pthb integrated medium term plan - powys …€¦ · pthb integrated medium term plan 2015-2018 ......
TRANSCRIPT

Page 1 of 230
PTHB Integrated Medium Term Plan
2014-2017
March 2015
PTHB Integrated Medium Term Plan
2015-2018
“Truly integrated care centred on the needs of the individual”

Page 2 of 230
MESSAGE FROM THE CHAIR & CHIEF
EXECUTIVE
Health and wellbeing plays such an important part at every stage of our lives, and whilst we all hope
to lead healthy lives we know that there are times when we will need the services of health or social
care. This Plan sets out how over the next 3 years Powys teaching Health Board intends to work
together with the population of Powys, professionals and others to help achieve better health and
better health and care services. We start from a strong base of having a population that is generally
healthy, communities that are generally strong, health care services that generally serve the
population well and a health and care workforce that is truly committed to Powys. We know
however that there are areas where health is poorer that it could be and that inequalities exist; that
some health and care services are fragile; that some service provision is outdated and doesn’t
provide the best experience possible for people; and that some staff (whether doctors, nurses,
therapists, critical support staff, or managers) are stretched. Importantly, we also know that staff
across the county; individuals, communities and the groups that represent them; and leaders of
health, social care and other services are highly motivated to work together to continue to improve
the lives of people and communities in Powys.
Whilst the period of financial austerity for public services continues, we are determined that we use
such challenging times as a means to help us work more innovatively and creatively with the
population to improve health and provide better health and care services. Being ‘prudent’ is going
to be essential, and spending public money efficiently and effectively is critical, and is something
that we all collectively have responsibility for. Our plan focuses on 3 key elements:
Enhancing Primary and Community Care - Providing high quality and efficient care in or close to home makes sense on all fronts, especially in our rural county. Supporting GP teams, pharmacists, optometrists/opticians and dentists is key, as is developing a wide range of services in health and social care settings and our community hospitals.
Integrated Working – Finding new and better ways to work jointly with people who use our services, with other health organisations in and outside of Wales who provide services to the people of Powys, and essentially with our key partner Powys County Council. Powys, with its often complex arrangements and multiple borders, can demonstrate leadership and expertise on integrated working to others.
Excellent Commissioning – There are services we will continue to need to ‘buy’ from others for the people of Powys. We want these to be high in quality and effectiveness, innovative in approach and sensitive to the needs of the individuals who use them.
We anticipate that over the coming 3 years there will be change. Firstly, we intend to support people
to make positive changes in their own health and wellbeing. Secondly many of the services we ‘’buy’
on behalf of the people of Powys are needing to change and we will be working together with others
to help design and implement those changes, and last but certainly not least, the services we
provide in Powys will also need to change and we look forward to engaging positively with people to
deliver better services for all.

Page 3 of 230
TABLE OF CONTENT Message from the Chair & Chief Executive............................................................................................. 2
Table of Content ..................................................................................................................................... 3
1. Summary .................................................................................................................................... 5
2. Progress in Delivering 2014/15 Plan ........................................................................................ 14
3. Health Board Profile ................................................................................................................. 17
3.1. HEALTH ECONOMY OVERVIEW ...................................................................................................... 17 3.2. POWYS TEACHING HEALTH BOARD PROFILE ..................................................................................... 19 3.3. PARTNERSHIPS ............................................................................................................................ 20 3.4. HOSTED NATIONAL SERVICES ........................................................................................................ 29 3.5. OUR WORKFORCE ....................................................................................................................... 30 3.6. FINANCE .................................................................................................................................... 35 3.7. CURRENT PERFORMANCE ............................................................................................................. 36
4. Local Health Needs and Challenges ......................................................................................... 39
4.1. WORKING WITH PARTNERS TO UNDERSTAND HEALTH NEEDS .............................................................. 39 4.2. POWYS POPULATION DEMOGRAPHICS............................................................................................. 40 4.3. WIDER DETERMINANTS OF HEALTH ................................................................................................ 42 4.4. HEALTH SERVICE UTILISATION ....................................................................................................... 50 4.5. FOCUSING ON OUTCOMES ............................................................................................................ 52
5. Strategic Approach to Transformation .................................................................................... 55
5.1. NATIONAL POLICY DRIVERS ........................................................................................................... 55 5.2. STRATEGIC DIRECTION ................................................................................................................. 56 5.3. STRATEGIC FRAMEWORK .............................................................................................................. 57 5.4. DEMAND, CAPACITY AND FINANCIAL MODELLING ............................................................................. 58 5.5. TRANSFORMATION PROGRAMME ................................................................................................... 59 5.6. ORGANISATIONAL DEVELOPMENT .................................................................................................. 64
6. Quality and Safety Improvement ............................................................................................. 67
6.1. QUALITY DELIVERY PLAN .............................................................................................................. 67
7. Health Board Priorities ............................................................................................................. 73
7.1. PRIMARY CARE ........................................................................................................................... 74 7.2. EXCELLENT COMMISSIONING ......................................................................................................... 94 7.3. INTEGRATED WORKING .............................................................................................................. 103
8. Service Delivery Plans and Initiatives ..................................................................................... 107
8.1. PREVENTION AND HEALTH IMPROVEMENT ..................................................................................... 108 8.2. UNSCHEDULED CARE ................................................................................................................. 117 8.3. PLANNED CARE ......................................................................................................................... 122 8.4. INTEGRATED CARE FOR OLDER PEOPLE .......................................................................................... 131 8.5. MENTAL HEALTH ...................................................................................................................... 133 8.6. LEARNING DISABILITIES SERVICE ................................................................................................... 145 8.7. CANCER SERVICES ..................................................................................................................... 147 8.8. HEART DISEASE SERVICES ........................................................................................................... 149 8.9. DIABETES SERVICES ................................................................................................................... 151 8.10. SERVICES FOR END OF LIFE .......................................................................................................... 153 8.11. CRITICALLY ILL .......................................................................................................................... 156 8.12. STROKE SERVICES ...................................................................................................................... 157 8.13. RESPIRATORY SERVICES .............................................................................................................. 159

Page 4 of 230
8.14. NEUROLOGICAL CONDITIONS ....................................................................................................... 161 8.15. LIVER DELIVER PLAN .................................................................................................................. 163 8.16. ORGAN DONATION ................................................................................................................... 163 8.17. SUBSTANCE MISUSE .................................................................................................................. 164 8.18. MATERNITY SERVICES ................................................................................................................ 166 8.19. CHILDREN’S SERVICES ................................................................................................................ 167 8.20. SEXUAL HEALTH ........................................................................................................................ 169
9. Workforce & Organisational Development ........................................................................... 170
9.1. AN ENGAGED WORKFORCE ......................................................................................................... 171 9.2. A SUSTAINABLE AND SKILLED WORKFORCE .................................................................................... 175 9.3. PROFESSIONAL DEVELOPMENT............................................................................................ 181 9.4. WORKFORCE CHANGES .............................................................................................................. 183
10. Finance ................................................................................................................................... 186
10.1. FINANCIAL STRATEGY AND APPROACH TO COST REDUCTION .............................................................. 186 10.2. “SHIFT LEFT”............................................................................................................................ 188 10.3. SCOPE AND SCALE AND MANAGEMENT APPROACH TO COST REDUCTION ............................................. 190 10.4. THREE YEAR SUMMARY FINANCIAL PLAN AND FINANCIAL ASSUMPTIONS ............................................. 193 10.5. COST PRESSURES ...................................................................................................................... 196 10.6. SAVINGS PLAN .......................................................................................................................... 199 10.7. SUMMARY FINANCIAL THREE YEAR PLAN ....................................................................................... 201 10.8. RISKS AND FURTHER ACTIONS...................................................................................................... 203 10.9. FUTURE YEAR PLANNING SCENARIOS ............................................................................................ 204 10.10. CONCLUSION ............................................................................................................................ 206
11. Building Capability & Delivery ................................................................................................ 207
11.1. INFORMATION TECHNOLOGY ....................................................................................................... 207 11.2. CAPITAL & ESTATE .................................................................................................................... 210 11.3. RESEARCH & DEVELOPMENT ....................................................................................................... 214 11.4. INNOVATION ............................................................................................................................ 216
12. Stewardship and Governance ................................................................................................ 218
12.1. THE PLANNING PROCESS ............................................................................................................ 218 12.2. THE ENGAGEMENT PROCESS ....................................................................................................... 221 12.3. THE DELIVERY PROCESS .............................................................................................................. 222 12.4. FINANCIAL ASSURANCE .............................................................................................................. 226 12.5. THE ASSURANCE PROCESS AND CORPORATE GOVERNANCE ............................................................... 226

Page 5 of 230
1. SUMMARY
Powys has a unique opportunity to place healthcare services secured for the citizens in the County
on a sustainable footing. This Integrated Medium Term Plan (IMTP) sets out how the Powys
Teaching Health Board (PTHB) will set out on this path, through being a leader in Wales in the way in
which primary care and community services lead and drive healthcare services. The THB will achieve
this through strengthening the approach to planning and commissioning high quality services from
neighbouring organisations, and accelerating our joint ambitions for integration with Powys County
Council for the benefit of citizens.
The plan is grounded in the principles of prudent healthcare. Providing as much care as can
appropriately delivered in Powys is better care, is what patients are asking for, and for many services
can be provided at lower cost on a sustainable basis. This is an ambitious plan that invests in service
transformation in both the lifetime of the plan and beyond. In 2014-15 the THB is well placed to
have achieved a balanced financial outturn. In addition to reshaping its own resources, the THB has
secured additional funding from Invest to Save and set how additional funding from Welsh
Government will be applied to transformation in Powys. This Plan therefore sets out investment in:
Primary care and community services to continue our approach to provide more services in
Powys, and to secure robust and sustainable primary care sector;
Maintaining performance against access targets, and delivering improvement where required
through investment in primary care, greater focus on efficiency and effectiveness and delivery of
additional capacity to meet demand;
Securing delivery of a sustainable healthcare and social care system through investment in the
organisation’s capacity to plan, deliver and performance manage change.
The THB and the residents of Powys know that the primary care and community based services
provided within Powys are highly regarded and help people to stay safe and healthy. We want to
ensure that when care is required across our borders that this is provided on a timely basis, is of high
quality, and returns people to local services as soon as possible – using it only when necessary.
Integrated working with Powys County Council across the range of services provided by both
organisations is also central to our ambition to citizens receiving a well-coordinated and local service
within Powys.
This IMTP covers the period 2015-18 and is designed around the vision set out by the Board to
deliver “truly integrated care centred on the needs of the individual”. The Plan is built on the Joint
Strategic Needs Assessment (JSNA) that has been further developed in the last year with an
additional focus on understanding poverty in the County. The THB faces unique challenges in Wales.
The County covers 25% of the land-mass of Wales with only 5% of the population, and that
population has the fastest growing proportion of older people in Wales. The level of rurality,
challenging transport links and reliance on neighbouring health boards in Wales and NHS Trusts in
England for acute services inform this Plan.
The THB has three strategic challenges of its own for the future:
Designing and delivering a clinically and financially sustainable rural service model, providing as
much care as local to home as possible through a continued shift from hospital to community
based models of care;
Page 6 of 230
Meeting the changing needs of Powys residents as demographic change and improvements in
healthcare continue to make their impact felt on demand for, and cost of, services;
Working with partners and the public to support sustainable rural communities in a period of
public sector austerity.
The success of our plan will be measured by progress in the seven domains of the NHS Outcomes
Framework that was published in 2014. These outcomes are defined as:
People in Powys are well informed and supported to manage their own health;
People in Powys are protected from harm and protect themselves from known harm;
People in Powys receive the right care and support as locally as possible and are enabled to
contribute to make that care successful;
People in Powys are treated with dignity and respect and treat others the same;
People in Powys have timely access to services based on clinical need and are actively involved in
decisions about their care;
People in Powys are treated as individuals with their own needs and responsibilities;
People in Powys can find information about how their NHS is resourced and make careful use of
them.
The plan is set out to broadly follow the requirements of the NHS Planning Framework for Integrated
Medium Term plans. It is framed by our strategic priorities and associated strategic objectives in
three areas:
Primary Care and Community Services;
Commissioning;
Integration with Powys County Council.
The plan also sets out our focus and aspirations for improving the health of the population, our
response to the NHS Wales Service Delivery Plans and our supporting strategies for workforce and
organisation development, IT and estates, supported by the focussed work around our
transformation agenda.
Primary Care and Community Services Powys THB has three mature GP clusters in the north, mid and south of the County. Their views,
articulated though local ‘cluster plans’, have strongly influenced the developing priorities set out in
this Plan. Delivery of this plan will build resilience in primary care and community services and by
securing and expanding strong general medical services, work alongside other high street health
providers to support citizens in the County. Supporting and building GP leadership of the local rural
healthcare system is a key feature of this Plan. Developing a new rural model of healthcare with
primary care at its heart is the main focus of the THB’s response to the Mid Wales Study
recommendations. Primary Care will be therefore central to leading the Health Board’s Plans for
transformation of service delivery in the short, medium and long term.
Commissioning The THB is primarily a commissioning organisation with over half its financial resource devoted to
securing services on both an unscheduled and planned basis from neighbouring health boards and
NHS Trusts. Each of these organisations are moving forward with strategic change programmes to
deliver sustainable service models for the future, and the THB will work with partner NHS
organisations to both re-shape services in the medium to long term and secure effective, high
quality and efficient service delivery through the contract arrangements with these organisations. In
2014 the THB has reviewed its approach to commissioning and following this will strengthen these

Page 7 of 230
arrangements through establishing a Commissioning Programme, with a new Commissioning Board
at its heart. Strong commissioning is a key enabler to the delivery of this Plan, driving performance,
quality and efficiency.
Figure 1: PTHB Strategic Priorities and Objectives
Integration with Powys County Council The strategic partnership with Powys County Council through the Local Service Board and our single
integrated plan; the One Powys Plan, is central to the THB’s approach to the integration of health
and social care services at all levels within the organisations. Mental health services and services for
people with learning disabilities, older people and carers are key joint areas for attention. Powys
THB and Powys County Council are also focussed in their response to the Commission for Public
Service recommendation for greater integration of the two organisations. The two organisations
have a strong track record in integrated approaches to wider functions such as IT and the utilisation
of property and assets, and will further build on this work in strategic areas of joint interest.
Achievements Powys already works from a strong base in respect of the degree to which its primary care and
community service led approach drives service delivery, quality and drives down cost through a
prudent approach. The THB’s business is structured around three GP Clusters, and in 2014 the THB
has for the first time given these clusters a voice on the Board through the creation of a new
appointment of a Director of Primary Care and Community Services. This Plan takes significant
Commissioning
•Commission sufficient capacity to meet the need for timely and high quality healthcare services across the community and hospital system, with a shift in emphasis to prevention and early intervention
•Embed an innovative and prudent approach to service commissioning focused on patient outcomes
•Provide assurance on the quality and effectiveness of healthcare services across the healthcare system
Primary Care and Community
Services
•Increase the capacity of primary care and community services to deliver a greater proportion of care in Powys
•Increase the resilience of primary care and community services direct service provision
•Strengthen the clinical leadership role of primary care and community staff in service planning, commissioning and delivery
Integration
•Place the citizen at the centre of integrated service delivery through joined up systems, processes and teams, delivered at neighbourhood level
•Develop integrated approaches to support systems and functions across all areas of our shared business with Powys Council
•Put in place joint strategy, governance and scrutiny arrangements with Powys Council
Strategic Priorities

Page 8 of 230
account of the work Practices have undertaken to develop their own cluster plans. These have been
developed in response to the local challenges that GPs and their local multi-disciplinary teams face.
The THB has already demonstrated the power that GP clusters can bring to delivering new
approaches to patient care. In South Powys the ‘Virtual Ward’ provides an enhanced multi-
disciplinary GP led primary care and community service model; here early evaluation demonstrates a
reduction in the level of emergency admissions to out of county Hospitals. This model provides the
evidence for how GP leadership can design and deliver new models of care; the THB, following a
successful Invest to Save bid, plans to roll out this approach across the County over the next year.
The implementation of technology will also enable a step-change in the way in which multi-
disciplinary teams communicate with, and about patients. The THB with Powys Council will aim to
implement the Community Care Information System in 2015, supported by other innovative
technology developments including the learning the THB is gaining through its European technology
partnership projects, Carewell and Mastermind.
During 2014 the THB has taken action to focus attention on the performance of both its own services
and those of its secondary care providers. The THB has achieved close to 100% delivery of the 26
week Referral to Treatment Time. The THB has also delivered an improving position for diagnostics
and therapy waits. With its partners the THB is aiming to eliminate waits in excess of 52 weeks by
the end of March 2015 and for 2016 will aim for no patients to wait longer than 36 weeks. Across all
of its commissioned and directly provided services the THB is tantalisingly close to its aspiration of
achieving the 95% threshold for 26 week waits.
Both the Glan Irfon Integrated Health and Social Care Centre and the ‘Virtual Ward’ model are
examples of how the THB is transforming its service delivery to support the unscheduled care
system. The THB has also worked with the Welsh Ambulance Service to implement new pathways of
care that enable ambulance crews to assess patients and transfer their care safely to Powys services
including our Minor Injury Units, to avoid conveyance out of county. Conveyance rates by WAST
from Powys to Emergency Departments are the lowest in Wales. The IMTP sets out further work in
respect of unscheduled care to further strengthen the flow of patients back to Powys, particularly
where this has been compromised through capacity challenges in social care services in the
community. The THB will also work with the Emergency Ambulance Service Committee to develop a
specification for services that matches the local service model. The commissioning of the Emergency
Medical Retrieval and Transfer Service (EMRTS) will also provide a significant improvement in access
to services for people from Powys with acute health needs including stroke, myocardial infarction
and major trauma as well as significant progress in ambulance response times.
The THB’s ambition is to make significant progress against the requirements set out within Welsh
Government’s ‘Together for Health’ strategy and the associated plans, and to strive to deliver the
targets set out in the NHS Outcomes Framework for Wales. Progress with these Plans are set out in
Section 7 of this Plan and the profiles for delivery of targets are set out in Section C1. Delivering this
ambition for Powys residents within the current financial envelope, without compromising on
quality is extremely challenging and will take all of the efforts of the organisation, its partners and
the community to deliver. The THB is confident that it will meet this challenge.
In 2014 the THB has further strengthened its musculo-skeletal services in-county that operate on the
principles of prudent healthcare to avoid escalation of care to specialist orthopaedic services. These
are popular and well-received local services and such models are at the heart of our planned care
programme, grounded in the capacity and demand modelling. Creating new opportunities to

Page 9 of 230
harness the skills of nurses, therapists, and professionals working in ‘High Street’ primary care
services, are identified throughout this plan.
Case for Change The achievements in service change to date have been based on an emerging model that will
continue to inform the Health Board’s future transformation of service delivery. A core goal is to
refocus current investment to support health and wellbeing and the delivery of effective disease
prevention services and when people need services to secure them as close to home as possible
using a range of new models of delivery including use of new technology and integrated service
models to ensure safe, sustainable and economic deliver of care. The impact of the Transformation
Programme is to shift the balance of integrated care to secure a sustainable shift of activity towards
prevention, self-care and primary and community intervention, as illustrated in the diagram below:
Figure 2: Shifting the Balance of Care
In 2015 the teaching Health Board plans to launch a dialogue with the public around its own
Strategic Change Programme. In the past year the THB has commissioned and received independent
strategic modelling of capacity and demand for the Powys population that further strengthens the
evidence for change in the way in which services are provided for Powys in the future. The findings
of the Mid-Wales Study also re-enforce the evidence in respect for the need for strategic change.
The key messages include:
Our status as having the fastest rising number of elderly population will become an
unsustainable problem for the health board both in service sustainability and financial
affordability if we do nothing
There is clear evidence that we can create more sustainable and affordable services in Powys
that will limit the impact of our challenge, through the creation of innovative, primary care
driven models of care, facilitated through improvements in technology and integrated services.
There is a recognition however that there will always be services for which is it clinically safer for
patients to travel to settings outside of Powys
Our future model will be capital dependent given 50% of our buildings predate the NHS and our
technology is outdated
A dialogue with the public on these matters will be challenging. The work the THB and Powys
Council has undertaken in Builth Wells, with the public, to build a new service model, providing
reassurance that the THB’s ambitions are to provide more care in Powys rather than remove services
from communities provides a blue-print for how change can be co-produced and managed. Glan

Page 10 of 230
Irfon in Builth Wells was fully opened in 2014; it is an integrated health and social care delivery
model led by primary care that avoids the escalation of care and makes prudent use of resources,
and physical assets, which has been recognised as good practice by the Wales Audit Office.
Quality and safety improvement remains the golden thread underpinning our planning processes
and is central to our work and the activities that staff and teams undertake in providing safe care for
our patients. Sustaining and embedding this work is crucial to ensuring Powys residents receive the
highest standards of care. We recognise our duty in ensuring this focus is strengthened for the
services we commission and purchase from other organisations for our population.
In setting out our achievements and challenges through our Annual Quality Statement we are
continuously assessing and informing Powys residents about how well we are doing across all our
services. In 2013/2014 we set to engage all teams in organisation wide learning focusing on the
failings in Mid Staffordshire: we reached 55% of our workforce. Following the publication of the
report ‘Trusted to Care’ all ward areas and supporting teams have been engaged in self assessment
and peer review. We will continue to strengthen our approach to organisation-wide learning so that
we can assure our public that we are giving safe levels of care especially in the fields of hydration,
night sedation, continence and medicines management.
The fragility of the rural service model continues to be a major risk for service delivery in Powys.
Recruitment to the medical workforce in Powys has been a challenge to the THB in 2014, however
our GP partners have stepped up to ensure that vital local services remain open in our community
hospitals. The fragility of primary care is in itself a risk for the continued local delivery of services.
During 2014 the THB has worked with GPs to fully understand how it can support practices to ensure
primary care in Powys can be sustainable for the future. This plan therefore sets out action in three
interlinked areas:
Enhancing the leadership role of GP clusters in the strategic direction of the Health Board;
Supporting practices in new approaches to collaboration at cluster level to enhance their
sustainability, supported by a proactive approach to recruitment and retention;
Enabling practices to increase the portfolio of services they directly provide.
PTHB has highly unusual and complex arrangements for NHS adult mental health services. Around
250 NHS staff working in local teams and hospital wards in the county are employed by three other
health boards, following a transfer of services. The arrangements implemented in 2009 have failed
to deliver the required strategic changes needed to deliver modern mental health services that meet
local need. After an extensive stakeholder engagement and option appraisal exercise, the case for
returning the majority of mental health services to the direct management of the Health Board was
accepted by the Board
Powys teaching Health Board and Powys County Council are working together to implement an
ambitious programme to improve the mental health of local people, following public consultation.
The predicted rise in the number of people with dementia in the county means physical and mental
health services, and all local services, must work together even more closely.
Extensive further transformation work covering the domains of commissioning, quality, and the
model of service delivery is required to deliver a sustainable rural model for mental health care for
Powys.

Page 11 of 230
Approach to Transformation Capacity within Powys Health Board to drive change is a risk to delivery. This has been identified by
the Wales Audit Office through their Structured Assessment of the THB. The THB is addressing this
through implementing a programme approach to change and has invested in its change capability
through the creation of the Programme Management Office. The PMO has delivered its first major
project, the Strategic Capacity and Demand Financial Modelling report that provides a strategic
analysis of service activity to guide transformation for the THB. The overall Transformation
Programme has already been designed under the leadership of the Chief Executive with Executive
level leadership of the portfolio of change programmes.
Transformation Programme
Core Programmes Enabling Programmes
Strategic Delivery Model: programme designed and considered by the Board, will be launched in 2015. Will design and deliver the medium to long term clinical service change strategy Director of Planning and Performance Lead
Organisational Development Programme: programme design developed following the THB’s ‘Chat to Change’ engagement programme with staff Director of Workforce and OD Lead
Mental Health Programme: launched and will deliver strategic change in the management and service delivery for mental health services. A key decision will be taken by the Board on management arrangements in February 2015. Director of Nursing
Estates Programme: this programme is currently being scoped and will develop and deliver a short to medium term estates strategy as a bridge to the development of a medium to longer term Strategic Outline Programme for Estates based on the outcome of the SDM Programme Director of Planning and Performance Lead
Service Reform Programme: will deliver the short to medium term service change programme in planned and unscheduled care services in response to delivering capacity and demand Director of Primary Care and Community Services
ICT Programme: this programme is currently being scoped to build on and encompass previous change arrangements for the delivery of the NWIS IT Programme, the Information Programme and the Powys joint IT strategy with Powys County Council. Director of Finance Lead
Commissioning Programme: this programme is due to report before the end of March 2015 and will result in strengthened arrangements for commissioning to support strategic service change and commissioning cycle processes. Director of Planning and Performance Lead
Stakeholder Engagement Programme: will be delivered to support the delivery of all programmes and ensure a legacy of embedded engagement. Director of Planning and Performance Lead
The role and scope of the Transformation Board that oversees this programme has been reviewed
and strengthened in the year, including clear accountability through to the THB Board.
Strengthened Board governance arrangements have also been put in place during 2014 including the
creation of a Finance and Performance Committee that oversees Performance of the THB’s Annual
Plan, Outcomes Framework Targets and the Transformation Programme. The THB also has a shared
programme of transformation delivered through the Local Service Board arrangements that includes
integrating health and social care and the development of the wider integration of PTHB and Powys
County Council building on previous successes in, for example, our integrated IT service.

Page 12 of 230
Financial Plan In April 2013, the THB commissioned two independent and external provided reviews to consider
both the way in which the THB develops its financial planning and the scope of opportunities to
reduce costs. The diagnostic review undertaken by Deloitte tested the financial position and cost
reduction plans of the THB. This high level diagnostic, benchmarking the THB over a number of
areas, with other similar organisations, indicated that it would not be possible for the THB to deliver
a balanced financial plan over a five year timescale without reducing service quality. This work has
been acknowledged by Welsh Government and recognised through the additional allocation of
resources in 2014-15 to support the THB’s underlying financial position. During 2014 the THB has
undertaken a further detailed demand and capacity study that has provided an opportunity to
consider the Deloitte work in further detail – the outcome of this work underpins the financial
strategy in this Plan. Deloitte also stated that “the Welsh Tariff system makes life difficult for the
THB” and that local tariffs are opaque and make it difficult to manage providers. The modelling
work that has been undertaken identifies the potential scope for savings that can be made through
changes in service models, and this is linked to the need to reduce expenditure with all secondary
care providers. Given the scale of the THB’s expenditure on services provided by Welsh LHBs the
Welsh system remains a significant constraint on the ability of the THB to drive efficiency from its
providers in Wales.
Effective delivery of our plans therefore means the need to continue to strengthen the capacity of
our organisation to effectively plan and commission high quality services across the five health
systems that serve Powys. This means delivering a programme of organisational development that
will incrementally enable locality teams, led by GPs and other clinicians, to design, specify,
commission and performance manage services to meet local need, ensuring improvements in quality
while driving out unnecessary costs.
The financial strategy as presented in this IMTP builds upon the principles adopted in previous years,
focussing on the opportunities to “shift left” in terms of service delivery and fully embed the prudent
healthcare principles embraced by the organisation. Our financial plan for the next three years is
extremely challenging, it will rely on a high concentration of focus on efficiency and delivery through
all forms of leadership across the organisation and carries with it a high level of risk of achievement.
However, our ambition is clear in that we have set out a plan that, if delivered, will achieve break
even over the next 3 years of the Health Board. We believe this sets a powerful message of intent of
moving from a deficit culture to one of successful delivery of service and financial improvement.
The plan includes a high level of assumption of resourcing which will need to be fully confirmed with
Welsh Government through the approval process.
Strategy on a Page The following page summarise the IMTP through the development of a strategy on a page that will
form the basis of the every day version of the IMTP. This is in progress and will be fully completed
by April 2015.

Page 13 of 230
Develop rational outcome based system for planning and commissioning
Introduce framework for commissioned services ensuring quality and safety across providers and services
A L W A Y S W I T H O U R S T A F F
Commission sufficient capacity to meet the need
for timely and high quality healthcare services across the
community and hospital system,
with a shift in emphasis to
prevention and early intervention
TRULY INTEGRATED CARE CENTRED ON THE NEEDS OF THE INDIVIDUAL
Outcomes
Strategic Priorities COMMISSINING PRIMARY CARE & COMMUNITY SERVICES INTEGRATION
Embed an innovative and
prudent approach to service
commissioning focused on patient
outcomes
Increase the capacity of primary
care and community
services to deliver a greater
proportion of care
in Powys
Increase the resilience of
primary care and community
services direct
service provision
Strengthen the clinical leadership
role of primary care and
community staff in service planning,
commissioning and
delivery
Place the citizen at the centre of
integrated service delivery through
joined up systems, processes and
teams, delivered at neighbourhood
level
Develop integrated approaches to
support systems and functions
across all areas of our shared
business
Put in place joint strategy,
governance and scrutiny
arrangements with
Powys Council
Provide assurance on the quality and
effectiveness of healthcare services
across the
healthcare system
Staying Healthy
People in Powys are well informed and supported to manage their
own physical health
Safe Care
People in Powys are protected from harm and protect
themselves from known harm
Effective Care
People in Powys receive the right care and support as locally as possible and are enabled to
contribute to making that care successful
Dignified Care
People in Powys are treated with dignity and respect and treat
others the same
Timely Care
People in Powys have timely access to services based on clinical need and are actively involved in
decisions about their care
Individual Care
People in Powys are treated as individuals with their own needs
and responsiblities
Our Staff and Resources
People in Powys can find information about how their NHS is resourced and make careful use
of them
Strategic Objectives
Transformation Programme
Agree best future model of care and configuration of future services for the long term
Ensure public, patients and staff engagement Ensure processes are robust and rigorous
Deliver priorities for service development over 5 years
Manage implementation of efficiency, and quality improvement projects
Manage delivery and performance of service change
Prevention and Health Improvement : Make Every Contact Count• Reduction in Smoking prevalence • Reduction in Childhood obesity • Increased resilience of children and young people • Increased flu vaccination
Improve early diagnosis Complete review of cancer
chemotherapy Introduce cancer pathway
management
Develop specialist nursing services
Ensure action plans for at risk patients in community
Ensure self-management plans in place
Develop knowledge and skills framework
Develop evidence based standards for care
Develop local symptom management services
Birth 30% of women in Powys by 2016 Maximise usltrasound scanning and day
assessment in Powys Promote use of remote technology
Awareness campaign and identification of those with Atrial Fibrillation
Improve access to community rehabilitation
Support development of hyper acute services
Ensure equitable access to care at home
Ensure availability of appropriate carers
Ensure governance arrangements for hospice care
Strengthening diagnosis and management in primary and community services
Strengthen education and self management
Ensure waiting times targets are met
Develop consistent model for delivery of risk assessment
Improve participation in National Clinical Audit
Deliver NHS Adult Management arrangements project
Delivery of integrated Adult Service Model Strengthen partnership working
Finalise approach to integrated services for CAMHs
Develop management of elective and emergency paediatric pathways
Further develop community, School Health Nursing and Health Visiting
Develop co-ordinated processes for health and social care needs
Develop county-wide reablement service Review and deliver older people’s
commissioning strategy
Improve demand management through alternative pathway and virtual ward
Improve capacity management Improved escalation management
Enabling Strategies
Ensure optimum level of planned care provided in Powys within agreed target times
Repatriate appropriate planned care services Evaluate local MRI, deliver sustainable
audiology, sonography and opthalmology services
Delivery Plans
Implement estates compliance programme Deliver ‘first impressions’ programme Take forward proposals for Bronllys and Llandrindod
Wells
Build on chat to change programme Ensure 90% compliance with appraisals Recruitment and retention strategy across Powys
Implement Community Care Information Service Roll out primary care based systems Deliver further benefit of IT integration with PCC

Page 14 of 230
2. PROGRESS IN DELIVERING 2014/15 PLAN
In 2014 Powys THB prepared an Integrated Medium Term, however this plan was not signed off by Welsh
Government, and an Annual Plan was requested by Welsh Government and duly submitted by the Health
Board.
Progress with delivery of the THB’s Annual Plan has been monitored through the newly formed Health
Board Finance and Performance Committee. In its submission to Welsh Government in June 2014 with the
Annual Plan, the THB made a number of strategic commitments and progress against these are described
below.
Delivery and Performance In 2014 we set out our ambition to deliver against the Tier 1 targets for the Powys population. There have
been significant achievements against the Tier 1 targets, including:
Improvement in Powys as a provider to 100% at 26 weeks and the 95% wait no more than 18 weeks
Elimination of 52+ weeks in English providers
Improvement in the aggregate RTT performance across all providers;
Therapy waiting times have been held at 14 weeks from mid-year, other than audiology, where
significant improvement has been made;
Diagnostic waits have also demonstrated an improved position with only Sonography exceeding a wait
of 8 weeks, with action taken to deliver an improving position across year.
The THB has worked to improve performance management in respect of the specific pathways around
Stroke, Mental Health, Cancer and Unscheduled Care and has also developed an overall Quality Framework
for Commissioned services that will now be introduced across providers. Hospital acquired infections have
been reduced, and Powys achieved the 19% target for population level smoking prevalence in the year.
There remain areas of challenge, including full compliance with waiting times targets, ambulance response
times, mental health services performance and delayed transfers of care that feature highly in this Plan.
In 2014 the Health Board signalled its intention to prepare a strategic capacity and demand modelling
approach that covers both commissioned and directly provided services. This work was completed in
December 2014, procured from an independent health care planning organisation. This study has
informed this Plan and provides additional evidence to support the focus of where the THB is targeting
efforts to drive productivity and efficiency in its approach to commissioned and direct service delivery.
Workforce In 2014 we set out that our overall approach to workforce, given the size and turnover of the organisation
is to opportunistically develop the workforce including skill-mix changes. During the year the Health Board
has strengthened its leadership capacity and competency in change management with the appointment of
a Director of Primary Care and Community Services, the Director of Planning and Performance and an
extension to the Programme Management Office. As we indicated, our workforce has workforce has
remained relatively static with performance delivered through increased productivity.
Mental Health In 2014 we set out that Mental Health Services were a critical priority for the Board. The Board had an
approved strategy ‘Hearts and Minds; Together for Mental Health in Powys’ and has been working to deliver

Page 15 of 230
this ambitious programme of change. Significant improvements in the delivery of mental health services
have been achieved in the year with the full introduction of crisis teams, stabilisation and improvement in
Out of Hours provision, and close management of out of area placements to reverse a concerning and rising
trend. In February 15 the Board approved the transfer of the management arrangements for mental health
services to Powys following an extensive process of engagement and option appraisal. This process of
change is significant and a project approach is being used to ensure a smooth and safe transition to the new
arrangements is achieved.
Shift to out of hospital provision Through the appointment of the Director of Primary Care and Community we have strengthened the role of
GP clusters at both Board and operational level. A central tenet of the locality model in Powys has been to
‘do more in Powys’ and GPs and local teams have already made significant shifts in delivery to out of hospital
care models. An example of this is demonstrated through the Wales Audit Office audit of orthopaedic
services which shows that Powys has moved from being the THB that invested the least in community to
models, to be the highest performer in this category. The virtual ward is another example of a community
service that has reduced emergency admissions through a strengthened primary care model and we intend
to roll this out across the County. During the year the GP clusters have produced their own plans and they
are at the heart of this plan, to continue this shift in the model of care.
Finance Based on Month 11 financial performance the THB has a high level of confidence that it will achieve a
balanced outturn position for 2014-15 in line with the financial plan set out at the beginning of the year, and
with the underlying deficit being supported by Welsh Government. The THB has undertaken further
strategic modelling through an independent capacity and demand modelling exercise that further
demonstrates and supports the THB’s understanding of its medium to long term financial prospects. This
work underpins the Financial Plan in this IMTP and also forms the basis of the plans to formally launch work
on its Strategic Delivery Model during 2015, to establish the service model that is sustainable for the long
term future of the organisation.
Capital and Estates During the year the THB completed a Strategic Outline Programme to outline a five year programme of
investment in the THB’s Estate to address the considerable concerns in respect of health and safety
compliance in the THB’s estate. In 2014-15 the THB has secured an additional £2M in capital investment to
both address compliance matters and rationalise the estate, and this programme of work will continue over
the period of this IMTP.
The diagram below highlights a number of key strategic work programmes from our Annual Plan that have
been delivered in the year that also inform this IMTP, and will contribute to the design of a sustainable
organisation into the future.

Page 16 of 230
Figure 3:Key Strategic Work Programmes - Annual Plan 14/15
Refreshed Joint Strategic Needs
Assessment
Three GP Cluster Plans produced
Independent Strategic Demand
and Capacity completed
Revised Financial Allocation Acheived based supported by financial modelling
Transformation Programme Established
Chat to Change staff engagement programme launched
Quality framework for Contracted
Services introduced
Governance Review implemented at
Board level
Joint Planning with WHSSC and PHW
strengthened
Operational Demand and Capacity
modelling introduced
Active role in Future Fit, Acute Care
Alliances and Mid Wales Study
Further strengthened
Integration with Powys Council
Estates Compliance SOP
Developed second Joint IT Strategy
with PCC
Commissioning Review Complete
Audit Reports underpin change
programme

Page 17 of 230
3. HEALTH BOARD PROFILE Powys THB and its co-terminous County Council cover a quarter of the landmass of Wales, but with less
than 5% of the population, it is England and Wales’ most sparsely populated area. Powys THB is
responsible for commissioning services for approximately 132,000 people resident in the County.
A primary issue in health service need and delivery in Powys is access to appropriate services. The
population is rural, spread thinly across a large area and consequently, where facilities and services require
a critical mass of people to be economically or socially sustainable, they will out of necessity be spread out,
making factors of accessibility and transport critically important. A key resulting factor of this is the
absence of a District General Hospital and the consequent outflow of patients to hospitals and health
services out of county for treatment, this out of county activity equivalent to a virtual DGH of over 400
beds. While this generates complexities and challenges it also drives the strategic direction of the THB in
developing a rural service delivery model that balances prevention, integration with other public services
and care closer to home with the need to achieve economies of scale, sustainable service delivery and
access to specialised services.
3.1. HEALTH ECONOMY OVERVIEW
Powys THB is primarily a commissioning organisation, with the largest proportion of its budget devoted to
commissioning NHS services from primary care contractors and secondary care providers on both an
emergency and planned basis from neighbouring Health Boards, Welsh Ambulance Services Trust and
English NHS Trusts. The THB also commissions in excess of £1.7M of service delivery through the Third
Sector and holds contracts with care home providers for long term care as well as providing a range of
community services.
Powys is in a unique position in Wales in managing care over five main health systems that span its
borders. Each of these systems link into their own wider health economies to facilitate access to tertiary
services such that residents of Powys are required to travel as far as Stoke, Birmingham, Cheltenham,
Cardiff and Swansea. PTHB directly provides non-specialist healthcare services, through its network of
community services and community hospitals. The local community healthcare model is increasingly led
by the GP clusters in Powys in the design and delivery of local services and in advising on the
commissioning of specialist services. A key driver for the local healthcare economy is to provide as much
care as possible in Powys, avoiding out of county travel and providing a better experience for the
individual. The current hospital model is proving increasingly challenging to sustain, and a key future goal
is to redesign this clinical model and in the process strengthen the primary care sector to support a
sustainable future for healthcare in the community. The Welsh Government Primary Care Strategy
published in 2014 is a significant supporting driver to this work. There is also provision of an increasing
range of consultant led outpatients, day theatre and diagnostics in our community facilities, bringing care
out of the acute hospital setting.
The Health Board delivers operationally to its population through the leadership of three GP clusters
supported by locality management teams for North, Mid and South Powys in a single Directorate of
Primary Care and Community Services. These teams are also responsible for commissioning adult
secondary care services for their population.
Powys is the only Health Board in Wales to be co-terminous with a single local authority, Powys County
Council. The Health Board has forged strong partnership arrangements with Powys County Council at both

Page 18 of 230
GP cluster level and across the County. Joint projects such as the Glan Irfon Health and Social Care Centre
in Builth Wells and the Joint IT team under a Section 33 agreement are key joint achievements. The
organisations are key partners in the One Powys Plan, Local Service Board (LSB) and the LSB
Transformation Board. Both organisations are fully committed at Board and Cabinet level to further
integration as set out in the unique Powys response to the Commission on Public Service Governance and
Delivery, published in Jan 14.
An overview of our provider services e.g. general practices, community hospitals, is depicted below
alongside the flow of patients, and associated contract value out of county to help demonstrate the
complexity of relationships across our borders. Each of the five health systems in which Powys operates
has its own planning arrangements in which the THB takes a lead role to ensure that the interests of Powys
residents are considered in the process of change and transformation of NHS services. The forthcoming
year will see further engagement in the Future Fit programme that will determine the future service model
provided in Shrewsbury and Telford NHS Trust, the roll out of the outcomes of the consultation on service
change in South Wales through the Acute Care Alliances and the establishment of the Mid-Wales
Healthcare Collaborative in May 15 following the publication of the Mid-Wales Study by the Welsh
Institute of Health and Social Care.

Page 19 of 230
3.2. POWYS TEACHING HEALTH BOARD PROFILE
Community Hospital
Inpatient /Day
Hospital
Birth Centre
MIU Outpatients Mental Health
Services Other
Ystradgynlais X-Ray
Brecon Theatre, Endoscopy, Children’s Centre, Stroke Rehab, X-Ray
Bronllys
Llandrindod Wells Theatre, Endoscopy, Renal Unit, X-Ray
Knighton
Newtown Stroke Rehab
Llanidloes
Welshpool Renal Unit, X-Ray
Machynlleth X-Ray
Glan Irfon Health & Social Care Centre
Short stay shared care re-ablement beds
Primary Care Facilities Number GP Practices 17 Main & 12 Branch Sites
Community Dental Service 5
General Dental Practices 24
Optometry Practices 25
Community Pharmacies 23
External Funding Flows – Main Secondary Care Providers
Betsi Cadwaladr UHB £5M incl £3M Mental Health
South Staffordshire Trust £1M
Robert Jones & Agnes Hunt Hospital £7M
Shrewsbury & Telford Trust £22M
Wye Valley Trust £12M
Aneurin Bevan UHB £17M incl £6M Mental Health
Cwm Taf UHB £1M
Cardiff & Vale UHB £1M
Abertawe & Bro Morgannwg UHB £9M incl £2M Mental Health
Hywel Dda UHB £6M
WHSSC £29M
Figure 5: Location of Community Hospitals/Health & Social Care Centre
= Community Hospital
= Health & Social Care
Centre
Bronllys
Brecon
Ystradgynlais
Builth Wells
Llandrindod
Wells
Knighton
Llanidloes
Newtown
Welshpool
Machynlleth
Figure 4: Location of Community Hospitals/Health & Social Care Centre
Table 1: Community Hospital Services
Table 3: PTHB External Funding Flows
Table 2: Primary Care Facilities in Powys

Page 20 of 230
3.3. PARTNERSHIPS
To deliver the THB’s vision and strategic objectives, the THB is committed to working in partnership
to develop collaborative solutions that will improve people’s lives for the better, and make the
greatest positive impact on our population now and in the future.
The THB works closely with a wide range of stakeholders including Local Authorities, neighbouring
providers and commissioners of health services within Wales and across the border, Third Sector,
the independent sector, other public bodies, Academic partners, the Community Health Council,
volunteers and not least service users and carers.
Working in partnership supports the Health Board to deliver with partners the six statutory well
being goals contained within the draft Well-Being of Future Generations (Wales) Bill:
A prosperous Wales
A resilient Wales
A healthier Wales
A more equal Wales
A Wales of cohesive communities
A Wales of vibrant culture and thriving Welsh Language.
The forthcoming bill also highlights governance principles that underpins the development of our
strategy as a Health Board with partner bodies:
Long term thinking – public bodies should seek to consider the likely effect over a 25 year period
An integrated approach – how well-being objectives impact upon each other and in turn on the
objectives of other public bodies
Preventative action – deploying resources now in order to prevent problems occurring or getting
worse
Collaboration – acting collaboratively with other bodies to assist in the achievements of the
objectives of all
Engagement – involving the people and communities whose well-being is being considered and
engaging them and others in finding sustainable solutions.
The THB engages in a complex series of partnerships: internal, Powys and cross border
arrangements, both within the NHS Sector and on a multi-agency basis. The following section
highlights some of our key partnerships.
The Integration Agenda and the One Powys Plan The THB has a long history of working in partnership across a wide range of service areas. Agencies
in Powys came together in 2009 through the Local Service Board to take collective action to develop
effective services. Powys was an early adopter of the single integrated planning process and adopted
its first ‘One Powys Plan’ in 2011.
Our approach to improving health and well-being and reducing inequity within Powys is to work with
our partners, particularly through the Local Service Board (LSB), to develop a joint approach to
improving health now and laying the foundations for maintaining good health for the future as part
of the wider public service offer in Powys.

Page 21 of 230
The THB and Powys County Council have set a clear direction of travel for greater integration of
services between both organisations prior to the publication of the Commission on Public Service
Governance and Delivery in January 2014.
The Commission proposed changes to the 22 Local Authorities. For Powys, the report went further
and recommended that, because of the unique characteristics of the county of Powys and the
distinctive patterns of service delivery that this creates, Powys County Council and Powys Teaching
Health Board should merge. The report outlines that this should be a two stage process.
The Health Board and the Council, with the support of the Welsh Government, should
immediately begin action to integrate all their governance, management and delivery structures.
They should define these arrangements by the end of 2014-15, and implement them
immediately thereafter; and
The Welsh Government and the National Assembly for Wales, in consultation with the County
Council and the Health Board, should define and legislate for a new single body to provide
integrated health and local government services in the county. The new body must be
established as a going concern, that is, with no historic health deficit, and with stable ongoing
funding arrangements consistent with the approach to health and local government services in
the rest of Wales.
In response to the Commission, Powys County Council and Powys teaching Health Board are
progressing particular opportunities to integrate more governance, management and delivery
services under the umbrella of the One Plan, and in support of the One Plan through more effective
and sustainable use of resources. The benefits of integration therefore are focused on the following
key areas and priorities:
Integrating Front-line Services
Integrating Professional & Business Services
Organisational and Integration Development
One Powys Plan Through the vision set by Powys Local Service Board in the One Powys Plan to drive for integrated
service change in the County, there have been improvements to services in Powys, particularly in
relation to children’s services through the Children and Young People’s Partnership and for older
people. There has also been strong collaboration in developing shared support functions. The THB
and Powys County Council have in place an over-arching Section 33 agreement through which the
organisations manage joint arrangements for IT services, reablement services, the Glan Irfon
Integrated Health and Social Care project, joint equipment and substance misuse services.
To achieve the vision of "Strong Communities in the Green Heart of Wales" One Powys Plan (2014-
2017) is focused on 5 strategic change programmes.
Integrated Health and Adult Social Care
Transforming Learning and Skills
Children, Young People and Families
Stronger, safer and economically viable communities
Organisational and Partnership Development.
The priorities described in this IMTP for older people, mental health, children ad learning disabilities
are jointly owned, managed and delivered change programmes. The One Powys Plan is delivered

Page 22 of 230
through a joint Transformation Board that operates across all partners, governed by the Local
Service Board (LSB).
Figure 6: PTHB & PCC Joint Transformation Board
NHS Partnerships The THB is engaged in strategic planning for the NHS in Wales and across its borders in England to
ensure that the interests of Powys residents are taken into account as services change and develop.
Managing these partnerships is a key element of our strategic delivery model. Powys Teaching
Health Board is currently a partner in the following strategic change programmes illustrated in the
diagram below:
Mid Wales Healthcare Collaborative;
South Wales and South Powys Programme;
Future Fit Programme;
Wye Valley Transformation Programme;
Transforming Cancer Services in South East Wales Programme.
Figure 7 below illustrates the complexity of strategic planning arrangements when the additional
requirements of other regional planning is overlaid with the geography of Powys. The challenge for
the THB, and its Powys partners, is to ensure an approach is taken by the organisations that leads
the service model for the County and responds to neighbouring plans, rather than being driven by
them.

Page 23 of 230
Figure 7: Strategic Change Programmes with PTHB Involvement
Mid Wales Collaborative During 2014 – 15, a study of healthcare for the Mid Wales population was undertaken by the Welsh
Institute for Health and Social Care to identify key issues and potential solutions (including models)
for providing accessible, high quality, safe, and sustainable healthcare services, which are best suited
to meet the specific needs of those living in Mid Wales. The study highlighted the impact of travel on
patients, serious challenges facing primary care; the difficulties retaining skilled staff and developing
resilient services.
The study presented a series of recommendations to deliver significant changes in ways of working
that strengthens the role of Bronglais General Hospital as a key centre for secondary care for the
foreseeable future. The Mid-Wales Study proposed the three Health Boards (Hywel Dda, Powys and
Betsi Cadwaladr) should establish a joint governance mechanism, The Mid Wales Healthcare
Collaborative, alongside other partners, to both plan sustainable services for rural mid-Wales and
provide a focus for thinking around rural health models of service delivery for Wales.
Welsh Government has appointed co-Chairs to take forward the Collaborative, which was launched
in March 2015. This highlighted areas of focus for the Collaborative and was a mechanism to engage
wider stakeholders in the initiation of its work. The Collaborative will hold its first meeting in May 15
and arrangements are currently being established to support the Collaborative’s work through the
appointment of a Clinical Director and Project Team.
The Powys focus on a sustainable primary care and community service model, commissioning of safe
and effective services for its population and integrated service delivery with Powys Council is entirely
aligned to the work that the Collaborative will take forward and the added value the Collaborative
will provide both as a focus for Rural Health Practice and in new, innovative and collaborative

Page 24 of 230
models of service delivery. Key to the success of the Collaborative will be re-building the trust of the
public in the NHS offer in highly rural and isolated areas of Wales.
The Study provides a comprehensive framework against which this new Collaborative will be taken
forward. The accountability arrangements between the Collaborative and the Health Boards will
need to be considered in the early part of 2015-16 to ensure clarity on the scope of the work of the
Collaborative. The starting point is the recommendations from the Study contained in the following
table;
Recommendation Initial Response
The three Health Boards should establish a joint governance mechanism (working title: The Mid Wales Healthcare Collaborative) as described in the report, in order to implement many of the recommendations below.
Welsh Government has appointed joint chairs and each health board is committed to putting in place the necessary arrangements to establish the Collaborative in following the launch in March 2015.
Public engagement in Mid Wales should be established on a new basis, and coordinated by The Mid Wales Healthcare Collaborative.
Powys is re-framing its public engagement process as a consequence of changes to the role and function of the CHCs in Powys, and in developing an engagement process around its strategic delivery programme. Powys will work with the Collaborative to harmonise approaches and with those of other strategic change programmes that affect the population of rural mid-Wales.
The three Health Boards should re-double their efforts to address the pressures facing local primary care, developing complementary services, creating new models, sharing functions and providing business support, looking at new organisational models for general practice, and where possible providing targeted financial support. There is traction to be gained by the Boards coordinating their efforts to meet the specific circumstances of Mid Wales, and considering shared solutions where appropriate.
The response to this recommendation is laid out in our Strategic Objectives for primary care and the primary care section of this. Collaboration on this matter will be an early issue for the Collaborative, building on existing relationships.
The Welsh Government national Primary Care Plan should address the many common and systemic challenges facing primary care, which lie beyond the scope of the Health Boards.
This is a matter for Government. The Plan has subsequently been published and will be taken into account, as per the primary care chapter of this Plan.
Hywel Dda University Health Board, supported by the other two Boards, should confirm publicly its vision of the future strategic role of Bronglais General Hospital and the strategic direction which it intends to pursue. The Health Board’s submission to this study (Appendix 13) provides a good basis for such a vision. It will require subsequent detailed consideration of pathway and service options, but should be sufficiently specific to reassure potential and current staff and the public that the hospital will remain an acute centre, and that urgent and non-urgent provision will address the challenges of remoteness. It should state explicitly the criteria which must be met, based on the Six Key Service Criteria set out in this report.
The three Heath Boards accept this requirement, and will deliver this by March 2016.
Clinical staff in all the specialties should now be actively engaged in clinical discussions with their colleagues about how services should develop. This process will require active leadership and facilitation by the Hywel Dda University Health Board, working on behalf of the Mid Wales Healthcare Collaborative. It must address the difficulties in the relationships between the hospitals, and should include representatives from primary care, the Royal Colleges, the Deanery and service providers from Scotland and elsewhere who have successfully addressed some aspects of rural acute care provision. This process, including reviews by professional bodies, should address the specialty- specific issues (see below), but also their interdependencies, and the linkages with pre-hospital care
Powys Health Board has its own clinical engagement mechanisms as identified in this plan, both at cluster level, and in support of developing the Powys Strategic Delivery Model. These mechanisms strengthen the capability of the THB to engage with this discussion that follows form this recommendation.

Page 25 of 230
and between hospitals, along the patient pathways. It is important that the medical Royal Colleges are all engaged in this work, along with the learned bodies drawn from the other professions.
A further examination of the options for providing cardiology services in Bronglais General Hospital should now be started, which takes full account of the broad range of presenting conditions at this hospital, and evaluates alternative ways of constructing the sort of clinical network support that is needed. This should build upon the initial discussions held as part of this study, and the submission to this study from the Royal College of Physicians (see Appendix 14), both of which offer some grounds for optimism that alternative solutions are worth exploring.
The three Heath Boards accept this requirement, and will deliver this by March 2016.
A similar process should take place in relation to general surgery, building on the discussions initiated by this Study and scheduled for October 2014, and for Maternity and Obstetric services in Bronglais General Hospital.
The three Heath Boards accept this requirement, and will deliver this by March 2016.
Unnecessary journeys to access care should be eliminated, with a coordinated and comprehensive examination of relevant pathways to ensure care is actually provided closer to home, clinics and other provision is organised to reflect travel difficulties, patient’s are encouraged to choose options which suit their needs, and patients and visitors are provided with information to help them access remote services. This will require a coordinated effort crossing hospital and Health Board boundaries.
The three THBs will initiate a detailed analysis of the journeys that patients are required to make, those that are essential and those can could be delivered through alternative means. This work will be completed by March 2016.
Plans to develop more advanced skills in the ambulance service in Mid Wales should be supported and expedited.
The three Heath Boards accept this requirement, and will set out a plan to deliver this partnership with WAST and in conjunction with the new Emergency Ambulance Service Committee.
There should be a coordinated effort by all three Health Boards to identify the opportunities for much greater use of telehealth capacity and a determined drive to hasten its implementation.
The three Heath Boards accept this requirement. Powys teaching Health Board is currently developing a shared telehealth/care Strategy with Powys Council that can link in with a more regional approach.
The three Health Boards, working with local universities and others, should develop and support a centre of excellence in rural healthcare, with a particular focus on research, development and dissemination of evidence in health service research which addresses the particular challenges of Mid Wales. This has great potential to carry out work of relevance internationally. A high-profile conference on Mid Wales healthcare as described in the report should be organised immediately.
The conference has been held, organised by Welsh Government. Options to take forward this recommendation will be considered by the Health Boards with a proposal coming forward by March 2016.
South Wales and South Powys Programme ‘The South Wales Programme’ is a Board of five health boards and WAST that is planning strategic
service change for unscheduled care, children’s services and obstetric services across the South
Wales region. The collaborative works through its Acute Care Alliances, and whilst the THB has a link
to each of these, the main focus is the changes to be delivered through the South East ACA. In the
period that this Plan covers there will be significant changes in the configuration of services across
South Wales. Whilst this has a relatively minor impact on the direct service delivery within Powys,
there are significant areas of change in which the THB will engage as commissioner of services for
residents of South Powys, to protect the interests of and access to services. In particular the THB
will be concerned that any interim service change arrangements that are put in place in advance of

Page 26 of 230
the full implementation of new models retain appropriate access to the rural population of South
Powys. Specific attention will therefore be paid to the arrangements for:
Access to emergency paediatrics across the Heads of the Valleys;
Transition arrangements for clinical support to the Powys Midwife service, and arrangements to support a potential shift in choice of location of birth by women from Powys;
Access to hyper-acute stroke services in the Heads of the Valleys area;
Due attention to public transport links to Prince Charles Hospital;
Due attention to on-going equality impact assessment.
Future Fit Programme The ‘Future Fit Programme’, is a partnership programme with Telford and Wrekin and Shrewsbury
Clinical Commissioning Groups to plan the future pattern of service delivery in Shrewsbury and
Telford NHS Trust. The programme is looking at how future services need to be designed to best
meet the needs of the population and to provide excellent healthcare services for decades to come.
Some of the key benefits to be secured from this programme are:
Highest quality clinical services;
A service pattern that will attract the best staff and be sustainable;
A service pattern which delivered the right care in the right place at the right time;
A service which supports care closer to home and minimises the need to go to hospital;
A service pattern which meets the distinct needs of both our rural and urban populations across Shropshire, Telford and Wales;
Ensures a positive experience of care.
The programme is being developed in full dialogue with patients, public and staff. In 2014 the THB
has been part of an engagement process with Powys residents in respect of the future service model
for Shrewsbury, Telford and North Powys.
Work is progressing to agree and appraise the options for delivering care and a recommended short
list of options was presented in early 2015 in preparation for formal public consultation on a short
list of options later in 2015 with a view to a decision on the preferred option by early 2016.
The shortlist of scenarios for transforming emergency, planned and urgent care that will also serve
patients from mid Wales were made by an expert Evaluation Panel of which there were Powys
representatives. The recommended shortlist is:
1. Emergency Centre (EC) and Diagnostic & Treatment Centre (DTC) on a New site;
2. EC on a New site, DTC at Princess Royal Hospital (PRH)
3. EC on a New site, DTC at Royal Shrewsbury Hospital (RSH)
4. EC at PRH, DTC at RSH
5. EC at RSH, DTC at PRH
6. Do minimum (existing dual site acute services maintained, provider and commissioner efficiency
strategies implemented but no major services change).
These options will be developed further in preparation for public consultation later in 2015. There is
also further work planned to look at:
The best and safest configuration of obstetric services within these scenarios. This will include
reviewing the clinical evidence and workforce models to understand whether obstetrics could
operate on a site alongside a DTC, alongside an Emergency Centre or alongside either.

Page 27 of 230
To prototype two urban Urgent Care Centres, one in Shrewsbury and the other in Telford and to
explore the most appropriate rural urgent care solutions in partnership with local communities
and considering current facilities/services. All existing Minor Injuries Units will be considered as
potential sites for Urgent Care Centres.
Powys THB is currently reviewing the minor injury service provision across Powys and will be
establishing an internal working to ensure appropriate community based models of care in Powys
for our local population; this will take into account the rural urgent care solutions under the Future
Fit programme, and make links to other neighbouring programmes around Powys.
Securing sustainable healthcare for our population is a key priority for the Health Board and we will
continue to actively participate in the Future Fit programme and to ensure that we are aligned in our
thinking around the development of new models of care and to ensure we can provide the best and
appropriate level of healthcare for our population.
Wye Valley Trust Transformation Programme During 2014 Wye Valley NHS Trust was placed in special measures following an inspection by the
Care Quality Commission. The THB works closely with both the Trust and the Hereford Clinical
Commissioning Group to monitor progress against the patient care improvement plan and ensure
that Powys patients access safe ad effective high quality care. The THB will be a partner in taking
their transformation programme led by Hereford CCG which is anticipated to be taken forward in
2015.
Transforming Cancer Services in South East Wales Programme In the changing landscape of cancer survival rates increasing and the number of people getting
cancer increasing, Velindre Cancer Centre is launching a programme of engagement to help shape a
shared vision to transform cancer services in South East Wales.
Velindre Cancer Centre provides specialist cancer treatment but recognise that future models of
care need to be developed as part of the bigger picture of cancer care. It means any discussion
about specialist services needs to be done in the context of a shared understanding of how cancer
care in South East Wales might look in the future.
Velindre Cancer Centre developed a strategic outline programme for future cancer care in South
East Wales and the principles of this have been approved by the Welsh Government. This
engagement programme will test the principles outlined in the strategic outline programme and will
firm up the details around the service model and the ways in which we can improve outcomes for
patients.
Mid and West Wales Health and Social Care Collaborative The Future Generations (Wales) Bill sets a clear strategic direction for the Health Board to support
communities to ensure they are protected from pressures that threaten their viability and survival.
The Health Board will work with partners at a local and regional level to safeguard the long term
interests of local communities by addressing intergenerational challenges such as health inequalities,
mitigating the impact of climate change and raising skills.
The Mid and West Wales Health and Social Care Collaborative provides a strategic framework for co-
ordinating and delivering a range of health and social care programmes across the region,
maximising the resources available and bringing about service improvement and transformational
change in how we jointly provide services and achieve efficiencies and improved outcomes for

Page 28 of 230
citizens in the region. The collaborative brings together the six local government and health
organisations in the region.
The Mid and West Wales Regional Collaborative is a mandated partnership on the same footprint
that brings together the four Supporting People teams in Mid and West Wales and reports to the
Supporting People National Advisory Board. The collaborative was established in 2012 and during its
first year has made strides towards regional collaborative working through understanding and
debating regional approaches and barriers to working collaboratively across Mid and West Wales in
the housing and homelessness sector.
The Local Resilience Forum (LRF) is the partnership also at Mid and West Wales level that responds
on a partnership basis to the Civil Contingencies Act, and Powys falls into this region for the
purposes of this Act. The LRF works on a risk based approach to plan and practice for civil
contingencies, and Powys is an active partner in this approach focussing on high level risks of
Pandemic Flu, Major Incident and risks to Business Continuity.
International Partnerships The THB was successful in gaining funding to participate in two European funded projects. CareWell
is a project in which the THB is one of six pilot sites across Europe and considers multi-level
integration for patients with complex needs and has two key areas of focus: Integrated Care
Coordination Pathway, Patient Empowerment and Home Support Pathway and Mastermind is a
project that will implement online access to cognitive behavioural therapy.
The THB is a signatory to the International Charter for Health Partnerships and aims to develop an
‘International Office’ to develop innovation with European and international partners. Our vision is
to make links across the world to support service improvement and innovation and place ourselves
in a global partnership. We aim to add to our portfolio through establishing a new partnership in
each year and form a strategic partner with one region in Europe.
The THB is also an active partner in Wales for Africa programme and has on active local links with
Molo in Kenya, primarily focussed on maternal and child health.
Ensuring Integration with our Partners’ 3 Year Plans We have ensured our three year plan integrates effectively with strategic plans of our partners by
sharing our emerging plan and priorities with our NHS partners to ensure we support each other in
taking forward our mutual priorities.
For example we have shared a draft plan with Public Health Wales, the Wales Ambulance Services
Trust, WHSCC and Shared Services Partnership and Betsi Cadwaladr University Health Board to seek
their engagement and comments. We are also considering their draft plans and in discussion on key
elements of mutual interest and priority. The following provides a short summary of they key areas
of interface with some of our key NHS partner plans.
Emergency Ambulance Services Commissioner and Welsh Ambulances Trust;
NHS Wales Shared Services Partnership;
Public Health Wales;
Welsh Health Specialised Services Committee;
National Wales Information Service.

Page 29 of 230
Powys Teaching Health Board’s Strategic Delivery Model Programme During 2015 the THB plans to launch its own engagement process with the people of Powys to
discuss the future clinical services strategy in Powys. This is the Health Board’s primary focus and is
driven by challenges in sustaining high quality and safe care through the current delivery model; the
need for renewal of the estate in Powys; the need to see a step change in the prevention, primary
care and community service provision in the County, and to respond to changes to models of service
delivery across our borders.
This work will need to engage with all of our neighbouring strategic partnerships and ensure that the
emerging model takes into account service changes planned around our borders, and aligns with the
One Powys Plan.
The Programme will be underpinned by working within Powys and across our borders in partnership
with all our key stakeholders and the public in the spirit of co-production – we must deliver services
with people not to people. The empowerment of people and partners to enable their proactive and
meaningful engagement in the design and delivery of the programme will be integral to the success
of the programme.
3.4. HOSTED NATIONAL SERVICES
Powys THB provides leadership and support to Wales through hosting three functions on behalf of
NHS Wales.
NISCHR AHSC Powys THB currently has a contract with NISCHR Welsh Government to host the NISCHR AHSC.
NISCHR AHSC facilitates collaboration between NHS organisations, higher education institutions and
the industry sector across Wales and currently has 29 members of staff based across Wales. NISCHR
AHSC facilitates and supports research being undertaken in NHS Wales and has 13 strategic
objectives in order to provide this support including running dedicated funding schemes,
implementing NHS R&D funding policy, delivering the research ethics service and permissions co-
ordinating process in Wales.
From the 01 April 2015, the NISCHR AHSC will no longer exist and will be replaced by the new
NISCHR Support Centre.
The establishment of the NISCHR Support Centre will also include the receipt of 17 new staff through
TUPE transfer (from Velindre NHS Trust- host for CRC) from 01 April 2015. Once again, NISCHR AHSC
has been working closely with Velindre NHS Trust and Powys THB HR team to ensure the transfer
goes smoothly.
Community Health Councils The Health Board currently hosts the eight Community Health Councils in Wales, and the national
team representing CHCs. Community Health Councils are governed by their own statutory
framework, so the hosting role relates mainly to financial and human resource processes. The total
number of staff hosted by Powys under this agreement is 105 people. The Health Board meets on a
monthly basis with the Chief Executive of CHCs in Wales to ensure that the Health Board is
supporting CHCs appropriately. During 2015 Powys Teaching Health Board will support the
reorganisation of CHCs in Wales in terms of structural realignment and management of change
following the implementation of the outcome of the review of CHC’s in Wales.

Page 30 of 230
Continuing Healthcare Retrospective Project The Health Board hosts the Continuing Healthcare Retrospective Project and its 26 staff. The project
has been phased as follows:
Phase 1- The project was established in June 2011 to review 2454 claims received by Health
Boards in response to the cut off date advertised by Welsh Government in December 2009. The
project achieved this within the 3 year timeframe set. Phase 1 covered the claim period 01 April
1996- 15 August 2010.
Phase 2- The project has agreed to review a percentage of cases currently held by Health Boards
that have not yet been reviewed. The number of cases transferred to the project for review is
726 (circa 50%). It is planned that Phase 2 will finish on 31 December 2014 although this will be
impacted on due to the delay in receiving cases to activate. Phase 2 covers the claim period 01
April 2003- Present
Phase 3- The project will review all applications made for a retrospective CHC review (relating to
the claim period April 2003 to July 2013) received in response to the recent cut off date
advertised by Welsh Government. There are potentially 2486 claims although all applicants have
until 31 December 2014 to submit all evidence required to validate their claim. The final number
of cases to be reviewed will be known at this time. It is planned that phase 3 will begin on 01
January 2015 with a 2 year timeframe in which to review all cases. Phase 3 covers the claim
period 01 April 2003- 31 July 2013
The project aims are:
To review all claims relating to phases 2 & 3 within the target timeframes.
To ensure the standard of review and the governance arrangements of the project stands up to
scrutiny
A detailed business plan is being produced for phase 3, Welsh Government is providing £1.35m for
phase 2 with Health Boards providing £0.1m. The Minister has indicated that the funding of phase 3
will be the responsibility of Health Boards.
3.5. OUR WORKFORCE
As primarily a commissioning organisation, Powys has a unique workforce profile. 19% of the total
revenue budget or £47.5M is attributable to the paybill within the Health Board, with the variable
pay element being approximately 6%. Pay costs of other NHS Wales organisations typically account
for 70 - 80% of total budget.
Figure 8: Workforce Profile by Staff Group

Page 31 of 230
The Health Board employs 1517 people (Headcount) or 1189.61 FTE (Full Time Equivalent) posts.
This refers to directly employed staff only and excludes hosted services.1 The composition of the
staff group is presented above in terms of staff group and age profile. Staff working in clinical
services account for 65% of our workforce.
In comparison to last year, this equates in a reduction of 62.01 FTE. However, this is due to All
Wales Continuing Care and NISCHR now being classed as Hosted Services. If we exclude these
from last year there has been a decrease of 2.11 FTE for Powys only staff.
Over 86% of our workforce are female. This is slightly higher than the NHS Wales profile of 77%
Across Powys the average FTE worked by each member of staff is 0.78. This is the participation
rate and it enables increased opportunities for meeting temporary workforce requirements in
areas where is a greater proportion of part-time staff.
Our Workforce by Pay Band
Figure 9 shows 44% of our staff are in Bands 1 – 4 and 50% of staff are in Bands 5 – 7, 6% in
Bands 8 and above and 2% are Medical and Dental staff.
In addition, 56% of staff are on the top incremental point (64% of nurses).
Turnover for the last 12 months is 7.84%, which equates to 93 FTEs. This is a slight increase on
the previous 3 years which equated to 76 FTEs (6% average turnover) and is attributable to the
age profile of our staff.
Our Workforce by Age Profile
Figure 10 shows 746 (48%) of our current workforce are already over the age of 50, of which
327 (21%) are aged 50 – 54, 240 (15%) are aged 55 – 59
129 (8%) are aged 60 – 64 and 50 (3%) are aged over 65
1 The Hosted Services for Powys total 132.73 FTE which comprises All Wales Continuing Health Care 24.40 FTE, (27 Headcount) NISCHR
26.53 (28 Headcount) and Community Health Councils 80.8 0 FTE (97 Headcount) and 1.00 FTE (1 Headcount) Ambulance Services
Figure 9: FTE of Staff by Pay Band

Page 32 of 230
Figure 11 shows that in the majority of our workforce groups, the age profile has increased since
2010 to 2014. Significant areas for concern are Medical and Dental, Nursing and Midwifery and
Estates and Ancillary.
Whilst Powys has a very small employed Medical and Dental workforce, the age profile with the
General Practitioner workforce is also of concern. Data from December 2014 shows that 43%
(59) of the Partner 26%(36) and Locum13% (23) GP workforce are aged 51 and over with a
further 26% (36) in the 46 to 50 age group, a proportion of which may take early retirement.
One of the implications of an ageing workforce is higher sickness absence rates and this is
explored further in the following section.
Figure 10: Age Profile of Workforce
Figure 11: Shift in Workforce age Profile from 2010 to 2014

Page 33 of 230
Health & Wellbeing Since June 2014, the Health Board has developed “A New Approach to Attendance Management” based on the Department of Health’s 5 High Impact Changes to improve sickness rates.
Figure 12 which gives the Rolling, Actual and Target sickness percentage highlights
A consistent drop in actual sickness rates from the peak in June 2014.
In November 2014, actual sickness absence dropped to 4.39%, the lowest rate this year which is below the 4.42% target.
In December 2014, actual sickness absence for the month was only 0.03% above the target.
Rolling Sickness Absence has been below 5% for the past 3 winter months and is averaging 4.52%, which is only 0.1% above the rolling target.
The majority of staff sickness absence is due to long term sickness and detailed analysis shows that a contributing factor is our ageing workforce.
Figure 12: Sickness Absence
Figure 13: Age Comparison and Sickness Absence

Page 34 of 230
The age profile of our workforce therefore presents significant challenges in terms of managing
sickness absence, despite this however, the Health Board is currently able to demonstrate falling
actual sickness absence rates and show that sickness absence rates in all age groups from 50 upwards
is significantly below the NHS Wales percentage.
Performance and Development Review As of January 2015 the rate for Performance and Development Reviews (PaDR) is 65.69%. Since March
2014 peak of 78.61%, there has been a gradual decline in performance in this area. The impact of
organisational change at a senior level has been a significant contributing factor to this decline. There
are continued efforts being made to ensure that the Health Board gets back on track with this to mirror
and improve on the success of 2013 – 2014.
Despite a drop in July and August 2014, Medical Appraisals (Figure 15) have made considerable
improvement and are currently at 95.65%
Implications for Workforce Development Low turnover and the constraints of national terms and conditions inhibit the capacity to re-skill
mix and employ staff on lower bands or at the bottom of pay scale. In addition, national
Figure 14: Performance and Development Reviews Progress
Figure 15: Medical Performance and Development Reviews Progress

Page 35 of 230
organisational change arrangements prohibit the release of savings from workforce redesign as
staff would be on long term protection.
The age profile of the workforce poses risks and opportunities for the Health Board, as
experienced staff could leave whilst creating opportunities for workforce redesign to meet
changing service needs.
A downward trend in sickness absence rates will increase productivity, staff engagement and
have a positive impact on reducing costs and increasing Performance and Development Review
rates
The impact of organisational change within the Health Board with such a small infrastructure
cannot be underestimated.
3.6. FINANCE
As is set out in the finance chapter, the Health Board is funded by Welsh Government to secure a
range of healthcare services to the population of Powys. We are the smallest Health Board in Wales
in terms of population and accordingly receive just over 4% of the total resource available to NHS
Wales. To date, the health board has struggled to live within the resource allocation provided by
Welsh Government. The reasons for this is set out in the finance chapter of this plan. However this
difficulty has been recognised by Welsh Government who have provided additional financial support
to the organisation is recognition of our unique and structural challenges.
Given the “money follows the patient” in the NHS Wales finance regime, the Health Board secures
its services from a range of NHS and non NHS providers as well as directly delivering a full range of
community based services within county based on the healthcare services they provide to the
county’s residents.
How we deploy our resources is set out in in the pie chart below. As can be seen, we currently spend
nearly half of our resource on organisations who deliver healthcare to our population beyond our
boundaries making us a uniquely shaped organisation in the context of other Health Boards NHS
Wales where more services are delivered “in-house” than beyond their geographical borders.
Figure 16: PTHB Annual Spend with External Providers

Page 36 of 230
Whilst we have no District General Hospital within the boundaries of the county, we purchase the
equivalent of a very small DGH from a range of providers beyond our borders. Given our geography,
it is extremely unlikely that we will ever create the critical mass to warrant or sustain a purpose built
DGH in county and therefore our commissioning relationships with the organisations to whom our
population naturally flow are critical to the continued care provision of our population. All other
services are secured or provided in much the same way as any other health body and are delivered
by a range of voluntary, independent and primary care organisations including our own.
Our financial strategy going forward as set out in the finance chapter is founded on creating in-
county critical mass and efficiency through the establishment of strong, strategic and operational
relationships with our range of partners including other Health Boards, the Primary Care Sector and
with Powys county Council. This is necessary to prepare for the inevitable rise in service demands
that will be placed by our fast rising elderly population in future. We have described this as “Shift
Left”, avoiding growth in the secondary care sector through building capacity and capability not just
within the primary / community sector, but through partnership with our patients in terms of their
management of their conditions.
3.7. CURRENT PERFORMANCE
Table 4 shows the THB’s performance against the Outcomes Framework targets set out within the
IMTP Guidance C1 Template. Due to the complex commissioning arrangements for the THB,
performance is set out in two columns.
PTHB Performance: This column reflects performance of Powys where it is a direct provider of
services, but not providing the whole range of services for the population.
All-Powys Residents: This column reflects performance of Powys as a commissioner of services
for the whole population, including where known the performance of provider organisations that
provide services for Powys residents.
Actions to address those areas where performance is not in line with expectations are set out in the
detail of this plan. High priority areas for attention are:
Achieve no waits longer than 36 weeks for RTT by March 2016 and deliver 95% performance at
26 weeks;
Incrementally improve ambulance performance over the three year life of the plan;
Deliver sustainable performance in diagnostic and therapy services;
Reduce delayed transfers of care;
Deliver sustained performance against smoking cessation and flu immunisation targets;
Deliver sustainable performance in mental health services against the mental health measure.
The following table details the latest available performance for 2015/16 against new framework
targets.

Page 37 of 230
Table 4: Current Performance against Targets
Domain Deliverable Targets 2015/16
Detail PTHB
Provider Performance
Performance for all Powys
Residents
STA
YIN
G H
EALT
HY
Number of emergency admissions for basket of 8 chronic conditions Reduction
Admissions (Powys Residents)
126
Number of emergency readmissions for basket of 8 chronic conditions
Emergency Readmissions (Powys Residents)
7
% uptake of the influenza vaccine in the following groups:
75%
Patients >65 years 66.5%
< 65 years at risk 48.1%
All Pregnant women 2014/15
46.4%
50% Staff Uptake 50.2%
Uptake of scheduled immunisations for children < 2 years
95%
5 in1 age 1 93%
MenC age 1 95%
MMR1 age 2 94%
PCV age 2 94%
HibMenC Booster age 2 93%
% estimated LHB smoking population treated by NHS smoking cessation services
5% (end of fin year)
1.9%
% smokers treated by NHS smoking cessation services who are CO- validated as successful
40% (end of fin year)
38.5%
% of reception class children (aged 4/5) classified as overweight or obese
Reduction
*23.2%
EFFE
CTI
VE
CA
RE
Crude Mortality Reduction
Powys Provider 11.22%
RAMI 2013 Welsh Commissioners 103
% valid principle diagnosis code 3 months after episode end date
95% Monthly 98.3%
% valid principle diagnosis code 3 months after episode end date
98% Rolling 12 Months 99.8%
Number of NISCHR clinical research profile studies and Commercially Sponsored studies
Improvement Reported Annually 16
Number of Audits the organisation is participating in against the national clinical Audit Programme
Improvement Reported Annually 8
% people aged 45+ who have a GP record of blood pressure measurement in the last 5 yrs.
Improvement
**39.76% 2013/14
TIM
ELY
CA
RE
% GP practices offering appointments between 17:00 and 18:30 at least 2 days a week
Improvement
Powys GP surgeries 100%
% of GP practices open during daily core hours or within 1 hour of the daily care hours
Powys GP surgeries 100%
% of patients waiting less than 26 weeks for treatment – all specialties
95% Under 26 Weeks Powys Provider
99.7% 92.80%
Number of 36 week breaches – all specialities 0 Patients waiting > 36 weeks Powys Provider
0 101
% of patients waiting less than 8 weeks for diagnostics
Improvement % waiting less that 8 weeks
97.5%
% of new patients spend no longer than 4 hours in MIU
95% Total Powys MIU
99.8%
Number of patients spending 12 hours or more in MIU
0 Total Powys MIU
0
% of Cat A Ambulance responses within 8 minutes 65% WAST Performance (Powys) 50.2%
Number of over 1 hour handovers WAST Performance (Powys)
No data available
Cancer Referral to treatment targets (Welsh Providers)
98% 31 day target 95.1%
95% 62 day target 93.2%
Cancer Referral to treatment targets (English Providers)
96% 31 day target 96.4%
85% 62 day target 81.5%
Patients treated by an NHS dentist in the last 24 months as % of population
Improvement
60%

Page 38 of 230
% compliance with acute stroke bundles:
1 - First hours bundle
No data available
2 - First days bundle
No data available
3 - First 3 days bundle
No data available
4 - First 7 days bundle
No data available
IND
IVID
UA
L C
AR
E
% of assessments by the LPMHSS undertaken within 28 days from the date of referral
80%
82.6%
% of therapeutic interventions started within 56 days following assessment by LPMHSS
90%
86.9%
% of LHB residents (all ages) to have a valid CTP completed at the end of each month
90%
95.3%
% of hospitals with arrangements to ensure advocacy available to qualifying patients
100%
100%
% of over 65 registered as having dementia with their GP practice
Improvement
***0.75% all ages
DIG
NIF
IED
CA
RE
% procedures postponed on >1 occasion, had procedure <=14 days/earliest convenience
Improvement 0
SAFE
CA
RE
Delayed Transfer or Care Reduction rolling
12 months
Mental Health DToC patients (rate per 10k pop)
7.6
Non Mental Health DToC patients +75 years age (rate per 10k pop)
232.6
Number of healthcare acquired pressure sores in a hospital setting
Reduction Powys hospital's pressure damage incidents monthly
5
Number of total cases of C Difficile Reduction Cumulative yearly figure 14 cases
Number of total cases of MRSA per month Reduction Cumulative yearly figure 0
% compliance with patient safety solutions - alerts
Improvement
100%
% compliance with patient safety alerts - rapid response notices
100%
Number of new Serious Incidents Reduction
41
Number of new Never Events 0
OU
R S
TA
FF
&
RES
OU
RC
ES
% staff absence due to sickness Reduction Internal Target 4.42% 4.84%
% of total medical staff undertaking performance appraisals
Improvement Internal Target 85%
90.9%
% of total non medical staff undertaking performance appraisals
Improvement Internal Target 85% 67.2%
*% of reception class children (aged 4/5) classified as overweight or obese The latest data available is from 2012/13 but measurements only happened to 534 out of 1267 which is a 42.1% uptake
** % people aged 45+ who have a GP record of blood pressure measurement in the last 5 yrs. Currently blood pressure information is collected from QOF (BP001). The new requested measure does not relate to the current measurement which is Age 40+ for 2013/14 financial year (*latest available). The measure for the current financial year is set at Age 50+ 2014/15 but the annual figure will not be available until the end of March 2015. Currently we are investigating a new data source to allow the measure to be profiled and reported.
***% of over 65 registered as having dementia with their GP practice The Health board currently has access to Dementia data via CMWEB interface and QOF. *Unfortunately they currently only provide dementia figures without the age cut-off requested in the measure there is a request out to NWIS for a relevant data source.

Page 39 of 230
4. LOCAL HEALTH NEEDS AND CHALLENGES
In Powys…
There is a greater proportion of people aged over 50 years and a smaller proportion of working
age adults compared with Wales. There will be a substantial growth in the number of those aged
over 65 years and 75 years, this growth will rise at a faster rate than for Wales.
While economic wellbeing is above the Wales average, there is hidden poverty associated with
rural communities and in the larger towns. Ystradgynlais is the most deprived area of Powys and
is among the worst 10% of Lower Super Output Areas (LSOA) in Wales.
13% of children in Powys are living in poverty; this is higher in some areas – 34.8% of children in
Brecon St John.
Powys is the most deprived Local Authority in Wales for access to services.
Between 2004 and 2013, there has been a reduction in the proportion of Year 11 leavers not in
education, employment or training.
A greater proportion of adults in Powys engage in healthy behaviours compared with Wales,
however there is considerable room for improvement.
Powys adults report using health services less than adults across Wales, except for dental
services.
46% of adults in Powys report being treated for “any illness”.
There has been no significant reduction in the proportion of babies born with low birth weight
between 2004 and 2013.
Dental health for five and 12 years olds is improving overall in Powys and Wales.
There are significant gaps in mortality between the least and most deprived quintiles in Powys
for all age, all cause mortality for males and females, mortality from circulatory disease and
mortality from respiratory disease.
4.1. WORKING WITH PARTNERS TO UNDERSTAND HEALTH NEEDS
In 2013/14, a “refreshed” Joint Strategic Needs Assessment (JSNA) was developed by Local Service
Board partner organisations and provided an overview of health and wellbeing in Powys. The JSNA
was used as the basis for deciding joint priorities and led to the development of the Powys Single
Integrated “One” Plan.
The findings from the 2013/14 JSNA were used by Powys teaching Health Board (THB) to link local
health needs with the three year vision, strategy and service delivery plans, enabling a more
evidence driven approach. In addition, as part of a Neighbourhood Management pilot in Newtown,
data was segmented (where possible) at a Neighbourhood level, enabling a better understanding of
community population profiles and needs.
Following on from this, the JSNA 2014/15 has focused on poverty within Powys. This JSNA adds to
the data and intelligence developed in 2013/14, providing further depth to understanding the Powys
population. Much of the data for the JSNA 2014/15 has been presented at Lower Super Output Area
and therefore provides a detailed profile of communities in Powys.
Key findings from the JSNA (both 2013/14 and 2014/15) are presented below and provide a brief
overview of health needs of the Powys population.

Page 40 of 230
In addition, data and intelligence from other sources e.g. Public Health Wales Observatory, Welsh
Government are included to give a fuller picture of health status and health need.
4.2. POWYS POPULATION DEMOGRAPHICS
The demographic trends for Powys present a significant challenge to Powys THB in delivering a
sustainable health care system. The population pyramid for Powys shows that there is currently a
greater proportion of people aged over 50 years and a smaller proportion of working age adults (20
to 39 year olds) compared with Wales.
The projected population pyramid for Powys for 2033 shows that there will be a smaller proportion
of under 54 year olds in Powys compared with Wales and there will be a substantial growth in the
number of those aged over 60 years, who will form a large proportion of the Powys population.
Population projections for Powys show that by 2033, the over 65 age group is set to increase
dramatically, with an 80% increase between 2008 and 2033. A 20% rise has already been seen in the
five years since 2008 and during the life of this plan this is set to rise by a further 10%. If current
trends continue, the proportion of people aged under 65 will decrease by the year 2033.
14 12 10 8 6 4 2 0 2 4 6 8 10 12 14
00-0405-0910-1415-1920-2425-2930-3435-3940-4445-4950-5455-5960-6465-6970-7475-7980-84
85+
Proportion (%) of population
Proportion of population by age and sex, Powys &
Wales: 2010
Powys LA females Powys LA males Wales females Wales males
Produced by the Public Health Wales Obseravtoryusing data from 2010 mid year population estimates, Office for National Statistics
00-04
05-09
10-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
80-84
85+
14 12 10 8 6 4 2 0 2 4 6 8 10 12 14
Projected proportion (%) of population
Powys LA females Powys LA males Wales females Wales males
Produced by the Public Health Wales Obseravtory, using population projections from Stats Wales (WG)
Proportion of projected population by age and sex, Powys & Wales, 2033
Produced by the Public health Wales Observatory using data from 2010 mid year population estimates, Office for national Statistics and using population
data from Stats Wales (WG).
Figure 18: Proportion of Population by Age and Sex, Powys & Wales: 2010
Figure 17: Proportion of Projected Population by Age and Sex, Powys & Wales: 2033

Page 41 of 230
Figure 20 illustrates how the proportion of Powys residents aged over 75 years is higher than Wales
and will continue to rise at faster rate than for Wales.
1.6% of the Powys population identify themselves as Black & Minority Ethnicity (BME), an increase of
0.8% from 2001. The highest proportions of BME population in Powys are in Brecon, Llandrindod and
Newtown North East.
Source: Public Health Wales Observatory
Produced by Public Health Wales Observatory, using data from the Welsh Assembly Government.
Figure 19:2008 Based Population projections for Powys THB
Figure 20: Projected Population, 2008-2033, % Aged 75 and over

Page 42 of 230
4.3. WIDER DETERMINANTS OF HEALTH
Our population’s health is determined by not just factors specific to an individual e.g. genetic
predisposition or age, but also by the community in which they live, their living and working
conditions and the socio-economic and environmental conditions they are subject to.
Figure 21: The Determinants of Health
Economic Wellbeing and Poverty Poverty is accepted as being relative to the place and time in which a person lives. In the UK, those
who have an income below 60% of the median are classified as living in poverty.
Deprivation is a broader concept than poverty and includes a lack of resources and opportunities
which individuals would expect to be able to access.
The Welsh Index of Multiple Deprivation (WIMD) provides a measure of relative deprivation for
small areas in Wales. The WIMD can be used to give an overall deprivation rank for each Lower
Super Output Area (LSOA) for eight domains (income, employment, health, education, access to
services, housing, physical environment, community safety). Key facts for Powys include:
LSOA Ystradgynlais 1 is the most deprived area in Powys and is among the worst 10% in Wales.
Five LSOAs are among the worst 30% of areas in Wales (St John 2 (Brecon), Llandrindod
East/West, Newtown South, Welshpool Castle, and Newtown Central 2)
Powys is the most deprived Local Authority in Wales for access to services. 42 LSOAs are among
the worst 10% of areas in Wales.
There is hidden poverty in Powys associated with rural communities, with pockets of poverty in
larger towns such as Ystradgynlais, Brecon, Llandrindod and Newtown.
Overall in Powys, 13% of children in Powys are living in Poverty, compared with 21.9% of children in
Wales. However, there are 11 LSOAs where poverty rates are higher than the Welsh average, with
the highest rate being in St John 2 (Brecon), where 34.8% of children are living in poverty. The
proportion of children in Powys living in a workless household is 11.3%, which is below the Welsh
average.
Whilst there is uncertainty about the impact of welfare reform on Powys residents, it is estimated
that by 2017, 56% of working age population will be affected. By 2015/16, the average loss per
working age adult will be £391 per annum.

Page 43 of 230
Although fewer households in Powys (19.6%) are workless compared with the Wales average, wages
for full and part time workers are lower. The mean average full time annual wage in Powys is just
under £3,000 less than the Welsh average and the median annual wage is just over £4,000 less. On
average, Powys residents earn consistently less than many other Welsh Local Authorities, ranking
third lowest in Wales.
35% of households in Mid Wales are classified as being in fuel poverty. More specifically, 42% of
pensioner households and 19% of families with dependent children are in fuel poverty.
Powys has a disproportionately high number of small businesses, alongside a high proportion of self-
employed workers. This needs to be seen in the context of 11.3% of men and 8.9% of women of
working age in Powys having no formal qualifications.
In 2004, 4.4% of Year 11 school leavers in Powys were not in education, employment or training,
compared to 7% across Wales; by 2013, this figure had improved to 2.7% in Powys, lower than the
Wales rate of 3.7% (figure 22). It is not possible to determine if these differences are statistically
significant.
Source: Powys Children and Young Peoples Partnership, using data from Careers Wales
Community Wellbeing A higher proportion of Powys residents (83%) report that they feel they belong to their local area
when compared to the Welsh average (76%). However this is less in Newtown (76%) and
Llandrindod (59%) and also amongst residents with a disability (80%).
In 2012, the number of people killed or who were casualties in serious road accident was higher in
Powys compared with Wales (Powys = 91 per 100,000 population and Wales = 34 per 100,000
population). However, in relation to the length of road network, Powys experiences fewer numbers
of accidents per 100km of road than any other authority in Wales. Powys has the lowest number of
accidents (7.3 per 100km) and casualties (10.8 per 100km) compared to 56.1 accidents and 72.9
casualties in Cardiff.
Powys is the second most expensive place to buy a house in Wales. Residential property in Powys
costs 8.7 times the median annual gross pay for a full time job in Powys, which is higher than Wales,
where prices are 6.4 times annual pay, making housing in Powys less affordable. Results from a
0.4
0.8
2.7
3.7
0%
1%
2%
3%
4%
5%
6%
7%
8%
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Perc
en
tag
e
% of Year 11 leavers not in education, employment or training
Powys - Noresponse to surveyWales - Noresponse to surveyPowys
Wales
Figure 22: School Leavers in Powys were not in Education, Employment or Training

Page 44 of 230
resident survey show that there a considerable concerns amongst Powys residents about the lack of
affordable housing in the County.
Housing quality in Powys is worse than Wales, with 24 of the 75 Electoral Divisions among the worst
20% of areas for housing quality in the Welsh Index of Multiple Deprivation 2000. A survey
commissioned by Powys County Council in 2004 concluded that only one in a thousand private
sector dwellings would meet the Welsh Housing Quality Standard if it were applicable to private
housing stock.
Homelessness is a growing problem, with the number of homeless households accommodated
temporarily by Powys County Council rising from 125 in Quarter 1 2009-10 to 160 in Quarter 1 2012-
13. Over the same period, the annual total of those accepted as homeless increased from 190 to
260, representing a 37% increase.
Health Inequalities In order to have a better understanding of health inequalities, a health inequalities action plan is
being developed. This includes working with Public Health Wales Observatory to review progress
against three health inequalities targets:
By 2020, to improve healthy life expectancy for everyone and to close the gap between each
quintile of deprivation by an average of 2.5%
The population of Powys experiences the highest life expectancy at birth in Wales, as well as
experience better health outcomes e.g. lower levels of premature mortality compared with the
Wales average. However, inequities in health outcomes remain. Figure 23 shows the difference in
life expectancy, healthy life expectancy and disability free life expectancy between the most and the
least deprived fifths of the Powys population (inequality gap) over two time periods. The greatest
inequality gap is seen for healthy life expectancy for females, where females in the least deprived
fifth of the Powys population experienced a 13.6 years greater healthy life expectancy compared
with most deprived fifth of the population.
63.3
62.8
67.5
66.7
82.7
81.2
62.5
61.6
67.7
66.7
79.1
77.5 6.0
5.5
6.4
5.9
7.1
6.3
5.7
4.9
13.7
13.6
9.6
9.3
2001-05 2005-09
Life expectancy
Healthy life
expectancy
Disability-free life
expectancy
Life expectancy
Healthy life
expectancy
Disability-free life
expectancy
Males
Females
Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD/WHS (WG)
Life expectancy with 95%
confidence intervalInequality gap
(SII in years)
Comparison of life expectancy, healthy life expectancy and disability-free life
expectancy at birth, Powys THB 2001-05 and 2005-09
62.5
62.1
65.9
65.4
81.7
80.6
59.8
59.2
63.7
63.0
76.9
75.9 12.9
12.8
22.5
22.7
17.2
17.1
8.8
10.0
21.0
22.0
12.312.9
2001-05 2005-09
Life
expectancy
Healthylife
expectancy
Disability-free life
expectancy
Life
expectancy
Healthylife
expectancy
Disability-free life
expectancy
Males
Females
Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD/WHS (WG)
95% confidence interval
Inequalitygap (SII in years)
Comparison of life expectancy, healthy life expectancy and disability-free
life expectancy at birth, Cardiff 2001-05 and 2005-09
62.5
66.1
81.0
61.5
64.7
77.3
62.0
65.5
79.9
60.8
63.9
75.9
0 10 20 30 40 50 60 70 80 90
Disability-free life expectancy
Healthy life expectancy
Life expectancy
Disability-free life expectancy
Healthy life expectancy
Life expectancy
2001-05 2005-09
Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD 2008 (WAG)
Comparison of life expectancy, healthy life expectancy and disability-free life expectancy
at birth, Wrexham 2001-05 and 2005-09
Females
Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD/WHS(WG)
Males
Source: Public Health Wales Observatory
Figure 23: Life Expectancy in Powys

Page 45 of 230
Life expectancy for those aged over 65 years is higher in Powys compared with Wales. Life
expectancy for men at aged 65 years is 19 years, compared with 17.7 years for Wales. For females,
life expectancy at age 65 years is 21.6 years in Powys, compared with 20.3 years for Wales.
To reduce the number of babies born under 2500g
The proportion of babies in Powys born with a low birth weight has not changed significantly
between 2004 and 2013 (figure 24). In 2013, 4.8% of babies in Powys had a low birth weight which is
not statistically significantly different from Wales (5.4%).
Source:
Produced by Public Health Wales Observatory, using NCCHD (NWIS)
Figure 25 highlights the variation in low birth weight babies born by Middle Super Output Area in
Powys over a 10 year period (2003 to 2012). The numbers in brackets indicate the number of Middle
Super Output Areas that fall into each of the five low birth weight ranges. Llandrindod and Newtown
have the highest proportion of low birth weight (between 6.2% and 7.0%), although the map does
not show if these areas are significantly different to rates for Powys.
95% confidence interval
0
1
2
3
4
5
6
7
8
9
10
11
12
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Powys THB Wales
Percentage of singleton live births with a low birth weight (less than 2500g), Powys tHB
and Wales, 2004-2013
Produced by Public Health Wales Observatory, using NCCHD (NWIS)
Perc
en
tage (
%) o
f sin
gle
ton
liv
e b
irth
s
Figure 24: Percentage Low Birth Rates 2004-13
Percentage of Singleton live births with a low birth rate (less
than 2500g), Powys THB and Wales, 2004-13
Figure 25: Low birth weight by Middle Super Output Area in Powys, 2003-2012

Page 46 of 230
To improve the dental health of 5 and 12 year olds in most deprived quintile to that found in the
middle quintile of deprivation.
The sum of decayed, missing and filled teeth (dmft) in five year olds and Decayed, Missing and Filled
teeth (D3MFT) in 12 year olds is a measure of the decay experienced by the average child. It is
therefore the burden of disease which theoretically could have been prevented and is therefore key
data for evaluation of efforts to prevent decay. In Powys, the average dmft for five year olds
improved from 1.6 in 2007/08 to 1.3 in 2011/12, although this is not a statistically significant
reduction.
The average D3MFT for 12 year olds in Wales has reduced significantly from 1.1 to 0.6 in Powys
between the 2004/05 and 2012/13.
Active decay is measured by the number of decayed teeth that children have. Between 2007/08 and
2011/12, there was a reduction in the average decayed teeth in five year olds in Powys from 1.2 to
0.9, although this change was not statistically significant. Between 2004/05 and 2012/13, there was
no statistically significant reduction in the average decayed teeth (D3T) in 12 year old children in
Powys
Inequalities in mortality in Powys There is a significant gap in mortality from all causes for males under 75 years between the most and
least deprived fifth of the Powys population. The gap for females is not statistically significant.
Figure 26: Mortality from all Causes for Males and Females under 75 Years in Powys
There is a statistically significant gap in mortality from all causes, all ages between the most and
least deprived fifth of the Powys population, for both males and females.
1.5 1.7 1.8 1.9 1.9 1.7 1.60
100
200
300
400
500
600
700
2001-03 2002-04 2003-05 2004-06 2005-07 2006-08 2007-09
Most deprived within Powys Wales EASR
Least deprived within Powys Powys overall
Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD 2008 (WAG)
All-cause mortality, under 75, males, European age-standardised rate (EASR) per
100,000, Powys THB and Wales, 2001-09
Rate Ratio - most deprived divided by least deprived
1.4 1.6 1.9 2.0 1.5 1.4 1.20
50
100
150
200
250
300
350
400
450
500
2001-03 2002-04 2003-05 2004-06 2005-07 2006-08 2007-09
Most deprived within Powys Wales EASR
Least deprived within Powys Powys overall
Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD 2008 (WAG)
All-cause mortality, under 75, females, European age-standardised rate (EASR)
per 100,000, Powys THB and Wales, 2001-09
Rate Ratio - most deprived divided by least deprived

Page 47 of 230
Figure 27: All Cause Mortality, all Ages for Males and Females in Powys
There are also statistically significant gaps for both males and females between the most and least
deprived quintiles of deprivation for the following indicators:
Life expectancy at birth;
Mortality from circulatory disease;
Mortality from respiratory disease.
There is no significant difference in mortality rates from cancer (excluding skin) for males and
females between the least and most deprived quintiles. However, the mortality rate for males has
not fallen between 2001-03 and 2007-09. There has been a significant reduction in mortality for
females over this time period (figure 12).
Figure 28: Mortality from Cancers for all Ages, Males and Females in Powys
Comparing mortality rates with other areas The Local Authority peer group mortality comparison tool (Public Health Wales Observatory)
compares all cause age standardised and age specific mortality rates for Welsh local authorities with
the equivalent rates with alike Local Authorities in the UK.
Comparing all-cause mortality for all ages for Powys and other “Coastal and Countryside” Local
Authorities shows that:
Powys is statistically significantly lower than the all Wales rate for both males (559/100,000 in
Powys compared to 666/100,000 for all Wales) and females (442/100,000 in Powys compared to
485/100,000 for all Wales)
1.4 1.4 1.5 1.6 1.6 1.5 1.40
200
400
600
800
1000
1200
2001-03 2002-04 2003-05 2004-06 2005-07 2006-08 2007-09
Most deprived within Powys Wales EASR
Least deprived within Powys Powys overall
Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD 2008 (WAG)
All-cause mortality, all ages, males, European age-standardised rate (EASR) per
100,000, Powys THB and Wales, 2001-09
Rate Ratio - most deprived divided by least deprived
1.6 1.6 1.7 1.8 1.6 1.6 1.40
100
200
300
400
500
600
700
800
900
2001-03 2002-04 2003-05 2004-06 2005-07 2006-08 2007-09
Most deprived within Powys Wales EASR
Least deprived within Powys Powys overall
Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD 2008 (WAG)
All-cause mortality, all ages, females, European age-standardised rate (EASR) per
100,000, Powys THB and Wales, 2001-09
Rate Ratio - most deprived divided by least deprived
1.1 1.1 1.2 1.3 1.3 1.1 1.10
50
100
150
200
250
300
2001-03 2002-04 2003-05 2004-06 2005-07 2006-08 2007-09
Most deprived within Powys Wales EASR
Least deprived within Powys Powys overall
Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD 2008 (WAG)
Mortality from cancers (excl. other skin), all ages, males, European age-
standardised rate (EASR) per 100,000, Powys THB and Wales, 2001-09
Rate Ratio - most deprived divided by least deprived
1.0 1.2 1.3 1.3 1.2 1.2 1.00
50
100
150
200
250
2001-03 2002-04 2003-05 2004-06 2005-07 2006-08 2007-09
Most deprived within Powys Wales EASR
Least deprived within Powys Powys overall
Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD 2008 (WAG)
Mortality from cancers (excl. other skin), all ages, females, European age-
standardised rate (EASR) per 100,000, Powys THB and Wales, 2001-09
Rate Ratio - most deprived divided by least deprived

Page 48 of 230
Powys male, age specific, all causes, crude mortality rates are significantly higher than the
equivalent rates in the best five in peer group in 10-14 and 70-74 age groups. In females, rates
are significantly higher than the equivalent rates in the best five in peer group in 65-69 and 20-24
age groups (figure 29)
Figure 29: Age Specific Mortality Rates in Powys Compared with “Coastal and Countryside” Local Authorities
Lifestyle A greater proportion of adults in Powys engage in healthy behaviours compared with Wales, as seen
in the table below. However, these difference may not be statistically significant.
Table 5: Healthy Behaviours in Adults
Source: Welsh Health Survey, 2012 and 2013 (Welsh Government)
In addition, Powys residents aged over 65 years are also more engaged in healthy behaviours
compared with older people across Wales.
Table 6: Healthy Behaviours in Adults Aged over 65
Source: Welsh Health Survey, 2008-2010 (Welsh Government)
0 10 20 30 40 50 60
00-01
01-04
05-09
10-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
Age-specific rate per 1,000 with 95% confidence intervals
Powys Best 5 in peer group combined
All cause mortality & excess deaths, males under 75, Powys, Coastal and Countryside local
authorities group, 2012
Produced by Public Health Wales Observatory using ONS, NISRA & GROS data
Excess deaths
-16
-13
5
2
3
6
-3
0
0
-1
1
1
1
1
2
30
(red & green = statistical significance)
0 5 10 15 20 25 30 35 40
00-01
01-04
05-09
10-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
Age-specific rate per 1,000 with 95% confidence intervals
Powys Best 5 in peer group combined
All cause mortality & excess deaths, females under 75, Powys, Coastal and Countryside local
authorities group, 2012
Produced by Public Health Wales Observatory using ONS, NISRA & GROS data
Excess deaths
12
13
8
7
0
4
-3
0
0
2
0
3
0
0
0
0
(red & green = statistical significance)
Healthy Behaviours in Adults (2012-13) (Age standardised) Powys Wales
Adults who report being a current smoker 19% 22%
Adults who reported drinking above guidelines on at least one day in the previous week
40% 42%
Adults who reported eating 5 or more portions of fruit and vegetables the previous day
37% 33%
Adults who reported being physically active on 5 or more days in the past week
35% 29%
Adults who were overweight or obese 57% 59%
Healthy Behaviours in Adults Aged Over 65 (2008-10) Powys Wales
Adults who report being a daily or occasional smoker 10% 12%
Adults who reported drinking above guidelines on at least one day in the previous week
23% 24%
Adults who reported eating 5 or more portions of fruit and vegetables the previous day
41% 36%
Adults who reported meeting physical activity guidelines in the past week
19% 16%
Adults who were overweight or obese 59% 59%

Page 49 of 230
However, there still remains a significant challenge in further improving health behaviours in order
to reduce the burden of chronic diseases in Powys and reduce demand on the health and social care
system.
Health Status Powys has a lower teenage conception rate (19.1 conceptions per 1,000 females aged under 18
years) compared with Wales (30.8 per 1,000 females aged under 18 years).
Childhood immunisation uptake rates have increased over recent years and are now similar to
Wales’ rates, except for measles, mumps and rubella immunisation uptake in teenagers, which is
below Wales’ levels and below target levels.
A lower proportion of the Powys adult population report being treated for any illness compared with
Wales. Overall, Powys residents also report better health.
Table 7: Reported Health Status in Adults
Source: Welsh Health Survey, 2012- 2013 (Welsh Government)
A smaller proportion of adults in Powys report being treated for various long term conditions
compared with adults across Wales.
Table 8: Reported Key Illnesses in Adults
Source: Welsh Health Survey, 2012-2013 (Welsh Government)
Flu immunisation uptake rates are increasing in people with long term health conditions (49.5% in
2013-14) and are similar to Wales’ rates (51.1%), although they remain below target levels (75%).
The table below shows how Powys residents aged over 65 years report better quality of life
compared with older adults in Wales.
Table 9: Quality of Life Indicators - Aged 65 and Over
Source: Welsh Health Survey, 2008-10 (Welsh Government)
Adults Who Reported Health Status (2012-13) (Age Standardised) Powys Wales
Currently being treated for any illness 46% 50%
Limited by health problems / disability a lot 14% 16%
Limited by health problems / disability at all 31% 34%
General health status fair or poor 18% 20%
SF-36 Physical component summary score 49.3 48.5
SF-36 Mental component summary score 51.1 49.6
Adults Who Reported Key Illnesses (2012-13) (Age Standardised) Powys Wales
High blood pressure 17% 21%
Ay heart condition excluding high blood pressure 8% 9%
Any respiratory illness 12% 14%
Any mental illness 8% 12%
Arthritis 10% 12%
Diabetes 5% 7%
Any illness 46% 50%
Quality of Life Indicators (observed) for Persons Aged 65 and Over (2008-10)
Powys Wales
General health status: fair or poor 37% 40%
Limiting long term illness 49% 56%
SF-36 Physical component score 41 39
SF-36 Mental component summary score 53 51

Page 50 of 230
The table below provides a breakdown of Powys residents aged over 65 years who report being
treated for specific long term conditions. Overall, older Powys residents are less likely to be treated
for a long term condition.
Table 10: Selected Conditions Observed in Persons Aged 65 and Over
Source: Welsh Health Survey, 2008-10 (Welsh Government)
However, the increase in the proportion of older people living in Powys means that the number of
people with long term conditions such as diabetes will increase. There will also be an increase in the
number of people with dementia - it is estimated that whilst the number of people in Powys aged
over 65 years with dementia was 2,225 in 2011, this is likely to rise to 4,256 in 2030.
Powys has 16,154 carers, an increase of 14% from 2001, when there were estimated to be 14,118
carers in Powys. This is of particular significance as unpaid carers, usually family members,
contribute significantly to maintaining individuals with complex needs due to long term physical or
mental ill health, disability or old age in the community. The health and wellbeing of carers is
affected by their caring responsibilities, as many may experience ill health, poverty and problems
accessing employment.
4.4. HEALTH SERVICE UTILISATION
Powys adults report using health services less than adults across Wales, except for dental services.
The table below summarises health service usage for Powys residents compared with Wales.
Table 11: Health Service Use for Adults
Source: Welsh Health Survey, 2012 and 2013 (Welsh Government)
Understanding Localities / GP Clusters in Powys GP Cluster Profiles produced by Public Health Wales Observatory (2013) provide an overview of
demographics and burden of chronic disease at local level. Of note:
The three GP Clusters have similar age / sex profiles compared with Powys overall
Selected Conditions (observed) in Persons Aged 65 and Over (2008-10)
Powys Wales
High blood pressure 50% 51%
Heart condition 25% 29%
Respiratory condition 17% 22%
COPD 5% 7%
Mental Illness 8% 10%
Arthritis 27% 33%
Diabetes 14% 15%
Health Service Use for Adults (aged 16+) 2012-13 (Age Standardised)
Powys Wales
GP in the past 2 weeks 15% 17%
Attended casualty in the past 12 months 14% 17%
In hospital as an inpatient in the past 12 months 7% 9%
Attended outpatients in the past 12 months 31% 32%
Saw a pharmacist in the past 12 months 65% 70%
Attended a dentist in the past 12 months 77% 70%
Attended an optician in the past 12 months 49% 50%

Page 51 of 230
South Powys has the greatest proportion of patients (5.3%, 2,370 patients) who are in the most
deprived quintile of deprivation. Mid and north Powys have no patients who are living in the
least deprived quintile.
22.6% of patients in North Powys, 21.9% of patients in Mid Powys and 11.9% of patients in South
Powys have a drive time of over 15 minutes to their registered main GP Practice.
Figures 30 to 32 show the recorded burdens of chronic disease for the three GP clusters in Powys.
These tables show the observed prevalence (thereby providing a guide to the actual burden of
disease in Powys) and adjusted recorded burden of disease (providing an indication of whether the
cluster is higher or lower than other clusters in Powys and Wales).
North Powys All indicators (except asthma) in the North Powys cluster have an adjusted prevalence in the lower
quartile compared with clusters across Wales.
Mid Powys All indicators (except epilepsy and heart failure) in the Mid Powys cluster have an adjusted
prevalence in the lower quartile compared with clusters across Wales.
Health
Board
Wales
count % min % max % % %
Hypertension 8,860 15.4 15.4 17.9 16.6 15.3
Asthma 3,710 6.4 6.3 6.6 6.5 6.7
Diabetes 2,710 4.7 4.7 5.6 5.1 5.2
CHD 2,320 4.0 4.0 4.1 4.1 4.0
COPD 1,160 2.0 2.0 2.2 2.1 2.1
Epilepsy 390 0.7 0.6 0.7 0.7 0.7
Heart Failure 450 0.8 0.8 1.3 1.0 0.9
Produced by Public Health Wales Observatory, using Audit+ (NWIS)
Indicator
Your Cluster:Other Clusters in
your Health Board:
Middle
50%
Lowest
25%
Highest
25%
Recorded burden of disease Adjusted recorded burden of disease
Your Cluster
Other Clusters: in your Health Board
in other Health Boards
Figure 30: Burden of Chronic Disease - North Powys GP Cluster

Page 52 of 230
Figure 31: Burden of Chronic Disease - Mid Powys GP Cluster
South Powys All indicators (except asthma, heart failure and hypertension) in the South Powys cluster have an
adjusted prevalence in the lower quartile compared with clusters across Wales.
4.5. FOCUSING ON OUTCOMES
To ensure that Powys THB is making progress towards improving population health, it is important
to have an understanding of key health outcomes across domains. The table below shows
population level indicators that can be used for this purpose.
Health
Board
Wales
count % min % max % % %
Hypertension 4,790 16.9 15.4 17.9 16.6 15.3
Asthma 1,790 6.3 6.3 6.6 6.5 6.7
Diabetes 1,500 5.3 4.7 5.6 5.1 5.2
CHD 1,150 4.0 4.0 4.1 4.1 4.0
COPD 610 2.1 2.0 2.2 2.1 2.1
Epilepsy 210 0.7 0.6 0.7 0.7 0.7
Heart Failure 320 1.1 0.8 1.3 1.0 0.9
Produced by Public Health Wales Observatory, using Audit+ (NWIS)
Indicator
Your Cluster:Other Clusters in
your Health Board:
Middle
50%
Lowest
25%
Highest
25%
Recorded burden of disease Adjusted recorded burden of disease
Your Cluster
Other Clusters: in your Health Board
in other Health Boards
Health
Board
Wales
count % min % max % % %
Hypertension 8,110 17.9 15.4 17.9 16.6 15.3
Asthma 2,990 6.6 6.3 6.6 6.5 6.7
Diabetes 2,550 5.6 4.7 5.6 5.1 5.2
CHD 1,880 4.1 4.0 4.1 4.1 4.0
COPD 980 2.2 2.0 2.2 2.1 2.1
Epilepsy 270 0.6 0.6 0.7 0.7 0.7
Heart Failure 570 1.3 0.8 1.3 1.0 0.9
Produced by Public Health Wales Observatory, using Audit+ (NWIS)
Indicator
Your Cluster:Other Clusters in
your Health Board:
Middle
50%
Lowest
25%
Highest
25%
Recorded burden of disease Adjusted recorded burden of disease
Your Cluster
Other Clusters: in your Health Board
in other Health Boards
Figure 32: Burden of Chronic Disease - South Powys GP Cluster

Page 53 of 230
Table 12: Population Level Indicators of Key Health Outcomes
Indicators Powys Wales
Staying healthy
Healthy and active long
life
Life expectancy at age 65 (2008-10) Females 21.6yrs
Males 19.0yrs
Females 20.3yrs
Males 17.7yrs
Adults reporting general health as
poor or fair (2013) 19% 20%
Adults reporting any limitation in
their daily activities due to a health
problem or disability (2013)
34% 33%
Children have a good
healthy start in life
Percentage of children reaching,
exceeding or within one age band
below developmental norm at 3
years (2013/14)
74% 82%
Percentage of reception class
children (aged 4/5) classified as
overweight or obese (2011/12)
29.2% 28.2%
Percentage of live births with a birth
weight of less than 2500g (2004-11) 5.2% 5.4%
Safe Care
safe and protected from
avoidable harm through
appropriate care,
treatment and support
Suicide rate per 100,000 (2010/11)
13.62 10.18
Effective Care
receive the right care
and support to either
improve or manage my
own health and
wellbeing
Circulatory disease mortality rate
under 75 years per 100,000 (2011)
Females 111.18
Males 160.06
Female 122.33
Males 196.55
Respiratory disease mortality rate
under 75 years per 100,000 (2011)
Females 44.16
Males 51.11
Females 63.64
Males 85.74
Percentage of GP patients on the
diabetes register (2012) 5.1% 5.2%
Percentage of 5 year olds with
decayed teeth (2005/6) 46.4% 47.7%
Timely Care
To ensure the best
possible outcome, my
condition is diagnosed
early and treated in
accordance with clinical
need
One & five year relative survival
rates reported for all cancers
(excluding non melanoma skin
cancer)
1 year (2007-11)
Females 73.3%
Males 71.1%
5 year (2003-7)
Females 60.2%
Males 52.3%
1 year (2007-11)
Females 71.5%
Males 68.5%
5 year (2003-7)
Females 55.0%
Males 50.0%
Individual Care
Inequalities that may
prevent me from leading
a healthy life are
reduced
The gap in life expectancy between
the least and most deprived
(2005/9)
Females 4.9 yrs
Males 5.5 yrs
Females 7.1 yrs
Males 9.2 yrs
Sources: Public Health Wales Observatory, Health Maps Wales & Welsh Health Survey

Page 54 of 230
Using Data and Health Intelligence to Best Effect in Powys In addition to locally developed intelligence, data and health intelligence from other sources, for
example from Public Health Wales Observatory or Welsh Government Statistics and Research, is
used in Powys to increase local understanding of health needs and influence local service planning
and delivery. Examples of relevant data that has been produced and how it has been “actioned”
locally are highlighted below.
Table 13: Local Health Intelligence Data and Actions
Health Intelligence / Data Source Examples of Local actions
Health of Children and
Young People in Wales
Public Health
Wales
Observatory
Used as part of the Director of Public Health Annual
Report 2013/14.
Cascaded through the Children and Young People’s
Partnership
Atlas of Variation in
Elective Surgical
Procedures
Public Health
Wales
Observatory
Data has been used to better understand Powys THB
activity, benchmarking with other Health Boards and
Local Authority Areas.
Welsh Health Survey
obesity web resource
Public Health
Wales
Observatory
Intelligence used to inform local healthy weights strategy.
Quality and Outcomes
Framework: Atrial
Fibrillation and
Hypertension
Public Health
Wales
Observatory
Used by localities and Primary Care directorate with GP
Clusters. Informed Heart Disease Delivery Plan.
Local authority mortality
comparison tool
Public Health
Wales
Observatory
Shared with Local Authority and Localities.
Alcohol and Health in
Wales
Public Health
Wales
Observatory
For action through the Powys Area Planning Board.
Welsh Health Survey 2012-
13
Welsh
Government
Used to inform prevention and health improvement
strategies. Shared with Local Authority.
Local Area Summary
Statistics
Welsh
Government Used to understand socioeconomic profile in Powys.
The data and health intelligence summarised in this section has informed our plan and the Joint
Strategic Needs Assessment (JSNA) developed by Local Service Board partner organisations was used
as the basis for deciding joint priorities and led to the development of the One Powys Plan.

Page 55 of 230
5. STRATEGIC APPROACH TO
TRANSFORMATION
The focus and direction of the Powys Integrated Medium Term Plan (IMTP) is determined by a range
of drivers which brings together national policy, local needs and the need to comply with statutory
requirements for organisational delivery.
5.1. NATIONAL POLICY DRIVERS
The Welsh Government Strategy ‘Together for Health’ (2012) and its 19 supporting delivery plans
which are cross-referenced as appropriate throughout this document ;
The Welsh Government Prudent Healthcare principles (2012);
The Primary Care Plan (2014) and Integrated Services for Older People Plan (2001);
The themes emerging from the development of the single integrated plan for Powys (2013), the
Powys One Plan: Yn Un (2011);
The Welsh Government Outcomes Framework (2014).
Learning from reviews of external organisations, specifically the Report of the Francis inquiry into
the Mid-Staffordshire NHS Trust (2013), the Joint Wales Audit Office and Healthcare Inspectorate
Wales (HIW) review into the governance arrangements at Betsi Cadwaladr Health Board (2013)
and the ‘Trusted to Care’ Andrews Report and the ‘Gifts of Complaint’ Report (2014);
The Mid-Wales Study (2014);
Clinical and service strategies of neighbouring Health Boards and NHS Trusts: South Wales
Collaborative;
Annual self-assessment against the Standards for Health Services;
Improvements required as set out within the THB’s Annual Quality Statement;
Setting the challenge of meeting efficiency and effectiveness targets benchmarked against other
organisations, including the review of the organisation’s finances by Deloitte, commissioned by
the Health Board (2013);
The Demand and Capacity Report commissioned by the Health Board and received in December
2014;
The Director of Public Health’s Annual Report (2014);
Public Health Wales supports Health Boards in delivering a number of local priorities plan;
Working Differently, Working Together, the workforce and OD framework that supports
Together for Health (2012).
Commission on Public Service Governance and Delivery (2014) (Williams Commission);
Devolution, Democracy and Delivery Welsh Government (2014).
Primary Care Strategy (Welsh Government (2014).
Social Services and Wellbeing Act (2014).
Wellbeing of Future Generations Bill (2014).

Page 56 of 230
5.2. STRATEGIC DIRECTION
This plan sets out the THB’s approach to planning and delivery of services for the residents of Powys
for the three year period 2015-18. The plan is designed around the vision set out by the Board to
deliver “truly integrated care centred on the needs of the individual” through six inter-related
values:
Improving Health and Wellbeing Our approach to improving health and well-being is to work with our partners, particularly through
the Local Service Board (LSB), to develop the capacity in the community and across agencies to
improve health now and lay the foundations for maintaining good health for the future. It
recognises that all of our communities are individual; in their nature, and our response to improving
health will reflect both nationally driven programmes for health improvement, while allowing room
to recognise local difference, and reduce inequality in experience of health and health outcomes.
A neighbourhood management approach led through the LSB will promote and enable greater
ownership of health behaviours by communities. The priorities of the LSB is contained within the
One Powys Plan and this work is underpinned by a Joint Strategic Needs Assessment (JSNA), with
focus on actions that have the greatest impact on improving health and wellbeing and reducing
health inequity. Every member of staff has a part to play in taking opportunities to improve the
health and wellbeing of the population.
Ensuring the Right Access The THB is responsible for securing safe and high quality health services for the residents of Powys
and achieves this through commissioning services across care pathways from primary care
contractors, directly managed services and securing services from neighbouring LHBs and NHS Trusts
and other care providers. Ensuring access to coordinated care through partnership working with
Powys County Council is key. A primary care and clinically led approach to commissioning across the
health system is central to driving improvements in the quality of the patient experience of care and
delivering a sustainable health system.
“…truly integrated care centred on the individual.”
Making Every
Pound Count
Involving the
People of Powys
Improving Health & Wellbeing
Ensuring
the Right
Access
Striving for
Excellence
…and always
with our staff …and always
with our staff
Figure 33: PTHB Vision

Page 57 of 230
Striving for Excellence The public must have confidence in the excellence of the services provided by its NHS. The THB will
be relentlessly concerned with high quality care and believes it to be of paramount importance for
patients and their carers to be treated with dignity, respect and compassion whilst in our care or in
the care of services we fund. Staff need to be developed to take responsibility for improving
standards and practice and to make the best use of resources. Local and devolved management has
brought increasing control over local working environments, contributing to practical improvements
and the satisfaction of seeing clearer benefits for patients. In publishing our Annual Quality
Statement, the THB will routinely assess and inform the public about how well we are doing across
all of our services, including areas that need to improve. The opportunities for the THB to lead and
contribute to research and development will also be supported, giving definition and direction to the
‘teaching’ status of the Health Board.
Involving the People of Powys Maintaining confidence in local services and enabling service change requires the THB to
continuously engage with local communities in respect of the service, quality and financial
challenges that the THB faces. Transparency in the service delivery, quality and financial
performance of the organisation will enable a greater understanding of the challenges Powys faces
in meeting the needs of a rural population. In return the THB will look to the people of Powys to use
that information and those services well and appropriately, and to take more responsibility for
themselves and those around them. Our staff are key local advocates for the THB and are central to
helping deliver the message of positive change, and there are many opportunities for partnership
working to gain a shared public sector perspective across Powys.
Making Every Pound Count The NHS in Wales is facing an unprecedented financial challenge in meeting the health needs of the
population in an environment of zero growth funding. To meet this financial challenge, Powys THB
recognises that general year on year efficiencies will be insufficient to enable a sustainable financial
footing over coming years. Under these conditions, the financial strategy has to be founded on re-
engineering the way services are designed and delivered in order to reduce cost. We are embarking
on an ambitious Transformation Programme during 2015 to engage the public on the future design
of services for our population.
Always with our staff The Health Board will only be able to deliver its strategic direction with our staff. Our staff have the
skill, ambition and drive to deliver the vision of services for the population of Powys. We will
continue to engage, support and develop the skills and knowledge of our workforce, our ambition
being, to be the employer of choice.
5.3. STRATEGIC FRAMEWORK
In Powys, Primary Care and Community Health services have evolved over many years and although
they have served the local population well, the current arrangements are unplanned and to an
extent have not responded to changes in population demand. As a consequence the current service
provision is inequitable and its resilience needs to be strengthened across the County.
The THB has agreed a strategic approach which will provide a framework for the delivery of future
services across Powys over the next 10 years. The focus of the THB will be to achieve all national
priorities, improve access to services delivered in primary care and in the community, develop

Page 58 of 230
partnership working, and expand patient and public engagement, whilst maintaining financial
balance. The approach will be designed and delivered through the THB’s Transformation
Programme which has been underpinned by a substantial and independent Capacity and Demand
Modelling exercise that was completed in December 2014.
Despite investment in resources to change clinical practice and repatriate services, the pressures
remain enormous on all health and social care services as volumes of activity have risen
substantially, particularly in the acute sector. The level of this demand continues to place very
severe pressure on the capacity and capability of local providers, and presents the THB with
significant commissioning challenges.
The THB will focus on strengthening its commissioning function to manage demand and to increase
productivity of acute and specialist services but this will only be possible through substantially
increasing the range of services available within Primary Care, Social Care and Community Health
Service.
5.4. DEMAND, CAPACITY AND FINANCIAL MODELLING
The demand, capacity and financial modelling project was commissioned in April 2014 and involved
an independent strategic Demand, Capacity and Financial Modelling exercise with Strategic
Healthcare Planning LLP. The process was clinically led via the establishment of a Clinical Reference
Group and two stakeholder events which involved clinical and operational teams from within the
organisation and our external provider organisations and Primary Care clinical leaders. The process
also involved regular input from the Executive Team.
The modelling work is based on a number of assumptions which have been applied to our 12/13
dataset. This identified the impact of future demand on both our commissioner and provider
functions. This has helped us to understand strategically the potential impact of future demand on
our services over a 5 and 10 year horizon, and the potential intervention opportunities which are
based on an evidence base of best practice and which have been validated through our Clinical
Reference Group and our Stakeholder Group.
The modelling work reviewed both the scale of demand and cost increases as well as potential
solutions to reduce costs. Over the next 5 years, the Health Board has modelled that:
In doing nothing, costs will increase by between £20 – £25M with the assumption that there
would be no corresponding funding increases from Welsh Government.
£4.8M intervention opportunities identified in the modelling which produces a net increase of
£1.9M on top of our previous financial planning assumptions. These will be pursued through the
3-5 year service reform programme which will broadly focus on delivering efficiency through new
models of care. We currently assume that this will be delivered at minimal additional
infrastructure costs although this has yet to be validated through the service modelling process.
Further opportunities of £4.6M could be pursued through service reconfiguration of our
community hospital services and repatriation agenda but would require investment in skills and
capacity of £2.240M to deliver over the coming 3 years.
The Health Board’s Transformation Programme Board approved the extension of the demand and
capacity modelling project in December 14 to undertake further work to understand the potential
intervention opportunities. This includes further increasing our repatriation of services within Powys

Page 59 of 230
through increasing our efficiency and developing new models of care. These interventions will
reduce our reliance on secondary care and consider how we invest in technology to support people
independently and access specialist resource remotely. Further work will include working with
primary care clinical leadership, partners and stakeholders through managed engagement and the
continuation of the Clinical Reference Group, agreeing priorities to improve the patient experience
and clinical outcomes to help scope the Service Reform Programme. The key outputs of the
extended Demand and Capacity project will be:
A point prevalence study of all community hospital sites in Powys looking at the case mix within
hospitals and highlighting opportunities for alternative means of delivering care.
Report on comparative site visits to 2 comparable health economies outlining the ways in which
Powys can learn from examples of innovation and best practice to support the SDM and service
reform programmes.
Identify priorities for service reform over 3 years to deliver the £1.9M increased scope of cost
reductions opportunities through efficiency in alternative service models
Demand & capacity modelling report on 2013/14 data and operational process established for
continued modelling to support planning cycle.
Robust process in place for the development of short to medium term delivery plans aligned to
the strategic planning process and development of commissioning intentions.
An agreed Service Reform Programme brief.
5.5. TRANSFORMATION PROGRAMME
Powys Teaching Health Board has established a Transformation Programme; an internal programme
to the Health Board, focused on strengthening primary and community health services in Powys to
deliver sustainable services which provide value for money for our population and for future
generations. This will be delivered through co-production with our public, patients, staff and key
stakeholders, and through strengthening our partnership arrangements to deliver greater
sustainability in our provider organisation capacity and capability. The Transformation Programme
will be managed through four core programmes, which will:
Develop our strategic delivery model for how future services will be provided;
Strengthen our commissioning arrangements;
Reconfigure our provider organisation;
Bring adult mental health services management arrangements back into Powys.
These will be supported by the enabling programmes which are required to deliver new technology,
prepare and develop the organisation for change, engage with our key stakeholders and deliver a
robust investment plan to improve our estate.

Page 60 of 230
Figure 34: PTHB Transformation Programme Structure
The following high level benefits are anticipated to be delivered via the Transformation Programme.
Improved Patient Experience
Reduction in unnecessary hospital visits and time spent in hospital;
Improved health and well being of patients;
Patients empowered to self manage;
Deliver clinically viable and sustainable services
Robust strategic plan to develop future services;
Reduce unnecessary out of county referrals and admissions;
Improve direct access to diagnostics;
Reduce variation in referrals;
Improved staff experience
Sustainable workforce in place to support new models of care;
Staff empowered and motivated to change;
Programme and project management capacity and capability to deliver change;
Fit for Purpose Estate
Improve environment for patients and staff and utilisation of existing estate;
Move towards compliance of HBN and HTM via potential developments;
Reduce backlog maintenance and decommission redundant estate;
Improved effectiveness and clinical efficiency
Improve clinical outcomes;
Reduce length of stay, unnecessary visits to acute hospital, increase use of facilities;
Improve patient flow, reduce waste and variation in practice;
The future service model will require wider development of community-based alternatives to
hospital admission and greater emphasis on health promotion, social wellbeing and disease
prevention for both physical and mental ill health. This will support people in making lifestyle

Page 61 of 230
changes necessary to reduce future levels of chronic disease and ill health, and where appropriate
enable people to manage their own conditions. This model will require a more integrated multi-
disciplinary team approach with greater specialisation in the Primary Care workforce. Future
advances in technology and medicine will continue to drive an increase in the range of services that
can be provided safely from within the community; allowing more people to be diagnosed, treated
and cared for near or at home. This will result in a change in care pathways as more people will be
attended to by a specialist in local Primary Care and Community Health centres and other care
settings, reducing the need for referral into the acute hospital.
Transformation Outcomes - Shifting the Balance of Care The impact of the transformation programme is to shift the balance of integrated care to secure an
increased emphasis and shift of activity towards prevention, self-care, and primary and community
intervention, as illustrated in the diagram below:
Figure 35: Shifting the Balance of Care
Organisational Model An organisational model has been developed to re-organise service delivery to ensure that the
objectives within the strategic framework are delivered. The model aims to provide services as local
as possible for the population of Powys, refocusing current investment to support health and
wellbeing and the delivery of effective disease prevention services. The model focuses on integrating
general practices within locality and neighbourhood settings to deliver out of hospital activity.
However it recognises the different levels of demand for services, the need for staff specialisation,
critical mass and service economies to ensure high quality outcomes and therefore considers five
tiers of access for future service provision.
Home
Neighbourhood Population for Federated Primary Care Model/Linked with 7 X
LA neighbourhoods = 2,000 – 15,000
Locality Population 60,000 +
County Wide 130,000 +
Supra
County
Figure 36: Future Organisational Model: Five Tiers of Access

Page 62 of 230
The tiers of access are designed to offer a range of locally accessible services, providing increased
choice to the population of Powys. The acute services provided outside Powys will need to develop
links with the locality and neighbourhood services (i.e. GP practices, Primary Care Networks) to
provide seamless care for patients and to support staff training and specialisation or transfer of
appropriate skills and services to the community.
The locality and neighbourhood networks will have a strong emphasis on promoting self care,
disease prevention and early intervention; providing services which promote health, independence
and well being. These networks will bring together public services spanning health and social care
and will require joint focus with the local authority to improve other services which contribute
towards health and wellbeing such as housing standards, deprivation and levels of unemployment.
This is likely to result in a greater level of differentiation of Powys community hospitals, building on
the learning from Glan Irfon in Builth Wells. This will result in a network of diagnostic and treatment
hubs at locality level supported by integrated health and social care centres in neighbourhoods to
support the growing demand for care closer to home.
Strategic Delivery Model Programme The SDM programme over the next 3 years will enable the Health Board to develop a clinical service
strategy and appraise a number of strategic options around how best to configure our future
services to ensure future clinical viability for our local population and which address our key
challenges.
It is anticipated the duration of the delivery of the programme will be over a 5 -10 year horizon. The
programme will be clinically led and stakeholder and public engagement and co-production will be
central to this programme.
The SDM Programme will:
Reconfigure our Services
Undertake a robust process that develops and appraises options of how we can best configure
future services to meet demand in an affordable way.
Engage our public, patients and staff in reviewing existing services and appraising options to
ensure the best configuration of services for Powys for the foreseeable future.
Continue to utilise opportunities and strengthen our integrated working and governance
arrangements with the Local Authority and our other key partner organisations.
Improve patient experience and outcomes by improving access, developing new models of care
and repatriating services from external providers (based on a robust clinical case for change)
Work more creatively in addressing some of the key workforce challenges to support new
models of care locally within Powys.
Significantly Improve our Environment for Patients and Staff
Improve the work environment for staff.
Deliver an estate which is fit for purpose and release any redundant buildings.
Strengthen our Financial Position
Develop robust plans to ensure sustainable services for the foreseeable future.
Contribute towards a sustainable balanced financial position.
Contribution towards wider Organisational Objectives
This programme will help the Health Board address its 3 strategic challenges for the future:

Page 63 of 230
Designing and delivering a clinically and financially sustainable rural service model, to provide as
much care as local to home as possible
Meeting the changing needs of Powys residents as demographic change and improvements in
healthcare continue to make their impact on services
Working with partners and the public to support sustainable rural communities in a period of
public sector austerity.
SDM Programme Goals and Benefits
The high level goals of the programme are:
To agree the best models of care and configuration of services to deliver clinically viable and
economically sustainable services that meet the needs of the rural population of Powys.
Ensure the public, patients and staff are engaged and supportive of our future strategic delivery
model.
To prepare business cases to support proposed service and capital infrastructure changes.
To secure all necessary approvals and implement the proposed changes as part of the strategic
delivery model and preferred option.
The SDM Programme will also deliver significant non-financial benefits:
Improve the patient experience, quality of care and patient outcomes
Provide clinically viable services for the local population
Enable us to repatriate additional services more economically
Improve productivity and efficiency through configuration of services
Develop a sustainable infrastructure which is fit for purpose.
High Level Timetable
The following table highlights the key milestones for the SDM Programme.
Table 14: Strategic Delivery Model Programme High Level Timetable
Phase 1 Start Date End Date
Stage 0 Programme start up February15 September 15
Stage 1 Clinical Design November 15 August 16
Stage 2 Configuration of options March 16 September 17
Stage 3 Consultation on preferred option September 17 July 18
Stage 4 Strategic Outline Programme and Programme Closure September 17 October18
Current status of the Transformation Programme The current status of the programmes and projects under the Transformation programme is
provided below:
Adult Mental Health NHS Arrangements Project
After an extensive stakeholder engagement and option appraisal exercise, the case for returning the
majority of mental health services to the direct management of the Health Board was accepted by
the Board and a decision to engage and consult NHS adult mental health staff working in Powys
about being managed by PTHB was agreed at the February 15 PTHB Board Meeting
Strategic Delivery Model Programme
A programme mandate /investment case for the SDM has been prepared and approved by the
internal Transformation Programme Board and the PTHB Board on 19th March 15. Key aspects of the
work programme have begun.

Page 64 of 230
Service Reform Programme
The Service Reform programme is currently being established, a programme mandate is being
prepared for approval at the Transformation Programme Board in April with a view to establishing
the governance arrangements by May 15. This programme will be fully established by October 15.
Commissioning Programme
A review of our current commissioning arrangements was undertaken during 2014 and early 2015.
A programme brief is being prepared for approval at the Transformation Board in May 15 with a
view of implementing a commissioning development programme to strengthen our commissioning
arrangements including establishing strengthened leadership arrangements through the
establishment of a Commissioning Board and appointment of an Associate Director of
Commissioning.
Enabling Programme – Stakeholder Engagement
The stakeholder engagement enabling programme will be driven and resourced by the SDM
programme given the significant stakeholder engagement associated with the delivery of the SDM
programme.
Enabling Programme – Estates and Facilities
The estates and facilities enabling programme will be largely driven and partly resourced by the SDM
programme due to the dependency around the development of clinical service strategy and the
technical work required to support the configuration of the options and development of an estate
strategy and strategic outline case for future investment into the estate.
Enabling Programme -Organisational Development Programme
A programme mandate /investment case for the OD Programme has been prepared and approved
by the internal Transformation Programme Board. The investment case is approved by the Board as
part of the IMTP in March 15, with a view to establishing the programme by October 15.
Enabling Programme –Information/Information Technology
The Health Board has already established a joint IT strategy with Powys county council which sets
out the core deliverables to respond to existing local and national priorities. Further scoping work
will be undertaken during 2015 to assess the further IT and Information needs of the organisation in
order to support both the requirements of Strategic Change Programme process and to deliver the
resultant IT reliant service solutions within future service models. Governance arrangements will
also be reviewed to aid alignment to the aspects relevant to the Transformation Programme.
5.6. ORGANISATIONAL DEVELOPMENT
The Health Board intends to ensure that we have a flexible, skilled and motivated workforce ready to
support the effective delivery of quality services to our population. The Board has adopted an
organisational development approach to the maturing Health Board with the intention of building
capacity and capability from within to enable staff to continuously improve the quality of service
delivery and enhance performance.
Always with our Staff At the heart of the Health Board’s strategic vision in delivering “truly integrated care centred on the
individual” is staff engagement. “Always with our staff” is the sixth key principle within our vision. Our
staff contribute to the other 5 principles and organisational success by:

Page 65 of 230
- Providing care to improve the health and wellbeing of the population.
- Delivering care as close to home as possible and in a variety of settings to ensure the right
access.
- Developing themselves and contributing towards improving standards, practice and making
best use of resources in our quest of striving for excellence and making every pound count.
- Living and working in Powys. So as well as involving the people of Powys, in many cases our
staff are the people of Powys.
“Vision into Action, Success through Teams”2 Workforce and Organisational Development (OD) is an enabling programme to achieve the future service vision. The OD strategy “Vision into Action, Success through Teams” aims for Powys teaching Health Board to be recognised as:
an organisation that delivers exceptional care to the people of Powys
being a fantastic organisation to work in
This will be achieved by our staff gaining recognition for the things that they do and the way that they do it
achieving satisfaction in their work and feeling positive about working in the Health Board
feeling trusted to deliver exceptional care
Organisational Development is defined as a “planned and systematic approach to enabling sustained organisational performance through the involvement of its people” (Chartered Institute of Personnel and Development 2014). 3“Vision into Action, Success through Teams” aligns four key elements of:
“Strategy, People, Systems and Processes with Structure” to achieve sustained organisational performance and create a positive culture. Figure 37 shows
these four key components and the goals associated with each one.
Figure 37: Four Key Element of Organisational Performance
2 Powys Teaching Health Board (2015) “Vision into Action, Success through Teams” An Organisational Development (OD) Programme
Brief for the Transformation Programme Board. Powys teaching Health Board 3 Chartered Institute of Personnel and Development (CIPD) (2014) Organisational Development Factsheet. CIPD. April 2014
•That make sense and enable improvements
•Ways of working that work for patients
•Valued and engaged staff
•Vision with clarity and action
Strategy People
Systems and
Processes Structure

Page 66 of 230
1. Strategy
To define a strong vision for the Health Board that excites and challenges
Create clarity and common understanding of the organisation’s direction and strategy
2. People
To increase the level of staff engagement within the Health Board as measured through the Staff Survey.
To improve the health and wellbeing of our staff through the creation of a positive working environment and culture that produces a happy, motivated and high performing employee.
To develop our staff to meet the needs of the people in Powys through the delivery of high quality, patient led, innovative primary and community care services
3. Systems and Processes
Set clear, ambitious, measureable and achievable goals within the organisation that links the strategy to staff individual job roles
Embed Improving Quality Together and Team Based Working as the way which we do things in Powys.
To have systems and processes in place and joined up which make sense and enable staff to do their jobs to the best of their ability.
To fully realise the benefits from full deployment of electronic systems, in particular Electronic Staff Record (ESR) and ensure integration with other systems.
4. Structure
Create ways of working that promote collaboration within and outside of the Health Board.
Create ways of working that reduce the boundaries and barriers between and around services.
Review of the organisational structure to ensure that it enables the achievement of the strategic goals and enables new ways of working.
In achieving these goals, the THB will meet the Organisational Principles developed in March 14
(PTHB 2014)4 and exemplify the characteristics of a “teaching” organisation (PTHB2012)5
Organisational Principles “Teaching” Health Board Characteristics Putting patients, quality and safety at the core of everything
we do by maintaining and further developing locality based working;
Organisational models to provide sustainable, safe and effective solutions from both a clinical, safety and financial perspective;
Role clarity at all levels from the Board to frontline with clear accountability and decision making responsibilities;
Balancing strategy and operations in the right measures so one doesn’t get divorced from the other;
A focus on multi-disciplinary and multi agency team working with a balance between clinical leadership and operational management;
An equal balance between managing finance and managing patient processes and innovation;
Achieving the right balance between regulation, compliance and must dos and enabling creativity and innovation;
A strong focus on organisational development, team building, team development, and succession planning, coaching and leadership development.
• A drive for innovation;
• A drive for continuous improvement and learning;
• Empowering the workforce - allowing staff and teams to try things in a 'no blame culture';
• Improved communication through use of conversations at all levels to build confidence, relationships and openness;
• Acting on ideas both at a local level - 'just do its' and corporately through more formal implementation programmes;
• Routinely identifying, celebrating and sharing good practice and success;
• Multi professional, multi-disciplinary and multi-organisational learning - erosion of silos;
• Effective team working at all levels;
• Delegated decision making;
• Alignment of staff objectives and development activity with innovation and improvement.
4 Powys teaching Health Board (2014) Organisational Principles to Improve Effectiveness. Powys teaching Health Board 5 Powys teaching Health Board (2012) Maximising the Health Board’s Teaching Status Board Paper December 2012. Powys teaching
Health Board

Page 67 of 230
6. QUALITY AND SAFETY IMPROVEMENT Quality and safety improvement remains the golden thread underpinning our planning processes
and is central to our work and the activities that staff and teams undertake in providing safe care for
our patients. Sustaining and embedding this work going forward is crucial in ensuring Powys
residents receive the highest standards of safe care. We recognise our duty in ensuring this focus is
strengthened going forward for services we commission and purchase from other organisations for
our residents
We recognise there is work to be done. In setting out our achievements and challenges through our
Annual Quality Statement we are continuously assessing and informing Powys residents about how
well we are doing across all our services. In 2013/2014 the priority we set to engage all teams in
organisation wide learning focusing on the failings in Mid Staffordshire. Following the publication of
the report ‘Trusted to Care’ all areas and teams have been engaged in learning and improving, and
throughout 2014/15 and we will continue to strengthen organisation-wide learning and assure our
public that we are giving safe levels of care especially in the fields of hydration, night sedation,
continence and medicines management.
6.1. QUALITY DELIVERY PLAN
The Board’s Quality Delivery Plan is based simply around the following four themes:
Putting quality and safety above all else: Embed a culture of continuous improvement in safety,
quality and patient experience in all settings. Ensure absolute compliance with fundamental
standards, professional conduct and competence across disciplines;
Patient-centred care: Create a culture that places the patient first in everything that is done.
Patients and their carers to be treated with dignity, respect and compassion;
Integrating improvement into everyday working: Eliminating harm, variation and waste by
adopting a quality improvement methodology;
Investing in our staff: Through training and development, enabling them to influence decisions
and providing them with the tools, systems and environment to work safely and effectively.
Emphasising the importance of listening and learning from our patients and ensuring care is person
centred as set out in our vision to deliver ‘truly integrated care centred on the needs of the individual’,
we developed an initial draft of a Patient Experience Strategy in July 2014. This sets out our aim to
provide high quality, safe and effective care that reflects the needs of patients and our local
population. Further work is underway to further structure the strategy and develop an
implementation plan in conjunction with service users and representative groups.
To ensure a consistent approach to patient experience across the Health Board we are working with
individuals with research and evaluation skills to produce a framework to use for patient experience
Key Aim:
Embed a culture of continuous improvement in safety, quality and patient
experience in all settings
Create a culture that places the patient first in everything that is done
Ensure absolute compliance with fundamental standards, professional conduct and
competence across all disciplines

Page 68 of 230
survey work and data collection. This will provide our Board and others with greater confidence in the
data and its methods. This framework will serve to strengthen our approaches to listening and learning
from patients, taking action and making changes to put improvements in place. In turn providing
greater opportunity to capture and share the learning across Powys.
Our Annual Quality Statement http://www.wales.nhs.uk/sitesplus/867/document/248640 sets out
where we now and where we want to be. Our focus is on providing as much patient care as possible
close to home and in working towards this we have set out our main quality improvement aims for
2014/15.
Throughout 2013/14 we were working to strengthen links with commissioners providing services to
Powys residents. Progress has been made with our English providers and quality monitoring has
been strengthened in 2014 with formal links with clinical commissioning groups and individual
providers; this will continue going forward. However, we recognise we need to put arrangements in
place with our Welsh providers to ensure that we gain assurance on the quality and patient safety of
services they provide. Alongside this assurance on specialist services will be reported to our Board
through the Welsh Health Specialised Services Committee strategic quality framework. Focusing on
safety, effectiveness, experience and leadership a suite of high level indicators will provide
assurance on services commissioned on our behalf. This will link to strengthening the capability and
systems around commissioning for quality for both Welsh and English providers, care homes and
primary care.
Work is being taken forward to develop our commissioning performance framework and escalation
plan which sets out the requirements within the Long Term Agreements and who and how we will
monitor provider performance; whether it is being achieved and associated escalation points. The
framework setting out a step-by-step process to source quality and patient safety information and
providing assurance will be piloted throughout 2015.
Peer review of ward and department areas has progressed over the past year. Operational peer
review visit have been trialled as part of our response to the Trusted to Care report, in addition to
executive and independent member ’15-step challenge’ walkrounds, which are now embedded
within Powys. Improvements are being implemented in response to learning from the ‘Trusted to
Care’ report and plans include the improvement of signage in some areas and the development of a
Medication Practice Development Forum. Assurance on these actions is reported alongside other
improvements to our Quality & Safety Committee.
Issues of health and safety have been at the forefront of many discussions over the past year. Our
revised Health and Safety Strategy and Implementation Plan will ensure we provide a safe and healthy
environment for all employees, patients, visitors, contractors and other members of the public who
have contact with the organisation. This will include ensuring access to and compliance with the full
suite of statutory and mandatory training as required by each member of the workforce. Our focus
going forward will be broadened to ensure we consider the environment as part of our quality
monitoring, such as ensuring basic furnishings exist for patients’ use and they are functional to meet
their needs, one example being improving the environment of care for patients with dementia with
large clocks on walls, painted doors and toilet seats. To ensure we have the right strategic and local
arrangements for health and safety within Powys we are currently in the early stages of procuring an
external consultant to advise on a model that befits the needs of the Health Board. Where necessary,
this will strengthen the current system and approach supported by staff with recognised skills and
capacity to manage the whole system.

Page 69 of 230
Over the past few years, access to specialist infection prevention and control advice and microbiologist
support for Powys has been problematic and has featured as a key risk on the corporate risk register.
Although ad hoc advice has been sought and provided from neighbouring health boards, this has not
been consistent and efforts to firmly secure a named infection control doctor have been unsuccessful.
However, throughout 2014/15 we have successfully recruited to an infection prevention control nurse
and are working with Public Health Wales to finalise arrangements for medical support, including
microbiology. This will ensure we have a robust and sustainable service Powys for the advice they give
with regards to infection prevention and control positively impacting on patients, safety and care.
The ‘Gift of Complaints’ Report (Evans 2014) has identified some key areas for improvement, namely
the variability in which Putting Things Right has been implemented across Wales and the need for
appropriate infrastructures within organisations to support this. Within Powys we need to review the
capacity and ways of working in support of this alongside reviewing some key processes to ensure
they remain robust and are effective in their expected outcome, such as our processes for dealing
with serious incidents. In 2014, we appointed a patient experience/ concerns officer to work as part
of the concerns team. Strengthening of this area further will be through growing the capacity and
capability to manage concerns across the health board. The appointment of the senior clinical quality
and patient safety analyst will support this area of work focusing on interpreting of data, trend analysis
and ensuring organisation-wide learning.
Limited capacity to manage medical records, in particular the lack of an effective system in place to
manage archived records, is an identified risk on our corporate risk register. Actions have been taken
to mitigate the risks to patient safety and care but the lack of a central store and manual/electronic
systems in place pose potential risks to patients. In order to address this it has been recognised that a
project management approach to addressing the issues is required. It is intended to appoint a project
manager to undertake a records appraisal across Powys and develop a business case proposing
solutions, one such example being a joint central records solution with Powys County Council.
As indicated there are key areas of quality and patient safety for improvement. Below are key quality
and safety objectives for 2015/2016 supported by further information on planned improvements over
the next three years, these include:
Improve compliance with statutory and mandatory training;
Publish the Patient Experience Strategy and supporting implementation plan;
Produce a framework to use for patient experience survey work and data collection;
Pilot the commissioning performance framework and escalation plan;
Systematically review risk in relation to clinical quality and patient safety;
Secure an external consultancy to advise on a health and safety model that befits the needs of the
Health Board;
Finalise the arrangements with Public Health Wales to secure and implement infection control
doctor and microbiology support to provide medical advice on infection prevention & control
issues;
Develop a business case proposing solutions for managing patient’s medical records.

Page 70 of 230
Table 15: Quality Delivery Plan Domain In Partnership with the NHS People Can Expect How will we measure improvement 2015-16 2016-17 2017-18
STAYING HEALTHY
People in Wales are well informed and supported to manage their own physical and mental health
I have a healthy and active long life Key performance indicators reported to Quality & Safety to include mortality data √ √ √
My children have a good healthy start in life
I can access the support and information I need, when I need it, in the way that I want it.
Monitoring of sensory care standards √ √ √
SAFE CARE
People in Wales are safe and protected from harm and protect themselves from known harm
I am supported to protect my own and my family’s health
Review of the health and safety capacity and support within the organisation
Implementation of the Health & Safety Strategy and supporting strategic action plan for 2014-2017
Implementation of the risk management strategy and implementation plan
√
√
√
√
√
√
I am kept safe and protected from avoidable harm through appropriate care, treatment and support
Consistent and transparent incident reporting across organisation, and effective management responses
When things go wrong, proportionate investigation, including root cause analysis methodology is routinely used
Through Putting Things Right process, effective and transparent approaches to staff and organisational responsiveness and learning from concerns
Regular review of local and national trends to inform quality improvement and understanding of risk
Strengthened capacity, skills and knowledge in the wake of the Evans report to ensure timely responsiveness to concerns at a local level and embedding learning
Review of systems, processes, capacity and capability going forward reflecting the recommendations of the ‘Gift of Complaint’s review and recommendations
Improved analysis of complaints and action taken
A focus on understanding patterns and themes from concerns and using risk as the basis for prioritisation
Strengthen working across Health Boards and NHS organisations through all wales networks and networks outside of Wales, sharing learning and good practice to inform improvements, e.g. NHS Wales service user experience group
Care home governance objectives to be included.
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
I receive a high quality safe service whilst in the care of the NHS
Strengthen Inspection and audit processes through effective monitoring and reporting e.g. CHC, Children/Older People Commissioners, HIW, WAO
√ √
EFFECTIVE CARE
People in Wales receive the right care and support as locally as possible and are enabled to contribute to making that care successful
Health care and support are delivered at or as close to my home as possible
Evidence-based and patient focussed service planning and commissioning
Engage as stakeholders with commissioners when planning services
√
√
√
√
√
√

Page 71 of 230
Domain In Partnership with the NHS People Can Expect How will we measure improvement 2015-16 2016-17 2017-18
I receive the right care and support to either improve or manage my own health and wellbeing
Readily accessible fundamental standards and means of compliance
Build on the learning from ‘Trusted to Care’ to improve safety in medicines management, hydration, continence and the use of night sedation
Use clinical audits and outcome reviews to test quality of care and drive improvement
Rolling programme of local clinical audit, appropriately planned and robustly monitored
Use internal and external audit assessment and recommendations to inform service improvement
Develop and implement effective and comprehensive quality assurance measures
Explore developing a systematic approach/ framework to monitor provider performance and assurance to underpin contract meetings e.g. Powys internal assurance group
o Use quality trigger tool o Complaints in/against providers o Patient related incidents o Clinical Governance for GDS o GMS QOF monitoring o CHC visits feedback
Strengthen quality monitoring in the contract review process
√
√
√
√
√
√
√ √
√
√
√
√
√
√
√ √
√
√
√
√
√
√
Interventions to improve my health are based on good quality and timely research and best practice
75% of staff trained in bronze level quality improvement skills
Staff participation in 1000 Lives Plus programme
To embed the revised Standards for Health Services/ outcome themes to underpin continuous self assessment and improvement actions and link with risk assessment
Share and spread successful and effective developments across the THB
Systematic use of national and professional guidance, e.g. NICE
Education, research and development built into workforce planning and personal development plans
Research and innovation driving improvements in care and uptake of new interventions and technology
√ √
√
√
√
√ √
√
√
√
√ √
√
√
√
√ √
DIGNIFIED CARE
People in Wales are treated with dignity and respect and treat others the same
I receive a quality service in all care settings
Routinely use relevant quality triggers as early warning system, e.g. incidents, risks, complaints pressure ulcers, falls, infection control rates
Monitor Fundamentals of Care audit results
Further develop IFOR (Intelligence Focused Online Reporting) to provide quality data from the Datix system, as above and medication incidents, risks, mortality, Tier 1 targets, etc.
Each Powys care home (nursing) to have a contract monitoring visit annually, the action plan developed from the visit will be monitored by PTHB and PCC.
Develop routine data forms covering unscheduled admissions, falls, deaths etc
√
√ √
√
√
My voice is heard and listened to
Implementation of the Patient Experience Strategy to include training, information for service users to ensure single point of contact, service user engagement events
Improve the web-site and use of social media
Patient satisfaction survey and feedback, e.g. roll out the NHS Wales User Experience Survey to additional services
Engagement in service change, working with Powys residents to improve services
Through co-production, using patient stories and feedback from surveys, make changes resulting in better outcomes and improved efficiency
√
√ √
√
√
√
√
√
√
√
√
√
I experience a care system where all participants are treated with compassion, dignity and respect
Ensure the environment meets the need of the public and is compliant with expected standards, such as improving the environment of care for dementia sufferers
√ √

Page 72 of 230
Domain In Partnership with the NHS People Can Expect How will we measure improvement 2015-16 2016-17 2017-18
TIMELY CARE People in Wales have timely access to services based on clinical need and are actively involved in decisions about their care
I have easy and timely access to primary care services
Publication scheme – look at working with PCC for website support/ development to support FOIA/ publication scheme.
Improved level of data on quality and patient safety published
Publication of Annual Quality Statement
√
√ √
√
√ √
√ √
To ensure the best possible outcome, my condition is diagnosed early and treated in accordance with clinical need
Review quality and patient safety requirements in all contracts
Undertake a Quality Impact Assessment on any proposed change to services
Strengthen capability and systems around commissioning for quality, both Welsh and English providers, care homes and primary care
Swift action where needed when quality triggers or measures highlight potential for substandard care/problems
√ √
√
√
√ √
√
√ √
√
INDIVIDUAL CARE People in Wales are treated as individuals with their own needs and responsibilities
Inequalities that may prevent me from leading a healthy life are reduced
My individual circumstances are considered Monitoring of spiritual care standards √ √ √
I get care and support through the Welsh language if I need it
STAFF AND RESOURCES People in Wales can find information about how their NHS is resourced and make careful use of them
Financial resources are used efficiently and effectively to improve my health outcomes
Working collaborately with Powys County Council in our work in information governance and quality improvement
√
√
I work with the NHS to improve the use of resources
Review and strengthen the governance framework around quality, including committee/management group structure, reporting mechanisms
Further develop IFOR (Intelligence Focused Online Reporting) to provide quality data from the Datix system, as above and medication incidents, risks, mortality, Tier 1 targets, etc
Routinely use relevant quality triggers as early warning system, e.g. incidents, risks, complaints pressure ulcers, falls, infection control rates
Strengthen Inspection and audit processes including external through effective monitoring and reporting e.g. CHC, Children/Older People Commissioners, HIW, WAO
Enhanced approach to Quality and Safety ‘Walkrounds’, e.g. ‘walkround’ scheme, peer review site visits, ministerial unannounced spot checks
Quality impact assessment of Powys service changes
√
√
√
√
√
√
√
√
√
√
Quality trained staff who are fully engaged in delivering excellent care and support to me and my family
Strong leadership across professional groups supported by training, e.g. Institute in Leadership & Management training
100% mandatory and statutory training
100% PaDR
Robust personal and professional development and career framework in place
Establish direct link between training and development for staff to identified quality concerns
Training and development for: Care homes, GP practices
√
√ √ √
√
√
√
√ √ √
√
√ √ √
√

73
7. HEALTH BOARD PRIORITIES
This section outlines the approach the THB is taking in respect of he three strategic priority areas of
Primary Care and Community Services, Commissioning and Integration. These are set out to meet
the strategic objectives as follows:
Commissioning
•Commission sufficient capacity to meet the need for timely and high quality healthcare services across the community and hospital system, with a shift in emphasis to prevention and early intervention
•Embed an innovative and prudent approach to service commissioning focused on patient outcomes
•Provide assurance on the quality and effectiveness of healthcare services across the healthcare system
Primary Care and Community
Services
•Increase the capacity of primary care and community services to deliver a greater proportion of care in Powys
•Increase the resilience of primary care and community services direct service provision
•Strengthen the clinical leadership role of primary care and community staff in service planning, commissioning and delivery
Integration
•Place the citizen at the centre of integrated service delivery through joined up systems, processes and teams, delivered at neighbourhood level
•Develop integrated approaches to support systems and functions across all areas of our shared business with Powys Council
•Put in place joint strategy, governance and scrutiny arrangements with Powys Council
Strategic Priorities
Figure 38: PTHB Strategic Priorities and Objectives

74
7.1. PRIMARY CARE
This chapter describes the specific programme of work that we are undertaking to support and
develop primary care, and to place primary care in a leadership role. Primary care and community
services are also a vital element of our overall approach and the readers should also look to other
parts of this plan to see this reflected, for example:
The role of primary care working alongside community services to shape our response to
planned care;
The leadership of primary care in commissioning;
Our plans for integrated health and social care at local level, encompasses primary care and
community services;
A single IM&T system across our services;
An integrated approach to estate across our service delivery and with partners.
The THB has already put in place a strong primary care and community service resource framework
to support the management of patients as far as possible in Powys that goes significantly beyond the
core contracted service models and will be extended in this IMTP:
Enhanced role for GPs to manage patients in the community, access to GP managed beds;
Highly developed community resource teams led by GPs: specialist nurses are community based
and work alongside GPs, nurse and therapy teams;
Specialist nursing and therapy support services provided from community hospitals and in the
community;
Extended District Nursing and Hospice at Home services;
Joint working with Powys Council to provide reablement services.
Developing Primary and Community Care services The Health Board has a clear ambition to place primary care at the heart of its service strategy in
both a leadership and delivery role to maintain and develop strong, vibrant Primary and Community
Care services. The PTHB Director of Primary and Community Services will continue to work closely
with the Medical Director, who will provide professional leadership for primary care services in
Powys.
The role these services play are also part of the bigger picture of health care provision. Being very
much at the ‘sharp end’ of the health service, the role they play is pivotal in reducing dependence on
secondary care services, and the clinical perspective staff working in primary care can bring to
strategy is central to our approach to transformation of services. The Health Board will develop, at
pace, a Primary Care focussed service, which provides far more care closer to where the patient lives
and reduces the need for travel to a District General Hospital.
GP Clusters are developing well in Powys. Examples of innovative working have emerged and been
implemented. In 2014, the first round of service development plans specific to each GP Cluster has
identified a broad range of actions GPs wish to address. The Health Board will continue to work with
Increasing the capacity of primary care and community services to deliver a greater
proportion of care in Powys
Increasing the resilience of primary care and community services direct service
provision
Strengthening the clinical leadership role of primary care and community staff in
service planning, commissioning and delivery

75
the GP Clusters and develop the role they serve in ensuring the people of Powys enjoy safe, effective
and efficient health care services.
Understanding the strategic environment around Primary Care Primary Care is facing a future that provides challenges on one hand, but considerable opportunities
on the other. Our Plan for a Primary Care Service for Wales1 refers to a Primary Care service for
Wales, based on the principles of prudent healthcare, becoming the mainstay of the NHS: tackling
the root causes of ill health, preventing people from being admitted to hospital unnecessarily,
helping those who have been admitted to get home quickly with the right support, motivating and
supporting people with chronic conditions and long-term illnesses to manage their health at home.
These are the fundamental aims the Health Board will continue to deliver at an increased pace.
The Bevan Commission2 report on improving primary and community care in Wales goes on to
recognise that Primary Care is a highly effective means of health care delivery in terms of cost and
quality, however, its full potential is rarely realised. This is recognised in Powys and the Health Board
is at the point where it can tap into this potential.
Much focus in healthcare is currently on the acute sector, particularly unscheduled care and accident
and emergency, though many of the solutions to the pressures rest in primary and community care.
The Health Board’s objective over the next 3 years is to accelerate the pace by which it capitalises
upon these opportunities for the benefit of all its population.
In Delivering Local Health Care3 it is acknowledged that accessible, person centred primary care
services sit at the core of local care. The document goes on to acknowledge that general
practitioners (GPs) and their teams continue to be the first point of contact for their patients, where
all their needs are considered – physical, mental and general well-being. This places GPs in a key
position to take a full and balanced view on the overall needs of the population they serve and the
Health Board is capturing this view within its plans.
As part of its Integrated Medium Term Plan, the Health Board has developed a set of actions which
support local providers of Primary Care services to work together imaginatively to further improve
and extend the range and quality of services they deliver to the people of Powys.
Priorities for 2015/16 and beyond Strategically, the Health Board’s priorities for the further development of Primary Care services in
2015/16 and 2016/17 are heavily influenced by the following the requirements of Our Plan for a
Primary Care Service for Wales; the recommendations from the Bevan Commission as they relate to
the improvement of Primary Care; and the requirements of Together for Health: Eye Health Care –
Delivery Plan for Wales & Together for Health: A National Oral Health Plan for Wales.
Drawing on the above, and in particular that of Our Plan for a Primary Care Service for Wales, the
Primary Care development priorities fall into five categories:
1. Strong leadership
2. Planning care locally
3. Improving access and quality
4. Equitable access
5. A skilled local workforce
The Health Board’s action plan in relation to each of these is as follows:
1. Strong leadership: Adapting for the future Primary Care is not a service delivered by a single, or even a small number, of providers. In Powys,
Primary Care services are provided by in excess of 60 individual organisations, all autonomous from

76
each other. Each has at least one contract with the Health Board; far exceeding, by comparison, the
number of service level agreements the Health Board has with secondary care providers.
To ensure the very best from Primary Care, it is essential the Health Board is in a position to provide
an adequate level of leadership and support to develop the service to its maximum effectiveness.
Not to do so creates a risk of a fractured, inequitable service in terms of availability and quality of
care provided.
This requirement for adequate leadership and support goes much further than the traditional
Primary Care services alone. It must also be available to help Primary Care fully respond to the
opportunities set out in this plan which push the boundaries within which Primary Care has
traditionally operated.
To ensure the level of support available to Primary Care is sufficient to meet the task being set, the
Health Board will undertake a review of the resources available at both Locality and corporate levels.
2. Planning care locally: GP Clusters Delivering Local Health Services4 requires health boards to support and develop the fledgling
networks of general practitioners to embrace the full set of functions and accountabilities envisaged
in Setting the Direction5. This work is further strengthen by the introduction, in April 2014, of the GP
Cluster Network Development (CND) Domain of the Quality & Outcomes Framework component of
the General Medical Services Contract in Wales.
Powys Health Board is divided into three locality-based management teams; these are located in the
North, Mid and South of the county. The development of strong links between each Locality and its
local Primary Care providers, especially GPs, is extremely important. Each Locality already had
arrangements in place to regularly engage with GP representatives, as well as having provision for a
lead GP to be a part of its management team. The introduction of the CND Domain has, however,
refocused this work in order to meet the requirements the domain now demands. During the last
year, the 17 medical practices in Powys have been supported in the development of their individual
Practice Development Plans. These have fed into the GP Cluster Network Plans each of the three GP
Clusters in Powys have produced in autumn 2014.
Approximately 180 separate actions were identified across the three GP Cluster plans, culminating in
each GP Cluster identifying its top-five priority actions.
The Welsh Government has announced £6m of funding to support the service development
intentions of GP Clusters. The Health Board will support the GP Clusters in Powys with the utilisation
of this funding in support of their priority areas for service development. We have assumed to this
end, £0.3M funding from Welsh Government to support this work.
Action: The Health Board will pro-actively support GP Clusters in the delivery of the actions identified as having the greatest priority in the GP Cluster Network Plans; these are set out in accompanying plan-on-a-page.
There is, however, much more to be done in supporting the development of the GP Clusters.
2014/15 was the first of a three year cycle supporting the development of GP Clusters and the
production of their annual plans. During 2015/16 and beyond, the Health Board will work to ensure
the influence of the GP Clusters is reflected in its longer-term plans and that processes that support
the work of the GP Clusters is strengthened with improved access to relevant information (such as
that relating to patient activity and projected future demand), together with enhanced support from
Public Health Wales in terms of needs assessment on a local basis

77
Action: The Health Board will continue to develop the resources it provides, via the Locality teams, to support the development of GP Clusters. The Health Board remains focussed on the ambition set out in Delivering Local Health Services in terms of the advanced level of maturity which involves each Locality/GP Cluster achieving the following:
Devolved budgets in place
Robust governance and accountability arrangements in place
Hard evidence to demonstrate the delivery of agreed outcomes
Engaging with Primary Care providers is not, however, just about harnessing expertise in the design
of care pathways for patients, it also about identifying the part those providers play in the delivery of
those pathways.
3. Improving access and quality: Pushing the boundaries of traditional Primary Care services The delivery of high quality Primary Care services has long been a cornerstone of health care
provision in Powys. Maintaining this standard of service provision will, however, be a challenge in
the future.
Increasing workload and the demands on Primary Care providers to further improve patient access
to services are challenges which need to be addressed.
The baseline contracts are a foundation upon which the delivery of additional services can be
negotiated between the Health Board and the provider. These additional services can be secured
through the enhanced services arrangement which sets-out the nature of the service to be provided,
the quality and patient safety standards to be met, and the reward the provider will receive in
return. The development of the primary care quality dashboard for Powys will strengthen the THB’s
assurance on quality and safety standards.
Considerable scope exists for the Health Board to secure additional services via this approach;
services that fit both with the needs of patients and the direction the Health Board is travelling in
strategically. The enhanced services component of the current General Medical Services contract
demonstrates the range of additional services that can be secured (via individual medical practices
or federations of medical practices), over and above those required as part of the core contract the
Health Board has with medical practices across Powys. The scope for securing additional services
does not just involve medical practices, however; the Health Board will, where possible, negotiate
the provision of additional services with the other Primary Care providers too.
A number of Primary Care providers in Powys have expressed a willingness to work with the Health
Board to increase still further the range of services they provide to patients, there is considerable
reflection of this in the GP Clusters plans that have been submitted in 2014. The Health Board will
work with primary care providers to maximise this opportunity. The Health Board will, in particular,
be working with GPs in the Mid and North Powys GP Clusters to introduce a virtual ward model
which builds upon that already successfully operating in South Powys. Figure 39 illustrates the strp
change reduction in emergency admissions following the introduction of the Virtual Ward in South
Powys in April 13.The overall aim is to provide a greater focus on anticipatory care, thereby reducing
the number of un-planned admissions to an out-of-county District General Hospital. The advantages
of doing so include improved patient experience, reduced demand on District General Hospital
services and the delivery of a more cost effective service for the Health Board. In addition, this will
release funding from secondary care, enabling the enhancement of Primary Care services and the
acceleration of care provision closer to home. The Health Board has successfully secured Invest to
Save funding to partially support the development the roll out of the virtual ward. In addition, we
have assumed use of £0.235M to support the residual costs out of the Welsh Government £30M
primary care fund.

78
Figure 39: Impact of the Virtual Ward in South Powys
Source - PTHB Contracted dataset
Action: Working with the Mid and North Powys GP Clusters, the Health Board will work to introduce the Virtual Ward model which are sensitive the local needs in these two areas of the county.
Progress has also been made during 2014 in developing the way GPs are engaged in providing
medical cover to local community hospitals. At the beginning of 2015, the responsibility for the
acute in-patient beds at both Bronllys and Newtown hospitals transfers to Powys medical practices.
Under previous arrangements, the beds were either solely consultant-led or a shared responsibility
between a consultant and GPs.
In the case of Bronllys, the new agreement with GPs does not just involve the in-patient beds;
working with Health Board staff, it also includes the provision of an integrated community service
specifically aimed at avoiding hospital admissions, or where admissions have needed to take place,
supporting patients to be safely discharged back home at the earliest opportunity. This enables the
provision of care much closer to home; reduced reliance on District General Hospitals; improved
access; and greater sustainability for medical practices.
Working in partnership with GPs, the Health Board intends to further develop this model in other
parts of the county. Doing so, results in the provision of a more sustainable service and drives
integration between the services provided at both community hospital and community level. It also
stands to attract a broader cross-section of new GPs looking to pursue careers that involve more
than just core General Medical services alone. To this end, we have assumed funding from the £30M
Primary Care fund to underpin the GP Medical Model of £0.4M.
Action: Building on the work involving Bronllys and Newtown hospitals, the Health Board will work with local GPs to develop similar models of care in other parts of Powys, most notably in areas where current services are fragile or there are long distances to secondary care provision.
70
80
90
100
110
120
130
140
150
160
Num
be
r o
f p
atie
nts
Month of discharge
Number of Emergency Admissions of South Powys Patients - April 2012 to Oct 2014 - all Providers - Specialities of General Medicine,
Gastroenterology, Endocrinology, Respiratory.
No. of admissions Median Lower Control Limit Upper Control Limit

79
Developing the extent to which patients can have local access to diagnostic services is another key
aim for the Health Board. Local access to readily available diagnostic services not only reduces the
distances patients travel to receive a service, but also increases the GPs’ ability to safety care for
patients nearer to where they live, be that in their own homes or in a community hospital.
GPs in the South Powys GP Cluster have commenced work to explore the opportunities that exist to
develop more locally based diagnostic services in their area; the provision of a mobile MRI scanning
service is one example. This has involved looking at what more can be done using the community
hospital estate, but also what can be secured using mobile facilities. We have assumed £0.1M from
the £30M primary care funding to support this development.
Action: Building on work already commenced in South Powys, the Health Board will work with GPs to maximise the local delivery of diagnostic services where it is both safe and cost effective to do so.
To support the further delivery of services in a Primary Care or community setting, there is a need
for further investment and this investment must come, in the main, from that currently used by the
Health Board in securing secondary care services. Compared to Wales, the repatriation of funds
spent with NHS England is easier to achieve, due to the nature of the agreements that exists
between Health Board and provider. Securing a redirection of funds is, however, pivotal to the
success of a shift in care delivery from secondary care to one more orientated to the where the
patient lives. It is this re-direction of resources that the Health Board will aim to achieve.
Action: Building upon the successful repatriation of funding in previous years, the Health Board will work to ensure the resources required to support a shift of care provision from secondary to a primary care/community setting are readily available.
4a. Equitable access: meeting the needs of patients Securing equitable access to all Primary Care services can be a challenge in a large, sparsely
populated county such as Powys. There are, however, a number of factors to consider. They include:
How reasonable access to services in secured not just during the extended working day, but also
overnight and at weekends;
How other methods of accessing services are used to maximum effect, not just face-to-face
contact; and
How a wider range of health care professionals can be used to meet the needs of patients
4b. Equitable access: securing access to services Understanding the needs of patients is of paramount importance to the Health Board. The following
is a summary of the issues the Health Board knows patients raise as concerns to them:
Having ready access to appointments, including those conducted over the telephone (probably
the greatest concern overall);
Having continuity of care when moving from Primary Care into secondary care and vice versa;
Ensuring the communication needs of those with a sensory impairment are understood and
respected;
Having more time during consultations for explanation and checking it are understood;
Respecting the needs of those with a caring responsibility;
A smooth transition between health and social care and having the services clearly sign-posted
and explained;
Being treated as an equal and with dignity and respect;

80
Professionals taking the time to understand the needs of patients, providing informed choice,
and helping them get timely access to the right help;
Having the confidence to accept the help and advice of other members of the Primary Care team
and note feel they are receiving a lessor service.
The Health Board regularly works with Primary Care providers to test their ability to meet the needs
of patients. This is not just confined to identifying the hours when a service is available, but also the
level of resources a provider has to reasonably meet patient need during those hours of opening.
Where necessary, the Health Board examines how resources can be moved around the county to
ensure as equitable a service as possible. A good example of this is dental services and the
adjustments the Health Board makes to contracts with dental providers to secure greater capacity
where the level of patient need dictates.
Action: The Health Board will support Primary Care providers to regularly assess the appropriateness of their hours of availability and their ability to understand and meet the needs of their patients.
The hours in which a Primary Care service is available is an important consideration for the Health
Board. Most services now extend beyond the normal working day, but the extent of this will vary
between services. The Health Board has access to emergency dental care 7 days a week, but for
General Medical Services (GMS) the requirement is for a 24 hours service, 365 days a year. To deliver
an around-the-clock service for GMS, the Health Board has developed a solid, long-standing
relationship with Shropdoc, its out-of-hours provider. Shropdoc has an excellent performance record
and has recently been very favourably assessed by the Care Quality Commission. Going back over 15
years, the Health Board and Shropdoc have worked together to provide high quality, accessible
services to the people of Powys. All out-of-hours calls from people in Powys are dealt with by
Shropdoc, together with the face-to-face contact in the majority of areas (Ystradgynlais being the
only exception). Shropdoc’s input into Powys does not stop with out-of-hours GMS; it also provides
all out of hours medical cover for the network of community hospitals in the county as well as
providing the Care Co-ordination Centre (CCC) service where referrals by GPs are actively tested
against other alterative pathways of care before resorting to a hospital admission, thereby
contributing to the Health Board’s unscheduled care plan.
A clinically led triage service is a widely valued component of the Shropdoc service. Although
currently very much a feature of the out-of-hours service only, there are now expressions of interest
from some of the GP community in Powys to explore how clinically-led triage, provided at scale, can
be used to support the in-hours service provided by individual medical practices. This will enhance
patient access to services; facilitate signposting to other appropriate services; and improve the
sustainability of medical practices in the longer-term. We have assumed £0.150M from the £10M
primary care fund to support this work.
Action: The Health Board will continue to develop its relationship with Shropdoc and in so doing maintain access to sustainable Primary Care services in the county. This will include exploring further the role of clinically-led telephone triage in the delivery of in-hours General Medical Services.
Acceptable access to a service cannot just be confirmed by testing the number of hours it is
available; the ability for patients to take full advantage of a service must take into account other
factors too. They include the needs of language, cultural need, physical or learning disability, sensory
loss, low health literacy, frailty, and those who don’t routinely seek help from the NHS.

81
The Welsh Language Commissioner reviewed the use of the Welsh language in Primary Care and
published My Language, My Health: Inquiry into the Welsh language in Primary Care8 in June 2014.
In its response, the Welsh Government reflected on the role of the GP Clusters, saying:
‘Clusters will need to consider the language needs of their local populations in agreeing their plans,
including signposting where the services are available in Welsh – this could be a nearby service, not
necessarily the closest, which can meet a person’s Welsh language need’
Action: During 2015, the Health Board will work with its GP Clusters to consider the finds of the Welsh Language Commissioner’s report and in particular their response to the Welsh Government’s requirement as set out above.
5. A skilled local workforce: securing a sustainable workforce Powys also has a changing workforce and amongst GPs in particular there is a comparatively high
proportion of the current workforce over the age of 50, with retirement decisions amongst many of
them considered a possibility in the short to medium tum. Recruitment to vacant GP posts is already
a challenge for some medical practices in Powys. There is evidence of interest in vacant posts being
minimal and in some cases non existent.
The practice nursing workforce also has its challenges. Again, the workforce is disproportionately
weighted towards those aged over 50 and medical practices are reporting difficulties in filling vacant
posts, especially with suitably experienced nurses.
These challenges need to be overcome if the sustainability of Primary Care provision in Powys is to
be preserved, and furthermore, in a position to accommodate a greater workload as service
provision continues to shift from secondary care to a Primary Care setting.
The Primary Care workforce has changed over the last 10 years and will continue to do so. The role
of the traditional practice nurse has changed, with a transfer of duties that previously would have
been undertaken by a GP. In turn, the role of the health care assistant has also changed with a
transfer of duties previously undertaken by a practice nurse. Increasingly too, a greater range of
professionals can be seen working as part of the Primary Care Team. These include pharmacists,
physiotherapists and nurses with extended skills.
The Health Board is being pro-active in addressing these challenges and has established a Primary
Care Workforce Group chaired by the Executive Director for Workforce and Organisational
Development. Membership of the Primary Care Workforce Group includes representation from
Primary Care providers, including a GP and Practice Manager.
The Primary Care Workforce Group draw up an action plan reflecting a range of initiatives being
pursued to assist Primary Care providers secure a sustainable workforce in the future. Amongst
these initiatives is a proposal to undertake a structured recruitment campaign for GPs with the
assistance of external recruitment experts, and an examination of the role of Physician Associate and
how it may play a part in the wider Primary Care workforce. Work on the latter involves some of the
UK’s leading experts in the training and deployment of Physician Associates. The Health Board has
assumed that it will utilise £0.250M of the £30M of Primary care development fund to aid the
sustainability of primary care services in Powys and workforce testing.
Action: The Health Board to ensure, via the Primary Care Workforce Group, the development and implementation of an action plan which reflects a range of initiatives to assist Primary Care providers in securing a sustainable workforce for the future.

82
Finding innovative solutions to meeting increasing patient need The effect of poor lifestyle choices and those associated with an ageing population, combine to
create increased demand on Primary Care services, in particular those provided by GPs, from people
with long-term conditions. Strengthening and developing our Primary Care services will contribute to
developing the person centred approach required to support people with long term conditions
through successful self management and adequate access to information. The mechanisms for
delivering the vision for long term conditions management in Powys are managed via multiple
appropriate delivery plans such as the development of community resource teams and virtual ward
model through the Unscheduled Care delivery plan.
In order to encourage patients with long term health conditions to maximise their own health and
wellbeing, the Health Board’s Pain and Fatigue Management Service is broadening its remit to help
such patients develop self management techniques, including those that are psychologically based.
The Invest in Your Health programme is designed to help these patients learn skills and strategies to
make their health more resilient, and provide upstream prevention which will have significant
benefits in terms of chronic disease management in future years.
The platform from which this programme will be launched, is the Chronic Conditions Management
Local Enhanced Service developed in Powys for delivery by GPs. Staff from the Pain and Fatigue
Management Service will provide medical practices with training and quality assurance input to
enable patients identified via the Lifestyle Local Enhanced Service to have made available to them
the resources of the Invest in Your Health programme. We have assumed up to £0.5M of the £30M
Primary Care Development Fund to support this work.
Action: The Health Board will develop the Invest in Your Health programme and make it available to medical practices across Powys in support of the Lifestyle Local Enhanced Service.
Dental services During 2013, two key Primary Care related delivery plans were published by the Welsh Government:
Together for Health: Eye Health Care – Delivery Plan for Wales5, and Together for Health: A National
Oral Health Plan for Wales6. Both set out a range of actions the Health Board are required to address
and which are reflected in the IMTP.
In dental services, good progress has already been made in developing services at the interface
between Primary Care providers and the Health Board’s own community dental service.
Recently introduced into Powys is a service for complex endodontic treatment. Although the service
has an external consultant overview, the service is delivered in county by a member of the Health
Board’s own staff. Inhalation sedation for children is also now available from three sites in Powys. By
training more of its dental officers and dental therapists, the service avoids the need for general
anaesthetic and journeys out-of-county for patients with less complex needs.
This service development work will continue as there is considerable potential to increase services
that are tailored to meet the needs of patients, but are delivered cost effectively, especially those
that support a transfer of service provision away from more traditional pathways involving
secondary care. The Health Board will, for example, pursue the development locally delivered
specialist level special care dentistry and also target nursing homes in the county with a view to
addressing the dental hygiene needs of their residents. A further development involves the dental
service providing dermatological services such as the removal of some low grade facial carcinomas.
This service already exists in South Powys where a visiting consultant undertaking the procedure is
linked into the multi-disciplinary team at Prince Charles Hospital, Merthyr Tydfil. A similar
development is planned for Mid and North Powys when linkage with a District General Hospital
83
multi-disciplinary team is established. We have assumed utilisation of £0.040M from the Primary
Care Development fund to support this work.
Action: Delivery of the Health Board’s Local Oral Health Plan will continue in 2015/16, with particular attention paid to developing the role of locally based and visiting dental staff, linking where necessary with the governance structures of partner secondary care providers.
Eye Care services In addition to Primary Care optometry services, the Health Board also provides an ophthalmic in-
reach service which provides out-patient access across all three localities in Powys, and also a day-
case surgical service from hospitals in Llandrindod Wells and Brecon. The Health Board works closely
with external providers to secure these services. Capacity for the visiting consultant staff has
recently been increased, thereby enabling more care to be delivered locally and avoiding the need
for patients to make a lengthy journey to a District General Hospital.
During 2014, Powys teaching Health Board established the Powys Eye Care Group. With a
membership which includes both Primary and Secondary Care eye care providers, the group has
developed the Powys Eye Health Care Delivery Plan; a plan produced in direct response to the Eye
Health Care Delivery Plan for Wales.
Being an organisation that is not focussed on the provision of acute services, the Health Board is
keen to explore and develop the role played in particular by its Primary Care providers.
Providers of the Health Board’s commissioned secondary care Ophthalmology service are in the
main struggling with capacity and as a consequence are not meeting waiting times targets, with
some areas having a back log of follow ups as reported nationally.
As a result of these pressures, the Health Board’s own in-reach service is not able to develop further
and expand the range of services it could provide in-county.
It is key that developments involving Primary Care providers go ahead at pace, freeing up capacity
within the ‘secondary care’ service to create the capacity required to meet increased demand. The
anticipated success of working with Primary Care providers is likely to delay the need for the Health
Board to secure additional secondary care services with new providers.
Working with Optometry Wales, the potential of optometrists working in Powys is being developed.
This includes amending the pathways of care to enable GPs to refer routine and urgent (not
emergency) eye cases such as suspected cataracts to an accredited optometrist as opposed to a
consultant. This enables the optometrist to assess the patient, provide a diagnosis and undertake a
range of checks prior to a consultant’s involvement. The optometrist can also provide a range of
monitoring services for patients who have had cataract surgery or have glaucoma.
Action: The Health Board will work with Optometry Wales, to maximise the potential of optometrists working in Powys in providing services that reduce pressure on secondary care provision and provide a wider range of services closer to where patients live.
The role GPs and pharmacists play in identifying and supporting those who may benefit from an eye
health examination is also being explored. Being fellow providers of Primary Care services in local
communities, the aim is to strengthen the relationship between GPs, pharmacists and optometrists
to ensure patients make the best use possible of services aimed at reducing the longer-term effect
of conditions which could have been detected earlier through regular eye health examinations.

84
Action: The Health Board will work with GPs and community pharmacists to support patients being opportunistically advised of the benefits of regular eye health examinations.
Community Pharmacy Services Community pharmacies in Powys provide dispensing services, for prescribed medicines, to about
60% of patients in the county. This involves over two million prescription items, together with ‘over
the counter’ medicines and self-care advice to both residents and visitors to the area.
In addition to providing advice and support for the taking of medicines, community pharmacies in
Powys provide a number of other services. These include the provision of Primary Care Emergency
Medicines Boxes; care home medicines management support; and post-hospital discharge
medicines reconciliation reviews. They also undertake a number of important roles in supporting the
public health agenda, such as providing smoking cessation services, brief interventions for alcohol
abuse, and substance misuse services.
Our Plan for Primary Care Services for Wales1 sets out an intention to maximise the skills of those
working in community pharmacy to support the provision of prudent healthcare in relation to the
usage medicines; and in developing the community pharmacist’s role in promoting better lifestyles
to prevent ill health.
Furthermore, Your Care, Your Medicines(ref) signals an intention to focus pharmacy services on
delivering, in different settings, safe and effective patient care. A bid to the Invest to Save
programme has been successful in securing £0.4M of the £0.7M investment that the THB will make
to delivering the medicines projects in community hospitals identified in this section.
Action: The Health Board will provide additional support to patients being discharged from hospitals, to ensure that their medication is safe, appropriate, and used as the clinicians involved intended.
Action: The Health Board will develop and implement integrated pharmaceutical care models to deliver prudent healthcare in relation to the usage of medicines.
Action: The Health Board will work with Welsh Government on developing models for Pharmaceutical Needs Assessment.
Action: The Health Board will continue to work with Social Services, District Nurses and Allied Health Professionals to develop safe processes for medicines administration by carers supporting patients in their own homes.
Developing the Primary Care estate Primary Care services in Powys are delivered from a large number of separate sets of premises, all of
which are either privately owned or rented by the service provider using them. The NHS has
arrangements to provide support for premises used by medical practices, but not for the other
Primary Care providers: for these providers, the cost of providing premises is met from the general
income derived from their NHS contracts.
In many cases, Health Board employed staff occupy accommodation that is either owned or rented
by a medical practice. There are other premises too that are used by the Health Board’s community
staff. In total, the number of separate sets of premises used across Powys to provide health care
services is approaching 100.

85
There is clearly scope to rationalise the number of premises used, and in so doing, reduce the overall
cost (wherever it is met, be that by the Health Board or Primary Care provider) as well as improving
the quality of the environment as a benefit for both patients and those providing their care.
Across Powys, considerable investment was made in the Primary Care estate during the 1990s and
early 2000s. By contract, however, investment over the last 10 years has been limited.
Looking forward, opportunities exist to enter a new phase of premises development which reflects:
A need to address the on-going efficiency of maintaining the number of separate sets of
premises that are currently used across the county to deliver Primary Care services.
The fact that some Primary Care premises no longer meet current standards for room sizes.
The fact some Primary Care premises have limited space to meet current need, as well as future
needs as the range of anticipated services delivered through Primary Care expand.
The age and inefficiency of many existing Health Board premises and the opportunity to co-
locate with Primary Care providers in new purpose built premises where possible to do so.
Action: The Health Board will develop an estates strategy which, in addition to reflecting the future needs of Primary Care providers, will also reflect the needs of the Health Board generally and how they can both be combined to achieve maximum efficiency in the way the health care estate is provided across Powys.
Action: The Health Board will continue to support the development of a significantly improved Primary Care facility at Llanfair Caereinon, and smaller scale developments at Newtown, Welshpool, and Llanfyllin.
The need for change The planning horizon for a sustainable Primary Care service must stretch into the future beyond the
period covered by this IMTP. The Royal College of General Practitioners has published a report5 that
looks 7 years hence, to 2022. The report describes the challenges of the NHS in 2022 as follows:
An increase in the volume and complexity of health and social care needs, as more people live
for longer with long-term and often multiple conditions
The move to deliver more complex care in the community, as a means of both bringing it closer
to patients and their families and reducing costs
The squeeze on public-sector expenditure and the resultant need to find ways of transforming
services to reduce costs, while maintaining and increasing quality
Ongoing changes to the structure of health and social care
The potential for greater service fragmentation as a result of the use of multiple competing
providers and continuing barriers to better integration between health and social care
The challenge of promoting healthy lifestyles and behaviours, while engaging patients and
communities in supporting their own care and participating in shared decision-making
Growing health inequalities and the impact of these on services and the economy.
With these challenges as a backdrop, the report suggests that by 2022 patients will face more
complexity, more choice and more uncertainty and will rely on the expertise, skill and compassion of
their GP like never before.
In meeting these challenges, the report identifies a need for the medical practices of the future to be
working with groups of other practices and providers, as federated or networked organisations. Such
organisations permit smaller teams and individual practices to retain their identity, but combine
‘back-office’ functions, share organisational learning and co-develop clinical services.

86
Federated or networked practices will be well positioned to act as the provider arm of local
communities, working together to provide extended services (such as those currently defined as
enhanced services), as well as providing community nursing services and having GPs with extended
clinical roles.
The report goes on to envisage the service available in 2022 as one that can deliver:
Accessible, high-quality, comprehensive healthcare services available for all communities
A good in- hours and out-of-hours care experience for patients, carers and families
Patients and carers routinely sharing decisions and participating as partners
An expanded, skilled, resilient and adaptable general practice workforce
Investment in suitable community-based premises for delivering care, teaching, training and
research
Coordination and collaboration across boundaries, with less fragmentation of care
Reduced health inequalities and increased community self-sufficiency
Greater use of information and technology to improve health and care
Improved understanding and management of inappropriate variability in quality
More community-led research, development and quality improvement.
There is already evidence in Powys of medical practices wishing to work together. The four medical
practices that make up the South Powys GP Cluster have also declared their interest in formalising
the way they work together through the creation of an entity reflecting the principles of a social
enterprise.
Once established, the purpose of the new entity will be both inward and outward looking. By being
inward looking the new entity will undertake some of the back-room activities normally dealt with
by medical practices on an individual basis. This will build both efficiency and sustainability into
many of these functions, yet do so without undermining the ‘sovereignty’ of individual practices. By
being outward looking, the new entity will develop a solid governance foundation upon which to
position itself as a viable provider of health (and possibly social) care services which may not be
possible to achieve at an individual medical practice level. We have assumed usage of £0.050M from
the £30M to support the exploration of this model with the practices.
Action: Working in partnership with the South Powys medical practices, the Health Board will explore the creation of a new Social Enterprise.
The ambitions of the GPs in South Powys should be seen as the catalyst for similar developments
elsewhere in Powys. Although the principle role of the GP is recognised, the interest of other
professionals, health care staff and those of the local community generally should be encouraged to
ensure a board church of local interest and ownership for these new entities.
Action: Using the success of the South Powys experience as a platform, the Health Board will seek further expressions of interest from other groups of GPs in Powys with an interest in establishing a Social Enterprise and provide support their endeavours.
1Our Plan for a Primary Care Service for Wales (up to March 2018) – Welsh Government – November 2014 2Bevan Commission – Improving Primary and Community Health Care in Wales – December 2013 3Delivering Local Health Care – Welsh Government 4Setting the Direction – Primary & Community Services Strategic Delivery programme – Welsh Government – February 2010 5The 2022 GP – A Vision for General Practice in the future NHS – Royal College of General Practitioners – May 2013 6Together for Health: Eye Health Care – Delivery Plan for Wales – Welsh Government – 2013 7Together for Health: A National Oral Health Plan for Wales – Welsh Government – March 2013 8My Language, My Health: Inquiry into the Welsh language in Primary Care - Welsh Language Commissioner - June 2014 9Your Care, Your Medicines, Pharmacy at the heart of patient-centered care – Royal Pharmaceutical Society/NHS Wales - undated

87
Summary Plan 1: Primary Care
Primary Care Summary plan
Aim Strengthen the role of Primary Care providers in commissioning and delivering services closer to home and in the community
Current Status Current Primary care services consist of 17 Medical Practices; 23 dental Practices; 21 Optometric
Practices; and 23 Community Pharmacies
Objectives
1. Further develop patient access to sustainable and high quality Primary Care services across Powys
2. Support Primary Care to improve its ability to attract and retain health care professionals
working in Powys
3. Develop Primary Care’s role in the design of patient pathways
4. Strengthen the role of Primary Care as a local provider of care
5. Strengthen the role of Primary Care in the design and management of local services
6. Develop joint working between medical practices
7. Develop the Primary Care estate
Baseline Metrics
Number of different Enhanced Services in place as at 1st April 2015
17 practice development plans and 3 locality plans produced in 2014/15
No significant new Primary Care estate projects commenced in the last 10 years
Number of medical practices carrying a GP vacancy for more than 6 months as at 1st April 2015
Risks
Inability to successfully recruit to vacancies in the Primary Care workforce
Inability to transfer funding from Secondary Care to support service developments in Primary
Care
Progressively negative effect on medical practices of changes in their funding arrangements
Insufficient interest or capacity amongst Primary Care providers to support service
development opportunities in a Primary Care setting
Insufficient capacity/resources in the Health Board to adequately support GPs working
together in locality groups with their service change and development ambitions
Workforce, IM&T & Estates
Implications
Locally developed and funded action plan to support improved Primary Care workforce
recruitment and retention
Development of a clear action plan which sets out how, where and new funded technological
developments will improve the services available to patients being cared for in their own
communities and support those providing their care
Development of an integrated, locality sensitive, estates strategy which sets out how facilities
will progressively be improved, including at the Primary Care/Health Board interface
Related Welsh Government & Local Outcomes
Frameworks
Primary Care Plan for Wales
Bevan Commission – Improving Primary and Community Health Care in Wales
Together for Health Eye Care Plan – Delivery Plan for Wales 2013 to 2018
Together for Health – A National Oral Health Plan for Wales 2013 to 2018
Special care Dentistry in Wales Plan

88
Milestones
Task 15/16 16/17 17/18
Strong Leadership
Working in partnership with the South Powys medical practices, the Health Board will support the creation of a new Social Enterprise X
Using the success of the South Powys experience as a platform, the Health Board will seek further expressions of interest from other groups of GPs in Powys with an interest in establishing a Social Enterprise and provide support their endeavours
X X
Planning Care Locally
The Health Board to pro-actively support GP Clusters is the delivery of the actions identified as having the greatest priority in the GP Cluster Network Plans. These are as follows: X X X
- North Powys GP Cluster:
Improving & stabilising GP recruitment X X X
Develop an Enhanced Service for existing non-GMS activity required to be undertaken by medical practices X
Develop collaborative working with pharmacy X
Develop a local estates strategy for Primary Care X X
Establish a post of local cancer care co-ordinator X
- Mid Powys GP Cluster:
Increase the levels of successful recruitment and retention X X X
Review contracts and commitments for Enhanced Services X
Establish new model or the delivery of enhanced levels of community care via primary care providers X X
Secure improved diabetes care through care pathway changes X
Review individual practice viability and sustainability X X X
- South Powys GP Cluster:
Reduce incidence of DNAs at practice level by developing the use of texting appointment reminders X
Improve access to local diagnostic services X X
Re-establish local clinical services previously lost through non-replaced posts X X X
Establish same-day rapid access to secondary care assessment/advice to support people remaining in the community X X
Develop the concept of health and wellbeing centres in the Locality X X X
The Health Board will continue to develop the resources it provides, via the Locality teams, to support the development of GP Clusters. The Health Board remains focussed on the ambition set out in Delivering Local Health Services in terms of the advanced level of maturity which involves each Locality/GP Cluster achieving the following:
Devolved budgets in place
Robust governance and accountability arrangements in place
Hard evidence to demonstrate the delivery of agreed outcomes
X X
Improving Access & Quality
Working with the Mid and North Powys GP Clusters, the Health Board will work to introduce the Virtual Ward model which are sensitive the local needs in these two areas of the count X
Building on the work involving Bronllys and Newtown hospitals, the Health Board will work with local GPs to develop similar models of care in other parts of Powys, most notably in areas where current services are fragile or there are long distances to secondary care provision
X X
Building on work already commenced in South Powys, the Health Board will work with GPs to maximise the local delivery of diagnostic services where it is both safe and cost effective to do so
X X
Building upon the successful repatriation of funding in previous years, the Health Board will work to ensure the resources required to support a shift of care provision from secondary to a primary care/community setting are readily available
X X X

89
The Health Board will develop the Invest in Your Health programme and make it available to medical practices across Powys in support of the Lifestyle Local Enhanced Service X
Delivery of the HB’s Local Oral Health Plan will continue in 2015/16, with particular attention paid to developing the role of locally based and visiting dental staff, linking where necessary with the governance structures of partner secondary care providers
X
The HB will work with Optometry Wales, to maximise the potential of optometrists working in Powys in providing services that reduce pressure on secondary care provision and provide a wider range of services closer to where patients live
X
The HB will work with GPs and community pharmacists to support patients being opportunistically advised of the benefits of regular eye health examinations X
The HB will provide additional support to patients being discharged from hospitals, to ensure that their medication is safe, appropriate, and used as the clinicians involved intended X
The HB will develop and implement integrated pharmaceutical care models to deliver prudent healthcare in relation to the usage of medicines X
The HB will work with Welsh Government on developing models for Pharmaceutical Needs Assessment X
The HB will continue to work with Social Services, District Nurses and Allied Health Professionals to develop safe processes for medicines administration by carers supporting patients in their own homes
X
The HB will develop an estates strategy which, in addition to reflecting the future needs of Primary Care providers, will also reflect the needs of the Health Board generally and how they can both be combined to achieve maximum efficiency in the way the health care estate is provided across Powys
X X
The Health Board will continue to support the development of a significantly improved Primary Care facility at Llanfair Caereinon, and smaller scale developments at Newtown, Welshpool, and Llanfyllin
X X
Equitable Access
The HB will support Primary Care providers to regularly assess the appropriateness of their hours of availability and their ability to understand and meet the needs of their patients X
The HB will continue to develop its relationship with Shropdoc and in so doing maintain access to sustainable Primary Care services in the county. This will include exploring further the role of clinically-led telephone triage in the delivery of in-hours General Medical Services
X
During 2015, the Health Board will work with its GP Clusters to consider the finds of the Welsh Language Commissioner’s report and in particular their response to the Welsh Government’s requirement as set out above
X
A Skilled Local Workforce
The HB to ensure, via the Primary Care Workforce Group, the development and implementation of an action plan which reflects a range of initiatives to assist Primary Care providers in securing a sustainable workforce for the future
X X X

90
Medicines Use & Prescribing
Medicines are a valuable and effective means of delivering treatment for many patients. They also,
often, offer the most convenient and accessible option from the range of therapeutic choices. Over
70% of treatment regimens include medicines as an important element in treating or delaying
progression of serious disease. Development in medicines and therapeutic use is constant, leading to
therapeutic improvements and often increasingly complex regimens. The Powys population is
increasingly older with associated frailty, and has both an increased need for medicines, and
increased sensitivity to their unwanted effects. Dementia poses increasing challenges to safe choice
and use of medicines.
Medicines, and prescribable non-medicines, in Powys, account directly for almost £24M of Powys
THB spend and approximately a further £5.5M in secondary & tertiary care provision by providers
outside Powys. Ongoing developments in treatment, and newer, higher cost drugs, will improve
patient care, but also increase medication costs.
It is essential that medicines are handled safely and securely, and that appropriate choices are made
in maximising benefit while minimising cost and harm. Challenges in reconciling needs of
practitioners, patients, and the NHS, while balancing acquisition costs against patient care packages
and care pathway costs, need continued vigilance and review.
Medicines Management Strategy in Powys has the following priority goals:
Improving patient safety, and empowerment, reducing risk of harm related to medicines;
Improving the effectiveness of medicines use, leading to better care and better value;
Identifying and implementing cost savings in medicines choice and delivery;
Improving the appropriate use of available skills and resources to optimise medicines use;
Supporting Community Pharmacy deliverable Health Lifestyle Activity that reduces health risks
for people and avoids the need for future NHS intervention.
To meet these goals, over the next three years and beyond, the Powys Medicines Management
Team will work on engagement and activity with patient groups, professionals, voluntary
organisations and health and social care providers to Powys residents, consolidating current
achievements and aspiring to aid Powys becoming a leading Health Board in:
Minimising avoidable NHS interventions resulting from medication issues;
Minimising harm related to medicines;
Integrating pharmaceutical care across all health and social care sectors;
The availability of expert advice and guidance on medicines;
Meeting patient desired outcomes through safe effective medicines choice and use of medicines;
Empowering patients in understanding, and effectively using prescribed medicines, and in
choosing and using medicines for their self care;
Supporting effective (patient centred) medicines adherence;
Developing carer, dementia friendly, support mechanisms for prescribed medicines;
Developing innovative services for patients on medicines, or needing healthy lifestyle support,
that are deliverable through pharmacy (such as smoking cessation, alcohol brief interventions);
Efficient provision of prescribable non-medicines (e.g. dressings, appliances, food supplements);
Use of automation, and ‘at a distance’ technology, to safeguard patients and practitioners and
improve efficiency and effectiveness, and to support patient medicines use and experience;
Improving patient centred pharmaceutical care, safe and effective use of medications
and prudent prescribing

91
Skilling staff across settings in safe and secure medicines systems, administration and use;
Supporting wider use of Independent Prescribers;
Minimising avoidable medicines expenditure (taking a whole system view) to release money for
other aspects of patient care;
Obtaining value for money from medicines related treatments delivered by provider
organisations in England and Wales.
As illustrated below, the Health Board has the lowest, age weighted, prescribing costs in Wales.
Further improvements in patient centred use of medicines has opportunities for significant overall
savings to the THB, with improvements in use of nutritional supplements, and hydration, and further
savings from efficiencies in other prescribable non medicines.
The outcome of these planned approaches will help to meet the prudent healthcare agenda, support
antimicrobial stewardship, and minimise the risks of avoidable harm for patients.
Figure 40: Prescribing Costs of Health Boards in Wales
To support activity improving quality service provision to patients, there are some specific
infrastructure and compliance activities that need to be undertaken, including
re-provision of medicines supply to Powys provider units to comply with WDA changes
Re-design of pharmaceutical care provision to inpatients, including support for discharge and
other transfers between settings, and infrastructure for self administration.
provision of mental health pharmacy support
development of pharmaceutical services for patients in domiciliary & care home settings
100000
110000
120000
130000
140000
150000
160000
M…
Ju…
N…
M…
Ju…
N…
M…
Ju…
N…
M…
Ju…
N…
M…
Ju…
N…
M…
Ju…
£ P
ER 1
00
0P
U P
ER Y
EAR
, TO
MO
NTH
:
C O S T P E R 1 0 0 0 P U , H E A L T H B O A R D S T O A U G U S T 2 0 1 4 Cwm Taf
Aneurin Bevan
Abertawe BroMorgannwg
Hywel Dda
BetsiCadwaladr
Cardiff AndVale
PowysTeaching
Workforce Implications
•Skilling staff, and carers, in safe and secure medicines systems, administration and use
•Increased numbers of independent prescribers
•Increased pharmacy professional support to hospital and care home settings
Capital & Estate Implications
•Increase access to and use of remote communications
•Automated medicines supply systems
•Clinical Pharmacy remote support system for wards
•Ward based infrastructure for patient empowerment
•Wholesale Distribution Authorisation compliance
Finance Implications
•Prescribing savings are planned
•Savings for NHS provision from improved medicines use
•Increased pharmacy professional time, in carer support and ward based support

92
Summary Plan 2: Medicines Use & Prescribing
Medicines Use and Prescribing Summary plan Aim Safe, effective and efficient use of medicines, with supported and empowered patients
Current Status
Over 3M prescriptions are dispensed in Powys, every year, growing at 5% per year
Prescribing is of good quality, but with variation between practices
Community pharmacies not all engaged in enhanced service provision
Insufficient support to nursing and medical staff in Powys managed provider units
Risks to medicines access through changes in application of legislation, and changing provision from supplying DGHs
Prescribing costs are amongst the lowest in Wales, with the lowest cost per patient, when weighted by age
Wasted medicines are still an identifiable problem, with a potentially very significant impact on the health of patients who are consequently not receiving treatment, through poor adherence
Domiciliary carer medication support is challenging to achieve, across Health and Social care interfaces, and currently not always following agreed policies, putting patients at risk
Powys prescribers prescribe lower number of antibiotic prescriptions than average for Wales, but significant variation exists between areas, and usage is higher than average for UK
Powys prescribers use fewer hypnotics and anxiolytics than average in Wales, and also fewer anti-depressants
Care homes get very limited pharmaceutical input, but have more beds than our hospitals
Limited independent prescriber development
Objectives
1. Maximise the benefits from medicines for Powys residents
2. Minimise the harms from medicines for Powys residents
3. Integrate pharmaceutical care to minimise issues at changes in care setting
4. Minimise risks of avoidable admission, relating to medicines
5. Develop optimum access to medicines and pharmaceutical care, as determined by pharmaceutical needs assessment
Baseline Metrics
Performance against AWMSG indicators
Performance against prescribing budgets
Numbers of Medicines Usage Reviews undertaken
Numbers of medicines related admissions
Numbers of medicines related incident
Numbers of medicines supplied through all managed routes
Proportion of Pharmacies utilising each enhanced service
Performance against AWMSG indicators
Risks
Supply of medicines to wards may be disrupted without mitigation work being done
Prescribing costs will increase rapidly if GPs are unable to manage increasing demands, and make less than optimally efficient choices
Without increasingly close working with social services medicines issues in community may result in increased DTOCS, avoidable admissions, and/or overwhelming the DNS workforce
Identified insufficient support in Powys hospitals may lead to sub-optimal care in not corrected
Capacity and resources to implement plans may not be available
Workforce, IM&T & Estates
Enablers
Develop pharmacy systems to permit exchange of relevant information
Develop wireless capacity on wards for clinical systems
Maintain compliance with appropriate building regulations for medicines storage etc.
Ensure safe Medical Gases installations and training is in place
Related Welsh Government & Local Outcomes
Frameworks
Your Care Your Medicines 2014
Royal Pharmaceutical Society Hospital Standards
Trust to Care report

93
Milestones
Task 15/16 16/17 17/18
1. Minimise harm from medicines Plan/Pilot Implement Ongoing
Powys formulary choices updated
Support process mapping and system redesign for medicines safety on wards
Increase pharmacy involvement in MDTs
2. Maximise benefits from medicines
Review Current Planning with Social Services
Plan/Pilot
Implement
Introduce Common Conditions Formulary for ‘Choose Pharmacy approach’
Test alternatives Identify funding, begin implementation
Ongoing
Develop systems for medicines reconciliation and adherence review in community pharmacies Ongoing
Develop support for domiciliary carer medication management
3. Develop in-house integrated pharmacy service, strengthening pharmaceutical input to key areas Plan/identify funding Begin implementation Implement services
4. Medicines distribution system based in Powys Plan Implement Ongoing
5. Develop community pharmacy services to reduce impact of population changes on General Practice Pilot Implement Ongoing
6. Introduce MTeD to Powys hospitals Pilot Implement Ongoing
7. Research on effective support for adherence for patient population in Powys Panning/pilots Bid for funds Implementation
8. Develop safer systems for pharmacy medicines chain Process mapping, planning
Continue implementation
Ongoing
9. Further develop support for Non-Medical Prescribing Identify needs Establish support mechanisms
ongoing

94
7.2. EXCELLENT COMMISSIONING
Commissioning is a term often used interchangeably with contracting, purchasing and procurement.
Commissioning provides the context in which contracting, purchasing and procurement take place
and is defined as
“the process of identifying needs within the population and of developing policy directions, service
models and the market, to meet those needs in the most appropriate and cost effective way.” (The
Institute of Public Care)
Strengthening commissioning is a key strategic objective for the Health Board to
Ensure there is sufficient capacity to meet the need for healthcare services across the
community and hospital system, with a shift to prevention and early intervention.
Embed an innovative and prudent approach to service commissioning with the patient at the
centre.
Provide assurance on the quality and efficiency of healthcare services across the healthcare
system.
PTHB has responsibility for commissioning all healthcare services for the Powys population. The
remit includes:
Securing primary care services from local primary care practitioners, usually independent
contractors.
Securing local community and community hospital services. These services are provided by the
Health Board.
Securing appropriate secondary care services from District General Hospitals around the
periphery of Powys.
Working with WHSCC, developing a specialised services commissioning plan to meet the needs of
our population.
Working with the Emergency Ambulance Services Committee (EASC) to agree and deliver the
Emergency Ambulance Services Commissioning Plan.
The following diagram illustrates the complexity of our commissioning arrangements.
Commissioning sufficient capacity to meet the need for timely and high quality
healthcare services across the community and hospital system, with a shift in emphasis
to prevention and early intervention
Embedding an innovative and prudent approach to service commissioning focused on
patient outcomes
Providing assurance on the quality and effectiveness of healthcare services across the
healthcare system

95
Figure 41: PTHB Commissioning Arrangements
Review of Current Commissioning Arrangements In order to develop a strengthened approach to commissioning across the organisation, the Health
Board initiated a review of our current commissioning arrangements to inform the design and
content of our Commissioning Development Programme. The review was undertaken during 2014.
The high level objectives of the review were:
To design an agreed commissioning model for Powys THB that is based on best practice and:
Provides the health care services required by the population;
Ensures commissioning services will be clinically led;
Involves collaborative working with partners to exploit opportunities for integration;
Encourages long term strategic partnerships with providers;
Reinforces the delivery of a financially sustainable position;
Supports the development of organisational capability and capacity, including GP commissioning
leadership;
Provides effective and robust contracting with monitoring arrangements to ensure performance;
Provides assurance to the Board and the public that there is a comprehensive commissioning
framework in place;
System of commissioning, securing and reviewing services.
To inform our future strategic approach to commissioning, a literature review of the current
evidence base to identify best practice models and to confirm what world class commissioning looks
like was completed. Against the evidence base, the current arrangements were analysed to identify
gaps and opportunities for improvement. The review identified some examples of good practice in
Powys particularly in relation to mental health services and the work to redesign stroke services. The
review concluded in February 2014 confirmed the following recommendations:
A Commissioning Development Programme will be established to take forward the
implementation and design of the revised commissioning model in Powys;
Establish an Assistant Director of Commissioning post to increase capacity and to strengthen
leadership arrangements;
Strengthening our commissioning arrangements by re-establish a Commissioning Board;
Establish a Commissioning Development Programme to confirm the future design of the
commissioning model, ensuring alignment with the revised organisational structure;
62.99
60.18
41.26
49.53
29.31
12.53.71
Annual Spend £M
Services provided in Powys
Primary Care
Welsh Providers
English Providers
WHSCC
CHC
Voluntary/Independent

96
Review and develop the Health Board’s Commissioning Strategy and Framework including
revised processes and supporting tools;
Build capacity and capability by investing in and OD/training programme to build the
commissioning expertise within the organisation;
Work with Powys County Council to further strengthen the joint commissioning arrangements of
community support services, and consider potential of integrating some commissioning
functions;
Deloitte tested the financial position and plans of the Health Board in 2013 and concluded that “the
welsh tariff system makes life difficult for the Health Board” and that local tariffs are opaque and
make it difficult to manage providers. The Health Board is working with Welsh Government and
Welsh Health Boards to develop all Wales commissioning system rules that enables intelligent
commissioning.
The Health Board are establishing the Commissioning Board with immediate effect, initiated the
recruitment process for the Assist ant Director of Commissioning post and are currently scoping the
Commissioning Development Programme for approval by the Transformation Programme Board in
May 2015.
Commissioning Development Programme The Commissioning Development Programme will confirm the future commissioning model of the
Health Board to deliver a rational outcome based system for planning and commissioning within
Powys THB that will strengthen the THB’s capacity to systematically plan and commission services on
a strategic basis.
The two diagrams below illustrates the planning and commissioning cycle as a process that involves
analysis, design, delivery and evaluation as part of a dynamic process that needs to draw on a range
of skills and expertise across the organisation.
•procurement
•contracts
•powys provider change
•de-commissioning
•outcomes
•system performance
•contract monitoring
•clinically led
•stakeholder engaged
•powys vs local
•priorities and cost
•board approved
•need
•demand: spend
•policy/ evidence
Analysis Design
DeliverEvaluate
Figure 42: Planning and Commissioning Cycle

97
This is further illustrated by the diagram below that illustrates the key stages and tasks and skills
required in a mature planning and commissioning system.
Assessing needs – understanding health care needs for a population or service area.
Reviewing services and gap analysis – reviewing services currently provided across Powys
Provider and External Providers and partners including the third sector and specialist services
where appropriate in terms of reflecting on both volume and quality.
Risk Management – understanding the key health and health care risks and deciding on a
strategy to manage them.
Deciding priorities – given a list of desirable actions, using available evidence of cost
effectiveness and based on a robust and defensible ethical framework, prioritise areas for service
development and disinvestment.
Strategic options – using the PTHB Commissioning framework to bring together all the available
information to outline how the THB will deliver all its core objectives.
Procurement – put those strategic plans into action through procurement or other appropriate
mechanisms to secure services.
Provider development – support provider improvements or introduce new providers to deliver
services required (including setting up demand management systems and designing new care
pathways). This includes supporting providers in decommissioning of services where
appropriate.
Managing provider performance – monitor and manage the performance of providers against
their contracts, especially against KPIs.
Core Principles – Commissioning Model The model will support the clinical leadership role of Primary Care in respect of commissioning to
meet the needs of residents. The development of local primary care based clinical leadership,
supported by specialist advice as required has already been a significant step in driving change, and
this will be maintained and strengthened. The changes are based on a number of core principles:
Planning and commissioning will be the core approach to the planning and delivery of service
change and the need to embed the commissioning cycle into the routine business of the
organisation;
The development of partnering arrangements to secure commissioning and change;
Assessing Needs
Reviewing service and gapanalysisRisk Management
Deciding Priorities
Strategic options
Procurement
Provider development
Managing provider performance
Figure 43: Key Stages, Task and Skills of Commissioning and Planning Cycle

98
Clinically led outcome based service frameworks are required at a Powys level, across key areas:
mental health; acute services; children; dental and cancer etc.; from which local services will
develop;
Service plans will be supported by robust capacity and demand modelling;
Plans need to reflect both local issues and national plans and will be both prepared and delivered
by integrated teams that include key skills in public health; clinicians; strategic and service
planning; contracting; performance; finance; information and workforce;
The need to demonstrate stakeholder and user engagement in change plans;
Finance, workforce, IM&T and estates plans will be derived from clinical service frameworks;
Delivery of plans at local level through both direct delivery and contract arrangements with
providers;
Annual cycle of review and updating within a three year rolling context.
Commissioning Partnerships Increasingly commissioning will be a joint endeavour with Powys County Council and other potential
commissioning partners at local, regional and national level, for example EASC and WHSCC.
The nature and opportunities afforded by cross-border commissioning arrangements will also be
explored, and work to review all Wales system rules progressed to support the Health Board to
deliver its commissioning vision and intentions.
Commissioning for Quality Quality and safety improvement is a golden thread underpinning our planning and commissioning
processes. The Health Board is strengthening links with commissioners providing services to Powys
residents. Progress has been made with our English providers and quality monitoring has been
strengthened in 2014 with formal links with clinical commissioning groups and individual providers
and this will continue going forward. An overall quality framework for commissioned services will
now be introduced across all providers.
However, we recognise we need to put arrangements in place with our Welsh providers to ensure
that we gain assurance on the quality and patient safety of services they provide. Alongside this
assurance on specialist services will be reported to our Board through the Welsh Health Specialised
Services Committee strategic quality framework and assurance on Emergency Ambulance Services
will be reported to our Board through the Emergency Ambulance Services Committee. Focusing on
safety, effectiveness, experience and leadership a suite of high level indicators will provide
assurance on services commissioned on our behalf. This will link to strengthening the capability and
systems around commissioning for quality for both Welsh and English providers, care homes and
primary care.
Work is being taken forward to develop our commissioning performance framework and escalation
plan which sets out the requirements within the long term agreements and who and how we will
monitor provider performance; whether it is being achieved and associated escalation points. The
framework setting out a step-by-step process to source quality and patient safety information and
providing assurance will be piloted throughout 2015. The Medical Director will also be leading a
programme of work to develop and implement a primary care quality dashboard in Powys (including
down to Practice level) during 2015/16, based on emerging national policy and guidance and other
local experience to date.
In driving this agenda steps are being taken to put in place increased capacity and capability through
the appointment of a senior clinical quality and patient safety analyst whose role will focus on the
identification of trends emerging from quality and patient safety data across all commissioned

99
services and the Health Board’s provider services. This in turn will underpin learning and
improvement and build organisational assurance.
Peer review of ward and department areas has progressed over the past year. Operational peer
review visit have been trialled as part of our response to the Trusted to Care report, in addition to
executive and independent member ’15-step challenge’ walk-rounds, which are now embedded
within Powys.
The commissioning, contracting, and performance process will also incorporate and demonstrate
performance against the Welsh Government Quality Plan and the Performance Framework and
incorporate action to deliver against the Together for Health Plans. Compliance of commissioned
and provider services against key standards including compliance against the Welsh Language Act
will be monitored.
The THB is strengthening the planning and commissioning function such that this becomes the key
driver of change across local systems of care. The skills and expertise to support planning and
commissioning within the organisation will be organised and strengthened to most efficiently deliver
the scale of transformation that is required.
Specialised Services Commissioning The Integrated Plan for Commissioning Specialised Services for Wales 2015-18 has been structured
to support the delivery of the NHS Wales Specialised Services Strategy i.e. “to ensure equitable
access to safe, effective, and sustainable specialised services for the people of Wales.”, and to
ensure that the planning of specialised services is consistent with the Institute for Healthcare
Improvement “Triple Aim‟ to:
Improve the health of the population;
Enhance the patient experience of care (including quality, access, and reliability); and
Reduce, or at least control, the per capita cost of care.
A key feature of this plan is the integration of:
7 Health Board plans for commissioning local services (collaboratively along the patient
pathway); and
Provider plans (Health Boards, NHS Trusts in Wales and England).
As well as:
Quality (including patient experience and outcome);
Activity volume (to meet agreed targets);
Finance (including cost and affordability).
The plan highlights the key priorities for specialised services for Welsh patients over the next three
years, together with the financial implications, and key risks to delivery. The key priorities for the six
programme areas are set out in the following work programmes:
Mental Health
Cancer and Blood
Cardiothoracic
Neurosciences and Complex Conditions
Renal
Women and Children.

100
The plan is underpinned by detailed work plans for each of the programme areas, and a three year
financial plan. In addition to setting out the priorities and work plan for WHSSC over the next three
years, the plan also describes the WHSSC commissioning process.
The Specialised Services Commissioning Plan has been prepared across the seven health boards in
Wales and Powys has been fully engaged in both the development of the plan and its approval
through the WHSSC Joint Committee.
The WHSSC Plan specifically for Powys takes account of:
A significant proportion of the pathways for specialised services for Powys residents flow into
England, especially for the north and the west of the county: as a consequence Powys bears a
significant financial risk as a consequence of the volatility of these small but expensive pathways.
The financial plan reflects the forecast financial out turn of activity for Powys residents in
specialised services that has grown at a greater rate than primary or secondary care services
To offset investment requirements to accommodate growth, the THB will actively support the
implementation of the WHSSC Commissioning Framework following the service prioritisation
exercise
Commissioning to meet the Welsh standards for waiting times and other key targets and
standards for Health services
The THB will seek to take local action with WHSSC to actively manage patient pathways into the
most appropriate pathways through the development of decision gateways in provider
organisations: Powys residents are frequently onwardly referred to tertiary services by our
secondary care providers. New opportunities include to the soon to open Children’s Hospital for
Wales
The THB will support the commissioning of key service developments already committed to
through the joint committee, or by Welsh Government including the roll out of the Emergency
Medical Retrieval Service and Bariatric Services across the pathway
The THB will continue to work with the other Health Boards in Wales to gain best value through
its commissioning arrangements for secure mental health services and provision of CAMHS
services.
Specialised services are a significant component of the THB’s expenditure accounting for 10% of the
overall budget of the Health Board. Our service and financial strategy supports the work being
commissioned via WHSSC and to this end our financial plan for 2015/16 includes £29.1M funding for
WHSSC. At the time of preparing this plan, this figure is £0.350M less than the plan prepared by
WHSSC, but includes substantial investment to deliver against previous year’s performance ad cover
additional commitments made in the WHSSC plan. This is because the Health Board has provided a
clear message to WHSSC of the affordability of the plans prepared and our expectation of specific
actions we expect to be taken in respect of our population. We have noted this difference as a risk in
our financial plan. The THB will also be investing in additional capacity to work across the THB and
WHSSC commissioning process to undertake a detailed analysis of patient flows into England and act
on opportunities to manage costs. Developing the commissioning capacity of the Health Board,
linked to the implementation of the Commissioning Programme will be a significant development in
the implementation of this IMTP.
Rare Diseases In 2008 the UK agreed with the other Member States of the European Union to develop a national
strategy for rare diseases. The UK Rare Diseases Strategy was launched on the 22nd November 2013,
with the aim that it will be fully implemented by 2020. Within the UK, each nation has been required

101
to develop an implementation plan for achieving this aim. The Welsh implementation plan was
issued in December 2014.
The plan provides a framework for action by Health Boards, NHS Trusts, WHSSC and their partners in
local government, the third sector, the education and research communities and industry. It sets out
the Welsh Government’s expectations of the NHS in Wales to tackle rare diseases for people of all
ages, wherever they live in Wales and whatever their circumstances. The Plan is designed to enable
the NHS to deliver on its responsibility to meet the needs of people at risk of, or affected by, such
conditions. Powys THB will work through WHSSC to respond to the Rare Diseases Plan.
Commissioning of Ambulance Services Following the publication of the Mclelland Review in Ambulance Services in Wales, the Minister of
Health and Social Services has established the Emergency Ambulance Services Committee,
supported by the Ambulance Services Commissioner through which Health Boards will discharge
their commissioning responsibilities. These arrangements have been put in place in 2015 and the
THB will need, alongside other health boards in Wales, to rapidly specify its service requirements in
respect of emergency ambulance services. The THB also commissions significant volume of non-
emergency patient transport from the Welsh Ambulance Service.
There are a number of factors will affect how the THB will specify the service that it requires for
residents of Powys in the future including:
Setting response times appropriate to the rural and topographically challenging nature of Powys;
Ensuring the best outcomes for patients with time critical injuries and illnesses such as major
trauma, stroke and myocardial infarction;
Flow of ambulances out of the area, and the relationship between existing services and the
Emergency Medical Retrieval and Transfer service;
Managing increased on demand ambulance services through appropriate assessment referral,
and conveyance pathways, including increasing activity to Powys facilities;
Developing a workforce appropriate to the demands of Powys, working in partnership with local
services;
Planning and locating resources to most optimally meet demand.
Ambulance performance for Powys is currently below expected targets, however simply focussing
on this target will not improve patient experience of ambulance services and a more comprehensive
approach that considers the whole context of care is required. Work is progressing between the
Health Board and WAST and together working with other Health Boards as part of the Emergency
Ambulance Services Committee we will continuously improve the unscheduled care system. The
approach to commissioning of emergency ambulance services will be aligned to our overall
unscheduled care plan.

102
A dedicated Commissioning Support Unit for EASC to support the substantive appointment of the
Commissioner will be completed by the 2015/16 financial year. A Quality and Performance Review
Group comprising senior officials from all Health Boards has been established to oversee short term
delivery and to support WAST to improve current performance. Powys THB’s own strengthened
commissioning arrangements will also enable an enhanced and accelerated approach to
commissioning this services, and our plans include a modest additional investment in this service this
year.
The key priority for the Health Board is to ensure the implementation of successful and effective
commissioning arrangements under the EASC arrangements. A Collaborative Commissioning Group
has been established to develop the longer term commissioning strategy for emergency ambulance
services and we are currently working on a new Commissioning and Clinical Quality Delivery
Framework for 2015/16. We have made provision within our financial plan to fund the
establishment of the new commissioning arrangements at a cost of £0.026M per annum and a
further £178k, which relates to potential investment requirement for emergency ambulance services
pathway. The performance profile for ambulance response times currently performs well below 55%
and the THB has aspirations to achieve the 65% within a two year timeframe, with a year 1 target of
60%. The plan to achieve this is a combinations of more robust commissioning and performance
management of WAST through the specific needs of Powys residents, and the delivery of local
actions set out in our unscheduled care plan.
Figure 44: WAST Performance for Powys

103
7.3. INTEGRATED WORKING
Strategic Drivers There are clear drivers and opportunities for change that leads to real improvement for the citizens
of Powys through the integrated working of Powys teaching Health Board and Powys County
Council, in the context of wider multiagency collaboration. These include:
The Public Services Commission (Williams 2014);
Devolution, Democracy and Delivery (Welsh Government 2014);
Powys One Plan (Powys Local Service Board 2014);
Powys teaching Health Board Integrated Medium Term Plan (2014);
Primary Care Strategy (currently out for comment) (Welsh Government 2014);
Social Services and Wellbeing Act (2014);
Wellbeing of Future Generations Bill (2014).
There is real potential to deliver by working together a Powys that is a better place to grow up, work,
play, grow old and thrive.
Moving forward from a place of strength Powys teaching Health Board and Powys County Council are already co-terminous organisations,
serving the same population, largely experiencing the same challenges and opportunities of the
sparsely populated, highly rural county. The organisations have a track record of working together to
develop services for the people of Powys and have a history of working with communities and other
stakeholders/partners to deliver improvements. Such examples include:
The council and health board share ICT services with integrated email and backroom
functions to improve efficiency and reduce budget pressures. By combining resources and
increasing our critical mass we have been able to keep services within Powys and to improve
the quality of our existing services.
Community Resource Teams and Virtual ward developments have enabled a joined up
approach to support people in their own homes. This has brought direct benefits to the
people of Powys by reducing unnecessary admission to hospital and enable a return to
independence more swiftly wherever possible. This type of direct service is supported by a
Joint Community Equipment services that itself has a section 33 agreement (pooled budget)
and accountability arrangements in place.
The Children, Young People and Families agenda supported through the Children and Young
People’s Partnership has for a number of year been joined up, with integrated
commissioning working effectively in for example delivering schools based counselling
services as just one of the services established in this way.
Matching Actions to Ambitions - One Powys Plan Priorities (2014-17) The Local Service Board has continued to develop with active leadership from the range of public
sector organisations including Powys County Council, Powys teaching Health Board, Dyfed Powys
Police, Powys Association of Voluntary Organisations and other key partners. The result of this
• Placing the citizen at the centre of integrated service delivery through joined up
systems, processes and teams, delivered at neighbourhood level
• Developing integrated approaches to support systems and functions across all areas of
our shared business with Powys Council
• Putting in place joint strategy, governance and scrutiny arrangements with Powys
Council

104
collaboration is the ambitious One Powys Plan – a public services plan for improving Powys (2014).
The One Powys Plan and this IMTP are in alignment with a shared vision of working together to meet
the needs of Powys citizens.
The One Powys Plan provides the platform to delivering better outcomes with and for the people of
Powys and is structured around 5 key areas:
Integrated Health and Adult Social Care
Older People will be supported to lead fulfilled lives within their communities;
Carers have a good sense of wellbeing and are able to fulfil the caring responsibilities they
choose to do;
Powys citizens will lead fuller and longer lives, be resilient, have good health and be more able to
participate and contribute to their communities.
Children, young people and families
The needs of vulnerable children, babies and their families are identified as early as possible so
that they can enjoy safe and fulfilled lives;
Powys citizens will be supported and empowered to lead active and healthier lives.
Transforming learning and skills
All children and young people are supported to achieve their full potential;
More young people in Powys will be in full time education, gainful employment or employment
related training within the county.
Stronger, safer and economically viable communities
Bringing people together in Powys so they feel that they matter. Belong and can contribute to
their community;
Improving passenger transport services to enable them to be affordable, accessible and efficient.
Organisation and partnership development
Enabling ‘joined up’ services for Powys citizens through public and third sector partnerships;
Seeking to maximise capacity and efficiency, shared values and working together to integrate our
approach for example by sharing corporate and infrastructure support services; these services
are relatively invisible to the public, but efficiencies realised by working together will be re-
deployed and invested in front line care and support services.
Powys Teaching Health Board and Powys County Council’s Integration Agenda Powys County Council and Powys teaching Health Board have particular opportunities to integrate
more services under the umbrella of the One Plan, and in support of the One Plan through more
effective and sustainable use of resources. The benefits of integration therefore are focused on the
following key areas and priorities:
1. Integrating Front-line Services Integrated Care for Older People (including Integrated Primary Care) – focused on well
coordinated preventative and responsive care at a locality/cluster/neighbourhood level;
Emotional Wellbeing and Mental Health (integrated models for delivery across the
whole continuum of care – from primary care through to specialist services);
Integrated commissioning and delivery of services for people with a Learning Disability;
Integrated Commissioning and delivery of support for Carers;
Integrated Public Protection and Safeguarding service (all age, all safeguarding areas);
Integrated Commissioning for Care Homes/Home Care (across the age range);
Integrated Childrens services for Children with Disability (including Child and Adolescent
Mental Health).

105
2. Integrating Professional & Business Services Corporate and support functions;
Estates and asset management;
Public/community engagement;
Information Governance.
3. Organisational and Integration Development Integrating quality and service improvement approaches;
Integrated workforce planning, including flexible approaches to sharing staff;
Integrating education, training and development, including leadership development;
Joining up scrutiny and assurance – specifically around integrated service provision and
pooled budget arrangements – utilising existing Joint Partnership Board arrangements
where possible;
Integrating information governance and record keeping.
Realising the Potential – unlike any other It is essential to recognise that the scale and complexity of integration between two fundamentally
different bodies requires significant investment and commitment locally and from the Welsh
Government. The proposed merger outlined in the Commission on Public Service Governance and
Delivery is unlike any other integration seen elsewhere as it moves both beyond a merging of two
‘like’ organisations which have largely similar functions, services and governance; and beyond a
merely health and social care integration, understanding that the potential benefits to the people of
Powys extend beyond this into the wider public sector areas such as education and learning,
economic vibrancy, and leisure and wellbeing services.. Reducing complexity is essential, easing and
removing organisational barriers, actively assisting both organisations to move to a place where the
traditional norms of either local government or national health might be blurred or eased. It is only
expected therefore that such a change would require focused effort and resourcing to enable the
commitments to become reality and both organisations submitted an expression of interest to the
Welsh Government outlining the capacity and resource requirements needed to take forward our
agenda. The combined bid was valued at £0.950M over 2 years. The Health Board has assumed 50%
funding will be routed through the organisation and as such has built it into the plan for the next 2
years, but is subject to response and commitments made by Welsh Government.
Governance and Guiding Principles The existing governance arrangement for the One Powys Plan provides a platform to progress the
majority of the areas of integration described, however additional capacity and capability,
modifications and additions to governance and accountability arrangements will be required as the
agenda progresses.
A number of key principles are guiding our integration agenda and these determine the process and
transition issues that will need to be managed:
Principles The extensive work undertaken in developing and delivering the One Powys Plan remains
the foundation of integrated working.
Opportunities for further integration (above that cited in the One Powys Plan) are focused
on areas where there are clear benefits for citizens of Powys.
Integration work will be taken forward within the existing legal frameworks, whilst working
with others to explore the potential for other organisational/legal models.

106
Success will be recognised and celebrated, and learning form a key part of the ongoing
development of integration.
The key process issues therefore are:-
Identifying where the oversight for the whole integration (between Powys teaching
Health Board and Powys County Council) sits. Currently much of the Programme is
within the Local Service Board. There is potential to modify the Joint Partnership Board
that currently exists between PCC and PTHB to govern this work, linking through to
sovereign bodies (Board/Council).
Establishing sufficient leadership, management and support capacity to enable
integration areas to progress at pace.
Implementing an OD programme that equips and galvanises staff to drive forward
integrated working.
Establishing a clear route for sharing progress and outcomes of integrated working.
Working with Government and others to understand the potential models for
organisational form and function in the future.
Rising to the Challenge of the Integration journey The leadership teams across both organisations recognise the scale of the journey ahead. The
leadership and support for change is a critical success factor with a collective leadership approach
emerging. Key elements include a focus on:
Connecting People to Purpose – helping all staff to identify and realise the benefits
integrated working will deliver for the citizens of Powys.
Engaging staff in the development of the priorities set out and their translation into action,
engendering a relentless focus on delivery.
Clarifying the commitments and priorities that can be achieved, the boundaries within which
work takes place (reducing complexity) and the areas where priority will not be given in
order to best manage the capacity and capability that exists.
Prioritising the Integration Partnership - It will be important for Powys to be seen as a region
in its own right, both focusing on the co-terminosity and integration, whilst selecting key
broader partnerships (such as regional working) to progress areas where benefit is clear for
Powys.
Ensuring that integrated working involves the citizens of Powys and focuses on improving
outcomes, through innovation and improvement.
Building capacity - ensuring staff are equipped with the tools and resources needed to make
things happen.
Learning - developing transparent evaluation, assessing and measuring progress on the
journey, its impact and outcomes.
Accountability – finding ways to enable accountability to work across both organisations
within the current legal framework, enabling transparency and openness.

107
8. SERVICE DELIVERY PLANS AND INITIATIVES This section outlines the THB’s assessment and response to the IMTP guidance in respect of
pathways, specific needs and system shifts including the Welsh Government Delivery Plans and areas
of joint working with Powys Council included in the Powys One Plan.
The THB has had some challenges in responding to the breadth and scope of delivery plans that have
been issued by Welsh Government and is in the process of reviewing the process by which clinical
leadership and planning, response and reporting arrangements are put in place systematically across
all of the requirements. Those areas where the organisation has specific challenges have a greater
level of representation in the pages that follow, for example mental health and stroke services, but
the health board recognises the need to ensure that at the highest level a consistent approach is
taken to these plans.
At the heart of developing the response is the need to consider the plans in the context of the THBs
strategic objectives:
The role of our clinical leaders in the organisation and in primary care to provide leadership of
the response to plans, supported by external expert advice where appropriate;
Recognising the strengthened role of primary care and community services in the delivery of
service improvements outlined in the delivery plans;
Ensuring that the new commissioning arrangements that the THB is putting in place gain
assurance from provider organisations of delivery against the standards contained within the
national delivery plans;
Outlining the requirements of the planning that require an integrated and partnership approach
to delivery with Powys Council and other strategic partners through the One Plan.
The THB aims to complete this review in the first half of 2015-16.

108
8.1. PREVENTION AND HEALTH IMPROVEMENT
Understanding Health Need in the Powys Population The Prevention and Health Improvement programme is integral to successfully delivering the
objectives of Powys teaching Health Board’s (THB) service model.
Through the development of Powys Joint Strategic Needs Assessment (JSNA) with our partners and
ongoing work to better understand the needs of our population (for example through the Director of
Public Health Annual Reports), we are building a picture of health and health needs in our
communities.
Whilst a greater proportion of the Powys population may engage in healthy behaviours compared
with Wales, there remains significant challenge in further improving health behaviours and health
outcomes, including:
smoking prevalence remains high (19%) and not enough smokers are being treated by smoking
cessation services
childhood overweight and obesity rates in Powys (24.4%) are not significantly different to Wales
not enough children are up to date with their vaccinations at four years of age and flu
vaccination uptake rates for over 65’s, under 65’s at risk and pregnant women remain below
national target
over a fifth (22%) of Powys adults report alcohol binge drinking and two fifths report drinking
above current guidelines
Health outcomes data has been more fully articulated in the Health Needs section of the Plan. Key
areas of concern include:
the high burden of disease, with 46% of the Powys adults reporting receiving treatment for
“any illness” and nearly a third of adults being limited by illness or disability
an unacceptable gap in life expectancy and healthy life expectancy and all age all cause
mortality between the most and least deprived areas in Powys
The Prevention and Health Improvement programme will be essential in increasing the
capacity of individuals and communities to self care and share ownership of decisions and
health outcomes.
Tacking Health Inequalities Health inequalities are unjust difference in health outcomes between individuals or groups.
Numerous factors contribute to health inequalities, including differences in social and economic
conditions that influence people’s behaviours and lifestyles, their risk of illness and actions taken to
deal with illness when it occurs.
Powys THB is committed to working with partner organisations through the Single Integrated Plan in
order to address the broader determinants of health that contribute to health inequalities in Powys.
The most recent iteration of the Powys JSNA has focused on poverty, with detailed mapping (at a
Lower Super Output Area) of deprivation. This work, in conjunction with health intelligence data, will
provide Powys THB with a more granular picture of health inequalities. The development of a Powys
THB Health Inequalities Action Plan will ensure that the Health Board is working to tackle health
Improving health now and laying the foundations for maintaining good health for the
future

109
inequalities, as well as addressing the Inverse Care Law. The Action Plan will provide a mechanism
for monitoring progress against actions, milestones and outcomes.
Reducing health inequalities is a core strand of the Prevention and Health Improvement programme,
with actions embedded within each of the five priority areas e.g. by targeting services in
communities with greater levels of deprivation. More specifically, there is a commitment by Powys
THB to undertake the following pieces of work in 2015/16, which will contribute towards reducing
inequalities:
Reducing smoking prevalence:
Explore opportunities to further develop and tailor support for pregnant smokers, based on
lessons learned from the local breast feeding programme
Map differences in smoking prevalence, access to services in Powys and deprivation levels
Increasing uptake of childhood vaccinations:
Explore the relationship between local vaccination rates and socioeconomic status and
update immunisation plans in light of this review
Dental health of children and young people
Explore and address local inequities in the uptake of NHS dental services amongst children
and young people
From 2015/16 onwards, there will be additional Consultant in Public Health capacity within the
Powys Local Public Health Team to lead the Health Inequalities work programme for the first time.
Prudent Healthcare Prevention (both primary and secondary) is a core principle of Prudent Healthcare, enabling a shift
away from the current model of healthcare that focuses on management of acutely unwell patients
to a model where, through partnership with our patients, we are able to prevent disease, reduce
demands on the health service and help our population to stay healthier for longer. For example, a
Local Public Health team led initiative has been undertaken in Newtown to map social connections
and community assets and identify “Community Connectors” who are able to spread accurate and
consistent key health messages in communities through their existing social networks, reaching
those who may not be reached through traditional engagement methods or who are “hard to
reach”.
Planning with our partners Further strengthening the integration of prevention into everyday working, Healthy Lifestyles is a
focus of joint working with the Local Authority and other Local Service Board partners, with the
programme jointly managed under the governance of the Powys One Plan, thus ensuring that the
promotion of positive health behaviours underpins all transformational change within Powys.
Powys THB has an ongoing commitment to work with Public Health Wales and has agreed system
wide health improvement priorities. Core areas of partnership work between Powys THB and Public
Health Wales, which are relevant to the Prevention and Health Improvement Programme include:
1. Improving health in the early years
The early years (pre-birth to 7 years of age) are a critical period in life when many factors influence a
child’s health, life chances and progress. Continuing the implementation of the Building a Brighter
Future: Early Years and Childcare Plan remains a joint priority. Key elements of the plan include:

110
Reducing exposure to tobacco smoke in pregnancy and early years
Reducing childhood and maternal obesity
Developing the Early Years Setting Framework through the Healthy and Sustainable Pre-
school Scheme
Improving data collection and surveillance
2. Developing and supporting the public health impact of primary care
Primary care (GPs, community nursing, community pharmacies, dental services, optometrists and
other allied health professionals) provides a virtual team around individuals and families. Powys
THB, alongside Public Health Wales, aim to increase the impact of public health activities in primary
care by helping:
Planners and providers to take a population approach
Develop and implement a Making Every Contact Count programme
3. Supporting NHS Wales to improve healthcare outcomes
Actions in this area compliment the Early Years and Primary Care plans and aim to ensure that
appropriate national support is provided to primary, community and acute care to achieve improved
healthcare outcomes. The priorities build upon good practice and evidence, recognising the need to
integrate the principles of Prudent Healthcare. The priorities and actions have been grouped under
three headings:
Prevention as a treatment
Patient safety
Getting evidence into practice systematically
Priority Action Areas The five priority action areas targeted through the Powys THB Prevention and Health Improvement
Programme are based on local health need and the potential to have the greatest impact on
population health. The priority areas have been reviewed and four areas remain unchanged from
2014/15:
Reduction in smoking prevalence
Reduction in childhood obesity
Increased resilience of children and young people
Increased rates of flu vaccination
In 2014/15, Making Every Contact Count was identified as a key enabler to progressing the priority
areas. Make Every Contact Count consists of empowering all staff to recognise their role in
supporting behaviour change, making public health ‘everyone’s business’ by embedding prevention
within the working practices of all staff. For 2015/16, it is proposed that delivering a Making Every
Contact Count approach is escalated to becoming a priority action.
Alcohol Brief Intervention training (a priority action area identified in 2014/15) will continue to be
delivered in Powys, but will be an element of the Making Every Contact Count approach, rather than
being a specific priority action area. The reasons for this change in approach are:
Making Every Contact Count will enable delivery of a broader range of key health messages
to a larger proportion to our population

111
A greater focus is required to deliver Making Every Contact Count at sufficient scale and
pace to have an impact
Feedback from participants in Brief Intervention Training (smoking or alcohol) has
highlighted that staff would value generic skills to be able to raise awareness of issues and
signpost to appropriate services, rather than deliver brief intervention themselves. Making
Every Contact Count will enable a more patient centred approach, whereby the issues that
concern patients are addressed.
Progress and performance for the priority areas is regularly reviewed, for example through reports
to Board and Committees.
Key to achieving progress in the priority action areas is embedding prevention and health
improvement into all care pathways so that it is core to Primary, Community or Secondary services,
whether directly provided or commissioned by Powys THB.
Delivery of Public Health Targets There are three Prevention and Health Improvement programme areas that have associated Public
Health targets. Detailed trajectories for each of the targets are provided elsewhere in this document.
The table below provides a summary of the latest position for each of the Public Health targets, as
well as the 2015/16 target for Powys THB. Targets for 2015/16 have been selected based on:
performance to date
the potential impact of delivering service change priorities
demonstrating the ambition to achieve Welsh Government targets
Table 16: Performance against Public Health Targets
Welsh
Government Target 2015/16
Latest position (11 March
2015) 2015/16 target
Smoking
% estimated LHB smoking population treated by NHS smoking cessation services
5%
1.9%*
4.4%
% smokers treated by NHS smoking cessation services who are CO- validated as successful
40% 38.5% (at end
of Q2) 40%
Flu vaccination
uptake
Over 65’s 75% 66.5% 70%
Under 65’s at risk 75% 48.1% 52%
Pregnant women 75% 46.4% 50%
Clinical staff 50% 50.2% 53%
Childhood vaccination
uptake
5 in 1 age 1 95% 93% 95%
MenC age 1 95% 95% 95%
MMR1 age 2 95% 94% 95%
PCV age 2 95% 94% 95%
HibMenC Booster age 2 95% 93% 95%
Childhood obesity
% of reception class children (aged 4/5) classified as overweight or obese
Reduction 24.4% Reduction
*= This is an interim position as at January 2015 and does not capture activity submitted through NECAF at a later date by pharmacies.
Therefore, this information needs to be treated with caution.
Of note, smoking prevalence will also be used as an internal target within Powys THB, to reflect the
overarching aim of the tobacco control strategy and action plan.

112
The table below summarises service changes that have been identified to help deliver these targets.
These service change priorities will be delivered through the Local Public Health team.
Programme area Target Service Change Priorities
Reducing smoking prevalence
5% of smokers to be treated by NHS smoking cessation services
40% of treated smokers to be CO validated as successful
Decrease smoking prevalence to 18% (as reported by WHS in 2015/16)
Undertake a strategic review of smoking cessation services
Strengthen referral pathways to smoking cessation services, focusing on referrals from GPs, out-patients, midwives and partner organisations
Implementation of a communication action plan to raise awareness of smoking cessation services
Hold a Tobacco Control Conference to develop a community of practice to Champion “Smoke Free Powys”
Increase the number of women accessing smoking cessation services
Identify evidence based interventions in to prevent uptake of smoking in children and young people e.g. in school settings
Address smoking amongst Powys teaching Health Board staff by undertaking a staff survey, developing smoking cessation pathways for staff and launching the refreshed Powys THB Smoke Free Policy
During 2015/16, there will be a focus on articulating the need for investment in 2016/17 to increase smoking cessation activity and reduce smoking prevalence
Increasing flu vaccination uptake rates
75% uptake in over 65’s, under 65’s at risk and pregnant women
50% uptake in healthcare workers
Roll out of a Flu Partnership programme, to enable Third Sector staff to promote flu vaccination
Further consider the role of midwives in vaccination of pregnant women
Implement lessons learned from 2014/15 to strengthen the Flu Vaccination Action Plan for 2015/16
Increasing childhood vaccination uptake rates
95% of children up to the age of 2 years to be up to date with scheduled vaccines
95% of children aged 4 years up to date in the schedule
Pilot pathways for health visitors and GP practices to follow up children who have missed scheduled vaccinations
Scope the feasibility and potential impact of an Active Follow Up approach in Powys, and develop a business case for implementation, if appropriate

113
Work with schools to increase pupil knowledge of vaccination, in order to increase teenage vaccination uptake rates
Increase Child Health Data accuracy and ensure data is used to best effect
Articulate the need for further investment in 2016/17 to increase childhood vaccination rates
Reducing childhood obesity
Reduction in the % of children in Reception Year who are classified as overweight or obese
Identify priority interventions that will have an impact on childhood obesity levels and develop a business case for implementation of interventions
Ongoing Prevention and Health Improvement Activity In addition to the priority action areas, there is significant ongoing work in Powys THB, led by the
Local Public Health team, in the following workstreams:
Healthy weights
o Ensure that Powys patients (adults and children) are able to access Level 3 obesity
services
o Strengthen Level 2 obesity services and develop a business case if gaps are identified e.g.
as a result of loss of funding in MEND
Improving Mental Health and Wellbeing
o Delivery of a 5 Ways to Wellbeing approach
Reduce Alcohol and Substance Misuse
o Contribute to the development and delivery of the substance misuse prevention plan
through the Area Planning Board
Improve uptake of Screening Programmes
o Work with Public Health Wales to promote screening and increase uptake of screening
programmes to national target levels
Healthy Schools Programme
o Support Schools to increase the proportion who achieve Phase 4 accreditation and
increase the number of accredited Pre-School settings
Public Health Dietetics
o Delivery of range of courses, including Agored Cymru, Get Cooking Courses, Eating for
One and Foodwise

114
Summary Plan 3: Prevention and Health Improvement
Prevention and Health Improvement Summary Plan
Aim Prevent long term conditions by reducing smoking prevalence, reducing obesity levels, promote wellbeing and resilience of children and young people, preventing morbidity and mortality due to influenza and embedding a Making Every Contact Count approach in Powys.
Current Status
Access to smoking cessation services in Powys remains below WG Tier 1 target (5% of smokers
to become treated smokers)
Making Every Contact Count training materials have been developed
Alcohol Brief Intervention Training programmes are available to staff across the public and third
sector in Powys. Uptake needs to be widespread and large scale in order to have an impact.
Flu vaccination uptake rates amongst all groups (except healthcare staff) are below Tier 1 target
levels.
Children in Powys have high rates of overweight and obesity at reception year, which will lead
to significant cost in future years. A Childhood Obesity Task and Finish group has developed an
Action Plan in partnership with key agencies in Powys.
A range of programmes is provided that promote resilience and positive mental health in
children & young people but not at sufficient scale to have an impact at population level.
Objectives
1. Reduce smoking prevalence in Powys
2. Increase proportion of staff delivering health promotion messages as a routine part of their
role
3. Reduction in childhood obesity in Reception Year children
4. Promote the resilience and wellbeing of Children and Young People
5. Increase flu vaccination uptake rates amongst at risk patients and health and social care staff
Baseline Metrics
Smoking prevalence in Powys = 19% (2012/13)
3.6% of smokers in Powys accessed smoking cessation services in 2012/13. Target is 5%
Monthly figures available for access to Stop Smoking Wales services
Monthly data available on Pharmacy smoking cessation service (although data completeness
is a concern)
Monitoring of staff undergoing Brief Intervention training & brief advice given out by staff
(latter is monitored by PHW as part of their evaluation of the programme)
Alcohol consumption data
Alcohol related / attributed harm
Uptake of influenza vaccination in Welsh Health Boards for patients and healthcare staff
CMP results. 24.4% of children are overweight or obese in Powys, not significantly different to
Wales (26.2%)
Data re mental health prevalence and suicide rates
Health behaviours of children (Health Behaviour of School Children Survey)
Mental health services activity data and the number of people referred to tier 2 and above
Risks
Public Health Team capacity
Lack of engagement from staff in Powys THB, due to capacity concerns
Some programmes may require initial investment, with cost benefits not being realised within
the three year period
Strong partnership working required for delivery of plans
Engagement with Primary Care Services e.g. GP Practices, pharmacies
Stability of funding for community pharmacy smoking cessation scheme & developing a Stop
Smoking Wales Service that would best suit the needs of Powys
Staff capacity to undertake Making Every Contact Count training
Staff capacity to vaccinate & promote flu vaccination. In addition, the Immunisation Co-
ordinator is 0.5wte only (the role is 1wte in all other Health Boards)
Measuring impact on childhood obesity beyond reception year is problematic at present, as
CMP is for Reception Year Children only

115
Healthy schools and pre-schools have funding confirmed on an annual basis, making planning
future delivery problematic
The Public Health Wales Health Improvement Review has identified areas for disinvestment.
The local impact will include reduced investment in MEND (childhood weight management
programme), which may result in the programme not being sustainable in Powys
Related Welsh Government & Local Outcomes
Frameworks
Welsh Government (2010) Our Healthy Future
Welsh Government (2011) Fairer Outcomes for All.
One Powys Plan - Single Integrated Plan
Welsh Government (2008) The Substance Misuse Strategy for Wales (2008 -2018)
Welsh Government (2005) Raising the Standard
Welsh Government (2009) Thinking Positively: Emotional Health and Well-being in Schools
and Early Years Settings
Welsh Government (2008) Working together to reduce harm
Welsh Government (2012) Together for Mental Health.
Welsh Government (2011) Child Poverty Strategy for Wales
Powys Vision for Mental Health (Sept 2012)
Powys Mental Health (Wales) Measure 2010 Implementation Plan
Welsh Government (2010) Breaking the Barriers - Better Support for Children and Young
People with Emotional Well-being and Mental Health Needs - An Action Plan for Wales Chief
Medical Officer Obesity Pathway
Welsh Government Together for Health Delivery Plans: Diabetes, stroke, heart disease,
respiratory, eye health,
Welsh Government Flu Plan
All Wales Tobacco Control Delivery Plan
Chief Medical Officer Obesity Pathway

116
Milestones
Task 15/16 16/17 17/18
1. Reduce smoking prevalence in Powys
1. Further develop and embed Tobacco Control Action Plan & strengthen engagement from partners X
2. Develop Smoking Cessation Services in Powys, including pharmacy services X X
3. Mainstream Brief Intervention Training and e- learning (linking in to the Making Every Contact Count approach) X X X
4. Develop local campaigns and enhance national smoking cessation campaigns X X X 2. Develop and deliver a Making Every Contact Count approach in Powys
5. Develop local training materials to enable delivery of Making Every Contact Count X
6. Facilitate the development of co-created training options, consolidating existing work, in line with national direction X
7. Develop a model for sustainable delivery of training, allied to / integrated with existing activity X
8. Establish and enable Making Every Contact Count community of practice across Powys X X
9. Evaluate the engagement with and outputs from the programme X 3. Reduce childhood obesity levels
10. Map current interventions for pre-school children X
11. Identify priority interventions and establish mechanism for delivery of interventions X X
12. Delivery, monitoring & evaluation X X
4. Increase flu immunisation uptake rates amongst patients and staff
13. Develop the concept of a flu partnership programme and engage with stakeholders X
14. Implement and embed flu partnership programme and X
15. Peer staff immunisation programme X X
5. Promote the resilience and wellbeing of Children and Young People through the development of a strategy to deliver a range of programmes
16. Develop a strategy to deliver a range of programmes X X
17. Implement the Resilience building programme X X
18. Support the Healthy Schools and Pre-schools programme across Powys X X X
19. Promote further anti-bullying wok X X

117
8.2. UNSCHEDULED CARE
The vision for unscheduled care in Wales is that “people should be supported to remain as
independent as possible, that it should be easy to get the right help when needed and that no one
should have to wait unnecessarily for the care they need, or to go back to their home. We will
achieve this by working with patients and carers as equal partners to provide prudent care. We will
put quality and safety first, working with staff to improve the care we deliver by identifying and
removing any waste from our work, and openly sharing our outcomes or learning”. The Way Ahead
for Unscheduled Care in Wales
In essence this means that we must ensure that people access care at the right level for their needs
(right care; right person; right place; right time) and this provides the focus for the development and
delivery of our Unscheduled Care Improvement Action Plan.
Powys teaching Health Board differs to the other Health Boards and Trusts in both Wales and
England in that it is predominantly rural and does not have a major District General Hospital within
its borders. As a consequence the focus and contribution we have to the delivery of unscheduled
care services is different from other organisations, focussing less on the internal performance of
individual Emergency Departments and associated activities and more on:
a) Keeping people healthy and living independently in their own homes and communities as much as possible, thus reducing inappropriate demand on more acute healthcare services, and
b) Returning people back to their communities from acute care as quickly as safety allows, thus improving the flow through the healthcare system.
Over the past year we have introduced, developed and enhanced a number of services which have
been geared towards achieving these two aims. These services include:
Increased specialist nurse capacity to help people better manage their long term conditions at home;
Community Resource Teams and Virtual Wards in South Powys to provide local services that help prevent avoidable admission to hospital;
Increased Minor Injury Unit capacity to prevent unnecessary Accident and Emergency Department attendance and allow alternatives for Ambulance crews;
Increased local diagnostic and assessment capabilities to prevent unnecessary admission to acute hospital departments;
Improved evidence based patient pathways that prevent unnecessary admissions to acute hospitals;
Care Transfer Coordinators working to both prevent unnecessary lengths of stay in acute hospitals and ensure safe and timely discharge to home or a community hospital bed
Increased community nursing and therapy services targeted at reablement to allow quicker discharge back home or to the community.
The results of these, and other, developments, delivered in partnership with Primary Care
Practitioners, Powys County Council, Welsh Ambulance Service Trust, Shropdoc and other Third
Ensuring that people access the most appropriate care for their level of need by
maximising the capacity available at local level to manage people’s needs at home or
within community facilities where appropriate

118
Sector partners have put Powys at the forefront of non acute unscheduled care delivery and have
provided considerable success:
Accident & Emergency attendances o 174/1,000 population v all Wales average of 239.
Emergency admissions o 99/1,000 population v all Wales average of 111.
Shropdoc triage o 1,196 per month average.
95% dealt with in house; 3% referred to WAST and 2% to Accident & Emergency.
Average Length of Stay for Emergency Admission in District General Hospital o 5.1 days compared to all Wales average of 6.7.
Set against these successes there is room for improvement. The Delayed Transfers of Care levels
within Powys are relatively high, at over 20%, and this impacts significantly on patient flow. The
consequence of high levels of DTOC affects the length of stay, ability to repatriate from DGHs and
increases costs with the need to open surge capacity for lengthy periods of time. This is an area of
key focus for the Board and its partner Powys County Council in 2015/16.
There is still more we can do to improve local care provision and to clarify care pathways to ensure
that unnecessary care is avoided and that the experience of care when needed is improved.
However, it is clear that to improve in some of these areas a more integrated approach to care
delivery must be found that crosses traditional sector and organisational boundaries.
Over the past 12 months there has been considerable work undertaken as part of the Strategic
Demand and Capacity project. This process has been clinically led via a clinical reference group and
wider stakeholder reference group involving our external provider organisations and has had
executive input and guidance around the modelling assumptions.
This work looked at the impact of future demand on our services over a 5 and 10 year horizon and
considered the opportunities to reduce reliance on secondary care using evidence based best
practice. It identified through the Clinical Reference Group a level of opportunity for developing
ambulatory care and intermediate care services. A number of efficiency benchmarks were included
within this modelling for example the Directory of Ambulatory Emergency Care (DECS).
Further work is required in the short term to confirm the level of opportunity for delivering
ambulatory and intermediate care services that will ensure people access the most appropriate car
for their level of need by maximising the capacity available at local level to manage people’s needs
at home or within community facilities where appropriate.
Recognising Powys’ unique position as a Health Board in Wales, and taking on board the lessons
learned from previous years, we have developed an approach to improvement that plays to our
strengths and is based on three key themes:
Demand Management -ensuring that people do not access levels of care that are inappropriate
for their needs;
Capacity Management -ensuring that we can manage as many care needs as possible locally;
Escalation Management -ensuring that we work together across organisations to achieve the best outcome for the individual.
To respond to the specific challenges in each of these areas an Unscheduled Care Improvement
Action Plan has been developed, overseen by an Unscheduled Care Board. This arrangement allows

119
the Health Board and its main care partners to develop a more integrated approach to unscheduled
care development and delivery.
Through these combined actions, the Health Board is planning to reduce or avoid nearly £1M
expenditure on unscheduled care within secondary care providers in 2015/16
Unscheduled Care Plan Priorities for Delivery in 2015/16
Key Theme/Action Organisations Rationale/expected outcome
Improved Demand Management
Roll out GP led Community Resource Team/Virtual Ward model across Powys
Develop alternative MIU pathways and consistent WAST Diversion Protocols
Introduce community based catheter care bundles
Roll out COPD Personal Care Plans across Powys
PTHB/Primary Care PTHB/WAST PTHB PTHB
Reduced unscheduled care admissions to hospital
Reduced inappropriate 999 calls and ambulance conveyances to DGH
Reduced 999 calls and ambulance conveyance to DGH
Reduced 999 calls and ambulance conveyance to DGH
Improved Capacity Management
Introduce twice weekly multiagency review of all DToCs
Introduce “10 day Review” process for all in patients
Revise Operational Bed Management Policy for Community Hospitals
Increase domiciliary and care home capacity within Powys
Increase use of Shropdoc Care Coordination Centre for bed management
PTHB/PCC PTHB PTHB/Shropdoc PCC/3rd Sector PTHB/Shropdoc
Reduced DToC length of stay and improved flow
Improved discharge and lower unnecessary length of stay
Improved discharge planning and lower unnecessary length of stay
Lower DToCs
Improved systems and processes for bed management leading to lower avoidable hospital admission
Improved Escalation Management
Introduce improved validation process for all DToCs
Base Care Transfer Coordinators more in acute hospitals
Include PCC representatives on daily conference calls
PTHB/ other HBs/Trusts PTHB/other HBs/Trusts PTHB/PCC
Clarity of daily position and increased system understanding
Clarity of daily position and increased system understanding
Clarity of daily position and increased system understanding

120
Summary Plan 4: Unscheduled Care Summary
Unscheduled Care Summary Plan
Aim
a) Keep people healthy and living independently in their own homes and communities as much as possible, thus reducing inappropriate demand on more acute healthcare services, and
b) Return people back to their communities from more acute levels of care as quickly as safety allows, thus improving the flow through the healthcare system
Current Status
• Lack of evidence base for some services.
• Patient voice needs more emphasis in service planning and delivery.
• No single electronic patient record for Health and Social Care.
• Recruitment and retention of workforce difficulties in some areas, e.g. home/domiciliary care and general practice
• Differences systems in Wales and England.
• Limited integration of health and social care.
• A largely DGH based healthcare model.
• Lack of resilience in some current services.
Objectives
• Reduce inappropriate 999 calls
• Reduce unnecessary ambulance conveyances
• Reduce unnecessary A&E attendances
• Reduce delayed transfers of care
• Reduce unscheduled hospital admissions for key conditions
• Reduce unnecessary hospital length of stay
• Improve bed flexibility
• Increase local service availability and usage
• Improve integration between partner organisations
Baseline Metrics
Risks
• Difficulty in transferring money flows within Welsh System.
• Transferability across Localities / Directorate.
• On going recruitment and retention of the GP workforce.
• Ability to undertake standard & volume of training to develop workforce to implement alternative pathways.
• Ability to undertake Stakeholder Engagement at a pace to maintain change momentum.
• Shift required in organisational culture from a bed base culture to a service led culture.
Workforce, IT and Estates
Enablers
Community staff links to central informatics systems via mobile devices
Estate Strategy and Capital Programme
Estates Compliance Programme
GP EMIS access in Community Hospitals
Rural Practitioner models for primary and community staff training and development
Health Board support for primary care practitioner development
Related WG & Local Outcomes
Frameworks
• Delivering Local Health Care, Accelerating Pace of Change.
• Tier 1 target areas.
• National Unscheduled Care Plan and Unscheduled Care Improvement Programme.

121
Milestones
Task Key Output/Outcomes 15/16 16/17 17/18
Demand Management
Roll out of GP led CRT/VW CRT/VW operational around each Practice X
Develop alternative MIU pathways Pathways in place for key conditions X X X
Introduce Community Care based catheter bundles Bundles in operation X
Roll out COPD Personal Care Plans Care Plans in place for all registered patients X
Capacity Management
Introduce multiagency DToC review Weekly DToC Reports X
Introduce 10 Day Patient Review process Monthly Bed Occupancy Reports X
Revise Operational Bed Policy Policy operational X X X
Increase domiciliary and care home capacity Increased capacity X
Increase use of Shropdoc Coordination Centre Improved bed management X
Escalation Management
Introduce DToC validation process Weekly DToC Reports X
Base Care Transfer Coordinators more in DGH Validated Medically Fit for Transfer Lists X
Include PCC representatives on daily conference call Daily DToC Action Report X

122
8.3. PLANNED CARE
Planned care focuses on planned appointments or interventions that fall within an individual’s
treatment journey and the Health Board commissions care across the whole patient pathway from a
range of healthcare providers within Wales and in England. Within Powys, the Health Board
provides a range of planned services including consultant outpatient appointments and
interventions like endoscopy, therapies, diagnostics and day case surgery.
Our key aims are to ensure that we commission high quality, effective and timely elective care that
meets treatment targets. We are seeking to shift the balance of outpatient, day care, diagnostic and
elective inpatient services to community or primary care and community settings to improve access
and quality of care within Powys, and to reduce demand on acute services. People will continue to
have rapid access to specialist services and expertise where they, in discussion with their GP, think it
necessary.
We also seek to drive efficiency of elective care pathways through our commissioning approach,
through a prudent approach that directs activity to the most appropriate health professional and
through the introduction of new technology. Our demand and capacity planning work has identified
considerable scope to both improve efficiency and undertake a greater proportion of activity in
Powys. The latter is an important step in improving the patient experience for Powys residents,
reducing the need for unnecessary travel.
Our GP clusters are key partners, and provide clinical leadership alongside our in-house professionals
to identify opportunities and re-design pathways that improve the service offer in Powys and reduce
the requirement for patients to wait. We will continue to use this approach, strengthening our
approach through the delivery of both the Commissioning Programme and the Service Reform
Programme described in this plan as the route to drive change.
Current Performance In reviewing the Board’s performance on planned care over the previous financial year it is clear that
the Board as a provider of services has more than achieved the 95% performance threshold for the
26 waiting for Referral to Treatment consistently through the year. In fact, this is now exceeding
99%, and 95% of patients accessing Powys services waiting no more than 18 weeks. Improvements
in the design of patient pathways, effective management of the patient lists and a more robust
planning and management of visiting clinicians led to in year improvements. We are planning to
deliver this level of performance will continue to be delivered in 2015/16.
The Health Board has focused on strengthening its operational demand and capacity planning
system to plan and manage the services provided within Powys. During 2015/16, further work is in
progress to standardise the demand and capacity planning approach across Powys enabling the
Health Board to build further flexibility into the design and delivery of its services to support the
ongoing attainment of treatment targets and drive out inefficiency.
A key risk to performance in Powys is related to the rural and dispersed nature of service delivery.
There remain some areas of service fragility that are compounded because some of the services
Ensuring that within Powys an optimum level of planned care is provided in County
within agreed treatment targets; commissioned elective care is of a high quality, cost
effective and delivered in line with agreed treatment targets and repatriating, over time,
appropriate planned care provision into a safe, high quality, cost effective and locally
accessible environment

123
provided are small in scale and are delivered infrequently resulting in staffing and access issues. We
are currently working to improve the resilience of Audiology and Sonography within Powys as the
areas of performance that have fallen short of targets in 2014-15. Improvements in performance
have been achieved for both these services in 2014-15, however there is further work to do to
deliver a sustainable service. A new approach to delivering the service model is being implemented
for Audiology. Alongside working with national agencies to address the national recruitment issues
in Sonography, we are implementing a longer term localised training plan to develop the current
workforce. Both of these services have been subject to detailed review over previous years and are
at a point where new service models that have greater resilience and stability can be introduced in
the coming year, with a full year effect into 2016/17. At the end of 2014-15 the THB has
commissioned a pilot mobile MRI service in South Powys to test the impact of this service on patient
experience and waiting times in the South of the County. The impact of this pilot will be evaluated
to determine if a longer term mobile solution will be of benefit to Powys, and to help determine if
NHS Wales should consider the operation of a mobile MRI facility as part of its offer to the rural
population of Wales. These service reviews and subsequent implementations are cross referenced
in the C6 section.
The Board’s performance as a commissioner of services is less successful in terms of delivery of
agreed treatment time guarantees. The current position based upon January 2015 data shows that
the overall achievement of RTT is 92.8 %, 88.8 % is associated with commissioned services which is
made up of 83.9% for ‘Welsh commissioned services’ and 93.2% for ‘English commissioned services’,
however this has also been an improving picture over the year, although performance has once
again dipped over the winter period. The THB has put in place active management of long waiting
patients in England which has succeeded in eliminating waits over 52 weeks in English providers. A
similar approach will need to be considered in Welsh pathways as our NHS Wales providers continue
not be able to deliver against waiting times for our residents.
The number of patients waiting over 52 weeks not booked currently stands at 67 though everyone
waiting over 52 weeks will be offered an alternative treatment package before the end of the year.
During the course of the year there has been work undertaken with commissioners to ensure that
lists are validated and that the correct booking rules are being applied. In working with the Trusts in
England there has been a real focus on ensuring that the data is accurate due to the Payment By
Results (PBR) regime. In addition more work is now being routinely undertaken into the quality of
the services provided and not just the volumes across English and Welsh providers.
Work has been undertaken to identify the capacity gaps for 2015/16 for the elective programme and
this is analysed carefully at Appendix C2, 3, 4 and 5 templates. On the basis of the performance in
2014/15 to date the pressurised specialties in externally commissioned services remain
Orthopaedics and Ophthalmology and these will continue to be the focus of attention to reduce
waiting times and achieve a system where capacity and demand is in balance. This will be achieved
through a combination of pathway developments to intervene earlier in pathways in a primary care
and community setting, and seek alternative capacity to rebalance the system A calculation has been
undertaken in regard to the volume of activity that would be required on a non recurrent basis to
remove the over 52 weeks and move to patients waiting no longer than 36 weeks. Our estimate of
the cost of achieving this level of delivery ranges between £0.7M and £1.3M in 2015/16 dependent
upon which organisation might be used and the contractual terms that would be adopted i.e.
marginal cost within an existing welsh contract or full cost within a private sector organisation. Our
financial plan has included an assumed requirement of £0.750M. We will continue to review and
remodel as the year progresses.

124
Providers of the Health Board’s commissioned secondary care Ophthalmology service are in the
main struggling with capacity and as a consequence are not meeting treatment targets, with some
areas having a back log of follow ups as reported nationally. As a result of these pressures, the
Health Board’s own in-reach service is not able to develop further and expand the range of services
it could provide in-county. The anticipated success of working with Primary Care providers is likely to
delay the need for the Health Board to secure additional secondary care services with new
providers. Working with Optometry Wales, the potential of optometrists working in Powys is being
developed. This includes amending the pathways of care to enable GPs to refer routine and urgent
(not emergency) eye cases such as suspected cataracts to an accredited optometrist as opposed to a
consultant. This enables the optometrist to assess the patient, provide a diagnosis and undertake a
range of checks prior to a consultant’s involvement. The optometrist can also provide a range of
monitoring services for patients who have had cataract surgery or have glaucoma.
Delivery of cancer waiting times performance is an area of concern for the Health Board and we are
closely monitoring and working through our commissioning arrangements to achieve the treatment
targets for our population.
The commissioning team are currently working to ensure all breaches are thoroughly investigated by
directly contacting the providers. For English providers we monitor monthly via Open Exeter and
Welsh providers are monitored by South Wales Cancer Network on a monthly basis.
Demand and Capacity Modelling Over the past 12 months there has been considerable work undertaken as part of the Strategic
Demand and Capacity project. This process has been clinically led via a clinical reference group and
wider stakeholder reference group involving our external provider organisations and has had
executive input and guidance around the modelling assumptions.
This work looked at the impact of future demand on our services over a 5 and 10 year horizon and
considered the opportunities to reduce reliance on secondary care using evidence based best
practice. It identified through the Clinical Reference Group a level of opportunity for repatriating
outpatient and day case services and broadly identified what potential capacity would be required in
terms of physical outpatient clinics to support this. A number of efficiency benchmarks were
included within this modelling, however there were not cost savings allocated to repatriation of care
within the current hospital configuration.
Further work is required in the short term to confirm the level of opportunity for repatriating
services into Powys without significantly reconfiguring the estate. We are currently undertaking
detailed work to assess the level of these opportunities to deliver a shift left of activity from
secondary care back into Powys across the following areas
Reduce outpatient follow ups across commissioned secondary care services and provider
services.
BADS Shift to daycase with our commissioners.
The level of outpatient activity for repatriation and impact on current capacity.
The level of day case and endoscopy repatriation and impact on current capacity.
This programme of work will be implemented through the Service Reform Board, which reports to
the Transformation Programme Board. The Service Reform Programme will also take a responsibility
for the unscheduled and planned care activities of the Board as well as the interface with the Council
in regard to older people’s services. It will focus on work that can be achieved within the current
configuration of estate spread over a 0 to 5 year timeframe.

125
Service Reform Programme The Service Reform Programme will look to design new services to meet population needs, based
around disease or condition specific pathways. Strengthening our commissioning approach will be a
key enabler to drive the programme in term of assuring quality, efficiency and cost and this work
forms another programme. We will also seek to use modern technology and alternative methods of
remote monitoring of patients where appropriate to improve access to specialist advice and to keep
people active in their own homes for as long as possible through the IT and Information Programme.
There are a number of interdependencies between the programmes to deliver transformational
change within Powys and to support the management and co-ordination of the work, all
programmes report to the Transformation Programme Board.
The following themes that underpin the delivery of the Service Reform Programme’s aim and
objectives:
Planned care will be organised according to care pathways based on clinical evidence, tailored
for individual patient need and clinical condition where appropriate;
Care pathways will be integrated across organisational and professional boundaries so that
people experience as seamless care as possible, irrespective of who provides it;
Where possible, pathways and service specifications will include provision for “one stop shops”
and single site visits for assessment, diagnosis and treatment;
Referral to secondary care will be made only for parts of the pathway that cannot be delivered in
a community or Primary Care setting e.g. Day Case Surgery will be the norm for most routine
surgical procedures, and will be provided in Powys where appropriate, and Rehabilitation and
Outpatient services will take place in community or primary care settings where possible, with
home-based Re-ablement services available as needed to support a return to independence;
Service demand and capacity will be managed to ensure optimum value for money is secured;
Service capacity will be commissioned on the basis of assessed population need to ensure that
everyone receives care according to clinical need.
Commissioning Programme
We have described elsewhere in this plan the establishment of a Commissioning Programme to
considerably strengthen the THB’s approach to service planning and commissioning including quality
monitoring of services provided by external providers. This programme will provide considerable
additional focus to both the cost and quality of the services that the THB commissions, and help the
THB to ensure sustainable service delivery for the medium to long term.
Priorities A significant range of new models of planned care will be explored during the next three years
across the multiple partner agencies with whom the THB commissions services. Each of these can in
themselves be small scale changes relating to a single provider of services, but in aggregate they
have proven in the past to reduce pressure on secondary care provision and provide a wider range
of services within Powys, contributing to our overall high level of performance. Each of these are at
different stages of development and further work will be required to develop the specific business
cases and to priorities based on the demand and capacity modelling work, national priorities and
fragile services/pressure points within the localities.
This would include
appointment of a Nurse Endoscopist and team, revising the Gynaecology model that will deliver
a more effective delivery of a local Gynaecology service with a neighbouring health board in line
with NICE guidelines;
Implementation of new Audiology service model and introduce revised care pathways;

126
Delivery of localised Sonography training plan;
Implement project to reduce OPD follow up appointments and to reduce waiting times for follow
ups;
Working with Optometry Wales to maximise the potential of optometrists working in Powys;
Enhanced use of urologist specialist nurses;
Development of a 24hr stay surgical ward and increased theatre utilisation;
A review of orthopaedic service provision including “ knee in a box” and the laminar flow
theatre;
Development of a more local ENT day surgery facility;
Enhancement of telemedicine especially around dermatology;
Potential options for a 5 day surgical ward within 2 years;
Development of a proactive referral management centre;
Review of outpatient accommodation and repatriation of routine work to Powys hospitals;
Mobile MRI pilot in South Powys and increased access to diagnostics including point of care
testing;
Extension of CMATS;
Development of GP led services.
In 2015/16 we are planning on the basis that the net combination of these actions will reduce or
avoid over £1M of expenditure within secondary care providers.
The priorities will be assessed through a business case approach and against criteria to demonstrate how
they will deliver improved outcomes in:
Reducing avoidable emergency admissions (converting unplanned care to planned care);
Reducing unnecessary outpatient admissions, follow ups and Did Not Attends (DNA);
Avoiding unnecessary procedures;
Improving day case performance (as a percentage of overall cases, and done in Powys);
Reducing wasted bed days;
Reducing variation in length of stay;
Improving productivity of Powys provider and commissioned services;
Improving patient experience and involvement in care planning;
Improving patient outcomes from planned care interventions.

127
Summary Plan 5: Planned Care
Planned Care Summary Plan
Aim
Truly integrated planned care systems where non complex activity that can be delivered locally is delivered locally; and where standards of care are high, waiting times are short and people get the right care, at the right time, in the right place, by the right person.
Current Status
Demand for healthcare resources is rising due to an increasingly ageing population and this is likely to be a particular issue for orthopaedics and for managing long term conditions. Further pressures on services will come from rising costs associated with new drugs and medical technology. Current Model The THB is working within five healthcare systems within Wales and in England. The THB has focused delivery of Powys provider elective services in three locations across Powys that differentiates them as centres that provide rural acute services across the spectrum of minor injuries, diagnostic and treatment facilities and elective care. These sites are not the exclusive locations for service
delivery but the three centres are: Breconshire War Memorial Hospital as a centre for outpatient and elective
day-case procedures delivered in association with strategic partners;
Llandrindod Wells Hospital as a centre for outpatient and elective day case procedures;
A centre in North Powys for outpatients in a network arrangement centred
on Newtown Hospital.
Objectives
• Improve the patient journey.
• Emphasise primary care prevention.
• Where possible provide routine care closer to home.
• Improve the quality of the service people receive.
• Improve clinical outcomes.
• Ensure joined up pathways deliver value for money and eliminate waste and duplication.
• Empower and enable patients to self manage conditions.
• Make optimum use of new technologies.
Baseline Metrics
Trends in activity are as follows:
OPD First appointments: 2013/14 = 59,806
OPD Follow up appointments: 2013/14 = 103,909
OPP: 2013/14 = 33,628 (included in above)
TOTAL cost for all Outpatient activity: £16,483,396
Day Case rates: 2013/14 = 11,942 appointments. £8,802,389
Elective Inpatients 2013/14 = 5,170 Episodes. £26,340,610
A range of between 10 and 15 pathways are being reviewed however Gynaecology, Orthopaedics, Ophthalmology, Cardiology, Urology and Dermatology are the priorities during 2015/16.
Risks
• Insufficient resource to deliver Projects could lead to delay or failure to deliver improved outcomes
• Inability to agree funding transfer mechanisms with NHS Wales providers would restrict the ability to move care packages.
• Inability to secure appropriate Clinical time from secondary care providers to deliver services within Powys.

128
• Sustainability of existing services/providers.
• Lack of GP engagement could restrict effectiveness of Projects.
• A perceived fragility of the Health Board may lead to instability of key staff. Groups.
• The impact of NHS and Social Care finances may limit the willingness of potential service providers to bear/share risks.
Workforce, IT and Estates
Enablers
• Development of new workforce models and roles to further enhance local access to planned care services.
• Re-model current estate to deliver new models of care and Clinical Services Strategy. (This will be taken forward as part of the SDM Programme.)
• Develop a coherent and coordinated approach to the deployment of modern technology and techniques for Telehealth/Telemedicine
Related Welsh Government & Local Outcomes
Frameworks
RTT – 95% of patients will be waiting less than 26 weeks for treatment – Powys Provider
RTT – a maximum wait of 26 weeks for treatment – Powys Provider
RTT –26 weeks
Reductions in Outpatient follow up rates.
Day case activity undertaken in Powys as a proportion of total day case activity for Powys residents for all specialties.
Increase in OPP corresponding decrease in Day Case activity
Improvement in Delayed Transfers of Care Delivery
Bed occupancy levels – 85% indicative target – Powys Community hospitals – With DTOC
Average length of Stay.

129
Milestones
Task Key Output/Outcomes 15/16 16/17 17/18
Improve Provider Therapy performance and sustainability of services including enhanced access to diagnostics.
Improved rapid access to diagnostics
Improved access to sonography to achieve diagnostic waiting time.
Improved access to audiology to achieve waiting time.
Implement a sustainable Audiology service model.
Evaluate MRI Pilot scheme.
Development of orthopaedics services to include fracture clinics and enhanced CMATS.
Development of sonography services for local ultrasound scanning.
Ongoing implementation and review.
Evaluation.
Maximise day case and endoscopy performance (as a percentage of overall cases, and done in Powys).
More care in Powys
Reduced secondary care admissions
Improved day care performance
Improved productivity
Improved patient experience
Appointment of a Nurse Endoscopist and team, revising the Gynaecology model in line with NICE guidance.
Development of a 24hr stay surgical ward and increased theatre utilisation.
A review of orthopaedic service provision including “ knee in a box” and the laminar flow theatre.
Development of a more local ENT day surgery facility.
Potential options for a 5 day surgical ward within 2 years.
Implement consistent approach to demand and capacity planning across Powys provider.
Improved productivity.
Matching demand and capacity to maximise throughput.
Predictive modelling of future demand reviewed on an annual cycle.
Design and implement consistent demand and capacity operational planning system for Powys provider.
Review and updated strategic demand and capacity modelling on an annual basis.
Business as usual
Business as usual
Review and Enhance the current Powys Referral Management System (A set of GP agreed referral guidelines and a dedicated, clinically led, management system/centre to manage referrals through the system)
More Care in Powys
Reduced avoidable admissions
Avoidance of unnecessary procedures
Improved productivity.
GP Governing established
Performance Monitoring Framework – pathway variation and INNU (Interventions not normally undertaken), patients need to be assessed against the INNU criteria before they are referred
Enhanced use of urologist specialist nurses.
Development of respiratory specialist nurses.
Operating model established Clinical Guidelines developed for a range of specialities e.g. : *Chronic fatigue *Dermatology *Diagnostics * Gynaecology *Ophthalmology *Cardiology *Orthopaedics *Rheumatology *Urology *Create dedicated web site
Clinical Guidelines developed for: *Allergy *ENT *Endocrinology *Gastroenterology *Haematology *Paediatrics *Renal *Vascular *Neurology

130
Value based Care Pathways (Based on groups of patients or disease areas e.g. Frail Elderly or Diabetes, setting out the elements of the pathway and the desired location for delivery)
More care in Powys
Reduced avoidable admissions
Improved productivity
Improved patient experience and involvement in care
Increase in follow up care provided by GP and Specialist nurse.
Mechanisms/arrangements in place to oversee and co-ordinate pathways
Pathways agreed for: *Diabetes *Respiratory Disease *Heart Disease.
Working with Optometry Wales to maximise the potential of optometrists working within Powys
Enhancement of telemedicine especially around Dermatology Outpatients;
Priorities and Work Plan agreed for 2015/16 and 2016/17
Pathways agreed and implemented for Work Plan Priorities
Pathways agreed and implemented for Work Plan priorities
Commissioning for Quality (Outcome based Service Specifications, based on agreed care pathways, that will shape primary, community and secondary care provider contracts)
More care in Powys
Reduced secondary care admissions
Reduced unnecessary appointments
Improved day care performance
Reduction in wasted bed days
Improved productivity
Improved patient experience and involvement in care planning
Funding transfer mechanism agreed within NHS Wales
Mechanism to develop Service Specifications agreed
Outpatient and Day Care Repatriation models implemented for agreed priorities:
*Orthopaedics *Ophthalmology *Rheumatology *Dermatology *Cardiology *Endoscopy *Urology.
Service specifications agreed for key priorities. Models implemented for agreed specifications
Service specifications agreed for Pathway priorities
Models implemented for agreed specifications

131
8.4. INTEGRATED CARE FOR OLDER PEOPLE
People in Powys are living longer and healthier lives than ever before, and services to meet their
needs must keep up. The number of Powys residents aged 85 or over is projected to rise between
2012 and 2030 by 108%. This will significantly increase demand on our services. The percentage of
residents aged 80 or over in Powys is projected to rise from 6.3% in 2008 to 13.8% in 2033.
Older people have higher levels of frailty, dementia and multiple chronic conditions, often in
combination with each other. This will drive a growing demand for services. Community services
and home based care will have to expand at a time when real term resource increases to meet this
growing demand is no longer assured.
The vision for services supporting older people in Powys is set out in the joint Health and Council
Statement of intent ‘Delivering Integrated Health and Social Care Services for Older People in Powys’
and is a key component of the Powys One Plan. Integrated Services for Older People is a key change
programme within the joint Health and Adult Social Care Leadership Board and a key area of
integrated working between the Health Board and the Council. The change programme for older
people has come to the end of its first year and the programme will be reviewed during 2015.
In Powys, some traditional models of service delivery need to modernise to meet these demands.
Considerable progress has already been made in re-shaping services but the further intent is
ambitious. We need to reshape the expectations of people and the communities in which they live
around care for our older population. By bringing together health with social care we will be able to
respond to the needs of the population pro-actively and flexibly with the aim of enabling individuals
to remain safe and independent in their homes for as long as possible. Through shared processes,
information systems and co-location, staff working in the community will help maximise
opportunities for individuals to be treated and supported at home, whenever possible.
Accommodation options for people need to support independence, rather than encourage
dependency. We need to ensure that service responses are needs driven and not simply the act of
fitting people to what we provide.
Central to the service model is the role of the individual as the expert, taking responsibility for, and
at the centre of planning future support and care. The integrated model will be based on early
assessment, treatment and care as close to home as possible. This service model relates to the key
outcome for the Council, THB, voluntary and private sector within the One Powys Plan “that people
in Powys are healthy and independent”. Specific outcomes are:
Maximised quality of life for the local population;
People maintain as far as possible, a normal pattern of life within their community;
The local population supported to achieve improving levels of health;
People receive enhanced services closer to home;
Individual’s needs for hospital admission reduced;
Once in hospital, people’s length of stay minimised;
People able to stay at home for as long as possible;
Increased network of community based services.
Delivering these outcomes will require a new approach to working with people and their
communities to strengthen local responses to need, a refreshed approach to medical care based
Enabling individuals to feel supported, independent, happy, safe; that they are treated
with dignity and respect and are valued, informed and empowered to maintain fulfilled
lives

132
around support at home, the integration of health and social care teams at the local level and a
radical shift in the options offered to people to avoid the need for institutional care.
The Health Board is anticipating that £0.861M of funding will be routed through the Health Board
from Welsh Government for delivering Intermediate Care Services to the population with our
partner organisations. Our proposals developed in partnership for use of this fund range from
developing community capacity through social foot care and dementia friendly service models,
expanding capacity through implementation of intermediate care services and responding to
demographic changes through implementing enhanced reablement and 7 day discharge pilots.
The table below sets out the joint programme of activity in relation to the Older People’s
Programme as part of the Powys One Plan
Project Capability to be provided by Project
outputs Contributes to Outcome(s)
Single Point of Contact A simple and coordinated process by which the health and social care needs of an individual are assessed and recorded Services will work seamlessly together
Individual’s needs for hospital admission will be reduced Increasing the network of community based services
Single assessment process / joint assessment framework
A simple and coordinated process by which the health and social care needs of an individual are assessed and recorded Services will work seamlessly together
Individual’s needs for hospital admission will be reduced Increasing the network of community based services
A Countywide Re-ablement Service
Improved capability for early intervention
Individual’s needs for hospital admission will be reduced People will be able to stay at home for as long as possible People will receive enhanced services closer to home
Reconfiguration of Older People’s Day Time Opportunities including the decommissioning of Meals on Wheels
A coordinated and accessible range of services for older people (including those with dementia), and their carers
Increasing the network of community based services The local population will be supported to achieve improving levels of health
Joint Older Person’s Commissioning Strategy
Improved service design and delivery by engaging the individuals who use them
Increasing the network of community based services
I

133
8.5. MENTAL HEALTH
Hearts and Minds: Together for Mental Health in Powys is the strategy for improving the mental
health and emotional wellbeing of the people of Powys. It was published in January 2013 by Powys
teaching Health Board (PTHB) and Powys County Council (PCC) following consultation. It is the local
response to Welsh Government’s ambitious programme for improving mental health in Wales which
includes legislation known as the Mental Health (Wales) Measure 2010 (“the Measure”); and a 10
year cross-departmental strategy for people of all ages. A multiagency Partnership Board is in place
to drive forward the implementation of the strategy through a detailed 5 year delivery plan.
Mental Health (Wales) Measure 2010 The intended effect of the Measure is to:
expand the provision of local primary mental health services
ensure all people within secondary care have a statutory care co-ordinator and care and
treatment plan
provide adult secondary care users with a mechanism for re-assessment following discharge
expand specialist mental health advocacy
Together for Mental Health This plan for people of all ages aims to:
improve the mental health and wellbeing of the population
reduce the impact of mental health problems and illness
reduce inequalities, stigma and discrimination
improve the individual’s experience of treatment and support – including their feeling of input
and control
improve prevention and early intervention
improve the values, attitudes and skills of those providing treatment and support
Hearts and Minds: Together for Mental Health in Powys sets out what local partners are seeking to
achieve in Powys. It combines local and national priorities. The vision in Powys is to promote mental
and emotional health and wellbeing for all and to enable the provision of truly integrated care
services for those who need them, thus making a positive difference in their lives and the lives of
carers. It will achieve this through:
developing a wider partnership for health and wellbeing
building strength and resilience, promoting mental and emotional health and wellbeing– for
individuals and communities- and tackling stigma
improving awareness of information, support and services
improving early recognition of and response to mental and emotional health and wellbeing
issues across all ages
enabling access to well co-ordinated services that meet the needs of the individual as close to
home as possible
promoting hope and wellbeing through effective services
targeting support and intervention based on need
Improving the mental health and emotional wellbeing of the people of Powys

134
Adult Service Model A service model for adult mental health services has been agreed on a multiagency basis. The adult
service model for Powys focuses on 4 main areas.
1. Enhanced primary care
Co-location – building more support in or near to GP practices, co-locating mental health
practitioners and services wherever possible.
Collaboration – developing shared care/co-management arrangements between GPs/primary
care practitioners and ‘secondary’ care.
Flexibility – identifying people with specific or specialist mental health needs (including for
example those with hearing or sight issues, homeless people, transient populations) and working
to provide flexible local solutions.
2. Acute care in the community (“hospital at home”)
A single point of access over the 24 hour period will be provided in order to gain access to acute
care services. The access point will work with the referrer to ensure appropriate and timely
response for assessment and intervention based on the needs of the individual.
Integrating Crisis Resolution and Home Treatment Team with the inpatient team – enabling a
single team/function with flexibility of where ‘acute’ care is provided based on need/risk.
Day Recovery and Treatment Centres as an alternative to admission. The emphasis being to
provide a wide range of interventions including clinics, psychological therapies, medication
titration and memory assessment.
Crisis Houses as an alternative to admission. The development of one or more crisis houses (a
house where supportive services usually provided by the 3rd sector can be provided based on
need/risk and supported by statutory mental health team). The evidence suggests this can
reduce admissions by 50%. Crisis Resolution and Home Treatment will continue to be an
essential part of providing acute care in the person’s home.
Inpatient care will be considered in 2 categories. The first is for people who with an anticipated
short length of stay in an inpatient unit can return to their communities/home for ongoing
support and recovery. This would be based on a ‘triage ward model’ of daily consultant-led
wards rounds; and a staffing level, culture and orientation to discharge planning with a bias to
enabling recovery in the community setting. It’s anticipated that there would be one such unit
for Powys (the initial planning assumption was 12 beds – based on evidence that a Crisis House
reduces admissions. The evidence is being reviewed). The second category of inpatient provision
is that where the intensity or complexity of the care and treatment required necessitates more
specialist service provision, for example in psychiatric intensive care units. These services would
be commissioned (and probably delivered outside of Powys) using a robust framework that
includes the return of the service users to a care setting as close to home as possible. A care
coordinator will always be allocated to the service user from Powys to enable the return home,
or close to home, as soon as possible.
3. Repositioned services for older people – access based on need not an adult’s age
Services will no longer be based on age categorisation, but will consider the natural impact of the
aging process. This means that there will no longer be a distinction as to which service is
provided based on age alone but on the need of the person
An emphasis on shared care arrangements for people who have both physical and mental health
problems, particularly but not only for those people with dementia.

135
People aged over 65 will have access to all services based on their need. Specific consultation
and advice will be provided by professionals who have expertise in aging in order that those
aspects can be adequately addressed.
Specialist teams of professionals in the area of dementia will be formed strongly linked into
physical health teams (such as virtual ward and inpatient facilities). Their role will also extend
into Care Homes and will have particular focus on supporting carers.
The model moves away from having mixed ‘functional and organic’ in-patient wards. The impact
of the repositioning of older peoples mental health will need to be fully determined in relation to
inpatient provision. It is anticipated however that a different configuration of inpatient beds will
be required.
4. Integration
The NHS and local authorities are, by law, both strategic planners (commissioners) and providers
of mental health services. The intention is to join these organisations together in order to
improve communication, care and treatment planning and efficiency in delivery.
The integration will occur at each level including leadership and management as well as front-
line provision.
The 3rd sector will be seen as part of the integrated service, with a key role in leadership and
management as well as front line service provision.
The aim would be for enablers such as estate/assets, financial management (for example Section
33 agreement), IT (including telehealth/telecare and new technologies to be made available),
learning and development, performance management to be integrated.
Current Service Configuration The majority of mental health care in Powys is delivered by Powys organisations. NHS secondary
mental health services for adults within the county are provided by three main neighbouring health
boards. In addition in-patient units in England provide services for Powys patients.
GPs and their teams are the main providers of mental health services in Powys. Out of hours services
are provided by Shropdoc (with an interface with services covering ABMUHB for the Ystradgynlais
area). There are over a thousand people with serious mental illnesses registered with GPs.
Community pharmacies and medicines management: Whilst greater use is being made of “talking
therapies” more than 90% of patients with diagnosed mental illness will be on one or more
prescribed drugs. Ensuring the safe, efficient and effective use of medication is a key issue, as is
working with the Area Planning Board to tackle the misuse of prescribed medicines.
Local Primary Mental Health Support Services (LPMHSS): PTHB and Powys County Council (PCC)
have agreed a Scheme for LPMHSS which began on the 1st October 2012. It covers all ages and
includes: primary mental health assessments for individuals who have first been seen by their GP (in
some cases, individuals may be referred into the local primary mental health support service by
secondary mental health services); treatment, by way of short-term interventions, either individually
or through group work; the making of referrals following a primary mental health assessment;
provision of support and advice to GPs and other primary care workers; provision of information and
advice to individuals and their carers about treatment and care, including the options available to
them, as well as ‘signposting’ them to other sources of support (such as support provided by third
sector organisations).
NHS child and adolescent mental health services (CAMHS): NHS community child and adolescent
mental health services (CAMHS) are funded and directly managed by PTHB. There are two teams of
professionals, one based in the north and one in the south of the county, providing community

136
based services, for those below their 18th birthday. There is nowhere to admit a child within Powys –
of any age – with any condition.
NHS adult mental health services: Mental health services for adults of all ages are provided within
Powys by three main neighbouring health boards:
Ystradgynlais – (ABMUHB)
1. Montgomeryshire: Betsi Cadwaladr University Health Board BCUHB (covering 48% of the population-
63,771):
local primary mental health support service
community mental health teams (CMHTs)
a crisis resolution home treatment team (operating until 9pm during the week and up to 7pm at
weekends)
in-patient provision for organic illness at Fan Gorau in Newtown (8 beds)
in-patient admission (including some provision for people with Dementia) at the Redwoods
Hospital in Shrewsbury (equivalent to 7 beds for Powys for functional mental illness; 1 bed for
organic illness (Dementia);.
admission to the independent hospital Phoenix House in Montgomeryshire (up to 7 beds for
adult mental illness – with additional admissions for rehabilitation.)
Occasionally Section 136 patients are taken to Wrexham (admissions there are predominantly
EMI and equivalent to 2 beds)
Memory clinics
RAID and psychiatric liaison services are also commissioned covering the Royal Shrewsbury
Hospital
2. Brecknock and Radnorshire: Aneurin Bevan Health Board (ABHB) (covering 44% population 58,978)
local primary mental health support service
community mental health teams (CMHTs)
access to a crisis resolution home treatment team (operating until 9pm during the week and up
to 7pm at weekends)
access to a community forensic team
access to a Memory Clinics for rapid assessment following referral
admission to Brecon Hospital (Crug Ward 10 beds) and Llandrindod Hospital (Clywedog Ward 10
beds for dementia)
admission to Bronllys Hospital (Felindre unit – 12 beds) for functional mental illness
s136 suite for south Powys
(psychiatric liaison for Powys people attending the DGH in Hereford is commissioned from a
separate provider)
3. Ystradgynlais: Abertawe Bro Morgannwg University Health Board (ABMUHB) (8% population 10,203)
local primary mental health support service
community mental health team (CMHT)
access to a crisis resolution home treatment team
access to rapid assessment following referral for memory concerns
access to an first episode psychosis team
access to adult in-patient beds (Neath)
access to in-patient assessment (Ystradgynlais – Tawe Ward 8 beds) for dementia
older adult mental health day hospital

137
Powys County Council Adults Social Services provides the Emergency Duty Team and staff, including Approved Mental Health Professionals and care co-ordinators co-located with the NHS mental health services provided by neighbouring health boards. Welsh Ambulance Service NHS Trust (WAST) The Welsh Ambulance Service provides frontline services to mental health patients in Powys and contributes to the development of pathways here, such as for attempted suicide and self-harm.
Dementia in Care Homes: two thirds of people with dementia live in the community while one third
live in a care home. 80% of people living in care homes have a form of dementia or severe memory
problems. There are 1,130 care home places in Powys. These are registered as follows: 587
Residential; 79 Nursing; 464 dual registered.
Adult Mental Health Services NHS Management Arrangements PTHB has highly unusual and complex arrangements for NHS adult mental health services. Around 250
NHS staff working in local teams and hospital wards in the county are actually employed by three
other health boards. The Board of PTHB has agreed to seek to directly manage NHS adult mental
health staff working in:
Local Primary Mental Health Support Services within Powys
Community Mental Health Teams within Powys
Crisis Resolution Home Treatment Teams within Powys
Mental health wards within Powys hospitals (for adults of all ages)
and associated clinical psychologists and occupational therapists. This proposal is not about making changes to the range or location of patient services but is simply
about NHS employment and management arrangements. A great deal has changed since a review in
2008 which led to the transfer. Adult mental health services are now mainly delivered in or close to
home. Powys teaching Health Board and Powys County Council are working together to implement an
ambitious programme to improve the mental health of local people, following public consultation. The
predicted rise in the number of people with dementia in the county means physical and mental health
services, and all local services, must work together even more closely. The Board of PTHB is dedicated
to ensuring that mental health has equal priority with physical health.
A Project Board involving all the employing health boards is in place. Phase 2 of the Project is
underway working towards a provisional transfer date of 1 December 2015/16. PTHB spends just
over £20 million on adult mental health services. Around half of this will remain commissioned
(including specialised services such as psychiatric intensive care and secure services). In 2014/15
the HB was projected to spend £28.8m on Mental Health services (across all ages and all sectors)
against a ring fenced sum of £27.1m.

138
Table 17: Adult Mental Health Key Developments Adult mental health: summary of key developments across the whole span of services
Self help & health promotion NHS Direct, PHW &, PTHB funded information services: 5 ways to wellbeing & suicide prevention strategy [TalktoMe2 Nov 2014] Dementia Friends. (Brecon first dementia friendly town in Wales).
Primary Care
(Early intervention; enhanced primary care; shared care; co-located services; flexible solutions for hard to reach people including the homeless).
PTHB (GPs, pharmacies) Lead GP for mental health North Powys, South Powys & Ystradgynlais in place. Progressing GP /speciality doctor pilot (physical health needs of mental health patients greatest inequality of all). Participate in Wales Mental Health in Primary Care Network
Local Primary Mental Health Support Service (LPMHSS)
(Enhanced primary care)
PTHB and PCC are therelevant Partners for Powys Part 1 Scheme (see trend): Level of referral higher then elsewhere in Wales (inclusion of counselling? Review Scheme) On- line CBT project (€500k over 3 yrs;- Beating the Blues; unlimited licenses; Project Board rolling out). Book Prescription Scheme. Group work. Improved information about commissioned third sector services.. 50+ people trained in Living Life to the Full - now being used.
Community Mental Health Teams* (CMHTs)
(Integrated and well co-ordinated care for people in the community)
Part 2 compliant (see trend). PCC manage co-located social workers. Written care and treatment plan must include crisis plan to anticipate deterioration. Implement new all-Wales “user lens” feedback forms (Part 1 and Part 2). Extend community memory clinics –dementia all ages (Dementia Plan)
Extending Talking Therapies and modernising prescribing
Significant difficulties adult (all ages) mental health psychology. Piloting co-production in south. Rigorous waiting list management and initiative. Psychological Therapies Committee. Mental Psychological Therapies Demand and Capacity – submitted to WG. Funding secured for Cognitive Stimulation Therapy – training underway; + further work on Mindfulness; (on-line CBT above); veterans: not using available capacity despite need, review awareness/ access. Psychological therapies wider then mental health e.g. stroke.
Crisis Resolution Home Treatment Teams*
Other out of hours/DGH/Raid – Liaison Psychiatry
(Alternatives to admission at home);planning to prevent crises)
CRHTTs fully functioning – see trend. Crisis House scoping – to impact on admissions (test evidence of 50%). Explore solution in north Powys with Hywel Dda in response to the Mid and west wale Review. Gatekeeping admissions. Care co-ordination strengthened to reduce distant OOC admissions (success – see trend). PCC = Emergency Duty Team new rotas. OOHs flow-chart circulated. S12 lists up-dated (however opportunity for more dynamic approach?). Pilot psychiatrist cover after 9pm north Powys. RAID in place north Powys –but extend awareness of benefits. Develop virtual ward round approach for people with dementia. Reduction in inappropriate use of s136: considerable success – inspector gatekeeping (see trend).
In-patient (functional and organic)
(services based on need not an adult’s age)
48/64 beds in Powys Hospitals. Plus 7 Phoenix House. 8 Redwoods & 2 Wrexham. Success in reducing admissions north Powys and distant out of county admissions. 15/16 re-establish bed flexibility across Powys: to be able to admit Powys residents to Powys funded beds. (4 DTOC policies in one county not working – weekly DToC telephone conferences; legal advice.) 16/17 dependent on return to direct management decision. Implement findings of WG spot check.
Tertiary/Specialised/ Welsh Framework Perinatal; secure estate. Drive forward step-down to supported living.
Continuing health care
Actually s117 (ensure constant accuracy of register); low secure; joint funding and CHC. Monitor trends – one new dementia patient per week across CHC/FNC? Establish Local Solution Approach prior to CHC. Seek to develop core service solutions e.g. medication visits and ABI service. Director panel for some decisions. Address DToC; develop home based assessment. Ensure IPFR correctly routed. Appointing FNC reviewer. DoLS (wider than mental health– but impacting on mental health assessors’ core role). Develop “framework approach” for CHC (67 different contracts). Further strengthen governance arrangements.
CAMHS
£222k secured for community intensive team – implementation underway
Ensure Mental services for the YOT are sustainable; and improve arrangements for vulnerable children living away from home.
Alcohol and substance misuse services Revising strategy Q4 14/15. Re-commission Q2 15/16
Estates Immediate issues – including those identified by inspectors and general compliance.
Capital: Confirm medium term project to modernise mental health estate
IT Mental Health Services will be part of the implementation of the Community Care Information Service (include goal based outcomes from the perspective of people using services)
Workforce Up to 250 staff could return following Board decision 25th February and then TUPE (including engagement and consultation)

139
Acute Beds in Relation to Benchmarking and Commissioned Beds Demand, capacity and developments have been considered within a “whole system” approach.
PTHB has been commissioning, on average, just over 64 beds in relation to mental health excluding
continuing care (but including independent sector hospital admissions for the Montgomeryshire
population). Powys is moving to a model where adult patients with dementia or mental illnesses
(such as Bi-Polar Disorder) will be seen by the right service based on need not age. On average 35
beds for patients with dementia/organic illness have been commissioned and 29 for
mental/functional illness. The national benchmarks would mean Powys would expect to have 22
functional beds and 25 dementia beds (based on the upper quartile – due to the underlying number
of older people in the population).
It is essential that existing expenditure is spent effectively in line with the new strategy and model.
In the medium term the configuration of “functional” in-patient mental health services needs to be
consolidated and integrated with the Crisis Resolution Home Treatment Teams to provide the
opportunity for sustainable medical staffing; assessment; home treatment and admission of patients
24/7 within Powys – with fair and equitable access across the county. The impact on admissions of
the “Crisis House” approach needs to be scoped and tested. Evidence is that admissions could be
reduced by up to 50%. For Montgomeryshire a crisis-house type solution with the Ceredigion area of
Hywel Dda Health Board will be explored.
For adults with organic illness such as dementia - there needs to be more flexible access to existing
in-patient provision across shires in the short-term (particularly for assessment and for those with
challenging behaviour). Medium term plans need to be aligned with community hospitals in order to
develop shared care arrangements for people who have both physical and mental health problems,
particularly but not only for those people with dementia. The role of specialist teams of
professionals in the area of dementia - strongly linked into physical health teams (such as virtual
ward and inpatient facilities) will need to support home care teams and extend into Care Homes –
with a particular focus on supporting carers. This is an area which requires particularly close planning
and management with the local authority. The mental health beds run in Powys hospitals by
neighbouring health boards have the highest rates of delayed transfer of care in Wales. The plan to
address this includes changes to NHS management arrangements within Powys.
Some RAID and/or specialist psychiatric liaison services are commissioned for Powys patients
attending neighbouring DGHs. However, the next stage of the RAID evaluation needs to be
completed and work undertaken to extend the model - if positive. Specialised services are
commissioned through all-Wales arrangements. PTHB will continue to commission services such as
psychiatric intensive care from neighbouring health boards. There is a gap in female rehab within the
county – predominantly in Montgomeryshire. The demand is currently the equivalent of 1140 bed
days totalling just under £450k per year.

140
Key Performance Indicators
LPMHSS Powys is compliant with Welsh Government targets for assessments under Part 1 of the Measure.
Performance in relation to waiting time for interventions is just below WG targets. (Currently there
are just over 200 referrals a month; 185 assessments; and just over 130 interventions).
CMHTs Powys is compliant with WG targets for Part 2 of the Measure. Around 1200 people in Powys have
care and treatment plans.
CRHTTs A team was established in north Powys in 2014/15 which is now performing well.
(There are about 50 referrals and over 40 assessments each month. Ystradgynlais is averaging 2
referrals and assessments per month.)
Delayed Transfer of Care 48 of the 64 mental health beds that PTHB commissions for adults of all ages are in Powys hospitals.
However the beds are managed by three neighbouring health boards. These beds have the highest
rates of DToC in Wales. In 2014/15 Powys has been able to return to the best position since transfer.
Figure 45: LPMHSS Interventions against Target
Figure 46: LPMHSS Assessments against Target
Figure 47: CRHTT Assessments and Referrals

141
Action has been taken through strengthened commissioning and governance to reduce distant high
risk and high cost admissions in Montgomeryshire. The Crisis Resolution Home Treatment Team is
fully functioning; the contract with South Staffordshire NHS Foundation Trust was re-negotiated;
funds were transferred to care co-ordination locally; and the contract with Wrexham was re-
negotiated.
Psychological therapies For adults of all ages psychology services have been provided by neighbouring health boards since
February 2011. It was thought that strategic and operational service development was more likely to
be achieved within larger and more comprehensive mental health departments, and that the
embedding of psychology services within core mental health services was more likely to be achieved.
(Other aspects of psychology including Learning Disability and CAMHS remained directly managed
within Powys).
At the time of transfer (2011) waiting times for adult services had been falling and was 5 months and 3 weeks, and for older adults it was also falling and was 67 weeks.
In north Powys in July 2014 there were 99 people (adults all ages) on the psychology waiting list and the longest wait was 32 months.
In south Powys in September 2014 there were 121 patients (adults all ages) on the waiting list, with
4 people waiting 43 months and over.
S136 The police have powers to detain people in a public place who are thought to be mentally ill and to
take them to a place of safety.
Successful multiagency work in Powys has i) led to an overall reduction in the use of such powers ii)
ensured the power is being used appropriately for people requiring hospital admission.
Figure 48: Inpatient Provision Montgomeryshire

142
Summary Plan 6: Mental Health
Milestones ACTIONS 15/16 16/17 17/18
SIMPLIFY AND STRENGTHEN NHS ADULT MENTAL HEALTH ARRANGEMENTS
i) Develop, commission and implement mental health services for the people of Powys in line with service specification
Commission services not directly managed within Powys in line with Feb 2015 Board decision. Develop “framework approach” for continuing health care
X X
ii) Agree and implement NHS Adult Mental Health management arrangements in order to deliver strategy, adult model and specification. Phase 1: Board decision about extent to which services will be directly managed in Powys; Phase 2 implementation
Implement Phase 2 following board decision
Integrate management
arrangements with PCC
X
iii) Re-commission third sector provision in line with strategy, adult model and service specification Re-commission in line with timetables for specific services X
DELIVERY OF ADULT SERVICE MODEL Review in-patient provision and ensure maximum use of alternatives to admission. Ensure flexibility of bed use
within Powys. Establish estates plan and business case to ensure appropriate standards, capacity and efficiency Ensure whole-system approach to reducing use of emergency out of hours services – including s136. Review Acquired Brain Injury Pathway Ensure robust care and treatment planning under Part 2 of the Measure. Scope plans for crisis house Reposition services for older people
Implement Dementia Plan Enhanced Primary Care
Extend use of evidenced based psychological therapies, particularly as part of Local Primary Mental Health Support Services.
Improve the physical health of mental health patients
Ensure physical health assessment of patients in primary and secondary health care
Develop estates plan and business case/s.
Achieve recovery plan for Part 1 of the Measure.
Ensure continued compliance with Part 2 requirements
Implement next phase of on-line CBT and next stage of Psychological Therapies Plan.
Implementation of Dementia Plan.
Implement PTHB approach to DTOC
X
X
X
X
X
Wider Partnership working for mental health and integration with PCC
Implement Hearts and Minds: Together for Mental Health.
Prepare for integration with Powys County Council.
Prepare for implementation of Social Services and Wellbeing Act. Improve prevention and early intervention: implement “Talk to Me”: to reduce suicide and self-harm. Reduce inequalities, stigma discrimination
Roll out of “Time to Change”
Ensure best practice in place with regard to employees with mental health.
Ensure appropriate impact assessments of PTHB policies xand plans.
Ensure service development is informed by people using services (of all ages) parents, carers, referrers and providers
Implement next stages of Hearts and Minds Together for Mental Health delivery plan.
Ensure sustainable mental health partnership support arrangements
Prepare for implementation of CCIS (integration of information system including mental health services)
Agree and implement revised “Talk to Me” plan
X X
CAMHS The priorities for child and adolescent mental health services include:
finalising the approach to integrated services with the local authority, especially for vulnerable children and
those with additional learning needs;ensuring equity of access to a community intensive team for Powys
residents, especially for those with eating disorders, to minimise disruption of home and school-life;
Implement CAMHS community intensive teams Review YOT provision to ensure sustainability Implement agreed plans within CYPP
X X

143
Child and Adolescent Mental Health Services Services aiming to improve children and young people’s emotional and mental health span from
before birth to adult services; and cover health promotion for all children through to hospital and
intensive teams for those with conditions such as Eating Disorders, Bi-polar Disorder and
Schizophrenia. Children, families, communities and other agencies play a crucial role in helping to
protect how children think and feel by preventing bullying, abuse, neglect, domestic violence and
substance misuse; and by supporting educational attainment and positive parenting.
PTHB has developed innovative services for children, in collaboration with other agencies, aimed
early intervention to help prevent problems escalating: PTHB has:
funded a psychologist to work with other agencies to introduce the Webster Stratton approach to
early parenting support, for which it has won the NHS Excellence award;
helped fund a successful internet based counselling service which links with school counselling, which
has improved clinical outcomes and increased up-take by young males – and which takes account of
every child’s feedback;
secured £222k to implement a new community intensive team, which will prevent some hospital
admissions and will reduce lengths of stay;
benchmarked its service with others across England and Wales showing it spends just above average
on staffing (however, the Mental Health Measure has changed how some staff can be used for certain
assessments and for care co-ordination);
one of lowest rates of “DNAs” across England and Wales because it has a “Was Not Brought Policy”
which it closely monitors and audits with the safeguarding team;
taken on the leadership of the CAMHS Network in Wales;
introduced nurse prescribing in NHS child and adolescent mental health services;
age specific participation arrangements at a service and partnership level
low levels of admission, with only one young person in 2013/14 admitted to an age appropriate bed
or an adult ward;
and a multiagency social communication team, so young people with ASD can be assessed swiftly.
PTHB’s NHS CAMHS team has been struggling to maintain Welsh Government targets for
assessments and interventions within the Local Primary Mental Health Support Service (LPMHSS). It
has been working with other professionals to ensure referrals are appropriate. In Powys in 2014/15
the number of children referred to the LPMHSS has reduced slightly and the number of assessments
has increased. However, the underlying volatility remains difficult to manage.
Table 18: CAMHs Assessments and Interventions Performance
Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15
Total number of referrals received during the month 32 36 12 25 19 19 34 12 31 23
Total number of assessments undertaken during the month 15 18 11 12 7 23 9 14 24 27

144
Summary Plan 7: CAMHs Milestones
Span of Services PTHB child and adolescent mental health services - key milestones and actions
2015/16 2016/17 2018/19
Overall Work with Professor Dame Sue Bailey to strengthen child and adolescent mental health services in Wales Implement
improvement plan X
Self help, health promotion, prevention
5% of Powys schools awarded Network of Healthy School Schemes National Quality Award (currently 4.5%). PHW to support the Healthy and Sustainable Pre-School Scheme. Implement final version of Talk 2 Me 2 to reduce suicide and self-harm
X 20%
Universal services for every child and young person – including primary care
Monitor up-take Youth Mental Health First Aid Training and “Safe Talk” training (monitor up-take). Agree arrangements to re-commission blended internet and school counselling service with CYPP
X X
Local Primary Mental Health Support Services
Implement Part 1 recovery plan to ensure compliance with WG targets Ensure compliant X
Immediate, urgent and routine assessment
Strengthen demand and capacity planning based on robust information collection and analysis Ensure compliant with WG targets
X
Statutory care and treatment plans following assessment
Strengthen demand and capacity planning based on robust information collection and analysis Ensure compliant with WG targets
X
Specialised teams in the community and admission
Implement Powys Community Intensive Team (CAT) – ensure available from April; extend nurse prescribing initiative following audit; strengthen community eating disorder services following completion of Master Practitioner qualification (2 WTE); sustain access to Tier 3 forensic CAMHS and mental health provision for children in the Youth Justice Team; ensure sustainable and effective access to mental health services for looked after children; strengthen DBT provision for emerging personality disorders, hard to reach children and repeated self-harm following completion of DBT training.
X X
Tertiary mental health services Leadership of CAMHS Network in Wales to strengthen commissioning arrangements, including Tier 4 X X
Transition Work with adult services to strengthen joint working for First Episode Psychosis; parental and infant mental health; emerging personality disorder; continued access to an age appropriate bed; and out of hours arrangements.
X X
Continuing care and residential care Ensure compliance with Towards a Stable Life and a Brighter Future for Vulnerable Children Living Away from Home
Workforce Strengthen demand and capacity planning. Work with adult mental health services to build shared resilience of services X X
Information and IT Implement CCIS X X
Listening to Children and Young People
Ensure age specific participation arrangements influencing service improvement X X

145
8.6. LEARNING DISABILITIES SERVICE
There are approximately 670 people registered with a Learning Disability in Powys. This includes
people with a mild to moderate learning disability through to those with a high level of need. The
model of care is generally recognised as a tiered system. This includes:
Tier 1 – largely primary care based with support provided to primary care teams (such as GP and
Practice Nurses) to ensure the needs of people with a Learning Disability are recognised by
mainstream services. Approx. £1.3M is spent by the THB in partnership with the Local Authority
on services such as supported tenancy, day services, etc.
Tier 2 – community based services, including some specialist in nature, supporting people with a
learning disability to live fulfilled lives within their own homes and communities. The team based
care is provided on a multi-disciplinary basis and approximately £1.5M is spent on this tier of
service.
Tier 3 and 4 - in-patient care services are no longer provided in Powys as the focus on
community services has resulted in fewer clients needing such care. Highly specialist services for
clients which cannot safely and adequately be supported at home are procured from specialist
centres. The THB currently spends approx. £149,000 on such placements.
Services must continue to evolve in order to deliver highly effective citizen focused outcomes and
represent good value for money. Practitioners continue to drive forward service developments and
innovations aimed at continuous improvement and the priorities identified have been influenced by
those within the service.
The future direction for Learning Disabilities is governed by the need for a joint commissioning
strategy with Powys County Council and a joint service delivery model that will improve the user
experience and deliver financial efficiencies. The key priorities for Powys THB Learning Disabilities
services are:
Developing Partnerships and Joint Working Powys THB acknowledges that Powys County Council should have the main responsibility for all non-
health related needs of people with learning disabilities and their families. This includes providing
accommodation, education, social care and support, day services, employment, leisure and
recreation and transport, to that effect we are currently developing a joint adult learning disability
strategy which is currently out for Consultation (the Commissioning Strategy) into which the
strategic direction for health services for people with a learning disability will be embedded.
Relationships and Family Life In supporting clients to develop their personal lives, build friendships and establish personal
relationships we will be supporting people to live fulfilled lives. The team work closely with other
Creating a joint service delivery model with Powys County Council to improve user
experience and deliver financial efficiencies
Developing partnerships and joint
working
Relationships and family life;
Improving community care Ensuring
seamless transition;
Access to specialist in-patient care;
Improving the resilience of services;
Improving access to general healthcare;
Improving communication;
Empowering staff;
Cost effective services including
continuing healthcare.

146
services like People’s First and other support services to help clients establish meaningful, non-day
centre related social activities. Many clients have accessed the Learning Disability team for
therapeutic support at the point when their ability to maintain their role as parents has broken
down. The team are supported by the University of South Wales in relation to Sexuality and
relationship work to ensure the best research is available to support the intervention working with
individuals. Links have also been developed with Midwifery services to offer support.
Improving Community Care Ensuring Seamless Transition Transition planning involving the young person, their family, the children’s services and the adult
Learning Disability Service can start on an individual basis at 15/16 years. Effective involvement and
transition planning should result in a good service user experience.
Access to Specialist In-patient Care The THB have currently one patient in a Low Secure Hospital, the focus has been to ensure that
individuals are treated within their own community with a joint support package. The THB have
reviewed its workforce planning and employed a full time Consultant who is able to work alongside
clients when the need arise rather than crises management which has an implication into tier 4
provision. Learning Disabilities are part of the Care Assurance and Performance system.
Improving the Resilience of Services Develop challenging behaviour services, the team have reviewed the current trends within referrals
and we have to work to prevent or delay the need for more intensive health services. The
appointment of a Clinical Behavioural Specialist with additional support for psychology will
strengthen the resilience of services.
Improving Access to General Healthcare PTHB signed up to Mencap’s ‘Getting it right’ charter to show their commitment to ensuring that
people with a learning disability get the healthcare they have a right to.
Workforce Implications
•Develop commissioning expertise in learning disabilities
•Develop joint service delivery model with PCC.
Finance Implications
•Joint commisioning of this service with PCC is planned to achieve revenue savings.

147
8.7. CANCER SERVICES
Welsh Government published its Cancer Strategy, ‘Together Against Cancer in March 2012’. This
placed renewed emphasis on the need for tackling cancer by delivering fast, effective and personal
care. For the period 1995-2009 for Powys, there was an average of 380 new cases of cancer per
year. The most commonly diagnosed cancers were breast, lung, bowel and prostate cancer.
Powys commissions all specialist cancer services from external organisations, and its direct service
provision relates to prevention, diagnosis and end of life care. Both of these areas are covered
elsewhere in the Plan. Mortality in Powys is below the national trend, and the one year survival rate
of cancer exceeds the all-Wales trend. The Cancer Implementation Group led by Welsh Government
have developed and agreed a set of well defined priorities. These priorities will ensure that is a
national focus and a clear sense of direction for the next 12 months. Health Boards, Trusts, Welsh
Government, Cancer Networks and advisory structures are expected to work together to ensure
these priorities are delivered. There was also the expectation that these priorities are included
within this plan. In summary the 5 national priorities are as follows:
Organisation of cancer support services to ensure improved services, delivery, planning and
performance;
Primary care oncology;
Develop and pilot a single urgent cancer pathway;
Patient experience;
A National focus on lung cancer.
Focusing on these 5 areas will drive services and performance across Wales over the next 12
months. However, the prioritisation at a national level in these areas does not mean that other
work will not continue. Delivering high quality cancer services that result in good clinical
outcomes and improved survival rates is a key priority for us. In addition to delivering the national
priorities we are focusing on a range of priorities which include the following:
Ensure the delivery of the public health programme and strengthen the early detection of cancer in
primary care;
Ensure the standards for cancer services, including access targets, are met for commissioned
services;
Develop care pathway co-ordination for people with cancer in Powys, being treated out of
County, in partnership with Macmillan;
Complete the feasibility study of chemotherapy outreach services in mid-Powys
Participate in the development plans for Velindre Cancer Centre and the Transforming Cancer
Services in South East Wales Programme.
Preventing Cancer The prevention agenda for cancer aligns closely with the broader public health agenda for the
lifestyle issues of smoking, obesity, health eating and physical activity and alcohol mapped out
elsewhere in this Plan. In addition the continuation of the HPV vaccine programme is a long term
action that will in time reduce the incidence of the cervical cancer.
Tackling cancer by delivering fast, effective and personal care

148
Detecting Cancer Quickly Eligible women aged 50-70 years are invited for breast screening every three years and women over
the age of 70 years can self refer to be screened.
Continue to support screening programmes and target shortfall and inequalities in uptake;
provide training for primary care practitioners in cancer awareness and diagnosis;
Participate in cancer symptom awareness programmes.
Delivering Fast, Effective Treatment and Care The THB will ensure that services are commissioned in line with the standards set out in the Cancer
Delivery Plan, and in line with the Welsh waiting times for access to services. English waiting times
will be used as a proxy for Welsh waiting times. During 2014-15 the waiting times have not been
met for the 62 day urgent suspected cancer route and the THB continues to scrutinise each case to
determine further action that can be taken to improve access.
The THB will commission services to meet the 31 and 62 day targets;
Plan and commission chemotherapy and radiotherapy as close to home as possible;
Commission new technologies through WHSSC as appropriate.
Meeting People’s Needs Further develop capacity within Powys for the delivery of cancer rehabilitation;
Determine an approach to assigning a key worker for each person with cancer and preparation of
care plan;
Delivery of the cancer and non-cancer Lymphoedema Service.
Improving Information Further develop data and information collection for Powys residents irrespective of the location
for treatment;
Report cancer information performance annually.
Workforce Implications
•Develop capacity and skills within community workforce to deliver cancer rehabilitation
•Develop commissioning skills in cancer services
•Upskill workforce through training in primary prevention
Estate Implications
•Develop palliative suite in Powys
•Co-location of primay care and community services
•Enhanced use of e-technology in patient pathways
•Re-patriation of outpatient care to Powys

149
8.8. HEART DISEASE SERVICES
Cardiovascular disease (and within this, heart disease) is one of the most significant population
health issues in Powys. In its commissioning role and through its locality model, Powys THB has a
responsibility to support and ensure that the vision and quality requirements of the national
approach to heart health are being realised in all its provider organisations. Opportunities for this
include close working with and through the South Wales Cardiac Network and WHSSC in their
commissioning and assurance roles.
In line with national expectations, the Powys Heart Disease Delivery Plan sets out action to improve
outcomes from heart disease across key areas, up to 2016.
The Promotion of Healthy Hearts The prevention agenda for heart disease aligns closely with the broader public health agenda for the
lifestyle issues of smoking, obesity, healthy eating and physical activity and alcohol mapped out
elsewhere in this Plan. In addition actions include;
Plan and deliver services to meet the ongoing needs of people with heart disease as locally as
possible to their home and in a manner designed to support self management and independent
living;
To further consolidate local partnership working and to support and facilitate GPs, practice
nurses and community pharmacists to deliver a proactive approach.
The Timely Detection of Heart Disease To identify and implement ways of raising public awareness of the symptoms of heart disease
and provide GPs with timely access to diagnostic testing and procedures for heart disease,
increasing direct access to testing without need for secondary referral, where appropriate;
To provide GPs with timely access to specialist cardiology advice through telephone and email,
speeding diagnosis for people who may not need referral to a clinic.
Fast and Effective Care Development of PTHB locality commissioning plans; Living with heart disease;
Complete work in hand to deliver an outreach outpatient FH service for Powys in Llandrindod, as
part of the wider Powys repatriation programme to deliver prompt and equitable access to
appropriate interventions;
Undertake regular continuing professional development of relevance to the care of patients with
heart disease and establish appropriate educational and clinical audit programmes.
Improving Information Continued roll-out of tele-presence to support rural health care delivery and reduce transport
costs for staff and patients.
Living with Heart Disease Ensure the needs of patients with chronic heart disease (including secondary prevention) are
adequately reflected in the Powys long term conditions and carers programmes and actions;
Plan and deliver services to meet the on-going needs of people with heart disease as locally as
possible to their home and in a manner designed to support self management and independent
living.
Reducing the likelihood of heart disease and improving early detection and long term
care for those living with heart disease

150
In addition to the actions already detailed in the Powys Heart Disease Delivery Plan and following
the publication of the first annual report into heart disease service in Wales (2014) the Heart Disease
Implementation Group have agreed a set of All Wales Heart Disease Priorities supported by a short-
term action plans.
The agreed priorities are:
1. Developing a consistent model for the delivery of cardiovascular risk assessment
2. Delivering the cardiac waiting time target through more effective pathways
3. Developing and piloting component or differential waiting time targets
4. Consider new workforce models of delivery that release capacity
5. Improving participation and case ascertainment in National Clinical Audit
These short-terms priorities will be the focus for Powys THB until September 2015 and will be
reviewed and if appropriate refreshed on an annual basis. Following this the priorities for 2015/16
will include improvement in cardiac rehabilitation and cardiovascular research participation and
uptake of research finding.
Delivery is in line with the requirements of the national General Medical Services contract and the
Quality and Outcomes Framework (as confirmed by the Powys Heart Disease Delivery Plan Needs
Assessment). Powys teaching Health Board has also implemented a number of Local Enhanced
Service agreements with Powys general practices, to further improve the local prevention and
management of cardiovascular disease, including for heart failure and diabetes
The local strategy is to move away from disease-specific expert groups, as such an approach would
not be sustainable or effective in Powys. Further work will be taken forwards under the Powys Long
Term Conditions programme, recognising that patients often have multiple and complex needs
which are more efficiently and effectively managed through an integrated approach.
Workforce Implications
•Development of commissioning expertise in heart disease
•Profesisonal development of Public health, pimary care and community staff in prevention & management of heart disease
Capital & Estate Implications
•Enhanced use of technology in patient pathways
•Local access to diagnostics

151
8.9. DIABETES SERVICES
The incidence of diabetes is increasing as the prevalence of obesity is rising. Diabetes among adults in
Wales is predicted to rise to 10.3% in 2020 and 11.5% by 2030. The current rate of increase in spend
on diabetes is unsustainable, so action must be taken now to address this, focusing on prevention and
condition self management. Type 1 diabetes is not linked to lifestyle behaviours and is one of the most
common chronic diseases in childhood, with significant impact on health, lifestyle and life expectancy.
Whilst prevention is not possible, the active management of care can help prevent complications and
ensure children and young people with type 1 are able to lead full, active lives.
Poor diet and a sedentary lifestyle are major contributors to obesity and many cases of type 2
diabetes. The proportion of adults not maintaining a healthy body weight is increasing in Wales and a
third of children are classed as overweight or obese. Childhood measurement results show that 29%
of children in reception year are overweight or obese, compared with 28% across Wales. Lifestyle
interventions promoting moderate weight loss together with an increase in physical activity can result
in more than 50% reduction in the risk of type 2 diabetes amongst at risk individuals. To improve
individual health outcomes and ensure the sustainability of our health and social care services, it is
essential that people take responsibility for their health and well being and attention is given to the
environmental factors that can assist healthier lifestyles.
“Together for Health – a Diabetes Delivery Plan” was published in 2013 and provides a framework
for action by Local Health Boards and NHS Trusts working together with their partners. It sets out
the Welsh Government’s expectations of the NHS in Wales in delivering high quality critical care
ensuring the right patient has the right care at the right time. For the Powys population, we want:
People of all ages to have a minimised risk of developing diabetes;
Where diabetes does occur, an excellent chance of living a long and healthy life;
To manage the majority of diabetes care within primary care.
The national Diabetes priorities or 2015/16 ensures a national focus and a clear sense of direction
for the next 12 months. In summary the national priorities are as follows:
Focus on improving outcomes in paediatric care for children with Type 1;
Prevention of Diabetes – evidence review and supporting General Practice;
Improving Structured Education and Self Management;
Introduction of Patient Management Information System;
Focus on foot care for inpatients;
Focus on inpatient insulin management.
Focusing on these areas will drive services and performance across Wales over the next 12
months. However, the prioritisation at a national level in these areas does not mean that other
work will not continue. Delivering high quality diabetes services that result in good clinical
outcomes. In addition to delivering the national priorities we are focusing on a range of priorities
which include the following:
Minimising the risk of developing diabetes whilst maximising ability of people to
effectively self care

152
1. Delivery of the THB’s public health programme that will contribute to primary prevention and
secondary prevention of diabetes and its complications
2. Strengthening diagnosis and management of diabetes in primary care and community services
3. Strengthening education programmes for people with Type I and II diabetes including increased
use of e-learning
4. Gaining assurance on the quality of services commissioned from other organisations for diabetes
and that this is aligned to the Diabetes Delivery Plan
This will require the full engagement of primary care as long term partners, as well as joint working
with third sector partners who are supporting the THB in securing clinical leadership and designing
patient education.
Workforce Implications
•Develop commisioning expertise in diabetes treatment and management
•Develop skills of specialised diabetes, practice and community nurses
•Upskill workforce (training in primary prevention)
Estate Implications
•Re-patriation of outpatient care to Powys
•Enhanced use of e-technology in patient pathways

153
8.10. SERVICES FOR END OF LIFE
“Together for Health End of Life Delivery Plan” published in 2013 provides a framework for action by
Local Health Boards and NHS Trusts working together with their partners. It sets out the Welsh
Government’s expectations of the NHS in Wales in delivering high quality end of life care, regardless
of diagnosis, circumstance or place of residence in Wales.
The first all-Wales End of Life Annual Report was published in October 2014 and identified the
following priorities:
Encouraging more people to make a will and share their final wishes with family and friends;
Supporting GPs to ensure that patients are being identified earlier as being in their last year of
life, and can therefore receive support from primary care teams;
Ensuring that systems are in place that supports more people to be cared for and to die in the
place of their choice;
Ongoing implementation of the Welsh integrated care priorities guidance;
Further development of iWantGreatCare in Wales.
Currently funding for hospices is directly distributed and monitored by Welsh Government. The
Minister has agreed, on advice from the End of Life Care Board that with effect from the 2015-2016
financial year, funding for hospices will be distributed and managed by Health Boards and Trusts.
Funding will be ring-fenced for three years and will continue to be allocated on the formula
established by the End of Life Care Board. This will provide greater clarity in the governance of
hospices, with health boards and trusts being accountable for the clinical governance of
organisations from which they are commissioning services. It will also place hospices in a better
position to work with Health Boards and Trusts in service planning by encouraging greater
engagement between them and hospice providers.
PTHB produced its first delivery plan in 2014. For our population we want:
People to have a healthy, realistic approach to dying, planning appropriately for the event;
People to have access to high quality care wherever they live and die whatever their underlying
disease or disability, devoid of any prejudice in relation to their personal situation.
We are monitoring three high-level outcomes to track over time how well we are doing. These are:
whether people are cared for and die in their preferred place of care, whether that is at home, in
hospital, a hospice or in a care home;
the number of individuals whose care is supported by integrating their priorities in care prior to
their death and recognising the inevitable closing of their life;
what individuals and their families say about the care they receive.
Within Powys, palliative care is organised on a local basis for each community around the GP
practice and local community services, including access to community hospital services where
appropriate. There is no in-patient hospice provision within the County, and Hospice Services are
commissioned from the third sector based on a ‘Hospice at Home model.’ Palliative care within
secondary care is commissioned from neighbouring Health Boards in Wales and NHS Trusts in
England. The THB employs Care Transfer Co-ordinators who in-reach to secondary care hospitals to
Ensuring end of life care that is dignified, supported and equitable for all people in
Powys
154
identify Powys residents on the end of life pathway and fast-track their return to Powys where
appropriate.
During 2014/15 a number of service improvements have been implemented locally that have had a
real impact on patient care. Examples of this include:
Service developed in north Powys to support patients and carers at home delivering increased
access to services;
Advanced communication skills and advanced CBT training for the CNS team resulting in very
positive feedback from patients in terms of the difference it had made to how they manage their
diagnosis;
Training programme for carers was well evaluated.
The 2015/16 Delivery Plan sets out actions to improve outcomes in the following key areas:
Supporting living and dying well; informing and supporting patients to make arrangements in advance for the end of life
To ensure that there is a Macmillan GP facilitator to facilitate some of the strategic developments for Powys;
To ensure that there is strategic leadership to drive developments;
Develop an educational plan to ensure ongoing teaching for health care professionals in Powys;
Develop and promote communication skills training for all frontline clinical staff.
Detecting and identifying patients early; people with palliative care needs are identified early to enable the best care to be planned in advance
Continue and develop 7/7 audit to include specialist palliative care advice out of hours, accessing the services;
Continue to identify patients who are expected to enter into a palliative phase in the future
through Virtual Wards, Community Teams and Community Resource Teams around each GP
practice and to develop a process to identify patients approaching end of life to ensure advanced
care planning.
Delivering fast, effective care - People receive fast, effective person-centred care in order to maintain quality of life for as long as possible
Reduce inequalities of service provision across Powys, maintaining access to on-call specialist nurses 24/7 and improving access to community equipment for care at home;
Equitable access to H@H for Ystradgynlais;
Increase local access to treatments and minimise the need for travel by strengthening the commissioning arrangements for end of life care, through contracting arrangements to scope the level of end of life care that occurs in the acute hospital units and monitoring arrangements and work with the Hospice Providers to scope commissioning plans for end of life care;
Annual internal validation of the Powys community specialist palliative care in preparation for peer review;
Increase IWGC returns;
Gather patient stories- one in each team for 2015/16.
Reducing the distress of terminal illness for patients and their families; patients entering the terminal phase of their illness and their families feel well cared for
Ensure that there are appropriate carers available to provide timely care at end of life;
Work alongside Powys carers to identify needs of carers and implement training and support in response to these needs;
Ensure that support is available for replacement of ICP;
Robust roll out of new DNACPR guidance;
Progress the development of end of life suites in identified community hospitals.

155
Improving Information Ensure managers and clinical leaders have effective management information to lead and develop
the service and ensure local research projects are supported;
Develop the resilience of palliative care services with clear transitions of care arrangements in place and improved access to clinical information;
Review intranet site for palliative care and ensure signposting to relevant sites;
Promote the patient / citizen awareness over the preparation and planning for end of life care by improving availability and standard of patient information;
Link with information gathered from harm and mortality reviews in each community hospital.
Targeting research Promote the All Wales Governance toolkit;
Develop audit plan for 2015.
Repatriation of Hospice Funding Ensure commissioning and clinical governance arrangements for hospice care are implemented
during 2015/16, building on the workshop held in December 2014 with hospice providers and
health board palliative care leads to support working arrangements and funding issues.
Workforce Implications
•Developing communication and clinical skills of community workforce in end of life care
Capital & Estate Implications
•Developing fit for purpose accommodation for end of life suites in community hospitals
Finance Implications
•As per specialised plan for integrated care for older people

156
8.11. CRITICALLY ILL
Together for Health – A delivery plan for the Critically Ill sets out the Welsh Governments
expectations of the NHS in Wales in delivering high quality critical care ensuring the right patient has
the right care at the right time. It focuses maximising efficiency and effectiveness, tackling variation
in access and reducing inequalities in service provision across 5 themes:
Delivery Themes: 1. Delivering appropriate, effective ward based care – The Right Patient
2. Timely Admissions to Critical Care – The Right Patient receiving the
3. Right Care at the Right Time
4. Effective critical care provision and utilisation – The Right Care
5. Timely Discharge from Critical Care – The Right Patient receiving the
6. Right Care at the Right Time
7. Improving information and Research.
Powys Critically Ill Delivery Plan The Vision – for our population we want as laid out in the Welsh Government Together for Health –
A delivery plan for the Critically Ill:
Patients and clinicians to discuss and agree appropriateness of critical care and level of escalation
of care in time of need
Patients to have timely access to (where appropriate for their condition and needs) and
discharge from critical care
Patients to be cared for in the correct facility with highly qualified specialists
Patients and carers to be as involved in their care as they feel appropriate
Patients to receive care that is clinically effective.
Powys Teaching Health Board commissions Critical Care services for its population from relevant
NHS provider organisations through its Long Term Agreements in both England and Wales. The NHS
provider is expected under the contract terms to provide continuous access to critical care services.
The Long Term Agreement sets out the quality measures and standards which the NHS Provider
should work to. The agreement also sets out the services our population will have access to in line
with our strategic agenda taking into account clinical and other quality standards. In line with the
National plan, the Powys Critically Ill Delivery Plan sets out actions to strengthen commissioning
arrangements across the key areas and monitor performance of its providers by including the:
National Themes
Assurance Measures
Tiers of Critical Care available
As part of its monitoring arrangements of Commissioned Services through the Long Term Agreement
with Providers
Ensuring that people who are critically ill have timely access to high quality services

157
8.12. STROKE SERVICES
There are on average 230 people admitted from Powys to a District General Hospital with a stroke
each year. On average 15% of these die during their acute admission, 40% are discharged direct
back to their usual place of residence and 45% are transferred back to a Powys hospital for ongoing
inpatient rehabilitation and discharge planning. Powys currently commissions hyper-acute and acute
stroke services from 5 main providers and has a multi-agency Stroke Steering Group which meets on
a quarterly basis to oversee the delivery of the Stroke Delivery Plan. Inpatient stroke rehabilitation
services are based in Brecon and Newtown Hospitals. Emergency hospital admissions with primary
diagnosis of cerebro-vascular disease (stroke), European age-standardised rate per 100,000 persons,
2008-2010 in Wales is 100 for Powys against the Wales average of 124. The national priorities for
2015/16 ensures a national focus and a clear sense of direction for the next 12 months. In summary
the national priorities are as follows:
Identification of individuals with Atrial Fibrillation and awareness campaign for Atrial Fibrillation;
Improve access to Community Rehabilitation;
Reconfiguration of stroke services in Wales including the development of hyper-acute services in
Wales.
Focusing on these areas will drive services and performance across Wales over the next 12
months. However, the prioritisation at a national level in these areas does not mean that other
work will not continue. Delivering high quality stroke services that result in good clinical
outcomes. In addition to delivering the national priorities we are focusing on a range of priorities
which include the following:
Preventing Stroke The prevention agenda for stroke aligns closely with the broader public health agenda for the
lifestyle issues of smoking, obesity, healthy eating and physical activity and alcohol. In addition
Improving the percentage of the population who have cardiovascular risk factors, arterial
fibrillation and high risk Transient Ischemic Attacks (TIA)’s appropriately managed;
Embedding secondary prevention measures into inpatient care and long term follow up reviews.
Detecting Stroke Quickly Supporting public health campaigns on detecting and acting on signs of stroke quickly;
Working with and monitoring performance of WAST to ensure their ambulance clinicians are
competent at identifying suspected stroke and responding accordingly;
Ensuring all GPs are aware of the stroke pathway of their local acute stroke unit.
Delivering Fast, Effective Treatment and Care Engaging in the implementation of recommendations arising from the NHS Midlands and East
Stroke Review and the South Wales Programme to ensure that Powys patients are able to access
high quality hyperacute stroke units within 90 minutes of onset of symptoms;
Ensuring Powys patients are able to access high quality acute stroke and TIA services, including
carotid endarterectomy, in a timely way.
Supporting Life after Stroke Increasing number of stroke survivors;
Who are supported to leave hospital by a stroke skilled community team;
Reducing the likelihood of stroke and improving the quality of life after stroke

158
Who are reviewed by an appropriately skilled health or social care professional six weeks, six
months and 12 months after leaving hospital;
Improving Information Developing service user involvement and having a focus group for stroke survivors as part of
planning Life after Stroke Services;
Develop register of interest for people in Powys affected by stroke to get involved in stroke
service development.
Targeting Research Developing research capacity and registering as a research site with appropriate multicentre
trials.
Workforce Implications
•Development of commissioning expertise in heart disease
•Professional development of pimary care and community staff in stroke rehabilitiation
•Upskill workforce through training in primary prevention
Capital & Estate Implications
•Co-location of primay care and communtiy services

159
8.13. RESPIRATORY SERVICES
Respiratory disease is the cause in one in seven of all deaths in Wales; this is the third largest cause
of death for both women and men in Wales. At the same time, one in seven adults in Wales reports
being treated for a respiratory condition. In Powys, we know that there are over 2,750 people
registered as having Chronic Obstructive Pulmonary Disease (COPD), and 8,480 people diagnosed
with asthma. Respiratory disease is a common cause of severe acute illness, and therefore is a
significant cause of many emergency hospital admissions which for Powys residents can be far from
home.
In 2014, Welsh Government published “Together for Health- a Respiratory Health Delivery Plan”,
which provides a framework for action by Local Health Boards and NHS Trusts to improve respiratory
care across Wales. It sets out the Welsh Government’s expectations of the NHS in Wales in
delivering high quality respiratory care for its population. Powys teaching Health Board will continue
to develop a local respiratory delivery plan in response to this framework.
The Delivery Plan will focus around the following priorities, as identified in the Together for Health
plan:
1. Preventing poor respiratory health Raising awareness with the public on how to live healthy, active lifestyles to help maintain
respiratory health, developing on the work already being undertaken as part of the Invest in Your
Health scheme already being delivered within Powys;
Continuing to promote smoking cessation services with the local population and Primary Care
providers;
Treating every patient contact as an opportunity to promote health and wellbeing;
Encouraging both staff and patients to have the influenza vaccination.
2. Detecting respiratory disease quickly Ensuring respiratory disease is detected quickly where it does occur.
3. Delivering fast, effective treatment and care Ensuring people receive prompt, effective treatment and care for their respiratory condition,
whether adult or child, so that they have the best chance of optimising their quality of life and
improving survival;
We will continue to develop the Respiratory Specialist Nursing Service across Powys. Investment
has already been made in South Powys to employ additional Respiratory Nurses, working with
each of the G.P. practices under the guidance of the Respiratory Specialist Nurse. Plans are now
underway to further develop services across the whole of Powys during 2015;
Ensuring access to Pulmonary Rehabilitation Programmes;
Working with local partners such as the National Exercise Referral Scheme;
Building relationships with the Specialist Nurses , the Community Resource Teams and Minor
Injury Units to develop action plans for those patients in the community most at risk of
emergency admission to support people locally for as long as it is safe to do so;
Where appropriate, working closely with Palliative Care teams to ensure patients with
respiratory disease are fully supported in their care through to the end of life;
Improving respiratory health for the people of Powys, and ensuring timely, effective care
for those with respiratory disease

160
4. Supporting people living with lung disease People to be placed at the heart of respiratory health care with their individual needs identified
and met so that they feel well supported, informed and able to manage the effects of poor lung
health;
Ensuring all patients have self-management plans in place;
Ensuring access to patient information to support people live with and manage their respiratory
condition. This will require work with Third Sector partners to signpost to local services available.
5. Improving Information Working with G.P. practices to undertake Peer Review of emergency respiratory admissions
Regularly analysing service data available on respiratory disease admissions;
Ensuring that the patient’s experiences of respiratory care are captured and used to inform
development of respiratory services;
Using risk stratification tools available to identify patients most at risk in the community to
provide early, preventative interventions to prevent emergency admissions.
Workforce Implications
•Develop business case to recruit additional Respiratory Nurses as part of wider specialist team.
Capital & Estate Implications
•None
Finance Implications
•Investment in Specialist Nursing Team.
•Reduction in cost for emergency admissions through timely interventions to keep people at home.

161
8.14. NEUROLOGICAL CONDITIONS
The Powys delivery plan for neurological conditions has been developed with our partners in
response to the all Wales “Together for Health – A Neurological Conditions Delivery Plan” (2014).
Powys has an above average prevalence of people with a long term neurological condition. It is
nearly 29% higher than expected based on projected data from data from 13 out of 17 GP practices
and there are 2100 people registered with a Powys GP with one or more of 12 main neurological
conditions. The geography and rurality of Powys presents challenges to maintaining a skilled
workforce and ensuring equity of service provision. Many people with long term neurological
conditions have complex disabilities or significant fatigue which can limit their ability to travel. It is
important therefore to ensure that the people living with a Long Term Neurological Condition (LTNC)
in Powys are clear what services and support are available for them locally and what specialist
services they need to access outside of the county. A summary of priorities within the plan is
presented below:
Raising awareness of neurological conditions Work with partners to promote awareness of neurological conditions and related symptoms;
Ensure all staff involved in managing care for people with a neurological condition have an
appropriate understanding of the condition and how it impacts on the individual and their
family;
Develop and maintain a knowledge and skills framework to identify specialist knowledge and
skills available in Powys.
Timely diagnosis of neurological conditions Improve effectiveness of referral pathways to neurology, neurorehabilitation and specialist
services by working with WHSSC, service providers and local GPs;
Monitor quality of commissioned services to ensure timely access to assessments and
investigations;
Develop local services for symptom management to reduce demand on follow up neurology
appointments.
Fast and effective care Develop clear evidence based standards for services and support people with LTNC should
expect, recognising need for different models in different parts of the county;
Work with locality management and commissioning teams and providers to ensure standards of
service are monitored and evaluated;
Build a skilled, competent and flexible network of health and social care professionals working
across Powys to provide services as close to home as possible.
Living with a neurological condition Work with service users, carers and third sector organisations to ensure that people with
neurological conditions have the information and support they need from the time of diagnosis
onwards to manage their own condition proactively to maximise their independence and quality
of life;
Review and build on existing areas of good practice and ensure there is equity of access across
Powys;
Develop new services and the skilled workforce to meet the current gaps in demand.
Ensuring all people with neurological conditions have access to high quality care.

162
Children and young people Develop information systems that can support targeted and coordinated interventions and
support for children and young people, maximising staff capacity and team effectiveness;
Continue to build a competent and flexible workforce and a sound knowledge and skills
framework, ensuring that specialist skills are available when and where required;
Work with service users and providers to ensure clear referral pathways are in place and
standards of care can be monitored;
Have appropriate estate facilities for children and young people to facilitate assessments,
treatments and emotional and psychological support for both them and their families;
Work closely with our local community paediatricians and support them to deliver diagnosis as
much as possible close to the patient’s home.
Improving Research Facilitate the research and development approval process within Powys to ensure that people
from Powys can be included in any specialist centre trials in England or Wales;
Improve links with research centres and explore opportunities to register for any relevant
multicentre trials;
Ensure research evidence and best practice is disseminated widely and forms the basis of any
education, training or service development.
Improving information Ensure service users, carers, health board and social care staff, specialist providers and third
sector organisations are clear about what services and support are available and how to access
them;
Improve data management to improve understanding of demand for, uptake and coordination of
services to inform planning, monitoring and evaluation;
Work with third sector colleagues and public health nationally and locally to promote awareness
of neurological conditions and related symptoms;
Ensure all staff involved in managing care for people with a neurological condition have an
appropriate understanding of the condition and how it impacts on the individual and their
family;
Develop a knowledge and skills framework to identify specialist knowledge and skills available in
Powys, ensure they are maintained and identify gaps where further knowledge and skills are
needed.
Implementation of the plan will be overseen by an implementation group that includes
representation from locality management teams, healthcare professionals, social care and the
third sector as well as service users.

163
8.15. LIVER DELIVER PLAN
The Liver Delivery Plan was published by Welsh Government in 2014 for consultation that closed in
January 2015. The full plan has yet to be finalised and published by Welsh Government. The
consultation planned outlined six areas for action by Health Boards:
1. preventing liver disease
2. timely detection of liver disease
3. fast and effective care
4. living with liver disease
5. improving information
6. targeting research
The Health Board will during 2015 assess its performance against the Plan when it is published in it
final form. The focus of the THB, including the allocation of any additional resources, in line with its
overall strategic objectives will be to:
Consider how to secure clinical leadership for liver disease for the population of Powys;
Consider the implications of the Delivery Plan in relation to the THB’s existing priorities and
programme for public health and adjust as required;
Support primary care to strengthen their approach to early diagnosis of liver disease;
Put in place mechanisms to ensure that services commissioned for people with Liver Disease,
including those commissioned through WHSSC, are aligned to the standards set out in the Liver
Delivery Plan.
8.16. ORGAN DONATION
The THB will secure expert advice to determine its specific role in relation to the new Organ Donation
Bill, with specific reference to deaths in community settings and any associated opportunities to
support the collection of donated organs in this setting. The THB will participate in the other
requirements of the Bill to support awareness raising in the community of the implications.

164
8.17. SUBSTANCE MISUSE
A key component in improving the health and wellbeing of people living and working in Powys is in
developing and implementing a strategy to reduce the harm that substance misuse can cause to
individual people, families and communities.
Actuarial data for Powys suggest that for the adult population (16 to 64 years) incidents of drug and alcohol misuse per 100,000 of the population, while lower than the average for Wales, are significant. Referrals for drug treatment are currently in excess of 400 per year, of which one-third are heroin users. Referrals for alcohol services are in excess of 600 per year, but estimates of the prevalence of harmful or hazardous drinking would suggest that up to 43% of the local population could be at risk of misusing alcohol. It is expected that the Health Board’s expenditure on alcohol and substance misuse should be 0.4% of its overall expenditure. Strengthening individuals and communities to enable them to identify and tackle substance misuse
issues, supported by agencies increasingly working together to integrate services tailored to meet
local need, is the underpinning goal of the Powys commissioning strategy.
The Powys Substance Misuse Commissioning Strategy has been developed in partnership through
the Powys Community Safety Partnership (CSP) and the Substance Misuse Area Planning Board
(APB). The overarching goals of the strategy are to improve outcomes for people at one or more of
the following levels:
Enhancing community capability for self-reliance against misusing substances;
Strengthening families’ skills and abilities to prevent substance abuse and its consequences;
Improving people’s capacity to be safe, healthy and independent from substance misuse.
Commissioning priorities reflect gaps in provision identified in various needs analyses commissioned
by the CSP and APB. These priorities are configured around three key action areas:
Prevention – Initiatives and services which seek to forestall the misuse of substances by groups
of local populations at large or on groups which may be specifically targeted because of the
particular vulnerability to engage in the misuse of substances;
Intervention – Initiatives and services which seek to improve the quantity and/or quality of
support to those who have, or will have, their substance misuse need identified;
Partnerships – Initiatives which seek to improve either the working arrangements between
providers of substance misuse services themselves or their relationships with those organisations
who otherwise provide services or support to individuals whom they may identify as having, or
are at risk of having, a substance misuse need.
The Powys Substance Misuse Commissioning Strategy is due for renewal through consultation in 2015 and the detailed delivery plan will be developed in line with the updated strategy. And priorities for 2015-16 outlined in the Substance Misuse National Delivery Plan:
LHBs to establish alcohol specialist nurses in A&E departments;
Establishing clear protocols and integrated pathways for those with co-occurring substance
misuse and mental health issues in line with revised Welsh Government guidance;
Implement the NHS related activity set out in the Substance Misuse Treatment Framework
‘Improving access to the substance misuse for older people’;
Reducing the harm that substance misuse can cause to individual people, families and
communities

165
Consider and respond to the rise in deaths relating to Tramadol, other prescription only
medicines and over the counter medicines;
Reduce drug and alcohol related deaths;
Reduce the harm associated with substance misuse.
The objectives over the next three years are:
1. Re-commission the generic alcohol and substance misuse service with the Powys Area
Planning Board;
2. Strengthen the clinical governance of PTHB commissioned community and residential
detoxification services;
3. Ensure robust investigation and reporting of fatal and non-fatal poisonings;
4. Strengthen support to primary care to reduce misuse of prescribed medication;
5. Work with the providers to “make the most” of the first contact with alcohol and
substance services – especially for young people under the age of 25;
6. Ensure compliance with joint working protocols between mental health and substance
misuse services.

166
8.18. MATERNITY SERVICES
Powys cares for 1200 women in pregnancy per year, of which 250 currently births in Powys either at
home or in free standing birth centres in community hospitals. The service aims to birth 30% of
women in Powys by 2016, current figures range between 17-20% and anecdotal evidence from other
areas across the UK suggests that Powys is leading the way in ensuring low risk women birth in the
most appropriate low risk service . Steps have already been taken since September 2012 to ensure
that ‘low risk’ women are booked to Powys services as the first option to enable this target to be
reached. In addition the midwifery team will work to maximise the level of ultrasound scanning and
day assessment of pregnant women that is undertaken in Powys facilities, using remote technology
as appropriate. Modernisation of the ante-natal and birth centre facilities currently provided in
Powys hospitals is a key component to increasing local access to services. As strategic service
change in obstetric led maternity care moves forward around Powys’ borders, access to local
services and the use of technology to support local service delivery is increasingly important.
Developing midwifery skills to deliver care traditionally located in District General Hospitals, where it
is safe to do so, will develop a less fragmented pathway for all pregnant women.
A particular public health foci will be to capture the smoking status of pregnant women,
strengthening the promotion of smoking cessation and increasing uptake of influenza vaccination.
Workforce Implications
•Developing skills within midwifery teams
•Skill mix and workforce redisign of midwifery service
Capital & Estate Implications
•Impovements in quality of bithing environments
•Increased ante-natal care provided locally
Finance Implications
•Saving to be achieved with developing in county ultrasound and day assessment services.
Increasing the number of women choosing to give birth within Powys and at home
167
8.19. CHILDREN’S SERVICES
The THB’s children’s services deliver a significant portfolio of public health services and services for
children with urgent and acute health needs. The THB’s vision for these services is to provide as
much of the care pathways as possible within Powys to improve the service offer, experience for
patients and manage cost. Results of a series of consultations with children and families in Powys
demonstrate they want safe responsive services delivered as locally as possible. They want
integrated services for children with a disability and they want to know that when they travel for
specialist NHS services that these are of good quality, and link seamlessly with local services in
Powys. The Plan for Children’s Services is organised into the following principle domains based on
total care pathway management.
Children with Acute and Urgent Health Needs Pilot work undertaken in 2012/13 established that it is possible to review and divert appropriate
referrals into Powys services for children. The service is aspiring to full management control of
elective and emergency paediatric care pathways utilising the professional expertise within the THB,
working alongside Primary Care. Health Visiting, School Health Nursing and Community Childrens
Nursing will review methods of working and undertake analysis of workload and staff requirements
to create additional capacity in consultant community paediatrician sessions to manage the
additional activity being undertaken in-house, a fundamental component in this will be the
development of the community children’s nursing team. Further development of the CNN team will
be rolled out across elective referrals with support provided to general practice to advise on child
health and appropriate referral pathways. As strategic service change in acute paediatrics moves
forward around Powys’ borders, access to local services and the use of technology to support local
service delivery is increasingly important.
Integrated Teams Through its joint working arrangements the THB is following a path of incremental integration of
services for children in relation to services supporting Disability, Emotional Health & Wellbeing and
Family Support. Working in partnership with Social Services and Education this includes service,
management and where possible physical integration in fit for purpose facilities that enable the
seamless delivery of services to children and their families. This will be taken forward as a
transformational programme through the LSB, taking advantage of opportunities such as ‘21st
Century Schools’ to provide the appropriate integrated facilities for children that are required.
Child and Adolescent Mental Health The THB’s overall approach to modernisation of mental health services across all ages,
encompassing the requirements of the Mental Health (Wales) Measure are described in the mental
health chapter. A specific focus for children will be in the development of Community Assessment
and Treatment Team as a more appropriate alternative to avoiding where possible out of county
placements for children.
Safeguarding Safeguarding of children, jointly with statutory partners will continue to be a focus for THB given the
complexity of in-county and cross-border arrangements for children’s services for the County.
Particular proprieties over the life of this plan are to address:
Developing an integrated service providing as much of the care pathways as possible
within Powys
168
compromised parenting;
domestic violence;
safety of looked after children (including those in out of county placements) and those in the
youth justice system.
Workforce Implications
•Increase the joint working arrangements with social services and education.
•Develop skills and capacity within community teams
•Upskill workforce through training in primary prevention
Capital & Estate Implications
•Co-located health and social care and education facilities including CAMHS services

169
8.20. SEXUAL HEALTH
The community based sexual health services in Powys are currently under review with the purpose
of developing a more responsive local service.
Up until July 2014 Genito-urinary medicine consultant led sessions were held once a week in Builth
and Newtown Hospitals (both sessions were held on the same day). This post was a joint post with
Hywel Dda University Health Board. Since the retirement of the consultant there has been no
replacement. Powys residents are able to access services outside of the County. Due to long
standing agreed funding arrangements this does not cause a financial pressure for the organisation
as sexual health service funding is the responsibility of the provider organisation NOT the
organisation of patients’ residence.
Contraceptive services are provided solely through GP Practices. Patients may attend Family
Planning clinics out of county; there is no such service provision within Powys;
Emergency Hormonal Contraception is available through community Pharmacists and Minor
Injury Units;
Medical terminations of pregnancy are provided in the north of the county in Welshpool. The
service is provided by BPAS and commissioned by the north locality;
A small number of surgical terminations are undertaken at Brecon hospital;
HIV and Blood Borne Viruses are managed through accessing specialist services based in
hospitals outside Powys, as there are no specialist / consultant led sessions held in Powys;
The Network Psychosexual Partnership Cymru provides psychosexual counselling sessions in
Powys.
To better understand the health needs of the Powys population, a needs assessment of local sexual
health services will be undertaken during 2015/16. This will encompass services provided and
commissioned by the Health Board, to ensure effectiveness and value for money. The following
national Sexual Health and Wellbeing priorities for 2015/16 will inform the Health Board’s Plan:
Raising awareness of Long Acting Reversible Contraception (LARC) and increase the referrals for LARC for under 18s from maternity services.
Ensure Sexual Health services are available to teenagers;
Provision and delivery of LARC within Substance Misuse services in Wales.
Ensuring access to sexual health services for the population of Powys
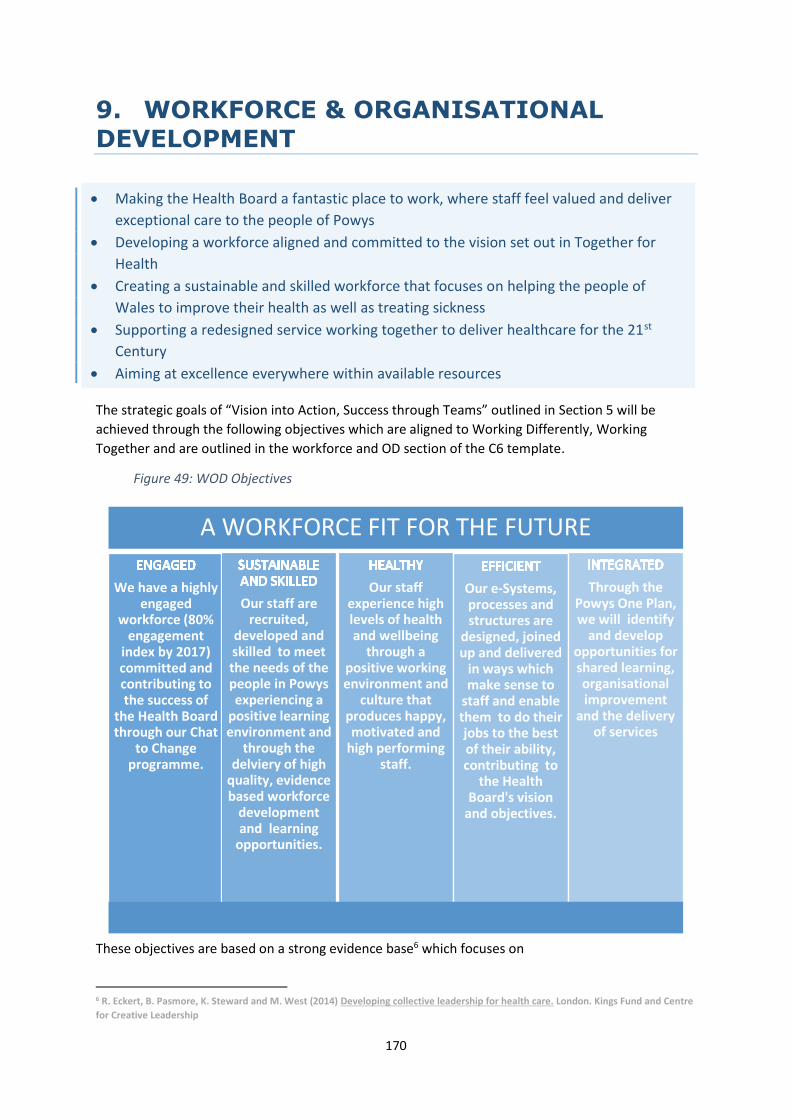
170
9. WORKFORCE & ORGANISATIONAL DEVELOPMENT
The strategic goals of “Vision into Action, Success through Teams” outlined in Section 5 will be
achieved through the following objectives which are aligned to Working Differently, Working
Together and are outlined in the workforce and OD section of the C6 template.
Figure 49: WOD Objectives
These objectives are based on a strong evidence base6 which focuses on
6 R. Eckert, B. Pasmore, K. Steward and M. West (2014) Developing collective leadership for health care. London. Kings Fund and Centre
for Creative Leadership
A WORKFORCE FIT FOR THE FUTURE
We have a highly engaged
workforce (80% engagement
index by 2017) committed and contributing to the success of
the Health Board through our Chat
to Change programme.
Our staff are recruited,
developed and skilled to meet the needs of the people in Powys experiencing a
positive learning environment and
through the delviery of high
quality, evidence based workforce
development and learning
opportunities.
Our staff experience high levels of health and wellbeing
through a positive working environment and
culture that produces happy, motivated and
high performing staff.
Our e-Systems, processes and structures are
designed, joined up and delivered
in ways which make sense to
staff and enable them to do their jobs to the best of their ability, contributing to
the Health Board's vision
and objectives.
Through the Powys One Plan, we will identify
and develop opportunities for shared learning, organisational improvement
and the delivery of services
Making the Health Board a fantastic place to work, where staff feel valued and deliver
exceptional care to the people of Powys
Developing a workforce aligned and committed to the vision set out in Together for
Health
Creating a sustainable and skilled workforce that focuses on helping the people of
Wales to improve their health as well as treating sickness
Supporting a redesigned service working together to deliver healthcare for the 21st
Century
Aiming at excellence everywhere within available resources

171
fulfilment of an inspiring and compelling strategic narrative
clear objectives and priorities at every level from board to front line
supportive people management and leadership
high levels of staff engagement
learning and innovation the responsibility of everyone
high levels of genuine team working and co-operation across boundaries
9.1. AN ENGAGED WORKFORCE
Chat to Change is our flagship staff engagement programme launched in
September 2014 in partnership with our Staff Representatives and with full
support of the Executive Team and Local Partnership Forum. The Chat to
Change concept was based on the findings of the Staff Survey in 2013 and the
key themes which emerged from the Francis Presentations, of which 76% of
our workforce participated. The three key themes that emerged from the
triangulation of this data with the evidence base around staff engagement
were:
- Need for “improved and better communication”;
- Importance of “listening to staff” and “acting on” what is heard;
- Creating a “common culture”, a “culture of care”, “openness”, ”honesty”, with “more focus
on dignity, kindness” and “respect”
Given that the Staff Survey also showed a low degree of confidence that things would change within
the Health Board, Chat to Change needed to give a firm commitment that actions would happen as a
result, hence the focus on turning talk into action.
Our OD Strategy “Vision into action, Success through Teams” fully reflects the evidence base in the
NHS7,8 that links engagement to employee wellbeing, patient satisfaction and clinical outcomes and
it is becoming increasingly clear that engagement is vital to high quality care in the NHS. High
performing NHS organisations which have either sustained or improved engagement significantly
over time have the following characteristics which are endorsed within our Chat to Change
programme:
A strong set of organisational values developed in partnership with employees. These values will
be consistently communicated to employees and upheld within the organisation and informing
all systems, processes and policies. In addition, these values will be lived through all levels of the
organisation and visibly demonstrated in behaviours and decision making.
Visible and approachable Senior Leadership setting the tone at the top of the organisation, with
regular and effective communication between senior leaders and staff, using a variety of
channels.
Whilst Seniors Leaders set the tone, it will be our line managers who are the people who really
make the difference to engagement. They will coach and support their teams, helping remove
7 Dromey (2014) Meeting the Challenge: Successful Employee Engagement in the NHS. The Involvement and Participation Association.
(IPA) London. IPA.
MacLeod D., Clarke N. (2009) engaging for Success: enhancing performance through employee engagement. London. Department for
Business Innovation and Skills. 8 The King’s Fund (2015) Staff Engagement: Six building blocks for harnessing the creativity and enthusiasm of NHS staff. London. King’s
Fund.

172
the barriers that get in the way of their teams doing their jobs. Meaningful appraisals and team
based working will be at the heart of the way we do things in Powys.
A strong employee voice throughout the organisation. Staff will be able to raise concerns and
trusted to take forward improvements within their services as well as being involved in decision
making across the Health Board. A central principle of how we work together will be for decision
making to take place as close as possible to where services are delivered.
Partnership working with our recognised Trade Unions plays an important part in staff
engagement. We already have a good foundation on which to build and enable us to take
partnership working forward based on trust, early engagement, and real involvement in decision
making.
The following achievements and future objectives to achieve an engaged workforce are outlined in
the Figure below aligned with to the “Six Building Blocks for harnessing the creativity and
enthusiasm of NHS Staff.9
9 The King’s Fund (2015) Staff Engagement: Six building blocks for harnessing the creativity and enthusiasm of NHS staff. London. King’s
Fund.

173
Table 19: WOD Achievements and Future Objectives 1. Developing a compelling, shared strategic direction
What has been achieved so far? What else have we planned? When will it happen?
2014/2015 2015 2016 2017
Vision for Health Board shared with staff through 3 Chat to Change
workshops.
Development of social media and the use of blogs to engage staff
Q1
Summary booklet from Chat to Change given to all staff. Development of a Communication Strategy and website development Q2
Strategic Delivery Model and Demand and Capacity work shared
with strategic groups including Local Partnership Forum
Development of vision into simple and persuasive version that engages both
staff and the public
OD Strategy / Programme Brief to support Transformation
Programme agreed
Implementation of OD strategy across organisation “Vision into Action,
Success through Teams”
2. Build Collective and distributed leadership
Launch of Leadership and Management Core Competence
Framework
All Supervisors and Managers to self assess against framework. Learning
needs identified through appraisal process
Q1
Core competences (minimum level) determined for all Supervisors
and Managers
Implementation of redesigned appraisal materials to support Values and
Behaviour Framework and to ensure meaningful appraisals.
Q1
Induction - Delivery of Corporate Induction Day, Workforce
Systems Induction effectiveness and assurance of local induction
processes and induction of New Managers
A refreshed and more bespoke Team Based Working programme will take
place alongside Leadership and Management development pathway using the
on-line Team Journey resource.
Q1 - Q4
3. Adopt supportive and inclusive leadership styles
Linking together appraisal, team based working, IQT, values and behaviour framework with the annual planning process and vision for the organisation
Delivery of a blended learning Coaching programme for managers to develop
a coaching and mentoring style of leadership
Q1
National pilot of NextGen Managers programme attended by
Workforce and OD and Staff Side representative
Delivery of Next Gen programme based on staff engagement evidence , values
and behaviours and coaching as a management style
Q1
ILM Level 5 programme commenced with 19 staff Developing manager’s skills to induct new staff and develop staff through
meaningful appraisals, increasing levels of engagement and developing
effective relationships when managing staff remotely.
Q2
Appraisal rates have dropped this year and have not reached the
target of 85% following the success of 2013/14.
Ensure each Appraiser has no more than 12 staff (optimum 8 -10) to appraise
and a standard that all staff will have meaningful appraisals during 2015/16
(Minimum 95%)
4. Give staff the tools to lead service transformation

174
Staff trained in Project Management, Prince II and Managing
Successful Programmes (MSP)
Managing Change Successfully Programme implemented
Q2
40% Staff trained in IQT and 5 completed Silver Training. Further promote and embed IQT across the organisation: locality based Silver cohorts linked to Chat to Change improvements and Transformation programmes
5. Establish a culture based on integrity and trust
3 Chat to Change workshops held in September/October Values and Behaviour Framework developed and used to inform
recruitment, appraisals, staff development and ways of working.
Q1
Values and Behaviour Framework developed from Chat to Change
Workshops
Values Based Recruitment implemented
Q2
Trained Facilitator in the Strengths Deployment Inventory (SDI) a self
assessment tool that increases people’s self awareness of what
motivates them from a values base and how this can be used to
enhance relationships.
To further roll out SDI feedback to support management and team
development. Used by Powys County Council, this tool supports leadership
development, teamwork and change management.
Q2
Executive Team feedback on SDI as part of Board Development.
6. Place staff engagement of the board agenda
Chat to Change booklet given to all Board Members To identify a Board Level Champion for Staff Engagement Q1
Chat to Change Update presented at Workforce and OD Committee
in February 2014
To have Staff Engagement as a regular/standing item on the Board agenda
Q2
Chat to Change Champion becomes Associate Member of the Board To develop Staff Stories and feature at Board Meetings and other key
events
Q2

175
9.2. A SUSTAINABLE AND SKILLED WORKFORCE
The overarching workforce development plan to ensure a sustainable and skilled workforce to
deliver the planned service changes includes:
Recruitment and Attraction: Succession planning to meet the challenges of the loss of skills and
experience as a consequence of an ageing workforce; governance arrangements for delivery and
access to specialist services. Marketing Powys as an employer of choice in Wales;
Organisational Development and Culture: Further developing the culture as a listening and
learning organisation; adopting evidence based practice;
Health Board as a Public Health Organisation: Embedding public health skills across all levels of
the organisation. Strengthening the focus on health promotion and illness prevention, early
intervention to avoid hospital admission;
21st Century Healthcare Skills: Developing evidence base practices and adopting prudent
healthcare principles; maximising opportunities for using technology to enhance service delivery
and workforce development;
Better Use of Resources / Productivity: Investing in and valuing staff; developing skills in
managing risk within a rural environment, ensuring services are safe and effective; broadening of
roles, developing rural practice, including Advanced Practitioners, extended and new roles,
particularly within clinical workforce;
Integrated Working: Maximising opportunities for inter professional and interagency
relationships; promoting knowledge and understanding of roles across organisational and
professional boundaries;
Use of Technology: Maximising opportunities for Tele-health, Tele-medicine on-line e-health
information and using technology to better manage the workforce;
Support Functions' Capacity and Skills: Developing the THB as a data driven organisation;
developing commissioning and information capacity and capability.
From the C6 Service Change Templates, we have also identified the key workforce implications that
are likely to arise in terms of:
Recruitment and Attraction
Training and Development
Extended Roles and New Skills
Skill Mix
New Ways of Working
Use of Technology
Recruitment Challenges We also have to recognise the context in which these workforce developments will happen.
Although, staff turnover across the Health Board is low, this is likely to increase in the future as a
consequence of an ageing workforce. This has been identified within the Workforce Profile and
presents a significant risk to the Health Board. In particular, there are significant risks identified in
the following staff groups due to the age profiles:
Medical and Dental, including General Practitioners
Nursing and Midwifery
Estates and Facilities

176
In addition, we have current “hotspots” for recruitment in the following areas (identified in C22
template).
Medical and Dental: Consultant CAMHS, Consultant Care of the Elderly and General Practitioners
which also reflects national shortages
Nursing and Midwifery: Currently have recruitment difficulties with Registered Nursing Band 5
vacancies in Machynlleth and Knighton and an Emergency Nurse Practitioner Team Leader Role
in Brecon.
Allied Health Professionals: Physiotherapists, Bands 5 to 7, which also reflects national shortages

177
Whilst the numbers are comparatively small, because of the geographical spread of services across Powys, the impact of even low vacancies in small teams
has an increased impact. To address the challenges for Registered Nurses, we have actively explored Return to Practice which was unsuccessful.
Table 20: WOD Achievements and Objectives - Sustainable and Skilled Workforce A Sustainable and Skilled Workforce
What has been achieved so far? What else have we planned? When will it happen?
2014/2015 2015 2016 2017
Medical Workforce workshop in July 2014 Work in partnership with GP practices on recruitment and attraction
Recruitment and Retention Strategy developed and implemented.
To actively explore new opportunities for introducing Modern Apprentices Q2 continue with success of Work Experience placements and development of Succession Planning/Talent Management. Q3 Overseas Recruitment (Nursing and possibly Physiotherapists) Q1 Assess the implications for Nursing and Midwifery Revalidation Q1
In partnership with GPs, Wales Deanery, British Medical Association (BMA), Consultant colleagues from Health Boards and Trusts have:
Increased opportunities for the placements of medical students and trainee doctors. Raised the profile of Powys as a rewarding place for GPs to work and live
Evaluate the impact of actions taken and further explore: opportunities for GPs wishing to work in Powys but have a portfolio based career Support the modernisation of the way General Medical Services are delivered
Primary Care Workforce Development Group established
Develop Advanced Practitioners in the following fields 1. CMATS (Clinical Musculo-Skeletal Assessment Treatment Service) Physiotherapy 2. Stroke and Neuro-rehabilitation 3. Paediatric and 14+ Physiotherapy Service 4. Cardiac and Heart Failure Service 5. Continence and Urology 6. Diabetes Service 7. Lymphedema Nurse Services 8. Minor Injury Services 9. Parkinson’s Service 10. Respiratory Service 11. Tissue Viability 12. Primary Care
Development of a new GP model and exploring opportunities for networking with other Health Boards and Trusts to secure Consultant sessions
Develop our HCSW Strategy based on our known priorities for the next 3 years and to implement the NHS Wales Skills and Career Framework for Clinical Healthcare Support Workers

178
A Healthy Workforce The Workforce Profile section demonstrates the positive impact of the interventions to decrease
sickness absence which is being achieved despite the challenges of an ageing workforce and the
higher percentage of long term sickness. Reducing sickness absence levels is not just about
application of policy and procedures and there is compelling evidence that high levels of staff
engagement10 can also have a positive impact, supporting the 5 High Impact Changes as
recommended by NHS Employers:
1. Develop local evidence based improvement plans
2. …….with strong visible leadership
3. ………supported by improved management capability
4. ………….with access to better, local high quality accredited occupational health services
5. ……………..where all staff are encouraged and enabled to take more personal responsibility
The Health Board’s Health and Wellbeing Strategy embeds employee health and wellbeing into the
culture of the organisation. The main intention of the strategy is:
A focus on providing integrated prevention and promotion activity and initiatives;
To champion lifestyle improvements, which will enable our staff to benefit from improvements
to their health and wellbeing.
Table 21: WOD Achievements and Objectives - A Healthy Workforce A Healthy Workforce
What has been achieved so far? What else have we planned? When will it happen?
2014/2015 2015 2016 2017
Sickness Focus Group established, driven by high quality workforce information and Absence Call Back Scheme piloted
Continued reduction in sickness absence to less than 4.42% Absence call back scheme rolled out across the whole of the organisation Well being at Work Roadshows
Q1
50.2% of clinical staff vaccinated against flu and 48.5% staff in total Occupational Health Team won the 2015 award for “Most Improved Flu Fighter Team” on behalf of the Health Board.
Year on year increase in flu vaccinations across all staff groups Integration of the Occupational Health Interface with ESR
Q4
Health and Wellbeing strategy developed
Alignment of the Health and Wellbeing workstream with the OD strategy
Q1
Gold Corporate Health Standard achieved in 2012 and maintained
Self Assessment against Gold Standard and work towards Platinum
Q3
10 Dromey (2014) Meeting the Challenge: Successful Employee Engagement in the NHS. The Involvement and Participation Association.
(IPA) London. IPA.
MacLeod D., Clarke N. (2009) Engaging for Success: enhancing performance through employee engagement. London. Department for
Business Innovation and Skills.

179
An Efficient Workforce As a rural organisation which covers 25% of the land mass of Wales and having staff geographically
spread across the county, working efficiently and effectively is a key priority for us. Maximising the
use of electronic systems to support the workforce and enable them to apply the principles of
prudent healthcare is essential to the delivery of high quality care.11 Prudent healthcare principles
that are realised through electronic workforce systems are:
Achieve health and wellbeing with the public, patients and professionals as equal partners
through co-production; All staff having access to e-Systems, understanding their needs to use
the system effectively and working in partnership with key stakeholders to realise the benefits of
e-Systems
Making the most effective use of all skills and resources; using ESR to record staff skills and
competencies and full utilisation of the Learner Management System
Do only what is needed, no more, no less; and do no harm; Enter data once, ESR is the system
Reduce inappropriate variation using evidence base practices consistently and transparently;
Managers and staff with ready access to workforce information and acting on it.
As technology advances and more flexibility and benefits can be realised through ESR 2 and other
workforce e-Systems, we will need to continually review how job roles are designed or updated,
whilst ensuring staff having the necessary skills to fully utilise the e-Systems. Our commitment to
the Employer Pledge and the support of staff to undertake an Essential Skills training programme
in the Application of Number, Communication and Information, Communication and Technology
support this strategy.
The integration of ESR with an e-rostering system will also enhance both the efficiency and
effectiveness of the workforce through effective deployment of the workforce, enhancing patient
safety and providing monitoring and scrutiny of resource allocations.
The management of pay progression in line with national policy which meets the needs of the
service will require:
Realignment of structures at all levels of the Health Board to achieve the vision and objectives
Updating of all job roles to ensure that they are fit for purpose
Table 22:WOD Achievements and Objectives - An Efficient Workforce An Efficient Workforce
What has been achieved so far? What else have we planned? When will it happen?
2014/2015 2015 2016 2017
e-Expenses implemented and 95% registered for ESR self service
Implementation and benefits realisation of Establishment Control and Manager Self Service and ESR 2
Reviewed structural alignment of the provider services to ensure they are fit for purpose
Implement a revised structure and review all structure below Tier 3 Update all Job Descriptions to ensure they are fit for purpose and can be used as a mechanism to realise benefits from national Terms and Conditions
11 Bradley, P. & Willson, A. (2014) Achieving prudent healthcare in NHS Wales (revised). Cardiff: Public Health Wales
Bevan Commission (2015) A Prudent Approach to Health: Prudent Health Principles. Cardiff. Bevan Commission

180
High quality workforce information
Implementation of Business Intelligence
Invest to Save Bid submitted for e-Rostering
Implementation of e-Rostering
Independent review of Communication completed
Implementation of Communication Strategy including upgraded website
AN INTEGRATED WORKFORCE Powys teaching Health Board and Powys County Council are already co-terminous organisations,
serving the same population, largely experiencing the same challenges and opportunities of the
sparsely populated, highly rural county. There is real potential to deliver by working together a
Powys that is a better place to grow up, work, play, grow old and thrive. The Organisation and
Partnership Development Programme for the One Plan covers 3 main themes12:
1. Developing a shared learning organisational approach; with a focus on the successful delivery
of the One Plan, this includes development of shared values and behaviours, a focus on staff
engagement, a shared approach to team development and leadership and management
development
2. Organisational Improvement; identifying opportunities for joining up and integrating systems,
processes, joint business intelligence functions and delivering shared governance and scrutiny
arrangements.
3. Emergent Structures; identifying opportunities for the pooling of budgets, resources and
investments in property, customer services and support services.
Table 23: WOD Achievements and Objectives - An Integrated Workforce An Integrated Workforce
What has been achieved so far? What else have we planned? When will it happen?
2014/2015 2015 2016 2017
Joint workshop with representatives from Workforce and OD from the Health Board and the Council to explore opportunities for integrated working
3 projects exploring an integrated approach to: - - 1) Shared Corporate Services, commencing with Workforce and OD 2) Leadership and Management Development and Talent Management 3) Staff Engagement
Powys teaching Health Board adopted the Strengths Deployment Inventory used within the Council.
12 Local Service Board (2015) Organisation and Partnership Development Programme Brief Local Service Board.

181
KEY OPPORTUNITIES AND CHALLENGES As a primary care commissioning organisation, Powys teaching Health Board is unique in comparison
with other Health Boards and subsequently has some unique opportunities and challenges.
Challenges The main challenge is capacity and this manifests in several ways:
Small teams of staff offering services within a geographical area or specialist services across
the whole of Powys. These services are vulnerable in the event of short term absence or staff
leaving which may lead to services not being offered consistently. This issue is particularly
compounded by the impact of an ageing workforce.
As a small organisation, we do not have the depth of a large infrastructure. This means that
corporate functions and management roles have very broad portfolios with which to
implement national strategy and policy. Within clinical services this translates to staff having a
much broader skill base.
The time it takes to recruit to vacancies will have more of an impact on an organisation the
size of Powys than when compared to other larger organisations.
Opportunities As a primary care commissioning organisation, the future workforce developments within Powys are likely to see increases in the workforce as the flexibility in commissioning services is realised to repatriate service into Powys.
9.3. PROFESSIONAL DEVELOPMENT
Nursing and Midwifery Council Revalidation In January 2016, the Nursing and Midwifery Council are introducing a new revalidation process from
January 2016. As a Health Board, we currently employ 622 nurses and midwives who are registrants
on the Nursing and Midwifery Council (NMC) register. Revalidation will replace the current Post
Registration Education and Practice (PREP) standards with the overarching aim of driving up
professional standards and thereby improving patient care and improving public protection.
Revalidation will reinforce the duty placed on registrants to remain fit to practice.
We are currently in the process of ensuring its readiness for the introduction of the new revalidation
process for registered nurses and midwives. Early indications are that there will be a requirement
for:
Awareness raising for all registrants and training for managers.
Assess the implications for appraisals and ensure appropriate governance as staff approaching
their re-registration date will need to include a ‘professional review discussion’ and ‘sign off’ by
their line manager or, if the line manager is not a Nursing and Midwifery Council registrant, a
‘confirmer’ who meets this criteria.
Within the first year, 206 nurses and midwives, which is a third of our total staff group will be
affected. Coupled with the fact that a high proportion of this staff group are also eligible to retire
and the impact of national changes to the Pensions Scheme, this could potentially a significant
negative impact on our ability to provide a sustainable and skilled workforce. This will be addressed
through our work in recruitment and retention and a specific project on revalidation has also been
established.

182
Moving Care Close to Home and Repatriation Our service strategy clearly outlines our strategic intent to move care closer to home, realising the
benefits of being a commissioning organisation through repatriation. We also need to increase our
community clinical workforce to meet the demands of an ageing population. Whilst, this will focus
on treating ill-health, in parallel we also need to have a strong public health approach, with an
emphasis on preventative health, early intervention and self management. This has implications for
us growing our workforce in Powys as well as investment in new skills.
We have identified the workforce pressures already, namely a small workforce which is geographically
distributed over a wide area and the challenges of recruiting within a rural setting. We therefore have
to be innovative in our approach to workforce development and in line with the principles of Prudent
Healthcare13 we need to focus on:
Principles 1 and 4
Achieve health and wellbeing with the public, patients and professionals as equal partners
through co-production; Reduce inappropriate variation using evidence based practices
consistently and transparently;
We will achieve these principles by working across the whole care system within Powys to ensure
a sustainable service within all settings. Care pathways will be integrated across organisational
and professional boundaries so that people experience as seamless care as possible, irrespective
of who provides it; Planned care will be organised according to care pathways based on clinical
evidence, tailored for individual patient need and clinical condition where appropriate;
Principles 2 and 3
Care for those with the greatest health need first, making the most effective use of all skills
and resources and do only what is needed, no more, no less; and do no harm:
We have identified the challenges for recruitment with regards to General Practitioners, Practice
Nurses, Therapists and Nursing. In response to this need and to achieve these principles, we will
develop Advanced Practitioners across both the Health Board and Primary Care and explore the
opportunities for Physician Associates. To ensure that Registered Clinical Staff are maximising their
own skills, we will develop our Clinical Health Care Support Workers to maximise their contribution
to delivering clinical services.
Education Commissions Education commissions are just one source of where our future workforce will come from, other
mechanisms are through recruitment, retention and attraction strategies and innovative and
prudent workforce development. The workforce assumptions we are working with as part of the
IMTP are that:
1. No plans for workforce reductions;
2. Likely to see that our workforce numbers will increase as we consider the impact of moving care
closer to home through repatriation;
3. We may need to increase our numbers of Registered Clinical Staff because of the impact of
working in a rural community and the broad range of skills that we require to deliver our
services;
13 Bradley, P. & Willson, A. (2014) Achieving prudent healthcare in NHS Wales (revised) Cardiff. Public Health Wales
Bevan Commission (2015) A Prudent Approach to Health: Prudent Health Principles Cardiff. Bevan Commission

183
4. We have an ageing workforce, so over the next 10 years our turnover is likely to increase, so it is
important not to commission based on previous turnover rates but on potential increases;
5. We are not including any provision for Mental Health services as the transfer will not happen
until after March 2015. The education commissions for these services are being submitted by the
managing Health Boards.
From a detailed analysis, from 2008 to 2014, our FTE numbers of Registered Clinical Professionals has
remained largely unchanged. As we move to provide services closer to home, this is unlikely to be a
trend that can continue. Within the education commissioning template (C22), the biggest change is
within Registered Adult Nurses for which the commissions have increased significantly to 75, taking
into the account the needs of our population across all sectors. There have also been slight increases
within Allied Health Professionals which is attributable to high numbers of part-time staff working in
Diagnostic Radiotherapy and Podiatry in particular as well as increases due to moving care closer to
home.
Welsh Language Workforce planning and development will also take into account the requirement to increase the capacity
of the workforce to provide bi-lingual health services. This will be achieved through our Welsh Language
Scheme Strategy. A language skills audit is currently underway will identify any shortfalls which will be met
through a combination of recruitment, training and partnership arrangements and is fundamental to
delivery of the “Active Offer”. For our education commissions for Speech and Language Therapy, we have
identified the requirement for this to be commissioned in Welsh.
9.4. WORKFORCE CHANGES
As a Primary Care Organisation with commissioning responsibilities, we have the flexibility to repatriate services back into Powys to meet the strategic vision of delivering care closer to home. This along with some invest to save schemes is showing that we are forecasting a small increase in our workforce in 2015 by 20.6 FTE in 2015/16 and an anticipated increase in the workforce scheduled for 2016/17 of 0.6 FTE. It is anticipated that there will be an increase in staff in post during the first two quarters of the year as vacancies are filled when compared with the 31st January 2015. As a result, there may be a reduced requirement for the use of temporary staffing, although for the purposes of this plan, we are assuming that current usage will continue. The budgeted projection of 1333.8814 FTE projected for the duration of this plan will never be fully realised through staff in post as this includes headroom for the use of temporary staff. The effective use of temporary staffing will be continued and currently represents 7% of the total workforce. Based on what we currently know, the total contracted workforce FTE is set to increase to 1245.12 by 2018. This expansion is likely to increase further as the workforce implications of Clinical Design and Service Change schemes in C6 are more fully developed. The detail of the increases is provided in Figure 25 and are attributable to service developments and repatriation. There will also be a further increase to this figure to reflect the repatriation of Mental Health Services into the Health Board during 2015/16. These figures are excluded as the decision was only made by the Board in February 2015.
14 The staff in post figures provided in the templates includes secondments from other organisations but EXCLUDES all hosted services.
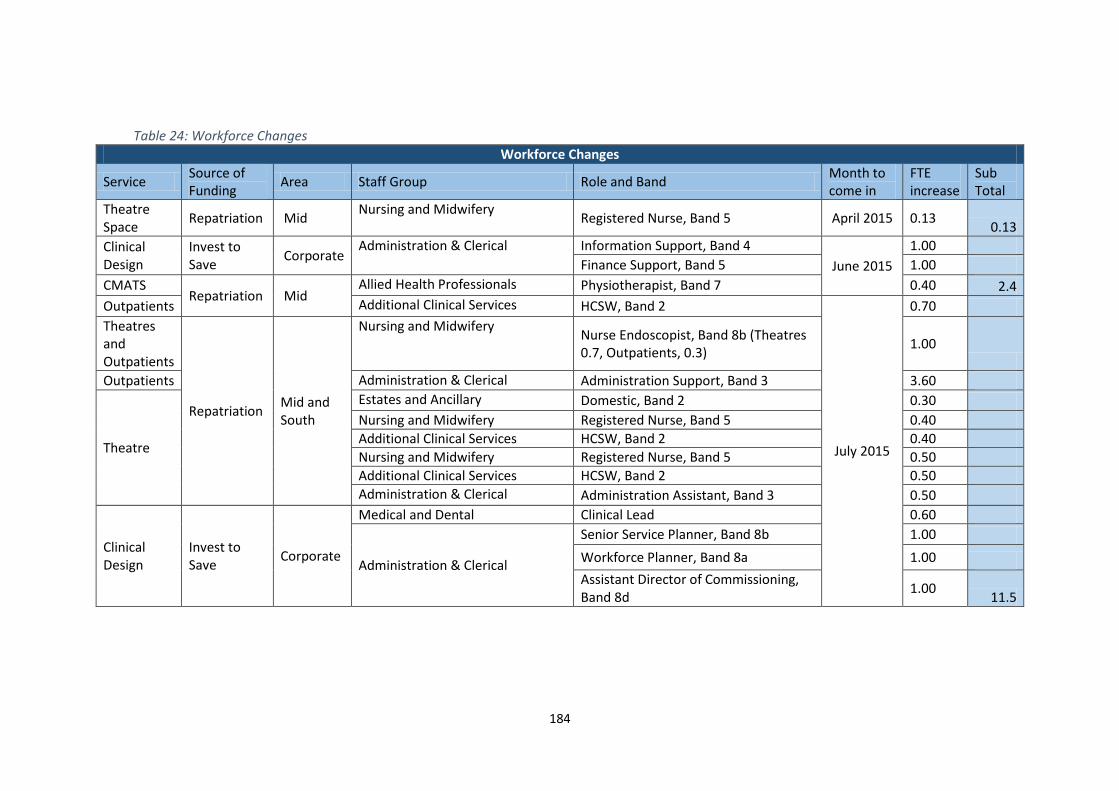
184
Table 24: Workforce Changes
Workforce Changes
Service Source of Funding
Area Staff Group Role and Band Month to come in
FTE increase
Sub Total
Theatre Space
Repatriation Mid Nursing and Midwifery
Registered Nurse, Band 5 April 2015 0.13 0.13
Clinical Design
Invest to Save
Corporate Administration & Clerical Information Support, Band 4
June 2015
1.00
Finance Support, Band 5 1.00
CMATS Repatriation Mid
Allied Health Professionals Physiotherapist, Band 7 0.40 2.4
Outpatients Additional Clinical Services HCSW, Band 2
July 2015
0.70
Theatres and Outpatients
Repatriation Mid and South
Nursing and Midwifery Nurse Endoscopist, Band 8b (Theatres 0.7, Outpatients, 0.3)
1.00
Outpatients Administration & Clerical Administration Support, Band 3 3.60
Theatre
Estates and Ancillary Domestic, Band 2 0.30
Nursing and Midwifery Registered Nurse, Band 5 0.40
Additional Clinical Services HCSW, Band 2 0.40
Nursing and Midwifery Registered Nurse, Band 5 0.50
Additional Clinical Services HCSW, Band 2 0.50
Administration & Clerical Administration Assistant, Band 3 0.50
Clinical Design
Invest to Save
Corporate
Medical and Dental Clinical Lead 0.60
Administration & Clerical
Senior Service Planner, Band 8b 1.00
Workforce Planner, Band 8a 1.00
Assistant Director of Commissioning, Band 8d
1.00 11.5

185
Service Source of Funding
Area Staff Group Role and Band Month to come in
FTE increase
Sub Total
Respiratory Services
Admission Avoidance
North Nursing and Midwifery
Clinical Nurse Specialist,Band 7
August 2015
0.20
Registered Nurse, Band 6 0.37
Community Nurse, Band 5 1.00
Administration & Clerical Administration Support, Band 2 0.60 2.17
Engagement
Invest to Save
Corporate Administration & Clerical
Senior Communication Lead, Band 8c
October 2015
0.40
Engagement Officer, Band 5 1.00
Programme Management Office
Programme Manager, Band 8a 1.00
Programme Manager, Band 8a 1.00
Administration Support, Band 4 1.00 4.40
Clinical Design
Senior Finance Lead, Band 8b April 2016 0.60 0.6
Total
21.20 21.20

186
10. FINANCE
Powys teaching Health Board has a long history of struggling to meet its statutory financial duty. The
dispersed nature of the population which is rapidly ageing makes economic service delivery difficult
to achieve. Therefore, whilst the Health Board has managed to achieve its statutory duty to break
even each year, this has been with additional annual support provided by Welsh Government either
through non recurrent financial support or through the permission for early draw down from future
financial year’s allocations.
This is within the context of the wider unprecedented financial challenge facing the NHS in Wales in
meeting the rising cost of population health needs in an environment of zero growth funding. This
has put a further strain on the Health Board’s ability to break even.
The 3 year financial plan as set out in 2014/15 identified that the gap between income and expenditure
was likely to be £41.7M in 2014/15 rising to £85M in 2016/17 if previous years deficits were to be
made repayable.
During the course of 2014/15 the Health Board has been working hard to make clearer its service
strategy for the longer term and in doing so, defining the scale of opportunity to design and implement
a service that meets the needs of the population whilst striving for the best economic models given
the pressures and constraints as set out above.
In working through our future service models, we have also been successful in gaining financial
recognition by Welsh Government of the structural nature of our challenge and to this end received
in-year £25M additional funding from Welsh Government in recognition of our underlying financial
deficit (ignoring any repayment requirements at this stage) with a commitment to securing funding to
the organisation in the longer term as a demonstration of this recognition.
Whilst this financial commitment from Welsh Government is very much welcomed by the Health
Board, there is a need to ensure that there is no room for complacency. The financial environment for
Health Bodies remains an issue for the foreseeable future and living within our means is a fundamental
component of our three year strategy and beyond.
10.1. FINANCIAL STRATEGY AND APPROACH TO COST REDUCTION
Powys THB’s financial strategy is one of improving services and reducing cost. The THB fervently
believes that the ‘triple aims’ of improving health, enhancing quality and access and controlling costs
go hand in hand. This must be demonstrated across the entire patient pathway regardless of setting
Achieve the statutory duty for financial balance in each financial year
Build an organisation with effective planning and financial management capacity and
capability

187
or organisational boundary. To this end, we fully embrace the opportunities afforded through our
coterminous boundary with Powys County Council and the joint Integration agenda we are pursuing.
Improved quality at reduced cost is at the heart of the prudent healthcare idea and the Health Board
fully embraces the 5 principles as set out by the Health Minister in his written statement in July 2014
•Do no harm. The principle that interventions which do harm or provide no clinical benefit are
eliminated;
•Carry out the minimum appropriate intervention. The principle that treatment should begin with
the basic proven tests and interventions. The intensity of testing and treatment is consistent with
the seriousness of the illness and the patient’s goals;
•Organise the workforce around the “only do, what only you can do” principle. The principle that all
people working for the NHS in Wales should operate at the top of their clinical competence. Nobody
should be seen routinely by a consultant, for example, when their needs could be appropriately
dealt with by an advanced nurse practitioner.
•Promote equity. The principle that it is the individual’s clinical need which matters when it comes
to deciding NHS treatment;
•Remodel the relationship between user and provider on the basis of co-production.
These directly link in with the financial strategy as set out by the board in the previous 3 year plan
and further builds in further some additional aspects, particularly around patient engagement.
The updated financial strategy is set out below along with its associated link to prudent healthcare.
Figure 50: Financial Strategy
Clear pathways of care that demonstrate the most appropriate care in the most appropriate setting. The intended consequence is a reduction in unnecessary steps and delays which in themselves can drive costs upwards through poor clinical outcomes. There is a real opportunity in Powys given the coterminous boundary with Powys County Council to develop integrated services (Do no harm, carry out minimum appropriate intervention, Organise the workforce around only do what you can do)
Each component of the clinical pathway to be efficiently commissioned. Our costing work has observed that there is variation in our cost bases where delivery is at similar scale and complexity. This is observed across a range of service. Again, there is opportunity to do this in partnership with Powys County Council (do no harm, carry out minimum appropriate intervention, organise the workforce around only do what you can do)
Improvements in clinical systems and processes. This will reduce demand for higher cost healthcare, and deliver a higher quality, more efficient right first time system with improved patient experience and outcomes (do no harm)
Tackling inequalities in resourcing. We have identified that our geographical spend profile is weighted significantly more towards the Mid/South end of the county across both general and mental health services as compared to the North (Promote equity)
Economic model - Care closer to home. The preferred approach is to promote care at or closer to home where the evidence indicates this will provide the right outcomes for the patient and can be demonstrated to provide value for money (co-production)

188
10.2. “SHIFT LEFT”
The fundamental approach to the 5th element of our financial (and service) strategy as set out above
is the push to shift services from specialist to mainstream, from secondary to primary and from
primary to self care. In planning the management of patient needs, designed in partnership with
them, we aim to provide care at an early point of intervention that meets needs in the way a patient
needs it, not necessarily based on the Heath Service’s traditional perception of needs and aids to
prevent the escalation to higher levels of care. Key to achieving this will be to use anticipatory care
models to shift from unplanned to planned care.
The concept of “shift left” and how it is framed within the financial strategy and prudent healthcare
approach is presented in the diagram below.
Figure 51: SHIFT LEFT
As a commissioner of services in Wales, enacting this strategy poses some challenges within the
current financial regime. The ability to robustly challenge providers on costs and seek the benefit
from changes in approach is problematic given the lack of a means to shift costs appropriately
between organisations. This is an issue with which we continue to work at a national level and with
Welsh Government.
For Primary Care and in particular General Practice, the concept of shifting left poses both problems
and solutions. With the impending removal of the Minimum Practice Income Guarantee (MPIG) from
mainstream GMS services, we are mindful that the capacity for practices to take on new and
additional work could be limited without the requisite investment. The ability to release funding to
enable service development and expansion in the primary care arena is therefore critical to the
success of the health board in enacting our service and financial strategy and to ensure sustainability
of services for the population.

189
The Health Board is already making progress in shifting resources left and this will continue to be the
targeted approach which we will track through our financial investment and disinvestment
processes. Figure 52 below demonstrates through our programme budget cost returns how progress
is already being made in shifting costs from secondary care to primary for diabetes and other related
conditions.
Figure 52: Programme Budget expenditure extract
Within our plan for the coming three years whilst we have specifically targeted cost reduction /
growth avoidance within secondary care and consciously invested any new funding into primary and
community care. Figure 53 below presents our 2015/16 Financial Plan compared to 2014/15
outturn. The scale of shifting left is still only small scale and it may take many years to truly make
substantial inroads in reducing secondary care (whilst facing rising annual growth in demand) and
demonstrate the shift towards primary secondary care.
Figure 53:2014/15 outturn to 2015/16 budget
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
2010-11 2011-12 2012-13 2013-14
£
Endocrine, Nutritional and Metabolic Conditionsspend £000s
Primary care total
Total secondary care
£60.10
£58.90
£66.30
£62.60
£90.20
£90.40
£29.40
£29.30
£0.00 £50.00 £100.00 £150.00 £200.00 £250.00 £300.00
£M
£M
15
/16
Bu
dge
t1
4/1
5 O
utt
urn
2014/15 outturn to 2015/16 budgetShift Left
Primary care services Provider services Externally Commissed Services WHSSC

190
During 2015/16 we will further develop our systematic approach to gathering cost intelligence on
the effectiveness of investments in primary care with a view to reducing costs/ slowing growth in
secondary care.
10.3. SCOPE AND SCALE AND MANAGEMENT APPROACH TO COST REDUCTION
As reflected in last year’s financial plan, the Health Board commissioned two independent reviews to
consider both the way in which the health board develops its financial planning and the scope of
opportunities to reduce costs. The conclusion of both reviews made clear that there are insufficient
opportunities for the Health Board to make the cost reductions required to meet the THB’s
underlying financial challenge without significant detriment to access to services. This has been
recognised by Welsh Government with their commitment to funding our underlying structural deficit
of £25M.
During 2014/5 the Health Board further commissioned an independent review for a more detailed
analysis on the scope of opportunities to reduce costs. Unsurprisingly, the scope of cost reduction
was of a similar scale to that reported by the first review, but its conclusions have allowed the
Health Board to plan in a more granular way the approach it will take to cost reduction.
As set out in the previous chapters of this plan, our ambition is to become system leaders in
Commissioning, Primary Care and Community Models and through Integration with Powys County
Council.
This approach is exactly mirrored in the Health Board’s approach to cost reduction and future
sustainability.
Commissioning The two independent reviews conducted at the invitation of the Health Board have identified that
there is opportunity for service efficiency across the range of services the health board both
commissions and directly provides. The Commissioning Development Programme will aid the Health
Board to develop the service redesign which is in its gift without major transformation to
commission greater efficiency in services from externally commissioned services. Further, the
development of a clear commissioning plan for the Health Board will enable better procurement
Commissioning
•Capacity and demand
• facilitating shift left
•prudent approach
• driving quality & efficiency
Primary Care and Community Model:
•Resilient primary care sector
• increased direct service provision
•clinical leadership of system
Integration
• Joint neighbourhood teams
• joint supporting systems eg CCIS;
•Mature partnerships with all providers

191
relationship with service providers with a view to improving both quality and cost. Our savings
programme over the life of this plan assumed significant avoidance of growth and cost reduction
from our externally commissioned services, strengthening our arrangements will be fundamental to
delivery.
The Health Board will work closely with the national programme emerging around a national
infrastructure around commissioning in order to maximise benefits through system efficiencies.
Primary Care and Community Model The Health Board is uniquely placed in Wales to be at the forefront of developing services in
partnership with primary care contractors. Further, the independent review has identified that there
is scope for greater future service and financial sustainability through the redesign of community
services.
Developing robust, sustainable primary and community care services are at the heart of our “Shift
Left” agenda and care closer to home as the protective guard against the predicted growth in
secondary care service demands for our aging population.
Integration The Health Board has successfully implemented a robust Section 33 agreement with Powys County
Council with the intention of developing and implementing a range of integrated services under its
umbrella. Further the development of the Powys “One Plan” signals the clear intent of Integration.
Whilst there are only a few services fully pooled at present, the implementation of the One Plan will
demonstrate a steady growth in integrated services which will provide a platform of greater service
efficiency through partnership working.
To help facilitate taking our relationship with the council a stage further, the Health Board has been
invited by Welsh Government to prepare a bid for support which was submitted as an expression of
Interest called “Working Together” in November 2014. The value is £0.950M over the next two years
and will facilitate the closer working arrangements between the two organisations through
programme management and front line leadership of integrated services. This financial plan
assumes the Health Board will receive a positive response to the invited bid and as such 50% of the
bid has been included in our income and expenditure assumptions.
Of course of Powys, Integration is not just about our relationship with the council, our future success
will also be wholly reliant upon creating in-county critical mass and efficiency through the
establishment of strong, strategic and operational relationships with our range of other partners
including other Health Boards, the Primary Care Sector and with the Voluntary / Independent Sector.
This is necessary to prepare for the inevitable rise in service demands that will be placed by our fast
rising elderly population in future.
Information for Decision Making An underpinning strategy to the development of the above three ambitions is the need for robust
financial information upon which to make reliable decision making. Good progress has been made in
recent years to develop the commissioning database which enables the Health Board to model the
implications of commissioning vs direct provision. This database was used by the recent independent
review to complete the financial modelling work which unpins our current savings programme.
During 2015/16 we will continue with our costing development programme to underpin
assumptions within the developing Strategic Delivery Model. We will further develop our cost

192
intelligence gathered across the different sectors from whom we commission to help guide our focus
for attention for the further development of our future year’s savings programmes.
Primary Care led Service Development At the heart of our transformation agenda is the engagement and anticipated leadership from the
primary care clusters to aid the development of our service improvement programme. The
organisation’s budgets are currently delegated to locality level based on geographical spend with
performance against commissioned services shared with clusters to help spark the debate for service
improvement. Coupled with the Information for Decision Making outputs, these have been powerful
hooks from which debate around the potential for alternative models of care to improve both
patient experience and securing local sustainability and efficiency.
It is from this approach that a number of service models have been debated and developed including
the Virtual Ward models across Powys. A range of care pathways are being further developed at
locality level with lead input from primary care whose aims are to achieve care closer to home within
an affordable / reduced cost envelope. During 2015/16 we will explore the feasibility and benefits of
delegating budgets to cluster or practice level.
Enabling Delivery Achieving delivery of this 3 year plan will not be easy and relies on a number of key investments the
health board has judged to be essential to successful delivery. These are referenced throughout the
plan but summarised here are the following
Investment in the strategy delivery programme. We have profiled in 0.2M towards the additional
resources needed to deliver our key outputs for 2014/15 but in totality, the health board plans to
resource up to £2.2M over the next 3.5 years. It is our intention to secure funding for this vital
programme during the course of this planning cycle through invest to save or other means
Investment in an associate director of commissioning to support the organisation in developing
its commissioning programme at £0.085M per annum
Investment in resource to support our working relationship with WHSSC at £0.050M per annum.
We have assumed this will be afforded through the corresponding cost reduction we expect to
result in our WHSSC commissioned services, thereby neutral to the health board
Investment in our iteration agenda with Powys County Council. The Health Board has assumed its
success in the expression of interest to Welsh Government with our 50% share of the £0.950M
over two years included in our plan
Investment in the establishment of EASC, our share of which is £0.020M
Investment in Future Fit and the South Wales Programmes at £0.2M per annum. Our anticipation
is that the expected contribution – both financial and our staff time – will only grow with the
significant change programmes taking place around our borders as demonstrated in the previous
chapters and in particular with Wye Valley Trust and the Mid Wales Programme. This will
continue to be the basis of discussion with Welsh Government given our capacity to manage not
only our own change programme but the necessary active engagement with those around us.
During 2015/16 we will again review our financial governance arrangements with the Finance and
Performance Committee to ensure we are focussing our efforts in the right place, targeted at the
higher risk delivery of the plan. As part of this process, we will review our budgetary control
procedure to ensure it remains fit for purpose.

193
10.4. THREE YEAR SUMMARY FINANCIAL PLAN AND FINANCIAL ASSUMPTIONS
The three year financial plan has been developed using the latest assumptions regarding the Health
Board’s likely funding from Welsh Government, the likely cost pressures facing the organisation and
the most up to date position in respect of the cost saving potential of the service and workforce
strategy.
Our major modelling assumptions are as follows
There will be no repayment of the debt incurred with Welsh Government in 2013/14
The £25M funding allocated by Welsh Government in 2014/15 will be repeated in each of the
three years of this plan
Our base assumptions for years 2 and 3 are a 2% cash uplift from Welsh Government across all
income streams which will be passed onto Welsh providers and Primary Care contractors
Cost reduction opportunities identified within the external reviews have been factored into the
three years savings programme where they have been assessed as a feasible delivery model.
The recently announced invest to save funding has been factored into the plan in terms of both
income and repayment.
The recently announced additional funding for the NHS in Wales (£80M across various priorities)
has been assumed to attribute upto £3.120M additional funding to Powys THB. The plan
identifies how this investment will be used if successful and therefore remains a risk to the plan
until / unless approved.
In summary, our financial plan for the following 3 years is presented in Table 25 below.
Table 25: Summary Financial Plan 2014/15 – 2016/17
The Financial plan presents a break even solution for 2015/16 and a modest surplus in future
years based on the base scenario requested by Welsh Government.
Pay & Employee Benefit Expenses 50.026 50.576 51.183
Non Pay 23.145 24.119 23.990
Primary Care Contractor 34.504 35.627 36.323
Medicine Management 26.877 27.371 27.866
Continuing Care and Funded Nursing Care 13.764 14.095 14.429
Commissioned Services 123.264 124.170 126.069
Depreciation 2.540 2.540 2.540
Other Income (6.499) (6.525) (6.542)
Resource Limit (267.621) (272.973) (278.433)
Net position 0.000 1.000 2.575
2015/16
£M
2016/17
£M
2017/18
£M
Financial Plan Summary - by Category of Spend
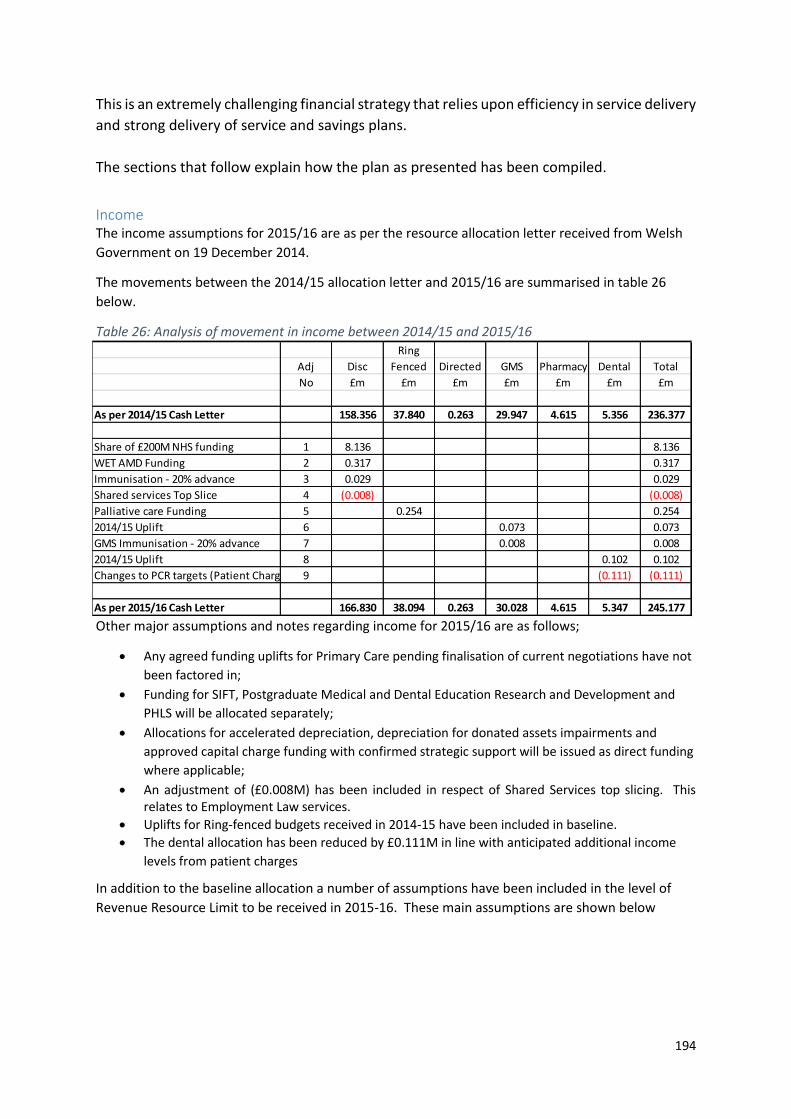
194
This is an extremely challenging financial strategy that relies upon efficiency in service delivery
and strong delivery of service and savings plans.
The sections that follow explain how the plan as presented has been compiled.
Income The income assumptions for 2015/16 are as per the resource allocation letter received from Welsh
Government on 19 December 2014.
The movements between the 2014/15 allocation letter and 2015/16 are summarised in table 26
below.
Table 26: Analysis of movement in income between 2014/15 and 2015/16
Other major assumptions and notes regarding income for 2015/16 are as follows;
Any agreed funding uplifts for Primary Care pending finalisation of current negotiations have not
been factored in;
Funding for SIFT, Postgraduate Medical and Dental Education Research and Development and
PHLS will be allocated separately;
Allocations for accelerated depreciation, depreciation for donated assets impairments and
approved capital charge funding with confirmed strategic support will be issued as direct funding
where applicable;
An adjustment of (£0.008M) has been included in respect of Shared Services top slicing. This relates to Employment Law services.
Uplifts for Ring-fenced budgets received in 2014-15 have been included in baseline.
The dental allocation has been reduced by £0.111M in line with anticipated additional income
levels from patient charges
In addition to the baseline allocation a number of assumptions have been included in the level of
Revenue Resource Limit to be received in 2015-16. These main assumptions are shown below
Ring
Adj Disc Fenced Directed GMS Pharmacy Dental Total
No £m £m £m £m £m £m £m
As per 2014/15 Cash Letter 158.356 37.840 0.263 29.947 4.615 5.356 236.377
Share of £200M NHS funding 1 8.136 8.136
WET AMD Funding 2 0.317 0.317
Immunisation - 20% advance 3 0.029 0.029
Shared services Top Slice 4 (0.008) (0.008)
Palliative care Funding 5 0.254 0.254
2014/15 Uplift 6 0.073 0.073
GMS Immunisation - 20% advance 7 0.008 0.008
2014/15 Uplift 8 0.102 0.102
Changes to PCR targets (Patient Charges) 9 (0.111) (0.111)
As per 2015/16 Cash Letter 166.830 38.094 0.263 30.028 4.615 5.347 245.177

195
A major assumption within the plan is that whilst £8M additional funding has been allocated by
Welsh Government as part of the £200M funding for NHS Wales in 2015/16, the Health Board has
assumed that this will be made up to £25M.
This income level includes the assumption that £3.160M will be received in respect of WG primary
Care and other funding priorities. This represents an assumed 4% share of the £80M funding
announced.
The proposed use of this funding which has been built into our expenditure assumption is set out in
the table below and presents the Health Board’s priority development areas around primary care,
Integration and other Welsh Government priorities as set out in previous chapters to this plan.
These proposed investments and their rationale are set out in the previous chapters to this plan and
are critical to the success in delivering our proposed service change programmes in line with our
strategic direction.
£000's
2015-16 Baseline - as per WG letter 245,177
Resource funding - assumed uplift from
£8.136M to £25.000M
16,864
Primary Care Funding 3,160
Working Together 285
Pay Award 542
Post Allocation letter recurrent allocations 24
Other 1,569
Total RRL 2015-16 267,621
Primary care
Fund
Primary care
developments
Intermediate
Care Fund
Implementing
delivery
Technology
FundsTOTAL
Assumed Income 0.360 1.200 0.800 0.400 0.400 3.160
Details of proposed expenditure
Virtual ward 0.235 0.235
Medical models 0.380 0.380
Lifestyle LES 0.390 0.390
Social enterprise 0.050 0.050
Workforce testing 0.150 0.150
GP triage 0.150 0.150
Diagnostics 0.075 0.075
Sustainability 0.100 0.100
CCIS 0.160 0.160
Stroke 0.085 0.085
Dental 0.040 0.040
0.275 0.275
ICF 0.800 0.800
GP Clusters 0.270 0.270
Proposed Expenditure 0.420 1.380 0.800 0.400 0.160 3.160
Delivery programme, i.e. cancer, diabetes,
respiratory

196
In addition it has been assumed that WG funding will be received in respect the costs of the pay
award and Working Together our joint bid with Powys County Council.
Taking into account the income from Welsh Government together with anticipated
allocations and other income, the opening funding within the financial plan for Powys
teaching Health Board is £274.120M.
10.5. COST PRESSURES
The Health Board has estimated that its costs will grow by £6.682M (2.5%) in 2015/16 and
cumulatively by £19.49M over the next 3 years, averaging at around 2.5% per year.
The current analysis of cost pressures captured over the 3 years of the plan is summarised in table
27 below with explanatory notes beneath.
Table 27: Analysis of Cost Pressures 2015/16
Underlying Financial Deficit (£3.6M) At the time of preparing this report, the Health Board is forecasting a financial deficit of £1.0M at
month 11. Due to the non recurrent underspends achieved in 2014-15 we have assessed the
recurrent impact of 2014/15 on the organisation to be an underlying deficit of £3.6M.
Old Year Recurrent Impact on 2015/16 (-£1.3M) There are a number of issues which commenced in 2014/15 and will have an increased impact in
2015/16. These are summarised as follows;
Externally Commissioned Services £2.4M
Continuing Healthcare £1.4M
Joint financing £0.2M
Primary Care (Improvement Grants) (£0.4M)
Total 14-15 Recurrent Cost pressures £3.6M
Less Non recurrent mitigation in 14-15
Underspend on provider services (notably pay) £2.3M
Income received above plan £0.3M
Forecast Outturn (as at Month 11 ) £1.0M
Cost Pressure2015/16 £M
% of
Funding
2016/17
£M
2017/18
£M
Underlying Financial Deficit 3.597 1.37%
Old Year Recurrent Impact on 2015/16 (1.315) -0.50% (1.940) (0.192)
New Year Cost Pressures 9.959 3.78% 8.764 6.176
Reduction in Contingencies (1.350)
Assumed WG funding (4.209)
Total cost pressures 6.682 6.824 5.984
Additional WG funding in line with 2% increase (3.284) (3.332)
Total Anticipated Cost Pressures before savings applied 6.682 2.54% 3.540 2.652

197
Table 28: Impact of 2014/15 on 2015/16
Repayment of VERs funding
The repayment in 2014/15 of VERS funding received in 2013/14 is a non recurrent expenditure item
only.
Non recurrent achievement of savings in 2013/14
The reviews with budget holders have identified £1.165M of savings which, in their view, cannot be
achieved again in 2014/15. The major component within this sum is posts that have been
temporarily held as vacancies but have now been filled.
Non Recurrent Provisions
The Health board provided for potential costs in respect of meeting the RTT target in 2014/15. This
has been removed from the baseline taken forward, but will be addressed in the plan under new
year pressures
New Year Cost Pressures (£9.95M) New Year cost pressures are those we anticipate being incurred as new additional expenditure in
2015/16 and include issues such as inflationary increases / cost of living and the expected impact of
demographic growth.
These have been collated and compiled on a national basis and therefore the Health Board’s
planning assumptions are in line with intelligence on likely cost increases at a national level.
Old Year impact on new year2015/16
£M
% of
Funding
2016/17
£M
2017/18
£M
Repayment of VERs funding (0.800)
Non Recurrent achievement of savings in 2014/15 1.165
Non recurrent provisions (1.750) (1.940) (0.192)
Other Cost Pressures 0.070
Total Impact of 2013/14 on 14/15 (1.315) -0.50% (1.940) (0.192)

198
Table 29: New Year Cost Pressures
Inflationary / cost of living (£1.18M)
This includes
o 1% pay increase to total pay costs (£0.464M)
o Staff increments (£0.473M)
o Increase in employers pension contributions (£0.107M)
o Reduction in travel mileage rates (-£0.290M)
o Non pay increases on budgets for statutory and unavoidable costs (£0.158M)
o 1.2% CHC price increases (£0.141M)
o 1.2% NHS Funded Nursing Care (FNC) (£0.025M)
o 1% increase for the voluntary / independent sector (£0.020M)
Apart from pay, incremental drift and FNC which will follow a national approach, the Health Board
will consider how or whether these assumed cost increases will be directed on a case by case basis,
dependent upon the nature and value of agreements in existence.
The Health Board has also included the WG funding that will be received in respect of the cost of the
nationally agreed 1% pay award to partially offset these pressures
Impact of demographic growth / demand on services (£3.743M)
Quantifying the impact of demographic growth is difficult to assess. We have taken some judgement
from past experience and applied to the future and as such remains somewhat speculative. This is a
highly volatile area and therefore one which invariably could have the greatest in-year impact (both
good and bad).
Commissioning Costs 3% (£2.315M)
NICE / High Cost Drugs expansion, assessment taken from national intelligence (£0.210)
Continuing Healthcare/FNC 3% (£0.416M)
Prescribing volume growth 3% (£0.802M)
Local Cost demands (£5.033)
The THB has included a number of local cost demands for the coming financial year.
New Year Cost Pressures2015/16
£M
% of
Funding
2016/17
£M
2017/18
£M
Inflation / Cost of Living Increases 1.184 0.45% 1.913 1.471
Impact of Demographic Growth 3.743 1.42% 4.162 3.705
Local Cost Demands 9.959 3.78% 2.689 1.000
Reduction in contingencies (1.350)
Assumed WG funding (4.209)
Total New Year Cost Pressures 9.327 3.54% 8.764 6.176

199
Reserve to meet RTT target (£0.725M) - The Heath Board has estimated that between £0.7M
and £1.3M will be required to meet the RTT backlog to meet the 36 week target dependent upon
whether capacity can be secured within welsh secondary care at marginal cost or with the
private sector at full cost. This plan assumes we will achieve efficiency in delivery from our
partners and ourselves to limit the financial impact of meeting these targets
Commissioning pressures (0.597M) – predominantly WHSSC (£0.377M) as per their latest plan
Cost of capacity – Strategic delivery model (£0.213M)
*Rollout of the Virtual Ward across North and Mid Powys (£0.182M)
*Implementation of E Rostering (£0.056M)
*Energy Management schemes (£0.056M)
*Pharmacy support to Community hospitals (£0.044M)
Welsh Risk pool (£0.360M)
IMT, predominantly Community Care Information Service (£0.160M)
Investment in Primary Care and other WG priorities (1.873M)
HQ support (£0.265M)
For several of the items listed above (*), the health board were successful in securing Invest to save
funding to cover 75% of the costs. The costs included above relate to residual 25% of the costs.
The costs have been partially mitigated by the release of unallocated contingency of (£1.350M) and
assumed WG primary care funding of £3.160M
10.6. SAVINGS PLAN
The Health Board has estimated that £15.5M cost reductions could be realised over the coming
three year period (average 2.0% per year) across the range of our services as summarised in Table 30
below.
Table 30: Details of Savings Plans 2014/15 – 2016/17
As set out at the start of this chapter, the Health Board is employing a variety of approaches to cost
reduction with the intention of reducing or eliminating the current financial deficit. Our approach to
reduce costs and the corresponding expected cash releasing savings are set out below
Commissioning The Health Board set up a review of commissioning in 2014/15 which is referenced earlier in this
IMTP and the recommendations will feature as part of our plan for the coming three years.
There is also growing recognition between NHS Wales organisations that given the significant
programmes of service change emerging across Wales i.e. South Wales Programme, the mode of
Details of Savings Plans2015/16
£000's
2016/17
£000's
2017/18
£000's
Commissioned Services 3,070 3,436 3,182
Primary & Community Care 3,612 1,106 1,050
Total Savings Plans 6,682 4,541 4,231

200
effecting financial flows needs a far more sophisticated approach to reflecting the altered burden of
cost between organisations in reflecting changes in patient flows.
A major assumption to our financial planning is that these out of date processes will be modernised
during the lifetime of this plan to enable the Health Board to move its funding for the further benefit
of care to its residents. Our approach will follow both strands which encompass better efficiency as
well as service redesign. We will achieve this through
Robust contract management with both English and Welsh NHS providers
Decommissioning of nationally recognised procedures of limited clinical effectiveness
Robust contract management with the independent sector
Implementing the recommendations falling out of the service reform programme as
highlighted by our recent demand and capacity modelling work
Specifically, the £9.5M commissioning cost reduction / growth avoidance programme targeted at the
external secondary care sector over next three years the will focus on the following work
programmes which are referenced in previous chapters. From our experience, it is typically the
combination of all actions, rather than any individual schemes, which generate success in managing
overall flows to the secondary care sector, these include
Implementation of the planned care programme, including pathway redesign and repatriation
Implementation of the unscheduled care programme, including rollout of the virtual ward
Developing a stronger relationship with WHSSC, including strengthened management of waiting
times
Robust contract management, including using English based opportunities for English based
contracts
Implementing our primary and community care strategy, including rollout of the virtual ward
Implementing our integration plans with Powys County Council for front line service resilience
We are now also a partner commissioner with both EASC for Ambulance services and WHSSC for
specialist tertiary services. We will use these fora to influence the service requirements for our
population
Primary and Community Care The delivery of the £5.8M savings programme over this three year plan will be delivered through the
implementation of our primary and community care programme. This has been set out in the
previous chapters and will focus on a range of both efficiency and transformation approaches in
order to limit spend or reduce cost.
For the next 3 years we will continue to focus on the following
Workforce configuration and managing sickness and absences, using E Rostering as a key
enabler
Better non pay procurement and efficiency in utilisation
Better estate utilisation
Maximisation of efficiency with Prescribed / Dispensed drugs, using prudent healthcare
principles and quality as key drivers
Exploring opportunities for increased income either through service delivery or securing
alternative funding sources i.e. through European Union funding
Service redesign, workforce design and robust contract management to deliver cost
reductions within continuing NHS healthcare

201
Integration
Our Section 33 agreement with Powys County Council along with the associated governance arrangements means we are well placed to roll out a programme of integrated services across Health and Social Care.
During the lifetime of this 3 year plan, we have not anticipated that there will be cash releasing
benefits through our closer working, but recognise that our closer working and where possible
pooled resources will mean a stronger platform of delivery care jointly to the local population. This
will help us secure the limit on growth in volume of patients travelling out of county for care as built
into our planning assumptions above.
Stretch of Savings Plans in 2015/16 The current proposed savings plans will impact on budget levels in 2015/16 as shown in Table 31
below.
Table 31:% cost reduction by budgeted area
10.7. SUMMARY FINANCIAL THREE YEAR PLAN
The three year plan has been set out in high level summary form below in Tables 21 and 23 and
identifies that having taken into account
The likely increase pressures arising from demographic changes and cost of living and
Our plans to reduce costs through service improvement.
Category 15/16
Planned
Savings
£000's
% of Total
spend (%)
Pay & Employee Benefit Expenses 2,222 4.34%
Non Pay 260 1.18%
Primary Care Contractor 0 0.00%
Medicine Management 580 2.15%
Continuing Care and Funded Nursing Care 550 4.49%
Commissioned Services 3,070 2.57%
Total Cost Reduction by Budgeted Area 6,682 2.53%

202
Table 32: Summary 3 year plan
Table 33: Financial Plan – by Category of Spend
Table 34 below provides a summary of the amounts held as a non allocated contingency.
Underlying Position 3.597 0.000 (1.000)
Old Year recurrent impact on 2014/15 (1.315) (1.940) (0.192)
New Year cost pressures 9.959 8.762 6.175
Reduction in Contingencies (1.350)
Assumed WG funding (4.209)
Aniticipated Cost Pressures Before Savings Applied 6.682 6.822 4.983
Savings Plans (6.682) (4.544) (4.227)Net WG Funding based on flat in real terms 0.000 (3.278) (3.331)
Net Position 0.000 1.000 2.575
2015/16
£M
2016/17
£M
2017/18
£M
Financial Plan Summary
Financial Plan Summary - by category of Spend
2015/16
£M
2016/17
£M
2017/18
£M
Pay & Employee Benefit Expenses 50.026 50.576 51.183
Non Pay 23.145 24.119 23.990
Primary Care Contractor 34.504 35.627 36.323
Medicine Management 26.877 27.371 27.866
Continuing Care and Funded Nursing Care 13.764 14.095 14.429
Commissioned Services 123.264 124.170 126.069
Depreciation 2.540 2.540 2.540
Other Income (6.499) (6.525) (6.542)
Resource Limit (267.621) (272.973) (278.433)
Net Position 0.000 1.000 2.575

203
Table 34: Summary of Non Allocated Contingency
10.8. RISKS AND FURTHER ACTIONS
In examining the scale of both upside and downside risks to the financial plan as set out above, a risk
assessment has been completed which gives an indication of the scale of risk being carried by the
organisation in setting out the financial plan.
The risks include a range of delivery issues, partner compliance issues and risks arising from the
relative robustness of the assumptions made. N.B. there is an element of cross over with the
“further actions” as set out above.
Table 35: Financial Risk Assessment
The following provides the basis for the Health Board’s financial risk assessment
SUMMARY of NON ALLOCATED CONTINGENCY
£M
Uncommitted
General reserve 0.50
Committed
Service developments not allocated to budget holders 2.15
RTT 15-16 0.73
Welsh Risk Pool 0.36
NICE 0.21
Other 0.49
TOTAL 4.44
Worst
Case
£M
Most
Likely
£M
Best
Case
£M
2016/17 £M 2017/18 £M
Current Financial Plan 0.000 0.000 0.000 (1.000) (2.575)
Additional resource funding 16.864 16.864
Commissioning - marginal rates to full cost 0.726 0.726 0.726
Additional retrospective arising from Phase 3 cases 0.500 1.000 0.500
Delivery of savings programme 2.076 2.076 2.076
Reduction of contingency 0.500 0.500 0.500
RTT - possible expenditure above plan 0.275 0.275 0.275
WHSSC - difference in planning assumptions 0.350 0.350 0.350
Income risk - WG primary care funding 1.287 1.287 1.287
Assumed funding for Working Together 0.285 0.425 0.425
Potential use of non allocated contingency (0.500)
Rephased SDM delivery
Potential impact of proposed service transfer of Mental Health
Potential Financial Challenge 5.999 0.000 (0.500) 22.503 20.428
2015/16 Worst Case

204
The Health Board has had confirmation of funding from Welsh Government of an additional
£17M above the £8M new funding included in the Allocation letter for 2015/16. This plan
assumes the total of £25M will remain as income to the health board annually over the life of
this plan. If this is not forthcoming the health board will not be able to achieve a break even plan
in future years.
The Health Board assumes in the plan that, in 2015/16, it will contract for any additional activity
over and above 2014/15 contract levels at the prevailing marginal rate for the respective
organisation. This is contrary to the principles included in the Funds Flow proposals which
indicated that any in year variations would be charged / recovered at marginal rates but that the
full year effect in the following year would be at full cost. This assumption has given rise to a risk
of £0.726M
The Health Board is aware of a potential 88 Phase 3 cases which could result in a cost pressures
of £0.500M for the next three financial years
A risk assessment around the delivery of the savings programme has been completed which
suggests a degree of pessimism in delivery of up to £2M. These risks are spread across the
breadth of our operations including commissioning, direct delivery and continuing nhs
healthcare saving
For the purpose of developing a balanced plan, contingency has been reduced by £0.5M to just
£1M and means the organisation will need to secure delivery of plans in order to avoid
overspends against plan
The assessment of expenditure requirement to deliver RTT is between £0.7M to £1.3M. We have
assumed resource requirement of £0.75M on the assumption that increased efficiency will be
delivered by both the direct delivery arm of the organisation and through our commissioned
services to limit the cost of meeting this target
The current WHSSC plan assumes a higher level of planned expenditure that included within this
plan by £0.350M. This is on the assumption that the measures proposed by the Health Board to
WHSSC to limit expenditure will be adopted
The Health Board has assumed a range of income from Welsh Government in respect of the new
£80M funding allocated to the health board along with associated spend. The risk assessment
completed on not receiving additional income as assumed is £1.3M.
The health board has submitted a joint expression of interest to Welsh Government for further
integration. The assumed share for health board is £0.425M over the first 2 years of the plan.
There is a risk to the plan’s assumptions if this is not approved.
We have rephrased our SDM programme in order to contain costs in-year. There is a risk that this
curtailment of the programme will reduce the planned savings assumed in future years although
this has yet to be quantified
The board took the decision in February 2015 to seek to return the direct management of mental
health services to Powys THB. Any associated managerial or service financial risk has yet to be
fully quantified
However there is a potential to mitigate the position by
Possible use of the uncommitted non allocated contingency (£0.500M)
10.9. FUTURE YEAR PLANNING SCENARIOS
In line with WG planning guidance we have prepared two further scenarios based on income
assumptions for years 2 and 3 of the plan.

205
Scenario 2 - Flat cash – 0% increase per annum
In this scenario, we have assumed no financial increase in future years. We have also reversed our
assumption that additional funding will be allocated to primary care and welsh secondary care as
assumed within the base scenario. This analysis demonstrates that within a flat cash scenario the
health board would be unable to live within its means.
Scenario 3 – as per base scenario plus funding for loss of NI rebate
Pay & Employee Benefit Expenses 50.026 50.576 51.183
Non Pay 23.145 24.119 23.990
Primary Care Contractor 34.504 35.627 36.323
Medicine Management 26.877 27.371 27.866
Continuing Care and Funded Nursing Care 13.764 14.095 14.429
Commissioned Services 123.264 124.170 126.069
Depreciation 2.540 2.540 2.540
Other Income (6.499) (6.525) (6.542)
Resource Limit (267.621) (273.696) (279.156)
Net position 0.000 1.723 3.298
Financial Plan Summary - by Category of Spend 2015/16
£M
2016/17
£M
2017/18
£M
Pay & Employee Benefit Expenses 50.026 50.576 51.183
Non Pay 23.145 24.119 23.990
Primary Care Contractor 34.504 34.961 34.981
Medicine Management 26.877 27.371 27.866
Continuing Care and Funded Nursing Care 13.764 14.095 14.429
Commissioned Services 123.264 122.762 123.209
Depreciation 2.540 2.540 2.540
Other Income (6.499) (6.525) (6.542)
Resource Limit (267.621) (267.621) (267.622)
Net position 0.000 (2.278) (4.034)
Financial Plan Summary - by Category of Spend 2015/16
£M
2016/17
£M
2017/18
£M

206
This scenario presents the most optimistic model based on 2% increased funding in years 2 & 3 for
which we have assumed we will fund 2% to primary care services and welsh secondary care services
and assumes we receive funding for the cost of national insurance costs in future years. In this
modelled scenario the health board would be in a position to start addressing the underlying deficit
position which is currently assumed to be covered by Welsh Government.
10.10. CONCLUSION
The Health Board’s three year financial planning process has identified a break even plan for
2015/16 and small surpluses in 2016/17 – 2017/18 based on Welsh Government’s directed financial
planning assumptions.
The financial planning assumptions contained within the 2015/16 financial plan in particular are high
risk of delivery. The organisation will need to demonstrate and deliver increased efficiency and
delivery of service change in order to achieve all that is set out.
This plan demonstrates the organisation’s determination to live within the means allocated to it and
will continue to be a matter of discussion at board level and with Welsh Government in terms of its
achievability throughout 2015/16 and beyond.

207
11. BUILDING CAPABILITY & DELIVERY
11.1. INFORMATION TECHNOLOGY
In 2012 Powys THB and Powys Council agreed a Section 33 agreement that formally bought together
the two organisations’ IT functions and teams into a single management structure with a single
strategic and operational approach. This model enables the THB to implement a local integrated IT
system across health and social care, including primary care, based on a common platform including
incremental implementation of the NWIS strategy. Powys needs both organisations working
together to make significant strategic change in the way that services are delivered and to support
integration of health and social care provision and wider public sector support services. The
approach to integration places Powys in a unique position to inform the development of the Digital
Health and Care Strategy at national level.
Figure 54: Information Technology Joint Strategy
Digital First
Strategy
ICT strategy
for Public
Sector
Wales
Powys LSB
‘One Plan’
PCC service
plans
PtHB
Integrated
Medium
Term Plan
NWIS 3 year
plan
PCC / PtHB Joint ICT
strategy
The Powys Council and Powys THB Joint ICT Strategy draws from a number of sources to ensure that
the direction of travel is aligned both to local business needs and national strategy. This chapter
provides a high level summary of this strategy, with specific reference to the implications for the
THB. The top priority for both organisations in respect of ICT is the joint implementation of the
Community Care Information Service across all elements of health and social care provision in the
County in 2015-18 period. This will provide for a step change in the way that community services
Supporting Powys teaching Health Board and Powys County Council to deliver their
ambitions for integration
Supporting the business in transformation agenda through technology enabled
change both through innovation and integration.
Equipping and maintaining Powys teaching Health Board and Powys County Council
with a flexible, up to date infrastructure

208
are enabled through ICT to integrate care around the citizen. The capital and revenue consequences
to its implementation for the Health Board are fully costed into this plan.
ICT is a key enabler to strategic change as well as a key component of current operational delivery of
services. We will ensure that our outcomes, business needs and business processes drive the shape
and form of our ICT systems and inform national delivery programmes. We will base on programme
on the following underpinning principles:
We will keep our ICT simple and adaptive
We will make it easy for our citizen and staff
customers to access services through ICT.
We will enable staff to self-serve ICT where
appropriate.
We will make our systems safe and secure.
In supporting business needs we will seek
solutions based on a ‘Once for Wales’, ‘Once
for the Region’ or ‘Once for Powys’ approach
to reduce duplication.
Where our population can, and want to, we
will utilise online channels and transactions
utilising e-business as much as possible
We will support and encourage innovation in
self help and self care technologies as these
begin to emerge.
We will use technology that supports widely
geographically dispersed organisations
Our technology will help to drive efficiency
Our technology will be resilient to support
incident response and allow quick disaster
recovery and business continuity planning.
Our ICT solutions will be of appropriate
scale. Where possible, and appropriate, we
will use cloud services, existing solutions and
shared services.
ICT systems will be bi-lingual where possible
and appropriate.
ICT systems will up-hold our environmental
principals, devices will be of low power
consumption where possible and will enable
users to communicate effectively avoiding
unnecessary travel.
Our systems will be available to our users
24/7 (when they need them) in multiple
locations

209
During the life of the joint strategy and evidenced in this IMTP we will:
Commissioning of new systems and services Supporting system development
Implement the Community Care Information
system across Health and Social Care Services
Support the national GP test requesting
(GPTR) project.
Implement PTHB element of the National
desktop Video Conferencing (VC) for health
(Microsoft Lync)
Support delivery of EU funded Mastermind
Project to deliver remote access to clinical
mental health services including on-line
Cognitive Behavioural Therapy
Engage where appropriate with emerging
national projects e.g. National Records
project, National Open Eyes project
Seek to establish a shared infrastructure
between PCC and PTHB and NWIS
Identify and share opportunities e.g. shared
printer rationalisation
Respond to service re-commissioning
opportunities using digital Powys as a test
bed for these opportunities.
Review support services systems under the
Powys One plan Organisation and
partnership development programme with a
view to standardisation and rationalisation of
systems.
Extending the use of existing systems Supporting Primary Care
Pilot a Cross border Project
Complete Phase 1 of the Powys NWIS
programme including Welsh Clinical portal
including MTeD
Master Patient Index (MPI) notably its
integration with the CCIS
Support further use of My health On-line
(MHOL)
Consider the implementation of Case note
tracking capability of the Myrddin system
Maintain the links between the National
program and the EU Carewell project
Continue to rollout WIFI including patient
access to WiFi
Support the National GP system replacement
programme
Continued improvements with Welsh Clinical
Communication gateway (WCCG) as secure
communications between sectors (GP,
Hospitals, Social care via CCIS)
Support further use of the Individual Health
Record (IHR)
Support the development and delivery of
integrated Tele-health and tele-care services.
Support the Single point of access to health
and social services
Implementing the Community Care Information System in Powys will be a powerful enabler to
integration. It will not simply be a new IT system for use by both organisations but potentially the
catalyst for a whole new mode of working, requiring system redesign within team and the need for
an innovative response. To this end, given Powys is proposing move into unchartered territory, the
Health Board with the council, is proposing to put a bid into the Innovation Fund to support this
“first in Wales” development. The value we have estimated to be required to achieve the
introduction (beyond any Welsh Government funding for CCIS) is £0.160M.

210
11.2. CAPITAL & ESTATE
Powys THB will seeking to significantly raise local and national aspirations in respect of the quality of
the patient environment in which the THB provides its services. The THB currently delivers services
through nine community hospital sites and one other facility for children. Powys staff also work
from GP premises and increasingly the THB is seeking joint accommodation solutions with Powys
County Council for both clinical and support services. The Glan Irfon Health and Social Care Centre
shows how the THB is committed to innovation in shared used of assets and this has been
recognised by the Wales Audit Office as best practice in the use of public assets. The THB has also
recently moved its Corporate Hub into Powys Council premises, and is working on plans to move
services for children in a 21st Century school project in Brecon. As the THB moves forward to ensure
that its estate supports the delivery of its service strategy, shared and innovative approaches to the
use of public sector assets and alternative funding models will be the primary route through which
the THB delivers its Estates Strategy.
Forty five per cent of the Powys estates pre-dates 1948, the highest percentage in Wales, with only
25% being post 1995. The risk adjusted backlog maintenance across the estate assessed in 2012-13
was £5.2M of which £3.1M relates to the Bronllys Hospital site. The closure and disposal of the
Builth Wells Hospital site in 2013 reduced the backlog maintenance by £0.13M. The building and
engineering maintenance budget for the estate is approximately £1.3M per annum. Only 68% of the
estate is in condition category B or above, the worst performing estate in Wales.
The THB’s Primary Care Estate is relatively modern, although there have been no new build facilities
in the County since 2004. Many practices remain in direct GP ownership. GP practices are beginning
to articulate the cost of the burden of the estate in securing new GPs to join rural practices, and
alternative models of premises ownership alongside a review of opportunities to bring facilities
together will be undertaken as part of the development of the THB’s is required. The THB has
demonstrated its ambition for modern facilities through the campus approach to health and social
care facilities in Builth Wells, which has been designed along primary care principles.
Estates Strategy The THB has been working to deliver an estates programme based on the Strategic Outline
Programme agreed by the Board in 2011. This SOP now requires significant review and key elements
of work are taking place to inform a strategic 10 year plan for the Estate. The first phase of this has
been completed through the development of a Strategic Outline Programme that covers the capital
requirements for the Estate over a five year period to ensure that the current patient environment is
maintained and that the THB is compliant with its core responsibilities in respect of Health and
Safety. The Capacity and Demand planning exercise completed in November 2014 identifies where
the current estate falls short of the clinical requirements of the services. Core to this is the number,
location and configuration of bed capacity. Other aspects of service delivery such as the quality of
birthing environments, the requirement for dementia friendly environments, and facilities suited to
integrated service delivery for children and changes in the mental health model lead the THB into
the need to engage the public in a comprehensive review of the future of the estates aligned to
discussions around the future service delivery model. The timetable for this, and the place of a
comprehensive estates strategy in this context, is mapped out elsewhere in this Plan. In the
Aligning estate and service strategies to ensure services are delivered in fit for purpose
premises

211
meantime the THB is developing an Estates Strategy that bridges the immediate requirements of
developing the estate to maintain services, whilst the work to complete service strategy is
completed and consulted upon with the public. This bridging strategy will cover three key
components:
Ensuring patient and staff safety through Estates Compliance, and taking opportunities to
consolidate estate utilisation, including taking forward opportunities with other public sector
partners
Maintaining the patient environment through investment in a ‘First Impressions’ programme –
this programme will further add to the compliance of the estate in respect of key environmental
aspects of care such as clear single entry points, dementia friendly environments, signage
including Welsh Language, Disability Discrimination compliance, patient dignity standards.
Taking forward specific programmes in respect of renewal of accommodation in Llandrindod
Hospital, Brecon Campus Scheme (children’s services) and taking forward the plans for the long
term future of the Bronllys site mapped out through the Enquiry by Design process undertaken
by the Prince’s Foundation for the built environment.
Compliance The THB has undertaken a risk based programme of re-assessment of the estate in relation to
estates compliance and summarised this in the SOP approved by the Board and currently under
consideration by Welsh Government.
Re-assessment of asbestos through asbestos survey and implementation of asbestos database
system
Preparation of schematics of water systems in all facilities following legionella incidents, to
inform water risk management plans for each site;
Re-assessment of fire compliance and associated works programme
Fixed wiring assessment completed across all sites during 2014;
Re-Assessment of ventilation and medical gas systems.
A carbon strategy has been developed with the Carbon Trust that aims to reduce the THB’s carbon
emissions and thus reduce the impact of rising energy prices on the overall financial position of the
THB. The capital requirements of these works will be factored into the Estates Strategy. Space
utilisation within sites is also currently being assessed in detail as this is currently reported as 100%,
which is likely to be over-stated.
Service Strategy The service strategy is the key driver for the future of the estate and the work to date on service
models have identified significant changes in the estates requirements of most services as the THB
takes forward its programme. This strategy has now been underpinned by the Capacity and Demand
modelling exercise which has confirmed many of the assumptions previously driving the THB in
developing its Estate. As most of these services are currently provided in integrated facilities in
community hospital settings this has significant implications for all of Powys hospital sites, as the
THB will need to move to rightsizing and modernising facilities. The service requirements also lend
themselves to new approaches to developing estates solutions, with other public sector partners
and through innovative funding routes, and the THB will work with Welsh Government and other to
build on its previous experience in taking this forward.
The Health Board has been successful in securing invest to save funding from the Welsh Government
for two schemes to upgrade street, floodlights and voltage optimisation which will reduce energy
usage, reduce carbon emissions and reduce energy costs.

212
Table 36: Future Estate Requirements
Service Area Future Estate Requirements
Planned Care
Repatriation of out-patient care to Powys
Enhanced use of e-technology in patient pathways
Local access to diagnostics
Increased Day Surgery in Powys
Primary Care
Enhanced role for primary care requiring expansion of estate in GP practices and other high street health services
Co-location of primary care and community services
Four practices requiring new premises, and on-going upgrading required in other premises
Long Term Conditions Growing demand for out-patient based care from demographic changes
Enhanced use of e-technology in patient pathways
Integrated Care for Older People
Integrated health and social care accommodation model, including for people with dementia
Reduced requirement for traditional consultant led in-patient facilities.
Requirement for modern en-suite dementia friendly facilities where provided
Unscheduled Care Continuation of Minor Injury unit provision and extended role for
community pharmacy
Mental Health
Enhanced community service provision
Requirement for crisis house model
Reduced overall requirement for traditional acute mental health beds in Powys
End of Life Palliative care facilities
Children’s Services Co-located health, social care and education facilities, including CAMHS
services
Maternity Services Increased ante-natal care provided locally
Improvements in quality of birthing environments
Medicines Use Automated dispensing
Workforce Fit for purpose office accommodation, co-located with other public
services
Increased use of flexible and e-working
Further work is required to refine the service models in each of these areas and apply the capacity
demand modelling to enable an overall strategic approach to estates development to be taken
forward. However a number of key actions with the estate will need to be taken forward in advance
of the delivery of this strategy as follows:
Acceleration of work to ensure statutory compliance of the estate through delivery of the works
described in the SOP over three years;
Completion of business case for refurbishment and upgrading of Llandrindod Hospital to enable
works to commence in 2015;
Further consolidation and rationalisation of property on Bronllys site including disposal of
Mansion House and demolition of redundant buildings during 2015-16
Improvements to Ystradgynlais Hospital to enable disposal of The Larches, to be compleed in
2016;
Maintenance and up-grading of patient environments over the life of the plan;
Partnership with Powys Council in respect of estate utilisation, specifically in relation to office
accommodation, integrated children’s services in Brecon and joint health and social care
accommodation strategy.

213
Table 37: Property and Asset Investment Summary
Property & Asset Investment
The table below provides an estimate of the capital expenditure required by the THB to meet its obligations over the next five years in respect of:
Maintenance and compliance (not otherwise covered in revenue budgets); Development schemes;
IT strategy;
Equipment and new technologies;
Primary care
Summary
2014-15 2015-16 2016-17 2017-18 2018-19
£m £m £m £m £m
Gross Capital Expenditure (approved and unapproved)
5.729 6.749 7.179 5.042 4.679
less: Receipts (see note below) 0.800 0.240 0.050 0.050 0.050
Net Capital Expenditure 4.929 6.509 7.129 4.992 4.629
2014-15 2015-16 2016-17 2017-18 2018-19
£m £m £m £m £m
Welsh Government Funding
Discretionary 0.954 0.954 0.954 0.954 0.954
Approved Schemes 0.100 2.000 2.500 0.363 0
Unapproved Schemes 3.875 3.555 3.675 3.675 3.675
WG Funding Required 4.929 6.509 7.129 4.992 4.629

214
11.3. RESEARCH & DEVELOPMENT
Research, and the evidence produced from it, shapes the care patients receive. Participation in
research is known to produce better outcomes for patients, regardless of whether they are receiving
treatments under test, or normal care. Research activity in Powys is limited compared to other parts
of Wales, but work continues to increase the access to participants.
The National Institute for Social Care and Health Research (NISCHR) is the funding body of Welsh
Government that leads the research infrastructure across Wales, and provides Powys with a small
allocation to fund research governance. The NISCHR strategy is to support only high quality research,
and activities that lead to, or support, high quality research activity.
The benefits of enhanced research activity include, but are not limited to:
Service users: higher quality services, better and quicker access to evidence based treatments;
better treatment outcomes; and the opportunity to contribute to knowledge generation –
leading to better care for others; increased confidence in, and therefore increased recruitment
into studies in both Primary and Secondary Care.
Health Staff: The willingness and motivation of staff is essential to high quality healthcare, but
research can lead to personal rewards that promote higher motivation and reduced burn out.
Health Board: Research activity can support recruitment and retention of high quality staff;
improve reputation through publications and conference presentations; and financial benefits to
support further research from the Activity Based Funding mechanism.
The R&D Office have been working hard to increase activity within Powys, in particular to
increase involvement in studies eligible for the Clinical Research Portfolio (CRP). Currently we
have 19 commercial and non-commercial studies recruiting in Powys, with 13 CRP eligible
studies, up significantly from previous years. Similarly we have an increasing number of GP
practices making a commitment to be involved in primary care research with 4 PICRIS registered
practices, up from 2 registered in the previous year.
Year Total Studies CRP eligible Approved in year
2013-2014 12 4 4
2014-2015 19 13 10
In order to achieve growth in research activity Powys will:
Ensure Powys is open to as many types of clinical research portfolio trials as possible
Support recruitment of patients to portfolio eligible studies;
Promote local research activity and identify and support interested staff where they present
ideas that could become high quality research studies (i.e. on Pathway to Portfolio), or who wish
to become Principle Investigators or Chief Investigators.
Raise the profile of research at the Powys teaching Health Board, to stimulate thinking and
support for potential research practitioners.
Promoting high quality rigorous research, for patient benefit, and safeguard participants

215
Aims and Objectives of Research and Development within Powys The overriding principle is to ensure that Powys THB and its partners improve the Health and Wealth
of the population of Powys, through developing the evidence base on appropriate areas of practice
and by supporting high quality research initiated elsewhere – ensuring that the needs of rural
patients are also part of the research outcomes.
Key areas for Research and Development in Powys THB:
Develop a Research Network Infrastructure (RNI) in conjunction with relevant interested
academic partners. The RNI should create and facilitate a rich research environment for both
Health and Academic researchers, to assist patient recruitment, and continue to liaise with
regional groups to disseminate research concepts/ideas further. The network would be used as a
platform to stimulate research within Powys THB, and improve research engagement with
clinical staff.
Ongoing refinement of the R&D Committee processes, for review and scrutiny of proposed and
active research activity. This will ratify management approval for studies to run in Powys, and
quality assure the process, to ensure all research is of high quality, and safe, for the residents of
Powys.
Introduce and maintain criteria for a fair, reliant, transparent and strategic system for allocating
funds to researchers who submit projects on ‘pathway to portfolio’.
Identify opportunities for accessing other funds for pump-priming research activity, such as
charitable funds.
Raise the profile of research through submissions to the Executive Team and Board members,
with Board level reporting on Research and Development activity, and of the use of available
funds to support progress.
Support for dissemination and promotion of research will continue through local and national
conferences
Continue strategies to keep Research and Development high on the agenda and promoted
throughout the THB. The continued development of workshops, drop in centres and
conferences, with other promotional material, need to be sustained to provide the opportunities
to inform clinical staff from all backgrounds about local research outcomes and the research
support available.
Continue work to establish links with Academic Institutes, and with Industry partners to develop
technology and innovation within Powys THB. These partnerships can used to develop additional
income and revenue, whilst stimulating novel treatment approaches, and the development of
technology based research.
Continue to work on research promotion in Primary Care. The Primary Care Research Incentive
Scheme (PiCRiS) offers an opportunity for practices to become involved in formal research
activity, with support from the Wales R&D infrastructure. Developing a role to promote and
support uptake of this opportunity is a priority for Powys.
The success of the strategy and will be judged on the quantity and quality of research activity,
partnerships formed and maintained, and innovation into practice from the published evidence base,
and revisions will be made accordingly.

216
11.4. INNOVATION
The approach to Innovation by Powys THB will be based around the things at which the Health Board
excels. The teaching Health Board is primarily a Primary Care and Community Service driven
organisation, and it is this that will drive its approach to innovation, both through its direct service
delivery and the way in which it commissions services to maintain and build local access and local
responses to support people in need.
Continued austerity and tightened budgets across the public sector are driving innovation in the way
that people and communities are sustaining themselves, including for health and social care
purposes. The THB will look to build innovative partnerships with communities for sustainable
health and social care, seeking to facilitate for example the development of co-operative business
models across primary care, the development of Community Interest Companies to manage public
assets and the exploration of the Joint Venture Company model for the delivery of support services
to the public sector.
The use of technology in the community is also developing and Powys is only at the start of its
journey in respect capturing the technology revolution that is underway in our communities.
General trends in the consumer led approach and the sharing economy will inevitably impact on the
way in which healthcare is delivered. The THB will need to take a co-production approach to
understanding how people will use technology in the future to support their own health and to
access health and social care services. With an ageing population the THB needs to develop its
approach to using the ‘internet of things’ and the public increasingly using their own devices to
monitor their health. The THB will be responsive to this, in particular working with the technology
industry and Powys Council through the Digital Powys project to pilot new ways of working with the
industry sector to develop innovative solutions to care problems.
The strategic challenges that the THB faces: a rapidly ageing population, the impact of rurality on
service access, and recruitment challenges are exactly those matters where we will seek to
determine innovative solutions. Specifically we will seek to pursue resources in respect of the
following:
Digital Patient Education and Service Delivery
The Health Board is currently investing in and rolling out a web based Cognitive Behavioural Therapy
service (e-CBT) called Mastermind, matched funded by the European Union. As a sector leader in
this technology in Wales the THB will seek to extend the range of education programmes delivered
via the web, specifically considering diabetes and chronic condition management, where there is a
high level of demand, shortfall in capacity and logistical challenges in providing traditional group
based programmes in rural areas.
Digital Professional Advice
GPs and others often resort to traditional outpatient referrals to obtain a professional opinion on an
individual patient, when other, quicker and more efficient means could be established through
developing the logistical processes, through the use of existing technologies to enable this advice to
be gained.
Local Informal Carer Networks
There are often people in communities willing to support other local residents, but who not wish to
participate in formal volunteering programmes. A web-based solution could be developed to ma
people in need in communities with those willing to provide support.

217
The space for innovation will also be recognised and celebrated through the THB’s existing
structures and systems through:
Recognising innovation through internal and external awards and publications
Widening the engagement of THB in research through the THB’s research facilitator
Raising the profile of the THB in Europe through the THB’s International Office, and its existing
European partner projects, and building on these networks and bringing the learning back to
Wales
Adoption of best practice from elsewhere and early recognition of innovative models of rural
service delivery through the Mid Wales Collaborative and the THB’s own Transformation
Programme
Through the Integration work with Powys Council, and the Powys One Plan
Further developing the Digital Powys project and other specific digital programme.
The concept of innovation will be taken forward through:
Through our primary care, commissioning, and integration delivery processes, seeking
opportunities to roll-out proven innovation across Powys. For example in 2015 we will be rolling
out the Virtual Ward Project across the County that is proven to reduce emergency admissions
Creating the space within the organisation to support and develop new innovative practice,
particularly to resolve key challenges of the organisation: rurality and the ageing population. In
particular innovative approaches to patient education and self care using technology will be a
key area of delivery for the organisation
The Health Board recognises that delivering innovation is reliant on developing an organisational
culture and structure which enables and promotes innovation adoption and diffusion. The enabling
programmes identified in the IMTP seek to build an environment which will deliver the seven key
factors identified in the diagram below.
Figure 55: Seven Success Factors for Change in the NHS
Source: ‘Constructive Comfort’: accelerating change in the NHS’ (2015) The Health Foundation

218
12. STEWARDSHIP AND GOVERNANCE
12.1. THE PLANNING PROCESS
This section addresses the improvements that the Wales Audit Office has recommended in its
Structured Assessment of the THB as part of the 2014-15 audit process. The Board is clear on its
annual planning model and cycle, which includes the planning, engagement, approval, delivery and
assurance model for this Plan. This process is described below:
Figure 56: PTHB Corporate Planning Cycle
This process helps the Board to:-
Implement a clinically led planning environment for service planning, annual planning and
medium term (three year horizon) planning;
Meet requirements of the NHS Wales Planning Framework to integrate our service, workforce
and financial planning into a continuous cycle; and
Build on lessons learned from the 2014/15 Integrated Medium Term Plan process.
Key principles of the process are to ensure:
There is a clinically led planning environment with multi professional input;

219
Patients are at the centre of service design and delivery;
There is whole system planning, ensuring alignment with neighbouring providers plans;
There is a transformation of commissioning and provider functions;
Promotion of integration at a strategic and service level;
There are internal relationships including staff side/trade unions;
There are external relationships with key stakeholders;
There are Community Health Council planning links.
The planning process will be continuously reviewed at the teaching Health Board’s integrated
planning approach matures. In doing so, the process will build on:
GP Cluster and primary care development plans;
Service/locality/directorate plans;
One Powys Plan and partnerships plans;
Workforce, training and education plans;
Quality, safety and performance reports;
Service redesign plans;
Resource and financial plans;
Audit, research and development.
This planning process has informed the underpinning Integrated Planning Process to deliver the
Integrated Medium Term Plan 2015-18 and 2015/16 Annual Plan:-

220
Table 38: Integrated Planning Process
Integrated Planning Process
Process
Annual Plan 6 month progress review completed.
IMTP/Annual Plan Production Project Team established
Timetable and Production Plan approval.
Stakeholder Engagement Plan.
Peer Review of IMTP.
Engagement of key advisory/governance bodies with latest draft.
Refinement of plans.
IMT First draft completed.
IMTP/Annual Plan approval
2015/16 Annual IMTP/Annual Plan Production Project Team disbands.
Start up Q1 of corporate integrated annual planning and performance framework.
Governance
Executive Team
Finance and Performance Committee
Project Team
Executive Team
Finance and Performance Committee
Peer Review
Executive Team
Finance and Performance Committee
Informal Board Session
Board Briefing.
Executive Team
Finance and Performance Committee
Board Approval
Q&D Meetings
WG quarterly reviews.
Outcome
Baseline position confirmed for 2014/15 annual plan (six month review)
IMTP/Annual Plan capacity/resources identified to develop and author plans.
Production Plan/Timetable approved.
Agreed stakeholder engagement plan.
Ongoing delivery against annual plan
Current draft IMTP
Peer review feedback
Ongoing delivery against annual plan.
Develop content for IMTP/Annual Plan
Ongoing delivery against annual plan.
Final edit of IMTP/Annual Plan
Ongoing delivery against annual plan.
PTHB approval of Annual Plan and IMTP.
Ongoing delivery against annual plan.
2015/16 annual plan initiated.
Month End October 14 November 14 December 14 January 15 February 15 March 15
Q3 Q4

221
12.2. THE ENGAGEMENT PROCESS
The Health Board’s approach to stakeholder engagement ensures: a multi-disciplinary clinically led
approach to developing the Integrated Medium Term Plan; appropriate balance between Powys-
wide and locality/directorate groups; empowerment of staff and local decision making.
The table below provides a summary of the Health Board’s key stakeholder groups:-
The planning approach for the development of our Plan has been designed as a three-fold process.
Developing GP Cluster/Locality Plans ‘bottom up’ and in parallel developing plans based on cross
cutting themes and other organisation wide plans. Working with our partners, the One Powys Plan
has driven a number of the strategic priorities being taken forward by the Health Board over the
next three years. The building blocks of our integrated planning are closer integration between
service, quality, performance, IT, estate, workforce and financial plans. Our intention is to further
strengthen our planning and delivery approach together with Powys County Council as part of our
journey towards integration.
The development of the Plan has been an iterative process underpinned by formal and informal
engagement processes and feedback. In the course of the year, a series of public engagement events
have taken place to shape the Council and Health Board’s ongoing priorities and plans. The joint
priorities contained within the One Powys Plan and Health Board’s Plan have been approved by the
Powys Local Service Board.
In addition the planning assumptions have been tested with
The Local Partnership Forum
Powys Teaching Health Board – meetings and development sessions
Montgomeryshire, Brecknockshire and Radnorshire Community Health Councils.
Figure 57: Summary of Key Stakeholders

222
In addition we have participated in the NHS led Peer Review process which was facilitated by the
Good Governance Institute in December 2014 and we have responded to this feedback in our Plan.
The Health Board recognises areas of planning which require further strengthening and which will be
part f the ongoing planning cycle. The Finance and Performance Committee provides Board
assurance on the management of the planning cycle.
Engagement is embedded in Powys at local level and has informed this IMTP at a number of levels,
however the THB recognises that it needs to strengthen its overall corporate arrangements for
continuous engagement and this will be undertaken in 2015 in conjunction with partners in the Local
Service Board. There is reference to considerable engagement throughout this plan
Areas of geographical interest following the pathways of care and around local services,
demonstrated in local cluster plans for example around areas of specific common interest, such
as mental health services and stroke services;
As part of strategic service change such as FutureFit and the Mid-Wales Study and the public
engagement to develop the One Powys Plan
12.3. THE DELIVERY PROCESS
Powys THB is developing its Performance Management Framework alongside the development of the
IMTP to recognise the complexity of the arrangements that the THB needs to have in place to manage
both its internal business and the performance of external stakeholders. Performance Management
can be defined as a set of management processes, often supported by information technology, that
help to improve the management, strategy execution and decision making in organisations.
Performance Management is what organisations do to become more successful. If organisations get
it right, their performance management processes allow them to define and communicate their
strategies, measure, report and monitor progress in order to manage and improve business
performance as well as align people and culture.
A basic performance management model integrates processes for defining strategic objectives,
measuring performance, analysing performance and reporting and reviewing performance and
aligning people and culture. The THB has utilised the IMTP planning process to develop these
processes within the organisation and begin to align these in preparation for the development of the
full performance framework. All of these are focused on performance improvement which is the
central premise of performance management (see Figure below).

223
Figure 58: Performance Management Framework
Integrated Performance Management Organisations can also choose to move beyond the basic model shown in the figure above and
integrate it with other key business processes (see Figure below). In order to gain maximum benefits
from performance management organisations need to ensure they align and integrate processes
including financial planning and budgeting, project and programme management, people
management, performance reporting, risk management as well as business intelligence and
analytics. These are the performance management principles that underpin the integrated nature of
the IMTP.
Defining and Communicating
Strategy
Measuring Performance
Analysing Performance
Reporting and Reviewing
Performance
Aligning People and Culture
Performance ManagementDefine and Communicate Strategy, Measuring Performance, Analysing Performance, Reporting
Performance, Aligning People and Culture
Financial Planning
Project and Programme
Management
People Performance
and Recognition
Performance Reporting,
Dashboards and
Scorecards
Risk Management
Business Intelligence and Analysis

224
Performance Management – the Basics Using the basic strategic performance management model, an organisation starts with defining
strategy, then moves to measuring performance, then use these indicators to analyse performance
in order to extract insights and make better informed decisions which lead to actions and
performance improvements.
Strategic Planning – This step involves creating a business model and strategy. Informed by
strategic analyses organisations identify what strategic objectives they plan to accomplish and
how they plan to accomplish them – strategic objectives have been set out, at the top of this
plan.
Performance Measurement and Monitoring – Here organisations design key performance
indicators to measure and monitor how well they are delivering on their strategic objectives.
Most important is to ensure the metrics are relevant and meaningful and not fall into the trap of
measuring what is easy to measure instead of what will provide the best insights – in this plan
the starting point is the requirements around national performance set out in the outcomes
framework, but the organisation will move beyond these as its framework develops.
Business Intelligence, Analytics and Modelling – using performance data and metrics to analyse
performance. This step is all about creating a solid evidence-base to inform decision making – the
THB has invested in these functions to support the development of this plan and support
performance management.
Reporting & Reviewing Performance – In this step organisations translate the insights gained
from their performance information into management reports and dashboard and put the
review processes in place to act on the data. It is about evidence-based decision making
facilitated by the performance review processes – at the top level performance against corporate
objectives and key performance indicators is undertaken through the THB’s Finance and
Performance Committee.
Aligning People and Culture – In this final step organisations ensure the people, culture and
leadership approaches are focused on performance improvement. It is about creating the soft
elements of a high performance organisation to ensure the performance management processes
actually lead to improved performance – the performance framework is supported by the Chat
to Change Programme and the appraisal process to align people and culture to the Plan.
Integrated Performance Management More advanced performance management approaches integrate with other key management
processes.
Financial Planning, Budgeting – By integrating budgeting and financial planning with corporate
objectives and priorities an organisation ensures that the financial resources are spent on the
things that actually matter the most – finances are integrated into this Plan, and monitored
alongside performance through a single Committee.
Project and Programme Management – The delivery of projects and programmes needs to be
aligned with the corporate objectives and priorities in order to ensure efforts are focused on
what matters the most. The activities (projects and programmes) need to be prioritised based on
strategic needs and therefore have to be aligned with the strategic performance framework of
an organisation. The THB’s Transformation Programme focusses on supporting the strategic
objectives of the organisation and reports directly to the Finance and Performance Committee.
People Performance and Recognition – people are the most valuable and most expensive assets
for the organisation and it is people who deliver the projects and implement strategic plans.
Aligning reward and recognition systems as well as personal performance management
processes to the performance framework creates a tight integration between what matters the

225
most and what people perceive as important – the THB has some mechanisms in place to
support additional rewards to staff through recognition programmes, and this will need to be
aligned to the performance framework.
Risk Management The performance framework has identified the key drivers of future
performance (e.g. staff with the right competencies, corporate reputation or key partnerships)
and it is therefore important to assess and monitor any risks in relation to all performance
drivers in order to achieve alignment between your risk management and what matters the most
for future performance. The approach to risk is outlined below.
Performance Reporting, Dashboards and Scorecards – Relevant performance information is not
only crucial for better decision making and performance improvement, it is also a requirement
for most organisations to demonstrate to external stakeholders and regulators that they have
delivered desired levels of performance and that they have complied with rules and regulations.
Integrated solutions allow organisations to use any of their data to produce and deliver reports,
dashboards and scorecards for their stakeholders – internally or externally. The THB will be
moving to a balanced scorecard approach to monitoring organisational performance in addition
to specific Welsh Government Targets.
Business Intelligence By aligning and integrating the above processes with the performance
framework organisations create an invaluable set of data which they can use, in an integrated
way, to inform decision making.
Significant work has been undertaken during 2014/15 to develop the business intelligence capability
of the Health Board. The establishment of a contracted dataset over the last year has enabled the
Health Board to gain a better understanding of our patient activity which has informed our planning,
commissioning and transformational change agenda. The dataset development and the completion
of the strategic demand and capacity modelling enhanced the Health Board’s knowledge and skills
and a work plan has been developed to further develop detailed analyses, pathway costings and
benchmarking opportunities. During 2015/16 the Health Board will further develop the business
intelligence function to coordinate the Health Board’s intelligence system and analysis that relate to
costed patient activity and/or forms an integral part of patient pathway analysis. This work will
support the Health Board to drive its transformation agenda in relation to commissioning,
developing the Powys clinical services strategy and implementing the service reform programme.
Alongside this, work is progressing with Powys County Council on the JSNA and joint priorities for
business intelligence.
Welsh Language The THB is required to implement its Welsh Language Scheme and the Welsh Language Framework,
“More than Just Words”. Implementation is monitored by Welsh Government and the Welsh
Language Commissioner. The Workforce and OD sub committee of the THB Board has oversight of
Welsh Language and provides assurance to the Board.
Activity is currently well underway to understand the linguistic profile of the workforce by recording
language competency onto ESR. Together with the analysis of the population, and service users this will
inform the language skills strategy which is due to approved by July 2015. The strategy will address any
identified workforce shortfalls through a combination of training, recruitment and partnership
arrangements with other organisations to ensure as complete an implementation of the Active Offer as
possible. The environmental aspects of the active offer will be addressed initially as premises are re-
furbished and will be built into other relevant capital schemes. As the All Wales work to develop patient
record flagging systems advances, the associated operational processes will be developed.
That the Welsh language needs are picked up as part of the needs assessment process.

226
Welsh Language is included as part of the Equality Impact Assessment requirement embedded
into needs assessment processes. Examples of this are the South Wales Programme Equality
Impact Assessment and the One Plan activities.
12.4. FINANCIAL ASSURANCE
The organisation’s financial control framework is set out within the Standing Financial Instructions
(SFIs) of the organisation. SFI’s set out the regulation of financial proceedings and business and are
designed to achieve probity, accuracy, economy, efficiency, effectiveness and sustainability in the
conduct of business. They translate statutory and Assembly Government financial requirements for
the NHS in Wales into day to day operating practice. Together with the adoption of Standing Orders
(SOs), a scheme of decisions reserved to the Board and a scheme of delegations to officers and
others, they provide the regulatory framework for the business conduct of the THB.
In addition to Standing Orders and Standing Financial Instructions there are a series of Financial
Control Procedures that cover core financial systems of the Health Board including a budgetary
control policy that sets out the accountability framework for budgets and processes that are to be
followed when budget variances arise.
There are many other control systems within the Health Board that contribute to good financial
control. The Audit Committee provides assurance to the board that the organisation’s systems of
internal control are effective. In seeking assurance as to their effectiveness the Audit Committee
approve a programme of internal audit of systems and processes to seek assurance and to drive
improvement. Internal Audit is provided by NWSSP Audit and Assurance. Further assurance is also
gained from external audit work provided by Wales Audit Office in relation to their role in providing
an opinion on the organisation’s statutory accounts and their work on structured assessment and
performance reviews.
The development of the annual and three year financial plan is an integrated process overseen by
the Finance and Performance Committee, including their attendance at the planning development
meetings. The IMTP is signed by the Board annually and monitored on a monthly basis by either the
Finance and Performance Committee or the Board (dependent upon the reporting month). Financial
reporting for the organisation follows a firm monthly cycle. The financial position is reported to WG
on working day five of the month end with a full and a comprehensive financial report developed for
the organisation and Welsh Government.
Delivery of the financial plan for the year is monitored through Finance Director’s monthly meeting
with lead Directors and also through the supporting finance staff with delegated budget holders on a
monthly basis. These sessions provide both challenge and support to budget holders in the delivery
of their plan and also follow the escalation process as set out in the budgetary control procedure
where required. During early 2015/6 we will review our budgetary control procedure to assure the
Finance and Performance Committee and ourselves that we are taking a proportionate risk based
approach to financial review and monitoring, tailored to the areas of most risk of delivery.
12.5. THE ASSURANCE PROCESS AND CORPORATE GOVERNANCE
The governance arrangements within NHS Wales and the THB continue to be developed to ensure
that there is clarity on objectives, risks and performance management arrangements from the Welsh
Government through to the THB and then to all operational management areas.

227
Our Board is accountable for governance and internal control in the organisation, with the Chief Executive (as Accountable Officer) responsible for maintaining appropriate governance structures and procedures. This responsibility includes a sound system of internal control that supports the achievement of the organisation's policies, aims and objectives, whilst also safeguarding the public funds and this organisation's assets (in accordance with the responsibilities assigned by the Accounting Officer of NHS Wales). The THB has continued to develop a system of governance and assurance. The Board sits at the top of the organisation’s governance and assurance systems and sets strategic objectives, monitors progress, agrees actions to achieve these objectives and ensures appropriate controls are in place and are working effectively throughout the organisation. To do this the Board also takes assurance from its Committees and also its assessments against the Standards for Health Services in Wales and other professional standards and regulatory frameworks. The THB’s governance and assurance arrangements have been established in accordance with Standing Orders and Standing Financial Instructions. The THB’s agreed objectives also seek to ensure national and locally determined priorities and professional standards are achieved throughout the conduct of our business. Reporting and monitoring against these objectives, and the risks associated with their delivery and achievement, are received by the THB and its Committees. This Plan sets the foundation of the Board’s Annual Plan objectives, by which the Board monitors performance. During 2014, the Board undertook a review of its governance arrangements and established a revised assurance structure to address gaps in assurance identified. The Wales Audit Office Annual Report 2014 concluded that the necessary changes to the Health Board’s governance arrangements are not yet embedded or fully effective, outlining specifically:-
The Health Board recognises the need to clarify and strengthen the devolved accountability although it is still in the process of making these changes
Changes made to improve Board assurance and internal controls are appropriate although not yet fully effective and there have been some weaknesses in the governance arrangements identified as part of the annual review.
The THB acknowledges that there are improvements to be made in its governance arrangements, as outlined by WAO, and will establish an action plan to ensure improvements are made in the coming year. Some of these improvements are referred to below. The Board has recently established a Finance and Performance Committee. This Committee will
oversee the development of the Board’s Performance Management Framework and, in doing so, will
oversee the development of a Risk Assurance Framework (RAF). The RAF will be designed to ensure
the Board is informed on principle risks threatening the delivery of objectives associated with the
strategic goals of the Health Board.
The Risk Assurance Framework will align principle risks, key controls and assurances alongside each
objective. Gaps are identified where key controls and assurances are considered insufficient to
mitigate the risk of non-delivery of objectives. The RAF will enable the Board and Committees to
identify where additional assurances might be required and to direct additional measures to
mitigate unacceptable risk.
The Finance and Performance Committee will take a key role in reviewing the financial risks to the
Health Board, both in terms of the year to date and forecast position; and seeking assurance on the
corrective actions necessary and being undertaken to ensure delivery of the financial plan.

228
The Board will continue to maintain overall oversight of performance against delivery of the plan on
a routine basis.
The Board’s Quality and Safety Committee continues to oversee the development of a Quality
Assurance Framework (QAF). The QAF provides detailed mapping of sources from which assurance
can be gained in order to monitor the quality of services provided to the population of Powys. This
information is intended to assure the Board of the standards and quality of care for both provided
and commissioned services. The Quality and Safety Committee also continues to oversee
performance against a set of quality performance indicators for both provided and commissioned
services.
A Board Assurance Map (BAM) has been established which determines the Board’s assurance
requirements in respect of the following key areas of Board business:
Legal and legislation
Governance arrangements
Change and transformation
Quality and safety
Health and safety
Procurement
Partnership working
Finance and Performance.
The BAM identifies the Board’s assurance requirements under these areas in order that assurance
sources can be identified. This allows the Board to determine its gaps in assurance and the actions
required to address these. The BAM will be seen as a dynamic document and reported to the Board
throughout the year. Reporting of the BAM will align assurance reporting of the Board’s Committees
to demonstrate any gaps or duplication amongst the work of the Board’s assurance structure.
The Board’s Committees continue to develop and work plans for each established. These work plans
bring together: key requirements of the Committee as set out within Terms of Reference; areas of
risk and concern; and priorities identified by the Board.
The Board’s Committee have also ensured audit reports and audit recommendations are a key factor
of work plans, and where possible audit recommendations will be embedded into risk registers. This
will ensure that audit recommendations are considered within the risk profile of the organisation
and the impact of non-delivery is understood. These will be considered in developing and delivering
this Plan.
Embedding effective risk management within the organisation remains a key priority, through
delivery of the Board’s Risk Management Strategy. There is no separation of clinical and non-clinical
risk management, rather there is a commitment to identify and manage risk across the broad
spectrum of governance to ensure that organisational objectives are delivered successfully for the
benefit of patients and the population of Powys.
The Board is currently undertaking a review of its Corporate Risk Register and in doing so has
identified 8 key principle risks to the organisation:
Failure to secure and maintain the quality of patient services;
Failure to secure financial sustainability;
Failure to deliver required organisational performance;
Failure to effectively commission;

229
Failure to sustain an engaged and effective workforce;
Failure to deliver the required transformation of services;
Failure to deliver effective strategic partnerships;
Failure to effectively govern the organisation.
Each principle risk is underpinned by a number of detailed risks, some of which may impact of
achievement of the Board’s strategic objectives. These include:-
Failure to deliver optimal outcomes for patients
Failure to prevent avoidable harm to patients
Failure to ensure an appropriately designed and compliant estate
Failure to ensure an appropriate robust IT system
Failure to deliver the Health Boards financial and performance targets
Failure to secure high quality clinical services for the HB’s responsible population
Failure to become an effective commissioning organisation
Failure to be assured of the quality of services commissioned
Failure to deliver the Board’s Organisational Development strategy
Failure to secure an effective, appropriately skilled, workforce
Failure to maximise opportunities for integration with Powys County Council
Failure to engage in service change plans of provider organisations
Failure to fully engage in the Mid Wales Collaborative
Failure to implement communications strategy
Failure to ensure business continuity
Failure to effectively manage patient, staff and corporate records
The Board’s objectives, set by the Integrated Medium Term Plan, will be risk assessed against each
of these principle risks, understanding and cause, effect and impact, and monitored by the Board to
ensure mitigating actions are in place.
The Board will receive training from the Good Governance Institute in March 2015 in relation to risk
management, including risk appetite and tolerance. This will allow the Board to begin to articulate
its tolerance and appetite for risk in agreeing its strategic objectives and maintaining an oversight of
performance.

230