prognostic value of the copper transporters, ctr1 and ctr2, in patients with ovarian carcinoma...
TRANSCRIPT

Gynecologic Oncology 122 (2011) 361–365
Contents lists available at ScienceDirect
Gynecologic Oncology
j ourna l homepage: www.e lsev ie r.com/ locate /ygyno
Prognostic value of the copper transporters, CTR1 and CTR2, in patients with ovariancarcinoma receiving platinum-based chemotherapy
Yoo-Young Lee a, Chel Hun Choi a, In-Gu Do b, Sang Yong Song c, Wooseok Lee a, Hwang Shin Park a,Tae Jong Song a, Min Kyu Kim a, Tae-Joong Kim a, Jeong-Won Lee a, Duk-Soo Bae a, Byoung-Gie Kim a,⁎a Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Republic of Koreab Experimental Pathology Center, Samsung Cancer Research Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, 135-710c Department of pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, 135-710
⁎ Corresponding author at: Department of ObstetriMedical Center, Sungkyunkwan University School oGangnam-gu, Seoul 135-710, Republic of Korea. Fax: +
E-mail address: [email protected] (B.-G. Kim).
0090-8258/$ – see front matter © 2011 Elsevier Inc. Aldoi:10.1016/j.ygyno.2011.04.025
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 1 February 2011Accepted 18 April 2011Available online 13 May 2011Keywords:CTR1CTR2Ovarian neoplasmChemotherapyDrug resistance
Objective. CTR1 and CTR2 are copper transporters that have been associated with platinum sensitivity inseveral human cancers. We investigated the prognostic significance of CTR1 and CTR2 in women with ovariancarcinoma.
Materials and methods. We evaluated the expression of CTR1 and CTR2 using real-time PCR in 40 womenwith ovarian carcinoma (IIb=2, IIIb=2, IIIc=30, IV=6). We compared the expression of CTR1 and CTR2with participants' clinicopathological findings.
Results. We found lower expression of CTR1 and CTR2 mRNA in ovarian cancer cells against normalovarian tissue with statistically significant differences (p=0.018 and 0.011, respectively). High CTR1expression was a prognostic factor for improved survival after adjusting for age, tumor grade, stage, residualtumor, and CTR2 mRNA expression (HR, 0.35; 95% CI, 0.15–0.84). However, CTR2 expression did not exhibit
any prognostic significance. Of the 20 women with elevated CTR1 expression, 17 (85%) were sensitive toplatinum-based chemotherapy. Of the 7 women with low CTR1 expression and high CTR2 expression, 6(85.7%) were resistant to platinum-based chemotherapy and had the shortest progression-free survival of allwomen in our study sample.Conclusion. In our sample of 40 women with ovarian carcinoma, high CTR1 expression was significantlyassociated with sensitivity to platinum-based chemotherapy and longer progression-free survival.Conversely, low CTR1 expression and high CTR2 expression were significantly associated with resistance toplatinum-based chemotherapy and the shortest survival.
© 2011 Elsevier Inc. All rights reserved.
Introduction
Cancer of the ovarian epithelium is the leading cause of death fromgynecological malignancies [1], as more than 60% of patients presentwith advanced disease. The 5-year survival rate is 11% in stage IVdisease and ranges from 23% to 41% for stage III disease [2]. Standardtreatment consists of debulking surgery followed by combinationchemotherapy with taxane and platinum [3]. Although most cancersrespond to chemotherapy initially, the tumor may recur with newlyacquired drug resistance, leading to a poor prognosis. For example,patients with platinum-resistant recurrent disease, defined as tumorrecurrence less than 6 months after the completion of primarytherapy, have shorter survival than platinum-sensitive patients [2].
Given the poor outcomes of platinum-resistant ovarian carcinoma,investigation into the mechanisms of platinum resistance is urgently
cs and Gynecology, Samsungf Medicine, 50 Irwon-dong,82 2 3410 0630.
l rights reserved.
needed. Recent in vitro studies have associated the copper transporter,CTR, with platinum resistance [4]. In particular, CTR1, the main copperuptake transporter, hasbeen shown toplaya regulatory role in the cellularaccumulation of platinum drugs. CTR2, another copper uptake protein,may alsoplay a regulatory role in cisplatinuptake andhas shownoppositeeffects on platinum sensitivity compared to CTR1 in in vitro studies [5,6].However, these findings have not been replicated in patients with cancer.
The purpose of the current study is to investigate the roles of CTR1and CTR2 in women with ovarian carcinoma who were treated withprimary debulking surgery followed by platinum-based chemotherapy.
Materials and methods
Tumor samples
We retrospectively enrolled the patients with IRB approval (IRBno. 2005-11-025-004). We obtained fresh frozen tumor specimensfrom the primary ovary during surgery fromwomenwith serous-typeepithelial ovarian carcinoma (n=40: IIb=2, IIIb=2, IIIc=30,

362 Y.-Y. Lee et al. / Gynecologic Oncology 122 (2011) 361–365
IV=6). As controls, we also obtained normal ovarian tissue (n=11)from women who underwent hysterectomies for benign disease. Wecould use all available samples collected and clinical data werecollected prospectively. All operations were performed by theDepartment of Obstetrics and Gynecology at Samsung Medical Centerbetween October 2003 and November 2005. All women with cancerunderwent primary maximum cytoreductive surgery followed byintravenous paclitaxel (175 mg/m2) or docetaxel (75 mg/m2) pluscarbolatin (AUC 5) combination chemotherapy every 3 weeks for6–8 cycles. We divided the women into 2 groups according to theirsensitivity to first-line platinum-based combination chemotherapy:platinum-resistant was defined as a recurrence after a platinum-free interval of less than 6 months; platinum-sensitive was definedas a recurrence after a platinum-free interval greater than or equalto 6 months [2].
RNA isolation and real-time quantitative PCR
We extracted total RNA from ovarian carcinomas and normalovarian tissues using a mirVana™Total RNA Isolation Kit (Ambion, TX,USA) according to the manufacturer's protocol. RNA was extracted inthe tumor samples which consisted of more than 70% of cancer cellsand in the surface epithelium of the normal ovary as a control. Wequantified the RNA concentration using the NanoDrop ND-1000Spectrophotometer (Nano-Drop Technologies, USA) and performedcDNA synthesis with the High-Capacity cDNA Archive Kit (4368813;
Fig. 1. (A) CTR1 and (B) CTR2 mRNA expression in normal ovarian tissues and serous ovatumor).
Applied Biosystems, Foster City, CA, USA) following the kit's protocol.We performed TaqMan PCRwith an ABI PRISM 7900HT Fast-Time PCRSystem (Applied Biosystems) according to the manufacturer's in-structions. We purchased real-time PCR primers and probes forhuman CTR1 (Hs00977268_g1), human CTR2 (Hs00156984_m1), andglyceraldehyde 3-phosphate dehydrogenase (GAPDH) (4310884E)from Applied Biosystems [7]. The relative expression levels of CTRmRNA were normalized to the amount of GAPDH in the same cDNAusing the ΔΔCt method described by the manufacturer [8].
Immunohistochemical (IHC) stains
IHC for CTR1 was performed in another patient set (n=20) whohad stage III high grade serous ovarian cancer with suboptimaldebulking at initial surgery and followed by platinum basedchemotherapy. IHC studies were carried out on formalin-fixed,paraffin-embedded, 4 μm-thick tissue sections. The primary anti-bodies used were rabbit polyclonal to SCL31A1/CTR1 (Abcam,Cambridge, UK; 1:250). Tissue sections were deparaffinized 3 timesin xylene for a total of 15 min and subsequently rehydrated. Antigenretrieval was carried out at 97 °C, PTLink (DAKO, Glostrup, Denmark)for 20 min in EDTA buffer (pH 8.0). After blocking the endogenousperoxidase activity with 3% hydrogen peroxidase for 5 min, theprimary antibody incubation was carried out for 30 min at roomtemperature. The antigen–antibody reaction was detected using theDAKO REAL™ Envision™ Detection System, Peroxidase/DAB K5007
rian carcinomas according to real-time quantitative PCR (N indicates normal ovary; T,
363Y.-Y. Lee et al. / Gynecologic Oncology 122 (2011) 361–365
(DAKO, Glostrup, Denmark). Counter-staining was performed withMayer's hematoxylin. Negative controls (substitution of primaryantibody for TBS) were run simultaneously. The slides were assessedwithout knowledge of the clinical outcome by a pathologist (Dr. In-GuDo). Staining for CTR1 was considered to be positive when tumor cellsshowed cytoplasmic reactivity. The intensity of IHC staining wasgraded on a semiquantitative scale from 0 to 3, where 0=no staining,1=weak staining, 2=moderate staining, and 3=strong staining.
Statistical analysis
After confirming whether the data were normally distributed withthe Shapiro–Wilk test, we used the Wilcoxon rank sum test tocompare median values, the two-sample t-test to compare meanvalues, and the Cox proportional hazards model for multivariateanalyses. We compared the frequency distributions between categor-ical variables using the Chi-square test and used the Fisher's exact testif the expected frequency was less than 5. We calculated the overalland progression-free survival curves according to the Kaplan–Meiermethod using the log-rank test. We used SPSS software (version 12.0;SPSS, Chicago, IL, USA) for all statistical analyses. All p-values weretwo-sided and considered statistically significant if p≤0.05.
Results
CTR1 and CTR2 mRNA expression
We could obtain 51 samples in total. CTR1 and CTR2 transcriptswere quantified in the serous ovarian carcinomas of 40 women andthe normal ovarian tissues of 11 women (Fig. 1). We found lowerexpression of CTR1 and CTR2 mRNA in ovarian cancer cells againstnormal ovarian tissue with statistically significant differences(p=0.018 and 0.011, respectively).
Clinicopathological features according to CTR1 and CTR2 mRNAexpressions in ovarian carcinomas
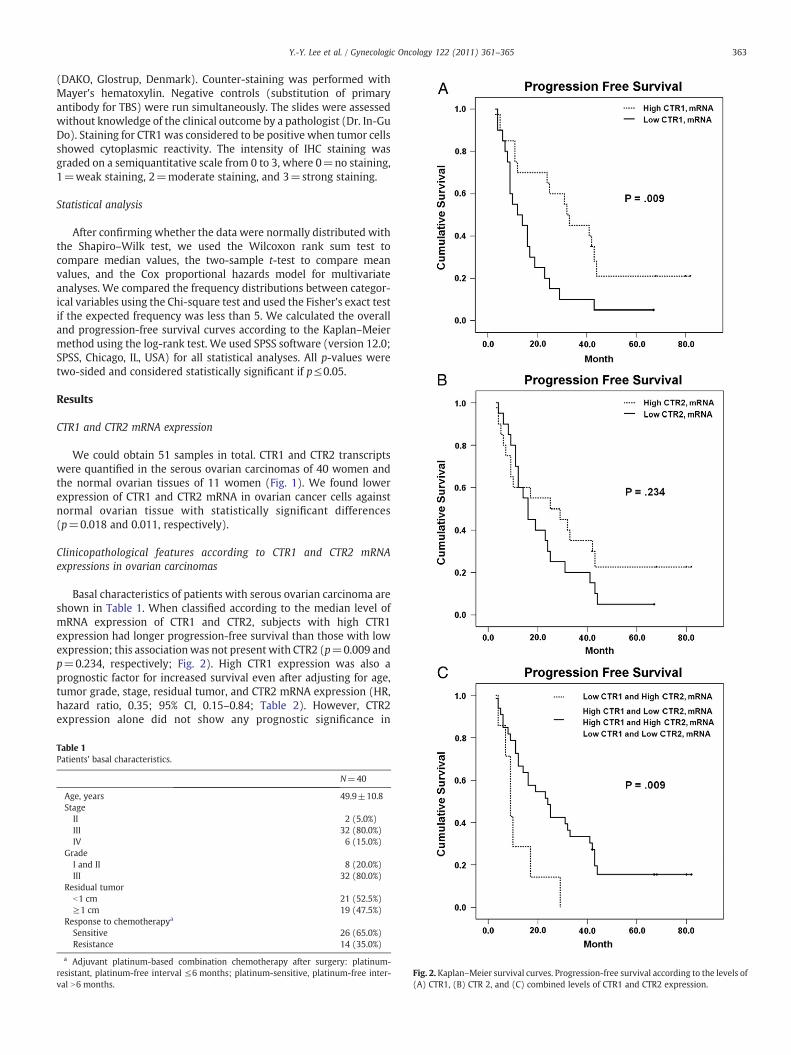
Basal characteristics of patients with serous ovarian carcinoma areshown in Table 1. When classified according to the median level ofmRNA expression of CTR1 and CTR2, subjects with high CTR1expression had longer progression-free survival than those with lowexpression; this associationwas not present with CTR2 (p=0.009 andp=0.234, respectively; Fig. 2). High CTR1 expression was also aprognostic factor for increased survival even after adjusting for age,tumor grade, stage, residual tumor, and CTR2 mRNA expression (HR,hazard ratio, 0.35; 95% CI, 0.15–0.84; Table 2). However, CTR2expression alone did not show any prognostic significance in
Table 1Patients' basal characteristics.
N=40
Age, years 49.9±10.8Stage
II 2 (5.0%)III 32 (80.0%)IV 6 (15.0%)
GradeI and II 8 (20.0%)III 32 (80.0%)
Residual tumorb1 cm 21 (52.5%)≥1 cm 19 (47.5%)
Response to chemotherapya
Sensitive 26 (65.0%)Resistance 14 (35.0%)
a Adjuvant platinum-based combination chemotherapy after surgery: platinum-resistant, platinum-free interval ≤6 months; platinum-sensitive, platinum-free inter-val N6 months.
Fig. 2. Kaplan–Meier survival curves. Progression-free survival according to the levels of(A) CTR1, (B) CTR 2, and (C) combined levels of CTR1 and CTR2 expression.

Table 2Univariate and multivariate analyses of progression-free survival.
Univariateanalysis
Multivariateanalysis
HR (95% CI) p-Value HR (95% CI) p-Value
Age 1.00 (0.96–1.03) .803 1.00 (0.96–1.04) .959Stage (II vs. III vs. IV) – .984 – .993Grade
I and II 1 1III 1.55 (0.64–3.75) .333 1.91 (0.69–5.27) .210
Residual tumorb1 cm 1 1≥1 cm 1.63 (0.82–3.20) .161 1.48 (0.72–3.05) .289
CTR1, mRNALow (n=20) 1 1High (n=20) 0.41 (0.20–0.82) .012 0.35 (0.15–0.84) .018
CTR2, mRNALow (n=20) 1 1High (n=20) 0.67 (0.34–1.32) .244 1.35 (0.57–3.19) .496
CTR1 and CTR2, mRNALow and high 1The others 3.02 (1.25–7.34) .015 4.39 (1.46–13.23) .009a
HR indicates hazard ratio; CI, confidence interval; Cox proportional-hazards model wasused for the analyses.
a Adjusted by age, stage, grade, and residual tumor.
364 Y.-Y. Lee et al. / Gynecologic Oncology 122 (2011) 361–365
women with ovarian carcinoma. When combining the expressionpatterns of CTR1 and CTR2, women with low CTR1 expression andhigh CTR2 expression had the shortest progression-free survival of allparticipants (p=0.009;Fig. 2). This particular expression patternremained a poor prognostic factor in multivariate analysis (HR, 4.39;95% CI, 1.46–13.23; Table 2).
In regard to chemosensitivity, 85% of women with high CTR1expression (17/20) were sensitive to platinum-based chemotherapy,while only 45% of women with low CTR1 expression (9/11) werechemosensitive (p=0.008). Contrary to CTR1, the relationshipbetween low CTR2 expression and chemosensitivity (15/20, 75.5%)was not statistically significant. Of the women with low CTR1expression and high CTR2 expression, 85.7% (6/7) were resistant toplatinum-based chemotherapy (Table 3). When we divided thepatients based on response to chemotherapy (platinum-resistant orplatinum-sensitive), CTR1 expression could not be an independentprognostic factor for survival in each group.
Fig. 3. Immunohistochemical evaluation of CTR1 in the serous ovarian carcinoma((A), +1; (B), +3; all photographs were taken at original magnification ×100).
Immunohistochemical staining of CTR1
In another group of patients (n=20; sensitive cases=12,resistance cases=8) who had stage III high grade serous ovariancancer with suboptimal debulking at initial surgery and followed by
Table 3Correlation of CTR1 and CTR2 mRNA levels with chemosensitivity.
Resistancea Sensitivea p-Value
N=14 N=26
CTR1, mRNA .008b
Low 11 (55.0%) 9 (45.0%)High 3 (15.0%) 17 (85.0%)CTR2, mRNA .185b
Low 5 (25.0%) 15 (75.5%)High 9 (45.0%) 11 (55.0%)CTR1 and CTR2, mRNA .004b
Low CTR1 and high CTR2 6 (85.7%) 1 (14.3%)The others 8 (24.2%) 25 (75.8%)
a Adjuvant platinum-based combination chemotherapy after surgery: platinum-resistant, platinum-free interval ≤6 months; platinum-sensitive, platinum-free inter-val N6 months.
b Fisher's exact test or Pearson Chi-square.
platinum based chemotherapy, patients with the strongest expressionof CTR1 (+3) showed platinum-sensitivity in 80% (8/10), but theother patients (0, +1, +2), in 40% (4/10) (p=0.170; Fig. 3).
Discussion
In this study, we found that the expression of CTR1 and CTR2 wassignificantly lower in primary serous ovarian carcinoma tissuecompared to normal ovarian tissue. Among women with cancer,high CTR1 expression was significantly associated with increasedsensitivity to platinum-based chemotherapy and longer progression-free survival in multivariate analysis. Subjects with low CTR1expression and high CTR2 expression had the poorest response toplatinum-based chemotherapy and the shortest progression-freesurvival of the study sample.
In kinetic studies of platinum drug accumulation, it has beenreported that substantial fraction of the transport and intracellular

365Y.-Y. Lee et al. / Gynecologic Oncology 122 (2011) 361–365
distribution of the drug are influenced by copper homeostasisproteins [4,9]. In regard to CTR1, the major copper uptake transportprotein [10], several studies found that deletion of the CTR1 gene inyeast and mammalian cells markedly reduced cisplatin uptake andincreased resistance to cisplatin cytotoxicity [11,12]; further studieson CTR1 in cancer cell lines reported similar findings [13–18]. Morerecently, CTR2, a copper transport protein with substantial structuralhomology to CTR1, was shown to regulate sensitivity to the cytotoxiceffects of cisplatin, with a function opposite to that of CTR1 [5,6].However, none of these findings have been correlated with clinicalresistance to platinum-based chemotherapy in cancer patients.
The results of our study correspond well with those of in vitrostudies that implicated CTR1 in the influx of platinum drugs [18] andidentified the protein as a major determinant of responsiveness tocisplatin [15,16]. After adjusting for several clinical factors related toprognosis, we found that high CTR1 expression was an independentprognostic factor for survival in women with ovarian cancer.However, high CTR2 expression showed only a trend towards higherrates of platinum resistance, a result that was not statisticallysignificant, which is inconsistent with the results of previous in vitrostudies [5,6]. For example, Blair et al. reported that CTR2 geneknockout increased cisplatin uptake regardless of CTR1 expression [6]and, after a follow-up study, concluded that CTR1 and CTR2 haveopposite effects on cisplatin sensitivity [5]. Given that little is knownabout the function of CTR2 in mammalian cells and cancer cells,especially in relation to cisplatin sensitivity, further study is needed todraw such a conclusion. Nonetheless, our finding that those womenwith low CTR1 and high CTR2 had theworst prognosis and the highestrate of platinum resistance (85.7%) supports the hypothesis that theseproteins play opposite roles in platinum sensitivity.
Platinum drugs appear to enter the cell by a variety of mechanisms[19,20], including passive diffusion and various endocytic routes [4].Several other copper transport proteins have been found to beassociated with cisplatin regulation, including Atox1 [21], ATP7A [22],and ATP7B [23], all of which are associated with copper efflux fromthe cell. The relationship among copper transport proteins and theway in which they collectively control intracellular cisplatin levelsremain unclear and warrant further investigation.
One limitation of our study is the relatively small patientpopulation. Moreover, the difference of protein expression of CTR1in another patient set showed only marginal significance on platinumsensitivity, which means our findings must be validated at the proteinlevel in future study with larger cohort. Furthermore, we could notfind available CTR2 antibody for IHC. Finally, we should be concernedthat obtaining epithelial tissue from the normal ovary might becontaminated by the mesenchymal component. As a result, theepithelial component of the ovary may be diluted in patients withnormal ovaries, which might have resulted in unreliable results ofdifference in mRNA expression of CTR1 and CTR2 between normalovary and tumor. Nevertheless, of particular interest, several recentstudies on ovarian cancer suggest that an in vitro chemosensitivity testcan improve the response rate and possibly even increase survival incertain patients [24]. The promising results of our study suggest thatmeasurement of CTR1 and CTR2 expression may be useful to predictplatinum response in the future.
In conclusion, our study has demonstrated that high CTR1expression is significantly associated with longer progression-freesurvival regardless of CTR2 expression. In particular, low CTR1expression along with high CTR2 expression was associated withplatinum resistance and with the worst prognosis of all women withovarian carcinoma in our study sample.
Disclosure of potential conflicts of interestNo potential conflicts of interest were disclosed.
Acknowledgments
This study was supported by a grant of the Korea HealthcareTechnology R&D Project, Ministry for Health and Welfare Affairs,Republic of Korea (A092255).
References
[1] Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer JClin 2009;59:225–49.
[2] Berek JS. In: Berek JS, editor. Berek & Novak's gynecology, 14th edition; 2007.p. 1426.
[3] du Bois A, Luck HJ, Meier W, Adams HP, Mobus V, Costa S, et al. A randomizedclinical trial of cisplatin/paclitaxel versus carboplatin/paclitaxel as first-linetreatment of ovarian cancer. J Natl Cancer Inst 2003;95:1320–9.
[4] Safaei R. Role of copper transporters in the uptake and efflux of platinumcontaining drugs. Cancer Lett 2006;234:34–9.
[5] Blair BG, Larson CA, Adams PL, Abada PB, Safaei R, Howell SB. Regulation of coppertransporter 2 expression by copper and cisplatin in human ovarian carcinomacells. Mol Pharmacol 2010;77:912–21.
[6] Blair BG, Larson CA, Safaei R, Howell SB. Copper transporter 2 regulates the cellularaccumulation and cytotoxicity of cisplatin and carboplatin. Clin Cancer Res2009;15:4312–21.
[7] Ishida S, McCormick F, Smith-McCune K, Hanahan D. Enhancing tumor-specificuptake of the anticancer drug cisplatin with a copper chelator. Cancer Cell2010;17:574–83.
[8] Lee JW, Choi CH, Choi JJ, Park YA, Kim SJ, Hwang SY, et al. Altered microRNAexpression in cervical carcinomas. Clin Cancer Res 2008;14:2535–42.
[9] Safaei R, Holzer AK, Katano K, Samimi G, Howell SB. The role of copper transportersin the development of resistance to Pt drugs. J Inorg Biochem 2004;98:1607–13.
[10] Moller LB, Petersen C, Lund C, Horn N. Characterization of the hCTR1 gene:genomic organization, functional expression, and identification of a highlyhomologous processed gene. Gene 2000;257:13–22.
[11] Lin X, Okuda T, Holzer A, Howell SB. The copper transporter CTR1 regulatescisplatin uptake in Saccharomyces cerevisiae. Mol Pharmacol 2002;62:1154–9.
[12] Ishida S, Lee J, Thiele DJ, Herskowitz I. Uptake of the anticancer drug cisplatinmediated by the copper transporter Ctr1 in yeast andmammals. Proc Natl Acad SciU S A 2002;99:14298–302.
[13] Holzer AK, Manorek GH, Howell SB. Contribution of the major copper influxtransporter CTR1 to the cellular accumulation of cisplatin, carboplatin, andoxaliplatin. Mol Pharmacol 2006;70:1390–4.
[14] Holzer AK, Howell SB. The internalization and degradation of human coppertransporter 1 following cisplatin exposure. Cancer Res 2006;66:10944–52.
[15] Song IS, Savaraj N, Siddik ZH, Liu P, Wei Y, Wu CJ, et al. Role of human coppertransporter Ctr1 in the transport of platinum-based antitumor agents in cisplatin-sensitive and cisplatin-resistant cells. Mol Cancer Ther 2004;3:1543–9.
[16] Holzer AK, Samimi G, Katano K, Naerdemann W, Lin X, Safaei R, et al. The copperinflux transporter human copper transport protein 1 regulates the uptake ofcisplatin in human ovarian carcinoma cells. Mol Pharmacol 2004;66:817–23.
[17] Holzer AK, Katano K, Klomp LW, Howell SB. Cisplatin rapidly down-regulates itsown influx transporter hCTR1 in cultured human ovarian carcinoma cells. ClinCancer Res 2004;10:6744–9.
[18] Larson CA, Blair BG, Safaei R, Howell SB. The role of the mammalian coppertransporter 1 in the cellular accumulation of platinum-based drugs. MolPharmacol 2009;75:324–30.
[19] Mann SC, Andrews PA, Howell SB. Modulation of cis-diamminedichloroplatinum(II) accumulation and sensitivity by forskolin and 3-isobutyl-1-methylxanthine insensitive and resistant human ovarian carcinoma cells. Int J Cancer 1991;48:866–72.
[20] Binks SP, Dobrota M. Kinetics and mechanism of uptake of platinum-basedpharmaceuticals by the rat small intestine. Biochem Pharmacol 1990;40:1329–36.
[21] Safaei R, Maktabi MH, Blair BG, Larson CA, Howell SB. Effects of the loss of Atox1 onthe cellular pharmacology of cisplatin. J Inorg Biochem 2009;103:333–41.
[22] Samimi G, Safaei R, Katano K, Holzer AK, Rochdi M, Tomioka M, et al. Increasedexpression of the copper efflux transporter ATP7Amediates resistance to cisplatin,carboplatin, and oxaliplatin in ovarian cancer cells. Clin Cancer Res 2004;10:4661–9.
[23] Nakayama K, Kanzaki A, Terada K, Mutoh M, Ogawa K, Sugiyama T, et al.Prognostic value of the Cu-transporting ATPase in ovarian carcinoma patientsreceiving cisplatin-based chemotherapy. Clin Cancer Res 2004;10:2804–11.
[24] Cree IA. Chemosensitivity and chemoresistance testing in ovarian cancer. CurrOpin Obstet Gynecol 2009;21:39–43.