pulmonary hypertension secondary to hiv - campania · pulmonary hypertension secondary to hiv...
TRANSCRIPT

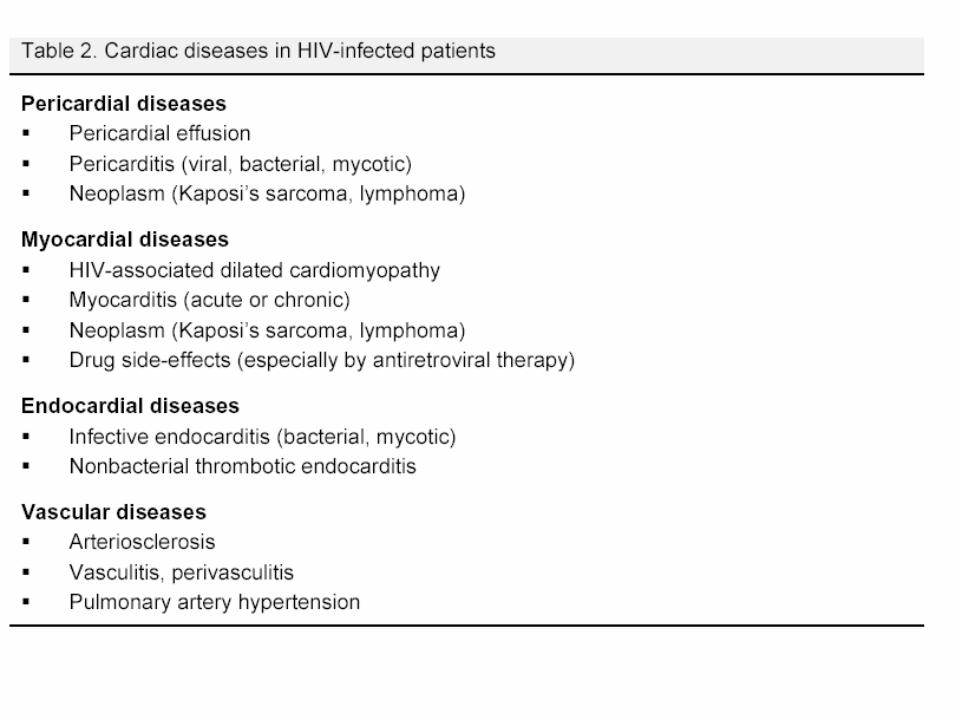
Pulmonary Hypertension secondary to HIV
Nicola Petrosillo MD
National Institute for Infectious Diseases “Lazzaro Spallanzani” – Rome, Italy


The emergence of chronic diseases
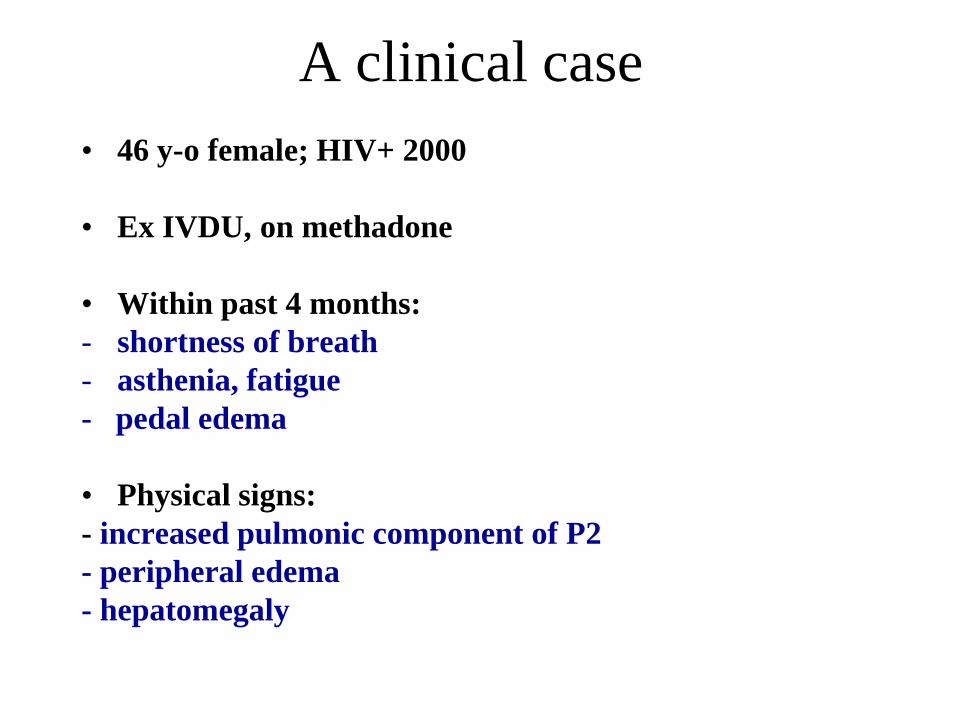
A clinical case
• 46 y-o female; HIV+ 2000
• Ex IVDU, on methadone
• Within past 4 months:
- shortness of breath
- asthenia, fatigue
- pedal edema
• Physical signs:
- increased pulmonic component of P2
- peripheral edema
- hepatomegaly

• Chest X rays
• ECG

• Echocardio
PASP: 50 mmHg
• Right heart catheterization: mean PASP 50 mmHg, no reply to NO
•HIVRNA 4000 cp/ml CD4+ 690/mmc •HCVAb+ cryoglobulinemia IgGk and cryocrite 4% •HCVRNA 285,000 cp/ml NO TARV
HIV-related pulmonary hypertension NYHA 3

Simonneau G et al. J Am Coll Cardiol 2009; 54: S43-45
Clinical Classification of Pulmonary Hypertension (Dana Point)
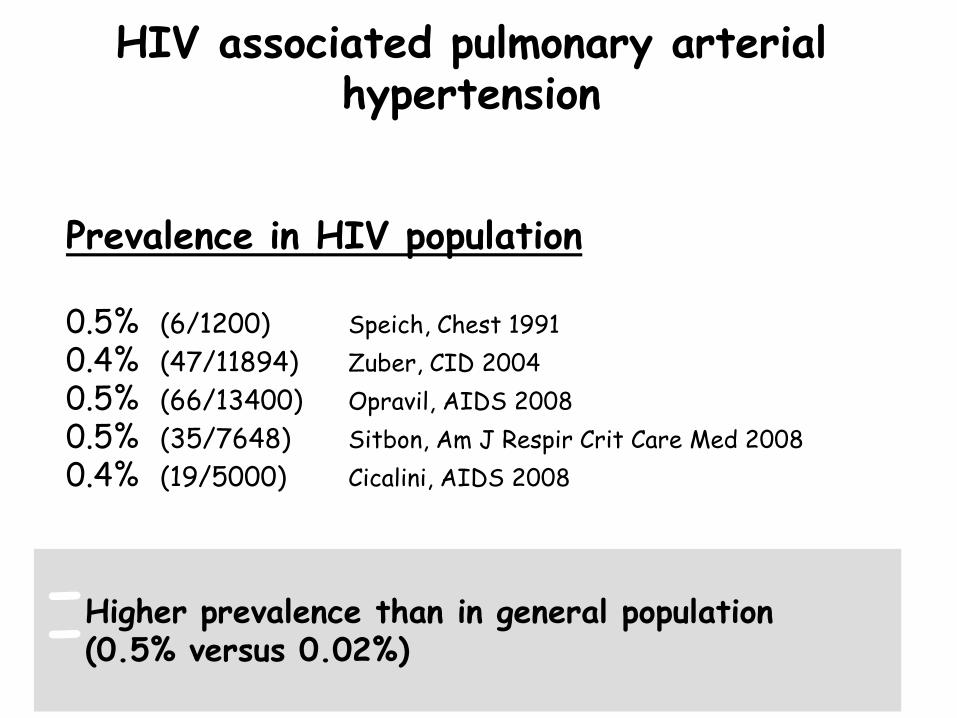
HIV associated pulmonary arterial hypertension
-Higher prevalence than in general population -(0.5% versus 0.02%)
Prevalence in HIV population 0.5% (6/1200) Speich, Chest 1991 0.4% (47/11894) Zuber, CID 2004
0.5% (66/13400) Opravil, AIDS 2008
0.5% (35/7648) Sitbon, Am J Respir Crit Care Med 2008
0.4% (19/5000) Cicalini, AIDS 2008

Sitbon O et al. Am J Respir Crit
Care Med 2008; 177: 10813
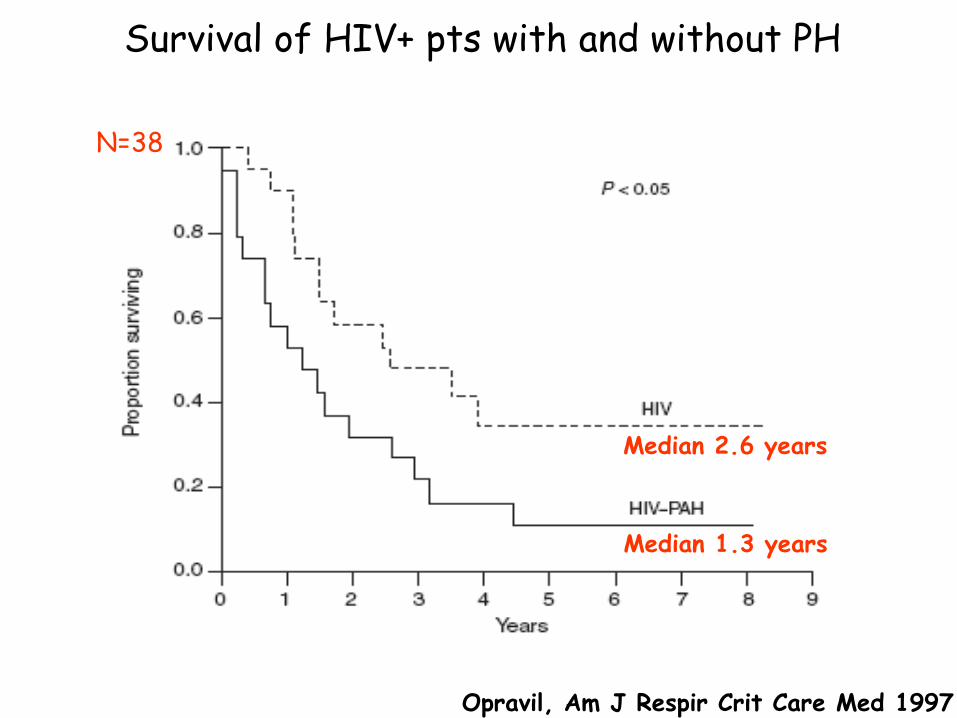
Opravil, Am J Respir Crit Care Med 1997
N=38
Median 2.6 years
Median 1.3 years
Survival of HIV+ pts with and without PH
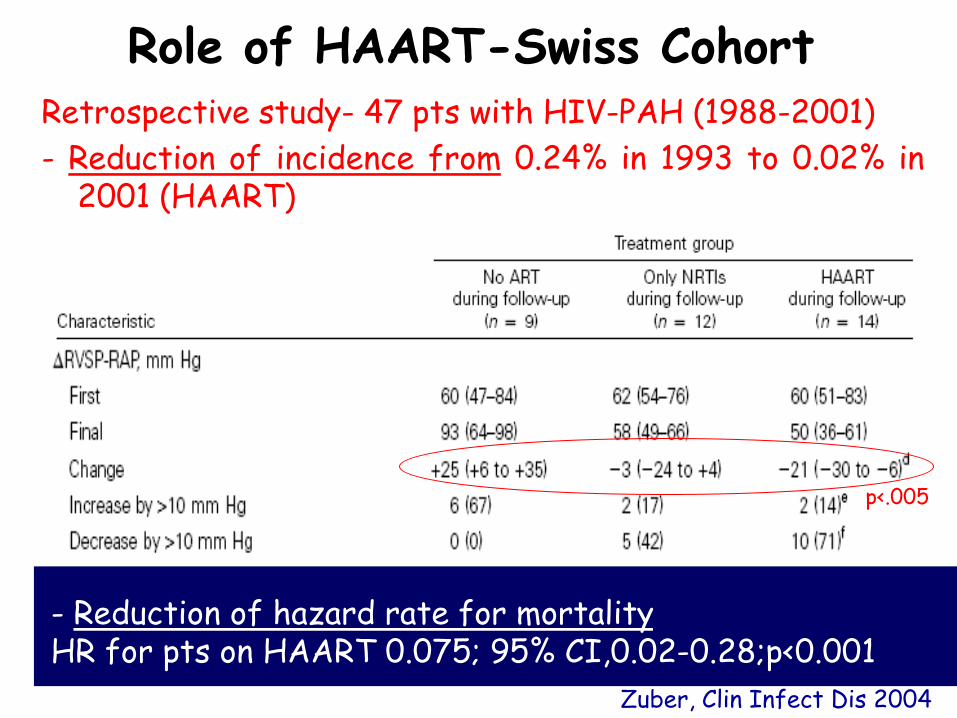
Zuber, Clin Infect Dis 2004
p<.005
- Reduction of hazard rate for mortality HR for pts on HAART 0.075; 95% CI,0.02-0.28;p<0.001
Role of HAART-Swiss Cohort Retrospective study- 47 pts with HIV-PAH (1988-2001)
- Reduction of incidence from 0.24% in 1993 to 0.02% in 2001 (HAART)
HAART does not prevent the occurrence of PAH
- 66 pts (1988-2006 )
-19 pts with a new PAH diagnosis after 2001
-2/3 of pts on HAART since at least 3 months at the
diagnosis of HIV-PAH
Opravil, AIDS 2008
Role of HAART-Swiss Cohort

N=66
Sopravvivenza mediana 3.6 anni 84% dei pazienti sopravvissuti ad 1 anno
Role of HAART-Swiss Cohort
Opravil, AIDS 2008
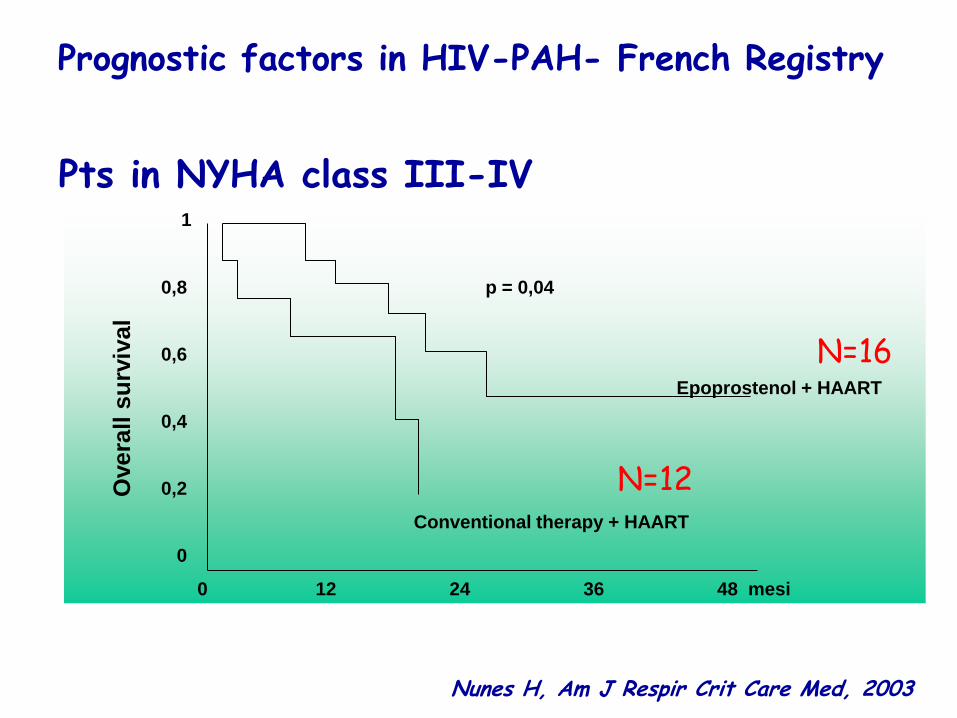
Prognostic factors in HIV-PAH- French Registry
Pts in NYHA class III-IV 1
0,8 p = 0,04
0,6
Epoprostenol + HAART
0,4
0,2
Conventional therapy + HAART
0
0 12 24 36 48 mesi
Overa
ll s
urv
ival
Nunes H, Am J Respir Crit Care Med, 2003
N=16
N=12
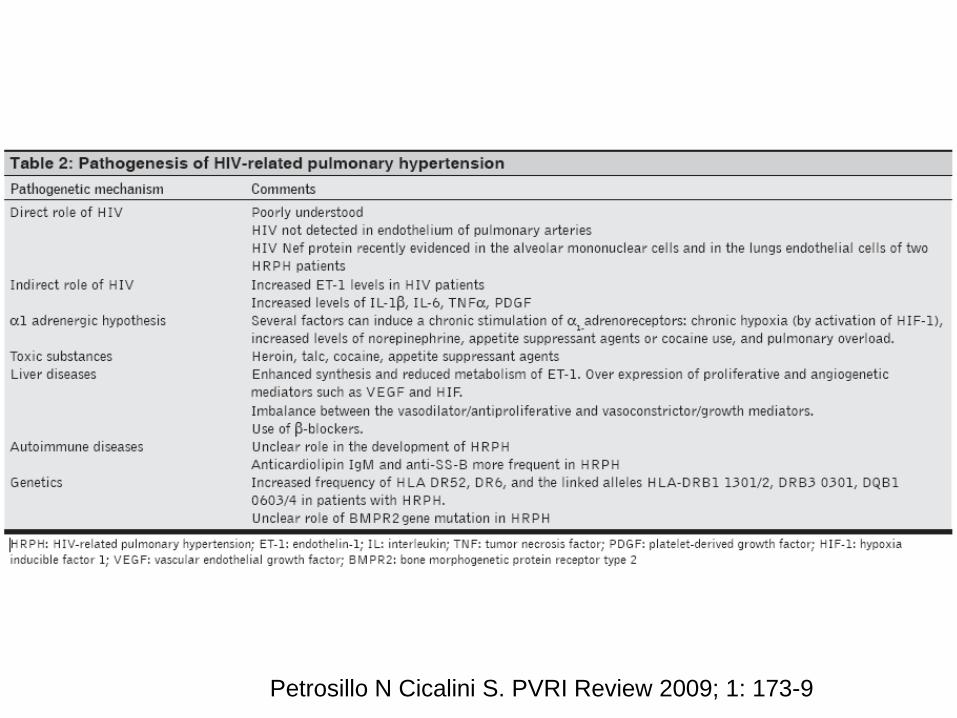
Petrosillo N Cicalini S. PVRI Review 2009; 1: 173-9

Pathogenesis
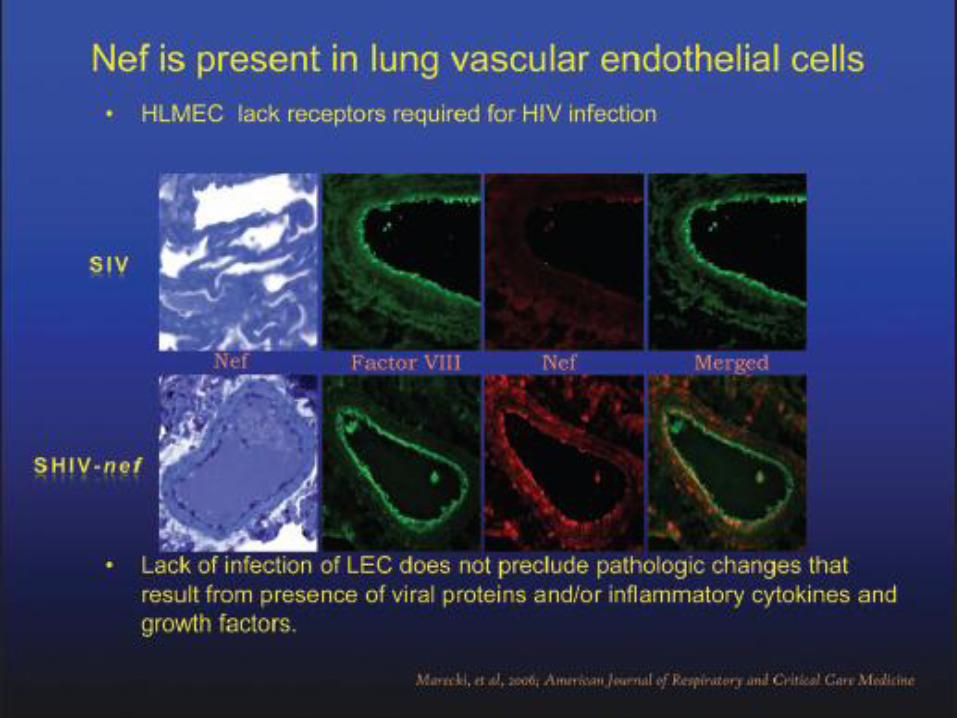
Direct role of HIV • - HIV never isolated in endothelial cells of affected pulmonary
vessels • - Protein Nef in mononucleolar alveolar cells and in endothelial cells
of lung Indirect role of HIV Increased levels of ET-1, IL-1 beta, IL-6, TNF alpha and PDGF alpha 1 adrenergic hypotesis - Chronic stimulation (chronic hypossia, high circulating levels of
norepinephrine, cocaine, appetite suppressant agents) of alpha1adrenergic receptors => excessive proliferation of smooth muscle cells and fibroblasts, pulmonary vascular hypertrophy and excessive vasoconstriction of pulmonary vascular medium-sized arteries

Pathogenesis
Coinfection with hepatitis viruses -Enhanced synthesis and reduced metabolism of ET-1 (in
cirrhosis) - PAPS higher in HIV+ pts with PH and cirrhosis vs
HIV+ pts with PH without cirrhosis Genetic factors HLA DR52 e DR6 ? HHV8 -HHV-8 antigens and genoma in pts with HP (no HIV) -HHV8 represents a common infection in HIV + pts
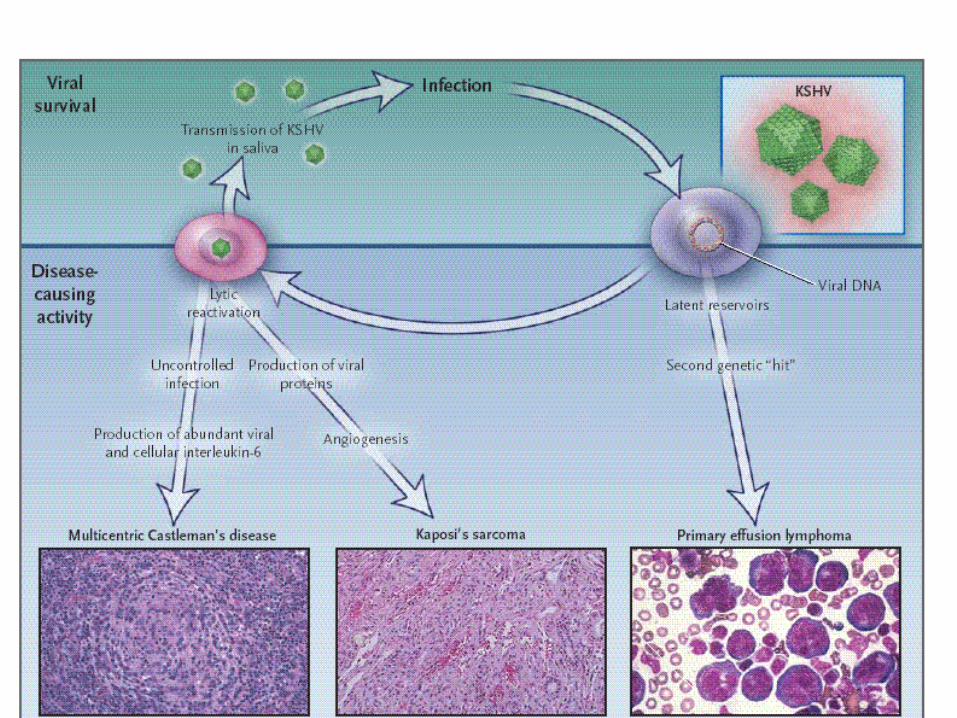
HHV8 and related clinical manifestations
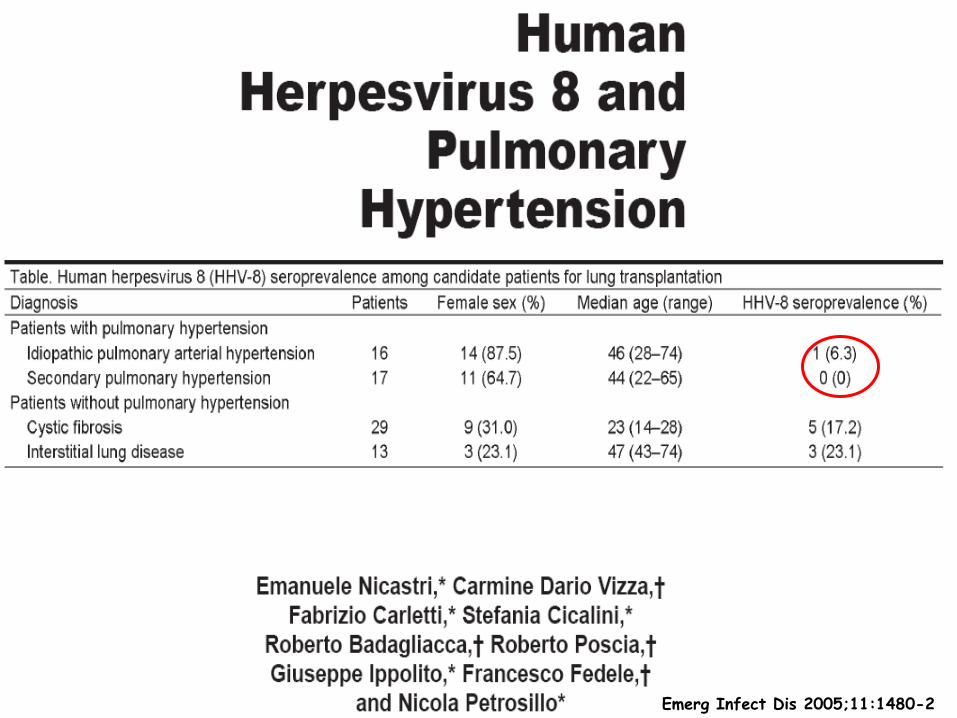
Emerg Infect Dis 2005;11:1480-2



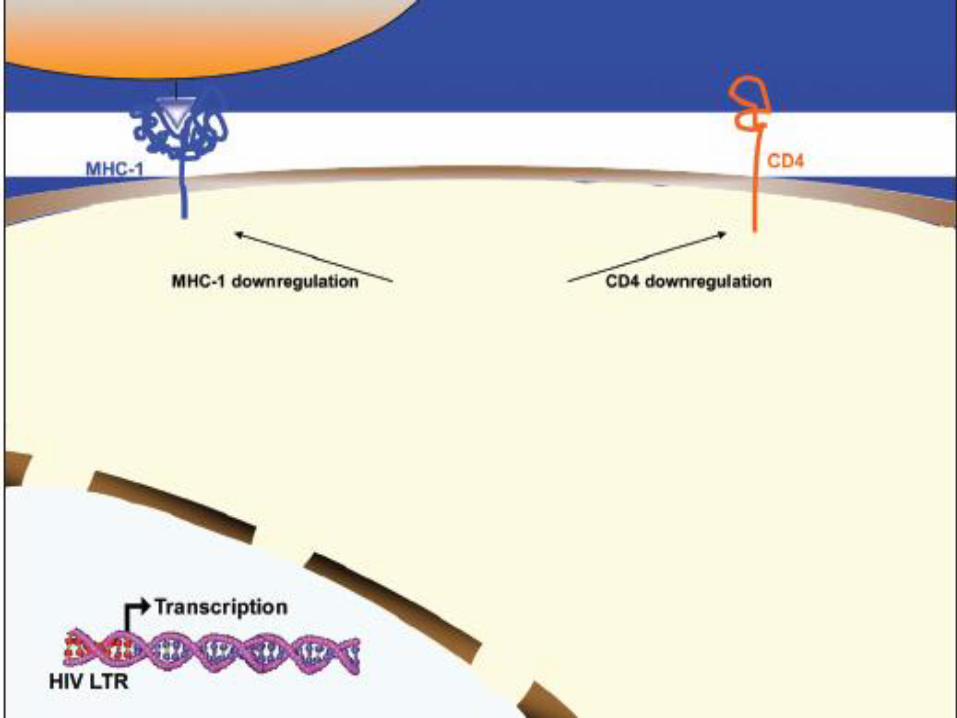
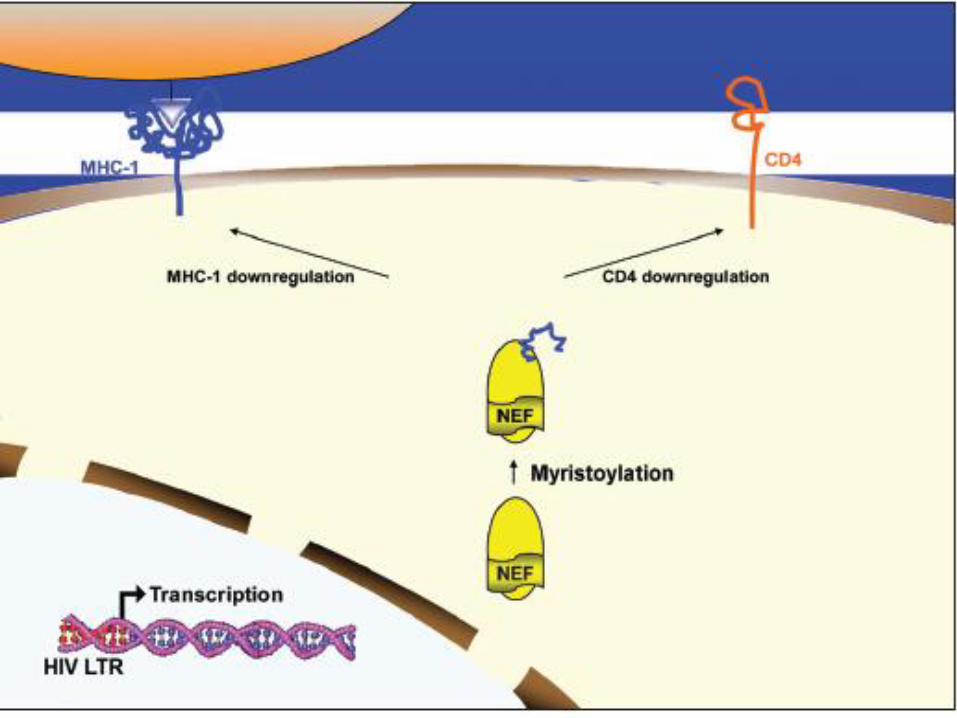



•is an accessory protein expressed early
during viral infection, together with Tat.
•The Nef protein is a molecular adaptor and is
a key player in HIV pathogenesis.
•For example, Nef complexes with several host
cell proteins (including members of the p21-
activated kinase family), and recruits host
adaptor proteins to commander trafficking of
intracellular vesicles participating in secretory
and endocytic pathways.
HIV Nef (negative factor)
Fackler OT et al. Mol Cell Biol 2000; 20:2619-2627.
Roeth JF et al. Microbiol Mol Biol Rev 2006; 70:548-563.

•Nef downregulates essential molecules such
CD4 receptor by targeting it to the endocytic
degradation pathway in clathrin-coated vesicles
and MHC-1 by sequestering it in the trans-Golgi
and hence, preventing the recycling of this
receptor from the Golgi to the membrane.
HIV Nef (negative factor)
Miller MD et al. J Exp Med 1994; 179:101-113
•Also, Nef is a migratory stimulus for monocytes
and induce the release of inflammatory
molecules. Lehmann MH et al. Exp Cell Res 2006; 312:3659-3668.
Olivetta E et al. J Immunol 2003; 170:1716-1727.
Capoccia BJ et al. J Leukoc Biol 2008; 84:760-768

•The potential of Nef as a vascular insult is underscored by its
capacity to enter lymphocytes via the human chemokine
receptor CXCR4 and exert apoptotic effects (James CO et al. J
Virology 2004; 78:3099-3109).
•Endothelial cells express this receptor and therefore, it is
conceivable that Nef may be present in endothelial cells in the
absence of infection.
•Nef localizes to vascular and perivascular cells (Marecki J et al.
Chest 2005; 128(6 Suppl):621S-622S; Marecki JC et al. Am J Respir Crit Care Med
2006; 174:437-445) and induces apoptosis in brain endothelial cells
when expressed intracellularly or exogenously.
•Nef also impairs vasomotor functions in pulmonary artery
cells, decreases the expression of endothelial nitric oxide
synthase and increases oxidative stress (Duffy P et al. J Surg Res
2009. 53).
Potential clinical role of Nef

Nef is mutated in the lung of a patient
with HRPAH. •Nef sequences in the blood of patients with pulmonary
hypertension show signature patterns that are specific
to this disease phenotype, compared to their
normotensive counterparts (Almodovar S et al. Am J Respir Crit Care
Med 2009; 77:A440.55).
•Peripheral blood samples are the main biological
specimens analyzed in clinical research because lung
tissues from these patients are extremely difficult to
obtain.
•Nevertheless HIV-1 nef sequences from archived lung
tissue from an HRPAH patient from the Italian Latium
Registry of HRPAH (Petrosillo N et al. AIDS 2006; 20:2128-2129) were
amplified and cloned.
Almodovar S et al. Chest 2010; 137(6 Suppl):6S-12S.

Nef is mutated in the lung of a
patient with HRPAH.
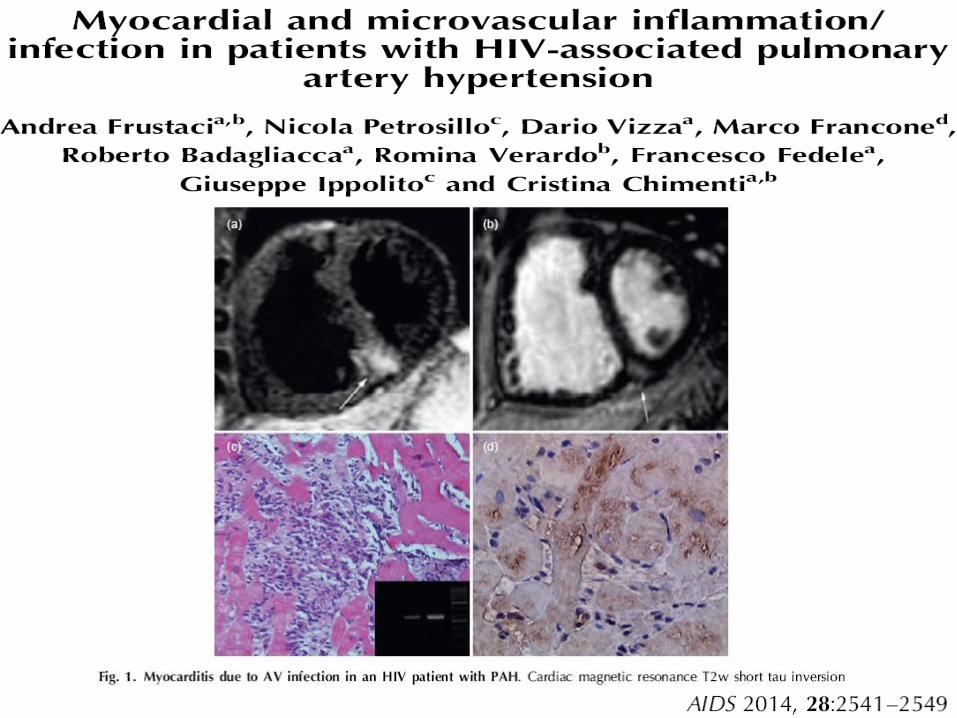
The patient was diagnosed with HIV infection in 2000 and with HRPAH in 2006, the same year the patient died.
The lungs were collected during autopsy and subsequently analyzed.
Sequence analyses of the HIV nef showed the presence of 4/5 Nef mutations reported in SHIVnef-infected macaques (Mandell CP et al. Virology 1999; 265:235-251) with plexiform lesions.
Furthermore, this Nef sequence had six Nef functional domains mutated, all of them found only in the lung tissues collected in 2006, and interestingly, none of the mutations was found in PBMC collected at the time of HIV diagnosis.
Almodovar S et al. Chest 2010; 137(6 Suppl):6S-12S.

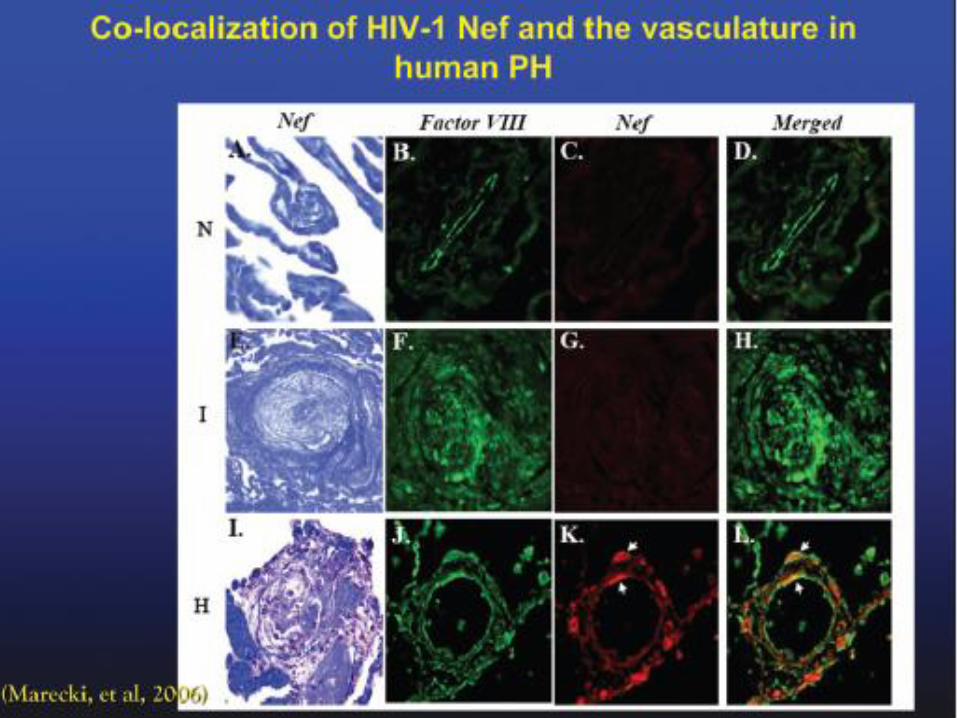



Figure 2. Phylogenetic reconstruction of HIV-1 nef sequences from a patient diagnosed with HRPAH. Archived PBMC and
lung tissue was obtained from a patient diagnosed with HRPAH by echocardiography, and enrolled in the Latium Registry of HRPAH
in Rome. HIV nef was PCR-amplified, cloned and sequenced; sequences were aligned using BioEdit and the phylogenetic tree was
created using MEGA4. The analysis was statistically supported by 1000 boostrapre-samplings and only values >70% are shown.
Tissue-specific clustering of the nef quasispecies suggest differential evolution at the level of blood (closed circles) and lung (open
circles).
99
99
9992
99
0.03
Peripheral blood
Lung
Chest 2010; 137(6 Suppl):6S-12S.
There are clear
phylogenetic differences
between the
quasispecies of the lung
vs the periphery
Nef is mutated in the lung of a
patient with HRPAH. •These findings suggest either that the viral quasispecies in the lung arose later in the course of infection, or that these variants are replicating more efficiently in the lung than in the periphery.
•These aspects warrant further research efforts in order to validate (and possibly implement) the use of Nef sequences as potential screening tools to identify subjects at risk of HRPAH, especially in the low-resource settings
Almodovar S et al. Chest 2010; 137(6 Suppl):6S-12S.



Inibisce aggregazione PLT
Vasocostrizione
e proliferazione
+ clearance ET
+ produzione NO
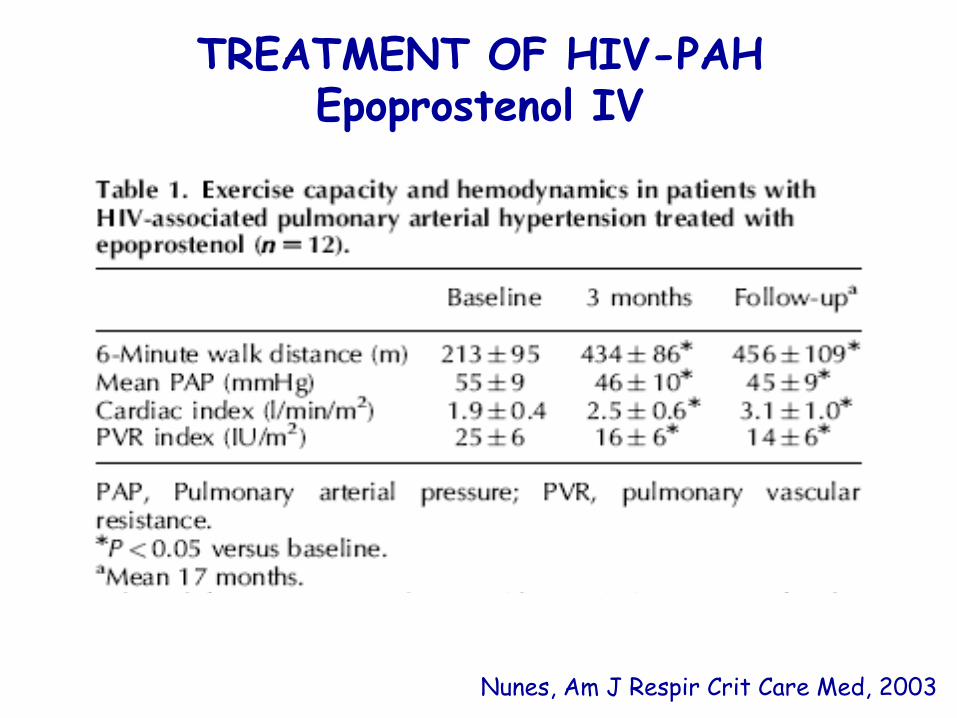
TREATMENT OF HIV-PAH Epoprostenol IV
Nunes, Am J Respir Crit Care Med, 2003
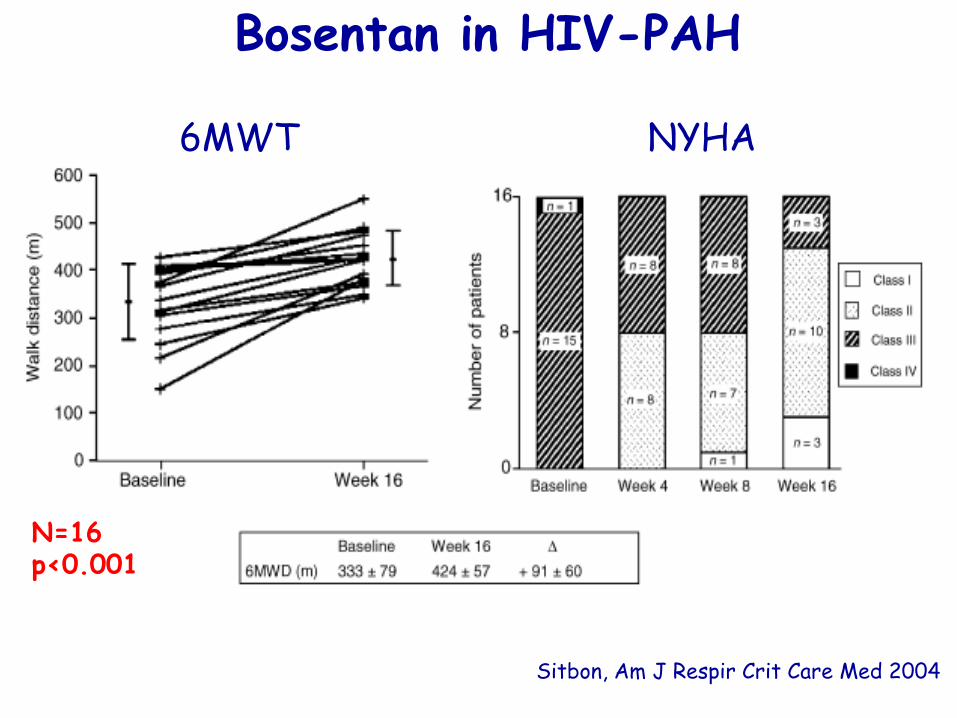
Bosentan in HIV-PAH
Sitbon, Am J Respir Crit Care Med 2004
N=16 p<0.001
6MWT NYHA
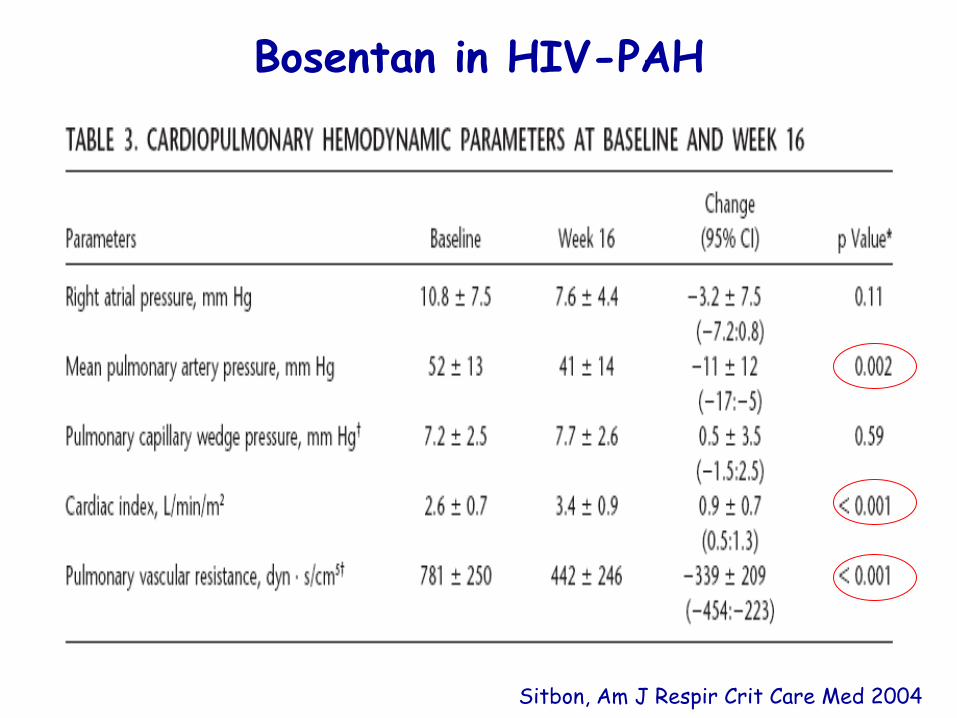
Bosentan in HIV-PAH
Sitbon, Am J Respir Crit Care Med 2004

Sildenafil and HIV-PAH
• No controlled studies on its efficacy.
• Data on efficacy derive from case series
Schumacher, AIDS 2001
Alp, AIDS 2003

• P.A. 40 mm, right P.A. 22,
left P.A. 14 mm
• Right Ventricle
• Major axis 90 mm
• Minor axis 43 mm
• ED volume 88 ml
• ES volume 62 ml
• EF: 30 % (n.v. 40-60%)
Feb 5, 2007
PAP 41
TPR 15
CI 1,7
WT 470
Feb 13, 2008
PAP 37
TPR 5,6
CI 2,5
WT 576
• P.A. 35 mm, right P.A. 20, left P.A. 15 mm
• Right Ventricle
• Major axis 78 mm
• Minor axis 43 mm
• ED volume 87 ml
• ES volume 46 ml
• EF: 46 % (n.v. 40-60%)
Cardiac NMR at the beginning of sildenafil therapy and 1 year later
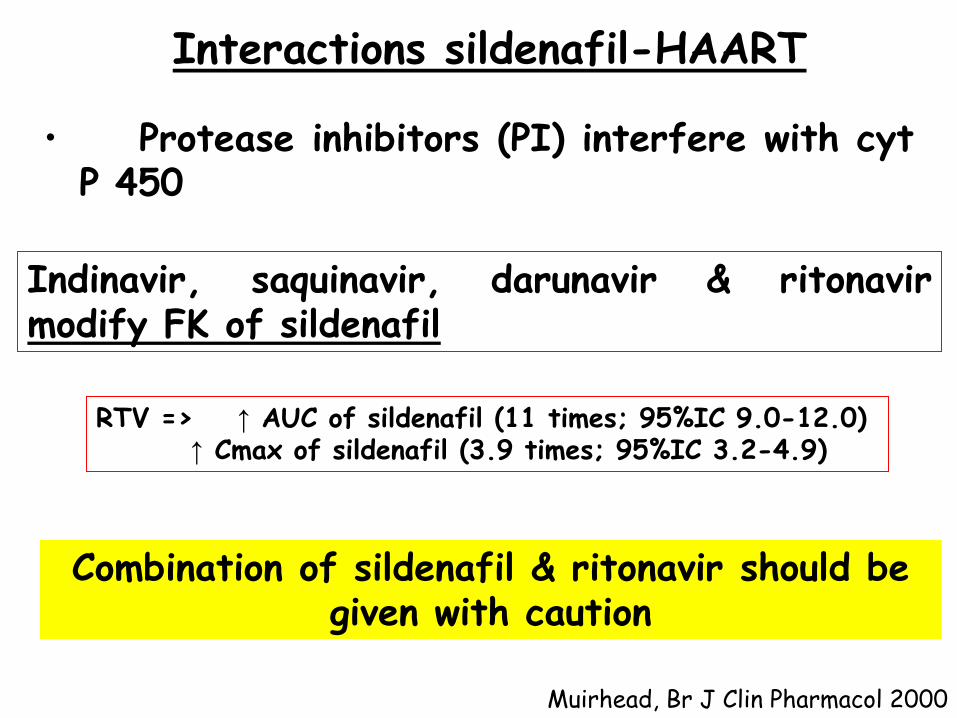
• Protease inhibitors (PI) interfere with cyt P 450
Indinavir, saquinavir, darunavir & ritonavir modify FK of sildenafil
Muirhead, Br J Clin Pharmacol 2000
Interactions sildenafil-HAART
RTV => ↑ AUC of sildenafil (11 times; 95%IC 9.0-12.0) ↑ Cmax of sildenafil (3.9 times; 95%IC 3.2-4.9)
Combination of sildenafil & ritonavir should be given with caution
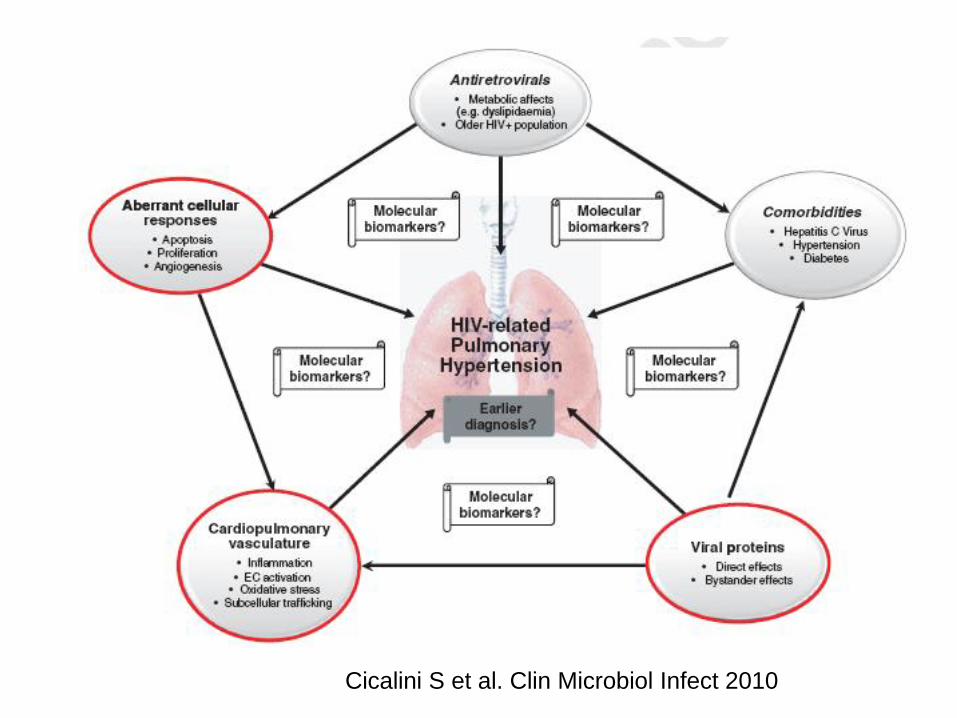
Cicalini S et al. Clin Microbiol Infect 2010

CONCLUSIONS
The current interest in this severe and life
threatening manifestation is based on the
following facts:
• the frequency of pulmonary arterial
hypertension is higher (>600 times) than in the
general population.
• This estimate means that only in North America
and Western Europe, where almost 3.8 million
people are living with HIV, there are about 8 –
10 000 cases of HIV infected patients with likely
severe and life-threatening pulmonary arterial
hypertension.

• PAH occurs independent of the CD4+ cell
count, it is not dependent on presence or
absence of antiretroviral treatment, and may
develop before a patient meets criteria for the
initiation of antiretroviral treatment.
• Recent advances in the pathobiology of PAH
suggest a role of nef gene mutatiopns, viral
coinfections, such as herpes viruses, viral
hepatitis viruses, etc. This could partly explain
the higher frequency of pulmonary arterial
hypertension in HIV infected individuals,

• New and potent drugs against pulmonary
arterial hypertension are available, and
additional drugs are under development. Some
of these drugs can interact with antiretroviral
drugs.
• Finally, there are some controversies in the
role of antiretroviral treatment regarding the
clinical course of PAH.