psychological correlates of sensory processing · pdf filepsychological correlates of sensory...
TRANSCRIPT

REVIEW PAPER
Psychological Correlates of Sensory Processing Patternsin Individuals with Autism Spectrum Disorder:A Systematic Review
Magdalena Glod1& Deborah M. Riby2 & Emma Honey3 & Jacqui Rodgers4
Received: 28 November 2014 /Accepted: 24 March 2015 /Published online: 15 April 2015# Springer Science+Business Media New York 2015
Abstract Existing evidence suggests that there is a relation-ship between sensory processing difficulties and the clinicaland non-clinical features of autism spectrum disorder (ASD).The current review aimed to evaluate evidence of the psycho-logical correlates of sensory processing patterns in individualswith ASD. Primary studies investigating sensory processingpatterns in children and adolescents with ASD were identifiedthrough systematic searches of electronic databases and eval-uated for methodological rigor and reporting quality. In 21studies, associations between sensory processing patternsand psychological correlates were found. Sensory hypore-sponsiveness was correlated with core features of ASD.Social awareness difficulties and affective disorders were as-sociated with hyperresponsiveness. Mixed results were foundfor repetitive behaviours. Further research is needed to con-firm, clarify and extend these findings.
Keywords Autism spectrum disorder . Sensory processingpatterns . Psychological correlates . Children . Adolescents .
Systematic review
Sensory Atypicalities in ASD
Effective reception, integration and processing of sensory in-put, as visual, auditory or proprioceptive information, enablesus to respond to environmental signals in an adaptive manner(John and Mervis 2010), which is essential to everyday func-tioning and learning. In autism spectrum disorder (ASD), ithas been reported that sensory processing atypicalities arepresent in over 90 % of children (Leekam et al. 2007) andadults (Crane et al. 2009). Sensory processing difficulties arenow included in the most recent diagnostic criteria for ASD(Diagnostic and Statistical Manual of Mental Disorders—5thedition, DSM-V, APA 2013) with ‘hyper- or hyporeactivity tosensory input or unusual interests in sensory aspects of theenvironment (e.g. apparent indifference to pain/temperature,adverse response to specific sounds or textures, excessivesmelling or touching of objects, visual fascination with lightsor movement)’ (APA 2013 p.50) as one of the diagnosticfeatures.
Sensory Processing Patterns in ASD
There are several theoretical approaches to the classificationof sensory processing difficulties in ASD. The DSM-V (APA2013) highlights two sensory processing patterns, hyper- andhyporesponsiveness, understood as exaggerated behaviouralreaction and lack of, or insufficient behavioural reaction to,sensory stimuli (Boyd et al. 2009). It has been claimed, forexample, that features associated with the hyporesponsivenesspattern can discriminate between children with autism, devel-opmental delay and those of typical development (Baraneket al. 2006). In addition, sensory atypicalities associated withdifferent patterns of sensory processing may be present withinthe same individual with ASD (Baranek 2002; Baranek et al.
* Jacqui [email protected]
1 Institute of Neuroscience, Sir James Spence Institute, 3rd Floor,Royal Victoria Infirmary, Newcastle upon Tyne NE1 4LP, UK
2 Department of Psychology, Science Laboratories, DurhamUniversity, South Road, Durham DH1 3LE, UK
3 School of Psychology, Newcastle University, 4th Floor, RidleyBuilding 1, Newcastle upon Tyne NE1 7RU, UK
4 Institute of Neuroscience, Newcastle University, 4th Floor, RidleyBuilding 1, Newcastle upon Tyne NE1 7RU, UK
Rev J Autism Dev Disord (2015) 2:199–221DOI 10.1007/s40489-015-0047-8

2006; Ben-Sasson et al. 2009). Another approach taken ininvestigating sensory atypicalities focuses on sensory mod-ulation disorder (SMD). SMD is characterised by difficul-ties in regulating and organising appropriate behaviouralresponses to sensory input (Miller et al. 2007). The disor-der has distinct three subtypes—overresponsivity,underresponsivity and sensory seeking associated with thecraving of sensory experience (Miller et al. 2007). Thisclassification system has been acknowledged by theDiagnostic Classification of Mental Health andDevelopmental Disorders of Infancy and Early Childhood,Revised (known as the DC: 0–3R) (Zero to Three 2005),the Diagnostic Manual for Infancy and Early Childhood ofthe Interdisciplinary Council on Developmental andLearning Disorders (ICDL 2005), and the PsychodynamicDiagnostic Manual (PDM Task Force 2006). Other re-searchers examine sensory difficulties in ASD by applyingDunn’s model of sensory processing (Dunn 1997). In thatapproach, hyper- and hyporesponsiveness are further divid-ed depending on whether passive and active self-responding strategies are used to respond to sensory stim-ulation. As a result, four patterns of sensory processing aredistinguished: Low Registration, Sensation Seeking,Sensory Sensitivity and Sensation Avoiding. All four sen-sory processing patterns have been reported as present inindividuals with ASD (Kern et al. 2007). These multipletheoretical stands present in investigating sensory processingatypicalities in ASD are reflected in the current literature.
Symptom Comorbidity
Research suggests that there is a relationship between sen-sory processing difficulties and the clinical features ofASD. Some studies reported significant associations be-tween sensory processing atypicalities, communication andsocial impairments (Watson et al. 2011) as well as repeti-tive behaviours (Boyd et al. 2009), the presence of mal-adaptive behaviours, antisocial behaviours, self-absorptionand parent-reported child anxiety (Baker et al. 2008) orperseveration and overfocusing attention (Liss et al.2006). There is also evidence of significant associationsbetween sensory processing atypicalities and other non-clinical psychological constructs such as temperament(Brock et al. 2012), emotion dysregulation (Samson et al.2013) or eating difficulties (Nadon et al. 2011). However,there is variability in the methodological approaches usedin those studies, including the selection of measures, diag-nostic subgroups and specified inclusion criteria. Due to avast number of psychological constructs that have beeninvestigated, and a wide range of methods of investigationemployed, both interpretation and comparison of findingshas been hampered.
Previous Reviews
Four literature reviews of sensory atypicalities in individualswith ASD have been published to date (Ben-Sasson et al.2009; Iarocci and McDonald 2006; O’Neill and Jones 1997;Rogers and Ozonoff 2005). However, these evaluations fo-cused on differently defined sensory difficulties: Ben-Sassonet al. (2009) reviewed sensory modulation symptoms in indi-viduals with autism, Iarocci and McDonald (2006) investigat-ed multisensory integration, O’Neill and Jones (1997) studiedunusual sensory responses, while Rogers and Ozonoff (2005)concentrated on sensory dysfunction. Secondly, the previousreviews employed different methodological approaches, rang-ing from experimental laboratory findings combined with the-oretical and conceptual papers (Iarocci and McDonald 2006;Rogers and Ozonoff 2005), through reviewing clinical andexperimental studies (O’Neill and Jones 1997) to the inclusionof only clinical findings (Ben-Sasson et al. 2009). Thirdly, theprevious reviews focused more on the discriminant validity ofsensory atypicalities between ASD and typical groups. Thereis also growing number of studies investigating physiologicalreactivity to different types of sensory stimuli (for review seeLydon et al. 2014). However, none of the published reviewshave described evidence of associations between sensory pro-cessing patterns in individuals with ASD and other psycho-logical constructs. Therefore, this current approach to the re-view is important because, while there is growing interest andresearch in sensory processing in individuals with ASD andsensory processing patterns are included in the diagnosticcriteria for ASD (APA 2013), a systematic summary of therecent findings is lacking.
Aim of the Review
The current review therefore aims to systematically summa-rise and evaluate available evidence, recognise and discussany shortcomings, and identify goals for future research inorder to address the following question: What are the psycho-logical correlates of sensory processing patterns in individualswith ASD?
Method
Inclusion/ Exclusion Criteria
Inclusion and exclusion criteria were defined prior toconducting the literature search. Studies were eligible for in-clusion if they investigated sensory processing patterns in in-dividuals with ASD and explicitly reported associations withpsychological correlates such as cognition, emotions, behav-iour or interpersonal relationships. Studies were searched from
200 Rev J Autism Dev Disord (2015) 2:199–221

1997 onwards. Non-primary studies were excluded from thesearch (e.g. reviews, book chapters). Also, single case studiesand case series designs were excluded. This decision wasbased upon the consideration that results from single casestudies would not provide quantitative statistical data whichis important from the point of this review and do not allowfurther generalisation of the findings. The search was neitherrestricted to any particular age group nor particular diagnosticsubgroup.
Search Strategy
A systematic literature search aimed to identify studiesreporting sensory processing patterns of individuals withASD conducted up to February 2014. The search used fiveelectronic databases: Scopus, Web of Knowledge, PsychInfo,Embase and Medline. For both Scopus and Web ofKnowledge, which allow authors to search for a number ofkeywords, the search terms were based on the keywords usedin the Ben-Sasson et al. (2009) meta-analysis. After identify-ing relevant papers, additional keywords that were used incategorising those papers were added into the search terms.The combinations of the following search terms were used: adiagnostic term (autis* or Bpervasive developmentaldisorder*^ or Asperger), a sensory term (sensory or reactivityor responsivity or sensation*) and a descriptor term (process-ing or integration or modulation or regulation or stimul* orinput or event* or dysfunction or respons* or profile* orsymptom* or unusual or difficulties or interest* or feature*or experience* or hypo* or hyper* or pattern* or sensitiv* orseeking or avoid* or registration or threshold* or defensive-ness). In PsychInfo, Embase and Medline databases, searchesare based on controlled vocabularies. However, because dif-ferent types of headings are used for each database (e.g. med-ical subjects headings for Medline, but APA thesaurus forPsychInfo), the vocabulary used in the databases varied. ForPsychInfo, autism or pervasive developmental disorders orAsperger syndrome were used as diagnostic terms, combinedwith sensory integration or intersensory processes or percep-tual motor processes or sensorimotor measures or sensoryadaptation or adaptation or thresholds or self stimulation. Inthe Embase database, Asperger syndrome or infantile autismor autism terms were used, combined with sensory dysfunc-tion or abnormal sensation or sensory defensiveness or senso-ry stimulation or sensation or abnormal sensation or sensationseeking or self stimulation or perceptive threshold or sensori-motor function or sensorimotor integration. When searchingin Medline, a combination of terms child development disor-ders, pervasive or autistic disorder or Asperger syndrome, andsensory thresholds or sensation disorders or self stimulation oroccupational therapy were used.
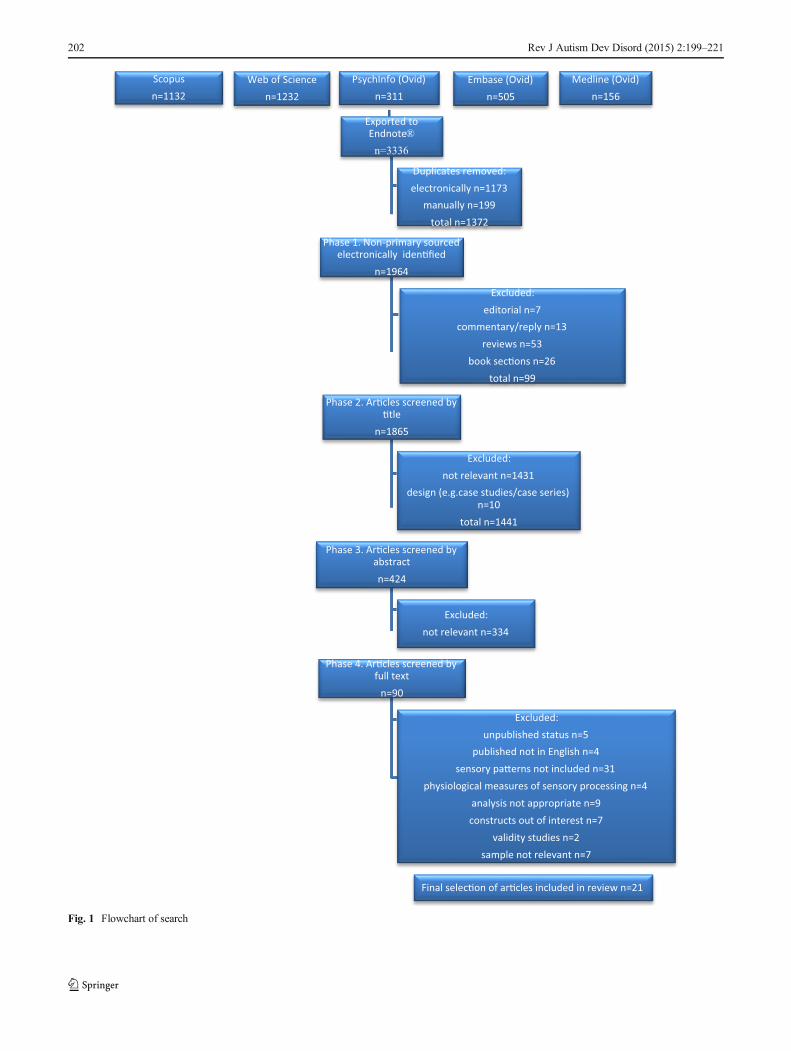
A flowchart of the search strategy and numbers of articlesidentified and excluded at each stage is outlined in Fig. 1. All
databases were searched between 1997 and the 2nd ofFebruary 2014.
Electronic Search
Results from five electronic databases were exported toEndnote® referencing software resulting in 3336 records intotal. Most duplicates of the papers were identified byEndnote’s duplicate identification function and removed fromthe records’ list. Further duplicates not recognised by the soft-ware were removed manually, and 1964 records were carriedforward to the screening stage.
Screening of Electronic Search Results
Screening of the search results consisted of four main phases.In phase 1, the non-primary sources were electronically iden-tified and removed (a total of 99 records). In phase 2, theremaining titles of the records were screened considering theirrelevance to the search question and 1441 studies were re-moved. In phase 3, remaining article abstracts were screened.Only 90 met inclusion criteria and those were carried forwardto the final phase in which articles were screened by full textand the final selection was made.
Final Selection
Sixty nine papers were excluded after screening the full text.Five papers were excluded due to unpublished status (threetheses, two conference papers). Four were excluded due tobeing published in languages other than English (Japanese,Italian, Portuguese and Chinese). Four papers focused on sen-sory modalities (such as auditory or tactile modality) ratherthan sensory patterns, which were a main interest of this re-view. In another 27 papers, sensory atypicalities in generalwere investigated (mainly reporting the Short SensoryProfile total score). Four studies used physiological measuresof sensory processing. Nine papers were not found appropriatedue to the lack of correlational analysis (four were descriptivein nature, reporting, for example, cross-group comparisonsand another five presented onlymeans for different constructs,without reporting relations between the constructs or present-ing sensory clusters). Seven papers did not include any psy-chological constructs, but examined relationships betweensensory processing and for example oral care difficulties, lei-sure activities, or family life impairment and maternal parent-ing stress. Two papers were validity studies (investigatingpsychometric properties of tools). In seven papers, a clearASD sample was not recruited, either studies included partic-ipants from the general population, with or without someASD-traits, or the results were presented for a combinedASD sample with another group (e.g. developmental delay).The remaining 21 papers were included in the systematic
Rev J Autism Dev Disord (2015) 2:199–221 201
Medline (Ovid)
n=156
Embase (Ovid)
n=505
PsychInfo (Ovid)
n=311
Exported to Endnote®
n=3336
Phase 1. Non-primary sourced electronically iden�fied
n=1964
Phase 2. Ar�cles screened by �tle
n=1865
Phase 3. Ar�cles screened by abstract
n=424
Phase 4. Ar�cles screened by full text
n=90
Final selec�on of ar�cles included in review n=21
Excluded:
unpublished status n=5
published not in English n=4
sensory pa�erns not included n=31
physiological measures of sensory processing n=4
analysis not appropriate n=9
constructs out of interest n=7
validity studies n=2
sample not relevant n=7
Excluded:
not relevant n=334
Excluded:
not relevant n=1431
design (e.g.case studies/case series) n=10
total n=1441
Excluded:
editorial n=7
commentary/reply n=13
reviews n=53
book sec�ons n=26
total n=99
Duplicates removed:
electronically n=1173
manually n=199
total n=1372
Web of Science
n=1232
Scopus
n=1132
Fig. 1 Flowchart of search
202 Rev J Autism Dev Disord (2015) 2:199–221

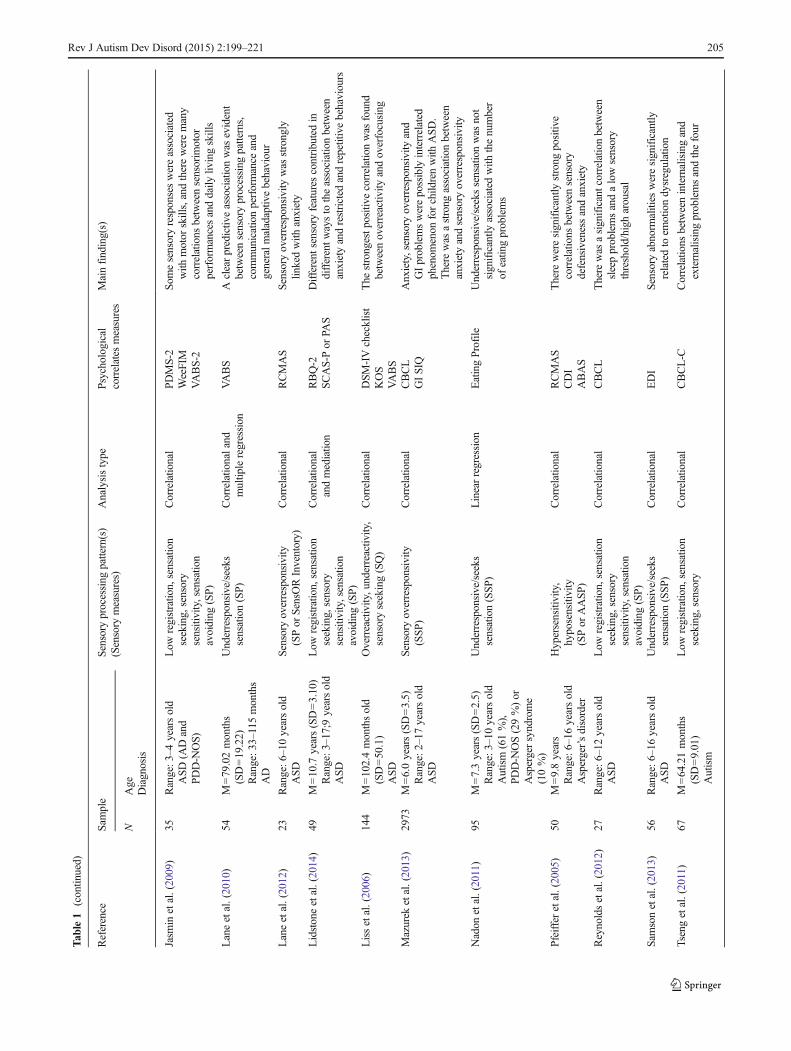
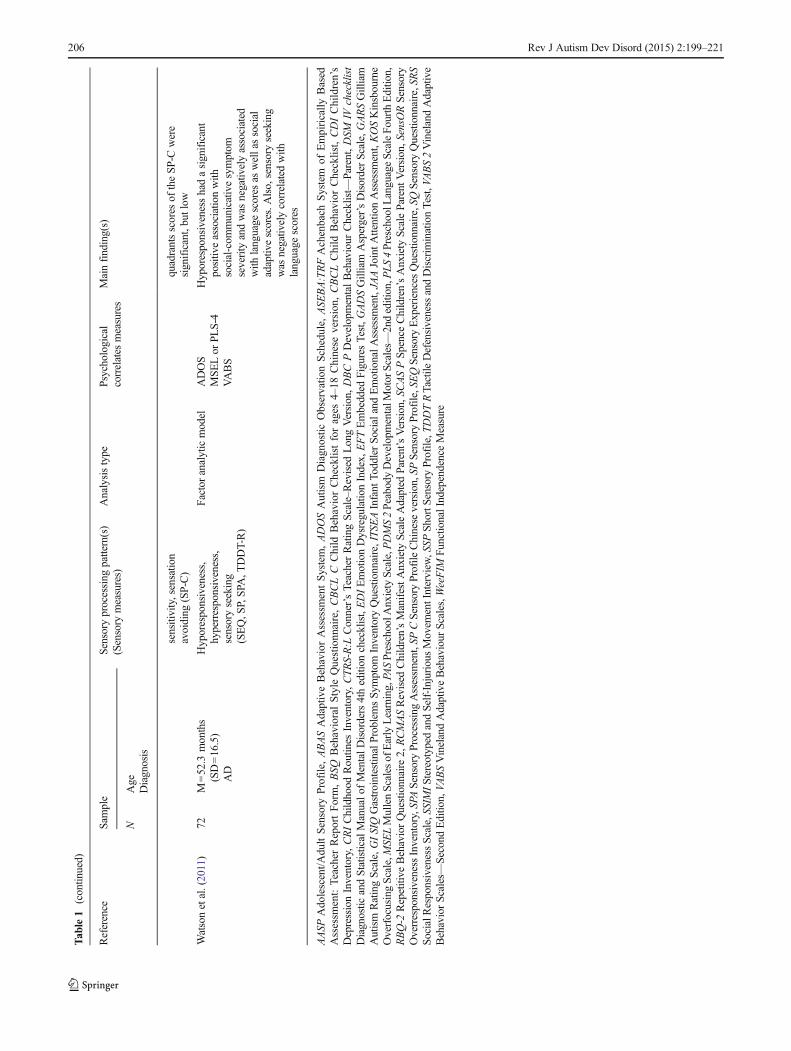
review. The summary of the descriptive characteristics of the-se studies can be found in Table 1.
Critical Evaluation
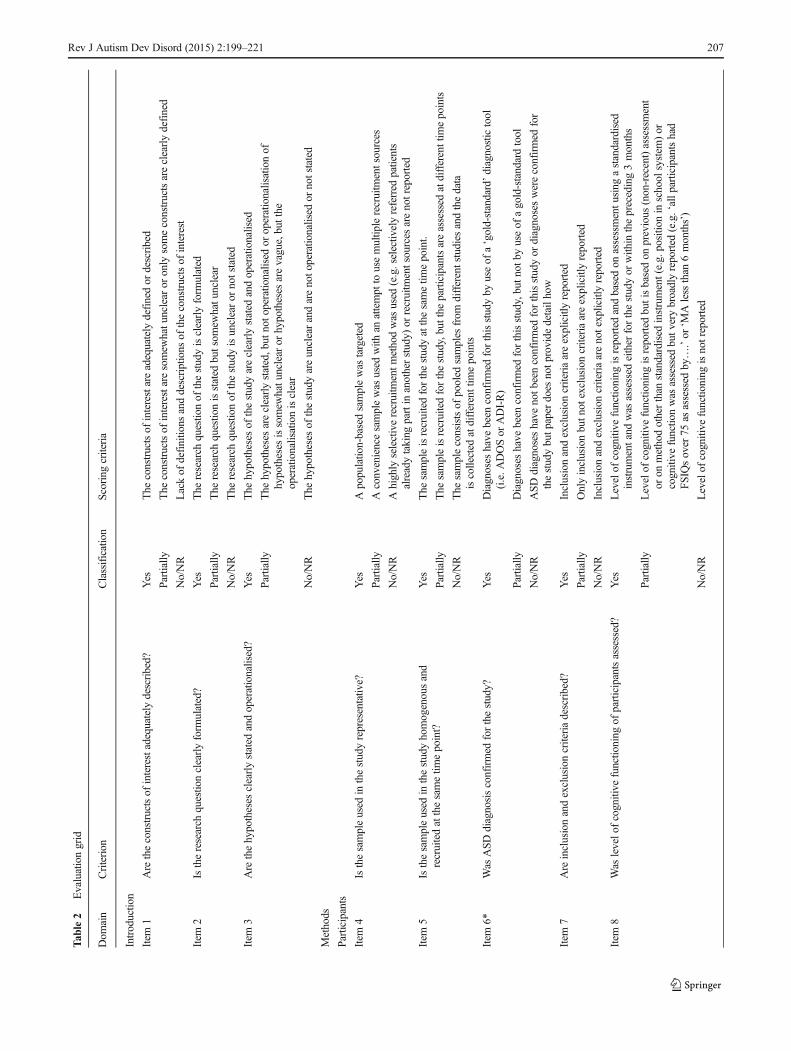
Each of the retained papers was evaluated against a reviewquality evaluation grid developed for the purpose of this re-view. The available checklists for the quality assessment ofstudies (e.g. PRISMA,Moher et al. 2009; QUADAS,Whitinget al. 2003) or well-known guidelines for conducting system-atic reviews in health care (e.g. the Cochrane Collaboration)focus on diagnostic accuracy, evaluation of randomised trialsand intervention studies. The newly developed grid aimed tosystematically evaluate the overall quality of the studies, theirstrengths and limitations or potential sources of bias. The gridwas divided into four main sections, following the IMRaDstructure: introduction, methods, results and discussion(Sollaci and Pereira 2004). The methods section was of par-ticular importance including items evaluating a studies qualityin participants and method selection. To adequately evaluatethe methodology used in the studies, the grid contained itemsconcentrating on appropriate sample characteristics and con-firmation of ASD diagnosis. The methods section of the eval-uation grid also highlighted the importance of sound psycho-metric properties of the tools used in the studies as suggestedby the COnsensus-based Standards for the selection of healthMeasurement INstruments (COSMIN) guideline (Mokkinket al. 2010). The total number of criteria that the studies werescored against was kept within the recommended limit to keepclear focus of the review (SIGN 2008).
Subjective judgement is a part of the evaluation process(Deeks et al. 2003; SIGN 2008); to minimise the reviewer’ssubjectivity, the following steps were undertaken. First, allscoring criteria were explained in detail. Second, three levelsof quality ratings were used, the equivalent of the levels ofratings proposed by SIGN (high, acceptable and low quality).Finally, a proportion of the studies included in the review(19 %) were evaluated by an independent rater. The inter-rater reliability between the author’s and independent rater’sscorings calculated as percentage agreement on individualcriteria was 87.5 %.
Results
Of the 1964 unique references identified via the electronicsearches, 21 papers met the inclusion criteria and wereretained for review.
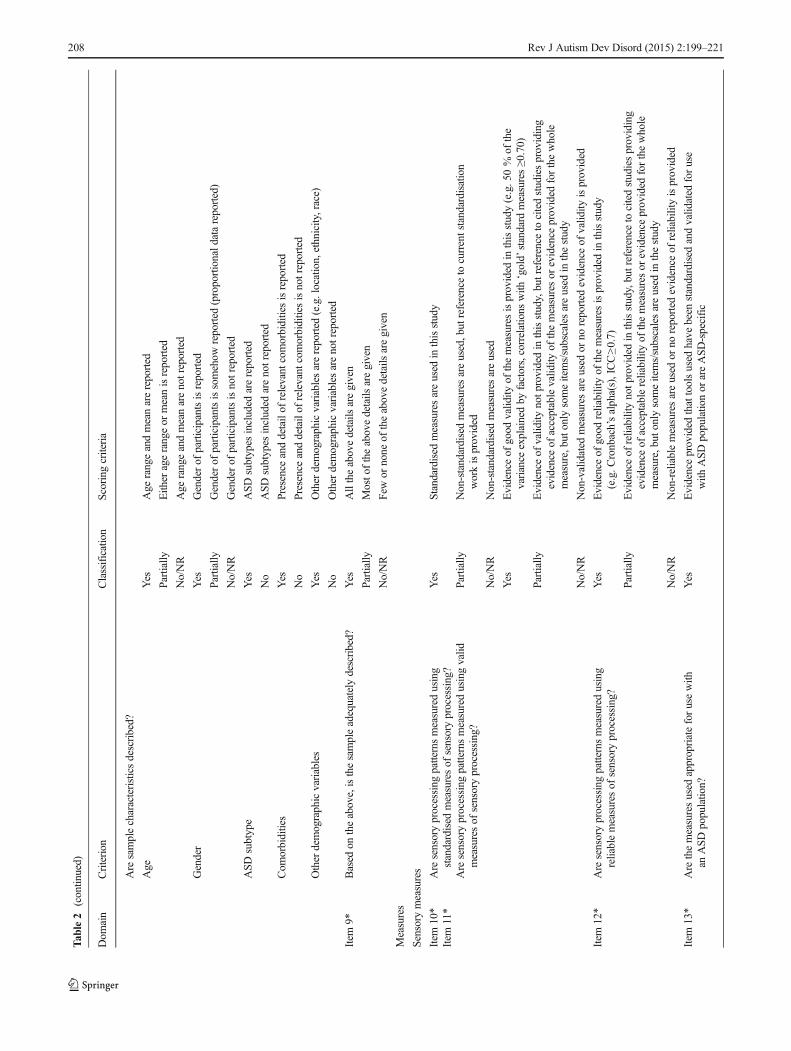
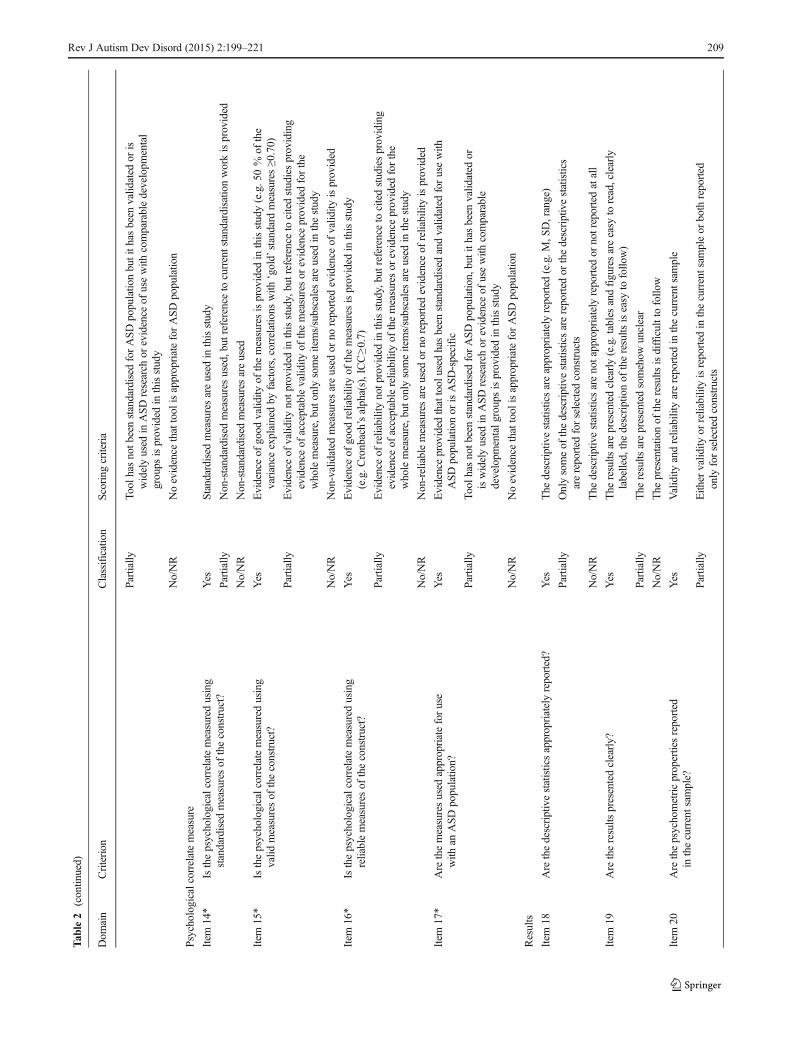
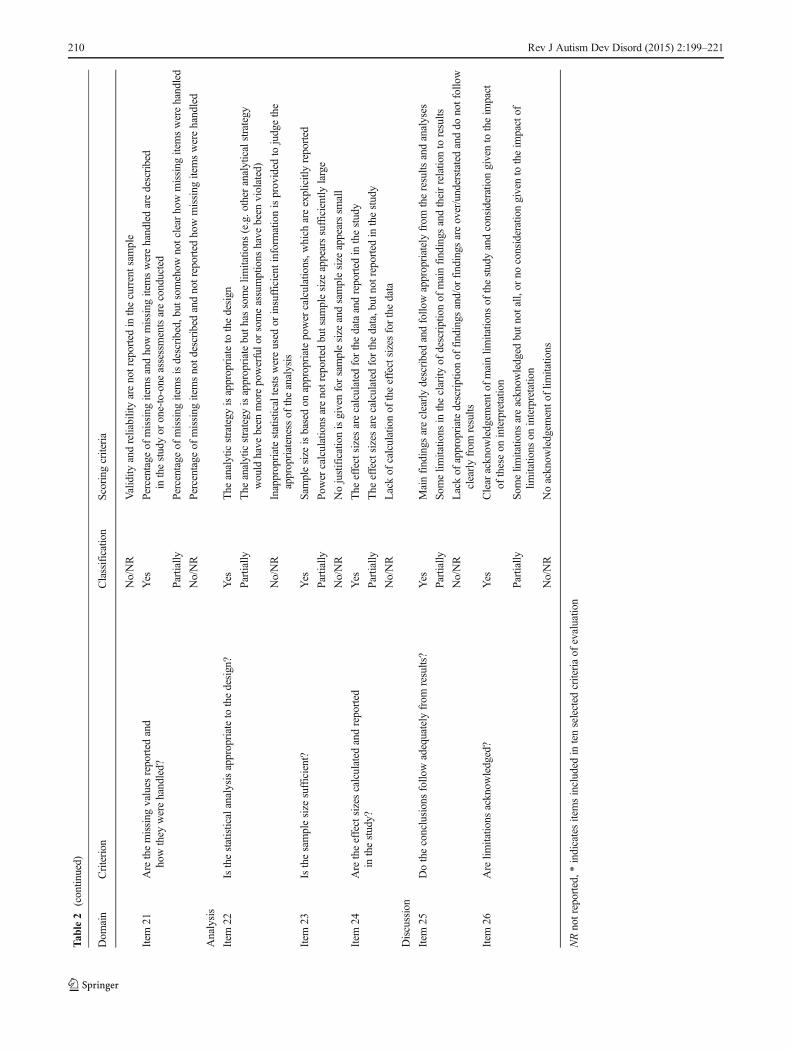
Evaluation Grid—Papers’ Quality
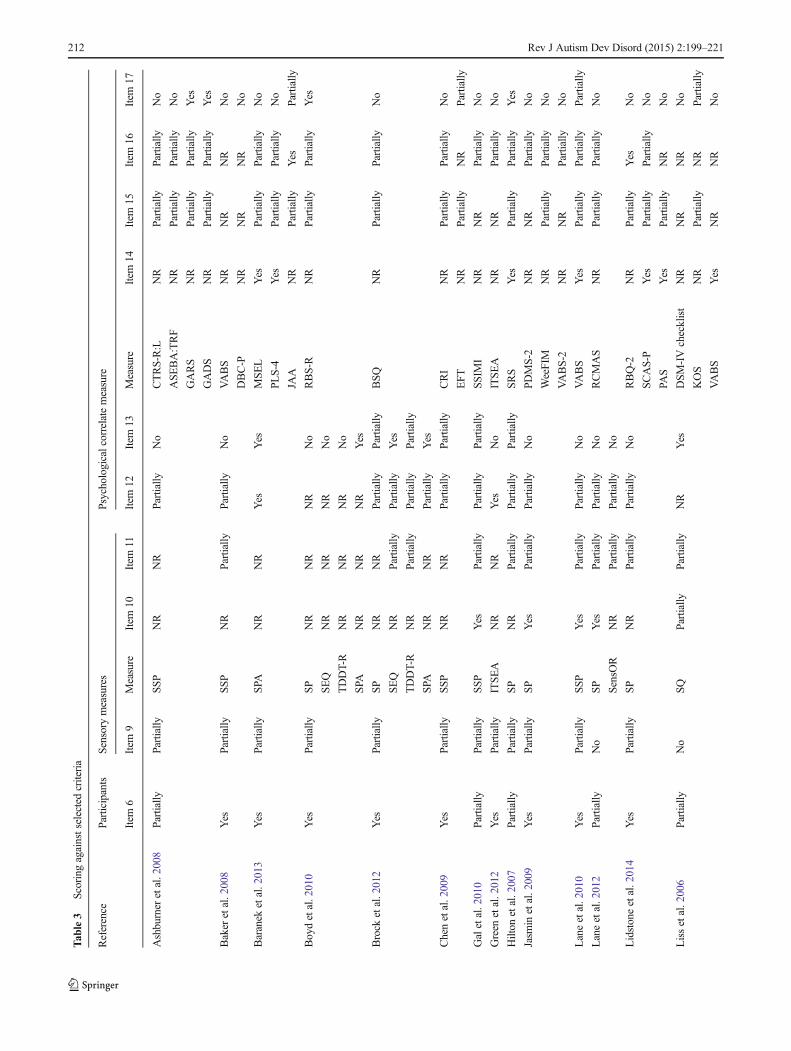
Originally, the papers included in the review were scoredagainst 26 criteria. Ten criteria were emphasised during the
evaluation. Two criteria were selected from the participants’section (‘Was ASD diagnosis confirmed for the study?’ and‘Is the sample adequately described?’). They allowed us toassess whether the sample of interest was included in the studyand whether the authors reported participants’ characteristicsin a high-quality manner. Items from the ‘Sensory measures’and ‘Psychological correlate measure’ sections were also con-sidered as the criteria of the key importance. They allowed usto evaluate the appropriateness, reliability and validity of thetools used in the studies. The chosen criteria are fundamentalto evaluate the quality of the studies in the light of the researchquestion asked in this review. For the summary of the infor-mation included in the evaluation grid and ten selectedcriteria, see Table 2.
Participants’ Section
The two items describing participants’ characteristics are es-sential to establish whether the particular clinical group ofinterest was selected according to widely accepted researchstandards. In addition, it was important to confirm whetheror not the characteristics were described well enough to allowother researchers to replicate the study and identify some pos-sible important covariates that might influence the study find-ings. All the studies provided a confirmation of diagnosis ofparticipants. In 14 papers, the assessment of children was car-ried out prior to inclusion in the study by using ‘gold-stan-dard’ diagnostic tools such as the Autism DiagnosticObservation Schedule (ADOS) or the Autism DiagnosticInterview-Revised (ADI-R). In the remaining seven papers(Ashburner et al. 2008; Gal et al. 2010; Hilton et al. 2007;Lane et al. 2012; Liss et al. 2006; Nadon et al. 2011; Tsenget al. 2011), documents stating children’s and young people’sdiagnosis were gathered or non-‘gold-standard’ tools wereused to confirm diagnosis, e.g. medical chart review.However, sample characteristics were not always well de-scribed. Three studies (Lane et al. 2012; Liss et al. 2006;Tseng et al. 2011) reported only gender and age of their par-ticipants. Only Nadon et al. (2011) provided all thedemographics selected in the evaluation grid characteristics(e.g. age, gender, ASD subtype, comorbidities and demo-graphic variables). The remaining studies reported three orfour of these features.
Sensory Measures Section
Nine different tools were used to assess sensory processingpattern or patterns in the selected studies (additionally theSensory Profile was used in two language versions—Englishand Chinese). Three authors (Boyd et al. 2010; Brock et al.2012; Watson et al. 2011) used more than one sensory mea-sure and selected items from each measure to inform a factoranalytic model of sensory processing patterns. These models
Rev J Autism Dev Disord (2015) 2:199–221 203

Tab
le1
Summaryof
included
studies
Reference
Sam
ple
Sensory
processing
pattern(s)
(Sensory
measures)
Analysistype
Psychological
correlates
measures
Mainfinding(s)
NAge
Diagnosis
Ashburner
etal.(2008)
28Range:6
–10yearsold
ASD
Underresponsive/seeks
sensation(SSP)
Correlatio
nal
CTRS-R:L
ASE
BA:TRF
GADS
GARS
Underresponsive/seeks
sensationwas
significantly
negativ
elyassociated
with
academ
icperformance
andattentionto
cognitive
tasks
andwith
autism
quotient
Baker
etal.(2008)
22M=64.86months
(SD=20.70)
Range:3
3–101
monthsold
AD
Underresponsive/seeks
sensation(SSP)
Correlatio
nal
VABS
DBC-P
Poor
sensoryprocessing
ability
was
associated
with
higher
levelsof
behaviouraland/or
emotionalp
roblem
s
Baranek
etal.(2013)
63Range:2
0–83
monthsold
AD
Hyporesponsiveness(SPA
)Inferential(series
ofregression
models)
JAA
MSE
LPL
S-4
Sensoryhyporesponsiveness
was
significantly
negativ
elyassociated
with
jointattention
andlanguage
skills
Boydetal.(2010)
67M=51.69months
(SD=17.07)
AD
Hyporesponsiveness,
hyperresponsiveness,
sensoryseeking
(SEQ,S
P,SPA
,TDDT-R)
Inferential(series
ofregression
models)
RBS-R
Higherhyperresponsivescores
wererelatedto
avarietyof
repetitivebehaviours.T
hesignificantassociatio
nwas
foundbetween
sensoryseekingandritualistic/sam
eness
behaviours
Brock
etal.(2012)
54M=56.17months
(SD=3.67)
Range:3
6–84
monthsold
ASD
Hyporesponsiveness,
hyperresponsiveness,
sensoryseeking(SEQ,
SP,SPA
,TDDT-R)
Inferential(series
ofregression
models)
BSQ
Hyporesponsivenesswas
mostassociated
with
distractibility,slowness
toadapt
andthethresholdsubscale.H
ighlevels
ofsensoryfeatures
wereassociated
with
increasedwith
draw
alandmorenegativ
emood
Chenetal.(2009)
29Range:8
–16yearsold
Aspergersyndromeor
ASD
Underresponsive/seeks
sensation(SSP)
Correlatio
naland
multip
leregression
CRI
EFT
Nosignificantrelationshipwas
found
betweenthepresence
ofsensoryabnorm
alities
(underresponsiveness)andrestricted
and
repetitivebehavioursanddetail-focused
cognitive
style
Galetal.(2010)
56M=9.71
years(SD=1.86)
Autism
Underresponsive/seeks
sensation(SSP)
Correlatio
nal
SSIMI
Atypicalsensory
processing
was
strongly
relatedto
stereotypedmovem
ents
(underresponsiveness
was
thebestpredictor
ofstereotypedmovem
ents)
Green
etal.(2012)
149
M=28.3
months(SD=5.5)
ASD
orPDD-N
OS
Sensoryoverresponsivity
(ITSEA)
Correlatio
nal
ITSE
ASensoryoverresponsivity
was
positiv
ely
associated
with
anxiety(and
positiv
ely
predictedincreasesin
anxiety)
Hilton
etal.(2007)
36Range:6
–10yearsold
HFA
SD
Low
registratio
n,sensation
seeking,sensory
sensitivity,sensatio
navoiding
(SP)
Correlatio
nal
SRS
The
SRSscores
show
edmoderateto
strong
relatio
nships
with
SensoryProfile
quadrant
scores
204 Rev J Autism Dev Disord (2015) 2:199–221
Tab
le1
(contin
ued)
Reference
Sam
ple
Sensory
processing
pattern(s)
(Sensory
measures)
Analysistype
Psychological
correlates
measures
Mainfinding(s)
NAge
Diagnosis
Jasm
inetal.(2009)
35Range:3
–4yearsold
ASD
(ADand
PDD-N
OS)
Low
registratio
n,sensation
seeking,sensory
sensitivity,sensatio
navoiding
(SP)
Correlatio
nal
PDMS-2
WeeFIM
VABS-2
Somesensoryresponseswereassociated
with
motor
skills,andthereweremany
correlations
betweensensorim
otor
performancesanddaily
livingskills
Laneetal.(2010)
54M=79.02months
(SD=19.22)
Range:3
3–115months
AD
Underresponsive/seeks
sensation(SP)
Correlatio
naland
multip
leregression
VABS
Aclearpredictiv
eassociationwas
evident
betweensensoryprocessing
patterns,
communicationperformance
and
generalm
aladaptiv
ebehaviour
Laneetal.(2012)
23Range:6
–10yearsold
ASD
Sensoryoverresponsivity
(SPor
SensO
RInventory)
Correlatio
nal
RCMAS
Sensoryoverresponsivity
was
strongly
linkedwith
anxiety
Lidstoneetal.(2014)
49M=10.7
years(SD=3.10)
Range:3
–17;9yearsold
ASD
Low
registratio
n,sensation
seeking,sensory
sensitivity,sensatio
navoiding
(SP)
Correlatio
nal
andmediatio
nRBQ-2
SCAS-P
orPA
SDifferent
sensoryfeatures
contributedin
differentw
aysto
theassociationbetween
anxietyandrestricted
andrepetitivebehaviours
Lissetal.(2006)
144
M=102.4monthsold
(SD=50.1)
ASD
Overreactivity,underreactiv
ity,
sensoryseeking(SQ)
Correlatio
nal
DSM
-IVchecklist
KOS
VABS
The
strongestp
ositive
correlationwas
found
betweenoverreactiv
ityandoverfocusing
Mazurek
etal.(2013)
2973
M=6.0years(SD=3.5)
Range:2
–17yearsold
ASD
Sensoryoverresponsivity
(SSP
)Correlatio
nal
CBCL
GISIQ
Anxiety,sensory
overresponsivity
and
GIproblemswerepossibly
interrelated
phenom
enon
forchild
renwith
ASD
.There
was
astrong
associationbetween
anxietyandsensoryoverresponsivity
Nadon
etal.(2011)
95M=7.3years(SD=2.5)
Range:3
–10yearsold
Autism
(61%),
PDD-N
OS(29%)or
Aspergersyndrome
(10%)
Underresponsive/seeks
sensation(SSP)
Linearregression
EatingProfile
Underresponsive/seeks
sensationwas
not
significantly
associated
with
thenumber
ofeatin
gproblems
Pfeifferetal.(2005)
50M=9.8years
Range:6
–16yearsold
Asperger’sdisorder
Hypersensitivity,
hyposensitivity
(SPor
AASP
)
Correlatio
nal
RCMAS
CDI
ABAS
There
weresignificantly
strong
positiv
ecorrelations
betweensensory
defensivenessandanxiety
Reynoldsetal.(2012)
27Range:6
–12yearsold
ASD
Low
registratio
n,sensation
seeking,sensory
sensitivity,sensatio
navoiding
(SP)
Correlatio
nal
CBCL
There
was
asignificantcorrelatio
nbetween
sleepproblemsandalowsensory
threshold/high
arousal
Sam
sonetal.(2013)
56Range:6
–16yearsold
ASD
Underresponsive/seeks
sensation(SSP)
Correlatio
nal
EDI
Sensory
abnorm
alities
weresignificantly
relatedto
emotiondysregulation
Tsengetal.(2011)
67M=64.21months
(SD=9.01)
Autism
Low
registratio
n,sensation
seeking,sensory
Correlatio
nal
CBCL-C
Correlatio
nsbetweeninternalisingand
externalisingproblemsandthefour
Rev J Autism Dev Disord (2015) 2:199–221 205
Tab
le1
(contin
ued)
Reference
Sam
ple
Sensory
processing
pattern(s)
(Sensory
measures)
Analysistype
Psychological
correlates
measures
Mainfinding(s)
NAge
Diagnosis
sensitivity,sensatio
navoiding
(SP-C)
quadrantsscores
oftheSP-Cwere
significant,butlow
Watsonetal.(2011)
72M=52.3
months
(SD=16.5)
AD
Hyporesponsiveness,
hyperresponsiveness,
sensoryseeking
(SEQ,S
P,SPA
,TDDT-R)
Factor
analyticmodel
ADOS
MSELor
PLS-4
VABS
Hyporesponsivenesshadasignificant
positiv
eassociationwith
social-com
municativesymptom
severity
andwas
negativ
elyassociated
with
language
scores
aswellassocial
adaptiv
escores.A
lso,sensoryseeking
was
negativ
elycorrelated
with
language
scores
AASP
Adolescent/A
dultSensory
Profile,ABASAdaptiveBehaviorAssessm
entSystem,ADOSAutism
Diagnostic
Observatio
nSchedule,
ASE
BA:TRFAchenbach
System
ofEmpirically
Based
Assessm
ent:Teacher
ReportForm,BSQ
BehavioralStyle
Questionnaire,CBCLC
Child
BehaviorChecklistforages
4–18
Chinese
version,
CBCLChild
BehaviorChecklist,CDIChildren’s
DepressionInventory,CRIChildhood
Routin
esInventory,CTRS-R:L
Conner’sTeacherRatingScale–Revised
LongVersion,DBCPDevelopmentalBehaviour
Checklist—
Parent,DSM
IVchecklist
Diagnostic
andStatisticalManualof
MentalDisorders4thedition
checklist,EDIEmotionDysregulatio
nIndex,
EFTEmbedded
Figures
Test,G
ADSGilliam
Asperger’sDisorderScale,G
ARSGilliam
Autism
RatingScale,G
ISIQGastrointestin
alProblemsSym
ptom
InventoryQuestionnaire,ITS
EAInfant
ToddlerSo
cialandEmotionalA
ssessm
ent,JA
AJointA
ttentionAssessm
ent,KOSKinsbourne
OverfocusingScale,M
SELMullenScales
ofEarlyLearning,PA
SPreschoolAnxietyScale,PDMS2PeabodyDevelopmentalM
otor
Scales—2ndedition,P
LS4PreschoolL
anguageScaleFourthEditio
n,RBQ-2
Repetitive
BehaviorQuestionnaire
2,RCMASRevised
Children’sManifestAnxiety
ScaleAdapted
Parent’s
Version,S
CASPSpenceChildren’sAnxiety
ScaleParent
Version,S
ensO
RSensory
OverresponsivenessInventory,SPASensoryProcessing
Assessm
ent,SP
CSensoryProfileChinese
version,SP
SensoryProfile,SEQSensoryExperiences
Questionnaire,SQSensoryQuestionnaire,SRS
SocialR
esponsivenessScale,SSIMIStereotypedandSelf-Injurious
Movem
entInterview
,SSP
ShortS
ensory
Profile,T
DDTRTactile
Defensiveness
andDiscrim
inationTest,V
ABS2VinelandAdaptive
BehaviorScales—Second
Editio
n,VA
BSVinelandAdaptiveBehaviour
Scales,WeeFIM
Functio
nalIndependenceMeasure
206 Rev J Autism Dev Disord (2015) 2:199–221
Tab
le2
Evaluationgrid
Dom
ain
Criterion
Classification
Scoring
criteria
Introductio
n
Item
1Are
theconstructsof
interestadequately
described?
Yes
The
constructsof
interestareadequately
definedor
described
Partially
The
constructsof
interestaresomew
hatu
nclear
oronly
someconstructsareclearlydefined
No/NR
Lackof
definitio
nsanddescriptions
oftheconstructsof
interest
Item
2Istheresearch
questio
nclearlyform
ulated?
Yes
The
research
questio
nof
thestudyisclearlyform
ulated
Partially
The
research
questio
nisstated
butsom
ewhatu
nclear
No/NR
The
research
questio
nof
thestudyisunclearor
notstated
Item
3Are
thehypotheses
clearlystated
andoperationalised?
Yes
The
hypotheses
ofthestudyareclearlystated
andoperationalised
Partially
The
hypotheses
areclearlystated,but
noto
peratio
nalised
oroperationalisationof
hypotheses
issomew
hatu
nclear
orhypotheses
arevague,butthe
operationalisationisclear
No/NR
The
hypotheses
ofthestudyareunclearandarenoto
peratio
nalised
ornotstated
Methods
Participants
Item
4Isthesampleused
inthestudyrepresentativ
e?Yes
Apopulatio
n-basedsamplewas
targeted
Partially
Aconveniencesamplewas
used
with
anattempt
tousemultip
lerecruitm
entsources
No/NR
Ahighly
selectiverecruitm
entm
ethodwas
used
(e.g.selectiv
elyreferred
patients
alreadytaking
partin
anotherstudy)
orrecruitm
entsources
arenotreported
Item
5Isthesampleused
inthestudyhomogenousand
recruitedatthesametim
epoint?
Yes
The
sampleisrecruitedforthestudyatthesametim
epoint.
Partially
The
sampleisrecruitedforthestudy,butthe
participantsareassessed
atdifferenttim
epoints
No/NR
The
sampleconsistsof
pooled
samples
from
differentstudies
andthedata
iscollected
atdifferenttim
epoints
Item
6*Was
ASD
diagnosisconfirmed
forthestudy?
Yes
Diagnoses
have
been
confirmed
forthisstudyby
useof
a‘gold-standard’diagnostictool
(i.e.A
DOSor
ADI-R)
Partially
Diagnoses
have
been
confirmed
forthisstudy,butn
otby
useof
agold-standardtool
No/NR
ASD
diagnoseshave
notb
eenconfirmed
forthisstudyor
diagnoseswereconfirmed
for
thestudybutp
aper
does
notp
rovide
detailhow
Item
7Are
inclusionandexclusioncriteriadescribed?
Yes
Inclusionandexclusioncriteriaareexplicitlyreported
Partially
Onlyinclusionbutn
otexclusioncriteriaareexplicitlyreported
No/NR
Inclusionandexclusioncriteriaarenotexplicitlyreported
Item
8Was
levelo
fcognitive
functio
ning
ofparticipantsassessed?
Yes
Levelof
cognitive
functio
ning
isreported
andbasedon
assessmentu
sing
astandardised
instrumentand
was
assessed
either
forthestudyor
with
inthepreceding3months
Partially
Levelof
cognitive
functio
ning
isreported
butisbasedon
previous
(non-recent)assessment
oron
methodotherthan
standardised
instrument(e.g.positio
nin
school
system
)or
cognitive
functio
nwas
assessed
butv
erybroadlyreported
(e.g.‘allp
articipantshad
FSIQ
sover
75as
assessed
by….’or
‘MAless
than
6months’)
No/NR
Levelof
cognitive
functio
ning
isnotreported
Rev J Autism Dev Disord (2015) 2:199–221 207
Tab
le2
(contin
ued)
Dom
ain
Criterion
Classification
Scoring
criteria
Are
samplecharacteristicsdescribed?
Age
Yes
Age
rangeandmeanarereported
Partially
Eith
eragerangeor
meanisreported
No/NR
Age
rangeandmeanarenotreported
Gender
Yes
Genderof
participantsisreported
Partially
Genderof
participantsissomehow
reported
(proportionald
atareported)
No/NR
Genderof
participantsisnotreported
ASD
subtype
Yes
ASD
subtypes
included
arereported
No
ASD
subtypes
included
arenotreported
Com
orbidities
Yes
Presence
anddetailof
relevant
comorbiditiesisreported
No
Presence
anddetailof
relevant
comorbiditiesisnotreported
Other
demographicvariables
Yes
Other
demographicvariablesarereported
(e.g.location,ethnicity,race)
No
Other
demographicvariablesarenotreported
Item
9*Based
ontheabove,isthesampleadequately
described?
Yes
Alltheabovedetails
aregiven
Partially
Mosto
ftheabovedetails
aregiven
No/NR
Fewor
none
oftheabovedetails
aregiven
Measures
Sensory
measures
Item
10*
Item
11*
Are
sensoryprocessing
patternsmeasuredusing
standardised
measuresof
sensoryprocessing?
Yes
Standardised
measuresareused
inthisstudy
Are
sensoryprocessing
patternsmeasuredusingvalid
measuresof
sensoryprocessing?
Partially
Non-standardisedmeasuresareused,but
referenceto
currentstandardisatio
nworkisprovided
No/NR
Non-standardisedmeasuresareused
Yes
Evidenceof
good
valid
ityof
themeasuresisprovided
inthisstudy(e.g.50%
ofthe
variance
explainedby
factors,correlations
with
‘gold’
standard
measures≥0
.70)
Partially
Evidenceof
valid
itynotp
rovidedin
thisstudy,butreference
tocitedstudiesproviding
evidence
ofacceptablevalid
ityof
themeasuresor
evidence
provided
forthewhole
measure,but
only
someitems/subscalesareused
inthestudy
No/NR
Non-validated
measuresareused
orno
reported
evidence
ofvalid
ityisprovided
Item
12*
Are
sensoryprocessing
patternsmeasuredusing
reliablemeasuresof
sensoryprocessing?
Yes
Evidenceof
good
reliabilityof
themeasuresisprovided
inthisstudy
(e.g.C
ronbach’salpha(s),ICC≥0
.7)
Partially
Evidenceof
reliabilitynotp
rovidedin
thisstudy,butreference
tocitedstudiesproviding
evidence
ofacceptablereliabilityof
themeasuresor
evidence
provided
forthewhole
measure,but
only
someitems/subscalesareused
inthestudy
No/NR
Non-reliablemeasuresareused
orno
reported
evidence
ofreliabilityisprovided
Item
13*
Are
themeasuresused
appropriateforusewith
anASD
populatio
n?Yes
Evidenceprovided
thattoolsused
have
been
standardised
andvalid
ated
foruse
with
ASD
populatio
nor
areASD
-specific
208 Rev J Autism Dev Disord (2015) 2:199–221
Tab
le2
(contin
ued)
Dom
ain
Criterion
Classification
Scoring
criteria
Partially
Tool
hasnotb
eenstandardised
forASD
populatio
nbutith
asbeen
valid
ated
oris
widelyused
inASD
research
orevidence
ofusewith
comparabledevelopm
ental
groups
isprovided
inthisstudy
No/NR
Noevidence
thattool
isappropriateforASD
populatio
n
Psychologicalcorrelatemeasure
Item
14*
Isthepsychologicalcorrelatemeasuredusing
standardised
measuresof
theconstruct?
Yes
Standardised
measuresareused
inthisstudy
Partially
Non-standardisedmeasuresused,but
referenceto
currentstandardisatio
nworkisprovided
No/NR
Non-standardisedmeasuresareused
Item
15*
Isthepsychologicalcorrelatemeasuredusing
valid
measuresof
theconstruct?
Yes
Evidenceof
good
valid
ityof
themeasuresisprovided
inthisstudy(e.g.50%
ofthe
variance
explainedby
factors,correlations
with
‘gold’
standard
measures≥0
.70)
Partially
Evidenceof
valid
itynotp
rovidedin
thisstudy,butreference
tocitedstudiesproviding
evidence
ofacceptablevalid
ityof
themeasuresor
evidence
provided
forthe
wholemeasure,but
only
someitems/subscalesareused
inthestudy
No/NR
Non-validated
measuresareused
orno
reported
evidence
ofvalid
ityisprovided
Item
16*
Isthepsychologicalcorrelatemeasuredusing
reliablemeasuresof
theconstruct?
Yes
Evidenceof
good
reliabilityof
themeasuresisprovided
inthisstudy
(e.g.C
ronbach’salpha(s),ICC≥0
.7)
Partially
Evidenceof
reliabilitynotp
rovidedin
thisstudy,butreference
tocitedstudiesproviding
evidence
ofacceptablereliabilityof
themeasuresor
evidence
provided
forthe
wholemeasure,but
only
someitems/subscalesareused
inthestudy
No/NR
Non-reliablemeasuresareused
orno
reported
evidence
ofreliabilityisprovided
Item
17*
Are
themeasuresused
appropriateforuse
with
anASD
populatio
n?Yes
Evidenceprovided
thattool
used
hasbeen
standardised
andvalid
ated
forusewith
ASD
populatio
nor
isASD
-specific
Partially
Tool
hasnotb
eenstandardised
forASD
populatio
n,butith
asbeen
valid
ated
oriswidelyused
inASD
research
orevidence
ofusewith
comparable
developm
entalg
roupsisprovided
inthisstudy
No/NR
Noevidence
thattool
isappropriateforASD
populatio
n
Results
Item
18Are
thedescriptivestatisticsappropriatelyreported?
Yes
The
descriptivestatisticsareappropriatelyreported
(e.g.M
,SD,range)
Partially
Onlysomeof
thedescriptivestatisticsarereported
orthedescriptivestatistics
arereported
forselected
constructs
No/NR
The
descriptivestatisticsarenotappropriately
reported
ornotreportedatall
Item
19Are
theresults
presentedclearly?
Yes
The
results
arepresentedclearly(e.g.tablesandfiguresareeasy
toread,clearly
labelled,thedescriptionof
theresults
iseasy
tofollo
w)
Partially
The
results
arepresentedsomehow
unclear
No/NR
The
presentatio
nof
theresults
isdifficulttofollo
w
Item
20Are
thepsychometricpropertiesreported
inthecurrentsam
ple?
Yes
Validity
andreliabilityarereported
inthecurrentsam
ple
Partially
Eith
ervalid
ityor
reliabilityisreported
inthecurrentsam
pleor
both
reported
only
forselected
constructs
Rev J Autism Dev Disord (2015) 2:199–221 209
Tab
le2
(contin
ued)
Dom
ain
Criterion
Classification
Scoring
criteria
No/NR
Validity
andreliabilityarenotreportedin
thecurrentsam
ple
Item
21Are
themissing
values
reported
and
howthey
werehandled?
Yes
Percentage
ofmissing
itemsandhowmissing
itemswerehandledaredescribed
inthestudyor
one-to-one
assessmentsareconducted
Partially
Percentage
ofmissing
itemsisdescribed,butsom
ehow
notclear
howmissing
itemswerehandled
No/NR
Percentage
ofmissing
itemsnotd
escribed
andnotreportedhowmissing
itemswerehandled
Analysis
Item
22Isthestatisticalanalysisappropriateto
thedesign?
Yes
The
analyticstrategy
isappropriateto
thedesign
Partially
The
analyticstrategy
isappropriatebuth
assomelim
itatio
ns(e.g.other
analyticalstrategy
would
have
been
morepowerfulo
rsomeassumptions
have
been
violated)
No/NR
Inappropriatestatisticaltestswereused
orinsufficient
inform
ationisprovided
tojudgethe
appropriatenessof
theanalysis
Item
23Isthesamplesize
sufficient?
Yes
Samplesize
isbasedon
appropriatepower
calculations,w
hich
areexplicitlyreported
Partially
Power
calculations
arenotreportedbutsam
plesize
appearssufficiently
large
No/NR
Nojustificationisgivenforsamplesize
andsamplesize
appearssm
all
Item
24Are
theeffectsizescalculated
andreported
inthestudy?
Yes
The
effectsizesarecalculated
forthedataandreported
inthestudy
Partially
The
effectsizesarecalculated
forthedata,but
notreportedin
thestudy
No/NR
Lackof
calculationof
theeffectsizesforthedata
Discussion
Item
25Dotheconclusionsfollo
wadequately
from
results?
Yes
Mainfindings
areclearlydescribedandfollo
wappropriatelyfrom
theresults
andanalyses
Partially
Somelim
itatio
nsin
theclarity
ofdescriptionof
mainfindings
andtheirrelatio
nto
results
No/NR
Lackof
appropriatedescriptionof
findings
and/or
findings
areover/understated
anddo
notfollow
clearlyfrom
results
Item
26Are
limitatio
nsacknow
ledged?
Yes
Clear
acknow
ledgem
ento
fmainlim
itatio
nsof
thestudyandconsiderationgivento
theim
pact
oftheseon
interpretatio
n
Partially
Somelim
itatio
nsareacknow
ledged
butn
otall,or
noconsiderationgivento
theim
pactof
limitatio
nson
interpretatio
n
No/NR
Noacknow
ledgem
ento
flim
itatio
ns
NRnotreported,*indicatesitemsincluded
intenselected
criteriaof
evaluatio
n
210 Rev J Autism Dev Disord (2015) 2:199–221

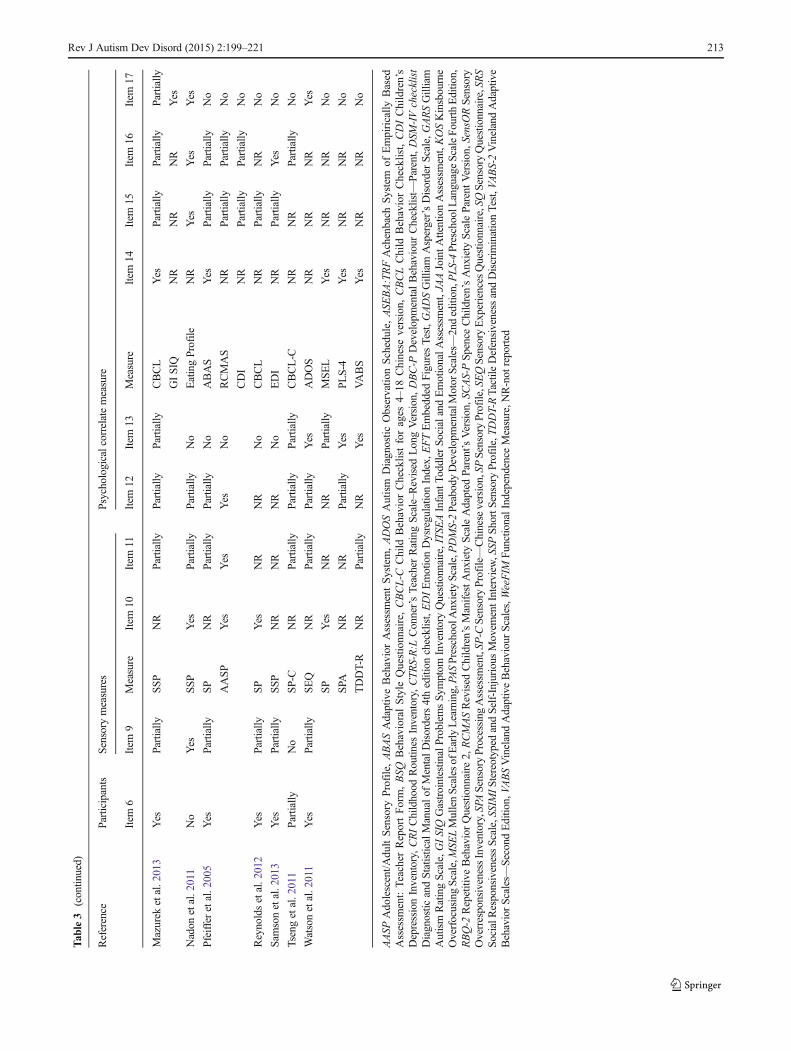
were informed with both observational data and parent re-ports, and in both studies further confirmatory factor analysiswas performed to ensure appropriate model fit to the data (inTable 3, information on each measure separately rather thanthe final models can be found). Pfeiffer et al. (2005) used twomeasures depending on the age of their participants and Laneet al. (2012) used two tools, reporting their outcomes as equiv-alent to each other. Hence, overall there were ten differentsensory measures used across the 21 selected papers (with38 tool’s references in total), with the Sensory Profile andShort Sensory Profile being used most frequently.
In eight studies, there was information about a sensory mea-sure being standardised (Gal et al. 2010; Jasmin et al. 2009;Lane et al. 2010, 2012; Nadon et al. 2011; Pfeiffer et al. 2005;Reynolds et al. 2012;Watson et al. 2011) with Liss et al. (2006)providing a reference to a current standardisation work.Remaining studies did not report on the measures’standardisation. Reliability was more often reported than valid-ity of the measures, with three studies providing calculations ofreliability—test-retest reliability (Baranek et al. 2013) and in-ternal consistency (Green et al. 2012; Pfeiffer et al. 2005, butonly for the Adolescent/Adult Sensory Profile, AASP). OnlyPfeiffer et al. (2005) provided discriminative and convergentvalidity calculations (for the AASP). Across the papers includ-ed in the review, there was no information regarding reliabilityof nine of the referenced tools used compared to 14 measuresmissing information on validity. Across the studies, four mea-sures were referenced as being appropriate for use with ASDpopulation or being ASD specific (Sensory ProcessingAssessment, SPA; Tactile Defensiveness and DiscriminationTest, TDDT-R; Sensory Experiences Questionnaire, SEQ; andSensory Questionnaire, SQ). Sensory Profile and Short SensoryProfile, in four and three studies, respectively, were reported aswidely used within the ASD research.
Psychological Correlate Measure Section
Thirty one different measures of psychological correlates wereused in the reviewed papers. Some of the tools were used inseveral publications, Child Behavior Checklist (CBCL) wasused in two language versions—English and Chinese, andVineland Adaptive Behaviour Scales were used in their orig-inal version and newest revision (VABS and VABS-2),resulting in 37 references to psychological correlate measuresacross selected papers. Only in six papers (Hilton et al. 2007;Lane et al. 2010; Lidstone et al. 2014; Mazurek et al. 2013;Pfeiffer et al. 2005; Watson et al. 2011) some measures werereported as standardised (SRS, VABS, SCAS-P, PAS, CBCL,ABAS, MSEL and PLS-4). The remaining papers did notindicate standardisation status of the tools used. In Liss et al.(2006), a tool measuring exceptional memory was used; how-ever, no information on tool development, measurement prop-erties or scoring criteria was given. Reliability calculations
were performed for four tools: inter-rater reliability for theJAA (Baranek et al. 2013), RBQ-2 (Lidstone et al. 2014),EDI (Samson et al. 2013) and test-retest for Eating Profile(Nadon et al. 2011). Structural validity was only calculatedfor the RBQ-2 in Lidstone et al. (2014) and face validity forEating Profile in Nadon et al. (2011). Across the reviewedstudies, there was no information about the reliability of the13 referenced measures and about the validity of 14 selectedtools. Across the studies, seven measures were referenced asbeing appropriate for use with ASD population or being ASDspecific (GARS, GADS, GI SIQ, Eating Profile, ADOS,RBS-R and SRS), and further five were reported as widelyused in ASD research or developmental disorders (JAA, EFT,VABS, KOS, CBCL).
Results—Associations
The authors selected different sensory patterns for their inves-tigation. Hyporesponsiveness was examined in Baranek et al.(2013); hyperresponsiveness in Green et al. (2012), Lane et al.(2012) andMazurek et al. (2013); hypo-, hyperresponsivenessand sensation seeking in Boyd et al. (2010), Brock et al.(2012) and Watson et al. (2011); a pattern combiningunderresponsiveness and sensation seeking in Ashburneret al. (2008), Baker et al.(2008), Chen et al. (2009), Galet al. (2010), Lane et al. (2010), Nadon et al. (2011) andSamson et al. (2013); and sensory processing patterns fromDunn’s model in Hilton et al. (2007), Jasmin et al. (2009),Lidstone et al. (2014), Reynolds et al. (2012) and Tsenget al. (2011). Liss et al. (2006) used terms sensory seekingand over- and under-reactivity, which were treated as syno-nyms of hyper- and hyporesponsiveness. Pfeiffer et al. (2005)examined hypo- and hypersensitivity which were treated sameas hypo- and hyperresponsiveness. Some authors preferredusing responsiveness, some responsivity—both were alsotreated as synonyms in this review.
In 12 papers (Baranek et al. 2013; Boyd et al. 2010; Brocket al. 2012; Gal et al. 2010; Green et al. 2012; Hilton et al.2007; Lane et al. 2010, 2012; Liss et al. 2006; Nadon et al.2011; Reynolds et al. 2012; Samson et al. 2013), investigationof associations between sensory processing patterns and a sin-gle psychological construct was carried out. Three of thesepapers have multiple hypotheses on the sub-constructs of thephenomenon under investigation that were tested. Baraneket al. (2013) looked at joint attention and reported the resultsfor both initiation of and response to joint attention. Brock et al.(2012) were interested in sensory patterns’ association withseveral dimensions of temperament such as withdrawal, dis-tractibility, persistence or slowness to adapt, and in Liss et al.(2006) the concept of overarousal was characterised byoverfocused behaviour, perseverative preoccupation and ex-ceptional memory for self-selected material. In the remainingstudies, the relationship between sensory processing
Rev J Autism Dev Disord (2015) 2:199–221 211
Tab
le3
Scoringagainstselectedcriteria
Reference
Participants
Sensory
measures
Psychologicalcorrelatemeasure
Item
6Item
9Measure
Item
10Item
11Item
12Item
13Measure
Item
14Item
15Item
16Item
17
Ashburner
etal.2008
Partially
Partially
SSP
NR
NR
Partially
No
CTRS-R:L
NR
Partially
Partially
No
ASEBA:TRF
NR
Partially
Partially
No
GARS
NR
Partially
Partially
Yes
GADS
NR
Partially
Partially
Yes
Baker
etal.2008
Yes
Partially
SSP
NR
Partially
Partially
No
VABS
NR
NR
NR
No
DBC-P
NR
NR
NR
No
Baranek
etal.2013
Yes
Partially
SPA
NR
NR
Yes
Yes
MSEL
Yes
Partially
Partially
No
PLS-4
Yes
Partially
Partially
No
JAA
NR
Partially
Yes
Partially
Boydetal.2010
Yes
Partially
SP
NR
NR
NR
No
RBS-R
NR
Partially
Partially
Yes
SEQ
NR
NR
NR
No
TDDT-R
NR
NR
NR
No
SPA
NR
NR
NR
Yes
Brock
etal.2012
Yes
Partially
SP
NR
NR
Partially
Partially
BSQ
NR
Partially
Partially
No
SEQ
NR
Partially
Partially
Yes
TDDT-R
NR
Partially
Partially
Partially
SPA
NR
NR
Partially
Yes
Chenetal.2009
Yes
Partially
SSP
NR
NR
Partially
Partially
CRI
NR
Partially
Partially
No
EFT
NR
Partially
NR
Partially
Galetal.2010
Partially
Partially
SSP
Yes
Partially
Partially
Partially
SSIM
INR
NR
Partially
No
Green
etal.2012
Yes
Partially
ITSEA
NR
NR
Yes
No
ITSEA
NR
NR
Partially
No
Hilton
etal.2007
Partially
Partially
SP
NR
Partially
Partially
Partially
SRS
Yes
Partially
Partially
Yes
Jasm
inetal.2009
Yes
Partially
SP
Yes
Partially
Partially
No
PDMS-2
NR
NR
Partially
No
WeeFIM
NR
Partially
Partially
No
VABS-2
NR
NR
Partially
No
Laneetal.2010
Yes
Partially
SSP
Yes
Partially
Partially
No
VABS
Yes
Partially
Partially
Partially
Laneetal.2012
Partially
No
SP
Yes
Partially
Partially
No
RCMAS
NR
Partially
Partially
No
SensO
RNR
Partially
Partially
No
Lidstoneetal.2014
Yes
Partially
SP
NR
Partially
Partially
No
RBQ-2
NR
Partially
Yes
No
SCAS-P
Yes
Partially
Partially
No
PAS
Yes
Partially
NR
No
Lissetal.2006
Partially
No
SQ
Partially
Partially
NR
Yes
DSM-IVchecklist
NR
NR
NR
No
KOS
NR
Partially
NR
Partially
VABS
Yes
NR
NR
No
212 Rev J Autism Dev Disord (2015) 2:199–221
Tab
le3
(contin
ued)
Reference
Participants
Sensory
measures
Psychologicalcorrelatemeasure
Item
6Item
9Measure
Item
10Item
11Item
12Item
13Measure
Item
14Item
15Item
16Item
17
Mazurek
etal.2013
Yes
Partially
SSP
NR
Partially
Partially
Partially
CBCL
Yes
Partially
Partially
Partially
GISIQ
NR
NR
NR
Yes
Nadon
etal.2011
No
Yes
SSP
Yes
Partially
Partially
No
EatingProfile
NR
Yes
Yes
Yes
Pfeifferetal.2005
Yes
Partially
SP
NR
Partially
Partially
No
ABAS
Yes
Partially
Partially
No
AASP
Yes
Yes
Yes
No
RCMAS
NR
Partially
Partially
No
CDI
NR
Partially
Partially
No
Reynoldsetal.2012
Yes
Partially
SP
Yes
NR
NR
No
CBCL
NR
Partially
NR
No
Sam
sonetal.2013
Yes
Partially
SSP
NR
NR
NR
No
EDI
NR
Partially
Yes
No
Tsengetal.2011
Partially
No
SP-C
NR
Partially
Partially
Partially
CBCL-C
NR
NR
Partially
No
Watsonetal.2011
Yes
Partially
SEQ
NR
Partially
Partially
Yes
ADOS
NR
NR
NR
Yes
SP
Yes
NR
NR
Partially
MSEL
Yes
NR
NR
No
SPA
NR
NR
Partially
Yes
PLS-4
Yes
NR
NR
No
TDDT-R
NR
Partially
NR
Yes
VABS
Yes
NR
NR
No
AASP
Adolescent/A
dultSensory
Profile,ABASAdaptiveBehaviorAssessm
entSystem,ADOSAutism
Diagnostic
Observatio
nSchedule,
ASE
BA:TRFAchenbach
System
ofEmpirically
Based
Assessm
ent:Teacher
ReportForm,BSQ
BehavioralStyle
Questionnaire,CBCL-C
Child
BehaviorChecklistforages
4–18
Chinese
version,
CBCLChild
BehaviorChecklist,CDIChildren’s
DepressionInventory,CRIChildhood
Routin
esInventory,CTRS-R:L
Conner’sTeacherRatingScale–R
evised
LongVersion,DBC-P
DevelopmentalBehaviour
Checklist—
Parent,DSM
-IVchecklist
Diagnostic
andStatisticalManualof
MentalDisorders4thedition
checklist,EDIEmotionDysregulatio
nIndex,
EFTEmbedded
FiguresTest,G
ADSGilliam
Asperger’sDisorderScale,G
ARSGilliam
Autism
RatingScale,G
ISIQGastrointestin
alProblemsSy
mptom
InventoryQuestionnaire,ITS
EAInfant
ToddlerSo
cialandEmotionalA
ssessm
ent,JA
AJointA
ttentionAssessm
ent,KOSKinsbourne
OverfocusingScale,M
SELMullenScales
ofEarlyLearning,PA
SPreschoolA
nxietyScale,P
DMS-2PeabodyDevelopmentalM
otorScales—2ndedition,P
LS-4PreschoolL
anguageScaleFourthEditio
n,RBQ-2
Repetitive
BehaviorQuestionnaire
2,RCMASRevised
Children’sManifestAnxiety
ScaleAdapted
Parent’sVersion,S
CAS-PSp
ence
Children’sAnxiety
ScaleParent
Version,S
ensO
RSensory
OverresponsivenessInventory,SPASensory
Processing
Assessm
ent,SP
-CSensoryProfile—Chineseversion,SP
SensoryProfile,SEQSensoryExperiencesQuestionnaire,SQSensoryQuestionnaire,SRS
SocialResponsivenessScale,SSIMIStereotypedandSelf-Injurious
Movem
entInterview
,SSP
ShortSensory
Profile,T
DDT-RTactile
DefensivenessandDiscrim
inationTest,V
ABS-2VinelandAdaptive
BehaviorScales—
Second
Editio
n,VA
BSVinelandAdaptiveBehaviour
Scales,W
eeFIM
Functio
nalIndependenceMeasure,N
R-not
reported
Rev J Autism Dev Disord (2015) 2:199–221 213

atypicalities and two (Baker et al. 2008; Chen et al. 2009;Jasmin et al. 2009; Lidstone et al. 2014; Mazurek et al. 2013;Tseng et al. 2011;Watson et al. 2011) or more (Ashburner et al.2008; Pfeiffer et al. 2005) constructs were explored. Data ex-traction was carried out for each construct separately and forthis reason those papers investigating multiple constructs wereincluded in the review results’ sections more than once.
Participants
Across the 21 studies included in the review, a total of 4149children and adolescents with ASD were included. One studyrecruited 2973 participants (Mazurek et al. 2013); the remain-ing studies involved between 22 and 149 participants.
The age of participants ranged from 20 months to 17 years(overall mean age=7.09 years). One study focussed particular-ly on toddlers (Green et al. 2012; with a mean of 28.2 months).Nine studies (Baker et al. 2008; Baranek et al. 2013; Boydet al. 2010; Brock et al. 2012; Jasmin et al. 2009; Lane et al.2010; Nadon et al. 2011; Tseng et al. 2011; Watson et al. 2011)focussed on early and middle childhood (20 to 115 months). Afurther nine studies (Ashburner et al. 2008; Chen et al. 2009;Gal et al. 2010; Hilton et al. 2007; Lane et al. 2012; Liss et al.2006; Pfeiffer et al. 2005; Reynolds et al. 2012; Samson et al.2013) included children and adolescents betweenmiddle child-hood and mid-teens (6 to 17 years). Two studies included bothchildren and adolescents; Lidstone et al. (2014) recruited 3–17-;9-year-old participants and Mazurek et al.(2013) used asample between 2 and 17 years old.
In all the studies, the gender of the participants was report-ed and 84.3 % of participants were male. This percentagemirrors the widely reported uneven sex ratio for theprevalence of ASD in males, with males being fourtimes more likely of having this condition than females(Anello et al. 2009).
A minority of studies were highly selective when recruitingparticipants with a particular diagnosis. Pfeiffer et al. (2005)included only children and adolescents who had Asperger’ssyndrome, while Hilton et al. (2007) included only childrenwith High Functioning ASD. Four studies included partici-pants across the spectrum. Chen et al. (2009) included thosewith a diagnosis of ASD or Asperger’s syndrome; Green et al.(2012) recruited toddlers with either autism or PDD-NOS;Jasmin et al. (2009) included in their study children with ADor PDD-NOS. In a couple of studies, participants werecharacterised as diagnosed with autism (Tseng et al. 2011;Gal et al. 2010) and further five (Baker et al. 2008; Baraneket al. 2013; Boyd et al. 2010; Lane et al. 2010; Watson et al.2011) included those with autistic disorder. In the remainingstudies, participants fell into the general diagnostic categoryfor ASD. Only Mazurek et al. (2013) and Nadon et al. (2011)reported an exact percentage of ASD children in each diag-nostic category (AD, Asperger’s disorder, PDD-NOS).
The method of reporting cognitive ability varied markedlyacross the reviewed studies. Ability in the form of an IQ scorewas reported by Lane et al. (2012), Reynolds et al. (2012) andSamson et al. (2013), with the following means (standarddeviations): 95.5 (18), 95.88 (17.8) and 82.75 (23.61), respec-tively. Standard score of 61.3 (26.5) was reported in Jasminet al. (2009). Green et al. (2012) stated non-verbal and verbaldevelopmental functioning (78.1 (18.06) and 58.62 (25.15))of their participants, whereas Baranek et al. (2013), Boydet al. (2010), Brock et al. (2012) and Watson et al. (2011)reported mental age (23.25 (14.04), 31.97 (20.84), 36.11(19.88) and 32.0 (20.6), respectively). Ashburner et al.(2008) included only participants with IQ above 80, whileChen et al. (2009) and Hilton et al. (2007) included indi-viduals with ASD with IQ above 70. Mazurek et al.(2013) reported that 3.9 % of their sample had an IQlower than 70, while the remaining sample had IQ above70. Remaining authors did not provide any indicators ofcognitive functioning of their participants.
Only two studies reported co-occurring medical con-ditions for their participants. Nadon et al. (2011) report-ed attention deficit disorder, hyperactivity and mentalretardation as the most common co-occurring conditions,while in Hilton et al. (2007) attention deficit/hyperactivitydisorder, learning disability, anxiety disorder, depressionand Tourette syndrome were reported as additionaldiagnoses.
Psychological Constructs
In the selected studies, the authors examined relationshipsbetween sensory processing patterns and a variety of psycho-logical constructs. In order to present our findings in a system-atic way, the papers have been grouped. In the most recentDiagnostic and Statistical Manuals of Mental Disorders, corefeatures of ASD, such as impairments in the social use of bothnon-verbal and verbal communication and presence of re-stricted, repetitive patterns of behaviour, interests or activities,are diagnostic components for the disorder (APA 2013). Inaddition to these core features that are present in individualswith ASD, a number of associated difficulties have been listedin the Diagnostic and Statistical Manual of Mental Disorders(DSM-IV-TR; APA 2000); these include emotional, attention-al, cognitive and behavioural problems. The psychologicalconstructs examined in the selected papers have been groupedaccordingly, either belonging to the core features of ASD,such as social functioning and repetitive behaviours, orcharacterised as associated conditions of ASD, e.g. affectiveand cognitive difficulties. As a result, six main groups of psy-chological constructs were created: symptom severity, socialfunctioning, restricted and repetitive behaviours, emotionaland behavioural functioning, affective and cognitive symp-toms, and physical skills.
214 Rev J Autism Dev Disord (2015) 2:199–221

In the identified groups, the following constructs were in-cluded (as indicated by the authors):
& symptom severity: social communicative symptoms(Watson et al. 2011), social competence (Hilton et al.2007), social symptoms/communication impairment(Liss et al. 2006), autism quotient and Asperger’s disorderquotient (Ashburner et al. 2008);
& social functioning: language skills (Watson et al. 2011),language abilities (Baranek et al. 2013), social and com-munication adaptive skills (Watson et al. 2011) and jointattention (Baranek et al. 2013);
& restricted and repetitive behaviours: restricted and repeti-tive behaviours (Chen et al. 2009; Boyd et al. 2010;Lidstone et al. 2014) and stereotyped movement (Galet al. 2010);
& emotional and behavioural functioning: emotional, behav-ioural and educational outcomes (Ashburner et al. 2008),emotional and behavioural problems (Tseng et al. 2011),emotion dysregulation (Samson et al. 2013), adaptive/maladaptive functioning (Baker et al. 2008; Lane et al.2010; Liss et al. 2006; Pfeiffer et al. 2005), behaviouralresponsiveness (Baker et al. 2008), gastrointestinal prob-lems (Mazurek et al. 2013), eating (Nadon et al. 2011) andsleep (Reynolds et al. 2012) problems;
& affective and cognitive symptoms:
affective: temperament (Brock et al. 2012), anxiety(Green et al. 2012; Lane et al. 2012; Lidstone et al.2014; Mazurek et al. 2013; Pfeiffer et al. 2005), depres-sion (Pfeiffer et al. 2005),cognitive: memory (Liss et al. 2006), cognitive style(Chen et al. 2009), attention (Liss et al. 2006);
& physical skills: motor skills (Jasmin et al. 2009) and dailyliving skills (Jasmin et al. 2009).
Symptom Severity
Four papers investigated associations between sensoryatypicalities and symptom severity. Ashburner et al. (2008)found a significant negative correlation between theunderresponsive/seeks sensation subscale of the ShortSensory Profile and GARS autism quotient (r=−0.53 p=0.003), but not with GADS Asperger’s disorder quotient, sug-gesting more sensory problems being associated with moreautism symptoms (low score on the SSP indicates more sensoryissues). Hilton et al. (2007) reported significant associationsbetween all sensory processing patterns as measured by theSensory Profile and SRS scores, both total score (correlationswith Sensory Sensitivity, r=−0.745, p<0.01; SensoryAvoiding, r=−0.796, p<0.01; Low Registration, r=−0.578,
p<0.01; and Sensation Seeking, r=−0.527, p<0.01) and sub-scales, with the exception of SRS social awareness for whichonly sensory sensitivity and sensation avoiding were found tobe negatively correlated. Liss et al. (2006) found significantcorrelations between overreactivity, underreactivity and sensa-tion seeking and all the subscales of DSM-IV checklist. Onlythe DSM-IV communication impairment subscale was not sig-nificantly associated with overreactivity. Watson et al. (2011)used ADOS as one of the outcome measures in their study andfound associations between social-communicative algorithmscores and both hyporesponsiveness (β=0.48, SE=0.023,p=0.040) and sensation seeking (β=0.78, SE=0.025,p=0.002).
Social Functioning/Social Skills
The relationship between sensory processing patterns and ver-bal and non-verbal communication skills in individuals withASD was investigated in two studies. Baranek et al. (2013)were interested in associations between sensory difficultiesand language abilities and joint attention. Watson et al.(2011) explored the relationships between sensory atypical-ities and language skills, social and communication adaptiveskills. All verbal and non-verbal variables were associatedwith sensory hyporesponsiveness (Receptive language ratioscores, β=−2.0, SE=0.68, p=0.004; Expressive language ra-tio scores, β=−2.1, SE=0.73, p=0.005; Receptive JointAttention, β=−0.83, SE=0.37, p=0.025; Initiating JointAttention, β=−1.63, SE=0.59, p=0.006; Aggregate languagequotient scores, β=−0.010, SE=0.004, p=0.018; Social adap-tive scores, β=−0.017, SE=0.007, p=0.011). Also in Watsonet al. (2011) language skills (aggregate language quotientscores) were correlated with sensory seeking (β=−0.011,SE=0.004, p=0.005).
Restricted and Repetitive Behaviours (RRBs)
Restricted and repetitive behaviours (RRBs) is a broad termwhich includes behaviours ranging from self-injurious behav-iour and stereotyped motor mannerisms through insistence onsameness and circumscribed interests (Bodfish et al. 2000).Turner (1999) suggested distinguishing two levels of behav-iours—‘lower level’ including motor repetitions and stereo-typed behaviours, and ‘higher level’ relating to insistence onsameness and circumscribed interests. This division of RRBsinto two separate levels is present in the studies included inour review, hence we present the results distinguishing be-tween ‘lower’ and ‘higher’ levels of RRBs.
Four papers looked at the relationship between sensory pro-cessing patterns and the presence of restricted and repetitivebehaviours. Boyd et al. (2010) reported a significant associationbetween hyperresponsiveness and stereotypy (β=3.40, SE=1.35, p=0.012). Gal et al. (2010) found a significant negative
Rev J Autism Dev Disord (2015) 2:199–221 215

correlation between the number of Different StereotypedMovements and the underresponsiveness/seeks sensation sub-scale of Short Sensory Profile (r=−0.43, p<0.001). Lidstoneet al. (2014) reported significant negative correlations betweenrepetitive motor behaviours and sensation avoiding and sensa-tion seeking (r=−0.42, p<0.01 for both). In the same study,significant negative correlations were found between all sensoryprocessing patterns and insistence of sameness (correlationswith Sensory Sensitivity, r=−0.43, p<0.01; Sensory Avoiding,r=−0.49, p<0.01; Low Registration, r=−0.38, p<.01; andSensation Seeking, r=−0.49, p<0.01). Chen et al. (2009),however, did not f ind any associat ions betweenunderresponsiveness/seeks sensation patterns and ‘compul-sive-like behaviours’. Compulsions were associated withhyperresponsiveness in Boyd et al. (2010) study (β=3.50,SE=1.41, p=0.013). The authors found also significant associ-ations between rituals and both hyperresponsiveness (β=4.47,SE=1.35, p=0.001) and sensory seeking (β=5.92, SE=2.97,p=0.046).
Emotional and Behavioural Functioning
Seven papers examined associations between sensorydifficulties and the emotional and behavioural functioning ofindividuals with ASD. Ashburner et al. (2008) reported sig-nificant correlations between the underresponsive/seeks sen-sation subscale of the Short Sensory Profile and three sub-scales of Conner’s Teacher Rating Scale–Revised LongVersion, cognitive problems/inattention (r=−0.48, p<0.01),social problems (r=−0.32, p<0.05) and inattentive (r=−0.42, p<0.05). They also found significant associations ofthe Short Sensory Profile underresponsiveness/seeks sensa-tion subscale and two of the subscales of the AchenbachSystem of Empirically Based Assessment: Teacher ReportForm, namely thought problems (r=−0.39, p<0.05) and aca-demic performance (r=0.62, p<0.01). Baker et al. (2008)using the Short Sensory Profile reported correlations withthe following subscales of the Developmental BehaviourChecklist subscales: self-absorbed (r=−0.523, p=0.012),Autism Screening Algorithm (r=−0.533, p=0.011) and totalscore (r=−0.491, p=0.020); and maladaptive behaviour scaleof Vineland Adaptive Behaviour Scales (r=−0.482, p=0.023). Lane et al. (2010) also found similar associations withthe maladaptive behaviour scale of the VABS. Using theVABS, Liss et al. (2006) reported correlations between thesocialisation subscale and hyperresponsiveness (r=−0.195,p<0.05), VABS daily living and adaptive behaviour compos-ites and hyporesponsiveness (r=−0.326, p<0.01 andr=−0.221, p<0.01, respectively) and sensory seeking withthe VABS communication (r=−0.263, p<0.01), daily living(r=−0.165, p<0.05) and adaptive behaviour composite(r=−0.235, p<0.01). Pfeiffer et al. (2005) investigated rela-tionships between sensory processing patterns and adaptive
behaviours. They found significant negative associations be-tween both hypo- and hypersensitivity and community use(r=−0.271, p=0.05 and r=−0.291, p=0.041, respectively)and social skills subscales of the Adaptive BehaviorAssessment System (r=−0.298, p=0.036 and r=−0.278,p=0.05, respectively). Samson et al. (2013) looked at emotiondysregulation and its relationship with sensory atypicalities,reporting higher emotion regulation difficulties in those indi-viduals with ASD who also had high scores on theunderresponsive/seeks sensation subscale of the SSP(r=−0.57, p<0.001). Tseng et al. (2011) were interested insensory processing dysfunction and children’s emotional andbehavioural problems. They used the Child BehaviorChecklist to measure both internalising and externalising dif-ficulties and found a number of significant associations ofthose dimensions with all the sensory processing patterns.Internalising was negatively associated with SensorySensitivity: r=−0.24, p=0.047, Sensory Avoiding: r=−0.43,p<0.001, Low Registration: r=−0.28, p=0.020 and SensationSeeking: r=−0.43, p<0.001, while externalising correlatedsignificantly with Sensory Sensitivity: r=−0.30, p=0.013,Sensory Avoiding: r=−0.29, p=0.016 and SensationSeeking: r=−0.29, p=0.016.
The relationship between associated behavioural problemswith ASD and sensory processing difficulties was investigatedin three studies. Mazurek et al. (2013) reported that thosechildren with ASD who had chronic GI problems such aschronic constipation, chronic abdominal pain, chronicbloating, chronic nausea and chronic diarrhoea had signifi-cantly lower sensory overresponsivity scores (greater levelsof overresponsivity) than those children with ASD who hadno additional GI problems (d=−0.36 to −0.71, p<0.0001).Nadon et al. (2011) did not find any significant associationsbetween underresponsive/ seeks sensation subscale of theShort Sensory Profile and the mean number of eatingproblems in children with ASD. Reynolds et al. (2012) report-ed significant positive correlation between sensation avoidingand sleep problems (r=0.502, p=0.11); associations with oth-er sensory processing patterns were not significant.
Affective and Cognitive Difficulties
Affective Symptoms
Six papers investigated the relationships between sensory pro-cessing patterns and affective symptoms such as dimensionsof temperament, anxiety and depression. Brock et al. (2012)looked at how sensory atypicalities relate to temperament di-mensions in children with ASD. Three out of the nine inves-tigated dimensions were associated with only one particularpattern, namely hyporesponsiveness (adaptability, β=0.38,p=0.001; distractibility, β=−0.46, p<0.0001; reactivity,
216 Rev J Autism Dev Disord (2015) 2:199–221

β=−0.28, p=0.04), reporting that children with ASD whoshow hyporesponsive behaviours may be more susceptibleto various distractions and their optimal level of engagementwith the environment may be narrower, elongating ad-justment to change. In all five papers in which the re-lationship between anxiety and sensory patterns was ex-amined (Green et al. 2012; Lane et al. 2012; Lidstoneet al. 2014; Mazurek et al. 2013; Pfeiffer et al. 2005),correlations between hyperresponsiveness and anxietywere found and reported by four authors although a numberof different measures were used across the studies (Green et al.2012: r=0.52, p<0.001 (time 1) and r=0.60, p<0.001 (time2); Lane et al. 2012: r=0.18, p<0.001; Mazurek et al. 2013:r=−0.45, p<0.0001; Pfeiffer et al. 2005:r=0.476, p<0.001).Lids tone et a l . (2014) looked a t dimensions ofhyperresponsiveness (both sensory sensitivity and sensationavoiding), and further moderate to strong correlations werereported (r=−0.61, p<0.01 and r=−0.71, p<0.01, respective-ly). Only Lidstone et al. (2014) stated a relationship betweenanxiety and low registration (r=−0.40, p<0.01). Depressionwas associated with hyperresponsiveness (r=0.394, p=0.005for the total sample, and for the younger children r=0.449,p=0.013, but not for the teenage group) as reported by Pfeifferet al. (2005), but also with hyporesponsiveness (r=0.214,p=0.05 for the total sample, non-significant associations forthe younger children and significant for the teenagers,r=0.492, p=0.027) and hyporesponsiveness dimensions(low registration was significantly associated with depressiononly in the teenage group r=0.483, p=0.031, and sensationseeking correlated with depression when the total sample wasused r=0.299, p=0.035).
Cognitive Symptoms
The relationship between cognitive functioning and sensoryabnormalities in children with ASD was examined in twostudies. Chen et al. (2009) were interested in exploring therelationship between sensory difficulties and an individual’sdetail-focused cognitive style. Only non-significant associa-tions between the under responsive/seeks sensation subscaleof the Short Sensory Profile and the Embedded Figure Testwere reported. Liss et al. (2006) looked at both ability to shiftattentional focus and exceptional memory for self-selected material in individuals with ASD. They showedthat although underreactivity and sensory seeking weresignificantly correlated with Kinsbourne OverfocusingScale (r=0.293, p<0.01 and r=0.235, p<0.01, respec-tively), the strongest positive correlation was found withoverreactivity (r=0.608, p<0.01). Overreactivity was alsonegatively correlated with the reverse log of the exceptionalmemory score (r=−0.196, p<0.05), showing an associationbetween greater exceptional memory and individual’soverreactivity to sensory stimuli.
Physical Skills
Only one study investigated the relationship between sensoryprocessing patterns and motor skills with daily living skills (asself-care skills) in children with ASD. Jasmin et al. (2009)reported significant correlations between only one sensorypattern, namely sensation avoiding and self-care domain ofthe WeeFIM (r=0.388, p<0.025), personal (r=0.457,p<0.011) and daily living skills (r=0.372, p<0.033) domainson the VABS-2. Also, sensation seeking was positively corre-lated with gross motor skills as measured by PDMS-2(r=0.39, p<0.03). The authors also looked at the associationseparately for AD and PDD-NOS groups. For the AD group,significant correlations were reported between the sensationavoiding and self-care (r=0.44, p<0.04), personal (r=0.56,p<0.01) and daily living skills (r=0.48, p<0.02) domains,and between low registration and personal skills (r=0.44,p<0.05). For the PDD-NOS group, however, the only signif-icant correlation was found between sensation seeking and theself-care domain (r=0.71, p<0.03).
Discussion
This systematic review focused on 21 studies that examinedrelationships between sensory processing patterns and psy-chological constructs in individuals with ASD.
Evaluation Grid—Papers’ Quality
The evaluation grid was designed for the purpose of this re-view, although it could be used in other reviews evaluatingstudies using correlational analysis methods in ASD research.The grid could be also easily adapted to be used in a widercontext of developmental disorders research or even typicaldevelopment. However, as it was used first time in the review,its validity is not established.
A confirmation of the diagnosis of ASD is provided in allthe papers included in the review. Some authors selected par-ticipants with a particular ASD subtype, with most of the au-thors reporting their participants as children and/or young peo-ple with ASD. In the new DSM-V (APA 2013), all the ASDsubtypes that were present in the previous version of theManual (APA 1994), namely, autistic disorder, Asperger’s dis-order and PDD-NOS (pervasive developmental disorder nototherwise specified), were merged together under the umbrellaof one term—autism spectrum disorder. This is important tobear in mind because findings from those studies, in whichparticipants with only one ASD subtype were included, mightbe less generalisable to future studies, in which participantsfrom across the spectrum will be included. Interestingly, inthe study in which the results were presented for a total sample,and for two subtypes separately—AD and PDD-NOS groups
Rev J Autism Dev Disord (2015) 2:199–221 217

(Jasmin et al. 2009), the findings differed for each subtype andfor the total sample. ASD is a very heterogeneous disorder, witha diverse presentation across individuals. It seems thereforeimportant to report both basic participants’ characteristics suchas gender and age, as well as features such as cognitive abilityin order to make some comparisons and generalisations be-tween and within such a varied population.
A wide variety of measures were used to assess sensoryprocessing difficulties in individuals with ASD in the selectedreview papers. Some authors, however, did not report whetherthe selected tools were appropriate to use with this clinicalpopulation. Only a few were reported as widely used withinthe ASD population or were ASD specific. Also, reliabilityand particularly validity of the tools were poorly reported.There is a lack of reliable and valid measures of sensory pro-cessing designed for use with ASD individuals. By usingmeasures developed with and for typically developing indi-viduals in ASD research without at least reporting their psy-chometric properties in this population, we have little evi-dence that the tools selected are appropriate. Therefore, re-searchers should consistently report psychometric propertiesof the tools used in the sample selected. Moreover, there are agreat number of questionnaires and observational measures ofsensory atypicalities available for use for researchers. Thedecision regarding which tools should be used to examine aresearch question might be based on a number of reasons, e.g.the measures selected in the previous studies, common use oftools by particular research group. There is no consensus be-tween researchers about which measures of sensory process-ing should be used in future studies. This lack of consensus on‘best-measures’ makes the comparison and interpretation ofthe results, obtained by employing different measures, prob-lematic. Time spent identifying and developing ‘gold-stan-dard’ sensory processing measures would help in understand-ing and interpreting the findings. Some authors (Boyd et al.2010; Brock et al. 2012; Watson et al. 2011), rather than usinga single measure, developed a sensory processing modelbased on information obtained from a range of measures andinformants. Through this approach, the authors tried to over-come some limitations associated with using single, mainlyparent-report-based measures and they yielded stronger sen-sory constructs scores. Building the factor analytic models isan interesting suggestion in sensory atypicalities measurementfield. The models not only conglomerate information fromdifferent measures but also have excellent structural validityscores. Researchers might consider implementing this form ofmeasuring sensory processing patterns in their studies.
Across the nine instruments of sensory atypicalities used inthe paper selected for this review, the Sensory Profile andShort Sensory Profile were most frequently used. It shouldbe remembered, however, that the Short Sensory Profile pro-vides very limited information in regards to sensory process-ing patterns of individuals with ASD. Researchers might
consider using tools which provide information on at leasthypo- and hyperresponsivity to follow the dimensions of sen-sory atypicalities as suggested by DSM-V (APA 2013).
Thirty two different measures were used in the reviewedpapers to assess psychological constructs in the ASD samplesstudied. Similar to the sensory processing measures, the psy-chometric properties of the selected tools were poorly reported(particularly the validity of the measures). Also, their appropri-ateness for use with this particular population was not justified.If excluding those tools which were used for both diagnosis andoutcome measurements, only eight were reported as appropri-ate for use in autism research. There is not only a lack of toolsdesigned specifically to assess a number of problems associatedwith the ASD, but also a lack of consensus regarding whichmeasures are best suited to each specific phenomenon. As aresult, researchers use different measures to investigate thesame constructs (e.g. anxiety). Interpretation of the results andtheir generalisability is therefore hampered. As alreadyhighlighted in the systematic review conducted by theMeASURe team (McConachie et al. 2015, in press), for chil-dren with ASD under 6, psychometric work still needs to bedone in order to select those tools which are reliable and validwithin autism research.
Sensory Processing Patterns and Correlates
Concentrating on two main dimensions of sensory responsive-ness—hyper- and hyporesponsiveness, as distinguished andsuggested in DSM-V (APA 2013), most of the measures ofautism symptom severity were associated with hyporespon-siveness (GARS autism quotient in Ashburner et al. 2008,DSM-IV communication impairment in Liss et al. 2006,ADOS social-communicative algorithm score in Watson et al.2011 and DBS ASA in Baker et al. 2008). What is notable,however, is that in those papers investigating the relationshipsbetween symptom severity and sensory atypicalities, associa-tions were found despite a wide range of symptom severityoutcome measures being used, different groups included(HFASD in Hilton et al. 2007; ASD in Ashburner et al. 2008and Liss et al. 2006; AD inWatson et al. 2011) and different agegroups of participating children (although they all were up to10 years old). It might indicate that those sensory atypicalitieswere so prevalent that they could be detected across ASD sub-types and with different measures. However, when the SRSwas used (Hilton et al. 2007), correlations were found with bothhypo- and hyperresponsiveness, with the social awareness sub-scale correlating only with hyperresponsiveness. Also, DMS-IV social symptoms subscale (Liss et al. 2006) was associatedsolely with hyperresponsiveness. Language and socio-communication variables (Baranek et al. 2013; Pfeiffer et al.2005; Watson et al. 2011), joint attention (Baranek et al. 2013),stereotyped movement (Gal et al. 2010), a number of cognitiveand social problems (Ashburner et al. 2008), maladaptive
218 Rev J Autism Dev Disord (2015) 2:199–221

behaviours (Baker et al. 2008; Lane et al. 2010), some mooddimensions (Brock et al. 2012), emotion dysregulation(Samson et al. 2013) and gross motor skills (Jasmin et al.2009) were all associated with hyporesponsiveness. On theother hand, self-care variables (Jasmin et al. 2009), anxiety(Green et al. 2012; Lane et al. 2012; Lidstone et al. 2014;Mazurek et al. 2013; Pfeiffer et al. 2005), socialisation subscaleon the VABS (Liss et al. 2006), GI problems (Mazurek et al.2013) and sleep difficulties (Reynolds et al. 2012) were corre-lated with hyperresponsiveness. Some variables were also as-sociated with both sensory patterns, repetitive motor behav-iours (Lidstone et al. 2014), insistence on sameness (Lidstoneet al. 2014), depression (Pfeiffer et al. 2005), anxiety inLidstone et al. (2014), attention (Liss et al. 2006), communityuse and social skills in Pfeiffer et al. (2005) study, andinternalising and externalising scores (Tseng et al. 2011).
This evidence suggests that sensory hyporesponsiveness ismore often associated with core features of ASD such as com-munication impairment, emotional, cognitive and behaviouralproblems while social awareness difficulties and affectivedisorders are associated with hyperresponsiveness. Similarly,Gay et al. (2008) suggested that hyporesponsiveness and sen-sory seeking may be more associated with difficulties insocio-communication domains in children with ASD. Thatsupports the findings of Baranek et al. (2006) proposing thatsensory hyporesponsiveness discriminated individuals withautism from those diagnosed with other developmental disor-ders or typically developing individuals. However, investigat-ing other sensory processing patterns in the light of the find-ings of this review seems as important. Not only are highfrequencies of hyperresponsiveness also present in individualswith ASD but also hypo- and hyperresponsiveness were re-ported to be present in the same individuals (Baranek et al.2006), and some associations between both hypo- andhyperresponsiveness and other ASD features remain unclear(e.g. repetitive behaviours). Hyperresponsiveness, neverthe-less, seems to be an under-researched sensory pattern. Forexample, in the studies investigating association between sen-sory processing patterns and anxiety, primarily the relation-ship between anxiety and overresponsivity was examined.While the link between children’s sensory overresponsivity,negative reactivity to complex sensory events and anxiety hasbeen made in the reviewed papers, other associations were notexplored. Only Lidstone et al. (2014) investigated other sen-sory processing patterns’ associations with more sensory atyp-icalities than hyperresponsivity and did find significant asso-ciations between anxiety and other sensory processing diffi-culties. Furthermore, because researchers widely use the ShortSensory Profile which includes an underresponsive/seeks sen-sation subscale only, finding and reporting associations withhyperresponsiveness is impossible.
It should also be noted that in some papers relatively smallsample sizes were used (Ashburner et al. 2008; Baker et al.
2008; Chen et al. 2009; Lane et al. 2012; Reynolds et al. 2012)and therefore type II error might have occurred and some ofthe associations might have not been detected although a re-lationship between sensory atypicalities and measured con-structs could exist in the population (Field 2009).
Study Limitations
The current review evidenced the sample selection process ishighly varied across studies. There was also a lack of consis-tency in the methods employed. First, in some reviewed areas,a small number of studies were included, which limits theconclusions that can be drawn. Secondly, studies with a wideage range of participants were often pooled together, ignoringpossible age-related differences in the presentation of bothsensory atypicalities and ASD-related difficulties. Thirdly,the wide variety of methods assessing sensory processing pat-terns and psychological constructs used in the reviewed stud-ies made the interpretation of the results very difficult.
Conclusions
In summary, the current research reports a number of associ-ations between sensory processing patterns and the clinicaland non-clinical features of ASD, highlighting that sensoryatypicalities play an important role in the disorder. However,there are several theoretical and measurement approaches tothe classification of the sensory processing patterns.Consensus on using a singular theoretical framework and setmeasures would help with clarifying results, but should bepreceded with more psychometric work. In the absence ofthe agreement on measurement tools, multiple informant mea-sures and sensory processing models based on informationobtained from a range of measures and informants might bea bridging alternative.
There are also several questions that require further investi-gation. Hyperresponsiveness remains an under-researched sen-sory processing pattern; hence, establishing its associationswith psychological constructs is an apparent research need.The current evidence provided for some constructs (e.g. repet-itive behaviours) has mixed findings. Further research examin-ing these correlations and establishing whether there are clearassociations with a particular processing pattern or whethersome psychological constructs correlate with a number of sen-sory atypicalities would benefit our understanding of the com-plexity of sensory processing difficulties in ASD.
Finally, at present, the research focuses on children andadolescents with ASD, without including adult participantsin the recruited samples. Investigating associations betweensensory processing patterns and psychological constructs inadults might shed some light into developmental changes ofASD characteristics.
Rev J Autism Dev Disord (2015) 2:199–221 219

Acknowledgments This research was supported by PhD funding fromthe Estate of DavidMurray Garside (awarded to authorMG). The authorswould like to thank Dr Sarah Wigham for her contribution in estimatinginter-rater reliability of the evaluation grid used in the study.
Conflict of Interest The authors declare that they have no conflict ofinterest.
References
*Study included in the review
American Psychiatric Association. (1994). Diagnostic and statisticalmanual of mental disorders (4th ed.). Washington DC: AmericanPsychiatric Association.
American Psychiatric Association. (2000). Diagnostic and statisticalmanual of mental disorders, fourth edition, text revision (DSM-IV-TR). Washington DC: American Psychiatric Association.
American Psychiatric Association. (2013). Diagnostic and statistical man-ual of mental disorders (5th ed.). Arlington: American PsychiatricPublishing.
Anello, A., Reichenberg, A., Luo, X., Schmeidler, J., Hollander, E.,Smith, C. J., et al. (2009). Brief report: parental age and the sex ratioin autism. Journal of Autism and Developmental Disorders, 39,1487–1492.
*Ashburner, J., Ziviani, J., & Rodger, S. (2008). Sensory processing andclassroom emotional, behavioral, and educational outcomes in chil-dren with autism spectrum disorder. American Journal ofOccupational Therapy, 62, 564–573.
*Baker, A. E., Lane, A., Angley, M. T., & Young, R. L. (2008). Therelationship between sensory processing patterns and behaviouralresponsiveness in autistic disorder: a pilot study. Journal of Autismand Developmental Disorders, 38(5), 867–875.
Baranek, G. T., David, F. J., Poe, M. D., Stone, W. L., & Watson, L. R.(2006). Sensory experience questionnaire: discriminating sensoryfeatures in young children with autism, developmental delays, andtypical development. Journal of Child Psychology and Psychiatry,47(6), 591–601.
*Baranek, G. T., Watson, L. R., Boyd, B. A., Poe, M. D., David, F. J., &McGuire, L. (2013). Hyporesponsiveness to social and nonsocialsensory stimuli in children with autism, childrenwith developmentaldelays, and typically developing children. Development andPsychopathology, 25(02), 307–320.
Baranek, G. T. (2002). Efficacy of sensory and motor interventions forchildren with autism. Journal of Autism and DevelopmentalDisorders, 5, 397–422.
Ben-Sasson, A., Hen, L., Fluss, R., Cermak, S., Engel-Yeger, B., & Gal,E. (2009). A meta-analysis of sensory modulation symptoms inindividuals with autism spectrum disorders. Journal of Autism andDevelopmental Disorders, 39, 1–11.
Bodfish, J. W., Symons, F. J., Parker, D. E., & Lewis, M. H. (2000).Varieties of repetitive behaviour in autism: comparisons to mentalretardation. Journal of Autism and Developmental Disorders, 30(3),237–243.
*Boyd, B. A., Baranek, G. T., Siders, J., Poe, M. D., Watson, L. R.,Patten, E., & Miller, H. (2010). Sensory features and repetitive be-haviors in children with autism and developmental delays. AutismResearch, 3, 78–87.
Boyd, B. A., McBee, M., Holtzclaw, T., Baranek, G. T., & Bodfish, J. W.(2009). Relationships among repetitive behaviors, sensory features,
and executive functions in high functioning autism. Research inAutism Spectrum Disorders, 3(4), 959–966.
*Brock,M., Freuler, A., Baranek, G.,Watson, L., Poe,M., & Sabatino, A.(2012). Temperament and sensory features of children with autism.Journal of Autism and Neurodevelopmental Disorders, 42, 2271–2284.
*Chen, Y. H., Rodgers, J., & McConachie, H. (2009). Restricted andrepetitive behaviors, sensory processing and cognitive style in chil-dren with autism spectrum disorders. Journal of Autism andDevelopmental Disorders, 39, 635–642.
Crane, L., Goddard, L., & Pring, L. (2009). Sensory processing in adultswith autism spectrum disorders. Autism: The International Journalof Research and Practice, 13(3), 215–228.
Deeks, J.J., Dinnes, J., D’Amico, R., Sowden, A. J., Sakarovitch, C.,Song, F. & Altman, D.G. (2003). Evaluating non-randomised inter-vention studies. Health Technology Assessment, 7(27).
Dunn, W. (1997). The impact of sensory processing abilities on the dailylives of young children and families: a conceptual model. Infantsand Young Children, 9(4), 23–25.
Field, A. (2009). Discovering statistics using SPSS: (and sex and drugsand rock’n’ roll) (3rd ed.). Los Angeles: Sage.
*Gal, E., Dyck, M. J., & Passmore, A. (2010). Relationships betweenstereotyped movements and sensory processing disorders in chil-dren with and without developmental or sensory disorders.American Journal of Occupational Therapy, 64, 453–461.
Gay, E., Watson, L. R., Baranek, G. T., Poe, M., & Boyd, B. (2008).Sensory processing patterns in relation to social communicative skillsin young children with autism. San Diego: Gatlinburg Conference onResearch and Theory in Intellectual and Developmental Disabilities.
*Green, S. A., Ben-Sasson, A., Soto, T. W., & Carter, A. S. (2012).Anxiety and sensory over-responsivity in toddlers with autism spec-trum disorders: bidirectional effects across time. Journal of Autismand Developmental Disorders, 42, 1112–1119.
*Hilton, C., Graver, K., & LaVesser, P. (2007). Relationship betweensocial competence and sensory processing in children with highfunctioning autism spectrum disorders. Research in AutismSpectrum Disorders, 1(2), 164–173.
Iarocci, G., & McDonald, J. (2006). Sensory integration and the percep-tual experience of persons with autism. Journal of Autism andDevelopmental Disorders, 36(1), 77–90.
Interdisciplinary Council on Developmental and Learning Disorders(ICDL-DMIC) Work Groups. (2005). Interdisciplinary Council onDevelopmental and Learning Disorders Diagnostic manual for in-fancy and early childhood mental health disorders, developmentaldisorders, regulatory-sensory processing disorders, language disor-ders, and learning challenges. Bethesda: Author.
*Jasmin, E., Couture,M.,McKinley, P., Reid, G., Fombonne, E., &Gisel,E. (2009). Sensori-motor and daily living skills of preschool chil-dren with autism spectrum disorders. Journal of Autism andDevelopmental Disorders, 39, 231–241.
John, A. E., & Mervis, C. B. (2010). Sensory modulation impairments inchildren with Williams syndrome. American Journal of MedicalGenetics. Part C, Seminars in Medical Genetics, 154, 229–248.
Kern, J. K., Garver, C. R., Carmody, T., Andrews, A. A., Trivedi, M. H.,& Mehta, J. A. (2007). Examining sensory quadrants in autism.Research in Autism Spectrum Disorders, 1(2), 185–193.
*Lane, A. E., Young, R. L., Baker, A. E. Z., & Angley, M. T. (2010).Sensory processing subtypes in autism: association with adaptive be-havior. Journal of Autism and Developmental Disorders, 40, 112–122.
*Lane, S. J., Reynolds, S., & Dumenci, L. (2012). Sensoryoverresponsivity and anxiety in typically developing children andchildrenwith autism and attention deficit hyperactivity disorder: causeor coexistence?American Journal of Occupational Therapy, 66, 595–603.
220 Rev J Autism Dev Disord (2015) 2:199–221

Leekam, S. R., Nieto, C., Libby, S. J., Wing, L., & Gould, J. (2007).Describing the sensory abnormalities of children and adults with au-tism. Journal of Autism and Developmental Disorders, 37, 894–910.
*Lidstone, L., Uljaveric, M., Sullivan, J., Rodgers, J., McConachie, H.,Freeston, M., et al. (2014). Relations among restricted and repetitivebehaviors, anxiety and sensory features in children with autism spec-trum disorders. Research in Autism Spectrum Disorders, 8, 82–92.
*Liss, M., Saulnier, C., Fein, D., & Kinsbourne, M. (2006). Sensory andattention abnormalities in autism spectrum disorders. Autism, 10,155–172.
Lydon, S., Healy, O., Reed, P., Mulhern, T., Hughes, B.M., & Goodwin,M.S. (2014). A systematic review of physiological reactivity tostimuli in autism. Developmental Neurorehabilitation, 1–21. doi:10.3109/17518423.2014.971975.
*Mazurek, M. O., Vasa, R. A., Kalb, L. G., et al. (2013). Anxiety, sensoryover-responsivity, and gastrointestinal problems in children with au-tism spectrum disorders. Journal of Abnormal Child Psychology, 41,165–176.
McConachie H., Parr, J. R. , Glod, M., Hanratty, J., Livingstone, N.,Oono, I. P. et al. (2015). Systematic review of tools to measureoutcomes for young children with autism spectrum disorder.Health Technology Assessment. In press.
Miller, L. J., Anzalone, M. E., Lane, S., Cemak, S., & Osten, E. (2007).Concept evolution in sensory integration: a proposed nosology fordiagnosis. American Journal of Occupational Therapy, 61, 135–140.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & The PRISMAGroup. (2009). Preferred reporting items for systematic reviewsand meta-analyses: the PRISMA statement. Open Medicine, 3(3),123–130.
Mokkink, L. B., Terwee, C. B., Patrick, D. L., Alonso, J., Stratford, P. W.,Knol, D. L., Bouter, L. M., & de Vet, H. C. W. (2010). TheCOSMIN checklist for assessing the methodological quality of stud-ies on measurement properties of health status measurement instru-ments: an international Delphi study. Quality of Life Research, 19,539–549.
*Nadon, G., Feldman, D. E., Dunn, W., & Gisel, E. (2011). Mealtimeproblems in children with autism spectrum disorder and their typicallydeveloping siblings: a comparison study. Autism, 15(1), 98–113.
O’Neill, M., & Jones, R. S. P. (1997). Sensory-perceptual abnormalitiesin autism: a case for more research. Journal of Autism andDevelopmental Disorders, 27(3), 283–293.
PDM Task Force. (2006). Psychodynamic diagnostic manual. SilverSpring: Alliance of Psychoanalytic Organizations.
*Pfeiffer, B., Kinnealey, M., Reed, C., & Herzberg, G. (2005). Sensorymodulation and affective disorders in children and adolescents withAsperger disorder. American Journal of Occupational Therapy, 59,335–345.
*Reynolds, S., Lane, S. J., & Thacker, L. (2012). Sensory processing,physiological stress, and sleep behaviors in children with and with-out autism spectrum disorders. Occupational Therapy Journal ofResearch, 32, 246–257.
Rogers, S. J., & Ozonoff, S. (2005). Annotation: what do we know aboutsensory dysfunction in autism? A critical review of the empiricalevidence. Journal of Child Psychology and Psychiatry, and AlliedDisciplines, 46(12), 1255–1268.
*Samson, A. C., Phillips, J. M., Parker, K. J., Shah, S., Gross, J. J., &Hardan, A. Y. (2013). Emotion dysregulation and the core featuresof autism spectrum disorder. Journal of Autism and DevelopmentalDisorders, 44, 1766–1772.
Scottish Intercollegiate Guidelines Network (SIGN) (2008). SIGN 50—aguideline developer’s handbook. Retrieved from www.sign.ac.uk(28th July 2014).
Sollaci, L. B., & Pereira, M. G. (2004). The introduction, methods, re-sults, and discussion (IMRAD) structure: a fifty-year survey.Journal of the Medical Library Association, 92, 364–367.
*Tseng, M. H., Fu, C. P., Cermak, S. A., Lu, L., & Shieh, J. Y. (2011).Emotional and behavioral problems in preschool children with au-tism: relationship with sensory processing dysfunction. Research inAutism Spectrum Disorders, 5, 1441–1450.
Turner, M. (1999). Annotation: Repetitive behaviour in autism: a reviewof psychological research. Journal of Child Psychology andPsychiatry, 40(6), 839–849.
*Watson, L. R., Patten, E., Baranek, G. T., Poe, M., Boyd, B. A., Freuler,A., et al. (2011). Differential associations between sensory responsepatterns and social-communicationmeasures in children with autismand developmental disorders. Journal of Speech, Language, andHearing Research, 54, 1562–1576.
Whiting, P., Rutjes, A., Reitsma, J., Bossuyt, P., & Kleijnen, J. (2003).The development of QUADAS: a tool for the quality assessment ofstudies of diagnostic accuracy included in systematic reviews. BMCMedical Research Methodology, 3(25).
Zero to Three. (2005). Diagnostic classification of mental health anddevelopmental disorders of infancy and early childhood, revised(DC:0–3R). Arlington: National Center for Clinical Infant Programs.
Rev J Autism Dev Disord (2015) 2:199–221 221