products - northern speech services€¢ products. aspiration pneumonia ... james l. coyle, phd,...
TRANSCRIPT

Providing Quality A!ordable Continuing Education and Treatment Materials for over 30 years.
117 North Elm AvenueP.O. Box 1247
Gaylord, Michigan 49734Phone: 888.337.3866
Fax: 888.696.9655Email: [email protected]
www.northernspeech.com
• CE Seminars• On-line CEUs• Products

2/6/2010
1
Dysphagia Practice: Aspiration Pneumonia and the Role of the Speech‐Language PathologistMarch 6th, 2010Pittsburgh, PA
James L. Coyle, Ph.D., CCC‐SLP, BRS‐S ([email protected])Department of Communication Science and DisordersUniversity of Pittsburgh
Outline
• 8:00–8:30 Anatomy and Physiology of the Respiratory System R/T Dysphagia
• 8:30–9:30 Pneumonia Types; Differential Diagnosis of Aspiration Pneumonia
• 9:30–9:45 Break• 9:45–11:15 Differential Diagnosis of AP (continued)• 11:15–12:15 Lunch (on your own)
2
5 5 ( y )• 12:15–1:00 Non‐Dysphagia Pneumonia Risk Factors:
Attributing Risk With Logic• 1:00‐1:45 Pulmonary Function Tests and Treatments for
Respiratory Diseases• 1:45–2:00 Break• 2:00–2:45 Dysphagia Interventions and Aspiration: Thick
Liquids, Water Protocols, (Tubes), and Common Sense• 2:45–3:45 Case Studies
Dysphagia is Not a Disease
D h i
Disease, Condition:
Disease, Condition:
3
DysphagiaNeurologicTraumaticNeoplasticStructuralIatrogenic
“Deconditioning”Pulmonary
Others
PulmonaryNutritional
Community -AcquiredSocial
PsychologicalOthersAging
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
2
Medical SLP
Role of Modern Medical SLP
What is the nature of the patient’s dysphagia?
How likely is current disease related to dysphagia?
What is risk of future disease due to dysphagia?
Can that risk be lowered?
How?
These questions are far less commonly asked by referring physicians, of other professionals
4
Medical SLP
Adverse outcomes in our patients
Pulmonary diseases
Malnutrition, dehydration
Blood glucose managementg g
Airway obstruction
Social isolation, depression
All are costly (economic cost)
Most can cause premature death (human cost)
5
Essential Knowledge
Anatomy, physiology respiratory system
Pathophysiology of common conditions
Natural history of common conditions
Eff t d id ff t f di ti Effects and side effects of common medications
What do test results mean
Imaging, laboratory, bacteriology, PFT, etc.
What is considered “normal” swallowing function?
6
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
3
Pre‐test
Where does diaphragm’s innervation originate?
What cranial nerve supplies facial sensation?
What about tongue sensation?
All i t h i ll i ti All pneumonias are technically aspiration pneumonias. True or false?
Feeding tubes prevent aspiration. True or false?
Eliminating dysphagia is the best way to reduce aspiration pneumonia risk. True or False?
7
Aerodigestive tract anatomy
8
Digestive:
9
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
4
Digestive System
FOOD
10
Inside the body, cells, absorbed nutrients
waste
Digestive System
Esophagus ‐Transports food to digestive system
Stomach ‐ Breaks down proteins
Duodenum ‐ Breaks down fats, carbohydrates
Jejunum ‐Absorbs carbohydrates and proteins
Ileum –Absorbs fats
Colon: transport waste, absorb water Cecum, ascending, transverse, sigmoid, rectum…
11
Digestive System
Esophagus
Muscular tube
Sphincters
Pierces diaphragm
Bolus transit
12
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
5
Digestive System
Stomach
GE junction
Fundus, body, pylorus
Pyloric sphincter
13
Pyloric sphincter
Mucosa secretes:
HCl
Proteolytics
Hormones
Mucus
Digestive System
Duodenum
14
Digestive System
Jejunum
Villi absorb dissolved nutrients
Nutrients transported in blood to target organs
15
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
6
Digestive System
Large intestine
Removes water from remaining waste
Eliminates waste FO
16
OD
waste
Aero:
17
Respiratory System Functions
Ventilation
Transfer of oxygen rich air into lungs
Transfer of oxygen depleted/waste air out of lungsg
Respiration
Transfer of oxygen to circulatory system, then to working organs
Removal of some metabolic waste from working organs, via circulatory system
18
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
7
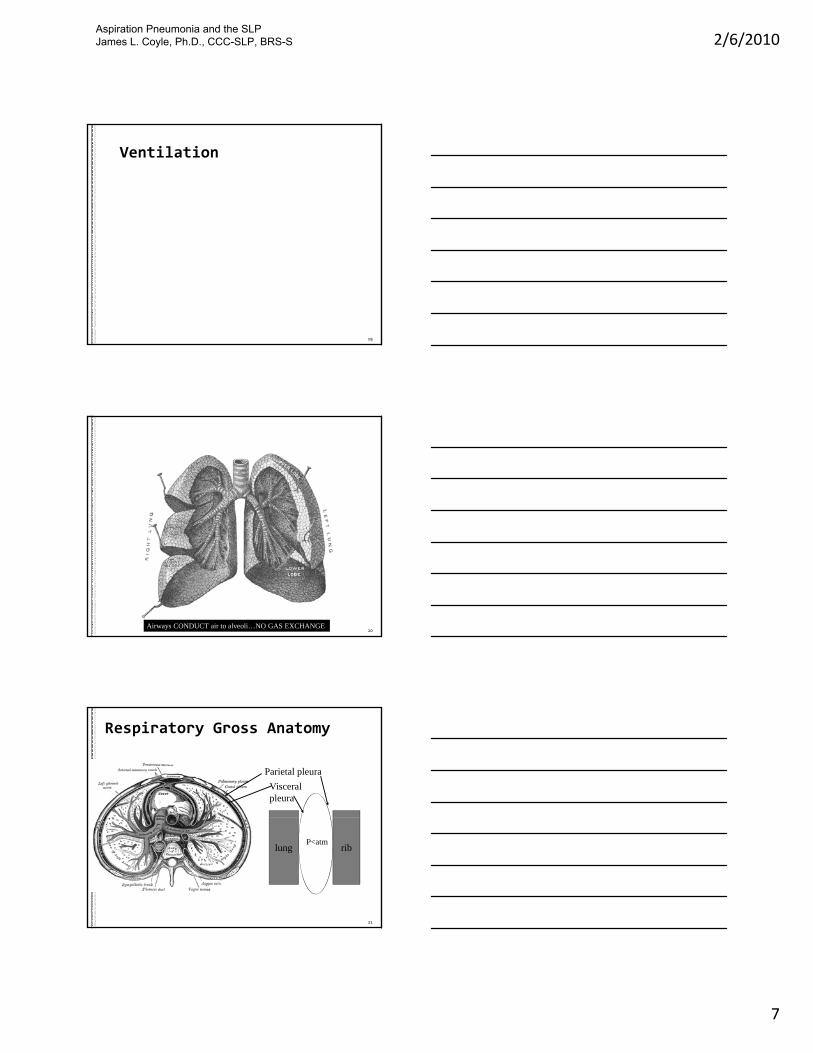
Ventilation
19
20Airways CONDUCT air to alveoli…NO GAS EXCHANGE
Respiratory Gross Anatomy
Parietal pleura
Visceralpleura
21
riblungP<atm
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
8
Ventilation Principles
Lungs (alveoli) have a tendency to collapse
Elastance (or surface tension)
Chest wall has a tendency to expand
Elastance Elastance
Chest wall is connected to lungs, which
Maintains lungs partially inflated at rest
Maintains chest wall partially collapsed at rest
22
Major Events in Ventilation
PhrenicNerve
activates diaphragm
Diaphragm contracts,
pulling on lung and pushing on
viscera
Alveolar inertia
overcome, lung volume increases
Atmospheric air fills
Intra‐alveolar pressuredecreases
(Boyle’s Law)
Al l i i
Inspiration
Expirationair fills
pressure void in lungs
Phrenic nerve impulses cease,
diaphragm relaxesElasticity of
viscera, alveoli are now
unopposed
Compressed viscera, stretched
alveoli, recoil
Alveolar volume
decreases, pressure increases
Alveolar air is “pushed” out
to atmosphere
23
Ventilation‐Rest= Pleural linkage
24
ribrib
Diaphragm
lunglung
P=Patm P=Patm
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
9
Ventilation‐Inspiration
25
ribriblunglung lunglung
P<Patm P<Patm
Ventilation‐Expiration
26
ribrib
Diaphragm
lunglung
P>Patm P>Patm
27
Inspiration Expiration
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
10
Respiration
28
Terminal Respiratory Structures
Respiratory Gross AnatomyRespiratory Gross Anatomy
29
Terminal Respiratory Structures
Respiratory Gross AnatomyRespiratory Gross Anatomy
30
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
11
Respiration
Physiologic requirements
Eliminate accumulated waste
Acquire nutrients
Oxygen and Carbon Dioxide concentrations Oxygen and Carbon Dioxide concentrations are balanced by the respiratory system
31
Medullary, peripheral centers sensitive to pH changes
Rate, depth of ventilation quickly altered by response to pH
32
Photo: John A Beal, PhDDep't. of Cellular Biology & Anatomy, Louisiana State University Health Sciences Center Shreveport
Lungs
Circulation&
Respiration
ExternalRespiration
(Blood Atmosphere)
capillaries
Right Heart Left
Heart
33
Give Off CO2Pick Up O2
InternalRespiration
Blood Organs
Working Tissues & Organs
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
12
External External RespirationRespiration
Alveoli exchangewith blood
34
with blood
Breathing and Swallowing
35
Respiration and Deglutition
Upper aerodigestive tract is shared
Ventilation stops Ventilation stops with swallowing (apnea)
Larynx closes “bottom to top”
36
Charbonneau et al., 2005; Hiss et al., Charbonneau et al., 2005; Hiss et al., 2003; 2003; Perlman et al., 2005 Perlman et al., 2005
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
13
Normal Spirometry
IRVInspiration (expansion)
Max. lung volume
37
TV
ERV
REL
RV
Expiration (“collapse”)
Seconds>. . . . . .
20 s.
RR=20
breaths
Respiration and Deglutition
In Normals...
Exhale Swallow Exhale; Young and Old1
Respiratory rate (young) is about 16/min.2
“ “ (elderly) “ “ 20/min.y
Total Swallow Duration, Swallow Apnea Duration3
Increase with age
Decrease with lower lung volumes
38
1.1. Perlman et al., 2005; Hiss et al., 2002; Leslie et al., 2002; Perlman et al., 2005; Hiss et al., 2002; Leslie et al., 2002; 2.2. Leslie et al., 2002;Leslie et al., 2002;3.3. Gross et al., 2003; Hiss et al., Gross et al., 2003; Hiss et al., 2003; 2003; Leslie et al., 2005.Leslie et al., 2005.
inspiration Swallow apnea1.5 – 2.5 seconds
Total Swallow Duration=1.5 – 2.5 seconds
Normal Respiratory Rate‐swallow on expiration
expiration
Seconds
Respiratory Rate = 16/min
39
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
14
Exhalation begins Swallow begins Swallow ends, exhalation resumes
40
One swallow
Respiration and Deglutition
Subglottic pressure
volume
swallow
41
pressurepA
+
_
tongue
mandible
Thyrohyoid
mandiblemandible
epiglottis
mandible C4
bolus
velumvelum
valleculae
Rest breathingInhalation: pressure above atmosphericExhalation: pressure below atmospheric
42
larynxlarynx
C7
C6
C5Post. Phar.
wall
UES
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
15
mandible
tongue
mandiblemandiblemandible C4
bolus
velumvelum
Thyrohyoid
Swallow breathing‐swallow onsetTakes place at onset of exhalation
4343
larynxlarynx
C7
C6
C5Post. Phar.
wall
Airflow from lungsPressure > atmospheric
mandiblemandible
Tongue
mandiblemandible C4
bolus
velum During SwallowExhaled airflowobstructed by
mechanical closure
444444
larynx
C7
C6
C5Post. Phar.
wall
UES
Airflow from lungsPressure > atmospheric
Breathing and swallowing
Abnormalities
Stroke: volumes, duration, airflow direction
Shorter cycle duration at rest*
Direction of airflow after swallow**
Normals: 96% expiration after swallow
Stroke: 60% expiration after swallow (p<.01)
Laryngectomy ***
Evidence of maintained pattern in laryngectomy
45
*,**Leslie et al., 2002 a,b***Charbonneau et al., 2005
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
16
Breathing and swallowing Abnormalities
Cheyne Stokes respiratory pattern
Periodic apnea 1 minute
46
inspiration
Swallow apnea1.5 – 2.5 seconds
Breathing and swallowingAbnormalities: Tachypnea
Abnormalities
expiration
Seconds
Respiratory Rate = 36/min
Abnormalities
47
Pneumonia and Respiratory Diseases
480830
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
17
Aging and Disease
2005: 20 million chronic‐disease deaths
Cardiovascular 30%
Cancer 13%
Chronic respiratory 7%p y 7
Diabetes mellitus 2%
Devastating events and comorbidity
Stroke, neurodegenerative disease PLUS above
49
Pneumonia
Most frequent infectious cause of death*
2nd most common nosocomial infection (UTI) in hospitals*** 13%‐48% of all Nursing Home Infections
6 d h i ** 63,000 deaths in 2003**
40% higher incidence in elderly
Case fatality rate 55% (elderly)
50
Marston, et al., 1997*; National Center for Health Statistics, 2003**; ***Niederman, et al., 2002;
What is Pneumonia?
Causes
Microbiological etiology
Pneumococcal, Legionnaire’s, RSV, bacterial
Location (site)
h l l l b l l b Bronchoalveolar, lobular, lobar
Type
Primary (inhale or aspirate pathogen)
Secondary (opportunistic pathogen infects damaged epithelium)
51
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
18
What is Pneumonia?
Setting of onset
Community acquired pneumonia
Health care associated (nosocomial) pneumonia
Predisposing factors
Ventilator associated pneumonia
Aspiration pneumonia
52
What is Pneumonia?
An inflammation of pulmonary parenchyma (alveoli, airways, both)…
C d b i f ti …Caused by infectious pathogens
Treatment:
Infection must be treated
Respiratory distress, failure must be treated
53Illustration: Patrick J. Lynch
What is Pneumonia?
Phase 1: Edema
Pathogen infiltrates, infects alveoli
Draws nourishment from alveolar epithelium
O2
p
Damaging alveolar epithelium
Producing metabolic byproducts (toxins)
Irritants to alveoli
Inflammation
54
Mandell & Wunderink, 2007Capillary – RBC, WBC
O2
O2
O2
O2O2
O2
CO2
CO2
CO2
CO2
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
19
What is Pneumonia?
Phase 2: Red hepatization phase.
Alveoli become excessively permeable
O2
permeable Red blood cells “leak” from capillaries
Immunological response Inflammation of the lung = Pneumonitis
55Capillary – RBC, WBC
O2
O2
O2
O2
O2
O2
CO2
CO2
CO2
CO2
What is Pneumonia?
Alveoli fill with RBC, WBC, serum, infectious debris
Respiratory surface area is reduced by infiltrate
Dyspnea, hypoxemiaO2
O2O2
O2
O2
CO2
Dyspnea, hypoxemia
Epithelium thickens
Surfactant production is diminished
Reduces compliance of lung
…further source of dyspnea
Can spread with cough
56capillary
O2
O2 CO2
CO2
CO2
Infiltrates Clear alveoli
57
Thickened epithelium
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
20
What is Pneumonia?
Phase 3: Gray hepatization phase
RBC’s destroyed
Infection contained
Bacteria absent
O2
Bacteria absent
Infiltrates diminish
Phase 4: Resolution
Immunological “clean‐up”
Epithelium “heals”, surfactant restored
58capillary
O2
O2
O2
O2
O2
O2
CO2
CO2
CO2
CO2
Types of Pneumonia
CAPNosocomialPneumonia
All PneumoniaBacterial, viral, Legionella, RSV, etc.
59
DAPNon‐DAP
TypicalVAP
Atypical
AspirationPneumonia
DAP = Dysphagia‐related Aspiration Pneumonia
Non‐VAP
Types of Pneumonia
Community Acquired Pneumonia (CAP)
Pneumonia not acquired in a health care facility
4‐5 million cases per year* **
600 000 hospitalizations 45 000 deaths** 600,000 hospitalizations, 45,000 deaths**
Incidence**
12 per 1000 persons
20 per 1000 elderly persons (60% greater)
60
*Niederman, 2002; **Mandell & Wunderink, 2007
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
21
C.A.P.
Pathogens responsible
Typical: Streptococcus, Klebsciella pneumoniae
Atypical *: H. influenzae, RSV, Legionella, E. coli, Staph. aureus, others
61
*El Solh, et al., 2001; CDC guidelines
Cost of CAP
Human Costs of Community Acquired Pneumonia
Pneumonia after stroke*
26.9% mortality, vs. 4.4% in stroke w/o pneumonia
Economic Costs of Community Acquired Pneumonia
Cost of pneumonia: $8‐10 billion (1998)** ***
62
*Katzan, et al., 2003; ** Niederman, et al., 1998; Mandell & Wunderink, 2007
Types of Pneumonia
Nosocomial Pneumonias: Ventilator Associated, Nursing Home Acquired Pneumonia
Pathogens:
Pseudomonas aeruginosa, Proteus species, staph. Aureus
63MRSA P.mirabilis
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
22
Types of Pneumonia
Ventilator Associated Pneumonia
Exposure to mechanical ventilation
Contaminated respiratory circuits
Contaminated suction, bronchoscopic equipment
Gastroesophageal reflux common in Ventilation
Early, late onset
Early: typically CAP pathogens
Late: MRSA, other drug‐resistant pathogens
64
Aspiration Pneumonia (AP)
Aspiration
Foreign matter enters the respiratory system
Pneumonia
Infectious acute inflammation
Reaction to pathogen
Aspiration Pneumonia
Pulmonary infectioncaused by aspiration of colonizedmatter
65
Aspiration pneumonia
CAP
Nosocomial
Aspiration Pneumonia
AP can originate in the community or in a hospital/HCF
Has reached epidemic proportions in the US*
66*Baine, Yu, & Summe, 2001
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
23
Aspiration Pneumonia
Human Costs of Aspiration Pneumonia
AP admissions highest case‐fatality rate
23.1% during hospitalization*
Is fatal in 20%‐50% of confirmed cases Is fatal in 20%‐50% of confirmed cases
Annual mortality (1998 numbers) >25,000 annual deaths due to AP
Economic Costs of Aspiration Pneumonia
$1.5 billion
67
*Baine et al, 2001;
Importance:
If we reduce the incidence of AP by a modest 20%
5,000 saved lives each year
If we reduce the admissions or length of stay for AP by a modest 20%
$300 million saved
68
Data extrapolated from Mandell & Wunderink, 2007; Baine et al, 2001
Patient with dysphagia
…and other risk factors favoring pneumonia
aspirates colonized oral secretions
What is Dysphagia‐Related Aspiration Pneumonia (DAP)?
…aspirates colonized oral secretions
…causing infection of airways and/or alveoli
Where do these pathogens come from?
69
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
24
Oral biofilm development
70http://bioinfo.bact.wisc.edu/themicrobialworld/streptococci_biofilm.jpg; Public health image library #3074, Centers for Disease Control
Oral biofilm
Variety of microorganisms in dental plaqueOral anaerobes
How Does DAP Develop?
Host Risk Factors
Mental status, immunological health, oral condition, upper GI obstruction, etc.
What was aspirated?
And what is its pathogen load?
Iatrogenic Risk Factors (institutionalized)
Feeding tube, postoperative impairments, medications, etc.
71* CDC/MMWR 46, RR‐1, (1997); **Langmore et al, (1998)
Where Does DAP Develop?
Site of occurrence:
Can occur in a health care facility (HCF)
Nosocomial Aspiration Pneumonia
Can occur outside of the HCF
Community Acquired Aspiration Pneumonia
72
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
25
Aspiration Pneumonitis
Non‐Infectious
Acute Lung Injury caused by aspiration of caustic or particulate matter
Inflammation of alveoli by effects of irritants
No infection (sterile/non‐pathogenic material)
Inflammatory edema reduces surface area
Gastric contents
Sterile, acidic, caustic
Damage to airways, alveoli
73
O2O
O2
CO2
74capillary
2O2
O2
O2
O2O2
CO2CO2
CO2
O2
O2O2
O2
O2
O2
O2O2
CO2
CO2
CO2
CO2
CO2 CO2
A new source of AP?
Gastric contents are normally sterile
pH : 2‐3* (nothing can survive)
However….
When stomach is de‐acidified and patient When stomach is de acidified, and patient exhibits GE reflux or emesis, , aspirated, colonized gastric contents can produce pneumonia
Increased use of acid suppressing drugs**
Raise gastric pH to 4.0 to 6.0*
75
*Feldman & Barnett, 1991; **Laheij, et al., 2004.
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
26
A new source of AP?
Laheij et al., 2004*
365,000 patients
Users and non‐users of acid suppression drugs
Some were prior usersp
5,551 patients developed pneumonia
PPI users were twice as likely to develop pneumonia
OR = 1.94‐2.28
H2 receptor agonist users
OR = 1.36‐1.64
AND…Eurich, et al., 2010; Herzig, et al., 2009
76*Marik, 2001; Marik and Zaloga, 2002; Laheij, et al., 2004;
Distinguishing AP, Aspiration Pneumonitis, Other Pneumonias
77
The Medical Record contains important clues
HISTORY OF ONSET
The course and progression of the disease
Presence/absence of underlying source/cause of Presence/absence of underlying source/cause of aspiration
Results of lab, radiographic tests
78
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
27
Differential Diagnosis
Dysphagia‐related Aspiration Pneumonia (DAP)
Non‐dysphagia‐related Aspiration Pneumonia (NDAP)Pneumonia (NDAP)
Other pneumonias
79
DAP
Associated with dysphagia
Non‐dysphagia related AspirationPneumoniaPneumonia
Aspiration does not occur because of dysphagia
Safely swallowed material
Gastroesophageal reflux or emesis (colonized)
Deacidified gastric contents
80
DAP vs. other Pneumonias
1. Location of chest infiltrates
DAP: typically gravity dependent segments
Lower lobes an segments
DAP
segments
Position while aspirating
81
NDAP
Giorgio Conrad (P.D.)
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
28
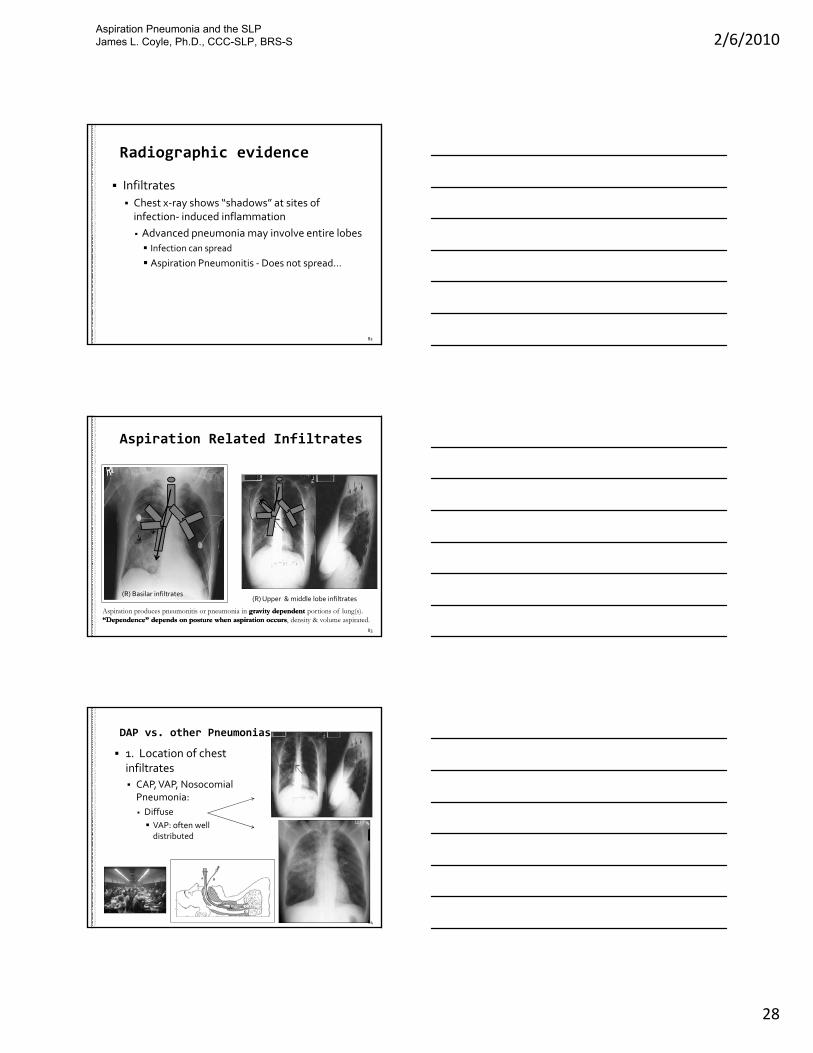
Radiographic evidence
Infiltrates
Chest x‐ray shows “shadows” at sites of infection‐ induced inflammation
Advanced pneumonia may involve entire lobes Advanced pneumonia may involve entire lobes
Infection can spread
Aspiration Pneumonitis ‐Does not spread…
82
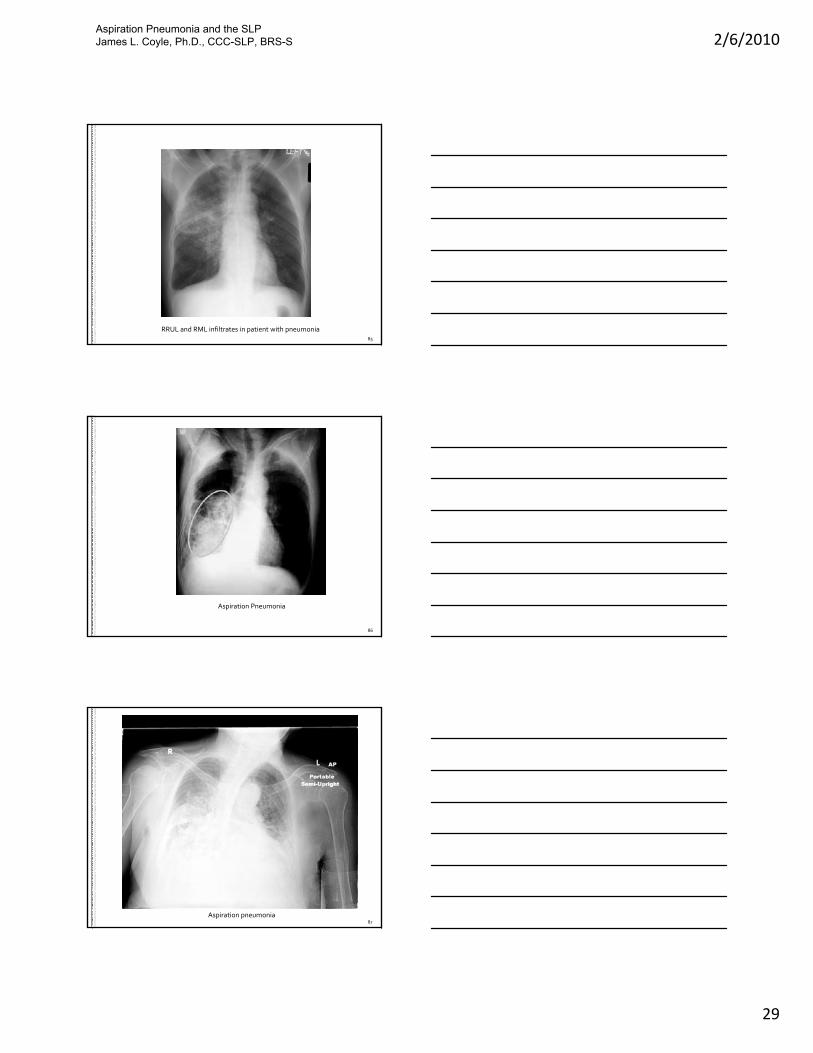
Aspiration Related Infiltrates
83
Aspiration produces pneumonitis or pneumonia in gravity dependentgravity dependent portions of lung(s).“Dependence” depends on posture when aspiration occurs“Dependence” depends on posture when aspiration occurs, density & volume aspirated.
(R) Basilar infiltrates(R) Upper & middle lobe infiltrates
DAP vs. other Pneumonias
1. Location of chest infiltrates
CAP, VAP, NosocomialPneumonia:
Diffuse
VAP: often well distributed
84
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
29
85
RRUL and RML infiltrates in patient with pneumonia
86
Aspiration Pneumonia
87
Aspiration pneumonia
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
30
88
Multilobar community acquired pneumonia
2. Signs and symptoms
DAP, CAP, Nosocomial Pneumonia: similar.
Dyspnea
Hypoxemia
Malaise
DAP vs. other Pneumonias
Malaise
Fever
Productive cough
Purulent sputum
Leukocytosis
89
3. Bacteriology
DAP: oral pathogens/oral flora
CAP: Strep. pneumoniae, Klebsciella pneumoniae, H. influenzae, RSV, Legionella, E. coli, Staph. aureus
VAP: pseudomonas, proteus species, Staph. Aureus
DAP vs. other Pneumonias
p , p p , p
Typically multiple organisms
Nosocomial pneumonia: pseudomonas, proteusspecies, Staph. aureus
Leukocytosis (elevated WBC)
Normal: 4.5 – 10.5 k cells/microliter
90
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
31
4. History
DAP: Dysphagia! Dysphagia‐producing disease, Symptom onset following oral intake; position during oral intake; esophageal dysmotility
Dependent for feeding/oral care, oral biofilm
DAP vs. other Pneumonias
91
4. History
CAP: pt. not institutionalized; insidious onset
Nosocomial Pneumonia: institutionalized patient, insidious onset
VAP: mechanically ventilated patient; typically
DAP vs. other Pneumonias
VAP: mechanically ventilated patient; typically NPO at onset
92
Examination data collection
5. Course of Pneumonia
What you see on assessment is not baseline
Elevated respiratory rate
Mental status
Cough is present in background
Count coughing before, during, and after oral trials
93
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
32
Examination data collection
Sign Interview Oral Facial Exam
Swallow Trials A
Swallow Trials B
Post‐swallow trials
Cough 112
0.4 sx/min all phases
11 3
0.4 before oral trials, 1.1 during oral trials, 0.2 after oral trials
Throat clear
Vocal quality
other
94
TimeTime Time TimeTime Time
duration duration duration duration duration
5 min 5 min 5 min 5 min 5 min
2
1
1
11 1
1 3
32
1
Summary‐pneumonia
Knowledge of normal and abnormal function is essential
Not just swallowing function…
Elderly possess many risk factors for pneumonia that are unique to the elderly
There are many clues pointing to, or away from, a diagnosis of DAP
95
Things to remember
Aspiration can occur without dysphagia
Aspiration is one potential source of pneumonia pathogens
Summary‐pneumonia
All respiratory illnesses are NOT dysphagia related
ALL PNEUMONIAS ARE NOTASPIRATION RELATED
Patient appearance with pneumonia is NOT baseline
History, course, physical signs are data for the SLP
96
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
33
Respiratory System & Diseases
The structures involved
The respiratory conditions seen in the elderly
Are they suspicious for a dysphagia etiology?
970945
Aging and Disease
Obstructive Diseases
Inspired air is obstructed from the respiratory membrane
Obstructed gas exchange
Respiratory pump works
Restrictive Diseases
Airflow or volume is mechanically restricted
Gas exchange is intact
Patient cannot inhale sufficient volume
98
Aging and Disease
Chronic respiratory conditions
COPD
Progressive airway/alveolar destruction (emphysema)
Chronic bronchitis
Congestive Heart Failure
Hypertension
Right heart, left heart
Pulmonary Edema, Pleural Effusions
Pulmonary Fibrosis
Asthma
99
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
34
Aging and Disease
Acute respiratory conditions
Pneumonia
Pneumothorax
Atelectasis
ARDS
Other acute pneumonitis
100
Respiratory Disease‐obstructive
Obstructive diseases air is “obstructed” from
contact with respiratory membrane
R d d l
obstruction
Reduced oxygen supply
Reduced waste elimination Acidosis
Increased respiratory rate Overlap with swallow
101
Alveolarmembranedestroyed
Airway Obstruction
Caused by dysphagia?
Very possible
Causes dysphagia?
Respiratory Disease‐obstructive
y p g
No
102
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
35
COPD
Chronic bronchitis
chronic mucus…obstruction
Emphysema
Alveoli and capillary destruction,
Respiratory Disease‐obstructive
p y ,
Resistance to blood flow into lungs
Can cause heart failure
Increased rate
Decreased cough effort
Reduced mucociliary clearance
103
Obstructive Pulmonary Disease
Respiratory membrane Respiratory membrane surface area is destroyedsurface area is destroyed
emphysemaemphysema
Respiratory membrane surface area is obstructed Chronic bronchitis
104
COPD: Caused by dysphagia?
Rarely but possible…
Chronic aspiration can produce
Alveolar destruction
Respiratory Disease‐obstructive
Airway disease
Asthmatic bronchitis
Chronic irritation due to chronic aspiration
105
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
36
CHF
106
Lungs
capillaries
CHF
Lungs
1. “Bottlenecked” Pulmonary Circulation (R) Ventricle Fails
2. “Bottlenecked” Systemic Circulation (L) Ventricle Fails
Right Heart
Left Heart
107
Give Off CO2Pick Up O2
Working Tissues & Organs
IntakeOutput
InterstitialFluid
Plasma
Lymphatics
Na+
Na+
Capillary membraneBlood Vessel
108
IntracellularFluid
Cell membrane
Fluid
Na+ Na+
Na
osmosis
Hypertension and Edema:Normal Fluid “Balancing” Working Organs
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
37
Intake HIGH PRESSUREOutput
Hydrostatic pressurepushes water into interstitial space around organs Interstitial
Fluid
PlasmaHIGH PRESSURE
Na+
Na+
Capillary membrane
Hypertension
Hypertension and Edema:
Abnormal Fluid “Balancing”
109
Cells/Organs
Cell membrane
Fluid
Na+ Na+
Na
osmosis
Cells/Organs
Common in CHF hypertension
Caustic ingestion Increased capillary permeability
Obstructive Pulmonary Disease
Pulmonary Edema
Pneumonitis
Increased rate / reduced inspiratory capacity
110
Respiratory Disease‐Restrictive
Restrictive Diseases
Limit amount of air that can be inhaled
Mechanical
restriction
Pain, paralysis, fibrosis
Poor compliance
111
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
38
Restrictive Pulmonary Disease
Asthma
A. Allergic/reactive
bronchial smooth muscle spasm
narrow airway, yincreased resistance, reduced flow
B. Asthmatic bronchitis
Mucus production
Obstructive component
112
Asthma Dysphagia related? Maybe. Chronic aspiration can cause
asthmatic bronchitis
Cause of dysphagia? Short‐term/acute, maybe
Respiratory Disease‐Restrictive
113
Restrictive Pulmonary Disease
Mechanically restrictive disease
Disable complete expansion of thoracic cavity
Kyphosis
Abnormally flexed thoracic spine, compressed thorax
Pulmonary fibrosis
Tough, leathery segments tether adjacent segments
Paralysis
114
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
39
Restrictive Pulmonary Disease
Dysphagia related?
Kyphosis, no
Pulmonary fibrosis? Maybe
Chronic aspirationp
Effects on respiration/swallow
Increased rate / reduced inspiratory capacity
115
Restrictive Pulmonary Disease Pneumothorax
Perforation caused by empyema/abscess
Chronic aspiration
116
Atelectasis
Areas of collapsed alveoli
Restrictive Pulmonary Disease
117
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
40
Restrictive Pulmonary Disease
Pleural Effusion
118
CHF (transudative), Inflammatory (exudative)
Aspiration and Lung Damage
Idiopathic Pulmonary Fibrosis (IPF)
Fibrosis: toughening
Idiopathic: from an unknown cause/etiology
Tobin et al., 1998
119
IPF
Aspiration Pneumonitis
Acute Lung Injury caused by aspiration of caustic or particulate matter
Restrictive Plus Obstructive
Restrictive
Inflammation of alveoli by effects of irritants
No infection Pulmonary edema
Obstructive
Fluid filled alveoli
120
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
41
Aspiration Pneumonitis
Gastric Contents: Massive Acute Inflammation
Sterile acidic Sterile, acidic
Airways, respiratory membrane damage
Opportunistic secondary infection
ARDS
121
ARDS
122Ware & Matthay, 2000
Normal acute resolution
Iatrogenic causes of respiratory conditions
Iatrogenic condition: a disease cause by treatment of another disease
Sedation (restrictive)
CNS depression
Disruption of pleural linkage (restrictive)
Cardiothoracic surgery
Phrenic nerve injury (restrictive)
Cardiothoracic surgery
123
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
42
Respiratory Swallow Tactics
Effects on interventions
Mainly on behavioral interventions
Timing of airway closure
Consider added fatigue of “eating and drinking”g g g
Increase respiratory rate even more?
Mitigating rate increases with supplemental O2
…because we can’t pull off more CO2.
124
Summary
Pulmonary disease affects swallow/breathing coordination
Pulmonary disease can cause, or be caused by, dysphagiaby, dysphagia
Mainly characterized by disruption of swallow‐respiratory coordination
1251115
Next – Risk Factors Favoring Pathogenesis of Pneumonia (Besides Dysphagia!)
126
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
43
Risk Factors for Pneumonia
Host Risk Factors
Something about the host (patient) predisposing them to an adverse outcome
Oral colonization, aging, dependence, underlying pulmonary, neurological or digestive disease
Iatrogenic Risk Factors
Increased risk for an adverse event caused by treatment of another condition
Medications, intraoperative injury, artificial airway
127
1215
Dysphagia‐a host risk factor
Little disagreement regarding dysphagia
Aspiration obstructs airways
Enables secondary infection
Stroke, neurological diseases, cause dysphagia, g , y p g
But pneumonia is always multifactorial…
We often CANNOT eliminate dysphagia
What else can we do to mitigate pneumonia risk?
128
Non‐Dysphagia Risk Factors
Langmore, et al., 1998
189 institutionalized males (non‐ICU)
CSE, VFS, 3 scintigraphic exams (GE reflux, esophageal motility)
Half also had FEES test
VFS repeated if dysphagia suspected
Dental exam, salivary flow measurement, saliva and throat cultures, interview (repeated annually)
Outcome: pneumonia
SBC >12,000 + fever >100.5F + new infiltrate on CXR
129
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
44
Non‐Dysphagia Risk Factors
Patients who developed pneumonia had significantly more:
Feeding tubes in place
COPD, CHF, GI diagnoses, , g
Decayed teeth, periodontitis, did not brush teeth
Multiple medical diagnoses, multiple medications
Dependent for oral care and feeding
Reduced activity
What is the evidence in these areas?
130
Feeding Tubes‐iatrogenic
Feeding tubes as pneumonia risk factor
Bacterial contamination of stomach and mouth*
44% PEG, 54% NG
E. coli, Proteus, multi‐organism: NG > PEG (p<.001)
Feeding tube reservoirs contaminated**
44% stroke patients with NG develop pneumonia***
…without worsening dysphagia****
131
Segal, et al., 2006; **Wagner, et al., 1994; ***Dzeiwas et al., 2004; Dzeiwas et al., 2008
Feeding Tubes
Pneumonia incidence is high *, **, ***, ****
Short‐term, long‐term
Other complications
Agitation and self extubation*g
Do not improve risk of death or poor outcome #
132
*Ciocon, et al., 1988; Dzeiwas et al., 2004; Finucane, et al., 1996; Gomes et al., 2004# Lindeboom, 2005
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
45
Pulmonary Disease‐host risk
COPD
Alters swallow physiology
Inspiration following swallow more frequent*
Damaged mucociliary clearanceg y
Reduced ability to clear contaminants
Impaired cough
133*Gross et al., 2009;
Pulmonary Disease
CHF
Increased respiratory rate due to
Pleural effusion, pulmonary edema
COPD and CHF: present significantly more in patients diagnosed with pneumonia *, **
134
Langmore et al., 1998; Langmore et al., 2002
Pulmonary Disease
Active smoking
4.1 times higher pneumonia risk *
Pharyngeal and glottic protective reflexes are attenuated by active smoking**
135
Langmore et al., 1998; Dua et al., 2002
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
46
Medications‐iatrogenic
Antipsychotics*
60% increase pneumonia risk in a case‐control study of elderly patients
Risk in first week of treatment: 450% increase
Subsides (does not disappear) over time
Most events with atypical antipsychotics
Clozapine, Abilify, Risperdal
Extrapyramidal effects, sedation
Typical drugs: sedation (haloperidol, chlorpromazine
136
*Knol, et al., 2008;
Medications
Multiple medications
Increase risk of pneumonia 15% *
Medications that reduce LES tone
Cholecystokinin secretin progesterone Cholecystokinin, secretin, progesterone, glucagon, neurotensin, dopamine, atropine, butylscopolamine, theophylline, nitrates, alcohol, fat, chocolate
Barbiturate, cigarettes, benzo., Ca channel blockers (cardizem), caffeine, anticholinergics
137
*Langmore et al., 1998;
Medications
Acid suppression medications
Administered for stress ulcer prophylaxis in ICU
3 studies show increased incidence of pneumonia in patients taking acid suppressing drugs
Proton pump inhibitors (omeprazole, etc.)
H2 receptor antagonists (ranitidine, etc.)
Increased pneumonia risk (discussed earlier)
Enables survival of pathogens in stomach
138
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
47
Medications
LaHeij et al., 2004 (>300,000 OP subjects)
Treated patients who developed pneumonia were matched to up to 10 age/gender/lifestyle
Currently using PPI: 89% higher pneumonia risk over those who stopped using PPI
H2 antagonists: 63% higher pneumonia risk
Herzig et al., 2009 (>60,000 IP subjects)
52% inpatients treated
5% treated patients, 2% untreated, pneumonia
30% higher risk of pneumonia (adjusted)
139
Medications
Eurich et al., 2010
248 patients post‐pneumonia admission, compared to 2500 patients with no pneumonia hx.
5.4 years average follow up
Some continued, some stopped PPI use
Acid suppression (current/past): 12% incidence
Current users: all of the incidence was with current
Non‐acid suppression: 8% incidence
140
Medications
Interesting contrast
SDD (selective decontamination of the digestive tract (sterilizes gastric contents without acid suppression)
Reduced pneumonia incidence in CVA patients*
141
Gosney et al., 2006
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
48
Medications
There is evidence that acid suppression therapy may increase pneumonia risk
…and that the stomach is a reservoir for pathogens
Mechanism: alteration of gastric pH (normally 2‐3) allows bacterial survival and colonization
142
Colonization‐host risk or iatrogenic Gastric colonization
Discussed previously
Oral colonization
Systematic review Systematic review
Good evidence that aggressive oral care/hygiene reduces pneumonia in high risk adults
Relative risk reduction=34‐83%
Causes: oral, dental disease, xerostomia, medications
143
Azarpazhooh, et al., 2002
Colonization
Oral Colonization (cont’d)
Worsened with*:
Antibiotic use
Oral disease
Xerostomia
Malnutrition
Presence of teeth! **
144
*Gomes et al., 2003; **Wan et al., 2003
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
49
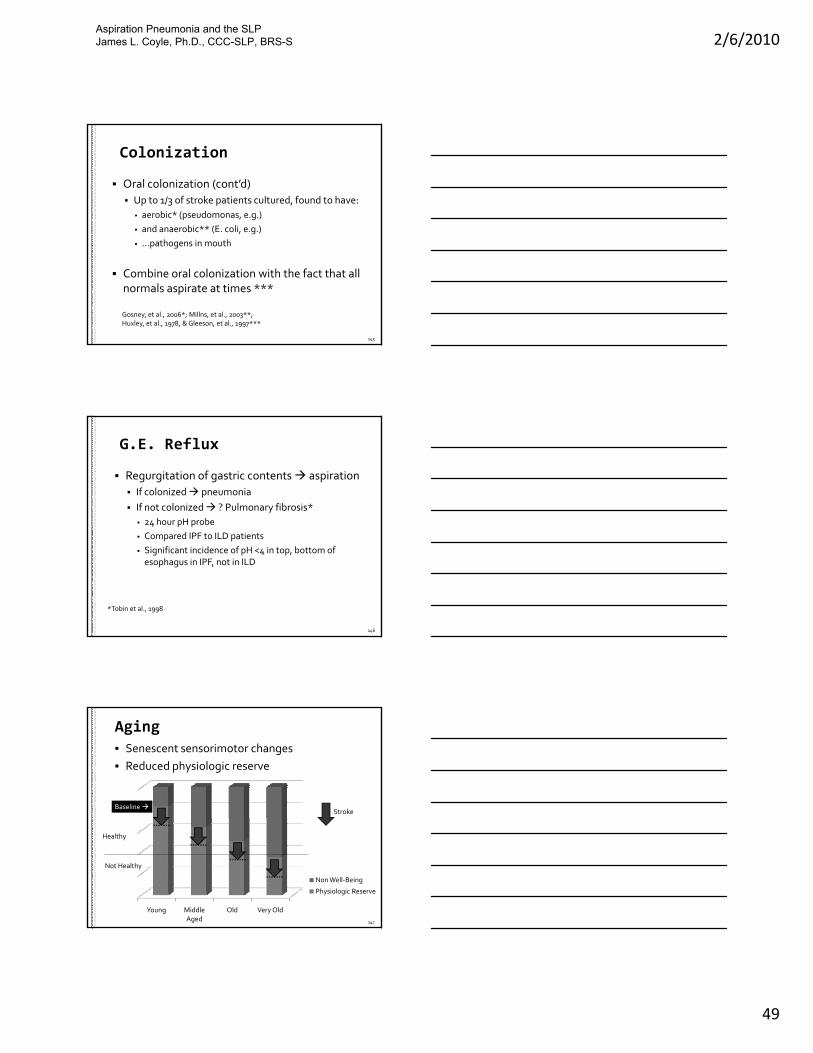
Colonization
Oral colonization (cont’d)
Up to 1/3 of stroke patients cultured, found to have:
aerobic* (pseudomonas, e.g.)
and anaerobic** (E. coli, e.g.)
…pathogens in mouth
Combine oral colonization with the fact that all normals aspirate at times ***
145
Gosney, et al., 2006*; Millns, et al., 2003**; Huxley, et al., 1978, & Gleeson, et al., 1997***
G.E. Reflux
Regurgitation of gastric contents aspiration
If colonized pneumonia
If not colonized ? Pulmonary fibrosis*
24 hour pH probe4 p p
Compared IPF to ILD patients
Significant incidence of pH <4 in top, bottom of esophagus in IPF, not in ILD
146
*Tobin et al., 1998
Aging
Senescent sensorimotor changes
Reduced physiologic reserve
StrokeBaseline
147
Young Middle Aged
Old Very Old
Non Well‐Being
Physiologic Reserve
Healthy
Not Healthy
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
50
Aging
Diminished esophageal motility
Reduced cricopharyngeal compliance
Reduced intrabolus pressure generation (swallowing)(swallowing)
Immune system degradation
148
Other iatrogenic risk factors
Postoperative sensorimotor impairments
Predispose to dysphagia
Anterior cervical fusion*
Esophagectomy**
Thyroidectomy, carotid endarterectomy
Aortic repairs
Phrenic, vagus n.
149*Kriskovich, et al., 2000; **Atkins, et al., 2007)
Airway manipulation
Mechanical ventilation
Endotracheal intubation
Tracheostomy
Other iatrogenic risk factors
y
All raise the patient’s pneumonia risk (VAP)
150
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
51
Mechanical Ventilation
Complications of PPV Barotrauma (alveolar damage, excessive pressure) Pneumothorax
Diffuse alveolar damage
At l t i ( l l ll i ffi i t P ) Atelectasis (alveolar collapse, insufficient P a)
Infection ETT, tracheostomy: direct pathogen route Nosocomial pathogens VAP
Respiratory deconditioning
Alveolar hypo‐ hyperventilation
Hypotension
151
Endotracheal Intubation
Complications
malfunction, mucus plug, leak, position
Self extubation
Mucosal necrosis
Pneumonia
Laryngeal edema
Tracheal erosion
152
Prolonged Intubation
Definition
Generally, >24‐48 hours
Dependent on other host risk factors
Age, method of intubation, underlying disease
>24 hours (frail elderly)
153
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
52
Prolonged Intubation
Evidence
Ajemian et al., 2001
48 patients > 48 hours intubation, < 48 hours extubated
27/48 (56%) aspirated 12/27 (44%) silent aspiration 27/48 (56%) aspirated, 12/27 (44%) silent aspiration
19/27 thin liquid aspirators, 9/27 puree
154
ElSohl et al., 2003
42 elderly, 42 nonelderly; all > 48 hours intubation
FEES at 2 days post‐extubation, and 5,9,14 days (aspirators)
/ ld l / ld l i i 22/42 elderly, 15/42 non‐elderly, aspiration
13% elderly persistent dysphagia after 2 weeks
0% non‐elderly)
155
Tracheostomy
Open pathway for pathogens to colonize lung
156
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
53
Respiratory System Testing and Treatments
1300‐1345
Testing the Respiratory System
158
Pulmonary Function Parameters
FVC = forced vital capacity
VC = vital capacity
FEV1 = forced expiratory volume in 1 second
TLC = total lung capacity TLC = total lung capacity
Reduced in restrictive disease
RV = residual volume
159
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
54
Normal Resting Spirometry
inspired
160
expired
Spirometry Subtests
Post‐bronchodilator FEV1
FEV1/FVC
Rate of decline
B d l th h Body plethysmography
Exhaled CO (carbon monoxide)
Confirms current smoking status
161
Imaging of the Chest
Chest x‐ray
Chest CT
162
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
55
Chest x‐ray
Shadows
X‐rays penetrate air filled areas and strike film
X b b d b d ti X‐rays are absorbed by denser tissue
Differences in grayscale color indicate areas of “more solid” matter
Cases a shadow on the film
163
Posterior AnteriorRight Left
Right lung
164
RUL, RML, RLL, LLL
Anterior PosteriorRight Left
Left lung
165
LUL, LLL
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
56
Chest x‐ray
Film
BodyPart
X‐ray source
166
Shadow
Chest x‐ray
Film
BodyPart
Same
X‐ray source
167167
SameShadow
Chest x‐ray: AP Film
Ant. Post
Film
BodyPart
X‐ray source
Ant. Post
Film
BodyPart
X‐ray source
168
Shadow
ShadowShadow is near the bottom = Shadow is near the bottom???
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
57
Chest x‐ray: AP & lateral
Film
BodyPart
X‐ray source
Right Left
Lateral filmAP film
Ant. Post
Film
BodyPart
X‐ray source
169
Shadow
Shadow
Shadow is near the bottom of body part + Shadow is on the left= Shadow is on bottom left
Chest x‐ray reports
Terms
Consolidation, density, opacity:
“I see a shadow.”
Does not indicate nature of “more solid” matter
Infiltrates:
More solid matter has infiltrated a space
Alveolar, airway
Edema: Fluid saturating area
Alveolar, interstitial
Effusion: fluid fills a body cavity (pleural)
170
Chest x‐ray reports
Terms
Atelectasis: collapsed alveoli
Obstructive
Blocked airways; gas within alveoli absorbed into blood
Non‐obstructive
Compressive
Alveoli pressed closed – extrinsic
Dependent
Pt. position prevents inflation of alveoli; poor inspiration
Adhesive: lack of surfactant cause collapse
Passive: widened pleural space enables collapse
171
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
58
Chest x‐ray reports
Terms
Pulmonary vascular congestion
NOT airway congestion
Blood back‐up in pulmonary vessels
Poor perfusion, (R) heart failure
pulmonary artery congestion
Arterial hypertension, (L) heart failure
pulmonary vein congestion
Alveolar infiltrates are inside alveoli!
The rest of these are NOT alveolar infiltrates.
172
173
Pneumothorax
174
ARDS (bilaterally) with (R) Pneumothorax
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
59
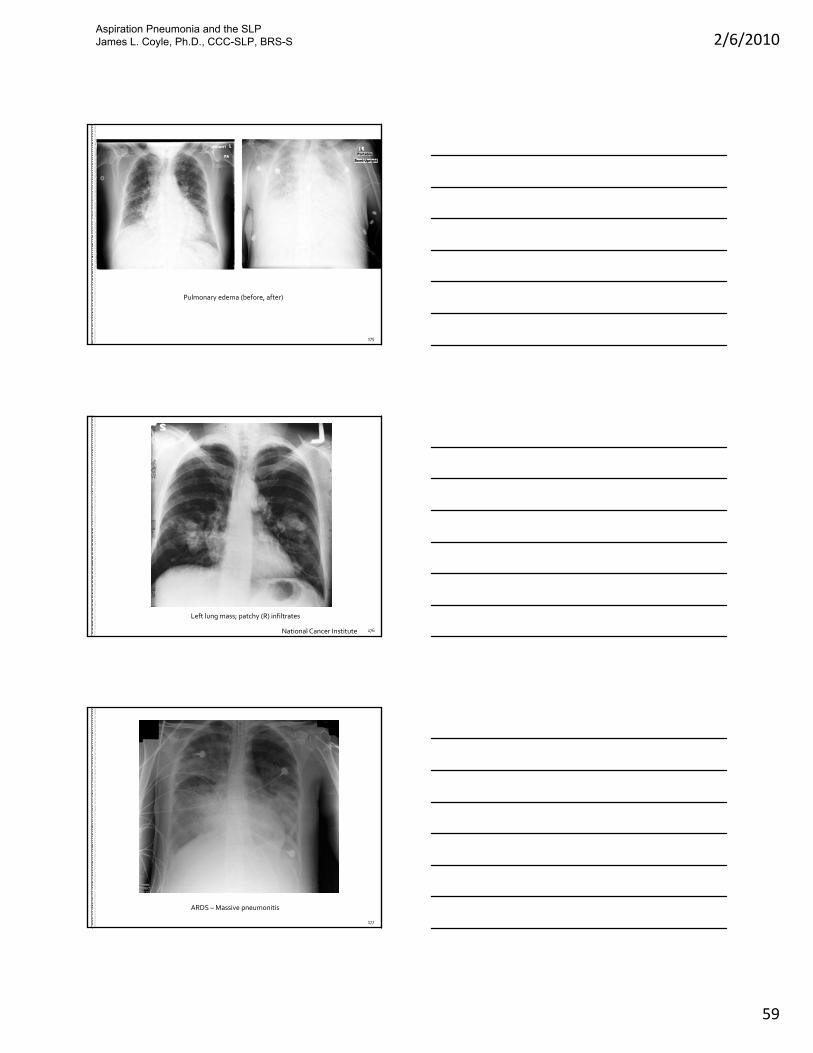
175
Pulmonary edema (before, after)
176
Left lung mass; patchy (R) infiltrates
National Cancer Institute
177
ARDS – Massive pneumonitis
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
60
178
Pleural Effusions (R>L)
Chest CT
Slices of body part are looked at
179
right
Rostralslice
Caudal slice
Middle slice
top
Plane film wouldlook like this
180
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
61
Chest CT
Reduced parenchyma
COPD
181
Emphysematous “holes”
Loss of alveolar surface area
Other tests
Exercise tolerance
Treadmill test, 6 minute
Resting SpO2
After 10 minutes rest After 10 minutes rest
Biomarkers
Sputum, exhaled gas condensate, metabolites
DNA; Markers for surfactant, etc.
Questionnaires
Depression, QOL, fatigue, dyspnea
182
Other tests
Body Plethysmography: TLC and RV
Inhalation Challenge Tests: allergen
Exercise stress test
G diff i Gas diffusion
ABG
183
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
62
Blood Gases Reading Blood Gas Data (ABG)
p = partial pressure (mm/Hg)
a = arterial
v= venous (blood gases from venous l )sample)
O2= oxygen, CO2= carbon dioxide
S = saturation
H = hydrogen ion
Index of acidity
184
Blood Gases
Arterial blood gases & normal ranges
paCO2 = partial pressure of CO2
38‐45 mmHg
paO2 = partial pressure of O2 paO2 = partial pressure of O2
85‐100 mmHg
pH: acidity
~7.4
SaO2 = % hemoglobin O2 saturation
90‐100%
185
Pulmonary Disease Treatment
…and adapting the SLP evaluation to accommodate them…
186
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
63
Treatment of Respiratory Conditions
Bronchodilators
Nebulizer
Metered Dose Inhaler (MDI)
187
Pulmonary Disease Treatment
Oxygen monitoring
ABG
Pulse oximetry
Continuous
Intermittent
188
Pulmonary Disease Treatment
Hyperinflation therapy Patient generated Incentive spirometry (IS)
Positive pressure “Mechanical bronchodilator”
CPAP One level
Bipap‐2 level IPAP, EPAP
IPPB
189
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
64
Pulmonary Disease Treatment
Bronchopulmonary Hygiene
Percussion and postural drainage
Suctioning
190
Pulmonary Disease Treatment
Supplemental oxygen
Nasal cannula
Facemask
Non‐rebreather
Prevents inspiration of
Room air
Exhaled air
Delivery parameter = LPM flow
Adaptations?
Facemask: can pt. use cannula/oximizer?
191
Pulmonary Disease Treatment
Venturi mask
Mixes room air with O2 to a fixid FiO2
Delivery parameter = FiO2, not flow (LPM)
192
Adaptations: Can patient use cannula during PO?
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
65
Pulmonary Disease Treatment
Observe all important vital signs
Respiratory rate in context of…
Oxygen saturation
Pulse oximetry does not help with dysphagia assessment; identifies hypoxemia over longer periods
Endurance/fatigue
Speaking, feeding, etc.
Overall mental status
Can the rate be brought down, temporarily?
i.e. the duration of a “meal”
193
Examination considerations
Medication timing and the evaluation
Assess patient functions r/t recent medications
Bronchodilators, sedating medications, anxiolytics
Timing of “breathing treatments”g g
Duration of endurance
Can influence meal duration/frequency
Patient who is “safe” for short periods
Mix and match
The above parameters can be flexibly manipulated
194
Tracheostomy Management
Establishment of OralEstablishment of Oral‐‐Nasal Nasal AirflowAirflow
Screening for Aspiration of Screening for Aspiration of Oropharyngeal SecretionsOropharyngeal Secretions
Tolerance of Cuff DeflationTolerance of Cuff Deflation
Patient Fails to Wean from Patient Fails to Wean from Mechanical VentilationMechanical Ventilation
Patient Survives Acute Patient Survives Acute Illness/DiseaseIllness/Disease
Acute Illness Requiring Acute Illness Requiring Mechanical VentilationMechanical Ventilation
195
Tolerance of Tolerance of InspiratoryInspiratory and and Expiratory OcclusionExpiratory Occlusion
Clinical / Clinical / Instrumental Instrumental Evaluation of SwallowingEvaluation of Swallowing
Tolerance of Expiratory Tolerance of Expiratory Occlusion; SpeechOcclusion; Speech
Patient is Patient is DecannulatedDecannulated
Patient Successfully Weans Patient Successfully Weans from Mechanical Ventilationfrom Mechanical Ventilation
Tracheostomy is Placed*Tracheostomy is Placed*
*Heffner & Zamora, 1990; Holevar et al., 2008
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
66
High End Life Support ECMO
Extracorporeal membrane oxygenation
196
After Mechanical Ventilation
Weaning
Prolonged endotracheal intubation
Ventilator associated pneumonia
Cli i l l ti f t h t ti t Clinical evaluation of tracheostomy patients
Instrumental Testing
197
Dysphagia Interventions
198
1400‐1445
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
67
Interventions
Designed to
Prevent adverse events
Biomechanical
Aspiration, bolus misdirection, etc.
Global health outcomes
Pneumonia, malnutrition, dehydration
Psychosocial impairments
Isolation etc.
199
Interventions
Topics
Thickening of liquids for dysphagia management
“Free water” protocols
Enteral feeding tubes in dysphagic patientsg y p g p
Common theme:
hydration/nutrition vs. aspiration…
Choosing the better of 2 or more bad choices
200
Water
Main fluid medium of all cells (except fat)
75‐80% cell volume = water
Necessary for normal cellular functions
Other chemicals dissolved suspended Other chemicals dissolved, suspended
Concentrations at cell membrane
2011540‐1625
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
68
Water
Intake of water: ~2300 mL per day
2100mL through intake
200 mL synthesized by body (CHO metabolism)metabolism)
Variations in water intake
Climate, habits, physical activity
202
Water
Loss of water: ~2300 mL per day
Evaporation: 700 mL per day
Respiratory system (300mL), through skin (400mL)(400mL)
Not sweating
Urine: 1400 mL
Sweat: 100 mL
Feces: 100 mL
203
IntakeOutput
InterstitialFluid
Plasma
Lymphatics
Na+
Na+
Capillary membrane
204
IntracellularFluid
Cell membrane
Fluid
Na+ Na+
Na
osmosis
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
69
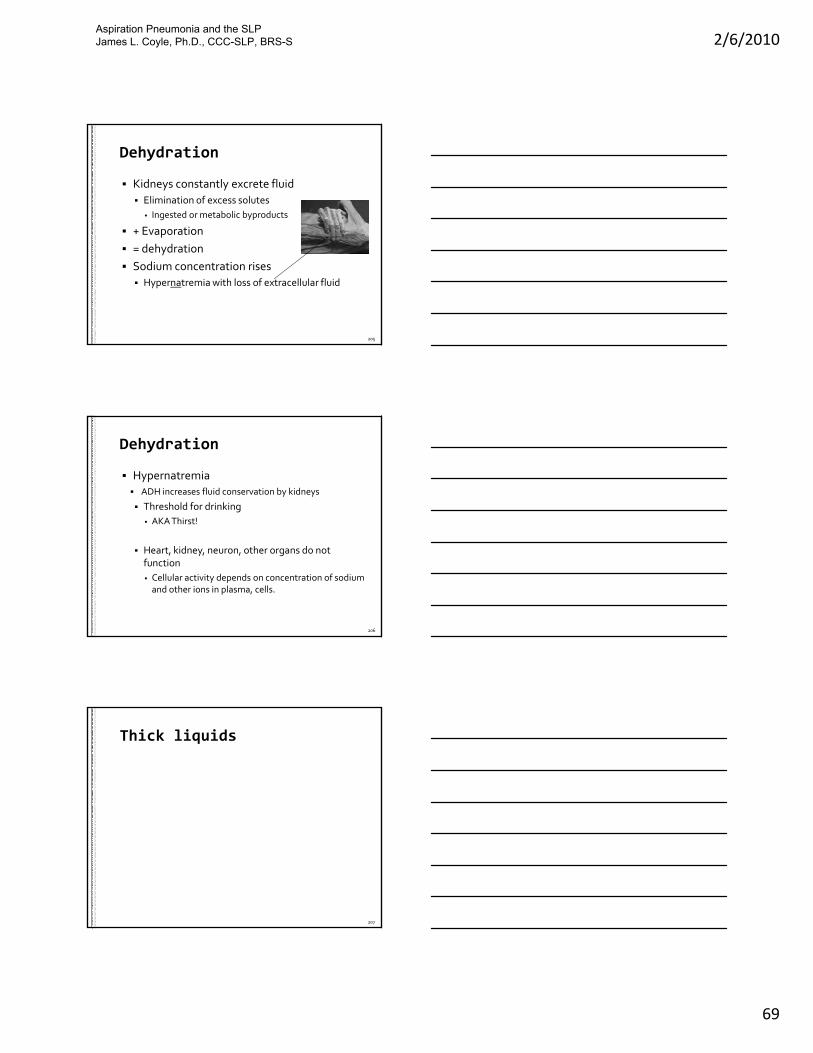
Dehydration
Kidneys constantly excrete fluid
Elimination of excess solutes
Ingested or metabolic byproducts
+ Evaporation Evaporation
= dehydration
Sodium concentration rises
Hypernatremia with loss of extracellular fluid
205
Dehydration
Hypernatremia ADH increases fluid conservation by kidneys
Threshold for drinking
AKA Thirst!
Heart, kidney, neuron, other organs do not function
Cellular activity depends on concentration of sodium and other ions in plasma, cells.
206
Thick liquids
207
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
70
Pneumonia and aspiration
Thin liquids aspirated most frequently
Compared to other viscosities
Spawned experimentation with thick liquids
208
Thickened liquids
Theory for dysphagia use:
Slowing the flow
Compensates for mistimed airway closure
What do we know about them?
209
Thickened liquids
Use in SNF’s
11 companies that own 20% of all SNF’s in US
Randomly selected facilities to avoid bias
252facilities in 41 states (~29000 beds)
Analyzed by CMS region
210Castellanos et al., 2004)
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
71
Results by facilities
Use in SNF: 0% to 100%
Facilities that use thickened water: 91.6%
Results by patients
8.3% patients receive thick liquids
Nectar (60%), Honey (33%), Pudding (6%)
Assessedwith instrumentation:45% (0‐100%)
211Castellanos et al., 2004)
Thickened liquids
Reduces aspiration of thin liquids
Kuhlemeier et al., 2001; Logemann et al., 2008
Does not increase pharyngeal residue
B dt t l Bogaardt, et al., 2007.
Swallow apnea later/longer with thick liquids
Hiss et al., 2004; Butler et al., 2004
More effort needed to clear thick
Nicosia et al., 2001
212
Thickened liquids
Patients do not like thick liquids
Garcia, 2005: prepackaged vs. mixed
Prepackaged better : Whelan, 2001
Great variability in thick liquids Great variability in thick liquids
Prepackaged & mixed: UW/VA Swallowing Research Lab, 1999
Prepackaged: Garcia, et al., 2005; Steele, 2005
Mixed by clinician: Glassburn & Deem, 1998
213
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
72
Thickened liquids
And…
Mixed vs. packaged thick liquids
Not same viscosity
And…And…
Barium mixtures vs. packaged thick drinks:
Not same viscosity
Other properties make up “thickness”
…not just viscosity
214
Thickened liquidsAdd liquid to
cylinder Remove cylinderSpread distance over time (50 mm)
Line Spread Testvs.
Brookfield Viscometer
215
LST: Similar Viscosity Fluids
Material Viscosity Line Spread - 50Pre-thickened honey 1 675 9Pre-thickened honey 2 832 8.75Pre-thickened honey 3 909 10.42P thi k d h 4 1117 9 33
Dysphagia Treatment Methods
216
Pre-thickened honey 4 1117 9.33Honey thick barium 710 18.75Karo syrup (93%) 1038 13.6
Pre-thickened nectar 1 260 12.8Pre-thickened nectar 2 300 13Pre-thickened nectar 3 264 11.7
Nectar thick barium 200 17.2
UW/VA Swallowing Research Lab, 1999
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
73
Thickened liquids
Among 25 experienced SLP’s
Nectar: r= +0.02, Honey: r= ‐0.03
Within subject (1st vs. second mixing of h i t )each consistency)
Nectar: r= +0.26‐0 to +0.33
Honey: r= +0.67
Glassburn and Deem, 1998
217
Thickened liquids
0.6
0.8
1
ability
Moderate relationshipModerate relationship
Strong relationshipStrong relationship
218
‐0.2
0
0.2
0.4
Nectar Honey Nectar Honey
Repeata
No relationshipNo relationship
Weak relationshipWeak relationship
Moderate relationshipModerate relationship
N=25 experienced SLP’s
Glassburn and Deem, 1998.
interjudge intrajudge
Thickened liquids
Hydration and thick liquids
Sharpe et al., 2007
Assessed water absorption
>95% water absorbed from thick mixtures95
No difference between water, thick water
219
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
74
Thickened liquids
Hydration and thick liquids
Reduced fluid intake when thick prescribed
Whelan, 2001
24 stroke patients24 stroke patients
Mean fluid intake = 455 mL/day
220
Thickened liquids
Hydration and thick liquids
Reduced fluid intake when thick prescribed
Finestone, et al., 2001
2 groups: 2 groups:
1‐enteral diets with thick liquids (21 days)
2‐diets with thick liquids (21 days)
Both groups inadequate fluid intake with thick liquids
Reduced fluid intake as weaned from tube
221
Thickened liquids
Large study data
Logemann et al., 2008; Robbins et al., 2008
711 Patients with Parkinson disease, dementiadementia
Aspiration on qualifying VFSS
Randomized order of presentation
Chin‐down/thin, Nectar, Honey
Results…
222
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
75
Thickened liquids
Part 1: eliminating liquid aspiration
Honey nectar chin down posture (all groups)
Overall aspiration: 53%, 63%, 68%Overall aspiration: 53%, 63%, 68%
Half of patients aspirated on all 3
More aspiration on later trials
Patient preference:
Chin down posture, nectar, honey
Part 2
223
Thickened liquids
Protocol 201 Part 2 (515 patients)
Patients with aspiration on none or all:
½ chin down posture with thin liquids (259)
½ thick liquids (256) ½ thick liquids (256)
½ nectar, ½ honey (133, 123)
3 month follow up
Pneumonia, hydration, other outcomes
Results:
224
Thickened liquids
Results – Protocol 201 Part 2
52/515 patients developed pneumonia (11%)
Much less than expected
Other adverse outcomes Other adverse outcomes
More dehydration in thick liquids patients
6% vs. 2%
More UTI in thick liquid patients
6% vs. 3%
225
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
76
Thickened liquids
Median hospital LOS with pneumonia
Honey (18 d.), nectar (4 d.), CDP (6 d.)
226
Thickened liquids
Summary on thickened liquids
Reduces aspiration but is not preferred
Thick liquids do not dehydrate
Reduced intake of fluidsReduced intake of fluids
Probable source of dehydration
Test results do not match diet thickness
Anticipated results cannot be expected
227
Thickened liquids
Summary on thickened liquids
Compliance
Patient preferences
Patient satisfaction
Aspiration of thick liquids may produce a worse pulmonary consequences than thin liquids
If treatment plan will not be implemented…
2281625
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
77
Evidence Summary for using Free Water Protocols
“Free Water” Protocols
2291625‐1700
Frazier Rehab Institute Water Protocol Kathy Panther, M.S., CCC, Louisville, Kentucky
“... Concern over patient and family non‐compliance with thin liquid restrictions compliance with thin liquid restrictions both within the facility and after discharge led us to alter our protocol in 1984. …oral intake of water became a major feature in both treatment and day to day hydration. Features of Frazier’s program …”
230
Retrieved 01/20/09 from http://www.speech‐languagepathologist.org/archives/chat/SLP/April212003.html
Free Water Protocols
Literature search
1. “Free Water”, + Deglutition Disorders
2. Panther, K.
One citation on semantic relations in JSHD 1983
Perspectives article in 03/05 describing protocolPerspectives article in 03/05 describing protocol
“Currently there is no published evidence that will give dysphagia clinicians a definitive scientific basis for the safe delivery of water to patients with dysphagia”
ASHA journal (pre “Leader”) piece in 1998
231
Leonard, L. B., Steckol, K. F., & Panther, K. M. (1983). Returning meaning to semantic relations: some clinical applications. Journal of Speech and Hearing Disorders, 48, 25‐36.
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
78
Developers discuss
Safety of Water
Hydration
Compliance
“Free Water” Protocol Principles
p
232
1. “Safety of Water”
“Small amounts of water … are quickly absorbedinto the body pool.”
“Free Water” Protocol Principles
Large amounts are not.
“Water has a neutral pH…is free of bacteria…”
“Aspiration of other liquids can lead to respiratory infections and pneumonia.”
Cited evidence: animal studies, drowning case studies
233
Retrieved 01/20/09 from http://www.speech‐languagepathologist.org/archives/chat/SLP/April212003.html
Pneumonia and aspiration
Drowning
Water fills air spaces
Plasma is hypertonic
Meaning: it contains lower concentration of water
At membrane, water flows into capillary
234capillary
Na+Na+ Na+
Na+
water
Effros, et al., 2000
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
79
Pneumonia and aspiration
Example: seawater contains
High NaCL concentration
Is hypertonic Is hypertonic
Compared to plasma
Seawater drowning
Plasma enters lung
Similar with aspiration of any hypertonic solution
235capillary
Na+Na+ Na+
Sea waterNa+
Na+Na+
Na+
Na+
Na+
Na+
Na+
Na+
1. “Safety of Water”
“Water provides a safe means of assessing patients”
Opinion
“Free Water” Protocol Principles
Opinion
“All patients (of any diagnosis) referred to Speech Pathology are screened for dysphagia with water.
OK
“Water is safely utilized in daily treatment
“Swallow compensations can be practiced with thin liquid.
236
2. “Hydration”
“Free water consumption is encouraged for all patients and makes a significant contribution in hydration for many.”
“Free Water” Protocol Principles
hydration for many.
Evidence?
“The risk and cost of IV fluids should be decreased.
“Post‐discharge surveys… indicate water often is the primary means of hydration.”
237
Retrieved 01/20/09 from http://www.speech‐languagepathologist.org/archives/chat/SLP/April212003.html
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
80
3. “Compliance”
“Patients reported thickened liquids did not quench thirst.
“ ti t l i t h l ”
“Free Water” Protocol Principles
“…patient complaints are now much less”
“…patients object to thickened liquids.
“…patients appear more likely to comply with the thin liquids restriction.”
238
Retrieved 01/20/09 from http://www.speech‐languagepathologist.org/archives/chat/SLP/April212003.html
“Free Water” Protocol Principles
3. “Compliance”
“…preparation of thickened liquids (is) burdensome.
“family may tire of patient complaints and abandon thi k d li idthickened liquids.
“Availability and cost of thickening may preclude compliance.
“Thick liquid preparation, … can overwhelm many families.”
239
Free Water Protocols Evidence
Bronchoalveolar lavage
Whelan et al. (2001) reduced fluid intake in patients prescribed thick liquids
Numerous citations on dehydration in Numerous citations on dehydration in dysphagia
Animal studies of water aspiration
240
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
81
Free Water Protocols Evidence
Garon et al., 1997
20 aspiration‐documented CVA patients
Aspirated liquid only on VFSS
Randomized to
(C): Thick liquids only at all times (10)
(E): All liquids thickened, AND free water (10)
Duration: treatment + 30 day follow up
Small and underpowered study
Yet the main evidence for protocol
241
Garon et al., 1997
Exclusion
“Severe cough” when aspirating
Cannot rinse and expectorate
Cannot self‐feed
Pre‐existing hydration concern
148 patients screened: 13% enrolled
34 patients declined participation
94 patients ineligible
242
Garon et al., 1997
Water placed out of reach
No water with meal or within 1hour
No compensatory swallow therapyp y py
Outcome variables
Pneumonia, hydration, time to no aspiration
Fluid intake
243
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
82
Garon et al., 1997
Results
No patient in either group developed pneumonia, dehydration, complications
Intake of fluids comparable between groups
1210 mL (C) ‐ all thick
1318 mL (E): 855mL thick, 463mL thin
244
Free Water Protocols Evidence
Garon et al., 1997
Time to recovery of aspiration
Experimental: 19.1 days (range 7‐35 days)
Control: 27.2 days (range: 8‐64 days)
Control: 42% longer to recover
More severe aspirators in control so OK
Small sample
Time to pneumonia outcome: adequate?
245
Free Water Protocols Evidence
Garon et al., 1997
“Much less water than expected” by investigators (“we were surprised…”)
Satisfaction: only one control patient was satisfiedwith thick liquid
“all study patients satisfied with water”
246
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
83
Free Water Protocols Evidence
Robbins et al. 2008. Protocol 201
Pneumonia‐no difference
Thin liquids/chin‐down posture: 10%
Thick liquids: 11%
Nectar: 8%, Honey: 15%
Dehydration: Thin: 2%, Thick: 6%
UTI: Thin: 3%, Thick: 6%
3 times longer hospital stay in honey‐thick who developed pneumonia
247
Two recent studies
Two presented at ASHA 2008
Bronson‐Lowe, et al., 2008. Effects of a free water protocol for patients with dysphagia.
Free Water Protocols
Becker et al., 2008. An oral water protocol in rehabilitation patients with dysphagia for liquids.
248
Bronson‐Lowe, et al., 2008
1. Retrospective study comparing patients with historical controls (via chart review)
Pneumonia, dehydration: no difference
Free Water Protocols (#1)
Fluid intake greater in treatment group (p=.03)
2. Sample of convenience concurrent comparison
Fewer pneumonia and more fluid intake
249
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
84
Authors’ discussion
Authors could not determine whether results were influenced by
Increased oral hygiene in the treatment group
Increased oral hydration in the treatment group
More compliance with aspiration precautions in treated More compliance with aspiration precautions in treated patients
Hydration not affected by treatment/control assignment
This needs to be replicated prospectively
250
Bronson‐Lowe, et al., 2008
Free Water Protocols (#2)
Randomization to water protocol or prescribed dietary fluid (26 patients)
17 patients requiring feeding assistance
8 assigned to control 9 to treatment8 assigned to control, 9 to treatment
9 independent feeding patients
3 assigned to control, 6 to treatment
All received oral care four times per day
Becker, et al., 2008
251
Dependent Variables
Adverse events (pneumonia, UTI, death)
Objective measures not assigned by clinician/judges
FIM, FCM scores
Free Water Protocols (#2)
,
not blinded, assigned by treating clinician/judges
Length of stay
252
Becker, et al., 2008
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
85
Results
Pneumonia: 1 patient in each group
UTI: 2 patients in each group
Death: 2 treatment deaths, no control deaths
Free Water Protocols (#2)
,
FIM: no significant difference
FCM: no significant difference
Length of stay: 29.1 days (control) vs. 15.8 (tx)
Diet influence length of stay?
253
Becker, et al., 2008
Other findings:
Independent patients consumed significantly lessfluid than dependent patients (p<.01), regardless of group
254
Free Water Protocols (#2)
255Becker, et al., 2008
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
86
Discussion
The presence of two deaths in the treatment group cannot be ignored
…and may underscore the importance of clinical
Free Water Protocols (#2)
judgment in applying this and other treatments
Both patients that died had chronic pulmonary conditions
256
Becker, et al., 2008
Other issue – implied endorsement
257
“Free water protocols”
Summary
25 years experience by developers
No published, peer reviewed data
anecdote only
Minimal objective evidence
No pneumonia difference
Other differences seem to exist
258
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
87
“Free water protocols”
Summary
Physiologic justification exists
But not for all patients
Severe pulmonary disease
One size does not fit all
Developers obligation to publish data
Opinion here: there is no one protocol that is appropriate for every patient
259
Feeding tubes
260
Feeding tubes
Indications
Artificial nutrition
Gastric decompression
Digestive system incompetenceg y p
Paralysis, obstruction, absorption disease
“Transfer dysphagia”
Oropharyngeal transfer disorder
Delivery:
Directly to gut blood (enteral)
Directly to blood (parenteral)
261
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
88
Non‐Oral Nutrition Enteral nutrition Delivered to the gut
Utilizes digestive system
Tube name entry, deliverydelivery Naso‐gastric (NG); gasatrojejunostomy (GJ)
Depth: sphincters, absorption
262
Non‐Oral Nutrition
Parenteral nutrition Bypasses the digestive system‐intravenous
Central, peripheral Percutaneous Intravenous Central Catheter
i f b h d proteins, fats, carbohydrates, etc.
Peripheral vein – few nutrients can be delivered
TPN, PPN
263
Non‐Oral Nutrition
Nasopharyngeal entry
Fluoroscopic
Blind
264
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
89
Non‐Oral Nutrition
Surgical entry
Fluoroscopically guided
Endoscopically guided
PEG
Open surgical
All involve opening abdominal wall so all are surgical
265
Non‐Oral Nutrition
PEG
266
267
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
2/6/2010
90
Enteral Tube Indications
Intractable aspiration
Failed interventions
Recurrent illness attributed to prandialaspirationp
Permanenttemporary
Replacement/substitute for oral intake
Supplement to oral intake
Replacement for types of materials aspirated
268
Contraindications
Ileus/Gastroparesis, SBO
Paralysis, obstruction
Absorption Deficits
Default to parenteral nutrition Default to parenteral nutrition
Prior abdominal resections/anatomy diff.
Surgically inserted abdominal enteral tubes
GER, severe.
269
Feeding Tubes
Aspiration
Is not mitigated (25‐40% in PEG)
Saliva production
may increase – new site (Metheny et al., 2006)y ( y , )
270
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
91
Complications
271
Feeding Tubes Evidence
272
Enteral Tube Feeding
N= 70 tube fed patients, age 65‐95, over 11 mo. Indications refusal to swallow 50%
dysphagia without obstruction 47%
h l b i % esophageal obstruction 3%
Nutrition: weight, hgb, hct, serum albuminCiocon et.al, (1988)
273
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
92
Enteral Tube Feeding
NGT complications in first two weeks self‐extubation (67%) , AP (43%)
GT complications in first two weeks pneumonia (56%), dysfunction 50% self‐extubation 44% self extubation 44%
Late NGT complications pneumonia (44%), self‐extubation (39%)
Late GT complications pneumonia (56%),dysfunction 38% self‐extubation 0%
40% died
274
Ciocon et.al, (1988)
Mortality in tube fed patients is high
Because they have multiple conditions
Dementia: 25‐50% mortality
¼ d ti ti t di i h it l f ll i PEG
Enteral Tube Feeding
¼ dementia patients die in hospital following PEG placement (McClave & Chang, 2003)
Callahan et al., 2000 (150 PEG cases)
7‐14 days 16%
30 day 22%, 1 year 50%
275
The SLP and the Feeding Tube
1. Patient education most important
Empower patient to ask questions
Neutral pro’s and con’s
2 Clinician personal opinion irrelevant2. Clinician personal opinion irrelevant
3. Clinician understanding of all the “ins and outs”
Our patients are sick
Balance of risks = medical care
276
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S

2/6/2010
93
Thank you.
And now for some cases…
277
Aspiration Pneumonia and the SLP James L. Coyle, Ph.D., CCC-SLP, BRS-S
Coyle, Pneumonia Seminar References
Acheson, D. E. (2003). FDA Public Health Advisory: Reports of blue discoloration and death in patients receving enteral feedings tinted with the dye, FD&C blue No. 1. http://www.cfsan.fda.gov/~dms/col-ltr2.html.
Ajemian, M. S., Nirmul, G. B., Anderson, M. T., Zirlen, D. M., & Kwasnik, E. M. (2001). Routine fiberoptic endoscopic evaluation of swallowing following prolonged intubation: implications for management. Archives of Surgery., 136(4), 434-437.
Alia, I., & Esteban, A. (1999). Protocol-guided weaning: a key issue in reducing the duration of mechanical ventilation. Intensivmed, 36(5), 429-435.
Alkhuja, S. (1998). Dysphagia in the patient with a tracheostomy: six cases of inappropriate cuff deflation or removal. Heart & Lung: Journal of Acute & Critical Care., 27(1), 74.
Almirall, J., Bolibar, I., Vidal, J., Sauca, G., Coll, P., Niklasson, B. et al. (2000). Epidemiology of community-acquired pneumonia in adults: a population-based study. European Respiratory Journal, 15, 757-763.
Apfelbaum, R. I., Kriskovich, M. D., & Haller, J. R. (2000). On the incidence, cause, and prevention of recurrent laryngeal nerve palsies during anterior cervical spine surgery. Spine, 25(22), 2906-2912.
Atkins, B. Z., Fortes, D. L., & Watkins, K. T. (2007). Analysis of respiratory complications after minimally invasive esophagectomy: preliminary observation of persistent aspiration risk. Dysphagia, 22(1), 49-54.
Azarpazhooh, A., & Leake, J. L. (2006). Systematic review of the association between respiratory diseases and oral health. Journal of Periodontology, 77(9), 1465-1482.
Baine, W. B., Yu, W. M., & Summe, J. P. (2001). Epidemiologic trends in the hospitalization of elderly medicare patients for pneumonia, 1991-1998. American Journal of Public Health, 91, 1121-1123.
Barquist, E., Brown, M., Cohn, S., Lundy, D., & Jackowski, J. (2001). Postextubation fiberoptic endoscopic evaluation of swallowing after prolonged endotracheal intubation: A randomized, prospective trial. Critical Care Medicine, 29(9), 1710-1713.
Becker, D. L., Tews, L. K., & Lemke, J. H. (2008). An oral water protocol in rehabilitation patients with dysphagia for liquids. 2008 ASHA convention technical session.
Belafsky, P. C., Blumenfeld, L., LePage, A., & Nahrstedt, K. (2003). The accuracy of the modified Evan's blue dye test in predicting aspiration. Laryngoscope., 113(11), 1969-1972.
Blunt, M. C. (2008). Gel lubrication of the tracheal tube cuff reduces pulmonary aspiration. Anesthesiology, 95(2), 377-381.
Brady, S. L., Hildner, C. D., & Hutchins, B. F. (1999). Simultaneous videofluoroscopic swallow study and modified Evans blue dye procedure: An evaluation of blue dye visualization in cases of known aspiration. Dysphagia., 14(3), 146-149.
Bronson-Lowe, C. R., Leisling, K., Bronson-Lowe, D., Lanham, S., Hayes, S. M., Ronquillo, A. M., et al. (2008). Effects of a free water protocol for patients with dysphagia. 2008 ASHA convention technical session.
Butler, R., Keenan, S. P. M., Inman, K. J. M., Sibbald, W. J. M., & Block, G. (1999). Is there a preferred technique for weaning the difficult-to-wean patient? A systematic review of the literature. Critical Care Medicine, 27(11), 2331-2336.
Cameron, J. L., Reynolds, J., & Zuidema, G. D. (1973). Aspiration in patients with tracheotomies. Surgical Gynecology and Obstetrics, 136, 68-70.
Centers for Disease, C., & Prevention (2003). Guidelines for preventing health-care associated pneumonia, 2003 (No. MMWR, 53 (RR-3)).
Charbonneau, I., Lund, J. P., & McFarland, D. H. (2005). Persistence of respiratory-swallowing coordination after laryngectomy. Journal of Speech Language & Hearing Research, 48(1), 34-44.

Coyle, Pneumonia Seminar References
Ciocon, J. O., Silverstone, F. A., Graver, L. M., & Foley, C. J. (1988). Tube feedings in elderly patients: indications, benefits, and complications. Archives of Internal Medicine, 148(2), 429-433.
Coyle, J. L., Davis, L. A., Easterling, C., Graner, D. E., Langmore, S., Leder, S. B., et al. (2009). Oropharyngeal dysphagia assessment and treatment efficacy: setting the record straight (response to Campbell-Taylor). Journal of the American Medical Directors Association, 10(1), 62-66.
Coyle, J. L., & Robbins, J.A. (1997). Assessment and behavioral management of oropharyngeal dysphagia. Current Opinion in Otolaryngology & Head & Neck Surgery, 5(3), 147-152.
Czop, M., & Herr, D. L. M. (2002). Green skin discoloration associated with multiple organ failure. Critical Care Medicine, 30(3), 598-601.
Davis, L. A., & Thompson, S. S. (2004). Characteristics of dysphagia in elderly patients requiring mechanical ventilation. Dysphagia, 19(1), 7-14.
deLarminat, V., Montravers, P., Dureuil, B., & Desmonts, J. M. (1995). Alteration in swallowing reflex after extubation in intensive care unit patients. Critical Care Medicine, 23(3), 486-490.
Dettelbach, M. A., Gross, R. D., Mahlmann, J., & Eibling, D. E. (1995). Effect of the Passy-Muir Valve on aspiration in patients with tracheostomy. Head & Neck, 17(4), 297-302.
Dikeman, K., & Kasandjian, M. (2003). Communication and swallowing management of tracheostomized and ventilator-dependent adults. Clifton Park, N.J.: Thomson Delmar Learning.
Doggett, D. L., Tappe, K. A., Mitchell, M. D., Chapell, R., Coates, V., & Turkelson, C. M. (2001). Prevention of pneumonia in elderly stroke patients by systematic diagnosis and treatment of dysphagia: an evidence-based comprehensive analysis of the literature. Dysphagia, 16(4), 279-295.
Doggett, D. L., Turkelson, C. M., & Coates, V. (2002). Recent developments in diagnosis and intervention for aspiration and dysphagia in stroke and other neuromuscular disorders. Current Atherosclerosis Reports.4(4):311-8.
Donzelli, J., Brady, S., Wesling, M., & Craney, M. (2001). Simultaneous modified Evans blue dye procedure and video nasal endoscopic evaluation of the swallow. Laryngoscope., 111(10), 1746-1750.
Dua, K., Bardan, E., Ren, J., Sui, Z., & Shaker, R. (2002). Effect of chronic and acute cigarette smoking on the pharyngoglottal closure reflex. Gut, 51(6), 771-775.
Duchin, S., & van Houte, J. (1978). Colonization of teeth in humans by Streptococcus mutans as related to its concentration in saliva and host age. Infection & Immunity, 20(1), 120-125.
Dziewas, R., Ritter, M., Schilling, M., Konrad, C., Oelenberg, S., Nabavi, D. G., et al. (2004). Pneumonia in acute stroke patients fed by nasogastric tube. Journal of Neurology, Neurosurgery & Psychiatry, 75(6), 852-856.
Dziewas, R., Warnecke, T., Hamacher, C., Oelenberg, S., Teismann, I., Kraemer, C., et al. (2008). Do nasogastric tubes worsen dysphagia in patients with acute stroke? BMC Neurology, 8, 28.
Effros, R. M., Jacobs, E. R., Schapira, R. M., & Biller, J. (2000). Response of the lungs to aspiration. The American Journal Of Medicine, 108(4, Supplement 1), 15-19.
Eibling, D. E. & Gross, R. D. (1996). Subglottic air pressure: a key component of swallowing efficiency. Annals of Otology, Rhinology & Laryngology, 105, 253-258.
El Solh, A., Okada, M., Bhat, A., & Pietrantoni, C. (2003). Swallowing disorders post orotracheal intubation in the elderly. Intensive Care Medicine, 29(9), 1451-1455.
El Solh, A. A., Sikka, P., Ramadan, F., & Davies, J. (2001). Etiology of severe pneumonia in the very elderly. American Journal of Respiratory & Critical Care Medicine., 163(3 Pt 1), 645-651.
Engoren, M., Arslanian-Engoren, C., & Fenn-Buderer, N. (2004). Hospital and long-term outcome after tracheostomy for respiratory failure. Chest, 125(1), 220-227.

Coyle, Pneumonia Seminar References
Eurich, D. T., Sadowski, C. A., Simpson, S. H., Marrie, T. J., & Majumdar, S. R. (2010). Recurrent community-acquired pneumonia in patients starting acid-suppressing drugs. The American Journal of Medicine, 123(1), 47-53.
Feldman, M. & Barnett, C. (1991). Fasting gastric pH and its relationship to true hypochlorhydria in humans. Digestive Diseases and Sciences, 36, 866-869.
Feinberg, M. J., Knebl, J., & Tully, J. (1996). Prandial aspiration and pneumonia in an elderly population followed over 3 years. Dysphagia, 11, 104-109.
File, T. M., Tan, J. S., Thomson, R. B., Stephens, C., & Thompson, P. (1995). An outbreak of Pseudomonas aeruginosa ventilator-associated respiratory infections due to contaminated food coloring dye--further evidence of the significance of gastric colonization preceding nosocomial pneumonia. Infection Control & Hospital Epidemiology, 16(7), 417-418.
Finucane, T. E., & Bynum, J. P. (1996). Use of tube feeding to prevent aspiration pneumonia. Lancet, 348(9039), 1421-1424.
Garren, K. C., & Meyers, A. D. (1999). The use of simultaneous videofluoroscopic swallow study and modified Evans blue dye procedure: An evaluation of blue dye visualization in cases of known aspiration. Dysphagia., 14(3), 150-151.
Girard, T. D., & Ely, E. W. (2008). Protocol-drived ventilator weaning: reviewing the evidence. Clinics in Chest Medicine, 29(241), 252.
Gleeson, K., Eggli, D. F., & Maxwell, S. L. (1997). Quantitative aspiration during sleep in normal subjects. Chest, 111(5), 1266-1272.
Gomes, G. F., Pisani, J. C., Macedo, E. D., & Campos, A. C. (2003). The nasogastric feeding tube as a risk factor for aspiration and aspiration pneumonia. Current Opinion in Clinical Nutrition and Metabolic Care, 6(3), 327-333.
Good-Fratturelli, M. D., Curlee, R. F., & Holle, J. L. (2000). Prevalence and nature of dysphagia in VA patients with COPD referred for videofluoroscopic swallow examination. Journal of Communication Disorders, 33(2), 93-110.
Gosney, M., Martin, M. V., & Wright, A. E. (2006). The role of selective decontamination of the digestive tract in acute stroke. Age & Ageing, 35 (1), 42-47.
Gotfried, M. H. (2001). Epidemiology of clinically diagnosed community-acquired pneumonia in the primary care setting: results from the 1999-2000 respiratory surveillance program. American Journal of Medicine., 111(Suppl 9A), 25S-29S.
Griffiths, J., Barber, V. S., Morgan, L., & Young, J. D. (2005). Systematic review and meta-analysis of studies of the timing of tracheostomy in adult patients undergoing artificial ventilation, from http://www.bmj.com/cgi/content/abstract/bmj.38467.485671.E0v1 doi:10.1136/bmj.38467.485671.E0 (published 18 May 2005)
Gross, R. D., Atwood, C. W., Jr., Ross, S. B., Olszewski, J. W., & Eichhorn, K. A. (2009). The coordination of breathing and swallowing in chronic obstructive pulmonary disease. American Journal of Respiratory & Critical Care Medicine, 179(7), 559-565.
Gross, R. D., Mahlmann, J., & Grayhack, J. P. (2003). Physiologic effects of open and closed tracheostomy tubes on the pharyngeal swallow. Annals of Otology, Rhinology & Laryngology., 112(2), 143-152.
Gross, R. D., Atwood, C. W., Jr., Grayhack, J. P., & Shaiman, S. (2003). Lung volume effects on pharyngeal swallowing physiology. Journal of Applied Physiology, 95, 2211-2217.
Hale, K. J., American Academy of Pediatrics Section on Pediatric, D., & Hale, K. J. (2003). Oral health risk assessment timing and establishment of the dental home. Pediatrics, 111(5 Pt 1), 1113-1116.
Hall, J. B., Schmidt, G. A., & Wood, L. D. H. (2003). Principles of Critical Care Medicine (3rd ed.): McGraw Hill.
Hassett, J. M., Sunby, C., & Flint, L. M. (1988). No elimination of aspiration pneumonia in neurologically disabled patients with feeding gastrostomy. Surgery, Gynecology & Obstetrics, 167(5), 383-388.

Coyle, Pneumonia Seminar References
Heffner, J. E., & Zamora, C. A. (1990). Clinical predictors of prolonged translaryngeal intubation in patients with the adult respiratory distress syndrome. Chest, 97(2), 447-452.
Herzig, S. J., Howell, M. D., Ngo, L. H., & Marcantonio, E. R. (2009). Acid-suppressive medication use and the risk for hospital-acquired pneumonia. JAMA, 301(20), 2120-2128.
Hiiemae, K. M., & Palmer, J. B. (1999). Food transport and bolus formation during complete feeding sequences on foods of different initial consistency. Dysphagia, 14(1), 31-42.
Hiss, S. G., Strauss, M., Treole, K., Stuart, A., & Boutilier, S. (2003). Swallowing apnea as a function of airway closure. Dysphagia, 18(4), 293-300.
Hiss, S. G., Treole, K., & Stuart, A. (2001). Effects of age, gender, bolus volume, and trial on swallowing apnea duration and swallow/respiratory phase relationships of normal adults. Dysphagia, 16(2), 128-135.
Huxley, E. J., Viroslav, J., Gray, W. R., & Pierce, A. K. (1978). Pharyngeal aspiration in normal adults and patients with depressed consciousness. American Journal of Medicine, 64(4), 564-568
Katzan, I. L., Cebul, R. D., Husak, S. H., Dawson, N. V., & Baker, D. W. (2003). The effect of pneumonia on mortality among patients hospitalized for acute stroke. Neurology, 60, 620-625.
Kerby, G.S., Deterding, R.R., Balasubramaniam, Vivek, S.S.D., Cavanaugh K.L., Federico M.J.,(2006). Respiratory Tract & Mediastinum. (Chapter). Hay WW, Jr., Levin MJ, Sondheimer JM, Deterding CURRENT Diagnosis & Treatment: Pediatrics, 19th Edition: http://www.accessmedicine.com/content.aspx?aID=3402130.
Knol, W., van Marum, R. J., Jansen, P. A., Souverein, P. C., Schobben, A. F., & Egberts, A. C. (2008). Antipsychotic drug use and risk of pneumonia in elderly people. Journal of the American Geriatrics Society, 56(4), 661-666.
Kononen, E., Asikainen, S., Saarela, M., Karjalainen, J., & Jousimies-Somer, H. (1994). The oral gram-negative anaerobic microflora in young children: longitudinal changes from edentulous to dentate mouth. Oral Microbiology & Immunology, 9(3), 136-141.
Kriskovich, M. D., Apfelbaum, R. I., & Haller, J. R. (2000). Vocal fold paralysis after anterior cervical spine surgery: incidence, mechanism, and prevention of injury. Laryngoscope, 110(9), 1467-1473.
LaCroix, A. Z., Lipson, S., Miles, T. P., & White, L. (1989). Prospective study of pneumonia hospitalizations and mortality of U.S. older people: the role of chronic conditions, health behaviors, and nutritional status. Public Health Reports, 104(4), 350-360.
Langmore, S. E., Skarupski, K. A., Park, P. S., & Fries, B. E. (2002). Predictors of aspiration pneumonia in nursing home residents. Dysphagia, 17, 298-307.
Laheij, R. J., Sturkenboom, M. C., Hassing, R. J., Dieleman, J., Stricker, B. H., & Jansen, J. B. (2004). Risk of community-acquired pneumonia and use of gastric acid-suppressive drugs. JAMA: The Journal of the American Medical Association, 292, 1955-1960.
Langmore, S. E., Terpenning, M. S., Schork, A., Chen, Y., Murray, J. T., Lopatin, D. et al. (1998). Predictors of aspiration pneumonia: how important is dysphagia? Dysphagia, 13, 69-81.
Langmore, S. E., Skarupski, K. A., Park, P. S., & Fries, B. E. (2002). Predictors of aspiration pneumonia in nursing home residents. Dysphagia, 17(4), 298-307.
Leder, S. B. (1999). Effect of a one-way tracheotomy speaking valve on the incidence of aspiration in previously aspirating patients with tracheotomy. Dysphagia., 14(2), 73-77.
Leder, S. B., & Ross, D. A. (2000). Investigation of the causal relationship between tracheotomy and aspiration in the acute care setting. Laryngoscope., 110(4), 641-644.
Lederman, D. S., Klein, E. F., Drury, W. D., Donnelly, W. H., Applefeld, J. J., Chapman, R. L., et al. (1974). A Comparison of Foam and Air-Filled Endotracheal-Tube Cuffs. Anesth Analg, 53(4), 521-526.
Leonard, L. B., Steckol, K. F., & Panther, K. M. (1983). Returning meaning to semantic relations: some clinical applications. Journal of Speech and Hearing Disorders, 48(1), 25-36.

Coyle, Pneumonia Seminar References
Leslie, P., Drinnan, M. J., Ford, G. A., & Wilson, J. A. (2002). Resting respiration in dysphagic patients following acute stroke. Dysphagia, 17(3), 208-213.
Leslie, P., Drinnan, M. J., Ford, G. A., & Wilson, J. A. (2002b). Swallow respiration patterns in dysphagic patients following acute stroke. Dysphagia., 17(3), 202-207.
Leslie, P., Drinnan, M. J., Ford, G. A., & Wilson, J. A. (2005). Swallow respiratory patterns and aging: presbyphagia or dysphagia? Journals of Gerontology Series A-Biological Sciences & Medical Sciences, 60(3), 391-395.
Lindeboom, R. (2005). Timing and route of enteral tube feeding did not affect death or combined death or poor outcome in stroke and dysphagia. Evidence-Based Nursing, 8(4), 117.
Logemann, J. A., Gensler, G., Robbins, J., Lindblad, A. S., Brandt, D., Hind, J. A., et al. (2008). A randomized study of three interventions for aspiration of thin liquids in patients with dementia or Parkinson's disease. Journal of Speech Language & Hearing Research, 51(1), 173-183.
Lucarelli, M. R., Shirk, M. B., Julian, M. W., & Crouser, E. D. (2004). Toxicity of food drug and cosmetic blue no. 1 dye in critically ill patients. Chest, 125(2), 793-795.
Maloney, J. P., Halbower, A. C., Fouty, B. F., Fagan, K. A., Balasubramaniam, V., Pike, A. W., et al. (2000). Systemic absorption of food dye in patients with sepsis. New England Journal of Medicine, 343(14), 1047-1048.
Mandell, L. A., Wunderink, R. G., Anzueto, A., Bartlett, J. G., Campbell, G. D., Dean, N. C., et al. (2007). Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical Infectious Diseases, 44(Suppl 2), S27-72.
Marik, P. E. (2001). Aspiration pneumonitis and aspiration pneumonia. New England Journal of Medicine, 344, 665-671.
Marik, P. E. & Kaplan, D. (2003). Aspiration pneumonia and dysphagia in the elderly. Chest, 124, 328-336.
Marik, P. E. & Zaloga, G. P. (2003). Gastric versus post-pyloric feeding: a systematic review. Critical Care (London), 7, R46-R51.
Marston, B. J., Plouffe, J. F., File, T. M., Jr., Hackman, B. A., Salstrom, S. J., Lipman, H. B. et al. (1997). Incidence of community-acquired pneumonia requiring hospitalization. Results of a population-based active surveillance Study in Ohio. The Community-Based Pneumonia Incidence Study Group. Archives of Internal Medicine, 157, 1709-1718.
Martin-Harris, B. (2000). Optimal patterns of care in patients with chronic obstructive pulmonary disease. Seminars in Speech & Language, 21(4), 311-321.
McClave, S. A., & Chang, W. K. (2003). Complications of enteral access. Gastrointestinal Endoscopy, 58(5), 739-751.
Meert, K. L., & Metheny, N. A. (2004). Incidence and risk factors for oropharyngeal aspiration in mechanically ventilated infants and children. Pediatric Critical Care Medicine, 5(2), 194-196.
Metheny, N. A., Clouse, R. E., Chang, Y.-H., Stewart, B. J., Oliver, D. A., & Kollef, M. H. (2006). Tracheobronchial aspiration of gastric contents in critically ill tube-fed patients: Frequency, outcomes, and risk factors. Critical Care Medicine, 34(4), 1007-1015.
Millns, B., Gosney, M., Jack, C. I., Martin, M. V., & Wright, A. E. (2003). Acute stroke predisposes to oral gram-negative bacilli -- a cause of aspiration pneumonia? Gerontology, 49(3), 173-176.
Mokhlesi, B., Logemann, J. A., Rademaker, A. W., Stangl, C. A., & Corbridge, T. C. (2002). Oropharyngeal deglutition in stable COPD. Chest., 121(2), 361-369.
National Center for Health Statistics (2003). National vital statistics report. Deaths: Leading causes for mortality in 2003. Preliminary data for 2003.
Niederman, M. & Fein, A. (1991). Community-acquired pneumonia in the elderly. In M.Niederman (Ed.), Respiratory Infections in the Elderly (pp. 45-62). New York: Raven Press.

Coyle, Pneumonia Seminar References
Niederman, M. S. (2002). Community-acquired pneumonia: management controversies, part 1; practical recommendation from the current guidelines. Journal of Respiratory Diseases, 23, 10-17.
Niederman, M. S., McCombs, J. S., Unger, A. N., Kumar, A., & Popovian, R. (1998). The cost of treating community-acquired pneumonia. Clinical Therapeutics, 20, 820-837.
Nseir, S., Di Pompeo, C., Jozefowicz, E., Cavestri, B., Brisson, H., Nyunga, M., et al. (2007). Relationship between tracheotomy and ventilator-associated pneumonia: a case control study. European Respiratory Journal, 30(2), 314-320.
O'Neil-Pirozzi, T. M., Lisiecki, D. J., Jack, M. K., Connors, J. J., & Milliner, M. P. (2003). Simultaneous modified barium swallow and blue dye tests: a determination of the accuracy of blue dye test aspiration findings. Dysphagia., 18(1), 32-38.
Owayed, A. F., Campbell, D. M., & Wang, E. E. L. (2000). Underlying causes of recurrent pneumonia in children. Arch Pediatr Adolesc Med, 154(2), 190-194.
Perlman, A. L., He, X., Barkmeier, J., & Van Leer, E. (2005). Bolus location associated with videofluoroscopic and respirodeglutometric events. Journal of Speech Language & Hearing Research, 48(1), 21-33.
Peruzzi, W. T., Logemann, J. A., Currie, D., & Moen, S. G. (2001). Assessment of aspiration in patients with tracheostomies: comparison of the bedside colored dye assessment with videofluoroscopic examination. Respiratory Care, 46(3), 243-247.
Power, K. J. (1990). Foam cuffed tracheal tubes: Clinical and laboratory assessment. Br. J. Anaesth., 65(3), 433-437.
Raghu, G. (2003). The role of gastroesophageal reflux in idiopathic pulmonary fibrosis. American Journal of Medicine,115 Suppl 3A:60S-64S.
Ravelli, A. M., Panarotto, M. B., Verdoni, L., Consolati, V., & Bolognini, S. (2006). Pulmonary aspiration shown by scintigraphy in gastroesophageal reflux-related respiratory disease. Chest, 130(5), 1520-1526.
Saitoh, E., Shibata, S., Matsuo, K., Baba, M., Fujii, W., & Palmer, J. B. (2007). Chewing and food consistency: effects on bolus transport and swallow initiation. Dysphagia, 22(2), 100-107.
Sandhu, R. S., Pasquale, M. D., Miller, K., & Wasser, T. E. (2000). Measurement of endotracheal tube cuff leak to predict postextubation stridor and need for reintubation. Journal of the American College of Surgeons., 190(6), 682-687.
Santos, P. M., Afrassiabi, A., & Weymuller, E. A., Jr. (1994). Risk factors associated with prolonged intubation and laryngeal injury. Otolaryngology - Head & Neck Surgery, 111(4), 453-459.
Sarkar, M. M. D., Hennessy, S. P. P., & Yang, Y.-X. M. D. M. (2008). Proton-pump inhibitor use and the risk for community-acquired pneumonia. Annals of Internal Medicine, 149(6), 391-398.
Schreiner, A. (1983). Anaerobic pulmonary infections. Scandinavian Journal of Gastroenterology, 85S, 55-59.
Segal, R., Dan, M., Pogoreliuk, I., & Leibovitz, A. (2006). Pathogenic colonization of the stomach in enterally fed elderly patients: Comparing percutaneous endoscopic gastrostomy with nasogastric tube. Journal of the American Geriatrics Society, 54(12), 1905-1908.
Sheikh, S., Allen, E., Shell, R., Hruschak, J., Iram, D., Castile, R., et al. (2001). Chronic aspiration without gastroesophageal reflux as a cause of chronic respiratory symptoms in neurologically normal infants. Chest, 120(4), 1190-1195.
Stein, M., Williams, A. J., Grossman, F., Weinberg, A. S., & Zuckerbraun, L. (1990). Cricopharyngeal dysfunction in chronic obstructive pulmonary disease. Chest.97(2):347-52.
Suiter, D. M., McCullough, G. H., & Powell, P. W. (2003). Effects of cuff deflation and one-way tracheostomy speaking valve placement on swallow physiology. Dysphagia., 18(4), 284-292.

Coyle, Pneumonia Seminar References
Theodoropoulos, D. S., Pecoraro, D. L., & Efstratiadis, S. E. (2002). The association of gastroesophageal reflux disease with asthma and chronic cough in the adult. American Journal of Respiratory Medicine., 1(2), 133-146.
Thompson-Henry, S., & Braddock, B. (1995). The modified Evan's blue dye procedure fails to detect aspiration in the tracheostomized patient: five case reports. Dysphagia.10(3):172-4.
Tobin, R. W., Pope, C. E., Pellegrini, C. A., Emond, M. J., Sillery, J., & Raghu, G. (1998). Increased prevalence of gastroesophageal reflux in patients with idiopathic pulmonary fibrosis. American Journal of Respiratory & Critical Care Medicine, 158, 1804-1808.
Vestbo, J., Anderson, W., Coxson, H. O., Crim, C., Dawber, F., Edwards, L., et al. (2008). Evaluation of COPD longitudinally to identify predictive surrogate end-points (ECLIPSE). European Respiratory Journal, 31(4), 869-873.
Wagner, D. R., Elmore, M. F., & Knoll, D. M. (1994). Bacterial contamination of enteral feeding reservoirs. Journal of Parenteral & Enteral Nutrition, 18(6), 562-Dec.
Wan, A. K., Seow, W. K., Purdie, D. M., Bird, P. S., Walsh, L. J., Tudehope, D. I., et al. (2003). A longitudinal study of Streptococcus mutans colonization in infants after tooth eruption. Journal of Dental Research, 82(7), 504-508.
Ware, L. B. & Matthay, M. A. (2000). The acute respiratory distress syndrome. The New England Journal of Medicine, 342, 1334-1349.

Copyright 2010
No part of this material may be reproduced or utilized in any form or
by any means electronic or mechanical including photocopying,
recording, or by any information storage or retrieval systems without the prior permission of the copyright
owner.
© 2010 NSS-NRS, Inc.