product reference guide - controlsoft
TRANSCRIPT

Evidence Review
Using Clinical Pathways to Aid in the Diagnosisof Necrotizing Soft Tissue Infections Synthesisof Evidence
Lynn Schuster, RN, DNP, ACNP-BC, Diane E. Nunez, RN, DNP, ANP-BC
ABSTRACTBackground: Necrotizing soft tissue infections (NSTIs) are rare, rapidly spreading infections that
occur in the soft tissue compartments. The mortality rate is high and has been found to decrease ifpatients are treated early and aggressively with surgical debridement and broad-spectrum antibiotics.Unfortunately these infections present similarly to other types of skin and soft tissue infections (SSTIs)making diagnosis difficult.
Aims: This paper reviews the evidence surrounding the early diagnosis of NSTIs. This was usedto develop a clinical practice guideline (CPG) for implementation in the emergency department (ED)setting to assist the provider in distinguishing NSTIs from SSTIs to potentially decrease the time frompresentation to diagnosis.
Methods: A review of the literature was performed. Studies were identified and critiqued by tworeviewers independently for clinical relevance, study design, and statistical analysis.
Results: Signs and symptoms, or “hard signs,” associated with NSTIs include: pain out of proportionto the exam, rapidly spreading infection, presence of bullae, skin ecchymosis or sloughing, gas in thetissues, skin anesthesia, edema extending beyond the erythema, and symptoms of sepsis. Unfortunatelyonly 43% of the patients with an NSTI will present with these signs. Studies have found an associationbetween laboratory values and NSTIs with the most commonly associated findings being leukocytosis,azotemia, and hyponatremia. Using these complimentary clinical and laboratory values, the LaboratoryRisk Indicator for NECrotizing fasciitis (LRINEC) score is an emerging tool that providers can use todetermine the risk of an NSTI. A clinical pathway was developed and implemented in the ED for allpatients presenting with an SSTI to assist providers in confirming or negating the presence of an NSTI.
Implication for Practice: Educating ED providers about the signs, symptoms, and laboratory findingsassociated with NSTIs will lead to earlier diagnosis and treatment and decreased morbidity and mortality.
KEYWORDS necrotizing fasciitis, soft tissue infection, diagnosis, clinical practice guideline
BACKGROUND AND SIGNIFICANCE
Necrotizing soft tissue infections (NSTIs) are serious,rapidly spreading, infections of the skin, subcuta-
neous tissues, and muscle. Although the incidence ofNSTIs is low, only 3.5 cases per 100,000 people (Endorfet al. 2009), there is significant morbidity and mortality as-sociated with this condition. In a review of the literature,
Lynn Schuster, Director, Acute Care Nurse Practitioner Hospitalists, Banner Gateway Medical Center, Gilbert, AZ; Diane E. Nunez, Clinical Associate Professor, Arizona StateUniversity, College of Nursing & Health Innovation, Phoenix, AZ
Address correspondence to Dr. Diane E. Nunez, Arizona State University, College of Nursing & Health Innovation, 500 N. 3rd Street, Phoenix, AZ 85004; [email protected]
Accepted 19 March 2011Copyright ©2011 Sigma Theta Tau Internationaldoi: 10.1111/j.1741-6787.2011.00235.x
Endorf et al. (2009) reported a 24–40% mortality rate. Ifthe patients survive the infection they are often left withextensive soft tissue disfigurement or loss of extremities.
Necrotizing infections are difficult to diagnose as theyoften present similarly to other common skin and soft tis-sue infections (SSTIs) with symptoms of pain, erythema,warmth, and swelling. May and colleagues (2009) revealed
88 Second Quarter 2012 �Worldviews on Evidence-Based Nursing

Clinical Pathways to Aid in the Diagnosis of Infections
that 50% of patients with NSTIs are misdiagnosed on ad-mission. Some signs and symptoms that should alert thehealthcare provider to an NSTI are the presence of bul-lae, skin ecchymosis or sloughing, gas in the tissues, skinanesthesia, pain out of proportion to the exam, edema thatextends beyond the skin erythema, rapidly spreading infec-tion, and symptoms of sepsis such as hypotension, tachy-cardia and organ failure (Stevens et al. 2005). These areoften referred to as “hard signs” of an NSTI. Early recog-nition of these infections is essential, as they will spreadto the deep tissues creating fluid pockets that do not allowthe body’s healing cells to reach the tissues in need. Al-though soft tissue infections are more commonly seen inthe emergency room setting, with an incidence of 24.8 per1,000 person years compared with 0.04 per 1,000 per-son years for necrotizing infections (Ellis Simonsenet al. 2006), it is imperative that the healthcare provideris able to differentiate between necrotizing and nonnecro-tizing infections as delayed treatment increases mortality(May et al. 2009). Patients with necrotizing infections re-quire broad-spectrum antibiotics and immediate surgeryfor aggressive debridement of the necrotic tissue (Mayet al. 2009).
The Institute of Medicine has recommended the use ofevidence-based clinical pathways to reduce errors (Kohn2000). Wright and colleagues (2008) studied the im-plementation of evidence-based clinical pathways in theemergency room setting to decrease provider error. Pa-tients were given a higher quality of care after the im-plementation of clinical guidelines with patients receivingtreatments more rapidly, had decreased time spent in theemergency room, and had decreased readmission rates(Wright et al. 2008).
At a Southwestern tertiary care medical center in theUnited States; 90% of patients that presented to the emer-gency room were erroneously diagnosed with a soft tis-sue infection, when they were later determined to have anecrotizing infection (L. Schuster, personal communica-tions, August 21, 2010). There is often a knowledge deficitamong staff members when these patients present to thehospital about the warning signs that should trigger thedifferential diagnosis of a necrotizing infection. By imple-menting clinical practice guidelines (CPGs) to assist withthe triage of patients presenting to the emergency roomwith a soft tissue infection to rule out a necrotizing in-fection, it is anticipated that the time from presentationto diagnosis and treatment will decrease. This inquiry hasled to the clinically relevant question: in adult patientspresenting with an SSTI, how does the use of an evidence-based CPG for screening patients for NSTIs compare withnot using a clinical guideline in affect to the time to thediagnosis of a necrotizing infection?
SEARCH METHODS
To address the question of the impact of clinical guide-lines on early diagnosis of NSTI, an extensive review ofthe literature was performed. The search included reviewsof CINAHL, Medline/Ovid, MD Consult, Cochrane, Na-tional Guideline Clearinghouse, and Pub Med. The searchterms that were used included: “NSTIs,” “fasciitis,” “softtissue infections,” “diagnosis,” “early diagnosis,” “clinicalpathways,” “clinical guidelines,” and “Laboratory Risk In-dicator for NECrotizing Fasciitis (LRINEC) score.” Thefollowing limits were placed: English and adults. Initiallythe dates were limited from 2005 to present, however thedates were expanded to 1900 until present to ensure cap-ture of landmark studies prior to those dates. The searchfindings using these keywords resulted in numerous re-sults, up to 69,000. Therefore the results were further de-fined by applying controlled vocabulary, Boolean/phrasesearch mode, MeSH terms, and implode and explode. Inaddition to the search of the databases, the bibliographiesof the search results were scanned for additional studies.
Inclusion criteria for the studies included adult popu-lation, diagnosis of NSTIs, and use of diagnostic criteriafor NSTIs. Exclusion criteria included studies that solelyaddressed treatment of NSTIs.
The keywords search method for CINAHL yielded 1,038results. This was narrowed down to 13 relevant articles,with two of four clinical trials being relevant to this project;four clinical guidelines were retained for reference. A re-view was performed of the reference lists from the perti-nent articles and one further relevant article was obtained.A Medline/OVID keyword search yielded 37,674 results.The results were narrowed by using the focus feature with“diagnosis” for the subheading, refining the list to 237 re-sults. These results were focused by searching for “NSTI”and “diagnosis,” yielding three clinical trials, two of whichwere used in this study. A keyword search of MD Con-sult yielded 230 results. When “diagnosis” was added to“NSTI,” 18 results were obtained, four of which were per-tinent to this project.
The Cochrane reviews and libraries were searched us-ing the keyword SSTI AND diagnosis which yielded 15 re-sults. However, after reviewing the abstracts of these papersnone of them met the inclusion criteria for this study. TheNational Guideline Clearinghouse was searched using theprevious keywords; six results were obtained with one per-tinent guideline meeting inclusion criteria. To concludethe search, PUBMED was explored using the keywordsnecrotic soft tissue infection with 773 results. NSTIs anddiagnosis narrowed it down to 40 results. In review ofthe studies, many had already been captured by previ-ous database searches, however one new clinical trial was
Worldviews on Evidence-Based Nursing �Second Quarter 2012 89

Clinical Pathways to Aid in the Diagnosis of Infections
obtained. In total, 11 clinical trials, 9 review articles, and5 clinical guidelines were used for this evidence-based re-view through the exhaustive search of six databases. Tworeviewers, the chief of surgery and an associate professorat Arizona State University, reviewed the studies. Theirlevels of agreement about clinical relevance, study design,and statistical analysis were congruent.
CRITICAL APPRAISAL AND SYNTHESIS OFEVIDENCE
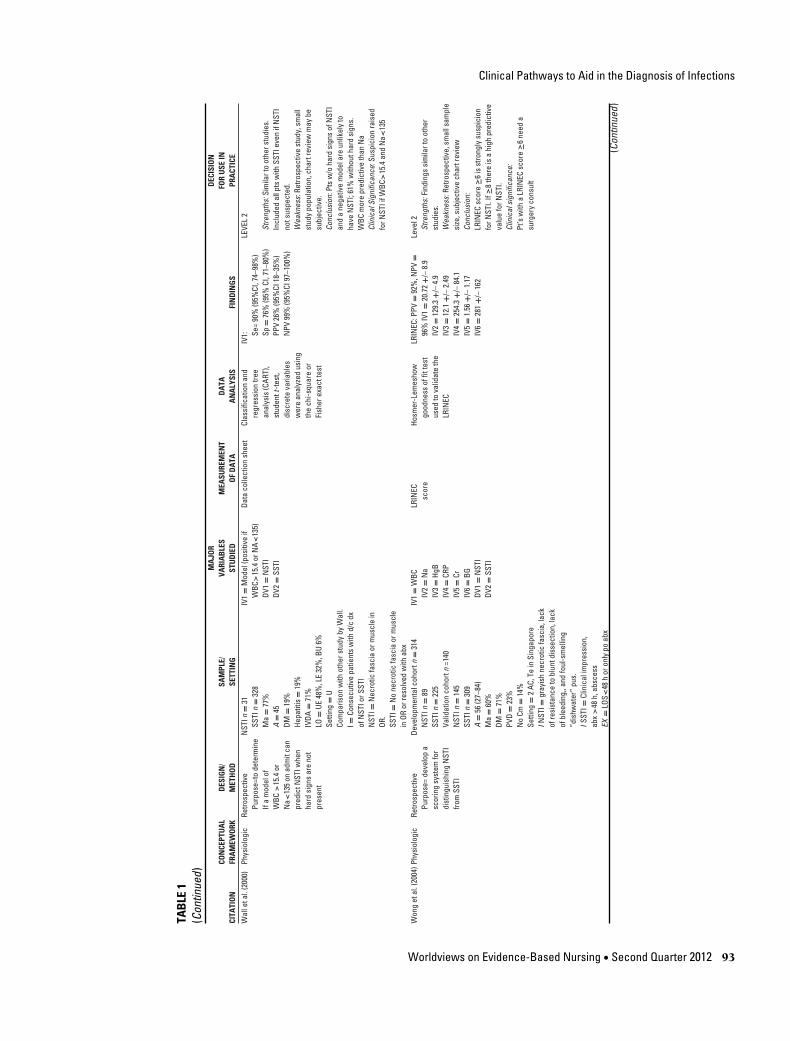
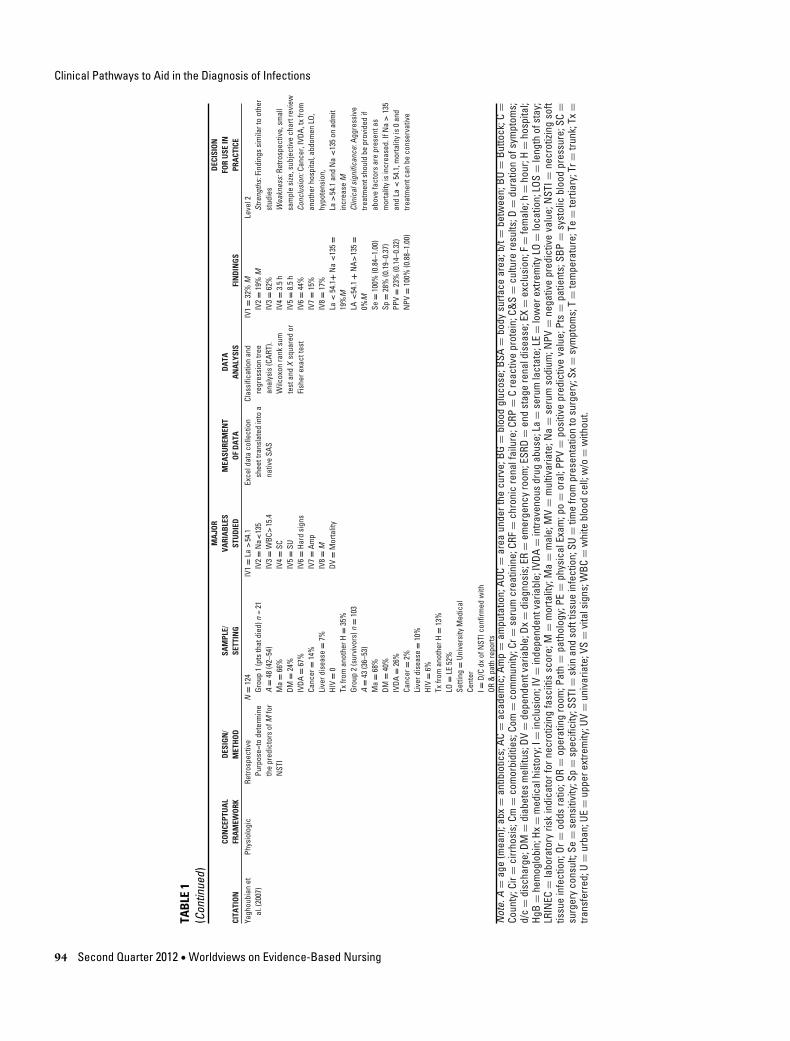
Overall, the chosen studies were of good quality, notingconfidence intervals (CI), standard deviations (SD), levelof significance (p), mean values (M), odds ratio (OR), sen-sitivities (Se), and specificities (Sp). Eight out of nine ofthe studies (evaluation table, Table 1) reviewed for thispaper were retrospective studies that showed level II ev-idence, the remaining study was prospective and showedlevel II evidence. Unfortunately, the majority of the studieson this subject matter are retrospective as it is unethicalto withhold diagnostic measures for these patients as theywould suffer from severe morbidity and mortality if theydo not have an adequate workup to rule out or confirm thediagnosis. This limits the potential validity of these studiesas bias can be introduced during the chart review process.The nine studies that were reviewed displayed a moderatedegree of homogeneity in regards to sample demographics(Table 2). The majority of the patients were males, in theirmid-40s to early 50s. The largest risk factors for necrotiz-ing infections in most of the studies were intravenous druguse (IVDA), diabetes, and liver disease (Table 3).
There was a moderate degree of sample heterogeneity inregards to the statistical measurements used, with the Stu-dent t-test being used most frequently in three of the ninestudies. Each of the studies had a relatively small samplesize, ranging from 21 to 359 subjects, likely representingthe rare nature of this disease; this could limit the validityof the findings. Another limiting factor is there are incon-sistent definitions for NSTIs throughout the studies. Thegold standard for diagnosing NSTIs is a tissue biopsy, how-ever some of the studies allowed surgeon opinion, whichcould limit the validity of the findings. Finally, there wassome heterogeneity among the independent and depen-dent variables that were studied; however, each study ex-cept for one (Frazee et al. 2008) found that a sodium (Na)level <135 mEq/L was associated with necrotizing infec-tions. Each study also found an association between ele-vated white blood cell (WBC) count and NSTIs; however,the definitions of an elevated WBC count were inconsis-tent throughout the studies. Three studies looked at thevalue of using the LRINEC scoring system as a promising
objective score that can be used to diagnose or rule out anNSTI.
CONCLUSIONS ABOUT EVIDENCE
The synthesis of study findings support early diagnostictesting to include complete blood count (CBC), compre-hensive metabolic panel (CMP), blood and wound cul-tures, C-reactive protein (CRP), and creatinine kinase oneach patient that presents to the emergency department(ED) with a soft tissue infection (CPG, Figure 1). If thereare hard signs of a necrotizing infection present (bul-lae, necrosis, pain out of proportion to the exam, rapidlyspreading infection, gas, skin anesthesia, sepsis) promptconsultation with surgical services should be initiated. Ifthe patient does not have hard signs, a LRINEC score can becalculated (Figure 1, LRINEC Score), and for scores ≥6,surgery consult should promptly occur to initiate rapidintervention. For scores <6 but with clinical concern, di-agnostic imaging such as an X-Ray, CT scan, or MRI isindicated depending on the location of the infection.
Among all studies reviewed, WBC >15.4 mm3 andNa < 135 mEq/L are the strongest predictors to early di-agnosis of necrotizing infections. Both of these values areincorporated in the LRINEC score. The LRINIC score is anemerging objective scoring system to aid in the predictionand early diagnosis of NSTIs, however it should be usedin conjunction with clinical judgment, as there is limitedstudy data to date.
DISCUSSION
The purpose of this review was to evaluate the efficacyof objective laboratory data and clinical measures to pro-mote early diagnosis of NSTIs. Using these measures inthe development of a CPG in the emergency room settingwill guide practitioners’ initial diagnostic workup whilesuggesting issues requiring attention for the translation ofthe intervention’s effectiveness in patients presenting withinitial SSTIs.
Interventions using early obtained laboratory diagnos-tics of CBC, CMP, blood and wound cultures, CRP, andcreatinine kinase showed improvements in clinical diag-nosis and referral for treatment interventions. In patientswith hard signs of an NSTI (bullae, necrosis, pain outof proportion to the exam, rapidly spreading infection,gas, skin anesthesia, sepsis) with positive data of elevatedWBC count and low sodium demonstrated a predictive cor-relate of clinical diagnosis of necrotizing infection. Thiseffect implies reduced morbidity and mortality in NSTIsas compared to usual care when measured across dimen-sions of health outcomes. If the health issue guiding the
90 Second Quarter 2012 �Worldviews on Evidence-Based Nursing

Clinical Pathways to Aid in the Diagnosis of InfectionsTA
BLE
1Ev
alua
tion
tabl
eM
AJO
RD
ECIS
ION
CON
CEPT
UA
LD
ESIG
N/
SAM
PLE/
VARI
AB
LES
MEA
SURE
MEN
TD
ATA
FOR
USE
INCI
TATI
ON
FRA
MEW
ORK
MET
HO
DSE
TTIN
GST
UD
IED
OF
DA
TAA
NA
LYSI
SFI
ND
ING
SPR
ACT
ICE
Chan
etal
.(20
08)
Phys
iolo
gic
Pros
pect
ive,
obse
rvat
iona
lPu
rpos
e=
Tode
term
ine
how
ofte
nth
e“h
ard
sign
s”of
NST
Isar
epr
esen
tand
toev
alua
teho
wla
bva
lues
can
assi
stw
ithdx
ofN
STIs
N=
21A
=42
Ma
=90
%DM
=52
%IV
DA=
29%
ESRD
=5%
Cir=
5%N
oCm
=19
%W
BC(m
ean)
=31
.5N
a(m
ean)
=12
7I=
Cons
ecut
ive
pts
pres
entin
gw
ithN
STIs
Setti
ng=
C,AC
Hard
sign
s:Cr
epitu
s,ne
cros
is,b
ulla
e,ga
son
X-ra
y,hy
pote
nsio
n
IV1=
NA
<13
5IV
2=
WBC
>15
.4IV
3=
NA
<13
5an
dW
BC>
15.4
IV4=
IV1
orIV
3IV
5=
Hard
sign
sIV
6=
IV5=
IV1
=IV
2DV
=Dx
ofN
STIs
Ques
tionn
aire
give
nto
the
surg
eon
prio
rto
and
afte
reva
luat
ing
lab
resu
ltsto
dete
rmin
eif
they
felt
the
ptha
da
NST
Iba
sed
onth
eph
ysic
alex
aman
dif
they
need
edsu
rger
y
UVan
alys
is.M
cNem
ar-
Xsq
uare
dIV
1=
90%
IV2=
90%
IV3=
81%
IV4=
100%
IV5=
43%
IV5=
86%
LEVE
L1
Stre
ngth
s:Fi
ndin
gssi
mila
rto
othe
rst
udie
s.W
eakn
ess:
retro
spec
tive
stud
yan
dsm
alls
tudy
popu
latio
n,ch
artr
evie
wm
aybe
subj
ectiv
e.Hi
ghin
cide
nce
ofN
STIs
seen
atfa
cilit
yCo
nclu
sion
s:Fe
wer
than
half
ofN
STIs
pts
will
pres
entw
ithha
rdsi
gns,
adm
issi
onW
BC>1
5.4
and
NA
<13
5in
crea
sesu
spic
ion
forN
STIa
ndar
eus
eful
inea
rlydi
agno
sis
Clin
ical
sign
ifica
nce:
Will
eval
uate
WBC
and
NA
toas
sist
with
diag
nosi
sof
NST
I
Fraz
eeet
al.(
2008
)Phy
siol
ogic
Retro
spec
tive
Purp
ose
=To
dete
rmin
eth
eER
pres
enta
tion
ofN
STI
and
iden
tify
seve
rity
mar
kers
N=
122
Non
seve
reN
STIn
=67
Seve
reN
STIn
=55
IVDA
=80
%A
=44
.1+/
–11
Ma
=64
%DM
=22
%HI
V=
4%Pr
iorN
STI=
7.4%
LO=
UE47
%,L
E27
%,B
U19
%,T
r16%
Setti
ng=
AC,U
,C,E
RI=
Path
repo
rtw
ithN
STI
Ex=
Hosp
itala
cqui
red
NST
I,N
egat
ive
path
repo
rt,no
tadm
itted
thro
ugh
ERSe
vere
NST
I=De
ath,
Amp,
ICU
stay
IV1=
SBP<
100
IV2=
HR>
100
IV3=
WBC
>20
IV4=
BUN
>18
IV5=
CR>
1.2
IV6=
Tiss
uega
sIV
7=SU
IV8=
Corr
ectD
xIV
9=
MIV
10=
Amp
DV1=
Non
seve
reN
STI
DV2=
Seve
reN
STI
(Dea
th,A
mp,
ICU
stay
)
Data
extra
ctby
five
EDph
ysic
ians
usin
gst
anda
rdize
dfo
rms,
and
ente
red
into
File
Mak
erPr
o6da
taba
se
Chi-S
quar
e,Fi
sher
’sex
act,
and
mul
tivar
iate
logi
stic
regr
essi
onte
stin
g
OR(9
5%CI
)+p
valu
eIV
1=
4.52
(1.7
3-11
.82)
,0.0
02IV
2=
3.40
(1.5
7-7.
37),
0.00
2IV
3=
3.73
(1.6
4-8.
51),
0.00
2IV
4=
6.82
(2.8
5-16
.34)
,.00
01IV
5=
3.77
(1.4
9-9.
57),
0.00
5IV
6=
3.84
(1.5
7-9.
4),0
.003
IV7=
501.
5m
inut
esIV
8=
59%
IV9=
16.4
%IV
10=
4.1%
LEVE
L2
Stre
ngth
s:Fi
ndin
gssi
mila
rto
othe
rst
udie
s.W
eakn
ess:
retro
spec
tive
stud
yan
dsm
alls
tudy
popu
latio
n,ch
artr
evie
wm
aybe
subj
ectiv
e.La
rger
num
bero
fIV
DA(8
0%).
Faile
dto
incl
ude
Na
inth
eir
data
anal
ysis
Conc
lusi
ons:
SBP
<10
0,BU
N>
18,s
oftt
issu
ega
s,ad
mit
toa
nons
urgi
cals
ervi
cean
dcl
ostri
dial
spec
ies
wer
eas
soci
ated
with
seve
reN
STI.
Clin
ical
sign
ifica
nce:
Ifa
ptha
sab
ove
findi
ngs,
will
obta
inst
atsu
rgic
alco
nsul
tHo
lland
(200
9)Ph
ysio
logi
cRe
trosp
ectiv
ePu
rpos
e=
toas
sess
the
usef
ulne
ssof
the
LRIN
EC
N=
28Gr
oup
1(b
iops
ypr
oven
NST
I)n
=10
Grou
p2
(SST
I)n
=18
Ma
=80
%LO
=50
%LE
,20%
abd,
20%
ches
t,10
%UE
I=Ad
mis
sion
dxof
NST
I(ad
ults
and
child
ren)
EX=
Labs
nota
vaila
ble
toca
lcul
ate
the
LRIN
EC
IV1=
LRIN
EC≥6
IV2=
LRIN
EC≥8
IV3=
LRIN
EC≥
5≥
8st
rong
pred
icto
rofN
STI,
DV1=
Dxof
NST
I
Char
trev
iew
Like
lihoo
dra
tio(L
R)LR
1=
0te
stut
ility
LR=
0.2–
5=
smal
lut
ility
LR<
0.2
or>
5=
mod
-to-la
rge
utili
ty
IV1=
80%
grou
p1,
33%
grou
p2.
Se80
%,S
p67
%,P
PV57
%,
NPV
86%
LR–0
.3,+
2.3
IV2=
Se50
%,S
p94
%’P
PV83
%,N
PV77
%LR
–0.5
3,+
9IV
3=
Se10
0%Sp
61%
NPV
=10
0%PP
V59
%
LEVE
L2
Stre
ngth
s:Lo
oked
atpr
edic
tive
capa
bilit
yof
othe
rLRI
NEC
valu
es(≥
5an
d8)
Wea
knes
s:Re
trosp
ectiv
ean
dsm
all
stud
ypo
pula
tion,
char
trev
iew
may
besu
bjec
tive.
Incl
uded
two
child
ren
ages
5an
d8
mon
ths
inan
alys
is,
dem
ogra
phic
data
notl
iste
dCo
nclu
sion
s:LR
INEC
≥8st
rong
pred
icto
rofN
STI,
<5
was
relia
ble
toru
leou
tNST
Ihow
ever
asc
ore
of≥6
isno
tast
rong
enou
ghpr
edic
toro
fNST
I.Cl
inic
alsi
gnifi
canc
e:Fi
ndin
gsar
eno
tas
prom
isin
gfo
rLRI
NEC
scor
e≥6
inpr
edic
ting
NST
Ias
prev
ious
stud
ies,
how
ever
ther
ew
asa
muc
hsm
all
sam
ple
size
and
child
ren
wer
ein
clud
edin
the
anal
ysis
,the
refo
reit
may
notb
eus
eful
toou
rstu
dypo
pula
tion.
Ifth
esc
ore
is<
5,an
NST
Iis
unlik
ely,
if≥8
stro
nglik
elih
ood
ofN
STI (C
ontin
ued)
Worldviews on Evidence-Based Nursing �Second Quarter 2012 91

Clinical Pathways to Aid in the Diagnosis of Infections
TAB
LE1
(Con
tinue
d)M
AJO
RD
ECIS
ION
CON
CEPT
UA
LD
ESIG
N/
SAM
PLE/
VARI
AB
LES
MEA
SURE
MEN
TD
ATA
FOR
USE
INCI
TATI
ON
FRA
MEW
ORK
MET
HO
DSE
TTIN
GST
UD
IED
OF
DA
TAA
NA
LYSI
SFI
ND
ING
SPR
ACT
ICE
Hsia
oet
al.(
2008
)Phy
siol
ogic
Retro
spec
tive
Purp
ose=
Toid
entif
yth
epo
sitiv
ean
dne
gativ
epr
edic
tors
ofM
inpt
sw
ithN
STI
N=
128
A=
61+/
–12
.9M
a=
67%
DM59
%Ci
rrho
sis
=11
%IV
DA=
4%Ca
ncer
=7%
ESRD
=4%
LO=
UE/L
E88
%,T
r4%
Setti
ng=
ACin
Taiw
anI=
ERad
mit,
d/c
dxof
NST
IEx
=N
otad
mitt
edth
roug
hER
,No
C&S,
A<
18,r
eadm
itted
forN
STI
with
in30
days
IV1=
SBP<
90IV
2=
Vibr
ioIV
3=
Aero
mon
asIV
4=
Mal
igna
ncy
IV5=
Band
s>0%
IV6=
Corr
ectD
xDV
=M
ofN
STIp
ts
Data
colle
ctio
nsh
eet
Sim
ple
and
mul
tivar
iate
logi
stic
regr
essi
onan
alys
is
OR(9
5%CI
)+p
valu
eIV
1=
6.62
(1.5
2–28
.77)
IV2=
7.03
(1.2
1–41
.03)
IV3=
10.2
2(1.
34–7
7.96
)IV
4=
46.5
4(5.
76–3
76.0
3)IV
5=
5.61
(1.4
8–21
.3)
IV6=
38%
Leve
l2St
reng
ths:
Blin
ded
data
extra
ctor
Wea
knes
ses:
Retro
spec
tive,
high
erin
cide
nce
ofvi
brio
,Aer
omon
asan
dci
rrho
sis
than
othe
rstu
dies
,not
allp
tsha
dtis
sue
confi
rmat
ion
ofN
STI.
No
IVDA
case
sCo
nclu
sion
:Aer
omon
asor
Vibr
ioin
fect
ion,
canc
er,h
ypot
ensi
onor
band
s>
10ha
vein
crea
sed
M.
Clin
ical
sign
ifica
nce:
Pts
with
abov
efin
ding
sw
illne
edag
gres
sive
treat
men
tas
Mis
high
er
Suet
al.(
2008
)Ph
ysio
logi
cRe
trosp
ectiv
e,ob
serv
atio
nalc
ohor
tst
udy
Purp
ose=
Tode
term
ine
the
rela
tions
hip
b/tt
heLR
INEC
scor
ean
dM
,LO
S,an
dne
edfo
rsu
rger
y
N=
209
pts
with
NST
I,di
vide
din
totw
ogr
oups
∗Gro
up1
LRIN
ECsc
ore
<6
n=1
09∗G
roup
2LR
INEC
≥6n
=10
0M
a=70
%A
=56
.8-1
5DM
=56
%Ci
r=28
%ES
RD=
22%
No
cm=
25%
Setti
ng:T
e,AC
,and
1Co
m,A
CTa
iwan
I=Ad
ultp
tsad
mitt
edth
roug
hth
eER
with
ad/
cdx
ofN
STI
EX=
<18
year
sol
d,tx
from
othe
rin
stitu
tions
,unc
erta
inLR
INEC
scor
e.On
ly1s
tadm
itus
edfo
rpts
with
mul
tiple
adm
issi
ons
forN
STI
IV1=
LRIN
ECSc
ore
DV1=
MDV
2=
Amp
DV3=
SU
LRIN
ECsc
ore
Man
n-W
hitn
eyU-
test
and
aSt
uden
tt-te
stw
ere
used
toco
mpa
reth
est
atis
tical
lysi
gnifi
cant
diffe
renc
esbe
twee
nth
etw
ogr
oups
.
Grou
p1:
DV1=
11%
DV2=
17.4
%DV
3=
30+/
–51.
8h
Grou
p2
:DV
1=
21%
DV2=
36%
DV3=
27.4
+/–5
1.8
hOv
eral
lDV1
=15
..8%
Over
allD
V2=
26.3
%AU
CDV
2=
0.75
1(0
.700
–0.8
02)
AUC
DV1=
0.60
7(0
.547
–0.6
66)Le
vel2
Stre
ngth
s:si
mila
rfind
ings
ofot
her
stud
ies
Wea
knes
ses:
retro
spec
tive,
med
ical
reco
rds
may
bein
com
plet
eor
inac
cura
tely
inte
rpre
ted,
nota
llca
ses
ofN
STIc
onfir
med
bytis
sue
path
olog
yCo
nclu
sion
:Pts
with
aLR
INEC
scor
e≥6
have
incr
ease
dM
and
Amp
Clin
ical
sign
ifica
nce:
Pt’s
with
aLR
INEC
scor
e≥6
will
need
surg
ery
cons
ultf
orfu
rther
eval
uatio
n
Wal
leta
l.(2
000)
Phys
iolo
gic
Retro
spec
tive
stud
yPu
rpos
e=to
iden
tify
obje
ctiv
eda
taon
adm
issi
onto
help
diffe
rent
iate
NST
Ifro
mSS
TI
N=
42pt
s,N
STIn
=21
Non
-NST
In=
21M
a=
81%
A=
39DM
=14
%IV
DA=
67%
HIV
=10
%LO
=UE
43%
,LE
43%
,BU
5%Se
tting
=U
NST
I=N
ecro
ticfa
scia
onOR
and
path
findi
ngs
Non
-NST
I=Ce
llulit
isor
absc
ess
w/o
necr
osis
onpa
thor
OR,r
esol
ved
with
abx
only
IV1=
WBC
>14
IV2=
BUN
>15
IV3=
Na<
135
DV1=
NST
IDV
2=
M
Data
colle
ctio
nsh
eet
MV
and
UVan
alys
is,
Stud
ent’s
t-te
st,
chi-s
quar
ete
stor
Fish
er’s
exac
ttes
t.
IV1:
Se=
81%
,Sp
=76
%,P
PV77
%,N
PV=
80%
IV2:
Se=
70%
,Sp
=88
%,
PPV
=88
%,N
PV=
71%
IV3:
Se=
75%
,Sp
=10
0%,
PPV
=10
0%,N
PV=
77%
DV2=
0if
WBC
<20
DV2=
46%
ifW
BC>
20DV
2=
100%
ifW
BC>
30
Leve
l2St
reng
ths:
mat
ched
com
paris
ongr
oup
Wea
knes
ses:
retro
spec
tive,
smal
lsa
mpl
esi
zeCo
nclu
sion
:ele
vate
dW
BCan
dBU
Nan
dde
crea
sed
Na
can
help
dist
ingu
ish
NST
Ifro
mSS
TI,e
leva
ted
WBC
isth
ebe
stob
ject
ive
pred
icto
rofM
.Tra
nsfe
rfro
man
othe
rfac
ility
incr
ease
dM
Clin
ical
sign
ifica
nce:
Susp
icio
nfo
rNST
Iw
illbe
rais
edw
hen
apt
pres
ents
with
anel
evat
edW
BCan
dBU
Nan
dlo
wN
a.W
illpr
ovid
eag
gres
sive
treat
men
tif
WBC
>20
(Con
tinue
d)
92 Second Quarter 2012 �Worldviews on Evidence-Based Nursing
Clinical Pathways to Aid in the Diagnosis of Infections
TAB
LE1
(Con
tinue
d)M
AJO
RD
ECIS
ION
CON
CEPT
UA
LD
ESIG
N/
SAM
PLE/
VARI
AB
LES
MEA
SURE
MEN
TD
ATA
FOR
USE
INCI
TATI
ON
FRA
MEW
ORK
MET
HO
DSE
TTIN
GST
UD
IED
OF
DA
TAA
NA
LYSI
SFI
ND
ING
SPR
ACT
ICE
Wal
leta
l.(2
000)
Phys
iolo
gic
Retro
spec
tive
Purp
ose=
tode
term
ine
Ifa
mod
elof
WBC
>15
.4or
Na<
135
onad
mit
can
pred
ictN
STIw
hen
hard
sign
sar
eno
tpr
esen
t
NST
In=
31SS
TIn
=32
8M
a=
77%
A=
45DM
=19
%He
patit
is=
19%
IVDA
=71
%LO
=UE
48%
,LE
32%
,BU
6%Se
tting
=U
Com
paris
onw
ithot
hers
tudy
byW
all.
I=Co
nsec
utiv
epa
tient
sw
ithd/
cdx
ofN
STIo
rSST
IN
STI=
Nec
rotic
fasc
iaor
mus
cle
inOR
.SS
TI=
No
necr
otic
fasc
iaor
mus
cle
inOR
orre
solv
edw
ithab
x
IV1=
Mod
el(p
ositi
veif
WBC
>15
.4or
NA<
135)
DV1=
NST
IDV
2=
SSTI
Data
colle
ctio
nsh
eet
Clas
sific
atio
nan
dre
gres
sion
tree
anal
ysis
(CAR
T),
stud
entt
-test
,di
scre
teva
riabl
esw
ere
anal
yzed
usin
gth
ech
i-squ
are
orFi
sher
exac
ttes
t
IV1: Se
=90
%(9
5%CI
,74–
98%
)Sp
=76
%(9
5%CI
,71–
80%
)PP
V26
%(9
5%CI
18–3
5%)
NPV
99%
(95%
CI97
–100
%)
LEVE
L2
Stre
ngth
s:Si
mila
rto
othe
rstu
dies
.In
clud
edal
lpts
with
SSTI
even
ifN
STI
nots
uspe
cted
.W
eakn
ess:
Retro
spec
tive
stud
y,sm
all
stud
ypo
pula
tion,
char
trev
iew
may
besu
bjec
tive.
Conc
lusi
on:P
tsw
/oha
rdsi
gns
ofN
STI
and
ane
gativ
em
odel
are
unlik
ely
toha
veN
STI;
61%
with
outh
ard
sign
s.W
BCm
ore
pred
ictiv
eth
anN
aCl
inic
alSi
gnifi
canc
e:Su
spic
ion
rais
edfo
rNST
IifW
BC>
15.4
and
Na<
135
Won
get
al.(
2004
)Phy
siol
ogic
Retro
spec
tive
Purp
ose=
deve
lop
asc
orin
gsy
stem
for
dist
ingu
ishi
ngN
STI
from
SSTI
Deve
lopm
enta
lcoh
ortn
=31
4N
STIn
=89
SSTI
n=
225
Valid
atio
nco
hort
n=1
40N
STIn
=14
5SS
TIn
=30
9A
=56
(27–
84)
Ma
=60
%DM
=71
%PV
D=
23%
No
Cm=
14%
Setti
ng=
2AC
,Te
inSi
ngap
ore
INST
I=gr
ayis
hne
crot
icfa
scia
,lac
kof
resi
stan
ceto
blun
tdis
sect
ion,
lack
ofbl
eedi
ng,,
and
foul
-sm
ellin
g“d
ishw
ater
”pu
s.IS
STI=
Clin
ical
impr
essi
on,
abx
>48
h,ab
sces
sEX
=LO
S<48
hor
only
poab
x
IV1=
WBC
IV2=
Na
IV3=
HgB
IV4=
CRP
IV5=
CrIV
6=
BGDV
1=
NST
IDV
2=
SSTI
LRIN
ECsc
ore
Hosm
er-L
emes
how
good
ness
offit
test
used
tova
lidat
eth
eLR
INEC
LRIN
EC:P
PV=
92%
,NPV
=96
%IV
1=
20.7
2+/
–8.
9IV
2=
129.
3+/
–4.
9IV
3=
12.1
+/–
2.49
IV4=
254.
3+/
–84
.1IV
5=
1.56
+/–
1.17
IV6=
281+/
–16
2
Leve
l2St
reng
ths:
Find
ings
sim
ilart
oot
her
stud
ies.
Wea
knes
s:Re
trosp
ectiv
e,sm
alls
ampl
esi
ze,s
ubje
ctiv
ech
artr
evie
wCo
nclu
sion
:LR
INEC
scor
e≥6
isst
rong
lysu
spic
ion
forN
STI.
If≥8
ther
eis
ahi
ghpr
edic
tive
valu
efo
rNST
I.Cl
inic
alsi
gnifi
canc
e:Pt
’sw
itha
LRIN
ECsc
ore
≥6ne
eda
surg
ery
cons
ult
(Con
tinue
d)
Worldviews on Evidence-Based Nursing �Second Quarter 2012 93
Clinical Pathways to Aid in the Diagnosis of Infections
TAB
LE1
(Con
tinue
d)M
AJO
RD
ECIS
ION
CON
CEPT
UA
LD
ESIG
N/
SAM
PLE/
VARI
AB
LES
MEA
SURE
MEN
TD
ATA
FOR
USE
INCI
TATI
ON
FRA
MEW
ORK
MET
HO
DSE
TTIN
GST
UD
IED
OF
DA
TAA
NA
LYSI
SFI
ND
ING
SPR
ACT
ICE
Yagh
oubi
anet
al.(
2007
)Ph
ysio
logi
cRe
trosp
ectiv
ePu
rpos
e=to
dete
rmin
eth
epr
edic
tors
ofM
for
NST
I
N=
124
Grou
p1
(pts
that
died
)n=
21A
=48
(42–
54)
Ma
=66
%DM
=24
%IV
DA=
67%
Canc
er=
14%
Live
rdis
ease
=7%
HIV
=0
Txfro
man
othe
rH=
35%
Grou
p2
(sur
vivo
rs)n
=10
3A
=43
(36–
53)
Ma
=68
%DM
=40
%IV
DA=
26%
Canc
er=
2%Li
verd
isea
se=
10%
HIV
=6%
Txfro
man
othe
rH=
13%
LO=
LE52
%Se
tting
=Un
iver
sity
Med
ical
Cent
erI=
D/C
dxof
NST
Icon
firm
edw
ithOR
&pa
thre
ports
IV1=
La>
54.1
IV2=
Na<
135
IV3=
WBC
>15
.4IV
4=
SCIV
5=
SUIV
6=
Hard
sign
sIV
7=
Amp
IV8=
MDV
=M
orta
lity
Exce
ldat
aco
llect
ion
shee
ttra
nsla
ted
into
ana
tive
SAS
Clas
sific
atio
nan
dre
gres
sion
tree
anal
ysis
(CAR
T).
Wilc
oxon
rank
sum
test
and
Xsq
uare
dor
Fish
erex
actt
est
IV1=
32%
MIV
2=
19%
MIV
3=
62%
IV4
=3.
5h
IV5
=8.
5h
IV6
=44
%IV
7=
15%
IV8
=17
%La
<54
.1+
Na
<13
5=
19%
MLA
<54
.1+
NA>
135=
0%M
Se=
100%
(0.8
4–1.
00)
Sp=
28%
(0.1
9–0.
37)
PPV
=23
%(0
.14–
0.32
)N
PV=
100%
(0.8
8–1.
00)
Leve
l2St
reng
ths:
Find
ings
sim
ilart
oot
her
stud
ies
Wea
knes
s:Re
trosp
ectiv
e,sm
all
sam
ple
size
,sub
ject
ive
char
trev
iew
Conc
lusi
on:C
ance
r,IV
DA,t
xfro
man
othe
rhos
pita
l,ab
dom
enLO
,hy
pote
nsio
n,La
>54
.1an
dN
a<
135
onad
mit
incr
ease
MCl
inic
alsi
gnifi
canc
e:Ag
gres
sive
treat
men
tsho
uld
bepr
ovid
edif
abov
efa
ctor
sar
epr
esen
tas
mor
talit
yis
incr
ease
d.If
Na
>13
5an
dLa
<54
.1,m
orta
lity
is0
and
treat
men
tcan
beco
nser
vativ
e
Not
e.A
=ag
e(m
ean)
;abx
=an
tibio
tics;
AC=
acad
emic
;Am
p=
ampu
tatio
n;AU
C=
area
unde
rthe
curv
e;BG
=bl
ood
gluc
ose;
BSA
=bo
dysu
rface
area
;b/t
=be
twee
n;BU
=Bu
ttock
;C=
Coun
ty;C
ir=
cirr
hosi
s;Cm
=co
mor
bidi
ties;
Com
=co
mm
unity
;Cr=
seru
mcr
eatin
ine;
CRF
=ch
roni
cre
nalf
ailu
re;C
RP=
Cre
activ
epr
otei
n;C&
S=
cultu
rere
sults
;D=
dura
tion
ofsy
mpt
oms;
d/c
=di
scha
rge;
DM=
diab
etes
mel
litus
;DV
=de
pend
entv
aria
ble;
Dx=
diag
nosi
s;ER
=em
erge
ncy
room
;ESR
D=
end
stag
ere
nald
isea
se;E
X=
excl
usio
n;F=
fem
ale;
h=
hour
;H=
hosp
ital;
HgB
=he
mog
lobi
n;Hx
=m
edic
alhi
stor
y;I=
incl
usio
n;IV
=in
depe
nden
tvar
iabl
e;IV
DA=
intra
veno
usdr
ugab
use;
La=
seru
mla
ctat
e;LE
=lo
wer
extre
mity
LO=
loca
tion;
LOS
=le
ngth
ofst
ay;
LRIN
EC=
labo
rato
ryris
kin
dica
torf
orne
crot
izing
fasc
iitis
scor
e;M
=m
orta
lity;
Ma
=m
ale;
MV
=m
ultiv
aria
te;N
a=
seru
mso
dium
;NPV
=ne
gativ
epr
edic
tive
valu
e;N
STI=
necr
otizi
ngso
fttis
sue
infe
ctio
n;Or
=od
dsra
tio;O
R=
oper
atin
gro
om;P
ath
=pa
thol
ogy;
PE=
phys
ical
Exam
;po
=or
al;P
PV=
posi
tive
pred
ictiv
eva
lue;
Pts
=pa
tient
s;SB
P=
syst
olic
bloo
dpr
essu
re;S
C=
surg
ery
cons
ult;
Se=
sens
itivi
ty;S
p=
spec
ifici
ty;S
STI=
skin
and
soft
tissu
ein
fect
ion;
SU=
time
from
pres
enta
tion
tosu
rger
y;Sx
=sy
mpt
oms;
T=
tem
pera
ture
;Te
=te
rtiar
y;Tr
=tru
nk;T
x=
trans
ferr
ed;U
=ur
ban;
UE=
uppe
rext
rem
ity;U
V=
univ
aria
te;V
S=
vita
lsig
ns;W
BC=
whi
tebl
ood
cell;
w/o
=w
ithou
t.
94 Second Quarter 2012 �Worldviews on Evidence-Based Nursing

Clinical Pathways to Aid in the Diagnosis of Infections
TABLE 2Synthesis table
CHAN FRAZEE HOLLAND HSIAO SU WALL WALL #2 WONG YAGHOUBIAN
Year 2008 2008 2009 2008 2008 2000 2000 2004 2007Retrospective X X X X X X X XProspective XNumber of subjects 21 122 28 128 209 42 359 314 124DemographicsMean age 42 44 61 57 39 45 56% Males 90 64 80 67 70 81 77 60 69% IV drug user 29 80 4 67 71 31% Diabetic 52 22 59 56 14 19 71 38% renal dz 5 4 22% liver dz 5 11 28 19 19%HIV 4 10% Cancer 7PVD 23No co morbidities 19 25 14Findings% Mortality 16 19 21 21 17% Amputation 4 17 26 15Time to SE 3.5 hTime to OR 8.4 h 60.4 h 28.7 +/– 51.7 h 8.5 h% Diagnosed correctly on admission 59 38 67SettingAcademic X X X X XTertiary X X X X XCommunity X X XUnited States X X X X XTaiwan X XSingapore XAustralia XIndependent variablesLRINEC X X XCRP X X XWBC >15 X X X X X X X X XBands > 10% XNa < 135 X X X X X X X XLactic acid> XCr X X X X XBUN X XSBP < 100 X X X X XSQ gas X X X X XTemp >38◦C X X X XHR >100 X X XRR>20 XPain X X XHard signs X X XAdmit to nonsurgical service XDependent variablesMortality X X X XDx of NSTI X X X XDx of SSTI XAmputation XNonsevere NSTI XSevere NSTI XNote. Cr = creatinine; CRP = C reactive protein; DV = dependent variable; Dz = renal disease; ER = emergency room; IVDA = intravenous; LRINEC = laboratoryrisk indicator for necrotizing fasciitis score; Na = serum sodium; NSTI = necrotizing soft tissue infection; OR = operating room; PVD = peripheral vasculardisease; SE = surgical evaluation; Temp = temperature.
Worldviews on Evidence-Based Nursing �Second Quarter 2012 95

Clinical Pathways to Aid in the Diagnosis of Infections
TABLE 3Laboratory risk indicator for necrotizing fasciitis (LRINEC) score
C REACTIVE PROTEIN
< 150 0 points≥ 150 4 points
White cell count< 15 0 points15–25 1 point> 25 2 points
Hemoglobin>13.5 0 points11–13.5 1 point< 11 2 points
Sodium≥135 0 points<135 2 points
Creatinine≤ 1.59 0 points> 1.59 2 points
Glucose≤ 180 0 points> 180 1 point
intervention (e.g., objective laboratory data with clinicaljudgment to diagnose NSTIs) was clearly delineated, theintervention would readily be described as effective in aparticular setting, for a particular population. From the re-ports reviewed, the diagnostic interventions as applied tothe development of a CPG for diagnosis of NSTIs appearsto be effective using a variety of patient cohorts, and is ef-fective in some settings, but not others, and is effective inoutcomes such as early diagnosis, morbidity, and mortalityoutcomes.
While this evidenced-based review of the clinical out-comes of interventions using the LRINEC scoring systemshow emerging support for the use of this intervention, theissues of applicability and generalizability remain a discus-sion point. Clinicians may perceive available evidence doesnot apply to their settings due to disparate participant char-acteristics or insufficient contextual information offered inreports to ascertain applicability. These issues present aschallenges associated with changing clinician behavior andwill impact clinical interventions for improved patient careoutcomes (Litaker et al. 2006). This application in healthcare has tended to be mechanistic, with undesirable vari-ation in health service delivery and should be consideredwhen designing and implementing any CPG. Standardiz-ing care using CPGs without identifying desirable variationor unique adaptations that take advantage of system op-portunities and strengths misses an important prospect to
implementing interventions in complex adaptive systems(Berwick 2003).
LIMITATIONS
While this review primarily focused on efficacy of the in-terventions, the discussion is not complete without a briefnotice of the translation of the intervention to acutely illpatients in the ED setting. And for this notice, the interven-tions reviewed need to be considered for their treatmentevaluation and in the case of LRINEC, the preliminary na-ture of the data. Applied to clinical practice change, inter-vention theory provides a systematic approach to interven-tion development, implementation, and evaluation, anddirects us in moving from outcomes focused approachesto those examining the central processes underlying inter-vention effects (Sidani & Sechrest 1999). When interven-tions are examined in light of explanations of the prob-lem amenable to treatment, critical inputs of the interven-tion, mediating processes, and expected outcomes of theintervention further an understanding of what interven-tions work, for whom, and under what conditions therebystrengthening causal inferences (Sidani & Sechrest 1999;Berwick 2003).
THEORETICAL APPLICATION
The problem in each of the reviewed interventions wasdefined as the “outcome” that is, reduced morbidity andmortality associated with this condition. More theoreti-cally appropriate would be a problem defined as “insuf-ficient means for rapid and accurate diagnosis” and theconceptual issue around a paucity of objective measures toguide clinical practice. This approach would clearly guideclinicians to include objective measures, diagnostics, andhard signs as measures of intervention applicability. Themajority of studies reviewed applied Physiologic Theoryas the conceptual framework guiding interventions. Thistheory provides an explanatory mediator of the degree ofbiologic response and potential for morbidity and mortal-ity in NSTIs.
These moderating variables influence the differential ef-fects of interventions across populations and settings andwill further strengthen our understanding of the evidenceavailable in development of CPGs to inform practice andimprove patient outcomes. Additional effort is needed todetermine the relevance of objective measures such as theLRINEC scoring system and its predictability in groupswith diverse cultural and socioeconomic backgrounds. Thefindings from this review suggest that evidence-based dis-ease management needs to focus on common underly-ing physiologic and prognostic constructs that will foster
96 Second Quarter 2012 �Worldviews on Evidence-Based Nursing

Clinical Pathways to Aid in the Diagnosis of Infections
NECROTIZING INFECTIONS
Pt presents to theemergency room with
signs of skin or soft tissueinfection (SSTI)
ER INITIATES WORKUP,CONSIDER FOLLOWING LABS:CBC, CMP, BLOOD AND WOUNDCULTURES, MAG,ESR, CRP, CK,
UA, LACTIC ACID
MEETADMISSIONCRITERIA?
ALOC, Sepsis, Rapidlyspreading lesion,
immunosuppression,failure of outpatienttreatment, co-morbidities,
noncompliance
Signs of a necrotizinginfection?
ORLRINEC >6?
Discharge homewith outpatienttreatment
STAT SURGICALCONSULT andANTIBIOTICS
(Vanco +Clinda +Zosyn). Consult IDand pharmacy for
Vancomanagement
YES
NO
YES
NO
LRINEC SCORE
CRP: < 150 0CRP > 150 4
WBC < 15 0WBC 15-25 1WBC >25 2
Hgb >13.5 0Hgb 11-13.5 1Hgb <11 2
Na> 135 0Na< 135 2
Cr < 1.59 0
Cr >1.59 2
Glucose <180 0Glucose >180 1
Bullae, skin ecchymosisor sloughing, presenceof gas in the tissues,skin anesthesia, painout of proportion to theexam, edema that
extends beyond the skinerythema, rapidlyspreading infection,
FollowHospital
Standard ofCare forFurtherTreatment
Figure 1. Clinical practice guideline.
improved diagnosis, early communication and referral, andprompt treatment to reduce morbidity and mortality in thepresence of NSTIs.
Bennet and Bennet (2004) discuss a theoretical frame-work underpinning system complexity. Advances in tech-nology are one factor contributing to the world becominga more complex organism. Complexity theory representsthe interconnectedness and the sharing of knowledge thatoccurs within systems. Though there are many benefits to
ease in sharing information, it has also led to an increasein uncertainty and rapid growth and in order to surviveand be competitive in the current environment, individu-als and organizations must learn to adapt to these changesby staying abreast of the latest technologies while findingways to keep track of the information that is at their fin-gertips. The Intelligent Complex Adaptive System model(ICAS) has been developed as a possible way to accomplishchange and was used as the theoretical framework guiding
Worldviews on Evidence-Based Nursing �Second Quarter 2012 97

Clinical Pathways to Aid in the Diagnosis of Infections
the application of a clinical pathway for NSTI diagnosis ina large healthcare system (Bennet & Bennet 2004).
The foundation for the ICAS model revolves aroundeight fundamental characteristics: Permeable Boundaries,Selectivity, Flow, Optimum Complexity, Knowledge Cen-tricity, Multidimensionality, Shared Purpose, and Organi-zational Intelligence. The development of these strategiesstrengthens the organization and gives it tools to cope withthe challenges of living in a rapidly changing environment(Bennet & Bennet 2004).
Permeable Boundaries allow a system to be interactivewith the external environment so that they can be awareof external needs and respond appropriately. Selectivityis the process of filtering out endless information to seekout information that is pertinent to the system. Flow rep-resents the internal movement of people and knowledgewithin the system and across boundaries in response todemands. Optimum Complexity is the necessity to cre-ate a diverse internal system so that external complexitycan be challenged. Knowledge Centricity is the dynamicsharing of knowledge within an organization so that col-laboration can occur among the various parts of a systemto develop solutions to problems. Multidimensionality isthe importance of developing a broad base of knowledgethat extends beyond the boundaries of ones’ specific job re-quirements. Shared Purpose provides a shared vision anddirection among members of the system, and Organiza-tional Intelligence is the process of using the knowledgegenerated by the system to follow through with the ob-jectives and goals of the organization (Bennet & Bennet2004).
Drawing on the principles from the ICAS model, devel-opment of a CPG for NSTIs, information is shared withthe knowledge workers (healthcare providers) regardingNSTIs and the evidence-based recommendations to guidediagnosis and treatment. The workers will not be forced tocomply with these standards; however, it is anticipated thatcompliance with recommendations are achieved throughimplementation of the ICAS model constructs. Each iden-tified stakeholder plays a vital role in practice change andfluid interdependence and communication will drive anypractice change success. Frequent evaluation of systemprocesses enhance performance and projected outcomesthroughout all stages of CPG development and implemen-tation.
While conceptual models and theoretical frameworkswere not clearly stated in the majority of the reviewedinterventions, what was clear is how theoretical mediat-ing variables contributed to outcome changes in terms ofaccurate diagnoses and guides for clinician judgment. Lim-itations to the efficacy of objective measures designed toevaluate the presence of predictors of NSTIs may be re-
lated to a simplistic “black box” approach that focuses ondetermining whether an intervention worked or did notwork, without consideration of the systems’ internal work-ings (Sidani & Sechrest 1999). A more effective emphasismight be on the interpretation of the causal connection be-tween the intervention (objective data plus clinician judg-ment) and the intended outcome. Understanding the bio-logic and physiologic mechanisms underlying the NSTIs,without consideration of contextual variables and clinicaljudgment, may lead to overestimation of the condition andimplementation of intervention protocols.
MEDIATING PROCESSES
This review demonstrated that contextual variables such asage, setting, location of infection, socioeconomic factors,and marital status were not specified as influencing out-comes and related interventions. What is unclear is that ifthese variables had additive or a singularly influential ef-fect on early diagnosis or outcome of disease. Missing fromthis review is information that assesses the confoundingdiversity that exists between initial case presentation, pop-ulation characteristics, factors related to clinical decisionmaking and its effect on time to diagnosis.
Examination of interventions for early diagnosis andprompt treatment of NSTIs requires attention to the pop-ulation experiencing the problem of interest, or clarify-ing for whom and under what conditions an interventionmight be most effective. In the ED setting, moderatorsare the context and characteristics of patients presentingfor care and are important considerations in the designand evaluation of intervention effectiveness and general-izability of any CPG. Salient moderators of interventioneffect were clearly addressed in the majority of studiesto explain intervention effects. The overall low incidence,general predominance of men, and lack of significant eth-nic representation in the reviewed studies would requireconsideration of gender and ethnicity in any interventionimplementation. Understanding the participant character-istics and biologic or sociologic interactions such as age,gender, ethnicity, and socioeconomic status, in additionto infection location, comorbid diagnoses, and time to di-agnosis will aid in the application and generalizability ofa CPG in the early diagnosis and prompt treatment ofNSTIs.
CONCLUSIONS
Specific interventions described in this review can be trans-lated to the development and implementation of a CPG asa process of evidence-based practice in acute care settings,specifically the ED where patients are most likely to first
98 Second Quarter 2012 �Worldviews on Evidence-Based Nursing

Clinical Pathways to Aid in the Diagnosis of Infections
present for care. Successful engagement of diagnostic andpathway protocols for relevant changes within complex or-ganizational systems can be initiated through applicationof clinical evidence, shared vision, organizational mission,and incorporation of individual values, while ensuring re-sources are strategically utilized. A complex healthcare sys-tem culture requires focus on translating diagnostic andcare improvements for acutely ill patients presenting withelusive and clinically challenging disease, while consid-ering the interdependent variables of complex adaptivesystems found in health care today. The evidence-basedpractice process is an integral part of translational researchusing champions of change to develop new pathways ofcare through individual mentorship and system-wide ed-ucation. These processes mediate the rapid engagement ofnew research, change clinician practice, and ultimately re-duce morbidity and mortality of patients presenting withSSTIs, preventing development of these early signs into lifethreatening NSTI.
ReferencesBennet A. & Bennet D. (2004). Organizational survival in
the new world: The intelligent complex adaptive system.Burlington, MA: Elsevier.
Berwick D. M. (2003). Disseminating innovations in healthcare. Journal of the American Medical Association, 289,1969–1975.
Chan T., Yaghoubian A., Rosing D., Kaji A. & de VirgilioC. (2008). Low sensitivity of physical examination find-ings in necrotizing soft tissue infection is improved withlaboratory values: A prospective study. American Journalof Surgery, 196(6), 926–30; discussion 930.
Ellis Simonsen S.M., van Orman E.R., Hatch B.E., JonesS.S., Gren L.H., Hegmann K.T. & Lyon J.L. (2006). Cel-lulitis incidence in a defined population. Epidemiologyand Infection, 134, 293–299.
Endorf F.W., Cancio L.C. & Kelin M.B. (2009). Necrotiz-ing soft-tissue infections: Clinical guidelines. Journal ofBurn Care and Research, 30(5), 769–775.
Frazee B.W., Fee C., Lynn J., Wang R., Bostrom A., Har-gis C. & Moore P. (2008). Community-acquired necro-tizing soft tissue infections: A review of 122 casespresenting to a single emergency department over 12years. The Journal of Emergency Medicine, 34(2), 139–146.
Holland M.J. (2009). Application of the laboratory riskindicator in necrotising fasciitis (LRINEC) score to pa-tients in a tropical tertiary referral centre. Anaesthesiaand Intensive Care, 37(4), 588–592.
Hsiao C.T., Weng H.H., Yuan Y.D., Chen C.T. & ChenI.C. (2008). Predictors of mortality in patients with
necrotizing fasciitis. The American Journal of EmergencyMedicine, 26(2), 170–175.
Kohn L. (2000). To err is human: An interview with the In-stitute of Medicine’s Linda Kohn. The Joint CommissionJournal on Quality Improvement, 26(4), 227–234.
Litaker D., Tomolo A., Liberatore V., Stange K.C. &Aron D. (2006). Using complexity theory to build in-terventions that improve health care delivery in pri-mary care. Journal of General Internal Medicine, 21, 530–534.
May A.K., Stafford R.E., Bulger E.M., Heffernan D., Guilla-mondegui O., Bochicchio G. & Eachempati S.R. (2009).Treatment of complicated skin and soft tissue infections.Surgical Infections, 10(5), 467–499.
Sidani S. & Sechrest L. (1999). Putting program theoryinto operation. American Journal of Evaluation, 20(2),227–238.
Stevens D.L., Bisno A.L., Chambers H.F., Everett E.D.,Dellinger P., Goldstein E.J.C., Gorbach S.L., HirshmannJ.V., Kaplan E.L., Montoya J.G. & Wade J.C. (2005).Practice guidelines for the diagnosis and managementof skin and soft-tissue infections. Clinical Infectious Dis-eases: An Official Publication of the Infectious DiseasesSociety of America, 41(10), 1373–1406.
Su Y.C., Chen H.W., Hong Y.C., Chen C.T., Hsiao C.T. &Chen I.C. (2008). Laboratory risk indicator for necro-tizing fasciitis score and the outcomes. ANZ Journal ofSurgery, 78(11), 968–972.
Wall D.B., de Virgilio C., Black S. & Klein S.R. (2000).Objective criteria may assist in distinguishing necrotiz-ing fasciitis from nonnecrotizing soft tissue infection.American Journal of Surgery, 179(1), 17–21.
Wall D.B., Klein S.R., Black S. & de Virgilio C. (2000).A simple model to help distinguish necrotizing fasciitisfrom nonnecrotizing soft tissue infection. Journal of theAmerican College of Surgeons, 191(3), 227–231.
Wong C.H., Khin L.W., Heng K.S., Tan K.C. & LowC.O. (2004). The LRINEC (laboratory risk indicatorfor necrotizing fasciitis) score: A tool for distinguishingnecrotizing fasciitis from other soft tissue infections.Critical Care Medicine, 32(7), 1535–1541.
Wright S.W., Trott A., Lindsell C.J., Smith C. & GiblerW.B. (2008). Evidence-based emergency medicine. Cre-ating a system to facilitate translation of evidence intostandardized clinical practice: A preliminary report. An-nals of Emergency Medicine, 51(1), 80–6, 86.e1–8.
Yaghoubian A., de Virgilio C., Dauphine C., Lewis R.J.& Lin M. (2007). Use of admission serum lactate andsodium levels to predict mortality in necrotizing soft-tissue infections. Archives of Surgery, 142(9), 840–846;discussion 844–846.
Worldviews on Evidence-Based Nursing �Second Quarter 2012 99