protrusio acetabulipresentationgrafix.com/_dev/cake/files/archive/pdfs/645.pdf · 2015-02-22 ·...
TRANSCRIPT

105 Bulletin• Hospital for Joint Diseases Volume62,Numbers3&4 2005
Intrapelvicprotrusionoftheacetabulumwasfirstrecog-nizedbyOtto1in1824onadesiccatedspecimenfromtheNaturalHistoryMuseumofBreslauinPoland(Fig.
1).Ottooriginallydescribedtheabnormalityasbeinganimportantconsiderationinobstetricdeliveryandascribedhisfindingsto“anabnormalgout.”Todate,hehasremainedtheonlyauthortomakethisassociation.WhitereportedthefirstcaseintheBritishliteraturein1883.2Protrusioacetabulireceivedscantattentionuntiltheturnof19thcentury.Sincethen, this conditionhasbeen the subjectofmuchdebateregardingdiagnosis,etiology,andmanagement.Thisinwardprotrusionof theacetabulum is commonly referred to asOtto pelvis, protrusio acetabuli, or arthrokatadysis (fromancientGreek:literallymeaningsubsidenceofajoint).ThetermOtto-ChrobakpelviswasusedforanumberofyearsafterEppingeraddedthenameofaProfessorChrobakasabirthdaytribute.3However,Chrobak’snamewasdroppedashehadnoconnectionwiththecondition.
Historical ConsiderationsOtto described the macroscopic appearance of theacetabulum and head of femur as being “smooth and
polishedwithalossofthecartilagecover.”Eppinger,in1903,reportingonfoursimilarpelvicspecimens,sug-gestedthatthedeformityresultedfromadisturbanceofgrowthaffectingthedelayedossificationofthetriradiatecartilage.Thecontinuedpressurefromthefemoralheadwasthensufficienttocausetheprotrusion. Over the following 30 years, a number of authorspublishedreportswhichsuggestedavarietyofalternativepathologies.Kuliga(citedinPomeranz4)andSchertlin5favoredan“osteo-arthritisdeformans,”whileHertzler,6Pomeranz,4andLewin(citedinPomeranz4)describedan“osteoarthriticprotrusionoftheacetabulum.”Infectionwasalsoidentifiedasapossiblecause,withtuberculo-sis,gonorrhea,andsyphilisbeing themostcommonlyreportedconditionsresponsible.Streptococcus,staphylo-coccus,andechinococcuswerealsoidentifiedindiseasedhips.4,7
In 1929, Doub8 found 50 cases of protrusio with awide variance of opinion as to the exact etiology. Hefailedtoidentifyanyoneetiologicalfactorandsuggestedthatthemostlikelyexplanationwasthatsomegeneraldiseaseinearlylifecausingsofteningofthebonesledtothedeformity,withosteoarthritisalaterstageintheprocess. Pomeranz,4 in 1932, identified 79 cases, acceptedthatitwasincorrecttoseekonecommonetiology,anddescribed twomaingroupsofpatients.Onegroupde-velopedprotrusiosecondarytoinfection.Inthesecondgroup, the protrusio was associated with generalizedosteomalacia. Schaap9andGolding,10in1934,agreedwithPomer-anz’shypothesisandincludedafurthergroupconform-ing with Eppinger’s opinion that, in some, a growthdisturbance primarily initiated the deformity. Schaapalsocomparedpatientsinthisgroup,whoweremostlyfemalesandinwhomtheconditiontendedtobebilateral,
Protrusio Acetabuli
Colin C.R. Dunlop, M.R.C.S., Charles Wynn Jones, F.R.C.S., and Nicola Maffulli, M.D., M.S., Ph.D., F.R.C.S.(Orth.)
ColinC.R.Dunlop,M.R.C.S.,isaSpecialistRegistrarinTraumaandOrthopaedicSurgery,DepartmentofOrthopaedicsandTrauma,Tayside University Hospitals NHSTrust, Ninewells Hospital,Dundee,Scotland.CharlesWynnJones,F.R.C.S.,isaConsultantOrthopaedic Surgeon, Department ofTrauma and OrthopaedicSurgery,KeeleUniversitySchoolofMedicine,StokeonTrent,England. Nicola Maffulli, M.D., M.S., Ph.D., F.R.C.S.(Orth.),isaProfessorofTraumaandOrthopaedicSurgery,DepartmentofTraumaandOrthopaedicSurgery,KeeleUniversitySchoolofMedicine,StokeonTrent,England.Correspondence: Nicola Maffulli, Department ofTrauma andOrthopaedicSurgery,KeeleUniversitySchoolofMedicine,NorthStaffordshire Hospital,Thornburrow Drive, Hartshill, Stoke onTrent,Staffordshire,ST47QB,England.

106 Bulletin• Hospital for Joint Diseases Volume62,Numbers3&4 2005
withpatientswithdevelopmentaldysplasiaofthehip.9 The suggestion of more than one etiology for theconditionbecamewidelyaccepted,with theexceptionofRechtman11who,in1936,suggestedthatall casesofprotrusio had an initially “too deep” acetabulum as acongenitaldeformity. Overgaard,12 in 1935, first distinguished betweenprimary and secondary protrusio. He subdivided theprimarygroupintothosewithosteo-asthenic protrusionandthosewithosteo-arthriticprotrusion.Thesecondarygroup showed evidence of a destructive inflammatoryprocessinthejoint. Gilmour,13 in 1939, further simplified this classifi-cation so that theprimarygroupcontainedonly thosepatients in whom no other underlying pathology wasdemonstrable, while subjects in the secondary groupdevelopedprotrusioasaresultofanyunderlyingpathol-ogy.Thisistheclassificationusedtoday.
EtiologySecondary ProtrusioThecausesofsecondaryprotusioacetabuliarenowwelldocumented(Table1).Inmostsubjectswithsecondaryprotrusion,theprogressionofthedeformitycanbeex-plainedintermsoftheunderlyingcondition. Wherethereisadestructiveprocess,suchasinfection,thefemoralheadwillmigrateaxially,closetothelineof
thejointreactionforceasthebonysubstructureisweak-ened.Similarly,ininflammatoryconditions,migrationwilloccurduetoincreasedboneturnoverunderload.Thejointreactionforceactsat69°fromthehorizontal14andmigrationof the femoralhead inprotrusiooccurs justmedialtothisat65°.15
Conditions which weaken the bone matrix, eitherlocally,suchasradiationinducedosteonecrosis,orglo-bally,suchasPaget’sdisease,willalsoallowthefemoralhead to migrate superomedially under normal loadingconditions. However,thesesimpleexplanationsdonotexplaintheprogressionoftheconditioninalltherecognizedcausesofsecondaryprotrusio.OneexampleistheoccurrenceofthedeformityinMarfan’ssyndrome.Marfan’ssyndromeiscausedbyadefectinthefibrillin1gene.Thisdefectgivesrisetocardiovascular,skeletal,ocular,pulmonary,integument,andduralabnormalities.Theskeletalmani-festationsofMarfan’ssyndromearebestexplainedbyovergrowthofthelongbonesasopposedtoaweaknessintheirstructure.Alackofnormalfibrillinintheperios-teummightgivelessrestrictiontolongitudinalgrowth,and subsequent overgrowth occurs due to this lack ofnegative feedback.16 To simply attribute the protrusiointhesepatientstoaweaknessintheacetabularfloorisunfounded.Itwouldbeequallylikelytoresultfromthegrowthdisturbancewhichgivesrisetotheotherfeatures.Thishypothesiswouldsupportapossibledevelopmental
Table 1 EtiologyofSecondaryProtrusioAcetabuli
Infection Gonococcus Echinococcus Tuberculosis Syphilis Streptococcus Staphylococcus Inflammatory RheumatoidArthritis Spondyloarthritides IdiopathicChondrolysis Metabolic Paget’sDisease Osteomalacia Hyperparathyroidism Genetic OsteogenesisImperfecta Acrodysostosis MarfanSyndrome Ehler-DanlosSyndrome Trisomy18 SticklerSyndrome Neurofibromatosis SickleCellDisease TrichorhinophalangealSyndrome Homocystinuria Neoplastic PrimaryNeoplasm(e.g.,Hemangioma) MetastaticDisease RadiationInducedOsteonecrosis Trauma AcetabularFracture
Figure 1LithographofpelvicspecimenoriginallydescribedbyAWOttoin1824.Hisdescriptionisasfollows:“Thispelviswithaglobularextendedacetabulumofanadultwomanhasanormalsizeandshapeingeneral.Thespecialfeatureisthatbothheadsoffemurreachquitedeepintotheacetabulum,thefloorsofwhichextendintothepelviccavity,andtheyshowanimperfectankylosis…Duetotheextensionoftheacetabulumintothepelvis…notonlytheheadofthefemurbutalsotheneckofthefemurareprojectedintotheacetabulumandthegreatertrochanterisarticulatingwiththeupperpartoftheedgeoftheacetabulum.”(Reproducedwithkindpermissionfrom:SteelHH:Protrusioacetabuli:itsoccurrenceinthecompletelyexpressedMarfanSyndromeanditsmusculoskeletalcomponentandaproceduretoarrestthecourseofprotrusioninthegrowingpelvis.JPediatrOrthop1996;16:705)

107 Bulletin• Hospital for Joint Diseases Volume62,Numbers3&4 2005
etiologyinsomeprotrusionpatients.
Primary ProtrusioPrimaryprotrusioacetabuliremainsadiagnosisofexclu-sion,andassuchmanyofthecasesreportedinthepastmayhaveinfactbeensecondarytoundiagnosedcondi-tions. In thesearchforanetiologyresponsiblefor theprimaryprotrusiogroup,mostinvestigatorshavereferredtothemechanismsresponsibleforsecondaryprotrusio.Thus,thepossibleetiologieshavebeenconsideredunderthefollowingthreeheadings:
1. Aninflammatoryordestructiveconditionofthehipjoints;
2. Aqualitativedeficiencyofacetabularbone;and
3. Adevelopmentalabnormalityorgrowthdisturbance.
Clinical FeaturesTheconditionpresentsinthreemainagegroups17:pa-tientspresentingintheirteens,thosepresentingbetween35and50years,andthosepresentingbetween51and85years.Thisdivisionwasbasedonagraphicalrepresenta-tionoftheageatpresentationin59patients.Whilethereisadefinitepeakintheyoungerpatients,18-21divisionofthe lateronsetpatients into twodistinctgroups is lesswell-defined. Inyoungerpatients,thediagnosisofprotrusioisoftenoverlooked,asitisunusualforanyfeaturesofdegenera-tivechangetobepresentatthisstage.Theconditioninthisagegroup,althoughproducingtheassociatedsignsandsymptomsofprotrusio,oftenlacksthestrikingradio-graphicalappearanceseeninlaterlife.18Belowtheageof25,osteoarthriticstigmataareminimal.Abovethisage,thedegreeofosteoarthriticchangescorrelatespositivelywiththeageofthepatient.22Theyoungerpatientspresentwhensymptomsarisefromtheanatomicalabnormality.Theolderpatients, instead,presentwhendegenerativechange occurs secondary to this abnormality. This isin agreement with Gilmour’s13 belief that there was aprimaryphaseinwhichthedeformityexistedinanun-complicatedstate,butthatitwasmoreoftendiscoveredwhenosteoarthritisorotherchangeshadset in. In theelderlypatientsstudiedbyHooperandJones,protrusiowas invariably accompanied by osteoarthritis,17whichinitselfisacauseofsecondaryprotrusio.Bythetimethatthegrosschangesofosteoarthritisaremanifest,itisimpossibletodistinguishthoseinwhomtheprotrusioresultsfromosteoarthritisfromthoseinwhomthepro-trusiopre-datedthedegenerativechanges. There is a marked female to male preponderance.Scandalisandcolleagues23reportedtheincidenceaccord-ingtosexof85%female(35outof41patients).Gilm-our13foundasimilarratioof30femalesto7males. The condition is characteristically bilateral.22,24 In
Overgaard’s12reviewin1935,35of44patientshadbilat-eralprotrusio.Oftheninepatientsreportedasunilateral,sixhadanabnormallydeepenedcontralateralacetabu-lum. Details of the contralateral hip of the remainingthreewereunavailable. Rechtman11firstsuggestedahereditarypatterninthreeofthefivepatientshedescribed.Thiswassuggestedfromhistoryalone,withtheprobandsreportingasimilarfunc-tionaldisabilityinmembersoftheirimmediatefamilies.Rechtmanwasunabletoaccesstheotherfamilymemberstoconfirmthisradiographically.Sincethen,thisfamiliallinkhasbeenconfirmedradiographicallybyanumberof investigators25-29 andhas alsobeendemonstrated inidenticaltwins.30Thesuggestedpatternsofinheritancehave been in accordance with an autosomal dominantgenewithincomplete27orcomplete29penetrance. There is also a racial influence on the condition,31withagreatlyincreasedincidenceintheBantuwomeninNatal.PelvicradiographsofpregnantBantu,Indian,andEuropeanwomenreferredforpelvimetrywerecom-pared.The incidenceofprimaryprotrusioacetabuli inthesegroupswas25.7%(58outof226),5.7%(6outof105),and2.9%(3outof105),respectively. In1939,Gilmour13reportedanabnormal“rhythmofadolescentdevelopment” inpatientswithprotrusio. Inanumberofhispatients,thesignsandsymptomsofthedeformityhadprecededmenarche,andthesegirlsshowedacceleratedepiphysealgrowthandfusionpriortothis.Friedenberg,32 in a report of two patients, commentedthat one of them experienced menarche at 9 years ofage and that both had experienced early fusion of theepiphyses. With theexceptionof twopatientswhohadrepeat-edlyelevatedcalciumlevelsintheseriesbyHooperandWyn Jones,17 all the patients reported showed normalbiochemistry.Anabnormalitymay indeedexist,but itmaybe too subtle tobedetectedby routine screeningmethods. Shoreandassociates21describedthehistologicalap-pearanceofbiopsyspecimensfromjuvenilepatientsasshowingasignificantbutnon-diagnosticinflammatoryreaction. Specimens from arthroscopic examinationshoweddegenerativechangeswithfibrocartilagereplace-ment.WroblewskiandHillman33performedhistologicalexaminationonspecimensoftheacetabularfloorfrompatientswiththefeaturesofidiopathicprotrusiounder-going total hip arthroplasty. The marrow spaces werereplacedwithactivevascularfibrousgranulationtissuewithdisruptionofthetrabecularpatterninsomeareas. Typically, patientswithprimaryprotrusio acetabulipresent with increasing stiffness rather than pain. Of-ten,stiffnesshasbeennoticedinadolescence.Historiesfrom the various series include one young lady whonoticedthatshecouldnotsitcrossleggedonthefloorand another who found that she lacked hip flexibility
108 Bulletin• Hospital for Joint Diseases Volume62,Numbers3&4 2005
while attempting gymnastics at school. Of those whopresentlaterwithsymptomsofsecondarydegenerativechange,closequestioningoftenrevealssimilarhistoriesofprecedinglimitationsofmovement.Deepeningoftheacetabulumleads topainful limitationofabductionasthe femoral neck impinges on the superior acetabularmargin.Thepainispresumedtoarisefromsynovialstruc-turesinthisregion.34Furtherprogressionleadstoadductorspasm,andfixedflexiondeformitiesdevelop.Thereisoftenhyperlordosisofthelumbarspinewhichcompensatesforthefixedflexiondeformitiesatthehips.Untreated,thepatientultimatelydevelopsankylosisoftheaffectedhip.
Radiological FeaturesTheterm“ProtrusioAcetabuli”simplyreferstothepro-trusionoftheacetabulumintothelesserpelvis,andthisoccurstovaryingdegrees.Itiscommonlyreportedasachronicprogressivedeformity.Brailsford,18followingtheprogressofthedeformityinyoungpatients,concludedthat theonsetof theconditionwasininfancyandthatthedeformityfollowedaslowlyprogressivecourse.Inthe same year, however, Friedenberg19 suggested that,althoughtheprotrusionoccurredatayoungage,itdidnotalwayscontinuetoincrease.Heprovidedevidenceforthisstatementwithoneofhisownpatientsashavingnoprogressionofdeformitybetweenradiographstakenat31yearsand39years.HealsopointedoutthatSchaap9andGolding10hadbothfollowedupfemalesof45and40yearsofage,respectively,forfiveyearswithnopro-gression of acetabular protrusion. Hubbard,35 in 1969,describinghisfindingson27patientswithprotrusion,confirmedthatnoteverycaseofprotrusiowasprogres-sive.Inhisseries,20hipsin15patientsprogressedbyanaverageof6mminameanof8.4years,10hipsinsixpatientshadnoprogressioninatimerangingfrom1to10years,and10hipsinsixpatientsactuallyshowed
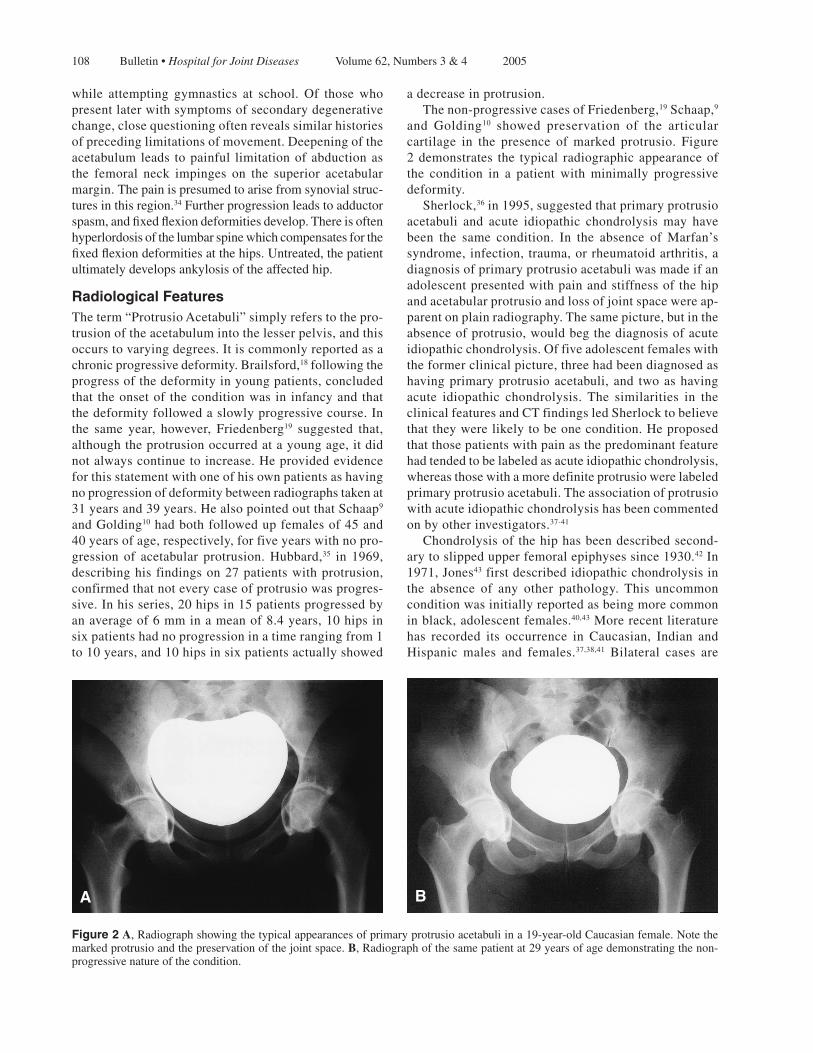
adecreaseinprotrusion. Thenon-progressivecasesofFriedenberg,19Schaap,9and Golding10 showed preservation of the articularcartilage in the presence of marked protrusio. Figure2demonstrates the typical radiographicappearanceofthe condition in a patient with minimally progressivedeformity. Sherlock,36in1995,suggestedthatprimaryprotrusioacetabuli and acute idiopathic chondrolysis may havebeen the same condition. In the absence of Marfan’ssyndrome,infection,trauma,orrheumatoidarthritis,adiagnosisofprimaryprotrusioacetabuliwasmadeifanadolescentpresentedwithpainandstiffnessofthehipandacetabularprotrusioandlossofjointspacewereap-parentonplainradiography.Thesamepicture,butintheabsenceofprotrusio,wouldbegthediagnosisofacuteidiopathicchondrolysis.Offiveadolescentfemaleswiththeformerclinicalpicture,threehadbeendiagnosedashavingprimaryprotrusioacetabuli,and twoashavingacute idiopathic chondrolysis. The similarities in theclinicalfeaturesandCTfindingsledSherlocktobelievethattheywerelikelytobeonecondition.Heproposedthatthosepatientswithpainasthepredominantfeaturehadtendedtobelabeledasacuteidiopathicchondrolysis,whereasthosewithamoredefiniteprotrusiowerelabeledprimaryprotrusioacetabuli.Theassociationofprotrusiowithacuteidiopathicchondrolysishasbeencommentedonbyotherinvestigators.37-41
Chondrolysisofthehiphasbeendescribedsecond-arytoslippedupperfemoralepiphysessince1930.42In1971,Jones43firstdescribedidiopathicchondrolysisinthe absence of any other pathology. This uncommonconditionwasinitiallyreportedasbeingmorecommoninblack,adolescentfemales.40,43Morerecentliteraturehas recorded its occurrence in Caucasian, Indian andHispanic males and females.37,38,41 Bilateral cases are
Figure 2A,Radiographshowingthetypicalappearancesofprimaryprotrusioacetabuliina19-year-oldCaucasianfemale.Notethemarkedprotrusioandthepreservationofthejointspace.B,Radiographofthesamepatientat29yearsofagedemonstratingthenon-progressivenatureofthecondition.
BA

109 Bulletin• Hospital for Joint Diseases Volume62,Numbers3&4 2005
exceptional.Theradiographicfindingsinacuteidiopathicchondrolysisshowagloballossofarticularcartilageonthefemoralheadandacetabulum. In the juvenile groupof patientswithprimarypro-trusioacetabuliofHooperandWynJones,17malesandfemaleswereequallyaffected.Insome,thesymptomsprogressedrapidly,becomingincapacitating.Therefore,intheyoungeragegroup,acuteidiopathicchondrolysisandprimaryprotrusioacetabulimaywellbetwodistinctpathologies thataredifficult toseparateat the timeofpresentation.Inacuteidiopathicchondrolysis,thechon-drolyticprocesscausesgloballossofarticularcartilageandsecondaryprotrusiodevelops.Thisgroupcontainsamoreevenmaletofemaleratioandtheprocessisoftenunilateral.Inprimaryprotrusioacetabuli,theprotrusiodevelops with sparing of the articular cartilage. Thisgrouphasthecharacteristicfemalepreponderanceandbilateraldeformity.Otherinvestigators7,44haveincludedacuteidiopathicchondrolysisintheirlistsofcausesofsecondaryprotrusioacetabuli. Several investigators have disagreed with Otto’sdescriptionofhisoriginal specimenashaving“anor-mal size and shape ingeneral.”Overgaard12describeda typical “clover leaf” appearanceon radiographs andseveralotherinvestigatorsfoundawidenedintercristaldistance on anteroposterior pelvic radiographs.13,22,30Alexanderalsodemonstratedthattheratiobetweentheintertuberousdistanceandtheintercristalmeasurementwas lower inpatientswithprimaryprotrusioacetabuliandhigherinpatientswithdevelopmentaldysplasiaofthehip.22Littlefurtherworkhasbeenpublishedinthisarea.Thisfindingcouldbeexplainedbyforwardtiltingofthepelvisduetofixedflexiondeformityatthetimeofradiography,but,toourknowledge,todatethiseffecthasnotbeeninvestigated. Coxa vara and decreased femoral anteversion havebeenlinkedwithprimaryprotrusioacetabuli.22,45Hooper17evaluatedthefemoralneck-shaftangleintheirpatients:allmeasurementswerewithinthenormalrange,averag-ingbetween123°and127°.Tonnis,45inacomprehensivereviewoffemoralandacetabularanteversion,foundthatprimary protrusio acetabuli was associated more withincreasedfemoralandacetabularanteversionratherthanretroversion,butheincludedtoofewpatientstodrawanydefinite conclusions. It would certainly seem unlikelythat there isanymarkedrelationshipbetweenprimaryprotrusio acetabuli and either coxa vara or decreasedfemoralanteversion. With these clinical and radiographical features, theetiologyofprimaryprotrusioacetabuliwouldmostlikelybedevelopmental.Abilateralconditionaffectingonlytheacetabula,withpreservationofthearticularcartilageandnormal inflammatorymarkers, isunlikely tohavean inflammatoryordestructiveetiology.Likewise, thenon-progressivenatureoftheacetabulardeformity,the
normalbiochemicalprofile,andthelackofothersitesaffected would make a qualitative deficiency of boneunlikely. Currently, two hypotheses exist regarding adevelopmentaletiology:
1. Adisturbanceofgrowthmayleadtoadelayinos-sification of the triradiate cartilage.3 Subsequentstressesontheunfusedepiphyseswouldproducethedeformity.
2. The converse of this might be the case: abnormalaccelerationofepiphysealossification in thepelvisreplacing the triradiatecartilagewithnew,vascularandplasticbone that allowsmoldingunderweightbearing.13
Alexander22showedthatadegreeofprotrusiowasnormalinchildren.Hedescribeda“beaking”ofthetriradiatecarti-lagewhichisatamaximumateightyearsofageandwhichsubsequentlyremodels.Healsosuggestedthatacceleratedepiphysealclosuremayleadtopreservationofthisphysi-ologicalprotrusiothatthenfailedtoremodel. Experiments on rabbits have shown, however, thatpremature surgical fusion of the triradiate cartilageleadstoathickmedialacetabularwallwithprogressiontosubluxationofthehip.46,47Thisfindinghasalsobeendemonstrated in children following acetabular frac-tures.47-49Prematureclosuresuspectedtobetheresultofsepticarthritisofthehiphasalsobeenreported50withsubsequentsubluxation.Surgicalclosureofthetriradiatecartilagehasalsobeendescribedasaneffectivetreatmentinarresting thedevelopmentofprotrusio in skeletallyimmatureMarfan’spatients.51,52SteelrecommendsthisprocedureinchildrenwithMarfan’swhoarebetweentheagesof8and10yearsandwhohavedocumentedpro-gressionofacetabulardeepening.Thisevidencewouldimplythatearlyepiphysealclosureleadstoashallow,dysplastic acetabulum rather than protrusio.Any linkbetweenlateepiphysealclosureandabnormalacetabulardevelopmenthasyettobedocumented.
Radiographic DiagnosisTheterm“protrusioacetabuli”simplyreferstothepro-trusionoftheacetabulumintothelesserpelvis.ThiswasfirstdemonstratedradiographicallybySchertlinin1910.5Grossexamplesoftheconditionareobviousonstandardantero-posteriorradiographsofthepelvis,withtheout-lineoftheacetabulumextendingbeyondtheiliopectinealline.Sotelo-GarzaandCharnley53gradedthedeformityin these patients.The distance between the projectionoftheuppermarginofthesuperiorpubicramusandtheoutlineoftheacetabulumprotrudingintothepelvis wasestimated,givingthreegradesofprotrusio.
GradeI(mildprotrusio)measured1to5mm; GradeII(moderateprotrusio),6to15mm;and GradeIII(severeprotrusio),morethan15mm.

110 Bulletin• Hospital for Joint Diseases Volume62,Numbers3&4 2005
Atearlierstagesintheprogressionoftheconditionthediagnosisisnotalwayssoapparent.Asaresult,variousradiographiccriteriahavebeenusedtotrytoidentifythemostconsistentmethodofdiagnosis.Beforethesemeth-odsaredescribed,ithastobestressedthatinaconditionsuchasprotrusio,wheretherangeofdeformityextendsalongacontinuumfromnearnormaltogrosslyabnormal,anyvaluechosenisnecessarilyarbitrary. Thethreemostwidelyusedcriteriaarethecenter-edgeangleofWiberg,54thedistancebetweenthemedialwalloftheacetabulumandKohler’s55ilioischialline,andtheconfigurationoftheteardrop. Thecenter-edgeangle,originallydescribedtodiag-nosedevelopmentaldysplasiaofthehip,54 isshowninFigure3A.Ananglelessthan20°wastakenasdiagnos-ticofdevelopmentaldysplasiaofthehip,andananglegreaterthan46°asdiagnosticofprotrusio.“Greyareas”probablyliebetween20°and25°,and40°and46°,withanormalrangebetween25°and40°.Someinvestigatorshavesupportedtheuseofthisangle,19,27butothershavefounditunreliableinthediagnosisofprimaryprotrusioacetabuli.17,22,56,57Freidenburg19andMacDonald27foundcenter-edgeanglesgreaterthan50°andashighas90°inradiographsofobviousprotrusion.Armbuster,57inananatomicalstudyoftheadulthip,foundnocorrelationbetween the center-edge angle and either the teardropconfigurationorthedistancebetweentheacetabularlineandtheilioischial line.Healsofoundawiderangeofvalues,ashighas59°,inthenormalpopulation. Sharp57observedseverallimitationsofthecenter-edgeangle.Thecenterpointofadeformedfemoralheadisdifficulttolocate,andsubluxationorsimplelossofjointspace of either hip leads to inaccurate measurements.These patients also develop superolateral osteophytesthat make identification of the superolateral edge dif-
ficult. Therelationshipoftheacetabularline,representingthemedialwalloftheacetabulum,toKohler’silioischialline,hasalsobeenusedbyseveralinvestigators(Fig.3B).Alexander,22asoneofhisdiagnosticcriteria, requiredthefemoralheadtoreachKohler’sline.Headmittedthathiscriteriaweretoorigidandleadtounder-diagnosis.Hubbard35requiredtheacetabularlinetocrosstheiliois-chiallineaspartofhisdiagnosticcriteria.InaseriesbyArmbusterandcoworkers,56however,inwomentheac-etabularlinecrossedtheilioischiallinebyanaverageof1mminthenormalpopulation,andinmen2mmlateralto it.They recommended thatadiagnosisofprotrusiobemadeiftheacetabularlinecrossedtheilioischiallineby3mminmenandby6mminwomen.Intheirhands,thismeasurementwasreliableevenwithminordegreesofrotation,astheyconsideredboththesestructurestobecentrallyplaced.Goodmanandcolleagues,58however,radiographeddriedpelvicspecimenswhileseriallysec-tioningandreamingthespecimens.Theydemonstratedthat,whiletheteardropwasaconsistentrepresentationofthemedialandlateralwallsoftheflooroftheacetabulumjustabovetheobturatorforamen,theilioischiallinewasaprojectionofaportionofthequadrilateralsurfacepos-teriortotheacetabulum.Thus,theseparationofthetwolineswouldbesensitivetorotationofthepelvisatthetimeofradiography.Theysuggestedthat,astheteardropwasaconsistentfinding,aCartesiancoordinatesystembasedonthisstructureshouldbeusedfordiagnosisandchartingprogression.ThissuggestionhasbeenfurtherreinforcedbyGates and associaties,59 and is useful tochartprogressionofthecondition. TheappearanceofKohler’s“teardrop”figurehaslongbeencommentedonwithregard toacetabulardeepen-ing. In 1935, Overgaard12 noted that inversion of the
Figure 3A,Center-edgeangleofWiberg.Alinepassingthroughthecentersofbothfemoralheadsisconstructedasabaseline.Twofurtherlinesaredrawnfromthecenterofthefemoralhead,oneperpendiculartothebaselineandonetangentialtothesuperolateralmarginoftheacetabulum.Thecenter-edgeangleismeasuredbetweenthesetwolines.B,DistancebetweentheacetabularlineandKohler’silioischialline(arrows).
A B

111 Bulletin• Hospital for Joint Diseases Volume62,Numbers3&4 2005
“pear-figure”(teardrop)representedadeepeningoftheacetabulum. The various appearances of the teardropareshowninFigure4.ThedefinitionsshownarethoseemployedbyArmbusterandcolleagues.56Alexander,22HooperandJones,17andHubbard35allusedthecross-ingoftheteardropasoneoftheirdiagnosticcriteriaforprotrusio. However,Armbuster56 showed that this ap-pearanceisalsoverysensitivetopelvicrotation.Kohlerhimselfdemonstratedthisvariabilityonpoorlycenteredfilms.55
In the absence of a proven “standard” diagnosticcriterion,itisimpossibletoseparatenormalhipsfromthosewithanabnormalprotrusion.Onemustthereforebecarefulinwhatconclusionsaredrawnfromcompari-sons between different proposed diagnostic measures.Theevidencewouldsuggestthatpatientswithprotrusiodemonstratehighcenter-edgeanglesabovethereportednormalrange.However,thismeasurementisunhelpfulindiagnosisduetoitslackofspecificity.Toovercomethese inaccuracies57 the inter-teardrop line should beusedasthebaselineratherthanthecenter-centerlineinthismeasurement.Boththeappearanceoftheteardropandtheseparationoftheacetabularandilioischiallinesarehelpful indiagnosis,providedthatcare is takentoensureaccuratecenteringof films.Theonlymeasure-mentmethodthatwouldeliminatetheeffectofrotationwouldbetouseCartesiancoordinateswiththeoriginatthetipoftheteardrop. Severalotherindicesofacetabularmorphologyhavebeen described in the investigation of developmentaldysplasiaofthehip.Theseincludetheacetabularindexor sourcil angle, the acetabular inclination angle, andthe acetabular depth-to-width index. Murphy and co-workers60assessedtheusefulnessof thesevariablesasprognosticindicatorsindevelopmentaldysplasiaofthe
hip.Thesourcil tends tobeconcaveinferomedially inprotrusion,12 givinganegative acetabular index.Apartfromthisobservation,noworkhasbeencarriedoutusingthesemeasurementsinagroupofprotrusiopatients.
ManagementThemanagementoptionsforprimaryprotrusioacetabulihavebeenrecentlyreviewed7(Table2).Themostappro-priatetreatmentisbasedontheageandskeletalmaturityofthepatient,thedegreeofprotrusio,andtheextentofdegenerativechangesinthejoint. Inskeletallyimmaturepatients,surgicalfusionofthetriradiate cartilage has been proposed.7 Steel52 recom-mendsthisprocedureinMarfan’sSyndromefollowinghis resultsonaseriesof22patients,as thesecondaryprotrusio thatdevelops isprogressive.Atpresent, it isnotpossibletoanticipatewhichcasesofjuvenileprimaryprotrusioacetabuliwillprogressandwhichwillfollowamoreindolentcourse.Therefore,theuseofthispro-cedureinprimaryprotrusioacetabulicurrentlyremainsunclear. Inthetimepredatingtotalhiparthroplasty,surgicalmanagementoftheconditionincludedresectionarthro-plasty,arthrodesis,andacetabuloplasty.34Acetabuloplastywithresectionoftheanteriorwalloftheacetabulumwasperformedforthefirsttimeona55-year-oldfemalewithbilateralprotrusiotoremovetheareaofimpingementthat
Figure 4Variationinappearanceoftheteardrop.
Table 2 OperativeProceduresforProtrusioAcetabuli
Arthrodesis ExcisionArthroplasty TotalHipArthroplasty Acetabuloplasty ValgusIntertrochantericOsteotomy SurgicalClosureofTriradiateCartilage

112 Bulletin• Hospital for Joint Diseases Volume62,Numbers3&4 2005
gaverisetoherpainfulsymptoms.Thepatientwasabletoreturntoworkasahousekeeperfourmonthslater.Atthetimeofpublicationtheprocedurehadbeenusedon11patients.Eightofthesewereperformedfor“malumcoxaesenilis,”twoforoldslippedcapitalfemoralepiphy-sis, and theoriginalprocedurewasperformed foronepatientwithprimaryprotrusioacetabuli.Nolong-termfollow-upstudyhasbeenpublishedonthisprocedure,although a similar acetabuloplasty or “rimectomy” isstillbeingperformedinsomecenters(C.Wynn-Jones,personalcommunication). Thetwomostwidelyusedoperativeproceduresforprimaryprotrusioacetabuliarevalgusintertrochantericosteotomy and total hip arthroplasty. Pauwels61 firstdescribedvalgusintertrochantericosteotomyforuseinprotrusio hips, and reasoned that the procedure led tomorecranialresultantforcesatthehipjoint,thusreduc-ingthepressureontheflooroftheacetabulum.Theotherbeneficialeffectoftheprocedureisthatitreducestheimpingement at the superior acetabular margin. Sincethen,severalinvestigatorshavereportedexcellentresultsin selected patients following valgus intertrochantericosteotomy,withthebestresultsinyoungerpatientswithminimalarthriticchangeinthehipjoint.62Inastudywitheightoperatedhipsinsixpatientsandamaximumfollowupof5years,theresultsweregoodexceptfor1patient,whowas49yearsoldatthetimeofoperationandhadmoderate arthritic changes visible radiographically.63McBrideandassociates7 reportedon19hipsoperatedonin12patientswithanaveragefollowupof7.2years.Goodtoexcellentresultsweredocumentedin12hipsinpatientsagedbetween21and33years.Poorresultswerenotedinfivehipsinthefourpatientsaged42andover.McBride and associates concluded that this procedureshould not be performed on patients over 40 years ofageor inwhomsignificantdegenerativechangeswereevidentonplainradiographs.7Ofthesevenpatientsinthepersonalseriesoftheauthorsofthisarticle,threeover40yearsofagewereoperatedonandalloftheseachievedagoodorexcellentresultatanaveragefollowupof5.3years.Noneofthesepatientshadsignificantdegenerativechangesevidentintheirpreoperativeradiographs. Inolderpatientsorinpatientswithsignificantdegen-erativechanges,thebestoperativeprocedureforprimaryprotrusioacetabuliistotalhiparthroplasty.Sotelo-Garzaand Charnley53 demonstrated no significant differenceinoutcomein totalhiparthroplastyperformedon253protrusiohipscomparedwiththoseperformedonnon-protrusiohips.Theimportanceofreplicatingtheoriginalanatomyofthehipjointhasbeenstressed.Ranawatandcoworkers64 demonstrated cement-bone demarcationaroundtheacetabularcupinallthreezones,asdescribedby DeLee and Charnley,65 in 16 of 17 hips positioned1cmormorefromtheanatomicalposition.Failureofacetabularprosthesesmalpositioned to thisdegreehas
been further confirmed by Gates and colleagues59 andBayleyandassociates.66Crowninshieldandcoworkers67performed finite element analysis on various types ofprosthesis when positioned anatomically or with me-dialdisplacement.Highermedialstressesresultedfrommedialplacementoftheacetabularcomponent.Lateralplacementwithmetalbackingofthecomponentortheuse of a protrusio cup lessened these medial stresses.Prosthetic reinforcement of the medial wall had littlebenefit other than that of containment of any cementused.Theuseofamorselizedorfragmentedbonegraftisaneffectivemeansoflateralizationofthecup.15,68Aswellasreturningthehipjointtoitsanatomicalposition,thegraftisincorporatedintothemedialwallimprovingbonestockinthisregion.7RanawatandZahn69reportedon27arthroplastiesperformedforprotrusio.Whenthedegreeofprotrusiowaslessthan5mm,theydidnotusebonegraft.Whenthedegreeofprotrusiowasgreaterthan5mmbut themedialwall remained intact,autologousbonegraftwithoutartificialfixationdeviceswasrecom-mended.Finally,inpatientswithagrosslydeficientme-dialwall,reconstructionwithbonegraftandadditionalfixationisrequired.Hirstandassociates70reportedtheirfindingson61hipsoperatedonin51patientsandfol-lowedupforanaverageof4yearsand3months.Inthesepatients,thedegreeofprotrusiowasdeterminedbythegradingusedbySotelo-GarzaandCharnley53ratherthanameasurementdefiningmigrationfromtheanatomicalposition.All patients were operated on with the sametechnique.Themedialwallwasreinforcedwithwafersof autologous bone graft cut from the femoral head,sufficienttolateralizethecup.Cementwaspressurizedoverthislayerandintoperipheralkeyholes.Aflangedcupwasthenpushedfirmlyintoposition.Therewasnorelapseofprotrusioinanyofthesecases.
ConclusionsPrimaryprotrusioacetabuliremainsadiagnosisofex-clusion inpatientswithabnormalmedializationof theacetabulumandinwhomthesecondarycauseslistedinTable1havebeenruledout. While the exact etiology remains obscure, primaryprotrusio acetabuli is a developmental condition withhereditaryandracialinfluences.Itisprogressiveinado-lescence,priortofusionofthetriradiatecartilage,afterwhichthedeformityremainsstaticuntilsuperimposedwithsecondarydegenerativechanges.It ismost likelythatdelayedossificationratherthanearlyfusionofthetriradiatecartilageisresponsible.Alternatively,thede-formitymaydevelopduringanacceleratedgrowthspurt.Furtherworkisrequiredtoidentifytheexactdevelop-mentalmechanismandanypossiblegeneticetiologicalfactors. The current methods employed in radiographicaldiagnosisofprotrusioacetabulialluseanarbitrarycut-

113 Bulletin• Hospital for Joint Diseases Volume62,Numbers3&4 2005
offpointbetweennormalandabnormalanatomy.Whenlookingataconditionwithaspectrumofdeformity,thisinevitablyleadstoover-orunder-diagnosis,dependingon the cut-off point chosen. Certainly, patients withprotrusio acetabuli tend to have a center-edge anglegreaterthanthereportednormalupperlimitof46°;theteardrop configuration tends to be closed, crossed, orreversed;andtheacetabularlinetendstocrossKohler’slinebymorethan3mminmenandmorethan6mminwomen.However,noneofthesemeasurementshavethesensitivityorspecificitytoprovideareliablediagnosticsystem.Gradingsystems,suchasthoseusedbySotelo-GarzaandCharnley53orRanawatandZahn69aremoreusefulastheyallowcategorizationofpatients. The management of protusio acetabuli depends onage and degree of degenerative change. In the young,skeletallyimmaturepatientwithprogressivesecondaryprotrusioaceabuli,earlysurgicalfusionofthetriradiatecartilagewithorwithoutvalgusintertrochantericoste-otomyisappropriate.Asitisnotpossibletoanticipatewhichpatientswithprimaryprotrusioacetabuli in theyoungeragegroupwillprogresstoaseveredeformity,fusionofthetriradiatecartilagecannotberecommendedforprimaryprotrusioacetabuli.Valgusintertrochantericosteotomyisrecommendedinskeletallymaturepatientswithnodegenerativechangeunder40yearsofage.Over40years,thisprocedurecanstillbecarriedoutinpatientswithnodegenerativechangesintheirhipjointandwhoarecapableofundertakingtheassociatedrehabilitation.In older patients, total hip arthroplasty with medialbonegraftingandmeticulousattentiontoreturningthehip joint to its anatomical center is the procedure ofchoice.
References1. OttoAW: Pfannenbeckenmissgestaltung Infolge deformie-
render Osteo-arthritis in neue Seltene. Beobachtungen surAnatomie,PhysiologieundPathologiegehorig1824:19-20.
2. White H: Case of Charcot’s Joint-disease. BMJ1883;2:1019.
3. EppingerH:Pelvis-Chrobak.Koxarthrolisthesisbecken.BietrdGehbvGynakol1903;2:176.
4. PomeranzMM:Intrapelvicprotrusionoftheacetabulum(OttoPelvis).JBoneJointSurg1932;14:663-86
5. Schertlin:UebereinenFallvonintrapelvinerVorwolbungundcentralerWanderung der Huftpfanne (Otto-Chrobak’schesBecken).BeitragesurKlinischenChirurg1910;71:406-19.
6. HertzlerAE: Osteoarthritic protrusion of the acetabulum(IntrapelvicPfannenvorwolbung).ArchSurg1922;5:691.
7. McBride MT, Muldoon MP, Santore RF, Trousdale RT,WengerDR:Protrusioacetabuli:diagnosisandtreatment.JAmAcadOrthopSurg2001;9:79-88.
8. DoubHP:Intrapelvicprotrusionoftheacetabulum.Radiology1929;12:369-76.
9. SchaapC:Intrapelvicprotrusionoftheacetabulum.JBoneJointSurg1934;16:811-5.
10. GoldingFC:Protrusioacetabuli(centralluxation).BritJSurg
1934;22:56-61.11. RechtmanAM:Etiologyofdeepacetabulumandintrapelvic
protrusion.ArchSurg1936;33:122-37.12. Overgaard K: Otto’s disease and other forms of protrusio
acetabuli.ActaRadiologica1935;16:390-419.13. Gilmour J:Adolescent deformities of the acetabulum: an
investigationintothenatureofprotrusioacetabuli.BritJSurg1939;26:670-99.
14. FrankelVH,BursteinAH:Orthopaedic Biomechanics.Phila-delphia:LeaandFebiger,1976,p.27.
15. McCollumDE,NunleyJA:Bonegraftinginacetabularpro-trusio:abiologicbuttress.TheHip1978;6:124-46.
16. GiganteA,ChillemiC,GrecoF:ChangesofelasticfibersinmusculoskeletaltissuesofMarfanSyndrome.JPaedOrthop1999;19:283-8.
17. HooperJC,JonesEW:Primaryprotrusionoftheacetabulum.JBoneJointSurgB1971;53:23-29.
18. Brailsford JF: Bilateral ProtrusioAcetabuli: a progressivedeformityfrominfancy.JIntCollSurg1953;19:555-67.
19. FriedenbergZB:Protrusioacetabuli.AmJSurg1953;85:764-70.
20. HughesRA,TemposK,AnsellBM:Areviewofthediagno-sesofhippainpresentationintheadolescent.BritJRheum1988;27:450-3.
21. ShoreA,MacauleyD,AnsellBM:Idiopathicprotrusioac-etabuliinjuveniles.RheumatolRehabil1981;20(1):1-10.
22. Alexander C:The etiology of primary protrusio acetabuli.BritJRadiol1965;38:567-80.
23. ScandalisR,GhormleyRK,DockertyMB:Arthrokatadysis(Ottopelvis).Surgery1951;29:255-9.
24. FrancisHH:Theetiology,development,andtheeffectuponpregnancyofprotrusioacetabuli(Ottopelvis).SurgGynecolObstet1959;109:295-308.
25. D’ArcyK,AnsellBM,BywatersEG:Afamilywithprimaryprotrusioacetabuli.AnnRheumDis1978;37:53-7.
26. HohleVonB:FamiliaresVorkommenvonProtrusioacetabuli.BeitrOrthopuTraumatol1978;25:261-265.
27. MacDonaldD:Primaryprotrusioacetabuli:reportofanaf-fectedfamily.JBoneJointSurgB1971;53:30-36.
28. PerezGarciaJJ,FidalgoA,MoralesL,PerezPradoC:Protru-sionacetabularprimaria.AnEspPediat1978;11:795-800.
29. VentrutoV,StabileM,CavaliereML,etal:Primaryprotru-sioacetabuliinfourgenerationsofanItalianfamily.JMedGenetics1980;17:404-5.
30. BilfieldBS,JaneckiCJ,EvartsCM:Primaryprotrusionoftheacetabulum.ClinOrthop1973;94:257-62.
31. CrichtonD,CurlewisC:Bilateralprotrusioacetabuli(Ottopelvis).JObstetGynaecolBrEmp1962;69:47-51.
32. Friedenberg ZB: Protrusio acetabuli in childhood. J BoneJointSurgAm1963;45:373-78.
33. WroblewskiBM,HillmanF:Idiopathicprotrusioacetabuli:ahistologicalstudy.ClinOrthop1979;138:228-30.
34. Smith-PetersonMN:Treatmentofmalumcoxaesenilis,oldslippedupperfemoralepiphysis,intrapelvicprotrusionoftheacetabulum,andcoxaplanabymeansofacetabuloplasty.JBoneJointSurg1936;18:869-80.
35. HubbardMJS:Themeasurementofprogression inprotru-sio acetabuli.Am J Roentgenol RadiumTher Nucl Med1969;106:506-8.
36. Sherlock DA:Acute ideopathic chondrolysis and primary
114 Bulletin• Hospital for Joint Diseases Volume62,Numbers3&4 2005
acetabularprotrusiomaybethesamedisease.JBoneJointSurgBr1995;77:392-5.
37. BleckEE:Idiopathicchondrolysisofthehip.JBoneJointSurgAm1983;65:1266-75.
38. HughesAW:Idiopathicchondrolysisofthehip:acasereportandreviewoftheliterature.AnnRheumDis1985;44:268-72.
39. LeBastardE,DiardF,FontanD,etal:Chondrolyseaiguesur coxopathie protrusive primitive de l’enfant. J Radiol1987;68:671-6.
40. MouleNJ,GoldingJSR:Idiopathicchondrolysisofthehip.ClinRadiol1974;25:247-51.
41. WengerDR,MickelsonMR,Ponsetti IV: Idiopathicchon-drolysisofthehip.JBoneJointSurgAm1975;57:268-71.
42. WaldenstromH:Onnecrosisofthejointcartilagebyepiphy-seolysiscapitisfemoris.ActaChirScand1930;67:936-46.
43. JonesBS:Adolescentchondrolysisofthehipjoint.SAfricanMedJ1971;45:196-202.
44. Kindynis P, Garcia J: Protrusion acetabulaire. J Radiol1990;71:415-424.
45. TonnisD,HeineckeA:Acetabularandfemoralanteversion:relationshipwithosteoarthritisofthehip.JBoneJointSurgAm1999;81;1747-70.
46. GepsteinR,WeissRE,HallelT:Acetabulardysplasiaandhipdislocationafterselectiveprematurefusionofthetriradiatecartilage.JBoneJointSurgBr1984;66:334-6.
47. HallelT,SalvatiEA:Prematureclosureofthetriradiatecar-tilage.ClinOrthop1977;124:278-81.
48. BlairW,HansonC:Traumaticclosureofthetriradiatecarti-lage.JBoneJointSurgAm1979;61:144-5.
49. BucholzRW,EzakiM,OgdenJA:Injurytotheacetabulartri-radiatephysealcartilage.JBoneJointSurgAm1982;64:600-9.
50. DiasL,TachdjianMO,SchroederKE:Prematureclosureofthetriradiatecartilage:reportofacase.JBoneJointSurgBr1980;62:46-49.
51. JosephKN,KaneHA,MilnerRS,etal:OrthopaedicaspectsoftheMarfanphenotype.ClinOrthop1992;277:251-61.
52. SteelHH:Protrusioacetabuli:itsoccurrenceinthecompletelyexpressedMarfanSyndromeanditsmusculoskeletalcompo-nentandaproceduretoarrestthecourseofprotrusioninthegrowingpelvis.JPediatrOrthop1996;16:704-18.
53. Sotelo-GarzaA, Charnley J:The results of Charnley ar-throplastyofthehipperformedforprotrusioacetabuli.ClinOrthop1978;132:12-18.
54. Wiberg G: Shelf operation in congenital dysplasia of theacetabulumandinsubluxationanddislocationofthehip.JBoneJointSurgAm1953;35:65-80.
55. KohlerA:Roentgenology: The Borderlands of the Normal and the Early Pathological in Skiagram(2nded).London:Balliere,TindallandCox,1935,p.222.
56. ArmbusterTG,GuerraJ,ResnickD,etal:Theadulthip:ananatomicstudy.Radiology1978;128:1-10.
57. SharpIK:Acetabulardysplasia:theacetabularangle.JBoneJointSurgBr1961;43:268-72.
58. GoodmanSB,AdlerSJ,FyhrieDP,SchurmanDJ:Theac-etabularteardropanditsrelevancetoacetabularmigration.ClinOrthop1988;236:199-204.
59. GatesHS,PolettiSC,CallaghanJJ,McCollumDE:Radio-graphicmeasurementsinprotrusioacetabuli.JArthroplasty1989;4:347-51.
60. MurphySB,GanzR,MullerME:Theprognosisofuntreateddysplasiaofthehip.JBoneJointSurgAm1995;77:985-9.
61. PauwelsF,FurlongRJ,MaquetP:Biomechanics of the Nor-mal and Diseased Hip: Theoretical Foundation, Technique and Results of Treatment – An Atlas.Berlin:Springer-Verlag,1976,pp.129-169.
62. Rosemeyer B,Viernstein K, Schumann HJ: MittelfristigeErgebnissederValgisierendenundMedialisierenden Inter-trochanteren Osteotomie mitVerkurzung des Coxalen Fe-murendesbeiderprimarenProtrusioAcetabuli.ArchOrthopUnfall-Chir1973;77:138-48.
63. VerburgA,ElzengaP:Intertrochantericvalgizationosteotomyfortreatmentofprimaryprotrusionoftheacetabulum(Otto-Chrobakpelvis).ArchChirNeerl1978;30:207-15.
64. RanawatCS,DorrLD,InglisAE:Totalhiparthroplastyinprotrusioacetabuliofrheumatoidarthritis.JBoneJointSurgAm1980;62:1059-65.
65. DeLeeJD,CharnleyJ:Radiologicaldemarcationofcementedsocketsintotalhipreplacement.ClinOrthop1976;121:20-32.
66. Bayley JC, Christie MJ, Ewald FC, Kelley K: Long-termresultsoftotalhiparthroplastyinprotrusioacetabuli.JAr-throplasty1987;2:275-9.
67. CrowninshieldRD,BrandRA,PedersonDR:Astressanalysisof acetabular reconstruction in protrusio acetabuli. JBoneJointSurgAm1983;65:495-9.
68. McCollumDE,NunleyJA,HarrelsonJM:Bone-graftingintotalhipreplacementforacetabularprotrusion.JBoneJointSurgAm1980;62:1065-73.
69. RanawatCS,ZahnMG:Roleofbonegraftingincorrectionofprotrusioacetabulibytotalhiparthroplasty.JArthroplasty1986;1:131-7.
70. HirstP,EsserM,MurphyJCM,HardingeK:Bonegraftingforprotrusioacetabuliduringtotalhipreplacement.JBoneJointSurgBr1987;69:229-33.