ptcog 49 educational workshop of head & neck cancer
TRANSCRIPT

PTCOG 49 Educational Workshop
Proton Therapy of Head & Neck Cancer
Robert S Malyapa, MD, PhD

Malyapa – PTCOG 49 Educational Workshop
Clinical experiences of H&N proton therapy
Loma Linda oropharynx study using the concomitant boost technique (IJROBP, 2005)
MGH study for skull base adenoid cystic carcinoma (Arch Otolaryngol Head Neck Surg, 2006)
UFPTI study on maxillary sinus cancer (AJCO, 2008)

Malyapa – PTCOG 49 Educational Workshop
Why protons for H&N cancer?
Protons are attractive to radiotherapy because of their physical dose distributionThe RBE of protons are indistinguishable from 250 kV X-rays, which means that they are 10-15% more effective than 60Co (RBE=1.1)The OER of proton beams is not distinguishable from X-rays (2.5 – 3)Protons are sparsely ionizing, except for a region at the end of particles’ rangeThis high LET component is restricted to a tiny portion of the terminal track, it does not have any significant effect (this should be kept in mind when planning treatment close to critical structures)
Malyapa – PTCOG 49 Educational Workshop
Why protons for H&N cancer?
Preservation of visual function by reduction in dose to optic appartusPotential to further improve quality of life
Improved salivary gland function by sparing of parotid and submandibular glandsImproved swallowing function
Potential to escalate dose for hypoxic tumors while maintaining improvement in quality of life
Malyapa – PTCOG 49 Educational Workshop
UFPTI approach to H&N proton therapy
Large amount of H&N conventional and IMRT radiotherapy experience at UFEstablished H&N outcome database for comparisonEstablished IMRT H&N protocolsProton therapy H&N protocols designed to maximize utilization of these experiences
Malyapa – PTCOG 49 Educational Workshop
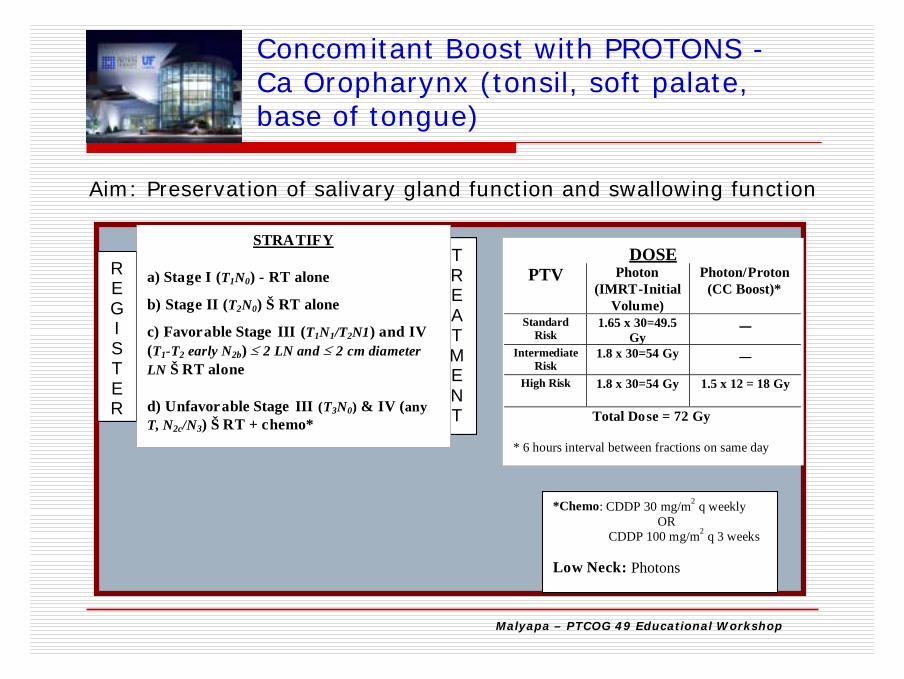
Concomitant Boost with PROTONS -Ca Oropharynx (tonsil, soft palate, base of tongue)
Aim: Preservation of salivary gland function and swallowing function
TREATMENT
REGISTER
STRATIFY
a) Stage I (T1N0) - RT alone
b) Stage II (T2N0) Š RT alone
c) Favorable Stage III (T1N1/T2N1) and IV (T1-T2 early N2b) ≤ 2 LN and ≤ 2 cm diameter LN Š RT alone
d) Unfavorable Stage III (T3N0) & IV (any T, N2c/N3) Š RT + chemo*
DOSEPTV Photon
(IMRT-Initial Volume)
Photon/Proton(CC Boost)*
Standard Risk
1.65 x 30=49.5Gy
__
IntermediateRisk
1.8 x 30=54 Gy __
High Risk 1.8 x 30=54 Gy 1.5 x 12 = 18 Gy
Total Dose = 72 Gy
* 6 hours interval between fractions on same day
*Chemo: CDDP 30 mg/m2 q weeklyOR
CDDP 100 mg/m2 q 3 weeks
Low Neck: Photons

Malyapa – PTCOG 49 Educational Workshop
Hyperfractionation with PROTONS –Carcinoma Nasal Cavity & Paranasal Sinuses
Aim: Preservation of visual functions (optic nerves, chiasm) andreduction of radiation dose to brain
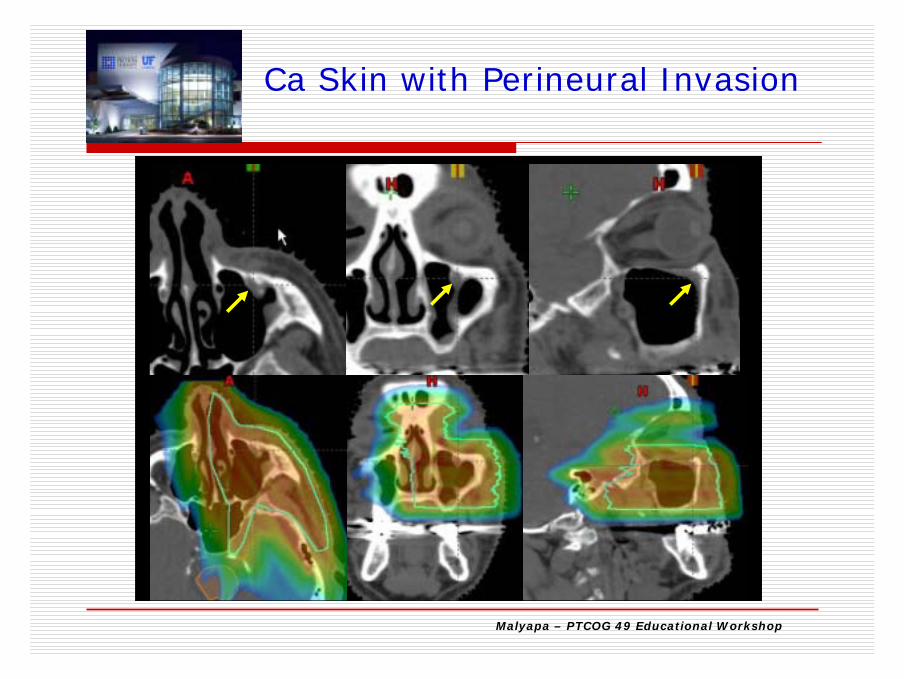
•Hyperfractionation @ 1.2 CGE BID•68.4 -69.6 CGE: post-op negative margins•74.4 CGE: post-op positive margins
close marginperineural invasion
•Low neck: photons•CHEMO: 30 mg/m2 weekly CDDP

Malyapa – PTCOG 49 Educational Workshop
TREATMENT
REGI STER
STRATIFY a) T1, T2, N0 → RT alone
b) T3 and any N+ →RT+Chemo
DOSE
Photon (IMRT-Initial Volume)
BID Tx
Photon/Proton (Boost) BID Tx
50.4 Gy (1.2 Gy BID)*
24.0 Gy (1.2 Gy BID)*
TOTAL DOSE = 74.4 Gy
* 6 hours interval between fractions on same day
*Chemo: CDDP 30 mg/m2 q weekly OR CDDP 100 mg/m2 q 3 weeks Neck Nodes: Photons
Aim: Preservation of visual functions (optic nerves, chiasm) andreduction of radiation dose to brain
Hyperfractionation with PROTONS- Ca Nasopharynx
Malyapa – PTCOG 49 Educational Workshop
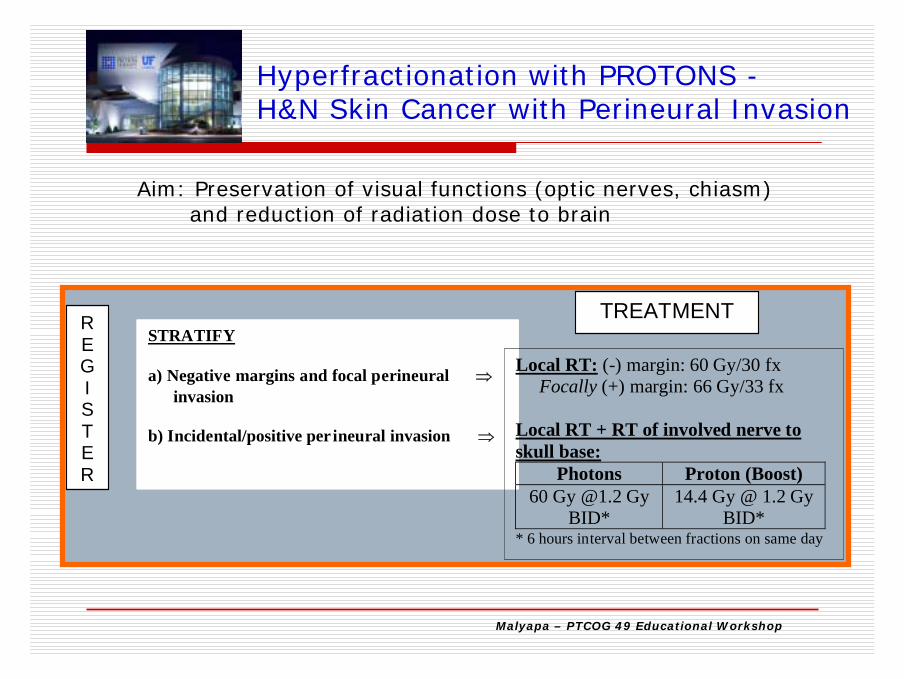
Hyperfractionation with PROTONS -H&N Skin Cancer with Perineural Invasion
REGI STER
STRATIFY a) Negative margins and focal perineural ⇒
invasion b) Incidental/positive per ineural invasion ⇒
TREATMENT
Local RT: (-) margin: 60 Gy/30 fx Focally (+) margin: 66 Gy/33 fx Local RT + RT of involved nerve to skull base:
Photons Proton (Boost) 60 Gy @1.2 Gy
BID* 14.4 Gy @ 1.2 Gy
BID* * 6 hours interval between fractions on same day
Aim: Preservation of visual functions (optic nerves, chiasm) and reduction of radiation dose to brain

Malyapa – PTCOG 49 Educational Workshop
Patient selection criteria for H&N proton therapy
Oropharynx:Must have only ipsilateral lymph nodes involved
Tumor extent that may require overly complex beam arrangements
Tumors extending from oropharynx to anterior cranial fossaTumors extending into low neck
Tumor location relative to high-Z dental implants

Malyapa – PTCOG 49 Educational Workshop
Patient immobilization and simulation
Patient immobilization devices must be proton-friendlyHomogeneous radiological lengths through potential beam pathsAll patient immobilization devices must be carefully evaluated for their physical properties
Malyapa – PTCOG 49 Educational Workshop
Evaluation of Immobilization Devices for Proton Therapy
Dosimetric Tests:CT scan of device to evaluate WET uniformityCompared TPS-calculated range pullback vs. measured range pullback at multiple locations on deviceThese tests must be performed with consideration of TPS dose calculation grid sizes, compensator smearing used, and proton scattering at depths of target after passing through device
Mechanical TestsDevice sagging as a function of time and weight on device
Malyapa – PTCOG 49 Educational Workshop
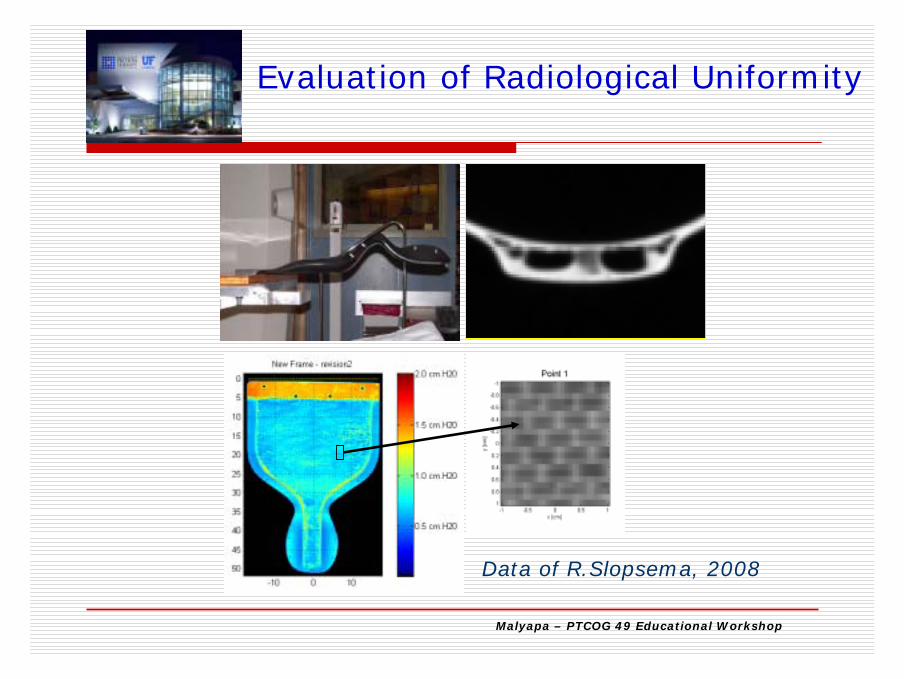
Data of R.Slopsema, 2008
Evaluation of Radiological Uniformity
Malyapa – PTCOG 49 Educational Workshop
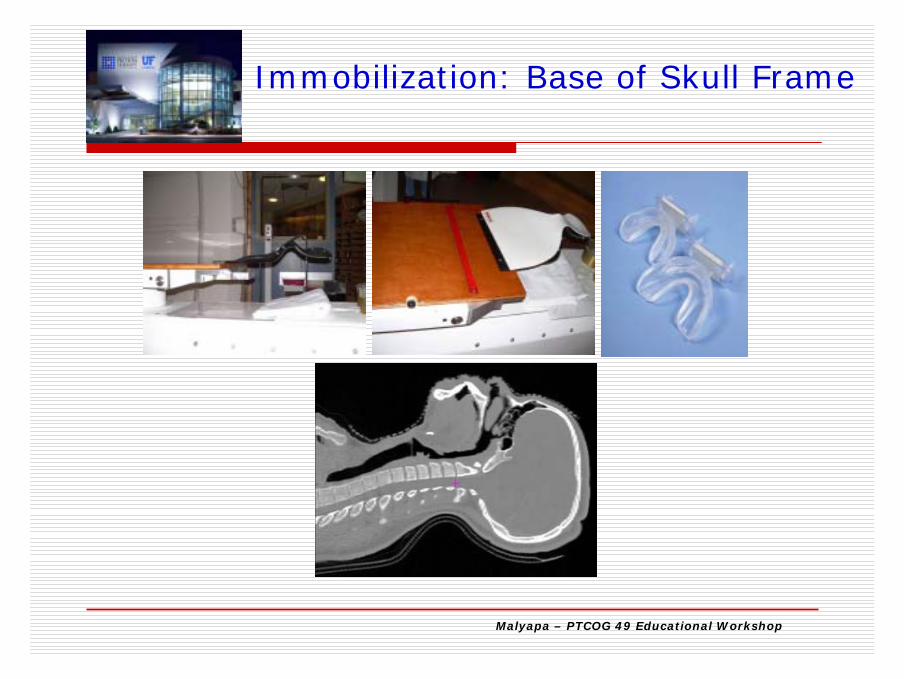
Immobilization: Base of Skull Frame

Malyapa – PTCOG 49 Educational Workshop
CT simulation for H&N proton therapy
CT scanning technique optimized for appropriate patient size and siteCT-HU to proton stopping power conversion curves are optimized for FOV because HU is dependent on FOV
large FOV on large-bore CT scannersmall FOV e.g. H&N/CNS on small-bore
Approx 1.5% difference in HU was observed between small and large FOVCT with contrast injection used for segmentation but not for dose calculation

Malyapa – PTCOG 49 Educational Workshop
Aperture Margin Selection
Aperture margins account for beam penumbra at target depthOverly tight aperture margins increase dose distribution inhomogeneity and reduce dose distribution calculation accuracyBeam penumbra is a function of beam option used for treatment, as well as target depth

Malyapa – PTCOG 49 Educational Workshop
R.Slopsema, 2007
Beam Penumbra in Air andin Water

Malyapa – PTCOG 49 Educational WorkshopR. Slopsema, 2008
Double-Scattering Uniform Scanning
Uniform scanning for H&N

Malyapa – PTCOG 49 Educational Workshop
DVH for four-field nasopharynx plan, comparing US ( ) and DS ( )delivery. Pink shows target coverage; the inset (blue) the dose to the brain stem.
Slopsema, 2008
DSUS
DS
US
Uniform scanning for H&N
Malyapa – PTCOG 49 Educational Workshop
Proton-Specific Treatment Planning Concepts
Distal MarginRelative Biological Effect (RBE): accounting for higher RBE near distal rangeAccounting for range uncertainties
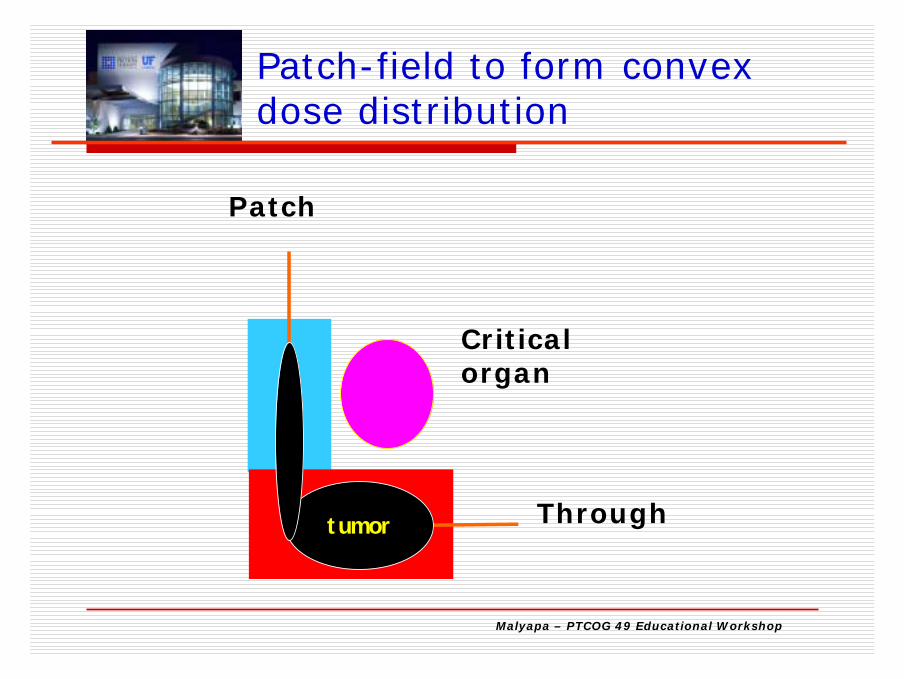
Proximal MarginCompensator smearing: 5 mm for H&NCompensator border smoothing: 10 mm for H&NThrough-patch fields (match fields preferred)
Malyapa – PTCOG 49 Educational Workshop
Patch
Through
Patch-field to form convex dose distribution
Criticalorgan
tumor
Malyapa – PTCOG 49 Educational Workshop
Metal Artifacts
Metal artifacts are often present within or near target region on CT images of H&N tumors
These need to be manually contoured and assigned appropriate HU for correct proton range calculations
Malyapa – PTCOG 49 Educational Workshop
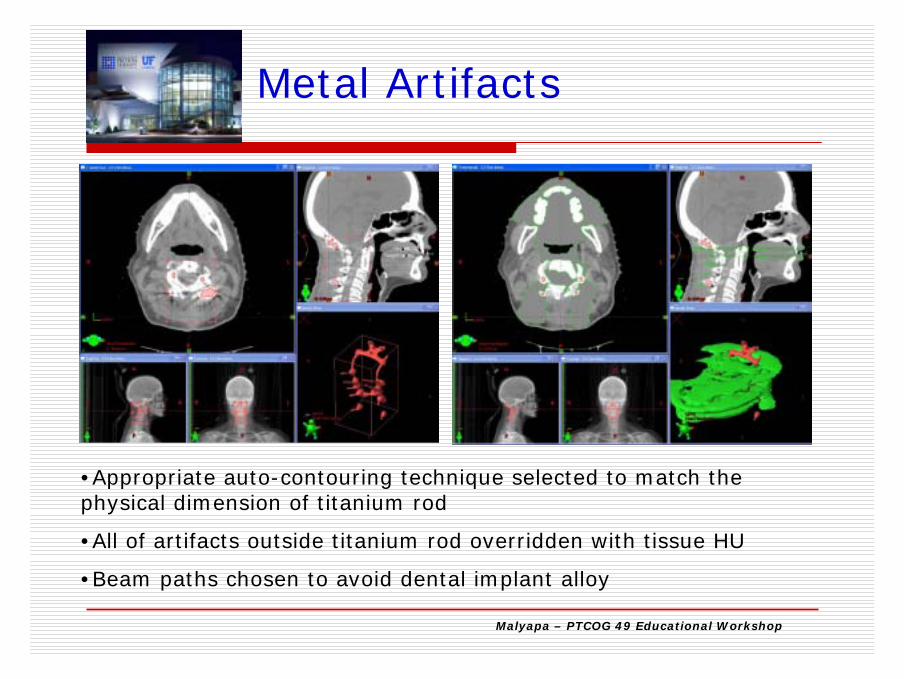
•Appropriate auto-contouring technique selected to match the physical dimension of titanium rod
•All of artifacts outside titanium rod overridden with tissue HU
•Beam paths chosen to avoid dental implant alloy
Metal Artifacts

Malyapa – PTCOG 49 Educational Workshop
Other considerations of treatment planning for H&N proton therapy
High skin dose: Selection of beam angles to minimize field overlap on skinHigher dose inhomogeneity at air-bone or tissue/implanted metal interfaces: Selection of beam angles to minimize beam parallel to such interfacesRange and penumbra uncertainties due to presence of metal objects: avoid beams passing through and stopping on cordIncreased RBE at the end of range:
Allow additional distal margin when beam exits on critical organsMinimize number of beams exiting on critical organs

Malyapa – PTCOG 49 Educational Workshop
Treatment

Malyapa – PTCOG 49 Educational Workshop
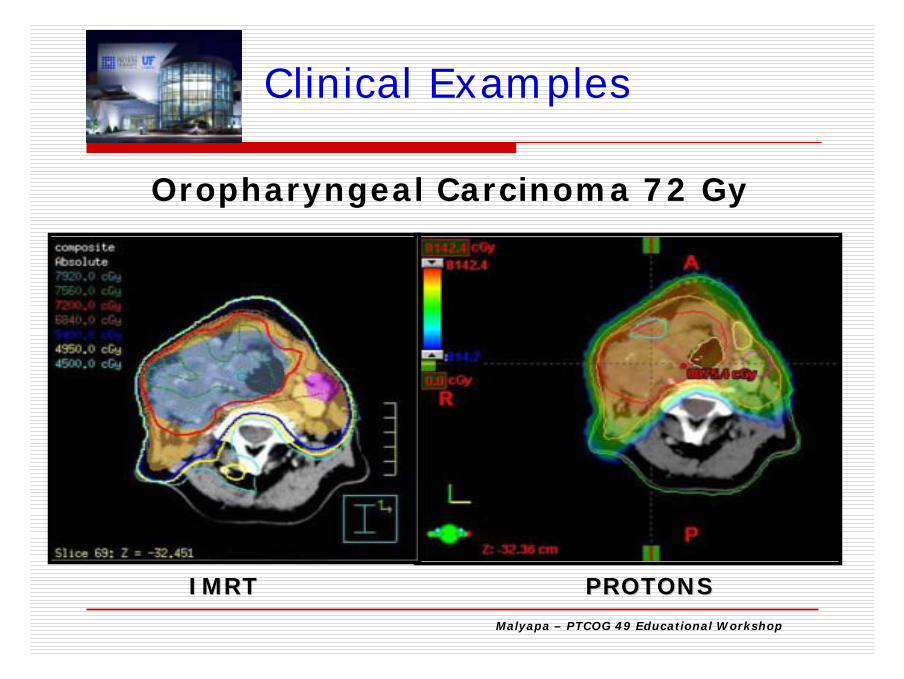
Clinical Examples
OropharynxNasal cavity and Paranasal sinus NasopharynxSkin with perineural invasionLacrimal glandRE-IRRADIATION
Malyapa – PTCOG 49 Educational Workshop
IMRTIMRT PROTONSPROTONS
Oropharyngeal Carcinoma 72 Gy
Clinical Examples

Malyapa – PTCOG 49 Educational Workshop
IMRT ProtonTherapy
% PRV Dose ↓
PTV coverage: ≥95% of PTV receives Rx dose
101.6% 99.7%
PTV coverage: 99% of PTV receives ≥ 93% of Rx dose
100.3% 96.7%
Hot spot in PTV72 (≤20% of PTV 72 receives 110% of prescribed dose )
107.3% 106%
Contralateral Parotid (mean dose <2600 cGy
2529 1482 43%
Brainstem (5500 cGy to 0.1 c.c.)
5020 2685 46%
Spinal cord (5000 cGy to 0.1 c.c.)
4400 546 87%
Ca Oropharynx

Malyapa – PTCOG 49 Educational Workshop
IMRT Proton TherapyComposite
72 GyCCB only
1.5x12=18 Gy
Composite72 CGE
CCB only1.5x12=18 CGE
Contralateral parotid (mean dose ≤ 2600 cGy
2529 460 1482 0
Brainstem (5500 cGy to 0.1 c.c.)
5020 890 2685 0
Spinal cord (5000 cGy to 0.1 c.c.)
4400 1106 546 0
Contralateral submandibular gland
6928 1533 6148 820
Ca Oropharynx

Malyapa – PTCOG 49 Educational Workshop
Maxillary Sinus IMRT vs Protons

Malyapa – PTCOG 49 Educational Workshop
SNUC

Malyapa – PTCOG 49 Educational Workshop
IMRT: 1.2 Gy/FX BID to 50.4 Gy
Proton Boost: 1.2 CGE/FX BID to 24.0 CGE
Total Dose: 74.4 CGE
SNUC: IMRT+Protons
Malyapa – PTCOG 49 Educational Workshop
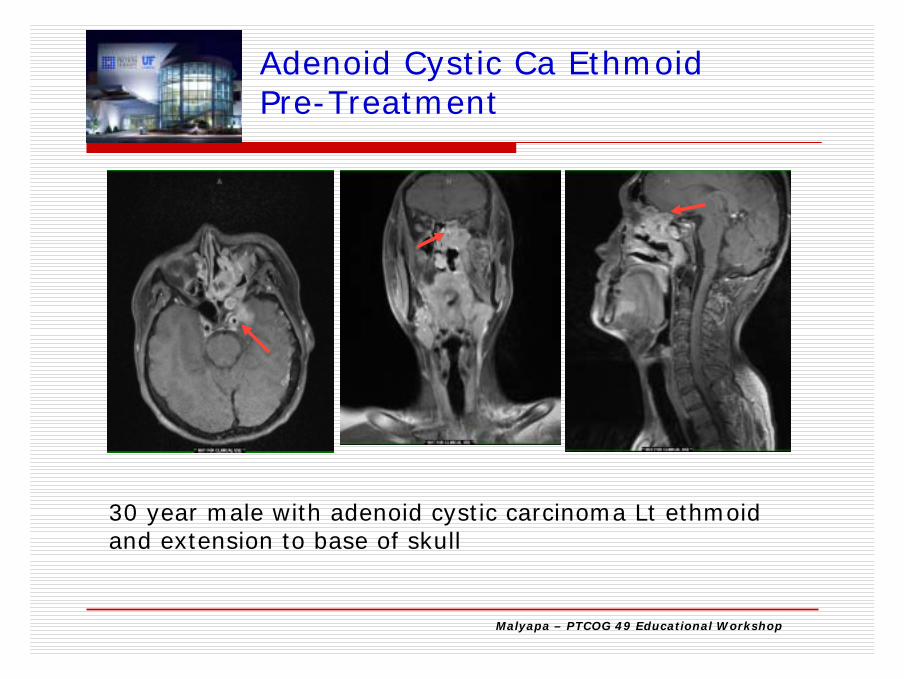
30 year male with adenoid cystic carcinoma Lt ethmoid and extension to base of skull
Adenoid Cystic Ca EthmoidPre-Treatment
Malyapa – PTCOG 49 Educational Workshop
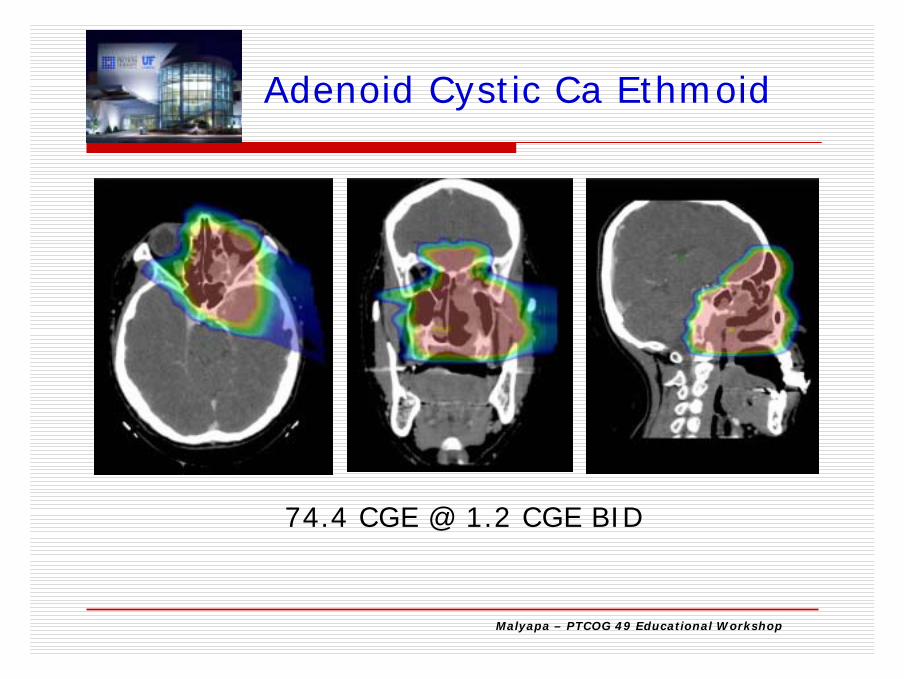
74.4 CGE @ 1.2 CGE BID
Adenoid Cystic Ca Ethmoid
Malyapa – PTCOG 49 Educational Workshop
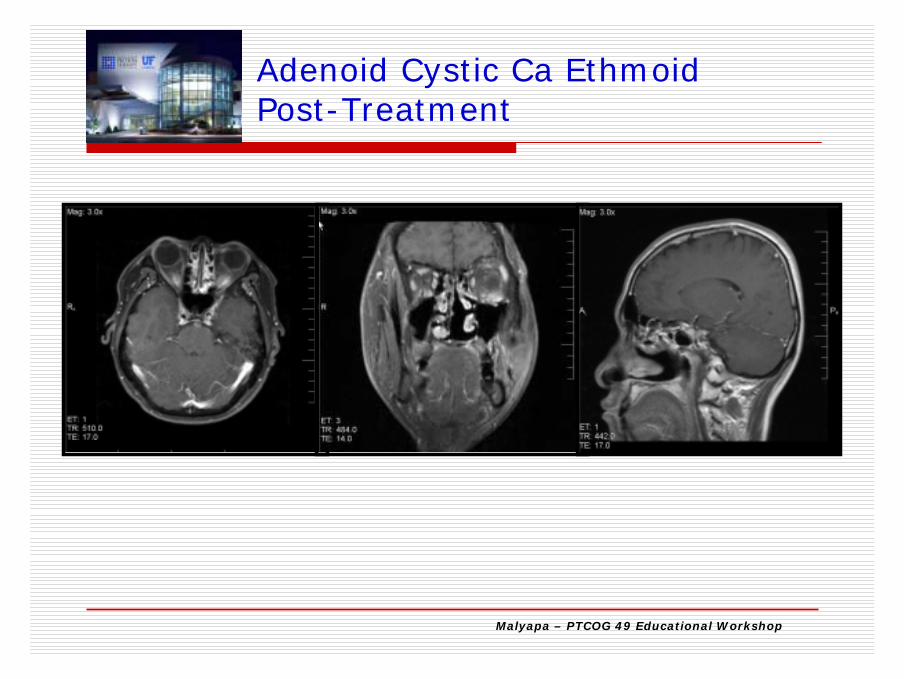
Adenoid Cystic Ca EthmoidPost-Treatment

Malyapa – PTCOG 49 Educational Workshop
IMRT: 50.4 + Proton Boost 24 = 74.4 CGE
LAN = 50.4 Gy
Ca Nasopharynx: IMRT + Protons
Malyapa – PTCOG 49 Educational Workshop
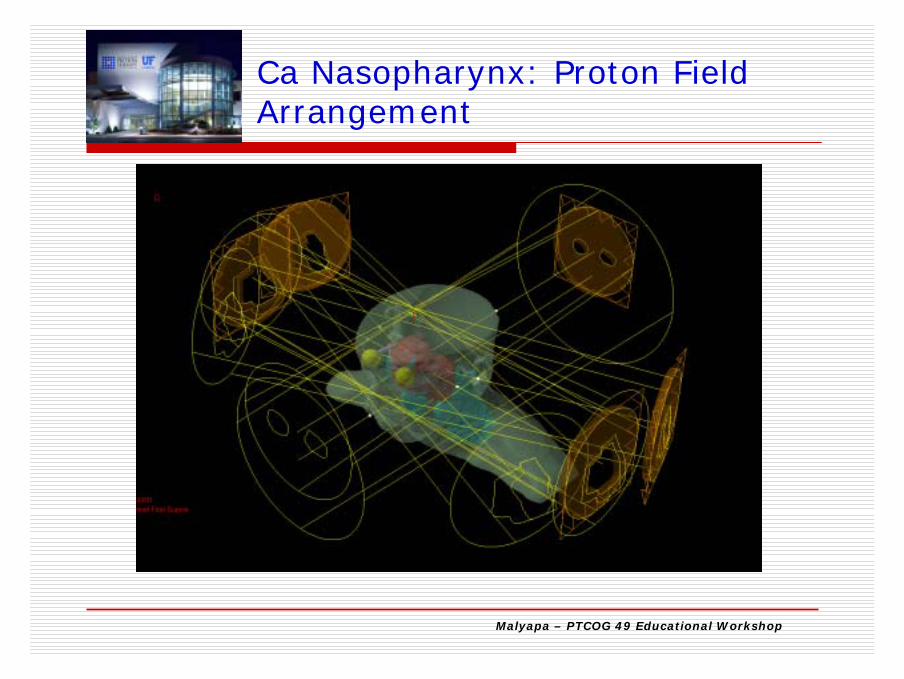
Ca Nasopharynx: Proton FieldArrangement
Malyapa – PTCOG 49 Educational Workshop
Ca Skin with Perineural Invasion
Malyapa – PTCOG 49 Educational Workshop
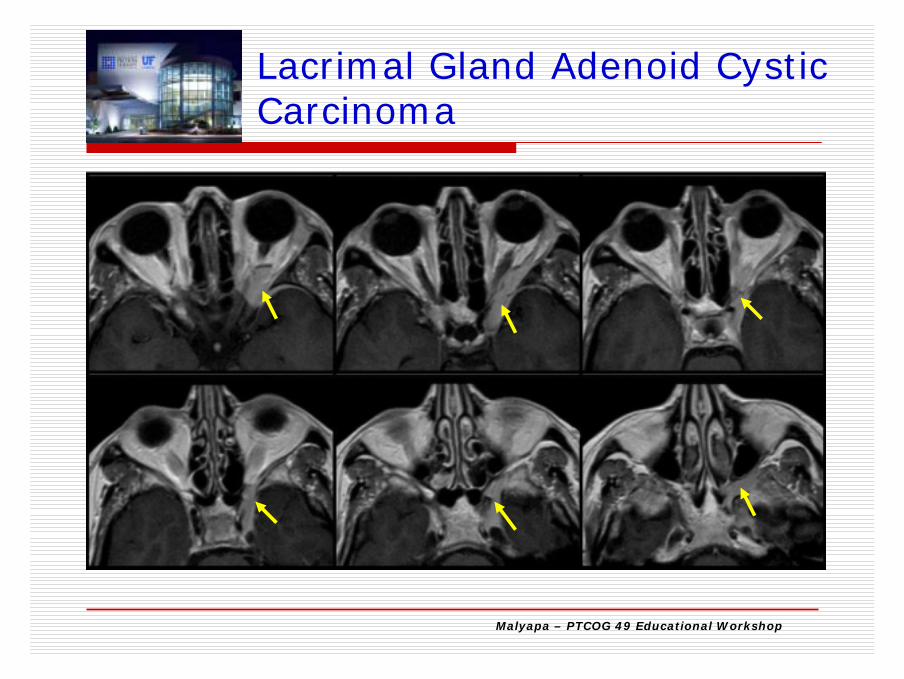
Lacrimal Gland Adenoid Cystic Carcinoma
Malyapa – PTCOG 49 Educational Workshop
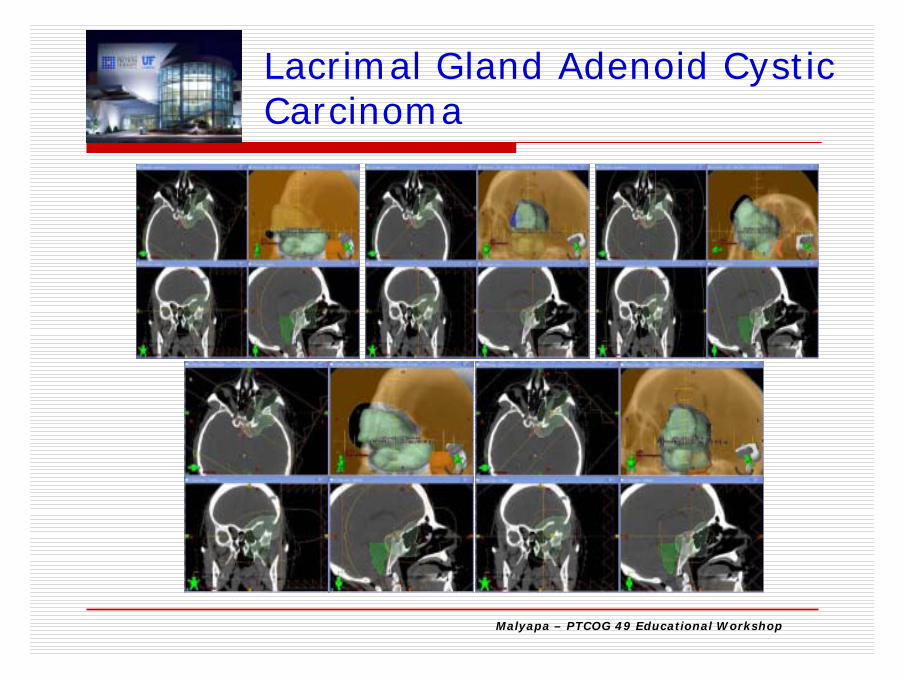
Lacrimal Gland Adenoid CysticCarcinoma

Malyapa – PTCOG 49 Educational Workshop
50407440
PTV50.4
RON
BS
Lacrimal Gland Adenoid CysticCarcinoma
Malyapa – PTCOG 49 Educational Workshop
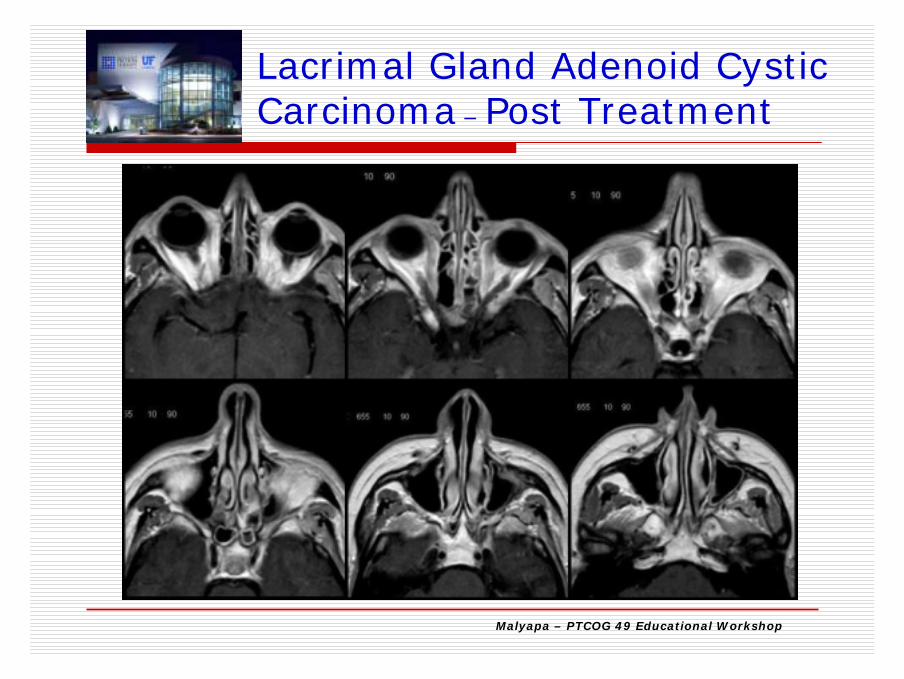
Lacrimal Gland Adenoid CysticCarcinoma – Post Treatment

Malyapa – PTCOG 49 Educational Workshop
IMRT
74.4 Gy
Protons
69.6 CGE
RE-IRRADIATION-Nasopharynx

Malyapa – PTCOG 49 Educational Workshop
H/O Multiple Cancers and RadiationTreatments Presented withCa Base of tongue

Malyapa – PTCOG 49 Educational Workshop
Acknowledgement
Daniel Yueng, PhDCraig McKenzie, CMDWilliam M. Mendenhall, MDZuofeng Li, DScNancy P. Mendenhall, MD