promoting the institutionalization of - world...
TRANSCRIPT

Promoting the Institutionalization of National Health Accounts
Global Consultation
October 20–21, 2010 Washington, DC
Summary
Human Development Network The World Bank

2
Global Consultation
Promoting the Institutionalization of National Health Accounts
October 20–21, 2010
Background
Resource tracking is a critical element of health systems strengthening in all countries, and
provides the essential basis for managing health financing and informing policy decisions.
The World Bank, with funding from the Bill and Melinda Gates Foundation, is working
closely with the World Health Organization (WHO), United States Agency for International
Development (USAID), and the Inter-American Development Bank to support the
institutionalization of national health accounts (NHA) to better understand the availability and
efficiency in use of resources in the health sector.
With partners and in consultation with countries, a Global Strategic Action Plan (GSAP) has
been prepared, proposing a framework for countries and development partners for routine
production and use of NHA. A Global Consultation was held on October 20–21 at Palomar
Hotel in Washington, DC, with officials from 36 countries, development partners,
foundations, and civil society organizations, to build consensus around the GSAP and to
ensure that it reflected the views and priorities of all stakeholders. The agenda and the country
participant lists are attached as Appendixes 1 and 2.
Objectives and expected outcomes of the Consultation
Facilitate a dialogue between countries and development partners around NHA
Build consensus and ensure that it reflects the views and priorities of all stakeholders
Develop a road map for a higher-level policy discussion in 2011
Encourage country participants to rally domestic support for the GSAP and begin
developing a full-fledged implementation plan.

3
Global Consultation
Promoting the Institutionalization of National Health Accounts
October 20–21, 2010
Brief summary notes
The consultation focused on discussing NHA within the broader context of resource tracking
for the Millennium Development Goals (MDGs), health policy and decision making. It
emphasized the importance of:
Accuracy and timeliness of data
Tracking resources to improve transparency and accountability
Measurement consistencies and inter-country comparisons.
NHA has positive impacts on health policy and decision making—accurate health expenditure
estimates result in better geographic allocation of resources, stronger implementation of
subsidy programs, and increased availability of free services for the poor. In Benin, NHA has
been useful in evaluation/planning and budgeting—out-of-pocket spending for families is
expected to drop to 30 percent by 2018 (currently it is over 50 percent). Also, universal
coverage in Benin was guided by the results of the country’s NHA work.
Country experiences and discussions showed that successful institutionalization/routine
production of NHA requires:
High-level buy-in from government counterparts, including enhanced ownership by the
Ministry of Finance
A political decision to institutionalize, i.e. a permanent ―institutional home‖ and a
government decree
An improved coordination role between different government agencies, government and
non-governmental actors, development partners at country level, and government and
development partners
Multi-sectoral cooperation and increased partnerships between users and producers of
NHA data
Sharing of positive experiences and best practices
Ongoing staff training in view of high turnover
Mutual accountability from countries and development partners, and sharing of data
Strategies to improve data quality over time and investing in the necessary programs and
software
Data to be useful for policy decisions, local levels to be involved, issues of budget
execution to be considered in use, and linking to other resource-tracking initiatives,
including IHP+.
Countries to produce their own ―strategic action plans.‖

4
The Global Strategic Action Plan (GSAP) was presented and discussed in groups. The major
focus of break-out groups on day 1 were on definition of institutionalization, measurement,
and the strategies listed in the action plan for institutionalization.
The five groups formed worked on the templates to discuss if they agreed on definitions,
measures, and strategies; if there were questions, issues, and challenges; and if they had
recommendations.
Group 1: Argentina, Ghana, Liberia, Mongolia, Sri Lanka, development partners
Group 2: Afghanistan, Bangladesh, Bosnia-Herzegovina, Montenegro, Jordan, Philippines,
Uganda, Zimbabwe, development partners
Group 3: Benin, Burkina Faso, Democratic Republic of the Congo (DRC), Mali, Morocco,
Niger, Senegal, Tunisia, development partners
Group 4: India, Indonesia, Kazakhstan, Kyrgyzstan, Malaysia, Maldives, Rwanda,
Tajikistan, Uzbekistan, development partners
Group 5: Botswana, Egypt, Georgia, Kenya, Tanzania, Zambia, development partners
While the individual group discussions for each of the categories are summarized in Tables
1a, 1b, and 1c below, the following broad points emerged:
On the validity of the definition of Institutionalization of NHA, there seemed to be a
general agreement with the definition with some convergence toward the need for a
strengthening of the wording with regard to the ―minimum‖ set of data and the strength of
the government ―mandate‖. An alternative definition might thus be:
Routine government-mandated and country-owned production and utilization of an
essential set of health expenditure data using an internationally accepted health
accounting framework.
On measurement, clarity was sought on the question of the regularity of the use of NHA
data with some asking for a precision of the interval and some suggesting the removal of
the notion of regularity. There were requests to add specificity to the element of
methodology; to add ―internal‖ to the use of data; to define indicators on institutional
home; and insert indicators showing the use of data for policy and planning. Comments
were also made to replace the terms ―adequacy‖ and ―use‖ in the second criteria for
institutionalization measurement. The ―use‖ indicator in second criteria in the
measurement can also be replaced with the ―dissemination‖ of indicators, as ―use‖ is
difficult to quantify. Suggestions were made to rearrange criteria with more emphasis on
―use‖ and ―government mandated‖.
On strategies. While there was general agreement on most of the strategies listed at the
country, regional, and international level, there was an emphasis on developing country-
specific strategies. There was a call for clarification on the role, rights, and responsibilities
of countries within regional networks; and a need for greater harmonization and alignment
of international efforts at country level. International agencies were asked to show greater
commitment by providing their own data, using the NHA data, discussing in the policy

5
debates, and supporting efforts for institutionalization. It was mentioned that there is value
in creating cross-country studies; clarifying the strategy on cost-reducing mechanisms;
harmonizing within the existing institutional framework, and showcasing the NHA data
within the wider macroeconomic framework. Use of data should be considered a goal and
not a strategy.
Table 1a: Group-specific Views on Definition Group Agree/disagree Questions, issues, challenges Recommendations
1
General
agreement
Suggested to add to the definition
―government led‖ as champion in
government is needed to lead the process; a
binding law is required
2
Agree with
suggestions
The terms ―standard‖ and ―minimum‖
need clarification
Instead of ―data‖ this group suggested to
use the term ―indicators‖ in order to be
more precise—indicators have specific
definitions and can be clearly measured.
Instead of standard framework use
specific framework.
3
Agree with
suggestions
Issue: does ―government-mandated‖
means government attribution?
Need to change wording: replacement of
―minimum‖ set of data by ―essential.‖
Minimum can be insufficient—essential
data is needed. ―Globally accepted‖ needs
to be defined. Suggested to specify in the
definition who is in charge: Finance,
Health Ministry
4
Agree changes
with
incorporation
of feedback
from this
consultation
Term ―mandated‖ is not enough: good
will, accountability and commitment
from government; link to existing
reporting and accounting systems is
needed. It should not be stand-alone,
needs to be aligned with current
systems/ structures.
The term ―minimum‖ needs
clarification
Suggested to reword to capture these
aspects.
Also need to consider global agreement vs.
country-level agreement.
5
Agreed with
reservations
The term ―minimum‖ needs
clarification. Does ―minimum‖ mean
basic?
The definition wording raises
question: global agreement vs.
country-level relevance?
Suggested alternative definition by the
group: ―Routine government-mandated and
country-owned production and use of
policy relevant health expenditure data in
line with a standard health accounting
framework and global norms‖

6
Table 1b: Group-specific Views on Measurement Group Agree/disagree Questions, issues, challenges Recommendations
1
Agree with
suggestions
1. Some indicators cannot be
answered as yes or no. For example,
how will we measure integration into
HIS?
2. Adequacy should be defined with
numbers and capacity
2
Agree with
recommendations
On (i): suggested to add an idea of
methodology;
on (ii): suggested swapping ―key
elements‖ with ―criteria for
institutionalization‖;
Pointed out that it’s necessary to be
more specific on how the ―institutional
home‖ gets identified—it needs to be
documented/ regulated/ put into law;
on (iii): suggested to be more specific on
what ―private‖ data and ―global key
indicators ―are
3
Agree with
suggestions
On (i): interval needs to be defined;
On (ii): indicated that the term ―use‖
is too vague—good dissemination,
and explanation of data is needed;
On (iv): the definition is too vague on
―methodology‖. It needs to be
replaced by ―international standard
classification‖
On (ii): suggested to switch ―use‖ for
―disseminate‖
On (iv): suggested to put the points in a
different order: 1) of NHA; 3)
Methodology/International Standard
classification; 2) Production
Dissemination; 4) Resources.
Added that there is a need to give ―legal
framework‖ more importance;
institutional arrangements are also very
important and need to be specified.
4
Suggested
recommendations
On (i/iii): expressed the same concern
on ―regular intervals‖ as Group 5;
On measurement: does it imply
coordination mechanism?
on (ii): the definition of ―adequate
capacity‖ is not clear
Recommended to replace ―adequate‖
with ―satisfactory‖
5
Recommendations
made
On (i): suggested to add word ―internal‖
before ―use‖ and remove ―regular
intervals‖ as it is hard to institutionalize
regular use;
Suggested to add indicators to show that
data are actually being used for policy
and planning
Using the measurement criteria, countries were asked to rank themselves on the continuum of
institutionalization scale – whether they were institutionalized, almost institutionalized,
insufficient progress or no progress to institutionalization. The feedback from the countries
ranking themselves using the measurement criteria showed that 4 countries are
institutionalized, 16 countries almost institutionalized and 14 countries stated insufficient
progress to institutionalization (2 countries did not provide the info). Appendix 3 provides
information on ranking of countries.

7
Table 1c: Group-specific Views on Strategies Group Agree/disagree Questions, issues, challenges Recommendations
1
General
agreement with
suggestion
On regional level: indicated that point 4 is
redundant
On international level: raised the
question of how to measure commitment
On country level: recommended to remove
―cost reduction‖ point and to emphasize
training and analysis.
Suggested to include comparative research
and analysis and pointed out that NHA
networks should be related to other
networks at regional level.
Recommended to focus on use, support,
and fund activities of regional networks.
Stressed that international partners should
use the country NHA data
2
General
agreement with
suggestion
On regional level: Felt countries not
properly involved
On international level: indicated that
international donors should align with
country level efforts, and that staff
turnover in country is a problem; pointed
out that when producing NHA from
donors, deliverable should not be the
report at the end of a year as one report is
not the ―institutionalization‖
Recommended to develop a standard
training package for the NHA.
On regional level: suggested to clarify
roles and responsibilities of regional
networks
Suggested cross-country studies and
comparisons are valuable
3
Agree with
suggestions
On country level: indicated that support
to institutionalization needs to include
points on national accounts; suggested to
use secondary data (use of administrative
data or others) as a cost-reducing
mechanism;
On regional level: insisted on the role of
regional networks: health economists and
political networks; subregional networks;
networks with politicians, civil society,
etc.
Stressed the need to produce accounts in
existing institutional frameworks
Suggested showcasing NHA data into
wider macroeconomic framework.
Need alignment of international efforts at
country level.
On international level: suggested to
introduce supply-side conditions and
incentives to promote NHA
institutionalization and to build NHA
institutionalization activities as part of
loans and grants for projects
4
Agree with
recommendations
Raised the question re the strategies on
country/international level: they are cost
reducing in terms of what?
Suggested need for a way to enhance
adherence to standards and to increase
utilization of NHA data.
Suggested to add an issue of sustainability,
especially when production of NHA is
outsourced.
Would like to add an extra point on cross-
country comparisons
5
Agree with
recommendations
On country level: indicated that
dissemination and use is a goal not a
strategy.
On international level: stressed that
international partners commit to providing
data at request of the country
Pointed out the need be more specific:
showcase NHA as a model for data
production/ collection to national level.
Indicated that, in general, country teams
need to make strategies country specific.
On regional level: suggested to say
―explore‖ innovative funding.
On day 2, the session on Partnership to Achieve GSAP: Vision, Roles and Responsibilities
addressed the issues of how the success of NHA can be defined and measured and the visions,
roles and responsibilities for NHA institutionalization.
In brief, the panelists expressed the following points.
First, NHA are successful when they lead to a better allocation and efficiency in the use of
the resources, systematically, over time, and not sporadically. Overall, it is important to

8
consider that spending in NHA brings a strong efficiency argument, which can make the
difference in a given country.
NHA is a resource-tracking process, not an end in itself, which responds to the need and to
the importance for a country of having a resource-tracking system.
NHA process needs to be country-led and seven elements are important to create a successful
NHA system: governance, agreements in place that lead to institutional framework, capacity
building though educating people (e.g. a university that educates students on the importance
of NHA), equipment, an information system, and reliable outputs.
Countries such as Rwanda are successful because they made a strong efficiency argument and
they developed a country-specific strategy that helped to link NHA with the country’s current
programs and plans. In addition, the government has kept reviewing the results of its
programs and plans over time, making the system clearly accountable for the production of
such information.
NHA needs to be considered as part of the health system, not separately. For this reason it is
important that a country connects the information produced in NHA to networks of users and
to the existing demand. Also, the information needs to be accurate, timely and of quality.
The following measures/indicators of success were identified:
the regular production of NHA;
how the numbers and data produced are used. The production of the data is not relevant
per se, but rather the way they are used, since the use of the data allows for the creation of
a culture of accountability.
Finally, the panel stressed more than once that for NHA to be successful is important to be
innovative on the use of the data and to think outside the box!
The second main point was on the question of how to shift the current dialogue on NHA,
which focuses mainly on NHA methodology for users and on concrete NHA
institutionalization. The panelists agreed that this is a major challenge and that:
it is important to have indicators of institutional strengthening that allow to measure how
the health systems are becoming stronger;
such a critical issue needs to be prioritized and addressed in different, country-specific
ways; and
once the environment is in place and once the leadership is aligned, as the next step, a
country should build institutional capacity.
In order to have successful NHA it is important to build institutional capacity in a country,
and to have clear leadership and accountability, since often it is not clear if the data produced
are the right ones or not, and who is accountable for them.
The third main point was on the relationship between the donors and countries, and how it
would be relevant to make the NHA system not overly dependent on the donors at the country
level.

9
The panelists stressed that at the beginning NHA was donor-driven and that this has been
changing over time. Currently, the country defines its priorities and action plans (this is the
country-specific connection between policy and planning), for which a system of incentives is
important in order to transform the local actors as main NHA stakeholders. A panelist stressed
the suggestion to the countries of using the Paris Aid Effectiveness Principles so that they
may know how the money is spent in the countries and can hold the donors accountable.
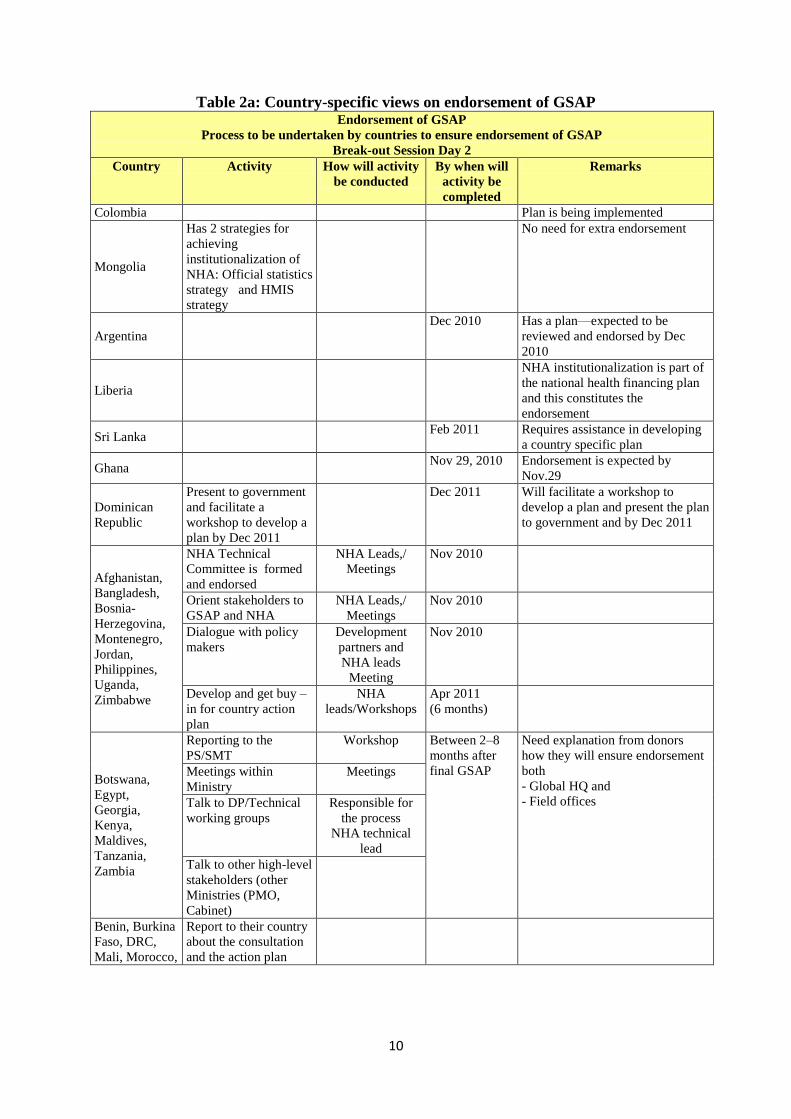
The break-out groups (same as day 1) discussed three main questions. While broad summary
of their views follow below, country- and group-specific views are outlined in Tables 2a and
2b and the Box.
10
Table 2a: Country-specific views on endorsement of GSAP Endorsement of GSAP
Process to be undertaken by countries to ensure endorsement of GSAP
Break-out Session Day 2
Country Activity How will activity
be conducted
By when will
activity be
completed
Remarks
Colombia Plan is being implemented
Mongolia
Has 2 strategies for
achieving
institutionalization of
NHA: Official statistics
strategy and HMIS
strategy
No need for extra endorsement
Argentina
Dec 2010 Has a plan—expected to be
reviewed and endorsed by Dec
2010
Liberia
NHA institutionalization is part of
the national health financing plan
and this constitutes the
endorsement
Sri Lanka Feb 2011 Requires assistance in developing
a country specific plan
Ghana Nov 29, 2010 Endorsement is expected by
Nov.29
Dominican
Republic
Present to government
and facilitate a
workshop to develop a
plan by Dec 2011
Dec 2011 Will facilitate a workshop to
develop a plan and present the plan
to government and by Dec 2011
Afghanistan,
Bangladesh,
Bosnia-
Herzegovina,
Montenegro,
Jordan,
Philippines,
Uganda,
Zimbabwe
NHA Technical
Committee is formed
and endorsed
NHA Leads,/
Meetings
Nov 2010
Orient stakeholders to
GSAP and NHA
NHA Leads,/
Meetings
Nov 2010
Dialogue with policy
makers
Development
partners and
NHA leads
Meeting
Nov 2010
Develop and get buy –
in for country action
plan
NHA
leads/Workshops
Apr 2011
(6 months)
Botswana,
Egypt,
Georgia,
Kenya,
Maldives,
Tanzania,
Zambia
Reporting to the
PS/SMT
Workshop Between 2–8
months after
final GSAP
Need explanation from donors
how they will ensure endorsement
both
- Global HQ and
- Field offices
Meetings within
Ministry
Meetings
Talk to DP/Technical
working groups
Responsible for
the process
NHA technical
lead
Talk to other high-level
stakeholders (other
Ministries (PMO,
Cabinet)
Benin, Burkina
Faso, DRC,
Mali, Morocco,
Report to their country
about the consultation
and the action plan

11
Endorsement of GSAP
Process to be undertaken by countries to ensure endorsement of GSAP
Break-out Session Day 2
Country Activity How will activity
be conducted
By when will
activity be
completed
Remarks
Niger, Senegal,
Tunisia
International partners
taking the lead—to
send the endorsement
letter with revised
document
Before end Dec 2010
Country to list
stakeholders—review
the document and
make suggestions
Validation: Health
Minister to send the
letter of endorsement
to WB
Before April 2011
Kazakhstan 2-3 months for
endorsement
6 months for
national
strategy
Tajikistan
Until
December
2010 to talk
with ministries
India
Consolidated
feedback from
this meeting will
be discussed
3-4 months
Kyrgyzstan National
strategy in
conjunction
with GSAP:
Feb-March
2011
Need Russian translation
Not clear on what sort of
endorsement is being sought
Indonesia
by April 2011
Uzbekistan Cabinet level
approval needed
by April 2011
Maldives
Implementation
plan in 6 to 12
months
Will need time as still Far behind –
Limited experience
Malaysia July 2011 Plans to be one of the first 15
Rwanda
6 months if
cabinet
approval
required

12
Table 2b: Willingness of countries and activities needed to develop implementation plans
Willingness to be one of the
first 15 countries
Compact needed between the
country and a development partner
Remarks
Yes Yes
Uganda Uganda
Montenegro Compact needed for technical
assistance for writing implementation
plan
Jordan, Zimbabwe,
Bangladesh, Uganda
Afghanistan, Bosnia-Herzegovina,
Montenegro, Jordan, Philippines,
Zimbabwe
Compact needed for implementation
Tanzania, Kenya, Georgia,
Botswana, Zambia
With plans: activities, responsible
actors, budgets: cost, sources of funds,
GAP
Benin, DRC, Morocco, Niger,
Senegal, Tunisia
No compact needed
Burkina Faso, Mali Are already involved in the process
Malaysia Already fairly institutionalized, only
need to conform to emerging
international standards and the
definition of institutionalization in the
GSAP
Table 2b (cont’d): Willingness of countries and activities needed to develop implementation plans
Implementation Plans (detailed)
Break-out session—Day 2
Country Activity needed to prepare
implementation plan
How will
activity be
conducted
Who is
responsible
for activity
By when will
activity be
completed
Afghanistan
Bangladesh
Bosnia-
Herzegovina
Montenegro
Jordan
Philippines
Uganda
Zimbabwe
Assess gaps and challenges; NHA producers Feb 2011 for those
with NHA
experience
Identify resources needed: a)
funding; b) technical assistance
NHA leads/ meetings Apr 2011
(6 months)
Draft the plan NHA leads Apr 2011
(6 months)
Revise the plan NHA leads and all agencies
involved
Apr 2011
(6 months)
Approve the plan Statistical Adv. board
NHA leads and all agencies
Apr 2011
(6 months)
Box: Endorsement of GSAP: Process to be undertaken by specific agencies
GTZ: It would advocate NHA institutionalization in the government and inform the Minister; promote the
NHA institutionalization in government negotiations with partner countries; inform HQ as well as colleagues in
partner countries about NHA/GSAP in order to be prepared for requests from partner countries; advise and
inform the German Ministry for Development about the process and generate demand on NHA analysis (e.g.
establish discussions on NHA in bilateral government consultations/negotiations); and try to integrate NHA
issue in the agenda/speech of World Health Report launching event
Global Fund: Considers this as very important as part of the monitoring framework of the Global Fund. They
would be committed to include this as part of negotiations for various rounds of funding.
REDACS – Regional Network Agency: It would prepare a newsletter on the GSAP and this meeting to
distribute among members; convene a teleconference with REDACS members to explain the GSAP and discuss
the role of each participant and commitment to foster institutionalization in his/her country; and distribute
among members a questionnaire to obtain feedback.

13
Implementation Plans (detailed)
Break-out session—Day 2
Country Activity needed to prepare
implementation plan
How will
activity be
conducted
Who is
responsible
for activity
By when will
activity be
completed
involved
Conduct public forum:
Sensitization of value of NHA
to various levels: Presidential,
Ministerial
Forming technical committee
and steering committee
Health financing policy
recognition: Recognition of
NHA as an output under the
National Health Strategy, as an
indicator under M&E tracking
Dissemination of the plan
Develop strategy for
implementation
Include production of NHA in
budget as a specific line item
Align (mapping) FM and
account systems to NHA
specifications (categories)
Develop country specific "data
manual"—record of procedure
of how NHA was carried out in
that country
Human resource training for
data collection
Identify/assign unit responsible
for NHA production
Legal framework/decree
Establish network with units
where data is located/owned for
their participation for
production (e.g. Statistics
bureau, Controller General)
Dominican
Republic
1. Presentation of the GSAP strategy
to the Minister of Health and Vice-
Minister of planning (where the
NHA unit is)
M. Rathe
Fundacion Plenitude
Nov 2010
2. With their approval, organizing a
workshop with the inter-institutional
committee of HA to: a) identify
constraints to fully institutionalize;
b) prepare the implementation plan
M. Rathe and team of
Fundacion Plenitude
Dec 2010
3. The government needs to take
charge from this point and send the
implementation plan to the WB
Sri Lanka
Appointment of a steering
committee comprising of officials
from Provincial Authorities of
Health, Ministry of Finance and
Planning, Central Bank of Sri
Lanka, Department of Census and
Statistics;
Conducting 5 meeting
Creation of cadre vacancies for
the implementation of the plan
Feb 2011

14
Implementation Plans (detailed)
Break-out session—Day 2
Country Activity needed to prepare
implementation plan
How will
activity be
conducted
Who is
responsible
for activity
By when will
activity be
completed
Allocation of funds;
Conducting 5 meetings;
Publication of developed
Implementation Plan
Colombia
Add more human resources at
DANE & MPS
DANE &
MPS
April 2011
Get an international expert in PH in
relation with methodology
Donors support
and technical
assistance
Donors—
DANE &
MPS
Dec 2010
Mongolia
Has two strategies for achieving
institutionalization of NHA:
1) Official statistic strategy;
2) HMIS strategy
Argentina
Adjust the draft already made:
timeline, funding (roles,
responsibilities ahead in place)
Technical
meeting->reports
MSN
(Ministry of
Health)
Nov-Dec 2010
Liberia
Draft plan based on tool; Filling in Excel
tool
Health
financing
Director
+Advisor
2nd week in Nov
2010
Circulate the draft plan for
comments from Task Force
members;
Hard and e-
copies sent to
members
Secretariat
of the Task
Force
3rd week of Nov
2010
Present the Plan at PCT for
approval;
PPT presentation Health
Financing
Director
End Nov 2010
Present the Plan to HSCC for
endorsement
PPT presentation Health
Financing
Director
Jan 2011
Ghana
Brief health sector partners group on
the outcome of the DC meeting and
share GSAP
At health
partners monthly
meeting
NHA team
attending
the DC
meeting
End week 1–Nov
2010
Develop country SAP Workshop of
NHA team and
technical staff
30 Nov 2010
Adopt GSAP— and develop country
SAP by Health partnership
At Health Partners meeting by
Chief Director/HoN Minister
Week 1—
Dec 2010
Develop Implementation plan Workshop NHA team End Jan 2010
Adjust Implementation plan Health partners
meeting
Chief
Director/H
ON
Minister
Week 1—
Feb 2011
Finalize plan for submitting to WB End Feb 2011
Tanzania,
Kenya,
Georgia,
Botswana,
Zambia
Get feedback from WB Meetings/
Workshops
By the time the
Global Convening
will be ready.
No compact is
needed
Provide rapid assessment TA/ Consultancy Ministries,
NHA focal
points Establish a group to foresee the
process
Benin,
Burkina Faso,
DRC, Mali,
Morocco,
Evaluation by the technical
committee using guidelines of the
World Bank
Preparation of the Strategic Plan

15
Implementation Plans (detailed)
Break-out session—Day 2
Country Activity needed to prepare
implementation plan
How will
activity be
conducted
Who is
responsible
for activity
By when will
activity be
completed
Niger,
Senegal,
Tunisia
adapted to the country
Validation by the lead
committee/Minister of Health
Advocating to the stakeholders
Including a document with a
financial scheme and costs
Kyrgyzstan Country’s Plan may
be available by
2011
On the endorsement of the GSAP: Overall, the participant countries believed that the GSAP
document is important and they agreed on the process for institutionalization but that some
follow-up needs to be done for endorsement at country level. They sought clarity on what
needs to be endorsed—the GSAP document or the institutionalization plans. Countries
pointed out the necessity of country plans to have endorsement and committed to have them
ready by the end of this year; others expected the development of the implementation plan
and endorsement of GSAP to be done by April 2011 and for some it may stretch to December
2011. Most countries will present a report on the Global Consultations to the Ministries of
Health which, after getting stakeholders’ opinions, will focus on the necessary institutional
arrangements and development of country-specific strategic plans. The majority of countries
expected to have support of the relevant institutions (Ministry of Health, the Prime Minister,
or the Cabinet). However, countries are at very different levels and stages, and to endorse
GSAP will require government consultations, also with CSOs, the private sector, etc. There
were suggestions that the WHO resolution style might be a viable alternative.
On the implementation plans: Most countries agreed that country-specific strategic plans need
to be developed to be part of phase 1. There was an overwhelming response to countries being
part of that phase. A few countries, such as India, Kyrgyzstan, and Tajikistan, could not
commit because of their internal processes. Countries expressed the requests of having the
assessment and workplan tool translated into more languages and some countries requested
technical assistance to develop the implementation plans. Countries planned to implement a
variety of activities to develop implementation plans including assessment of constraints and
gaps, stakeholder consultations, and holding workshops and public forums. A very few
countries would also need financial assistance to develop these plans, but more may need
support for workshops and public forums.
On the position papers: Discussions were held in break-out groups to know the views of
countries and the role they wished to play on preparing position papers on coordination
mechanisms, advocacy strategy and financing options for 2011 consultation. All countries
wished to be involved in position papers in some way or other. Table 2c presents whether the
countries wished to be a part of the writing, reviewing, or not be involved. The coordination
paper must also discuss coordination between national and international organizations at

16
country level and international level. Other suggestions for position paper were
standardization and the elaboration of data and its use. In order to review them, the papers
must be in other languages as well. Some groups stressed the importance of having clear
rules, so that the countries may know how they can receive funding, to further the work in this
area. The issue of the length of the documents was also raised. Further recommendations and
notes may be sent by countries. Finally, it was concluded that the next consultation may
possibly take place one year from now.
Table 2c: Country willingness to participate in position paper
Position Paper
Break-out session Day 2
Position
Paper
Consult after draft paper
prepared
Contribute to writing of paper Not
interested in
participating
Coordination
Mechanism
Malaysia, Zimbabwe, Argentina,
Uganda, Philippines,
Montenegro, Jordan,
Afghanistan, Benin, Burkina
Faso, DRC, Mali, Morocco,
Niger, Senegal, Tunisia
Bangladesh, Bosnia and Herzegovina,
Colombia, Ghana, Mongolia, Liberia, Sri
Lanka
None
Advocacy
Strategy
Malaysia, Zimbabwe, Argentina,
Uganda, Philippines,
Montenegro, Jordan,
Afghanistan, Bangladesh, Benin,
Burkina Faso, DRC, Mali,
Morocco, Niger, Senegal, Tunisia
Zimbabwe, Bosnia and Herzegovina,
Colombia, Ghana, Mongolia, Liberia, Sri
Lanka
None
Financing
Options
Bosnia and Herzegovina, Benin,
Burkina Faso, DRC, Mali,
Morocco, Niger, Senegal, Tunisia
Bosnia and Herzegovina, Colombia,
Ghana, Mongolia, Liberia, Sri Lanka
None
Next Steps
The World Bank will finalize the GSAP along the lines of the feedback received from
countries. All the tools and papers will be shared on the website (some documents may be
translated as requested). Along with its partners, World Bank will work to support countries
in developing implementation plans, prepare position papers, and plan the global convening
for endorsement of the GSAP.

17
Appendix 1
Global Consultation
Promoting the Institutionalization of National Health Accounts
October 20–21, 2010
Hotel Palomar, 2121 P Street, NW, Washington, DC 20037
Phillips Room
Agenda
Day 1 Wednesday, 20 October 2010
Time Description
08:00-09:00 Registration/Breakfast, Phillips Room Foyer
09:00-10:00 Achieving the Health MDGs – Importance of Resource Tracking Cristian Baeza (Director, HNP, World Bank)
Dorothée Yevide (Deputy Minister, Ministry of
Health, Benin)
Bob Emrey (Health Systems Divisions Chief, USAID)
Phil Hay, moderator (Communications Advisor, World Bank)
10:00-11:00 The Global Strategic Action Plan
Presentation of the framework for institutionalization of
NHA
Charu C Garg (Senior Health Economist, HNP, World Bank)
Phil Hay, moderator (Communications Advisor, World
Bank)
Discussion
11:00-11:30 Coffee/Tea break, Phillips Room Foyer
11:30-12:45 Operationalizing the Plan: Country Highlights
Experiences, success stories, and linking to the strategies
outlined in the GSAP
Boureima Ouédraogo (Director-General, Information and Health Statistics, Ministry of Health, Burkina Faso)
Alexander Turdziladze (Economist, Georgia)
Taher Abu–Elsamen (Secretary-General, High Health
Council, Jordan)
Jameela Zainuddin (Head of NHA Unit, Malaysia)
Luis César Priego Valdéz (Assistant Director of
Management and Institutional Coordination, Ministry
of Health, Mexico)
Phil Hay, moderator (Communications Advisor, World
Bank)
12:45-14:00 Lunch
14:00-16:00 Implementing the Global Strategic Action Plan
Overview of morning sessions and setting the stage for
afternoon activities
Elizabeth Ashbourne
(Senior Operations Officer, HNP, World Bank)
Break-out group discussions: Feedback on the Global
Strategic Action Plan
1. Discussion on definition and measurement
2. Strategies for overcoming the constraints, and
implementation plans going forward – roles and
responsibilities at country, regional and global levels.
Facilitators:
María Fernanda Merino Juárez (Social Development
Specialist, IDB)
Moulay Driss Zine Eddine El Idrissi (Senior Health
Economist, World Bank)
Stephen Muchiri (Associate, Abt Associates, Kenya)
Somil Nagpal (Health Specialist, SASHN, World
Bank)
Jens Wilkens (Managing Director, Swedish Committee
for International Health Care, Sweden).
16:00-16:30 Coffee/Tea break
16:30-17:45 Discussion and report back Elizabeth Ashbourne, moderator (Senior Operations
Officer, HNP, World Bank)
17:45-18:00 Group Photograph
18:30-20:30 Reception, National Room

18
Day 2 Thursday, 21 October 2010
Time Description
08:00-09:00 Breakfast, Phillips Room Foyer
09:00-09:15 Overview of previous day’s sessions Charu C. Garg (Senior Health Economist, HNP, World Bank)
09:15-10:30 Partnership to Achieve GSAP: Vision, Roles and Responsibilities Prasanta Bhushan Barua (Joint Secretary, Health
Economics Unit, Ministry of Health and Welfare, Bangladesh)
Charles Ntare (Head of Integrated Health Management
Information Systems, Ministry of Health, Rwanda) Magdalena Rathe (Executive Director, Fundación
Plenitud)
Daniel Kress (Finance and Policy, Global Health, Gates Foundation)
María Fernanda Merino Juárez (Social Development
Specialist, IDB) Bob Emrey (Health Systems Divisions Chief, USAID)
Tessa Tan Torres Edejer (Coordinator, Health Systems
Financing, WHO)
Mukesh Chawla (Sector Manager, HNP, World Bank)
Phil Hay, moderator (Communications Advisor, World
Bank)
10:30-11:00 Coffee/Tea break
11:00-12:00 The Road Map to The Global Convening in 2011 Introducing the session and setting the stage for group
discussions,
Break-out groups for:
1. Discussion on finalization and endorsement of the GSAP
2. Discussion and agreement on processes for implementation
of GSAP
3. Discussion and Agreement on position papers to be prepared
for the Global Convening
E.g. Prepare documents on the following topics
o Coordination and determination of roles and
responsibilities amongst and between institutional
partners, NHA networks, and countries
o An advocacy strategy to support GSAP implementation
o Financing the institutionalization effort
A.K. Nandakumar (Director, Institute for Global
Health and Development, Brandeis University)
Facilitators:
Tania Dmytraczenko (Senior Health Economist, World Bank)
Moulay Driss Zine Eddine El Idrissi (Senior Health Economist, World Bank)
Somil Nagpal (Health Specialist, SASHN, World Bank)
Nirmala Ravishankar (Associate, Abt Associates, World Bank)
12:00-13:00 Lunch
13:00-14:30 The Road Map to The Global Convening in 2011 (contd.)
14.30 -15.30 Report Back A.K. Nandakumar, moderator (Director, Institute for
Global Health and Development, Brandeis University)
15.30-16.00 Next steps Mukesh Chawla (Sector Manager, HNP, World Bank)

19
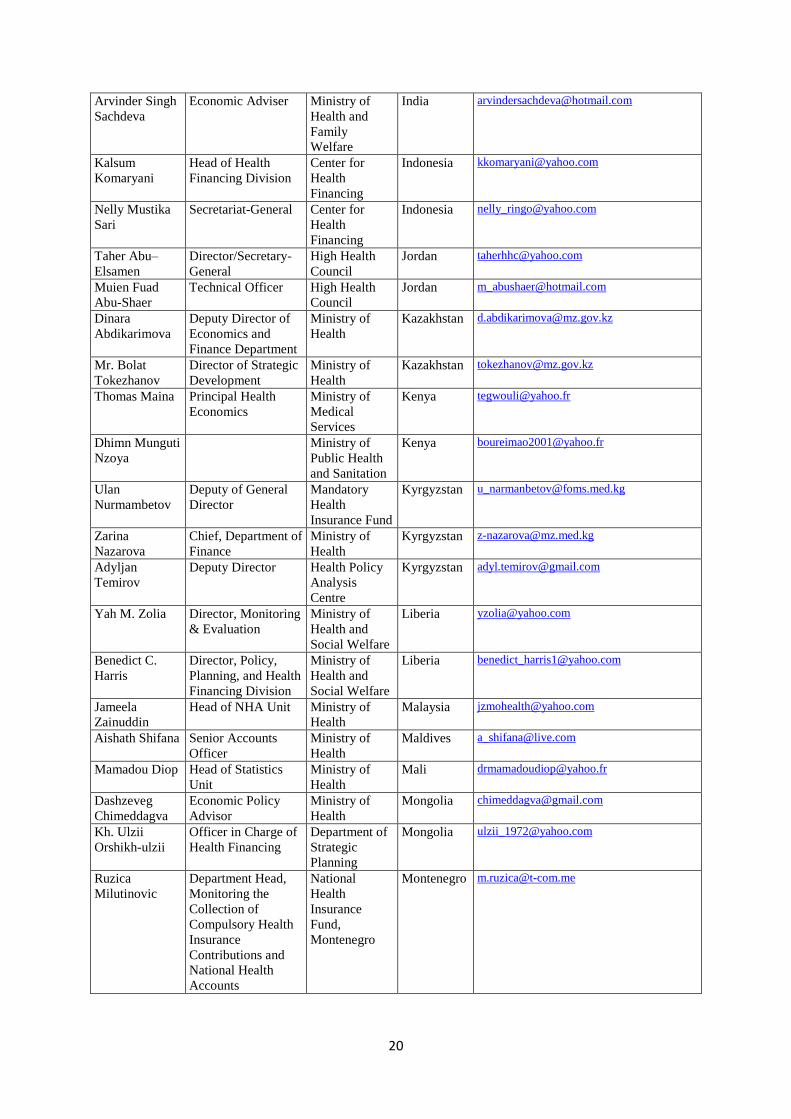
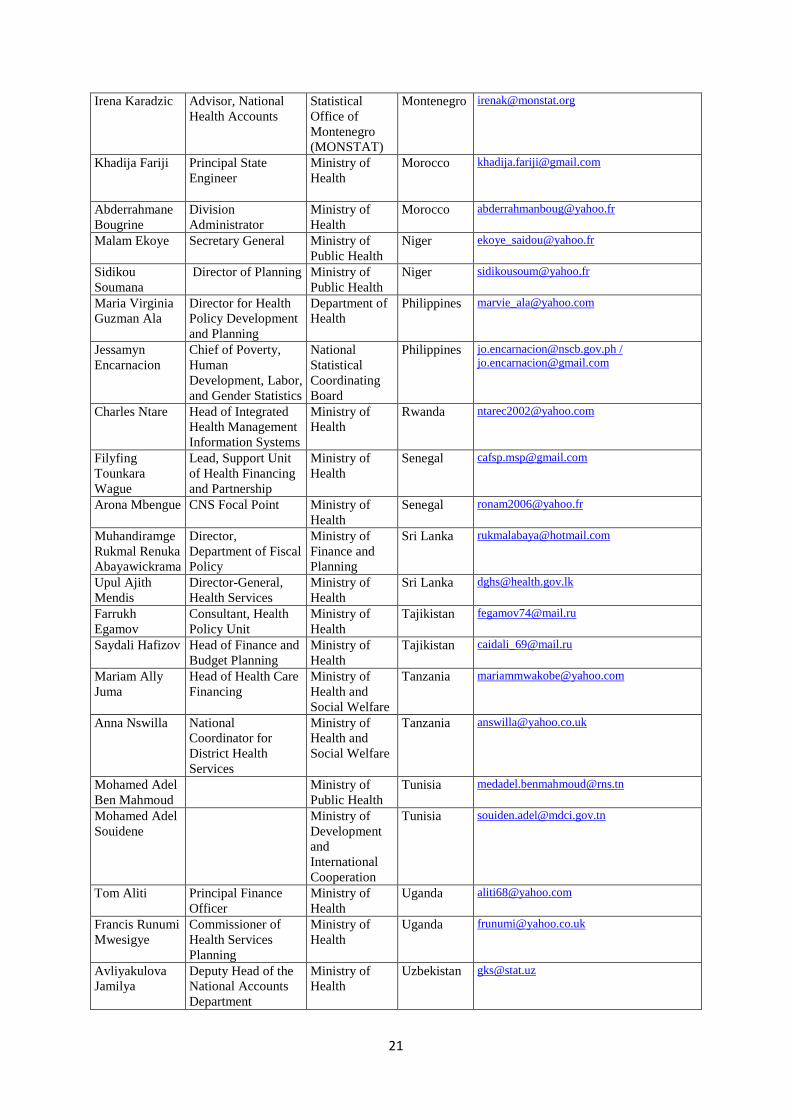
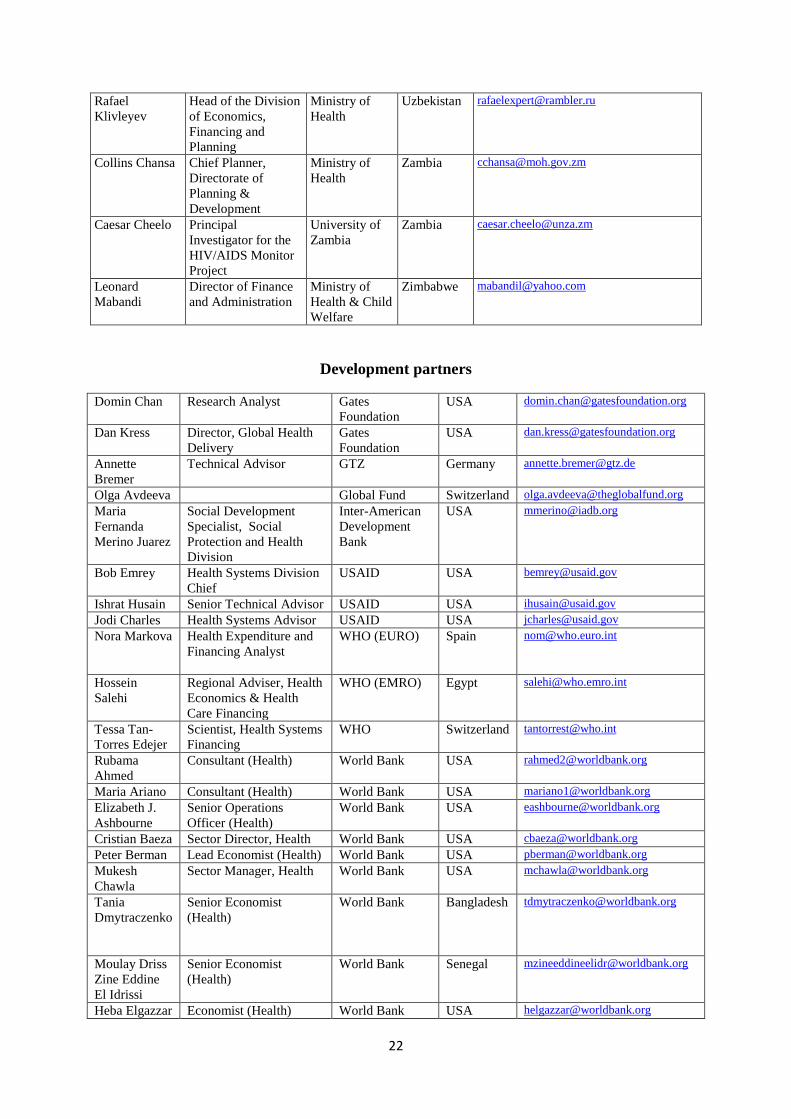
Appendix 2
Global Consultation
Promoting the Institutionalization of National Health Accounts
October 20–21, 2010
List of participants
Name Title Organization Country Email
Mohiburahman
Iqbal
NHA Team Lead Ministry of
Health
Afghanistan [email protected]
Mir Najmuddin
Hashimi
NHA Team Member Ministry of
Health
Afghanistan [email protected]
Tomás Augusto Director, Health
Economics
Ministry of
Health
Argentina [email protected],[email protected]
Martin Gustavo
Langsam
Ministry of
Economy and
Public Finance
Argentina [email protected]
Prasanta
Bhushan Barua
Joint Secretary,
Health Economics
Unit
Ministry of
Health and
Welfare
Bangladesh [email protected]
Dorothée
Yevide
Director of Cabinet Ministry of
Health
Benin [email protected]
Pascal Kora
Bata
Director of Planning
and Programming
Ministry of
Health
Benin [email protected]
Adnan Custovic FBH Health
Insurance Fund
Bosnia-
Herzegovina
Miroslav Brkic Ministry of
Finance
Bosnia-
Herzegovina
Onkemetsi
Mathala
Team Leader,
National Health
Accounts
Ministry of
Health
Botswana [email protected]
Christine
Malikongwa
Chief Finance
Officer
Ministry of
Health
Botswana [email protected]
Some Tegwouli
Romaric
Director of Studies
and Planning
Ministry of
Health
Burkina
Faso
Boureima
Ouédraogo
Director-General,
Information and
Health Statistics
Ministry of
Health
Burkina
Faso
Pierre Lokadi
Otete Opetha,
Secretary-General Ministry of
Health
Gérard Eloko
Eya Matangelo
Programme Director,
National Health
Accounts
Ministry of
Health
Merivat Taha Director-General,
Department of
Planning
Ministry of
Health
Egypt [email protected]
Alexander
Turdziladze
Economist Georgia [email protected]
Irma
Khonelidze
Program Manager Georgia Health
and Social
Projects
implementation
Center
Georgia [email protected]
Emmanuel
Kwakye Kontor
Senior Planning
Officer
Ministry of
Health
Ghana [email protected]
Dan Osei Deputy Director for
Planning and Budget
Ghana Health
Service
Ghana [email protected]
20
Arvinder Singh
Sachdeva
Economic Adviser Ministry of
Health and
Family
Welfare
India [email protected]
Kalsum
Komaryani
Head of Health
Financing Division
Center for
Health
Financing
Indonesia [email protected]
Nelly Mustika
Sari
Secretariat-General Center for
Health
Financing
Indonesia [email protected]
Taher Abu–
Elsamen
Director/Secretary-
General
High Health
Council
Jordan [email protected]
Muien Fuad
Abu-Shaer
Technical Officer High Health
Council
Jordan [email protected]
Dinara
Abdikarimova
Deputy Director of
Economics and
Finance Department
Ministry of
Health
Kazakhstan [email protected]
Mr. Bolat
Tokezhanov
Director of Strategic
Development
Ministry of
Health
Kazakhstan [email protected]
Thomas Maina Principal Health
Economics
Ministry of
Medical
Services
Kenya [email protected]
Dhimn Munguti
Nzoya
Ministry of
Public Health
and Sanitation
Kenya [email protected]
Ulan
Nurmambetov
Deputy of General
Director
Mandatory
Health
Insurance Fund
Kyrgyzstan [email protected]
Zarina
Nazarova
Chief, Department of
Finance
Ministry of
Health
Kyrgyzstan [email protected]
Adyljan
Temirov
Deputy Director Health Policy
Analysis
Centre
Kyrgyzstan [email protected]
Yah M. Zolia
Director, Monitoring
& Evaluation
Ministry of
Health and
Social Welfare
Liberia [email protected]
Benedict C.
Harris
Director, Policy,
Planning, and Health
Financing Division
Ministry of
Health and
Social Welfare
Liberia [email protected]
Jameela
Zainuddin
Head of NHA Unit Ministry of
Health
Malaysia [email protected]
Aishath Shifana Senior Accounts
Officer
Ministry of
Health
Maldives [email protected]
Mamadou Diop Head of Statistics
Unit
Ministry of
Health
Mali [email protected]
Dashzeveg
Chimeddagva
Economic Policy
Advisor
Ministry of
Health
Mongolia [email protected]
Kh. Ulzii
Orshikh-ulzii
Officer in Charge of
Health Financing
Department of
Strategic
Planning
Mongolia [email protected]
Ruzica
Milutinovic
Department Head,
Monitoring the
Collection of
Compulsory Health
Insurance
Contributions and
National Health
Accounts
National
Health
Insurance
Fund,
Montenegro
Montenegro [email protected]
21
Irena Karadzic Advisor, National
Health Accounts
Statistical
Office of
Montenegro
(MONSTAT)
Montenegro [email protected]
Khadija Fariji Principal State
Engineer
Ministry of
Health
Morocco [email protected]
Abderrahmane
Bougrine
Division
Administrator
Ministry of
Health
Morocco [email protected]
Malam Ekoye Secretary General Ministry of
Public Health
Niger [email protected]
Sidikou
Soumana
Director of Planning Ministry of
Public Health
Niger [email protected]
Maria Virginia
Guzman Ala
Director for Health
Policy Development
and Planning
Department of
Health
Philippines [email protected]
Jessamyn
Encarnacion
Chief of Poverty,
Human
Development, Labor,
and Gender Statistics
National
Statistical
Coordinating
Board
Philippines [email protected] /
Charles Ntare Head of Integrated
Health Management
Information Systems
Ministry of
Health
Rwanda [email protected]
Filyfing
Tounkara
Wague
Lead, Support Unit
of Health Financing
and Partnership
Ministry of
Health
Senegal [email protected]
Arona Mbengue CNS Focal Point Ministry of
Health
Senegal [email protected]
Muhandiramge
Rukmal Renuka
Abayawickrama
Director,
Department of Fiscal
Policy
Ministry of
Finance and
Planning
Sri Lanka [email protected]
Upul Ajith
Mendis
Director-General,
Health Services
Ministry of
Health
Sri Lanka [email protected]
Farrukh
Egamov
Consultant, Health
Policy Unit
Ministry of
Health
Tajikistan [email protected]
Saydali Hafizov Head of Finance and
Budget Planning
Ministry of
Health
Tajikistan [email protected]
Mariam Ally
Juma
Head of Health Care
Financing
Ministry of
Health and
Social Welfare
Tanzania [email protected]
Anna Nswilla National
Coordinator for
District Health
Services
Ministry of
Health and
Social Welfare
Tanzania [email protected]
Mohamed Adel
Ben Mahmoud
Ministry of
Public Health
Tunisia [email protected]
Mohamed Adel
Souidene
Ministry of
Development
and
International
Cooperation
Tunisia [email protected]
Tom Aliti Principal Finance
Officer
Ministry of
Health
Uganda [email protected]
Francis Runumi
Mwesigye
Commissioner of
Health Services
Planning
Ministry of
Health
Uganda [email protected]
Avliyakulova
Jamilya
Deputy Head of the
National Accounts
Department
Ministry of
Health
Uzbekistan [email protected]
22
Rafael
Klivleyev
Head of the Division
of Economics,
Financing and
Planning
Ministry of
Health
Uzbekistan [email protected]
Collins Chansa
Chief Planner,
Directorate of
Planning &
Development
Ministry of
Health
Zambia [email protected]
Caesar Cheelo Principal
Investigator for the
HIV/AIDS Monitor
Project
University of
Zambia
Zambia [email protected]
Leonard
Mabandi
Director of Finance
and Administration
Ministry of
Health & Child
Welfare
Zimbabwe [email protected]
Development partners
Domin Chan Research Analyst Gates
Foundation
Dan Kress Director, Global Health
Delivery
Gates
Foundation
Annette
Bremer
Technical Advisor GTZ Germany [email protected]
Olga Avdeeva Global Fund Switzerland [email protected]
Maria
Fernanda
Merino Juarez
Social Development
Specialist, Social
Protection and Health
Division
Inter-American
Development
Bank
Bob Emrey Health Systems Division
Chief
USAID USA [email protected]
Ishrat Husain Senior Technical Advisor USAID USA [email protected]
Jodi Charles Health Systems Advisor USAID USA [email protected]
Nora Markova Health Expenditure and
Financing Analyst
WHO (EURO) Spain [email protected]
Hossein
Salehi
Regional Adviser, Health
Economics & Health
Care Financing
WHO (EMRO) Egypt [email protected]
Tessa Tan-
Torres Edejer
Scientist, Health Systems
Financing
WHO Switzerland [email protected]
Rubama
Ahmed
Consultant (Health) World Bank USA [email protected]
Maria Ariano Consultant (Health) World Bank USA [email protected]
Elizabeth J.
Ashbourne
Senior Operations
Officer (Health)
World Bank USA [email protected]
Cristian Baeza Sector Director, Health World Bank USA [email protected]
Peter Berman Lead Economist (Health) World Bank USA [email protected]
Mukesh
Chawla
Sector Manager, Health World Bank USA [email protected]
Tania
Dmytraczenko
Senior Economist
(Health)
World Bank Bangladesh [email protected]
Moulay Driss
Zine Eddine
El Idrissi
Senior Economist
(Health)
World Bank Senegal [email protected]
Heba Elgazzar Economist (Health) World Bank USA [email protected]

23
Charu Garg Senior Health Economist World Bank USA [email protected]
Somil Nagpal Health Specialist World Bank India [email protected]
Juan Carlos
Salas
Consultant (Health) World Bank Colombia [email protected]
Mahesh
Shukla
Consultant (Health) World Bank USA [email protected]
Aparnaa
Somanathan
Economist (Health) World Bank USA [email protected]
UNIVERSITIES/RESEARCH INSTITUTIONS/CSOs/OTHER AGENCIES
Stephen
Muchiri
Associate Abt Associates Kenya [email protected]
Nirmala
Ravishankar
Associate Abt Associates USA [email protected]
Jeremy Snider Associate Abt Associates Rwanda [email protected]
A.K.
Nandakumar
Director, Institute for
Global Health and
Development
Brandeis
University
Ibrahim
Shehata
Senior Manager Deloitte USA [email protected]
Margareta
Harrit
Manager, Global Health
Systems Group
McKinsey UK [email protected]
Magdalena
Rathe
Executive Director Fundación
Plenitud
Dominican
Republic
Sakthivel
Selvaraj
Associate Public Health
Foundation of
India
India [email protected]
Jens Wilkens Director Swedish
Committee for
International
Health Care
Sweden [email protected]
Appendix 3: Using the measurement criteria, countries ranked themselves as follows on the
institutionalization continuum: BOX Table 1b: Institutionalization Status of National Health Accounts (by countries)
No progress Insufficient progress Almost institutionalized Institutionalized
Afghanistan Zambia Philippines
Sri Lanka Zimbabwe Malaysia
Liberia Dominican Republic Georgia
Ghana Columbia
Montenegro Jordan
Bosnia and Herzegovina Benin
DRC Burkina Faso
Mali Niger
Tunisia
Morocco
Kazakhstan India
Bangladesh Kyrgyzstan
Maldives Rwanda
Uzbekistan
Tajikistan Tanzania
Botswana Kenya
Senegal
Uganda

24