protein co-products effects, causes ofmalnutrition...
TRANSCRIPT
294
PROTEIN & CO-PRODUCTS
Effects, causes of malnutrition in Nigeriaprotein-energy malnutrition
This article was pf'f!pared by Nwe~ Nnakwe. Co/uge of Applied Science(PEM) results from prolongeddeprivation of essential amino and Technology, HOlM Economics lkpartmerat, Illinois 5une University,
acids and total nitrogen and/or energy Nonnal. Illinois.substrates. Dietary energy and pro-tein deficiencies usually occurtogether, but sometimes one predomi- age have suffered from PEM (2). (b) the hematological parameters ofnates the other and, if severe enough. Protein-energy malnutrition. espe- malnourished Nigerian children.may lead to the clinical syndrome of dally among young children.kwashiorkor (predominant protein remains one of the principal health Prevalence of PEM and causes ofdeficiency) or marasmus (mainly problems in the developing coun- death in Nigerian childrenenergy deficiency). tries. including Nigeria. It is estimat- A recent report shows that PEM is
The origin of PEM can be prima- ed that 40% of the children in Nige- still prevalent in Nigeria (5). Twentyry. when it is the result of inadequate ria who die under the age of five percent of children under five years offood intake. or secondary, when it is years were severely malnourished age seen at the Jos University Teach-the result of other diseases that lead (3). The causes of PEM are muhifac- ing Hospital were reported to beto low-food ingestion. inadequate torial though it is fairly well esteb- severely malnourished; the number ofnutrient absorption or utilization, lished that social and economic fac- malnourished children was also asincreased nutritional requirements tors are the most important determi- high as 48% in Zaria, and the inci-andlor increased nutrient losses. The nams in its etiology (4). Other condi- deuce of malnutrition is widespreadWorld Health Organization (WHO) tioning factors include lack of educe- throughout Nigeria (5,6). Various dis-(I) estimates that approximately 300 tion, infectious disease. low-food eases may contribute ro PEM. It hasmillion children have growth retar- availability and poor feeding habits. been reponed that all malnourisheddation related to malnutrition. In This review covers (a) the preva- children usually have one form ofmany developing countries 20-75% lence of PEM and causes of death in infection or another preceding or asso-of all children under five years of malnourished Nigerian children and elated with malnutrition. The most
common diseases associated withPEM include measles. malaria, diar-
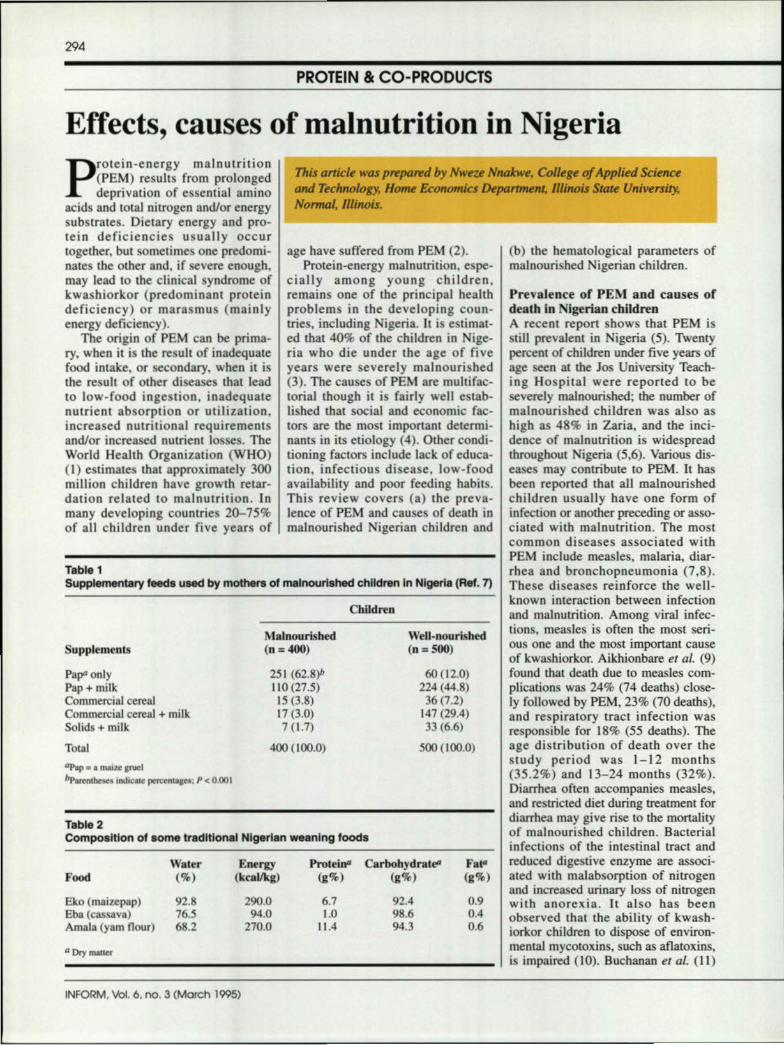
Table 1 rhea and bronchopneumonia (7,8).Supplementary feeds used by mothers of malnourished children In Nigeria (Rei. 7) These diseases reinforce the well-
known interaction between infectionChildren and malnutrition. Among viral infec-
Malnourished Well-nourished nons. measles is often the most seri-
Supplements (n::::400) (n:: 500) ous one and the most important causeof kwashiorkor. Aikhionbare et al. (9)
Pap<'only 251 (62.8)/, 60(12.0) found that death due to measles com-Pap + milk 110(27.5) 224 (44.8) plications was 24% (74 deaths) close-Commercial cereal IS (3.8) 36 (7.2) Iy followed by PEM, 23% (70 deaths).Commercial cereal + milk 17 (3.0) 147(29.4) and respiratory tract infection wasSolids + milk 7 (1.7) 33 (6.6) responsible for 18% (55 deaths). TheTotal 400 (100.0) 500 (100.0) age distribution of death over the
"Pap _I maiz.e IN<Istudy period was 1-12 months
bparenlbesu Indk:11II pem:nLa&U: P < 0.001 (35.2%) and 13-24 months (32%).Diarrhea often accompanies measles,and restricted diet during treatment for
Table 2 diarrhea may give rise to the mortality
Composition of some traditional Nigerian weaning foods of malnourished children. Bacterialinfections of the intestinal tract and
Water Energy Protein" Carbohydrates F.~ reduced digestive enzyme are associ-Food (%) (kcal/kg) (g%) (,%) (g%) ated with malabsorption of nitrogen
and increased urinary loss of nitrogenEko (maizep.ap) 92.8 290,0 6.7 92.4 0.• with anorexia. It also has beenEba (cassava) 76.5 94.0 1.0 98.6 0.4 observed that the ability of kwash-Amala (yam nour) 68.2 270,0 11.4 94.3 0.6 iorkor children to dispose of environ-IIDry mailer mental mycotoxins, such as aflatoxins,
is impaired (10). Buchanan et at. (II)
INFORM, Vol. 6, no, 3 (March 1995)

295
also found that the hepatic microso-mal oxidation and glucuronidationwas depressed in acute kwashiorkor,but in due course, on rehabilitation,normal activities were observed.
Ezedinachi and Chuks-Ejezie (12)compared mortalities due to malariaand those due to marasmic kwash-iorkor. The total number of childrenwho died from PEM was significantlyhigher than those who died due tomalaria. Malaria caused 42 deaths(3% of all the deaths occurring in thehospital during the study period),while malnutrition was responsible for174 deaths or 12.5% of the deaths.The most vulnerable age was 2-3years, of which 33.3% died of malariaand 40.8% died of PEM. The contri-bution of large family size to malnu-trition in the face of scarce resourceshas been well documented. In theIghogboja study (7), family sizes cor-related highly with childhood mortali-ty, and poor utilization of health facili-ties also contributed to childhoodmotality. Mortality pattern amongNigerian children appears to haveincreased over the years. In the past,the mortality rate among Nigerianchildren was not as high as it is today:14% mortality rate among childrenwas reported in lbadan (13), 12% inenugu (14), 11.6% in 1I0nn (15), 4.5%in Benin-city (16) and 8% in Calabar(17). Current studies have revealed amuch higher percentage of mortalityrate of over 40% in most of the Nige-rian cities. These findings were basedonly on those children who were takento the hospital. Data on the number ofchildren who were not taken to thehospital and who died at home is lack-ing; therefore, the mortality rate ofNigerian children is much higher thanwhat has been reported. The mortalityrate of Nigerian children, includingthose who died at home, needs to beinvestigated. In the past, malnutritionwas a problem of the "displaced"child from the age of two years, but itis now assuming a disturbing dimen-sion even in the first year of life. Thissuggests that breastfeeding is notbeing practiced sufficiently. This fact.combined with the economic reces-sion Nigeria is experiencing, isbelieved to cause high morality inchildren.
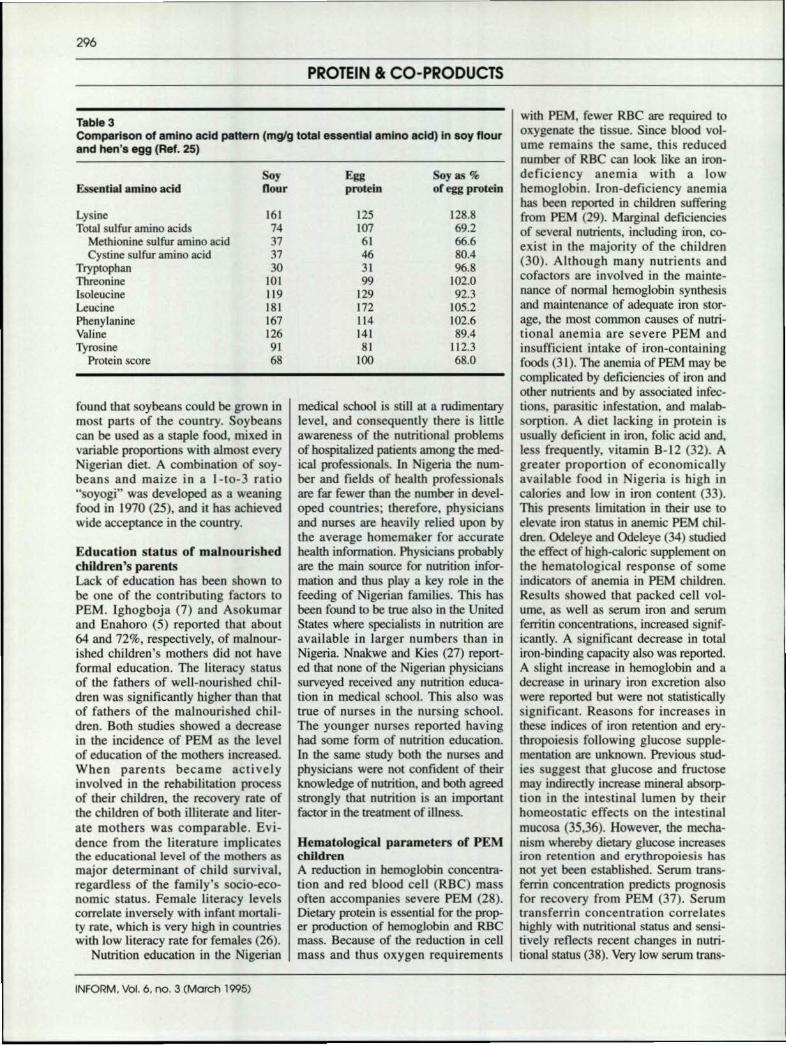
ment the family's income. Discontinu-ation of breastfeeding before the ageof six months was shown to have con-tributed significantly to malnutrition(7). Studies have reported that com-mercial formulas prepared by thesemothers were contaminated by bacte-ria and also were found to be overdi-luted and low in calorie and nutrientdensity (20,21). Supplementary feed-11i"~~~~~~~~~~~~~~1l1ing with semisolids usually startsbetween two and six months of age. Insome cases supplementary foods usedby the mothers of the malnourishedchildren included maize gruel (pap)with salt or sugar added to taste (asshown in Table 1) (7). In Nigeria, themajor weaning foods are made fromcom, millet or sorghum, often in theform of a thin gruel (8,18,22). Thecomposition of these paps have beenreported and is shown in Table 2. theprotein and energy composition ofsuch paps ("ogi") is reported to be aslow as I% protein and 30 kcal/ I00mL while the water content is as highas 90% (23). Other foods, such asboiled mashed yam, yam flour("amala"), and cassava meal ("eba"),which are given to older children, arealso starchy foods of low-nutritivevalue. Fortification of complementaryfoods to increase the energy and nutri-ent density can be achieved throughthe use of palm oil, sugar and legumes(cowpeas and soybeans, peanut andmelon). The most commonly usedcomplementary foods in Nigeria arecowpeas and soybeans. Both legumeshave the advantage of high nutrientcontent and fulfill the criteria of anideal complementary food. A combi-nation of soybeans with maize pap"soyogi" was found to be valuable inthe management of malnutrition(20,21). The comparison of soybeanand egg protein is shown in Table 3.Soybeans are high in energy, fat andprotein content. Soybeans are a richsource of vitamins and minerals whiletheir essential amino acids contentcompares well with that of eggs, andsoy protein is less expensive than ani-mal protein. Soybeans initially werenot accepted in Nigeria due to theirforeign origin. The realization of soyprotein's nutritional value hasincreased tremendously during thepast ten years, especially after it was
Effect of parent's income on PEMPoverty often accompanies PEM dueto low-food availability and lack ofmeans to produce or buy foods.Asokumar and Enahoro (5) andIghogboja (7) reported an increase inthe number of malnourished childrenamong parents who earned less than400 Niara per month. Parents with
This paperis dedicatedto the late
Dr. Constance Kies.She will be
regrettably missedand hopefullynot forgotten.
higher incomes of about 900 Niara permonth had well-nourished children. Afamily's food-buying capability maybe low due to low income, but thenursing mother's cultural food prac-tices do determine the types of foodsthe growing infants eat. Knowledge oflocal cultural food practices is veryimportant in the search for a penna-nent solution to the problems of PEM.
Feeding patterns and compositionof traditional Nigerian foodsSeveral studies have shown thatbreastfeeding is still universally prac-ticed throughout Nigeria (18,19). Thebreastfeeding patterns are reported tobe similar in mothers of both malnour-ished and nourished children. It wasreported that on the average over 70%of mothers breastfed their infants for12~24 months (8). Recent studies,however, have shown that the durationof breastfeeding has been reducedsignificantly in both rural and urbanareas, with commercial milk formulabeing introduced as early as onemonth of age (18,19). The drasticchange in the pattern of breastfeedingis because of the nursing mother'sneed for gainful employment to aug-
INFORM, Vol. 6. 00. 3 (March 1995)
296
PROTEIN Be CO-PRODUCTS
Table 3Comparison of amino acid pattern (mglg total essential amino acid) In soy flourand hen's egg (Ref. 25)
Soy Egg Soy as %Essential amino acid Dour protein of egg protein
Lysine 161 12' 128.8Total sulfur amino acids 74 107 69.2
Methionine sulfur amino acid 37 61 66.6Cystine sulfur amino acid 37 46 80A
Tryptophan 30 31 96.'Threonine 101 99 102.0Isoleucine 119 129 92.3Leucine 181 172 105.2Phenylanine 167 114 102.6Valine 126 141 89.4Tyrosine 91 81 112.3
Protein score 6' 100 68.0
found that soybeans could be grown inmost parts of the country. Soybeanscan be used as a staple food, mixed invariable proportions with almost everyNigerian diet. A combination of soy-beans and maize in a 1-10-3 ratio"soyogi" was developed as a weaningfood in 1970 (25), and it has achievedwide acceptance in the country.
medical school is still at a rudimentarylevel, and consequently there is littleawareness of the nutritional problemsof hospitalized patients among the med-ical professionals. In Nigeria the num-ber and fields of health professionalsare far fewer than the number in devel-oped countries; therefore, physiciansand nurses are heavily relied upon bythe average homemaker for accuratehealth information Physicians probablyare the main source for nutrition infor-mation and thus playa key role in thefeeding of Nigerian families. This hasbeen found to be true also in the UnitedStates where specialists in nutrition areavailable in larger numbers than inNigeria. Nnakwe and Kies (27) report-ed that none of the Nigerian physicianssurveyed received any nutrition educa-tion in medical school. This also wastrue of nurses in the nursing school.The younger nurses reported havinghad some form of nutrition education.In the same study both the nurses andphysicians were not confident of theirknowledge of nutrition, and both agreedstrongly that nutrition is an importantfactor in the treatment of illness.
Education status of malnourishedchildren's parentsLack of education has been shown 10be one of the contributing factors toPEM. Ighogboja (7) and Asokumarand Enahoro (5) reported that about64 and 72%, respectively. of malnour-ished children's mothers did not haveformal education. The literacy statusof the fathers of well-nourished chil-dren was significantly higher than thaiof fathers of the malnourished chil-dren. Both studies showed a decreasein the incidence of PEM as the levelof education of the mothers increased.When parents became activelyinvolved in the rehabilitation processof their children, the recovery rate ofthe children of both illiterate and liter-ate mothers was comparable. Evi-dence from the literature implicatesthe educational level of the mothers asmajor determinant of child survival,regardless of the family's socio-eco-nomic status. Female literacy levelscorrelate inversely with infant mortali-ty rate, which is very high in countrieswith low literacy rate for females (26).
Nutrition education in the Nigerian
Hematological parameters of PEMchildrenA reduction in hemoglobin concentra-tion and red blood cell (RBC) massoften accompanies severe PEM (28).Dietary protein is essential for the prop-er production of hemoglobin and RBCmass. Because of the reduction in cellmass and thus oxygen requirements
with PEM, fewer RBC are required tooxygenate the tissue. Since blood vol-ume remains the same, this reducednumber of RBC can look like an iron-deficiency anemia with a lowhemoglobin. Iron-deficiency anemiahas been reponed in children sufferingfrom PEM (29). Marginal deficienciesof several nutrients, including iron, c0-
exist in the majority of the children(30). Although many nutrients andcofactors are involved in the mainte-nance of normal hemoglobin synthesisand maintenance of adequate iron stor-age, the most common causes of nutri-tional anemia are severe PEM andinsufficient intake of iron-containingfoods (31). The anemia of PEM may becomplicated by deficiencies of iron andother nutrients and by associated infec-tions, parasitic infestation, and malab-sorption. A diet lacking in protein isusually deficient in iron, folic acid and,less frequently, vitamin 8-12 (32). Agreater proportion of economicallyavailable food in Nigeria is high incaJories and low in iron content (33).This presents limitation in their use toelevate iron status in anemic PEM chil-dren. Odeleye and Odeleye (34) studiedthe effect of high-caloric supplement onthe hematological response of someindicators of anemia in PEM children.Results showed that packed cell vol-ume, as well as serum iron and serumferritin concentrations, increased signif-icantly. A significant decrease in totaliron-binding capacity also was reported.A slight increase in hemoglobin and adecrease in urinary iron excretion alsowere reported but were not statisticallysignificant. Reasons for increases inthese indices of iron retention and ery-thropoiesis following glucose supple-mentation are unknown. Previous stud-ies suggest that glucose and fructosemay indirectly increase mineral absorp-lion in the intestinal lumen by theirhomeostatic effects on the intestinalmucosa (35.36). However, the mecha-nism whereby dietary glucose increasesiron retention and erythropoiesis hasnOI yet been established. Serum trans-ferrin concentration predicts prognosisfor recovery from PEM (37). Serumtransferrin concentration correlateshighly with nutritional status and sensi-tively reflects recent changes in nutri-tional status (38). Very low serum trans-
INFORM, Vol. 6, no. 3 (March 1995)
297
Ferrin levels have been reported inNigerian children suffering from PEM(37,39). lfeyimnwa et of. (40) used amostly plant protein-based diet plusiron supplement instead of the milk-based rehabilitation diets for PEM. ThePEM children fed plant protein-baseddiets needed longer periods of nutrition-al rehabilitation in the hospital than thechildren fed milk-based diets. And mor-tality was highest among children whoreceived iron supplementation early inthe study. McFarlane et ai. (37) repon-ed that hemosiderosis is seen often inkwashiorkor children and may lead tolow serum transferrin and may increasefree-circulating iron. An increase inserum iron, particularly during the firstweek of treatment, has been shown toencourage the growth of iron-requiringpathogenic bacteria. This could resultin, or aggravate, bacterial infection (41)and possibly increase the mortality ofPEM children.
Protein-energy malnutrition is stillprevalent in Nigeria. Lack of formaleducation of the mothers, poverty, adecline in breastfeeding and early intro-duction of overdiluted and often con-taminated commercial milk productswere some of the contributing factors toPEM. The use of weaning foods thatare low in energy and nutrients and thehigh prevalence of infectious diseasesalso contributed to PEM in Nigerianchildren. A combination of soybeanswith maize pap "soyogi" was found tobe valuable in the management of mal-nutrition. From available evidence, itseems that early iron supplementationduring the management of PEM is con-traindicated. And high levels of free-circulating iron in the presence of lowtransferrin concentration may bavedeleterious effects.
ReferencesI. WHO: Infant and Young Child
Nutrition, repon by tbe DirectorGeneral to the World HealthAssembly, March 1983 (docu-ment WHA 36/1983n).
2. DeMaeyer, E.M., in Nutrition illPreventive Medicine, edited byG.H. Beaton, and J.M Bengoa,World Health Organization,Geneva, 1976, pp. 23-54.
3. Ebrahim, GJ., in Pediatric Prac-tice in Developing Countries.
MacMillan. London, 1981, pp.17-22.
4. Fagbule, D., Nigerian Journal ofPediatrics 17:7 (1990).
5. Asokumar, B., and EO. Enahoro,Journal of Tropical Pediatrics37:77 (1991).
6. Cherian, A., M.B. Duggan and E.Sterken, Ecology of Food andNutrition 16:1 (1985).
7. Ighogboja, S.I., East AfrictanMedical Journal 69(10):566(1992).
8. Doyin, E. Nigerian Journal ofPaediatrics 17:7 (1990).
9. Aikhionbare, H.A., A.M. Yakubuand A.M. Naida, The CentralAfrican Journal of Medicine35(5):393 (1989).
10. Hendrickse R.G., Trans. Roy. Soc.Trop.Med. Hyg. 78:427 (1984).
II. Buchanan N., C. Eyberg andM.D. Davis, Amer. J. CUn. Nutr.32:2233 (1979).
12. Ezedinachi , E.N.U., and G.Chuks-Ejezie, Nigeria Tropicaland Geographical Medicine42:207 (1990).
13. Adeyokunnu, A.A., O. Taiwo andA.U. Anitia, Nigerian Journal ofPaediatrics 7: I (1980).
14. Kaine, W.N., and J.D. Okctie.Nigerian Medical lournal 7:2205(1977).
15. Fagbule, D., and K.T. Joiner,Nigerian Journal of Paediatrics14:1(1987).
16. Obi, J.~., Ibid. 6:69 (1976).17. Asindi, A.A., E.O. lbia and J.J.
Udo, Journal of TropicalMedicine and Hygiene 94: 152(1991).
18. Kazini, L.J., and H.R. Kazimi,Ecology of Food and Nutrition8:111 (1979).
19. Uwagbuete, A.C., and D.O.Nnanyelugo, Jou17l(J1of NutritionEducation, 19:83 (1987).
20. Elegbe, LA., and E.O. Ojofeitimi,Clinical Paediatric 23:261(1984).
21. Akinrele, I.A., and O. Bashir.Journal of TropicalMedicine andHygiene, 70:270 (1967).
22. Osuhor, P.c., Journal of HumanNutrition 273:280 (1980).
23. Abiodun, P.O., Acta PaediatricScand. Suppl. 374:175 (1991).
24. Omololu, A., in The Child in His
Family: Children at PsychiatricRisk. Vol Ill. edited by E.J.Anthony Kompermik, Wiley,New York, 1974, pp. 171-185.
25. Alkinrele, I.A., and C.C.A.Edwards, British Journal ofNutrition 26:171 (1971).
26. Caldwell, J.c., Population Study33:395 (1979).
27. Nnakwe, N.E., and C. Kies,Nutrition Reports International31(4):765 (1985).
28. viten, EE., and J. Alvarado, Rev.Col Med. (Guatemala) 21:175(1979).
29. Caballero, B., N.W. Solomons, R.Batres and B. Torun, Journal ofPediatric Gastroenterol. of Nutri-tion 4:97 (1985).
30. DeMaeyer, E.M., and M. Adiels-Tegman, World Health Stas. Q.38:302 (1985).
31. Knouenbelt, lD., Central AfricaJournal of Medicine 19:133(1973).
32. Monsen, E.R., American Journalof Dietetic Association 88(7):786(1988).
33. Mbofung, C.M., and T. Atinmo,World Review in Nutrition andDiet 51:105 (1987).
34. Odeleye, O.E., and A.A. OdeJeye,European Journal of ClinicalNutrition 46:367 (1991).
35. Krishnamurthy, K.A., and S.Rajamanickin, Guy's HospitalReport /15:183 (1966).
36. Dunn, R.R.D., American Jour-nal of Physiology 23(8):R301(1980).
37. McFarlane, H., S. Reddy, K.J.Adcock, H. Adeshina and A.R.Cooke, Brit. Med. J. 4:268(1970).
38. Crosby, L.O., A. Giandomenico,J. Foster and J.L. Mullen, J. Par-ent. Ent. Nutr. 8:274 (1984).
39. Golden, M.H.N., in NutritionalAdaptation in Man, edited byK.L. Blaxter, and J.C. Waterlow,John Libbey, London, 1985, p.169.
40. Ifeyironwa, ES., T. Olufisan andM. Payne-Robinson, EuropeanJournal of Clinical Nutrition43:705 (1989).
41. Masawe, A.EJ., and J. Rwabwo-go-Atenyi, Archive of Diseaseand Childhood 48:927 (1973). •
INFORM, Vol. 6, no. 3 (March 1995)