5 These arediscussed below
9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

3
CONTENTS
Introduction 5
Patient Perspective 6
Acknowledgements 7
Abbreviations 7
Introduction 8
Development of Methodology and Delphi Meeting 8
Definitions and Epidemiology of AL 8
Definition 8
Epidemiology 8
Avoidance of Anastomotic Leakage 9
Preoperative considerations 9
Modifiable risk factors 9
Non-modifiable risk factors 11
Intraoperative considerations 13
Operative technique 13
Goal directed fluid therapy 13
Interventions 14
Postoperative considerations 15
(NSAIDS) 15
Diagnosis of Anastomotic Leakage 16
Scoring systems 17
Treatment of AL 17
Initial management 17
Subsequent and Definitive Management 18
1 General principles 18
2 Source control 18
Management of Specific Patterns of Anastomotic Leakage 20
1 Intraperitoneal Anastomotic Leakage 20
2 Extra-peritoneal Anastomotic Leaks 21
4
Appendix 23
Summary of findings from Delphi process for colorectalanastomotic leaks 23
Demographics and Format of Delphi Process 23
Regions 24
Delphi Process 25
Definition of anastomotic leaks 25
Non-modifiable risk factors 25
Modifiable risk factors 25
Periintraoperative risk factors 25
Reduce risk of anastomotic leaks 25
Risk factors required to consider defunctioning 27
Air Leak Testing 27
Intraoperative endoscopy 27
Useful indicators for anastomotic leaks 27
Investigation of anastomotic leak 28
Factors to determine whether to resect an anastomosis 28
References 29
5
INTRODUCTIONAn anastomotic leak as all colorectal surgeons are aware is adevastating complication that may not only result in severemorbidity but can also unfortunately lead to the demise of thepatient We all fear it and will do all we can to prevent it Howeverno matter how skilled the surgeon may be there are times when thiscomplication will occur despite best efforts
These guidelines which have been developed by an exhaustivereview of the literature and meticulous scientific process provideextremely valuable advice as how to prevent diagnose treat and -very importantly - counsel patients about the possibility of thisdreaded complication The group have worked diligently to sift andinterpret the information and are to be commended on producing adocument that is clear concise and balanced If teams follow theiradvice there is no doubt in my mind that the incidence ofanastomotic leakage will be reduced but also when it occurs liveswill be saved
I do hope that all practicing surgeons will heed the current thinkingthat is embodied in the document and apply it appropriately
Professor Sir Norman WilliamsMS FRCS FMed Sci FRCP FRCP (Edin) FRCA FDS (Hon)FACS (Hon) FRCSI (Hon) FRCSEd (Hon)
Past President The Royal College of Surgeons of EnglandDirector National Centre for Bowel Research and SurgicalInnovation Barts amp The London School of Medicine amp Dentistry
6
Patient PerspectiveWhilst this document is intended to review the clinical evidence onthe prevention diagnosis and management of anastomotic leakage itis essential that the impact of anastomotic leakage on the patient andtheir family is also considered Good communication remains animportant aspect of care
Careful history taking may elicit important risk factors foranastomotic leakage (eg a history of smoking or alcohol abuse)which may not otherwise be evident and about which some patientsmay be reticent
It is important to prepare patients and their families for surgerywhere an anastomosis is being considered by giving a balancedassessment of the risk of anastomotic leakage This will allow better-informed decision-making regarding whether the risk of ananastomosis (in particular a higher risk anastomosis) is acceptableor whether a stoma may be preferable This may enable patients tomake a better-informed choice and to be better prepared to deal withthe consequences of an anastomotic leak should this occur
Good quality timely information before and after surgery is part ofthis process and should include input from an enterostomal therapistwhich may help allay the patientrsquos fears with regard to a stoma andits impact on future quality of life
Patients who have suffered from anastomotic leakage should notonly be offered prompt and appropriate medical attention but afrank open and honest discussion about the complication as soon astheir condition permits They should have access to psychologicalsupport to help them deal with associated anger grief and stress
Jo ChurchPatient Representative
7
AcknowledgementsThe authors wish to thank the following members of theASGBIACPGBI joint anastomotic leak working group for generouslygiving their time and effort in assessing the clinical evidence andproviding expert opinion
Austin Acheson Tan Arulampalam Arnie Bhowmick Cat BoereboomKen Campbell Jo Church (Patient Liaison) Mark Coleman JustinDavies Michael Davies Peter Dawson Nicola Fearnhead NaderFrancis Richard Guy Nigel Hall Athur Harikrishnan Deena HarjiCharles Hendrickse Stephen Holtham Kourosh Khosraviani RobinKennedy Anil Lala Gerald Langman Charles Maxwell-ArmstrongBrendan Moran Neil Smart Henry Tilney Jared Torkington JanindraWarusavitarne
Thank you to Louise Hull for her assistance with the DelphiMethodology
AbbreviationsAL Anastomotic leak
ASA American Society of Anaesthesiologists Physical StatusClassification
BMI Body mass index
CI Confidence intervals
CRP C-reactive protein
DFS Disease free survival
IR Interventional radiology
NSAID Non-steroidal anti-inflammatory drug
OS Overall Survival
OR Odd Ratio
RCT Randomised Control Trial
SDD Selective decontamination of the digestive tract
TNF Tumour necrosis factor
WHR Waist hip ratio
8
IntroductionAnastomotic leaks (AL) are potentially catastrophic complicationsof colorectal surgery The spectrum of clinical severity associatedwith AL is broad however ranging from a small-contained leakwithout sepsis in a patient with a defunctioning stoma to a patientwith four-quadrant peritonitis and septic shock ALs increase theneed for reoperation the risk of local recurrence1 and reduce bothoverall (OS) and disease free survival (DFS)2-4 Despite the gravityof the complication and potential sequelae data regarding riskfactors and optimal perioperative management of ALs are relativelypoor and few attempts have been made to bring together the datawhich are available in order to provide clinical guidance Thisdocument aims to present the current best evidence and utilisedDelphi methodology to provide expert colorectal opinion
Development Of Methodology amp Delphi Meeting A systematic review of the literature searching for colorectalanastomotic leaks was performed5 Due to low quality evidenceacross multiple domains of risk factors assessment and managementof ALs a Delphi methodology was proposed Following the reviewand Delphi process it was agreed that formal gradingstrength ofrecommendation would be inappropriate due to the lack of highquality evidence A formal cut-off for consensus was not used ratherthe evidence was discussed and the percentage consensus after 3rounds of discussion is presented in brackets
A steering group of colorectal consultants and trainees was formedand met at the Tripartite meeting in Birmingham in July 2014Current evidence was presented and on the basis of this it wasagreed that a Delphi format would be beneficial to help developguidelines A questionnaire was developed using Survey Monkey6
and distributed to ACPGBI members covering all ACPGBI regionalchapters The initial round was completed on-line by participantsprior to a meeting with a further 2 rounds (See Table 7 Appendix)
Definitions and epidemiology of ALDefinitionThe preferred definition for anastomotic leaks was lsquoA leak ofluminal contents from a surgical join between two hollow viscerarsquo7
EpidemiologyThe prevalence of AL varies from 1 to 19 depending uponanatomical site pre intra and postoperative factors5 These arediscussed below
9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

4
Appendix 23
Summary of findings from Delphi process for colorectalanastomotic leaks 23
Demographics and Format of Delphi Process 23
Regions 24
Delphi Process 25
Definition of anastomotic leaks 25
Non-modifiable risk factors 25
Modifiable risk factors 25
Periintraoperative risk factors 25
Reduce risk of anastomotic leaks 25
Risk factors required to consider defunctioning 27
Air Leak Testing 27
Intraoperative endoscopy 27
Useful indicators for anastomotic leaks 27
Investigation of anastomotic leak 28
Factors to determine whether to resect an anastomosis 28
References 29
5
INTRODUCTIONAn anastomotic leak as all colorectal surgeons are aware is adevastating complication that may not only result in severemorbidity but can also unfortunately lead to the demise of thepatient We all fear it and will do all we can to prevent it Howeverno matter how skilled the surgeon may be there are times when thiscomplication will occur despite best efforts
These guidelines which have been developed by an exhaustivereview of the literature and meticulous scientific process provideextremely valuable advice as how to prevent diagnose treat and -very importantly - counsel patients about the possibility of thisdreaded complication The group have worked diligently to sift andinterpret the information and are to be commended on producing adocument that is clear concise and balanced If teams follow theiradvice there is no doubt in my mind that the incidence ofanastomotic leakage will be reduced but also when it occurs liveswill be saved
I do hope that all practicing surgeons will heed the current thinkingthat is embodied in the document and apply it appropriately
Professor Sir Norman WilliamsMS FRCS FMed Sci FRCP FRCP (Edin) FRCA FDS (Hon)FACS (Hon) FRCSI (Hon) FRCSEd (Hon)
Past President The Royal College of Surgeons of EnglandDirector National Centre for Bowel Research and SurgicalInnovation Barts amp The London School of Medicine amp Dentistry
6
Patient PerspectiveWhilst this document is intended to review the clinical evidence onthe prevention diagnosis and management of anastomotic leakage itis essential that the impact of anastomotic leakage on the patient andtheir family is also considered Good communication remains animportant aspect of care
Careful history taking may elicit important risk factors foranastomotic leakage (eg a history of smoking or alcohol abuse)which may not otherwise be evident and about which some patientsmay be reticent
It is important to prepare patients and their families for surgerywhere an anastomosis is being considered by giving a balancedassessment of the risk of anastomotic leakage This will allow better-informed decision-making regarding whether the risk of ananastomosis (in particular a higher risk anastomosis) is acceptableor whether a stoma may be preferable This may enable patients tomake a better-informed choice and to be better prepared to deal withthe consequences of an anastomotic leak should this occur
Good quality timely information before and after surgery is part ofthis process and should include input from an enterostomal therapistwhich may help allay the patientrsquos fears with regard to a stoma andits impact on future quality of life
Patients who have suffered from anastomotic leakage should notonly be offered prompt and appropriate medical attention but afrank open and honest discussion about the complication as soon astheir condition permits They should have access to psychologicalsupport to help them deal with associated anger grief and stress
Jo ChurchPatient Representative
7
AcknowledgementsThe authors wish to thank the following members of theASGBIACPGBI joint anastomotic leak working group for generouslygiving their time and effort in assessing the clinical evidence andproviding expert opinion
Austin Acheson Tan Arulampalam Arnie Bhowmick Cat BoereboomKen Campbell Jo Church (Patient Liaison) Mark Coleman JustinDavies Michael Davies Peter Dawson Nicola Fearnhead NaderFrancis Richard Guy Nigel Hall Athur Harikrishnan Deena HarjiCharles Hendrickse Stephen Holtham Kourosh Khosraviani RobinKennedy Anil Lala Gerald Langman Charles Maxwell-ArmstrongBrendan Moran Neil Smart Henry Tilney Jared Torkington JanindraWarusavitarne
Thank you to Louise Hull for her assistance with the DelphiMethodology
AbbreviationsAL Anastomotic leak
ASA American Society of Anaesthesiologists Physical StatusClassification
BMI Body mass index
CI Confidence intervals
CRP C-reactive protein
DFS Disease free survival
IR Interventional radiology
NSAID Non-steroidal anti-inflammatory drug
OS Overall Survival
OR Odd Ratio
RCT Randomised Control Trial
SDD Selective decontamination of the digestive tract
TNF Tumour necrosis factor
WHR Waist hip ratio
8
IntroductionAnastomotic leaks (AL) are potentially catastrophic complicationsof colorectal surgery The spectrum of clinical severity associatedwith AL is broad however ranging from a small-contained leakwithout sepsis in a patient with a defunctioning stoma to a patientwith four-quadrant peritonitis and septic shock ALs increase theneed for reoperation the risk of local recurrence1 and reduce bothoverall (OS) and disease free survival (DFS)2-4 Despite the gravityof the complication and potential sequelae data regarding riskfactors and optimal perioperative management of ALs are relativelypoor and few attempts have been made to bring together the datawhich are available in order to provide clinical guidance Thisdocument aims to present the current best evidence and utilisedDelphi methodology to provide expert colorectal opinion
Development Of Methodology amp Delphi Meeting A systematic review of the literature searching for colorectalanastomotic leaks was performed5 Due to low quality evidenceacross multiple domains of risk factors assessment and managementof ALs a Delphi methodology was proposed Following the reviewand Delphi process it was agreed that formal gradingstrength ofrecommendation would be inappropriate due to the lack of highquality evidence A formal cut-off for consensus was not used ratherthe evidence was discussed and the percentage consensus after 3rounds of discussion is presented in brackets
A steering group of colorectal consultants and trainees was formedand met at the Tripartite meeting in Birmingham in July 2014Current evidence was presented and on the basis of this it wasagreed that a Delphi format would be beneficial to help developguidelines A questionnaire was developed using Survey Monkey6
and distributed to ACPGBI members covering all ACPGBI regionalchapters The initial round was completed on-line by participantsprior to a meeting with a further 2 rounds (See Table 7 Appendix)
Definitions and epidemiology of ALDefinitionThe preferred definition for anastomotic leaks was lsquoA leak ofluminal contents from a surgical join between two hollow viscerarsquo7
EpidemiologyThe prevalence of AL varies from 1 to 19 depending uponanatomical site pre intra and postoperative factors5 These arediscussed below
9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

5
INTRODUCTIONAn anastomotic leak as all colorectal surgeons are aware is adevastating complication that may not only result in severemorbidity but can also unfortunately lead to the demise of thepatient We all fear it and will do all we can to prevent it Howeverno matter how skilled the surgeon may be there are times when thiscomplication will occur despite best efforts
These guidelines which have been developed by an exhaustivereview of the literature and meticulous scientific process provideextremely valuable advice as how to prevent diagnose treat and -very importantly - counsel patients about the possibility of thisdreaded complication The group have worked diligently to sift andinterpret the information and are to be commended on producing adocument that is clear concise and balanced If teams follow theiradvice there is no doubt in my mind that the incidence ofanastomotic leakage will be reduced but also when it occurs liveswill be saved
I do hope that all practicing surgeons will heed the current thinkingthat is embodied in the document and apply it appropriately
Professor Sir Norman WilliamsMS FRCS FMed Sci FRCP FRCP (Edin) FRCA FDS (Hon)FACS (Hon) FRCSI (Hon) FRCSEd (Hon)
Past President The Royal College of Surgeons of EnglandDirector National Centre for Bowel Research and SurgicalInnovation Barts amp The London School of Medicine amp Dentistry
6
Patient PerspectiveWhilst this document is intended to review the clinical evidence onthe prevention diagnosis and management of anastomotic leakage itis essential that the impact of anastomotic leakage on the patient andtheir family is also considered Good communication remains animportant aspect of care
Careful history taking may elicit important risk factors foranastomotic leakage (eg a history of smoking or alcohol abuse)which may not otherwise be evident and about which some patientsmay be reticent
It is important to prepare patients and their families for surgerywhere an anastomosis is being considered by giving a balancedassessment of the risk of anastomotic leakage This will allow better-informed decision-making regarding whether the risk of ananastomosis (in particular a higher risk anastomosis) is acceptableor whether a stoma may be preferable This may enable patients tomake a better-informed choice and to be better prepared to deal withthe consequences of an anastomotic leak should this occur
Good quality timely information before and after surgery is part ofthis process and should include input from an enterostomal therapistwhich may help allay the patientrsquos fears with regard to a stoma andits impact on future quality of life
Patients who have suffered from anastomotic leakage should notonly be offered prompt and appropriate medical attention but afrank open and honest discussion about the complication as soon astheir condition permits They should have access to psychologicalsupport to help them deal with associated anger grief and stress
Jo ChurchPatient Representative
7
AcknowledgementsThe authors wish to thank the following members of theASGBIACPGBI joint anastomotic leak working group for generouslygiving their time and effort in assessing the clinical evidence andproviding expert opinion
Austin Acheson Tan Arulampalam Arnie Bhowmick Cat BoereboomKen Campbell Jo Church (Patient Liaison) Mark Coleman JustinDavies Michael Davies Peter Dawson Nicola Fearnhead NaderFrancis Richard Guy Nigel Hall Athur Harikrishnan Deena HarjiCharles Hendrickse Stephen Holtham Kourosh Khosraviani RobinKennedy Anil Lala Gerald Langman Charles Maxwell-ArmstrongBrendan Moran Neil Smart Henry Tilney Jared Torkington JanindraWarusavitarne
Thank you to Louise Hull for her assistance with the DelphiMethodology
AbbreviationsAL Anastomotic leak
ASA American Society of Anaesthesiologists Physical StatusClassification
BMI Body mass index
CI Confidence intervals
CRP C-reactive protein
DFS Disease free survival
IR Interventional radiology
NSAID Non-steroidal anti-inflammatory drug
OS Overall Survival
OR Odd Ratio
RCT Randomised Control Trial
SDD Selective decontamination of the digestive tract
TNF Tumour necrosis factor
WHR Waist hip ratio
8
IntroductionAnastomotic leaks (AL) are potentially catastrophic complicationsof colorectal surgery The spectrum of clinical severity associatedwith AL is broad however ranging from a small-contained leakwithout sepsis in a patient with a defunctioning stoma to a patientwith four-quadrant peritonitis and septic shock ALs increase theneed for reoperation the risk of local recurrence1 and reduce bothoverall (OS) and disease free survival (DFS)2-4 Despite the gravityof the complication and potential sequelae data regarding riskfactors and optimal perioperative management of ALs are relativelypoor and few attempts have been made to bring together the datawhich are available in order to provide clinical guidance Thisdocument aims to present the current best evidence and utilisedDelphi methodology to provide expert colorectal opinion
Development Of Methodology amp Delphi Meeting A systematic review of the literature searching for colorectalanastomotic leaks was performed5 Due to low quality evidenceacross multiple domains of risk factors assessment and managementof ALs a Delphi methodology was proposed Following the reviewand Delphi process it was agreed that formal gradingstrength ofrecommendation would be inappropriate due to the lack of highquality evidence A formal cut-off for consensus was not used ratherthe evidence was discussed and the percentage consensus after 3rounds of discussion is presented in brackets
A steering group of colorectal consultants and trainees was formedand met at the Tripartite meeting in Birmingham in July 2014Current evidence was presented and on the basis of this it wasagreed that a Delphi format would be beneficial to help developguidelines A questionnaire was developed using Survey Monkey6
and distributed to ACPGBI members covering all ACPGBI regionalchapters The initial round was completed on-line by participantsprior to a meeting with a further 2 rounds (See Table 7 Appendix)
Definitions and epidemiology of ALDefinitionThe preferred definition for anastomotic leaks was lsquoA leak ofluminal contents from a surgical join between two hollow viscerarsquo7
EpidemiologyThe prevalence of AL varies from 1 to 19 depending uponanatomical site pre intra and postoperative factors5 These arediscussed below
9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

6
Patient PerspectiveWhilst this document is intended to review the clinical evidence onthe prevention diagnosis and management of anastomotic leakage itis essential that the impact of anastomotic leakage on the patient andtheir family is also considered Good communication remains animportant aspect of care
Careful history taking may elicit important risk factors foranastomotic leakage (eg a history of smoking or alcohol abuse)which may not otherwise be evident and about which some patientsmay be reticent
It is important to prepare patients and their families for surgerywhere an anastomosis is being considered by giving a balancedassessment of the risk of anastomotic leakage This will allow better-informed decision-making regarding whether the risk of ananastomosis (in particular a higher risk anastomosis) is acceptableor whether a stoma may be preferable This may enable patients tomake a better-informed choice and to be better prepared to deal withthe consequences of an anastomotic leak should this occur
Good quality timely information before and after surgery is part ofthis process and should include input from an enterostomal therapistwhich may help allay the patientrsquos fears with regard to a stoma andits impact on future quality of life
Patients who have suffered from anastomotic leakage should notonly be offered prompt and appropriate medical attention but afrank open and honest discussion about the complication as soon astheir condition permits They should have access to psychologicalsupport to help them deal with associated anger grief and stress
Jo ChurchPatient Representative
7
AcknowledgementsThe authors wish to thank the following members of theASGBIACPGBI joint anastomotic leak working group for generouslygiving their time and effort in assessing the clinical evidence andproviding expert opinion
Austin Acheson Tan Arulampalam Arnie Bhowmick Cat BoereboomKen Campbell Jo Church (Patient Liaison) Mark Coleman JustinDavies Michael Davies Peter Dawson Nicola Fearnhead NaderFrancis Richard Guy Nigel Hall Athur Harikrishnan Deena HarjiCharles Hendrickse Stephen Holtham Kourosh Khosraviani RobinKennedy Anil Lala Gerald Langman Charles Maxwell-ArmstrongBrendan Moran Neil Smart Henry Tilney Jared Torkington JanindraWarusavitarne
Thank you to Louise Hull for her assistance with the DelphiMethodology
AbbreviationsAL Anastomotic leak
ASA American Society of Anaesthesiologists Physical StatusClassification
BMI Body mass index
CI Confidence intervals
CRP C-reactive protein
DFS Disease free survival
IR Interventional radiology
NSAID Non-steroidal anti-inflammatory drug
OS Overall Survival
OR Odd Ratio
RCT Randomised Control Trial
SDD Selective decontamination of the digestive tract
TNF Tumour necrosis factor
WHR Waist hip ratio
8
IntroductionAnastomotic leaks (AL) are potentially catastrophic complicationsof colorectal surgery The spectrum of clinical severity associatedwith AL is broad however ranging from a small-contained leakwithout sepsis in a patient with a defunctioning stoma to a patientwith four-quadrant peritonitis and septic shock ALs increase theneed for reoperation the risk of local recurrence1 and reduce bothoverall (OS) and disease free survival (DFS)2-4 Despite the gravityof the complication and potential sequelae data regarding riskfactors and optimal perioperative management of ALs are relativelypoor and few attempts have been made to bring together the datawhich are available in order to provide clinical guidance Thisdocument aims to present the current best evidence and utilisedDelphi methodology to provide expert colorectal opinion
Development Of Methodology amp Delphi Meeting A systematic review of the literature searching for colorectalanastomotic leaks was performed5 Due to low quality evidenceacross multiple domains of risk factors assessment and managementof ALs a Delphi methodology was proposed Following the reviewand Delphi process it was agreed that formal gradingstrength ofrecommendation would be inappropriate due to the lack of highquality evidence A formal cut-off for consensus was not used ratherthe evidence was discussed and the percentage consensus after 3rounds of discussion is presented in brackets
A steering group of colorectal consultants and trainees was formedand met at the Tripartite meeting in Birmingham in July 2014Current evidence was presented and on the basis of this it wasagreed that a Delphi format would be beneficial to help developguidelines A questionnaire was developed using Survey Monkey6
and distributed to ACPGBI members covering all ACPGBI regionalchapters The initial round was completed on-line by participantsprior to a meeting with a further 2 rounds (See Table 7 Appendix)
Definitions and epidemiology of ALDefinitionThe preferred definition for anastomotic leaks was lsquoA leak ofluminal contents from a surgical join between two hollow viscerarsquo7
EpidemiologyThe prevalence of AL varies from 1 to 19 depending uponanatomical site pre intra and postoperative factors5 These arediscussed below
9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

7
AcknowledgementsThe authors wish to thank the following members of theASGBIACPGBI joint anastomotic leak working group for generouslygiving their time and effort in assessing the clinical evidence andproviding expert opinion
Austin Acheson Tan Arulampalam Arnie Bhowmick Cat BoereboomKen Campbell Jo Church (Patient Liaison) Mark Coleman JustinDavies Michael Davies Peter Dawson Nicola Fearnhead NaderFrancis Richard Guy Nigel Hall Athur Harikrishnan Deena HarjiCharles Hendrickse Stephen Holtham Kourosh Khosraviani RobinKennedy Anil Lala Gerald Langman Charles Maxwell-ArmstrongBrendan Moran Neil Smart Henry Tilney Jared Torkington JanindraWarusavitarne
Thank you to Louise Hull for her assistance with the DelphiMethodology
AbbreviationsAL Anastomotic leak
ASA American Society of Anaesthesiologists Physical StatusClassification
BMI Body mass index
CI Confidence intervals
CRP C-reactive protein
DFS Disease free survival
IR Interventional radiology
NSAID Non-steroidal anti-inflammatory drug
OS Overall Survival
OR Odd Ratio
RCT Randomised Control Trial
SDD Selective decontamination of the digestive tract
TNF Tumour necrosis factor
WHR Waist hip ratio
8
IntroductionAnastomotic leaks (AL) are potentially catastrophic complicationsof colorectal surgery The spectrum of clinical severity associatedwith AL is broad however ranging from a small-contained leakwithout sepsis in a patient with a defunctioning stoma to a patientwith four-quadrant peritonitis and septic shock ALs increase theneed for reoperation the risk of local recurrence1 and reduce bothoverall (OS) and disease free survival (DFS)2-4 Despite the gravityof the complication and potential sequelae data regarding riskfactors and optimal perioperative management of ALs are relativelypoor and few attempts have been made to bring together the datawhich are available in order to provide clinical guidance Thisdocument aims to present the current best evidence and utilisedDelphi methodology to provide expert colorectal opinion
Development Of Methodology amp Delphi Meeting A systematic review of the literature searching for colorectalanastomotic leaks was performed5 Due to low quality evidenceacross multiple domains of risk factors assessment and managementof ALs a Delphi methodology was proposed Following the reviewand Delphi process it was agreed that formal gradingstrength ofrecommendation would be inappropriate due to the lack of highquality evidence A formal cut-off for consensus was not used ratherthe evidence was discussed and the percentage consensus after 3rounds of discussion is presented in brackets
A steering group of colorectal consultants and trainees was formedand met at the Tripartite meeting in Birmingham in July 2014Current evidence was presented and on the basis of this it wasagreed that a Delphi format would be beneficial to help developguidelines A questionnaire was developed using Survey Monkey6
and distributed to ACPGBI members covering all ACPGBI regionalchapters The initial round was completed on-line by participantsprior to a meeting with a further 2 rounds (See Table 7 Appendix)
Definitions and epidemiology of ALDefinitionThe preferred definition for anastomotic leaks was lsquoA leak ofluminal contents from a surgical join between two hollow viscerarsquo7
EpidemiologyThe prevalence of AL varies from 1 to 19 depending uponanatomical site pre intra and postoperative factors5 These arediscussed below
9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

8
IntroductionAnastomotic leaks (AL) are potentially catastrophic complicationsof colorectal surgery The spectrum of clinical severity associatedwith AL is broad however ranging from a small-contained leakwithout sepsis in a patient with a defunctioning stoma to a patientwith four-quadrant peritonitis and septic shock ALs increase theneed for reoperation the risk of local recurrence1 and reduce bothoverall (OS) and disease free survival (DFS)2-4 Despite the gravityof the complication and potential sequelae data regarding riskfactors and optimal perioperative management of ALs are relativelypoor and few attempts have been made to bring together the datawhich are available in order to provide clinical guidance Thisdocument aims to present the current best evidence and utilisedDelphi methodology to provide expert colorectal opinion
Development Of Methodology amp Delphi Meeting A systematic review of the literature searching for colorectalanastomotic leaks was performed5 Due to low quality evidenceacross multiple domains of risk factors assessment and managementof ALs a Delphi methodology was proposed Following the reviewand Delphi process it was agreed that formal gradingstrength ofrecommendation would be inappropriate due to the lack of highquality evidence A formal cut-off for consensus was not used ratherthe evidence was discussed and the percentage consensus after 3rounds of discussion is presented in brackets
A steering group of colorectal consultants and trainees was formedand met at the Tripartite meeting in Birmingham in July 2014Current evidence was presented and on the basis of this it wasagreed that a Delphi format would be beneficial to help developguidelines A questionnaire was developed using Survey Monkey6
and distributed to ACPGBI members covering all ACPGBI regionalchapters The initial round was completed on-line by participantsprior to a meeting with a further 2 rounds (See Table 7 Appendix)
Definitions and epidemiology of ALDefinitionThe preferred definition for anastomotic leaks was lsquoA leak ofluminal contents from a surgical join between two hollow viscerarsquo7
EpidemiologyThe prevalence of AL varies from 1 to 19 depending uponanatomical site pre intra and postoperative factors5 These arediscussed below
9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

9
Avoidance of Anastomotic LeakagePreoperative considerationsIdentification of significant preoperative risk factors may guide theproposed treatment and allow modification of risk Preoperativealteration of lifestyle andor treatment may not always be possibleparticularly in the emergency setting However consideration of riskfactors is relevant in the decision-making process with regard towhether an anastomosis is a safe option and whether a defunctioning(or permanent) stoma should be considered At the very least if apatient opts for a ldquohigh riskrdquo anastomosis despite the identification ofsignificant risk factors for AL this should be on the basis of clearlydocumented discussion regarding the alternative safer optionsPreoperative risk factors for AL may be modifiable or non-modifiable
Modifiable risk factors
AlcoholEthanol consumption in excess of recommended levels (gt105galcohol per week) is associated with an increased risk of AL8 In theUK 1 unit of alcohol is the equivalent of 8 grams of pure alcohol
SmokingTobacco smoking both current and historical is associated with anincreased risk of AL Several studies have demonstrated currentsmoking to be an independent risk factor9-13 Additionally a previoussmoking history (gt40 pack years) is an independent risk factor for AL14
ObesitySeveral studies have shown obesity to independently increase therisk of AL15-18 While obesity has often been poorly defined in thesestudies and the degree of obesity and associated increase in risk mayconsequently be open to interpretation it is nevertheless clearlyassociated with a measurable increase in the risk of AL Measuresof central obesity such as waist circumference and waist-hip ratiosmay be more sensitive than BMI in predicting AL19
MedicationTable 1 details medication reportedly associated with an increasedrisk of AL Some of the evidence is however weak orcontradictory There is experimental evidence of increased risk ofAL for several immunosuppressant drugs used in patients who haveundergone organ transplantation This is consistent with reports ofa higher AL rate in immunosuppressed patients after renaltransplantation20
10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

10
Table 1 Medication associated with increased risk of AL
Nutrition and HypoalbuminaemiaMalnutrition (defined as an unintentional loss of weight of gt10 in thepreceding 6 months) and a serum albumin concentration of lt35gLincreases the risk of AL32-36 Hypoalbuminaemia is more likely to beassociated with a systemic inflammatory response secondary to necroticor perforated tumours or sepsis (see below) than related to nutritionaldepletion per se Nutritional assessment should be undertaken in allpatients being prepared for surgery and an attempt made to correctmalnutrition The underlying cause of hypoalbuminaemia should also becorrected where possible (for example by treating infection) It shouldbe noted that it is not the hypoalbuminaemia itself which confers theadditional risk but the metabolic conditions which lead to it (systemicinflammation and increased capillary permeability) Thus preoperativeadministration of albumin to temporarily increase serum albuminconcentration will not abnegate the associated increase in risk of AL Inthe event that it is not possible to correct significant malnutrition (gt10unintentional weight loss) andor hypoalbuminaemia (lt32gL)preoperatively (for example in a patient with a large necrotic tumourandor because of impending intestinal obstruction or perforation) theoperative strategy should be modified so as to avoid undertaking ananastomosis at that time if it is possible to do so
Medication Type Evidence amp Recommendations
Corticosteroids Steroid Prolonged use may increase AL21 22
Infliximab Anti-TNFprop Slows woundmonoclonal healing but noanti-body impact on AL rate23 24
Mycophenolate Immunosuppressant Mycophenolate ALmofetil25 risk based on clinical
observational studyCyclosporine A26
For other drugs
Tacrolimus27 experimental evidencesuggests increased
Everolimus28 AL risk
Azathioprine Purine analogue Contradictoryimmunosuppressant evidence29 30
Bevacizumab VEGF inhibitor Should be stopped andnot restarted for at least 28 days either side of surgery (manufacturer advice)31
11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

11
Mechanical Bowel Preparation (MBP)Mechanical bowel preparation (MBP) has traditionally been usedto reduce stool burden in the colon with the additional benefitsof improving visualisation for intraoperative endoscopy andfacilitating the insertion of stapling devices Withholding MBPdoes not appear to have resulted in increased AL rate in severalrandomised trials and a systematic review37-41 The GRECCAR IIIRCT demonstrated an overall reduction in septic complications inrectal surgery alone in patients receiving MBP although therewas no difference in AL42 Bowel preparation is unpleasant forpatients and is not essential for colorectal surgery
RadiotherapyNeoadjuvant radiotherapy usually in combination withchemotherapy has been demonstrated to reduce local recurrenceand to downstage rectal tumours43 Retrospective series havepreviously suggested that chemoradiotherapy might increaseAL44 45 However this has not been supported by several RCTsincluding the MRC CR07 and Dutch TME trials46-48 A previoushistory of pelvic radiotherapy does however increase AL rateand is discussed in Table 2
Preoperative antibiotics and selective decontamination of thedigestive tractPreoperative broad-spectrum intravenous antibiotics are routinelyused in elective and emergency colorectal surgery with the goalof reducing postoperative infective complications and thispractice is recommended by ACPGBI49 In the USA somesurgeons routinely use non-absorbable oral antibiotics such asTobramycin and Amphotericin B - also known as selectivedecontamination of the digestive tract (SDD) A systematicreview has indicated that SDD reduces anastomotic leak ratesfrom 74 to 3350 This finding has also been replicated in arecent study of over 8000 colorectal resections demonstratingboth lower surgical site infection and anastomotic leak rates inthe treatment group51 Despite this SDD is not currently inwidespread practice in the United Kingdom and Ireland
Non-modifiable risk factors
Gender and ageMale gender and increasing age (especially age over 60) mayincrease the risk of AL While the effect of gender on rectalanastomotic leakage might be attributable to greater technicaldifficulty of undertaking surgery in the narrower male pelvis thisdoes not explain the higher rate of AL seen in colonic surgery Theeffect of chronological age is not observed consistently and is mostprobably accounted for by co-morbidity (Table 2)
12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

12
Table 2 Summary of non-modifiable risk factors for anastomotic leak
History of RadiotherapyWhile immediate preoperative radiotherapy might represent amodifiable risk factor a history of previous pelvic radiotherapyclearly does not Previous radical pelvic radiotherapy is associatedwith a very high risk of AL in the radiotherapy field Considerationshould be given to avoiding anastomoses in bowel previouslysubjected to radiation (however many years earlier) particularly inthe presence of other risk factors
Risk Factor Evidence
Gender Male gender increases AL rate in colonic10 andrectal45 52 anastomoses
Age Some studies have demonstrated that increasingage or age gt60 is associated with an increasedrisk of AL53 54 Other studies in elderlypopulations have failed to report this55 It isprobably more important to consider thebiological age of the patient and other riskfactors rather than chronological age per se
History of Patients previously treated with radiotherapy egradiotherapy for cervical or prostate cancer have AL rates
documented to be as high as 3656 This must beconsidered when planning an anastomosis
Diabetes The evidence is contradictory Two studies haveMellitus suggested an increased AL rate in ileocolic
anastomoses15 or low anterior resection57 whereasanother paper has demonstrated no change in ALrate but higher mortality in those who do sustaina leak58
Co-morbidity Increase in AL rate
bull Pulmonary disease21 22 59
bull Vascular disease44
bull Renal diseaserenal replacement therapyimmunosuppressed renal transplant patients20 60 61
(Haemodialysing patients pre and post-surgicalintervention reduces surgical complications butnot anastomotic leaks anastomosis should beavoided in emergency cases)
bull ASA of greater than 262 315 and 463 have beendemonstrated to increase risk of AL
13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

13
DiabetesAlthough there is conflicting evidence for an increased risk of AL inpatients with diabetes (see Table 2) there is evidence for increasedperioperative mortality64 and increased length of stay65 In additionthere is evidence of increased perioperative morbidity due to pre-existing complications including cerebrovascular cardiovasculardisease and nephropathy66-68 There are NHS guidelines published inconjunction with ASGBI and other organisations for the optimumperioperative management of diabetes69
Elective vs Emergency SurgeryEmergency surgery is predictably associated with higher AL ratescompared with elective practice However an emergency operationper se is not an absolute contraindication to an anastomosis withseveral studies demonstrating for example that an anastomosis with adefunctioning stoma is a safe option for perforated diverticulitis70-72However the risk factors outlined in this document and in particularhaemodynamic instability shock inotrope requirements andhypoalbuminaemia must be taken into account when considering ananastomosis and the need for a defunctioning stoma Wheneverpossible the risks and benefits of and alternatives to a primaryanastomosis should be discussed with the patient before surgery sothat an appropriately informed decision can be made However therewill be some emergency circumstances when this may not be possible
Tumour factorsDistal anastomoses particularly those of infraperitoneal rectum havethe highest anastomotic leak rates Distance from the anorectaljunction is an independent predictive risk factor for AL9 45 73 Otherfactors that increase AL rate are tumour size gt3cm74 or gt4cm75advanced tumour stage45 and in particular the presence of distantmetastases11 It is likely that many of these factors are interrelatedFor example late presentation with advanced disease is likely to beassociated not only with lower socioeconomic status but also poornutritional status smoking and medical comorbidity
Intraoperative considerationsOperative TechniquePoor operative technique for example failing to avoid tension on orpoor vascularity at an anastomosis will impact negatively onanastomotic healing and is likely to result in AL Operative duration ofgreater than 4 hours intraoperative contamination blood loss over100ml and blood transfusion are risk factors for AL76-79 as is hypoxia80The use of vasopressors is associated with a threefold increase in AL81
Goal directed fluid therapyThe National Institute for Health and Care Excellence (NICE)recommends the use of goal directed therapy eg the use ofoesophageal doppler82 Goal directed therapy has been shown to
14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

14
reduce postoperative complications for major surgery but it has notbeen shown to reduce anastomotic leak rates per se83 84
Interventions Suturing as opposed to stapling an anastomosis may be associatedwith a higher risk of AL although the difference may be only detectedradiologically and is not manifest clinically85 Specifically meta-analysis favours stapled anastomosis in ileocolic resections86 but nosuperiority has been demonstrated between anastomotic techniquesfor anterior resection of the rectum87 Other technical interventionsthat may reduce the risk of AL include utilising air leak tests88 lowversus high ties on vascular pedicles89 and open compared tolaparoscopic surgery90 although the last finding has not beensubstantiated on meta-analysis91
Irrespective of the quality of scientific evidence it is appropriate tonote that a recent legal judgement in England regarding the routineuse of air leak testing in rectal anastomoses (Shortall-v-Mid EssexHospital Services NHS Trust 2014) concluded that failure to use thistechnique was held to be negligent While the technique may not besupported by sufficient weight of clinical evidence (and clearlycannot provide reassurance regarding leakage caused by excessivetension or ischaemia) it seems sensible to recommend that all rectalanastomoses (and probably all left sided colonic anastomoses) forwhich a defunctioning proximal stoma is not being undertaken shouldroutinely be tested for immediate ldquotechnicalrdquo defects by airinsufflation (or a similar technique)
The use of a defunctioning stoma andor an omentoplasty to isolatethe anastomosis may reduce the adverse consequences of AL butdoes not appear to reduce the likelihood of AL per se 92 93
Drains have historically been used following colorectal anastomoseswith the perceived benefit of identifying and potentially reducingpostoperative complications The use of drains for both colonic andinfraperitoneal rectal anastomoses is debated However there havebeen several large systematic reviews including a Cochrane review onthe use of drains for colorectal anastomoses that do not demonstratea significant reduction in AL rate94-96 The Cochrane review assessed1140 patients from 6 RCTs and showed no reduction in clinical orradiological anastomotic leaks (or any other complications forcolorectal anastomoses) Specific to rectal infraperitonealanastomoses a meta-analysis combining 3 RCTs and 5 retrospectivestudies demonstrated a reduction in anastomotic leak (OR 051 95CI 036 ndash 073)97 This effect was not seen however when the 3 RCTswere analysed in isolation96 In summary drainage is not routinelyrequired for colonic anastomoses but to properly assess their use ininfraperitoneal rectal anastomoses would require an appropriatelypowered RCT Their use in this setting specifically with respect toavoidance of AL is therefore currently a matter of personal choice
15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

15
Table 3 Summary of preoperative and intraoperative risk factors
Postoperative considerationsNSAIDsThere is growing evidence that NSAIDs should be used with cautionin the postoperative period A meta-analysis has demonstrated thatnon-selective NSAIDs were associated with an increased risk of ALHowever many of the studies included were flawed and had selectionbias98 More recently a retrospective cohort study of over 13000bariatric and colorectal operations has demonstrated a 24 increasein the likelihood of AL with NSAID use This effect appears to have
Preoperative considerations Intraoperative considerations
Non-modifiable risk factors Increase risk
bull Male gender bull Intraoperative contamination
bull Distal rectal anastomosis bull Duration gt4 hours
bull Tumour size gt3cm bull Inotropes
bull Advanced tumour stage bull Blood loss
bull Metastatic disease bull Blood transfusion
bull History of radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units105g alcohol week)
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

16
been attributable to emergency colorectal operations 123 vs 83in the NSAID and non-NSAID group respectively (OR 17 [95 CI111 ndash 268] p = 001)99
Diagnosis of Anastomotic LeakagePrompt diagnosis of AL is essential for effective management Delayeddiagnosis of AL is associated with worse outcomes100 Clinicians musttherefore be alert to early and subtle signs of AL including non-specific signs notably cardiac arrhythmias including atrialfibrillation101102 Postoperative ileus is unusual after uncomplicatedlaparoscopic colorectal surgery and should lead to urgent assessmentfor anastomotic leakage Rectal bleeding or passage of bloody mucusper rectum should cause suspicion of anastomotic leakage after arectal anastomosis It cannot be emphasised strongly enough thatfailure to make anticipated postoperative progress in any patient witha colorectal anastomosis should above all raise the suspicion ofanastomotic leakage
In patients in whom there is a departure from the expected pattern ofpostoperative recovery frequently repeated assessment by a seniorexperienced clinician and careful analysis of trends in observationsremain the most valuable and reliable means of establishing earlydiagnosis of AL It can be difficult for any surgeon to remain entirelyobjective when considering the likelihood of leakage from ananastomosis they have created themselves Asking a similarlyexperienced colleague to provide a second opinion in thesecircumstances is therefore extremely valuable and is stronglyrecommended103
Raised concentrations of serum C-reactive protein and procalcitoninmay be useful (but non-specific) markers for AL particularly if CRPis very high (gt150mgL) on postoperative days 3-5104 105 andespecially if the serum albumin continues to fall or fails to return tonormal postoperatively The negative predictive value of a normalCRP in this context may be particularly useful In contrast white cellcount appears to be less reliable as a marker of AL44
Diagnostic imaging is not essential when a patient is unwell and a leakis clinically evident and imaging under these circumstances may giverise to unnecessary delay in management The sensitivity of commonimaging modalities such as CT scanning and water-soluble contrastenema is dependent on the timing of investigations the quality of thetechnique used and the skill and experience of the radiologist Thediagnostic accuracy of CT for suspected leakage from the distal colonmay be improved with the addition of rectal and intravenouscontrast106 Cross sectional imaging should not be undertaken in thepresence of haemodynamic instability unless invasive monitoring isavailable and the patient is accompanied throughout by critical carepersonnel who can provide immediate cardiorespiratory supportIntravenous contrast should be used with caution (or avoided) in thepresence of dehydration hypotension or acute kidney injury
17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

17
Scoring systemsA variety of scoring systems have been developed to assist inprediction diagnosis or grading the severity of AL None has provedsufficiently valuable to gain widespread acceptance or incorporationinto routine practice The colon leakage score (CLS) attempts topredict AL for left sided colonic resection using 11 patient andoperative factors107 The modified DULK score is an aid to thediagnosis of AL but has a low positive predictive value108 TheInternational Study group of Rectal Cancer devised a grading systemfor severity of leak but this is relatively simplistic suggesting only ldquonointervention active non-operative intervention or re-laparotomyrdquo109
Treatment of Anastomotic Leakage Initial ManagementThere is an international drive to improve the management of sepsiswhich remains the major cause of morbidity and mortality associatedwith AL Systemic inflammatory response syndrome (SIRS) consistsof 6 criteria temperature gt383˚C or lt36˚C respiratory rate gt20minheart rate gt90min white cell count lt4x109l or gt12x109l alteredmental state and a blood glucose level of gt77mmoll in the absenceof diabetes Sepsis is currently defined as the presence of at least 2of the SIRS criteria as a result of infection Severe sepsis is definedas sepsis with evidence of super-added organ dysfunction(hypotension oliguria high serum lactate) Septic shock is definedas failure of these parameters to respond to adequate fluidresuscitation Patients with severe sepsis are at particular risk ofdeveloping septic shock and it is imperative that septic shock isavoided in order to avoid associated high mortality rate A delay ofsource control in excess of 12 hours after the development ofhypotension compared with less than 3 hours has been previouslyshown to increase mortality from 25 to 60110
Timely and appropriate intervention is therefore imperative if apatient develops sepsis as a consequence of AL Initial managementshould include the ldquosepsis sixrdquo care bundle111 ldquoSepsis sixrdquo is a set of6 criteria which when implemented have been shown to result in a466 reduction in the relative risk of mortality from sepsis112 Theseinterventions are administering high flow oxygen taking bloodcultures measuring lactate and full blood count urine outputadministration of broad-spectrum antibiotics and intravenous fluidchallenge
18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

18
Subsequent and Definitive Management 1 General principles
Subsequent management requires a thorough assessment of thepatientrsquos clinical stability A stable patient may initially beadequately managed conservatively with fluids antibiotics andoxygen together with close clinical observation Conversely anurgent attempt to achieve source control should be undertaken inany patient with an AL and severe sepsis or septic shock withinthe time frame indicated below
A patient with an AL should be nursed in an environmentappropriate to their level of systemic illness and the consequentneed for monitoring Recommended time limits for interventionin the treatment of abdominal sepsis associated with AL havebeen identified previously and are determined by the severity ofsepsis113 In the absence of organ dysfunction surgical orradiological intervention to achieve source control should beundertaken as soon as possible (where this is required) but alwayswithin 18 hours of diagnosis If sepsis is complicated by evidenceof organ dysfunction source control should be achieved as soonas possible but always within 6 hours of diagnosis Septic shockshould result in source control immediately and always within 3hours if preventable death is to be avoided
2 Source controlControl of the source of infection associated with AL mayoccasionally be unnecessary Such patients will usually be stableand well without evidence of sepsis but may have some localisedabdominal tenderness raised inflammatory markers andgastrointestinal dysfunction (for example ileus andor diarrhoea)Imaging in these cases usually shows no evidence of anastomoticdiscontinuity and little more than a small perianastomoticcollection Complete resolution can be expected in most caseswith conservative treatment including intravenous antibioticsintestinal rest (oral fluids only or parenteral nutrition) and closemonitoring in the ward environment for signs of sepsis
A small contained AL in a haemodynamically stable patientwithout radiological evidence of anastomotic discontinuity maybe managed successfully by radiologically guided drainageandor washout and defunctioning rather than taking down theanastomosis and creating a stoma provided there is continuedclose observation and evidence of improvement Radiologicaldrainage should not be undertaken when there is radiologicalevidence of complete anastomotic discontinuity as it is unlikelyto control sepsis adequately and anastomotic healing cannotoccur Multiple separate foci of intraabdominal infectionassociated with AL are not usually suitable for radiologicaldrainage and if present on cross sectional imaging generally
19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

19
represent an indication for surgical source control Laparotomy isusually required
In low rectal ALs transanal drainage may be effective Endoscopicplacement of vacuum devices into the presacral cavity (eg anEndo-SPONGEreg) may also be of benefit under thesecircumstances but adequate evaluation of the efficacy and costeffectiveness of this technique is required114
Development of or deterioration in the severity of sepsis in apatient treated conservatively or by radiological drainage for ALshould be considered ldquofailedrdquo treatment and a low thresholdmaintained for taking a patient urgently to theatre and taking downthe anastomosis Attempts to ldquorepairrdquo an AL should never beundertaken in the presence of severe sepsis or septic shock inpatients with AL requiring inotropes and in those with significanthypoalbuminaemia (lt32gL) A repair should not be attempted ifthere is an established abscess cavity at the anastomosisSatisfactory healing under these circumstances is unlikely to occurand it is far safer to exteriorise the affected segments Similarlyenterotomies made during laparotomies under these circumstancesare unlikely to heal adequately and injured bowel should beresected andor exteriorised if further abdominal sepsis andintestinal failure is to be prevented103 Operating upon a patientwith an AL can not only be technically challenging but alsoemotionally difficult for the surgeon who constructed the ldquofailedrdquoanastomosis It may be associated with significant feelings of guiltand can impair objective decision-making Involving the assistanceof a second consultant colleague in re-operative procedures is notan admission of failure or inadequacy but is good practice underthese circumstances and is strongly encouraged103
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk
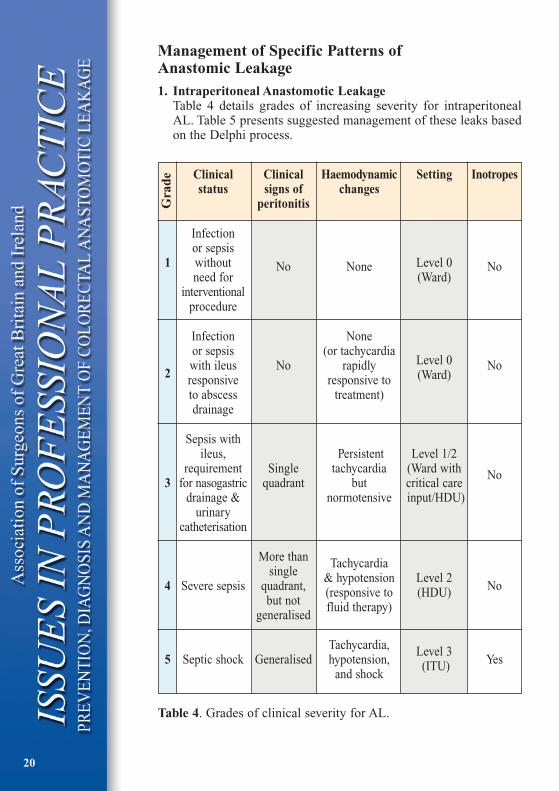
20
Management of Specific Patterns ofAnastomic Leakage1 Intraperitoneal Anastomotic Leakage
Table 4 details grades of increasing severity for intraperitonealAL Table 5 presents suggested management of these leaks basedon the Delphi process
Table 4 Grades of clinical severity for AL
Clinical Clinical Haemodynamic Setting Inotropesstatus signs of changes
peritonitis
Infectionor sepsis
1 without No None Level 0 Noneed for (Ward)
interventionalprocedure
Infection Noneor sepsis (or tachycardiawith ileus No rapidly Level 0 No
2 responsive responsive to (Ward)
to abscess treatment)drainage
Sepsis withileus Persistent Level 12
requirement Single tachycardia (Ward with No3 for nasogastric quadrant but critical care
drainage amp normotensive inputHDU)urinary
catheterisation
More than Tachycardiasingle amp hypotension
4 Severe sepsis quadrant (responsive toLevel 2
Nobut not fluid therapy)
(HDU)
generalised
Tachycardia Level 35 Septic shock Generalised hypotension (ITU) Yes
and shock
Gra
de
21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

21
Table 5 Suggested management of intraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In these scenariosit is assumed in all cases that patients are being appropriatelyresuscitated with oxygen intravenous fluids and antibiotics
2 Extra-peritoneal Anastomotic LeakageThe highest leak rates occur with extra-peritoneal (low pelvic)anastomoses9 45 115 116 However because peritoneal contaminationis less likely to occur and the majority of patients will have acovering loop stoma the clinical signs may be more subtleManagement (Table 6) will depend upon the patientrsquos clinical
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)1 Conservative None Level 0 1
(89) (96)
Sepsis contained leak abscess (Grade 2)
Drainage needed Radiological drainage if Level 0 -2(80) possible If unavailable (100)
laparoscopy laparotomy2 washout drain and repair AL
with proximal defunctioningstoma or resect anastomosisand create stoma(85)
Sepsis ileusSingle quadrant peritonitis (Grade 3) Level 2
Resuscitate and Laparoscopy Laparotomy (96)operation washout drain and proximal3(85) defunctioning stoma or resect
anastomosis and create stoma(92)
Severe sepsismore than single quadrant peritonitis (Grade 4)
4Resuscitate and Laparoscopy Laparotomy Level 23operation washout resect anastomosis (100)(100) and create stoma (85)
5 Septic shockgeneralised peritonitis (Grade 5)
Resuscitate and Laparoscopy Laparotomy Level 3operation washout resect anastomosis (96)(100) and create stoma (100)
22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

22
stability as indicated above (Table 6) Take down of the anastomosisis recommended for all patients who develop severe sepsis or septicshock after an extraperitoneal AL
Table 6 Suggested management of extraperitoneal AL based onDelphi meeting (percentage consensus in brackets) In thesescenarios it is assumed in all cases that patients are beingappropriately resuscitated with intravenous fluids and antibiotics
CaseManagement Source Control SettingScenario
No sepsis (Grade 1)
1 Conservative Drainage (IRtransperineal Level 0 1(89) transanal) plusmn proximal (96)
defunctioning stoma (76)
Sepsis with contained leak abscess lt3cm (Grade 2)
Drainage needed bull Transperinealtransanal drainage Level 0 -2(70) plusmn proximal defunctioning (100)
2a stoma (56)bull Laparoscopylaparotomy and Level 1
drain plusmn proximal (56)defunctioning stoma (33)
Sepsis with contained leak abscess gt3cm (Grade 2)
Drainage needed bull Radiological drainage (37) Level 2(93) bull Surgical drainage (56) (67)
deg LaparoscopyLaparotomywashout drain and proximal
2b defunctioning stoma (44)deg Transperineal drainage plusmn
proximal defunctioningstoma (26)
deg Laparotomy and take downanastomosis (22)
3 Sepsis ileusSingle quadrant peritonitis (Grade 3)
Resuscitate and bull Drain and proximal Level 2operation (82) defunctioning stoma (30) (74)
bull Take down anastomosis (48)
Severe sepsis more than one quadrant peritonitis (Grade 4)
4 Resuscitate and Laparoscopy Laparotomy washout Level 23operation (100) and take down anastomosis (93) (100)
Septic shock generalised peritonitis (Grade 5)
5 Resuscitate and Laparoscopy Laparotomy washout Level 3operation (100) and take down anastomosis (100) (100)
23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

23
Appendix
Summary of findings from Delphi process forcolorectal anastomotic leakage
bull Initial meeting at Tripartite meeting in Birmingham(July 2014)
bull Delphi meeting held on 14th October 2014 RCS England
bull Invited Consultants and colorectal trainees from ACPGBI
bull Round 1 completed prior to meeting with on-linequestionnaire
bull Further 2 rounds completed at meeting
bull Results presented here are after 3 rounds ofquestionnaires
Key (SD strongly disagree D ndashdisagree N ndash neither agree ordisagree A ndash agree SA ndash strongly agree)
Demographics and Format of Delphi Process
Table 7 Format and numbers completing rounds of Delphi process
Figure 1 Age groups of surgeons within anastomotic leakworking group
Round 1 Round 2 Round 3
No of participants 36 31 31
Format On-line Meeting Meeting
Num
ber
ofV
alue
s
0
5
0
5
20
31-40 41-50 51-60 61-65 65+
Age ofWorking Group
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk
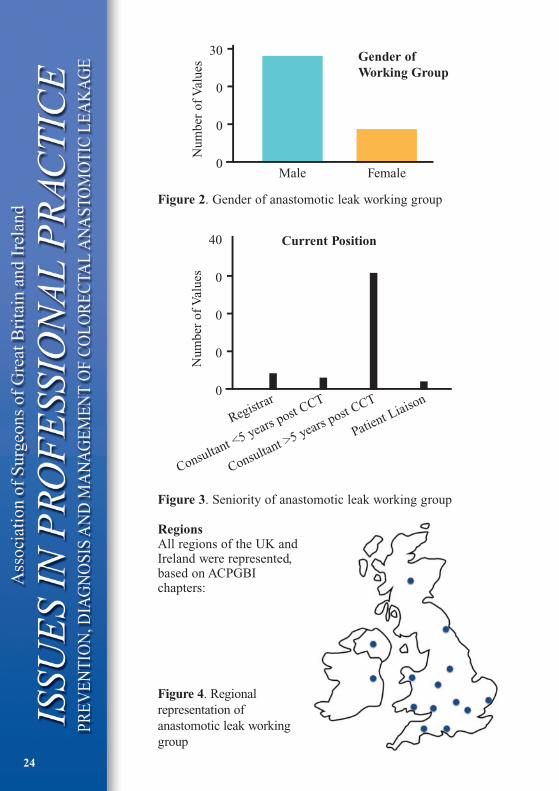
Figure 2 Gender of anastomotic leak working group
Figure 3 Seniority of anastomotic leak working group
RegionsAll regions of the UK andIreland were representedbased on ACPGBIchapters
Figure 4 Regionalrepresentation ofanastomotic leak workinggroup
24
Num
ber
ofV
alue
s
0
0
0
30
Male
Gender ofWorking Group
Female
Num
ber
ofV
alue
s
0
0
0
0
40
Registrar
Consultant lt5 years post CCT
Consultant gt5 years post CCT
Patient Liaison
Current Position
25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

25
Delphi ProcessDefinition of anastomotic leaks
Table 8 Percentage agreement of definitions for anastomotic leak
Non-modifiable risk factorsbull All gt70 Male gender distal anastomosis advanced
tumour stage metastatic disease historical radiotherapyASAgt2 diabetes vascular disease emergency surgeryex-smoker (gt40 pack years)
bull Others Tumours gt3cm (15) pulmonary disease (63)
Modifiable risk factorsbull All gt70 Smoking obesity alcohol excess
corticosteroids biological agents biologics in combinationwith steroids malnutritionhypoalbuminaemia pre-opshort and long course DXT
bull Others Bevacizumab (629) Age gt60 (42)
Periintraoperative risk factorsbull All gt70 contaminated surgery single and multiple
inotropes blood loss
bull Others Duration gt2 hours (23) blood transfusion (48)
Reduce risk of anastomotic leaksbull Preoperative intravenous antibiotics 26 agree or
strongly agree
bull Selective decontamination of digestive tract 741 (ASA)
bull Goal directed fluid therapy 78 (ASA)
A leak of luminal contents from asurgical join between two hollow viscera7 63
A breach in a surgical join between two hollowviscera with or without active leak of luminal contents 37
26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

26
Table 9 Pre and postoperative non-modifiable and modifiablerisk factors
Preoperative Intraoperative
Non-modifiable risk factors Increase risk
bull Male bull Intraoperative contamination
bull Distal anastomosis bull Duration gt4 hoursparticularly rectal bull Inotropes
bull Tumour size gt3cm bull Blood lossbull Advanced tumour stage bull Blood transfusionbull Metastatic disease
bull Historical radiotherapy
bull ASA gt2
bull Diabetes
bull Pulmonary disease
bull Vascular disease
bull Emergency surgery
bull Ex-smoker (gt40 pack years)
Potentially modifiable Reduce riskrisk factors
bull Smoking bull Preoperative antibiotics
bull Obesity (intravenous and selective
bull (High BMI Waist hip ratiodecontamination
Visceral fat)digestive tract)
bull Alcohol excess (gt21units bull Cardiac monitoringgoal 105g alcoholweek) directed fluid management
bull Corticosteroids
bull Bevacizumab
bull Malnutritionhypoalbuminaemia
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk
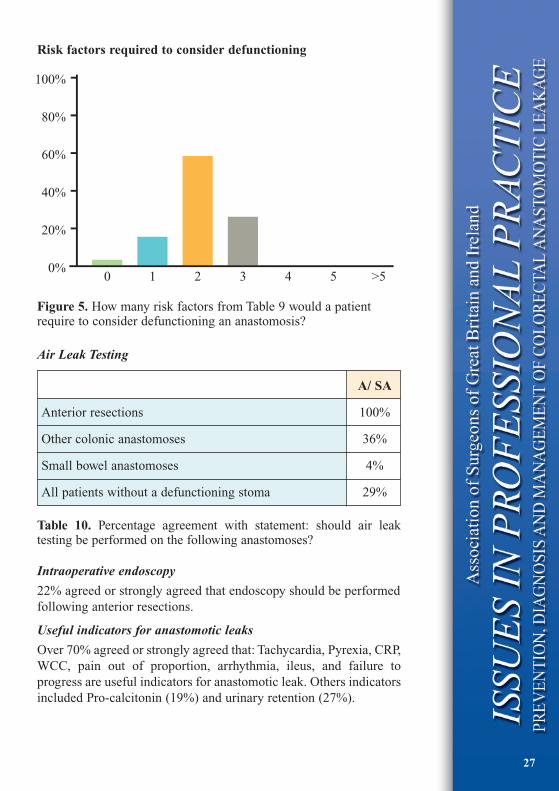
27
Risk factors required to consider defunctioning
Figure 5 How many risk factors from Table 9 would a patientrequire to consider defunctioning an anastomosis
Air Leak Testing
Table 10 Percentage agreement with statement should air leaktesting be performed on the following anastomoses
Intraoperative endoscopy
22 agreed or strongly agreed that endoscopy should be performedfollowing anterior resections
Useful indicators for anastomotic leaks
Over 70 agreed or strongly agreed that Tachycardia Pyrexia CRPWCC pain out of proportion arrhythmia ileus and failure toprogress are useful indicators for anastomotic leak Others indicatorsincluded Pro-calcitonin (19) and urinary retention (27)
0
20
40
60
80
100
0 1 2 3 4 5 gt5
A SA
Anterior resections 100
Other colonic anastomoses 36
Small bowel anastomoses 4
All patients without a defunctioning stoma 29
28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

28
Investigation of anastomotic leakbull Contrast enhanced CT (Oral or rectal contrast) 100 ASA
bull Right hemicolectomy contrast CT (100)
bull High anterior resection contrast CT (96)
bull Low anterior resection contrast CT (92)
Factors to determine whether to resect an anastomosis
bull gt70 Generalised pus faecal peritonitis severe sepsis
bull Others localised pus 16 elderly age of patient 63
bull Other comments size of defect ischemia of anastomosis
29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

29
References1 Mirnezami A Mirnezami R Chandrakumaran K Sasapu K
Sagar P Finan P Increased local recurrence and reducedsurvival from colorectal cancer following anastomotic leaksystematic review and meta-analysis Annals of surgery2011253(5) 890-899
2 Khoury W Lavery IC Kiran RP Impact of early reoperationafter resection for colorectal cancer on long-term oncologicaloutcomes Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201214(3) e117-123
3 Boccola MA Buettner PG Rozen WM Siu SK Stevenson ARStitz R Ho YH Risk factors and outcomes for anastomoticleakage in colorectal surgery a single-institution analysis of1576 patients World journal of surgery 201135(1) 186-195
4 Nachiappan S Askari A Malietzis G Giacometti M White IJenkins JT Kennedy RH Faiz O The Impact of AnastomoticLeak and Its Treatment on Cancer Recurrence and SurvivalFollowing Elective Colorectal Cancer Resection World journalof surgery 2014
5 McDermott FD Heeney A Kelly ME Steele RJ Carlson GLWinter DC Systematic review of preoperative intraoperativeand postoperative risk factors for colorectal anastomotic leaksThe British journal of surgery 2015102(5) 462-479
6 Survey Monkey httpwwwsurveymonkeycom [2014
7 Peel AL Taylor EW Proposed definitions for the audit ofpostoperative infection a discussion paper Surgical InfectionStudy Group Annals of the Royal College of Surgeons ofEngland 199173(6) 385-388
8 Sorensen LT Jorgensen T Kirkeby LT Skovdal J Vennits BWille-Jorgensen P Smoking and alcohol abuse are major riskfactors for anastomotic leakage in colorectal surgery TheBritish journal of surgery 199986(7) 927-931
9 Bertelsen CA Andreasen AH Jorgensen T Harling HAnastomotic leakage after anterior resection for rectal cancerrisk factors Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201012(1) 37-43
10 Bisgard AS Noack MW Klein M Rosenberg J Gogenur IPerioperative statin therapy is not associated with reduced riskof anastomotic leakage after colorectal resection Diseases ofthe colon and rectum 201356(8) 980-986
30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

30
11 Richards CH Campbell V Ho C Hayes J Elliott T Thompson-Fawcett M Smoking is a major risk factor for anastomotic leakin patients undergoing low anterior resection Colorectal disease the official journal of the Association of Coloproctology ofGreat Britain and Ireland 201214(5) 628-633
12 Enker WE Merchant N Cohen AM Lanouette NM SwallowC Guillem J Paty P Minsky B Weyrauch K Quan SH Safetyand efficacy of low anterior resection for rectal cancer 681consecutive cases from a specialty service Annals of surgery1999230(4) 544-552 discussion 552-544
13 Kruschewski M Rieger H Pohlen U Hotz HG Buhr HJ Riskfactors for clinical anastomotic leakage and postoperativemortality in elective surgery for rectal cancer Internationaljournal of colorectal disease 200722(8) 919-927
14 Kim MJ Shin R Oh HK Park JW Jeong SY Park JG Theimpact of heavy smoking on anastomotic leakage and strictureafter low anterior resection in rectal cancer patients Worldjournal of surgery 201135(12) 2806-2810
15 Volk A Kersting S Held HC Saeger HD Risk factors formorbidity and mortality after single-layer continuous suture forileocolonic anastomosis International journal of colorectaldisease 201126(3) 321-327
16 Benoist S Panis Y Alves A Valleur P Impact of obesity onsurgical outcomes after colorectal resection American journalof surgery 2000179(4) 275-281
17 Biondo S Pares D Kreisler E Rague JM Fraccalvieri D RuizAG Jaurrieta E Anastomotic dehiscence after resection andprimary anastomosis in left-sided colonic emergencies Diseasesof the colon and rectum 200548(12) 2272-2280
18 Senagore AJ Delaney CP Madboulay K Brady KM Fazio VWLaparoscopic colectomy in obese and nonobese patientsJournal of gastrointestinal surgery official journal of theSociety for Surgery of the Alimentary Tract 20037(4) 558-561
19 Kartheuser AH Leonard DF Penninckx F Paterson HM BrandtD Remue C Bugli C Dozois E Mortensen N Ris F Tiret EWaist Circumference Study G Waist circumference andwaisthip ratio are better predictive risk factors for mortality andmorbidity after colorectal surgery than body mass index andbody surface area Annals of surgery 2013258(5) 722-730
20 Krysa J Patel V Taylor J Williams AB Carapeti E George MLOutcome of patients on renal replacement therapy aftercolorectal surgery Diseases of the colon and rectum200851(6) 961-965
31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

31
21 Golub R Golub RW Cantu R Jr Stein HD A multivariateanalysis of factors contributing to leakage of intestinalanastomoses Journal of the American College of Surgeons1997184(4) 364-372
22 Slieker JC Komen N Mannaerts GH Karsten TM WillemsenP Murawska M Jeekel J Lange JF Long-term andperioperative corticosteroids in anastomotic leakage aprospective study of 259 left-sided colorectal anastomosesArchives of surgery 2012147(5) 447-452
23 Canedo J Lee SH Pinto R Murad-Regadas S Rosen L WexnerSD Surgical resection in Crohnrsquos disease is immunosuppressivemedication associated with higher postoperative infection ratesColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201113(11) 1294-1298
24 Krane MK Allaix ME Zoccali M Umanskiy K Rubin MAVilla A Hurst RD Fichera A Preoperative infliximab therapydoes not increase morbidity and mortality after laparoscopicresection for inflammatory bowel disease Diseases of the colonand rectum 201356(4) 449-457
25 Zeeh J Inglin R Baumann G Dirsch O Riley NE Gerken GBuchler MW Egger B Mycophenolate mofetil impairs healingof left-sided colon anastomoses Transplantation 200171(10)1429-1435
26 Petri JB Schurk S Gebauer S Haustein UF Cyclosporine Adelays wound healing and apoptosis and suppresses activin beta-A expression in rats European journal of dermatology EJD19988(2) 104-113
27 Schaffer MR Fuchs N Proksch B Bongartz M Beiter TBecker HD Tacrolimus impairs wound healing a possible roleof decreased nitric oxide synthesis Transplantation 199865(6)813-818
28 van der Vliet JA Willems MC de Man BM Lomme RMHendriks T Everolimus interferes with healing of experimentalintestinal anastomoses Transplantation 200682(11) 1477-1483
29 Myrelid P Marti-Gallostra M Ashraf S Sunde ML Tholin MOresland T Lovegrove RE Tottrup A Kjaer DW George BDComplications in surgery for Crohnrsquos disease after preoperativeantitumour necrosis factor therapy The British journal ofsurgery 2014101(5) 539-545
30 Subramanian V Pollok RC Kang JY Kumar D Systematicreview of postoperative complications in patients withinflammatory bowel disease treated with immunomodulatorsThe British journal of surgery 200693(7) 793-799
32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

32
31 Highlights of prescribing information for AVASTIN(Bevacizumab)httpwwwgenecomdownloadpdfavastin_prescribingpdf[1652014
32 Veyrie N Ata T Muscari F Couchard AC Msika S Hay JMFingerhut A Dziri C Anastomotic leakage after elective rightversus left colectomy for cancer prevalence and independentrisk factors Journal of the American College of Surgeons2007205(6) 785-793
33 Kang CY Halabi WJ Chaudhry OO Nguyen V Pigazzi ACarmichael JC Mills S Stamos MJ Risk factors foranastomotic leakage after anterior resection for rectal cancerJAMA surgery 2013148(1) 65-71
34 Telem DA Chin EH Nguyen SQ Divino CM Risk factors foranastomotic leak following colorectal surgery a case-controlstudy Archives of surgery 2010145(4) 371-376 discussion376
35 Suding P Jensen E Abramson MA Itani K Wilson SEDefinitive risk factors for anastomotic leaks in elective opencolorectal resection Archives of surgery 2008143(9) 907-911discussion 911-902
36 Hennessey DB Burke JP Ni-Dhonochu T Shields C WinterDC Mealy K Preoperative hypoalbuminemia is an independentrisk factor for the development of surgical site infectionfollowing gastrointestinal surgery a multi-institutional studyAnnals of surgery 2010252(2) 325-329
37 Vanrsquot Sant HP Weidema WF Hop WC Oostvogel HJ ContantCM The influence of mechanical bowel preparation in electivelower colorectal surgery Annals of surgery 2010251(1) 59-63
38 Scabini S Rimini E Romairone E Scordamaglia R DamianiG Pertile D Ferrando V Colon and rectal surgery for cancerwithout mechanical bowel preparation one-center randomizedprospective trial World journal of surgical oncology 20108 35
39 Zmora O Mahajna A Bar-Zakai B Hershko D Shabtai MKrausz MM Ayalon A Is mechanical bowel preparationmandatory for left-sided colonic anastomosis Results of aprospective randomized trial Techniques in coloproctology200610(2) 131-135
40 Slim K Vicaut E Launay-Savary MV Contant C Chipponi JUpdated systematic review and meta-analysis of randomizedclinical trials on the role of mechanical bowel preparationbefore colorectal surgery Annals of surgery 2009249(2)203-209
33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

33
41 Guenaga KF Matos D Wille-Jorgensen P Mechanical bowelpreparation for elective colorectal surgery The Cochranedatabase of systematic reviews 2011(9) CD001544
42 Bretagnol F Panis Y Rullier E Rouanet P Berdah S Dousset BPortier G Benoist S Chipponi J Vicaut E Rectal cancersurgery with or without bowel preparation The FrenchGRECCAR III multicenter single-blinded randomized trialAnnals of surgery 2010252(5) 863-868
43 Sauer R Becker H Hohenberger W Rodel C Wittekind CFietkau R Martus P Tschmelitsch J Hager E Hess CFKarstens JH Liersch T Schmidberger H Raab R GermanRectal Cancer Study G Preoperative versus postoperativechemoradiotherapy for rectal cancer The New England journalof medicine 2004351(17) 1731-1740
44 Warschkow R Steffen T Thierbach J Bruckner T Lange JTarantino I Risk factors for anastomotic leakage after rectalcancer resection and reconstruction with colorectostomy Aretrospective study with bootstrap analysis Annals of surgicaloncology 201118(10) 2772-2782
45 Park JS Choi GS Kim SH Kim HR Kim NK Lee KY KangSB Kim JY Lee KY Kim BC Bae BN Son GM Lee SI KangH Multicenter analysis of risk factors for anastomotic leakageafter laparoscopic rectal cancer excision the Koreanlaparoscopic colorectal surgery study group Annals of surgery2013257(4) 665-671
46 Sebag-Montefiore D Stephens RJ Steele R Monson J GrieveR Khanna S Quirke P Couture J de Metz C Myint ASBessell E Griffiths G Thompson LC Parmar M Preoperativeradiotherapy versus selective postoperative chemoradiotherapyin patients with rectal cancer (MRC CR07 and NCIC-CTGC016) a multicentre randomised trial Lancet 2009373(9666)811-820
47 Marijnen CA Kapiteijn E van de Velde CJ Martijn H SteupWH Wiggers T Kranenbarg EK Leer JW CooperativeInvestigators of the Dutch Colorectal Cancer G Acute sideeffects and complications after short-term preoperativeradiotherapy combined with total mesorectal excision inprimary rectal cancer report of a multicenter randomized trialJournal of clinical oncology official journal of the AmericanSociety of Clinical Oncology 200220(3) 817-825
48 Chang JS Keum KC Kim NK Baik SH Min BS Huh H LeeCG Koom WS Preoperative chemoradiotherapy effects onanastomotic leakage after rectal cancer resection a propensityscore matching analysis Annals of surgery 2014259(3) 516-521
34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

34
49 ACPGBI Guidelines for the management of colorectal cancer2007
50 Roos D Dijksman LM Tijssen JG Gouma DJ Gerhards MFOudemans-van Straaten HM Systematic review of perioperativeselective decontamination of the digestive tract in electivegastrointestinal surgery The British journal of surgery2013100(12) 1579-1588
51 Morris MS Graham LA Chu DI Cannon JA Hawn MT OralAntibiotic Bowel Preparation Significantly Reduces SurgicalSite Infection Rates and Readmission Rates in ElectiveColorectal Surgery Annals of surgery 2015
52 Lipska MA Bissett IP Parry BR Merrie AE Anastomoticleakage after lower gastrointestinal anastomosis men are at ahigher risk ANZ journal of surgery 200676(7) 579-585
53 Jung SH Yu CS Choi PW Kim DD Park IJ Kim HC Kim JCRisk factors and oncologic impact of anastomotic leakage afterrectal cancer surgery Diseases of the colon and rectum200851(6) 902-908
54 Damhuis RA Wereldsma JC Wiggers T The influence of ageon resection rates and postoperative mortality in 6457 patientswith colorectal cancer International journal of colorectaldisease 199611(1) 45-48
55 Fernandes R Shaikh I Doughan S Outcomes of electivelaparoscopic colorectal operations in octogenarians at a districtgeneral hospital in South East England World journal ofgastrointestinal surgery 20135(1) 9-11
56 Smith ST Seski JC Copeland LJ Gershenson DM EdwardsCL Herson J Surgical management of irradiation-inducedsmall bowel damage Obstetrics and gynecology 198565(4)563-567
57 Cong ZJ Fu CG Wang HT Liu LJ Zhang W Wang HInfluencing factors of symptomatic anastomotic leakage afteranterior resection of the rectum for cancer World journal ofsurgery 200933(6) 1292-1297
58 Ziegler MA Catto JA Riggs TW Gates ER Grodsky MBWasvary HJ Risk factors for anastomotic leak and mortality indiabetic patients undergoing colectomy analysis from astatewide surgical quality collaborative Archives of surgery2012147(7) 600-605
59 Tresallet C Royer B Godiris-Petit G Menegaux F Effect ofsystemic corticosteroids on elective left-sided colorectalresection with colorectal anastomosis American journal ofsurgery 2008195(4) 447-451
35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

35
60 Sarkio S Halme L Kyllonen L Salmela K Severe gastrointestinalcomplications after 1515 adult kidney transplantations Transplantinternational official journal of the European Society for OrganTransplantation 200417(9) 505-510
61 Haimov M Glabman S Schupak E Neff M Burrows LGeneral surgery in patients on maintenance hemodialysisAnnals of surgery 1974179(6) 863-867
62 Jestin P Pahlman L Gunnarsson U Risk factors for anastomoticleakage after rectal cancer surgery a case-control studyColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 200810(7) 715-721
63 Bakker IS Grossmann I Henneman D Havenga K Wiggers TRisk factors for anastomotic leakage and leak-related mortalityafter colonic cancer surgery in a nationwide audit The Britishjournal of surgery 2014101(4) 424-432 discussion 432
64 Frisch A Chandra P Smiley D Peng L Rizzo M Gatcliffe CHudson M Mendoza J Johnson R Lin E Umpierrez GEPrevalence and clinical outcome of hyperglycemia in theperioperative period in noncardiac surgery Diabetes care201033(8) 1783-1788
65 Moghissi ES Korytkowski MT DiNardo M Einhorn DHellman R Hirsch IB Inzucchi SE Ismail-Beigi F KirkmanMS Umpierrez GE American Association of Clinical EAmerican Diabetes A American Association of ClinicalEndocrinologists and American Diabetes Association consensusstatement on inpatient glycemic control Diabetes care200932(6) 1119-1131
66 Hollenberg M Mangano DT Browner WS London MJ TubauJF Tateo IM Predictors of postoperative myocardial ischemia inpatients undergoing noncardiac surgery The Study ofPerioperative Ischemia Research Group Jama 1992268(2)205-209
67 OrsquoBrien MM Gonzales R Shroyer AL Grunwald GK Daley JHenderson WG Khuri SF Anderson RJ Modest serumcreatinine elevation affects adverse outcome after generalsurgery Kidney international 200262(2) 585-592
68 Veglio M Chinaglia A Cavallo-Perin P QT intervalcardiovascular risk factors and risk of death in diabetes Journalof endocrinological investigation 200427(2) 175-181
69 Management of adults with diabetes undergoing surgery andelective procedures improving standardshttpwwwdiabetologists-abcdorgukJBDSJBDS_IP_Surgery_Adults_Fullpdf[162015
36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

36
70 McDermott FD Collins D Heeney A Winter DC Minimallyinvasive and surgical management strategies tailored to theseverity of acute diverticulitis The British journal of surgery2014101(1) e90-99
71 Constantinides VA Heriot A Remzi F Darzi A Senapati AFazio VW Tekkis PP Operative strategies for diverticularperitonitis a decision analysis between primary resection andanastomosis versus Hartmannrsquos procedures Annals of surgery2007245(1) 94-103
72 Oberkofler CE Rickenbacher A Raptis DA Lehmann KVilliger P Buchli C Grieder F Gelpke H Decurtins M Tempia-Caliera AA Demartines N Hahnloser D Clavien PABreitenstein S A multicenter randomized clinical trial ofprimary anastomosis or Hartmannrsquos procedure for perforatedleft colonic diverticulitis with purulent or fecal peritonitisAnnals of surgery 2012256(5) 819-826 discussion 826-817
73 Trencheva K Morrissey KP Wells M Mancuso CA Lee SWSonoda T Michelassi F Charlson ME Milsom JW Identifyingimportant predictors for anastomotic leak after colon and rectalresection prospective study on 616 patients Annals of surgery2013257(1) 108-113
74 Eberl T Jagoditsch M Klingler A Tschmelitsch J Risk factorsfor anastomotic leakage after resection for rectal cancerAmerican journal of surgery 2008196(4) 592-598
75 Nisar PJ Lavery IC Kiran RP Influence of neoadjuvantradiotherapy on anastomotic leak after restorative resection forrectal cancer Journal of gastrointestinal surgery officialjournal of the Society for Surgery of the Alimentary Tract201216(9) 1750-1757
76 Makela JT Kiviniemi H Laitinen S Risk factors for anastomoticleakage after left-sided colorectal resection with rectal anastomosisDiseases of the colon and rectum 200346(5) 653-660
77 Konishi T Watanabe T Kishimoto J Nagawa H Risk factors foranastomotic leakage after surgery for colorectal cancer resultsof prospective surveillance Journal of the American College ofSurgeons 2006202(3) 439-444
78 Buchs NC Gervaz P Secic M Bucher P Mugnier-Konrad BMorel P Incidence consequences and risk factors foranastomotic dehiscence after colorectal surgery a prospectivemonocentric study International journal of colorectal disease200823(3) 265-270
79 Leichtle SW Mouawad NJ Welch KB Lampman RM ClearyRK Risk factors for anastomotic leakage after colectomyDiseases of the colon and rectum 201255(5) 569-575
37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

37
80 Schietroma M Carlei F Cecilia EM Piccione F Bianchi ZAmicucci G Colorectal Infraperitoneal anastomosis the effectsof perioperative supplemental oxygen administration on theanastomotic dehiscence Journal of gastrointestinal surgery official journal of the Society for Surgery of the AlimentaryTract 201216(2) 427-434
81 Zakrison T Nascimento BA Jr Tremblay LN Kiss A RizoliSB Perioperative vasopressors are associated with an increasedrisk of gastrointestinal anastomotic leakage World journal ofsurgery 200731(8) 1627-1634
82 NICE CardioQ-ODM (Oesophageal Doppler Monitor) MTG-32011
83 Abbas SM Hill AG Systematic review of the literature for theuse of oesophageal Doppler monitor for fluid replacement inmajor abdominal surgery Anaesthesia 200863(1) 44-51
84 Walsh SR Tang T Bass S Gaunt ME Doppler-guidedintraoperative fluid management during major abdominalsurgery systematic review and meta-analysis Internationaljournal of clinical practice 200862(3) 466-470
85 Docherty JG McGregor JR Akyol AM Murray GD GallowayDJ Comparison of manually constructed and stapledanastomoses in colorectal surgery West of Scotland andHighland Anastomosis Study Group Annals of surgery1995221(2) 176-184
86 Choy PY Bissett IP Docherty JG Parry BR Merrie AFitzgerald A Stapled versus handsewn methods for ileocolicanastomoses The Cochrane database of systematic reviews2011(9) CD004320
87 Neutzling CB Lustosa SA Proenca IM da Silva EM Matos DStapled versus handsewn methods for colorectal anastomosissurgery The Cochrane database of systematic reviews 20122CD003144
88 Beard JD Nicholson ML Sayers RD Lloyd D Everson NWIntraoperative air testing of colorectal anastomoses aprospective randomized trial The British journal of surgery199077(10) 1095-1097
89 Cirocchi R Trastulli S Farinella E Desiderio J Listorti C ParisiA Noya G Boselli C Is inferior mesenteric artery ligation duringsigmoid colectomy for diverticular disease associated withincreased anastomotic leakage A meta-analysis of randomizedand non-randomized clinical trials Colorectal disease theofficial journal of the Association of Coloproctology of GreatBritain and Ireland 201214(9) e521-529
38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

38
90 Jayne DG Thorpe HC Copeland J Quirke P Brown JMGuillou PJ Five-year follow-up of the Medical ResearchCouncil CLASICC trial of laparoscopically assisted versus opensurgery for colorectal cancer The British journal of surgery201097(11) 1638-1645
91 Breukink S Pierie J Wiggers T Laparoscopic versus open totalmesorectal excision for rectal cancer The Cochrane database ofsystematic reviews 2006(4) Cd005200
92 Matthiessen P Hallbook O Rutegard J Simert G Sjodahl RDefunctioning stoma reduces symptomatic anastomotic leakageafter low anterior resection of the rectum for cancer a randomizedmulticenter trial Annals of surgery 2007246(2) 207-214
93 Tocchi A Mazzoni G Lepre L Costa G Liotta G Agostini NMiccini M Prospective evaluation of omentoplasty inpreventing leakage of colorectal anastomosis Diseases of thecolon and rectum 200043(7) 951-955
94 Petrowsky H Demartines N Rousson V Clavien PA Evidence-based value of prophylactic drainage in gastrointestinal surgerya systematic review and meta-analyses Annals of surgery2004240(6) 1074-1084 discussion 1084-1075
95 Karliczek A Jesus EC Matos D Castro AA Atallah ANWiggers T Drainage or nondrainage in elective colorectalanastomosis a systematic review and meta-analysis Colorectaldisease the official journal of the Association of Coloproctologyof Great Britain and Ireland 20068(4) 259-265
96 Jesus EC Karliczek A Matos D Castro AA Atallah ANProphylactic anastomotic drainage for colorectal surgery TheCochrane database of systematic reviews 2004(4) CD002100
97 Rondelli F Bugiantella W Vedovati MC Balzarotti R Avenia NMariani E Agnelli G Becattini C To drain or not to drainextraperitoneal colorectal anastomosis A systematic review andmeta-analysis Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland201416(2) O35-42
98 Bhangu A Singh P Fitzgerald JE Slesser A Tekkis PPostoperative nonsteroidal anti-inflammatory drugs and risk ofanastomotic leak meta-analysis of clinical and experimentalstudies World journal of surgery 201438(9) 2247-2257
99 Hakkarainen TW Steele SR Bastaworous A Dellinger EPFarrokhi E Farjah F Florence M Helton S Horton M PietroM Varghese TK Flum DR Nonsteroidal Anti-inflammatoryDrugs and the Risk for Anastomotic Failure A Report FromWashington Statersquos Surgical Care and Outcomes AssessmentProgram (SCOAP) JAMA surgery 2015
39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

39
100 Alves A Panis Y Trancart D Regimbeau JM Pocard MValleur P Factors associated with clinically significantanastomotic leakage after large bowel resection multivariateanalysis of 707 patients World journal of surgery 200226(4)499-502
101 Sutton CD Marshall LJ Williams N Berry DP Thomas WMKelly MJ Colo-rectal anastomotic leakage often masquerades asa cardiac complication Colorectal disease the official journalof the Association of Coloproctology of Great Britain andIreland 20046(1) 21-22
102 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2013
103 The Surgical Management of Patients with Acute IntestinalFailure (2010)httpwwwasgbiorgukenpublicationsissues_in_professional_practicecfm
104 Singh PP Zeng IS Srinivasa S Lemanu DP Connolly AB HillAG Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak aftercolorectal surgery The British journal of surgery 2014101(4)339-346
105 Garcia-Granero A Frasson M Flor-Lorente B Blanco F PugaR Carratala A Garcia-Granero E Procalcitonin and C-reactiveprotein as early predictors of anastomotic leak in colorectalsurgery a prospective observational study Diseases of the colonand rectum 201356(4) 475-483
106 Kaur P Karandikar SS Roy-Choudhury S Accuracy ofmultidetector CT in detecting anastomotic leaks followingstapled left-sided colonic anastomosis Clinical radiology201469(1) 59-62
107 Dekker JW Liefers GJ de Mol van Otterloo JC Putter HTollenaar RA Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score TheJournal of surgical research 2011166(1) e27-34
108 den Dulk M Witvliet MJ Kortram K Neijenhuis PA deHingh IH Engel AF van de Velde CJ de Brauw LM Putter HBrouwers MA Steup WH The DULK (Dutch leakage) andmodified DULK score compared actively seek the leakColorectal disease the official journal of the Association ofColoproctology of Great Britain and Ireland 201315(9)e528-533
40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

40
109 Kulu Y Ulrich A Bruckner T Contin P Welsch T Rahbari NNBuchler MW Weitz J Validation of the International StudyGroup of Rectal Cancer definition and severity grading ofanastomotic leakage Surgery 2013153(6) 753-761
110 Kumar A KM Ronald J Seleman M Roberts D Gurka D et alRapidity of source control implementation following onset ofhypotension is a major determinant of survival in human septicshock Crit Care Med 200432((12 Supp)) A158
111 Surviving Sepsis CampaignhttpwwwsurvivingsepsisorgSiteCollectionDocumentsSSC_Bundlepdf
112 Daniels R Nutbeam T McNamara G Galvin C The sepsis sixand the severe sepsis resuscitation bundle a prospectiveobservational cohort study Emergency medicine journal EMJ201128(6) 507-512
113 The Higher Risk General Surgical Patient Towards ImprovedCare for a Forgotten Grouphttpswwwrcsengacukpublicationsdocshigher-risk-surgical-patient
114 van Koperen PJ van Berge Henegouwen MI Rosman C BakkerCM Heres P Slors JF Bemelman WA The Dutch multicenterexperience of the endo-sponge treatment for anastomoticleakage after colorectal surgery Surgical endoscopy 200923(6)1379-1383
115 Matthiessen P Hallbook O Andersson M Rutegard J SjodahlR Risk factors for anastomotic leakage after anterior resectionof the rectum Colorectal disease the official journal of theAssociation of Coloproctology of Great Britain and Ireland20046(6) 462-469
116 Vignali A Fazio VW Lavery IC Milsom JW Church JM HullTL Strong SA Oakley JR Factors associated with theoccurrence of leaks in stapled rectal anastomoses a review of1014 patients
wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

wwwasgbiorguk wwwacpgbiorguk
Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk

Association of Surgeons of Great Britain and Ireland
35-43 Lincolnrsquos Inn Fields London WC2A 3PE
Tel 020 7973 0300 Fax 020 7430 9235wwwasgbiorguk
A Company limited by guarantee registered in England 06783090
wwwasgbiorguk