prothena corporation plc overview june 3, corporation plc overview jefferies 2014 global healthcare...
TRANSCRIPT

Prothena Corporation plc Overview Jefferies 2014 Global Healthcare Conference
June 3,
2014

2
Forward-Looking Statements
This presentation contains "forward-looking" statements that involve risks, uncertainties and assumptions. If the risks or
uncertainties materialize or the assumptions prove incorrect, our results may differ materially from those expressed or implied
by such forward-looking statements. All statements other than statements of historical fact could be deemed forward-looking,
including, but not limited to, any projections of financial performance, business prospects, our product candidates in research
and development, any statements about historical results that may suggest on-going trends for our business, any statements
of the plans, strategies, and objectives of management for future operations, any statements of expectation or belief regarding
future events, potential markets or market size or preclinical, clinical or other developments; and any statements of
assumptions underlying any of the items mentioned. These statements are based on estimates and information available to us
at the time of this presentation and are not guarantees of future performance. Actual results could differ materially from our
current expectations. You should not rely upon forward-looking statements as predictions of future events. Although we believe that
the expectations reflected in the forward-looking statements are reasonable, we cannot guarantee that the future results, levels of
activity, performance or events and circumstances reflected in the forward-looking statements will be achieved or occur. Moreover, we
undertake no obligation to update publicly any forward-looking statements for any reason to conform these statements to actual
results or to changes in our expectations.
We refer you to the documents that we file from time to time with the Securities and Exchange Commission, specifically our
Annual Report on Form 10-K and our Quarterly Reports on Form 10-Q. These documents, including the sections therein
entitled “Risk Factors”, identify important factors that could cause the actual results to differ materially from those contained in
forward-looking statements.

3
We target proteins in novel ways to
resolve unmet clinical need in patients
Prothena Vision
4
Prothena Overview
• Advancing and developing novel antibodies for diseases
involving protein misfolding or cell adhesion
• Team has track record of discovering and developing
immunotherapy products including abeta immunotherapy
and Tysabri®
• Lead programs in the pipeline (all mABs):
– NEOD001 for AL amyloidosis expected to enter P2/3 in 4Q14
– PRX002, α-synuclein immunotherapy, for Parkinson’s disease in
Phase 1 SAD (worldwide collaboration with Roche)
– PRX003, MCAM antibody, for inflammatory diseases and cancers
• $195M in cash at end of 1Q14
– Additionally, earned $15M clinical milestone (2Q14) from Roche

5
Team with Track Record of Bringing Significant Products to Market
SENIOR MANAGEMENT
Dale Schenk, PhD
Chief Executive Officer and Director
Gene Kinney, PhD
Chief Scientific Officer, Head of R&D
Tran Nguyen
Chief Financial Officer
Martin Koller, MD
Chief Medical Officer
Tara Nickerson, PhD, MBA
Chief Business Officer
Bill Homan
Chief Legal Officer
BOARD OF DIRECTORS
Lars Ekman, MD, PhD
Chairman
Richard T. Collier
Director
Shane Cooke
Director
Christopher S. Henney
Director
Dennis J. Selkoe, MD
Director
SELECTED LIFE SCIENCE EXPERIENCE MARKETED PRODUCTS
[
[
[
[ [
[
[
[
[
[
[

6
2014 Progress and Upcoming Milestones
• NEOD001 for AL Amyloidosis
Dr. Liedtke presented encouraging NT-proBNP results (responses and stabilization) from ongoing Phase 1 clinical trial at ISA in April 2014
Additional Phase 1 data updates expected later in 2014
Initiate Phase 2/3 clinical trial in patients with AL amyloidosis and cardiac involvement in 4Q14
• PRX002 for Parkinson’s disease (worldwide collaboration with Roche)
Initiated Phase 1 SAD study with successful first in human dosing
Earned $15M clinical milestone payment from Roche (April 2014), which is in addition to the $30M upfront payment from Roche (February 2014)
Initiate Phase 1 MAD study in patients with Parkinson’s disease
• PRX003 for inflammatory diseases and cancers
Announce initial indication(s)
Complete IND enabling toxicology studies
7
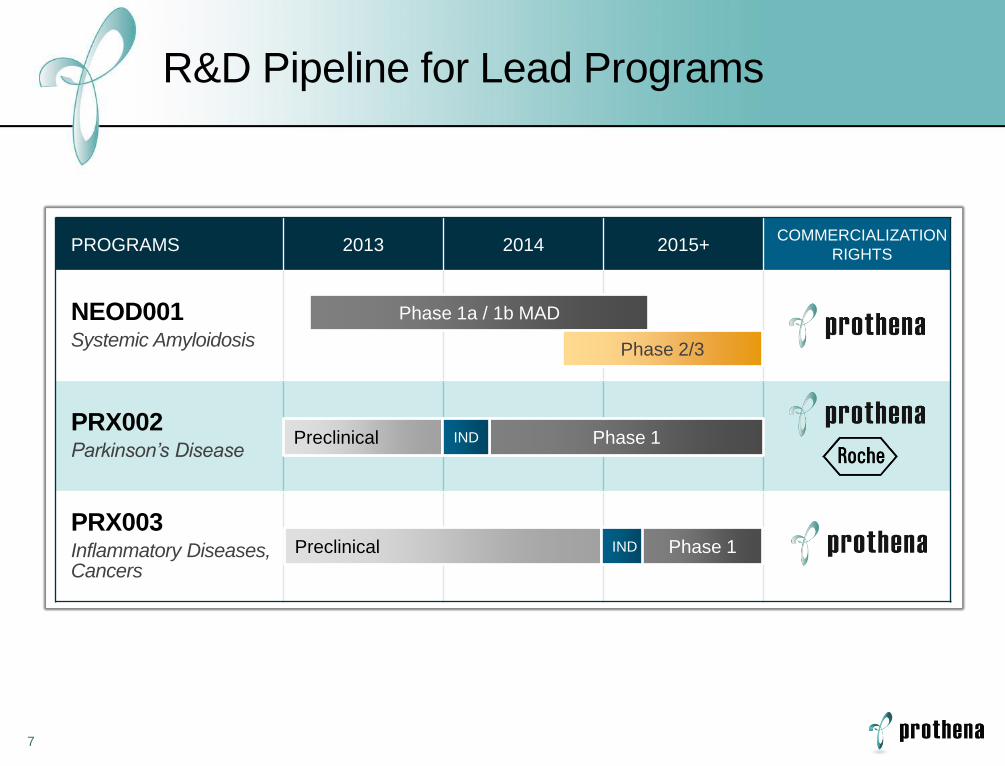
R&D Pipeline for Lead Programs
PROGRAMS 2013 2014 2015+ COMMERCIALIZATION
RIGHTS
NEOD001 Systemic Amyloidosis
PRX002 Parkinson’s Disease
PRX003 Inflammatory Diseases, Cancers
Phase 1a / 1b MAD
Phase 2/3
Preclinical Phase 1
Preclinical IND Phase 1
IND

NEOD001 for Systemic Amyloidosis

9
Amyloid Light Chain (AL)
Amyloidosis
• Antibody light chain deposits affect multiple organs (e.g., heart, kidney, etc.)
• Median survival < 3 years1
• ~15,000 patients in the US and Europe
Systemic Amyloidoses are Orphan Diseases with Unmet Need and No Approved Therapies
No Approved Therapies
Need for disease modifying
therapies that target organs
and slow damage or
improve function
• Existing AL chemotherapy reduces production, but does not address existing toxic amyloid
1. Palladini G, et al. Amyloid. 2005; 12:120 and Kumar, et al. Am J Hermatol. 2011; 86(3):251-5
Current
Treatment

10
AL Represents Majority of Systemic Amyloidoses and NEOD001 Targets AL Amyloid
AL Therapeutic Landscape2
1. van Gameren, I., et al. (2010) Arthritis Care Res, 62: 296–301
2. www.clinicaltrials.gov
• Melph+Dex
• HD Melph
• MLN9708 (P3)
• Pomalyst® (P2)
• Revlimid® (P2)
• Treanda® (P2)
• Velcade® (P2)
• Kyprolis® (P1)
Pla
sm
a c
ell
•NEOD001 (P1)
AL 55%
AA 30%
ATTR 15% A
L A
mylo
id
No A
ppro
ved T
hera
pie
s
Systemic Amyloidoses1
11
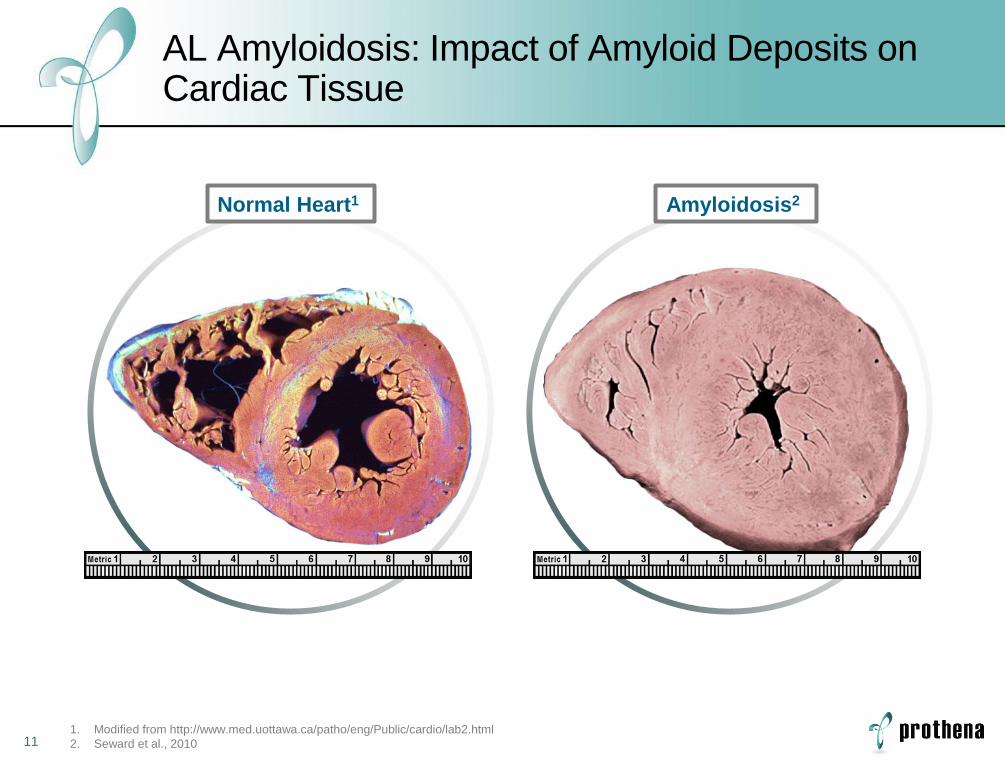
AL Amyloidosis: Impact of Amyloid Deposits on Cardiac Tissue
1. Modified from http://www.med.uottawa.ca/patho/eng/Public/cardio/lab2.html
2. Seward et al., 2010
Normal Heart1 Amyloidosis2

12
Potential NEOD001 MOA: Neutralizes Soluble Toxic Aggregates and Clears AL Amyloid Deposits
Soluble Aggregates
of Amyloid Protein
Monocyte/
Macrophage
Amyloid
Potential Mechanism of Action for NEOD001 Neutralize or facilitate clearance of amyloid protein
Neutralization
Clearance

13
Ongoing Phase 1 Trial in AL Amyloidosis Evaluating Safety and Markers of Organ Response
– Evaluate hematologic response (dFLC) and organ response
(e.g., NT-proBNP, proteinuria and alkaline phosphatase)
– Evaluate the safety and tolerability of NEOD001
– Determine maximum tolerated dose or Phase 2/3 recommended
dose of NEOD001
– Evaluate the serum pharmacokinetics (PK) of NEOD001
– Assess immunogenicity of NEOD001
1 Secondary Objectives
Primary Objectives
Exploratory Objectives
2
Data as of 3/11/14, interim, unaudited data
14
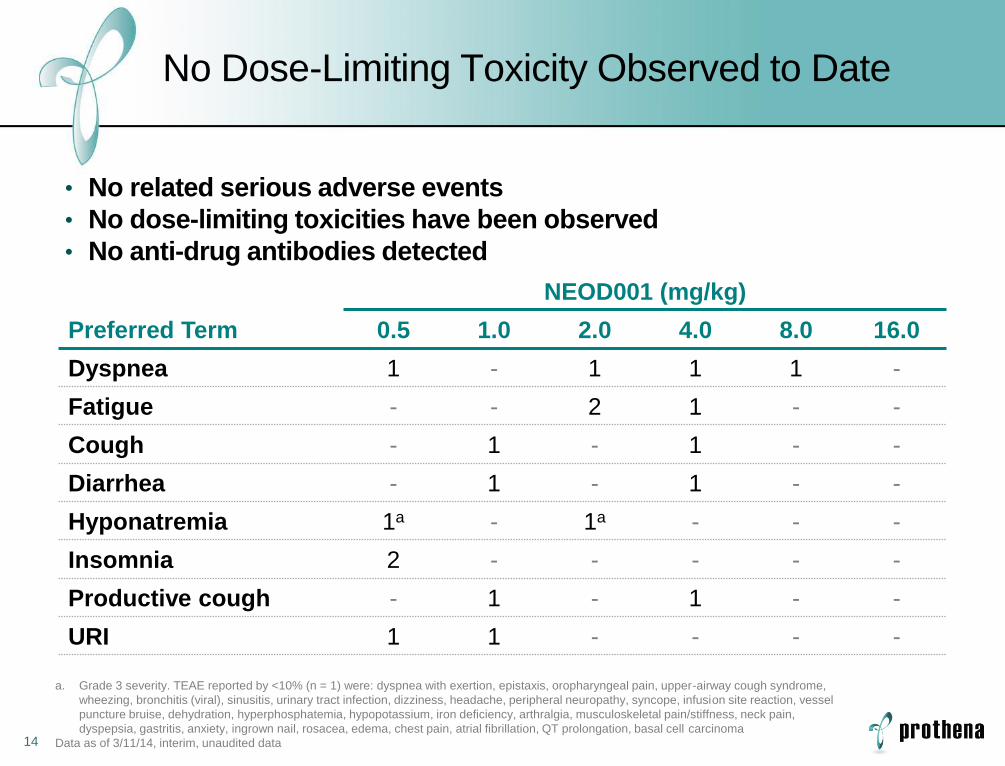
No Dose-Limiting Toxicity Observed to Date
Preferred Term
NEOD001 (mg/kg)
0.5 1.0 2.0 4.0 8.0 16.0
Dyspnea 1 - 1 1 1 -
Fatigue - - 2 1 - -
Cough - 1 - 1 - -
Diarrhea - 1 - 1 - -
Hyponatremia 1a - 1a - - -
Insomnia 2 - - - - -
Productive cough - 1 - 1 - -
URI 1 1 - - - -
a. Grade 3 severity. TEAE reported by <10% (n = 1) were: dyspnea with exertion, epistaxis, oropharyngeal pain, upper-airway cough syndrome,
wheezing, bronchitis (viral), sinusitis, urinary tract infection, dizziness, headache, peripheral neuropathy, syncope, infusion site reaction, vessel
puncture bruise, dehydration, hyperphosphatemia, hypopotassium, iron deficiency, arthralgia, musculoskeletal pain/stiffness, neck pain,
dyspepsia, gastritis, anxiety, ingrown nail, rosacea, edema, chest pain, atrial fibrillation, QT prolongation, basal cell carcinoma
Data as of 3/11/14, interim, unaudited data
• No related serious adverse events
• No dose-limiting toxicities have been observed
• No anti-drug antibodies detected

15
150
200
250
300
350
Pharmacokinetic Profiles Support 28-Day Cycle Across Dose Levels
Ser
um
NE
OD
001
Co
nce
ntr
atio
n, μ
g/m
L
Time, Days
Data as of 3/11/14, interim, unaudited data
0
10
20
30
40
50
28
0
50
100
150
0 7 14 21 28
0.5 mg/kg Cycle 1 (n=3) 0.5 mg/kg Cycle 3 (n=3)
1.0 mg/kg Cycle 1 (n=3) 1.0 mg/kg Cycle 3 (n=3)
2.0 mg/kg Cycle 1 (n=3) 2.0 mg/kg Cycle 3 (n=3)
4.0 mg/kg Cycle 1 (n=3) 4.0 mg/kg Cycle 3 (n=3)
8.0 mg/kg Cycle 1 (n=3) 8.0 mg/kg Cycle 3 (n=3)
16 mg/kg Cycle 1 (n=3)

16
-90
-60
-30
0
30
60
90
For Patients with Baseline NT-proBNP ≥650 pg/mL
Cardiac Biomarker Response/Progression Criteria1
No response or progression as defined
Decrease in NT-proBNP >30% AND >300 pg/mL
Increase in NT-proBNP >30% AND >300 pg/mL in patients
without progressive renal dysfunction
Response
Progression
Stable
30%
-30%
0
1. Comenzo RL, Reece D, Palladini G, et al. Leukemia. 2012;26:2317–25
Data as of 3/11/14, interim, unaudited data

17
NEOD001 Treatment Associated with High Rate of Cardiac Biomarker Response and Stabilization
N=18a
n=1, Progression (11%)
n=1, No Post-BL Data --
n=8, Response or Stable (89%)
a. 12 cardiac patients at diagnosis
Data as of 3/11/14, interim, unaudited data
N=10
N=18 n=6, No Cardiac Involvement (33%)
n=12, Cardiac Involvement (67%)
n=10
NT-proBNP ≥650 pg/mL
NT-proBNP <650 pg/mL
n=8
n=5, Response (56%)
n=3, Stable (33%)
At
Dia
gn
osis
P
er
Pro
toco
l

18
Highlights of Interim Phase 1 Data of NEOD001 in Patients with AL Amyloidosis
• Residual organ dysfunction following plasma cell dyscrasia treatment
remains a significant unmet medical need in patients with AL amyloidosis
• 18 patients in 6 dosing cohorts have received 106 cycles of NEOD001
in the ongoing Phase 1 study
• NEOD001 is safe and well-tolerated, with a PK consistent with dosing
every 28 days, and no hypersensitivity reactions or development of anti-
drug antibodies
• Of the 9 patients with a baseline NT-proBNP value ≥650 pg/mL and a
post-baseline NT-proBNP determination, 8 had cardiac biomarker
response or were stable
• Randomized, placebo-controlled Phase 2/3 study is warranted in
patients with AL amyloidosis who have cardiac involvement
Data as of 3/11/14, interim, unaudited data

PRX002 for Parkinson’s Disease (worldwide collaboration with Roche)

20
Parkinson’s is a Neurodegenerative Disease with No Approved Disease-Modifying Therapies
• Parkinson’s disease (PD) is the 2nd most common neurodegenerative
disorder
– Current treatments manage early symptoms, not disease
– There are an estimated 7-10 million Parkinson’s patients worldwide
– Genetic mutations cause early and aggressive disease
• Synuclein pathology strongly implicated in PD
– Also associated with other CNS and peripheral diseases, including some orphan indications
Synuclein is the predominant
component of Lewy bodies found
in Parkinson’s disease and other
synucleinopathies
21
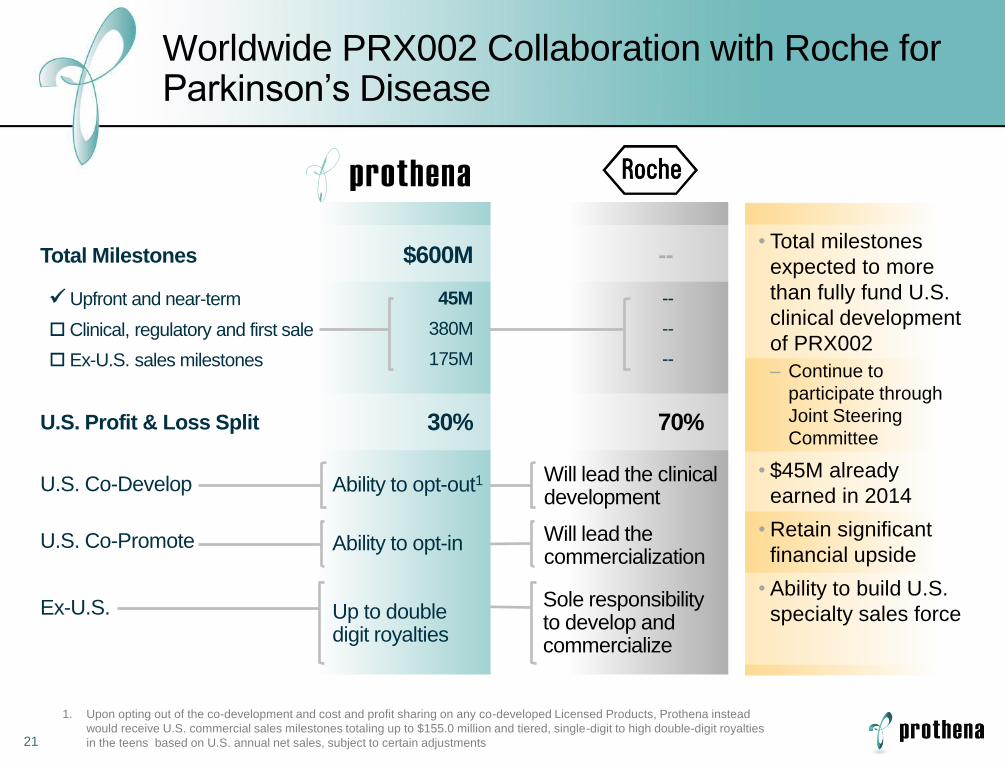
Worldwide PRX002 Collaboration with Roche for Parkinson’s Disease
Total Milestones $600M
Upfront and near-term
Clinical, regulatory and first sale
Ex-U.S. sales milestones
U.S. Profit & Loss Split
U.S. Co-Develop
U.S. Co-Promote
Ex-U.S.
45M
380M
175M
30%
Ability to opt-out1 Will lead the clinical development
Ability to opt-in Will lead the commercialization
Up to double digit royalties
Sole responsibility to develop and commercialize
--
70%
--
--
--
• Total milestones
expected to more
than fully fund U.S.
clinical development
of PRX002
– Continue to
participate through
Joint Steering
Committee
• $45M already
earned in 2014
• Retain significant
financial upside
• Ability to build U.S.
specialty sales force
1. Upon opting out of the co-development and cost and profit sharing on any co-developed Licensed Products, Prothena instead
would receive U.S. commercial sales milestones totaling up to $155.0 million and tiered, single-digit to high double-digit royalties
in the teens based on U.S. annual net sales, subject to certain adjustments

22
Synuclein Immunotherapy may Reduce Neuronal Toxicity and Prevent Cell-to-Cell Transfer
Synaptic Loss
and Pathogenic
Spread
Antibodies
Reduce
Pathogenic
Spread and
Decrease
Synuclein
Pathology
23
PRX002 Phase 1 SAD Study Underway
• Initiated Phase 1 SAD study in April 2014
• Initiate Phase 1 MAD study in patients with
Parkinson’s disease
• Biomarkers from CNS and periphery anticipated to
guide Phase 2 dose selection
• Potential development of follow-on antibodies for
other orphan synucleinopathies

PRX003 for Inflammatory Diseases and Cancers
25
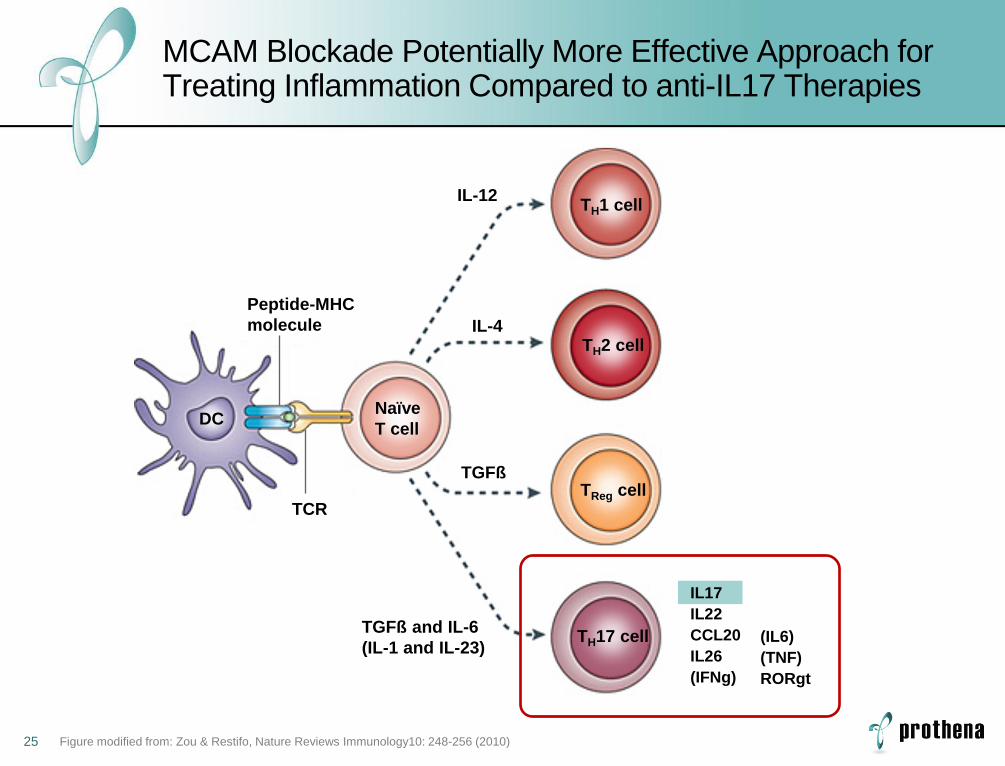
MCAM Blockade Potentially More Effective Approach for Treating Inflammation Compared to anti-IL17 Therapies
TH1 cell
TH2 cell
TReg cell
TH17 cell
IL-12
IL-4
TGFß and IL-6
(IL-1 and IL-23)
TCR
DC
Peptide-MHC
molecule
TGFß
Naïve
T cell
(IL6)
(TNF)
RORgt
IL17
IL22
CCL20
IL26
(IFNg)
Figure modified from: Zou & Restifo, Nature Reviews Immunology10: 248-256 (2010)

26
PRX003 Clinical Trial Expected to Initiate in 2015
• Lead candidate, PRX003, identified and
CMC initiated
• Announce initial indication(s)
• Expect to file IND and initiate Phase 1
trial(s) in 2015

Corporate Information

28
Financial Overview
SUMMARY INFORMATION
Cash and cash equivalents (March 31, 2014)1 $195M
Shares outstanding (April 25, 2014)2 21.9M
Full-time employees (December 31, 2013) 39
2014 GUIDANCE
Cash burn range3 $7 to $12M
Net loss range3 $13 to $18M
Projected year-end cash position (mid-point) ~$167M
1. Does not include $15M clinical milestone earned in 2Q14 from Dec-13 Roche collaboration
2. Does not include 2.4mm ordinary shares underlying options with a weighted average strike price of $12.19
3. Accounts for the $30M in upfront (1Q14) and $15M near-term clinical milestone (2Q14) from Dec-13 Roche collaboration

29
Upcoming Key Milestones
Timing Key Milestone Program
2013 PRX002 collaboration with Roche Parkinson’s Disease
2014 Initiate Phase 1 SAD trial of PRX002 Parkinson’s Disease
2014 Communicate interim data from ongoing Phase 1 trial of NEOD001 at ISA
AL Amyloidosis
2014 Initiate Phase 1 MAD trial of PRX002 Parkinson’s Disease
2014 Initiate Phase 2/3 trial of NEOD001 in 4Q14 AL Amyloidosis
2014 Communicate additional data from ongoing Phase 1 trial of NEOD001
AL Amyloidosis
2015 Initiate Phase 1 trial(s) of PRX003 Inflammation and cancers

Prothena Corporation plc June 3,
2014