proceedings from hospital kanak-kanak permata · proceedings from hospital kanak-kanak permata 194...
TRANSCRIPT

CONTENT
Page
Proceedings from HOSPITAL KANAK-KANAK PERMATA
Personalised and Precision Medical Care for Children 193
Professor Datuk Dr. A Rahman A Jamal
Controversies in Vaccination 198
Dato’ Dr. Musa Mohd Nordin
Controversies in Vaccination 206
Professor Dr. Sharifa Ezat Wan Puteh
Childhood Obesity and Nutrition 208
Miss Jill Koss
Child Safety 211
Professor Dato’ Dr. Mahmud Mohd Nor
Child and Family Friendly Healthcare 217
Miss Jill Koss

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
193
PLENARY:
PERSONALISED AND PRECISION MEDICAL CARE FOR CHILDREN
PROFESSOR DATUK DR. A RAHMAN A JAMAL
UKM Medical Molecular Biology Institute, Universiti Kebangsaan Malaysia, Jalan
Yaacob Latif, Bandar Tun Razak, Cheras, 56000 Kuala Lumpur, Malaysia
The completion of the human genome project in 2003 has paved the way for a deeper
understanding of diseases at the molecular level. The term genomics medicine has since
emerged as clinicians and researchers capitalized on the knowledge of the genome to
improve the management of many diseases. In the past decade, the term personalized or
precision medicine was introduced to represent the tailoring of treatment to each individual
based on a person’s unique genetic makeup, environment and lifestyle (Hodson, 2016). In
simple terms, it means giving the right treatment to the right patient at the right time with the
right outcome. The concept is not entirely new as in the practice of blood transfusion where
each patient is given the appropriate blood units based on their blood groups. However, the
emergence of genome data has allowed a more comprehensive application of personalized
medicine to make it more precise.
For a long time, doctors have been treating patients with the same disease using the same
approach, the same drugs and the same dose. The outcomes of treatment have strongly
suggested that the individual variation must be taken into account and the one-size fits all
approach is no more valid for many diseases. Studies have shown that anti-cancer drugs are
effective in perhaps 25% of cases only, that 6-8% of patients given medications will have
adverse reactions, that there is a wide variation in response to treatment from one patient to
another despite giving the same dose (adjusted per kg body weight) of the same drug, and
that many non-communicable diseases have the component of gene-environment interaction
in terms of disease pathogenesis.
The advances in genome sequencing technologies, and the cheaper cost, has allowed more
and more patients to be profiled at the molecular level. There are still a lot to be learned but
certainly we know more than before. In the case of cancers, the whole genome sequencing
of tumour tissues has enable us to understand that every tumour has its own molecular
signature which has both prognostic value but also has allowed researchers to identify what

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
194
is termed now as actionable or targetable mutations. The term ‘targeted therapy’, once
labeled decades ago as the magic bullet for the treatment of cancer, is now a reality for
many different types of cancer. Many tyrosine kinase inhibitors are now in the market and
used to improve the outcome of cancer patients.
Many developed nations have already launched big initiatives in precision medicine in the
past 5 years. In 2012, the Prime Minister of UK launched the 100,000 Genomes project in
England. The project aim was to sequence 100,000 genomes which will include cancers,
rare diseases and also pathogens. The project is spearheaded by the National Health
Service (NHS) with extensive collaboration with top university hospitals and the industry.
One of the earliest benefactor of the project was a young girl with a rare disorder. She
presented with a history of seizures and despite many tests and investigations, the doctors
failed to clinch a diagnosis. Whole genome sequencing was performed on her and both
parents. The bioinformatics analysis on the sequence data revealed a deletion in one copy
of her SLC2A1 gene. This gene plays a role in the uptake of glucose into the brain cells. She
was put on a ketogenic diet and her seizures have stopped. This was just one of the many
examples how whole genome or whole exome sequencing has enabled the diagnosis of
many rare diseases and in a proportion of the patients, to identify the specific intervention as
well. It is believed that the approach of precision medicine can solve between 30-40% of rare
diseases.
In the USA, President Obama launched a precision medicine initiative (PMI) in 2015 with a
USD215 million grant, focusing on non-communicable diseases, including cancers, and also
setting up of a Cohort project (Collins and Varmus, 2015). This initiative, similar to the UK
100,000 genomes project, will also performed whole genome sequencing on selected
diseases.
At the UKM Medical Molecular Biology Institute (UMBI), Universiti Kebangsaan Malaysia, we
have already started offering tests for precision medicine. We have recently performed
whole exome sequencing on patients with Pendred syndrome and VACTERL-H syndrome
and discovered disease-causing mutations in the cases (Chow et al, 2017). Our institute is
the first in the country to offer whole exome or whole genome sequencing for rare diseases.
UMBI has also performed whole exome sequencing on hundreds of tumour samples and
some of the results have been published. Our institute has also embarked on whole genome
sequencing of colorectal cancers. This project is the first and largest of its kind in the local
setting.
PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
195
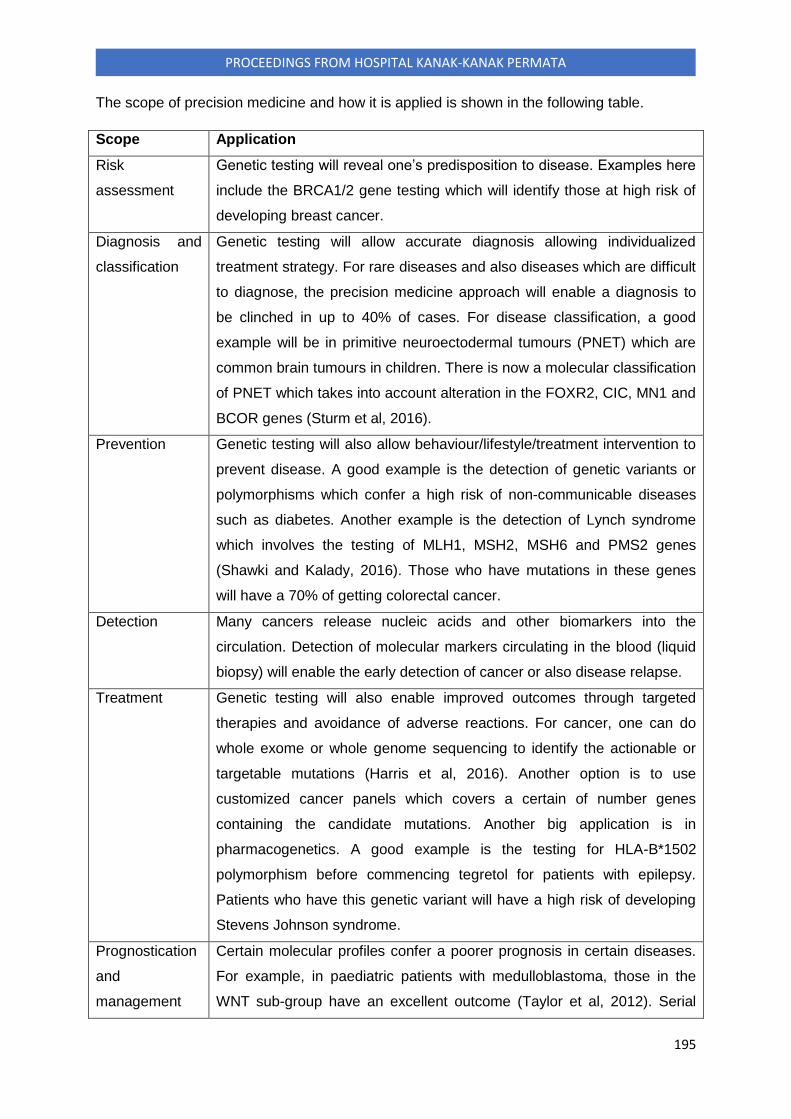
The scope of precision medicine and how it is applied is shown in the following table.
Scope Application
Risk
assessment
Genetic testing will reveal one’s predisposition to disease. Examples here
include the BRCA1/2 gene testing which will identify those at high risk of
developing breast cancer.
Diagnosis and
classification
Genetic testing will allow accurate diagnosis allowing individualized
treatment strategy. For rare diseases and also diseases which are difficult
to diagnose, the precision medicine approach will enable a diagnosis to
be clinched in up to 40% of cases. For disease classification, a good
example will be in primitive neuroectodermal tumours (PNET) which are
common brain tumours in children. There is now a molecular classification
of PNET which takes into account alteration in the FOXR2, CIC, MN1 and
BCOR genes (Sturm et al, 2016).
Prevention Genetic testing will also allow behaviour/lifestyle/treatment intervention to
prevent disease. A good example is the detection of genetic variants or
polymorphisms which confer a high risk of non-communicable diseases
such as diabetes. Another example is the detection of Lynch syndrome
which involves the testing of MLH1, MSH2, MSH6 and PMS2 genes
(Shawki and Kalady, 2016). Those who have mutations in these genes
will have a 70% of getting colorectal cancer.
Detection Many cancers release nucleic acids and other biomarkers into the
circulation. Detection of molecular markers circulating in the blood (liquid
biopsy) will enable the early detection of cancer or also disease relapse.
Treatment Genetic testing will also enable improved outcomes through targeted
therapies and avoidance of adverse reactions. For cancer, one can do
whole exome or whole genome sequencing to identify the actionable or
targetable mutations (Harris et al, 2016). Another option is to use
customized cancer panels which covers a certain of number genes
containing the candidate mutations. Another big application is in
pharmacogenetics. A good example is the testing for HLA-B*1502
polymorphism before commencing tegretol for patients with epilepsy.
Patients who have this genetic variant will have a high risk of developing
Stevens Johnson syndrome.
Prognostication
and
management
Certain molecular profiles confer a poorer prognosis in certain diseases.
For example, in paediatric patients with medulloblastoma, those in the
WNT sub-group have an excellent outcome (Taylor et al, 2012). Serial
PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
196
fluid biopsies and molecular testing can help the active monitoring of
disease response and disease progression.
What will our new UKM Permata Children’s Hospital (UPCH) offer in terms of precision or
personalized medicine? The UPCH will work closely with the UKM Medical Molecular
Biology Institute (UMBI) to develop and offer a wide array of genetic tests at an affordable
cost. UMBI is already offering molecular diagnostic tests for patients with thalassaemia,
cystic fibrosis (yes we do have a good number of cases in Malaysia) and also
pharmacogenetics testing for HLA-B*1502 (Then et al, 2013). UMBI is also already offering
whole genome and whole exome sequencing services to a wide variety of patients including
cancers and rare diseases.
The personalized and precision medicine approach is already driven by the genome
sequencing technologies and also Big Data. As we accrue more sequencing data from
patients, we will learn more about the diseases and potentially this can lead to better
approaches to management.
References
Chow YP, Abdul Murad NA, Zamzureena MR, Khoo JS, Chong PS, Wu LL, Jamal R. Exome
sequencing identifies SLC26A4, GJB2, SCARB2 and DUOX2 mutations in 2 siblings
with Pendred syndrome in a Malaysian family. Orphanet J Rare Dis. 2017. (Accepted for
publication)
Collins FS and Varmus H. A new initiative on precision medicine. N Engl J Med.
2015;372:793-795.
Harris MH, DuBois SG, Glade Bender JL, Kim AR, Crompton BD, et al. Multicenter
Feasibility Study of Tumor Molecular Profiling to Inform Therapeutic Decisions in Advanced
Pediatric Solid Tumors: The Individualized Cancer Therapy (iCat) Study. JAMA
Oncol. 2016;2(5):608-615. doi:10.1001/jamaoncol.2015.5689.
Hodson R. Precision medicine. Nature. 537;S49:doi:10.1038/537S49a
Shawki S, Kalady MF. Recent advances in understanding Lynch syndrome. F1000
Research. 2016;5:2889.doi:10.12688/f1000research.9654.1.

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
197
Sturm D, Orr BA, Toprak UH, Hovestadt V, Jones DT, et al. New Brain Tumor Entities
Emerge from Molecular Classification of CNS-PNETs. Cell. 2016;164(5):1060-72. doi:
10.1016/j.cell.2016.01.015.
Taylor MD, Northcott PA, Korshunov A, Remke M, Cho YJ, et al. Molecular subgroups of
medulloblastoma: the current consensus. Acta Neuropathol (2012) 123:465–472.
Then SM; Zamzureena MR; Azman Ali R and Jamal R. Pharmacogenomics screening of
HLA-B*1502 in epilepsy patients: How we do it in the UKM medical centre, Malaysia.
Neurology Asia. 2013;18:27-29.

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
198
SYMPOSIA:
CONTROVERSIES IN IMMUNISATION
DATO’ DR MUSA MOHD NORDIN FRCP, FRCPCH, FAMM
CONSULTANT PAEDIATRICIAN & NEONATOLOGIST
DAMANSARA SPECIALIST HOSPITAL
MALAYSIA
INTRODUCTION
“Those who do not remember the past are condemned to repeat it” George Santayana
We have now sadly become the victims of our success. Many have forgotten that, not long
ago, diseases like smallpox killed 1 out of 3 patients, while polio caused significant muscle
paralysis leading to breathing cessation. Children had to be placed in dreaded iron lung
chambers to help them breathe, and not many survived to recount their horror.
The global burden of Under-5 deaths was 8.8 million in 2008 (diagram 1) [1]. One child dies
every 20 seconds from a disease preventable by vaccines. To many global health agencies,
this is a preventable human tragedy. Hence, the World Health Organisation (WHO), the
United Nations Children’s Fund (UNICEF) and their global partners have undertaken serious
initiatives in the Expanded Programme on Immunisation (EPI). Approximately 2.5 million
deaths are prevented and 750,000 children are saved from disabilities every year by the EPI.
Vaccine preventable diseases (VPD) are still responsible for 2.5 million under-5 deaths each
year. If the currently available routine and new vaccines are better and more
comprehensively distributed, utilized and outreached to children in developing countries,
there is a potential to save more lives, prevent more disabilities, accrue more societal and
economic benefits and enhance national and global security (diagram 2 and 3) [2].
This will save more lives, further reducing under-five mortality by at least 25% to achieve the
Millennium Development Goal number 4 (MDG4), which is to reduce the under-5 mortality
rate by two-thirds between 1990 and 2015.

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
199

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
200
Diagram 2: Vaccine preventable disease cases and deaths averted in GAVI countries
extrapolated from 2011 – 2020 with universal immunization

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
201
Diagram 3: Immediate and long-term economic benefits in GAVI countries extrapolated from
2011 – 2020 with universal immunization
RESURGENCE OF VACCINE PREVENTABLE DISEASES
The decades of efforts by international agencies, governments and NGOs however, have
been hampered by the anti-vaccination movement of late. Unfortunately, a small number of
physicians support this movement, buoyed by the vast majority comprising individuals or
small groups of varying backgrounds who create noise through social media and blogs.
Virtually all of their opposition of vaccine is based on emotions, personal experiences and
quoting “anti-vaccine gurus” on social media who do not conduct research but thrive on
writing blogs for conspiracy theory websites. Realising they have insufficient data to prove
their allegations, these conspiracy theorists utilise emotional testimonies and
unauthenticated sweeping statements as their strategy.
There is virtually no credible research or studies from the anti-vaccination group. Many of
them quote blindly Wakefield’s study that linked the MMR (Measles, Mumps & Rubella)
vaccine with autism, which has since been withdrawn from the Lancet when it was

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
202
discovered that it was flawed and fraudulent [3]. The study raised great fear among parents
about MMR, leading to a significant decline in the coverage of MMR vaccination in many
countries. The US which had eliminated measles in 2000 is now suffering its worst measles
epidemic in 20 years. The Disneyland measles outbreak in 2015 spread to 24 states,
Canada and Mexico [4]. In the 2011 measles outbreaks in Europe, there were over 30,000
cases, 7 deaths, 27 cases of measles encephalitis, and 1,482 cases of pneumonia. In
Malaysia, there was a threefold increase in measles cases in 2015 compared to the previous
year, with 2 deaths.
The World Health Organisation (WHO), Centre for Diseases Control and Prevention (CDC)
and other global health agencies have unequivocally stated that MMR and all vaccines have
no link whatsoever with autism or other similar neurological disorders [5,6]. All parents and
guardians should feel totally reassured by this and not be influenced by anti-vaccine news
on social media.
VACCINE SAFETY CONTROVERSIES
Any medical intervention is bound to be associated with some degree of risks. The potential
adverse effects of immunization must be carefully weighed against the numerous individual,
societal and economic benefits accrued from the WHO Expanded Program of Immunisation.
It is not logical to avoid any form of medical intervention solely because one elect to avoid
risks. This paradigm of thought which is propagated by the anti-vaccine groups is incoherent
and irrational because doing nothing is also associated with risks, namely the increased risk
of acquiring VPD which can lead to outbreaks of epidemics and pandemics of diseases,
increased and prolonged hospitalisations, increased utilization of expensive treatment,
increased deaths and increased physical and intellectual disabilities.
It is like suggesting to us not to eat breakfast because 250 choke on their breakfast and die
each year or not to take our daily baths because 350 drown and die in the bath-tub each
year, which is quite obviously absurd! [7] The benefit risk ratio favours these daily acts of
living and that is why we continue to eat breakfast and bathe ourselves.
Similarly, the benefit risk ratio unequivocally favours the act of immunization. Our children
and our society enjoy monumental benefits compared to the small risks associated with
vaccinations. The common side effects associated with immunisations are pain, redness
and swelling at the injection site which often go away quickly, which may be considered as

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
203
mild and transient only. Serious side effects following vaccination, such as severe allergic
reactions, are extremely rare [8].
MISPERCEPTON ABOUT PARENTAL RIGHTS
The health care professional may have the greater knowledge of vaccine preventable
diseases, of possibilities, risks, treatment, outcomes and the options of prevention with
immunisations. Nonetheless, the principle of autonomy respects and values the individual (or
the parents or legal guardians) as the one who makes the self-defining choices upon which
he then acts and for which he is accountable.
The principle of individual autonomy however needs to be considered within the context of
the wider public interest and benefits. It is this vein that medical interventions, such as the
global immunization programs that have been proven to promote and protect the general
health and well-being of the public have priority over the considerations of the individual
interest.
Another important moral consideration is to ensure that the individual choices one makes
does not harm others. Those who do not immunize against VPD are at increased risk of
being infected. They therefore might pass on the infection to others, who may then be
harmed! Almost all of those infected with measles in the US, Europe and Malaysia outbreaks
were in the unvaccinated persons [9].
The omission to vaccinate has obviously impacted negatively on the well-being of the public,
which would be enough arguments for policy makers to impose an obligation to act. The
recent Australian “no jab, no pay” policy, plans to withdraw childcare and welfare benefits
from Australian parents who refuse to vaccinate their kids. Thus, parents who decide against
immunisations could be up to $15,000 worse off per child.
If sufficient numbers of people in a community are immunized, usually in excess of 80%,
then the protection against VPD is conferred to virtually all persons in the community. This is
known as herd immunity. This community immunity offers protection to vulnerable segments
of the community who cannot be immunized due to various reasons e.g. too young, have
cancers, have HIV/AIDS, are on chemotherapy or radiotherapy. The common good of the
community is served which extends beyond the individual. In addition, the community
benefits from the economic savings and improved security as a result of the immunization
programs [10].
A growing number of Muslim parents have fallen prey to the “anti-vaccine” camp. Some
believe that immunisation is part of the western or Zionist scheme to weaken Muslims and
undermine the health of their progeny. Others are led to believe that there is non-halal (non-
PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
204
permissible) substances in vaccines. Both groups are victims of misinformation. Muslim
scholars around the world have unanimously proclaimed that the Higher Objectives of the
Islamic Jurisprudence (Maqaasid Shariah) is the promotion of the common good and benefit
(maslahah) and the avoidance and protection from harm (mafsadah) towards the
enhancement and preservation of justice (adalah) and the welfare and wellbeing of the
community (ummah) [11].
RELIGIOUS MISINTERPRETATIONS
According to the Muslim scholars, the Quran and authentic traditions (hadiths) give utmost
priority to prevention and protection against all forms of personal and social misconduct [12].
In the context of health, it prioritises the golden rule that “prevention is better than cure”.
Immunisation enhances the immune system of a child and the effectiveness of vaccines has
been scientifically demonstrated in global immunisation programmes. The widespread use of
the smallpox vaccine has led to its eradication in 1980. The last few cases were from two
Muslim countries - Bangladesh and Somalia. Polio has been eradicated from most parts of
the world, but remains endemic in two Muslim countries - Afghanistan and Pakistan [13].
This, unfortunately, is due to conservative and ill-informed Muslim scholars who advised
against immunisation.
Immunisation exhibits all the hallmarks of a preventative health strategy that has saved lives
and prevented intellectual and physical disabilities. True to the principles of Islamic
jurisprudence (sadduz- zaraik), it has closed avenues to inflict harm, damage and
destruction. All the vaccines in the National Immunisation Programme (NIP) have been
scrutinised by experts in jurisprudence (JAKIM and the National Fatwa Council) and Science
(Ministry of Health), leaving no question of their efficacy, safety and permissibility (halal).
The global Expanded Program of Immunisation has been shown and proven to be a very
safe, effective and cost savings global child survival strategy. With the exception of clean
drinking water, immunisation is the most powerful public health intervention program. We
should therefore not be gullible nor easily persuaded by various irresponsible groups which
spread rumours in the various media that immunization is harmful, not effective and
irreligious.

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
205
REFERENCES
1. Black RE et al. Global, regional, and national causes of child mortality in 2008: a systematic
analysis. Lancet 2010 Jun 5;375(9730):1969-87
2. Stack ML, et al. Estimated Economic Benefits During The 'Decade of Vaccines' Include
Treatment Savings, Gains in Labor Productivity Health Affairs 30, no.6 (2011):1021-1028
3. The Editors of the Lancet, Feb 2, 2010. RETRACTED: Ileal-lymphoid-nodular hyperplasia,
non-specific colitis, and pervasive developmental disorder in children
4. MMWR. April 17, 2015
5. http://www.who.int/vaccine_safety/committee/topics/mmr/mmr_autism/en/
6. http://www.cdc.gov/vaccinesafety/concerns/autism.html
7. Paul AO, Louis MB. What every parent should know about vaccines. Macmillan USA. 1998
8. Alain Joffe. Anaphylaxis after vaccination is rare. Reviewing McNeil MM et al. J Allergy Clin
Immunol 2015 Sep 28. http://www.jwatch.org/na39392/2015/10/23/anaphylaxis-after-
vaccination-rare#sthash.l033ezuu.dpuf
9. 9. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6047a1.htm
10. Musa MN, Siti AI, Chan LJ. Immunisation controversies. What you really need to know.
August 2015
11. Shari’ah Intelligence. The basic principles and objectives of Islamic jurisprudence. Islamic
Education Trust Nigeria. 2015
12. Federation of Islamic Organisations in Europe: European Council for Fatwa & Research.
http://euro-muslim.com/en_u_foundation_details.aspx?news_id=343
13. http://www.polioeradication.org/Dataandmonitoring/Poliothisweek.aspx

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
206
SYMPOSIA:
CONTROVERSIES IN VACCINATION
PROF DR SHARIFA EZAT WAN PUTEH, MD, MPH, PhD
Head, Community and Industries Liaison Office
Faculty of Medicine and HCTM
PPUKM
Vaccine is one of the most cost effective and important measure to control vaccine
preventable diseases. It has contributed to reduced mortality, increased life years and
increased QoL amongst children and nations citizens. Vaccines are not cheap and are most
effective if coverage is high and proper targeting are available. Below are a few
controversies related with vaccines.
1. Relationship of MMR and Autism
The issue of Dr. Andrew Wakefield, a gastroenterologist in the UK, postulate the ‘leak-gut’
theory. However similar investigation with a larger sample failed to reveal persistence of
measles virus nucleic acids. The Lancet formally retracted the study in February 2010 and
The Institute of Medicine (IOM) has concluded no evidence.
2. Thimerosal in onset to Autism
Mercury-based preservative, used for decades in United States in multi-dose of medicines
and vaccines. No harm by the low doses, except for minor reactions like redness and
swelling. However, in July 1999, the Public Health Service agencies, the American Academy
of Pediatrics, and vaccine manufacturers agreed that thimerosal should be reduced or
eliminated in vaccines. With the exception of some in influenza vaccines, none of the
routinely recommended pediatric vaccines contain thimerosal as a preservative.
3. Moral & religious concerns.
Some parents have refused certain vaccinations for their children based on religious
objections. The moral opposition is due to the cell lines in which vaccine viruses are grown
from ‘non halal’ materials such as from aborted fetuses. Also some vaccines (e.g. the HPV

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
207
vaccine) promotes fradulent sexual practises. Used widely by anti-vax movements, as
reasons not to be vaccinated against sexual disease prevention.
4. Nervous system disorders: encephalopathy
Whole-cell pertussis vaccines in the 1940s marked the beginning of a dramatic decrease in
the morbidity and mortality associated with Bordetella pertussis infection. A controversy was
ignited by a study published in 1974 suggesting neurological complications associated with
the pertussis vaccine. A case–control study entitled the National Childhood Encephalopathy
Study (NCES) was conducted in the UK from 1976–1979, that suggested that the risk of
permanent brain injury from pertussis vaccination was extremely low (1 in 300,000).
5. An overwhelmed or healthy immune system?
The number of recommended childhood vaccines has increased exponentially in the last 50
years. A fully immunized child by the age of 2 years will have received 14 different vaccines
and up to 26 injections. Refusal leads to breadown of herd immunity, outbreaks and deaths.
A study in Sabah showed, the highest defaulters was DPT OPV Booster 56.6%, MMR
(43.4%), DPT-Hib/ OPV and Hep B 3rd dose (37.7%), and this is among employed mothers
with big family size are at higher risk.
Conclusion
If controversies and anti-vax movements are uncontrolled, vaccine preventable diseases
may resurge or occur again. Society needs to identify why certain communities/parents
refuse to get vaccination. We also need to deal with vaccine controversies in optimal manner
and cannot just depend on scientific preaching only. More ‘holistic’ response are needed
from religious teachers, preachers, school teachers, neighbor hood watch etc.
Keyword: Vaccines, controversies, autism, defaulters, herd immunity

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
208
SYMPOSIA:
CHILDHOOD OBESITY AND NUTRITION-PSYCHOSOCIAL IMPLICATIONS
MISS JILL KOSS, MS, CCLS*
COOK CHILDREN’S MEDICAL CENTER
FORT WORTH, TEXAS, US
Obesity in children has become a complex public health issue reaching, what some would
call, a worldwide epidemic. In the US, the Center for Disease Control’s most recent figure
says that 17% of children ages 2-19 years are obese, which is approximately 12.7 million
children/youth. (www.cdc.gov) Obesity is also complex because it is an interaction between
physiological and psychological factors, is it nature or nurture, or both? As well, there is still
the question as to whether obesity leads to mental health issues, or mental health issues are
causal for obesity. (De Niet & Naiman, 2011). Research demonstrates no clear answer to
that question.
While there are multiple health/medical complications for children and youth who are obese,
the psychological issues are real and immediate risks for these children. Addressing the
psychosocial aspects of the problem is essential, and weight loss programs will fall short if
they do not include that aspect of care. While much research has been conducted to better
understand the psychosocial concerns for children, who are obese there are conflicting
results in terms of inconsistent findings which provides a challenge in addressing potential
psychosocial and emotional needs. (Young-Hyman, et al, 2006) (Strauss, et al, 2000)
(Griffiths, et al, 2010)
When defining psychosocial/emotional aspects, a list of identified concerns includes
depression, anxiety, lower self-esteem and self-image, bullying and stigmatization, body
image/dissatisfaction, lack of social skills, and decrease in quality of life (De Niet & Naiman,
2011). There is a plethora of research that demonstrates children who are obese are bullied
and stigmatised which predicts children’s negative evaluation of body and self (Cinelli
&O’Dea, 2016). Based on these findings, it’s important to note that not all children who are
obese have the same set of psychological or psychosocial issues, and should not be
PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
209
stereotyped into a singular category of concerns. It takes assessing each child uniquely to
determine how best to support their weight loss plan.
Dr. Robert Pretlow (2010) has identified what he calls vicious cycles or circles that kids get
caught up in which prohibits them from moving forward with weight loss. Cycles in which the
situation contributes to the cause of the situation itself, thus making the situation continue
without resolve. These cycles revolve around some of the psychosocial issues already
identified, such as self-esteem and stress; but, they also highlight several other keys areas
that don’t stand out prominently in the literature, such as boredom and willpower. Several
key relationships are uncovered within these cycles, as well. Stress eating is a displacement
activity, and allows for removing the stressor, but not resolving it. Comfort eating provides
emotional numbing in the face of rejection and bullying. Boredom is associated with
feelings of helplessness and manifests in sadness, depression, anxiety and emotionally
detaching from life. Self-esteem is not caring about how one looks because you’ve given up.
Two other aspects that need to be understood are parental issues, as well as healthcare
provider issues. Parents seem to fall into to two categories; they are either very critical and
shame their child who is obese; or, they use food as a love language, and are the ones
providing the food. This enabling is probably the hardest to resolve because it has more to
do with the parent’s emotional needs which supersede the best interest of the child.
Research does demonstrate that parents and families should be included in all weight loss
interventions. Parents need to understand and be on board with a focus on healthy self-care
in order for the child to feel supported not victimized (Cinelli & O’Dea, 2016).
Healthcare professionals may unwittingly be contributors to an unhealthy cycle of being
overweight. ‘So many of these kids are in real pain – emotional, physical, and perhaps even
spiritual. I often wonder about the iatrogenic [provider-caused] effects of their contact with
health-care providers and obesity researchers, who have sub-optimal training or experience
in this area. Such persons may play the blame-game without adequately utilizing a problem-
solving approach to holistic management and support.’ (O’Malley, 2008).
Stopping a cycle takes perseverance, strength and support. In Pretlow’s program, he has
the advantage of thousands of comments, stories, and testimonies from obese children and
youth. In very real terms, they honestly share what has not worked and even made things
worse, to sharing stories of weight loss success. In thinking about interventions which will
help stop a cycle, it’s worth remembering that weight is not a behavior, and therefore is not
PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
210
an appropriate target for behavior modification. Interventions that have the strongest
potential to be effective are those that develop coping skills, enhance positive self-esteem,
and build resiliency. They are interventions that do not focus on weight loss, but rather on
positive change and motivation. Research demonstrates that children successfully lose
weight when the focus is on ‘fun’ not weight loss (Watson, et al, 2016). This study also
found that motivation for engaging in the fun could start as extrinsic, but it was most effective
for weight loss when the motivation became intrinsic. Connection with others was an
important part of the fun, finding relatedness with other children who were as equally
engaged in the activity.
As part of any weight loss program, a strategic intervention designed to align with the above-
mentioned focus starts with developing motivation, understanding the reason why the child
wants to lose weight. If there is no internal motivation with a reason for moving forward,
there will be limited success. Once a reason has been identified and owned, the next step is
to make a plan, which includes some of the following as a focus for supporting psychosocial
needs:
Create a support network for accountability
Become aware of what they feel when they seek food
Identify alternatives to eating – activities to participate in
Exercise – make it fun and with friends
Cope with life without using food
Become a helper
There are a multitude of interventions for all age groups, specifically designed to develop
coping skills, enhance natural resiliency, and promote positive self-esteem. Tapping in to
inherent strengths that kids already have plays an essential role in a successful plan.
A harsh reality about children and youth who are obese is that they sit on the sidelines and
avoid things in life because of their weight. It keeps them from fully enjoying life, so they turn
to food for happiness. That shouldn’t be any child’s reality. Healthcare professionals
working with children and youth who are obese will benefit their patients by focusing on
positive motivation, and including interventions which will help them successfully navigate
through weight loss.

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
211
WORKSHOP:
CHILD SAFETY- OUTSIDE AND INSIDE HOSPITALS
*PROFESSOR DATO’ DR. MAHMUD MOHD NOR
*President, Child friendly Healthcare Association of Malaysia
MBBS (Mal) FRCS (Edin) FRCS(Glasgow) FAMM
Professor of Surgery, Universiti Sains Islam Malaysia
Adjunct Professor of Surgery, Universiti Kebangsaan Malaysia
Introduction
To be safe is a universal human right. Competent adults under most circumstances are
expected to be capable of looking after their own safety and the safety of their families and
those under their responsibility to care. Children on the other hand have varying degrees of
competency depending on age to ensure their own safety. Children around the world are
subjected to different types of injuries and risks of injuries but all children rich or poor living in
the developed or under developed world have the right to grow up healthy and safe. It is thus
the responsibility of those caring for children to ensure the safety of children under their care
in these different and varied environment or circumstances. When a child dies, or sustains
serious injuries often leading to long term consequences the lives of families and community
can be severely affected and changed.
Magnitude of the problem and places where injuries occur
Unfortunately, the actual magnitude of the problem is not well documented except for some
developed countries. According to an organisation SAFE KIDS Worldwide based in USA it is
estimated that a million families lose a child to a preventable injury every year around the
world. It is the number one killer in the United States and it is estimated around the world
that a child dies from an unintentional injury every 30 seconds and millions of children are
injured in ways that can affect them for a lifetime. The injuries are sustained at home,
outside the home on roads, in vehicles, schools, playgrounds, child care centres, hospitals
and other places that are sometimes not expected for injuries to occur. Injuries suffered by
children can be truly accidental but often they are due to ignorance or negligence on the part
of those responsible for the safety of the child. Accidental injuries including drowning are the
leading causes of death in children ages 18 and younger. Those who survive with severe

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
212
injuries may be left with varying degrees of disabilities for life. In addition to these cases of
accidental trauma there are also increasing numbers of non-accidental trauma (NAT)
similarly leading to death and disability. Unfortunately, some are deliberately harmed by
those who are supposed to care for them at home. Non-accidental trauma as it is known is
also becoming a problem of increasing concern. In the USA, it is said to be the leading
cause of death for traumatic injury in childhood. There is substantial cost incurred to care for
all these children especially those that require long term care and rehabilitation.
In Malaysia, non-accidental trauma only reached public awareness in 1989 following the
death of a severely abused child. National data are collected by various agencies and it can
be assumed that there are many instances of under reporting. However, there is a trend of
increasing number of cases reported to the Social Welfare Department every year from
1,149 in 1997 to 3,257 in 2010
There are other causes of preventable injuries or harm to children. This can occur in the
health care setting. There are estimates of such harms in hospitals for patients worldwide
especially in the developed countries. It is estimated that in the United Kingdom one in ten
patients will experience some form of harm during their stay in hospital. Medicare USA
estimates 13.5% of its hospitalised patients suffer adverse events. Worldwide it is estimated
that one in ten patients experience preventable harm while in the hospital. The magnitude of
the problem especially in children however is not well documented as a separate entity. This
may be attributed to under reporting.
Child safety in healthcare facilities
Safety can be defined as the avoidance, prevention, detection and amelioration of adverse
outcomes of physical and psychological injuries. Safety is therefore part and parcel of
Quality Healthcare Delivery. Patient safety includes:
i. Freedom from physical danger or risks
ii. Avoiding harm or minimizing harm if unavoidable
iii. Includes psychological harm
iv. Early detection of harm or adverse outcomes
v. Rapid intervention to deal with and ameliorate harm
vi. Supporting staff involved (second victim)

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
213
Potential sources of danger in the healthcare environment
It must be recognised that a health facility like a hospital has an environment that is
potentially dangerous. This is in relation to the design of the physical structures including
building materials used for the walls and floors that are not child friendly. Some other
potential sources of dangers for children in hospitals include:
i. Equipments like lifts, incubators, ventilators
ii. Medical procedures and processes
iii. Transportation facilities and equipments
iv. Special facilities e.g. Operating Theatres, Intensive care units, Special care
nursery and Radiology
v. Playgrounds and playroom toys
Special needs and consideration for children in a health care setting
The World Health Organisation (WHO) has defined health not only as physical health but
linking health to wellbeing, in terms of “physical, mental and social well-being, and not
merely the absence of disease and infirmity”.
The World Health Organisation in a Report of a Commissioned Study stated that
“There is a clear lack of awareness in surprising large number of Hospitals of the special
need not only to cater for children’s technical, medical and nursing needs, but also to
minimise the adverse effects of being separated from their families and exposed to
frightening experience that are all too often magnified by the child’s lack of forewarning”
Therefore, in terms of the health needs of children in hospitals in addition to their physical
well-being and cure of their ailments the psychological effect and trauma of children must be
well managed. Children must be in an environment that also prevents or reduces emotional /
psychological harm which may result in a permanent scar with lifetime consequences.
Physical pain and frightening experiences while in a health care facility must also be
addressed adequately with competence so as to minimise the adverse psychological harm
to the child which may have long term consequences.
The requirements for safety in hospitals
Uppermost in patient safety is the availability of competent health human resources in every
category of staff. Medical and Allied Health personnel at undergraduate and post graduate

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
214
levels must be in accredited programs to ensure their quality and competencies are at the
appropriate level. Personnel caring for children must have the training and skills to
appropriately respond to the needs of children.
Health care facilities must be safe with well-designed infrastructures including buildings, safe
equipment and facilities for treatment.
To ensure continuing improvements in the quality of care there has to be good governance
and systems of healthcare delivery. Managers must instill the culture of patient safety and
continually promoting quality improvements efforts. Health care personnel must be educated
throughout the continuum of education in patient safety to reduce medical errors and
psychological harms
The health care facility must be accredited by an appropriate authority to ensure compliance
to quality standards and criteria. For children, special quality standards must be formulated
and complied.
Authorities established to ensure quality in the delivery of Health care in Malaysia
1. Malaysian Qualification Agency
Peculiar to the Malaysian scenario, by the enactment of the MQA act 2007 programmes of
higher educational institutions (HEI s) leading to professional qualification require that
accreditation be done by or in close collaboration with professional bodies established under
various Acts of Parliament to regulate the profession and ensuring quality of medical
personnel.
2. Malaysian Medical Council
The Malaysian Medical Council established under the Medical Act 1971 performs a licensing
and regulatory role. It institutes disciplinary action for breaching code of professional conduct
or failure to provide and maintain good standard of care to patients. It also develops
guidelines on good medical practice.
3. Malaysian Society for Quality in Health
The Malaysian Society of Quality in Health established in 1997 accredits hospital including
compliance to safety standards. At the moment accreditation of hospitals is voluntary and is
not a requirement under the law. This is the negative aspect of the current situation as this
has not enabled all hospitals to be compelled to comply with the quality standards and to
ensure processes for patient safety are put in place while they undergo treatment in the
medical facilities.

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
215
4. Child friendly Health Care Association
In 2001 The Child friendly Healthcare Association of Malaysia was established to address to
the special needs of children in a healthcare setting. The child friendly health care facility
initiatives seek to develop a child- sensitive approach that recognises the special psycho-
social, developmental and physical need of the child. Twelve standards with criteria for
compliance were developed. Although the emphasis was on the psychosocial aspect of
patient safety, physical safety was also encompassed in the standards. The standards were
submitted to the Ministry of Health to be implemented in the Ministry of Health hospitals and
to the Malaysian Society for Quality in Health to include them in their quality standards.
In addition to complying with the Child friendly health care standards it was hoped that in the
near future all hospitals and healthcare facilities will be required to undergo compulsory
accreditation to improve the quality of care so that more lives can be saved from accidental
injuries and medical errors.
5. Malaysian Patient Safety Council
This was established in 2003 following a Cabinet directive to advise the Minister of Health on
situation of preventable adverse events and measures to overcome them. The council is
also responsible to promote systemic improvements in safety and quality of healthcare in
Malaysia. Another important function of the council is to devise strategies to improve safety
and quality of care and publish reports on adverse incidents and patient safety. These
incidents are to be used for educational purposes to avoid similar incidents in future.
What needs to be done to improve child safety?
1. There must be greater effort taken to establish mechanisms to obtain reliable data to be
used to create greater awareness among Malaysians regarding the magnitude and
seriousness of the problem of preventable injuries and harm among Malaysian children.
2. More efforts must be taken by nongovernmental organisations and civil society to
disseminate information to the public regarding child safety and to undertake programmes to
educate the public on the importance of child safety.
3. Engaging corporations, foundations, governments for funding to support educational
programmes to families and general public to create safer environments at home and places
frequented by children.
4. Researching into the types of injuries causing the most harm in the community and
recommends appropriate interventional measures to prevent them from happening.

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
216
5. Advocating appropriate laws and regulations for better child safety.
Conclusion
Preventable injuries either accidental or non-accidental are a major cause of death and
disabilities in children all over the world. A more concerted effort must be undertaken in view
of its global epidemic proportion. Families and the public in general are ignorant or do not
have access to information or resources they need to keep their children free from all kinds
of injuries that may result in tragedies.
International collaboration is required to address this very important malady which is entirely
preventable with the right approach and the appropriate resources made available to combat
this global epidemic.
References
National Action Plan for Child Injury Prevention, Apr 30 2016, Injury is the # 1 killer of
children and teens in USA in 2009, Centers for Disease Control and Prevention.
10 leading causes of Injury Deaths. Unintentional Injury Deaths USA 2010, Centres for
Disease Control and Prevention.
Why Injury Prevention Matters, Safe Kids Worldwide.
C.Henry Kempe, M.D et.al The Battered- Child Syndrome, JAMA 1962;181(1);17-24.
Asvall JE. Forward to “Care of Children in Hospital” by Else Stenbak. Report of the WHO
Regional Office for Europe commissioned study into care of children in selected hospitals in
9 European Countries. WHO 1986 ISBN 92 890 10339.
UN Convention on the Rights of the Child 1989.
Total Cases of Child Abuse and Neglect Reported to Department of Social Welfare 1997-
2010. Department of Social Welfare, 2011.
Guidelines for Child Friendly Healthcare, Malaysian Child Friendly Health Care Association.
Malaysian Qualification Agency Act 2007. Malaysian Medical Council, Medical Act 1971.
Malaysian Hospital Accreditation Programme, Malaysian Society for Quality in Health.
Malaysian Patient Safety Council.
PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
217
WORKSHOP:
CHILD AND FAMILY FRIENDLY HEALTHCARE
MISS JILL KOSS MS, CCLS*
COOK CHILDREN’S MEDICAL CENTER
FORT WORTH, TEXAS, US
“We owe it to the future not to harm our children in their hearts and minds while we cure their
diseases and heal their broken bones.”
A Quiet Revolution
Starting several decades ago, countries like the United States, the United Kingdom and
others began to gradually address some of the psychosocial and emotional needs of
children, as well as the respect and partnership needs of their families in the hospital setting.
This initiation of child and family-centered healthcare was greatly impacted by the 1989
United Nations Convention on the Rights of the Child (UN-CRC), as that document
established the base premise that, in all situations, the best interests of the child should be a
primary consideration (art.3). These standards set a clear path for the protection of
children’s rights in relation to health care, education and legal, civil and social services,
fifteen of which are directly related to health care (www.ohchr.org). Multiple initiatives across
the globe continue to be created to address the psychosocial, psychological, social and
developmental needs of children based on these standards.
Currently there are several international organizations specifically promoting child and family
friendly health care in response to the UN-CRC standards. The European Association for
Children in Hospitals (EACH) is the umbrella organization for member associations involved
in the welfare of all children before, during or after a hospital stay. The member associations
of EACH, of which there are 15, aim to have the principles of the EACH Charter incorporated
in health laws, regulations and guidelines in each European country. (www.each-for-sick-
children.org). The Council of Europe has established Guidelines on Child-friendly Health
Care as an integrated approach to place children’s rights, needs and resources at the center
of all health care activities. (www.COE.INT).

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
218
The United Kingdom created the Child Friendly Health Care Initiative in response to the
UNCRC to address the physical, psychological, and emotional needs of children and their
families. “While there have been improvements in some clinical treatments, a visit to
hospital or clinic is still a frightening and traumatic experience for many children and their
families across the world.” (www.childfriendlyhealthcare.org). The focus for this initiative is
three-fold:
Reducing fear, anxiety and suffering in children and families
Improving their overall experience of health care
Improving mortality and morbidity
Both of these organizations follow 12 set standards based on the UN-CRC:
1. Children will be admitted to and kept in an in-patient health facility only when this is
in their best interests.
2. The highest attainable (best possible) level of care, evidence based when possible, is
provided for them and for pregnant women.
3. The environment in the health facility is secure, safe and clean.
4. The resources and expertise are available to provide separate, age-appropriate care
in partnership with parents in child friendly surroundings.
5. They and their parents/carers are kept consistently and fully informed and involved in
all decisions affecting their care.
6. They have equal access to health services and are approached without
discrimination as individuals, with their own and developmentally appropriate rights to
privacy, dignity, respect and confidentiality.
7. Their physical and psychological pain and discomfort is assessed and controlled.
8. When they are severely ill, undergoing surgery, or have been given systemic
analgesia and/or sedation, trained health workers and the necessary resources are
available to provide appropriate critical and emergency care.
9. They are able to play and learn when attending a health facility.
10. They are protected from child abuse by appropriate and clearly defined systems, and
are supported by health workers familiar with its signs and symptoms.
11. Their health and the health of pregnant women is monitored and promoted.
12. Breastfeeding is supported and optimal nourishment is provided by the promotion
and practice of globally acceptable feeding programmes.
How then are we to understand the application of these standards into the routine practices
of healthcare institutions? It takes understanding the impact of the environment on children
and families, identifying their unique needs, and providing interventions and services that

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
219
begin to meet those needs. If healthcare professionals and institutions are to be child and
family friendly, or centered, practice and policy must be ready to meet children and families
where they are.
Children’s Understanding and Experience of Healthcare:
A Developmental Perspective
The impact of injury, illness and hospitalization may be best understood by looking through
the lens of developmental theory. Drawing from the work of Erik Erikson (1963), theorist for
Psychosocial Development; Piaget (1962) whose theory focuses on Cognitive Development;
Bowlby (1973), identified with Attachment Theory; and Bandura (1977), theorist on Social
Learning, we begin to see the impact of the healthcare environment on development, learn
to identify the main stressors and fears experienced, and understand the behavioral
responses to those stressors. There are strategies specific for each group that have been
identified that will improve a child’s overall experience of healthcare. It should be noted that
when talking about development, there are no specific age limits, but broad age ranges.
Children may respond typically for a particular stage of development, but they can also
regress to an earlier stage of development when faced with stressful situations that are
overwhelming.
Infants
The goal for infants (ages 0 – 12 months) is the development of a relationship where basic
needs are met and security is given. The psychosocial/emotional stage is about learning to
trust their environment versus mistrusting. The hospital setting can be very challenging for
infants to be successful in the developmental stage. Stressors for infants in the hospital are
separation from primary caregiver, change in routine for eating and sleeping, lack of
developmental stimulation, pain, and parent anxiety to name a few. The impact of these
stressors can lead to responses such as being difficult to console, inconsistent use of self-
soothing behaviors, decrease in appetite, change in sleep patterns, crying, and disinterest in
environment. Strategies which promote better coping with stressors are parent presence,
adequate pain management, sensory stimulation, and consistency in daily routine.

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
220
Toddlers
The concept of autonomy versus shame and doubt in toddlers (ages 1-3 years) focuses on
developing a sense of independence and being able to do things for themselves while not
being shamed when trying new skills. In the hospital setting, toddlers can be very
challenging because of this growing sense of autonomy with little ability to self-control.
Stressors can then be loss of control and mobility, stranger anxiety, separation from primary
caregiver, pain, and inability to cope with overwhelming feelings. Behavioral responses to
these stressors are often being clingy and whiney, physically acting out and actively
resisting, and regression. Developmental strategies which can be utilised with this age
group are allowing for choices whenever possible, encourage parental presence, give
opportunities for play in a safe environment, and promote non-pharmacological pain
management.
Preschool/Young School Age
The developmental challenge for preschool/young school age (4-6 years) comes with an
increased ability for initiative to start new things independently and make their own choices,
but have the capacity to worry about doing it right. Challenges for the hospital setting relate
to a preschooler believing they are sick or in the hospital because they are being punished,
as their egocentrism has them at the center of all that happens to them. Main stress points
relate to loss of independence and control, as well as separation from primary caregiver.
Responses related to these stressors can be regressive behaviors, aggression and acting
out, becoming overly dependent on primary caregivers, and not eating or sleeping well.
Strategies which can promote normalisation of the environment are clarifying
misconceptions, setting limits, including them in their own care, providing safe spaces and
play, and encouraging them to express their feelings.
School Age
School age children (ages 7 – 12 years) are at the stage of being industrious while still
having feelings of inferiority. They have the capacity to understand most medical diagnoses
and treatments, can follow plans of care, and be responsible for much of their own care
while in the hospital. The stressors that can accompany this age group are separation from
peers and family, not fitting in and looking different, pain, and lack of structure, as they are
used to being in a school setting. The responses most likely to these stressors are
regressive behaviors, acting out, decrease in self-esteem, and either constantly asking
PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
221
questions, or never asking questions. The strategies most beneficial for decreasing stress
are to include them in decision making, provide developmentally-appropriate information,
encourage questions, provide structure through limit setting, encourage participation in
group activities, and to allow them to participate in their own care.
Adolescence
Adolescents (13 – 18 years) are not quite young adults even though they would often like to
consider themselves as such. They are still in the developmental stage of figuring out who
they are, establishing their identity, while in the midst of so many related pressures – family,
peers, school, etc. They have the capacity to understand diagnoses, treatments, and
outcomes, and should play a major role in making decisions about their medical care. The
healthcare experience can be very stressful for this age group as they are separated from
their peers, faced with body image issues, decrease in self-esteem, loss of control and
privacy; and, they often respond to these stressors by either acting out or withdrawing and
becoming passive. Strategies that will help adolescents cope with their illness experience
are to involve them in decision making, encourage self-advocacy and self-care, provide
opportunities for peer interactions, allow for privacy, and if possible, provide same sex care
provider.
Reducing psychological trauma
While there are specific nuances to each age grouping, there are core factors which cross all
developmental stages and have the potential to cause psychological trauma to children
experiencing illness and injury. These are:
Separation from primary caregiver and home
Painful or frightening procedures
Misconceptions around diagnosis and treatment, lack of information
Loss of control, and feelings of helplessness
Emotional distress
Physical restraints
There are also core interventions that decrease the influence of these factors, and support
children and families while in the healthcare environment.

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
222
Play
‘Play is the child’s symbolic language of self-expression, and for children to ‘play out’ their
experiences and feelings is the most self-healing process in which children can engage.’
(Erik Erikson, 1940) Play is how children experience the world. It is universal, and is critical
to human development as an opportunity to communicate feelings, problem solve, try on
new roles, make sense of experiences, and gain mastery. In the hospital setting, play has
the potential to become a healing modality through which growth and development are
fostered and promoted (Child Life Council, 2013). Play for hospitalised children focuses on
the process of mastering critical events such as hospitalisation and medical procedures.
Defining this as Therapeutic play, it refers to activities that are developmentally supportive
and facilitate the emotional well-being of the child. Empirical evidence supports the
effectiveness of therapeutic play in reducing psychological and physiological stress in
hospitalized children. (www.childlife.org/files/EBPPlayStatement-Complete.pdf). Medical
Play is another technique that allows for the expression of feelings related to hospital
experiences, while at the same time providing opportunities for understanding and mastery
of those experiences. Role reversal and being in control during medical play are powerful
tools for coping with helplessness, and building resiliency.
Coping
There are many stressors in the healthcare environment that can tax a child’s ability to cope.
Coping in this setting is viewed as ‘cognitive and behavioral efforts to manage specific
external and/or internal demands that … exceed the resources of the person’ (Lazarus &
Folkman, 1984). Healthcare professionals have the ability to affect a child’s coping process
through identification of the stressful event or stimulus, and assisting in minimizing that
stress through the development of coping strategies. When children learn to master
experiences, which are unfamiliar, frightening, or potentially painful, they may become more
complaint with healthcare treatment, and even get well quicker. So, whether the stressor is
a needle stick poke, separation from a parent, not being able to eat, having to lie still for an
x-ray, children can learn to cope with the situation. Specific strategies can be separated into
three categories – sensory, cognitive and behavioral – and include breathing and relaxation
exercises, distraction or alternate focus, positioning for comfort, sucking, music, rocking,
desensitization, and guided imagery.

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
223
Pain
Fear of needles is one of the greatest fears held by children in the hospital setting. In a
study of 1,024 children, Taddio et al (2012), found 63% reported a fear of needles and the
associated pain of needlesticks. While pain myths have largely been dispelled through
research (Collier, 1997) there still seems to be some question as to whether it is more
distressing for a child to be restrained during a procedure rather than any the pain being felt.
Being restrained is what leads to psychological trauma for children, so every effort should be
made to prevent children being held down during medical procedures (Bray, 2016).
Research also shows that for each exposure to procedural pain without effective pain
management, children demonstrate increased pain and anxiety with subsequent exposures
(Versloot, 2008). Children across all ages see themselves as an active agent in managing
their own pain responses, and feel most successful when they cope with pain on their own
(Franck, 2008).
Preparation
To psychologically prepare a child for a procedure or surgery, gives them the opportunity to
understand what to expect, create a coping plan, and successfully master any related
stressors. Goals for preparing a child for a procedure are to reduce fear and anxiety, and
enhance coping and compliance with medical care. The benefits of preparation are that it
clears up misconceptions, allows children to cooperate because they understand what is
happening, as well as what their role is in their own care. It also goes a long way in building
trust in their care providers which has huge benefit for future procedures or interventions.
Preparation is a process, not an event, and there are sequential steps to preparing children
and families which includes making sure children know what they will feel, see, hear, and
smell. Using either play or real medical equipment in a preparation session is dependent on
the age of the child, as well, many other tools have been developed to aid in that
preparation, such as teaching dolls, and picture or photo books.
Communication
Healthcare has its own language, and it’s one that healthcare professionals understand, but
children and families do not. What does it mean to child to have their blood drawn, or to go
to Cat scan? Do they understand what we mean when we say we are going to put an IV in
their hand? These are words and phrases that are foreign to most children, or out of
context, and can cause distress because of the lack of understanding. In describing pain,

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
224
there are hard words, such as hurt or burn, versus soft words, such as uncomfortable or
tight. Using softer words has the capacity to lessen a perceived threat, and helping a child
cope more successfully (Gaynard, et al, 1998). Providing explanation of words or phrases is
also important, such as a catheter is a small flexible tube, or taking your blood pressure
means “I’m measuring how fast your blood is moving through your body”. Taking care to
choose words that don’t cause more confusion, and allow for a greater understanding of
information helps for greater coping and compliance.
Environment
Environment can be both physical as well as emotional, but the common factor is about
safety. A child friendly physical environment is welcoming and inviting, and sets the tone
that this is a safe place for them. Having safe places includes have a playroom that allows
for play and development opportunities in which no medical procedures happen is important
for promoting positive coping. It is also best practice to not conduct painful medical
procedures while a child is in their own hospital bed. Moving to a treatment room for
needlestick, or any other invasive procedures allows the child’s bed to remain a safe space.
Family-Centered Care
Family involvement in the care of their child in the hospital is essential, with best practice
being a collaborative model that considers the expertise of both medical professionals and
the patient and family when making decision on medical care. Family-centered care is
based on four primary principles 1) respect and dignity, 2) information sharing, 3)
involvement in care, and 4) collaboration (www.ipfcc.org). It recognizes that parents know
their child best, and will ultimately be responsible for their care at home, so should be
integral part of the hospital experience. Working with families rather than to or for families in
providing services is at the core of being patient and family-centered, and creates a team
approach with the child’s best interest at the center of care. If a parent is non-anxious,
engaged in the care of their child, and working as a team with healthcare providers, their
child has a much greater chance of also being less anxious, and better able to cope with
their experiences.
To revisit the need to minimize psychological trauma for children in the healthcare
environment, and in keeping with standards created to make the healthcare environment a

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
225
place of healing for the whole child, it is becoming best practice for healthcare professionals
to begin the examination of their current practice, and move in a direction that transforms
care for the patients and families that reduces fear, anxiety and suffering, and improves their
overall experience of care.
REFERENCES
Bandura, Albert (1977) Social Learning Theory. Englewood Cliffs, NJ: Prentice-Hall
Bowlby, John (1982) Attachment and loss volume I: Attachment. London: Hogarth Press
Bray, L., B. Carter, J. Snodin (2016). Holding Children for Clinical Procedures: Perseverance
in Spite of or Persevering to be Child-Centered. Research in Nursing and Health, 39(1),
February, pp 30-41.
Child Friendly Healthcare Initiative www.childfriendlyhealthcare.org
Child Life Council (2002) Official Documents of the Child Life Council www.childlife.org
Child Life Council (2008), Evidence Based Play Statement, Therapeutic Play in Pediatric
Health Care: The Essence of Child Life Practice
Collier, J. and H. Pattison (1997) Attitudes to children's pain: exploding the 'pain myth'.
Paediatric Nursing, 9(10), December, pp 15-18
Council of Europe www.COE.int
Erikson, Erik (1963) Children and Society. New York: Norton
European Association for Children in Hospitals www.each-for-sick-children.org
Franck, L.S., A. Sheikh, K. Oulton (2008). What helps when it hurts: children's views on pain
relief, Child: care, health, and development, 34(4), July, pp 430-438
Gaynard, L., J. Wolfer, J. Goldberger, R. Thompson, L. Redburn, L. Laidley (1998)
Psychosocial care of children in hospitals: a clinical practice manual from the ACCH child life
research project
Institute for Patient and Family-Centered Care www.ipfcc.org
Lazarus, R.S. and S.F. Folkman (1984) Stress, appraisal, and coping. New York: Springer
Piaget, Jean (1962) Play, dreams, and imitation in childhood. New York: Norton

PROCEEDINGS FROM HOSPITAL KANAK-KANAK PERMATA
226
Taddio, A. M. Ipp, S. Thivakaran, A. Jamal, C. Parikh, S. Smart, J. Sovran, D. Stephens, J
Katz (2012). Survey of the prevalence of immunization non-compliance due to needle fears
in children and adults. Vaccine, 30(32), July 6, pp 4807-4812
Thompson, Richard (2009) The handbook of child life. Illinois: Charles Thompson
Publishers
United Nations Council on the Rights of Children www.ohchr.org
Versloot, J., J.S. Veerkamp, J. Hoogstraten (2008) Pain behaviour and distress in children
during two sequential dental visits: comparing a computerised anaesthesia delivery system
and a traditional syringe, British Dentist Journal, 205(1), 12 July, pp 30-1.