primary management of post-burn contracture neck with
TRANSCRIPT

Letters to Editor
Figure 1: Pre-operative photograph of the patient showing severe post-burn contracture of the neck
We use a simple technique to reliably splint the arm away from the body. A small pillow is folded and is anchored to the forearm and the hand with paper plasters [Figure 1a]. The paper plaster makes sure that, though loosely plastered around the forearm, it prevents movements of the padding from its place. This splints and supports the arm away from the body irrespective of the position of the arm [Figure 1b‑d]. These patients are usually under mild sedation for pain relief post‑operatively. This technique reliably splints the arm away, and there is no worry about the support moving away with patient’s movements. As it is secured well, there is no fear that the support itself will move into the axilla and cause pressure. The patient can keep the hand in any position comfortably. Another usual problem, if the patients are asked to maintain a particular position of the arm in the bed, is muscular strain causing pain around the shoulder and the neck. With the splint on, patients are very comfortable and are allowed free movement of the concerned arm. After the initial application, it usually does not need any attention and is generally removed on the 3rd or 4th day following the surgery. Flap monitoring is unhindered as there are no straps around the chest [Figure 1d].
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
Pravin H. P. Kumar, Vijay Dattatrya Kadam, Sushil Nahar, Rahul Krishnarao Patil,
Ashok Raj KoulDepartment of Plastic and Reconstructive Surgery,
Sparsh Hospital for Advanced Surgeries, Bengaluru, Karnataka, India
Address for correspondence: Dr. Rahul Krishnarao Patil,
Department of Plastic and Reconstructive Surgery, Sparsh Hospital for Advanced Surgeries, Infantry Road, Bengaluru - 560 001, Karnataka, India.
E‑mail: [email protected]
REFERENCES
1. Parrett BM, Caterson SA, Tobias AM, Lee BT. DIEP flaps in women with abdominal scars: Are complication rates affected? Plast Reconstr Surg 2008;121:1527-31.
2. Buford GA, Trzeciak MA. A novel method for lower-extremity immobilization after free-flap reconstruction of posterior heel defects. Plast Reconstr Surg 2003;111:821-4.
3. Venkataramani H, Jain DK, Sabapathy SR. A useful modification of the plaster backslab to off-load pressure from reconstructions of the heel and elbow. Indian J Plast Surg 2012;45:588-9.
How to cite this article: Kumar PH, Kadam VD, Nahar S, Patil RK, Koul AR. Simple way of splinting the arm following vascular anastomosis in the axilla. Indian J Plast Surg 2017;50:116‑7.© 2017 Indian Journal of Plastic Surgery | Published by Wolters Kluwer - Medknow
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
Access this article onlineQuick Response Code:
Website:
www.ijps.org
DOI:
10.4103/ijps.IJPS_34_15
Primary management of post-burn contracture neck with tracheostomy: A surgeon and an anaesthetist’s perspective
Sir,A 42‑year‑old female with severe post‑burn contracture neck (8‑year‑old), [Figures 1 and 2] with restricted mouth opening (1 finger), Mallampati 4, maxillo‑pharyngeal angle about 90° treated initially at a primary health centre, came to our setup for the surgical management of the contracture. After the patient was explained about the unavailability
Indian Journal of Plastic Surgery Volume 50 Issue 1 January‑April 2017117
Published online: 2019-07-05
Letters to Editor
Figure 3: Tracheostomy in situ as an interim procedure to allow further release of the contracture and correct the oropharyngolaryngeal axis
Figure 4: Post-operative photograph of the patient with skin graft after release Figure 5: Post-operative photograph of the patient showing the degree of release and the excellent take of the graft
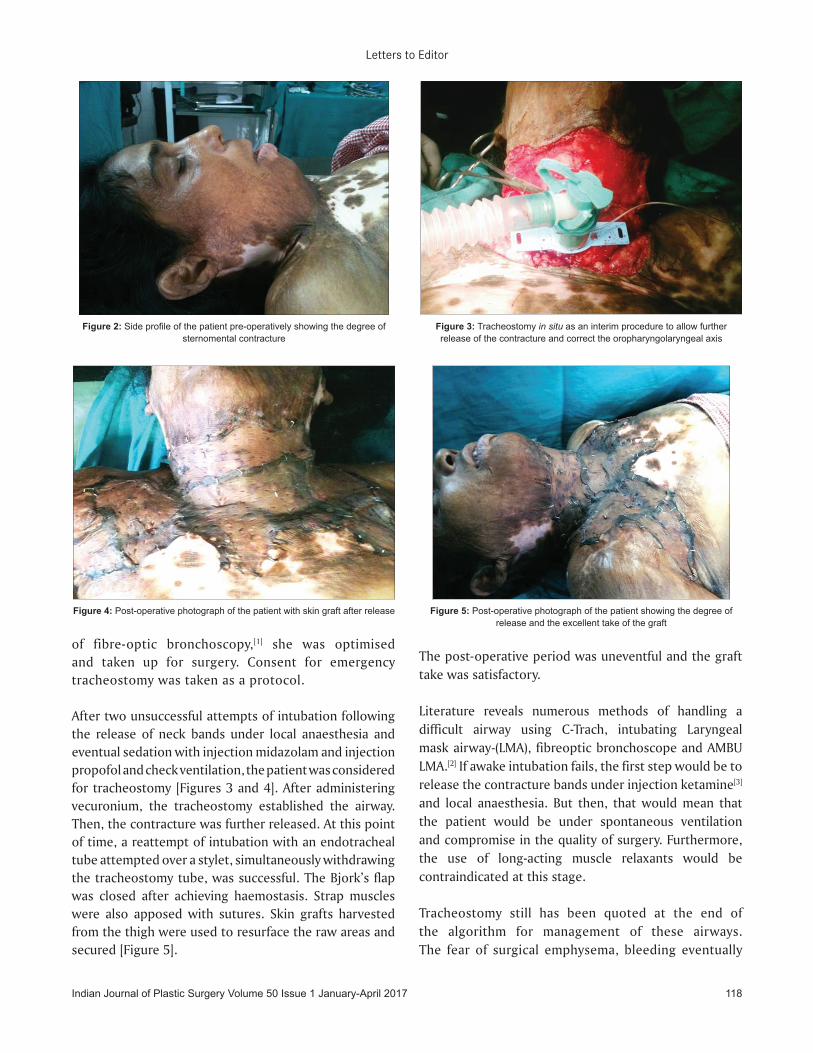
Figure 2: Side profile of the patient pre-operatively showing the degree of sternomental contracture
of fibre‑optic bronchoscopy,[1] she was optimised and taken up for surgery. Consent for emergency tracheostomy was taken as a protocol.
After two unsuccessful attempts of intubation following the release of neck bands under local anaesthesia and eventual sedation with injection midazolam and injection propofol and check ventilation, the patient was considered for tracheostomy [Figures 3 and 4]. After administering vecuronium, the tracheostomy established the airway. Then, the contracture was further released. At this point of time, a reattempt of intubation with an endotracheal tube attempted over a stylet, simultaneously withdrawing the tracheostomy tube, was successful. The Bjork’s flap was closed after achieving haemostasis. Strap muscles were also apposed with sutures. Skin grafts harvested from the thigh were used to resurface the raw areas and secured [Figure 5].
The post‑operative period was uneventful and the graft take was satisfactory.
Literature reveals numerous methods of handling a difficult airway using C‑Trach, intubating Laryngeal mask airway‑(LMA), fibreoptic bronchoscope and AMBU LMA.[2] If awake intubation fails, the first step would be to release the contracture bands under injection ketamine[3] and local anaesthesia. But then, that would mean that the patient would be under spontaneous ventilation and compromise in the quality of surgery. Furthermore, the use of long‑acting muscle relaxants would be contraindicated at this stage.
Tracheostomy still has been quoted at the end of the algorithm for management of these airways. The fear of surgical emphysema, bleeding eventually
Indian Journal of Plastic Surgery Volume 50 Issue 1 January‑April 2017 118

Letters to Editor
obstructing the airway, oedema and leaks has made tracheostomy unpopular among surgeons as well as anaesthetists for such cases. However, in our cases, scenario tracheostomy was fortunately advantageous as it enabled (1) the use of long‑acting muscle relaxants and (2) correcting the tracheobronchial axis by allowing further release of the extensive contracture bands and eventual introduction of endotracheal tube eventually. The main part of emphasis of the article is the ultimate successful closure of the tracheostomy and successful graft resurfacing and uptake contrary to the traditional fear of graft loss due to contamination. The authors would like to recommend the use of indirect laryngoscope[4] as one of the pre‑anaesthetic examinations for such patients to anticipate such airway difficulties.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
Madhubari Vathulya, Seema Shukla, Navin Shukla
Department of Surgery, Subharti Hospital, Dehradun,
Uttarakhand, India
Address for correspondence: Dr. Madhubari Vathulya,
401, Anandlegacy Apartments, Shastri Nagar, Haridwar Road,
Dehradun - 248 001, Uttarakhand, India. E‑mail: [email protected]
REFERENCES
1. Han TH, Teissler H, Han RJ, Gaines JD, Nguyen TQ. Managing difficult airway in patients with post-burn mentosternal and circumoral scar contractures. Int J Burns Trauma 2012;2:80‑5.
2. Mathur R, Jain PK, Chakotiya PS, Rathore P. Anaesthetic and airway management of a post-burn contracture neck patient with microstomia and distorted nasal anatomy. Indian J Anaesth 2014;58:210-3.
3. Al-Zacko SM, Al-Kazzaz DA. Initial release of severe post-burn contracture scar of the neck for intubation under ketamine. Ann Burns Fire Disasters 2009;22:196-9.
4. Law JA, Broemling N, Cooper RM, Drolet P, Duggan LV, Griesdale DE, et al. The difficult airway with recommendations for management – Part 1 – Difficult tracheal intubation encountered in an unconscious/induced patient. Can J Anaesth 2013;60:1089‑118.
Access this article onlineQuick Response Code:
Website:
www.ijps.org
DOI:
10.4103/ijps.IJPS_154_15
How to cite this article: Vathulya M, Shukla S, Shukla N. Primary management of post-burn contracture neck with tracheostomy: A surgeon and an anaesthetist’s perspective. Indian J Plast Surg 2017;50:117‑9.
© 2017 Indian Journal of Plastic Surgery | Published by Wolters Kluwer - Medknow
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
Indian Journal of Plastic Surgery Volume 50 Issue 1 January‑April 2017119
Pedicled transverse rectus abdominis myocutaneous flap: A method for tunnelling with Dilson Luz vascular dilation wands for breast reconstruction
Sir,Despite the popularity of free flaps and microsurgery, the pedicled transverse rectus abdominis myocutaneous (TRAM) flap remains a common autologous alternative for breast reconstruction. We describe a simple, quick and safe technique employed for the tunnelling process with the use of Dilson Luz vascular dilation wands (DLVDW).
Initial diathermy is used to set the plane and direction of undermining at both ends of the outlined tunnel, namely from the medial edge of the inframammary fold to the xiphoid process. This funnelling effect guides the blunt penetration of the initial wand with the smallest diameter. Once the tunnel dissection is complete, progressively larger bore wands are passed through to manipulate lateral detachment of the tunnel [Figures 1‑3]. Minimal diathermy is used at the end of the tunnelling procedure to achieve a consistent diameter throughout.