principles in treatment of type 2 diabetes · diabetes affects 6% of the global adult population....
TRANSCRIPT

PrinciplesPrinciples inin treatmenttreatment of of typetype 2 2 diabetesdiabetes
1 i
Dr hab. Jacek Dr hab. Jacek DaroszewskiDaroszewski Department of Department of EndocrinologyEndocrinology, , DiabetesDiabetes
and and IsotopeIsotope TherapyTherapy
[email protected]@umed.wroc.pl

0
50
100
150
200
250
300
350
400
450
500
1985 2000 2010 2030
mln
DiabetesDiabetes inin thethe worldworld
2 J.Daroszewski
160 000 000
550 000 000
370 000 000

„…„… DiabetesDiabetes affectsaffects 66%% ofof thethe globalglobal adultadult populationpopulation.. ItIt isis aa leadingleading causecause ofof blindness,blindness, heartheart disease,disease, stroke,stroke, kidneykidney failurefailure andand amputationamputation.. EveryEvery year,year, overover 33..88 millionmillion deathsdeaths areare duedue toto diabetes,diabetes, makingmaking diabetesdiabetes aa moremore significantsignificant globalglobal killerkiller thanthan HIV/AIDSHIV/AIDS andand malariamalaria combinedcombined.. EveryEvery 1010 secondsseconds aa personperson diesdies fromfrom diabetesdiabetes--relatedrelated causescauses.. InIn thatthat samesame 1010 seconds,seconds, twotwo peoplepeople developdevelop thethe diseasedisease.
((Prof. Jean Claude Prof. Jean Claude MbanyaMbanya, , presidentpresident of IDF )of IDF )
3 J.Daroszewski

United Nations, World Population Prospect: 2008
Number of patients 3,082 mln prevalence 9,3% world 8,3% Europe 6,7% type 1 diabetes 10% type 2 diabetes 90% not treated 1,105 mln (29%)
DiabetesDiabetes inin PolandPoland
4 J.Daroszewski

IDF ATLAS 2010
CostsCosts of of treatmentreatment (per t (per patientpatient 2010 2010 –– EUR)EUR)
3751
979 779 145 238
J.Daroszewski
Costs overall 600 000 000 PLN

Education
Life style intervention
Diet
Physical activity
Smoking cessation
Glycaemic control
Achieve and maintain body weight goals
Management of blood pressure
Management of lipid disorders
Antiplatelet therapy
Rudiments of DM2 managementRudiments of DM2 management:: compcomprerehensivehensive treatment treatment
6 J.Daroszewski

STENO-2
Steno-2: •
160 patients with type 2 diabetes and the metabolic syndrome including microalbuminuria were randomized conventional therapy at their GP’s or intensive care at Steno Diabetes Center
Conventional group assigned to GPs
Intensive group assigned to Steno Diabetes Center
Endpoint examinations
Microvascular Macrovascular
4 years 8 years
80
80
n=160

STENO-2
LIFESTYLE Percentage of patients obtaining treatment goals for the
intensive therapy group after 7.8 yrs
Fat intakeFat intake <30% E<30% E
Saturated fatSaturated fat <10% E<10% E
NonNon--smokerssmokers
ExerciseExercise >150 min/week>150 min/week
Intensive Convent Intensive Convent Intensive Convent Intensive Convent 0
10
20
30
40
50
60
70
80
1
p=0.09
p=0.02 p=0.13
p=0.58

STENO-2
0
5
10
15
20
1 2 3 4 5 6
PCI or CABG
Vascular surgery Amputation
Macrovascular complications
85 CVD events in 35 ’conventional’ patients 33 CVD events in 19 ’intensive’ patients
Stroke CVD death Myocardial infarction
Number of eventsNumber of events
Intensive Conventional

STENO-2
Percentage of patients achieving treatment goals set for the intensive therapy group at 7.8 yr
0
10
20
30
40
50
60
70
80
1
HbA1c<6.5% Cholesterol <4.5 mM
Triglycerides <1.7 mM
Systolic BP <130 mm Hg
Diastolic BP <80 mm Hg
Int Conv
%
p<0.0001 p=0.21
Int Conv Int Conv Int Conv Int Conv
p=0.06
p=0.19
p=0.001

Education
Life style intervention
Diet
Physical activity
Smoking cessation
Glycaemic control
Achieve and maintain body weight goals
Management of blood pressure
Management of lipid disorders
Antiplatelet therapy
Rudiments of DM2 managementRudiments of DM2 management:: compcomprerehensivehensive treatment treatment
11 J.Daroszewski

DiabeticDiabetic educationeducation
•• SelfSelf--monitoringmonitoring –– glucometer glucometer useuse •• DietDiet •• PhysicalPhysical activityactivity •• SymptomsSymptoms and management of and management of hypoglycaemiahypoglycaemia •• TechnicsTechnics of insulin of insulin injectioninjection •• FeetFeet inspectioninspection and and carecare ….….
•• InitialInitial educationeducation of of patientpatient treatedtreated withwith diet and diet and oraloral agentsagents –– min. 5 min. 5 hrshrs.. •• PatientPatient on insulin on insulin therapytherapy—— caca. 9 . 9 hrshrs..
12 J.Daroszewski
Don’t scold a patient

Self-monitoring of glycaemia – how often
OnlyOnly dietdiet 1x 1x inin monthmonth shortshort prolifeprolife ((fastingfasting and 2 and 2 hrshrs. . afterafter mainmain mealsmeals)) OralOral agentsagents oror GLPGLP--11 1x 1x inin weekweek shortshort prolifeprolife FixFix insulin insulin dosesdoses 11--2 measurements daily 2 measurements daily 1x in week short prolife1x in week short prolife 1x in month full prolife1x in month full prolife (fasting , (fasting , preprandialpreprandial, 2 hrs. after , 2 hrs. after maimainn
meals, at bed time)meals, at bed time)
J.Daroszewski 13

Reality Reality inin thethe diabeticdiabetic educationeducation inin PolandPoland
81,8 91,0 68,5
8,2 17,8 30,5
14 J.Daroszewski

Education
Life style intervention
Diet
Physical activity
Smoking cessation
Achieve and maintain body weight goals
Management of blood pressure
Management of lipid disorders
Antiplatelet therapy
Glycaemic control
Rudiments of DM2 managementRudiments of DM2 management:: compcomprerehensivehensive treatment treatment
15 J.Daroszewski

J.Daroszewski 16

Diet is a basic part of management in every case. Treatment cannot be effective unless adequate attention is given to ensuring appropriate nutrition.
Dietary treatment should aim at: ◦ ensuring weight control ◦ providing nutritional requirements ◦ allowing good glycaemic control with blood glucose
levels as close to normal as possible ◦ correcting any associated blood lipid abnormalities
Diet

Dietary fat should provide 25-35% of total intake of calories but saturated fat intake should not exceed 10% of total energy. Cholesterol consumption should be restricted and limited to 300 mg or less daily.
Protein intake can range between 10-15% total energy (0.8-1 g/kg of desirable body weight). Protein should be derived from both animal and vegetable
sources (50%-50%).
Carbohydrates provide 50-60% of total caloric content of the diet. Carbohydrates should be complex and high in fibre. GI> 50
Excessive salt intake is to be avoided. It should be particularly restricted in people with hypertension and those with nephropathy.
Diet (cont.)

Education
Life style intervention
Diet
Physical activity
Smoking cessation
Achieve and maintain body weight goals
Management of blood pressure
Management of lipid disorders
Antiplatelet therapy
Glycaemic control
Rudiments of DM2 managementRudiments of DM2 management:: compcomprerehensivehensive treatment treatment
19 J.Daroszewski

20 J.Daroszewski
LifestyleLifestyle interventionintervention preventsprevents the the progressprogress of of prediabeticprediabetic statesstates to to overtovert diabetesdiabetes

Education
Life style intervention
Diet
Physical activity
Smoking cessation
Achieve and maintain body weight goals
Management of blood pressure
Management of lipid disorders
Antiplatelet therapy
Glycaemic control
Rudiments of DM2 managementRudiments of DM2 management:: compcomprerehensivehensive treatment treatment
21 J.Daroszewski

The cover of "The Economist", Dec. 13-19, 2003.
100 -150 years
22 J.Daroszewski

Body mass Body mass isis connectedconnected withwith mortalitymortality inin DM DM typetype 22
Mulnier. Diabet Med 2006;23:516–21
(n=28 725)
Re
lati
ve
risk
23 J.Daroszewski
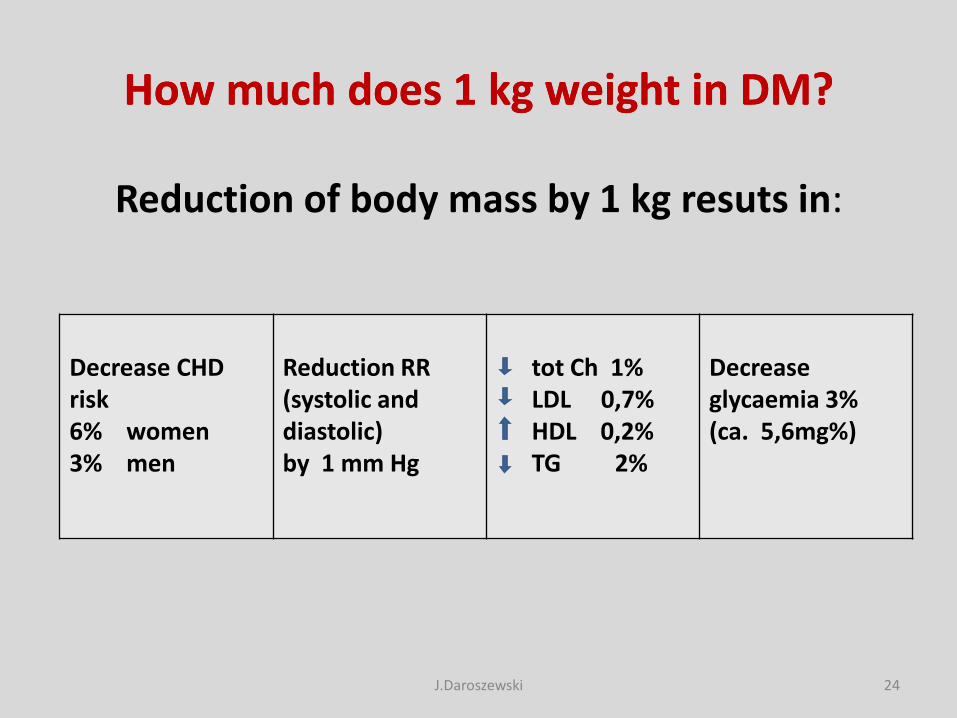
HowHow much much doesdoes 1 kg 1 kg weightweight inin DM?DM?
Reduction of body mass by 1 kg resuts in:
Decrease CHD risk 6% women 3% men
Reduction RR (systolic and diastolic) by 1 mm Hg
tot Ch 1% LDL 0,7% HDL 0,2% TG 2%
Decrease glycaemia 3% (ca. 5,6mg%)
24 J.Daroszewski

FemalesFemales
> 80 cm increased risk of complications > 88 cm need of treatment
MalesMales
> 94 cm increased risk of complications > 102 cm need of treatment
Lean MEJ, et al. Lancet;1998:351:853–6
cm
The role od The role od adiposeadipose tissuetissue distributiondistribution. . IncreasedIncreased waistwaist circumferencecircumference ((abdominal abdominal fatfat) )
is is associated with an increased associated with an increased riskrisk of CV of CV complicationscomplications
25 J.Daroszewski

CostsCosts of of treatmenttreatment inin relationrelation to BMI to BMI (per (per yearyear))
Data from Wolf and Colditz. Am J Clin Nutr 1996; 63(Suppl): 466S–9S
(bil US$)
Cholelithiasis Hypertension CHD Type 2 diabetes
12
10
8
6
4
2
0
BMI (kg/m2)
23–24.9
25–28.9
29
26 J.Daroszewski

Intensification of the treatment Intensification of the treatment isis usually connected usually connected with increase of body masswith increase of body mass
UKPDS 33. Lancet 1998;352:837–53
Years of follow up
Bad
y m
ass
gain
(kg
)
intensive therapy conventional therapy
27 J.Daroszewski

ChangesChanges inin body mass body mass duringduring differentdifferent medicationmedication inin DMDM
Na podstawie:Mitri and Hamdy. Expert Opin Drug Saf 2009;8:573–84
Ch
ange
in b
od
y m
ass
(kg)
28 J.Daroszewski

Education
Life style intervention
Diet
Physical activity
Smoking cessation
Glycaemic control
Achieve and maintain body weight goals
Management of blood pressure
Management of lipid disorders
Antiplatelet therapy
Rudiments of DM2 managementRudiments of DM2 management:: compcomprerehensivehensive treatment treatment
29 J.Daroszewski

0
10
20
30
40
50
60
24
PP=0.0046=0.0046
All end points
connected
with DM
32
PP=0.019=0.019
CV deaths
44
PP=0.013=0.013
strokes
37
PP=0.0092=0.0092
Microvascular
end points
34
PP=0.0038=0.0038
Progression of
retinopathy
47
PP=0.0036=0.0036
Sight
deterioration
56
PP=0.0043=0.0043
Heart feilere
UKPDS Group. BMJ. 1998, 317, 703-713
Tight blood pressure control leads to the reduction
of risk of vascular complications

Goals for arterial hypertension
• < 140/90 mmHg - if higher – need for therapy
Goals for lipids
• cholesterol total < 175 mg/dl (< 4,5 mmol/l)
• LDL-cholesterol < 100 mg/dl (< 2,6 mmol/l)
• LDL-cholesterol (CHD) < 70 mg/dl (< 1,9 mmol/l)
• HDL-cholesterol > 40 mg/dl (> 1,0 mmol/l)
• non-HDL-cholesterol < 130 mg/dl (< 3,4 mmol/l)
• Triglycerides < 150 mg/dl (< 1,7 mmol/l)
Zalecenia PTD 2011
31 J.Daroszewski

Education
Life style intervention
Diet
Physical activity
Smoking cessation
Achieve and maintain body weight goals
Management of blood pressure
Management of lipid disorders
Antiplatelet therapy
Glycaemic control
Rudiments of DM2 managementRudiments of DM2 management:: compcomprerehensivehensive treatment treatment
32 J.Daroszewski

Ramlo-Halsted i wsp. Prim Care. 1999;26:771–789.
DM DM isis a a chronicchronic and progressive and progressive diseasedisease
Disease progression
prediabetes
insulinemiainsulinemia
Insulin Insulin resistaneresistane
HepaticHepatic gluconeogenesisgluconeogenesis
Diagnosis DM
PostprandialPostprandial glycemiaglycemia
FastingFasting glycemiaglycemia
ΒΒ--cellcell functionfunction
overt diabetes
4–7 years
0
50
100
Re
lati
ve
Bew
ta c
ells
fu
nct
ion
%
33 J.Daroszewski

UKPDS: UKPDS: loweringlowering ofof HbAHbA1c1c decreasesdecreases DM DM connectedconnected complicationscomplications
REDUCTION
HbA1c by 1% REDUCED RiSK (P<0,0001)
1%
Death connected with DM
Myocardial infarction
Microvascular complications
Peripheral atheromatosis
UKPDS = Badanie Prospektywne Cukrzycy (ang. United Kingdom Prospective Diabetes Study) Opracowano na podstawie: Stratton IM i wsp. UKPDS 35. BMJ. 2000;321:405–412.
*P<0,0001 34 J.Daroszewski

Lowering of glycaemia:
•• As early as possibleAs early as possible
•• As low as possibleAs low as possible (?)(?)
•• As long as possibleAs long as possible
•• As safely as possibleAs safely as possible
•• As reasonably as possibleAs reasonably as possible
David N Kendall, ADA, New Orlean 2007
35 J.Daroszewski

„…whether intensive therapy to target normal glycated hemoglobin levels would reduce cardiovascular events in patients with type 2
diabetes who had either established cardiovascular disease or additional cardiovascular risk factors.”
ACCORD study
36 J.Daroszewski

ACCORD study - Median Glycated Hemoglobin Levels at Each Study Visit.
mediana HbA1c = 8.1%
mediana HbA1c = 7.5%
mediana HbA1c = 6.4%
ACCORD Study group, The NEJM 2008, vol. 358: 2545-2559

ACCORD: intensive therapy may be harmful?
Gerstein et al. N Engl J Med 2008;358:2545–59.
• Randomised study in type 2 DM (n=10251)
• Comparison intensive vs standard therapy
• Study has been stopped since increased mortality in intensive treated
group 25
10
0
Pai
en
ts r
em
ain
ing
in t
he
stu
dy
(%
)
5
20
YEARS
15
0 1 2 3 4 5 6 7
All cause mortality
Iloraz szans (CI) 1,22 (1,01; 1,46); p=0,04
standard
intensive

What was the reason of increased mortality in intensive arm?
% o
f p
atie
nts
wit
h a
t le
ast
1 in
cid
en
t o
f h
ypo
glyc
aem
ia
Duration of follow-up (years)
Yearly mortality in treated intensively:
• 2.8% - when hypoglycaemia occured
• 1.2% - without hypos
Hypoglycaemia?
ACCORD Study group, The NEJM 2008, vol. 358: 2545-2559

Both high and low HbA1c
values are connected with increased mortality
Currie et al. Lancet. 2010;375:481–9.
2,0
1,4
1,0
0,8
MO
RT
ALIT
Y H
R (
95%
CI)
1,2
1,6
HbA1c (%)
1,8
6,0 6,5 7,0 7,5 8,0 8,5 9,0 9,5 10,0 10,5 11,0 11,5
HbA1c = 7,5%
Patients with DM 2
Age 50 yrs <
n=47970
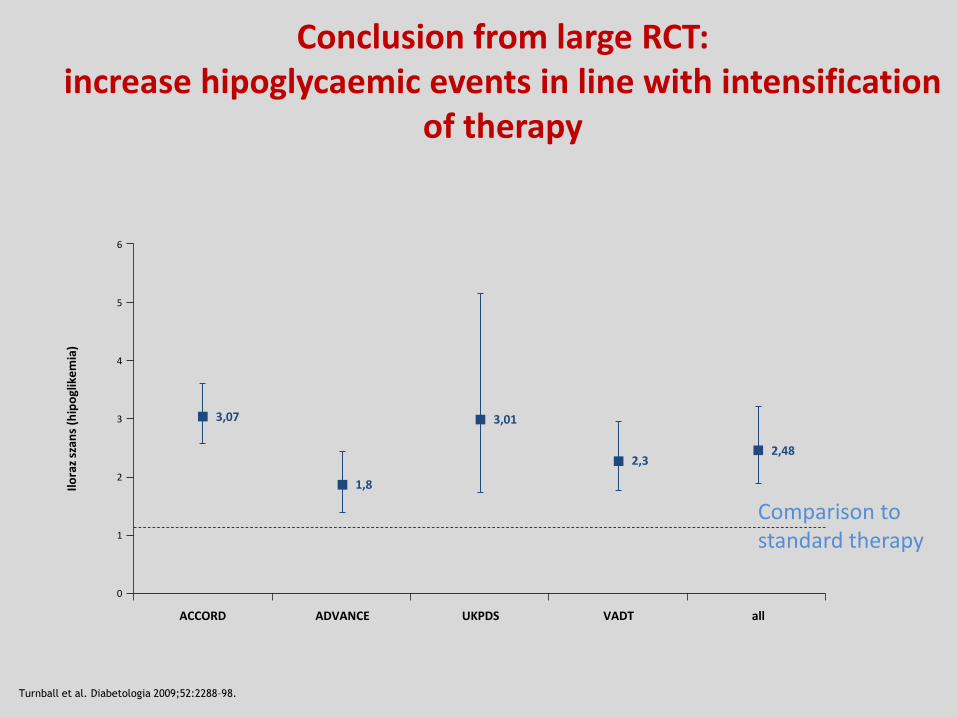
Conclusion from large RCT: increase hipoglycaemic events in line with intensification
of therapy
Turnball et al. Diabetologia 2009;52:2288–98.
6
3
1
0
Ilo
raz
szan
s (h
ipo
glik
em
ia)
2
4
ACCORD
5
ADVANCE UKPDS VADT all
3,07
1,8
3,01
2,3 2,48
Comparison to standard therapy

MetaanalysisMetaanalysis ACCORD, ADVANCE, ACCORD, ADVANCE, UKPDS, VADT i UKPDS, VADT i PROactivePROactive
Ray K i wsp. Lancet 2009; 373: 1765–72
In type 2 diabetics intensive reduction of glycaemia decreases macrovascular events but doesn’t influence death risk.
TheThe optimaloptimal modemode ofiofi HbAHbA1c1c reductionreduction maymay be be differentdifferent inin somesome patientspatients populationspopulations
42 J.Daroszewski
infarct
CHD
stroke
All cause mortality

IndividualisationIndividualisation of of goalsgoals inin antihyperglycemicantihyperglycemic treatmenttreatment
DM 2 DM 2 •• inin youngyoung, , •• newlynewly diagnoseddiagnosed, , •• withoutwithout vascularvascular complicationscomplications
DM 2 DM 2 •• inin elderlyelderly •• long long durationduration •• withwith vascularvascular episodesepisodes
43 J.Daroszewski

SO WHAT A1C TARGETS?

Glycemic goals in DM treatment (PTD 2014)
General General goalgoal HbAHbA1c 1c <<7.07.0%%
HbAHbA1c 1c << 6.56.5%% NewlyNewly diagnoseddiagnosed and of and of shortshort durationduration
HbAHbA1c 1c << 8.08.0%% PatientsPatients > 70 > 70 yrsyrs Long Long durationduration (> 20 (> 20 yrsyrs) ) MacroangiopathyMacroangiopathy ( MI / ( MI / strokestroke))
HbAHbA1c 1c < < 7.07.0%% PatientsPatients > 65 > 65 yrsyrs ExpectedExpected survivalsurvival > 10 > 10 yrsyrs
45 J.Daroszewski

Strategia Strategia ABCDABCD ((AAgege-- BBody ody weightweight-- CComplicationsomplications-- DDurationuration))
young middle Advanced
- + - + - +
<6,5 6,5 -7 <6 <6,5 < 7 7 - 8
A
C or D > 10 yrs
HbA1C%
HbA1C > 9%
HbA1C < 9%
Insulin
Metformin Pozilli P et al. Diabetes Metab Res Rev 2010;26:239-244 46 J.Daroszewski

Correlation between % of HbA1c and mean glycaemia
47 J.Daroszewski

Glycemic control in diabetes in Poland meanmean HbA1C 8.07%
J.Daroszewski PolDiab

Getting Patients to Goal Becomes More Challenging as Disease Progresses
NHANES= badanie NHANES (ang.National Health and Nutritional Examination Survey). Opracowano na podstawie: Lebovitz HE. Med Clin N Am. 2004;88:847–863; Turner RC i wsp. JAMA. 1999;281:2005–2012; UKPDS 16. Diabetes. 1995;44:1249–1258; Warren RE. Diabetes Res Clin Pract. 2004;65:S3–S8; Resnick HE i wsp. Diabetes Care. 2006;29:531–537; Koro CE i wsp. Diabetes Care. 2004;27:17–20.
Parameter (NHANES)
% of patients with HbA1c<7% 49,8% (2001–2002)
Mean HbA1c 7,9% (1999–2000)
100
0
Β -
cell
fu
nct
ion
( %
)
-10 0
DM diagnosis
Insulin therapy
Demand of insulin Failure of monotherapy
Combination of more agents
+/– insulin
Estimated time (years)
Combination of 2 agents
Monotherapy
80
60
40
20 Preclinical stage Prediabetic states Diabetes
10–20
49 J.Daroszewski
Life style modification

The choice of treatment mode in DM2 patient
•• Pathogenesis Pathogenesis of of DM 2DM 2
•• Presence of insulinPresence of insulin resistanceresistance
•• Duration of diseaseDuration of disease
•• Chronic complicationsChronic complications
•• CoCo--morbiditymorbidity
•• Economic ability of the patientEconomic ability of the patient
•• Cognitive ability of the patientCognitive ability of the patient
50 J.Daroszewski

Treatment algorithm (PTD 2013)
PSM – pochodna sulfonylomocznika
* na każdym etapie leczenia zalecana jest modyfikacja stylu życia ** rzadko, ewentualnie u osób szczupłych # agonista receptora GLP-1 (inkretynomimetyk) lub inhibitor DPP-4 (gliptyna)
metformin
(SU)
metformin
+
SU
metformin
+ 2 agents with
different
mechanisms
(SU or incretin
agent or
acarbose)
metformin
+ basal
insulina
or
metformin +
insulin
in 2 doses
(basal or
premixted)
metformin
+
Intensive
insulin
therapy
metformin
+
incretin
agent
Stage 1
Oral monotherapy
Stage 2a
Oral combined therapy *
Stage 2b
Elementary
Insulin thyerapy*
Stage 3
Combined Insulin therapy
premixted
insulin
51 J.Daroszewski
Life style Life style modificationsmodifications atat allall stagesstages

Features of oral antidiabetic agents
Metformin SU and glinids
alfa-glucosydase Inhibitors
Glitazons (TZD)
GLP-1 receptor agonists
DPP-IV Inhibitors
HbA1C 1-2% 1-2% 0,5-1,0% 0,5-1,0%
0,5-1,0%
0,5- 0,8%
Fasting Glycaemia
60-70 60-70
20-30 60-70 50 50
Insulin in plasma
Chol LDL
Chol HDL
TG
Body Mas
52 J.Daroszewski

Features of oral antidiabetic agents
Metformin SU and glinids
alfa-glucosidase Inhibitors
Glitazons (TZD)
GLP-1 receptor agonists
DPP-IV Inhibitors
HbA1C 1-2% 1-2% 0,5-1,0% 0,5-1,0%
0,5-1,0%
0,5- 0,8%
Fasting Glycaemia
60-70 60-70
20-30 60-70 50 50
Insulin in plasma
Chol LDL
Chol HDL
TG
Body Mas
53 J.Daroszewski

Metformin - mechanism of action
•• Increases periIncreases perippheralheral action of insulinaction of insulin
•• Inhibits gluconeogenesisInhibits gluconeogenesis
•• Decreases glucose absorption in gutDecreases glucose absorption in gut
•• Doesn’t induce hypoglycaemiaDoesn’t induce hypoglycaemia
•• Beneficial Beneficial oror neutralneutral for body massfor body mass
•• The most commonly used agent in treatment of DMThe most commonly used agent in treatment of DM
•• Be aware of contraindicationsBe aware of contraindications
54 J.Daroszewski

Contraindications for MTF use
•• AllergyAllergy to to biguanidesbiguanides
•• AcuteAcute diabeticdiabetic complicationscomplications
•• TypeType 1 1 DiabetesDiabetes (?) (?) –– inin monotherapymonotherapy
•• PregnancyPregnancy
•• DiabetesDiabetes withwith cachexycachexy
•• UncontrolledUncontrolled alcoholalcohol consumptionconsumption
•• ImpairedImpaired liverliver functionfunction
•• ImpairedImpaired renalrenal functionfunction
don’tdon’t start MTF start MTF ifif eGFReGFR < 60ml/min/1,73m< 60ml/min/1,73m2 2
stop MTF stop MTF eGFReGFR < 30ml/min/1,73m< 30ml/min/1,73m2 2
•• ShockShock, , inadequateinadequate bloodblood perfusionperfusion, , cardiaccardiac insufficiencyinsufficiency, , acuteacute coronarycoronary episodeepisode, ,
55 J.Daroszewski

Gastrointestinal symptoms during MTF treatment
(usually at the beginning)
•• DrynessDryness of of mouthmouth
•• MetallicMetallic tastetaste
•• AnorexiaAnorexia
•• NauseaNausea
•• FFlatulencelatulence
•• EpigastricEpigastric painpain
•• DDiarrheaiarrhea
56 J.Daroszewski

Treatment with metformin „start low go slow”
•• Start form a low dose (500 mg) 1x or 2x daily during meals Start form a low dose (500 mg) 1x or 2x daily during meals
(breakfast /supper)(breakfast /supper)
•• In 5In 5--7 days (if not GI side effects) titrate dose to 850 mg or 7 days (if not GI side effects) titrate dose to 850 mg or 1000 mg before breakfast and supper1000 mg before breakfast and supper
•• When GI side effects When GI side effects -- reduce a dose and try to increase in reduce a dose and try to increase in few daysfew days
•• MaMaxximalimal effect can be expected by the dose 2 x 850 effect can be expected by the dose 2 x 850 mg/day, with mg/day, with modermoderaatete increased effect by maximal dose increased effect by maximal dose 3000 mg/day3000 mg/day
Nathan i wsp. Diabetologia 2006 57 J.Daroszewski

Features of oral antidiabetic agents
Metformin SU and glinids
alfa-glucosidase Inhibitors
Glitazons (TZD)
GLP-1 receptor agonists
DPP-IV Inhibitors
HbA1C 1-2% 1-2% 0,5-1,0% 0,5-1,0%
0,5-1,0%
0,5- 0,8%
Fasting Glycaemia
60-70 60-70
20-30 60-70 50 50
Insulin in plasma
Chol LDL
Chol HDL
TG
Body Mas
58 J.Daroszewski

Sulfonylureas (gliclazide, glipizide, glimepiride)
•• Stimulate insulin secretionStimulate insulin secretion
•• Efficient in lowering glycaemiaEfficient in lowering glycaemia
•• ExtraExtra--pancreatipancreaticc action action -- liver, adipose tissue, muscles liver, adipose tissue, muscles (accelerated translocation GLUT(accelerated translocation GLUT--4, increase glucose 4, increase glucose use, use, adiponectinadiponectin ststiimulationmulation in adipose tisin adipose tisssueue))
•• PleiotropicPleiotropic action (antaction (antiitthhromboticrombotic, , fibrfibryynolyticnolytic, , antiantiooxxiidative)dative)
•• Commonly use in clinical practice Commonly use in clinical practice
•• Low costLow cost
59 J.Daroszewski

•• hepatotoxicityhepatotoxicity
•• leukopenialeukopenia
•• anemia anemia
•• thrombocytopeniathrombocytopenia
•• skin skin reactionsreactions
•• hypoglycaemiahypoglycaemia
•• interactionsinteractions: : salicylatessalicylates, , NSAD, NSAD, fibratesfibrates, , betabeta--blockersblockers, , alcoholalcohol
•• increseincrese inin body massbody mass
Sulfonylureas – side effects
60 J.Daroszewski

•• hepatohepatotoxicitytoxicity
•• leukopenia leukopenia
•• anemia anemia
•• thrombocytopeniathrombocytopenia
•• skin skin reactionsreactions
•• hypoglycaemiahypoglycaemia
•• interactionsinteractions: : salicylatessalicylates, , NSAD, NSAD, fibratesfibrates, , betabeta--blockersblockers, , alcoholalcohol
•• iincreasencrease in body massin body mass
Sulfonylureas – side effects
61 J.Daroszewski

Glinids (nateglinid, repaglinid)
•• SSimilarimilar to SU to SU -- anotheranother receptor on Breceptor on B--cellscells
•• ShortShort and and rapidrapid action action –– useuse beforebefore mealmeal
•• SStimulatetimulate insulin insulin secretionsecretion
•• ControlControl postprandialpostprandial hyperglycemiahyperglycemia
•• UseUse inin patientspatients withwith irregularirregular feedingfeeding
•• LowLow riskrisk of of hypoglycaemiahypoglycaemia
62 J.Daroszewski

Features of oral antidiabetic agents
Metformin SU and glinids
alfa-glucosidase Inhibitors
Glitazons (TZD)
GLP-1 receptor agonists
DPP-IV Inhibitors
HbA1C 1-2% 1-2% 0,5-1,0% 0,5-1,0%
0,5-1,0%
0,5- 0,8%
Fasting Glycaemia
60-70 60-70
20-30 60-70 50 50
Insulin in plasma
Chol LDL
Chol HDL
TG
Body Mas
63 J.Daroszewski
Alpha-glucosidase Inhibitors (acarbose)
•• InhInhiibit digestion of carbohydrates in gut and bit digestion of carbohydrates in gut and moderate their absorptionmoderate their absorption
•• Decrease postprandial glycemiaDecrease postprandial glycemia
•• UseUsedd in combined therapyin combined therapy
•• Frequent flatulence and diarrhoea Frequent flatulence and diarrhoea
•• AcarbosAcarbosee 22--3 x times daily (max. 3003 x times daily (max. 300 mg)mg)
•• Start form low dose and titrate weeklyStart form low dose and titrate weekly
64 J.Daroszewski

Features of oral antidiabetic agents
Metformin SU and glinids
alfa-glucosidase Inhibitors
Glitazons (TZD)
GLP-1 receptor agonists
DPP-IV Inhibitors
HbA1C 1-2% 1-2% 0,5-1,0% 0,5-1,0%
0,5-1,0%
0,5- 0,8%
Fasting Glycaemia
60-70 60-70
20-30 60-70 50 50
Insulin in plasma
Chol LDL
Chol HDL
TG
Body Mas
65 J.Daroszewski

Glitazons (pioglitazone, rosiglitazone -Avandia)
• PPAR-γ ligands
• Increase insulin action in adipose tissue and in muscles
• Reduce insulin resistance
• Beneficial effect on lipids
• Combine with MTF and SU
• Don’t use with insulin
66 J.Daroszewski

Controversy concerning glitazons - metaanalyses
• Increased risk of MI (rosiglitazone)
• Increased risk of bone fractures
• Increased risk o cardia insufficincy (rosiglitazone, pioglitazone)
• Acceleration of Graves’ orbitopathy?
67 J.Daroszewski

Features of oral antidiabetic agents
Metformin SU and glinids
alfa-glucosydase Inhibitors
Glitazons (TZD)
GLP-1 receptor agonists
DPP-IV Inhibitors
HbA1C 1-2% 1-2% 0,5-1,0% 0,5-1,0%
0,5-1,0%
0,5- 0,8%
Fasting Glycaemia
60-70 60-70
20-30 60-70 50 50
Insulin in plasma
Chol LDL
Chol HDL
TG
Body Mas
68 J.Daroszewski

Incretin effect
Wartości średnie SE; N = 6; *P .05; 01-02 = czas podawania glukozy we wlewie. Nauck MA, et al. Incretin effects of increasing glucose loads in man calculated from venous insulin and C-peptide responses. J Clin Endocrinol Metab.
1986;63:492-498. Copyright 1986, The Endocrine Society.
Gly
caem
ia (
mm
ol/
l)
time (min)
Pep
tyd
C (
nm
ol/
l)
11
5,5
0
01 60 120 180 01 60 120 180
0,0
0,5
1,0
1,5
2,0
time (min) 02
02
incretin effect
Glucose p.o.
Glucose i.v. *
*
*
*
* *
*
Glucose load orally vs. intraveously
69 J.Daroszewski

Incretin effect in MD2 is blunted
IR=Immunologicznie reaktywna Opracowano na podstawie: Nauck M i wsp. Diabetologia. 1986;29:46–52.
Czas min
Insu
lina
IR, m
U/L
nm
ol/L
0.6
0.5
0.4
0.3
0.2
0.1
0
80
60
40
20
0
180 60 120 0
Control group (n=8)
DM2 patients (n=14)
Czas min
Insu
lina
IR, m
U/L
nm
ol/L
0.6
0.5
0.4
0.3
0.2
0.1
0
80
60
40
20
0
180 60 120 0
Oral glucose load (i.v.) glucose infusion
Incretin effect - physiology Incretin effect in DM2
70 J.Daroszewski

Glucagon-like peptide 1 (GLP-1)
action in peripheral tissues
71 J.Daroszewski
Insulin secretion
Glucagon secretion
Stomach
emptying
Neuroprotection
Appetite
Insulin synthesis
Β cell proliferation
Β cell apoptosis Insulin sensitivity
Cardioprotection
Cardiac output
Gluconeugenesis

Secretion GLP-1 in gut
GLP-1 inactivatiion
MEAL
Native GLP-1
DPP-IV
Rothenberg P i wsp. Diabetes. 2000;49(supl 1):A39.
Incretins are new treatment option in typ 2 DM
GLP-1 deficincy i DM
Quick breakdown of native GLP-1 with
dipeptidylopeptidase IV (DPP- IV)
t½ = 1- 2 min

Dipeptydylopeptidase-IV Inhibitors (DPP- IV) inhibit GLP-1 breakdown
GLP-1 receptors agonists stimulate GLP-1 production, increasing insulin secretion
Secretion GLP-1 In gut
GLP-1 inactivatiion
MEAL
Native GLP-1
Inhibitor
DPP-IV
DPP-IV
Rothenberg P i wsp. Diabetes. 2000;49(supl 1):A39.
Incretins are new treatment option in typ 2 DM

IncretinIncretin agentsagents (i(in n combinedcombined therapytherapy))
GLP-1 receptor agonists (Egzenatide, liraglutide)
DPP-IV Inhibitors (saxagliptin, sita-, vida- alo-)
Gastro-intestinal (nausea,
vomiting)
Gastrio-intestinal neuropathy
Significant not accure
Renal insufficincy
Liver insufficincy
74 J.Daroszewski
SideSide effectseffects::

Lancet Vol 378 July 9, 2011
Drugs targeting β-cell dysfunction New incretin - based treatments Non-incretin - β-cell stimulants
Drugs targeting β-cell dysfunction Drugs targeting β-cell and α-cell dysfunction Insulin-action enhancers Drugs targeting non-insulin-dependent pathways
SGLT2 inhibitors Hepatic targets
Drugs targeting the metabolic syndrome GIP antagonists 11 β-hydroxysteroid dehydrogenase-1-inhibitors
PPAR modulators Drug with unknown mechanisms
Dopamine D2-receptor agonists Bile acid sequestrants
Matabolic surgery

„…„… DiabetesDiabetes affectsaffects 66%% ofof thethe globalglobal adultadult populationpopulation.. ItIt isis aa leadingleading causecause ofof blindness,blindness, heartheart disease,disease, stroke,stroke, kidneykidney failurefailure andand amputationamputation.. EveryEvery year,year, overover 33..88 millionmillion deathsdeaths areare duedue toto diabetes,diabetes, makingmaking diabetesdiabetes aa moremore significantsignificant globalglobal killerkiller thanthan HIV/AIDSHIV/AIDS andand malariamalaria combinedcombined.. EveryEvery 1010 secondsseconds aa personperson diesdies fromfrom diabetesdiabetes--relatedrelated causescauses.. InIn thatthat samesame 1010 seconds,seconds, twotwo peoplepeople developdevelop thethe diseasedisease.
((Prof. Jean Claude Prof. Jean Claude MbanyaMbanya, prezes IDF ), prezes IDF )
76 J.Daroszewski

PrinciplesPrinciples inin treatmenttreatment of of typetype 2 2 diabetesdiabetes
77 i
Dr hab. Jacek Dr hab. Jacek DaroszewskiDaroszewski Department of Department of EndocrinologyEndocrinology, , DiabetesDiabetes
and and IsotopeIsotope TherapyTherapy
[email protected]@umed.wroc.pl