proteomic strategies in the search of new biomarkers in atherothrombosis
TRANSCRIPT
Iemvcbmcp
te
Fds(20(IEAIbE
2
Journal of the American College of Cardiology Vol. 55, No. 19, 2010© 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00P
FOCUS ISSUE: BIOMARKERS IN CARDIOVASCULAR DISEASE State-of-the-Art Papers
Proteomic Strategies in the Searchof New Biomarkers in Atherothrombosis
José Tuñon, MD,*‡ José Luis Martın-Ventura, PHD,†‡ Luis Miguel Blanco-Colio, PHD,†‡Óscar Lorenzo, PHD,†‡ Juan Antonio Lopez, PHD,§ Jesús Egido, MD†‡
Madrid, Spain
Extensive research has focused on the identification of novel plasma biomarkers to improve our ability to predictcardiovascular events in atherothrombosis. However, classical techniques can only assess a limited number ofproteins at a time. Given that plasma contains more than 900,000 proteins, this approach will be extremelytime-consuming. Novel proteomic approaches make it possible to compare the expression of hundreds of pro-teins in several samples in a single experiment. The classical approach consists of separation of proteins on a2-dimensional gel followed by protein identification with mass spectrometry, although new complementary gel-free techniques are emerging. We can thus compare protein expression in an atherosclerotic plaque with that ina normal artery or study plasma proteins in patients with atherothrombosis as compared with healthy subjects.For such approaches, it is not necessary to study the published data to select potential biomarkers. However,because the number of patients that can be studied with most of these techniques is limited, what is really im-portant is the design of the studies, assessing carefully what kind of patients should be included to obtain validconclusions. Clinicians should thus play a key role in this design along with the basic scientist. In this article, wereview several proteomic strategies carried out by our group and others, and we make a call for collaborationbetween clinicians and experts in proteomics. This collaboration could greatly increase the likelihood of identify-ing new prognostic biomarker panels in atherothrombosis and other cardiovascular disorders. (J Am Coll Cardiol2010;55:2009–16) © 2010 by the American College of Cardiology Foundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2010.01.036
omapuortobifi
N
TibPphss
dentifying subjects at risk of developing an acute ischemicvent remains one of the great challenges of cardiovascularedicine. Classical approaches, such as the presence of cardio-
ascular risk factors, are unable to accurately predict cardiovas-ular events (CVE). In recent years, plasma biomarkers haveeen the focus of extensive study. Although many potentialolecules have been described, the results have not been
onsistent enough (1), and most of them are not used in clinicalractice.Plasma contains more than 900,000 proteins (2). Given
hat it takes approximately 10 years from biomarker discov-ry to the development of a commercial kit (2), testing each
rom the *Department of Cardiology and †Vascular Research Laboratory, Institutoe Investigacion Sanitaria Fundacion Jiménez Dıaz (IIS-FJD), ‡Autonoma Univer-ity, Madrid, Spain; and the §Centro Nacional de Investigacion CardiovascularCNIC), Madrid, Spain. This work was supported by SAF (2007/63648 and007/60896), CAM (S2006/GEN-0247), FIS (PI050451, PS09/01405 and CP04/0060), European Network (HEALTH F2-2008-200647), EUROSALUDEUS2008-03565), Fundacion Ramon Areces, Ministerio de Sanidad y Consumo,nstituto de Salud Carlos III, Red RECAVA (RD06/0014/0035), Fundacionspañola del Corazon, Sociedad Española de Arteriosclerosis, Mutua Madrileñautomovilista and Pfizer. The CNIC is supported by the Ministerio de Ciencia e
nnovacion and the Fundacion ProCNIC. Dr. Tuñon has served on the advisoryoards for Schering-Plough and Pfizer and has been a past advisor for Pfizer. Dr.gido has served on the advisory boards for Novartis and Pfizer.
1Manuscript received November 30, 2009; revised manuscript received January 20,
010, accepted January 25, 2010.
f these proteins individually by traditional techniquesight take an eternity. Moreover, when several studies
bout new potential biomarkers with negative results areublished, investigators might be discouraged about thesefulness of biomarkers. However, given the large numberf proteins present in the plasma, the reporting of negativeesults for a few potential biomarkers does not invalidatehis approach. Moreover, these studies are usually basedn individual biomarkers, whereas the use of a panel ofiomarkers reporting information of several mechanismsnvolved in this disorder might be more effective. There-ore we need new methods to screen for novel biomarkersn atherothrombosis.
ew Proteomic Approaches
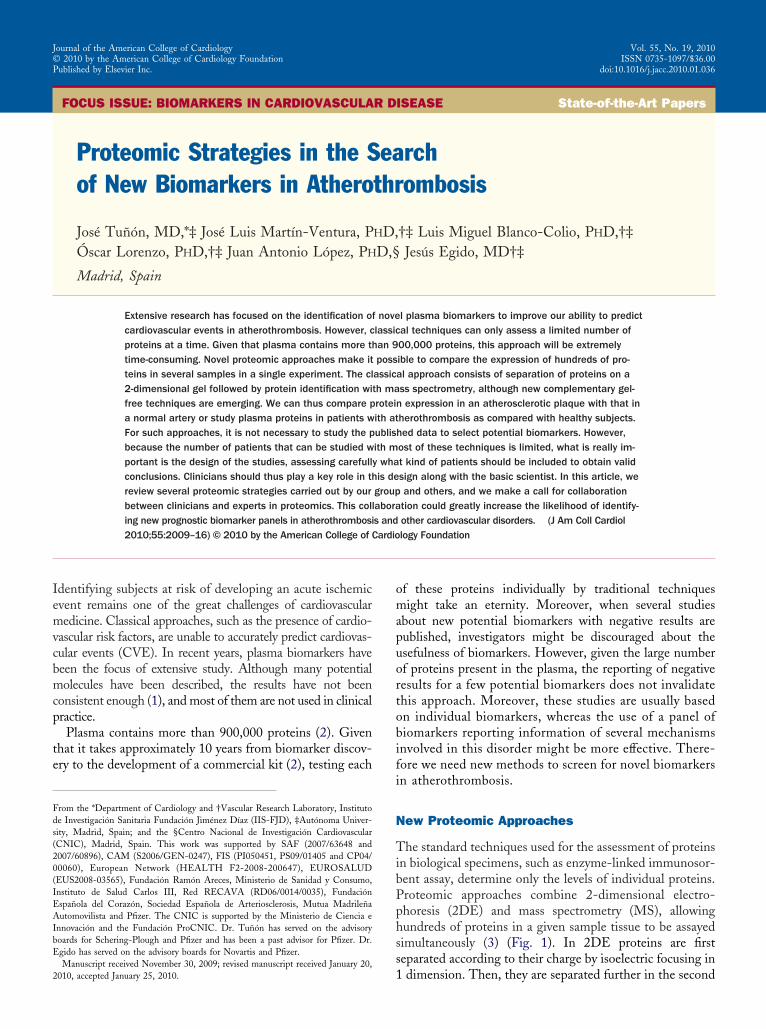
he standard techniques used for the assessment of proteinsn biological specimens, such as enzyme-linked immunosor-ent assay, determine only the levels of individual proteins.roteomic approaches combine 2-dimensional electro-horesis (2DE) and mass spectrometry (MS), allowingundreds of proteins in a given sample tissue to be assayedimultaneously (3) (Fig. 1). In 2DE proteins are firsteparated according to their charge by isoelectric focusing in
dimension. Then, they are separated further in the second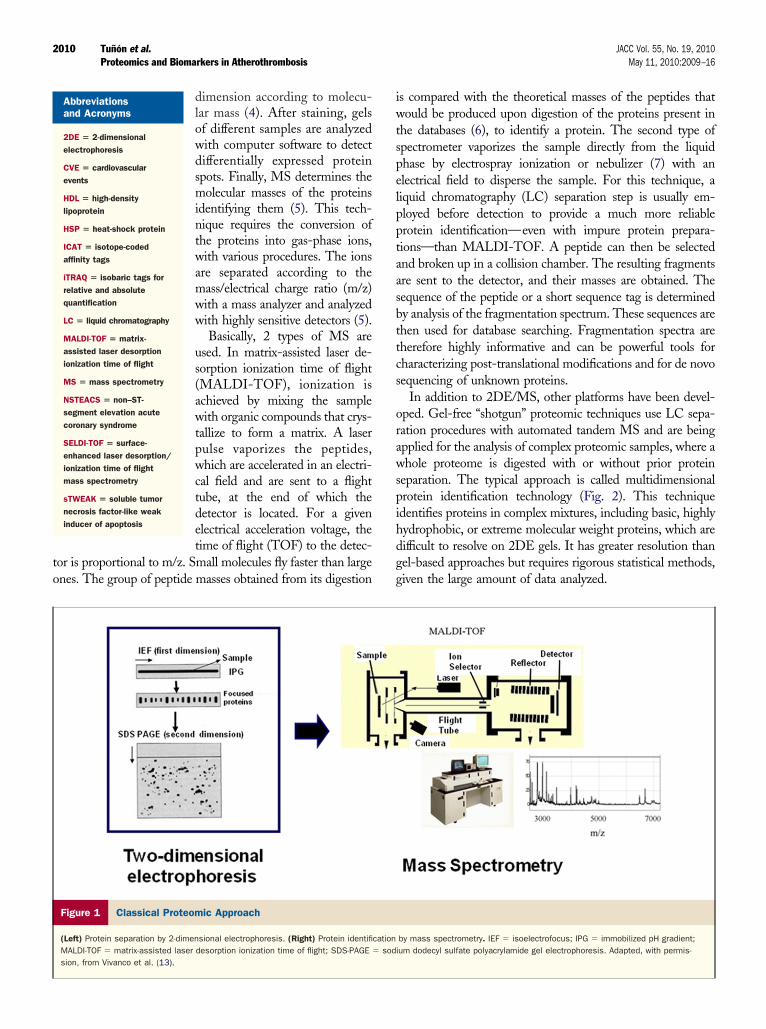
to
iwtspelpptaasbttcs
orawspihdgg
2010 Tuñon et al. JACC Vol. 55, No. 19, 2010Proteomics and Biomarkers in Atherothrombosis May 11, 2010:2009–16
dimension according to molecu-lar mass (4). After staining, gelsof different samples are analyzedwith computer software to detectdifferentially expressed proteinspots. Finally, MS determines themolecular masses of the proteinsidentifying them (5). This tech-nique requires the conversion ofthe proteins into gas-phase ions,with various procedures. The ionsare separated according to themass/electrical charge ratio (m/z)with a mass analyzer and analyzedwith highly sensitive detectors (5).
Basically, 2 types of MS areused. In matrix-assisted laser de-sorption ionization time of flight(MALDI-TOF), ionization isachieved by mixing the samplewith organic compounds that crys-tallize to form a matrix. A laserpulse vaporizes the peptides,which are accelerated in an electri-cal field and are sent to a flighttube, at the end of which thedetector is located. For a givenelectrical acceleration voltage, thetime of flight (TOF) to the detec-
or is proportional to m/z. Small molecules fly faster than largenes. The group of peptide masses obtained from its digestion
Abbreviationsand Acronyms
2DE � 2-dimensionalelectrophoresis
CVE � cardiovascularevents
HDL � high-densitylipoprotein
HSP � heat-shock protein
ICAT � isotope-codedaffinity tags
iTRAQ � isobaric tags forrelative and absolutequantification
LC � liquid chromatography
MALDI-TOF � matrix-assisted laser desorptionionization time of flight
MS � mass spectrometry
NSTEACS � non–ST-segment elevation acutecoronary syndrome
SELDI-TOF � surface-enhanced laser desorption/ionization time of flightmass spectrometry
sTWEAK � soluble tumornecrosis factor-like weakinducer of apoptosis
Figure 1 Classical Proteomic Approach
(Left) Protein separation by 2-dimensional electrophoresis. (Right) Protein identifiMALDI-TOF � matrix-assisted laser desorption ionization time of flight; SDS-PAGE �
sion, from Vivanco et al. (13).
s compared with the theoretical masses of the peptides thatould be produced upon digestion of the proteins present in
he databases (6), to identify a protein. The second type ofpectrometer vaporizes the sample directly from the liquidhase by electrospray ionization or nebulizer (7) with anlectrical field to disperse the sample. For this technique, aiquid chromatography (LC) separation step is usually em-loyed before detection to provide a much more reliablerotein identification—even with impure protein prepara-ions—than MALDI-TOF. A peptide can then be selectednd broken up in a collision chamber. The resulting fragmentsre sent to the detector, and their masses are obtained. Theequence of the peptide or a short sequence tag is determinedy analysis of the fragmentation spectrum. These sequences arehen used for database searching. Fragmentation spectra areherefore highly informative and can be powerful tools forharacterizing post-translational modifications and for de novoequencing of unknown proteins.
In addition to 2DE/MS, other platforms have been devel-ped. Gel-free “shotgun” proteomic techniques use LC sepa-ation procedures with automated tandem MS and are beingpplied for the analysis of complex proteomic samples, where ahole proteome is digested with or without prior protein
eparation. The typical approach is called multidimensionalrotein identification technology (Fig. 2). This techniquedentifies proteins in complex mixtures, including basic, highlyydrophobic, or extreme molecular weight proteins, which areifficult to resolve on 2DE gels. It has greater resolution thanel-based approaches but requires rigorous statistical methods,iven the large amount of data analyzed.
by mass spectrometry. IEF � isoelectrofocus; IPG � immobilized pH gradient;um dodecyl sulfate polyacrylamide gel electrophoresis. Adapted, with permis-
cationsodi

aoqaiimttdlIprmpatapptTic(plh
aopMnbdt
T“iapcwms
y(uwwrw
P
Ii4lgscitacmo(
PB
C
2011JACC Vol. 55, No. 19, 2010 Tuñon et al.May 11, 2010:2009–16 Proteomics and Biomarkers in Atherothrombosis
Quantitative analysis can be performed with LC-MS/MSfter differential isotopic or isobaric labeling of the proteinsr peptides from 2 cell extracts, which are simultaneouslyuantified and identified (8,9). These approaches can bepplied in different steps along the separation process andnclude stable isotope labeling by amino acids in cell culture,sotope-coded affinity tags (ICAT), tandem mass tags, and
ore recently, isobaric tags for relative and absolute quan-ification (iTRAQ). For example, in the iTRAQ methodagging is carried out on primary amines, eliminating theependence on cysteine-containing peptides, as in ICAT
abeling, yielding complementary results to ICAT. TheCAT method identifies a higher proportion of signalingroteins, whereas iTRAQ detects a larger percentage ofibosomal proteins and transcription factors (9). Theseethods are compatible with sample fractionation to reduce
rotein complexity, allowing the measurement of low-bundance proteins. Also, they could potentially be used ashe basis for automated, quantitative, and global proteomenalysis. However, most label-based quantification ap-roaches have important limitations, mainly complex sam-le preparation and handling, increased sample concentra-ion, incomplete labeling, or reduced protein coverage.herefore, classic label-free quantification is currently being
mproved to overcome some of these issues for quantifyingomplex protein mixtures in LC-MS–based strategies10,11). These methods use direct comparison of peptideeak areas between LC-MS runs without any isotopic
abeling. As a result, they do not require costly reagents andave the advantage of simplicity in sample preparation (10).Alternative approaches have been used in recent years. In
rray technologies, multiple binding antibodies are placedn a platform. However, it allows us to search only forre-specified proteins for which antibodies are available.oreover, the space available on the platform limits the
umber of antibodies that can be used. This approach mighte useful to confirm the data obtained with the techniquesescribed previously. With surface-enhanced laser desorp-
Figure 2 Nanoscale LC-MS/MS Setup
Multidimensional protein identification technology column: a reverse phase (RP) anin the emitter tip. High voltage is applied in front of the column. Samples move incess. (2) Peptides elute onto the SCX–pre-column while contaminants are washedin a single salt application step. (4) Peptides are separated on the RP-phase accospectrometer (MS), which ionizes the peptides, deflects them, and detects the ion
ion/ionization time of flight mass spectrometry (SELDI- s
OF), we might identify a pattern of MS peaks (known asproteomic fingerprint”) in a given disorder. This approachs suitable for completing characterization of a proteome,lthough it cannot directly identify differentially expressingroteins. Finally, MALDI imaging uses MALDI for re-ording the spatial distribution of proteins and peptidesithin tissue sections mounted together with a MALDIatrix and shows selected masses as color images. Figure 3
hows an overview of proteomic approaches.A thorough description of proteomic techniques is be-
ond the scope of this review and may be found in references2,3,11–13). However, we will focus on the design of studiessing proteomic approaches. Clinicians should be familiarith this field, because they have the potential to collaborateith proteomic specialists to improve the design of future
esearch to answer clinical problems of relevance to patientsith atherothrombosis.
roteomics Versus Genomics
t is important to study proteins, because they reflect whats happening in the organism. Humans have 30,000 to0,000 genes (14), only approximately twice the number ofess complex organisms, such as worms. However, a singleene might yield different proteins, due to alternativeplicing of transcripts and protein post-translationalhanges. Thus, although the genome is stable and givesnformation about the potential of an organism, the pro-eome is dynamic and reflects the biological processes thatre taking place in that organism. Both approaches areomplementary and, along with transcriptomics andetabolomics (which study the transcripts and the metab-
lites, respectively), integrate the so-called “omic” sciencesFig. 4).
roteomic Strategies in the Development ofiomarkers in Atherothrombosis: In Vitro Studies
ells involved in atherothrombosis can be cultured and
rong cation exchange (SCX)–pre-column are followed by an RP-separation phasefirst phase (1) and are trapped on RP–pre-column during the loading pro-
. (3) Trapped peptides elute from the SCX–pre-column onto RP-separation columno their hydrophobicity and elute in an acetonitrile gradient directly into a massa are delivered to a computer for analysis. LC � liquid chromatography.
d a stto theaway
rding ts. Dat
timulated with pro-atherothrombotic factors, and their
pFola1tztepapscara
gt
ciaeawl
ptspas
2012 Tuñon et al. JACC Vol. 55, No. 19, 2010Proteomics and Biomarkers in Atherothrombosis May 11, 2010:2009–16
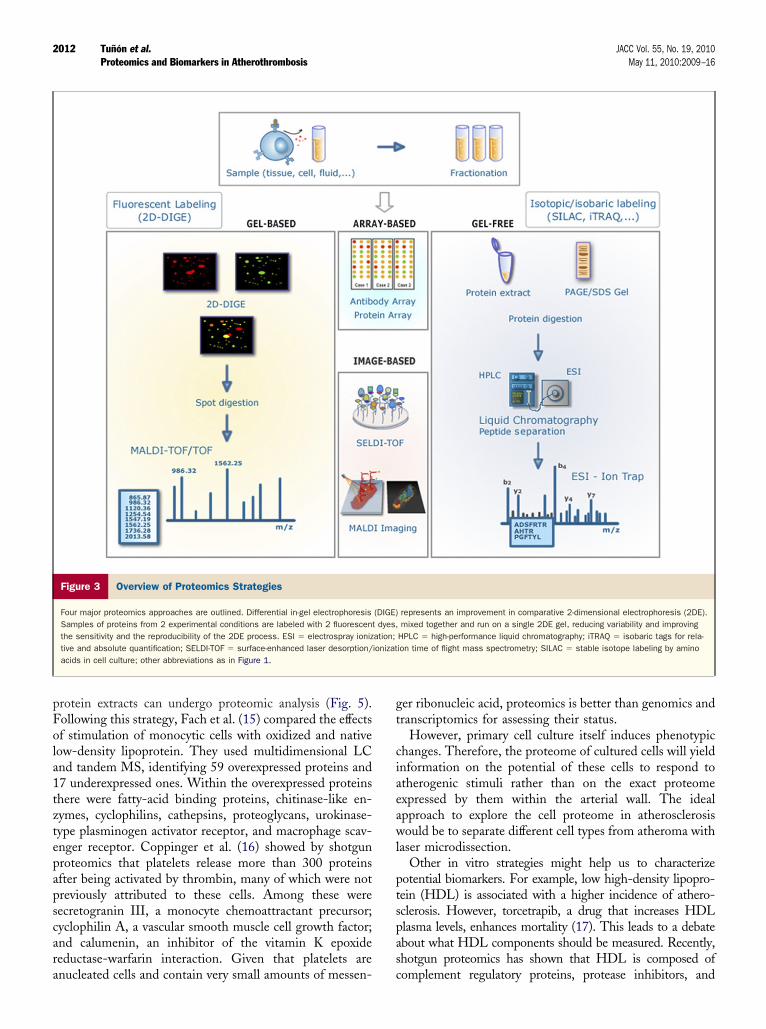
rotein extracts can undergo proteomic analysis (Fig. 5).ollowing this strategy, Fach et al. (15) compared the effectsf stimulation of monocytic cells with oxidized and nativeow-density lipoprotein. They used multidimensional LCnd tandem MS, identifying 59 overexpressed proteins and7 underexpressed ones. Within the overexpressed proteinshere were fatty-acid binding proteins, chitinase-like en-ymes, cyclophilins, cathepsins, proteoglycans, urokinase-ype plasminogen activator receptor, and macrophage scav-nger receptor. Coppinger et al. (16) showed by shotgunroteomics that platelets release more than 300 proteinsfter being activated by thrombin, many of which were notreviously attributed to these cells. Among these wereecretogranin III, a monocyte chemoattractant precursor;yclophilin A, a vascular smooth muscle cell growth factor;nd calumenin, an inhibitor of the vitamin K epoxideeductase-warfarin interaction. Given that platelets are
Figure 3 Overview of Proteomics Strategies
Four major proteomics approaches are outlined. Differential in-gel electrophoresisSamples of proteins from 2 experimental conditions are labeled with 2 fluorescentthe sensitivity and the reproducibility of the 2DE process. ESI � electrospray ioniztive and absolute quantification; SELDI-TOF � surface-enhanced laser desorption/acids in cell culture; other abbreviations as in Figure 1.
nucleated cells and contain very small amounts of messen- c
er ribonucleic acid, proteomics is better than genomics andranscriptomics for assessing their status.
However, primary cell culture itself induces phenotypichanges. Therefore, the proteome of cultured cells will yieldnformation on the potential of these cells to respond totherogenic stimuli rather than on the exact proteomexpressed by them within the arterial wall. The idealpproach to explore the cell proteome in atherosclerosisould be to separate different cell types from atheroma with
aser microdissection.Other in vitro strategies might help us to characterize
otential biomarkers. For example, low high-density lipopro-ein (HDL) is associated with a higher incidence of athero-clerosis. However, torcetrapib, a drug that increases HDLlasma levels, enhances mortality (17). This leads to a debatebout what HDL components should be measured. Recently,hotgun proteomics has shown that HDL is composed of
represents an improvement in comparative 2-dimensional electrophoresis (2DE).mixed together and run on a single 2DE gel, reducing variability and improving
HPLC � high-performance liquid chromatography; iTRAQ � isobaric tags for rela-ion time of flight mass spectrometry; SILAC � stable isotope labeling by amino
(DIGE)dyes,
ation;ionizat
omplement regulatory proteins, protease inhibitors, and

amscha
2ncvlp
2013JACC Vol. 55, No. 19, 2010 Tuñon et al.May 11, 2010:2009–16 Proteomics and Biomarkers in Atherothrombosis
cute-phase response proteins, among others (18). Further-ore, HDL3 from patients with coronary artery disease was
electively enriched in apolipoprotein E, suggesting that HDLomposition might be different in this disorder. Similarly,eat-shock protein (HSP)27 has anti-inflammatory and anti-poptotic effects and could be a candidate biomarker. With
DNAmRNA m
NUCLEUS
CELL
Transcription
Transport
Genomics~40,000 genes
Transcripto~250,000 g
Figure 4 The “Omic” Sciences
Genomics investigates the whole genome (deoxyribonucleic acid [DNA]) and its funmessenger ribonucleic acid (mRNA). From mRNA transcripts, proteins are translateolites are examined by metabolomics.
Figure 5 Proteomic Strategies for the Study of Atherothrombos
Abbreviations as in Figures 1 and 3.
DE, Trott et al. (19) found that phosphorylated HSP27 butot the hypophosphorylated form decreased expression ofycling proteins and ubiquitination enzymes in endothelial andascular smooth muscle cells. This suggests that phosphory-ated HSP27 might be an important regulator of vascular cellroliferation and could be a good candidate biomarker.
mRNA
Protein
mature Protein
Translation
Secretion
Proteomics~106 genes
Metabolom
ics
l relations. From DNA, ribonucleic acid is transcripted. Transcriptomics studiesteomics analyzes the protein expression profile. Endogenous synthesized metab-
ature
micsenes
ctionad. Pro
is

P
WHvfioNttandfCWofoCwifimue
scpdtaaiStatrpwvt
cp1nlciwew
liasanTii
tc6c
T
Bnts(esotmcpfdpttpr
mpAeas
nacdsmsPcp
2014 Tuñon et al. JACC Vol. 55, No. 19, 2010Proteomics and Biomarkers in Atherothrombosis May 11, 2010:2009–16
roteomic Analysis of Atherosclerotic Tissue
hole tissue. Atheroma can be explored by proteomics.owever, it is very heterogeneous, and the results might
ary according to whether we analyze the lipid core or thebrous cap. Laser capture microdissection allows extractionf specific tissue sections, reducing sample heterogeneity.evertheless, the subsequent proteomic analysis is limited
o techniques with extremely high analytical sensitivity, dueo the reduced amount of protein obtained (�10,000 cellsre usually collected). We can compare atheroma withormal arterial wall, and we can also explore the effect ofifferent therapies. Also, in human atheroma we can searchor differences between the proteome of those who developVE and that of those who remain stable during follow-up.ith this approach, Pasterkamp et al. (20) identified
steopontin as a candidate biomarker. After 3 years ofollow-up in a validation cohort, they confirmed that highsteopontin expression was associated with the incidence ofVE. Such an approach might help identify new proteinsith prognostic value, helping us to select patients for more
ntensive therapies. Additional studies are required to con-rm whether plasma levels of the proteins discovered by thisethod are related to prognosis. This approach would be
seful for the whole population and not just for those withndarterectomy.
Imaging MS is another emergent technology for thetudy of whole tissue. The MS is applied to thin-tissueryostat sections deposited onto MALDI plaques orrotein chip surfaces (SELDI), evidencing the spatialistribution of proteins in tissue sections (Fig. 5). Withhis technique, we have shown the presence of highmounts of non-esterified fatty acids and vitamin Eround intimal areas with high cholesterol accumulationn human atheroma (21).ecretome. Another problem working with whole tissue is
hat many constitutive proteins could mask others that haveltered expression and that could play an important role inhis disease. An alternative strategy is culturing atheroscle-otic plaques and analyzing the supernatant, obtaining theroteins secreted by the cells (i.e., the secretome). In thisay we can detect candidate biomarkers released from theascular wall into the blood, providing information abouthe processes taking place in the vascular tree.
Combining this approach with 2DE/MS, we found thatomplex human carotid atherosclerotic plaques released 202roteins to the supernatant, noncomplex plaques secreted52, and healthy arteries released only 42 (22). The super-atant of cultured atheroma showed a decrease in HSP27
evels as compared with that of normal arteries (23). Weonfirmed that the levels of this antiapoptotic and anti-nflammatory protein were lower in the plasma of patientsith carotid atherosclerosis than in healthy subjects. How-
ver, in healthy women we found that HSP27 plasma levels
ere not related to the incidence of CVE (24). tApplying SELDI-TOF to this strategy, we also detectedower levels of soluble tumor necrosis factor-like weaknducer of apoptosis (sTWEAK) (25), a protein involved inpoptosis, proliferation, and inflammation. Surprisingly,TWEAK plasma levels were lower in patients with carotidtherosclerosis than in healthy subjects and showed aegative correlation with carotid intima-media thickness.he coexistence of abnormal sTWEAK levels and an
nflammatory environment predicted mortality in patientsn hemodialysis (26).
Finally, we can also add drugs to the medium to assessheir effect on the secretome. Adding atorvastatin toultured complicated atherosclerotic plaques reverted6% of the proteins whose expression was altered toontrol values (27).
he Study of Blood by Proteomic Approaches
lood cells. In this setting, early treatment of the sample isecessary to avoid protein degradation. We studied the pro-eome of circulating monocytes in patients with non–ST-egment elevation acute coronary syndrome (NSTEACS)28). With 2DE/MS, we detected 17 proteins whosexpression was altered, as compared with expression inubjects with stable coronary artery disease. The numberf proteins with abnormal expression decreased withime. At 6 months, the proteome of the circulatingonocytes was similar to that of subjects with stable
oronary artery disease, suggesting that, by this time, therocesses that triggered NSTEACS had finished. Weound, among the proteins showing abnormal expression,ecreased levels of antiatherogenic proteins, such asaraoxonase I and HSP70, and anti-inflammatory pro-eins, such as protein disulfide isomerase. In contrast,here was overexpression of mature cathepsin D, withro-atherogenic effects, and enolase I, involved in mac-ophage transformation into foam cells.
With a similar approach we showed that atorvastatin 80g/day affected the expression of 20 proteins in NSTEACS
atients as compared with moderate statin therapy (29).mong them, there was a normalization of the decreased
xpression of HSP70, paraoxonase I, annexin I—which hasnti-inflammatory properties—and annexin II—involved inpontaneous fibrinolysis.
Although the study of circulating cells might uncoverew proteins involved in atherothrombosis, cell isolationnd protein extraction are time-consuming. Also, samplesannot be stored for more than 4 h, due to proteinegradation. Therefore studying plasma levels of the de-cribed proteins might be more appropriate, because plasmaay be obtained by simple centrifugation of the blood
ample and stored until processing.lasma. Study of the plasma with proteomic tools facesertain problems. Only 9 proteins represent 90% of therotein mass in plasma. Therefore, it is necessary to improve
he techniques to separate these high-abundance proteins
tiCtdttpTobmwtsscasi
laeimbMcafip
DR
Asbaiprbktcppmc
tfop
tsscaoFtmtentgpFsortepdl
b(ptatcpt
C
Icsasp
AB
Miil
2015JACC Vol. 55, No. 19, 2010 Tuñon et al.May 11, 2010:2009–16 Proteomics and Biomarkers in Atherothrombosis
hat might mask low-abundance proteins. Another pendingssue is the enhancement of the resolution of the techniques.urrently, by combining the results from different pro-
eomic platforms, more than 3,000 proteins have beenetected in plasma (2,30)—far less than the 900,000 pro-eins hypothesized to be present. Nevertheless, many ofhese proteins are different forms of immunoglobulin G,roduced throughout the person’s history of immune events.hese proteins hold a high similarity in sequence, and mostf them are unlikely to be biomarkers of atherothrombosis,eing possible to deplete them with an affinity-basedethod. Thus, the number of potential biomarkers will beell below this number, probably approximately several
housand. Another relevant question is whether to useerum or plasma samples. Although it is possible to studyerum, plasma contains the proteins of the coagulationascade. Given the leading role of this system in triggeringcute ischemic events, plasma would be the preferred type ofample, provided we can adequately isolate the proteins ofnterest from the more abundant proteins.
With 2DE/MALDI-TOF, Brea et al. (31) found highevels of plasma haptoglobin and serum amyloid A to bessociated with atherothrombotic rather than with cardio-mbolic stroke. Although these data need to be confirmedn larger populations, they might be useful in the manage-
ent of these patients, because cardioembolic stroke shoulde treated with anticoagulants. With the same approach,ateos-Caceres et al. (32) found a reduction in the con-
entration of several isoforms of alpha1-antitrypsin andpolipoprotein A-I and an increase in heavy chains ofbrinogen and gamma-immunoglobulin in the plasma ofatients with acute coronary syndrome.
esigning Proteomic Research:ole of the Clinician
s we have seen, new proteomic approaches provide re-earchers with a powerful tool in the search for newiomarkers. However, the clinician has a key role to play tovoid spending time and money conducting irrelevant stud-es with flawed approaches. For instance, studying plasmaroteins in patients during an acute ischemic event mighteveal new proteins implicated in atherogenesis that coulde potential biomarkers. However, clinical cardiologistsnow that some of the proteins detected might simply behe consequence of myocardial necrosis and not play aausative role in plaque thrombosis. Therefore it wouldrobably be more interesting to focus on NSTEACSatients rather than on those with ST-segment elevationyocardial infarction, because necrosis is more severe in this
ondition.Probably, the best approach in the future will be to study
he plasma from patients with atherothrombosis and toollow them for a period of time, comparing the proteomef those who develop recurrences of CVE with that of
atients who remain stable during follow-up. Because pro- meomic techniques are costly (Table 1) and time-consuming,tudying large numbers of patients is not possible. In thisetting, matching of cases and control subjects by relevantlinical variables not limited to age and sex is essential tovoid bias leading to confounding results. Also, the cardi-logist should carefully choose the end points of the study.or instance, although heart failure is a dreaded event for
hese patients, its development might be the result ofyocardial damage secondary to a previous infarction rather
han reflecting the progression of atherothrombosis. How-ver, once the experiment is completed, it is possible to findumerous proteins differing between stable patients andhose with recurrences. To select a panel with the minimalroup of proteins retaining the maximal discriminativeower for use in clinical practice, we can use several criteria.irst, we must take into account the strength of statisticalignificance by choosing those with lower “p” values. Sec-nd, we must focus on proteins whose function is potentiallyelated to the disorder studied. For this purpose, collabora-ive efforts among clinicians, scientists, and bioinformaticsxperts are warranted. Third, selecting proteins with stablelasma levels is also important. The clinician might help inesigning new experiments to test the stability of the plasma
evels of the proteins detected by proteomics.Once the proteomic approach has yielded a candidate
iomarker panel in studies with a limited number of patientsexploration cohort), the next step consists of testing thisanel in a validation cohort with conventional methods. Inhese studies, larger populations might be included, beinggain of prime importance to control for clinical variableshat could influence the outcome. Validation studies willonfirm whether the selected biomarker panel really addsrognostic value to the clinical variables used routinely inhe clinical practice.
onclusions
dentifying biomarkers by conventional methods is a time-onsuming task. Proteomics allows us to explore the expres-ion of hundreds of proteins involved in atherosclerosis withtheroma specimens, circulating blood cells, plasma, orerum. We might use strategies comparing samples fromatients with healthy control subjects, from patients receiv-
pproximate Costs of Someasic Proteomic TechniquesTable 1 Approximate Costs of SomeBasic Proteomic Techniques
Technique Cost
2DE $150–240
DIGE $1,200
Protein identification (MALDI-TOF) $60–150
Protein identification nanoLC-MS/MS $600
MudPIT $2,000
atrix-assisted laser desorption ionization time of flight (MALDI-TOF) costs are displayed/spotdentified. For the remaining techniques, costs are shown/sample analyzed except for differentialn-gel electrophoresis (DIGE) (2 samples). These prices are orientative and might vary in differentaboratories.
2DE � 2-dimensional electrophoresis; LC-MS/MS � liquid chromatography-mass spectrometry/ass spectrometry; MudPIT � multidimensional protein identification technology.

idGaaorRkmoiocclicaft
RmC
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
K
2016 Tuñon et al. JACC Vol. 55, No. 19, 2010Proteomics and Biomarkers in Atherothrombosis May 11, 2010:2009–16
ng different therapies or, more importantly, from subjectseveloping CVE with those remaining stable at follow-up.iven the large number of proteins present in the plasma
nd atheroma, this might be the only effective way to selectgroup of them that might improve our prediction of the
ccurrence of CVE. The proteomic approach does notequire previous knowledge of the proteins to be assessed.ather, patient selection, the strategy to follow, and theind of samples to be analyzed are critical to obtain theaximal yield from this technique. Moreover, the number
f patient samples to be analyzed is limited by the complex-ty and high cost of this approach. In this setting, matchingf the clinical characteristics of the populations to beompared is of great importance to avoid drawing wrongonclusions. Clinicians should then be encouraged to col-aborate in multidisciplinary studies with proteomic expertsn this task, to enhance the ability of cardiovascular medi-ine to predict which populations are at high risk oftherothrombotic events. Prevention programs could thenocus on these high-risk populations with the most intensiveherapies to decrease the incidence of CVE.
eprint requests and correspondence: Dr. José Tuñon, Depart-ent of Cardiology, Fundacion Jiménez Dıaz, Avenida Reyesatolicos 2, 28040 Madrid, Spain. E-mail: [email protected].
EFERENCES
1. Wang TJ, Gona P, Larson MG, et al. Multiple biomarkers for theprediction of first major cardiovascular events and death. N EnglJ Med 2006;355:2631–9.
2. Anderson L. Candidate-based proteomics in the search for biomarkersof cardiovascular disease. J Physiol 2005;563:23–60.
3. Arab S, Gramolini AO, Ping P, et al. Cardiovascular Proteomics:Tools to Develop Novel Biomarkers and Potential Applications. J AmColl Cardiol 2006;48:1733–41.
4. Gorg A, Obermaier C, Boguth G, et al. The current state oftwo-dimensional electrophoresis with immobilized pH gradients.Electrophoresis 2000;21:1037–53.
5. Mann M, Hendrickson R, Pandey A. Analysis of proteins and proteomesby mass spectrometry. Annu Rev Biochem 2001;70:437–73.
6. Jonssons AP. Mass spectrometry for protein and peptide characteriza-tion. Cell Mol Life Sci 2001;58:868–84.
7. Griffiths W, Jonson P, Liu S, Rai K, Wang Y. Electrospray andtandem mass spectrometry in biochemistry. Biochem J 2001;355:545– 61.
8. Gygi SP, Rist B, Gerber SA, Turecek F, Gelb MH, Aebersold R.Quantitative analysis of complex protein mixtures using isotope-codedaffinity tags. Nat Biotechnol 1999;17:994–9.
9. DeSouza L, Diehl G, Rodrigues MJ, et al. Search for cancer markersfrom endometrial tissues using differentially labeled tags iTRAQ andcICAT with multidimensional liquid chromatography and tandemmass spectrometry. J Proteome Res 2005;4:377–86.
0. Wang G, Wu WW, Zeng W, Chou CL, Shen RF. Label-free proteinquantification using LC-coupled ion trap or FT mass spectrometry:reproducibility, linearity, and application with complex proteomes. J
Proteome Res 2006;5:1214–23. p1. Duan X, Young R, Straubinger RM, et al. A straightforward andhighly efficient precipitation/on-pellet digestion procedure coupledwith a long gradient nano-LC separation and Orbitrap mass spec-trometry for label-free expression profiling of the swine heart mito-chondrial proteome. J Proteome Res 2009;8:2838–50.
2. Martın-Ventura JL, Blanco-Colio L, Tuñon J, et al. Proteomics inatherothrombosis: a future perspective. Expert Rev Proteomics 2007;4:249–60.
3. Vivanco F, Lopez-Bescos L, Tuñon J, Egido J. Proteomica y patologıacardiovascular. Rev Esp Cardiol 2003;56:289–302.
4. Venter JC, Adams MD, Myers EW, et al. The sequence of the humangenome. Science 2001;291:1304–51.
5. Fach EM, Garulacan LA, Gao J, et al. In vitro biomarker discovery foratherosclerosis by proteomics. Mol Cell Proteomics 2004;3:1200–10.
6. Coppinger JA, Cagney G, Toomey S, et al. Characterization of theproteins released from activated platelets leads to localization of novelplatelet proteins in human atherosclerotic lesions. Blood 2004;103:2096–104.
7. Barter PJ, Caulfield M, Eriksson M. Effects of torcetrapib in patientsat high risk for coronary events. N Engl J Med 2007;357:2109–22.
8. Heinecke JW. The HDL proteome: a marker—and perhaps mediator—ofcoronary artery disease. J Lipid Res 2009;50 Suppl:S167–71.
9. Trott D, McManus CA, Martin JL, Brennan B, Dunn MJ, Rose ML.Effect of phosphorylated hsp27 on proliferation of human endothelialand smooth muscle cells. Proteomics 2009;9:3383–94.
0. Pasterkamp G, Moll F, Hellings W, et al. Local atherosclerotic plaqueosteopontin is a prognostic biomarker for adverse cardiovascular eventsin heart, brain and periphery (abstr). Eur Heart J 2008;29:276–7.
1. Mas S, Touboul D, Brunelle A, et al. Lipid cartography of athero-sclerotic plaque by cluster-TOF-SIMS Imaging. Analyst 2007;132:24–6.
2. Duran MC, Mas S, Martin-Ventura JL, et al. Proteomic analysis ofhuman vessels: application to atherosclerotic plaques. Proteomics2003;3:973–8.
3. Martin-Ventura JL, Duran MC, Blanco-Colio LM, et al. Identifica-tion by a differential proteomic approach of HSP27 as a potentialmarker of atherosclerosis. Circulation 2004;110:2216–9.
4. Kardys I, Rifai N, Meilhac O, et al. Plasma concentration of heatshock protein 27 and risk of cardiovascular disease: a prospective,nested case-control study. Clin Chem 2008;54:139–46.
5. Blanco-Colio LM, Martın-Ventura JL, Muñoz-Garcıa B, et al.Identification of soluble tumor necrosis factor-like weak inducer ofapoptosis (sTWEAK) as a possible biomarker of subclinical athero-sclerosis. Arterioscler Thromb Vasc Biol 2007;27:916–22.
6. Carrero JJ, Ortiz A, Qureshi AR, et al. Additive effects of solubleTWEAK and inflammation on mortality in hemodialysis patients.Clin J Am Soc Nephrol 2009;4:110–8.
7. Duran MC, Martın-Ventura JL, Mohammed S, et al. Atorvastatinmodulates the profile of proteins released by human atheroscleroticplaques. Eur J Pharmacol 2007;562:119–29.
8. Barderas MG, Tuñon J, Dardé VM, et al. Circulating humanmonocytes in the acute coronary syndrome express a characteristicproteomic profile. J Proteome Res 2007:6:876–86.
9. Barderas MG, Tuñon J, Dardé VM, et al. Atorvastatin modifies theprotein profile of circulating human monocytes after an acute coronarysyndrome. Proteomics 2009;9:1982–93.
0. Ping P, Vondriska TM, Creighton CJ, et al. A functional annotationof subproteomes in human plasma. Proteomics 2005;5:3506–19.
1. Brea D, Sobrino T, Blanco M, et al. Usefulness of haptoglobin andserum amyloid A proteins as biomarkers for atherothrombotic isch-emic stroke diagnosis confirmation. Atherosclerosis 2009;205:561–7.
2. Mateos-Caceres PJ, Garcıa-Méndez A, Lopez Farré A, et al. Pro-teomic analysis of plasma from patients during an acute coronarysyndrome. J Am Coll Cardiol 2004;44:1578–83.
ey Words: atherothrombosis y biomarkers y mass spectrometry y
roteomics.