public health and psychoactive drugs · the paradox of prohibition s market regulation ......
TRANSCRIPT


Public Health Approach to Psychoactive Substances
Using cannabis as an example
February 3 2015
Dr. Brian Emerson
Chair, Health Officers Council of BC Psychoactive Substances Committee;
Medical Consultant, BC Ministry of Health
250-952-1701

Disclaimer – This presentation and my comments DO NOT represent the position of the Government of BC.
3
Disclosure - None of the information in this presentation has been
supported by commercial sources.

Participants in this session will be able to:
1. Describe a public health approach to psychoactive substances.
2. Identify the main determinants of benefits and harms of psychoactive substances.
3. Discuss how a public health approach could be applied to the management of cannabis.
4
Learning Objectives

Acknowledgements/References
Health Officers Council of BC Canadian Public Health Association

CPHA Alcohol and Tobacco Papers

1. Key Concepts 2. Public Health Approach
I. Directional Elements II. Strategies 3. Application to Cannabis 4. Concluding Remarks 5. Discussion
7
Outline

Control approaches developed in the early 20th century.
Based on racism, fear, political and economic agendas.
Limited scientific and medical knowledge or considerations.
Bewley-Taylor, D., Blickman, T., Jelsma, M., The Rise and Decline of Cannabis Prohibition. Transnational Institute, Amsterdam, Global Drug Policy Observatory, Swansea, March 2014, http://www.tni.org/rise-and-decline?context=595
8
Key Concepts
History Prohibition

9
Key Concepts – Morbidity & Mortality Canada 2002 Rehm, J et al, “The Costs of Substance Abuse in Canada”, 2002. Canadian Centre on Substance Abuse.
% of Total Acute
Care Days
Deaths % of Total
Tobacco 10.8 16.6
Alcohol 7.2 4.1
Illegal Drugs 1.5 0.7
Total (excludes
pharmaceuticals)
19.5 21.4
10
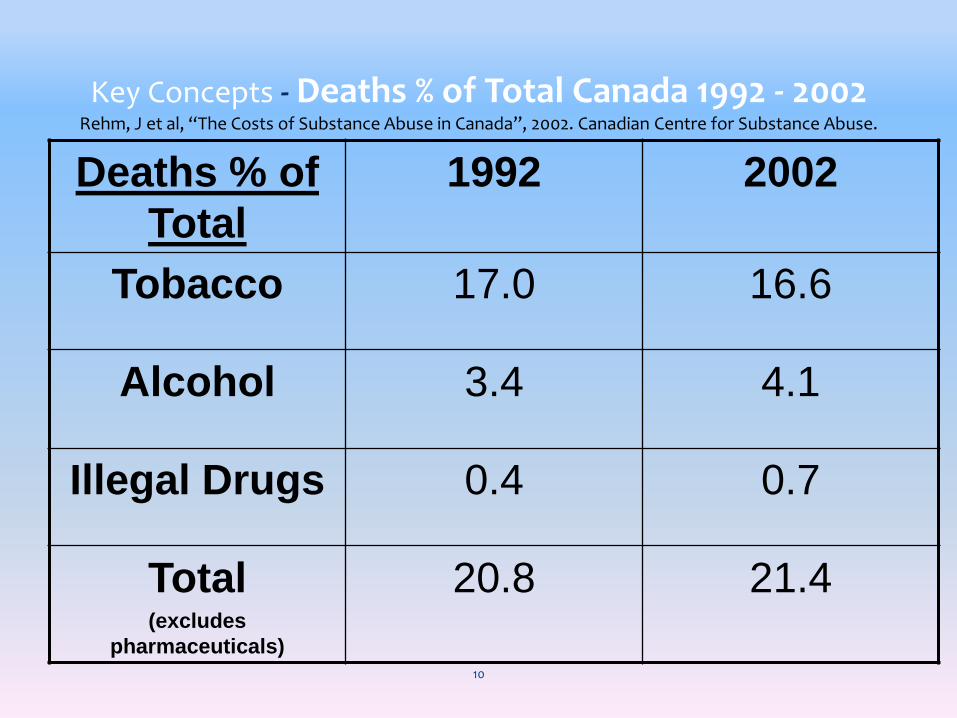
Key Concepts - Deaths % of Total Canada 1992 - 2002 Rehm, J et al, “The Costs of Substance Abuse in Canada”, 2002. Canadian Centre for Substance Abuse.
Deaths % of
Total
1992 2002
Tobacco 17.0 16.6
Alcohol 3.4 4.1
Illegal Drugs 0.4 0.7
Total (excludes
pharmaceuticals)
20.8 21.4

Key Concepts - Acute Care Days % Total Trends Rehm, J et al, “The Costs of Substance Abuse in Canada”, 2002. Canadian Centre for
Substance Abuse
11
% of Total
Acute Care
Days
1992 2002
Tobacco 7.3 10.8
Alcohol 2.8 7.2
Illegal
Drugs
0.1
1.5
Total (excludes
pharmaceuticals)
10.2 19.5

Key Concepts - Costs by substance (Billions $) Rehm, J et al, “The Costs of Substance Abuse in Canada”, 2002. Canadian Centre for
Substance Abuse
$ Billions % Per Capita
Tobacco 17.0 43 541
Alcohol 14.6 37 463
Illegal Drugs 8.2 21 262
Total (excludes
pharmaceuticals)
39.8 100 1,267
12

13
Key Concepts
Spectrum of Psychoactive Substance Use (Adapted From: BC Ministry of Health Services. ”Every Door is the Right Door: a British Columbia planning
framework to address problematic substance use and addiction” 2004)

Drug “use” is an indicator; “use” is not necessarily the problem, reducing drug use is not necessarily the objective.
Focus on “use” over-emphasizes personal responsibility and choice; tends to target, blame and stigmatize people who use drugs.
Focus on “use” distracts from systemic issues, risk conditions and risk behaviours that determine benefits and harms. 14
Key Concepts - “Use”

Approach
Definition
Prohibition and Criminalization
Criminal law to denounce, deter, punish, and rehabilitate - to reduce harms.
State Control Government monopolies or partial monopolies.
Commercialization Free market - managing substances as commodities.
Prescription Health professional gatekeepers
Social/Sacred Control Social norms –wine with food, no alcohol with breakfast Social rituals – Japanese tea ceremony, coca leaf ritual Sacred rituals – tobacco, peyote, ayahuasca
Self-Control Self imposed controls on use 15
Key Concepts – Control Approaches

Prohibit possession, production, import/export and trafficking through criminal law.
Criminal law purposes - reduce harms
Strategies - denounce, deter, punish, and rehabilitate.
Tactics - arrests, criminal trials, fines, imprisonment, probation orders and criminal records.
Limited to ineffective deterrent to substance use.
Results in many harms. 16
Key Concepts
Prohibition and Criminalization

Key Concepts
Harms of Prohibition/Criminalization Organized crime, illegal markets,
corruption, gangs ,crime, violence.
Accelerated spread HIV, hepatitis.
Enforcement drives users away from prevention and care services.
Increase potency, overdoses deaths.
Expending personal resources on substances, to detriment of basic needs.
Forced involvement in criminal activities.
17

Key Concepts
Harms of Prohibition/Criminalization Stigmatization and discrimination.
Crowding and slowing criminal justice.
Marginalization of people with difficult health, psychological, social problems.
Damaged houses, community disruption.
Substance displacement, users move to more hazardous products.
Restricted research on therapeutic and beneficial use. 18

Population levels of use and substance risk determine population levels harm.
E. g. Widespread use but limited risk of harm can result in as much adverse consequences as limited prevalence of use but higher risk of harm.
Benefits need to be considered, which complicates this assessment.
From a public health perspective ideal is low harm/benefit ratio, without unintended effects of control measures.
19
Key Concepts
Population Health Impact
20
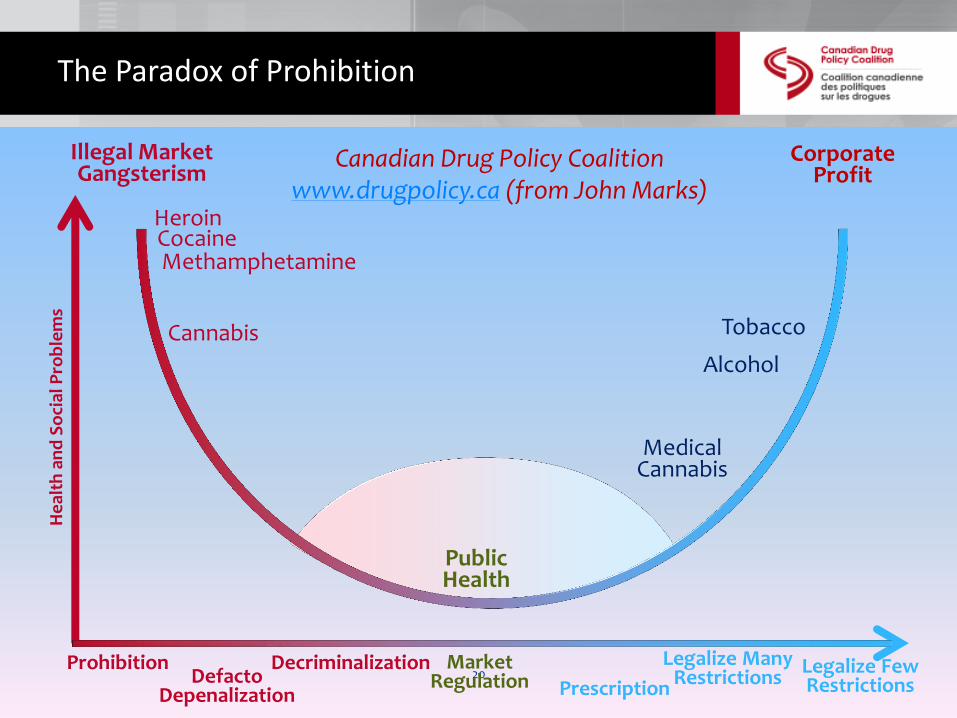
The Paradox of Prohibition H
eal
th a
nd
So
cial
Pro
ble
ms
Market Regulation
Public Health
Illegal Market Gangsterism
Corporate Profit
Heroin Cocaine
Prohibition Defacto
Depenalization
Decriminalization Prescription
Legalize Many Restrictions
Legalize Few Restrictions
Cannabis
Methamphetamine
Medical Cannabis
Tobacco
Alcohol
Canadian Drug Policy Coalition www.drugpolicy.ca (from John Marks)
21
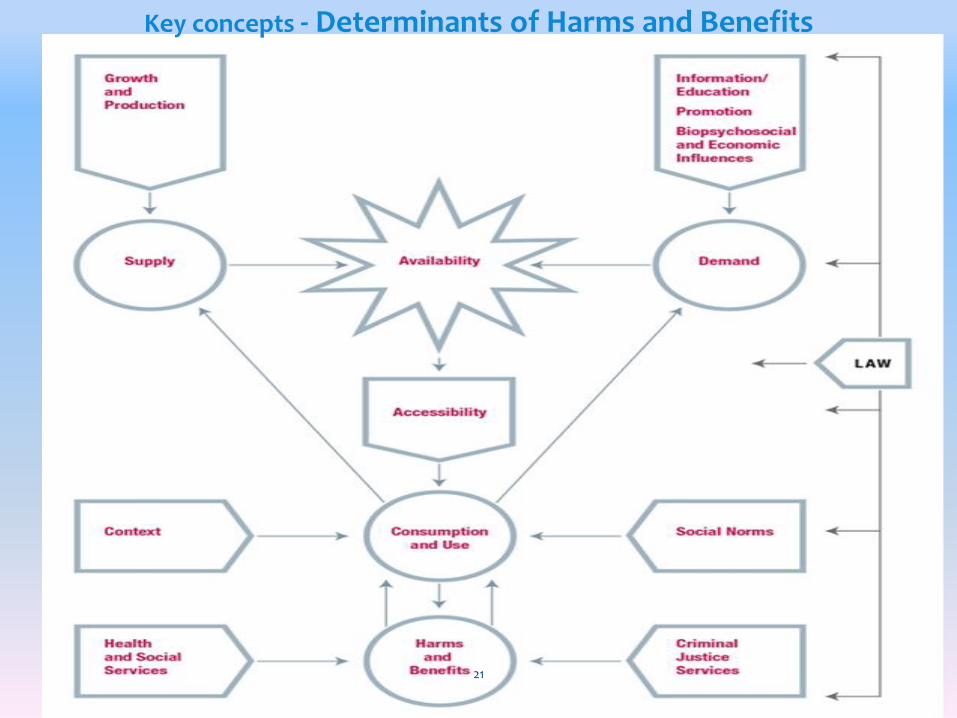
Key concepts - Determinants of Harms and Benefits

Availability – The probability of being able to encounter or be exposed to the option of obtaining a substance. For example, availability may be determined by numbers of outlets, restrictions on density of retail outlets, or hours of operation.
Accessibility – The ease with which one may obtain a substance. It is a function of availability and other control measures that limit or facilitate purchase such as price, age requirements, and social networks that may be a source.
22
Concepts Definitions

Advertising
Branding/naming
Sponsorship
Gifting
Product association with films
Leading personality recruitment
Associating use with attractive activities such as sporting, socialization, sex, and vacations;
Pricing reductions (i.e., loss leaders);
Labelling suggestive of pleasure, enhanced performance, over stated benefits;
Associations with pleasant activities;
Creating similar products for children (i.e., chocolate cigarettes) or youth-attractive products (e.g., alco pops, flavoured cigarettes, and cigars).
23
Key concepts - Product Promotion

I. Directional Elements Assumptions, Principles, Vision, Goal,
Objectives (by sector – Health, Social Welfare, Education, Safety, Public Order and Justice, Agriculture, Environment, Business and Finance)
II. Strategies Health Promotion Health Protection Prevention Harm-reduction Health Assessment and Surveillance Emergency Preparedness and Response Research Services for people who are at risk or develop
problems with substances
24
Public Health Approach

Consumption for both medical and non-medical purposes has long history and will continue in the future.
New substances will continue to be produced, and the consequences will need to be effectively managed.
Substantial, positive differences can be made with evidenced-based, coordinated, multi-sectoral, public health oriented strategies.
25
Directional Elements - Explicit Assumptions

Promotion and protection of life, health, security, human rights and freedoms.
Empowerment through evidence based information, education, and support for self determination.
Informed consent about harms and benefits.
26
Directional Elements - Explicit Principles

Emphasizes social justice, equity, respect for human rights, efficiency, and sustainability.
Includes perspectives of people who use and are affected by substances.
Respect for spiritual, traditional and therapeutic use.
Attentive to benefits and harms, as well unintended effects.
27
Directional Elements – Explicit Principles (continued)

Public health approach addresses
determinants of health (i.e. physical, biological, psychological, and social e.g. income distribution, education, housing)
determinants of social and health inequities (i.e. power imbalance, racism, classism, ageism, sexism).
Recognizes that problematic use is often symptomatic of underlying biological, psychological, social or health issues.
28
Directional Elements – Explicit Principles (continued)

Protection against false claims, unsafe products.
Respect for autonomy in making decisions about ones body.
Individuals held responsible, accountable for actions that harm others.
Criminal sanctions limited to harm to others (i.e. crimes of force, bodily harm, fraud and public safety).
29
Directional Elements – Explicit Principles (continued)

Evidence informed, incremental implementation and rigorous evaluation; not ideology.
Regulation intensity based on harm potential.
Variations that pose the least risk should be most accessible. E.g. incentives for oral or vapourized products vs smoked, incentives for low vs high concentration.
Easy and readily available access to help for people who do experience problems. 30
Directional Elements – Explicit Principles (continued)

Pragmatism
Compassion for people directly or indirectly adversely affected.
Non-stigmatization and non-discrimination of consumers and providers.
31
Directional Elements – Explicit Principles (continued)

Rational, respectful discussion, consensus. Inclusivity. Involve and gain support of affected people
and communities. Access to information and transparency. Where evidence is lacking, encouraging pilot
projects and evaluation. Where policies and strategies made without
evidence, make explicit and evaluate. Be prepared and willing to change course
based on evaluation.
32
Directional Elements – Process Principles

Vision – Aspirational description of future to guide decision making.
See CPHA paper for “A Vision for 2025”.
Goal - Maximize the health and wellness of population, minimize harms, and ensure that the harms associated with interventions are minimized and not disproportionate to the harms of the substances themselves.
33
Directional Elements

Benefits Harms
Physical Pain relief
Assistance with sleep
Decreased risk of
cardiovascular disease
Increased endurance,
stimulation or diminution of
appetite
Toxicity
Injury or death
Infectious and chronic diseases
Neurological damage and fetal alcohol
spectrum disorder
Aggravation of existing physical
disorders
Psychological Relaxation
Relief of stress and anxiety
Increase alertness
Assistance in coping with daily
life
Mood alteration
Pleasure
Performance or creativity
enhancement
Depression
Impaired thinking
Psychosis
Maladaptive coping behaviours
Dependency
Addiction
Aggravation of existing mental
disorders
Social Facilitation of social interaction
Religious, spiritual or
ceremonial use
Family violence
Financial hardship
Crime
Driving crashes
Stigmatization and discrimination
Economic Business and industrial activity
Wealth generation
Employment creation
Agricultural development
Tax revenue generation
Lost productivity
Costs of health, social, and criminal
justice services
Property damage
Fueling an illegal economy that avoids
taxation and distorts/impairs legal
markets
34

1. Health promotion
2. Health protection
3. Prevention
4. Harm-reduction
5. Emergency preparedness and response
6. Population health assessment
7. Disease, injury, and disability surveillance
8. Services to help people at risk or who develop problems.
35
Public Health Strategies

Over arching
Universal initiatives which apply to the entire population i.e. population wide social marketing campaigns.
Targeted initiatives such as providing harm reduction supplies i.e. needles, crack pipes, supervised consumption services.
36
Strategies

37

Health promotion as the process of enabling people to increase control over and improve their health,
Ottawa Charter for Health Promotion outlines prerequisites for health as peace, shelter, education, food, income, a stable eco-system, sustainable resources, social justice and equity. A key theme is “coordinated action by all concerned”.
defines the five components as: Building healthy public policy; Creating supportive environments for health; Strengthening community action; Developing personal skills; and Reorienting health services.
38
Strategies

Prevention measures include low barrier blood testing and immunization programs, screening and brief intervention, evidence based education, and social marketing
Harm reduction reduces adverse consequences without necessarily reducing drug use i.e. needle, crack pipe and other harm reduction supply distribution programs, take home naloxone programs to prevent overdose fatalities, substitution maintenance therapies, supervised consumption services, and street drug testing programs
39
Strategies

Health protection include policies and legal tools that control the supply chain to minimize the potential for harms from substances to individuals and those secondarily affected, and includes rules about governance of the system, production, manufacture, wholesale, distribution, retail, product promotion, purchase and consumption.
40
Strategies

Emergency preparedness and response
Population health assessment
Disease, injury, and disability surveillance
Services to help people at risk or who develop problems
41
Strategies

Application to Cannabis
42

Crude Estimates of Annual Cannabis-attributable Morbidity and Mortality (Fischer, B. et al, Journal of PH, 2015)
43
Mortality
MVA
Lung Cancer
Total
Low
89
130
219
High
267
280
547
MVA Injury 6,825 20,475
Incident
Schizophrenia
106 186
Cannabis Substance
Use Disorders
Treatment
Population
(Total = 380,000)
76,000 95,000

A for profit, free market approach can produce significant health and social harms.
Companies that sell products, which have potential for harm, prioritize profits over public health.
Production, distribution, sales, marketing, and consumption need to be carefully controlled.
Public health strategies have had some success, more is needed.
44
Application to Cannabis Lessons learned from Alcohol and Tobacco

International – Framework Convention Tobacco Control, WHO Global Alcohol Strategy, Proposed Framework Convention Cannabis Control (Room R, et al Cannabis policy: Moving beyond stalemate. http://www.beckleyfoundation.org/cannabis-policy-moving-beyond-stalemate/)
UN General Assembly Special Session 2016 on “World Drug Problem (http://www.unodc.org/ungass2016/)
Other Countries - Shift from strong state control alcohol to private system increases harms. Plain packaging tobacco in Australia and proposed for Britain.
Federal – Tobacco: national advertising limits, warning labels, national strategy, product constituents i.e. flavour restrictions, support research, coordinate with provinces. - Alcohol: Control with provinces, product
promotion controls 45
Learning from alcohol or tobacco

Other Countries
Uruguay, Mexico, Jamaica
Netherlands – coffee shops
Portugal – decriminalized all drugs, health based approach
Spain - collective cultivation
USA
Legalization - Colorado, Washington State, Washington DC, Alaska, Oregon
Medical marijuana states (21)
46
Cannabis Policy Context

Cannabis Legalization in the USA (Courtesy of Mark Haden) Washington
Oregon
Colorado Washington DC
Alaska
California
Nevada
Minnesota
Maine New Hampshire Vermont
New York
Massachusetts
Connecticut
Rhode Island
Maryland
Montana
Arizona New Mexico
Illinois
Michigan
Nebraska Ohio
North Carolina
Mississippi

Federal - Prohibition
– Medical Cannabis
Marihuana for Medical Purposes Regulation
Patients obtain authorization from physician, submit authorization to a licensed commercial producer
Categories of conditions or symptoms eliminated
Supply and distribution system of licensed producers
Patients no longer permitted to grow their own cannabis or designate others to grow it– injunction set aside – trial 2015. 48
Cannabis Policy Context Canada

Government regulation of consumer products to reduce risk and prevent harm is well established:
Food and water protection legislation
Consumer product legislation i.e. paint, cleaning products, toys etc.
Pharmaceutical and medical device legislation
Motor vehicle safety legislation 49
Health Protection e.g. Regulation

Health protection include policies and legal tools that control the supply chain to minimize the potential for harms from substances to individuals and those secondarily affected, and includes rules about governance of the system, production, manufacture, wholesale, distribution, retail, product promotion, purchase and consumption.
50
Strategies

51
Determinants of Harms and Benefits

52
June 9, 2014 http://www.openmedicine.ca/article/view/630/552

53
CAMH Policy Framework Link

Availability control – e.g. Governance - government monopoly; production controls; licensed retailers/lounges; regulation of density, locations, hours of operation; no co-sale with alcohol or tobacco.
Accessibility control - e.g. Retailers check age if appearance < 25 yrs; minimum pricing and taxation to influence price; required retailer/server training.
54
Public Health Oriented Regulation for Cannabis

Supply control – e.g. allow some home production; strictly regulate commercial production; product standards; quotas; encourage small-scale production; track production and sales; bulk product only i.e. not pre-made joints; processing controls.
Demand reduction - e.g. require provision of factual information on harms and benefits; labelling constituents and warnings; bans on product promotion such as advertising, branding, and sponsorship.
55
Public Health Oriented Regulations for Cannabis

Purchase, consumption, use controls - e.g. legal age of purchase, purchase quantity limits, public use limitations, impaired driving laws.
Revenue – Government monopoly mandate explicitly guided by public health vision, principles, goals and objectives; revenue generation explicitly not a primary function; revenue generated funds regulatory, public health related and other health and social initiatives.
56
Public Health Oriented Regulations for Cannabis
Public support for cannabis “legalization” is growing, in part because of increasing recognition of the lack of effectiveness and the harms of cannabis prohibition.
There is a pressing need for proactive action based on a public health approach.
Otherwise, a commercial exploitation model may result, such that public health and social problems similar to those associated with alcohol and tobacco may be repeated.
57
Closing Remarks

Provides opportunities to move away from prohibition/criminalization of opioids, stimulants, psychedelics to reduce harms of these substances and of the associated policies, and creates opportunities to realize benefits:
Psychedelics - MDMA and cannabis studies on PTSD, substance disorders
Stimulants maintenance therapy – ADHD
Opioids – public health approach to pain, less addiction and mortality
58
Implications of public health approach for managing other illegal drugs

Values and principles
Economics
Infrastructure
Canadian laws and international conventions
Programs and projects
Leadership
Evaluation
Research
Barriers and Facilitators to a Public Health Shift – CPHA Paper

Responses Available under Prohibition (Courtesy City of Vancouver)
Enforcement
Education and
awareness
Socially stigmatized
through criminalization
Treatment and
Harm Reduction

Responses Available under Public Health Approach (Courtesy City of Vancouver)
Age
Degree of intoxification
Volume rationing
Limited places to use
Required training prior to use
Registration of purchasers
Licensing of users
Tracking of consumption habits
Drug consumed on location of sale
Prescription only
Maximum volumes for purchase and possession
Training of supplier
Monitoring of use with driving
Illegal dealers pursued by enforcement
Retail outlets licensed and limited
Appearance of retail outlets
Pharmacy specialist required
Price and profit controls
Taxed
Licensing, location and opening hours of consumption facilities
Social controls
Prevention programs
Treatment available
Plain packaging
Concentration of product is restricted and labeled
Warning labels
No advertising or event sponsorships
Clean needles and health information provided with purchase Required membership in users group
Stop purchase orders
Previously negotiated limits

Acknowledgements/References Health Officers Council of BC “Public Health Perspectives for
Regulating Psychoactive Substances: What we can do about alcohol, tobacco, and other drugs” http://healthofficerscouncil.net/positions-and-advocacy/regulation-of-psychoactive-substances/ or http://www.phabc.org/modules.php?name=Contentpub&pa=viewdoc&cid=11
Canadian Public Health Association “A New Approach to Managing Psychoactive Substances in Canada” http://www.cpha.ca/en/default.aspx
Haden, Mark; Emerson, Brian. “A vision for cannabis regulation:
a public health approach based on lessons learned from the regulation of alcohol and tobacco” http://www.openmedicine.ca/article/view/630/552
Centre for Mental Health and Addiction “Cannabis Policy
Framework” http://www.camh.ca/en/hospital/about_camh/newsroom/news_releases_media_advisories_and_backgrounders/current_year/Pages/CAMH-releases-new-Cannabis-Policy-Framework.aspx
Rolles, S. How to Regulate Cannabis: A Practical Guide http://www.tdpf.org.uk/resources/publications/how-regulate-cannabis-practical-guide
Canadian Centre on Substance Abuse: Marijuana Policy Briefs http://www.ccsa.ca/Eng/topics/Marijuana/Pages/default.aspx
62

Thank you ! Questions and Comments
63
1. The negative public health and social impacts of both use of and policies related to alcohol, tobacco, prescription and illegal substances are substantial, and largely preventable.
2. Use the evidence from the alcohol and tobacco free market experiences and associated harms when developing a public health oriented regulation of all substances.
3. The prohibition of a number of substances is ineffective and causing much harm. As a result, many jurisdictions are moving away from criminalization to more public health oriented approaches.
64
Main Messages from HOC Paper

4. A public health oriented approach for all psychoactive substances is needed, together with appropriate health care, social, and criminal justice services
5. The effects of any changes in substance legality and regulation will need to be carefully monitored and evaluated. Local, provincial, and federal government innovation needs to be supported and encouraged.
6. A comprehensive public health approach is needed. All steps in the supply and demand chain should be under careful societal control.
65
Main Messages from HOC Paper