prostate cancer screening in african american men mark h. kawachi, md facs director, prostate cancer...
TRANSCRIPT

Prostate Cancer Screening in African American Men
Mark H. Kawachi, MD FACSDirector, Prostate Cancer Center
City of Hope, National Medical Ctr


Prostate Cancer Early Detection
• The National Comprehensive Cancer Network (NCCN) is an alliance of 21 of the world’s leading cancer centers.
• NCCN guidelines are widely recognized by oncology clinicians and payors.
• Where possible, the cancer guidelines are evidence-based.


Definition of “Screening”
• No universally accepted definition.
• Generally thought of as a method of applying a test to an at-risk population to determine the presence or absence of a particular disease.
• Utilizing this (or similar definition) ignores or discounts the individual’s ability to participate in the decision making process.

Prostate Cancer Early Detection
• The prostate cancer early detection guidelines stress the importance of involving the patient and informing him of the implications and potential consequences that may arise from the decision to embark on an early detection pathway.
• As such the pro’s and con’s of the early detection algorithm are thoroughly discussed.

Overview of AA Cancer Dilemma in the USA
• The age adjusted cancer related mortality in the USA is 1.4 times higher for black men than for white men.
• The disparity is greatest for prostate cancer, for which incidence rates are 1.7 times and mortality rates 2.4 times higher for black men.

Overview of AA Cancer Dilemma in the USA
• In the Medicare pt population, this is further quantified with a 1.8-year shorter survival for black men with localized CaP treated with surgery, 0.7 years shorter after radiation therapy, and 1.0 years shorter for watchful waiting. These findings persist even after accounting for covariates including education and income levels.

What’s the Difference
• Genetic predisposition?
• Differences in tumor initiation, promotion, and progression?
• Differences in higher fat diets, higher testosterone exposure/levels, or higher BMI?
• Structural, financial, and cultural differences to screening, early detection, or aggressive therapy?
• Physician bias?

There May Be Reason for Optimism in the USA
• There is data, that now suggests that in the PSA era, that the organ confined disease rate is increasing, and that the disparity in the mortality is lessening.
• It would also appears that stage for stage the same high cure rates can be achieved in black men as in their white counterparts

Family Hx and CaP Risk
Bostwick, Cancer 2004:101(10Sup):2371
Bratt J Uro 2002; 168:906Morganti,Acta Genet Stat Med 1956-1957; 6(2):304

AA CaP Incidence
USNIH SEER data accessed 2008

AA CaP Mortality By Age
Powell, J Urol 171,1508,2004

AA Mortality: Organ Confined vs Non-Organ Confined
Powell, J Urol 171,1508,2004

AA Recurrence: Before and After 1996
Bianco, J Urol, 168, 479, 2002

AA CaP Recurrence By Dates
Bianco, J Urol, 168, 479, 2002

AA CaP Recurrence By Dates
Catalona, J Urol, 168, 1980, 2002
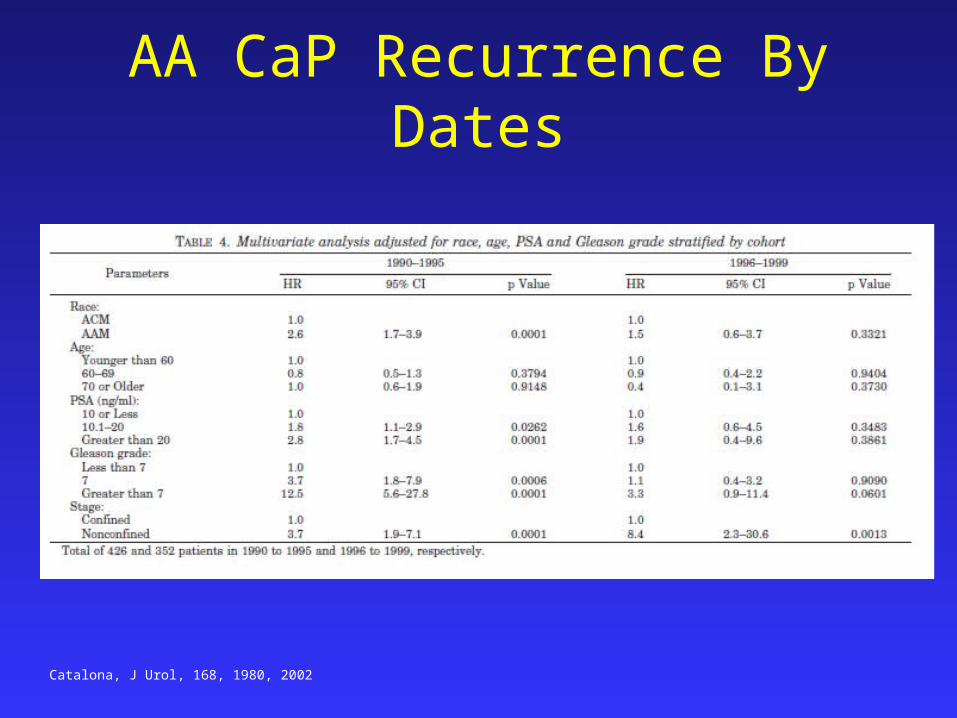
AA CaP Recurrence By Dates
Catalona, J Urol, 168, 1980, 2002

Impact of Race on CaP Outcomes
Cross, JCO, 20, No12, 2002, 2863





Summary
• At present the evidence does not suggest that the biology of prostate cancer in black men differs from that of any other group in any identifiable or clinically meaningful way.
• In fact, recent data suggests similar cure rates for organ confined disease.
• Therefore, the data would imply that race should not influence the decision on the need for initial or subsequent prostate biopsy or the decision for or choice of therapy for any stage of prostate cancer.

Conclusion
• It is intuitive to think that early detection of prostate cancer will lead to earlier and more effective therapies; however there is limited evidence to support this statement.
• For men who choose to be screened by digital rectal examination and PSA, those in the highest risk groups (AA/family history) should begin at a younger age (eg 40 years) than those of average risk.

Conclusion
• Despite the absence of known biological differences or firm evidence of a beneficial effect of screening on mortality, these recommendations seem prudent in the face of the higher age adjusted incidence and historical mortality rates for organ confined cancers in AA men in the USA.

Conclusion
• Future studies to help clarify the relationship between histologic and clinically evident prostate cancer and the true effect of PSA screening on prostate cancer mortality are necessary.