primary radiation therapy in the treatment of squamous cell carcinoma of the soft palate
TRANSCRIPT

Primary Radiation Therapy in the Treatment of Squamous Cell Carcinoma of the Soft Palate
DAVID HORTON, MD,' LUU TRAN, MD,t PETER GREENBERG, MD,' MICHAEL T. SELCH, MD," AND ROBERT G. PARKER, MD, FACR*
From 1970 to 1986, 45 patients received primary radiation therapy for squamous cell carcinoma of the soft palate a t the University of California Los Angeles (UCLA) Center for the Health Sciences and Wadsworth Veteran's Administration Hospital. Seven patients were lost to follow-up or had prior irra- diation, and were excluded. Thirty-eight patients received a median dose of 70 Gy (62.5 to 80 Gy) to the primary site. After a median follow-up of 48 months, initial control of disease at the primary site was accomplished in 74% of the patients. The initial control by stage was as follows: TI, 83%; T2, 67%; and T3, 63%. After surgical salvage, local control increased to 92%, SO%, and 75% for stages TI, T2, and T3, respectively. Twenty-nine percent (11 of 38) of the patients had cervical node metastases a t presentation. Radiation provided regional control in 96% (26 of 27) with NO disease and 86% (six of seven) with N1 disease at diagnosis. Sixteen patients (42%) had an additional malignancy of the upper aerodigestive tract. Because the incidence of second malignancies after treatment is high and surgical salvage of treatment failures is possible, close follow-up is essential in the management of this tumor. We conclude that radiation therapy is an effective modality for the treatment of squamous cell carcinoma of the soft palate. Primary radiation therapy may offer many patients the chance to avoid surgical procedures that are both cosmetically and functionally debilitating without compromising treatment outcome.
Cancer 63:2442-2445, 1989.
QUAMOUS CELL CARCINOMA of the Soft palate iS an S uncommon malignancy of the oropharynx.l.2 Be- cause of their superficial location, most of these tumors are easily visualized on simple examination, and can be diagnosed early in their development when successful treatment is possible. Numerous past reports have re- garded surgery as the primary modality for tumors of the soft palate. The best surgical results have shown a 3-year determinant survival rate of 86% for patients with Stage I disease at pre~entation.~.~ It is agreed, however, that sur- gical resection causes greater dysfunction than radiation the rap^.^ Numerous studies have reported encouraging local and regional control accompanied by minimal mor- bidity after primary radiation This retrospec- tive study was undertaken to determine whether primary radiation therapy can offer patients with squamous cell carcinoma of the soft palate the chance to avoid disabling
Presented at the 70th Annual Meeting of the American Radium So- ciety, Seattle, Washington, April 17, 1988.
From the *Department of Radiation Oncology, School of Medicine, University of California Los Angeles, Los Angeles, California, and the Jonsson Comprehensive Cancer Center; and tWadsworth Veteran's Ad- ministration Medical Center, Department of Radiation Oncology, West Los Angeles, California.
The authors thank Devi Naidoo, Karima Hambey, and Kathy Oka for aid in manuscript preparation.
Address for reprints: Michael T. Selch, MD, UCLA Medical Center, Department of Radiation Oncology, Center for the Health Sciences, Los Angeles, CA 90024.
Accepted for publication January 18, 1989.
surgical procedures while providing treatment results comparable to surgical resection.
Materials and Methods
The radiation therapy records of 45 patients treated for squamous cell carcinoma of the soft palate in the Radia- tion Oncology Departments of the University of California Los Angeles (UCLA) and Wadsworth Veteran's Admin- istration (VA) Medical Center, Los Angeles, between 1970 and 1986 were reviewed. Seven patients were excluded from the study due to inadequate follow-up (two), con- current advanced head and neck malignancies (three), and previous head and neck irradiation (two). The remaining 38 patients were treated primarily with megavoltage ra- diation therapy and form the substance of this review.
Pretreatment evaluation of all patients included head and neck examination with indirect endoscopy, biopsy of the primary site, chest radiograph, complete blood count (CBC), and a dental evaluation. Some patients were also evaluated by computerized tomography or triple endos- COPY *
The patient ages ranged from 42 to 73 years (mean, 58 years). All VA patients were men. The ratio of men to women was 1 : 1.6 in patients treated at UCLA. All patients had a history of smoking with or without frequent alcohol use. The patients were staged according to the American Joint Committee (AJC) staging system (1978) from the description of the tumor size and extent. Treatment tech- nique consisted of two opposed lateral fields encompassing
2442
No. 12 SQUAMOUS CELL CA OF T H E SOFT PALATE - Iforton et al. 2443
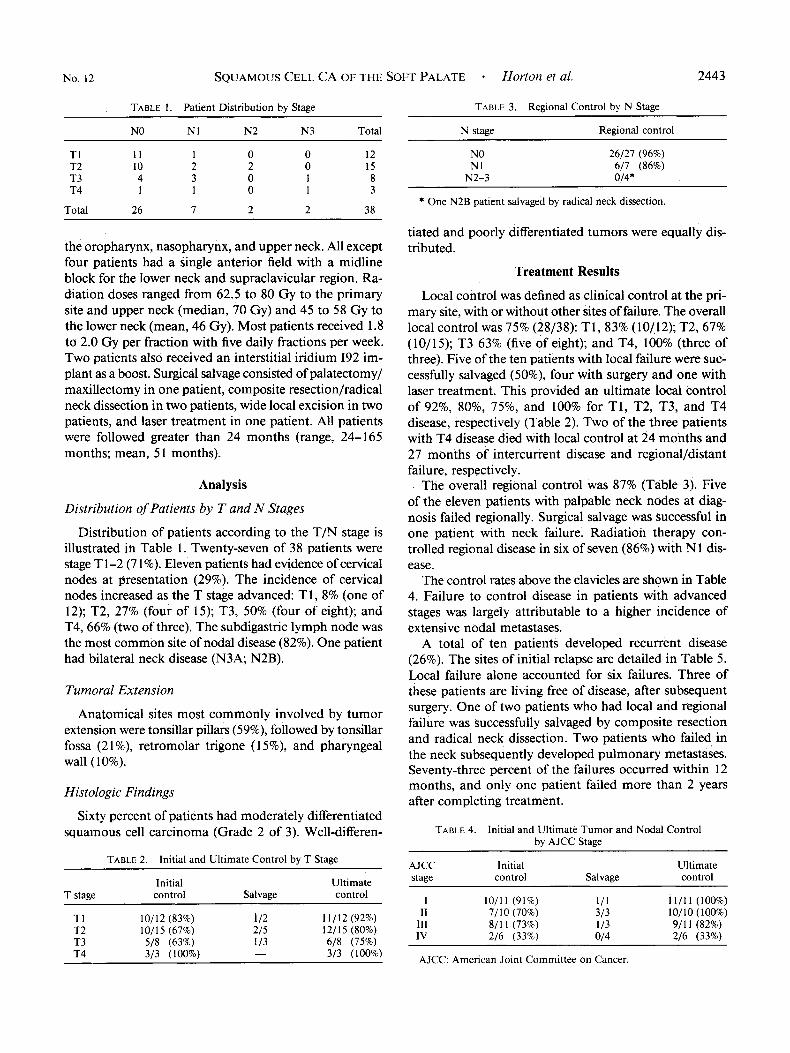
TABLE 1. Patient Distribution by Stage TABLE 3. Regional Control by N Stage ~~ ~~~
NO N1 N2 N3 Total
TI 1 1 1 0 0 12 T2 10 2 2 0 15 T3 4 3 0 1 8 T4 1 1 0 1 3
Total 26 7 2 2 38
the oropharynx, nasopharynx, and upper neck. All except four patients had a single anterior field with a midline block for the lower neck and supraclavicular region. Ra- diation doses ranged from 62.5 to 80 Gy to the primary site and upper neck (median, 70 Gy) and 45 to 58 Gy to the lower neck (mean, 46 Gy). Most patients received 1.8 to 2.0 Gy per fraction with five daily fractions per week. Two patients also received an interstitial iridium I92 im- plant as a boost. Surgical salvage consisted of palatectomyl maxillectomy in one patient, composite resection/radical neck dissection in two patients, wide local excision in two patients, and laser treatment in one patient. All patients were followed greater than 24 months (range, 24-165 months; mean, 5 1 months).
An a 1 y s i s
Distribution of Patients by T and N Stages
Distribution of patients according to the T/N stage is illustrated in Table 1. Twenty-seven of 38 patients were stage T 1-2 (7 1 %). Eleven patients had evidence of cervical nodes at presentation (29%). The incidence of cervical nodes increased as the T stage advanced: T1, 8% (one of 12); T2, 27% (four of 15); T3, 50% (four of eight); and T4,66% (two of three). The subdigastric lymph node was the most common site of nodal disease (82%). One patient had bilateral neck disease (N3A; N2B).
Tumoral Extension
Anatomical sites most commonly involved by tumor extension were tonsillar pillars (59%), followed by tonsillar fossa (21%), retromolar trigone (1 5%), and pharyngeal wall (10%).
Histologic Findings
Sixty percent of patients had moderately differentiated squamous cell carcinoma (Grade 2 of 3). Well-differen-
TABLE 2. Initial and Ultimate Control bv T Stage
Initial Ultimate T stage control Salvage control
TI 10/12 (83%) 1 /2 11/12 (92%) T2 10/15 (67%) 2/5 12/15 (80%) T3 5/8 (63%) 113 6/8 (75%) T4 3/3 (100%) - 3/3 (100%)
N stage Regional control
NO N1
N2-3
26/27 (9690) 6/7 (86%) 014'
* One N2B patient salvaged by radical neck dissection.
tiated and poorly differentiated tumors were equally dis- tributed.
Treatment Results
Local control was defined as clinical control at the pri- mary site, with or without other sites of failure. The overall local control was 75% (28/38): T1,83% (10/12); T2,67% (10/15); T3 63% (five of eight); and T4, 100% (three of three). Five of the ten patients with local failure were suc- cessfully salvaged (50%), four with surgery and one with laser treatment. This provided an ultimate local control of 92%, 80%, 75%, and 100% for T1, T2, T3, and T4 disease, respectively (Table 2). Two of the three patients with T4 disease died with local control at 24 months and 27 months of intercurrent disease and regional/distant failure, respectively.
The overall regional control was 87% (Table 3). Five of the eleven patients with palpable neck nodes at diag- nosis failed regionally. Surgical salvage was successful in one patient with neck failure. Radiation therapy con- trolled regional disease in six of seven (86%) with N1 dis- ease.
The control rates above the clavicles are shown in Table 4. Failure to control disease in patients with advanced stages was largely attributable to a higher incidence of extensive nodal metastases.
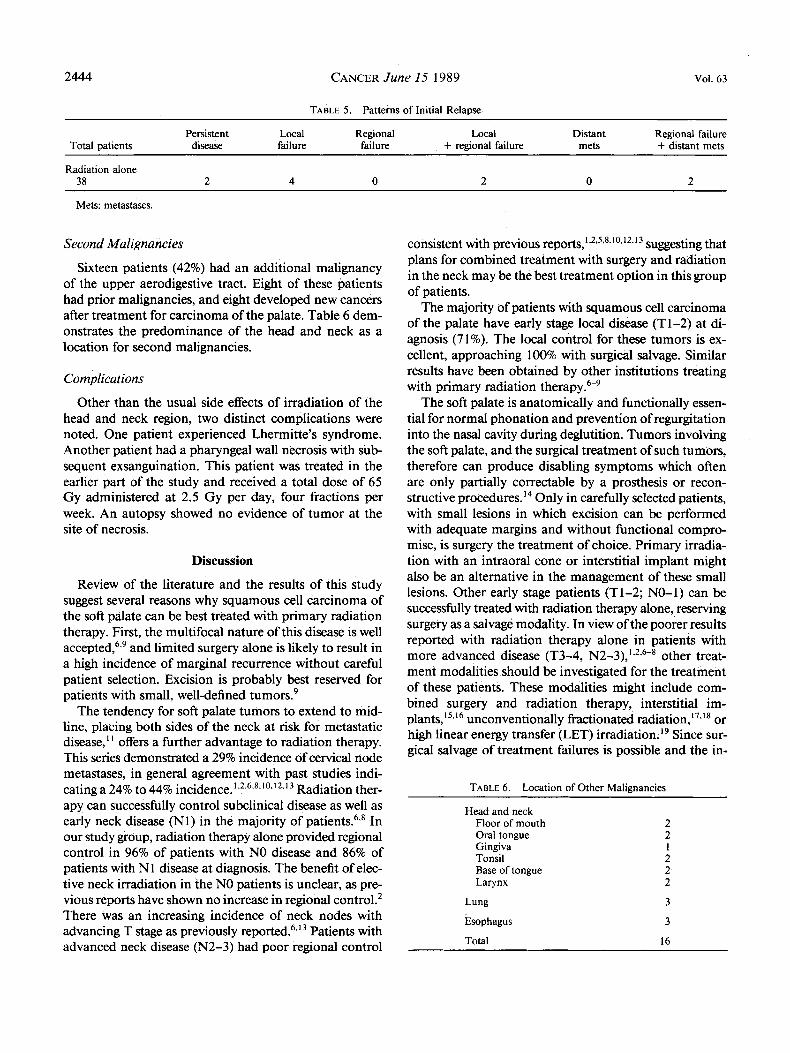
A total of ten patients developed recurrent disease (26%). The sites of initial relapse are detailed in Table 5. Local failure alone accounted for six failures. Three of these patients are living free of disease, after subsequent surgery. One of two patients who had local and regional failure was successfully salvaged by composite resection and radical neck dissection. Two patients who failed in the neck subsequently developed pulmonary metastases. Seventy-three percent of the failures occurred within 12 months, and only one patient failed more than 2 years after completing treatment.
TABLE 4. Initial and Ultimate Tumor and Nodal Control by AJCC Stage
AJCC Initial Ultimate staee control Salvage control
I 10/11 (91%) 111 11 /11 (100%) I1 7/10 (70%) 3/3 10/10 (100%)
111 8/1 I (73%) 1 /3 9/11 (82%) 2/6 (33%) IV 2/6 (33%) 014
AJCC: American Joint Committee on Cancer.
2444 CANCER June 15 1989 Vol. 63
TABLE 5 . Patterns of Initial Relapse
Persistent Local Regional Local Distant Regional failure Total patients disease failure failure + regional failure mets + distant mets
Radiation alone 38 2 4 0 2 0 2
Mets: metastases.
Second Malignancies
Sixteen patients (42%) had an additional malignancy of the upper aerodigestive tract. Eight of these patients had prior malignancies, and eight developed new cancers after treatment for carcinoma of the palate. Table 6 dem- onstrates the predominance of the head and neck as a location for second malignancies.
Complications
Other than the usual side effects of irradiation of the head and neck region, two distinct complications were noted. One patient experienced Lhermitte's syndrome. Another patient had a pharyngeal wall necrosis with sub- sequent exsanguination. This patient was treated in the earlier part of the study and received a total dose of 65 Gy administered at 2.5 Gy per day, four fractions per week. An autopsy showed no evidence of tumor at the site of necrosis.
Discussion
Review of the literature and the results of this study suggest several reasons why squamous cell carcinoma of the soft palate can be best treated with primary radiation therapy. First, the multifocal nature of this disease is well a~cepted,~.' and limited surgery alone is likely to result in a high incidence of marginal recurrence without careful patient selection. Excision is probably best reserved for patients with small, well-defined tumors.'
The tendency for soft palate tumors to extend to mid- line, placing both sides of the neck at risk for metastatic disease,' ' offers a further advantage to radiation therapy. This series demonstrated a 29% incidence of cervical node metastases, in general agreement with past studies indi- cating a 24% to 44% incidence. 1,2.6*8*10*12.13 Radiation ther- apy can successfully control subclinical disease as well as early neck disease (Nl) in the majority of In our study group, radiation therapy alone provided regional control in 96% of patients with NO disease and 86% of patients with N 1 disease at diagnosis. The benefit of elec- tive neck irradiation in the NO patients is unclear, as pre- vious reports have shown no increase in regional control.2 There was an increasing incidence of neck nodes with advancing T stage as previously r e ~ o r t e d . ~ . ~ ~ Patients with advanced neck disease (N2-3) had poor regional control
consistent with previous r e p ~ " s , ' ~ ~ ~ ~ " " ~ ' ~ ~ ' ~ suggesting that plans for combined treatment with surgery and radiation in the neck may be the best treatment option in this group of patients.
The majority of patients with squamous cell carcinoma of the palate have early stage local disease (Tl-2) at di- agnosis (71%). The local control for these tumors is ex- cellent, approaching 100% with surgical salvage. Similar results have been obtained by other institutions treating with primary radiation
The soft palate is anatomically and functionally essen- tial for normal phonation and prevention of regurgitation into the nasal cavity during deglutition. Tumors involving the soft palate, and the surgical treatment of such tumors, therefore can produce disabling symptoms which often are only partially correctable by a prosthesis or recon- structive procedures. l4 Only in carefully selected patients, with small lesions in which excision can be performed with adequate margins and without functional compro- mise, is surgery the treatment of choice. Primary irradia- tion with an intraoral cone or interstitial implant might also be an alternative in the management of these small lesions. Other early stage patients (Tl-2; NO-1) can be successfully treated with radiation therapy alone, reserving surgery as a salvage modality. In view of the poorer results reported with radiation therapy alone in patients with more advanced disease (T3-4, N2-3),'~*,~-' other treat- ment modalities should be investigated for the treatment of these patients. These modalities might include com- bined surgery and radiation therapy, interstitial im-
unconventionally fractionated radiati~n,",'~ or high linear energy transfer (LET) irradiation." Since sur- gical salvage of treatment failures is possible and the in-
TABLE 6. Location of Other Malienancies
Head and neck Floor of mouth Oral tongue Gingiva Tonsil Base of tongue Larynx
Lung
Esophagus
Total
2 2 1 2 2 2
3
3
16

No. 12 SQUAMOUS CELL CA OF THE SOFT PALATE * Horton et al. 2445
cidence of second malignancies after treatment is high (2 1 %), close follow-up is essential in the management of this tumor.
REFERENCES
I . Seydel HG, Scholl H. Carcinoma of the soft palate and uvula. Am J Roentgenol Radio1 Ther Mucl Med 1974; 120:603-607.
2. Fee WE, Schoeppel SL, Rubenstein R et al. Squamous cell carci- noma of the soft palate. Arch Otolryngol 1979; 105:710-718.
3. Strong MS, Di Troin JF, Vaughan CW. Carcinoma of the palative arch. Trans Am Acad Ophthalmol Otolaryngol 197 I ; 79957-967.
4.- Healy GB, Strong MS, Uchmakli A et al. Carcinoma of the palative arch. Am J Surg 1976; 132:498-503.
5. Konrad HR, Canalis RF, Calcaterra TC. Epidermoid carcinoma of the palate. Arch Otolaryngol 1978; 104:208-2 12.
6. Fletcher GH, Lindberg RD. Squamous cell carcinomas of the ton- sillar area and palative arch. Am J Roentgenol 1966; 96:574-587.
7. Fletcher GH. Squamous cell carcinomas of the oropharynx. Int .I Radiat Oncol Biol Phys 1979; 5:2075-2090.
8. Garrett PG, Beale FA. Carcinoma of the 0ropharynx:soft palate. J Otolaryngol 1984; 13: 165- 168.
9. Million RR, Cassisi NJ. Oropharynx. In: Million RR, Cassisi NJ, eds. Management of Head and Neck Cancer a Multidisciplinary Ap- proach, ed. I . Philadelphia: JB Lippincott, 1984; 299-314.
10. Cheng VST, Shetty KS, Deutsch M. Carcinomas of the anterior
tonsillar pillar and the soft palate-uvula: Treatment by radiation therapy. Radiology 1980; I34:497-50 I .
1 1. Perez CA. Carcinoma of the tonsillar fossa and facial arch. In: Perez CA, Brady LW, eds. Principles and Practice of Radiation Oncology, ed. 1. Philadelphia: JB Lippincott, 1987; 546-568.
12. Russ JE, Applebaum EL, Sisson GA. Squamous cell carcinoma of the soft palate. Laryngoscope 1977; 87: 1 15 I - I 156.
13. Ratzer ER, Schweitzer RJ, Frazelle EL. Epidermoid carcinoma of the palate. A m JSurg 1970; I19:294-297.
14. Armany MA, Myers EN. Prosthetic reconstruction following re- section of the hard and soft palate. Prosthet Dent 1978; 40: 174-178.
15. Puthawala AA, Syed AMN, Eads D, Neblett D, Gillin L, Gates TC. Limited external irradiation and interstitial iridium I92 implant in the treatment of squamous cell carcinoma of the tonsillar region. Int J Radiat Oncol Biol Phys 1984; 11:1545-1601.
16. Sealy R, Hering E, Buret E. The treatment of cancer of the uvula and soft palate with interstitial radioactive wire implants. Int J Radiat Oncol Biol Phys 1984; 10:1951-1955.
17. Million RR, Parsons JT, Cassisi NJ. Twice-a-day irradiation tech- nique for squamous cell carcinoma of the head and neck. Cancer 1985;
18. Wang CC, Blitzer PH, Suit HD. Twice-a-day radiation therapy for cancer of the head and neck. Cancer 1985; (Supp1)55:2100-2104.
19. Laramore GE, Griffin TW, Tong D et a/. Fast neutron teletherapy for advanced carcinomas ofthe oral cavity and soft palate. Cancer 1980; 46:1903-1909.
5512096-2099 SUPP.