pulmonary fibrosis associated with low-dose adjuvant methyl-ccnu
TRANSCRIPT

Medical and Pediatric Oncology 18:25&260 (1990)
Pulmonary Fibrosis Associated With Low-Dose Adjuvant Methyl-CCN U
Margaret Block, MD, FACP, Robert M. Lachowiez, PhD, Carlos Rios, MD, and Simon Hirschl, MD
Pulmonary fibrosis is a serious side effect only been reported once previously. The of nitrosourea therapy, occurring most fre- case of methyl-CCNU-induced pulmonaryfi- quently in patients treated with BCNU. Pul- brosis reported here occurred at a much monary fibrosis developed in a 63 year-old lower total dose than the first reported case male patient while being treated with adju- (604 mg/mz vs. 2,733 mg/m2). Details of the vant methyl-CCNU for rectal carcinoma. This case history, including radiographic and toxicity is rare with methyl-CCNU, having pathologic findings, are presented.
I Key words: nitrosourea, pulmonary toxicity, chemotherapy
INTRODUCTION
Pulmonary toxicity has been reported to result from a variety of chemotherapeutic agents including the ni- trosoureas [l-31. Of the nitrosoureas, BCNU has been the drug most commonly associated with pulmonary fi- brosis [2,4-71. To our knowledge, there has been only one case report of pulmonary fibrosis related to methyl- CCNU therapy [8]. That particular patient had received a relatively large dose of the drug (4.1 g) over 25 months of therapy. We present here a report of pulmonary fibro- sis developing in a patient given a low dose of methyl- CCNU as adjuvant therapy for rectal carcinoma.
CASE HISTORY
A 63 year-old white male underwent an abdominoper- ineal resection of a Duke’s C2 adenocarcinoma of the rectum in January 1984. His initial post-operative ther- apy consisted of radiation therapy and 5-fluorouracil; 4,320 rads was administered in 24 fractions over a 35 day period. 5-Fluorouracil was administered at a dose of 500 mg/m2 on each of the first and last three days of the radiation therapy.
In April 1984, the patient was started on adjuvant chemotherapy consisting of 5-fluorouracil and methyl- CCNU, and therapy was completed in March 1985. Five cycles of chemotherapy were administered according to the following schedule: initial methyl-CCNU was 100 mg/m2 plus 5-fluorouracil at 300 mg/m2 (five days). Five weeks later, 5-fluorouracil was given for five days at 375 mg/m2. Ten weeks after the start of the regimen, methyl-
CCNU was administered at a dosage of 130 mg/m2 with five days of 5-fluorouracil at a dose of 325 mg/m2. Five weeks later, 5-fluorouracil was given for five days at a dosage of 375 mg/m2. The subsequent three cycles of therapy were completed at the same dosages and sched- ule as the second cycle.
The patient suffered only mild myelotoxicity during therapy, and no dosage or schedule changes were re- quired. In August 1984, the patient’s chest x-ray was unremarkable (Fig. 1). In September 1984, the patient had a needle aspiration biopsy for a questionable pelvic recurrence on CT scan. Cytology was Class IV. In Sep- tember 1985, the patient’s chest x-ray revealed progres- sive fibrosis (Fig. 2) which had developed over the past year and a 2-cm lung nodule. Pre-operative pulmonary function tests revealed moderately severe obstructive dis- ease. The 1 second forced expiratory volume was 1.84 liters (2.76 liters predicted), FVC was 3.44 liters (3.55 liters predicted), and FEV,/FVC was 53%.
A thoracotomy was performed in November 1985 be- cause of the enlarging nodule in the right lung. Two
From the Regional Cancer Center at Lourdes Hospital (M.B.) Depart- ment of Pathology and Laboratory (S.H.), Lourdes Hospital, Bing- hamton, New York; Department of Pathology, Creighton University School of Medicine, Omaha, Nebraska (R.M.L.); University of Ha- waii School of Medicine, Honolulu (C.R.). Address reprint requests to Margaret Block, MD, FACP, Associate Professor of Medicine, Creighton Cancer Center, 24th at California, Omaha, NE 68178.
0 1990 Wiley-Liss, Inc.

Methyl-CCNU Pulmonary Fibrosis 257
Fig. 1. Chest x-ray, August 1984, after two cycles of adjuvant chemotherapy.
biopsies of the lung were obtained; the first from the nodule in the right upper lobe, and the second from an area distal to the nodule. The nodular lesion was consis- tent with metastatic rectal carcinoma. The second biopsy of the right upper lobe showed extensive fibrosis with a patchy distribution having small amounts of relatively normal lung between areas of severe interstitial fibrosis. Frequent aggregates of lymphocytes and distended alve- olar spaces filled by type I1 pneumocytes were evident. Throughout this fibrotic lung there were areas containing hemosiderin pigment within the scar tissue and there were a few areas of subacute inflammatory change with polymorphonuclear leukocytes and lymphocytes. The overall appearance was that of patchy diffuse fibrosis of recent onset. The normal alveolar pattern in the fibrotic areas was completely obliterated (Fig. 3).
The patient refused further therapy following the tho- ractomy, and his bone scan was negative in January 1986. However, by August 1986, the bone scan revealed diffuse skeletal metastases, and a CT scan demonstrated a right adrenal lesion. Radiation therapy was adminis-
tered to treat bone lesions between T-4 and L-2 and on the right scapula. A compression fracture of T-8 led to the patient’s admission to a hospice program, where he remained until his demise in November 1986.
DISCUSS 10 N
During the 50 weeks that this patient underwent ad- juvant chemotherapy, he received a total of 1.1 g (604 mg/m2) of methyl-CCNU. This is about one-fourth the dosage of methyl-CCNU previously reported to cause pulmonary fibrosis [8], although the 4. I g (2733 mg/m2) [9] of methyl-CCNU in that case was administered over a 25 month period.
Aronin and co-workers [4] have implicated tobacco use as a possible factor contributing to the development of pulmonary toxicity during treatment with BCNU. The patient described herein was a current cigarette smoker, consuming between one-half and one package per day. He had a prior history of about 20 pack-years of cigarette smoking. Lee et al. [8] reported that their patient was

258 Block et al.
Fig. 2. which has appeared since earlier x-ray and nodule in right lung.
Chest x-ray, September 1985, after completion of adjuvant chemotherapy. Note the fibrosis
also a cigarette smoker at the time of methyl-CCNU therapy. The patient we are presenting also received 5-FU in combination with Me-CCNU; we cannot ex- clude the possibility that either cigarette smoking or 5- FU contributed to the development of the pulmonary fibrosis.
The obstructive lung disease detected on pulmonary function testing is consistent with chronic obstructive pulmonary disease typical of long-term cigarette smok- ers. The chest x-rays show evidence of hyperinflation and peribronchial fibrosis consistent with emphysema. It is possible that restrictive changes may have been detect- able on pulmonary function tests if baseline studies had been available on this patient.
The appearance of pulmonary fibrosis in the patient reported here is unusual because of its low incidence in methyl-CCNU-treated patients [3,8] and because of the much lower dose of drug causing this effect compared to a previously reported case. Doses of BCNU associated with pulmonary toxicity have generally been 1,000 mg/ m2 or greater [4,10,11]. However, a few instances of
fibrosis were reported in patients receiving relatively low doses of BCNU while also receiving cyclophosphamide [ 121. This suggests a synergistic toxicity between these two agents. In addition, patients receiving high-dose BCNU pulse therapy have also developed pulmonary fi- brosis [ 131. Pulmonary toxicity has also been reported subsequent to high doses of CCNU [14].
The lack of reported pulmonary toxicity in patients treated with methyl-CCNU may be due to the relatively short survival of many of these patients [6]. Proposed mechanisms of nitrosourea pulmonary toxicity have been reviewed [ 1,3], but a clear understanding of the factor(s) leading to pulmonary fibrosis is lacking. To date, meth- yl-CCNU has had limited utility as an anti-neoplastic agent, but it is still utilized in some investigational pro- tocols. Reports such as the present one indicate a poten- tial for serious toxicity. The accumulation of more de- tails about cases developing pulmonary toxicity during therapy and more data on the possible role of tobacco exposure during therapy may help define risk factors for this serious complication.
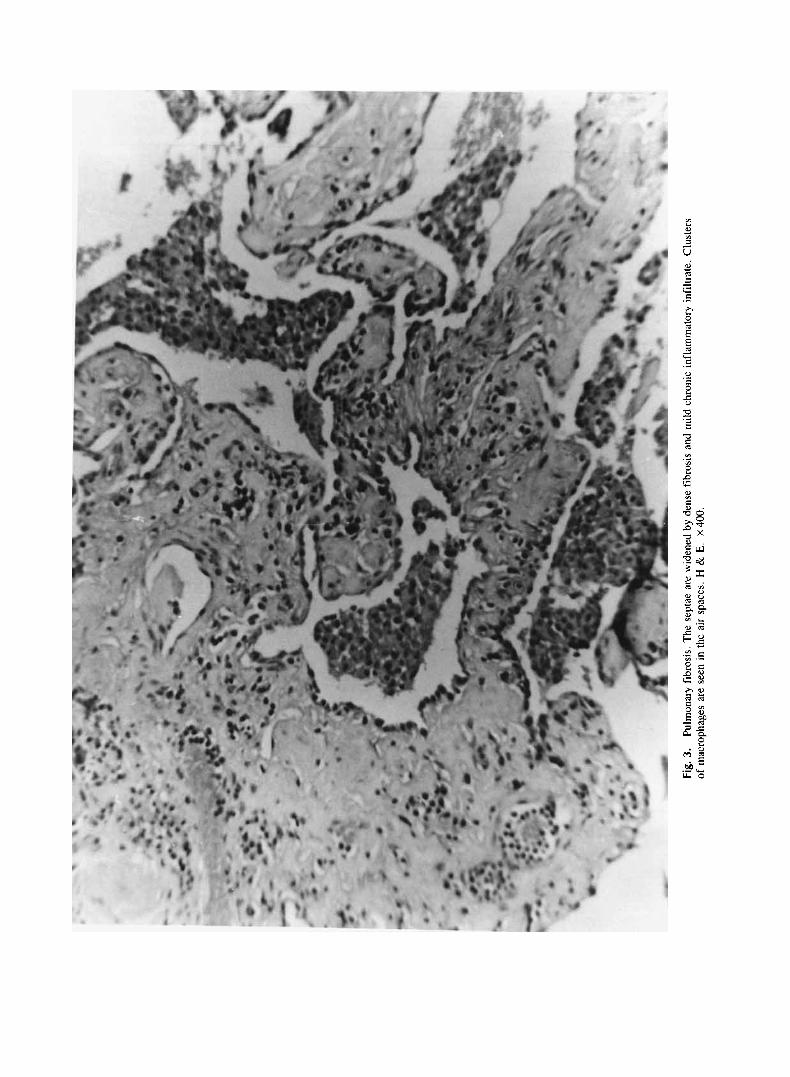
Fig.
3.
of m
acro
phag
es a
re s
een
in t
he a
ir sp
aces
. H &
E.
X 4
00.
Pulm
onar
y fib
rosi
s. Th
e se
ptae
are
wid
ened
by
dens
e fib
rosi
s an
d m
ild c
hron
ic in
flam
mat
ory
infil
trat
e. C
lust
ers

260 Block et al.
REFERENCES
I . Cooper JAD, White DA, Matthay RA: Drug-induced pulmonary disease. Am Rev Respir Dis 133:321-340, 1986.
2. Mitchell ES, Schein PS: Contribution on nitrosoureas to cancer treatment. Cancer Treat Rep 70:31-41, 1986.
3. Cooper JAD, Matthay RA. Drug-induced pulmonary disease. Dis Mon 2:61-120, 1987.
4. Aronin PA, Mahaley MS, Rudnick SA, Dudka L, Donohue JF, Selker RG, Moore P: Prediction of BCNU toxicity in patients with malignant gliomas. N Engl J Med 303:183-188, 1980.
5 . Weiss RB, Poster DS, Penta JS: The nitrosoureas and pulmonary toxicity. Cancer Treat Rev 8:111-125, 1981.
6. Weiss RB, Muggia FM: Cytotoxic drug-induced pulmonary dis- ease: Update 1980. Am J Med 68:259-266, 1980.
7. Muggia FM, Louie AC, Sikic B1: Pulmonary toxicty of antitumor agents. Cancer Treat Rev 10:221-243, 1983.
8. Lee W, Moore RP, Wampler GL: Interstitial pulmonary fibrosis as a complication of prolonged methyl-CCNU therapy. Cancer Treat Rep 62:1355-1358, 1978.
9. Hundley RF, Lukens JN: Nitrosourea-associated pulmonary fi- brosis. Cancer Treat Rep 63:2128-2130, 1979.
10. Melato M, Tuveri G: Pulmonary fibrosis following low-dose 1, 3-BIS (2-chloroethy1)- I -nitrosourea (BCNU) therapy. Cancer 45:
11. Weinstein AS, Deiner-West M, Nelson DF, Pakuris E: Pulmonary toxicity of carmustine in patients treated for malignant glioma. Cancer Treat Rep 70:943-946, 1986.
12. Durant JR, Norgard MJ, Murad TM, Bartolucci AA, Langford KH. Pulmonary toxicity associated with bischloroethylnitrosourea (BCNU). Ann Intern Med 90:191-194, 1979.
13. Litam JP, Dail DH, Spitzer G, Vellekoop L, Verma DS, Zander AR, Dicke KA: Early pulmonary toxicity after administration of high-dose BCNU. Cancer Treat Rep 65:39-44, 1981.
14. Cordonnier C , Vernant J, Mital P, Lange F, Bernaudin J, Rochant H: Pulmonary fibrosis subsequent to high doses of CCNU for chronic myeloid leukemia. Cancer 51:1814-1818, 1983.
1311-1314, 1980.