programme guidelines for trainees
TRANSCRIPT

DOCTOR OF ORTHOPAEDICS and TRAUMATOLOGY
(DOKTOR PAKAR ORTOPEDIK dan TRAUMATOLOGI)
Dr. Ortho & Trauma (UKM)
PROGRAMME GUIDELINES FOR TRAINEES
DEPARTMENT OF ORTHOPAEDICS and TRAUMATOLOGY
FACULTY OF MEDICINE
UNIVERSITI KEBANGSAAN MALAYSIA
2018/19
CONTENTS
1. Doctor of Orthopaedics and Traumatology 1.1 Introduction ..............................................................................3 1.2 Course Objectives ....................................................................4 1.3 Course Structure and Format ...................................................4 - 5 1.4 Entry Requirements ..................................................................6 1.5 Rules, Regulations and Monitoring ...........................................7 - 13
1.5.1 Log Book ...........................................................................7 - 8 1.5.2 Case Book .........................................................................8 - 9 1.5.3 Dissertation .......................................................................10 1.5.4 Fees and Annual Leave ....................................................11 1.5.5 Postponement, Deferment, Exemption and Termination ...11 - 12 1.5.6 Short Courses ....................................................................12 1.5.7 Awards ...............................................................................12 -13
1.6 Guidelines to Examinations .........................................................13
2. Part I Examination .................................................................................14 - 28
2.1 Syllabus for Part I .......................................................................14 - 26 2.2 Examination Structure and Format .............................................26 - 27 2.3 Recommended Texts and References .......................................27 - 28
3. Part II Examination .................................................................................28 - 32 3.1 Syllabus for Part II .......................................................................28 - 30 3.2 Examination Structure and Format .............................................31 - 32 3.3 Recommended Texts and References ........................................32
4. Attachments .............................................................................................33 - 43 4.1 Attachment I: Trainee Assessment Form ......................................33 - 41 4.2 Attachment II: Cover Page of Log Book of Operations .................42 4.3 Attachment III: Inside Page of Log Book of Operations ................43 4.4 Attachment IV: Mahmood Merican Award .....................................44 4.5 Attachment V: Candidate Portfolio..................................................45 - 62
2

1. DOCTOR OF ORTHOPAEDICS and TRAUMATOLOGY
1.1 INTRODUCTION
The Faculty of Medicine, Universiti Kebangsaan Malaysia (UKM) was the first in Malaysia to initiate the postgraduate programme in surgery: this began with Orthopaedic Surgery and General Surgery in June 1981. These were credited to the efforts of the late Prof QM Iqbal (Orthopaedic Surgery) and the late Prof Sir Harry Annanamuntodo (Dept of Surgery).
The postgraduate programme in Orthopaedic Surgery started with the intake of 3 orthopaedic trainee lecturers, all of whom graduated in 1986. The programme was in the form of a closed system, structured in-service training where trainees were taught and trained within the Department of Orthopaedics and Traumatology, UKM and the General Hospital, Kuala Lumpur (1981 – 1997) and later Hospital UKM (from 1998).
After discussions with the Ministry of Health (MOH) Malaysia, who became the major stakeholders, the Open System was started in June 1996 with an intake of 21 trainees (16 from MOH and the rest from Universities). The Open System involves trainees from MOH, where they were taught and trained in the initial 2 years in MOH hospitals accredited by the University (later by the Conjoint Board of Orthopaedics); the 3rd year in General Hospital, Kuala Lumpur (now known as Hospital Kuala Lumpur) and the 4th (final) year in the Department of Orthopaedics and Traumatology, UKM.
Demand for the need of orthopaedic surgeons from the MOH, Malaysia culminated in the largest intake in June 1997 of 23 trainees. In June 1995, the first female trainee from MOH entered the training programme and completed her training in May 1999.
The orthopaedic postgraduate programme then expanded further with the first intake of international trainees in June 2003 (1 from Sudan and another from Indonesia). As of June 2014, there were international trainees from 8 different countries. All international trainees are trained under the Closed System.
The year 2003 also witnessed the coming together of the orthopaedic departments of the 3 major universities in Malaysia [UKM, UM and USM (Universiti Sains Malaysia)] to form the Conjoint Board of Orthopaedics under the umbrella of the National Conjoint Board for postgraduate studies together with the Academy of Medicine and the MOH. The Part II examinations are now held conjointly involving the International Islamic University of Malaysia (IIUM) in 2007 and UNIMAS in 2014.
The Department of Orthopaedics and Traumatology, UKM has as of May 2014, produced 285 graduates, of whom 27 are women, in Orthopaedic Surgery in Malaysia. These orthopaedic surgeons, many of whom are now teachers and trainers in their own right as well as being sub-specialists in various fields of orthopaedic surgery, are now serving the country in the Ministry of Health, the Universities, the Ministry of Defence and private hospitals. Our international trainees are also working in their own countries as well as in Australia, England, Canada and United Arab Emirates.
3

1.2 COURSE OBJECTIVES
At the end of the course, the trainee is expected to have acquired sufficient
knowledge and surgical skills to perform as a safe and competent orthopaedic
surgeon at the level of a first year orthopaedic surgeon in a general hospital.
1.3 COURSE STRUCTURE and FORMAT
This is a 4-year in-service training programme covering a staged progression of
learning processes of acquiring knowledge and surgical skills. Teaching as well
as examinations are conducted in English. Trainees shall not be allowed to
remain in the programme for more than 7 years.
In-service training means that the trainee performs all duties required as a
medical officer in a surgical discipline which include carrying out ward
responsibilities, running outpatient clinics, performing operations or assisting in
operating theatre (OT) sessions and carrying out on-call duties.
Year 1 Trainees are expected to learn and acquire adequate basic sciences knowledge (anatomy, physiology, pathology, microbiology and immunology, basic biomechanic and biomaterial) and principles of orthopaedic surgery to enable appropriate application of knowledge for decision-making in solving clinical problems including executing accurate general surgical procedures as well as procedures related to orthopaedics and traumatology.
Year 2 Trainees are expected to use proactive learning concept to acquire specific surgical skills and skills in decision-making in a specialty training.
Year 3 Trainees are expected to be involved in proactive guidance to consolidate their skills in decision-making to a level equivalent to that of a surgical registrar and serve to assist and perform certain surgical procedures under supervision.
Year 4 Trainees are expected to assume the function of a senior registrar with competency to lead a team to handle common problems including management of critically ill patients. Trainees are allowed to perform operative procedures under the supervision of a consultant.
4

Course Programme
Year Course Content
1 Basic Sciences Basic Sciences General Orthopaedics Basic Trauma Rotation within specialties 12 weeks Rotation within specialties 12 weeks
2 General Orthopaedics Basic Trauma Basic Trauma Rotation within specialties 12 weeks
Rotation within specialties 12 weeks Elective (optional) : 3 – 6 months (in either 2nd or 3rd Year)
3 Rotation in Specialty Postings 3 months each
Advance Trauma Paediatric Orthopaedics Arthroplasty Rehabilitation Hand and Microsurgery Spine Orthopaedic Oncology Sports and Arthroscopy
Elective (optional) : 3 – 6 months (in either 2nd or 3rd Year)
4 Rotation in Specialty Postings 3 months each
Paediatric Orthopaedics Arthroplasty Rehabilitation Hand and Microsurgery Spine Advance Trauma Sports and Arthroscopy Orthopaedic Oncology
NOTE: From June 2014, all trainees including PGY4 will undergo a 3-monthly
rotation. There will be an end of posting assessment for all PGY3 and PGY4
trainees at the end of each rotation. The assessment will consist of a theory
and/or viva examination and a clinical assessment [short cases].
PGY3 trainees who fail 3 or more postings will not be promoted to Y4. PGY4 trainees who fail 2 postings will not be eligible to sit for the Part 2 examination and will be extended by another 6 months. PGY4 trainees are also required to teach medical students on clinical examination techniques. On completion of the course and passing the required examinations, the trainee
shall be conferred the degree of Doctor of Orthopaedics and Traumatology This is the highest professional and academic qualification awarded by
UKM in Orthopaedics and Traumatology. On obtaining the degree, the trainee is eligible for registration as a
specialist in Orthopaedics and Traumatology, after a period of 6 months
supervision under an orthopaedic surgeon. 5

1.4 ENTRY REQUIREMENTS
1.4.1 MALAYSIAN APPLICANTS
1. Graduates of medical schools in Malaysia with a credit in Bahasa Malaysia
at the Sijil Pelajaran Malaysia (SPM) level. 2. Malaysians who graduate from foreign universities (Commonwealth
countries) with MBBS, MBChB, MD or its equivalent from a recognized university by Malaysian Medical Council(MMC) with a credit in Bahasa Malaysia and English at the SPM level.
3. Registered with the Malaysian Medical Council. 4. Applicants must have at least 2 years clinical experience after
graduation from medical school.
1.4.2 INTERNATIONAL APPLICANTS
1. First medical degree is recognized by the Malaysian Medical Council (MMC).
2. Registration is required with the MMC.
3. Must have at least 3 years clinical experience after 1st
medical degree (1 year internship / housemanship and 2 years medical officer).
4. Must have a Medical Examination Report from a Malaysian medical practitioner.
5. Must have medical insurance. 6. Must be fluent in speaking and writing in English; must posses TOEFL
score of at least 750 or IELTS band 7. 7. Priority shall be given to trainees who posses scholarship / sponsorship. 8. Trainees without scholarship / sponsorship must submit a bank statement
of accounts and must possess at least USD 20,000.00. 9. A period of clinical attachment of 3 months followed by an interview to
determine eligibility is required before being accepted into the programme.
10. It is also mandatory for all foreign trainees to take the Malay language course organised by the university, which runs over period of 14 weeks. The course is conducted after office hours, and no one is exempted, including those from Indonesia, Brunei and Singapore.
METHOD OF APPLICATION
For Malaysian applicants, this shall be on application forms obtained from the
Unit Pusat Universiti (UPU) of the Ministry of Education following advertisement
in the Malaysian newspapers.
For international applicants, the application is through the university’s Centre for
Graduate Studies [Pusat Pengajian Siswazah (PSS)], available on the Internet at
www.ukm.my/pps
6

1.5 RULES, REGULATIONS and MONITORING
Commencing June 2014:
1. Upon entering the postgraduate programme, supervisors from the Orthopedic Department where the trainee is posted shall be allotted to trainees.
2. Trainees exempted from Part I [those who have passed the BSE Orth from November 2014 or those with membership of the Royal College of Surgeons (MRCS) degree or its equivalent] and those who have passed the Part I shall discuss with their supervisors regarding the nature and process of the research project for the dissertation.
3. Trainees shall meet with their supervisors regularly to discuss and report on their progress with regard to continuous assessment, research project for dissertation and case write-ups.
4. Supervisors shall submit their reports to the Trainee Coordinator/Head,
Department of Orthopaedics and Traumatology, UKM before the end of each
semester (i.e. before 31 May and 30 Nov) on the progress of the trainees as
stated in (3) above (c.f. ATTACHMENT I: Trainee Assessment Form).
5. For trainees who come to HUKM in the 3rd year, internal supervisors shall be appointed to them to ensure continuity of supervision.
6. Dissertations and case write-ups should be accepted as satisfactory by supervisors before being submitted in bound form (hard cover) 5 months before the Final (Part II) Examinations:
6.1 End of December for trainees sitting the May examination
6.2 End of June for trainees sitting the November examination.
NOTE:
Trainees who fail to submit their assessment forms or whose assessment
reports are poor may not be allowed to proceed to the next semester / year.
Trainees who fail to comply with article (6) above shall not be allowed to sit for
the CBO (Conjoint Board of Orthopaedics) Final (Part II) examinations.
As of June 2009, promotion to 2nd Year is only after passing Part I exams. The
trainee must complete the course within a minimum of 4 years and a maximum
of 7 years.
1.5.1 LOG BOOK
LOG BOOK of OPERATIONS:
1. The log book is important as one of the means of assessing the trainee’s progress in surgical exposure / experience.
2. Trainees are to required to enter surgical operations that they have assisted / performed under supervision / performed on their own into the log book.
7

3. As a standardisation procedure, the format of entry is as in the log book provided; no other format is to be used (cf ATTACHMENT II and ATTACHMENT III).
4. Trainees are advised to group their log books under various categories e.g. Trauma, General Orthopaedics, Spine, Paediatric Elective Orthopaedics, Arthroplasty, LLRS (Limb Lengthening and Reconstructive Surgery), Orthopaedic Oncology, Hand and Microsurgery and Sports Orthopaedics.
5. It is advised that these entries are made at the end of each surgical operation i.e. entry into the book is to be done sequentially and not in retrospect.
6. The book must be available for inspection on request by the supervisor. 7. It is advised that a digital copy is also made and kept by the trainee as a
back-up. 8. The hard copy of the log book must be safely-kept and maintained by the
trainee to be shown to his/her supervisor on a regular basis and also for perusal by the Department of Orthopaedics UKM towards the end of the final year.
9. Any deficiencies therein must be rectified to the satisfaction of the supervisor and the Department before allowing the trainee to proceed for the CBO Part II examination.
10. The logbook shall be shown to the external examiner before the CBO Part II examination and may be used in the viva examination as a platform to question the trainee.
1.5.2 CASE BOOK
1. The case book must be approved by the supervisor and the department
before it can be formally accepted as a complete work enabling the
trainee to be eligible to sit for the CBO Part II examination.
2. Trainees are required to write 10 case write-ups which are to be
submitted to the Department in bound form 5 months before the CBO Part
II examinations (i.e. end of December and end of June).
3. Four copies are required (one each for the Department, the Faculty, the
University and the trainee).
4. Case write-ups should be 3 on Trauma and one each on Paediatric
Orthopaedics, Spine, Arthroplasty, Hand and Microsurgery, Sports
Orthopaedics, Oncology and Rehabilitation.
5. Case write-ups should be on interesting, unique, unusual or rare cases
and should be good enough to be to be submitted to a journal for
publication.
6. Since the trainee is training to be an orthopaedic surgeon, the case write-
up should involve an operative procedure.
8

7. The general outline of the case write-up should be as follows:
i. Patient identification data
ii. Concise history and physical findings
iii. Diagnosis and differential diagnoses, if any
iv. Relevant investigations
v. An account of the operation performed
vi. Postoperative management and follow-up
vii. Discussion
viii. Conclusion or Summary
ix. References
8. The case book shall to be shown to the external examiner for comments before
the CBO Part II examination and may be used in the viva examination as a
platform to question the trainee.
9. The guideline / schedule of writing the case write-ups are as follows:
MINIMUM NO. of CASE WRITE-UPS
CATEGORY to be COMPLETED (cumulative)
During 1st Year 2
During 2nd Year 2
During 3rd Year 3
During 4th Year 3
TOTAL 10
No. of published Case Write-Ups Total no. of Case Write-Ups to
be submitted
1 9
2 8
3 7
4 or more 6
* Please take note that the total number of Case Write-Ups to be submitted (as above) is inclusive of
the published Case Write-Ups
New Policy Commencing 1.6.2009:
1. Failure to submit the required no. of case write-ups at the end of each study year
may lead to a 6-month extension in the course.
NOTE: Failure to comply results in failure to progress to the subsequent year of study or non-
permission to sit for the final examinations.
9

1.5.3 DISSERTATION / THESIS
1. The dissertation / thesis must be approved by the supervisor and the
Department before it can be formally accepted as a complete work enabling
the trainee to be eligible to sit for the CBO Part II examination.
2. The dissertation / thesis shall be shown to the external examiner for
comments before the CBO Part II examination and may be used in the viva
examination as a platform to question the trainee.
3. The general outline of the dissertation / thesis should be as follows:
i. Written in comprehensible language either in Malay or
English. ii. Preceded with a title and a synopsis. iii. Should be on 210 x 280mm paper, double-spaced type
written with 40mm margin on all sides. iv. The covers should be of hard cloth-covered cardboard.
4. The dissertation/thesis should be in the form of a manuscript ready to be
submitted for publication and must have relevant histograms, tables, charts, figures, photographs or schematic representation and should broadly follow the format below:
i. Abstract not exceeding 300 words ii. Introduction iii. Materials and methods iv. Results v. Discussion vi. Conclusion vii. Acknowledgement viii. References.
5. The trainee is required to present his dissertation at the department
upon completion and a soft copy of the dissertation has to be submitted
to the dept.
6. The trainee is required to submit the abstract of the dissertation / thesis to
the Malaysian Orthopaedic Association (MOA) for presentation in the MOA
Annual Scientific Meeting. The trainee is encouraged to vie for the Mahmood
Merican Award for best oral presentation.
7. The trainee is also required to submit the manuscript of the dissertation
to a local or international journal for publication.
10

1.5.4 FEES and ANNUAL LEAVE
1.5.4.1 FEES
Course fees as Semester I (June) 2018/19:
NOTE: Fees may vary with time.
1.5.4.2 ANNUAL LEAVE
1. Trainees’ application for leave is subject to approval by the department. Leave is allowed up to a maximum of 2 weeks per semester (including maternity / sick leave).
2. Only under special circumstances will leave exceeding this period is considered and will be determined on a case-by-case basis by the department.
1.5.5 POSTPONEMENT, DEFERMENT/SUSPENSION and TERMINATION
1. Postponement of registration into the programme (6 months or 1 year) is
allowed but with valid reasons and with prior notification to the
University/Department at least 1 month before the date of registration.
2. A trainee who is already in the course may apply for suspension/deferment of
1 or 2 semesters but with valid reasons and with prior notification to the
University/Department at least 1 month before the date of the examination.
3. Both the above situations must be approved by the Head of Department and
then by the Secretariat of Postgraduate Studies (SPS) in the Faculty.
11

1.5.5.A Termination of Candidature
The trainee may decide voluntarily to terminate his tenure in the course.
Otherwise, termination is as follows:
[UKM Act (Graduate Studies) 15/11/2000]
i. Infringement of Act and Regulations as stipulated by UKM. ii. Violation of civil law and order. iii. Problems with attitude and behaviour. iv. Poor progress or deterioration in study. v. Mental or physical disability. vi. Indulgence in subversive activities. vii. Contacting examiners to procure examination results.
1.5.6 SHORT COURSES and SKILLS WORKSHOPS
Trainees, at the discretion of the Department, are encouraged to attend short
courses and skills workshops during their 4 years in the programme. These are
held not only UKM Medical Centre (UKMMC) but also in other Universities and
MOH hospitals in the country. Examples of such courses are
i. Intensive courses (for Part I as well as for Part II)
ii. SPSS course
iii. Research Week Course
iv. Basic AO Course
v. Survival Skills Course
vi. Foot and Ankle Course
vii. Hand and Microsurgery Course
viii. Basic Arthroplasty Course
ix. Paediatric Orthopaedic Course etc. NOTE: Course fees (for MOH trainees) - JPA provides RM500.00 subsidy annually.
1.5.7 AWARDS
1.5.7.1 Dr Mohd Noor Manukaran Book Prize
For each semester year, a deserving final year trainee shall be awarded the
above prize in the form of RM500.00 cash. This deserving trainee will be
chosen from amongst all the final year UKM trainees who sat for both the
November and subsequent May CBO Part II examinations. The nominee
shall be the one with the highest score in examination marks and with a
satisfactory record of academic, social and community activities as well as
being of good character and a team player. This prize may not be awarded
if there is no eligible nominee for a particular semester year. This award to
the trainee shall be announced during the University Convocation.
12

1.5.7.2 Professor N Subramanian Award
For each semester year, the Malaysian Orthopaedic Association shall award
a deserving final year trainee with the above prize in the form of a gold
medallion. This deserving trainee will be chosen from amongst all the final
year trainees from the universities who sat for both the November and
subsequent May CBO Part II examinations.
1.6 GUIDELINES TO EXAMINATIONS
1.6.1 PART I
1. The Part I examinations are held every 6 months (May and November). 2. The CBO Part 1 examination will commence in November 2014. 3. Trainees who have obtained the BSE Orthopaedics from November 2014 or
MRCS are exempted from the Orthopaedics Specialty Committee (OSC) Part I examination.
4. Trainees must register for the examination, pay all required fees and meet all criteria for sitting for the examination as stipulated by the department and the University (cf Continuous Assessments, Log Book records and Case write-ups).
5. Trainees who run foul of the above conditions may be barred from sitting for the examination; this forfeiture is counted as one (1) attempt.
6. Trainees may sit for the examination for a maximum of 4 attempts. 7. If still unsuccessful after 4 attempts, the trainee may apply to sit for a 5th
attempt; however, sitting for the examination a 5th time is not automatic and depends on the support of the department which primarily bases its decision on whether the trainee has shown progressive improvement in the previous examination results. Failure in the examination after the 5th attempt eliminates the trainee from the course.
8. The trainee may only proceed to the 2nd year of the course when he/she has passed the Part I examination and has completed the 1st year of the course.
1.6.2 PART II
1. The Part II examination is a conjoint examination between UKM, UM, USM, IIUM, UNIMAS,UPM,MOA and AM under the auspices of the Conjoint Board of Orthopaedics.
2. It is held every 6 months (May and November). 3. Trainees must have passed the Part I examination or its equivalent and must
have gone through the 4-year in-service training before being eligible to sit for the Part II examination.
4. Trainees must register for the examination, pay all required fees and meet all criteria for sitting for the examination as stipulated by the department and the University (cf Continuous Assessments, Log Book, Case Book and Dissertation).
5. Trainees who run foul of the above conditions may be barred from sitting for the examination; this forfeiture is counted as one (1) attempt.
6. There is no limit in the number of attempts in the part 2 examination within the 7-year training period.
13
2. PART I EXAMINATION
Commencing November 2014:
2.1 SYLLABUS FOR CBO PART I
2.1.1 APPLIED ANATOMY
i. Upper Limb
i. Bones, joints, muscles, vessels, lymphatic drainage and nerves
ii. Hand, forearm, arm, shoulder, pectoral girdle, breast, axillary and scapular region
iii. The anatomy of extensile exposures of the bones and joints of the upper limb
iv. The anatomy related to surgical management of breast carcinoma
v. The anatomy of brachial plexus injuries and its clinical signs
vi. The anatomy of the rotator cuff injuries
vii. The anatomy of entrapment neuropathies
ii. Lower Limb
i. Bones, joints, muscles, vessels, lymphatic drainage and nerves
ii. Foot, lower leg, thigh, gluteal region
iii. The anatomy of surgical approaches to the hip joint, knee joint and ankle joint
iv. The anatomy of vascular anastomosis of the lower limb for trauma and atherosclerosis
v. The anatomy of the lower limb as it relates to external fixation
vi. The anatomy of the knee injuries
iii. Head and Neck
i. Scalp, skull, cerebrum, cerebellum, mid brain, brain stem
ii. Face, eyes, ears, nose
iii. Mouth, pharynx, larynx
iv. Neck
v. Bones, joints, muscles, vessels, nerves and cranial nerves. vi. Anatomy related to skull fractures and complications
vii. Anatomy of cerebral circulation
viii. Anatomy of facial palsies
ix. Anatomy of ocular palsies
x. Anatomy of facial fractures and complications
xi. Anatomy of the larynx as it related to deglutition, respiration, and intubations
xii. Anatomy of thyroidectomy and complications
xiii. Anatomy of the movement of the neck
xiv. Anatomy as it relates to cervical spine injuries
xv. Anatomy of lymphatic drainage of head and neck malignancies 14

iv. Thorax
i. Chest wall, ribs, diaphragm
ii. Airways and lungs
iii. Heart and great vessels
iv. Mediastinum
v. Anatomy of thoracic surgical approaches
vi. Anatomy of congenital malformations
vii. The circulatory anatomy of the heart and lungs related to
bypass surgery
v. Abdomen
i. Abdominal wall and peritoneum
ii. Liver, spleen, intestines, pancreas, kidneys and ureters
iii. Aorta and vessels
iv. Anatomy of inguinal ligament and hernia repair v. Anatomy of common surgical procedures: cholecystectomy,
gastrectomy, appendicectomy, colectomy, bowel resection, nephrectomy.
vi. Anatomy of congenital malformations
vii. Abdominal vascular anatomy
vi. Pelvis
i. Bones, joints, muscle
nerves, vessels
ii. Urinary and reproductive organs
iii. Congenital malformations
iv. Anatomy of urolithiasis and
surgical treatment
vii. Spine
i. Vertebral column
ii. Spinal cord and nerves
iii. Anatomy of traumatic paraplegia
viii. Tissues and Structures
i. Skin, mucous membrane, subcutaneous tissue, deep fascia
ii. Muscles, tendons, ligaments, joints, cartilage
iii. Peripheral nerves, vessels and lymphatic
iv. Anatomy of common pedicle and free flaps
v. Anatomy of surgical skin incisions
15

ix. Surface Anatomy
i. Basic Embryology of limbs and spine Notochord, mesoderm,
endoderm, limb formation, totipontential, pluripotential ii. Comparative Anatomy of the Child - Epiphyseal plates,
proportions, growth, osteology of the child
x. Anatomy of Regional Anaesthesia
i. Ankle block, digital block, wrist block, flexor tendon block,
axillary block, femoral n. block
2.1.2 PHYSIOLOGY
Greater emphasis is placed on understanding of pathophysiology and treatment of common surgical problems related to organs failure or dysfunction.
i. Cellular Physiology
i. Cellular function and signalling
ii. The genome and its expression
iii. Basic actions of cellular poisons
iv. Cell division
ii. Body Fluid and Electrolytes Physiology
i. Distribution and control of body fluid
ii. Osmotic pressure
iii. Oncotic pressure
iv. Fluid and electrolyte management in the postoperative period
v. Fluid resuscitation of the traumatised patient vi. Fluid resuscitation in the diabetic patient vii. Sodium homeostasis
viii. Potassium homeostasis
iii. Acid Base Balance
i. Buffer systems
ii. Respiratory regulation iii. Renal regulation iv. Interpretation of arterial blood gases
v. Changes with pathology: Vomiting, renal failure, hepatic failure, respiratory failure
vi. Changes during surgery and trauma
16
iv. Respiratory System
i. Normal respiratory mechanism
ii. Lung volumes
iii. Functional residual capacity
iv. Compliances
v. Changes in gaseous composition
vi. Gaseous exchanges
vii. Oxygen delivery and transport viii. Carbon dioxide transport ix. Central/peripheral control of respiration
x. Cyanosis
xi. Hypoxia and hypoxemia
xii. Changes during anaesthesia
xiii. Surgery to the chest wall xiv. Pneumathorax
xv. Flail chest xvi. Respiratory failure
xvii. Adult respiratory distress syndrome (ARDS) xviii. Post operative hypoxemia
v. Cardiovascular System
i. Mechanism of circulation: Cardiac circle and output
ii. Determinants of myocardial performance
iii. Central venous pressure and Pulmonary artery wedge pressure
iv. Venous return
v. Valsava manoeuvre
vi. Control of blood pressure
vii. Shock
viii. Coronary blood flow
ix. Cerebral blood flow
x. Hepatic blood flow
xi. Renal blood flow
xii. Pulmonary circulation
xiii. Autoregulation
xiv. Myocardial action potentials
xv. Myocardial muscle properties
xvi. Myocardial failure
vi. Renal System
i. Renal functions
ii. Counter current multiplier system
iii. Glomerular filtration rate
iv. Creatinine and Renal clearance
v. Excretion of bicarbonate 17

vi. Excretion of urea vii. Endocrines functions of kidney viii. Chronic renal failure
vii. Blood and Hematologic System
i. Composition of blood and role of its components
ii. Coagulation pathway
iii. Bleeding
iv. Anaemia
v. Compatibility testing of blood
vi. The immune system
vii. Abnormal conditions of blood-haemophilia, sickle cell, Caisson disease
viii. Alimentary System
i. Swallowing
ii. Digestion
iii. Gastric secretion
iv. Bile
v. Control of digestion
vi. Small bowel function
vii. Large bowel function
viii. Functions of liver
ix. Carbohydrate metabolism
x. Fat metabolism
xi. Protein metabolism
xii. Iron metabolism
xiii. Vitamins
xiv. Malabsorption syndrome
xv. Post gastrectomy syndrome
ix. Nervous System
i. Resting membrane potential ii. Propagation of action potential iii. Blood brain barrier iv. Effect of anaesthesia agents
v. Pain and its management vi. Nerve repair vii. Autonomic nervous system
viii. Glasgow coma scale
ix. Brain stem death
x. Changes with intracranial pressure
18

x. Muscle and Neuromuscular Junctions
i. Skeletal and smooth muscle
ii. Physiology of neuromuscular transmission
iii. Muscle contraction
iv. Muscle spindles
xi. Endocrine System
i. Hormones
ii. Insulin and regulation of blood glucose level
iii. Thyroid hormones and its regulation
iv. Calcium metabolism v. Adrenal gland
vi. Hypothalamic- pituitary- adrenal axis
xii. Miscellaneous Topics
i. Metabolism response to trauma
ii. Nutrition of surgical patients
iii. Heat Exhaustion
2.1.3 PATHOLOGY The Normal Cell
i. Cellular Injury and Tissue Response to Injury
i. Acute and chronic inflammation ii. Healing and repair
ii. Fluid and Hemodynamic Derangements
i. Haemorrhage, haemostasis, and thromboembolism
ii. Oedema, hyperaemia and congestion
iii. Shock
iv. Infarction Embolism
iii. Immune System
i. The immune system
ii. Hypersensitivity reactions
iii. Transplant rejections
iv. Autoimmune diseases
v. Immunodeficiency disorders
vi. Amyloidosis
19

iv. Infections
i. Infectious agents
ii. Host barriers to infectious agents
iii. Pathogenesis of infectious diseases
iv. Diagnosis of infectious diseases
v. Neoplasia
i. Nomenclature
ii. Carcinogenesis and Molecular Basis of Cancer
iii. Characteristics of benign and malignant tumours iv. Biology of tumour growth
v. Clinical features and laboratory diagnosis of cancer
vi. Genetic and Pediatric Disorders
i. Mutations
ii. Mendelian disorders
iii. Cytogenetic disorders
iv. Congenital anomalies
v. Paediatric disorders
vi. Diagnosis of genetic disorders
vii. Environmental Diseases
i. Environmental Pollution ii. Tobacco iii. Chemical agents iv. Physical agents v. Ionizing radiation vi. Nutritional disorders
The following topics are common conditions encountered in clinical practice and
students are encouraged to read them for further understanding of pathological
disorders.
viii. Respiratory System
i. Obstructive and restrictive lung diseases
ii. Pulmonary infections
iii. Tumours
iv. Disorders of the upper respiratory tract
20

ix. Cardiovascular System
i. Ischaemic heart disease
ii. Heart failure
iii. Valvular heart diseases
iv. Congenital heart diseases
x. Vascular Disorders
i. Normal vessels and response to injury
ii. Atherosclerosis
iii. Hypertensive
iv. Aneurysms and dissection
v. Vasculitis
vi. Venous diseases
xi. Gastrointestinal Disorders
i. Disorders of the oesophagus
ii. Gastritis, ulcers and tumours iii. Tumours of the small and large intestines
iv. Disease of the appendix
xii. Liver and Biliary Tract
i. Jaundice and hepatitis
ii. Cirrhosis and liver failure
iii. Gallbladder diseases
xiii. Pancreas
i. Exocrine pancreatitis
ii. Endocrine pancreas
xiv. Renal System
i. Manifestations of renal diseases
ii. Glomerular disorders
iii. Diseases of the tubules and the interstitium
iv. Acute and chronic renal failure
v. Hypertensive renal disease
vi. Urinary outflow obstruction
xv. Musculoskeletal System
i. Fractures
ii. Bone infections
iii. Bone tumours
iv. Metabolic bone disorders
v. Diseases of the joints
vi. Soft tissue tumours
vii. Myopathies
21

xvi. Haematopoietic System
i. Red cell disorders
ii. White cell disorders
iii. Bleeding disorders
xvii. Endocrine System
i. Pituitary
ii. Thyroid
iii. Parathyroid
iv. Pancreas
v. Adrenal
xviii. The Breast
i. Tumours of the breast
ii. The male breast
iii. Fibrocystic changes
xix. The Male Genitalia
i. Scrotum, testis and epidydimia
ii. Prostatic disorders
iii. Sexually transmitted diseases
xx. Diseases of Ageing
2.1.4 PRINCIPLES OF SURGERY Students are expected to understand basic processes and their applications in surgery.
i. Perioperative Management
i. Metabolic and Nutritional Support ii. Fluid & electrolyte management iii. Nutrition in the surgical patient iv. General surgical complications v. Respiratory failure vi. Acute renal failure vii. Systemic inflammatory response syndrome (SIRS) viii. Multiple organ dysfunction syndrome (MODS)
22

ii. Surgical Techniques and Technology
i. Surgical Wounds
ii. Classification of surgical wounds
iii. Principles of wound management iv. Pathophysiology of wound healing
v. Principles of safe surgery
vi. Incisions and wound closure
vii. Diathermy, laser, principles of cryosurgery
viii. Sutures and ligature materials
ix. Basic surgical instruments
x. Tourniquets in the Operating Theatre
xi. Indications for tourniquet use
xii. Tourniquet application
xiii. Effects and complications of tourniquets
iii. Good Clinical Practice and Legal Issues
i. Evidence Based Surgical Practice
ii. Decision making in surgery
iii. Statistics
iv. Principles of research and clinical trials
v. Management Aspects of Surgical Practice
vi. Clinical audit
vii. Clinical governance
viii. Medico-legal aspects of surgery
iv. Clinical Microbiology
i. Surgical Microbiology
ii. Sources of surgical infection
iii. Principles of asepsis and antisepsis
iv. Modern Antibiotic Usage
v. Commonly used antibiotics
vi. Preoperative prophylaxis
vii. Antibiotic resistance
viii. Surgery in Hepatitis and HIV Carriers
ix. Blood-borne viruses
x. Universal precautions
xi. Surgical precautions
xii. Immunization
23

v. Emergency Medicine and Trauma
i. Pathophysiology of Trauma
ii. Shock and cardiovascular physiology iii. Metabolic response to injury iv. Adult respiratory distress syndrome (ARDS) v. Traumatic Oedema and Compartment Syndrome
vi. Diagnosis and treatment of Environmental Emergencies
vii. Hypothermia
viii. Heat exhaustion
ix. Management of a radiation incident
vi. Principles of Oncology
i. Epidemiology of Common Cancers ii. Common cancers iii. Screening Programmes iv. Clinico-Pathological Staging of Cancer v. Principles of Cancer Treatment vi. The role of surgery – block dissections vii. Radiotherapy viii. Chemotherapy ix. Hormone therapy x. Immunotherapy xi. Palliative Care xii. The palliative care team xiii. Pain and other symptoms
2.1.5 BIOMATERIALS & BIOMECHANICS
2.1.5.1 BIOMATERIALS
Definition: Characteristics: Biocompatibility, Bioinert
i. Types of Material
i. Metal ii. Stainless Steel iii. Cobalt Chrome Alloys iv. Titanium v. Non-metal vi. Polymers such as polyethylene, hydroxylapatite vii. Ceramics such as alumina viii. Composites
24
ii. Mechanism Of Material Failure
i. Corrosion
ii. Fatigue
iii. Wear
iii. Material Properties
i. Load and Forces
ii. Stress and Strain
iii. Stress and Strain Curves (Yield point, Ultimate strength, Breaking point, Plastic deformation and Young’s Modulus)
iv. Strength
v. Elasticity
vi. Plasticity
vii. Ductility
viii. Toughness
ix. Brittleness
x. Viscoelastic
2.1.5.2 BIOMECHANICS
i. Kinetic And Kinematic
i. Newton’s Law: First, Second And Third ii. Forces And Moment (Torque) iii. Work And Energy iv. Friction v. Biomechanics Of Musculoskeletal Tissues vi. Bone vii. Mechanical Properties viii. Mechanism Of Fractures ix. Strain Theory On Fracture Healing x. Ligament And Tendons xi. Mechanical Properties xii. Mechanical Properties Of Synthetic Replacements xiii. Natural And Artificla Joints xiv. Hip Biomechanics xv. Knee Biomechanics xvi. Spine Biomechanics xvii. Biomechanics Of Fracture Fixation xviii. Tissue Response To Implants xix. Properties Of Screws, Plates, Nail xx. Plates Vs Nail (In Terms Of Rigidity And Function) xxi. Concept Of Load Sharing And Sparing xxii. Factors Of Internal Fixation Failure xxiii. External Fixation xxiv. Factors Enhancing Stability xxv. Hip Biomechanics
25
xxvi. An understanding of the lever arms, muscles and body weight
forces that produce the joint reaction force in both normal and
abnormal hips
xxvii. An understanding of the application of these principles to
replacement arthroplasty
xxviii. Knowledge of the biocompatibility and mechanical properties of
materials in common use in total hip arthroplasty
xxix. Knee Biomechanics
xxx. The mechanics of the patello-femoral mechanism
xxxi. Axis of Knee Joints
xxxii. The medial and lateral weight-bearing joints and their inter-
relationship
xxxiii. The cruciate and collateral ligaments and other ligamentous and
muscular supports
xxxiv. Menisci and articular cartilage
xxxv. Spine Biomechanics
xxxvi. Basic knowledge of the biomechanics of the cervical and
lumbosacral spines
xxxvii. An understanding of the biomechanics of spinal instability as
applied to trauma, tumour, infection and spondylolysis/listhesis
xxxviii. A knowledge of the basic mechanics of spinal instrumentation
2.2 EXAMINATION STRUCTURE and FORMAT
CBO Part I
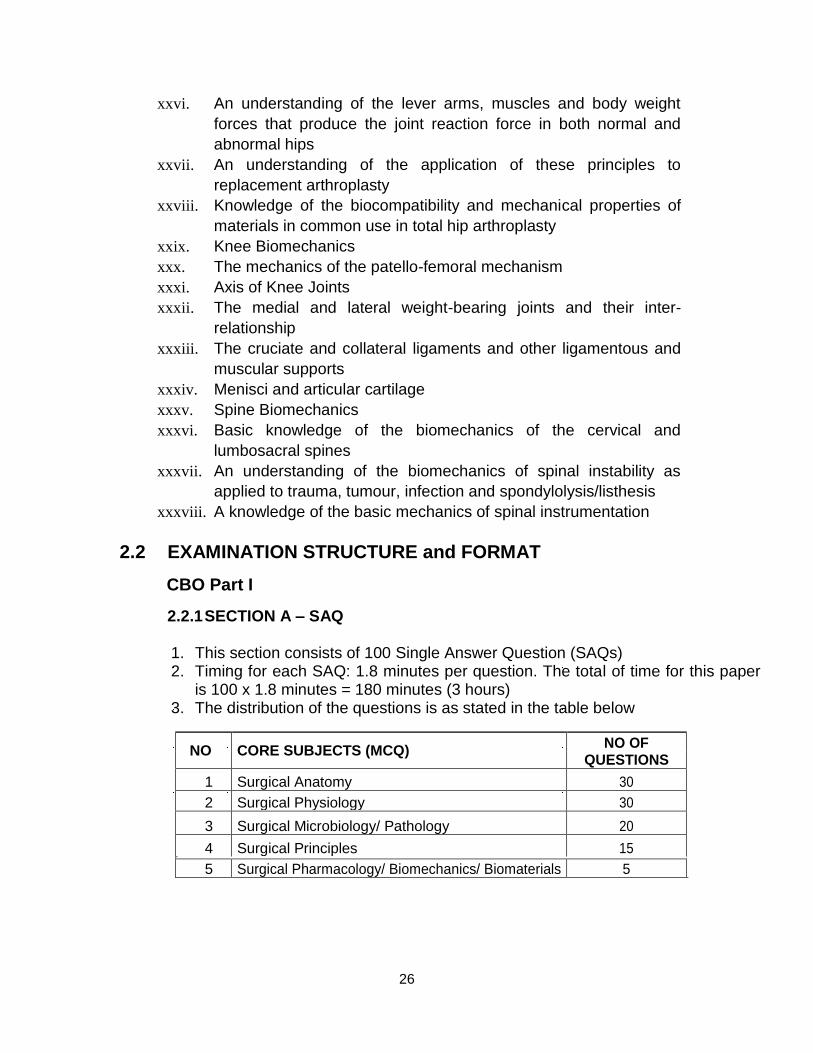
2.2.1 SECTION A – SAQ
1. This section consists of 100 Single Answer Question (SAQs) 2. Timing for each SAQ: 1.8 minutes per question. The total of time for this paper
is 100 x 1.8 minutes = 180 minutes (3 hours) 3. The distribution of the questions is as stated in the table below
NO CORE SUBJECTS (MCQ) NO OF
QUESTIONS
1 Surgical Anatomy 30
2 Surgical Physiology 30
3 Surgical Microbiology/ Pathology 20
4 Surgical Principles 15
5 Surgical Pharmacology/ Biomechanics/ Biomaterials 5
26

4. The total marks for Section A examination is 100 marks. The
passing mark for this section is 50 marks or 50% 5. Only those trainees who passed Section A will be allowed to proceed to
Section B.
2.2.2 SECTION B - OSCE AND VIVA VOCES
2.2.2.1 OSCE
1. OSCE examination consists of 10 OSCE stations. 2. The OSCE examination will include the following assessment of the
basic daily clinical surgical skills: i. Basic surgical skills e.g. suturing, dressing, aseptic technique
etc. ii. Three dimensional spatial orientation iii. Instrument identification iv. Communication skills
3. The total marks for OSCE examination is 100 marks. The passing mark for this section will be 70 marks or 70%.
2.2.2.2 VIVA Examination
1. This section consists of 3 viva voces i.e. Table 1 - Anatomy, Table 2
Physiology and Table 3 – Pathology, Principle of Surgery,
Biomechanics and Biomaterials 2. The total marks for all the three viva voces is 300 marks (100 marks
each). 3. The overall passing marks for the three viva voces are 150 marks
or 50%.
Special Rules: 40 or less in any section is unredeemable fail
41-49 in one section is a redeemable fail 41-49
in 2 sections is an unredeemable fail
The successful trainee will need to pass all three components
(i.e. SAQ, OSCE and Viva Voce) in order to pass the examination.
2.3 RECOMMENDED TEXTS and REFERENCES
1. Chummy S Sinnatamby. Last's Anatomy: Regional and Applied. 11th
Edition. Churchill Livingstone Elselvier. 2. Susan Standring. Gray's anatomy: the anatomical basis of clinical
practice. 39th Edition. Churchill Livingstone Elselvier. 3. Frank H Netter. Netter's Concise Atlas of Orthopaedic Anatomy. Sounders. 4. Richard S Snell. Clinical Anatomy
27

5. Barret KE, Barman SM, Boitano S, Brooks HL, Ganong’s Review of
Medical Physiology 23rd Edition. McGraw-Hill, 2009. 6. Guyton AC, Hall JE. Textbook of Medical Physiology 12th Edition. Saunders. 2011 7. Vinay Kumar, Abul K Abbas, Nelson Fauto, Mitchell. Robbins Basic Pathology. 8. Vinay Kumar, Abul K Abbas, Nelson Fauto, Jon Aster. 2010. Robbins &
Cotran Pathology Basic of Disease. 8th Edition. 9. Andrew Kingsnorth, Aljafri Majid. 2001. Principles of Surgical Practice.
Greenwich Medical Media Limited. 10. RM Kirk. Basic Surgical Techniques. 6th Edition. CL Elsevier. 11. Robert Steele, Alfred Cuschieri. Essential Surgical Practice: Higher Surgical
Training in General Practice. 4th Edition. Hodder Arnold Publication. 12. F. Brunicardi, Dana Andersen. 2010. Schwartz’s Principles of Surgery. 9th Edition.
13. Mark D Miller. Review of Orthopaedics. Saunders Elsevier. 14. Orthoteers Orthopaedic Resource (http:www.orthoteers.org) 15. Mark D Miller, Jennifer Hart, John MacKnight. Essential Orthopaedics.
Saunders Elsevier. 16. David J Warwick, Louis Solomon, Selvadurai Nayagam. Apley’s
system of orthopaedic and fractures. 8th Edition
3. PART II EXAMINATION
3.1 SYLLABUS FOR PART II 3.1.1 ORTHOPAEDICS AND TRAUMATOLOGY
Students are expected to gain clinical experiences in surgery of a wide variety
of orthopaedics and trauma cases commonly encountered in Malaysia. For
monitoring purposes, these experiences are recorded in the logbook
i. General Principles
i. Principles of fractures and dislocation
ii. Principles of open fractures treatment
iii. Multilply injured patients
iv. Principles of internal and external fixations
v. Healing of musculoskeletal tissues under different osteosynthesis
techniques
vi. Pathological fractures and stress fractures
vii. Complications of fracture and dislocation
ii. Upper Extremity
i. Fractures and dislocations of the shoulder joint ii. Injuries of the sternoclavicular joint iii. Injuries of the acromioclavicular joint
28
iv. Fractures of the clavicle
v. Fractures of the scapula
vi. Fractures of the humerus
vii. Fractures and dislocations of the elbow
viii. Fractures of the radius and ulna
ix. Fractures and dislocations of the wrist
x. Fractures and dislocations of the hand
iii. Spine
i. Fractures and dislocations of the cervical spine
ii. Fracture and dislocations of the thoracic spine
iii. Fractures and dislocations of the thoraco-lumbar spine
iv. Fractures of the sacrum
iv. Lower Extremity
i. Fractures of the pelvic ring and acetabulum
ii. Fractures and dislocations of the hip
iii. Fractures of the femur (proximal, diaphysis and distal)
iv. Peri- and intra-articular fractures of the knee
v. Knee dislocations
vi. Fractures and dislocations of the patella
vii. Fractures of the tibia and fibula
viii. Fractures and dislocations of the ankle
ix. Fractures and dislocations of the foot y.
v. Paediatric Orthopaedics
i. Embryology
ii. Chromosomal and teratologic disorders
iii. Birth injuries
iv. Cerebral palsy
v. Neuromuscular disorders
vi. Skeletal dysplasia
vii. Metabolic bone diseases
viii. Haemopoietic diseases
ix. Paediatric spine diseases and trauma
x. Hip diseases and trauma
xi. Knee disorders and trauma
xii. Foot deformities and trauma
xiii. Hand deformities and trauma
xiv. Other deformities and trauma of the upper limbs
vi. General Orthopaedics
i. Orthopaedic infections
29

ii. Osteoarthritis
iii. Osteonecrosis
iv. Osteoporosis and other metabolic bone diseases
v. Biomechanics related to bone, joint, tendon and ligament
vii. Adult Reconstruction Surgery/Arthroplasty
i. Shoulder
ii. Elbow
iii. Wrist and hand
iv. Hip
v. Knee
vi. Ankle
vii. Foot
viii. Principles of Illizarov /Taylor-Spatial external fixators in LLRS
viii. Sports Medicine and Arthroscopic Surgery
i. Shoulder and elbow
ii. Wrist and hand
iii. Hip
iv. Knee
v. Foot and ankle ix. Foot and Ankle
x. Hand and Reconstructive Microsurgery
xi. Spinal Surgery
xii. Musculoskeletal Oncology
xiii. Orthopaedic Rehabilitation
xiv. Imaging techniques in orthopaedics
i. General ii. Bone Scans and PET scans
iii. CT Scans including 3D Reconstruction images
iv. MRI v. Ultrasound
vi. Interventional radiology
vii. Nuclear medicine
30

3.2 EXAMINATION STRUCTURE and FORMAT
The CBO Part II examination consists of 3 Sections:
1. Section I – Theory 2. Section II – Clinicals 3. Section III – Viva and OSCE.
Trainees MUST PASS ALL THREE (3) Sections to pass the examination.
SECTION SECTION SECTION I II III
(THEORY) (VIVA and OSCE) (CLINICALS)
1. PAPER I 1. VIVA I 1. LONG CASES [from May - 3 long essays + 1 short - Principles of Orthopaedic 2015]
notes Surgery - 2 patients per trainee - 2 hrs - 30 min - examiners sit in
- 100 marks [50%] - 50 marks attendance throughout
2. PAPER II 2. VIVA II - 15 min clerking &
physical - 3 long essays + 1 short - Operative Orthopaedics examination
notes - 30 min - 15 min discussion
- 2 hrs - 50 marks (30 min per case)
- 100 marks [50%] 3. OSCE (VIVA III) * - 100 marks
3. MCQs 2. SHORT CASES
- 20 questions
- 60 questions (single-answer - 2 hrs - 3 patients per trainee type) - 200 marks - 10 min each patient
- 2 hrs (TOTAL 30 min) - 100 marks - 100 marks total
TOTAL 200 marks TOTAL 300 marks TOTAL 200 marks
PASS MARK 100/200 PASS MARK 150/300 ** PASS MARK 100/200
* O S C E (Objective Structured Clinical Examination) is in the form of a Powerpoint
Slide Presentation consisting of questions under the following categories:
i. Radiology ii. Pathology iii. Implants and Biomechanics iv. Orthotics, Prosthetics and Rehabilitation v. Clinical
** Special requirement for the Clinical Component:
In both the Long Case and Short Cases, the trainee must obtain a minimum of 40% i.e. if a trainee obtains less than 40% in either the Long or Short cases, he fails the entire examination (unredeemable fail).
31

VIVA VOCE
Viva I: Principles of Orthopaedic Surgery Viva II: Operative Orthopaedics
NOTE: Only those trainees who pass the Theory Section are allowed to
proceed with the Clinicals and Viva voce examination. From May 2015, there will be a change in the format of the long case
examination. Each trainee will be tested on 2 long cases of 30 mins each
i.e. 15 mins for clerking and examination and 15 mins for discussion
3.3 RECOMMENDED TEXTS and REFERENCES (Please refer to the most current issue of the references listed)
1. Operative Hand Surgery Volumes I and II. Edited by Green DP. 5th Ed,
Churchill Livingston, London, 2007. 2. Campbell’s Operative Orthopaedics Volumes I, II, III, IV, V, VI. Edited by
Canale ST, Beaty JH. 11th Ed, Mosby-Elsevier, Philadelphia, 2008. 3. AO Principles of Fractures Management Vol. I and Vol. II. Reudi TP, Murphy
WM. Stuggard, New York, Thieme, 2007. 4. AO Manual of Fracture Management: Hand and Wrist. Edited by Jupiter
JB, Ring DC. 1st Ed. Thieme, Sluggard-New York, 2005. 5. Rockwood and Green’s Fractures in Adults. Edited by Bushels RW, Heckman JD
and Court-Brown C. 6th
Ed. Lippincott, Williams and Wilkins, Philadelphia, 2006. 6. Rockwood and Green’s Fractures in Children. Edited by Rockwood CD and
Wilkins. 6th Ed. Lippincott, William and Wilkins, Philadelphia, 2006. 7. Skeletal Trauma : Basic Sciences, Management and Reconstruction
Volumes I and II. Edited by Browner B, Jupiter J, Levine A, Trafton P. 4th Ed, Saunders-Elsevier, Philadelphia, 2009.
8. Skeletal Trauma : In Children. Edited by Green NE, Kwiatkowski MF.
4th Ed, Saunders-Elsevier, Philadelphia, 2009. 9. Orthopaedics Surgical Approaches. Edited by Miller MD, Chakra AB, Hurwitz S,
Mishawka WM, Sheen FH. 1st Ed. Lippincott, Saunders-Elsevier, Philadelphia, 2008.
10. Tachdjian’s Paediatric Orthopaedic Volumes I, II and III. Edited by Herring J.
4th Ed, Saunders, Philadelphia 2008.
32

ATTACHMENT I
TRAINEE ASSESSMENT FORM
DEPARTMENT OF ORTHOPAEDIC AND TRAUMATOLOGY FAKULTI PERUBATAN
UNIVERSITI KEBANGSAAN MALAYSIA
TRAINEE ASSESSMENT FORM TRAINEE : TRAINEE YEAR : 1 2 3 4 SPECIALTY / CONSULTANT : HOSPITAL : ATTACHMENT ATTACHMENT START DATE : END DATE :
1. This is an official confidential document when completed. The original is the
property of the Department of Orthopaedic and Traumatology (DOT). Before
the end of each semester (i.e. before 31 May and 30 Nov), the trainee shall
submit this form to the consultant for completion.
2. On completion of the form signed by both the trainer and trainee, the consultant
in charge will send the completed from to the DOT, Fakulti Perubatan, UKM.
3. Trainees shall not start their new posting without the completion and
submission of this form to DOT.
TRAINER SIGNATURE: DATE :
AND NAME IN BLOCK CAPITALS
TRAINEE SIGNATURE : DATE :
Trainees who disagree with the contents of this report may appeal to the Head, Department of Orthopaedic and
Traumatology, Fakulti Perubatan, Universiti Kebangsaan Malaysia, Cheras, Kuala Lumpur
33

1 2 3 4 5
POOR DEFICIENT SATISFACTORY GOOD EXCELLENT
CLINICAL SKILL
KNOWLEDGE
TRAINEE ACTIVITIES
ATTITUDE
SOCIAL INTERACTION
TRAINER’S COMMENTS : Please summarise the trainee’s character and overall performance drawing
attention to any outstanding features or alternatively ways in which
the trainee failed to meet your expectations during this rotation. Do
you foresee any specific difficulties / gaps in training the trainee
will have in completing his / her training? 34

ATTACHMENT I
TRAINEE ASSESSMENT FORM
DEPARTMENT OF ORTHOPAEDIC AND TRAUMATOLOGY FAKULTI PERUBATAN
UNIVERSITI KEBANGSAAN MALAYSIA
TRAINEE ASSESSMENT FORM TRAINEE : TRAINEE YEAR : 3 4 POSTING: CONSULTANT : ATTACHMENT ATTACHMENT START DATE : END DATE :
1. This is an official confidential document when completed. The original is the
property of the Department of Orthopaedic and Traumatology (DOT) at the end
of the rotation, the trainee must submit this form to the consultant for completion.
2. On completion of the form signed by both the trainer and trainee, the consultant
in charge will send the completed from to the DOT, Fakulti Perubatan, UKM.
3. Trainees shall not start their new posting without the completion and
submission of this form to DOT.
TRAINEE SIGNATURE : DATE :
Trainees who disagree with the contents of this report may appeal to the Head, Department of Orthopaedic and
Traumatology, Fakulti Perubatan, Universiti Kebangsaan Malaysia, Cheras, Kuala Lumpur
35
TRAINER SIGNATURE: DATE:
AND NAME IN BLOCK CAPITALS
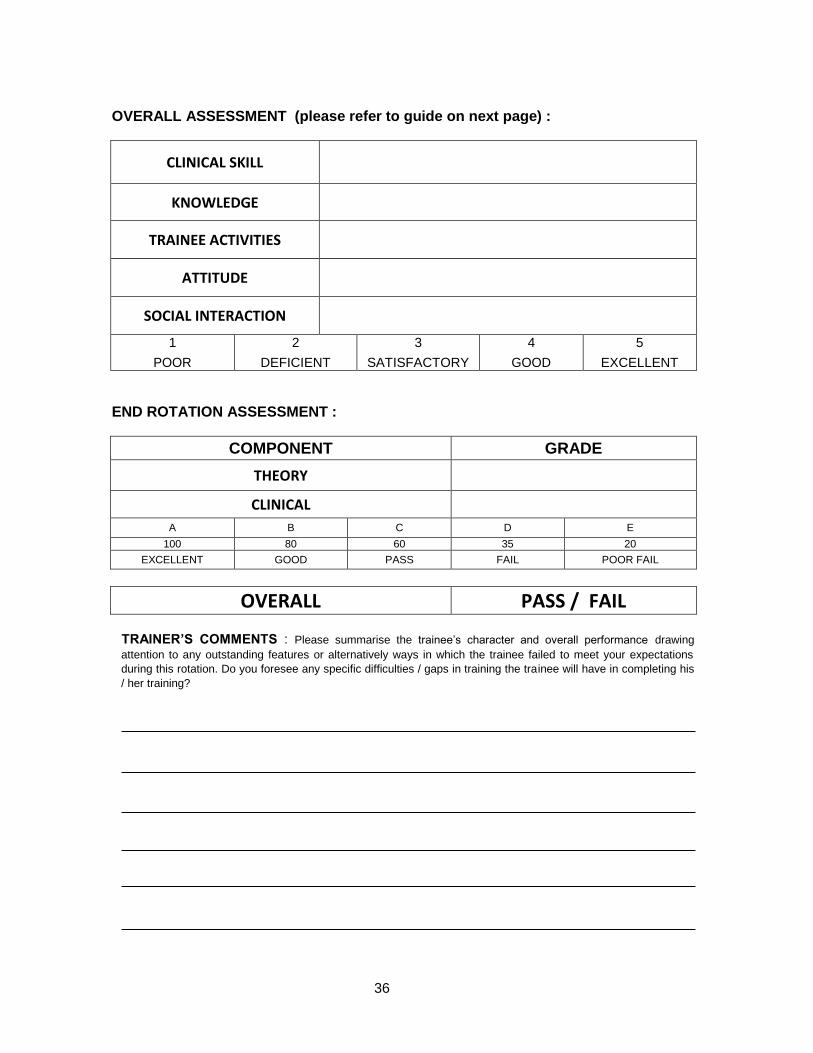
OVERALL ASSESSMENT (please refer to guide on next page) :
CLINICAL SKILL
KNOWLEDGE
TRAINEE ACTIVITIES
ATTITUDE
SOCIAL INTERACTION
1 2 3 4 5
POOR DEFICIENT SATISFACTORY GOOD EXCELLENT
END ROTATION ASSESSMENT :
COMPONENT GRADE
THEORY
CLINICAL
A B C D E
100 80 60 35 20
EXCELLENT GOOD PASS FAIL POOR FAIL
OVERALL PASS / FAIL
TRAINER’S COMMENTS : Please summarise the trainee’s character and overall performance drawing
attention to any outstanding features or alternatively ways in which the trainee failed to meet your expectations
during this rotation. Do you foresee any specific difficulties / gaps in training the trainee will have in completing his
/ her training?
36

ATTACHMENT I
TRAINEE ASSESSMENT FORM
UKM ORTHOPAEDIC DEPARTMENT
TRAINEE PEER-REVIEW FORM
The aim of this peer review form is to assess the professional behavior and attitude of
the trainees in Year 1,2 and 3 by the Year 4 trainees. Attendance at teaching sessions,
working with team members and time management will be assessed as follows:
A. Name of trainee/year of training :
B. Period of review (date) :
C. Subspecialty team :
Poor Fair Good Very Good Excellent
Attendance
Teamwork
Punctuality
Name of PGY4 Reviewer Name of Head of Unit
Signature Signature
Date Date
Heads of units will give feedback to their trainees in areas of concern
37

GUIDE
A. CLINICAL SKILLS 1 2 3 4 5 Poor Deficient Satisfactory Good Excellent
History taking Incomplete, Poorly recorded Complete, systematic Precise, detail, can spot rarity
Physical exam Lacks basic skills. Elicit correct signs. Recognizes most significant Thorough, accurate. Know and elicits specialist findings signs.
Investigations Inappropriate, random, Appropriate. Able to interpret results Appropriate to D diagnosis. Excellent at Inability to interpret tests. interpretation
Diagnosis Fails to interpret and synthesis symptoms, Competent clinician. Orderly approach to D Outstanding diagnostician. Excellent clinical signs and investigations diagnosis memory
Judgement Unreliable. Fails to take appropriate action. Reliable. Competent. Asks for advice Outstanding clinician who is aware of his/her Under or over reacts to emergencies appropriately limits
Operative skill Clumsy, rough with tissues. Poor surgical Competent. Good technique. Master technician.
technique.
After care Uninterested. Conscientious. Excellent on wards. Notices problems early. Fails to notice complications and act Aware of complications. Reliable in outpatients Outstanding in follow up outpatients. appropriately
B. KNOWLEDGE 1 2 3 4 5
Poor Deficient Satisfactory Good Excellent Basic Science Uninterested, does not read. Fails to apply Adequate knowledge and relates this Outstanding knowledge and understanding of the
basic science knowledge to clinical problems satisfactorily to patients care basic science. Widely read.
Clinical Poorly read. Lacks knowledge to constructs a Satisfactory knowledge. May fail to spot rarity Outstanding knowledge. Can be relied on to spot D diagnosis. Fails to learn from experience but learns from experience the rarity. Widely read.
C. TRAINEE ACTIVITIES 1 2 3 4 5 Poor Deficient Satisfactory Good Excellent
Teaching Uninterested in teaching. Contributes minimal Competent and conscientious in teaching Excellent enthusiastic teacher. Can inspire in educating junior trainees. others
Lecturing style Avoids if possible. Poor style, poorly delivered, Reasonably delivered. Competent but lacking Excellently delivered. Dynamic logical and clear. boring spark Can hold an audience
Case presentation Poor in history, signs, diagnosis and discussion Competent. History and signs. Good deduction Excellent presentation and discussion Presentations No interest. Does it badly. Fails to get across a Keen in presentations Well illustrated and well Fully researched. Original ideas. Answers
message delivered questions lucidly
Publications No interest. Devoid of ideas. Poor English Keen, tries hard but lacking originality. An excellent CV. Many original ideas which are Reasonable English translated into published articles.
Research ability and Has Neither inclination or ideas. Unable to Keen but needs considerable direction. Flair for original research with ability to carry it audit carry out directed projects. Not interested in Reasonable: statistic and research methods. our independently. Utilizes effective research
audit. methods.
D. ATTITUDE
Overall Grade 1 2 3 4 5 Poor Deficient Satisfactory Good Excellent
Reliability Unreliable. Forgets to do things to the possible Dependable. Needs no reminders. Highly conscientious. Anticipates problems detriment of patients. Conscientious in patient care
Self Motivation No inclination to organize work. Needs to be Organize without supervision. Looks for Constantly pro- active, always prepared to accept pushed constantly opportunities to learn additional opportunities to advance.
Leadership Very limited. Switches people off. Colleagues Competent but lacks inspiration. Gives clear Outstanding team leader with exceptional ability and other staff confused by his/her instructions. to motivate others.
instruction.
Administration Cannot be bothered. Always behind with Conscientious. Can be confidently left to deal Excellent at routine administration. He has a good letters and summaries. In a permanent with letters, summaries, waiting lists etc. grasp of hospital management and politics. muddle.
E. SOCIAL INTERACTION
Overall Grade 1 2 3 4 5 Poor Deficient Satisfactory Good Excellent
a. Colleagues Fails to get on with seniors, contemporaries or Good rapport. Willing to help in a crisis. Ever willing to help personally Able to defuse juniors. Undermine them. Refuse to help. Trusted, easy to work with team’s problems. Excellent colleagues
b. Patients Increases patients’ anxieties. Rude. Not Caring. Ally patients’ fears. Listens and Inspires confidence. Excellent rapport and wanted by patients. Poor listener and explains well. Trusted by patient communicator. Patients delighted to be looked communicator after by him / her
c. Other staff Treats them with disdain. Generates as Round and professional Approachable. Treats Inspires enthusiasm. Exceptional communication opposed to solving problems. Rude others with respect and is respected in return skills.
38

ATTACHMENT I THESIS PROGRESS REPORT
JABATAN ORTOPEDIK & TRAUMATOLOGI, FAKULTI PERUBATAN UNIVERSITI KEBANGSAAN MALAYSIA
39
Y
E
A
R
2
Comments by supervisor Signature
0-6 months
Title
Literature review
6-9 months Proposal preparation
and presentation
9-12 months Submission to ethical
committee
End of year Ethical committee ap-
proval

JABATAN ORTOPEDIK & TRAUMATOLOGI, FAKULTI PERUBATAN UNIVERSITI KEBANGSAAN MALAYSIA
40
Y
E
A
R
3
Comments by supervisor Signature
0-6 months
Data collection
6-12 months
Data collection
Manuscript preparation
End of year
Data collection
completion

JABATAN ORTOPEDIK & TRAUMATOLOGI, FAKULTI PERUBATAN UNIVERSITI KEBANGSAAN MALAYSIA
41
Y
E
A
R
4
Comments by supervisor Signature
0-3 months
Statistical analysis
3-6 months Manuscript preparation
End of year
Submission of
manuscript on 31st Dec

ATTACHMENT II
UNIVERSITI KEBANGSAAN MALAYSIA DOCTOR OF ORTHOPAEDICS and TRAUMATOLOGY (Dr. Ortho & Trauma), UKM
UNIVERSITI MALAYA MASTER OF ORTHOPAEDIC SURGERY, UM UNIVERSITI SAINS MALAYSIA MASTERS OF MEDICINE (ORTHOPAEDICS), USM INTERNATIONAL ISLAMIC UNIVERSITY OF MALAYSIA MASTERS OF SURGERY(ORTHOPAEDICS), IIUM UNIVERSITI PUTRA MALAYSIA MASTER OF SURGERY (ORTHOPAEDICS), UPM
CONJOINT BOARD ORTHOPAEDICS
LOG BOOK NAME : INSTITUTION : STUDENT NO. :
42

ATTACHMENT III
HIP
ARTHROPLASTY (HEMI)
Patient’s Name RN Date Remarks Observe Assisting Perform Outcome
ARTHROPLASTY (TOTAL)
Patient’s Name RN Date Remarks Observe Assisting Perform Outcome
MICELLANEOUS
Patient’s Name RN Date Remarks Observe Assisting Perform Outcome
ARTHROPLASTY (RESURFACING)
Patient’s Name RN Date Remarks Observe Assisting Perform Outcome
ARTHROPLASTY (REVISION)
Patient’s Name RN Date Remarks Observe Assisting Perform Outcome
ARTHROTOMY
Patient’s Name RN Date Remarks Observe Assisting Perform Outcome
EXTERNAL FIXATION
Patient’s Name RN Date Remarks Observe Assisting Perform Outcome
ARTHROCENTESIS
Patient’s Name RN Date Remarks Observe Assisting Perform Outcome
ARTHRODESIS
Patient’s Name RN Date Remarks Observe Assisting Perform Outcome
43
ATTACHMENT IV
MAHMOOD MERICAN AWARD
This is an annual award for the best original scientific or clinical paper submitted
by young trainees in orthopaedic surgery in Malaysia, and submitted for
presentation at the Annual Scientific meeting of the Malaysian Orthopaedic
Association (MOA). This award was initiated in 1997 to encourage a high
standard of research and scientific presentations among the young trainees. The prize A cash prize of RM1,000.00 donated by Dato' Dr Mahmood Merican. Regulations 1. The competition is open to all registered trainees currently working in
Malaysian hospitals. 2. The work may take the form of clinical trials, surveys, retrospective studies,
laboratory experiments or any other form of unpublished original work. 3. The bulk of the work which is submitted must be performed by the author
himself/herself even though he/she may have done the work in conjunction with other doctors or agencies either locally or overseas. However, the work must be carried out in Malaysia.
4. The author himself/herself should present the paper at the Annual Scientific Meeting of
the Malaysian Orthopaedic Association if the paper is short-listed for the award.
Procedure 1. An abstract of the paper must be submitted to the Malaysian
Orthopaedic Association. 2. The closing date for submission will be announced 3 months before the MOA
Annual general meeting and annual scientific meeting.
44

Photo.
ATTACHMENT V
Doctor of Orthopaedics and
Traumatology
(Dr. Orth. & Trauma)
Universiti Kebangsaan Malaysia
Profile of Candidate:
Name :
Matric Number :
Address :
Contact Number :
E-mail :
45

YEAR 1
Place of Attachment :
Hospital :
Supervisor :
E-mail :
Contact No. :
46

Progress of Candidate:
Year 1 (session ____/____)
Rotation:
Date: Supervisor/Signature:
1. ______________ _________________
2. ______________ _________________
3. ______________ _________________
4. ______________ _________________
Part 1 Examination
Signature:
Date : Result: Pass/Fail Supervisor: Candidate:__________
Date: Result: Pass/Fail Supervisor: Candidate:__________
Date: Result: Pass/Fail Supervisor: Candidate:__________
Date: Result: Pass/Fail Supervisor: Candidate:__________
47

Case Write Up
Case No: 1
Title :
Date Submitted: Assessor: Supervisor:
Candidate:
Date resubmitted: Assessor: Supervisor:
Candidate:
1.
2.
Date Accepted: Assessor: Supervisor:
Candidate:
Case No: 2
Title :
Date Submitted: Assessor: Supervisor:
Candidate:
Date resubmitted: Assessor: Supervisor:
Candidate:
1.
2.
Date Accepted: Assessor: Supervisor:
Candidate:
48
End of year Assesment/Interview:
Date of Assesment:
Report/Comment:
Outcome:
1. Remain in Year 1
Reason:
Signature: ___________________
Head, Candidate:
Dept of Orthopaedic and Traumatology
2. Promoted to Year 2
Signature: ___________________
Head, Candidate:
Dept of Orthopaedic and Traumatology
49

YEAR 2
Place of Attachment :
Hospital :
Supervisor :
E-mail :
Contact No. :
50
Progress of Candidate:
Year 2 (session ____/____)
Rotation:
Date: Supervisor/Signature:
1. ______________ _________________
2. ______________ _________________
3. ______________ _________________
4. ______________ _________________
Elective:
Place: ______________ __________________
Dissertation:
Name of Supervisor/Co-supervisor:
Topic:
1. Literature Review
Date:
Outcome/Plan:
Signature:
Supervisor: Candidate:
2. Proposal
Date:
Outcome/Plan:
Signature:
Supervisor: Candidate:
51

3. Ethics Committe Submission
Date:
Outcome/Plan:
Signature:
Supervisor: Candidate:
4. Date Approved by EC: (please attached letter of approval) _________________
5. Progress of Work
Date:
Outcome/Plan:
Signature:
Supervisor Candidate:
____________________________________________________________
Date:
Outcome/Plan:
Signature:
Supervisor Candidate:
____________________________________________________________
Date:
Outcome/Plan:
Signature:
Supervisor Candidate:
_____________________________________________________________
Date:
Outcome/Plan:
Signature:
Supervisor Candidate:
52

Case Write Up
Case No: 3
Title :
Date Submitted: Assessor: Supervisor:
Candidate:
Date resubmitted: Assessor: Supervisor:
Candidate:
1.
2.
Date Accepted: Assessor: Supervisor:
Candidate:
1.
Case No: 4
Title :
Date Submitted: Assessor: Supervisor:
Candidate:
Date resubmitted: Assessor: Supervisor:
Candidate:
1.
2.
Date Accepted: Assessor: Supervisor:
Candidate:
1.
53

YEAR 3
Place of Attachment :
Hospital :
Supervisor :
E-mail :
Contact No. :
54

Early of year 3 Assesment/Interview:
Date of Assesment:
Report/Comment:
Outcome:
1. Extension for 6 months
Reason:
Signature: ___________________
Head, Candidate:
Dept of Orthopaedic and Traumatology
2. No extension.
Signature: ___________________
Head, Candidate:
Dept of Orthopaedic and Traumatology
55
Progress of Candidate:
Year 3 (session ____/____)
Rotation:
Date: Supervisor/Signature:
1. ______________ _________________
2. ______________ _________________
3. ______________ _________________
4. ______________ _________________
Elective:
Place: ______________ __________________
Dissertation:
Name of Supervisor/Co-supervisor:
Topic:
5. Progress of Work
Date:
Outcome/Plan:
Signature:
Supervisor Candidate:
____________________________________________________________
Date:
Outcome/Plan:
Signature:
Supervisor Candidate:
____________________________________________________________
Date:
Outcome/Plan:
Signature:
Supervisor Candidate:
______________________________________________________________
56

Case Write Up
Case No: 5
Title :
Date Submitted: Assessor: Supervisor:
Candidate:
Date resubmitted: Assessor: Supervisor:
Candidate:
1.
2.
Date Accepted: Assessor: Supervisor:
Candidate:
1.
Case No: 6
Title :
Date Submitted: Assessor: Supervisor:
Candidate:
Date resubmitted: Assessor: Supervisor:
Candidate:
1.
2.
Date Accepted: Assessor: Supervisor:
Candidate:
1.
Case No: 7
Title :
Date Submitted: Assessor: Supervisor:
Candidate:
Date resubmitted: Assessor: Supervisor:
Candidate:
1.
2.
Date Accepted: Assessor: Supervisor:
Candidate:
1.
57

End of year 3 Assesment/Interview:
Date of Assesment:
Report/Comment:
Outcome:
3. Remain in Year 3( Extension 6 months)
Reason:
Signature: ___________________
Head, Candidate:
Dept of Orthopaedic and Traumatology
4. Promoted to Year 4
Signature: ___________________
Head, Candidate:
Dept of Orthopaedic and Traumatology
58

YEAR 4
Place of Attachment :
Hospital :
Supervisor :
E-mail :
Contact No. :
59

Progress of Candidate:
Year 4 (session ____/____)
Rotation:
Date: Supervisor/Signature:
1. ______________ _________________
2. ______________ _________________
3. ______________ _________________
4. ______________ _________________
5. _______________ _________________
6. _______________ _________________
Dissertation:
Name of Supervisor/Co-supervisor:
Topic:
7. Progress of Work
Date:
Outcome/Plan:
Signature:
Supervisor Candidate:
____________________________________________________________
Date:
Outcome/Plan:
Signature:
Supervisor Candidate:
Date
Outcome/Plan:
Signature:
Supervisor Candidate:
____________________________________________________________
60

Date:
Outcome/Plan:
Signature:
Supervisor Candidate:
Case Write Up
Case No: 8
Title :
Date Submitted: Assessor: Supervisor:
Candidate:
Date resubmitted: Assessor: Supervisor:
Candidate:
1.
2.
Date Accepted: Assessor: Supervisor:
Candidate:
1.
Case No: 9
Title :
Date Submitted: Assessor: Supervisor:
Candidate:
Date resubmitted: Assessor: Supervisor:
Candidate:
1.
2.
Date Accepted: Assessor: Supervisor:
Candidate:
1.
Case No: 10
Title :
Date Submitted: Assessor: Supervisor:
Candidate:
Date resubmitted: Assessor: Supervisor:
Candidate:
1.
2.
Date Accepted: Assessor: Supervisor:
Candidate:
1.
61

Assesment/Interview for eligibility to sit for Part 2:
Date of Assesment:
Report/Comment:
Outcome:
1. Remain in Year 4(extension for 6 months)
Reason:
Signature: ___________________
Head, Candidate:
Dept of Orthopaedic and Traumatology
2. Allow to sit for Part 2 Examination:
Signature: ___________________
Head, Candidate:
Dept of Orthopaedic and Traumatology
62
More Information : UKM Medical Centre Tel: +603-91455087 Fax: +603-91456640 Email: [email protected] Web: www.ppukm.ukm.my Centre for Academic Management Universiti Kebangsaan Malaysia 43600 UKM Bangi, Selangor Darul Ehsan, Malaysia Tel : +603-8911 8389 / 8468 Fax: +603-8911 8470 www.facebook.com/Pusat Pengurusan Akademik UKM Website: www.ukm.my/akademik / www.facebook.com/Pusat Pengurusan Akademik UKM Email: akad[at]ukm[dot]edu[dot]my