primary care dermatology society spring 2011 - pcds · every time i sit down to write this report...
TRANSCRIPT

Every time I sit down to write this report it seems there are new and more problems
that the primary care and the dermatology world in general have to face. It reminds
me of my borrowed phrase when moving into a large new medical centre 15 years
ago, when I warned my colleagues and staff that the only constant I could guarantee
was change!
If we listen to our current political masters we, as GPs, should be whooping with
pleasure at the power they are handing over to us, and the opportunity to configure
the future health service as we want. Notice the missing “National” since the
localising of commissioning is already and will, I believe, become ever more
post-coded. This means the blame will be passed onto our local heads and indeed for
some, the legal responsibility.
Where does this leave primary care dermatology or as I prefer to call it “care for
dermatology patients?” The Skin Care Campaign (SCC) is rightly concerned about
the future risk of high cost, rare and less glamorous diseases for which patients will
in future have to travel even longer distances for treatment, or not receive care at all.
In addition the lumping in of dermatitis as a minor ailment (at number two by
frequency of diagnosis to number one URTI) by the PAGB (Proprietary Association of
Great Britain) and supported by the great and the good in our RCGP. This makes us
very worried that patients with long term conditions such as atopic dermatitis will be
Primary Care Dermatology Society Spring 2011
Bulletinpcds.org.uk
Chairman’s Report
The PCDS Trustee Committee
Mr Peter Lapsley Dr Tom PoynerDr Stephen Hayes Dr Jane Rakowski Dr Julia Schofield

Epiduo Gel Abbreviated Prescribing InformationPresentation: 0.1% adapalene & 2.5% benzoyl peroxide Indications: Cutaneous treatment of acnevulgaris when comedones, papules and pustules are present. Dosage and Administration: A thin filmshould be applied to the entire acne affected areas once a day in the evening to clean & dry skin. If irritationoccurs, apply non-comedogenic moisturizers, use the medication less frequently, suspend use temporarily,or discontinue use altogether. Duration of treatment should be determined on the basis of clinical condition;early signs of improvement usually appear after 1 to 4 weeks. The safety and effectiveness of Epiduo havenot been studied in children below 12 years of age. Contraindications: Hypersensitivity to the activesubstances or to any of the excipients. Precautions and Warnings: Should not be applied to damaged,broken or eczematous skin, or come into contact with eyes, mouth, nostrils or mucous membranes (washimmediately with warm water if product enters eyes). Contains propylene glycol (E1520) which may causeskin irritation. Avoid excessive exposure to sunlight or UV light. Avoid contact with any coloured materialincluding hair and dyed fabrics as this may result in bleaching and discoloration. Epiduo should not be usedduring pregnancy. Interactions: No interaction studies have been conducted with Epiduo. There are noknown interactions with other medicinal products which might be used cutaneously and concurrently withEpiduo. However, other retinoids, benzoyl peroxide or drugs with a similar mode of action should not beused concurrently. Caution should be exercised if cosmetics with desquamative, irritant or drying effectsare used, as they may produce additive irritant effects with Epiduo. Absorption of adapalene & benzoylperoxide through human skin is low therefore interaction with systemic medicinal products is unlikely.
Undesirable Effects: Epiduo may cause the following localized adverse reactions: Common (≥ 1/100to <1/10): dry skin, irritative contact dermatitis, burning and skin irritation. Uncommon (≥ 1/1000 to≤1/100): pruritus and sunburn. Unknown (cannot be estimated from the available data): allergic contactdermatitis, swelling face. If skin irritation appears after application of Epiduo, the intensity is generallymild or moderate, with local tolerability signs and symptoms (erythema, dryness, scaling, burning andpain of skin (stinging pain)) peaking during the first week and then subsiding spontaneously. PackagingQuantities and Cost: 45g tube £17.91 (NHS) MA Number: PL 10590/0057 Legal Category: POM FullPrescribing Information is Available From: Galderma (UK) Limited, Meridien House, 69-71 ClarendonRoad, Watford, Herts, WD17 1DS. UK. Tel: +44 (0)1923 208950 Fax: +44 (0)1923 208998. Date ofRevision: November 2010.
Adverse events should be reported. Reporting forms and information can be found at www.yellowcard.gov.uk.
Adverse events should also be reported to Galderma (UK) Ltd.
She wants fast results. You want long-term results.
NEWIntroducing an acne therapy that keeps
you both happy
This weekend This summer This time next year
Date of preparation: January 2011 EPI/508/0111Copyright © 2011 Galderma (UK) Ltd.

pushed into self diagnosis and purchasing treatments rather than being diagnosed by
a GP. Important and appropriate medication prescribed is currently free to children and
pensioners.
On both these counts we at the PCDS are working with many agencies (All Party
Parliamentary Group on Skin; Dermatology Council for England; BAD and the
Department of Health (DH)) to ensure that commissioners will be obliged to provide
full dermatology services in their area and not just the cheapest basic service,
whether that be by GPSIs or private providers. It is important not to neglect the
training and research provision that is so vital for the long term. That is not to say that
Intermediate care and training cannot be provided by GPSIs. Indeed the opposite is
true, however, a fully integrated service incorporating secondary and tertiary care is
essential and must also be protected. To this end there is a DH supported
multidisciplinary committee working at present to provide standards for
commissioners and previous work on accreditation requirements for GPSIs; which is
a little less proscriptive but similar to the 2007 regulations.
We must not let local commissioners think of dermatology as an easy target for cuts
when for years in many areas it has been woefully neglected and patients suffer as a
consequence. Recently in North London we heard of pharmacy advisors verbally
advising GPs not to prescribe any emollients (despite ever increasing evidence of
effectiveness) and to tell patients to buy them! Note, they did not dare to write it
down since I believe this is against the NHS act, which requires a doctor to prescribe,
needed medication. Please let us and everyone know of any such outrageous acts.
The SCC are particularly keen to be informed.
On a cheerful note the “Essential Dermatology” series of 10, repeated, one-day
courses for VTS registrars, specialist nurses and GPs whose dermatology knowledge
is less than comfortable starts in April. The venues are listed on the website and
advertised in Pulse. These are in addition to our usual high standard meetings and will
provide the essential knowledge for day-to-day care of the common dermatology
diseases. Please make these known to your registrars, VTS course organisers,
colleagues and commissioners/PCTs, whom we will be contacting but who may need
reminding. Partners may risk becoming deskilled if they are not at present by your
very presence as a skin authority in the practice!
Stephen Kownacki
Executive Chair

Editorial Spring 2011
I’m writing the Spring Editorial inspired by the fact
that our Christmas Camellia is finally flowering and
we also suddenly have a wonderful show of irises in
the garden. It seems like a long time since I planted
them. I’ve also managed to survive a family skiing
holiday without any injuries for which I am very
grateful.
It’s been a busy time for the committee recently.
We have been involved in writing the new GPSI
guidance which is currently at the Department of
Heath and will be released shortly. Stephen
Kownacki has already mentioned the Essential
Dermatology series that will be starting this April in
his report. We are also currently involved with other
Stakeholders in writing guidance on Dermatology
Standards that the new commissioners will be able
to use when PCTs disappear …
Jason Davies, a Histopathologist in North Devon
has kindly agreed to write a couple of articles on the
subject that we all struggle to get to grips with. The
first article, I’m sure you will agree, explains in
simple terms how histopathology can help in the
diagnosis of skin cancers. The next article will focus
on common inflammatory dermatoses.
I also have articles on top 10 fungal tips and
teledermatology in the pipeline, in addition to our
regular features. If anyone has any ideas on future
articles or recommendations of authors please can
you let me know.
I’m very grateful to Stephen Hayes, who recently
resigned from the committee, but continues to
work with us on a regular basis. The article that he
has written on exciting developments in treatments
of melanoma is well worth a read.
4
The vitamin D consensus statement is definitely
worth a mention for those who haven’t seen it. It
represents the unified views of the British
Association of Dermatologists, Cancer Research
UK, Diabetes UK, the Multiple Sclerosis Society, the
National Heart Forum, the National Osteoporosis
Society and the Primary Care Dermatology Society.
In summary it was agreed that Vitamin D is
essential for healthy bones and that the most
important source was from sunlight. It was thought
that the amount of time needed to make vitamin D
was dependant on physical, environmental and
personal factors. It was impossible to state an exact
time of exposure but was thought to be short and
less that the amount of time taken for the skin to
redden and burn. It was thought that a matter of
minutes in the middle of the day without sunscreen
should be sufficient and that people should become
familiar with their skin types and learn how long
they could be exposed before burning. Whether
vitamin D protects against chronic diseases such as
cancer, heart disease and diabetes, and the benefits
and risks of widespread supplementation needs
further research. Sounds like common sense to me.
Lastly the BBC news health reported that sap from
the common garden weed petty spurge appears to
treat non-melanoma skin cancers. This was from an
article published in the British Journal of
Dermatology. Results were promising, 41 out of 48
cancers had completely resolved after a month’s
treatment. More work is obviously needed as this
was a small study. Experts suggest not trying this
at home!
Helen Frow

5
Sewing with Christy
If you want to be an excellent Skin Surgeon, you need to
be good at every step of the procedure; from introducing
yourself and inspiring immediate confidence in your
patients, to explaining clearly why their surgery is
necessary, the risks and benefits of the procedure, and the
most likely outcome. The more you can put your patient at
ease, the more successful the operation will be. Once your
patient is relaxed and ready you should start by injecting your
local anaesthesia in the least painful way.
This short article will concentrate on why anaesthesia is painful,
the best agents to use, equipment to have available, plus a few
personal tips from me. I perform more than 2000 skin surgery
operations per year under local anaesthetic. The important point
to mention here is; the more operations you do the more you
will learn from your own experiences and that ultimately, you
will become a better Skin Surgeon.
The most commonly used agent in surface anaesthesia is
Lidocaine (Xylocaine is the trade name). It is safe because of its
rapid onset, low risk of producing allergic reactions and is
extensively used in general practice and plastic surgery. It is
almost entirely metabolised by the liver, and renal excretion is a
minor pathway in the elimination process, due to extensive
re-absorption (less than 10% of the administered dose is found
unchanged in the urine). Lidocaine along with other
anaesthetics should be used with caution in patients with
epilepsy, respiratory, renal, liver or cardiac impairment. The
maximum safe dose for healthy adults should not exceed
200mg in a single dose (ie 20 ml of the 1% Lidocaine). If close
to this amount of local anaesthetic is used during your surgical
procedure you really need to ask yourself if you should be doing
this in your clinic or should the patient be referred to hospital?
There are several reasons that local anaesthesia is painful. The
most obvious one is that the needle is sharp! Also, Lidocaine is
acidic (ph 4-5.) and the physical volume will push the dermal
stretch receptors to the painful limit. Cold anaesthetic, straight
from the fridge is more uncomfortable than injecting it at room
temperature.
The smaller the gauge of your needle, the less painful as it
reduces frictional pain when the needle pierces the skin. The
best needle to use is the 27 gauge (Green needle is 21, Blue is
23 and Orange is 25). A sterican ophthalmic needle is the same
length as the green needle, yet is more flexible and you will
use less local anaesthetic agent as you inject. The longer barrel
of the needle will cover a larger area with each entry, reducing
the number of times you need to enter the skin.
Here are a few personal tips to make the injection less painful.
Relax and prepare the patient. A friendly, chatty assistant, who
distracts the patient and holds their nervously, shaking hands is
so important to reassure the patient and make them feel at
ease. Always use local at room temperature, massage and
manipulate the skin next to the injection site and inject slowly.

6
Plain local is less painful than those with added
Adrenaline. Always try to inject into the
subcutaneous tissue – although it will take longer
for the local to take effect ... be patient Doctor, it is
worth it in the end! Ask the patient to concentrate
on deep breathing and count in their head slowly to
a hundred – all steps to distract the patient. If Emla
cream (a combination of Lidocaine and Prilocaine) is
used, it must be applied to the site at least 90 mins
before the procedure. Preferably cover the Emla
with a film dressing such as Tegaderm or Opsite to
retain a thick application of the cream at the
injection site for the full 90 minutes.
After administering the anaesthetic always check
the patient is pain free before you start your
procedure. If you have to interrupt the operation half
way because the patient is experiencing pain, you
will have to remove your sterile gloves, draw up
extra local, re-inject then scrub up again. You will
disturb your surgical train of thought, increase the
risk of infection and above all it is very annoying. A
frustrated Surgeon tends to make more mistakes!
To test that the local anaesthesia is working
properly before you start your procedure, gently
press your needle tip to the injected area which
should appear white from infiltration by the local. Do
not simply ask whether they can feel the needle,
because they will be able to sense pressure due to
the stretch receptors in the skin, which have a
thicker myelin sheath and are less sensitive to the
actions of local anaesthetic. In other words the
patient will still feel pressure and touch sensations.
If local anaesthetic is injected close to a muscle it is
important to explain to your patient that there may
be temporary muscle weakness. Patients won’t
panic if they know what to expect.
One of the problems of plain Lidocaine is that it is
relatively short acting and does not allow you to
perform longer procedures. To get around this
problem the addition of Adrenaline to the Lidocaine
causes vasoconstriction, which prolongs the action
of the anaesthetic. This has the added benefit of
producing less blood in the operating site making it
easier for the Surgeon to see the tissue definition.
The combination of Lidocaine and Adrenaline also
reduces the amount of local anaesthesia used
making it much safer for the patient.
When using Lidocaine with Adrenaline in areas
supplied by end arteries such as the fingers, toes
and penis, there is a theoretical risk of tissue
necrosis, so, it is safer to use plain Lidocaine. It is
however safe to use this combination on the tip of
the nose as it is extremely vascular on the face.
Lidocaine with Adrenaline is routinely used in
plastic surgery on the nose without causing any
problems. But, if in doubt or, in cases where
patients have severe peripheral vascular disease or
uncontrolled diabetes then a low concentration of
Adrenaline 1 in 200,000 in 20ml should be used or
avoid Adrenaline all together.
Side effects from local anaesthetic are rare when
used within the safety dose. However, toxic
reactions are likely to occur when used in high
volumes or if accidental intravascular injection
occurs. Toxicity often presents as a sensation of
numbness or tingling. Other adverse reactions
include visual disturbance, anxiety, dizziness and
altered sensation around the lips and mouth. As
the toxic level increases patients may experience
slurring of speech, muscle twitching and seizures.
To minimise the risk of intravascular injection it is
recommended to aspirate prior to injection. If you
are using a small gauge needle, which will not
aspirate blood, insert the needle to the furthest
point, then inject while withdrawing the needle
towards you. Keep moving the needle while slowly
injecting small amounts.
In the next bulletin, I will describe the different
methods of administering local anaesthetic such
as field and nerve block. In the meantime practice
safely and enjoy cutting and stitching.
Christy Chou

I N T E L L I G E N T LY R E S T O R E D R Y S K I N
Name of the Class I Medical Device: Balneum Cream.Ingredients: Urea 5 %, Ceramide 3, Aqua, Glycine Soya Oil,Propylene Glycol, Cetearyl Alcohol, Liquid Paraffin, Isohexadecane,Sodium Lactate, Lactic Acid, PEG-20 Stearate, Polysorbate 60,Squalane, Stearic Acid, Disodium EDTA, Lecithin, Tocopherol,Ascorbyl Palmitate, Hydrogenated Palm Glycerides Citrate.Balneum Cream is free of fragrances, colourants and preservatives.Pharmaceutical form: Cream. White cream. Indications: For thesymptomatic relief of dry and very dry skin conditions. Dry and verydry skin is often associated with eczema, psoriasis and otherdermatological conditions in which the skin has low levels ofsubstances such as urea, ceramides and lipids. Balneum Creamcontains clinically proven ingredients such as urea, ceramide 3 and
lipids. It is formulated to protect the skin, to maintain skinmoisturisation and to restore the impaired skin barrier in conditionsgiving rise to dry skin. Method of administration: Using cleanhands, apply the cream to the skin twice daily. Contraindications:Patients with known hypersensitivity to any of the ingredients.Warnings and precautions: For external use only. Do not use onbroken or inflamed skin. Caution should be exercised withconcomitant use of some medicated topicals. If the conditionworsens on usage or if patients experience side effects, discontinueuse and consult a Health Care Professional. Undesirable effects:Very few side effects have been reported; typically local skinreactions. Special precautions for storage: Do not store above25°C. Use within 6 months of first opening. Pack sizes: Available
in 50g (£2.80) and 500g (£9.80) pump dispensers. CE markingheld by: Almirall Hermal GmbH, Scholtzstraße 3, 21465 Reinbek,Germany. Distributed in the UK by: Almirall Ltd, 4 The Square,Stockley Park East, Uxbridge, UB11 1ET.
References: 1. Balneum Cream label. 2. Puschmann M et al.Clinical Experimental Evaluation of the Effectiveness and Tolerationof a Urea-Ceramide Combination in Dry Skin. Akt Dermatol 2000;26: 70-75. 3. Cork M, Danby S. Skin Barrier Breakdown: ARenaissance in Emollient Therapy. British Journal of Nursing 2009;18(14): 872-877.
Date of preparation:January 2011. UKSOY0638.
Don't just rehydrate, help to restore the skin's natural barrier.1,2,3
A D VA N C I N G E M O L L I E N T T H E R A P Y
Urea 5% and ceramide 3
ANADVANCE
IN DRY SKINTREATMENT

8
Paediatric Vulval Problems
Introduction
Paediatric genital problems in childhood are less
common than in adults and occur more frequently
in females than males. I am unable to cover all
possible diagnoses in the next few paragraphs and
will instead focus on the most common problems
and their treatment.
The physiological differences between the vulva
due to the lack of oestrogen before puberty
explains many of the symptoms observed. It is also
important to appreciate that children may not have
the vocabulary to explain irritation and discomfort
in the anogenital region and this can sometimes
lead to behavioural problems and night terrors.
Vulvitis
In children the vulva is thin, easily damaged
epithelium with an absence of the lactobacilli
which are found post menarche. This makes
irritation from soaps and bubble baths more likely
with the possibility of secondary infection with
common skin infections rather than Candida
albicans. Inflammation in the vulval area is called
vulvitis.
The commonest causes of vulvitis (Fig 1) are;
• Atopic vulvitis
• Irritant Vulvitis
A history of eczema will increase the risk of vulvitis.
The disorder is easily managed by the following:
• Avoidance of soaps or bubble baths
• Wash with an emollient as a soap substitute
• Use an emollient each night on the genital region
before bed-time
• Treatment with mostly mildly potent topical
steroids without antifungal preparation for up to
6 days per month if needed
• Consider taking bacterial swabs of the area since
pain and discharge may be associated with a
staphylococcal or streptococcal infection
PsoriasisThis will often occur in the anogenital region in
children. It will often look worse than it feels
presenting as erythematous well demarcated vulval
skin lesions (Fig 2) which cause alarm to parents.
Dr Ruth Murphy PhD FRCP
Consultant Dermatologist, Queens Medical Centre, Nottingham

9
Whilst it is possible to completely control and
eradicate atopic vulvitis it is almost impossible to
completely clear genital psoriasis although it can be
managed so that symptoms are well controlled.
Treatment is similar for atopic vulvitis:
• Avoid irritants such as soap
• Use emollients to wash with
• Apply emollient each night before bed
• Consider secondary staphylococcal or
streptococcal infection
• Treat the inflammation with Trimovate ointment™
for up to 6 days per month
Lichen SclerosusThis is an autoimmune condition which causes
inflammation and thinning of vulval skin. It is often
itchy and on examination appears as white areas in
a figure of eight around the clitoral hood and
extending to the anus. The thinned skin is prone to
haemorrhage and tears easily (Fig 3). Patients may
present with constipation and issues around toilet
training. It is worth examining the skin elsewhere
for cutaneous patches. This condition is life long
and requires appropriate management to avoid
scarring. It is most often treated as thrush which I
have already explained in a pre-pubertal age group is
a very unlikely diagnosis. Suspected cases need
referral to secondary care.
Treatment of Lichen sclerosus is as follows:
• Avoid irritants and soaps
• Use emollients to wash with
• Switch off the inflammation with a decreasing
course of potent topical steroids with Clobetasol
Propionate ointment with the appropriate
specialist guidance.
ConclusionIn general it is possible to treat many vulval problems
in children with simple measures such as
discontinuation of soaps and bubble baths and use of
emollients. Most cases of vulvitis will easily be
managed in primary care. Other conditions such as
lichen sclerosus, vitiligo, aphthous ulceration etc may
need specialist input. It is important to remember that
vulval irritation in children is not likely to be thrush.
10
Understanding the Histology Report: Part One – Skin Cancer
Introduction
In this short article I will try to cover some of the main
problems and causes of confusion in histology reports. It is not
intended to be comprehensive but I hope that I can provide
some useful learning points.
Histology is useful for primary diagnosis and checking
diagnostic-accuracy, for providing prognostic information and
for medicolegal purposes. Always submit removed specimens
for histology. I have encountered several cases of recurrent or
metastatic melanoma where the previous “seborrheic wart”
had been thrown away.
Help the histopathologist by providing good clinical information,
including full patient demographics (usually computerised
anyway) and the lesion’s site and duration. The lesion’s
behaviour, appearance and stage of evolution are helpful.
Remember, formalin significantly changes a specimen’s
appearance and knowledge of the original colour may be useful
(e.g. Spitz naevi may be pink).
The histology report should be concise with clear diagnostic
and prognostic information, adhering to Royal College of
Pathologists (RCPath) minimum datasets (MDS). The RCPath
produces MDS for various tumour sites including skin1. This
document covers the common skin tumours. It is a concise,
useful reference and is available for download2.
The report should have sensible clinico-pathological correlation
and, if necessary, provide some advice on unusual diagnoses.
If the diagnosis is unexpected and not compatible with the
clinical picture then ask for a review, preferably at the local
multidisciplinary team meeting (MDT).
The excisional biopsy is most useful in the treatment and
investigation of skin tumours, and is the preferred method when
excision margins need to be assessed. Smaller biopsies produce
an increased risk of sampling error. Multiple rather than single
punch biopsies may help reduce this.
If removing facial lesions, where resection margins are more
critical, you might consider orientating the specimen. Use a
simple and consistent method, preferably with just one suture,
with or without diagrams for yourself and the pathologist. Use an
open loop so that the knot does not impinge on the skin, else the
specimen might be damaged during suture removal.
Resection margins are examined histologically using India ink
and other dyes, and carefully measured. Accuracy of
measurement can be agreed locally (e.g. “>1 mm” rather than a
specific measurement like “1.85 mm”). Recurrence is possible
even when margins are reported as “clear” for various reasons.
For example, tumours often appear as multiple separate nodules
with normal tissue between, rather than a single solid sheet –
though 3-dimensionally, these nodules may well link up. One of
these apparent nodules might “skip” onto the other side of the
resection margin. Fixation can shrink the specimen (and
therefore the size of the histological margin) by up to one third.
The wax tissue blocks produced from the specimen are up to
3 mm thick, but, after trimming, the material on a histology slide
Dr Jason Davies
Consultant Histopathologist, North Devon District Hospital, Barnstaple
11
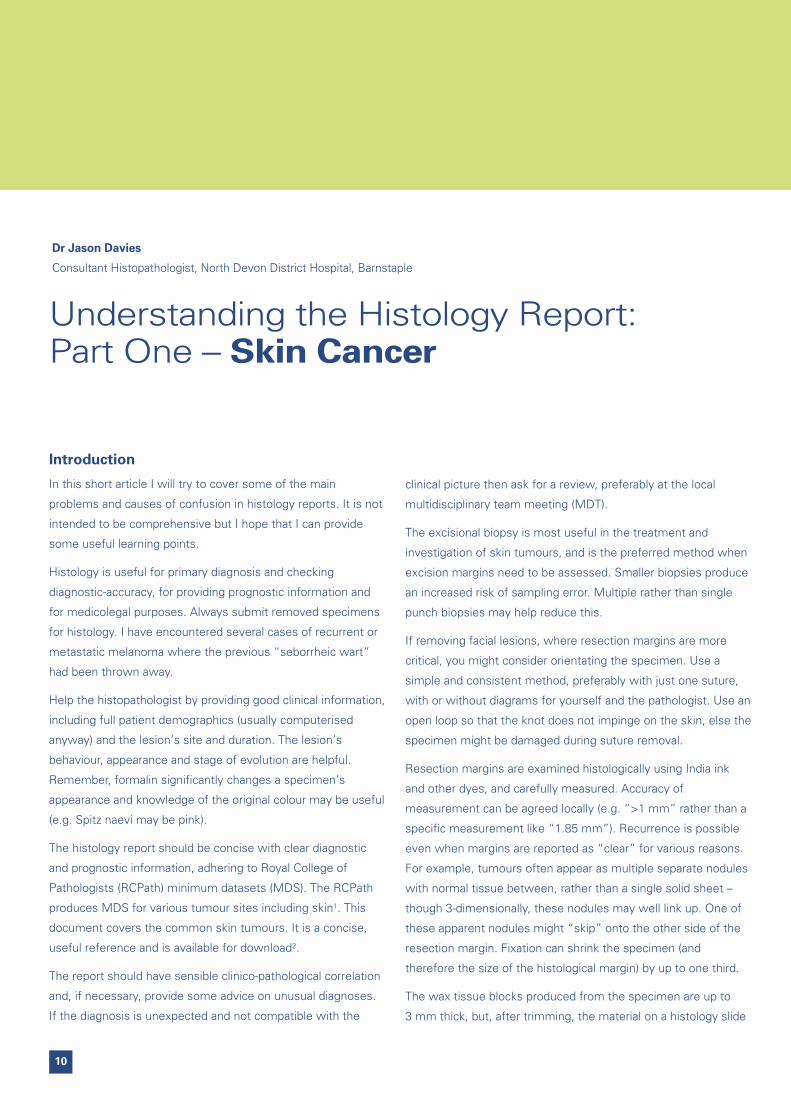
is only around 1/1000th of that (3 microns). So only a tiny
fraction of the specimen is actually viewed microscopically.
“Deepers”, “levels” and “serial sections” are all terms for
laboratory methods that involve cutting deeper into the wax
tissue block, to examine other areas (Fig 1). They all help reduce
the chance of sampling error.
Immunohistochemistry
Immunohistochemistry has largely displaced the use of special
stains in cancer diagnosis. It provides a method of
demonstrating specific antigens on a tumour cell and can help in
the differential diagnosis of morphologically similar tumours, in
separating benign from malignant lesions, in searching for early
invasion and in confirming provisional histological diagnoses.
Table 1 shows some of the commonly used antibodies that you
might see in histology reports.
Usually, a panel of several different antibodies is applied. As a
simple example, there are a variety of malignant spindle cell
tumours of the skin that look similar. A basic panel might show
no staining for S100 and MelanA (both melanoma markers) nor
for desmin (a muscle marker) but have positive staining for the
epithelial marker AE1/3, by which we could deduce the tumour
to be a spindle cell carcinoma.
Basal Cell Carcinoma (BCC)
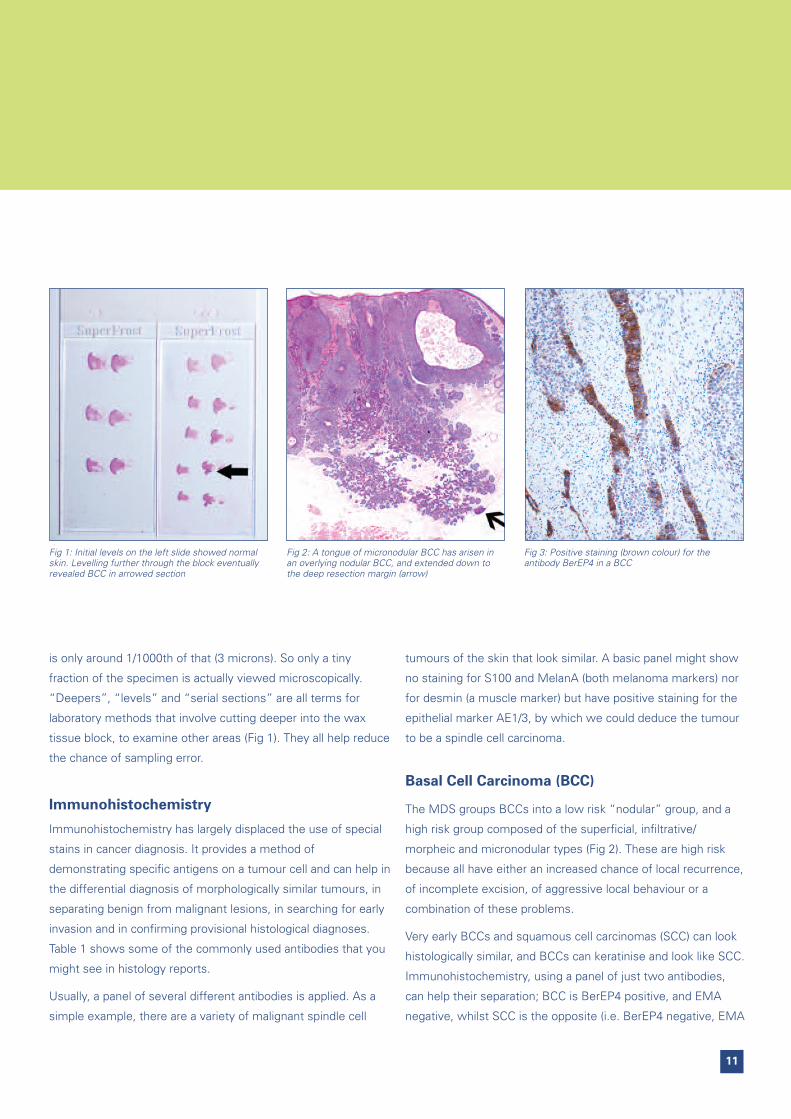
The MDS groups BCCs into a low risk “nodular” group, and a
high risk group composed of the superficial, infiltrative/
morpheic and micronodular types (Fig 2). These are high risk
because all have either an increased chance of local recurrence,
of incomplete excision, of aggressive local behaviour or a
combination of these problems.
Very early BCCs and squamous cell carcinomas (SCC) can look
histologically similar, and BCCs can keratinise and look like SCC.
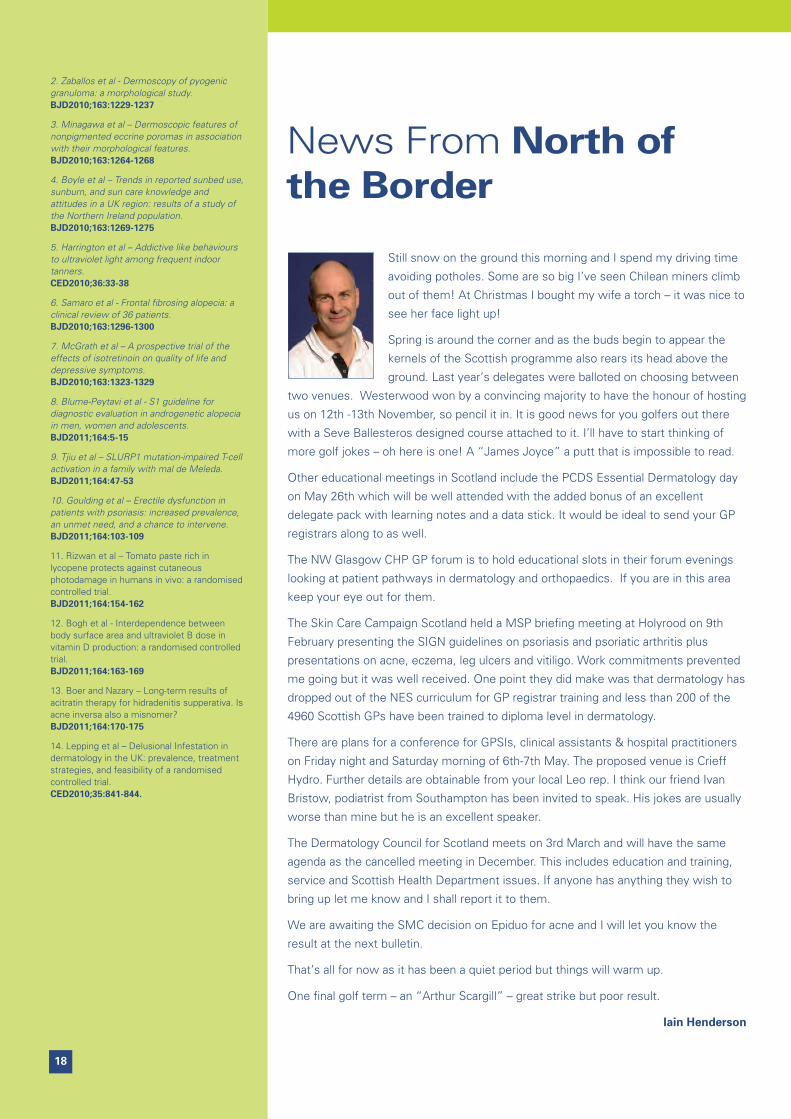
Immunohistochemistry, using a panel of just two antibodies,
can help their separation; BCC is BerEP4 positive, and EMA
negative, whilst SCC is the opposite (i.e. BerEP4 negative, EMA
Fig 1: Initial levels on the left slide showed normalskin. Levelling further through the block eventuallyrevealed BCC in arrowed section
Fig 2: A tongue of micronodular BCC has arisen inan overlying nodular BCC, and extended down tothe deep resection margin (arrow)
Fig 3: Positive staining (brown colour) for theantibody BerEP4 in a BCC

12
positive) (Fig 3). Most so-called basisquamous tumours stain
similarly to basal cell carcinomas, suggesting they are related
to the latter.
Squamous Cell Carcinoma
SCCs can arise in both actinic keratoses and Bowen’s disease,
both in-situ lesions with epidermal atypia/dysplasia (i.e.
abnormal cells). It can be very difficult to assess the very early
stages of invasion, which is usually seen as small tongues of
atypical squamous epithelium extending into the dermis.
However, several processes can closely mimic early invasion.
For example, the atypical epidermis can extend down eccrine
ducts and look invasive, as can crosscutting of the in-situ
component in a poorly orientated specimen (especially
fragments from curettage). These all might lead to uncertainty
in the histology report.
SCCs are graded as well, moderate, poorly or undifferentiated
tumours, which correspond with the alternative Broder’s
system of 1 (low grade) to 4 (high grade). Pathologists often
disagree about grading, in all tumour types, not just those in
the skin: a tumour that is called well differentiated by one
might be moderate to another.
Pathologists will measure the thickness of an SCC, as it is
required for staging, and will also provide a Clark’s level of
invasion, which you might be more used to seeing in reports of
malignant melanoma (Table 2).
Keratoacanthoma (KA)
Pathologists differ in their willingness to diagnose KA as a
separate entity; some believe they are simply variants of
well-differentiated squamous cell carcinoma. Even if KA is
diagnosed, many will add a sentence to say that SCC cannot be
excluded. Whilst some experts might accept biopsies, most will
want to see an excision biopsy, as the architecture can be the
key to diagnosis. If the pathologist is thinking about KA, you are
likely to see phrases such as “cup-shaped” or “crateriform” and
“ground-glass squamous epithelium”
Melanocytic Lesions
Dysplastic naevus can be difficult to diagnose histologically and
the threshold for diagnosis varies between pathologists. At one
end of the spectrum, there may be defensive over-diagnosis of
benign naevi as dysplastic, and in this circumstance you may
see a phrase such as “a naevus with some dysplastic features”.
Table 1: Some Common Immunohistochemical Antibodies
Tissue Type Antibody Comments
Melanocytic S100MelanA, HMB45
– sensitive but less specific (also stains neural tissue, etc)– more specific, less sensitive
Epithelial AE1/3Cam5.2CK 7, 20EMABerEP4
Smooth Muscle Smooth Muscle Actin (SMA)Desmin
Vascular CD 31, 34Factor 8 antigen
Lymphoid LCACD20CD 3, 4, 5, 8CD68
– Most Lymphocytes– B Cells– T Cells– Histiocytes

13
At the other end of the spectrum, their appearance merges with
in-situ malignant melanoma (MM), and these are sometimes
termed severely dysplastic.
Our practice is for MDT review of all possible dysplastic naevi.
We aim for complete excision in confirmed cases, and consider
wider excision for those described as severely dysplastic.
Some other terms that you might encounter in reports include
“Pagetoid” (after Paget’s disease of the nipple which it
resembles) which is a “buckshot”-like spread of melanocytic
cells into upper layers of epidermis (Fig 4). It is usually a feature
of superficial spreading MM. Lentiginous spread means single
melanocytes along the basal epidermis (e.g. in lentigo maligna).
Malignant Melanoma
The diagnosis of malignant melanoma can be difficult, and
research has shown that even expert pathologists can fail to
agree on the seemingly straightforward separation of benign
from malignant lesions3.
Melanoma can be an in-situ lesion (confined to the epidermis) or
invasive (infiltrating dermis). Melanomas are also separated into
2 different biological growth phases, which help predict their
behaviour, and these can cause some confusion.
The radial growth phase (RGP) includes both the in-situ lesions
and those showing the very earliest stage of invasion by a few
cells (so called micro-invasion). Theoretically, these have no risk
of metastasis.
However, in vertical growth phase (VGP), a more advanced
stage with a greater volume of invasive tumour, the melanoma
has metastatic potential.
The best prognostic indicator in melanoma is the lesion’s
thickness (the “Breslow depth” – measured from the granular
cell layer at the top of the epidermis to the deepest point of
tumour in the dermis), whilst the second most important
variable is the presence of ulceration, particularly greater than
3 mm. Both these indices have fairly good agreement between
pathologists and are used in the staging of melanomas.
Remember, if the melanoma is in-situ it will not have a depth.
References1. Minimum dataset for the histopathological reporting of common skin cancers –February 2002. Royal College of Pathologists
2. http://www.rcpath.org\resources\pdf\skincancers2802.pdf
3. Discordance among expert pathologists in diagnosis of melanocytic neoplasms.A. Ackerman. Human Pathology, Volume 27, Issue 11, Pages 1115-1116.
Table 2: Clark’s Levels for Malignant Melanoma and SCC
I Confined to epidermis (ie. in-situ, non-invasive)
II Invasion of papillary dermis
III Fills papillary dermis
IV Invasion of reticular dermis
V Invasion of subcutaneous fat
Fig 4: Pagetoid spread of melanoma cells labelled red with the antibody MelanA

14
Melanoma Sudy Group
The winter meeting of the Melanoma Study group was
held at the Royal Marsden Hospital in London on Friday
28th January, with 90 attending. The first presentation
discussed ultrasound with guided needle biopsy as a less
invasive potential alternative to sentinel lymph node biopsy
(SLNB) for staging melanoma. The speaker, Meiron Thomas,
felt SLNB was overrated. Interesting case reports were cited,
for example a surgeon, returning from an international
conference with a renewed interest in SLNB, did it on patients
who had been apparently disease free for 4 years since their
original surgery, finding occult micro metastases in some,
which had presumably sat there indolently for years.
Evidence was shown of melanoma being transferred via a
transplanted kidney, where the donor had been clinically
disease free for years. This was put down to occult dormant
micro metastases taking off in a new immune suppressed
host. Since we cannot detect micro metastases in vivo, this
raises all sorts of unanswered questions.
There was lively debate and no conclusion was reached. SLNB
is an invasive staging procedure which has not been
conclusively shown to improve survival. One issue around
lymph node biopsy that was raised, was that the benefits of
staging melanoma were questionable as we had no effective
therapy for metastatic disease. This, however, might change
soon, as we would hear from later speakers.
Better results from more radical node clearance?
Plastic surgeon Andrew Hayes advocated a more aggressive
surgical approach to ilio inguinal lymph gland dissection for
lower limb melanoma patients with inguinal spread. He
reminded us that the anatomical sub divisions we apply to the
various lymph gland basins were arbitrary: the lymphatic system
is a unitary whole. If groin glands were palpable, then iliac
glands would likely be involved. Also, our staging techniques
aren’t as good as we’d like, with many cancerous glands
undetected by PET scans, especially deep pelvic (obturator)
glands. He said many surgeons missed involved obturator
glands as it was so challenging to operate behind the iliac vein.
He said he ‘believed but couldn’t prove’ that patients with
biologically less invasive melanomas often experienced long
term survival or cure after radical removal of the deep pelvic
glands.
Another plastic surgeon explained how a new understanding of
cutaneous vascular anatomy was allowing better flap survival.
He also showed us a tour de force of heroic excisions and
reconstruction of catastrophically neglected scalp cancers. I
don’t think even the most experienced GPSIs should remove
the top of the skull, replace it with a titanium moulding and
swing a hand sized rotation flap over to cover the robo-cranium
and split skin graft the defect. I think we’ll leave that to the
glory boys.

15
BRAF and other melanoma mutations
If astounding advances are being made in plastic surgery, these
are arguably eclipsed by the new knowledge of the nature of
the genetic mutations which drive melanoma and the tools this
knowledge is giving oncologists. 50% of melanoma mutations
are BRAF, 25% NRAS and there are a few others. The
excitement has spilled over into the national press due to the
Plexxicon (TM) drug PLX4032 which targets BRAF mutations.
Some before and after PET scans showed liver and bone
secondaries shrink dramatically in 15 days. There are several
marvellous new drugs in trials, hoped to be marketed within 18
months.
Major side effects to wonder drugs
We heard that side effects had been somewhat played down.
Nearly all patients suffer skin problems including toxic
erythema, photosensitivity rashes and erythema nodosum. Of
more concern, a third of patients get squamous cell cancers
within months of starting therapy. These SCCs are apparently
sitting there sub clinically until the anti-BRAF drug releases
them (biology too complicated for me). Thankfully these
tumours are on the milder ‘keratoacanthoma like’ end of the
SCC spectrum and easily treated, but details are still scanty.
Polyarthralgia is also a problem with PLX4032, and price may be
as well.
Oncolytic viruses
The last excitement of the day concerned oncolytic viruses
which are once again being trialled. Several wild and
genetically modified viruses are being used, either
intravenously or directly injected into metastatic tumours.
Again, no trials but some impressive case studies. A
secondary deposit by the shoulder shrunk visibly after intra
lesional virus injection. CT scans showed distant metastases
shrinking also despite no other injections being made. A
biomed company which owns one of these GM viruses has
just changed hands for £400 million, prompting speculation
that someone might know something big!
Membership of the Melanoma Study Group is open to any
doctor or nurse involved in melanoma research or care.
Please see the web site for further details. The above is an
edited highlights of the day as seen by the only GP on the
Group. Much of it was above my head as this is mainly a
group for top specialists and researchers. Clearly these are
exciting times as far as the management of advanced
disease is concerned.
Stephen Hayes

December 2010 – January 2011
In a recent moment of clarity, it struck
us here at PCDS Towers that, by the
time we have written these articles,
they have been collated, edited,
processed, type set, printed and sent
out to you, our topical and timely
salutations bear little resemblance to
the real world. I would consequently
like to be the first to wish you a Happy
Christmas and hope that you enjoy the
coming Olympic Games, in Rio.
I start, this bulletin, with a trio of papers
from across the globe1,2,3. Apart from the
ongoing debate as to whether it should
be ‘dermatoscopy’ or ‘dermoscopy’,
these papers illustrate an exciting part of
our working lives. When any new
technique is developed, one of the first
things that needs to be decided upon is
its vocabulary. Then comes the most
useful applications, then the esoteric. We
are at the point where the dermoscopy of
the common lesions is fairly well
understood but we have yet to head
down in to the backwaters of the truly
bizarre. In these papers we have an
attempt to differentiate between
pigmented actinic keratoses and lentigo
maligna (you can’t), to try to create a
diagnostic algorithm for pyogenic
granulomas (you can’t) and to try to
determine characteristic features of
nonpigmented eccrine poromas (structures reminiscent of frog spawn, seeing as
you ask). We often look at dermoscopy as the next big thing, but we must
recognise and understand its limitations. Timely advice.
Another pair of papers. Firstly, from Northern Ireland4 is a population study looking
at attitudes towards sun bed use, suncare and sunburn in a region where there
has been two decades of sun-related health care campaigns. Sun care knowledge
was shown to be good, but there were major barriers to continuing improvement.
Men, in particular, appear resistant to sun care advice. Women have entrenched
attitudes towards the ‘attractiveness’ of a suntan and there is a common lack of
knowledge between both sexes of what an individual’s skin type is. More
encouraging is that sunbed use, as a result of recent campaigns, is falling. This,
however, is tempered by a companion paper from CED5. Here, the investigators
used a modified CAGE questionnaire to look at tanning behaviour in frequent
users of sunbeds. They showed the behaviour in a significant proportion of these
users to be representative of addiction. 41% showed ‘tanning addictive disorder’,
a further 33% showed ‘problem tanning behaviour’. This was particularly linked to
female gender and an early age of first tanning ‘fix’. I find this fascinating and
disturbing in turns.
A question I find myself pondering, in quiet moments, is whether Queen Elizabeth
I suffered from frontal fibrosing alopecia (FFA)? Her portraits may suggest this, but
we may never know for sure. What we do now know , as a consequence of work
from California and London6, is that FFA is accompanied by combinations of
hairline recession, scalp pruritus, perifollicular erythema and loss of the eyebrows
at presentation. As a rare disease, treatment strategies are poorly determined, but
here it is shown that hydroxychloroquine, used early, can give significant benefit –
at least for the first six months of use anyway.
We shall return to the scalp in a moment, pausing briefly to consider the
association of isotretinoin and depressive symptoms. This has long been a source
of contention – indeed, part of the consent process revolves around the reporting
of mood changes and depressive symptoms in individuals who take isotretinoin. A
nicely written paper from Bath7 goes a long way towards putting this particular
JournalWatch
16

shibboleth to bed. Basically, isotretinoin improves the quality of life indices of
those who take it for severe acne – particularly in those who were depressed at
the outset of treatment. I italicise this for emphasis – we sometimes forget that
acne itself is a condition that leads to depression and even suicide. This study
suggests an improvement, not a deterioration in mood in isotretinoin takers.
Powerful stuff indeed.
Hair is one of those human Goldilocks features – everyone seems to have either
too much or too little, rarely just the right amount. Androgenetic alopecia (AGA)
can affect both men and women, and even occasionally, adolescents. Amazingly,
there are little or no evidence based guidelines on the diagnosis and management
of this common and often distressing condition. This paper8 is the first step in that
process, giving definitions of AGA and presenting a consensus statement for sex
dependent stages in diagnosis. The definition is particularly interesting – ‘a
progressive non-scarring miniaturisation of the hair follicle with a characteristic
pattern in genetically predisposed men and women’. The hairs are often still there,
just too small, fine or fragile to see. Investigation is also interesting – the
suggestion is that it is not necessary to investigate men, but women should have
thyroid function, ferritin levels and free androgen index measured. I presume a
similar paper will be forthcoming on the treatment of this disorder, sadly I expect it
may be very short.
I make no apologies for including this next paper9. I must admit I had never heard
of mal de Meleda, nor am I ever likely to encounter a case but I think it joyous to
discover that there is a gene called SLURP1. For the record, it encodes a
lymphocyte antigen activator related protein. I think it sounds fab!
The regular reader of this column will have seen several papers showing that
psoriasis should really be considered to be a multi-system disease that just
happens to have a cutaneous manifestation. The increased incidence of ischaemic
heart disease is well documented, but the atherosclerosis that accompanies this
can also be a factor in the development of erectile dysfunction10. In psoriasis, this
appears to be almost 50% more common than in a matched control group –
although, in mitigation, psoriasis is probably not an independent risk factor. In an
increasingly holistic speciality, should assessment of sexual function become
routine for attendees at dermatology departments?
Now a first. I don’t think the humble tomato has been mentioned in these pages
before. Tomatoes, as I’m sure you know, are rich in lycopene – an increasingly
interesting antioxidant compound. It has been shown to be protective against
ultraviolet induced Erythema. Taking this one step further, this study11 takes a
group of women and feeds them either 55g of tomato paste rich in lycopene in
olive oil, or just the olive oil alone...for 12 weeks. This dose was shown to be
photoprotective as the experimental subjects had sequential skin biopsies taken
from both UV exposed and non-exposed sites. A remarkable study – not the least
because 55g of tomato paste is quite a quantity and to eat this every day for 12
weeks must demonstrate a degree of dedication on the part of the subject.
Contentious subject, number 873 – Vitamin D and UV radiation. Sometimes
research is needed to create an evidence base, even where the outcome seems
to be plain common sense. As here12. Serum Vitamin D increases with increasing
exposure to the sun. This increase is dependent upon the dose of UVB received.
However, if these doses of UVB are less, then the area of body exposed must be
greater to achieve the same levels of
serum vitamin. No wonder the Finns are
fond of naked bathing.
We near the end – for this bulletin. I reckon
one of the most frustrating dermatological
conditions to treat must be hidradenitis
supprativa – one can only imagine what it
must be like to have to suffer it. At least,
after this useful paper from The
Netherlands13, there is at least some
evidence to base treatment, or referral,
decisions upon. Although a small study
(only 12 subjects), acitretin was used as
monotherapy to treat cases that were
refractory to other treatment modalities.
The results were very encouraging with all
subjects achieving remission – this
remission was relatively long lived, in one
case the subject remained disease free
after 4 years. Hope, perchance?
Finally, a disease about which we have
only really scratched the surface –
delusional infestation (sorry!). It is a
disease that is considered rare, but
incidence data only really exists for
Germany. This paper14 attempts to look at
prevalence, treatment strategies and
assesses the feasibility of a randomised,
controlled trial. Although still rare, it would
appear that it is more common than
previously thought with a three year
prevalence around 5 cases per million
population. This would mean that most
dermatology departments will see it on a
regular basis. Treatment seems to still
revolve around the use of antipsychotic
medications, but the numbers appear too
small to make a true trial of treatments
feasible.
So there you go. Only 2 months of
journals, but a lot to digest. I’m off for a lie
down in a darkened room!
Julian Peace
References1. Akay et al – Dermatoscopy of flat pigmented faciallesions: diagnostic challenge between pigmentedactinic keratosis and lentigo maligna.BJD2010;163:1212-1217
17
18
Still snow on the ground this morning and I spend my driving time
avoiding potholes. Some are so big I’ve seen Chilean miners climb
out of them! At Christmas I bought my wife a torch – it was nice to
see her face light up!
Spring is around the corner and as the buds begin to appear the
kernels of the Scottish programme also rears its head above the
ground. Last year’s delegates were balloted on choosing between
two venues. Westerwood won by a convincing majority to have the honour of hosting
us on 12th -13th November, so pencil it in. It is good news for you golfers out there
with a Seve Ballesteros designed course attached to it. I’ll have to start thinking of
more golf jokes – oh here is one! A “James Joyce” a putt that is impossible to read.
Other educational meetings in Scotland include the PCDS Essential Dermatology day
on May 26th which will be well attended with the added bonus of an excellent
delegate pack with learning notes and a data stick. It would be ideal to send your GP
registrars along to as well.
The NW Glasgow CHP GP forum is to hold educational slots in their forum evenings
looking at patient pathways in dermatology and orthopaedics. If you are in this area
keep your eye out for them.
The Skin Care Campaign Scotland held a MSP briefing meeting at Holyrood on 9th
February presenting the SIGN guidelines on psoriasis and psoriatic arthritis plus
presentations on acne, eczema, leg ulcers and vitiligo. Work commitments prevented
me going but it was well received. One point they did make was that dermatology has
dropped out of the NES curriculum for GP registrar training and less than 200 of the
4960 Scottish GPs have been trained to diploma level in dermatology.
There are plans for a conference for GPSIs, clinical assistants & hospital practitioners
on Friday night and Saturday morning of 6th-7th May. The proposed venue is Crieff
Hydro. Further details are obtainable from your local Leo rep. I think our friend Ivan
Bristow, podiatrist from Southampton has been invited to speak. His jokes are usually
worse than mine but he is an excellent speaker.
The Dermatology Council for Scotland meets on 3rd March and will have the same
agenda as the cancelled meeting in December. This includes education and training,
service and Scottish Health Department issues. If anyone has anything they wish to
bring up let me know and I shall report it to them.
We are awaiting the SMC decision on Epiduo for acne and I will let you know the
result at the next bulletin.
That’s all for now as it has been a quiet period but things will warm up.
One final golf term – an “Arthur Scargill” – great strike but poor result.
Iain Henderson
News From North ofthe Border
2. Zaballos et al - Dermoscopy of pyogenicgranuloma: a morphological study.BJD2010;163:1229-1237
3. Minagawa et al – Dermoscopic features ofnonpigmented eccrine poromas in associationwith their morphological features.BJD2010;163:1264-1268
4. Boyle et al – Trends in reported sunbed use,sunburn, and sun care knowledge andattitudes in a UK region: results of a study ofthe Northern Ireland population.BJD2010;163:1269-1275
5. Harrington et al – Addictive like behavioursto ultraviolet light among frequent indoortanners.CED2010;36:33-38
6. Samaro et al - Frontal fibrosing alopecia: aclinical review of 36 patients.BJD2010;163:1296-1300
7. McGrath et al – A prospective trial of theeffects of isotretinoin on quality of life anddepressive symptoms.BJD2010;163:1323-1329
8. Blume-Peytavi et al - S1 guideline fordiagnostic evaluation in androgenetic alopeciain men, women and adolescents.BJD2011;164:5-15
9. Tjiu et al – SLURP1 mutation-impaired T-cellactivation in a family with mal de Meleda.BJD2011;164:47-53
10. Goulding et al – Erectile dysfunction inpatients with psoriasis: increased prevalence,an unmet need, and a chance to intervene.BJD2011;164:103-109
11. Rizwan et al – Tomato paste rich inlycopene protects against cutaneousphotodamage in humans in vivo: a randomisedcontrolled trial.BJD2011;164:154-162
12. Bogh et al - Interdependence betweenbody surface area and ultraviolet B dose invitamin D production: a randomised controlledtrial.BJD2011;164:163-169
13. Boer and Nazary – Long-term results ofacitratin therapy for hidradenitis supperativa. Isacne inversa also a misnomer?BJD2011;164:170-175
14. Lepping et al – Delusional Infestation indermatology in the UK: prevalence, treatmentstrategies, and feasibility of a randomisedcontrolled trial.CED2010;35:841-844.

Abbreviated Prescribing Information for Dovobet® 50 microgram/g + 0.5 mg/g gel. Indications: Topical treatment of scalp psoriasis in adults. Topical treatment of mild to moderate ‘non-scalp’ plaque psoriasis vulgaris in adults. Active ingredients: 50 µg/g calcipotriol (as monohydrate) and 0.5 mg/g betamethasone (as dipropionate). Dosage and Administration: Apply to affected areas once daily. Recommended treatment period is 4 weeks for scalp and 8 weeks for ‘non-scalp’ areas. If it is necessary to continue or restart treatment after this period, treatment should be continued after medical review and under regular medical supervision. When using calcipotriol containing medicinal products the maximum dose should not exceed 15g/day. Treated area should not exceed 30% of body surface. Safety and efficacy in children under 18 years have not been established. Safety and efficacy in severe renal insufficiency or severe hepatic disorders have not been evaluated. Shake bottle before use. Do not apply directly to the face or eyes. Wash hands after use. It is not recommended to take a shower or bath, or to wash the hair in case of scalp application, immediately after application as the gel should remain on the skin during the night or day. If used on the scalp usually between 1g and 4g/day is sufficient for treatment. Contra-indications: Hypersensitivity to any constituents. Erythrodermic, exfoliative or pustular psoriasis. Patients with known calcium metabolism disorders. Viral skin lesions, fungal or bacterial skin infections, parasitic infections, skin manifestations in relation to tuberculosis or syphilis, perioral dermatitis, atrophic skin, striae atrophicae, fragility of skin veins, ichthyosis, acne vulgaris, acne rosacea, rosacea, ulcers, wounds, perianal and genital pruritus. Precautions and Warnings: Avoid concurrent treatment with other steroids. Adrenocortical suppression or impact on the metabolic control of diabetes mellitus may occur. Avoid application on large areas of damaged skin, under occlusive dressings or on mucous membranes or skin folds. Do not use on the skin of the face or genitals. Avoid inadvertent transfer to face, mouth and eyes. Wash hands after applying. There may be a risk of generalised pustular psoriasis. With long-term use there is an increased risk of local and systemic corticosteroid adverse reactions in which case treatment should be discontinued. There may be a risk of rebound when discontinuing treatment. No experience of use in guttate psoriasis. No experience of concurrent use with other antipsoriatic products administered topically (to the
same treatment area) or systemically; or with phototherapy. Physicians are recommended to advise patients to limit or avoid excessive exposure to natural or artif icial sunlight. Use with UV radiation only if the physician and patient consider that the potential benefits outweigh the potential risks. Contains butylated hydroxytoluene which may cause local skin reactions or irritation to the eyes and mucous membranes. Use in Pregnancy and Lactation: Only use in pregnancy when potential benefit justifies potential risks. Caution when prescribed for women who breast-feed. Instruct patient not to use on breast when breast-feeding. Side Effects: Pruritus. Additional undesirable effects observed for calcipotriol and betamethasone: Calcipotriol: application site reactions, skin irritation, burning and stinging sensation, dry skin, erythema, rash, dermatitis, eczema, psoriasis aggravated, photosensitivity and hypersensitivity reactions including very rare cases of angioedema and facial oedema. Hypercalcaemia or hypercalciuria may appear very rarely. Betamethasone: local reactions, especially during prolonged application including skin atrophy, telangiectasia, striae, folliculitis, hypertrichosis, perioral dermatitis, allergic contact dermatitis, depigmentation, increase of intra-ocular pressure, cataract, colloid milia, generalised pustular psoriasis, infections. Systemic reactions occur more frequently when applied under occlusion, on skin folds, to large areas and long- term treatment. Legal Category: POM. Product Licence Number and Holder: 05293/0005 LEO Pharmaceutical Products Ltd. A/S, Ballerup, Denmark. Basic NHS Price: £36.50/60g, £67.79/2 x 60g. Last revised: November 2010. Further information can be found in the Summary of Product Characteristics or from: LEO Pharma, Longwick Road, Princes Risborough, Buckinghamshire, HP27 9RR. ® Registered Trademark. e-mail: [email protected]
Adverse events should be reported. Reporting forms and information can be found at www.yellowcard.gov.uk. Adverse events should also be reported to Drug Safety at LEO Pharma by calling 01844 347333.
* Mild to moderate plaque psoriasis
See the Dovobet® Gel di� erence
The bene� ts are clear. Dovobet® Gel is a treatment for both body* and scalp psoriasis.
Simple to apply, it’s designed with patients in mind. Giving them the con� dence they
need to reveal more of themselves.
For further information visit: morethanpsoriasis.co.uk
LEO® ©LEO Pharma, UK, All LEO trademarks mentioned belong to the LEO Group. Code: 1008/10888 February 2011