prof owen ung - racs qld regional committee - professional collaboration in and outside of the...
TRANSCRIPT

Operating Theatre Management Conference
Professional collaboration in and outside of the Operating Theatre Room
Prof Owen A UngChair RACS Queensland Regional Committee
University of QueenslandRoyal Brisbane and Women’s Hospital
Wesley and St Andrews Hospital
! !

Hills Private Hospital, Sydney 2003

Declaration
• No conflicts of interest
WestmeadPrivateHospital,Sydney2004
• A Multicenter Study – 7 hospitals– OR median raw utilization differed 94% - 85%
• Radboud University Medical Center (UMC Netherlands) redesigned their operating room (OR) scheduling method by implementing cross-functional teams (CFTs)– headed by dedicated anesthesiologist + surgeon, scheduler, OR,
anesthesia, recovery room & ward nurse– The team meets once a week to discuss the OR schedule of the next
week– evaluate the OR performance for previous week– Examines OR program day by day and inform colleagues about all
relevant issues needed for optimal planning and safety– given a full mandate by the Department Head Operating Rooms &
Anesthesiology to make operational decisions about OR schedule and to make alterations as required
Multidisciplinary Teamwork Improves Use of the Operating Room
4
vanVeen-BerkxJAmCollSurgVol.220,No.6,June2015

Multidisciplinary Teamwork Improves Use of the Operating Room
• A total of 30,203 OR days
• KPI - raw utilization calculated on 63,607 inpatient surgical procedures
5
vanVeen-BerkxJAmCollSurgVol.220,No.6,June2015
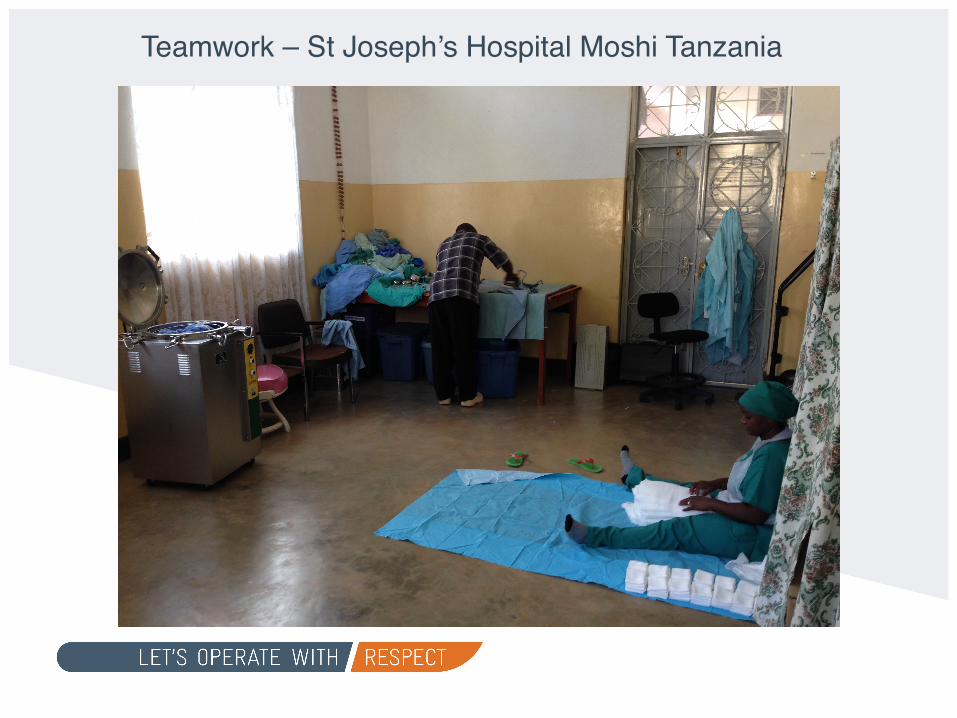
Teamwork – St Joseph’s Hospital Moshi Tanzania

• Paucity of literature on willingness to engage in collaborative practice, trust, respect, societal factors, and cultural factors
collaboration in the operating room
7
• World Health Organisation (WHO) Surgical Safety Checklist• UK teaching hospital - Identify any changes in safety culture
associated with the introduction of the 5 Steps to Surgical Safety in orthopaedic operating theatres– pre-list briefings, the three steps of the WHO Surgical
Safety Checklist (SSC) and post-list debriefings in one framework
• OR Safety Attitude Questionaire - pre-post intervention changes in the six safety culture domains
• The SAQ-OR survey response rate was 80% (60/75) at baseline and 74% (53/72) one year later.
Safety culture and the 5 steps to safer surgery: an intervention study
8
HillM.BriHshJofAnaes114(6):958–62(2015)

Safety culture and the 5 steps to safer surgery: an intervention study
9HillM.BriHshJofAnaes114(6):958–62(2015)
Conclusions:significantimprovementsinsafetyculture

Traditional model - top-down or hierarchical, control focusing upon technical expertise and neglecting the non-technical capability central in inter-professional work (such as good communication and awareness of others)
Promoting inter‐professional teamwork and learning – surgical operating theatre
10
CollinK.JEducWorkVol.23,No.1,February2010,43–63

Weallrelyonoursurgicalteams.Whenweshowthemrespect,webringouttheirbestperformance.
Let’s Operate with Respect
Prof Marianne VonauPast Treasurer

12CollinK.JEducWorkVol.23,No.1,February2010,43–63

St Joseph’s Hospital, Moshi, Tanzania 2013
13

• 60 hospitals - Safety Attitudes Questionnaire– Surgeons, anesthesiologists, certified registered nurse
anesthetists, and operating room nurses– Rated each other using a 5-point Likert scale
• Response 77.1% (2,135 of 2,769).• Perceived collaboration and communication:
– surgeons rated other surgeons “high” or “very high” 85% of the time– nurses rated their collaboration with surgeons “high” or “very high”
only 48% of the time.• Physicians rating the teamwork of others as good, but at the same
time, nurses perceive teamwork as mediocre
Operating Room Teamworkamong Physicians and Nurses:
Teamwork in the Eye of the Beholder
14Makary,MJAmCollSurgVol.202,No.5,May2006

• Hierarchical– Traditionally surgeon leads and dictates pace– Not always ideal
• Communication vital• Promote teamwork
– No specific tools– Doctors and non doctors perception of teamwork varies– Hesitancy to voice concerns – individual dissatisfaction and
potentially poorer patient outcomes
Perceptions of Teamwork in the OR:Roles and Expectations
15
“nursesoXendescribegoodcollaboraHonashavingtheirinputrespected,andphysiciansoXendescribegoodcollaboraHonashavingnurseswhoanHcipatetheirneedsandfollowinstrucHons”
Makary,MJAmCollSurgVol.202,No.5,May2006

SaferAustralianSurgicalTeamwork(SAST)Raisingawarenessofnon-technicalskills
ParHcipantsdevelopknowledge,skillsanda\tudestoimprovetheirperformanceintheoperaHngtheatreinrelaHonto:• CommunicaHon/teamwork,• Decisionmaking,• Taskmanagement/leadership,• SituaHonalawarenessUHlisesthreeframeworksdevelopedbyTheUniversityofAberdeen,RoyalCollegeofSurgeonsofEdinburghandtheNaHonalHealthService:• Non-TechnicalSkillsforSurgeons(NOTSS)• AnaestheHstsNon-TechnicalSkills(ANTS)• ScrubPracHHoners'ListofIntra-operaHveNon-TechnicalSkills(SPLINTS)
TheRoyalAustralasianCollegeofSurgeons(RACS),theAustralianandNewZealandCollegeofAnaestheGsts(ANZCA),theAustralianCollegeofNursing(ACN)andAustralianCollegeofOperaGngRoomNurses(ACORN)Aninter-professionalworkshopforsurgeons,anaestheGstsandscrubpracGGonersworkinginAustralia.

• Importance of leadership is recognized in surgery• Theory proposes - transactional (task-focused) leaders
achieve minimum standards and transformational (team-oriented) leaders inspire performance beyond expectations– Videorecorded 5 surgeons performing complex operations– Multifactor Leadership Questionnaire– Independent coders
Surgeons’ Leadership Styles and Team Behavior in the Operating Room
17Yue-YungHu,JAmCollSurgVol.222,No.1,January2016

Results• Similarly on transactional leadership (range 2.38 to 2.69)• Varied transformational leadership (range 1.98 to 3.60)• Each 1-point increase in transformational score corresponded to
– 3 times more information-sharing behaviors (p < 0.0001)– 5.4 times more voice behaviors (p . 0.0005) among the team– 10 times more supportive behaviors (p < 0.0001)– displayed poor behaviors 12.5 times less frequently (p < 0.0001)
Conclusions• Teams led by transformational surgeons demonstrate a statistically
significant increase in information sharing and voice behaviors, which can improve both safety and efficiency in the OR
Surgeons’ Leadership Styles and Team Behavior in the Operating Room
18
Yue-YungHu,JAmCollSurgVol.222,No.1,January2016

Chonburi Hospital, Thailand 2015

• Cultural change in surgery relies on leadership:– At work, in our roles– Leading by example– Through advocacy
Leadership: passing the baton
20

Stressispartofourwork,butisnoexcuseforunacceptablebehaviour.
Let’s Operate with Respect
Laurie MalisanoChair Professional Standards

Leadership.It’saboutdoingthe
rightthing.
Let’s Operate with Respect
John BattenChair Court of Examiners
Censor in Chief
RACS Action Plan
23
• Cultural Change and Leadership
• Education• Complaint Handling
• Two core principles :– Respect– Collaboration
• Eight goals and supporting actions
• 20 discrete projects

23 projects addressing:
• Strengthening complaints
CULTURE CHANGE & LEADERSHIP
Goal 1
Build a culture of respect and collaboration in surgical practice and education
Engagement and Collaboration Communication: Campaign Leadership Development Diversity & RACS Updating Policies / Procedures
1. Code of Conduct 2. Sanctions Policy 3. Accreditation of Hospital Training Posts 4. Selection of Supervisors 5. IMG oversight 6. Hospital Appointments 7. Appointment process for members of
Training Boards
Goal 2
Respecting the rich history of the surgical profession, advance the culture of surgical practice so there is no place for discrimination, bullying and sexual harassment (DBSH)
Goal 3
Build and foster relationships of trust, confidence and cooperation on DBSH issues with employers, governments and their agencies in all jurisdictions
Goal 4
Embrace diversity and foster gender equity
Goal 5
Increase transparency, independent scrutiny and external accountability in College activities


Let’s Operate with Respect Campaign
26
• Campaign: Phase one:– Information – posters,
web fact sheets etc• Campaign: Phase two:
– Supporting action– How do I ‘Call it out?’
• Knowledge + skills needed:– E-Learning module– Face to face training– Tips on website– Ongoing challenge

27

Whenweseebadbehaviour,it’suptoustocallitout.
Let’s Operate With Respect
Richard LanderExecutive Director Surgical Affairs NZ

Bullyingandharassment.Whenteams
suffer,paGentssuffer.
Let’s Operate with Respect
Dr Cathy FergusonChair Professional Standards

Education
• Mandatory component of CPD and in Surgical Education and Training by 2017 – on line module for all FRACS
• Training for all members of Training Boards, surgical, IMG and research supervisors/ assessors
• Foundation Skills for Surgical Educators– Increasing capacity. 800 per year

Campaign Approach
• Positive positioning that resonates with health workforce• “Building Respect, Improving Patient Safety”• Co-badging and co-branding with organisations in
collaborative model• Campaign communication & material – posters, joint press
releases, social media

Work with hospitals on initiatives
• aligned approaches to dealing with DBSH and information sharing in the public interest, within the law
• improve accreditation arrangements with hospitals to better deal with issues of DBSH
• identifying effective strategies and progressively extending successful models to other hospitals and employers
• ensuring surgical appointments are merit based • develop criteria for selection of heads of departments
and other senior positions, incorporating leadership on DBSH

• Intense media focus– old case of alleged sexual misconduct– new allegations of bullying
• RACS said to be– Misogynist– old boys club– perpetrator of bullying– condoner of bullying
March 2015
33

Establish Expert Advisory Group
• Literature review• Online survey• Narrative collection• Online discussion forums• Invited responses (hospital and other)• Uninvited responses• Draft report• Final report
34

Key Findings
• Results consistent across each review method • 49% of surgeons have experienced DBSH• 63% of trainees have experienced DBSH• 30% of women have experienced sexual
harassment• 71% of hospitals experienced DBSH by
surgeons• Many IMGs report discrimination• No difference across regions & NZ
35

Summary of Material• DBSH is widespread in healthcare, including
surgery• There are profound, negative impacts for
individuals, including patients• There is NO confidence in handling by employer,
College or regulator• Medical education is outdated and teaching by
humiliation is widespread• There has been a profound lack of leadership and
ownership of the problem
36

Find out more: www.surgeons.org/respect

NowistheGmetodealwithdiscriminaGon,bullyingandsexualharassmentandhowitaffectsthesurgicalprofession.
Let’s Operate With Respect
Prof. David WattersPast President RACS

Bullyingisarealproblemforourprofession.Most
ofushaveseenorexperiencedit.
Let’s Operate with Respect
Phil TruskettPresident RACS

Beingasurgeontakesmorethantechnicalexcellence.Howwebehaveshapesourcultureandprofession.
Let’s Operate with Respect
Spencer BeasleyVice President RACS

Wesley Hospital, Brisbane, Aug 2016
41