psychosocial support for maternal stress during pregnancy: effect on birth weight
TRANSCRIPT

Psychosocial support for maternal stress during pregnancy: Effect on birth weight
Alan D. Rothberg, MB, BCh, and Bernice Lits, MA
Johannesburg, South Africa
In a previous study we showed that moderate to severe stress during pregnancy was inversely related to infant birth weight. Using the same criteria for stress (according to the Social Readjustment Rating Scale of Holmes and Rahe), we studied 86 white mothers with singleton pregnancies and with no known medical or obstetric risk factors for reduced birth weight. After strict randomization, data were analyzed for 43 mothers who received psychosocial support between enrollment at ± 20 weeks and delivery at ± 38 weeks and for 43 control mothers who received standard care at the antenatal clinic. In the supported group seven infants weighed <3000 gm at birth versus 18 control infants (p = 0.008), and analysis revealed that this effect was more the result of improved intrauterine growth than of prolongation of pregnancy. These findings are of little clinical relevance as far as the neonate is concerned, but they do indicate that psychosocial support has a Significant effect on birth weight. It is possible that previous studies that have looked only for an effect on low- or very-Iow-birth-weight rates might have missed this clinically measurable benefit of counseling. (AM J OSSTET GVNECOL 1991 ;165:403-7.)
Key words: Psychosocial support, pregnancy, birth weight
A relationship between major life events and low birth weight «2500 gm) has been described by several authors.'·s This led us to a preliminary study in 1985,< in which a group of 118 mothers who were delivered prematurely at the Johannesburg Hospital were shown to have an excess of moderate to severe stressors as identified by the Social Readjustment Rating Scale of Holmes and Rahe.5 Our initial study was followed by a larger retrospective study of 535 mothers delivered at the same hospitals; moderate to severe stress factors were identified in 48% of the mothers, and a significant, inverse relationship was observed between cumulative stress score and birth weight. 6 Having thus confirmed an interaction between stress and birth weight in our local population, we faced the question whether stressed mothers attending the antenatal clinic would benefit from psychosocial support and whether such support would influence birth weight or gestational age. While descriptive studies have demonstrated the interaction between psychosocial stress and birth weight, '·3.7 as indicated in a recent overview,S no prospective, controlled trial has specifically evaluated the effects of intervention in mothers enrolled on the basis of psychosocial stress.
From the Department of Paediatrics and Child Health, University of the Witwatersrand, Johannesburg Hospital. Supported by grants from the Medical Faculty Research Fund, the Anglo American Chairman's Fund, and the Iris Ellen Hodges Trust. Received for publication October 29, 1990; revised January 16, 1991; accepted January 28, 1991. Reprint requests: Prof Alan D. Rothberg, Dept. of Paediatrics, Johannesburg Hospital, Private Bag X39, Johannesburg 2000, South Africa. 611128264
Subjects and methods
Data from the previous studt were used to determine sample size for this randomized, controlled study of support for mothers suffering from moderate to severe stress during pregnancy. Analysis of data from the previous studt indicated that a stress effect approached significance when a weight cutoff of 3000 gm was used; 25% of the 280 babies born to nonstressed mothers weighed <3000 gm versus 35% of the 255 babies born to those with stress. On the basis of these figures, the prospective study was designed with a minimum sample of 86 subjects required to determine whether intervention could achieve a 50% reduction in the number of babies weighing <3000 gm.
Mothers of singleton pregnancies were eligible for enrollment between the eighteenth and twenty-fifth weeks of pregnancy if they were free of medical or obstetric problems known to be associated with prematurity or low birth weight (LBW). In keeping with the objective of eliminating as many known causes of LBW «2500 gm) as possible, the study was confined to white mothers; this was because of the known association between lower birth weight and black race.9
As in the preliminary study,6 stress was defined as any factor scoring 239 on the Social Readjustment Rating Scale5 (Table I) and occurring within the 6 to 12 months before enrollment. Individual scores were added together, and analysis was therefore in terms of the cumulative stress score.
Mothers were interviewed at the antenatal clinic by one of the authors (B.L.). Those eligible for entry on the basis of a history of stress, and willing to participate in the study, were randomized into support or control
403

404 Rothberg and Lits
Table I. Criteria for entrt
Description of stress
Major marital problems Severe illness in a family member Dismissal from work (subject or baby's father) Marriage during pregnancy Significant personal injury Death of a close family member (including
abortion or stillbirth) Imprisonment (subject or baby's father) Separation from baby's father Divorce Death of baby's father
Score'
39 44 47 53 50 63
63 65 73
100
groups. Before randomization all mothers signed an informed consent form that indicated that they might or might not be selected for additional interviews or counseling sessions with a social worker involved in the study. Randomization was simple (unstratified), by means of sealed envelopes containing a green or pink slip of paper, indicating assignment to support or control groups, respectively. Mothers in the support group entered into a regular, individualized, client-centered relationship with one of two social workers contracted to the study. Both social workers were skilled counselors with experience in gestational support and crisis intervention. Support consisted of at least 20 minutes with the social worker at the time of each antenatal clinic visit. When mothers felt unable to wait for the social worker on a clinic day, arrangements were made to make up the missed visit, or for the social worker to have a 10- to 20-minute telephone counseling session with the subject. The psychosocial support was directed toward dealing with the stress factor(s) that had warranted enrollment in the study, assisting with problems in the home or work situation, and encouraging mothers to comply with instructions and advice of the antenatal clinic staff. Control motheJ's were treated according to the usual protocols of the antenatal clinic; those personnel, while obviously aware of the existence of our study, were largely unaware of the personal problems of the mothers.
Additional data collected in every case included maternal age, obstetric history, marital status, and number of clinic visits after enrollment. Smoking history was recorded and, while we did not include a specific antismoking program in the study design, mothers were exposed to the standard information in the form of educational posters and pamphlets at the clinic. At the time of delivery, birth weight and length were recorded for every baby by a labor ward staff member who was unaware of the subject's group assignment, and gestational age was assessed by one of the authors (A.D.R.) according to the Ballard score. 'O Mothers completing the study were interviewed within 2 weeks of delivery to assess the value of support for the study mothers
August 1991 Am J Obstel Gynecol
and perceptions regarding need for support on the part of controls.
Statistical analysis was by means of t tests for normally distributed data or otherwise by the Mann-Whitney test; Fisher's exact or X' tests were used to compare differences in proportions between groups. Interactive multiple linear regression analysis was used to explore the relationship between variables.
The study was approved by the University Committee for Research on Human Subjects.
Results
To be assured of the minimum sample size required (86 subjects, 43 per group), i.e., allowing for dropouts, abortions, and transfer of mothers to other hospitals, 104 subjects were enrolled between May 1989 and August 1990. Eight subjects were excluded (two aborted shortly after enrollment, two developed medical problems, twins were diagnosed in one, three transferred to other medical centers). Excluded subjects within each of these categories were equally distributed between support and control groups. Data collection was stopped when 43 subjects in each group had completed the study; however, the four remaining mothers in the support group continued to receive counseling until delivery, and the six remaining in the control group continued with routine care.
Table II shows the characteristics of the study population and also demonstrates how closely the present group of 86 resembles the 255 stressed mothers studied in 19856 in terms of maternal age, cumulative stress score, birth weight, and LBW rate. Mothers were entered into the present study at 20.7 ::t: 2.6 weeks of pregnancy (mean ::t: SD).
Interactive regression analysis of data for the total group showed that psychosocial support, gravidity, and smoking were significant determinants of birth weight, together accounting for 14.8% of the variance. Infant sex, maternal age, marital status, and previous stillbirth or abortion were not important in this model.
When the data were analyzed according to support and control groups, there was a significant reduction in the number of infants weighing <3000 gm in the supported group (7 of 43 vs 18 of 43; p = 0.008; odds ratio, 0.29; 95% confidence interval, 0.12 to 0.74); however, the number of LBW babies was similar in both groups (six of 43 in the supported group vs five of 43 in controls). While there was a trend toward a higher prematurity rate in the control mothers, the difference was not significant (20.5% of control mothers delivered before 37 completed weeks vs 10.8% of those who received support, p = 0.2). The above-mentioned weight and gestational age data suggest that psychosocial support had a greater effect on fetal weight than on du-

Volume 165 Number 2
Support for stress in pregnancy 405
Table II. Major similarities between study population and 1985 group of stressed mothers6
Maternal age (yr, mean ± SD) Cumulative stress score (mean ± SD) Birth weight (gm, mean ± SD) LBW rate (%)
ration of pregnancy, and neonatal length and weightto-length ratios appear to confirm this postulate. Mean neonatal length (± SD) was similar for both groups (49.3 ± 2.1 cm for control infants vs 50.0 ± 2.8 cm for those of supported mothers), while weight-to-Iength ratios were significantly different in the two groups (30% of controls weighed <55 gm/ cm length vs 11.4% born to supported mothers; p = 0.045). The change in the distribution of birth weight between the groups of infants is shown in Table III.
Two neonates from the supported group required admission to the neonatal intensive care area for ventilatory support. Both were of very low birth weight and one died (875 gm). One very-Iow-birth-weight neonate from the control group required admission to the intensive care area for management of hypoglycemia. No neonatal problems of note were encountered in the remaining 83 infants.
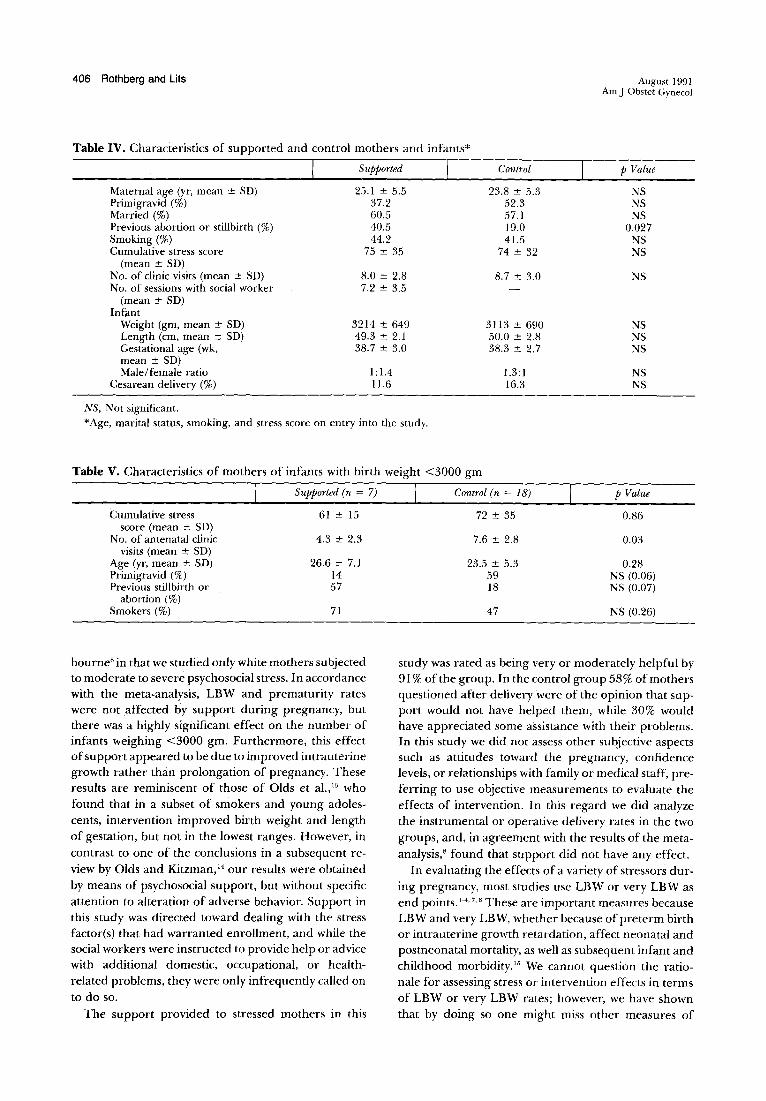
Characteristics of the two groups of mothers and infants are shown in Table IV. Of particular note are the following: relatively high percentage of smokers in both groups; mean birth weight difference of 101 gm between control and supported groups; and eight or more visits to the antenatal clinic for all mothers, with supported mothers receiving seven or more sessions with the social worker in the ± 18 weeks between enrollment and delivery. The significantly greater number of women with previous abortions or stillbirths in the supported group is a chance finding but even if significant would probably have acted to increase and not diminish the risk of lower birth weight in this group.!! The effect of counseling appeared to be independent of any effect on maternal smoking; similar numbers of supported and control mothers modified their smoking habits during the study.
In Table V, mothers of infants weighing <3000 gm are compared according to support or control status. Because of the small number of infants in the support group, most of the differences are not significant; however, it would appear that the seven mothers who were "unresponsive" to support were more likely to be older, multiparous smokers who, despite a poor obstetric history, were infrequent attenders of the antenatal clinic.
Fifty-one percent of supported mothers rated the sessions with the social worker as being very helpful,
Present study (n = 86)
24.5 ± 5.4 74 ± 33
3164 ± 668 12.8
Retrospective study (1985)"
(n = 255)
24.5 ± 5.2 72 ± 35
3147 ± 580 12.9
Table III. Birth weight distribution of infant groups
Supported Control Birth weight (gm) (n = 43) (n = 43)
<2000 2 2 2000-2499 4 3 2500-2999 1 13 3000-3499 22 II 3500-3999 11 11 2:4000 3 3
40% found the support to be of some help, 5% did not benefit at all, and 4% did not complete the questionnaire. In the control group, 58% felt that support was not needed, 30% would have appreciated some help, and 12% did not return the questionnaire. No mothers in the control group were referred for counseling by antenatal clinic staff.
Comment
Interactions between maternal behavior, inadequate social support systems, and personal maternal characteristics have been described which might lead to uteroplacental problems and premature labor.12 In the proposed model stress leads to catecholamine release, decreased placental function, and uterine irritability. While premature labor may be the end product of stress, it is clear that utero placental problems might also interfere with fetal nutrition and growth. Several authors have confirmed these effects of stress in retrospective·4
,6 and prospective7 studies, with most implying or concluding that randomized, controlled trials are required to establish whether the deleterious effects can be reversed by psychosocial support during pregnancy.
ElbourneB has commented on the data from 12 relevant controlled trials, which have been included in the Oxford Database of Perinatal Trials. In terms of the outcome measures applicable to the present study, the meta-analysis reveals that social support during pregnancy influences neither the LBW rate nor the preterm delivery rate (typical overall odds ratios, 0.89 and 0.99; 95% confidence intervals, 0.76 to 1.05 and 0.84 to 1.17, respectively).
This study differed from those reviewed by EI-
406 Rothberg and Lits August 199 1 Am J Obstet Gynecol
Table IV. Characteristics of supported and control mothers and infants*
Supported Control p Value
Maternal age (yr, mean :t SO) 25.1 :t 5.5 23.8 :t 5.3 NS Primigravid (%) 37.2 52.3 NS Married (%) 60.5 57 .1 NS Previous abortion or stillbirth (%) 40.5 19.0 0.027 Smoking (%) 44.2 41.5 NS Cumulative stress score 75 :t 35 74 ± 32 NS
(mean ± SO) No. of clinic visits (mean ± SO) 8.0 ± 2.8 8.7 ± 3.0 NS No. of sessions with social worker 7.2 ± 3.5
(mean ± SO) Infant
Weight (gm, mean ± SO) 3214 ± 649 3113 ± 690 NS Length (em, mean ± SO) 49.3 ± 2.1 50.0 ± 2.8 NS Gestational age (wk, 38.7 ± 3.0 38.3 ± 2.7 NS mean ± SD) Male/female ratio 1: 1.4 1.3: 1 NS
Cesarean delivery (%) 11.6 16.3 NS
NS, Not significant. *Age, marital status, smoking, and stress score on eml-Y into the study.
Table V. Characteristics of mothers of infants with birth weight <3000 gm
I Supported (n = 7) I Control (n = 18) p Value
Cumulative stress 61 ± 15 score (mean ± SO)
No. of antenatal clinic 4.3 ± 2.3 visits (mean± SO)
Age (yr, mean ± SD) 26.6 ± 7.1 Primigravid (%) 14 Previous stillbirth or 57
abortion (%) Smokers (%) 71
bourneS in that we studied only white rnothers subjected to moderate to severe psychosocial stress. In accordance with the meta-analysis, LBW and prematurity rates were not affected by support during pregnancy, but there was a highly significant effect on the number of infants weighing <3000 gm. Furthermore, this effect of support appeared to be due to improved intrauterine growth rather than prolongation of pregnancy. These results are reminiscent of those of Olds et al.,13 who found that in a subset of smokers and young adolescents, intervention improved birth weight and length of gestation, but not in the lowest ranges. However, in contrast to one of the conclusions in a subsequent review by Olds and Kitzman, 14 our results were obtained by means of psychosocial support, but without specific attention to alteration of adverse behavior. Support in this study was directed toward dealing with the stress factor(s) that had warranted enrollment, and while the social workers were instructed to provide help or advice with additional domestic, occupational, or healthrelated problems, they were only infrequently called on to do so.
The support provided to stressed mothers in this
72 ± 35
7.6 ± 2.8
23 .5 ± 5.3 59 18
47
0.86
0.03
0.28 NS (0.06) NS (0.07)
NS (0.26)
study was rated as being very or moderately helpful by 91 % of the group. In the control group 58% of mothers questioned after delivery were of the opinion that support would not have helped them, while 30% would have appreciated some assistance with their problems. In this study we did not assess other subjective aspects such as attitudes toward the pregnancy, confidence levels, or relationships with family or medical staff, preferring to use objective measurements to evaluate the effects of intervention. In this regard we did analyze the instrumental or operative delivery rates in the two groups, and, in agreement with the results of the metaanalysis,· found that support did not have any effect.
In evaluating the effects of a variety of stressors during pregnancy, most studies use LBW or very LBW as end points. 1-4. 7.8 These are important measures because LBW and very LBW, whether because of preterm birth or intrauterine growth retardation, affect neonatal and postneonatal mortality, as well as subsequent infant and childhood morbidity.15 We cannot question the rationale for assessing stress or intervention effects in terms of LBW or very LBW rates; however, we have shown that by doing so one might miss other measures of

Volume 165 Number 2
outcome, in this case the number of births between 2500 gm and 3500 gm. The significant effect of psychosocial counseling in increasing birth weight to above 3000 gm is of little consequence in terms of neonatal outcome but shows far more conclusively than before8
that support during pregnancy has a clinically measurable effect.
REFERENCES
1. Newton RW, Hunt LP. Psychosocial stress in pregnancy and its relation to low birth weight. BM] 1984;288: 1191-4.
2. Stein A, Campbell EA, Day A, et aJ. Social adversity, low birth weight and preterm delivery. BM] 1978;295:291-3.
3. Istvan ]. Stress, anxiety and birth outcomes: a critical review of the evidence. Psychol Bull 1986; 100:331-48.
4. Schreier RA, Rothberg AD. Stress factors in premature births. ] Perinatol 1985;5:28-3 1.
5. Holmes TH, Rahe RH . The social readjustment rating scale. ] Psychosom Res 1967; 11 :2 13-8.
6. Rothberg AD, Shuenyane E, Lits B, Strebel PM. Effect of stress on birth weight in two Johannesburg populations. S Afr MedJ 1991;79:35-8.
7. Pagel MD, Smilkstein G, Regen H, Montano D. Psychosocial influences on newborn outcomes; a controlled, prospective study. Soc Sci Med 1990;30:597-604.
Support for stress in pregnancy
8. Elbourne DR. General social support from caregivers during pregnancy. In: Chalmers 1, ed. Oxford database of perinatal trials. Oxford: Oxford University Press, Version 1.2, disk issue 4. August 1990.
9. Kramer MS. Intrauterine growth and gestational duration determinants. Pediatrics 1987;80:502-11.
10. Ballard JL, Novak KK, Driver M. A simplified score for assessment of fetal maturation of newly born infants. ] Pediatr 1979;95:769-74.
11 . Stubblefield PG. Causes and prevention of preterm birth: an overview. In : Fuchs F, Stubblefield PG, eds. Preterm birth: causes, prevention and management. New York: Macmillan, 1984:3-20.
12. Bragonier JR, Cushner PM, Hobel C]. Social and personal factors in the etiology of pre term birth. In: Fuchs F, Stubblefield PG, eds. Preterm birth: causes, prevention and management. New York: Macmillan, 1984:64-85.
13. Olds DL, Henderson CR, Tatelbaum R, Chamberlin R. Improving the delivery of prenatal care and outcomes of pregnancy: a randomised trial of nurse home visitation. Pediatrics 1986;77:16-28.
14. Olds DL, Kitzman H . Can home visitation improve the health of women and children at environmental risk? Pediatrics 1990;86: 108-16.
15. McCormick MC. The contribution oflow birth weight to infant mortality and childhood morbidity. N Engl] Med 1985;3 12:82-90.
Transvaginal removal of ovaries with endoloop sutures at the time of transvaginal hysterectomy
Mitchel S. Hoffman, MD
Tampa, Florida
Twenty patients were evaluated for possible oophorectomy during transvaginal hysterectomy. Of 40 ovaries, nine were removed with a standard clamp technique. Twenty-two ovaries could not be removed by the clamp technique but were successfully removed with endoloop sutures. Safe transvaginal removal was not thought to be possible for the remaining nine ovaries. (AM J OBSTET GVNECOL 1991 ;165:407-8.)
Key words: Oophorectomy, transvaginal; suture, endoloop
The purpose of this study was to evaluate the feasibility and safety of transvaginal oophorectomy by the endoloop suture at the time of transvaginal hysterectomy.
From the Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, H. Lee M of Jilt Cancer Center and Research Institute, University of South Florida College of M edicine. Received for publication February 6, 1991; revifed March 7, 1991 ; accepted March 15,1991. Reprint requests: Mitchel S. Hoffman, MD. H. Lee Moffitt Cancer Center and Research Institute, 12902 Magnolia Dr., Tampa, FL 33612-9497. 611 129568
Material and methods
This was a prospective observational study. Ovarian removal by the standard clamp technique was performed when possible. If the standard technique was not feasible but the ovaries appeared to be reasonably accessible, then removal with the endoloop suture (size o plain gut ligature; Ethicon Inc., West Germany) was attempted. When the uterus had been removed. each ovary was grasped with a long Babcock clamp and was pulled with moderate traction into the vagina. An endo loop suture was then brought around the Babcock and was secured above the ovary at the origin of the
407