primary hip arthroplasty cemented & uncemented frank r. ebert, md union memorial hospital...
TRANSCRIPT
Primary Hip ArthroplastyPrimary Hip ArthroplastyCementedCemented
&&UncementedUncemented
Frank R. Ebert, MDFrank R. Ebert, MD
Union Memorial HospitalUnion Memorial HospitalBaltimore, MarylandBaltimore, Maryland
Johns HopkinsJohns Hopkins
Union MemorialUnion Memorial
Orthopædic Review CourseOrthopædic Review Course
Anatomic ApproachAnatomic Approach
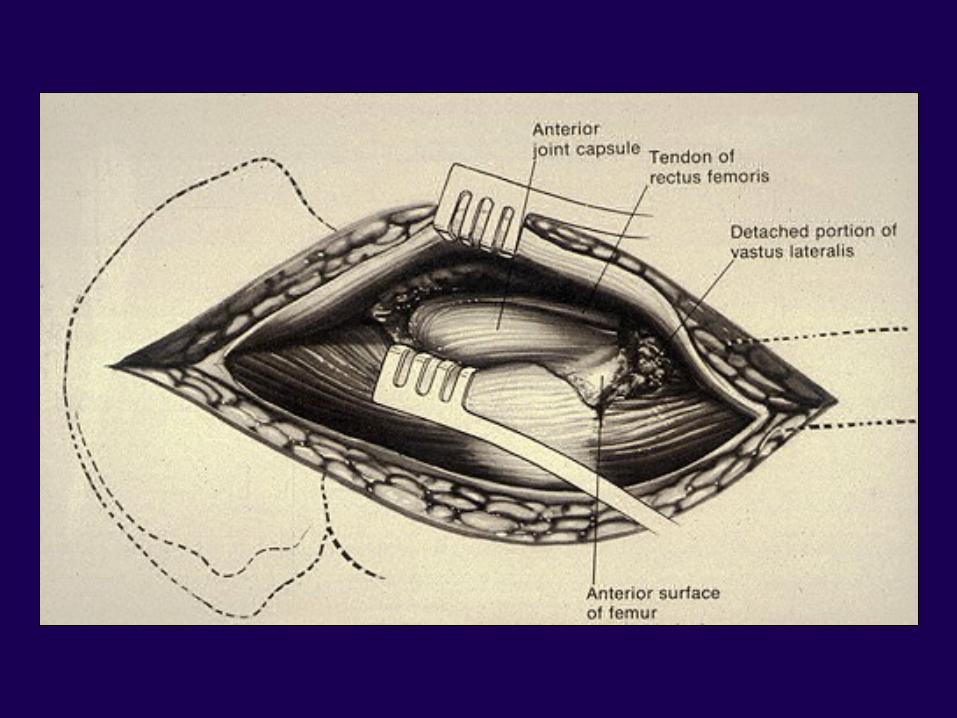
Anterior ApproachAnterior Approach
Anterior-Lateral ApproachAnterior-Lateral Approach
Posterior ApproachPosterior Approach
Medial ApproachMedial Approach
Anatomic ApproachAnatomic Approach
Open Reduction – CDHOpen Reduction – CDH
Pelvic OsteotomiesPelvic Osteotomies
Intra-Articular FusionIntra-Articular Fusion
Rarely Total HipRarely Total Hip
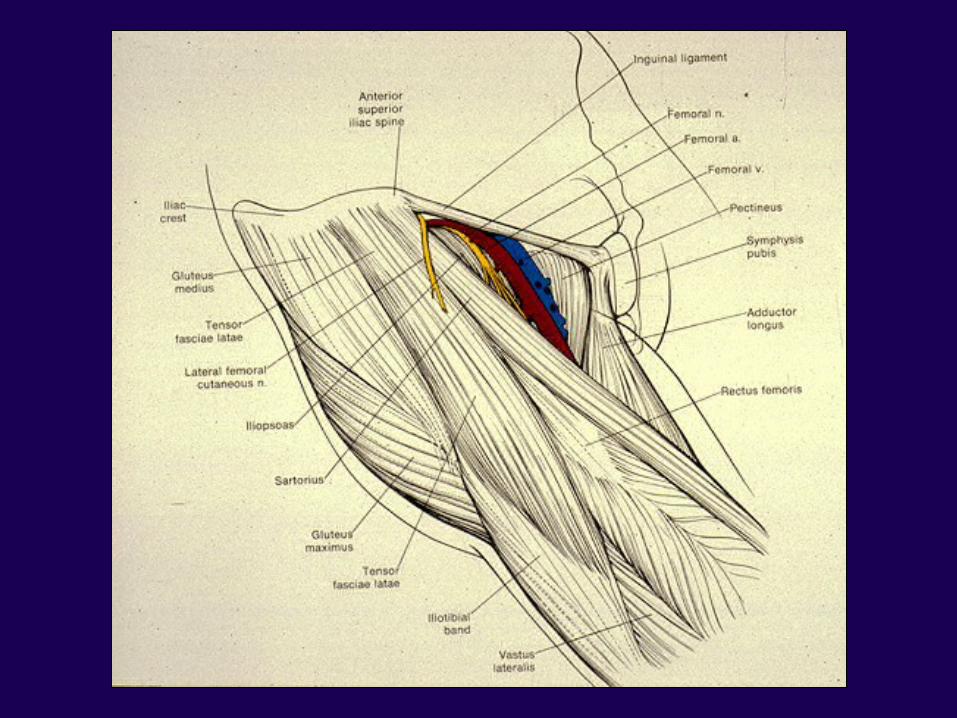
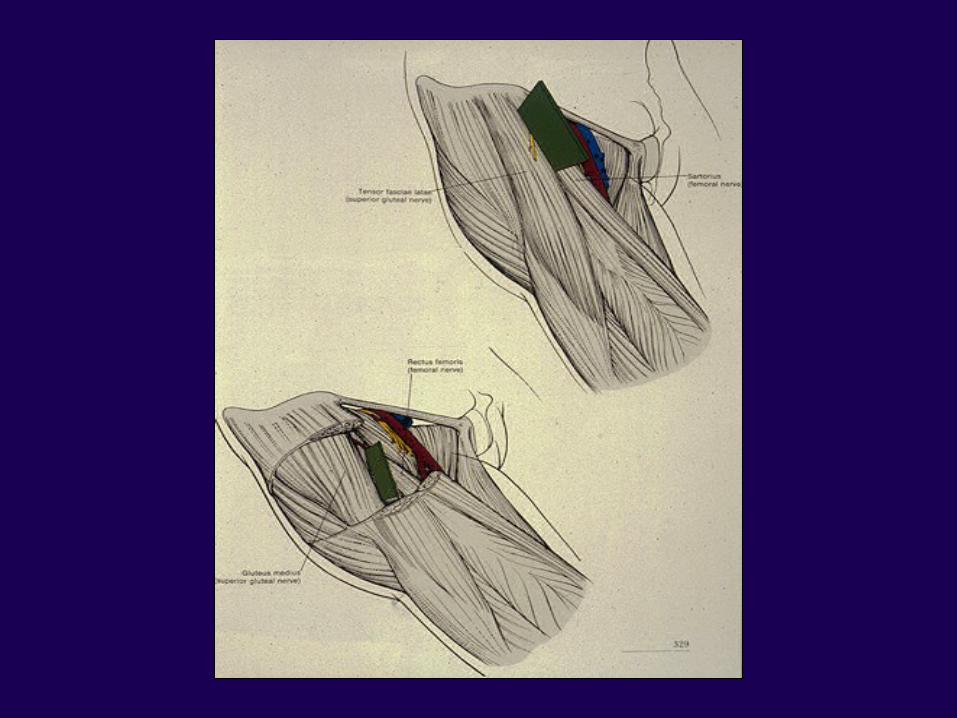
Internervous PlaneInternervous Plane
SuperficialSuperficial
–– Sartorius / TFL Sartorius / TFL ( Femoral/Superior gluteal )( Femoral/Superior gluteal )
DeepDeep
– – Rectus / gluteus mediusRectus / gluteus medius ( Superior gluteal )( Superior gluteal )
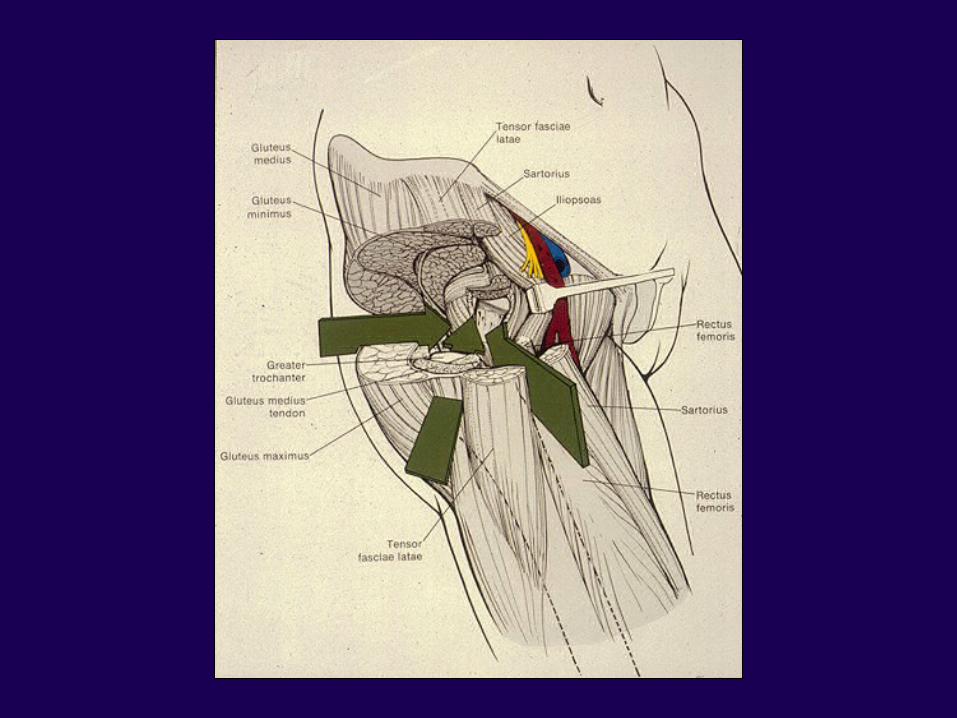
Anterolateral ApproachAnterolateral Approach
Most common for THAMost common for THA ORIF of femoral neckORIF of femoral neck Synovial biopsy of the hipSynovial biopsy of the hip
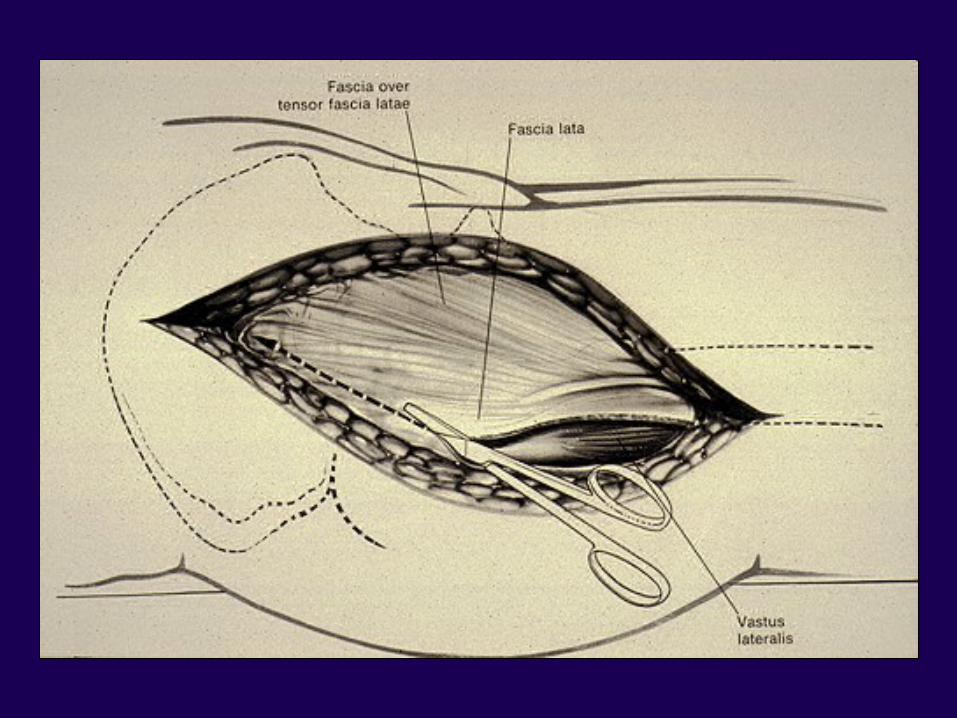
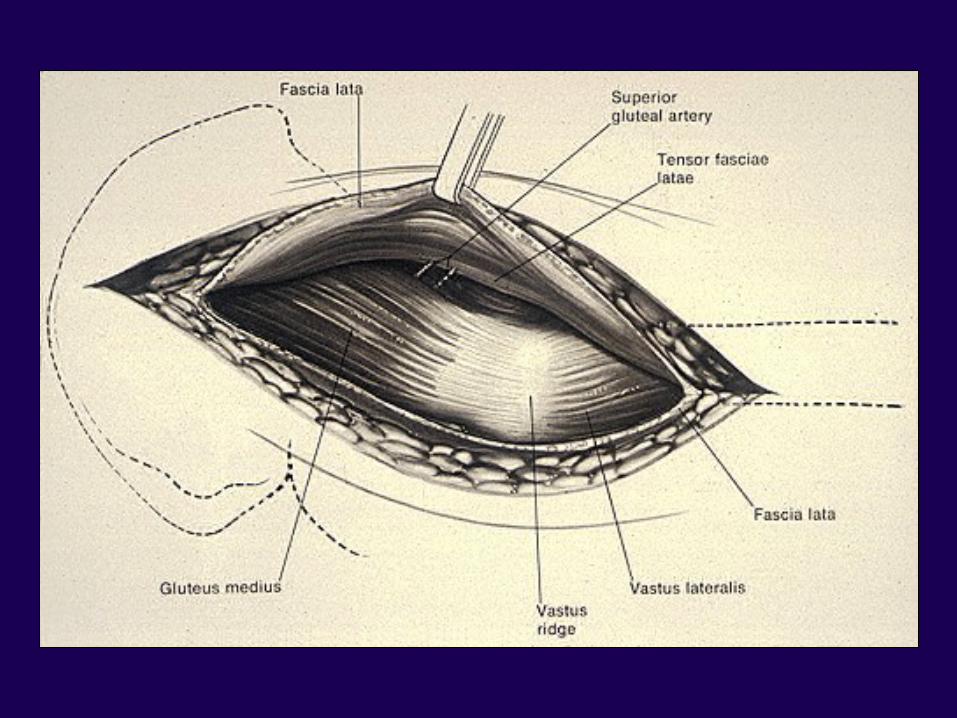
Anterolateral ApproachAnterolateral Approach
Internervous plane – noneInternervous plane – none
TFL / gluteus mediusTFL / gluteus medius
Superior gluteal / Superior glutealSuperior gluteal / Superior gluteal

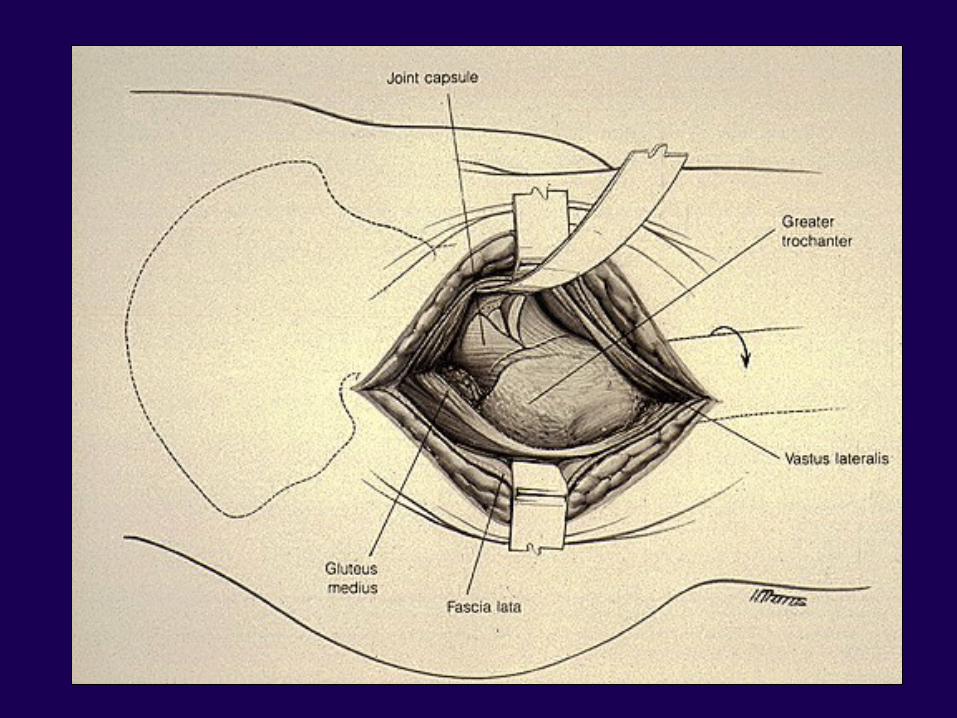
Lateral ApproachLateral Approach
DangersDangers
– – Superior gluteal nerveSuperior gluteal nerve
– – Femoral nerveFemoral nerve
Medial ApproachMedial Approach
CDH open reductionCDH open reduction
Psoas ReleasePsoas Release
Obturator NeurectomyObturator Neurectomy
Biopsy or Treatment of tumors Biopsy or Treatment of tumors of femoral neckof femoral neck
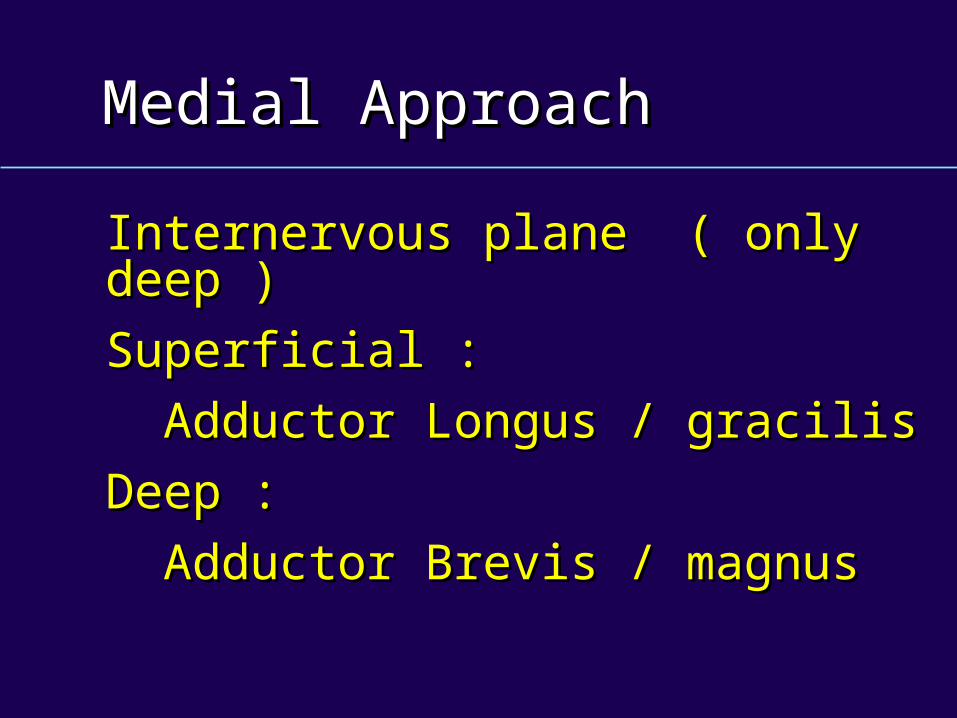
Medial ApproachMedial Approach
Internervous plane ( only deep )Internervous plane ( only deep )
Superficial :Superficial :
Adductor Longus / gracilisAdductor Longus / gracilis
Deep :Deep :
Adductor Brevis / magnusAdductor Brevis / magnus
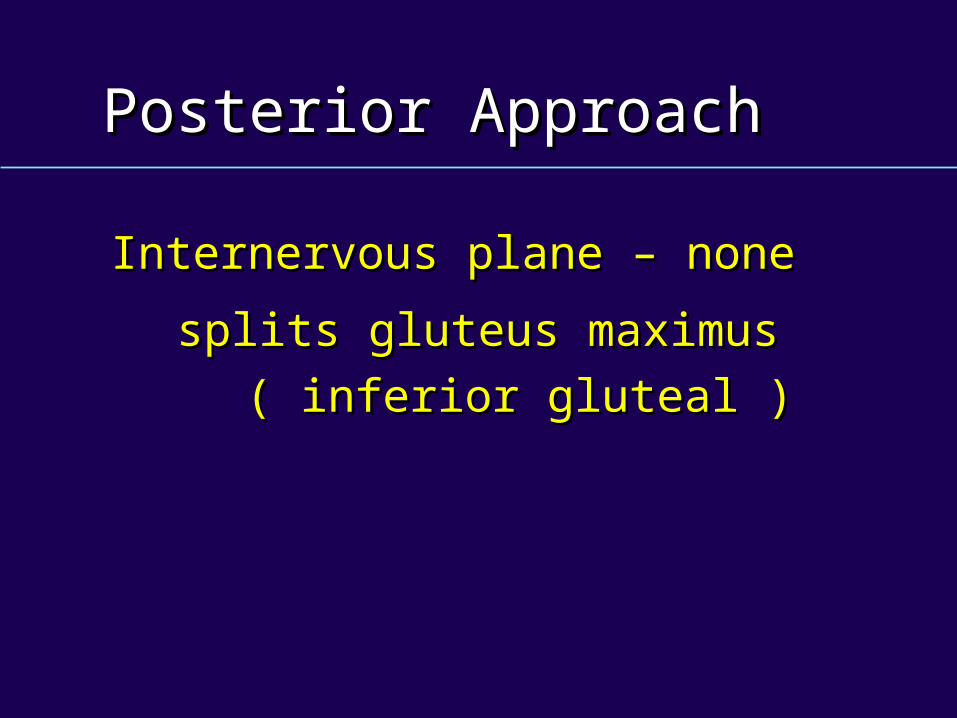
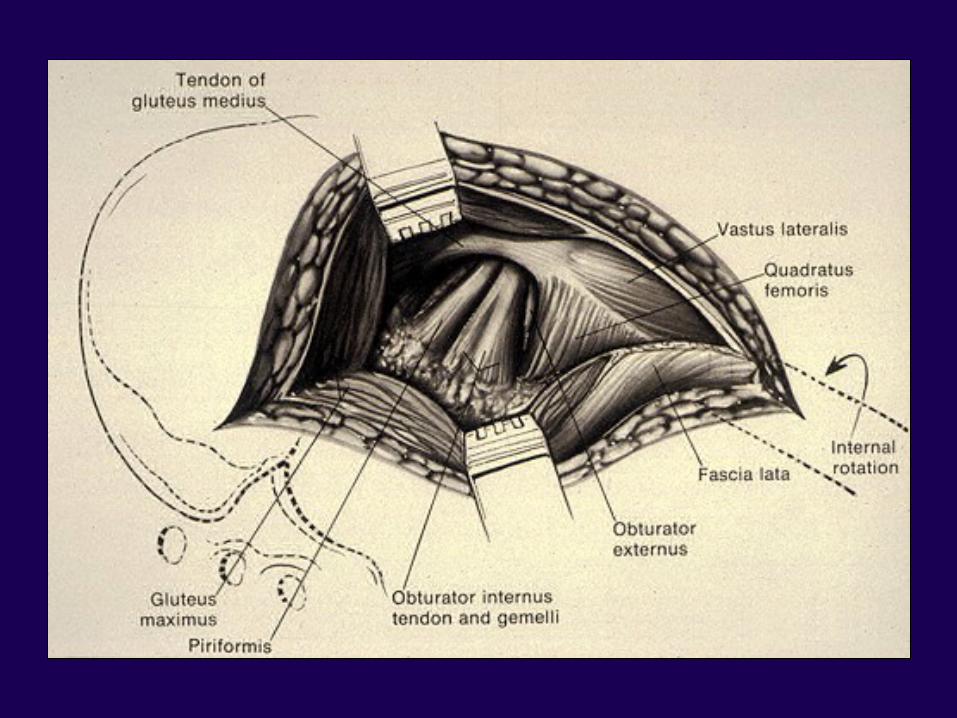
Posterior ApproachPosterior Approach
Internervous plane – noneInternervous plane – none
splits gluteus maximussplits gluteus maximus
( inferior gluteal )( inferior gluteal )

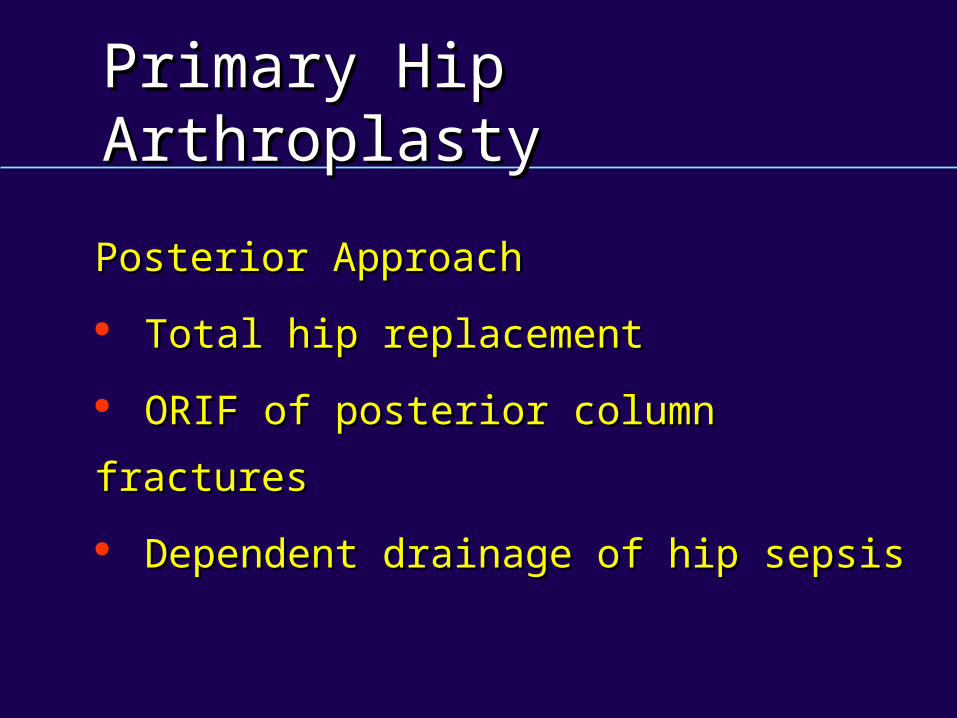
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Posterior ApproachPosterior Approach
Total hip replacementTotal hip replacement
ORIF of posterior column fracturesORIF of posterior column fractures
Dependent drainage of hip sepsisDependent drainage of hip sepsis
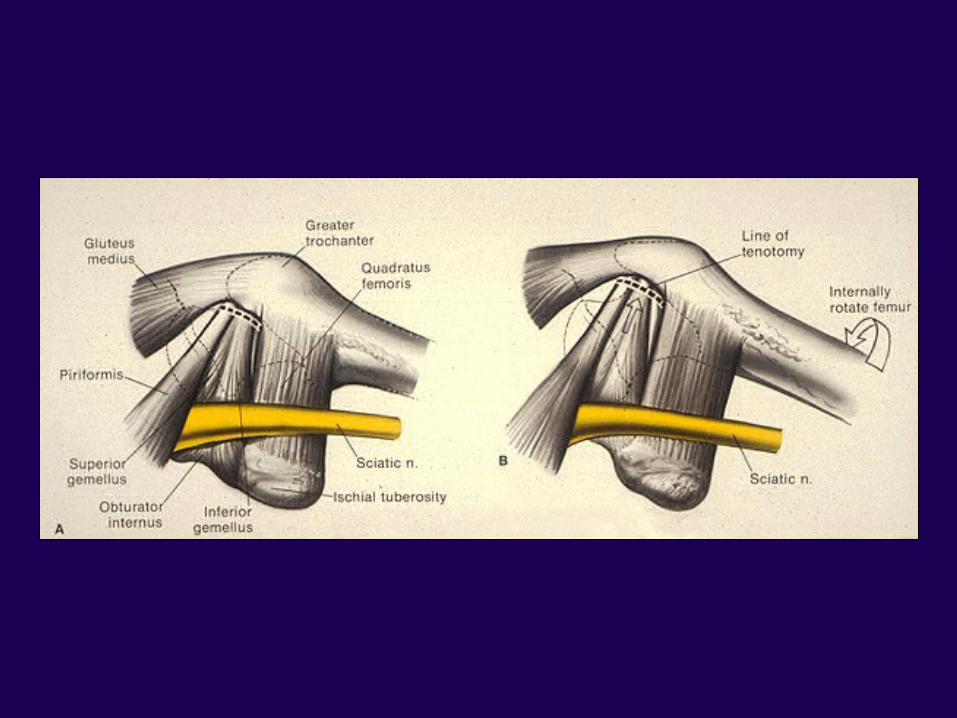
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Posterior ApproachPosterior Approach
Sciatic NerveSciatic Nerve Inferior gluteal arteryInferior gluteal artery
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Design FeaturesDesign Features SizeSize ShapeShape Device configurationDevice configuration Material / physical propertiesMaterial / physical properties
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Resist Composite FailureResist Composite Failure Prosthetic DeviceProsthetic Device Bone CementBone Cement Cancellous BoneCancellous Bone Cortical BoneCortical Bone
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Design Features Design Features Femoral HeadFemoral Head NeckNeck StemStem Collar Collar AcetabulumAcetabulum
Primary Hip ArthroplastyPrimary Hip Arthroplasty
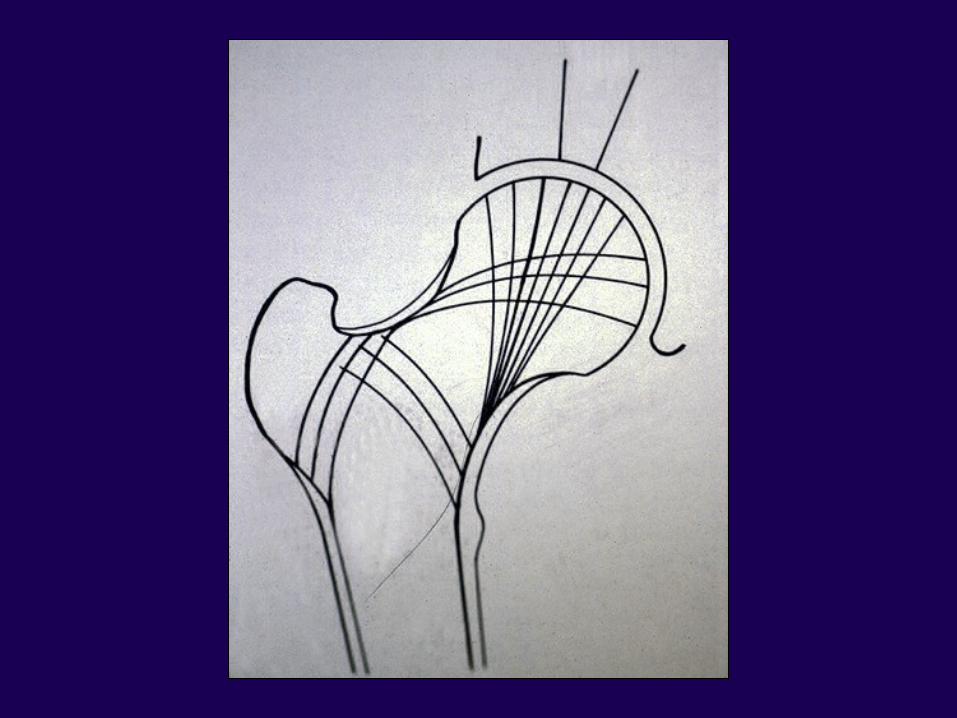
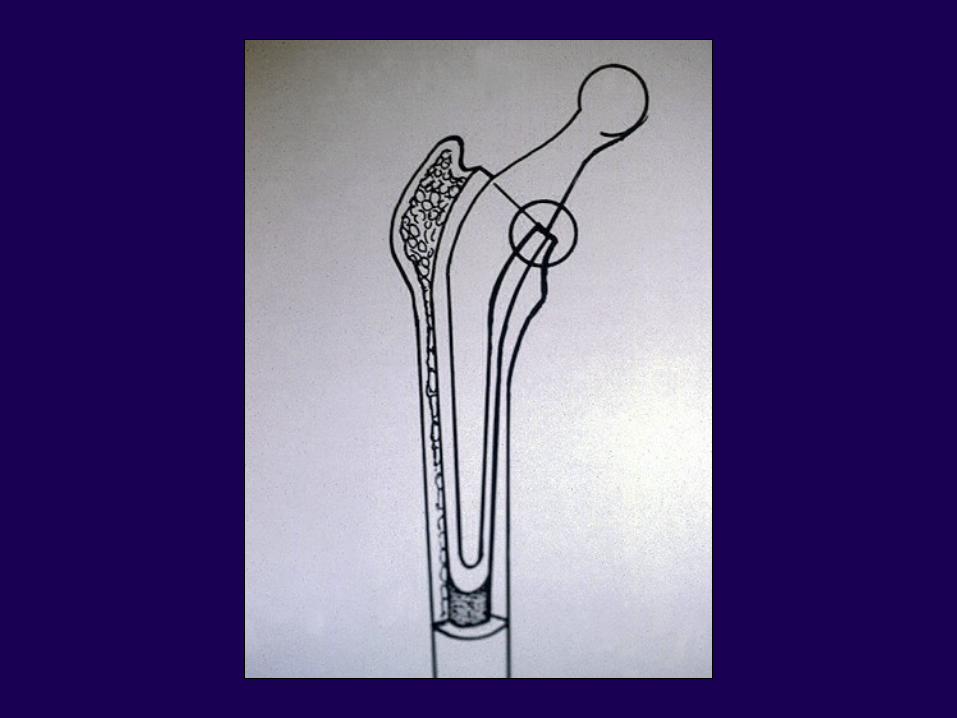
Prosthetic Hip LoadingProsthetic Hip Loading Changes from externally Changes from externally
loaded system to an internally loaded system to an internally loaded systemloaded system
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Femoral Head DesignFemoral Head Design
Articulating finishArticulating finish
Head diameterHead diameter
DDESIGNESIGN
FFEATURESEATURES
Primary Hip ArthroplastyPrimary Hip Arthroplasty
32 mm Head Size32 mm Head Size Greater acetabular looseningGreater acetabular loosening Greatest volumetric wearGreatest volumetric wear
Ritter COOR ‘76Ritter COOR ‘76Morrey Morrey JBJSJBJS ‘89 ‘89

Design FeaturesDesign Features22mm Head Size22mm Head Size
Greatest linear wearGreatest linear wear
Greatest acetabular Greatest acetabular penetrationpenetration
MorreyMorreyJBJSJBJS 1989 1989
Design FeaturesDesign Features
Charnley 22mm head diameterCharnley 22mm head diameter
Compromise friction / wearCompromise friction / wear
Design FeaturesDesign Features28 mm Head Size28 mm Head Size
Stable as 32mm head sizeStable as 32mm head size
Less torque than the 32mm headLess torque than the 32mm head
More favorable direct stress More favorable direct stress transmission patternstransmission patterns
Primary Hip ArthroplastyPrimary Hip Arthroplasty
28 mm Head Size28 mm Head Size
•• CompromiseCompromise
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Design Features Design Features Femoral Neck GeometryFemoral Neck Geometry Neck stem angle – 135ºNeck stem angle – 135º Neck stem offsetNeck stem offset
– – large offset . . . large offset . . . Bending momentBending moment
– – small offset . . . small offset . . . Decreases moment Decreases moment armarm

Primary Hip ArthroplastyPrimary Hip Arthroplasty
Design FeaturesDesign Features
Femoral StemFemoral Stem
– – LengthLength
– – ShapeShape
– – Material propertiesMaterial properties
– – Surface finishSurface finish
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Femoral Stem DesignFemoral Stem Design Cross sectional geometryCross sectional geometry Defines strength / stiffnessDefines strength / stiffness Avoid sharp cornersAvoid sharp corners
Primary Hip ArthroplastyPrimary Hip Arthroplasty
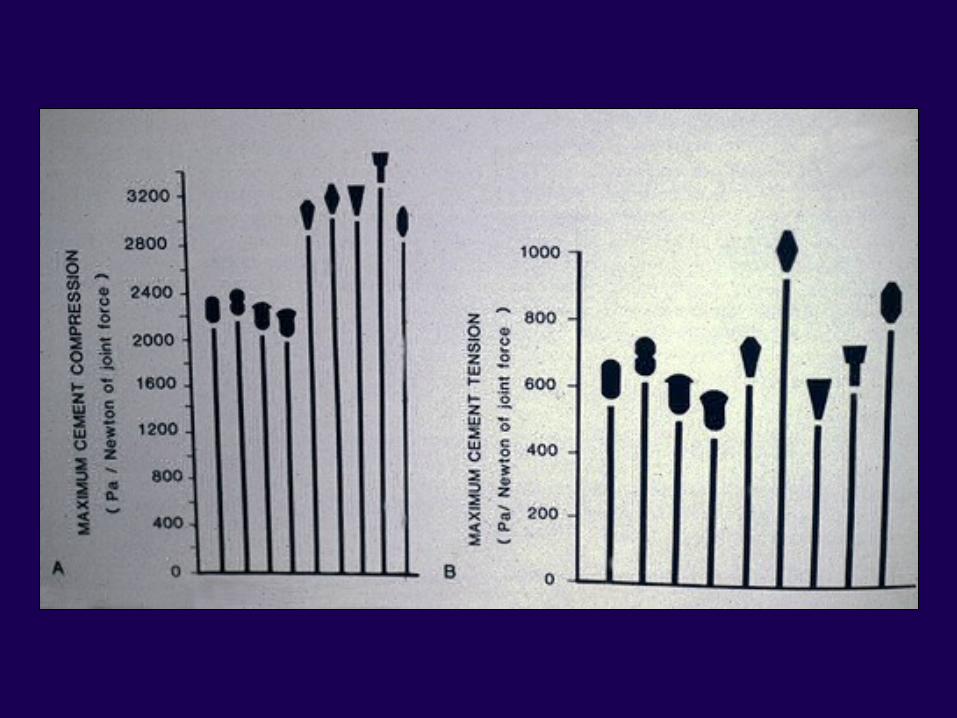
Femoral Stem DesignFemoral Stem Design Large lateral volumeLarge lateral volume Less tensile stress in the mantle Less tensile stress in the mantle
laterallylaterally Large medial volume less tensile Large medial volume less tensile
stressstress
Primary Hip ArthroplastyPrimary Hip Arthroplasty
CollarCollar
Primary role for optimal load transfer Primary role for optimal load transfer to proximal femurto proximal femur
Crowninshield Crowninshield JBJSJBJS ‘80 ‘80Andriacchi Andriacchi JBJSJBJS ‘76 ‘76
Primary Hip ArthroplastyPrimary Hip Arthroplasty
CollarCollar Reduces adaptive bone Reduces adaptive bone
resorptionresorption Reduce bending stress in the Reduce bending stress in the
componentcomponent Reduce stress in the distal Reduce stress in the distal
cementcement
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Fixation FeaturesFixation Features
PMMAPMMA
Weak linkWeak link
Poor fracture toughnessPoor fracture toughness
Low tensile and fatigue strengthLow tensile and fatigue strength
Elastic modulus 1/3 lower than Elastic modulus 1/3 lower than cortical bonecortical bone
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Fixation FeaturesFixation FeaturesPMMA ImprovementsPMMA Improvements
Carbon FibersCarbon Fibers Decreased cement Decreased cement intrusion / increased intrusion / increased viscosityviscosity
Low ViscosityLow Viscosity Lower fatigue strengthLower fatigue strength
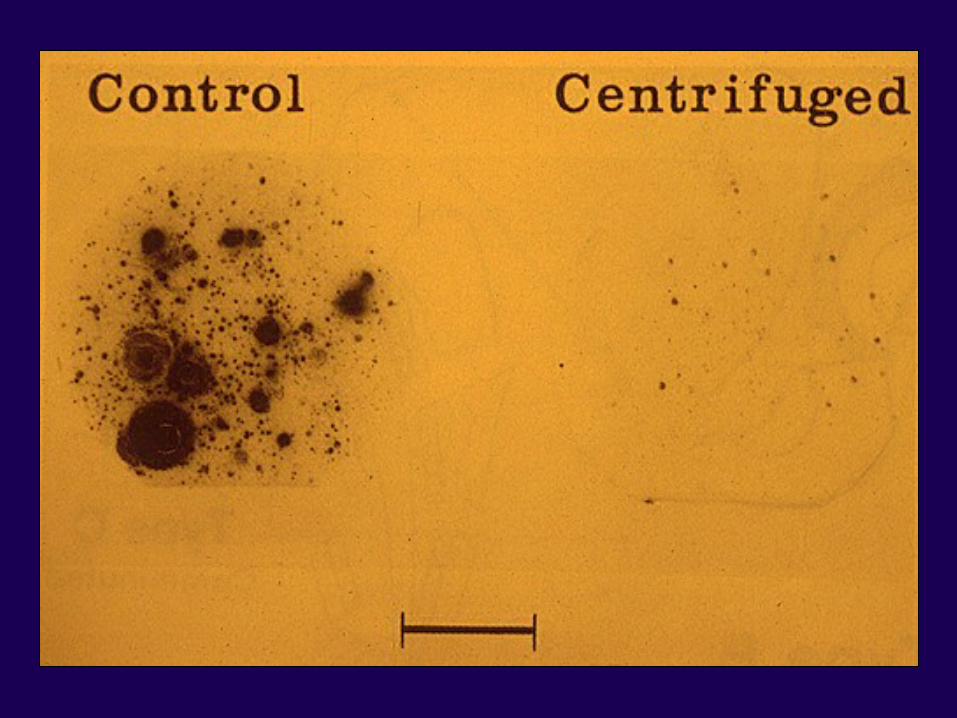
CentrifugationCentrifugation Improved tensile and Improved tensile and fatigue strengthfatigue strength
PMMA ImprovementsPMMA Improvements
CentrifugationCentrifugation 30 sec / 4000 rpm30 sec / 4000 rpm
VacuumVacuum
Burke Burke JBJSJBJS ‘84 ‘84Chin/Stauffer Chin/Stauffer JBJSJBJS ‘90 ‘90
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Material PropertiesMaterial Properties
Stainless SteelStainless Steel —— high elastic modulus / high elastic modulus / low fatigue strengthlow fatigue strength
Cobalt ChromeCobalt Chrome —— highest elastic modulus highest elastic modulus / / better yield / fatigue better yield / fatigue
strengthstrength
TitaniumTitanium —— lower elastic modulus / lower elastic modulus / less stiffnessless stiffness
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Acetabulum DesignAcetabulum Design Metal backedMetal backed All polyethyleneAll polyethylene
Primary Hip ArthroplastyPrimary Hip ArthroplastyCement Fixation :Cement Fixation :
The Femoral SideThe Femoral Side
Results directly related to Results directly related to Surgical TechniquesSurgical Techniques
Primary Hip ArthroplastyPrimary Hip Arthroplasty
Metal BackedMetal Backed
Increased linear and volumetric Increased linear and volumetric wearwear
Increased radiolucency, loosening, Increased radiolucency, loosening, revisionrevision
No series of documented superior No series of documented superior resultsresults
Improved Longevity – Improved Longevity – Femoral SideFemoral Side
Improved Longevity – Improved Longevity – femoral sidefemoral side Plug canalPlug canal Retrograde fillRetrograde fill Avoid varus / valgus > 5ºAvoid varus / valgus > 5º
MulroyMulroyJBJSJBJS ‘95 ‘95
Primary Hip ArthroplastyPrimary Hip Arthroplasty
AA White-OutWhite-Out
BB Complete DistributionComplete Distribution
CC11 Extensive Radiolucent LineExtensive Radiolucent Line
CC22 Thin mantle < 1 mmThin mantle < 1 mm
DD Gross deficienciesGross deficiencies
GradeGrade Radiographic AppearanceRadiographic Appearance
Primary Total HipPrimary Total Hip
1st Generation Cement Technique1st Generation Cement Technique
– – Finger Packing Finger Packing – No pressurization– No pressurization
– – No Canal PrepNo Canal Prep – Cast stem– Cast stem
– – No PlugNo Plug – Narrow med border– Narrow med border
– – No GunNo Gun – Sharp edges– Sharp edges
WH HarrisWH Harris

Primary Hip ArthroplastyPrimary Hip ArthroplastyCement TechniquesCement Techniques
Probable Improved LongevityProbable Improved Longevity
Femoral SideFemoral Side PressurizePressurize CentralizeCentralize Continuous Cement MantleContinuous Cement Mantle
HarrisHarrisCOOR ‘97COOR ‘97
Cemented Long TermCemented Long Term
Primary Total HipPrimary Total Hip22ndnd Generation Cement Generation Cement
William HarrisWilliam Harris Began 1975Began 1975
Gun 71 Gun 71 – – Super alloySuper alloy
Jet lavageJet lavage –– Broad Broad && round round medial bordermedial border
Canal PrepCanal Prep
Cement RestrictionCement Restriction
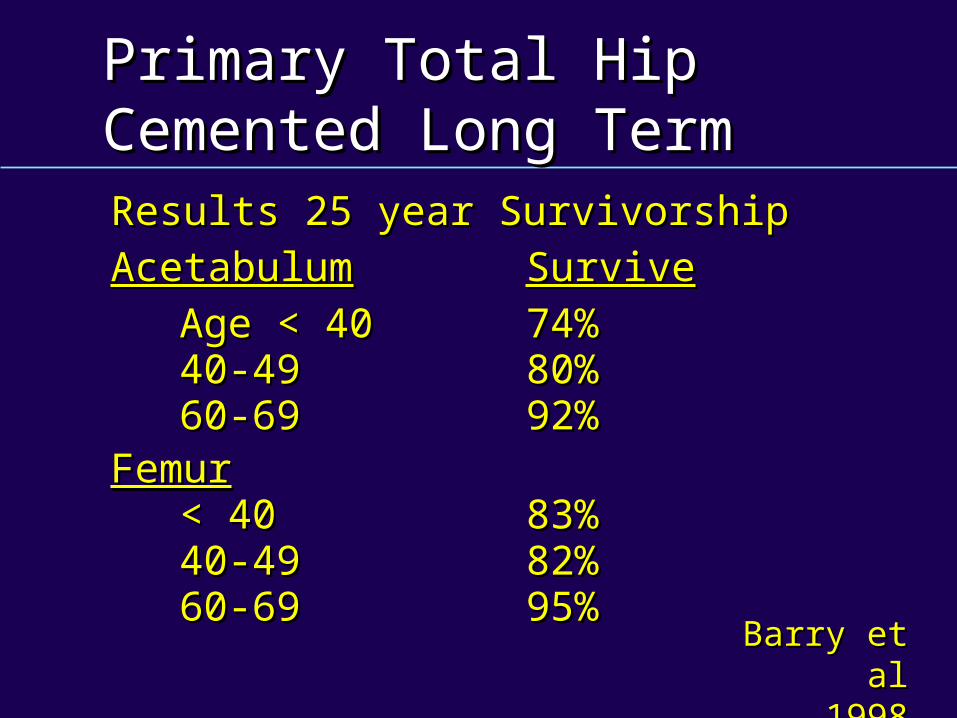
Primary Total HipPrimary Total HipCemented Long TermCemented Long TermResults 25 year SurvivorshipResults 25 year Survivorship
AcetabulumAcetabulum SurviveSurvive
Age < 40Age < 40 74%74% 40-4940-49 80%80% 60-6960-69 92%92%FemurFemur < 40< 40 83%83% 40-4940-49 82%82% 60-6960-69 95%95% Barry et alBarry et al
19981998
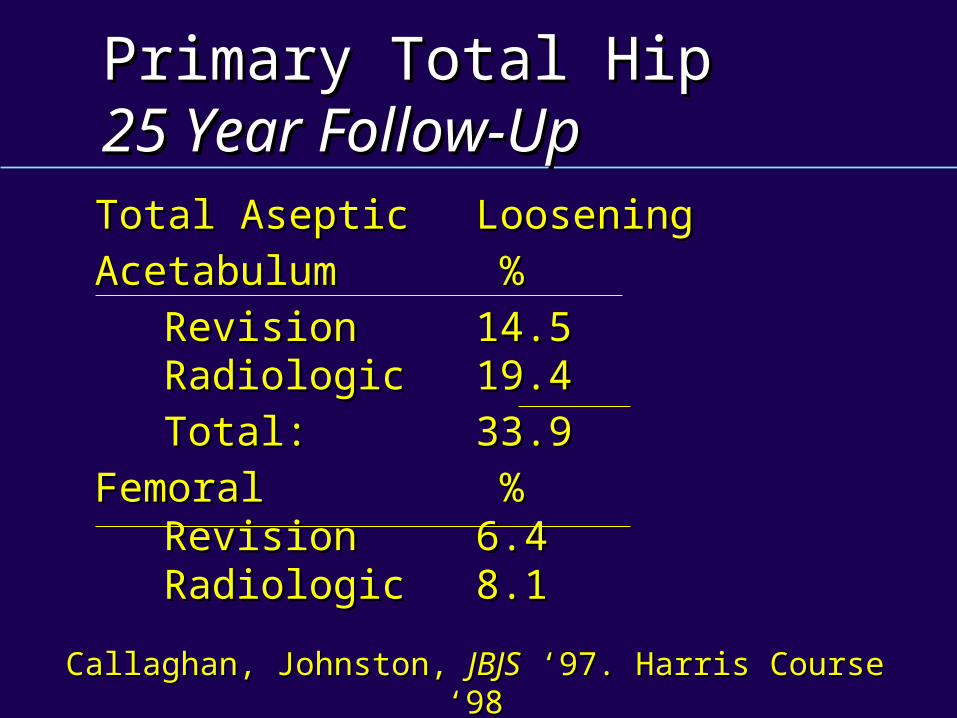
Primary Total HipPrimary Total Hip25 Year Follow-Up25 Year Follow-UpTotal Aseptic Total Aseptic LooseningLoosening
AcetabulumAcetabulum % %
RevisionRevision 14.514.5 RadiologicRadiologic 19.419.4
Total: Total: 33.933.9
FemoralFemoral % % RevisionRevision 6.46.4 RadiologicRadiologic 8.18.1
Callaghan, Johnston, Callaghan, Johnston, JBJSJBJS ‘97. Harris Course ‘98 ‘97. Harris Course ‘98
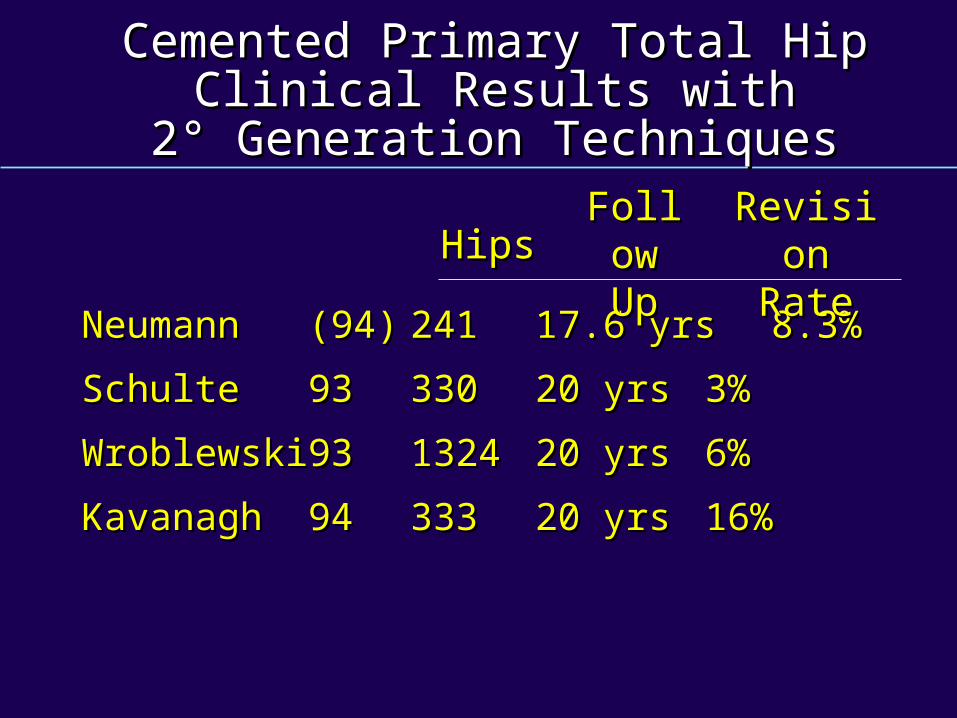
Cemented Primary Total HipCemented Primary Total HipClinical Results withClinical Results with
2° Generation Techniques2° Generation Techniques
Neumann Neumann (94)(94) 241241 17.6 yrs17.6 yrs 8.3%8.3%
SchulteSchulte 9393 330330 20 yrs20 yrs 3%3%
WroblewskiWroblewski 9393 13241324 20 yrs20 yrs 6%6%
KavanaghKavanagh 9494 333333 20 yrs20 yrs 16%16%
HipsHipsRevisionRevision
RateRateFollowFollow
UpUp
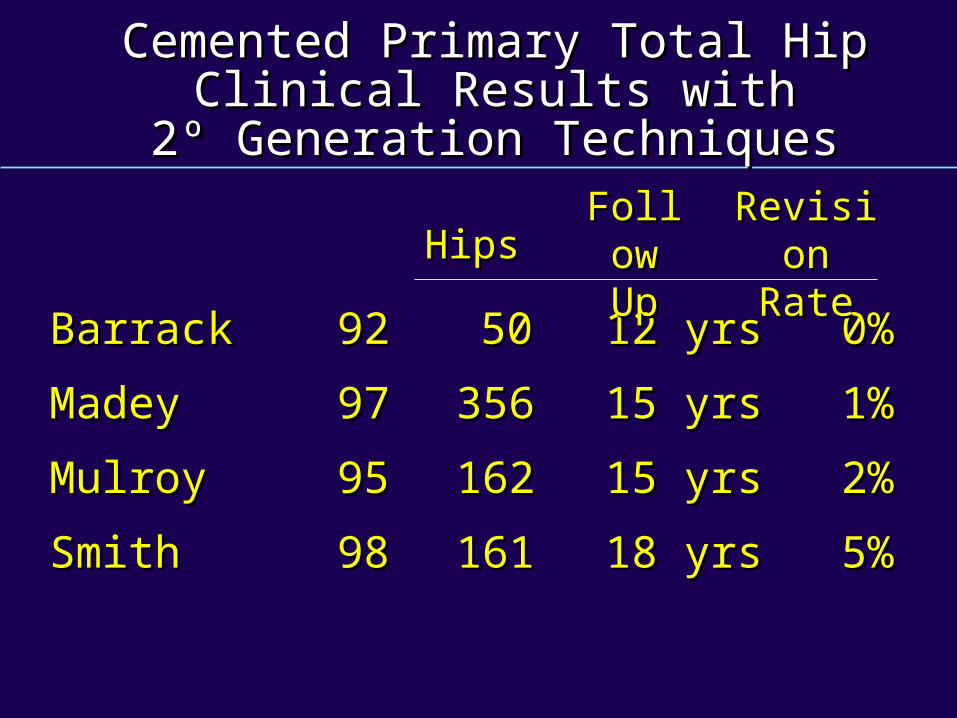
Cemented Primary Total HipCemented Primary Total HipClinical Results withClinical Results with
2º Generation Techniques2º Generation Techniques
Barrack Barrack 9292 5050 12 yrs12 yrs 0% 0%
MadeyMadey 9797 356356 15 yrs15 yrs 1% 1%
MulroyMulroy 9595 162162 15 yrs15 yrs 2% 2%
SmithSmith 9898 161161 18 yrs18 yrs 5% 5%
HipsHipsRevisionRevision
RateRateFollowFollow
UpUp
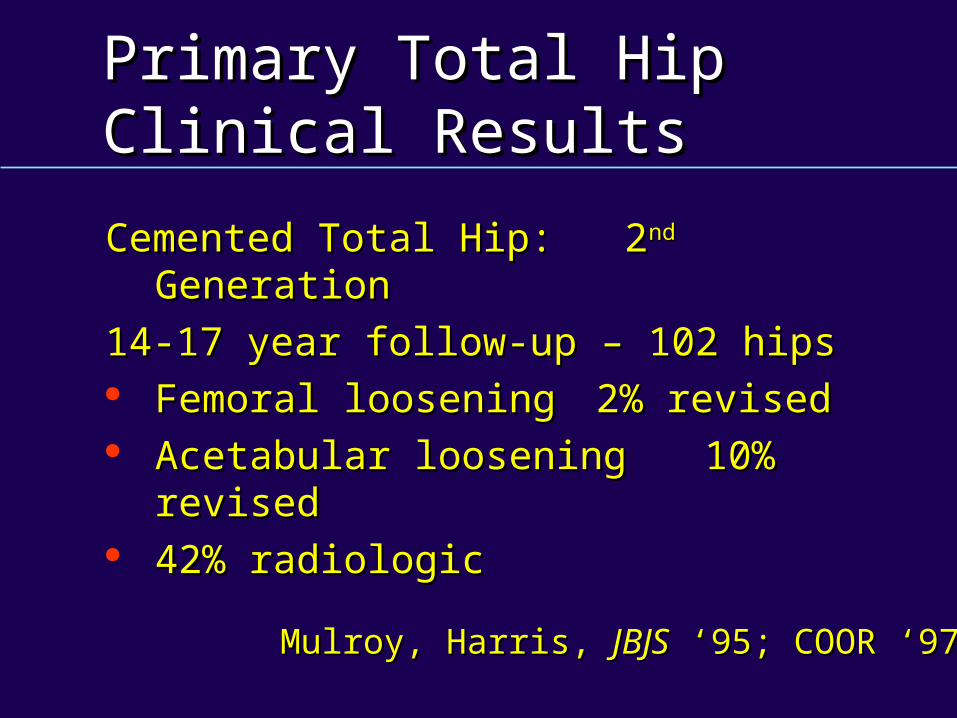
Primary Total HipPrimary Total HipClinical ResultsClinical Results
Cemented Total Hip: 2Cemented Total Hip: 2ndnd Generation Generation
14-17 year follow-up – 102 hips14-17 year follow-up – 102 hips Femoral looseningFemoral loosening 2% revised2% revised Acetabular looseningAcetabular loosening 10% revised10% revised 42% radiologic42% radiologic
Mulroy, Harris, Mulroy, Harris, JBJSJBJS ‘95; COOR ‘97 ‘95; COOR ‘97
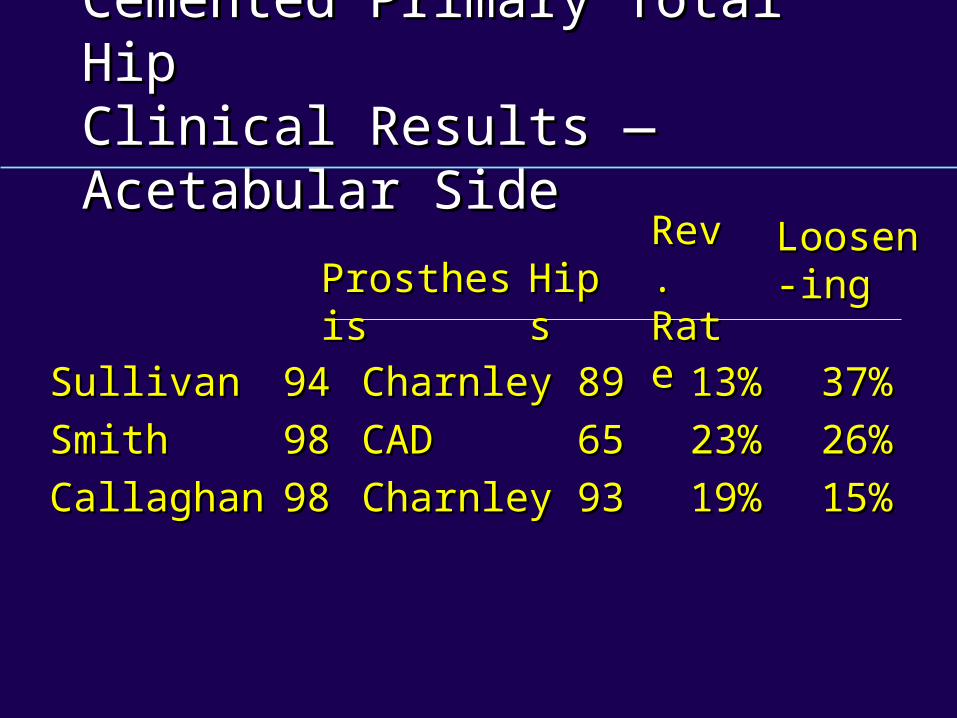
Cemented Primary Total HipCemented Primary Total HipClinical Results — Acetabular SideClinical Results — Acetabular Side
SullivanSullivan 9494 CharnleyCharnley 8989 13%13% 37%37%
SmithSmith 9898 CADCAD 6565 23%23% 26%26%
CallaghanCallaghan 9898 CharnleyCharnley 9393 19%19% 15%15%
ProsthesisProsthesis HipsHipsRev.Rev.RateRate
Loosen-Loosen-inging
Primary Total HipPrimary Total Hip33rdrd Generation Cement Technique Generation Cement Technique
Bill Harris – Began 1982Bill Harris – Began 1982 Porosity reductionPorosity reduction Rough surfaceRough surface CentralizationCentralization PressurizationPressurization Pre-coatPre-coat
Primary Total HipPrimary Total Hip
Plug and retrograde fillPlug and retrograde fill Avoid excessive varus/valgusAvoid excessive varus/valgus Strive for 3-5 mm prox/med > 2mm Strive for 3-5 mm prox/med > 2mm
distaldistal Do not ream / remove good Do not ream / remove good
cancellous bonecancellous bone
Conclusions — CementedConclusions — Cemented
Primary Total HipPrimary Total HipClinical ResultsClinical Results
Hybrid ConstructHybrid Construct
Galante -Galante - 95 f/u 5 years95 f/u 5 years Femoral Femoral 2% 2% rad looserad loose Acetabulum Acetabulum 2% 2% rad looserad loose
Woolson -Woolson - 96 f/u 6 years96 f/u 6 years Femoral Femoral 5%5% revisionrevision Acetabulum Acetabulum 0% 0% revisionrevision
Design FeaturesDesign Features
POROUS IMPLANTPOROUS IMPLANT
Uncemented THAUncemented THA
DefinitionDefinition
Press FitPress Fit
MacrointerlockMacrointerlock
MicrointerlockMicrointerlock
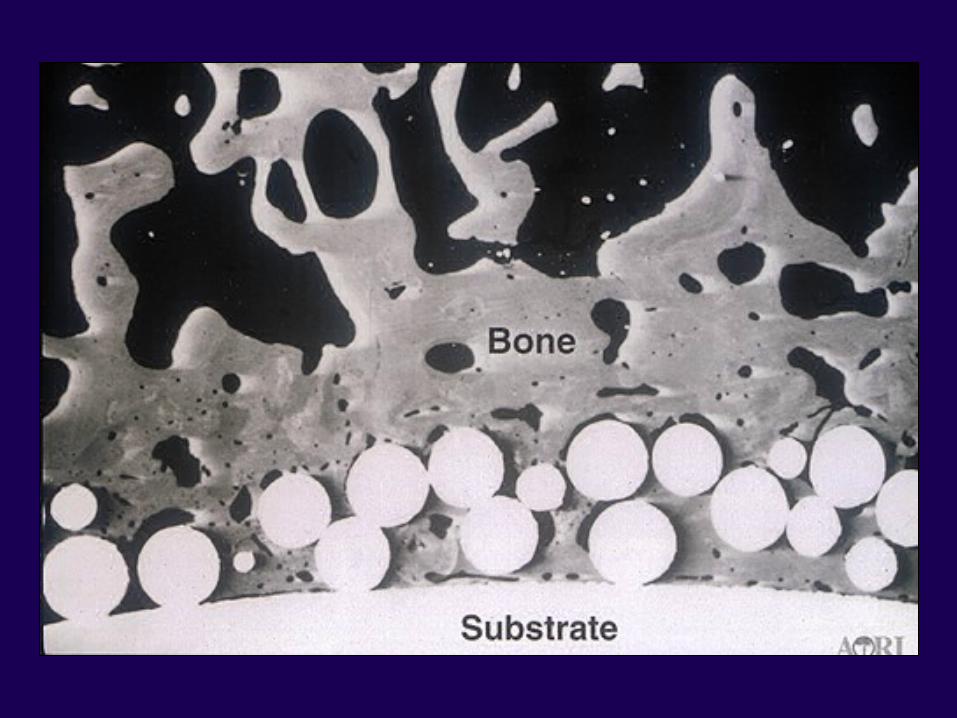
Design FeaturesDesign Features
Pore Size — Animal StudiesPore Size — Animal Studies
50 to 400 µm50 to 400 µm Optimal bone ingrowthOptimal bone ingrowth
Bobyn: Bobyn: Clinical OrthopedicsClinical Orthopedics; 1980; 1980Engh: Engh: JBJSJBJS; 1987; 1987Collier: Collier: Clinical OrthopedicsClinical Orthopedics; 1988; 1988
MicromotionMicromotion
40 Micron Motion Bone Ingrowth40 Micron Motion Bone Ingrowth ((JBJSJBJS 79-A) 79-A)
150 Micron Motion Fibrous Ingrowth150 Micron Motion Fibrous Ingrowth (CORR, 208)(CORR, 208)
Design Criteria –Design Criteria –Long Term Implant StabilityLong Term Implant Stability
Initial Implant StabilityInitial Implant Stability Implant micromotion < 50 mm Implant micromotion < 50 mm
of displacementof displacement Level of implant coatingLevel of implant coating Type of coatingType of coating
Kienapfel H.Kienapfel H.J. ArthroplastyJ. Arthroplasty 1999 1999
Design CriteriaDesign Criteria
Uncemented Total Hip ArthroplastyUncemented Total Hip Arthroplasty
Key —Key — Resistance to Rotation Resistance to Rotation Around the Long AxisAround the Long Axis
Design CriteriaDesign Criteria
Uncemented Total Hip Uncemented Total Hip ArthroplastyArthroplasty Resist translation in 3 planesResist translation in 3 planes
— AxialAxial
— Medial Medial - - laterallateral
— Anterior - Anterior - posteriorposterior
Design Criteria –Design Criteria –Uncemented ImplantsUncemented Implants
Level of Implant CoatingLevel of Implant Coating
— Apply circumferentialApply circumferential
— Avoid patch porous coatsAvoid patch porous coats
— Smooth surface – high failure Smooth surface – high failure raterate
Design Criteria –Design Criteria –Uncemented ImplantsUncemented Implants
Type of CoatingType of Coating
1. 1. Macro-texturing — doesn’t workMacro-texturing — doesn’t work
2. 2. Roughened titaniumRoughened titanium
3. 3. Porous coating made of CoCr or TiPorous coating made of CoCr or Ti
4. 4. Ti wire meshTi wire mesh
5. 5. Plasma-sprayed TiPlasma-sprayed Ti
6. 6. Bioactives —Bioactives — Hydroxyapatite / Hydroxyapatite / tricalcium phosphatetricalcium phosphate
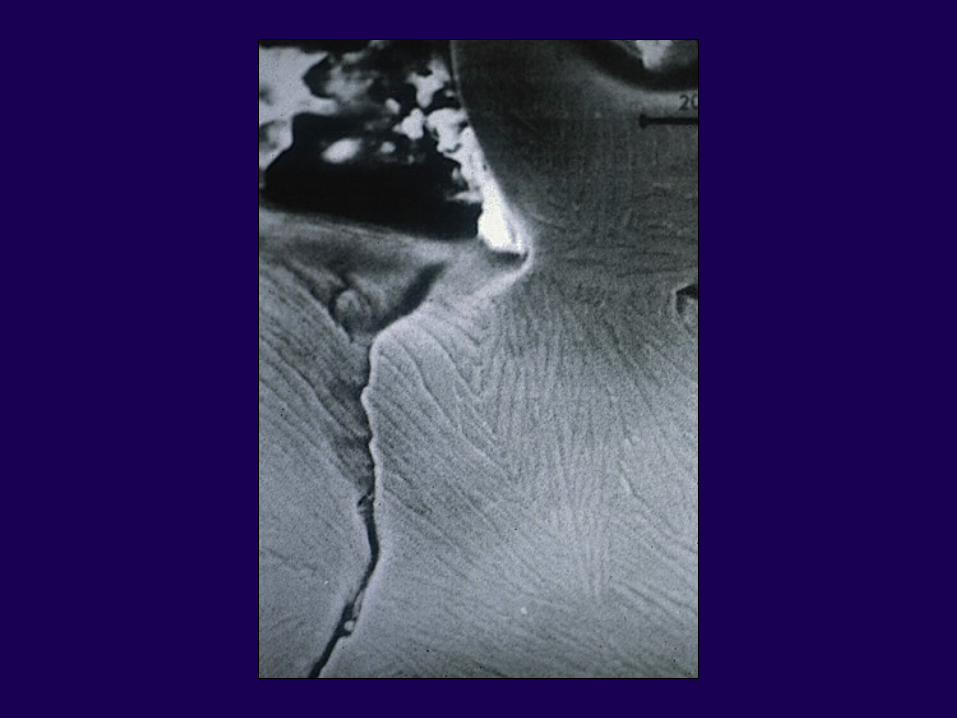
Design FeaturesDesign Features
Sintered Micro/Macro BeadsSintered Micro/Macro BeadsCr-Co-Mo/TiCr-Co-Mo/Ti
Pore dimensions 100 to 400 Pore dimensions 100 to 400 mm
AML ; PCAAML ; PCA
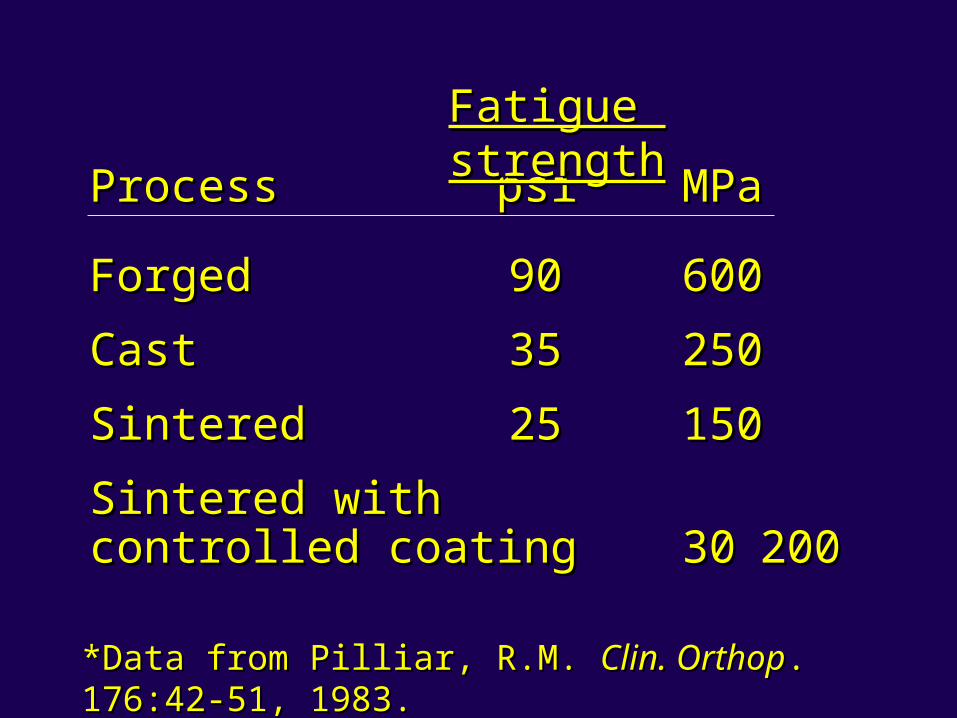
ForgedForged 9090 600600
CastCast 3535 250250
SinteredSintered 2525 150150
Sintered withSintered withcontrolled coatingcontrolled coating 3030 200200
ProcessProcess psipsi MPaMPa
Fatigue strengthFatigue strength
*Data from Pilliar, R.M. *Data from Pilliar, R.M. Clin. OrthopClin. Orthop. 176:42-51, 1983.. 176:42-51, 1983.
Design Criteria –Design Criteria –Uncemented ImplantsUncemented Implants
Implant Geometry – Implant StabilityImplant Geometry – Implant Stability
1) 1) Wedge-shaped metaphyseal fillingWedge-shaped metaphyseal filling
2) 2) Single wedge-shaped implantsSingle wedge-shaped implants
3) 3) Tapered stemsTapered stems
4) 4) Diaphyseal fixation — cylindrical Diaphyseal fixation — cylindrical or or fluted stemsfluted stems
Design CriteriaDesign Criteria
Uncemented ImplantsUncemented Implants Requires cortical fixationRequires cortical fixation
— MetaphysisMetaphysis
— Metaphysis – DiaphysisMetaphysis – Diaphysis
— DiaphysealDiaphyseal
Design Criteria –Design Criteria –Uncemented ImplantsUncemented Implants
Bioactives — OsteoconductiveBioactives — Osteoconductive Tricalcium dissolves more rapidly Tricalcium dissolves more rapidly
than hydroxyapatitethan hydroxyapatite Thickness 50 mmThickness 50 mm More crystalline hydroxyapatite More crystalline hydroxyapatite
slows resorptionslows resorption

Uncemented Primary Total HipUncemented Primary Total HipClinical Results Clinical Results •• Femoral Side Femoral Side
— — Titanium = Cobalt ChromeTitanium = Cobalt Chrome
— — Cobalt Chrome increased stress- Cobalt Chrome increased stress- shielding shielding
— — Straight Stems with varying degrees Straight Stems with varying degrees of medullary fill often used of medullary fill often used
— — Anatomic Stems have not been a Anatomic Stems have not been a great advantage great advantage
Design FeaturesDesign Features
Straight StemStraight Stem
An Anatomic StemAn Anatomic Stem
Design FeaturesDesign Features
Proximal CoatingProximal Coating
Design FeaturesDesign Features
Proximal coating – Anatomic designProximal coating – Anatomic design
Maximum fit in certain priority areasMaximum fit in certain priority areas
Maximal load transferMaximal load transfer
Resist axial loading and torsional Resist axial loading and torsional loadsloads
Poss: ClinicPoss: Clinic

Design FeaturesDesign Features
Both greater distal motion at Both greater distal motion at interface —interface —
Compared with proximal motionCompared with proximal motion
Callaghan, Callaghan, JBJSJBJS ‘92 ‘92
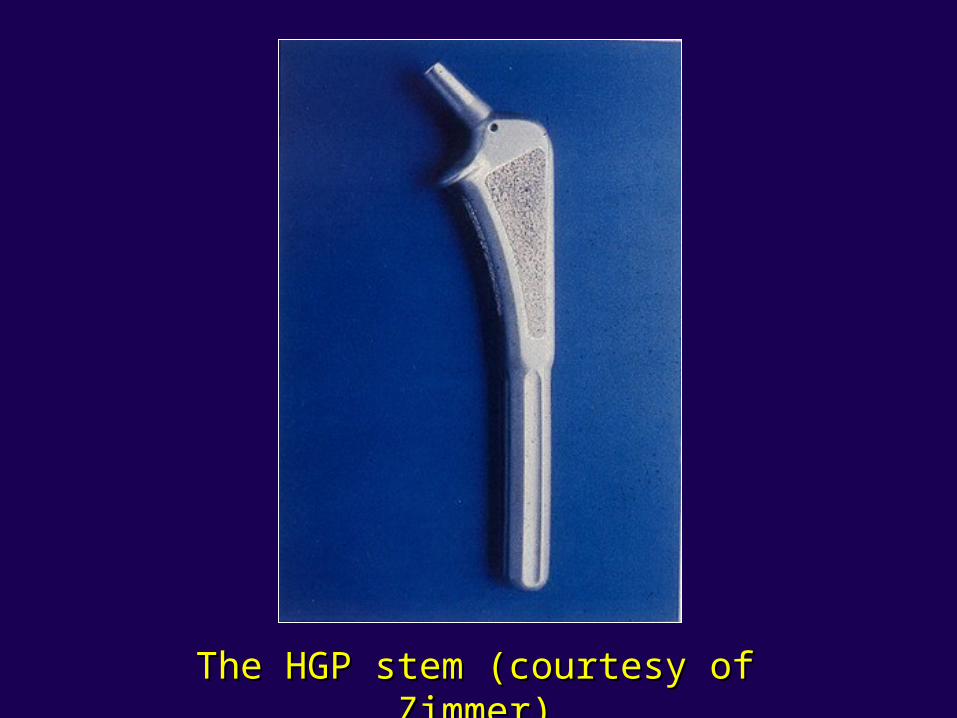
The HGP stem (courtesy of Zimmer)The HGP stem (courtesy of Zimmer)
Design FeaturesDesign Features
Porous ImplantPorous Implant
Proximal coatingProximal coatingFully coatedFully coated
Design Features — Design Features — Porous SurfacePorous Surface
2/3 or fully coated2/3 or fully coated
2 to 4 x increase in bone 2 to 4 x increase in bone resorptionresorption
Engh: Engh: Clinical OrthopedicsClinical Orthopedics; 1988; 1988
Design FeaturesDesign Features
Fully Coated Porous SurfaceFully Coated Porous Surface
Transfers stress distally under Transfers stress distally under axial load –axial load –
Engh: Engh: Clinical OrthopedicsClinical Orthopedics; 1988; 1988
Proximal bone resorptionProximal bone resorption
Retrieval StudiesRetrieval Studies
EnghEngh
Femur Femur 57% 57% ingrowthingrowth
Acetabulum Acetabulum 32% 32% ingrowthingrowth
Radiographic Criteria for Radiographic Criteria for Bone IngrowthBone Ingrowth
Engh et al, (CORR 257)Engh et al, (CORR 257)
Absence of Reactive LinesAbsence of Reactive Lines
Spot Welds Endosteal BoneSpot Welds Endosteal Bone
Implant Instability 2 mmImplant Instability 2 mm
PedestalPedestal
Calcar Atrophy / Stress ShieldingCalcar Atrophy / Stress Shielding
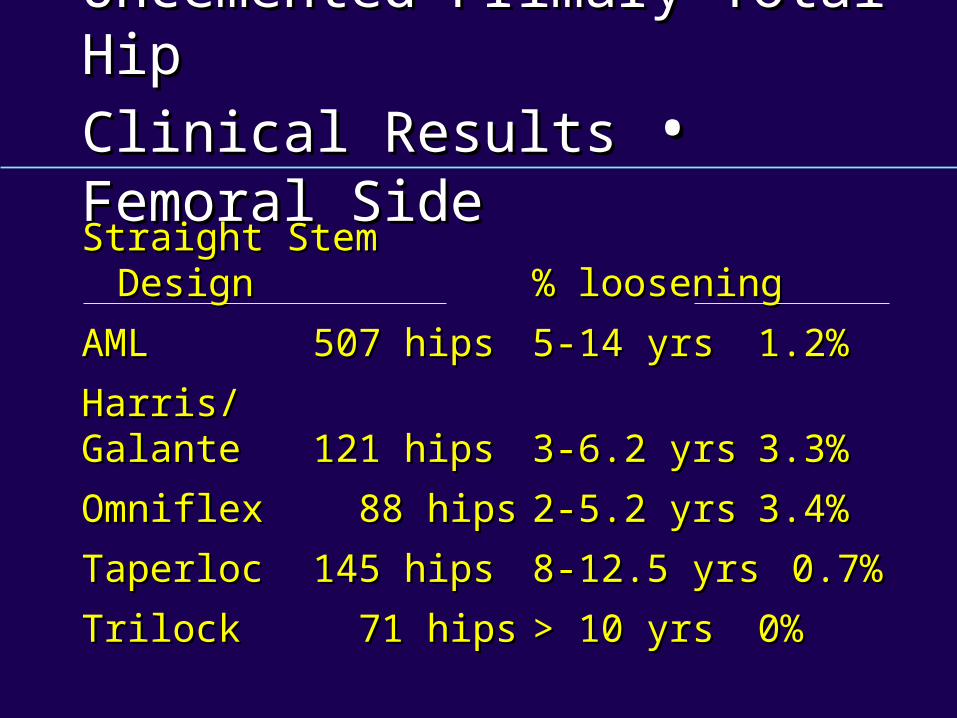
Uncemented Primary Total HipUncemented Primary Total Hip
Clinical ResultsClinical Results •• Femoral SideFemoral Side
Straight StemStraight StemDesign Design % loosening% loosening
AMLAML 507 hips507 hips 5-5- 14 yrs14 yrs 1.2%1.2%
Harris/ Harris/ GalanteGalante 121 hips121 hips 3-3- 6.2 yrs6.2 yrs 3.3%3.3%
OmniflexOmniflex 88 hips 88 hips 2-2- 5.2 yrs5.2 yrs 3.4%3.4%
TaperlocTaperloc 145 hips145 hips 8-8- 12.5 yrs12.5 yrs 0.7%0.7%
TrilockTrilock 71 hips 71 hips > > 10 yrs10 yrs 0%0%
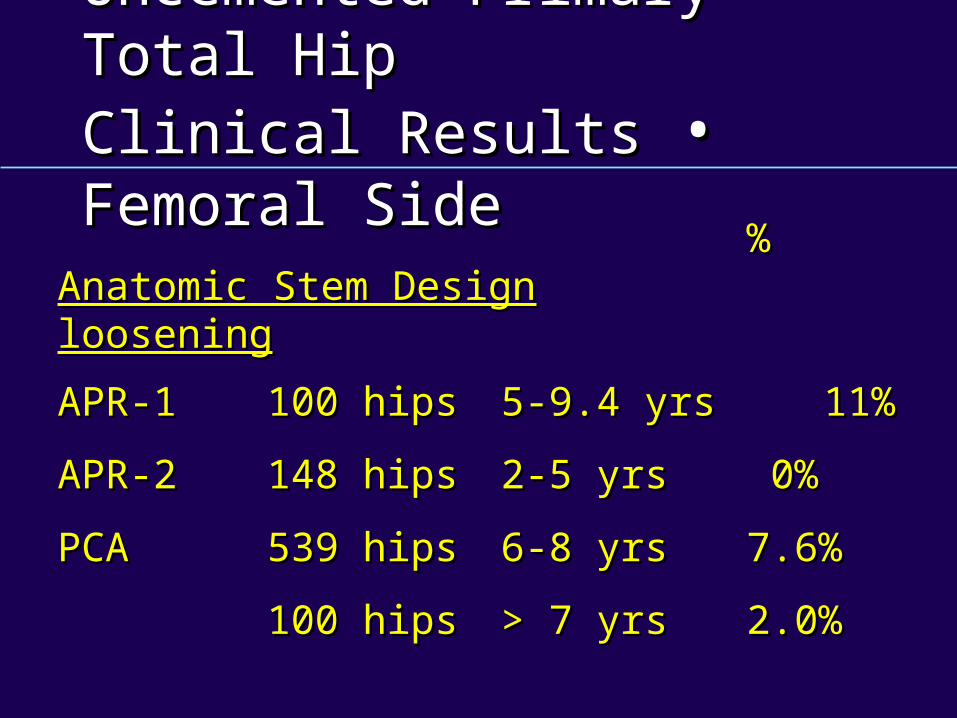
Uncemented Primary Total HipUncemented Primary Total HipClinical Results Clinical Results •• Femoral Side Femoral Side
% % Anatomic Stem DesignAnatomic Stem Design looseningloosening
APR-1APR-1 100 hips100 hips 5-9.4 yrs5-9.4 yrs 11%11%
APR-2APR-2 148 hips148 hips 2-5 yrs2-5 yrs 0% 0%
PCAPCA 539 hips539 hips 6-8 yrs6-8 yrs 7.6%7.6%
100 hips100 hips > 7 yrs> 7 yrs 2.0%2.0%
Screw FixationScrew Fixation
Less Micromotion, Better IngrowthLess Micromotion, Better Ingrowth
Conduit for Particulate DebrisConduit for Particulate Debris
Neurovascular InjuryNeurovascular Injury
Acetabular DesignAcetabular Design
HemisphereHemisphere
Screw FixationScrew Fixation
Locking MechanismLocking Mechanism
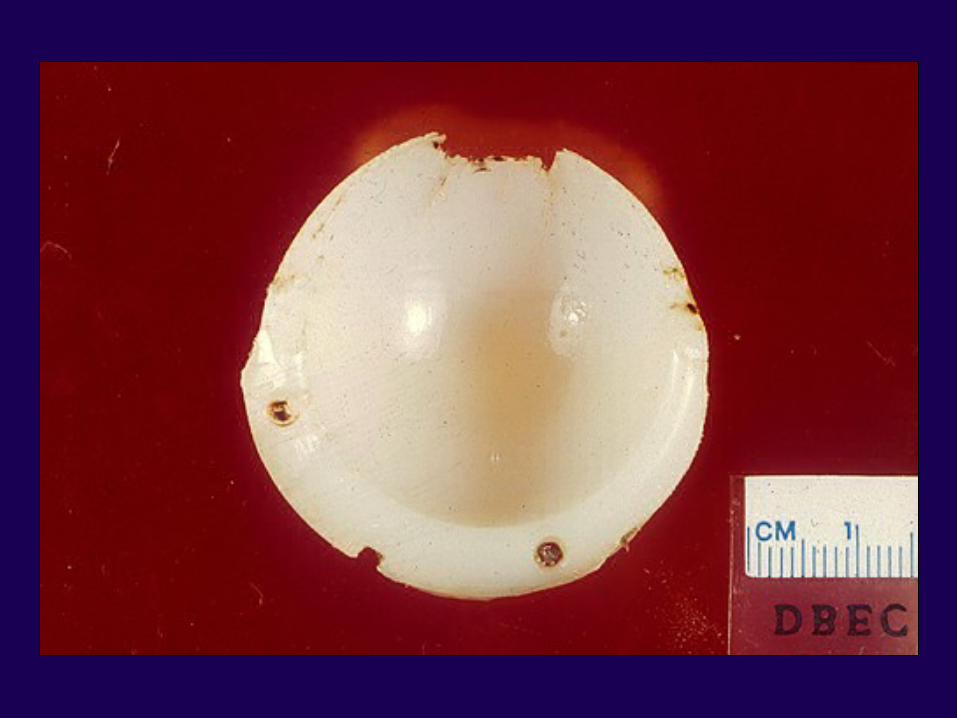
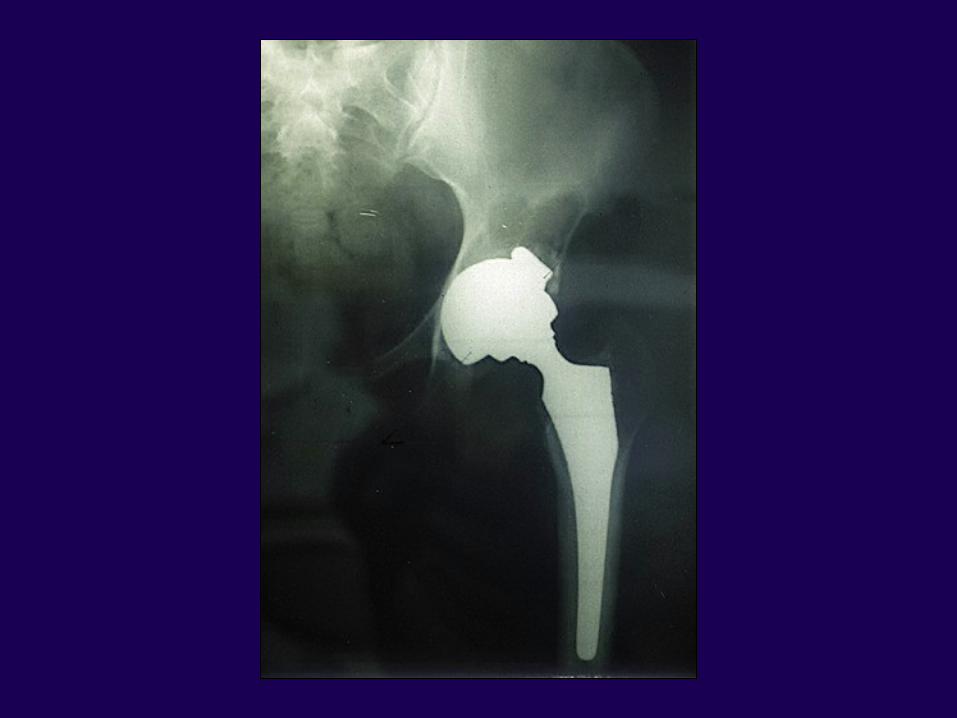
Uncemented Primary Total HipUncemented Primary Total Hip— Main Recurrent Concern— Main Recurrent Concern
Poly Wear – OsteolysisPoly Wear – Osteolysis
Uncemented Primary Total HipUncemented Primary Total HipClinical Results • Acetabular SideClinical Results • Acetabular Side
Femoral head size – Femoral head size – Acetabular Acetabular thicknessthickness
— PCAPCA 26 mm head26 mm head no osteolysisno osteolysis
— PCAPCA 32 mm head32 mm head 26% osteolysis26% osteolysis

Uncemented Primary Total HipUncemented Primary Total HipClinical Results Clinical Results •• Acetabular Side Acetabular Side
% loosening% loosening
ARCARC 72 hips 72 hips 12 yrs12 yrs 1.4%1.4%
Harris/Galante Harris/Galante 136 hips136 hips 5-10 yrs5-10 yrs 0%0%
PSL PSL smooth HA smooth HA 316 hips316 hips 6-10 yrs6-10 yrs 12%12% beaded HA beaded HA 2.7%2.7%
PCAPCA 241 hips241 hips 2-9 yrs2-9 yrs 11%11% 539 hips539 hips 7 yrs 7 yrs 13.2%13.2% 100100 > 7 yrs> 7 yrs 4% rev.4% rev.
Uncemented Primary Total HipUncemented Primary Total HipClinical Results • Acetabular SideClinical Results • Acetabular Side
— — Hemispherical shape — rim fitHemispherical shape — rim fit
— — Under ream No > 2 mmUnder ream No > 2 mm
— — Screws :Screws : produced durableproduced durable results - postopresults - postop
Disadvantage :Disadvantage : posterior sciatic N.posterior sciatic N. Ant supAnt sup – common iliac– common iliac Ant inf Ant inf – obturator art / ner– obturator art / ner
{{
Complications in Total Hip Arthroplasty Complications in Total Hip Arthroplasty – Heterotopic Ossification– Heterotopic Ossification
TreatmentTreatment—Radiation pre-op or post-op 500 Radiation pre-op or post-op 500
to 1000 Rad to 1000 Rad “Remember to shield implant”“Remember to shield implant”
—IndomethacinIndomethacin—IbuprofenIbuprofen—DiphosphonatesDiphosphonates
Complications In Total Hip Arthroplasty – Complications In Total Hip Arthroplasty – Heterotopic Ossification 0.6% to 61.7%Heterotopic Ossification 0.6% to 61.7%
Associated conditionsAssociated conditions
— Ankylosing spondylitisAnkylosing spondylitis
— Forestier’s diseaseForestier’s disease
— Post traumatic arthritisPost traumatic arthritis
— Bilateral male osteophytic Bilateral male osteophytic OAOA
Complications in Total HipComplications in Total HipArthroplasty – DislocationArthroplasty – Dislocation
Component ImpingementComponent Impingement— Proximal femurProximal femur— Femoral head skirtFemoral head skirt— Acetabular component (elevated liner)Acetabular component (elevated liner)— Osteophytes / cement massesOsteophytes / cement masses
Head SizeHead Size— No difference 22 - 28 - 32No difference 22 - 28 - 32— 28 mm head 28 mm head > > 60 mm acetabulum 60 mm acetabulum
—increased rate—increased rate— 22 mm head22 mm head > > 54 mm acetabulum 54 mm acetabulum
—increased rate—increased rate
Complications In Total Hip Complications In Total Hip Arthroplasty – Dislocation – 3%Arthroplasty – Dislocation – 3%
Posterior approach slightly higher 4.6%Posterior approach slightly higher 4.6% Neuromuscular problemsNeuromuscular problems Previous surgery (rate doubles)Previous surgery (rate doubles) MalpositionMalposition
>> 25º anteversion25º anteversion
>> 60º inclination60º inclination
RetroversionRetroversion
>> 15º femoral anteversion15º femoral anteversion
TreatmentTreatment
BracingBracing
Spica castSpica cast
SurgerySurgery
Complications In Total Hip Complications In Total Hip Arthroplasty – DislocationArthroplasty – Dislocation
Occult infectionOccult infection
TraumaTrauma
Profound weight lossProfound weight loss
Complications In Total Hip Complications In Total Hip Arthroplasty – ThromboembolismArthroplasty – Thromboembolism
Most common complicationMost common complication
DVTDVT –– 70%70% to to 8%8%
PE PE –– 1%1% toto 2%2%
Complications In Total Hip Complications In Total Hip Arthroplasty – ThromboembolismArthroplasty – Thromboembolism
Activation of clotting cascadeActivation of clotting cascade
Local vessel injuryLocal vessel injury
Stasis in the femoral veinStasis in the femoral vein
Ultra-High Molecular Weight PolyethyleneUltra-High Molecular Weight Polyethyleneis defined as what type of material ?is defined as what type of material ?
1.1. ElasticElastic
2. 2. Viscoelatic-plasticViscoelatic-plastic
3. 3. RigidRigid
4. 4. Shear thinningShear thinning
5. 5. High frictionHigh friction
The degradation of polyethylene following The degradation of polyethylene following gamma irradiation is related to what factor ?gamma irradiation is related to what factor ?
1.1. Increased ionic bondingIncreased ionic bonding
2.2. Surface ion implantationSurface ion implantation
3.3. Free radical formationFree radical formation
4.4. Decreased covalent cross- Decreased covalent cross- linkinglinking
5.5. Decreased polymer densityDecreased polymer density
Why is cobalt-chrome alloy preferred over Why is cobalt-chrome alloy preferred over a titanium alloy for a cemented femoral a titanium alloy for a cemented femoral component in a total hip arthroplasty ?component in a total hip arthroplasty ?
1.1. Less particulate metal debrisLess particulate metal debris
2.2. Less stiffnessLess stiffness
3.3. Elastic modulus closer to bone cementElastic modulus closer to bone cement
4.4. Cost-effectivenessCost-effectiveness
5.5. Better cement bonding abilityBetter cement bonding ability
What is the most common long-term What is the most common long-term complication of cemented total hip arthroplasty complication of cemented total hip arthroplasty in patients under 50 years of age?in patients under 50 years of age?
1.1. AgeAge
2.2. DislocationDislocation
3.3. Periprosthetic femur fracturePeriprosthetic femur fracture
4.4. Acetabular component looseningAcetabular component loosening
5.5. Femoral stem fractureFemoral stem fracture
During a posterior approach to the hip joint, During a posterior approach to the hip joint, profuse bleeding is encountered during profuse bleeding is encountered during incision of the quadratus femoris.incision of the quadratus femoris.
The bleeding is most likely from which The bleeding is most likely from which artery?artery?
1.1. Superior gluteal.Superior gluteal.
2.2. Inferior gluteal.Inferior gluteal.
3.3. Lateral femoral circumflex.Lateral femoral circumflex.
4.4. Medial femoral circumflex.Medial femoral circumflex.
5.5. Posterior femoral circumflex.Posterior femoral circumflex.
Which is the correct order of the elastic Which is the correct order of the elastic modulus of the following materials, from the modulus of the following materials, from the lowest to highest modulus?lowest to highest modulus?
1.1. Polyethylene, cancellous bone, cortical bone, Polyethylene, cancellous bone, cortical bone, titanium alloy, cobalt chrome alloytitanium alloy, cobalt chrome alloy
2.2. Cancellous bone, cortical bone, polyethylene, Cancellous bone, cortical bone, polyethylene, titanium alloy, cobalt chrome alloytitanium alloy, cobalt chrome alloy
3.3. Cancellous bone, cortical bone, polyethylene, Cancellous bone, cortical bone, polyethylene, cobalt chrome alloy, titanium alloycobalt chrome alloy, titanium alloy
4. 4. Cancellous bone, polyethylene, cortical bone, Cancellous bone, polyethylene, cortical bone, cobalt chrome alloy, titanium alloycobalt chrome alloy, titanium alloy
5.5. Cancellous bone, polyethylene, cortical bone, Cancellous bone, polyethylene, cortical bone, titanium alloy, cobalt chrome alloytitanium alloy, cobalt chrome alloy
Thank YouThank You