primary and secondary stroke prevention daniel ackerman, … · 3/18/2016 1 primary and secondary...
TRANSCRIPT
·:{iC0Fp'16ACOFP 53rd Annual Convention & Scientific Seminars
Primary and Secondary Stroke Prevention
Daniel Ackerman, MD


3/18/2016
1
Primary and Secondary Stroke Prevention
Dr. Daniel Ackerman MD
Director of Stroke and Vascular Neurology
St. Luke’s University Health Network
Clinical Assistant Professor of Neurology
Lewis Katz School of Medicine at Temple University
1
St. Luke’s University Health Network
Disclosures
I have no financial disclosures
2
St. Luke’s University Health Network
Objectives
Brief review of stroke epidemiology and pathophysiology
Primary prevention of stroke– Risk Factors
– Screening
– Special populations
Secondary prevention of stroke– Understanding etiology
– Monitoring and ongoing evaluation
Stroke prevention therapy– Antiplatelet agents
– Anticoagulation
– BP/Statins/DM
3
3/18/2016
2
St. Luke’s University Health Network
Ok…What is a stroke anyway?
Stroke, also known as a “brain attack” is the
damage resulting from an alteration in cerebral
blood flow.
87% of strokes are ischemic, 10% ICH and 3%
SAH
Stroke affects nearly 800,000 people per year
with a new stroke every 40 seconds.
It remains the 5th leading cause of death in the
US and a leading cause of long term disability.
4
Mozaffarian D, Benjamin EJ, Go AS, et al. Heart Disease and Stroke
Statistics—2016 Update.; 2015. doi:10.1161/CIR.0000000000000350.
St. Luke’s University Health Network 2
St. Luke’s University Health Network
So why is TIME = BRAIN??
Every minute that the brain is starved for blood,
2 million neurons, 14 billion synapses, and 12
Kilometers of myelinated fibers are destroyed…
Put another way, every hour the brain ages 3.6
years.
Every 30 minutes in delay to reperfusion
decreases the likelihood of a good outcome by
10%.
Several targets for neuroprotection have been
identified including inflammation, oxidative stress,
blood-brain barrier disruption, excitotoxicity,
apoptosis, autophagy…
6
no effective interventionsMozaffarian D, Benjamin EJ, Go AS, et al. Heart Disease and Stroke
Statistics—2016 Update.; 2015. doi:10.1161/CIR.0000000000000350.
3/18/2016
3
St. Luke’s University Health Network
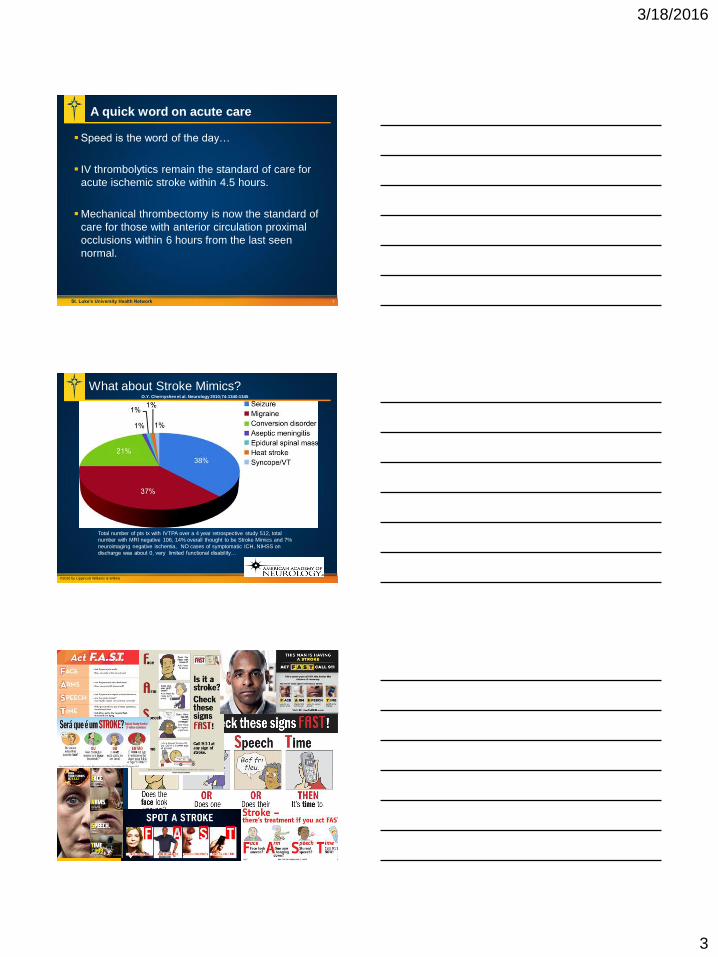
A quick word on acute care
Speed is the word of the day…
IV thrombolytics remain the standard of care for
acute ischemic stroke within 4.5 hours.
Mechanical thrombectomy is now the standard of
care for those with anterior circulation proximal
occlusions within 6 hours from the last seen
normal.
7
O.Y. Chernyshev et al. Neurology 2010;74:1340-1345
©2010 by Lippincott Williams & Wilkins
What about Stroke Mimics?
Total number of pts tx with IVTPA over a 4 year retrospective study 512, total
number with MRI negative 106, 14% overall thought to be Stroke Mimics and 7%
neuroimaging negative ischemia, NO cases of symptomatic ICH, NIHSS on
discharge was about 0, very limited functional disability…
3/18/2016
4
St. Luke’s University Health Network
Primary Prevention
10
St. Luke’s University Health Network
Some of the common risk factors
11
Non-Modifiable– Age
– Gender
– History of TIA/Stroke
Genetic– Hypercoaguable state
– Fabry Disease
– Sickle Cell
– Trisomy 21
– CADASIL
Modifiable– Hypertension
– Dyslipidemia
– Diabetes
– Obesity
– Obstructive Sleep Apnea
– Tobacco Use
– A-Fib
– Medication/iatrogenic
– Drug/Alcohol abuse
Meschia, J. F., et al (2014). Guidelines for the Primary Prevention of Stroke: A Statement for
Healthcare Professionals From the American Heart Association/American Stroke Association .
Stroke , 45 (12 ), 3754–3832. http://doi.org/10.1161/STR.0000000000000046
St. Luke’s University Health Network
Doc…am I at risk?
No single risk assessment tool captures all of the
complexities of age, race, gender, genetics, etc…
2 Different approaches– Lumping: Combining risk factor sets based on observed
associations. Easy to use on a relatively wide scale but may
have pitfalls in generalizability.
– Splitting: Evaluating risk factors separately on a patient specific
basis. More challenging and not necessarily more accurate as
some risk factors and the association/interaction between them
may not be well defined.
12

3/18/2016
5
St. Luke’s University Health Network
Doc…am I at risk?
No single risk assessment tool captures all of the
complexities of age, race, gender, genetics, etc…
13
St. Luke’s University Health Network
Started in 1948 with the recruitment of 5200
participants.
Additional cohorts have been added including the
children and grandchildren of the original group
and new additions to improve diversity.
There are questions about generalizability among
those with minimal risk factors and in people of
more diverse racial and geographic backgrounds.
14
www.framinghamheartstudy.org
St. Luke’s University Health Network 15
MEN 0 1 2 3 4 5 6 7 8 9 10
Age 54-56 57-59 60-62 63-65 66-68 69-72 73-75 76-78 79-81 82-84 85
SBP (untreated)
97-105 106-115 116-125 126-135 136-145 146-155 156-165 166-175 176-185 186-195 196-205
SBP (treated)
97-105 106-112 113-117 118-123 124-129 130-135 136-142 143-150 151-161 162-176 177-205
DM XXX
Tob XXX
CVD XXX
A-Fib XXX
LVH XXX
Variables were defined as follows: SBP, systolic blood pressure in mmHG; Diabetes, history of diabetes; Tob, smokes cigarettes; CVD
(cardiovascular disease), history of myocardiai infarction, angina pectoris, coronary insufficiency, intermittent claudication, or congestive heart
failure; AF, history of atrial fibrillation; LVH, left ventricular hypertrophy on electrocardiogram.
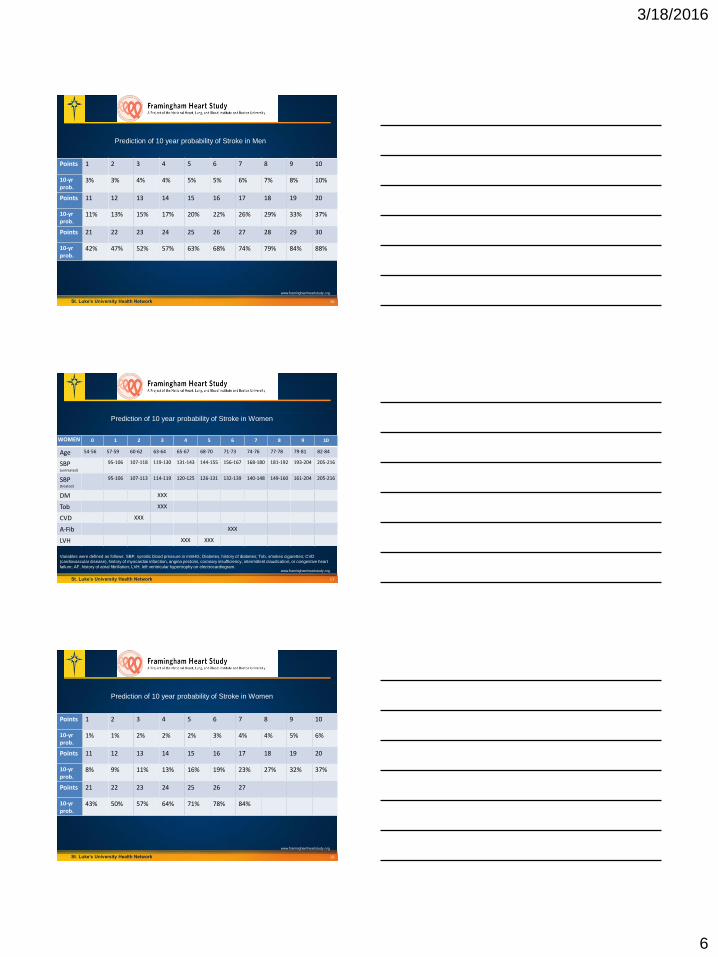
Prediction of 10 year probability of Stroke in Men
www.framinghamheartstudy.org
3/18/2016
6
St. Luke’s University Health Network 16
Points 1 2 3 4 5 6 7 8 9 10
10-yr prob.
3% 3% 4% 4% 5% 5% 6% 7% 8% 10%
Points 11 12 13 14 15 16 17 18 19 20
10-yr prob.
11% 13% 15% 17% 20% 22% 26% 29% 33% 37%
Points 21 22 23 24 25 26 27 28 29 30
10-yr prob.
42% 47% 52% 57% 63% 68% 74% 79% 84% 88%
Prediction of 10 year probability of Stroke in Men
www.framinghamheartstudy.org
St. Luke’s University Health Network 17
WOMEN 0 1 2 3 4 5 6 7 8 9 10
Age 54-56 57-59 60-62 63-64 65-67 68-70 71-73 74-76 77-78 79-81 82-84
SBP (untreated)
95-106 107-118 119-130 131-143 144-155 156-167 168-180 181-192 193-204 205-216
SBP (treated)
95-106 107-113 114-119 120-125 126-131 132-139 140-148 149-160 161-204 205-216
DM XXX
Tob XXX
CVD XXX
A-Fib XXX
LVH XXX XXX
Variables were defined as follows: SBP, systolic blood pressure in mmHG; Diabetes, history of diabetes; Tob, smokes cigarettes; CVD
(cardiovascular disease), history of myocardiai infarction, angina pectoris, coronary insufficiency, intermittent claudication, or congestive heart
failure; AF, history of atrial fibrillation; LVH, left ventricular hypertrophy on electrocardiogram.
Prediction of 10 year probability of Stroke in Women
www.framinghamheartstudy.org
St. Luke’s University Health Network 18
Points 1 2 3 4 5 6 7 8 9 10
10-yr prob.
1% 1% 2% 2% 2% 3% 4% 4% 5% 6%
Points 11 12 13 14 15 16 17 18 19 20
10-yr prob.
8% 9% 11% 13% 16% 19% 23% 27% 32% 37%
Points 21 22 23 24 25 26 27
10-yr prob.
43% 50% 57% 64% 71% 78% 84%
Prediction of 10 year probability of Stroke in Women
www.framinghamheartstudy.org
3/18/2016
7
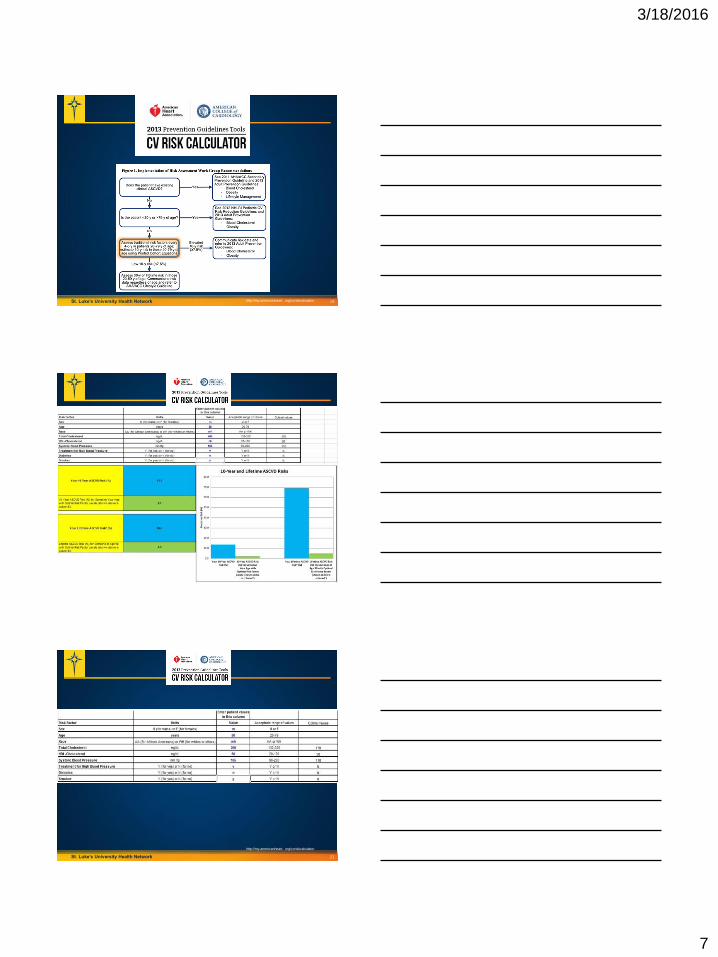
St. Luke’s University Health Network 19http://my.americanheart. org/cvriskcalculator
St. Luke’s University Health Network 20
St. Luke’s University Health Network 21
http://my.americanheart. org/cvriskcalculator

3/18/2016
8
St. Luke’s University Health Network
More specific screening tools may be available
22
Some more specific populations are challenging
in terms of general guidelines and risk tools.– Specific ethnic/racial considerations
– Local cultural effects
– Theoretical risks
Pubmed search for “primary stroke prevention”
limiting results to review papers published in the
last 5 years yields 554 results.
St. Luke’s University Health Network
Patient specific risk
Age
Low Birth Weight
Race/Ethnicity
Physical Inactivity
Dyslipidemia
Hypertension
Obesity
Diabetes
Tobacco
Atrial Fibrillation
23
Established cardiac disease
Carotid artery stenosis
(asymptomatic)
Migraine with aura
Alcohol use/abuse
Drug Abuse
Sleep disordered breathing
Hyperhomocysteinemia
Inflammation/infection
Meschia, J. F. et al (2014). Guidelines for the Primary Prevention of Stroke: A
Statement for Healthcare Professionals From the American Heart
Association/American Stroke Association . Stroke , 45 (12 ), 3754–3832.
Kernan, W. N. et al (2014). Guidelines for the Prevention of Stroke in Patients With
Stroke and Transient Ischemic Attack: A Guideline for Healthcare Professionals From
the American Heart Association/American Stroke Association . Stroke , 45 (7 ),
St. Luke’s University Health Network
Carotid Artery Disease…whom do we screen?
The risk for stroke in an asymptomatic carotid disease
(CAD) is not as high as symptomatic CAD but knowing
who to screen is challenging.
The prevalence of severe asymptomatic carotid stenosis
in the US population is estimated at 3.1%
There is clearly a subset of people who are at higher
risk…
The AHA/ASA recommends screening with doppler
ultrasound for select patients with bruits, symptomatic
PVD or coronary disease, or >/= 2 atherosclerotic risk
factors
24

3/18/2016
9
St. Luke’s University Health Network
Genetic Risk
Family History:– Those with a parent who suffered a stroke under age 65 were at
3X higher risk of stroke
Conditions associated with increased risk– Sickle Cell Disease
– Trisomy 21
– Fabry Disease
– MELAS
– CADASIL
– Intrinsic hypercoaguable state
– Autosomal dominant polycystic kidney disease
25
St. Luke’s University Health Network 26
St. Luke’s University Health Network
Ok…I’ve had a stroke, so now what?
A brief word on recovery
Etiology is key to understanding secondary
prevention.
Ongoing monitoring
27

3/18/2016
10
St. Luke’s University Health Network
Stroke Recovery
Requires a multidisciplinary effort and
takes…TIME (6-12 months or more).
May be complicated by loss of independence and
several changes in lifestyle.
Anxiety and depression are major common
barriers.
Education and re-education followed by
education and support… and then some
education.
28
St. Luke’s University Health Network
Common types/causes of ischemic stroke
Embolic– Cardioembolic
• Structure problem
• Rhythm problem
• Hypercoaguable state
– Atheroembolic (artery to artery)
– Septic
– Other (air, Onyx, fat)
Thrombotic– Small vessel ischemic disease
Hypoperfusion– Watershed area
29
St. Luke’s University Health Network
But he’s so healthy at home…
Frequently a stroke is the bridge to reveal
vascular risk.
Post stroke evaluation typically includes– Brain structure imaging (preferably Brain MRI without contrast)
– Vascular imaging
– Echocardiography
– Fasting lipid panel
– Diabetes evaluation
30

3/18/2016
11
St. Luke’s University Health Network
Extra’s that may be necessary
Long term heart rhythm monitoring– Holter vs. ILR
Hypercoaugable evaluation
Vasculitis evaluation– Primary Angiitis of the CNS
– Secondary vasculitis/vasculopathy
Inflammatory state/autoimmune disease
Drug and Alcohol use
Pregnancy test
OSA evaluation
In spite of all this, about 30% of strokes remain
cryptogenic.
31
St. Luke’s University Health Network
What about that drug I saw on TV?
32
St. Luke’s University Health Network
Treatment Options:
Antiplatelet agents
Anticoagulation
BP control
Lipid-lowering agents
Glycemic control
Surgical revascularization
Lifestyle modification program
OSA tx
Other*
33

3/18/2016
12
St. Luke’s University Health Network
Antiplatelet agents
34
http://www.australianprescriber.com/magazine/30/4/92/6/ with modification
St. Luke’s University Health Network
Antiplatelet agents
Aspirin– For primary prevention in those with 10 year risk >10%, may also
be considered in those with CKD (GFR between 30-45); unclear
if it is helpful in those with DM and low 10 year CVD risk.
– For patients with a bio-prosthetic heart valve
– Initial agent for secondary prevention without extenuating
circumstances (allergy, severe CKD, PUD, etc…)
Cilostazol– For primary prevention in those with peripheral arterial disease
Clopidogrel– May be considered for secondary prevention in patients who fail
aspirin therapy
– Need to consider hypo/non-responders
35
St. Luke’s University Health Network
Antiplatelet FAQ’s and Controversies
What about Aggrenox?– Reasonable for secondary stroke prevention but not often used.
Doses of Aspirin– There have not been any studies demonstrating a difference
between 81mg and 325mg for stroke prevention at this point.
Dual antiplatelet agents– One study suggested a benefit for secondary prevention when
initiated early but it was only done in China and has limited
generalizability.
– May be considered for those with severe intracranial
atherosclerosis, recent drug-eluting stent placement, or with
atrial fibrillation who cannot tolerate anticoagulants.
36
3/18/2016
13
St. Luke’s University Health Network
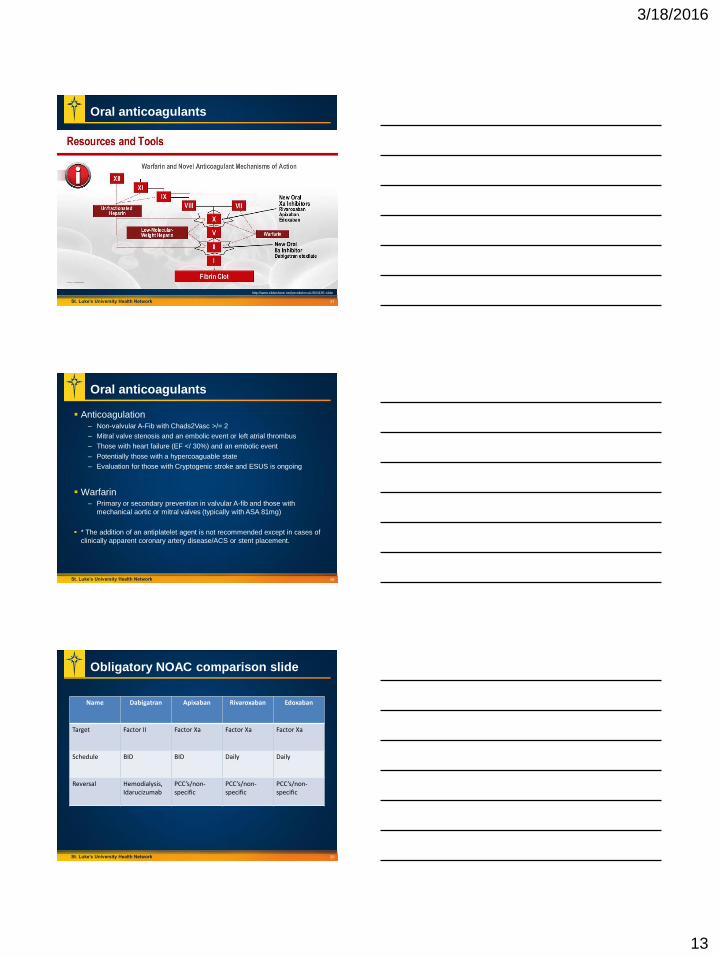
Oral anticoagulants
37
http://www.slideshare.net/peraltalorca1/804185-slide
St. Luke’s University Health Network
Oral anticoagulants
Anticoagulation– Non-valvular A-Fib with Chads2Vasc >/= 2
– Mitral valve stenosis and an embolic event or left atrial thrombus
– Those with heart failure (EF </ 30%) and an embolic event
– Potentially those with a hypercoaguable state
– Evaluation for those with Cryptogenic stroke and ESUS is ongoing
Warfarin– Primary or secondary prevention in valvular A-fib and those with
mechanical aortic or mitral valves (typically with ASA 81mg)
* The addition of an antiplatelet agent is not recommended except in cases of
clinically apparent coronary artery disease/ACS or stent placement.
38
St. Luke’s University Health Network
Obligatory NOAC comparison slide
Name Dabigatran Apixaban Rivaroxaban Edoxaban
Target Factor II Factor Xa Factor Xa Factor Xa
Schedule BID BID Daily Daily
Reversal Hemodialysis, Idarucizumab
PCC’s/non-specific
PCC’s/non-specific
PCC’s/non-specific
39

3/18/2016
14
St. Luke’s University Health Network
Hypertension
Represents the most important modifiable risk
factor.
For primary prevention, annual screening of
those with prehypertension with lifestyle
modification is recommended.
Effect of treatment is more important than the
specific agent considered.
The target for BP reduction is uncertain but goal
values <140/90 are reasonable. In some
circumstances SBP < 130 may be desirable.
40
St. Luke’s University Health Network
Dyslipidemia
Rather than a specific LDL target, for primary
prevention, low/moderate/high intensity statin
therapy is recommended for
low/intermediate/high risk as determined by the
AHA/ASA risk calculator.
Other agents may help lower cholesterol but are
not proven to help reduce the incidence of stroke.
For secondary prevention, when a stroke is
presumed to be atherosclerotic, high intensity
statin is recommended; even if LDL < 100.
41
St. Luke’s University Health Network 42
Stone NJ, et al. 2013 ACC/AHA guideline on the
treatment of blood cholesterol to reduce atherosclerotic
cardiovascular risk in adults: A report of the american
college of cardiology/american heart association task
force on practice guidelines. Circulation. 2014;129(25
SUPPL. 1).

3/18/2016
15
St. Luke’s University Health Network
Statin Therapy
Low Intensity Daily dose lowers LDL-C by >30%
Simvastatin 10mgPravastatin 10-20mgLovastatin 20mgFluvastatin 20-40mgPitavastatin 1mg
Moderate Intensity Daily dose lowers LDL-C by approximately 30-50%
Atorvastatin 10-20mgRosuvastatin 5-10mgSimvastatin 20-40mgPravastatin 20-40mgLovastatin 40mgFluvastatin XL 80mgFluvastatin 40mg BIDPitavastatin 2-4mg
High Intensity Daily dose lowers LDL-C by >/=50%
Atorvastatin 40-80mgRosuvastatin 20-40mg
43
St. Luke’s University Health Network 44
St. Luke’s University Health Network
Diabetes
For those with DM and otherwise low CV risk the
benefit of aspirin for primary prophylaxis is
unclear.
Patients with stroke/tia should be evaluated for
DM, HgB A1c is likely more accurate in the early
acute setting.
There are not guidelines from the AHA/ASA that
are specific for stroke but we typically counsel for
a goal HgB A1c <7%.
45

3/18/2016
16
St. Luke’s University Health Network
Surgical intervention
Intracranial:– Angioplasty and/or stenting is considered investigational and
should only be considered in the case of failure of medical
therapy.
Carotid revascularization:– May consider CEA in asymptomatic patients with >70% stenosis
if the risk of perioperative MI/stroke/death is <3%. CAS may be
considered in this setting but effectiveness compared to best
medical management is not clear.
– Consider CEA or CAS in symptomatic patients with >70%
stenosis by non-invasive imaging or > 50% by cath based
imaging (or non-invasive imaging with corroboration) as long as
periprocedural expected stroke/death rate is <6%.
46
St. Luke’s University Health Network
Lifestyle Modification
47
St. Luke’s University Health Network
Sleep disordered breathing
Represents a modifiable risk factor for
cardiovascular disease and stroke.
Would be reasonable to evaluate with forms such
as the Epworth sleepiness scale or via referral to
a sleep center/polysomnography.
Is among the interventions for stroke prevention
that will really help the patient feel better.
48
3/18/2016
17
St. Luke’s University Health Network
Potpouri
Cerebral Amyloid Angiopathy– Boston Criteria
Aortic arch atheroma
Sickle Cell disease– Transfuse to a goal of HgB S < 30%
Migraine with aura– Consider avoiding contraceptives and counsel strongly to avoid
tobacco use.
Pregnancy
49
St. Luke’s University Health Network
Summary
Stroke is ubiquitous, rapid, and unforgiving.
The best offense is a good defense.
Partnering with your local vascular neurologist
can help to clarify complex cases.
THANK YOU FOR YOUR ATTENTION!
50