pulse wave analysis digital plethysmography finger...
TRANSCRIPT
Pulse Wave Analysis Digital Plethysmography Finger Plethysmography
Accelerated Plethysmography
Clinical Bottom Line - The Simple Explanation
Brief BackgroundCardiovascular disease (CVD) is the leading cause of mortality and disability worldwide. Predictors of CVD risk include arterial stiffness, autonomic imbalance, and hypertension58-60, which may be measured by various invasive and noninvasive techniques.
The digital plethysmograph is a secondary output of the pulse oximeter, which is commonly used to measure arterial blood saturation (SaO2)61. Digital plethysmography provides noninvasive, continuous, and real-time measurement of arterial pressure with infrared light transmitted through a digit (finger or toe)62. This technique acquires the digital volume pulse (DVP), a waveform that estimates pulse wave velocity (PWV). Blood pressure is a component of the PWV, which is the standard measure of arterial stiffness (a major CVD risk factor)63,64. DVP measured by digital plethysmography has been shown to be a reliable and reproducible technique for indirectly determining arterial stiffness indices (SI)65.
Besides being noninvasive, digital plethysmography is easy to implement62,63 and does not require patient cooperation66. Current public health guidelines call for noninvasive screening of CVD risk in all asymptomatic men older than age 45 and women older than age 55 not only to prevent CVD mortality but also to curb rising CVD-related healthcare costs67. Thus, digital plethysmography may have an important role in detecting and monitoring parameters of CVD.
The plethysmograph is a waveform that represents pulsatile peripheral blood flow, which reflects both peripheral and central hemodynamics68. This waveform may be acquired noninvasively with infrared light transmitted through the skin to assess hemodynamic parameters69. Photoplethysmography (PPG) is thus a useful noninvasive measure of vascular dysfunction and heart rate variability68.
Growing evidence suggests that heart rate variability (HRV) may reflect established parameters of CVD risk, as well as emerging risk factors such as stress60. Because many CVD risk factors are modifiable, early detection is crucial for reducing CVD-related death and disability.
There is strong scientific evidence supporting the use of digital plethysmography as a diagnostic or prognostic tool for cardiovascular disease, peripheral vascular disease (including primary and secondary Raynaud’s phenomenon), and sleep apnea. There is good scientific evidence supporting digital plethysmography in the detection of diabetic neuropathy. This procedure has also been studied for numerous other disorders, though the diagnostic efficacy is not as clear.
www.level1diagnostics.com
2
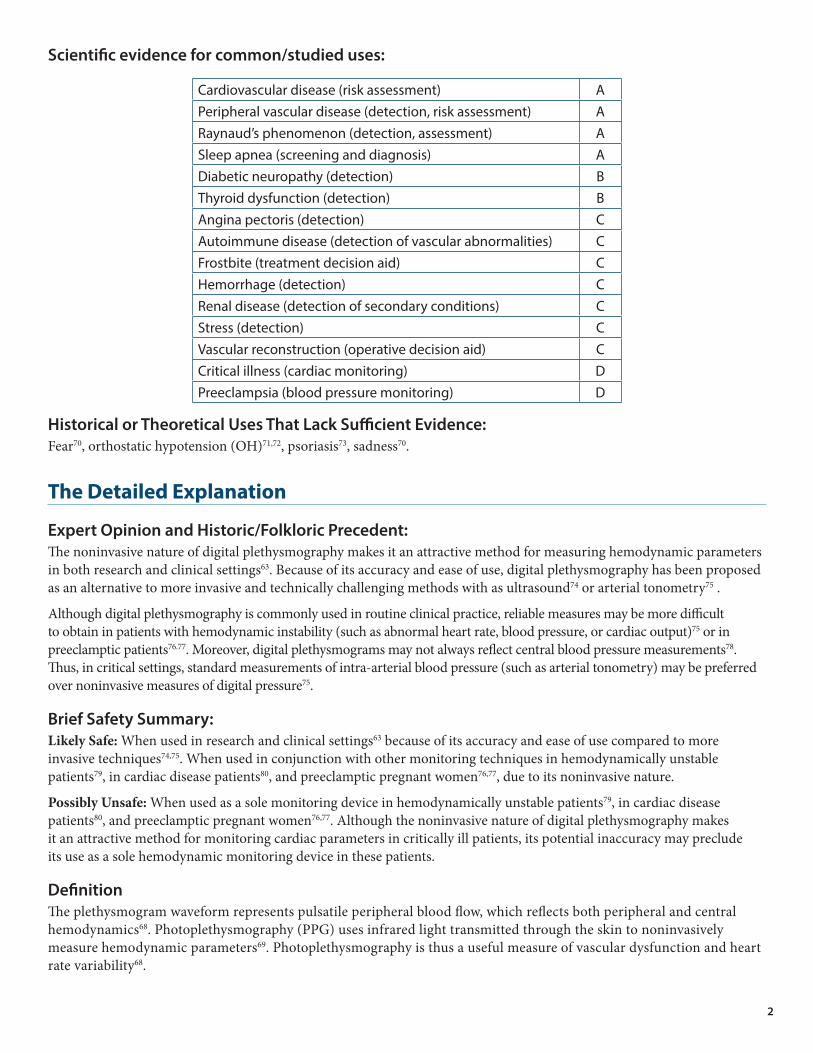
Scientific evidence for common/studied uses:
Cardiovascular disease (risk assessment) APeripheral vascular disease (detection, risk assessment) ARaynaud’s phenomenon (detection, assessment) ASleep apnea (screening and diagnosis) ADiabetic neuropathy (detection) BThyroid dysfunction (detection) BAngina pectoris (detection) CAutoimmune disease (detection of vascular abnormalities) CFrostbite (treatment decision aid) CHemorrhage (detection) CRenal disease (detection of secondary conditions) CStress (detection) CVascular reconstruction (operative decision aid) CCritical illness (cardiac monitoring) DPreeclampsia (blood pressure monitoring) D
Historical or Theoretical Uses That Lack Sufficient Evidence:Fear70, orthostatic hypotension (OH)71,72, psoriasis73, sadness70.
The Detailed Explanation
Expert Opinion and Historic/Folkloric Precedent:The noninvasive nature of digital plethysmography makes it an attractive method for measuring hemodynamic parameters in both research and clinical settings63. Because of its accuracy and ease of use, digital plethysmography has been proposed as an alternative to more invasive and technically challenging methods with as ultrasound74 or arterial tonometry75 .
Although digital plethysmography is commonly used in routine clinical practice, reliable measures may be more difficult to obtain in patients with hemodynamic instability (such as abnormal heart rate, blood pressure, or cardiac output)75 or in preeclamptic patients76.77. Moreover, digital plethysmograms may not always reflect central blood pressure measurements78. Thus, in critical settings, standard measurements of intra-arterial blood pressure (such as arterial tonometry) may be preferred over noninvasive measures of digital pressure75.
Brief Safety Summary:Likely Safe: When used in research and clinical settings63 because of its accuracy and ease of use compared to more invasive techniques74,75. When used in conjunction with other monitoring techniques in hemodynamically unstable patients79, in cardiac disease patients80, and preeclamptic pregnant women76,77, due to its noninvasive nature.
Possibly Unsafe: When used as a sole monitoring device in hemodynamically unstable patients79, in cardiac disease patients80, and preeclamptic pregnant women76,77. Although the noninvasive nature of digital plethysmography makes it an attractive method for monitoring cardiac parameters in critically ill patients, its potential inaccuracy may preclude its use as a sole hemodynamic monitoring device in these patients.
DefinitionThe plethysmogram waveform represents pulsatile peripheral blood flow, which reflects both peripheral and central hemodynamics68. Photoplethysmography (PPG) uses infrared light transmitted through the skin to noninvasively measure hemodynamic parameters69. Photoplethysmography is thus a useful measure of vascular dysfunction and heart rate variability68.
3
Digital photoplethysmography uses infrared light transmitted through a digit (finger or toe) to measure arterial pressure noninvasively, continuously, and in real time62. Digital volume pulse (DVP), an output of digital photoplethysmography, estimates pulse wave velocity (PWV), which in turn reflects aortic stiffness and blood pressure63,64.
Pulse transit time (PTT) is defined as the interval between the electrocardiogram (ECG) R wave and the foot of the PPG wave, or the elapsed time of a pulse wave between two arterial sites; altered PTT is an indirect indicator of various hemodynamic pathologies associated with aging, hypertension, cardiovascular disease, and diabetes mellitus81,82.
Accelerated plethysmography (APG) uses the second derivative of the photoplethysmograph (SDPTG), which allows more detailed analysis of the primary plethysmogram. SDPTG consists of four systolic waves (the “a” or early positive wave, “b” or early negative wave, “c” or late reincreasing wave, and “d” or late redecreasing wave) and one diastolic wave (“e” or early positive wave). Wave analyses are generally made using the ratios of waves b-e to the a-wave (b/a, c/a, d/a and e/a)83.
Commercially available photoplethysmographs can continuously record finger arterial pressure to 0.25kPa accuracy compared to direct (albeit invasive) intra-arterial recordings84.
Assessment TechniquesDigital plethysmography provides noninvasive, continuous, and real-time measurement of digital (finger or toe) arterial pressure62 and is generally performed according to the method described by Penaz85. The infrared light source is integrated into a pneumatic digital cuff, which is placed around a finger or a toe. The instantaneous digital blood volume is reflected in the light intensity. Thus, the photoplethysmograph measures blood flow and volume in tissues, and signal variations may reflect heartbeat and breathing86.
The light signal increases with cuff pressure elevation, and reduces when the intravascular pressure is exceeded. Maximal amplitude occurs when the arterial wall is completely relaxed and the transmural pressure ceases62. Commercially available digital photoplethysmographic devices may record finger arterial pressure to 0.25kPa accuracy84.
Venous refilling time, or the time it takes for the pulse trace to return to 90% of the baseline measurement87, is the most quantitative (and perhaps the most informative) parameter of photoplethysmography. Digital and other calibrated forms of photoplethysmography also allow drainage to be assessed88.
While photoplethysmography is generally performed with infrared light (880nm wavelength), green light at wavelength 525nm has also been studied. Green light photoplethysmography may better reflect ECG results, particularly at lower temperatures (e.g., 15°C)89.
Devices that produce plethysmographs may also produce other measurements, such as arterial blood saturation (SaO2)61, blood pressure, and cardiac output (CO)79,90.
Mercury strain-gauge plethysmography, which uses a mercury-filled tube wrapped around the limb under examination91, has also been used on the finger92.
A dual-channel photoplethysmography system has been used to calculate the finger-to-toe pulse transit time (PTT) and to monitor pulse wave velocity (PWV) during general anesthesia and surgery93.
Using the method of Penaz, digital plethysmography with the Finapres® noninvasive blood pressure monitor indirectly records the arterial waveform with little systemic bias compared to intra-arterial pressure (IAP) measurements, but this method has significant inaccuracy. A novel statistical resampling of 20 published studies (449 patients and 4,490 resamples) showed that the Finapres® can, in fact, provide accurate diastolic and mean arterial pressures compared with IAP; the apparent variability of Finapres® systolic pressures may be due to physiological differences that may contribute to “offset” errors. These may be prevented by calibrating the Finapres® against reliable reference arterial pressures94.
Peripheral arterial tonometry (PAT) is a plethysmographic technique that measures peripheral arterial tone. PAT measures pulsatile arterial volume changes that reflect sympathetic tone variations. PAT measurements are often taken from the fingertip, and the noninvasive nature makes this technique useful in ambulatory monitoring95.

4
Diagnostic TechniquesGeneral: For finger plethysmography performed with upper-arm occlusion, recommended occlusion time is five minutes (time to reach maximum response)96. High pulmonary artery pressure, which subsequently increases venous system pressure, has been suggested to affect digital photoplethysmographic screening in deep venus thrombosis (DVT); however, the effect of high pulmonary artery pressure (PAP) has been shown to be statistically insignificant, suggesting that it may be excluded as a confounding factor for this test97. A novel finger-occlusion plethysmograph (FOP) has been studied for estimating peripheral blood flow and peripheral vascular resistance (PVR), which may be a useful predictor of hypertension98.
Angina: Anginal attacks may have underlying disturbances in autonomic nerve activity, which may be monitored by digital plethysmography with auditory stimuli; thus, measurements of autonomic nervous tone by digital plethysmography may be useful in diagnosing angina and monitoring treatment.99.
Autoimmune disease: Digital plethysmography has been used to evaluate cardiovascular function in patients with scleroderma Sjögren syndrome associated spectrum disorders (SSSD), systemic scleroderma (SSc), and systemic lupus erythematosus (SLE)100.
Cardiovascular disease risk assessment: Digital volume pulse (DVP) measured by infrared light photoplethysmography may be used to determine large artery stiffness101. Measurements of pulse wave velocity (PWV), a predictor of cardiovascular disease (CVD) risk, have been obtained with PulseTrace, a fingertip photoplethysmographic device102. DVP has been measured using a PCA 2® photoplethysmographic device (Micro Medical) to calculate arterial stiffness index (SI)65. A dual-channel photoplethysmography system has been used to automatically measure the area under the curve of each DVP in assessing cardiovascular risk103. PWV has been measured using both dual-channel PPG (PWV-DVP) and PWV-applanation tonometry (AT) to record finger-to-toe digital volume pulse; PWV was calculated as the finger-to-toe distance divided by transit time104.
Accelerated plethysmography (APG) uses the second derivative of the photoplethysmograph (SDPTG); fingertip photoplethysmogram and its second derivative (a, b, c, and d wave in systole and an e wave in diastole) have been used simultaneously to record ascending aortic pressure; the ratio of the height of the late systolic peak to that of the early systolic peak in the pulse was defined as the augmentation index, and the second derivative aging index was defined as b-c-d-e/a83. SDPTG has been taken from the cuticle of the left forefinger, and indices (b/a and d/a) were calculated from the wave height105. SDPTG wave components have been used to calculate b/a and d/a ratios and aging index (AGI) and hypertension106. Accelerated plethysmography has been used to determine the prevalence of carotid atherosclerosis and its relation to aging; APG was performed using double-differentiation of the finger plethysmograph recording, and the APG index calculated from the distances between the a, b, c, and d waves107. APG has been performed on seated subjects, and wave patterns were compared to age and other cardiovascular risk factors108.
Critical illness (cardiac monitoring): Critical patients have been continuously monitored using the Nexfin HD system, which noninvasively monitors blood pressure and cardiac output based on pulsatile unloading of finger arterial walls via an inflatable finger cuff.79. However, the potential inaccuracy of PPG in hemodynamically unstable patients may preclude its use as a sole hemodynamic monitoring device in critical care.
Diabetic neuropathy (detection): Photoplethysmography may be an accurate and noninvasive alternative to standard nerve conduction velocity (NCV) testing for diabetic neuropathy, and may be used alongside other screening techniques such as the laser Doppler (LD) and the cold pressor test (CPT). On the index fingers and great toes of the subjects, PPG has measured blood volume changes while LD measured blood perfusion109,110. In a cold pressor test (CPT), digital PPG wave amplitudes have been recorded before and during a one-minute CPT111.
Frostbite (treatment decision aid): In frostbite injury patients, the degree of vascular response after treatment (rapid warming in saline baths) was determined using digital plethysmography and Doppler ultrasound mapping112.
Hemorrhage detection: In a controlled model of hemorrhage, the electrocardiogram (ECG) and the finger infrared photoplethysmogram were simultaneously measured; LVET (p), PTT and R-R interval (RRi) were computed113. Spectral analysis was performed on the finger infrared PPG waveform and on the ECG-derived cardiac beat-to-beat (R-R) intervals during blood donation114.
5
Peripheral vascular disease detection and risk assessment: Toe pressures and pulse wave amplitudes have been taken with digital plethysmographs for diagnosing peripheral vascular disease115,116. The infrared photosensor (IP) transmitter/receiver from the PPG apparatus has been placed on the pulp (pad) of the index finger and great toe117,118. Digital photoplethysmography has been suggested as an alternative to venous ultrasonography for detecting deep vein thrombosis119. Photoplethysmography and continuous wave Doppler (CW-Doppler) in assessing ankle brachial pressure index (ABPI) has been measured computationally via a PPG probe on the index finger and great toe; an 8MHz Doppler probe was used to manually measure ABPI, and statistical analysis was performed using Lin’s correlation coefficient and Bland-Altman plots120. Bilateral PPG has been used in a controlled environment to measure pulse wave timing, amplitude, and shape characteristics for both great toes121. Functional photoplethysmography (fPPG) has been used to acquire pulsatile arterial perfusion by placing an optical probe on the toe for 30 seconds, with the leg in supine position and raised at 45°122. Peripheral blood pulsations have been taken bilaterally from fingers and toes using a novel portable multi-channel PPG123. Pulse wave timing, amplitude and shape characteristics have been obtained simultaneously from both toes and for right-to-left toe differences124. Strain gauge digital plethysmography has been used to measure maximal digital pulse (MDP) on subjects with digital necrosis125.
Preeclampsia (blood pressure monitoring): Standard auscultatory blood pressure measurements have been made in preeclamptic women using the Finometer™ and the SpaceLabs 90207; the results were compared to auscultatory blood pressure measurements according to British Hypertension Society (BHS) and Association for the Advancement of Medical Instrumentation (AAMI) guidelines, and analyzed using Bland-Altman plots and BHS grades; while the SpaceLabs device performed well (consistent with a previous study), the Finometer™ only met AAMI criteria for diastolic blood pressure in normotensive patients76. Thus, the potential inaccuracy of some PPG devices in hemodynamically unstable patients may preclude its use as a sole hemodynamic monitoring device in this type of care.
Raynaud’s phenomenon (interferon-induced) assessment: Digital plethysmography has been a crucial diagnostic tool for this form of Raynaud’s phenomenon126.
Raynaud’s phenomenon (primary) assessment: Digital plethysmography plays an important role in assessing Raynaud’s phenomenon during routine evaluation127,128. An objective test for Raynaud’s syndrome involves immersing one hand in ice water, and hemodynamic variations measured in the contralateral hand using photocell plethysmography129. Cold recovery testing involves immersing one hand in water and cooling from 33°C to 3°C, followed by a 10min recovery period at ambient room temperature of 24°C130. The cooling test has been verified by computerized photoplethysmography of the fingertip plexus131. For cold tests, 11°C has been suggested as the optimal temperature132. Maximum digital pulse (MDP) has been measured using digital plethysmography after immersing hands in 45°C water for three minutes133. Digital plethysmographic signals have been expressed as a ratio to a reference warm amplitude (immersion in 45°C water for three minutes)134. Digital pressures, plethysmography, and digital pressure indices (DPI) have been calculated after cold stimulation at baseline, during, and after the treatment period to evaluate treatment effectiveness for Raynaud’s phenomenon135.
Raynaud’s phenomenon (vibration-induced) assessment: Digital plethysmography has been used to diagnose vibration-induced white finger (VWF), also known as occupational or vibration-induced Raynaud’s phenomenon. Systolic measurements are generally repeatable but may vary depending on the location tested, so recordings should be interpreted with a reference measurement136. For VWF, finger systolic blood pressure (FSBP) has been taken at 21°C and 23°C (±1°C) with a Digimatic® 2000 (Medimatic) strain-gauge plethysmograph137. Digital thermometry and plethysmography have been compared to the reference measurement, Stockholm Workshop Scale (SWS), in assessing hand-arm vibration syndrome (HAVS)138,139. Accelerated plethysmography of the dominant index fingertip has been used to evaluate peripheral circulation in occupational vibration disease140.
Renal disease assessment: Digital photoplethysmography has diagnostic potential for secondary conditions in renal disease, such as arterial stiffness and steal phenomena. Photoplethysmography has been performed on the index finger of either the dominant hand or the nonfistula arm, and computerized pulse curves were obtained; comorbidity was determined with an established index (141). Plethysmography has been used on the index fingers of both hands to determine digital pressures using the VasoGuard Nicolet, 8-MHz (Scimed Ltd, Bristol, UK), and digital pressures obtained by wrapping an inflatable cuff around the proximal phalanx of the index finger and positioning a sensor on the palmar side of the distal phalanx; the ratio of finger pressure to systolic blood pressure was the digital brachial index (DBI)142.
6
Sleep monitoring: Peripheral arterial tonometry (PAT) measures, taken from the fingertip, have been used in ambulatory sleep monitoring95. An automatic algorithm based on PAT has been shown to detect changes in sleep stages143. In sleep apnea patients, changes in finger blood flow have been determined using pulse wave amplitude (PWA) obtained from finger plethysmography144.
Stress: Digital plethysmography appears to detect some (but not all) forms of hemodynamic stress. Photoplethysmographs (PPG) have been measured by oximeter during the Bruce Protocol treadmill test145. A surgical stress index (SSI) has been computed as a combination of normalized heart beat interval (HBI[norm]) and plethysmographic pulse wave amplitude (PPGA[norm]) using the equation SSI=100-(0.7*PPGA[norm]+0.3*HBI[norm]), and validated patients before and during surgery.
Thyroid dysfunction (detection): There is some evidence suggesting that digital photoplethysmography may be used to detect hemodynamic changes caused by thyroid dysfunction. Alterations in finger microcirculation146 and systolic-diastolic index (SDI)147 have been measured in patients with thyroid dysfunction using finger planimetric photoplethysmography.
Vascular reconstruction (operative decision aid): Digital plethysmography is a valuable perioperative decision aid in vascular reconstruction surgeries, and has been used since at least the 1950s to monitor surgery of degenerative arterial disease148. Digital plethysmography has been used to detect non-reversal of flow, abnormal digital pressure, and inappropriate ulnar velocity increases in radial arteries during assessments for coronary artery bypass grafting (CABG)149. In 10 cases of ulnar artery aneurysm in nine male patients from 1978 to 1988, intraoperative digital plethysmography was useful in determining the necessity for microvascular reconstruction150.
Adverse Effects/Precautions/ContraindicationsAllergy: Insufficient evidence.
Adverse Effects/Post-Market SurveillanceGeneral: Digital plethysmography is generally regarded as a noninvasive hemodynamic monitoring technique. In a clinical trial using the cold face test (which involves digital plethysmographic monitoring of the finger and toe), subjects did not find the test to be “obnoxious”151.
Precautions/Warnings/Contraindications:Use cautiously in critical settings or in hemodynamically unstable patients, such as cardiac disease patients. Although the noninvasive nature of digital plethysmography makes it an attractive method for monitoring cardiac parameters in critically ill patients, its potential inaccuracy in hemodynamically unstable patients may preclude its use as a sole hemodynamic monitoring device in critical care79 or in cardiac disease patients80.
Use cautiously in pregnant women, as some digital plethysmographic devices may not be sufficient for measuring absolute blood pressure in pregnant women (particularly for hypertensive or preeclamptic pregnant women)76,77.
Pregnancy & Lactation:Digital plethysmography is a noninvasive technique that has been used in pregnant women to determine arterial stiffness indices152; however, the accuracy of some digital plethysmographic devices may not be sufficient for measuring absolute blood pressure in pregnant women, particularly those who are hypertensive or preeclamptic76,77.
7
Interactions
Procedure/Drug Interactions:ACE inhibitors: Finger pulse plethysmography has been used to study the circulatory effects induced by captopril and isosorbide dinitrate (ISDN), alone and in combination153. The effects of enalapril on blood vessels may be monitored by finger photoplethysmography (FPPG154. The angiotensin-I pressor response, as measured by photoplethysmographic finger blood pressure monitoring, was blocked by enalapril155.
Alpha agonists: Pulse-wave transit time (PWTT) (determined by ECG R-wave and finger pulse measured by photoplethysmographic finger probe) are affected by norepinephrine156. The effects of clonidine on digital vasculature have been analyzed using infrared light transmitted through a finger157. Similarly, vasoconstriction induced by methoxamine may be measured using strain gauge plethysmography, though this technique may underestimate oscillometric measurement158.
Alpha blockers: Tamsulosin-induced hemodynamic changes in patients with benign prostatic enlargement have been measured with finger plethysmography159. Finger blood flow measured by venous occlusion plethysmography has been shown to increase significantly with indoramin administration160.
Anesthetics: Sympatholytic and vasoconstrictive hemodynamic effects of anesthesia, including dexmedetomidine161, bupivacaine162,163, and general anesthesia may be detected by infrared light transmitted through the finger.
Angiotensin II: Pulse-wave transit time (determined by ECG R-wave and finger pulse measured by photoplethysmographic finger probe) is affected by angiotensin II156.
Angiotensin receptor II antagonists: The angiotensin-I pressor response, as measured by photoplethysmographic finger blood pressure monitoring, was blocked similarly by enalapril and the novel angiotensin receptor antagonist UP269-6155. Arterial compliance parameters measured by finger plethysmographic arterial pulse curves have been shown to be affected by losartan independently of blood pressure164. Losartan has been shown to reduce baroreflex sensitivity (BRS), blood pressure, and heart rate variability (HRV) as measured by servo-controlled infrared finger plethysmography165.
Antidiuretic agents: Finger and forehead plethysmographic signals have been found to be unaffected by arginine vasopressin, though ear plethysmographic signals decreased significantly166.
Antilipemic and antithrombotic agents: The effects of pyridinolcarbamate on atherosclerosis obliterans have been monitored by toe plethysmography167.
Antiulcer agents: An acute dose of misoprostol, a PGE1 analog with antiulcer activity, has not been shown to have clinically significant hemodynamic effects measured by light reflex finger plethysmography168.
Beta agonists: Pulse-wave transit time (determined by ECG R-wave and finger pulse measured by photoplethysmographic finger probe) is affected by salbutamol156.
Beta blockers: Peripheral circulation (measured by digital plethysmography) does not appear to be affected by metoprolol169, atenolol, labetalol, or propranolol170, suggesting that beta blockers are not contraindicated in patients with reduced peripheral circulation (such as Raynaud’s phenomenon). Atenolol has also shown lack of response by piezoelectric finger plethysmography, whereas nebivolol improved parameters of endothelial function171. In undisturbed subjects, pindolol has been shown to abolish the decrease D/H ratio of the digital plethysmographic pulse wave (with D representing the depth of the dicrotic minimum to the apex of the systolic maximum, and H representing the total height of the plethysmographic wave)172. Atenolol has been shown to reduce baroreflex sensitivity (BRS), blood pressure, and heart rate variability (HRV) as measured by servo-controlled infrared finger plethysmography165. Combination therapy with atenolol and flunarizine has been shown to significantly increase the photoplethysmographic wave amplitude in patients with Raynaud’s disease173. Digital arterial pressure (measured by plethysmography) is elevated in hypertensive patients and does not appear to vary when treated with metoprolol or propranolol; digital arterial tone also does not appear to be affected by metoprolol, but was shown to intensify with propranolol treatment174.
Calcium channel blockers: Combination therapy with atenolol and flunarizine has been shown to significantly increase the photoplethysmographic wave amplitude in patients with Raynaud’s disease173. Peripheral hemodynamic reflex
8
responses, measured by electrocardiograph-triggered venous occlusion plethysmography of the finger, were attenuated by isradipine175. Cold exposure finger plethysmography has been used to optimize felodipine treatment in patients with Raynaud’s phenomenon176. Venous occlusion plethysmography has suggested nifedipine retard has been suggested to be an ineffective treatment for Raynaud’s phenomenon by assessing digital blood flow by venous occlusion plethysmography177.
Glucocorticoids: Dexamethasone did not have any significant effect on cerebral autoregulation index (ARI) calculated from digital plethysmographic blood pressures in a study evaluating the pharmacological prevention of high altitude pulmonary edema178.
Narcotics: Large-amplitude low-frequency changes in digital plethysmographic measurements have been observed in patients receiving morphine for postoperative analgesia179.
Sedatives: The hemodynamic effects of the sedative haloperidol may be detected by digital plethysmography180.
Serotonergic agents: Dihydroergotamine has been shown to abolish the decrease D/H ratio of the digital plethysmographic pulse wave in undisturbed subjects172. The serotonergic receptor antagonist ketanserin has been shown to paradoxically reduce finger systolic blood pressure and fingertip temperatures (as measured by digital plethysmography) in Raynaud’s phenomenon patients in response to body warming181.
Vasodilators: Digital plethysmography has long been used to clinically to assess the hemodynamic effects of vasodilative drugs182. Digital plethysmography is often used to study the pharmacodynamics and pharmacokinetics of isoxsuprine183 and glyceryl trinitrate (GTN), also known as nitroglycerin156,184-198. Other nitric oxide-generating agents, such as sodium nitrite199 and sildenafil159, have also been studied with digital plethysmography. L-arginine, which increases nitric oxide (NO) production, has been shown to increase blood flow after infusion200 and may affect digital plethysmographic readings. Vasoactive drugs affect the second derivative (a, b, c, and d wave in systole and an e wave in diastole) of the fingertip photoplethysmogram; the ratio of the height of the d wave to that of the a wave (d/a) decreased after angiotensin, and nitroglycerin increased d/a83. Tadalafil did not have any significant effect on cerebral autoregulation index (ARI) calculated from digital plethysmographic blood pressures in a study evaluating the pharmacological prevention of high altitude pulmonary edema178.
Procedure/Herb/Supplement Interactions:Caffeine: Caffeine may reduce arterial compliance and increase systolic, diastolic, and mean blood pressure values as measured by digital plethysmography201.
Folic acid: Daily supplementation with 1,000mg vitamin C, 800mg vitamin E, and 10mg folic acid for 12 weeks has been shown to significantly decrease systolic blood pressure measured by digital plethysmography201. Folic acid may improve measures of large artery stiffness and hypertension, and changes may be reflected in digital plethysmographs202.
L-arginine: L-arginine, which increases nitric oxide (NO) production, has been shown to increase blood flow after infusion200 and may affect digital plethysmographic readings.
Vitamin C: Daily supplementation with 1,000mg vitamin C, 800mg vitamin E, and 10mg folic acid for 12 weeks has been shown to significantly decrease systolic blood pressure measured by digital plethysmography201.
Vitamin E: Daily supplementation with 1,000mg vitamin C, 800mg vitamin E, and 10mg folic acid for 12 weeks has been shown to significantly decrease systolic blood pressure measured by digital plethysmography201.
Procedure/Food Interactions:Dietary sources of nitrites and nitrates (such as fruits, green leafy vegetables, and cured meats) may influence cardiovascular parameters through production of nitric oxide (NO)203, which may in turn affect digital plethysmographic readings.
The effects of alcohol on circulation and blood pressure may be reflected in digital plethysmographic readings204.
Procedure/Lab Interactions:Patients determined by urodynamic tests to have atronic bladders may show reduced baroreflex sensitivity by plethysmographic techniques205.
9
Mechanism of Action
Scientific ResearchArterial stiffness measurements: Arterial stiffness, a major cardiovascular disease (CVD) risk parameter, is reflected by the pulse wave velocity (PWV) derived from digital volume pulse (DVP)63. DVP measured by digital plethysmography has been shown to be a reliable and reproducible technique for indirectly determining arterial stiffness indices (SI)65. Digital plethysmography has been used to measure arterial stiffness indices (SI) in numerous populations, including preeclamptic women using the Pulse Trace System™ digital plethysmograph (Micro Medical Ltd., Gillingham, Kent, UK) and found SI to be significantly higher in preeclamptic women than normotensive women152.
Blood flow measurements: Digital plethysmography measures pulsation and blood flow by occlusion and perfusion pressure206. Digital plethysmography has been proposed as a reliable alternative to the established Allen’s test for measuring blood flow to the hand66.
Blood hemoglobin measurements: Blood hemoglobin levels may be measured indirectly with digital photoplethysmography, which involves transmission of near-infrared light (905±10nm) through a finger. The ratio of pulsatile changes in light attenuation across a body part to light path length correlates strongly to hemoglobin levels measured by Coulter Counter®; although it has wide variability, digital plethysmography may, with further development, become a viable and noninvasive alternative to phlebotomy for measuring blood hemoglobin207.
Blood pressure measurements: Digital plethysmographic devices may detect small acute and long-term changes in blood pressure induced by caffeine and vitamin intake201. Digital plethysmography has been used to measure hemodynamic changes during head-up tilt testing, which may have prognostic value for orthostatic hypotension (OH)71,72. For measuring blood pressure variability, the newer Finometer™ device has been compared with the traditional Finapres® as well as the more invasive intra-arterial method for making blood pressure recordings80. Both the Finometer™ and the Finapres® overestimated variability of systolic pressure in the very low frequency (0.01-0.04Hz) and low frequency (0.04-0.15Hz) bands (p<0.01), with percentage median errors of 130% and 103%, respectively, for the Finometer™ very low and low frequency bands, and median errors of 134% and 78%, respectively, for the Finapres®. Both devices also underestimated baroreflex sensitivity (BRS) (-31% for the Finometer™, -24% for Finapres®). The Finometer™ showed poorer accuracy in blood pressure variability measurements than Finapres® in cardiac disease patients. Thus, these instruments may not be recommendable as sole monitoring devices for cardiac disease patients.
Nexfin noninvasive arterial pressure (NAP) measurement, which uses the Finapres® finger plethysmographic methodology, has been found to be accurate when compared to indirect blood pressure measurements using the auscultatory Riva-Rocci/Korotkoff method208.
The Finometer™ (FMS, Finapres® Measurement Systems, Arnhem, Netherlands), which is successor of the Finapres® (TNO Biomedical Instrumentation, Amsterdam, Netherlands), has been validated according to the revised British Hypertension Society (BHS) protocol and the criteria of the Association for the Advancement of Medical Instrumentation (AAMI) for making noninvasive finger blood pressure measurements and waveform measurements comparable to intra-arterial recordings209. It has thus been recommended for clinical and research purposes.
Brachial artery pressure measurements: Digital and brachial pressure (BAP) measurements have been found to correlate strongly in pulse wave analysis (PWA)210.
Finger arterial pressure has been used to estimate brachial artery pressure in patients after cardiac catheterization; after waveform filtering, level correction, and supine return-to-flow calibration, all pressure differences met the requirements of Association for the Advancement of Medical Instrumentation211.
Guelen et al. conducted a clinical trial to evaluate three methods for reconstructing brachial pressure (BAP) from non-invasive finger arterial pressure (FinAP) measurements212. The study was conducted on 37 subjects (41-83 years of age) after cardiac catheterization. The study utilized the Finometer™ (FMS, Finapres® Measurement Systems, Arnhem, Netherlands), the successor to the Finapres® (TNO Biomedical Instrumentation, Amsterdam, Netherlands). FinAP and BAP were recorded simultaneously; pulse shape variations between FinAP and BAP were removed with a generalized waveform filter, and pressure level variations were corrected with either a generalized correction equation or a level
10
calibration, which uses a return-to-flow (RTF) measurement as an additional parameter. After they were corrected and filtered, FinAP measurements were compared to BAP. The variation from BAP was -9.7±13.0mmHg for systolic pressure, -11.6±8.0mmHg for diastolic pressure, and -16.3±7.9mmHg for mean pressure. Filtered and level-corrected arterial pressure (flcAP) differed by -1.1±10.7mmHg, -0.2±6.8mmHg and -1.5±6.6mmHg; reBAP differed by 3.1±7.6mmHg, 4.0±5.6mmHg and 2.7±4.7mmHg. These techniques reduced the variability between FinAP and BAP, and may help optimize RTF calibration to meet AAMI requirements.
Cardiac output measurements: Pulse pressure profiles recorded with digital plethysmography do not accurately predict cardiac output (CO) (Q, L/min) and must be corrected with a previously calculated calibration factor by an independent measure of CO213.
Cold hyperreactivity measurements: Digital plethysmography has been used to measure arterial cold hyperreactivity in Raynaud’s phenomenon206.
Critical closing pressure (CrCP) measurements: The relative change in CrCP induced by hemodynamic challenges is a relevant indicator of cerebrovascular regulation, and may be recorded reliably using digital plethysmography or by applanatory tonometry214.
Digital plethysmography to measure left ventricular ejection time215, and continuous blood pressure monitoring has been used to optimize atrioventricular delay for cardiac resynchronization therapy216.
Drug-induced physiological responses: Digital photoplethysmography has been used to study the pharmacodynamics and pharmacokinetics of a number of drugs, including angiotensin83, angiotensin II156, antimigraine drugs158, arginine vasopressin166, atenolol165,170,171,173 bupivacaine162,163, caffeine201, captopril153, clonidine157, dexamethasone178, dexmedetomidine161, dihydroergotamine172, enalapril154,155, felodipine176, flunarizine173, general anesthesia (propofol-alfentanil-nitrous oxide)161, glyceryl trinitrate (nitroglycerin)83,156,184-198, haloperidol,180, indoramin160, isosorbide dinitrate (ISDN)153, isoxsuprine183, isradipine175, ketanserin181, labetalol170, losartan164,165, methoxamine158, metoprolol174,217, misoprostol168, morphine179, nebivolol171, nifedipine176,218, nifedipine retard177, nitroglycerin ointment169, norepinephrine156, pindolol172, propranolol170,174,217, pyridinolcarbamate167, salbutamol156, sildenafil159, spironolactone219,220, tadalafil178, tamsulosin159, UP269-6155, and various vasodilators182,199.
Digital plethysmography has also been used to assess hemodynamic parameters in acute mountain sickness, an early stage of high altitude cerebral edema178.
Heart rate variability (HRV) assessments: Digital plethysmography has been used to measure various factors that may affect HRV, such as circadian and nocturnal parasympathetic activity221, age222-229, and gender222,225.
Fingertip photoplethysmography (FPPG) has been reported to reliably estimate heart rate variability (HRV, with accuracy approaching that of electrocardiography (ECG)230.
Giardino et al. conducted an equivalence study comparing finger plethysmography (FP) to ECG for accurate heart rate variability (HRV) calculations231. In 10 healthy subjects, ECG and finger plethysmography were used simultaneously with the subjects at rest and during the Stroop color word test. Consistent with the previous study, band variances for high and low frequency HRV were highly correlated between finger plethysmography and ECG, and HRV readings were significantly higher with FP. However, the correlation between finger plethysmography and ECG diminished during the Stroop talk. These results suggest that finger plethysmography may be sufficient for measuring HRV at rest, but ECG may be more reliable for experimental purposes. Moreover, test-retest reliability remains uncertain. In a separate experiment, Giardino et al. conducted an equivalence study comparing finger plethysmography to ECG for accurate HRV calculations231. In 16 healthy subjects at rest, ECG and FP were used simultaneously. Band variances for high and low frequency HRV were highly correlated between finger plethysmography and ECG, and HRV readings were significantly higher with finger plethysmography. These results suggest that FP may be sufficient for measuring HRV at rest. However, test-retest reliability remains uncertain.
Theorell et al. conducted an equivalence study to evaluate noninvasive techniques, ultralow frequency ballistocardiography (UFB) and digital pulse plethysmography, for assessing heart rate and atrial activity in cardiac pacing232. UFB measured the force of contraction of the left ventricle (IJ amplitude) and digital pulse plethysmography measured relative changes in the peripheral pulse volume. Six patients with external artificial pacemakers were included in the study; in four patients,
11
measurements were made at 40, 50, 60, 70, 80, 90 and 100 beats per minute (bpm). LJ and pulse amplitudes decreased significantly when heart rate increased from 40 to 100bpm (p<0.001). Relative IJ and pulse amplitude were positively correlated in all subjects studied. On the ECG, PR interval for IG and pulse amplitudes varied between patients, as shown by beat-to-beat analysis. These results suggest that UFB and digital photoplethysmography may be useful for selecting optimal pacemakers for patients with slow heart rate.
In peripheral vascular disorders, the pulsatile curve is altered; in obstructive arteriopathy, the curve is delayed and flattened206.
Butter et al. conducted an equivalence case series to test finger photoplethysmography (FPPG) as a noninvasive method for optimizing cardiac resynchronization therapy (CRT) in heart failure patients233. In 57 heart failure patients, finger photoplethysmography and invasive aortic pressure measurements were taken concurrently. Data were collected at baseline and during intrinsic rhythm alternating with pacing at 4-5 AV delays. Data were corrected for artifacts, and responses (median percentage) were compared to baseline and recorded as positive, negative, or neutral using the Wilcoxon rank test. Aortic pulse pressure responses were identified using finger photoplethysmography with a 71% sensitivity (95% CI: 60-80%) and 90% specificity (95% CI: 84-94%); negative responses were recorded with 57% sensitivity (95% CI: 44-69%) and 96% specificity (95% CI: 91-98%). finger photoplethysmography change magnitudes were somewhat more strongly correlated with aortic pulse pressure changes (R-squared=0.73, p<0.0001) than with negative changes (R-squared=0.43, p<0.0001). In 78% of patients, finger photoplethysmography correctly identified positive aortic pressure changes to CRT. This suggests that the simple and noninvasive finger photoplethysmography technique may accurately identify aortic pulse pressure changes during CRT.
Motion sickness assessments: A method using digital photoplethysmography has been developed for evaluating the effects of visually-induced motion sickness (234). Further studies may determine whether this technique may be utilized in clinical or research settings.
Neurovascular measurements: Matoba et al. used digital plethysmography to clarify the functional conditions of the autonomic nervous system in vibration disease235, also known as vibration-induced Raynaud’s phenomenon or occupational Raynaud’s syndrome. In 15 healthy men, auditory stimuli caused rapid decreases in plethysmographic amplitudes, which recovered to normal values after 30 seconds. In subjects with vibration disease, the recovery was delayed. The results suggested that changes in the autonomic nervous system occur in vibration disease, and that digital plethysmography with auditory stimuli may be useful in detecting these changes.
Pulse wave velocity (PWV) and pulse wave transit time (PTT) measurements: PWV derived from the finger has a repeatability coefficient percentage (RC%) of 5-7%, which is comparable to PWV derived from the brain (RC% of 5-7) and more reliable than PWV derived from the ear (RC% 8-18). Digital PWV is also more repeatable that PWV from the brain or ear (RC% 10.7-12.1, 14.7-19.5, and 8.3-15, respectively)236.
Loukogeorgakis et al. conducted an equivalence study comparing photoplethysmography (PPG) with Doppler and intra-arterial measurements for measuring arterial pulse wave transit time (PTT) and pulse wave velocity (PWV)237. Photoplethysmographic pulse wave delay time, or the interval between the ECG-R wave and the foot of the arterial pulse, was compared to measures taken using the established Doppler ultrasound. In 17 subjects, aortic pulse wave delay time was measured with the noninvasive photoplethysmography technique and compared to values obtained using invasive intra-arterial pressure wave. Finally, repeatability measurements of PWV were made on the subjects. There was good correlation between all techniques (photoplethysmography, Doppler, and intra-arterial measurements), with repeatability at short timescales in good agreement (CV<6% for all sites measured). At longer timescales, the correlation was satisfactory in the aorta (CV=6.3), arm (CV=13.1), and leg (CV=16.0). PWV values were consistent with previously published reports. These results support the use of photoplethysmography as a complement to other methods, especially in large-scale epidemiological studies in which the simplicity and ease of use may be particularly valuable.
Vasodilation monitoring: Finger photoplethysmography has been used for monitoring of vasodilation caused by reactive hyperemia.238
12
HistoryPlethysmography has been used since the late 1800s to measure pharmacological effects of drugs, primarily the vasodilating effects of organic nitrates239.
The photoplethysmograph (PPG) waveform was first examined in the 1930s; however, it was not until the 1980s that this waveform gained widespread use in clinical research and practice. photoplethysmography is now integrated into routine clinical practice69.
Digital (finger or toe) photoplethysmography was developed in the 1980s, and presented a noninvasive technique for continuously measuring hemodynamic parameters in research and clinical settings. Digital photoplethysmography may be used alongside established measurements of hemodynamic parameters240. A commonly used photoplethysmographic technology is the Finapres® (an acronym for FINger Arterial PRESsure); ongoing studies aim to improve the diagnostic precision of this and other digital photoplethysmography devices (241;242). Several studies have also been conducted using the WatchPAT100 device, which is a portable finger plethysmographic device based on peripheral arterial tone (PAT) coupled to a constant volume, variable pressure, pneumatic system95.
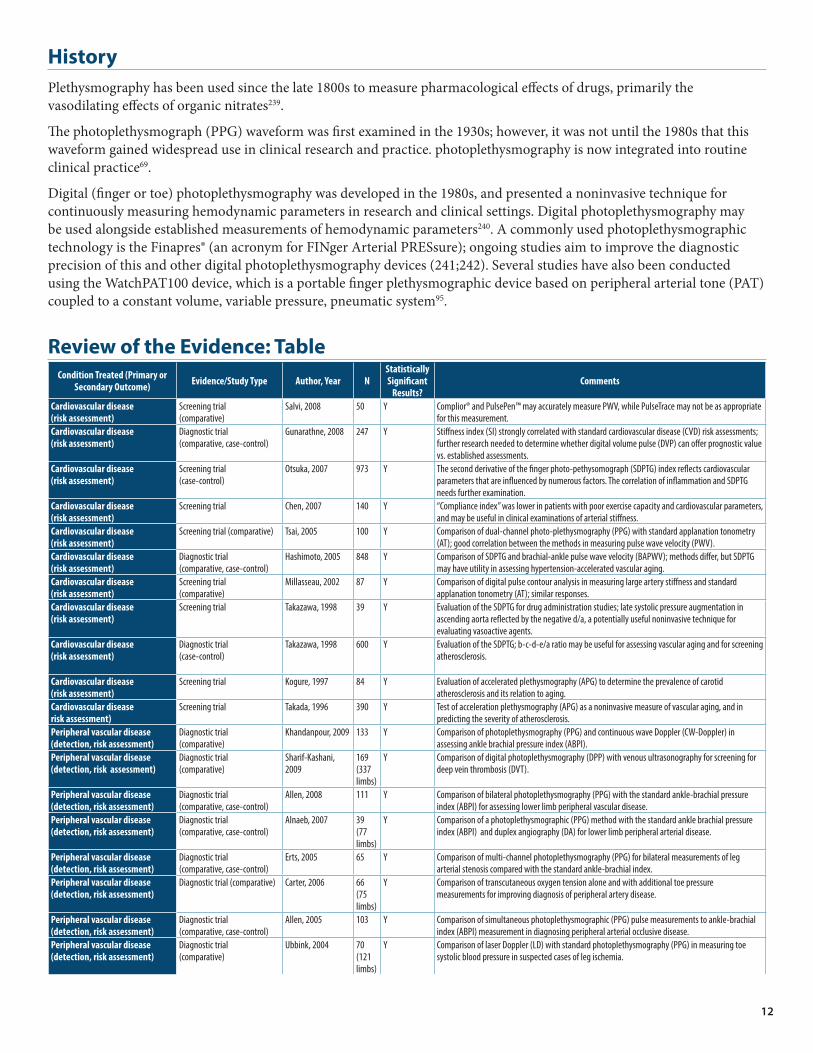
Review of the Evidence: TableCondition Treated (Primary or
Secondary Outcome) Evidence/Study Type Author, Year NStatistically Significant
Results?Comments
Cardiovascular disease (risk assessment)
Screening trial (comparative)
Salvi, 2008 50 Y Complior® and PulsePen™ may accurately measure PWV, while PulseTrace may not be as appropriate for this measurement.
Cardiovascular disease (risk assessment)
Diagnostic trial (comparative, case-control)
Gunarathne, 2008 247 Y Stiffness index (SI) strongly correlated with standard cardiovascular disease (CVD) risk assessments; further research needed to determine whether digital volume pulse (DVP) can offer prognostic value vs. established assessments.
Cardiovascular disease (risk assessment)
Screening trial (case-control)
Otsuka, 2007 973 Y The second derivative of the finger photo-pethysomograph (SDPTG) index reflects cardiovascular parameters that are influenced by numerous factors. The correlation of inflammation and SDPTG needs further examination.
Cardiovascular disease (risk assessment)
Screening trial Chen, 2007 140 Y “Compliance index” was lower in patients with poor exercise capacity and cardiovascular parameters, and may be useful in clinical examinations of arterial stiffness.
Cardiovascular disease (risk assessment)
Screening trial (comparative) Tsai, 2005 100 Y Comparison of dual-channel photo-plethysmography (PPG) with standard applanation tonometry (AT); good correlation between the methods in measuring pulse wave velocity (PWV).
Cardiovascular disease (risk assessment)
Diagnostic trial (comparative, case-control)
Hashimoto, 2005 848 Y Comparison of SDPTG and brachial-ankle pulse wave velocity (BAPWV); methods differ, but SDPTG may have utility in assessing hypertension-accelerated vascular aging.
Cardiovascular disease (risk assessment)
Screening trial (comparative)
Millasseau, 2002 87 Y Comparison of digital pulse contour analysis in measuring large artery stiffness and standard applanation tonometry (AT); similar responses.
Cardiovascular disease (risk assessment)
Screening trial Takazawa, 1998 39 Y Evaluation of the SDPTG for drug administration studies; late systolic pressure augmentation in ascending aorta reflected by the negative d/a, a potentially useful noninvasive technique for evaluating vasoactive agents.
Cardiovascular disease (risk assessment)
Diagnostic trial (case-control)
Takazawa, 1998 600 Y Evaluation of the SDPTG; b-c-d-e/a ratio may be useful for assessing vascular aging and for screening atherosclerosis.
Cardiovascular disease (risk assessment)
Screening trial Kogure, 1997 84 Y Evaluation of accelerated plethysmography (APG) to determine the prevalence of carotid atherosclerosis and its relation to aging.
Cardiovascular disease risk assessment)
Screening trial Takada, 1996 390 Y Test of acceleration plethysmography (APG) as a noninvasive measure of vascular aging, and in predicting the severity of atherosclerosis.
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative)
Khandanpour, 2009 133 Y Comparison of photoplethysmography (PPG) and continuous wave Doppler (CW-Doppler) in assessing ankle brachial pressure index (ABPI).
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative)
Sharif-Kashani, 2009
169 (337 limbs)
Y Comparison of digital photoplethysmography (DPP) with venous ultrasonography for screening for deep vein thrombosis (DVT).
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative, case-control)
Allen, 2008 111 Y Comparison of bilateral photoplethysmography (PPG) with the standard ankle-brachial pressure index (ABPI) for assessing lower limb peripheral vascular disease.
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative, case-control)
Alnaeb, 2007 39(77 limbs)
Y Comparison of a photoplethysmographic (PPG) method with the standard ankle brachial pressure index (ABPI) and duplex angiography (DA) for lower limb peripheral arterial disease.
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative, case-control)
Erts, 2005 65 Y Comparison of multi-channel photoplethysmography (PPG) for bilateral measurements of leg arterial stenosis compared with the standard ankle-brachial index.
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative) Carter, 2006 66(75 limbs)
Y Comparison of transcutaneous oxygen tension alone and with additional toe pressure measurements for improving diagnosis of peripheral artery disease.
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative, case-control)
Allen, 2005 103 Y Comparison of simultaneous photoplethysmographic (PPG) pulse measurements to ankle-brachial index (ABPI) measurement in diagnosing peripheral arterial occlusive disease.
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative)
Ubbink, 2004 70 (121 limbs)
Y Comparison of laser Doppler (LD) with standard photoplethysmography (PPG) in measuring toe systolic blood pressure in suspected cases of leg ischemia.

13
Condition Treated (Primary or Secondary Outcome) Evidence/Study Type Author, Year N
Statistically Significant
Results?Comments
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative, case-control)
Sadiq, 2001 181 limbs
Y Validation of photoplethysmography (PPG) in detecting flow and systolic arterial pressures compared to the standard continuous wave (CW) Doppler method.
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative)
Whiteley, 1998 32 (52 limbs)
Y Comparison of photoplethysmography (PPG) to hand-held Doppler and sphygmomanometer in measuring ankle/brachial pressure index (ABPI).
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial Planchon, 1987 10 Y Evaluation of stain gauge digital plethysmography as a diagnostic and prognostic test in digital arteriopathies.
Peripheral vascular disease (detection, risk assessment)
Diagnostic trial (comparative, case series)
Becker, 1985 1,000 limbs
Y Evaluation of Doppler, tetrapolar rheography, digital plethysmography, and transcutaneous measure of PO2 (Tc PO2) for measuring occlusive arterial disease.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (comparative, case-control)
Dyszkiewicz, 2006 169 Y Evaluation of a cooling test verified by computerized finger photoplethysmography (FPPG) for diagnosing vibration-induced Raynaud’s phenomenon.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (case-control, multicenter)
Nasu, 2008 289 N Evaluation of finger plethysmography after segmental cooling for vibration-induced white finger (VWF). Results did not support this use.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (comparative, cross-sectional)
Thompson, 2008 139 Y Correlation of finger thermometry and finger plethysmography with Stockholm Workshop Scale (SWS) in assessing hand-arm vibration syndrome (HAVS).
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (comparative, cross-sectional)
Thompson, 2007 139 Y Correlation between objective cold provocation tests (thermography and finger plethysmography) and Stockholm Workshop Scale (SWS) in hand-arm vibration syndrome (HAVS).
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (case review)
Schapira, 2002 24 NA Digital plethysmography, arteriography, and capillaroscopy were all central to diagnosis of interferon-induced Raynaud’s phenomenon.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (case-control)
Martinez, 1999 55 Y Evaluation of plethysmography and digital pressure indices (DPI) in assessing treatment effectiveness.
Raynaud’s phenomenon (detection and assessment)
Screening trial Miyashita, 1995 815 Y Study to establish accelerated plethysmography (APG) for evaluating occupational vibration disease.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (comparative)
Suiches, 1992 18 Y Comparison of digital photoelectrical plethysmography (PhEP) and laser Doppler flowmetry (LDF) for testing Raynaud’s phenomenon severity.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (comparative)
Maisonneuve, 1991)
104 Y Capillaroscopy and digital plethysmography were useful in diagnosing true Raynaud’s syndrome secondary to thoracic outlet syndrome (TOS); arterial Doppler was more reliable in distinguishing symptomatic and asymptomatic sides in the same patient.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (comparative)
Laroche, 1987 365 Y Comparison of digital plethysmography and the digital temperature recovery test to clinical evaluation in diagnosing Raynaud’s phenomenon.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (case-control)
de Faucal, 1986 69 Y Evaluation of digital plethysmography for studying rheological and hemodynamic parameters of vascular disorders, including Raynaud’s phenomenon.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (case-control)
Planchon, 1986 131 Y Evaluation of a vascular reactivity cold test using mercury strain gauge plethysmography.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (case review)
Zweifler, 1984 147 Y Retrospective study to determine the relationship between occlusive digital artery disease and systemic illness in patients with Raynaud’s phenomenon based on digital plethysmographic findings.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (case-control)
Samueloff, 1981 P Y Evaluation of an objective test for Raynaud’s syndrome using photocell plethysmography.
Raynaud’s phenomenon (detection and assessment)
Diagnostic trial (case-control)
Woulda, 1977 92 Y Evaluation of the cooling and warm-up test, which uses photoelectric plethysmography of the fingers, for assessing Raynaud’s phenomenon.
Sleep apnea (screening and diagnosis)
Diagnostic trial (nonrandomized, single-blind comparison study)
Pang, 2007 37 Yes Compared digital plethysmography with WatchPAT100 device with standard polysomnography in patients with suspected sleep apnea
Sleep apnea (screening and diagnosis)
Diagnostic trial (case-control comparison study)
Herscovici, 2007 60 Yes Compared digital plethysmography with WatchPAT100 device with standard polysomnography in patients with suspected sleep apnea vs. subjects in a validation set.
Sleep apnea (screening and diagnosis)
Screening trial (cohort study)
Zou, 2006 98 Yes Compared digital plethysmography with WatchPAT100 device with standard polysomnography in a population-based cohort.
Sleep apnea (screening and diagnosis)
Diagnostic trial (case control comparison study)
Hedner, 2004 228 Yes Compared digital plethysmography with WatchPAT100 device with standard polysomnography in patients with sleep apnea vs. normal patients.
Sleep apnea (screening and diagnosis)
Screening trial (monitoring)
Grote, 2003 44 Yes Tested finger plethysmography as a method for monitoring finger blood flow in sleep apnea.
Sleep apnea (screening and diagnosis)
Diagnostic trial (case-control comparison study))
Ayas, 2003 30 Yes Compared digital plethysmography with WatchPAT100 device with standard polysomnography in patients with suspected sleep apnea vs. normal patients.
Sleep apnea (screening and diagnosis)
Diagnostic trial (case-control comparison study)
Bar, 2003 102 Yes Compared digital plethysmography with WatchPAT100 device with standard polysomnography in patients with sleep apnea vs. normal patients.
Sleep apnea (screening and diagnosis)
Diagnostic trial (comparison study)
Schnall, 1999 42 Yes Compared digital plethysmography with WatchPAT100 device with standard polysomnography in patients with sleep apnea.
Diabetic neuropathy (detection)
Screening trial (case-control)
Jaryal, 2009 21 Y Used photoplethysmographic (PPG) readings during the cold pressor test (CPT) to monitor vascular reactivity in control and diabetic patients.
Diabetic neuropathy (detection) Diagnostic trial (comparative, case-control)
Kim, 2008 125 Y Compared a screening method for diabetic neuropathy using laser Doppler (LD) and digital photoplethysmography (D-PPG) with the standard nerve conduction velocity (NCV) test.
Diabetic neuropathy (detection) Diagnostic trial (comparative, case-control)
Kim, 2007 P Y Compared a screening method for diabetic neuropathy using laser Doppler (LD) and digital photoplethysmography (PPG) with the standard nerve conduction velocity (NCV) test.
Thyroid dysfunction (detection) Diagnostic trial (case-control)
Dyszkiewicz, 2007 66 Y Evaluated alterations in finger microcirculation and systolic-diastolic index (SDI) in hypothyroidism using finger planimetric photoplethysmography.
14
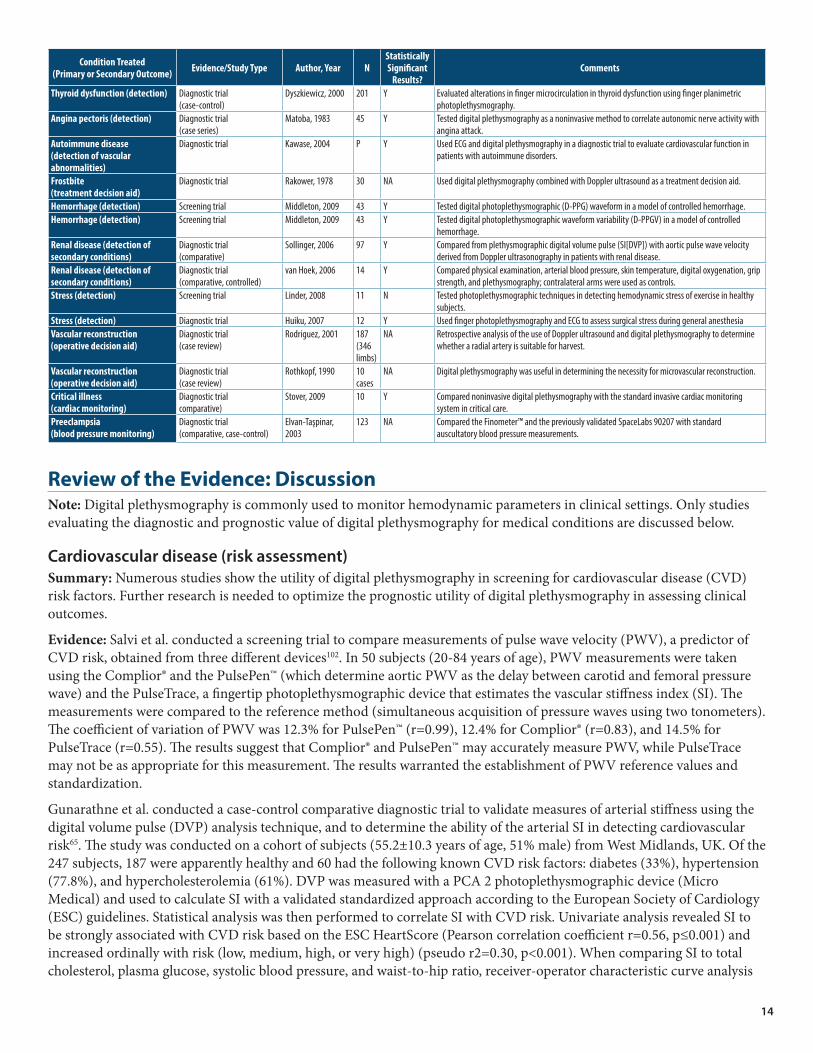
Condition Treated (Primary or Secondary Outcome) Evidence/Study Type Author, Year N
Statistically Significant
Results?Comments
Thyroid dysfunction (detection) Diagnostic trial (case-control)
Dyszkiewicz, 2000 201 Y Evaluated alterations in finger microcirculation in thyroid dysfunction using finger planimetric photoplethysmography.
Angina pectoris (detection) Diagnostic trial (case series)
Matoba, 1983 45 Y Tested digital plethysmography as a noninvasive method to correlate autonomic nerve activity with angina attack.
Autoimmune disease (detection of vascular abnormalities)
Diagnostic trial Kawase, 2004 P Y Used ECG and digital plethysmography in a diagnostic trial to evaluate cardiovascular function in patients with autoimmune disorders.
Frostbite (treatment decision aid)
Diagnostic trial Rakower, 1978 30 NA Used digital plethysmography combined with Doppler ultrasound as a treatment decision aid.
Hemorrhage (detection) Screening trial Middleton, 2009 43 Y Tested digital photoplethysmographic (D-PPG) waveform in a model of controlled hemorrhage.Hemorrhage (detection) Screening trial Middleton, 2009 43 Y Tested digital photoplethysmographic waveform variability (D-PPGV) in a model of controlled
hemorrhage.Renal disease (detection of secondary conditions)
Diagnostic trial (comparative)
Sollinger, 2006 97 Y Compared from plethysmographic digital volume pulse (SI[DVP]) with aortic pulse wave velocity derived from Doppler ultrasonography in patients with renal disease.
Renal disease (detection of secondary conditions)
Diagnostic trial (comparative, controlled)
van Hoek, 2006 14 Y Compared physical examination, arterial blood pressure, skin temperature, digital oxygenation, grip strength, and plethysmography; contralateral arms were used as controls.
Stress (detection) Screening trial Linder, 2008 11 N Tested photoplethysmographic techniques in detecting hemodynamic stress of exercise in healthy subjects.
Stress (detection) Diagnostic trial Huiku, 2007 12 Y Used finger photoplethysmography and ECG to assess surgical stress during general anesthesiaVascular reconstruction (operative decision aid)
Diagnostic trial (case review)
Rodriguez, 2001 187 (346 limbs)
NA Retrospective analysis of the use of Doppler ultrasound and digital plethysmography to determine whether a radial artery is suitable for harvest.
Vascular reconstruction (operative decision aid)
Diagnostic trial (case review)
Rothkopf, 1990 10 cases
NA Digital plethysmography was useful in determining the necessity for microvascular reconstruction.
Critical illness (cardiac monitoring)
Diagnostic trial comparative)
Stover, 2009 10 Y Compared noninvasive digital plethysmography with the standard invasive cardiac monitoring system in critical care.
Preeclampsia (blood pressure monitoring)
Diagnostic trial (comparative, case-control)
Elvan-Taşpinar, 2003
123 NA Compared the Finometer™ and the previously validated SpaceLabs 90207 with standard auscultatory blood pressure measurements.
Review of the Evidence: DiscussionNote: Digital plethysmography is commonly used to monitor hemodynamic parameters in clinical settings. Only studies evaluating the diagnostic and prognostic value of digital plethysmography for medical conditions are discussed below.
Cardiovascular disease (risk assessment)Summary: Numerous studies show the utility of digital plethysmography in screening for cardiovascular disease (CVD) risk factors. Further research is needed to optimize the prognostic utility of digital plethysmography in assessing clinical outcomes.
Evidence: Salvi et al. conducted a screening trial to compare measurements of pulse wave velocity (PWV), a predictor of CVD risk, obtained from three different devices102. In 50 subjects (20-84 years of age), PWV measurements were taken using the Complior® and the PulsePen™ (which determine aortic PWV as the delay between carotid and femoral pressure wave) and the PulseTrace, a fingertip photoplethysmographic device that estimates the vascular stiffness index (SI). The measurements were compared to the reference method (simultaneous acquisition of pressure waves using two tonometers).The coefficient of variation of PWV was 12.3% for PulsePen™ (r=0.99), 12.4% for Complior® (r=0.83), and 14.5% for PulseTrace (r=0.55). The results suggest that Complior® and PulsePen™ may accurately measure PWV, while PulseTrace may not be as appropriate for this measurement. The results warranted the establishment of PWV reference values and standardization.
Gunarathne et al. conducted a case-control comparative diagnostic trial to validate measures of arterial stiffness using the digital volume pulse (DVP) analysis technique, and to determine the ability of the arterial SI in detecting cardiovascular risk65. The study was conducted on a cohort of subjects (55.2±10.3 years of age, 51% male) from West Midlands, UK. Of the 247 subjects, 187 were apparently healthy and 60 had the following known CVD risk factors: diabetes (33%), hypertension (77.8%), and hypercholesterolemia (61%). DVP was measured with a PCA 2 photoplethysmographic device (Micro Medical) and used to calculate SI with a validated standardized approach according to the European Society of Cardiology (ESC) guidelines. Statistical analysis was then performed to correlate SI with CVD risk. Univariate analysis revealed SI to be strongly associated with CVD risk based on the ESC HeartScore (Pearson correlation coefficient r=0.56, p≤0.001) and increased ordinally with risk (low, medium, high, or very high) (pseudo r2=0.30, p<0.001). When comparing SI to total cholesterol, plasma glucose, systolic blood pressure, and waist-to-hip ratio, receiver-operator characteristic curve analysis

15
revealed SI to be the best discriminator between the categories of risk (area under curve: 0.76 (95% CI 0.64-0.88), p<0.001). SI also distinguished those with established CVD risk factors. Plethysmographic DVP thus shows utility as a noninvasive test for identifying CVD risk. However, further research is needed to determine whether DVP can offer prognostic value beyond established CVD risk assessments.
Otsuka et al. conducted a screening trial to test independent determinants of the second derivative of the finger photoplethysmogram (SDPTG) in cardiovascular risk105. The subjects included 973 male workers (mean age 44+/=6yr) during a company medical checkup. SDPTG was taken from the cuticle of the left forefinger; indices (b/a and d/a) were calculated from the wave heights. Independent determinants of increased b/a were: age (odds ratio [OR] 1.12 per one-year increase, 95% confidence interval [CI] 1.09-1.15); hypertension (OR 1.65, CI 1.03-2.65); dyslipidemia (OR 1.51, CI 1.09-2.09); impaired fasting glucose/diabetes mellitus (OR 2.43, CI 1.16-5.07), and a lack of regular exercise (OR 2.00, CI 1.29-3.08). Independent determinants of decrease d/a were: age (OR 1.11 per one-year increase, CI 1.08-1.14); hypertension (OR 3.44, CI 2.20-5.38); and alcohol intake six or seven days weekly (OR 2.70, CI 1.80-4.06). SDPTG indices were not independently associated with blood leukocyte counts or serum C-reactive protein. The authors concluded that SDPTG index reflects cardiovascular parameters that are influenced by numerous factors. The correlation of inflammation and SDPTG needs further examination.
Chen et al. conducted a multicenter screening trial to examine the clinical utility of a novel “compliance index” (using digital photoplethysmography) in assessing cardiovascular risk103. The study included 140 subjects (without left ventricular dysfunction) referred for treadmill exercise testing. After a 10min rest period, subjects were given a symptom-limited treadmill test (Bruce protocol). A dual-channel photoplethysmography system was used to automatically measure the area under the curve of each digital volume pulse; this represented the finger volume change with each heart beat. Compliance index was then calculated by dividing the area under the curve of digital volume pulse by pulse pressure. Compliance index correlated significantly with pulse-wave velocity (p=0.002), systolic blood pressure (p<0.001), and diastolic blood pressure (p<0.001). The compliance index was lower in patients who were male (p<0.001), hypertensive (p<0.001), and smokers (p=0.006). Because the compliance index was lower in patients with poor exercise capacity and cardiovascular parameters, the index may be useful in clinical examinations of arterial stiffness.
Tsai et al. conducted a comparative screening trial to compare a novel dual-channel photoplethysmographic (PPG) method with a standard applanation tonometry method (AT) to measure pulse wave velocity, a measure of cardiovascular disease (CVD) risk104. PWV was measured in 100 asymptomatic subjects (54 men, 46 women, 19-64 years old) using both dual-channel PPG (PWV-DVP) and PWV-AT to record finger-to-toe digital volume pulse. PWV was calculated as the finger-to-toe distance divided by transit time. There was a significant correlation between DVP and PWV-AT (r=0.678, p<0.01). After controlling for age, heart rate, systolic blood pressure, and diastolic blood pressure, PWV-DVP still correlated significantly with PWV-AT (r=0.669, p<0.01). Hypertensive and dyslipidemic subjects exhibited higher PWV measurements using both methods. These results demonstrated good correlation between the novel dual-channel plethysmographic system and traditional tonometry in measuring PWV.
Hashimoto et al. conducted a comparative case-controlled screening trial to examine the second derivative of the finger photoplethysmogram (SDPTG) and brachial-ankle pulse wave velocity (BAPWV) for assessing arterial function and hypertension106. Digital SDPTG and BAPWV were measured in 848 subjects (544 normotensive and 304 hypertensive but untreated) between 34 and 88 years old. SDPTG wave components were used to calculate b/a and d/a ratios and aging index (AGI). Determinants of SDPTG indices and BAPWV were evaluated using univariate and multivariate analyses. There was a positive and independent correlation between BAPWV and age, blood pressure (BP), heart rate (HR), and hemoglobin A1c. Both the d/a ratio and AGI correlated positively with age and BP; the b/a ratio had a negative independent correlation with age and BP. However, the d/a ratio and AGI correlated negatively with HR, while the b/a ratio correlated positively with HR. SDPTG indices associated independently with gender, but BAPWV did not. Compared to normotensive subjects, hypertensive subjects had significantly higher multivariate-adjusted d/a ratio, AGI, and BAPWV, and lower b/a ratio. Hypertensive subjects had two-fold greater adjusted risks of high d/a and low b/a ratios. While the SDPTG differs from BAPWV and depends on multiple factors, these results suggest that SDPTG may have utility in assessing hypertension-accelerated vascular aging.
Millasseau et al. conducted a comparative screening trial to evaluate the utility of digital pulse contour analysis in measuring large artery stiffness, using applanation tonometry as a standar101. In 87 healthy subjects (58 men, 29 women,
16
21-68 years old), digital volume pulse (DVP) measured by infrared light photoplethysmography was used to determine large artery stiffness. Stiffness index SI according to DVP (SI[DVP]) was compared to pulse wave velocity recorded by applanation tonometry or carotid-femoral PWV (PWV[cf]). Reproducibility of both methods and glyceryl trinitrate responses were assessed. SI(DVP) was highly correlated with PWV(cf) (r=0.65, p<0.0001), and each was independently correlated with age and mean arterial blood pressure (p<0.0001). In a subset of nine healthy men, intravenous glyceryl trinitrate (2, 20, and 300mcg/min for 15 min) produced similar responses as determined by SI(DVP) and PWV(cf). These results suggest that DVP contour analysis is a feasible measure of large artery stiffness.
Takazawa et al. conducted a screening trial to evaluate the application of the second derivative of the fingertip photoplethysmogram (STPTG) for drug administration studies (83). In 39 patients (54±11 years of age), fingertip photoplethysmogram and its second derivative (a, b, c, and d wave in systole and an e wave in diastole) were used simultaneously to record ascending aortic pressure. The ratio of the height of the late systolic peak to that of the early systolic peak in the pulse was defined as the augmentation index. After injection angiotensin (2.5mcg), ascending aortic pressure increased from 126/74 to 160/91mmHg. After sublingual nitroglycerin (0.3mg), ascending aortic pressure decreased to 111/73mmHg. The ratio of the height of the d wave to that of the a wave (d/a) decreased after angiotensin from -0.40+/-0.13 to -0.62+/-0.19 (p<0.001). After nitroglycerin, d/a increased to -0.25+/-0.12 (p<0.001). The increase in negative d/a was correlated with increased plethysmographic index (r=0.79, p<0.001) and in ascending aortic augmentation index (r=0.80, p<0.001). The late systolic pressure augmentation in the ascending aorta was reflected by the negative d/a, which was suggested to be a useful noninvasive technique for evaluating the effects of vasoactive agents.
Takazawa et al. conducted a case-controlled screening study to evaluate the clinical application of the second derivative of the fingertip photoplethysmogram (SDPTG)83. Six hundred subjects, with 50 men and 50 women in six age groups (30s, 40s, 50s, 60s, 70s, and 80s), were included in the study. The second derivative of the plethysmogram waveform (a, b, c, and d wave in systole and an e wave in diastole) was measured in each patient. The second derivative aging index was defined as b-c-d-e/a; as subject age increased, b/a ratio increased, and c/a, d/a, and e/a ratios decreased. The increase in second derivative wave aging index (y) was correlated with age (x) (r=0.80, p<0.001, y=0.023x-1.515). Compared to age-matched healthy controls, subjects with histories of diabetes, hypertension, high cholesterol, and ischemic heart disease (N=126) had higher second derivative aging index (-0.22+/-0.41 vs. -0.06+/-0.36, p<0.01). Women also had higher aging indices than men (p<0.01). These results suggest that the SDPTG and the b-c-d-e/a ratio may be useful for assessing vascular aging and for screening atherosclerosis.
Kogure et al. conducted a screening trial using accelerated plethysmography (APG) to determine the prevalence of carotid atherosclerosis and its relation to aging107. The trial examined 84 subjects in the fifth decade of life, 89 in the sixth decade, 67 in the seventh decade, and 30 in the eighth decade. Atheromatous plaque was defined as intima-media thickening of 2.1mm or greater. APG was performed using double-differentiation of the finger plethysmograph recording, and the accelerated plethysmography index calculated from the distances between the a, b, c, and d waves. Using multiple-regression analysis, the investigators found a significant correlation between age and both accelerated plethysmography index and intima-media complex thickness. These findings suggested that individuals over 60 years of age are at increased risk of plaque formation, and that their carotid arteries should be routinely examined even when other cardiovascular risk factors are absent. Low accelerated plethysmography index was correlated with pathophysiology distinct from artheromatous plaque formation.
Takada et al. conducted a randomized controlled trial testing acceleration plethysmography (APG) as a noninvasive measure of vascular aging, and to test its utility in predicting the severity of atherosclerosis108. The study examined 390 subjects (82 males and 308 females) between 30 and 69 years of age. accelerated plethysmography was performed on seated subjects. accelerated plethysmography wave patterns were compared to age and other cardiovascular risk factors (e.g., serum lipids, blood pressure, body composition, and smoking status). accelerated plethysmography wave patterns were strongly correlated with aging, pulse pressure (PP), body mass index, and current smoking status. Categorized wave patterns were strongly associated with high serum total cholesterol (TC). These results suggest that arterial status is reflected in accelerated plethysmography wave patterns, and that accelerated plethysmography may be used to predict atherosclerosis level. Although the clinical relevance of accelerated plethysmography warranted further examination of other factors (e.g., pulse pressure, sex, body height), accelerated plethysmography may be useful as a noninvasive measure of cardiovascular parameters.

17
Peripheral vascular disease (detection, risk factor assessment)Summary: The accuracy of digital photoplethysmography approaches that of the standard ankle-brachial pressure index (ABPI) measurement (Doppler) in assessing peripheral vascular disease. Moreover, the noninvasive nature of PPG and its ease of use may improve identification and risk factor management in peripheral vascular disease.
Evidence: Khandanpour et al. conducted a comparative diagnostic trial to compare the accuracy of digital photoplethysmography (PPG) and continuous wave Doppler (CW-Doppler) in assessing ABPI120. In 133 patients with claudication, ABPI was measured computationally via a photoplethysmography probe on the index finger and great toe; an 8MHz Doppler probe was used to manually measure ABPI. Statistical analysis was performed using Lin’s correlation coefficient and Bland-Altman plots, and a strong correlation was found between the two techniques (beta=0.79, 95% limits of agreement -0.23-0.24). These results suggest that automatic ABPI measurements using photoplethysmography may be an effective, fast, and objective alternative for Doppler in assessing peripheral vascular disease.
Sharif-Kashani et al. conducted a comparative diagnostic trial to compare digital photoplethysmography with venous ultrasonography for screening for deep vein thrombosis (DVT)119. In 169 asymptomatic patients at high risk for DVT, 337 limbs were assessed with ultrasonography and digital plethysmography. Ultrasonography detected 13 limbs with DVT. In limbs with normal ultrasound results, venous refilling time was >12 seconds; this was used as a cutoff point for digital plethysmography, which had 100% sensitivity, 73.8% specificity, 13.3% positive predictive value, and 100% negative predictive value for detecting DVT. Digital -PPG was suggested as a promising, noninvasive, and simple method for DVT screening.
Allen et al. conducted a case-controlled comparative diagnostic trial to compare bilateral photoplethysmography (PPG) with the standard ABPI for assessing lower limb peripheral vascular disease121. Photoplethysmography was used in a controlled environment to measure pulse wave timing, amplitude, and shape characteristics for both great toes in 111 subjects (42-91 years of age), 63 of whom were healthy and 48 with significant lower limb peripheral arterial disease. The parameters were compared with previous normative values, and accuracy determined for ABPI<0.9 (significant disease) and ABPI<0.5 (higher-grade disease). The pulse shape correlated highly with ABPI for detecting significant disease; diagnostic accuracy was 91% (kappa=0.80), sensitivity was 93%, and specificity was 89%. For higher-grade disease, accuracy was 90% (kappa=0.65). Bilateral pulse transit time (PTT) differences were also highly correlated with ABPI, with 86% accuracy for detecting significant disease and 90% for higher-grade disease. These results supported the use of photoplethysmography for diagnosing peripheral arterial disease, especially due to its noninvasive, nontechnical, and accurate nature.
Alnaeb et al. conducted case-controlled comparative diagnostic trial to evaluate a novel optical device based on the photoplethysmography method with the standard measuring techniques, ABPI and duplex angiography (DA)122. In 47 legs of 24 diabetic patients (age 70±3 years) and 30 legs of 15 healthy controls (66±5 years), functional photoplethysmography (fPPG) was used to acquire pulsatile arterial perfusion by placing an optical probe on the toe for 30 seconds, with the leg in supine position and raised at 45°. In diabetic patients, functional photoplethysmography was correlated significantly with both DA (r=-0.68, p<0.01) and ABPI (r=-0.65, p<0.01). The correlation between ABPI and DA was also significant (r=0.81, p<0.01). Compared to DA, ABPI had 80% sensitivity and 93% specificity; functional photoplethysmography had 83% sensitivity and 71% specificity. Functional photoplethysmography measurement time was shorter (5min) than ABPI (10-15min), and required no operator skills. These results suggest that functional photoplethysmography has diagnostic potential in lower-extremity peripheral arterial disease, though additional optimization of the technique is warranted.
Erts et al. conducted a case-controlled comparative diagnostic trial using a novel portable multi-channel photoplethysmography for bilateral measurements of leg arterial stenosis compared with the standard ankle-brachial index123. In 45 patients diagnosed with leg arterial stenosis and 20 healthy controls, peripheral blood pulsations were taken bilaterally from fingers and toes. Photoplethysmography pulses from the periphery of the affected leg were much weaker compared to the healthy contralateral leg, and pulse wave transit time (PWTT) was increased by 20-80ms. PWTT delays were ≤14ms in healthy subjects. Fingertip reference PWTT values also did not show any significant delays. The PWTT delays were correlated with differences in local blood pressure (Pearson’s coefficient r=0.93) and the ankle-brachial index (r=-0.96). These data support the utility of bilateral photoplethysmography for detecting and assessing peripheral arterial occlusions.
Carter et al. conducted a comparative diagnostic trial to determine whether risk of amputation in peripheral arterial disease is associated with low transcutaneous oxygen tension (TcPO2), and whether additionally measuring toe pressure/pulse wave amplitudes would improve diagnostic values of TcPO2 alone116. Foot TcPO2, ankle and toe pressures, pressure
18
indices, and toe pulse wave amplitudes were measured in 75 limbs of 66 patients with skin lesions and peripheral arterial disease. The Cox proportional hazards model was used to correlate the parameters with risk of subsequent amputation. Risk of amputation was significantly correlated with TcPO2 ≤10mmHg (relative risk 2.16, p<0.05). Relative risks associated with cutoff values of ankle and toe pressures and pressure indices ranged from 2.53 (toe ≤ 20mmHg, p<0.05) to 5.83 (ankle ≤50mmHg, p<0.001). The relative risk associated with wave amplitude ≤4mm was 3.41 (p<0.01). These results suggest that low TcPO2 is significantly correlated with risk of amputation in patients with skin lesions and arterial disease, and low wave amplitude provides significant information in addition to peripheral pressures.
Allen et al. conducted case-controlled comparative diagnostic trial comparing simultaneous photoplethysmographic pulse measurements from both great toes to the established ABPI measurement in diagnosing peripheral arterial occlusive (PAOD) disease124. In 44 patients with suspected lower limb disease and 63 healthy controls, pulse wave timing and amplitude and shape characteristics were obtained for both toes and for right-to-left toe differences. Normative pulse characteristics were calculated from the healthy subject group. Using the established ABPI for detecting lower limb arterial disease, the relative diagnostic values of the different pulse features were obtained. The degrees of bilateral similarity were established in healthy subjects; for different grades of arterial disease, the degrees of pulse delay, amplitude reduction, and damping and bilateral asymmetry were calculated. Pulse timing and amplitude and shape features were ranked in order of diagnostic performance, and the shape index was in agreement with ABPI (>90% accuracy, kappa 0.75). Shape index was able to detect severe disease with 100% sensitivity, for legs with ABPI <0.5. Timing differences between pulse peaks yielded diagnostic accuracies of 88% for all levels of arterial disease (kappa 0.70) and 93% for higher-grade disease (kappa 0.77). However, the discriminatory value of PPG pulse amplitude was limited. Nonetheless, the combined ease of use, low cost, noninvasive nature, and accuracy of photoplethysmography may make it a valuable diagnostic technique in PAOD.
Ubbink et al. conducted a comparative diagnostic trial using a new laser Doppler (LD) device and standard photoplethysmography in measuring toe systolic blood pressure (TBP) in suspected cases of leg ischemia115. The study was conducted on 121 legs of 70 patients with suspected leg arterial insufficiency. The mean toe pressures were 68.1mmHg with photoplethysmography, 67.2mmHg with unheated LD, and 75.5 mmHg with heated LD (37°C). Correlation to photoplethysmography was 0.91 for unheated LD and 0.93 for heated LD. However, there was considerable variation between LD and photoplethysmography (95% CI: 45mmHg) independent of TBP. The LD was suggested as a suitable alternative to the standard PPG for assessing TBP, though with greater variation.
Sadiq et al. conducted a comparative case-controlled diagnostic trial to assess the accuracy of photoplethysmography in detecting flow and systolic arterial pressures compared to the standard continuous wave Doppler method117. The two methods were tested on 181 limbs and compared to ankle/brachial indices (ABIs). Of the 181 limbs, 133 had normal and 48 had abnormal ABIs. The infrared photosensor (IP) from the photoplethysmograph apparatus was placed on the pad of the index finger and great toe. Photoplethysmography provided IPs with good correlation with the Doppler method (linear regression r=0.96 for normal and r=0.95 for abnormal ABIs). The two methods did not differ significantly (p<0.0001) in ABI calculations. However, photoplethysmography was faster, easier, and automated; the Doppler system was cumbersome. The authors concluded that photoplethysmography was ideal for noncompliant patients and superior to Doppler in advanced occlusive arterial disease, and routine photoplethysmography was recommended.
Whiteley et al. conducted comparative diagnostic trial to examine photoplethysmography as an alternative to hand-held Doppler and sphygmomanometer in measuring ankle/brachial pressure index (ABPI)118. In 32 vascular patients, 52 legs were examined by placing the photoplethysmography transmitter/receiver on the pulp of the index finger or great toe. ABIs obtained from both methods had excellent correlation (correlation coefficient 0.875). In four patients, photoplethysmography was not recordable in four lower limbs; one had an unrecordable Doppler. When these four patients were excluded from analysis, the correlation coefficient rose to 0.975. Because Doppler technique can be difficult to master, the authors suggested replacing hand-held Doppler with photoplethysmography for ABPI.
Planchon et al. conducted a diagnostic trial of digital plethysmography as a diagnostic and prognostic test in digital arteriopathies125. Strain gauge digital plethysmography was used to measure maximal digital pulse (MDP) on 10 subjects with digital necrosis. Arteriography was performed on the hands of each subject. A MDP value of less than 0.10% delta V was correlated with digital arteriopathy and high trophic complication risk. Normal MDP values (0.19±0.06% delta V) did not rule out arteriopathies, but may indicate lower risk of trophic complications.

19
Becker conducted a diagnostic case series to examine arterial occlusive disease of lower limbs using several vascular tests, including Doppler, tetrapolar rheography, digital plethysmography, and transcutaneous measure of PO2 (Tc PO2243. The continuous series included 1,000 lower limbs with arterial occlusive disease. Degradation of digital plethysmography and Tc PO2 was proportional to the degree of ischemia, particularly in stages III and IV as defined by Leriche and Fontaine. Combined data from digital plethysmography and Tc PO2 was suggested to be more discriminating than each method used singly, and may rule out false positives of stages III and IV disease.
Raynaud’s phenomenon (detection and assessment)Summary: Digital plethysmography is a common diagnostic and prognostic procedure for primary or secondary Raynaud’s phenomenon, and is particularly useful as an objective adjunct to clinical assessments and other objective procedures.
Evidence: Dyszkiewicz et al. conducted a comparative case-controlled diagnostic trial to evaluate a diagnosis test for vibration syndrome (vibration-induced Raynaud’s phenomenon), which consists of a cooling test verified by computerized photoplethysmography of the fingertip131. The study involved 128 subjects with vibration exposure, including 58 women (40.9±5.4 years of age) and 70 men (38.7±8.8 years of age). The control group contained 41 people, including 20 women (39.6±7.3 years of age) and 21 men (39.3±6.4 years of age) without vibration exposure. The patients were given a questionnaire, a vibration perception threshold test, and a cooling test. The cooling test was verified visually and computationally by photoplethysmography on the fingertip plexus. Measurements (S1, S2, and A) were taken from each patient from averaging three pulse graphs. The investigators did not use the established standard of ≥60 graphs, which may cause large variation in thermodynamic parameters, because of cooling test specifications. Longer measurement times were used to compensate for the reduced temperature. During the cooling test, controls had increases in planimetric indicators, which were verified by computerized photoplethysmography. In subjects who were exposed to vibration, eight (6.2%) tested positive in the cooling, and seven (5.5%) tested positive in the vibration perception threshold test by visual verification. However, the planimetric indicators decreased after cooling in 87 (67%) of vibration-exposed test subjects by computerized photoplethysmography. The novel computerized photoplethysmographic test thus showed greater sensitivity in detecting preclinical vibration syndrome compared to the other tests, and was proposed as a diagnostic test for this disorder.
Nasu et al. conducted a multicenter evaluation study to assess the diagnostic value of finger plethysmography after segmental cooling for vibration-induced white finger (VWF)137, also known as vibration-induced Raynaud’s phenomenon or occupational Raynaud’s syndrome. The study examined 154 men without vibration exposure (group A, control) and 135 men exposed to occupational vibration who were divided into four groups: 21 subjects without VWF (group B), 31 subjects with VWF history but symptom-free for one year (group C), and 83 subjects with active VWF (group D). Finger systolic blood pressure (FSBP) was taken at 21°C and 23°C (±1°C) with a Digimatic® 2000 (Medimatic) strain-gauge plethysmograph. At 23°C, the values differed significantly between groups A and D, and between groups B and D. At 21°C, the values differed between groups A and C, A and D, and B and D. Group D showed the lowest readings at both temperatures. The sensitivity was 65.2% and specificity was 87.5% at 23°C, assuming a cut-off value of 75%. At 21°C, the sensitivity and specificity were 73.9% and 82.5%, respectively. These results did not support diagnostic accuracy of this test at room temperature, which may be due to the fact that many subjects were retired and had not been exposed to vibration for the past year.
Thompson et al. conducted a comparative cohort diagnostic trial to test the specificity and sensitivity of finger thermometry and finger plethysmography in assessing hand-arm vibration syndrome (HAVS)139, also known as vibration-induced Raynaud’s phenomenon or occupational Raynaud’s syndrome. Previous research showed both of these objective tests to correlate poorly with vascular stage determined by the Stockholm Workshop Scale (SWS). The primary aim of the study was to determine the sensitivity and specificity of digital thermometry and plethysmography compared to the reference measurement, SWS. The secondary aim was to optimize sensitivity and specificity. A cross-sectional analysis was performed on 139 patients evaluated for HAVS. The objective tests were analyzed using vascular stage (determined by SWS) as an outcome variable. Age, smoking, time since last vibration exposure, and vasoactive medication use were controlled by logistic regression. The highest sensitivity was obtained with plethysmography stage ≥1 (94% sensitivity, 15% specificity). The highest specificity was obtained combining plethysmography stage 3 and thermometry stage 3 (98% specificity and 23% sensitivity). The highest diagnostic accuracy (70%) was obtained using plethysmography alone, with positive test criteria set at stage ≥1. The objective tests (plethysmography and thermometry) did not achieve the sensitivity required of an objective measure of SWS, when used alone or in combination. The objective tests did show greater sensitivity than specificity, and may be more sensitive in detecting vascular disorders than the SWS.
20
Thompson et al. conducted comparative diagnostic trial to examine the correlation between objective cold provocation tests (thermography and finger plethysmography), as well as the correlation between the objective tests and vascular staging determined by the Stockholm Workshop Scale (SWS) in a cohort of patients with hand-arm vibration syndrome (HAVS)138, also known as vibration-induced Raynaud’s phenomenon or occupational Raynaud’s syndrome. A cross section of 139 patients evaluated for HAVS were given questionnaires, clinical assessments, and objective tests. Correlation coefficients were then calculated using Spearman’s test. Although plethysmography and thermometry correlated with each other with statistical significance (rho=0.47, p<0.001), neither test correlated significantly with the SWS vascular stage. Logistic regression showed weak prediction of SWS vascular stage for plethysmography (OR=1.5) and thermometry (OR=1.3). Potential confounders did not have significant effects in these models. Although the tests did not appear to reliably predict SWS vascular stage in HAVS, the tests may still be reliable measures of other vascular disorders with related pathologies.
Schapira et al. reviewed case reports to assess clinical features, diagnosis, treatment, and prognosis of interferon-induced Raynaud’s phenomenon126. A MEDLINE search (using the search terms Raynaud, interferon, ischemia, thrombosis and necrosis) was conducted to identify medical publications between 1967 and November 2001. Qualitative analysis was performed on 24 cases of interferon-induced Raynaud’s phenomenon. Interferon-alpha was the most common cause of Raynaud’s phenomenon (14 cases), and symptoms ranged from mild vasospasm to occlusive digital arteriopathy and necrosis. Six cases required finger amputation. Digital plethysmography, arteriography, and capillaroscopy were central to diagnosis of interferon-induced Raynaud’s phenomenon. Because early diagnosis and withdrawal of interferon may prevent severe complications and amputation, digital plethysmography may be a crucial diagnostic tool for this form of Raynaud’s phenomenon.
Martinez et al. conducted a prospective case-controlled diagnostic trial to test the utility of plethysmography and digital pressure indices (DPI) in evaluating treatment effectiveness in Raynaud’s phenomenon135. The study followed 40 Raynaud’s patients and 15 control subjects over four months. The Raynaud’s patients were randomly allocated to groups of 20 receiving either active treatment (calcium antagonists) or placebo. Digital pressures, plethysmography, and DPI were calculated after cold stimulation at baseline, during, and after the treatment period. At baseline, the Raynaud’s group had lower DPI before and after cold provocation than the control group (p<0.001 and 0.0001, respectively). After treatment, the DPI increased significantly in the treatment subgroup compared to the placebo group (p<0.0001). The DPI had 97% sensitivity and 93% specificity for the cold provocation test, and the plethysmographic wave did not have significant variations (48% sensitivity and 100% specificity). These data indicate that digital plethysmography and DPI may accurately determine the degree of vasospasm in Raynaud’s phenomenon and treatment efficacy.
Miyashita et al. conducted screening trial to examine age-related variation in indices of accelerated plethysmography (APG) for fingers, and to establish accelerated plethysmography as a technique for evaluating occupational vibration disease140, also known as vibration-induced Raynaud’s phenomenon or occupational Raynaud’s syndrome. Indices of accelerated plethysmography were obtained from 815 non-hypertensive male subjects without vibration exposure, and used to establish standard aging curves. Workers exposed to occupational hand-arm vibration (number unclear) were used to evaluate peripheral circulation with accelerated plethysmography of the dominant index fingertip. For each age group (intervals of 5 years), accelerated plethysmography indices showed normal distribution in a logarithmic scale. When compared to this standard aging curve, subjects exposed to occupational vibration showed deteriorated indices of –b/a and a/d. These results suggested that accelerated plethysmography may be a reliable technique for evaluating vibration-induced peripheral circulatory disorders.
Suichies et al. conducted a comparative diagnostic trial comparing digital photoelectrical plethysmography (PhEP) and laser Doppler flowmetry (LDF) for testing Raynaud’s phenomenon severity130. Patients with primary or secondary Raynaud’s phenomenon (N=18) were subjected to cold recovery testing, which involved immersing one hand in water and cooling from 33°C to 3°C, followed by a 10min recovery period at ambient room temperature of 24°C. In the cooled hand, photoelectrical plethysmography decreased to 6.2±3.2% and LDF decreased by 10±12%, with correlation coefficients ranging from 0.79 to 0.99. In the opposite hand, PhEP decreased to 38±30% and 64±7.9% with correlation coefficients ranging from 0.26 to 0.95. The LDF/PhEP ratios allowed for more specific testing of red blood cell velocity during cooling. Although the data obtained from the contralateral hand were not consistent, both methods were comparable for diagnosing the severity of Raynaud’s phenomenon and testing the effects of treatment.

21
Maisonneuve conducted a comparative diagnostic trial to assess the diagnostic value of clinical and functional examinations in diagnosing true Raynaud’s syndrome secondary to thoracic outlet syndrome (TOS)244. The study involved 104 patients with TOS. Capillaroscopy and digital plethysmography were useful in diagnosing true Raynaud’s syndrome secondary to TOS, while arterial Doppler was more reliable in distinguishing symptomatic and asymptomatic sides in the same patient. These results support the usefulness of digital plethysmography as an adjunct to other objective measures in evaluating Raynaud’s phenomenon.
Laroche et al. conducted comparative diagnostic trial to determine the validity of digital plethysmography and the digital temperature recovery test in diagnosing the presence and severity of Raynaud’s phenomenon245. Objective testing (digital plethysmography and temperature recovery tests) were performed on 365 of 405 patients clinically evaluated for Raynaud’s phenomenon (210 of whom had vibration-induced white finger), and results were compared with qualitative clinical evaluation. When digital temperature recovery time was used alone, its sensitivity was 56.5% for primary Raynaud’s phenomenon and 49.1% for occupational Raynaud’s phenomenon. The sensitivity of digital plethysmography was 80.5% for primary and 67.8% for secondary Raynaud’s. When the two objective tests were used together, sensitivity increased to 85.5% for primary Raynaud’s phenomenon and 78.8% for vibration-induced Raynaud’s phenomenon. The objective tests did not reliably predict severity and degree of impairment caused by the disorders; however, these results support the usefulness of digital plethysmography and digital temperature recovery testing as adjuncts to clinical evaluation.
de Faucal et al. conducted a case-controlled diagnostic trial to examine digital plethysmography as a technique for studying rheological and hemodynamic parameters of vascular disorders, including Raynaud’s phenomenon133. The study involved 69 patients with idiopathic Raynaud’s phenomenon, 12 patients with scleroderma, 10 patients with digital arteritis, 15 patients with secondary Raynaud’s phenomenon, and 65 control subjects. Maximum digital pulse (MDP) was measured using digital plethysmography after immersing hands in 45°C water for three minutes. MDP was significantly decreased in patients with digital arteritis and scleroderma, normal in controls and patients with idiopathic Raynaud’s syndrome, and significantly increased in patients with secondary Raynaud’s phenomenon of rheologic origin. These findings suggest that digital plethysmography may distinguish vascular disorders of various pathologies.
Planchon et al. conducted a case-controlled diagnostic trial to develop a vascular reactivity cold test using mercury strain gauge plethysmography134. The test involved immersing the hand in 11°C water to determine local reactivity, thorax ventilation to determine general reactivity, and assessing both cooling modes to determine cumulative reactivity. The digital plethysmographic signals were expressed as a ratio to a reference warm amplitude (immersion in 45°C water for three minutes). The technique was optimized in 66 control subjects and used on 65 Raynaud’s disease patients. Cumulative reactivity differed significantly between control and test groups (p<0.0000000001). These results suggested that the test had diagnostic and prognostic value in vascular disorders134.
Zweifler et al. conducted a retrospective diagnostic case review to determine the relationship between occlusive digital artery disease and systemic illness in patients with Raynaud’s phenomenon based on digital plethysmographic findings128. The records of 147 Raynaud’s patients were subdivided into groups with and without occlusive artery disease determined by quantitative finger plethysmographic data. Patients with scleroderma were excluded from analysis. Of the 147 cases, occlusive artery disease was present in 62% of cases. A cause was determined at initial examination for Raynaud’s phenomenon in 34% of cases with occlusive digital artery disease and 24.9% of cases without occlusive artery disease. In 56 patients with no cause for Raynaud’s determined at initial examination, follow-up status was ascertained. Over an average 5.5-year follow-up, systemic illness occurred in 43.8% of cases with and in 16.7% of cases without occlusive digital artery disease. Connective tissue disorders (such as scleroderma) and carcinoma were major systemic illnesses that occurred during follow-up. These results suggest that occlusive artery disease in Raynaud’s phenomenon poses a concern for cancer and connective tissue disorders, even when the origin is idiopathic, and that digital plethysmography plays an important role in detecting occlusive artery disease during routine evaluation.
Samueloff et al. conducted a preliminary case-controlled diagnostic trial to evaluate an objective test for Raynaud’s syndrome using photocell plethysmography129. In a limited number of subjects (details unclear), one hand was immersed in ice water, and hemodynamic variations were measured in the contralateral hand using photocell plethysmography. After the cold stimulus, patients with Raynaud’s took significantly longer to recover than control subjects (p=0.0045). Relative changes in pulse amplitudes during cold stimulation were confounded by age and sex between the control and test groups.

22
Woulda conducted a case-controlled diagnostic trial with the cooling and warm up test, which uses photoelectric plethysmography of the fingers, on 58 outpatients with Raynaud’s phenomenon and 34 controls (17 men and 17 women) without Raynaud’s phenomenon127. In the control group, the hands of the women appeared to warm up more quickly, remain warm for longer periods of time, and cool more quickly (possibly due to differences in hand volume). Differences in amplitudes were apparent even at the lowest water temperatures tested (6°C and 3°C). Subjects tested positive in this assay when their lowest values were below the lowest control values. This test may be used objectively in severe cases of Raynaud’s phenomenon; less severe cases may test negative.
Sleep apneaSummary: Because standard polysomnographic (PSG) recordings of REM sleep are laborious and time-consuming, more non-invasive methods have been proposed for ambulatory in-home monitoring. Digital plethysmography may be used for noninvasive monitoring of blood flow in sleep apnea, though it may not entirely reflect measurements made on the forearm. Nonetheless, digital plethysmography may be valuable as a complement to other assessment techniques for monitoring vascular changes during obstructive sleep apnea (OSA). Several supportive studies have been conducted using the WatchPAT100 device, which is a portable finger plethysmographic device based on peripheral arterial tone (PAT) coupled to a constant volume, variable pressure, pneumatic system.
Evidence: Pang et al. conducted a nonrandomized, single-blind comparison study to compare polysomnography and the digital plethysmography using the WatchPAT100 device in diagnosing OSA246. A total of 37 patients (mean age 50.1 years) with suspected sleep apnea were monitored with the WatchPAT device simultaneously with polysomnography PSG. The WatchPAT100 had high correlation with the polysomnogram in apnea-hypopnea index (r=0.9288; 95% CI 0.8579-0.9650, p<0.0001), lowest oxygen saturation (r=0.989; 95% CI 0.9773-0.9947, p<0.0001), and sleep time of (r=0.5815, p=0.005). These results supported the use of WatchPAT100 in the diagnosis of sleep apnea.
Herscovici et al. conducted a comparative, case-control study to test an algorithm for automatic REM detection based on the peripheral arterial tone (PAT) signal and actigraphy recorded with theWatchPAT100 digital plethysmograph device247. Thirty patients referred for suspected obstructive sleep apnea syndrome (OSAS) (with an additional 30 patients in a validation set) were subjected to simultaneous recording with PSG and the WatchPAT100 device. An algorithm was developed by dividing sleep records into five-minute intervals, each of which contained two time series constructed from the PAT amplitudes and PAT-derived inter-pulse periods. The specificity and accuracy of the algorithm was assessed by comparison to the “gold standard” PSG and in the separate validation set of 30 patients, which identified the standard 30-second epochs of REM sleep with an overall sensitivity of 78%, specificity of 92%, and agreement of 89%. This method of REM detection may thus be useful for in-home, unsupervised ambulatory sleep monitoring. This study was conducted by employees of Itamar Medical Ltd., the manufacturer of the WatchPAT100.
Zou et al. conducted a validation study in a population-based cohort to assess the accuracy of a wrist-worn device based on peripheral arterial tonometry for diagnostic screening of OSA248. Subjects (N=98) were recruited from the Skaraborg Hypertension and Diabetes Project, and subjected to simultaneous polysomnography (PSG) and digital plethysmography (WatchPAT100) home recordings. Measures of respiratory disturbance index (RDI), apnea-hypopnea index (AHI), oxygen desaturation index (ODI), and sleep-wake state were compared between simultaneous WatchPAT100 and PSG recordings, and agreement between the two techniques for sleep-wake assessments (based on 30-second bins) was 82+/-7%. The in-home use of the WatchPAT100 simultaneously with PSG was proposed to be a reasonable standard for screening and diagnosing OSAS in the general population. This study was sponsored by Itamar Medical Ltd., the manufacturer of the WatchPAT100.
Hedner et al. conducted a comparative study to validate a novel automatic algorithm using adaptive wrist actigraphy for sleep-wake assessment249. The study was a prospective study in a cohort of 228 normal subjects and patients with obstructive sleep apnea. The subjects were monitored simultaneously with polysomnography and WatchPAT100 (which contains a built-in actigraph). The automatic sleep/wake algorithm was based on the magnitude and duration of motion, as well as various periodic movement patterns associated with moderate to severe obstructive sleep apnea. There was 89% sensitivity and 69% specificity to identify sleep, with good agreement between subjects (86% in normal patients, and 86% in mild, 84% for moderate, and 69% for severe obstructive sleep apnea. There was also good agreement There was a tight agreement between the two methods for determining sleep efficiency (78.4±9.9 vs. 78.8±13.4%), total sleep time (690±152 vs. 690±154 epochs), and sleep latency (56.8±31.4 vs. 43.3±45.4 epochs). The authors suggested that this method of
23
assessing total sleep time may prove useful in diagnosing sleep apnea at home. This study was sponsored by Itamar Medical Ltd., the manufacturer of the WatchPAT100.
Pittman et al. conducted a comparative study to validate a wrist-worn device based on peripheral arterial tonometry for diagnosing obstructive sleep apnea (OSA)250. The 30 subjects with suspected OSA were recorded for one night in the laboratory with standard polysomnography (PSG) simultaneously with the WatchPAT100, and an additional night in the home with only the WatchPAT100. Respiratory events measured with PSG were quantified using the respiratory disturbance index (RDI) (also known as the Chicago criteria or RDI.C), as well as the RDI defined by Medicare guidelines (RDI.M). The measures were analyzed statistically, and receiver-operator curves were used to determine sensitivity, specificity, and likelihood ratios. There was high concordance between RDI.C and WatchPAT100 RDI for in-lab measures, and good concordance for in-home measures. There were also no technical difficulties with the WatchPAT100 device during the in-home monitoring sessions. The authors concluded that the WatchPAT100 could reliably define respiratory events, even for self-administered testing. Authors of the study served as consultants to Itamar Medical Ltd., the manufacturer of the WatchPAT100.
Grote et al. conducted a screening trial to test finger plethysmography as a method for monitoring finger blood flow in sleep apnea144. In 44 subjects, changes in finger blood flow were determined using pulse wave amplitude (PWA) obtained from finger plethysmography and forearm plethysmography after administering norepinephrine (N=15), phentolamine (N=15), or isoproterenol (N=14). In eight patients, PWA was assessed during sleep with obstructed breathing. Vasoconstriction in the finger was stronger than that in the forearm (ANOVA, p=0.002). Isoproterenol increased forearm blood flow, but not finger blood flow (p<0.001). Finger PWA was significantly reduced during OSA in six patients (-37.5+/-16.1%, p=0.002). Although finger measurements did not completely mirror forearm measurements (likely due to anatomical and functional differences), finger plethysmography was suggested to be a useful complement to other vascular measurements.
Ayas et al. conducted a comparative study to evaluate the accuracy of digital plethysmography in diagnosing OSAS251. The study examined 30 adults (mean age 47.0+/-14.8 years, mean body mass index 31.0+/-7.6kg/m(2), mean PSG AHI 23+/-23.9 events/hour, and mean PAT AHI 23+/-15.9 events/hour) with and without suspected OSA. The study employed the WatchPAT100, a wrist-worn device with a finger-mounted optic/pneumatic sensor. The device was able to eliminate venous pulsations and continuously measure the pulse volume of the digit. The subjects were monitored for a full night with standard in-laboratory PSG as well as digital plethysmography with the WatchPAT100 device. An automated computerized algorithm was used to assess the WatchPAT output, and a PAT AHI was generated by calculating the frequency of respiratory events per hour of sleep using a combination of peripheral arterial tonometry (PAT signal attenuation, desaturation on pulse oximetry, and changes in heart rate. There was a significant correlation between AHIs measured by standard PSG and by the WatchPAT device (r=0.87, p<0.001). Receiver-operator characteristic curves also showed good sensitivity and specificity at 10, 15, 20, and 30 events/hour. These results suggested that the WatchPAT may be a useful and noninvasive method of detecting OSA. The lead author of the study served as a consultant to Itamar Medical Ltd., the manufacturer of the WatchPAT100, but did not have financial interests in the company. Itamar Medical Ltd., provided funding for the study.
Bar et al. conducted a comparative study to evaluate the efficacy, reliability, and reproducibility of a portable digital plethysmography device (based on peripheral arterial tone) for diagnosing OSAS in home sleep studies252. The study examined 69 patients with OSAS and 33 normal volunteers (102 subjects total; mean age 41.4±15.2 years, mean body mass index 26.8±5.5). The subjects underwent full in-lab recording with standard PSG simultaneously with the test WatchPAT100 device. A subset of 14 subjects underwent two additional unattended home sleep recordings using only the WatchPAT100 device alone. Blind scores of apnea/hypopnea for the PSG recordings were made using American Academy of Sleep Medicine criteria and were used to calculate RDI. A proprietary algorithm was used to analyze RDI for the WatchPAT100 data. The RDIs of WatchPAT100 and PSG were highly correlated (r=0.88, p<0.0001) and reproducible, with high correlation between home- and in-laboratory recordings (r=0.89, p<0.001). This study supported the use of ambulatory systems in preliminary diagnosis of OSAS in patients awaiting definitive diagnosis. This study was conducted by employees of Itamar Medical Ltd., the manufacturer of the WatchPAT100, and was supported in part by a grant from the company.
24
Schnall et al. described a novel approach to sleep apnea by measuring peripheral vasoconstriction using finger plethysmography95. The comparative study involved 42 patients with OSAS. A finger plethysmograph, coupled to a constant volume, variable pressure, pneumatic system, detected transient vasoconstriction and periodic tachycardia (abnormally rapid heart beating) during each apnea event; this was attributed to transient arousal. This was compared to measurements using standard total apnea-hypopnea scoring, and the results were in good agreement (p<0.0001). Measurements taken from the finger tip were believed to represent the scope of peripheral vascular responsiveness because of the abundant alpha sympathetic innervation and high degree of blood flow rate lability in the finger. Because elevated peripheral resistance is highly correlated with transient heart rate elevation in arousal and OSAS, this method may reliably and conveniently evaluate OSAS and other sleep-disordered breathing conditions. This study was conducted by employees of Itamar Medical Ltd., the manufacturer of the WatchPAT100.
Diabetic neuropathy (detection)Summary: Digital photoplethysmography may be an accurate and noninvasive alternative to standard nerve conduction velocity (NCV) testing for diabetic neuropathy, and may be used alongside other screening techniques such as the LD and the cold pressor test (CPT). Further research is needed to validate the use of digital photoplethysmography as a stand-alone diagnostic test for diabetic neuropathy.
Evidence: Jaryal et al. conducted screening trial using PPG readings during the CPT to monitor vascular reactivity in diabetic patients111. In 11 healthy subjects and 10 patients with type 2 diabetes mellitus (DM), Digital photoplethysmography wave amplitudes were recorded before and during a one-minute CPT. The digital photoplethysmography readings were continued for five minutes after CPT in healthy controls. Digital photoplethysmography amplitudes decreased after cold stress in both healthy (p<0.0001) and DM (p<0.003) subjects. However, the DM subjects exhibited a smaller wave decrease (0.42±0.08nu) than the control subjects (0.25±0.03nu), a difference that was statistically significant (p=0.04). The CPT also significantly shorted PTT measured by digital photoplethysmography in both control (p<0.006) and DM subjects (p=0.002), yet the decreased PPT was greater in magnitude in the DM patients compared to controls (p=0.03). Other digital photoplethysmography measurements (peak-to-peak interval, crest time, and decay time) did not differ significantly between the two study groups. This study suggests that digital photoplethysmography may be a valuable objective measure of sympathetic reactivity to cold stress, and may be used to detect neurovascular dysfunction in diabetic patients.
Kim et al. conducted a comparative, case-controlled diagnostic trial to evaluate a novel screening method for diabetic neuropathy using laser Doppler (LD) and digital photoplethysmography compared to the standard nerve conduction velocity NCV test110. The study involved 125 subjects: 40 healthy controls, 50 with diabetic neuropathy (19 mild, 17 moderate, and 14 severe based on NCV) and 35 diabetic patients without neuropathy. On the index fingers and great toes of the subjects, D-PPG measured blood volume changes while LD measured blood perfusion. The digital photoplethysmography and LD measurements showed higher toe-to-finger ratios in the neuropathic group compared to the healthy and non-neuropathic controls (p<0.001). Compared to NCV, the sensitivity of LD was higher than digital photoplethysmography (92.0% vs. 84.3%); however, digital photoplethysmography was more reproducible (5.5% vs. 9.5%) and its ratio increase was proportional to disease severity. These results support the accuracy, efficacy, and reliability of digital photoplethysmography for early detection of diabetic neuropathy.
Kim et al. conducted a study to evaluate a novel screening method for diabetic neuropathy using LD and digital photoplethysmography, which would be less invasive than the standard NCV test (109). The study involved 64 normal subjects and 50 with diabetic neuropathy. On the index fingers and great toes of the subjects, digital photoplethysmography measured blood volume changes while LD measured blood perfusion. According to digital photoplethysmography measurements, toe-to-finger ratios were higher in the neuropathic group compared to the healthy controls (p<0.001). Bilateral sensitivity of digital photoplethysmography was 98%, and left-side specificity was 98.4% while right-side specificity was 92.2%. These results suggest that digital photoplethysmography may be a valid, inexpensive, and noninvasive method for the early detection of diabetic neuropathy. Additional research is needed to validate this technique for use in standard clinical practice.
25
Thyroid dysfunction (detection)Summary: Digital photoplethysmography has been proposed as a diagnostic measure of hemodynamic changes caused by thyroid dysfunction. Although few trials have evaluated finger plethysmography in patients with thyroid dysfunction, there is ample evidence that autonomic function (which can be assessed using digital plethysmography) is altered in thyroid dysfunction, and that hypothyroidism carries an increased risk of heart disease. Spectral indices of heart rate variability (HRV) measured with electrocardiogram (ECG) recordings have demonstrated correlation with established parameters of thyroid dysfunction253-257. Estimates of autonomic nervous system function by HRV may reflect pharmacologically and surgically induced hyperthyroidism258,259. Numerous studies have shown that vascular function and arterial stiffness, determined by pressure waveforms recorded from the radial artery of the forearm, are altered in patients with hypothyroidism and/or taking thyrotropic agents (260-266). The effects of insulin in hypothyroidism have also been assessed using blood flow measurements in the forearm with strain-gauge plethysmography267. However, it remains unclear how photoplethysmography compares with radial artery (forearm) measurements and other established techniques in diagnosing vascular dysfunction in thyroid disorders.
Evidence: Dyszkiewicz et al. used finger planimetric photoplethysmography to measure alterations in systolic-diastolic index (SDI) and finger microcirculation in thyroid dysfunction147. In 20 subjects with confirmed hypothyreosis, 21 subjects with subclinical hypothyreosis, and 25 healthy controls, serum thyroid hormones (thyrotropin and thyroxine) were measured and psychometric analyses performed using the Mittenecker and Thoman test. A finger cooling test was assessed qualitatively, and SDI measured using planimetric photoplethysmography. Compared to healthy controls, hypothyroid patients (both subclinical and overt) showed increases in SDI that concurred with psychometric indices and thyroid hormone levels. These results suggest that the finger cooling test, used with planimetric photoplethysmography, may be useful for screening patients for thyroid dysfunction.
Dyszkiewicz et al. evaluated alterations in finger microcirculation in thyroid dysfunction using finger planimetric photoplethysmography146. The study involved 201 total subjects: 171 with thyroid dysfunction (31 overt hyperthyroidism, 10 latent hyperthyroidism, 79 overt hypothyroidism, 22 latent hypothyroidism); finger SDI was measured with planimetric photoplethysmography. Compared to healthy controls (SDI=0.345), SDI was decreased in patients with overt hyperthyroidism (0.121) and latent hyperthyroidism (0.158), yet increased in patients with overt hypothyroidism (0.617) and latent hypothyroidism (0.471). SDI correlated with serum levels of free thyroxine and thyreotropine, as well as clinical symptoms. However, it is not clear whether digital photoplethysmography is a viable alternative to established thyroid tests for diagnosing thyroid dysfunction.
Angina pectoris (detection)Summary: Anginal attacks may have underlying disturbances in autonomic nerve activity, which may be monitored by digital plethysmography with auditory stimuli; thus, measurements of autonomic nervous tone by digital plethysmography may be useful in diagnosing angina and monitoring treatment.
Evidence: Matoba et al. conducted a diagnostic case series using digital plethysmography as a noninvasive method to correlate autonomic nerve activity with angina attack99. The study involved 45 patients with spontaneous angina (excluding Prinzmetal’s angina). Digital plethysmography was used with auditory stimuli. In 13 (28.9%) cases, patients reported angina symptoms (primarily in the morning) and exhibited increased levels of autonomic nerve activity and positive stress tests. Calcium antagonists were given orally to these 13 patients, resulting in complete cessation of angina symptoms. This study suggests that autonomic imbalances factor into angina attacks, and that monitoring autonomic nervous tone with digital plethysmography and auditory stimuli may be valuable for diagnosing and treating angina.
Autoimmune disease (detection of vascular abnormalities)Summary: Digital plethysmography has potential utility in detecting peripheral vascular damage in patients with autoimmune disorders. Reference values and standardization need to be further established.
Evidence: Kawase et al. used ECG and digital plethysmography in a diagnostic trial to evaluate cardiovascular function in patients with scleroderma Sjögren syndrome associated spectrum disorders (SSSD), systemic scleroderma (SSc), and systemic lupus erythematosus (SLE)100. Digital plethysmogram data suggested the presence of peripheral vascular damage in SSSD and SSc, and its severity was lower in SSSD than SSc. Abnormal cardiovascular function test results were less in SSSD
26
relative to SSc. The results suggest that cardiovascular function tests such as digital plethysmography are useful for detecting cardiovascular abnormalities in autoimmune diseases.
Frostbite (treatment decision aid)Summary: Digital plethysmography, combined with Doppler ultrasound, has been used to aid in therapeutic decisions for frostbite injuries. Its utility as a stand-alone treatment decision aid is not clear.
Evidence: Rakower et al. conducted a diagnostic trial using digital plethysmography and Doppler ultrasound as a treatment decision aid for frostbite injuries112. In 30 patients, frostbite injuries were treated with rapid warming in saline baths. The degrees of vascular response were determined using digital plethysmography and Doppler ultrasound mapping. In patients lacking hyperdynamic responses, vascular compromise was treated with sympathectomy (using intra-arterial reserpine) with beneficial results.
Hemorrhage (detection)Summary: Because hemorrhage may be difficult to detect before the bleeding site is apparent, monitoring techniques may be useful for early detection. Finger photoplethysmography may detect changes in blood volume that occur during hemorrhage; however, further research is necessary to validate the clinical utility of this technique for detecting hemorrhage.
Evidence: Middleton et al. conducted a prospective screening trial using the left ventricular ejection time derived from the digital photoplethysmographic waveform (LVET[p]) and PTT for detecting hemorrhage113. This study used blood donation as a model of controlled hemorrhage. In a convenience sample of 43 healthy volunteer blood donors, the ECG and the finger infrared photoplethysmogram were simultaneously measured; LVET(p), PTT and R-R interval (RRi) were computed. Measurements taken pre- and post-donation showed shortened LVET(p) values from 303±2 to 293±3ms (mean±SEM; p<0.01) and prolonged PTT values from 177±3 to 186±4ms (p<0.01). Progressive blood loss during donation caused progressive falling trends in LVET(p) (p<0.01) and rising trends in PTT (p<0.01). Decreases in RRi (p<0.01) were only observed in the second half of donation, however. These results suggest that digital photoplethysmography and ECG may be used for early detection of hemorrhage before a bleeding site becomes apparent.
Middleton et al. conducted a prospective screening trial using frequency spectrum analysis of the finger photoplethysmographic waveform variability (PPGV) for detecting hemorrhage, using blood donation as a model of controlled bleeding113. In 43 healthy blood donors, spectral analysis was performed on the finger infrared digital photoplethysmography waveform and on the ECG-derived RRi during blood donation. Low frequency (LF), mid frequency (MF) and high frequency (HF) bands of the spectrum of HRV were used to calculate spectral powers and the coherence-weighted cross-spectrum of PPGV. The sum of the sympathetic-related MF and respiratory HF powers of PPGV (in mean-scaled units) increased significantly during the second half of blood donation and after donation (p<0.01). PPGV spectral measures increased in 77% of subjects post-donation. When the LF power of HRV was normalized, it rose significantly during the second half of donation (p<0.01) but not after donation. These results indicate that despite the model’s limitations, PPGV may be a useful additional measure to assess hypovolemic responses. Further research is necessary to validate the clinical utility of this technique for detecting hemorrhage.
Renal disease (detection of secondary conditions)Summary: Preliminary clinical evidence suggests that digital photoplethysmography has diagnostic potential for secondary conditions in renal disease, such as arterial stiffness and steal phenomena.
Evidence: Sollinger et al. conducted a comparative diagnostic trial in patients with renal disease to compare arterial stiffness index derived from plethysmographic digital volume pulse (SI[DVP]) with aortic pulse wave velocity (PWV) derived from Doppler ultrasonography, and to correlate SI(DVP) with comorbidity141. Two groups of patients with end-stage renal disease (ESRD) were analyzed: 49 renal transplant (TX) patients and 48 hemodialysis (HD) patients. Photoplethysmography was performed on the index finger of either the dominant hand or the nonfistula arm, and computerized pulse curves were obtained. Comorbidity was determined with an established index. SI(DVP) varied among subjects by 5.7%. There was a significant correlation between SI(DVP) and PWV (r=0.66, p=0.001); however, SI(DVP) measurements were unreliable in 25% of HD patients and 6% of TX patients. SI(DVP) increased with age in both groups
27
(r=0.61, p<0.001); SI(DVP) also increased in TX patients with systolic blood pressure (r=0.53, p<0.025), mean arterial pressure (r=0.47, p<0.05), and pulse pressure (r=0.52, p=0.02). Comorbid status severity was highly associated with individual residuals of age-adjusted SI(DVP) in both groups (p<0.001). These results suggest that DVP may be used to assess arterial stiffness in most (but not all) ESRD patients, and that SI(DVP) correlates with comorbidity.
Van Hoek et al. conducted a multicenter comparative controlled diagnostic trial to test various techniques for assessing the incidence and severity of steal phenomena in hemodialysis patients142. The study was conducted on 120 patients receiving chronic hemodialysis with access to functional hemodialysis for more than six months. Exclusion criteria were refusal and cognitive or language handicap. Steal assessment was performed on a pilot subpopulation of 14 patients identified as having steal by a questionnaire. The assessment techniques used were physical examination, arterial blood pressure, skin temperature, digital oxygenation, grip strength, and plethysmography; contralateral arms were used as controls. Plethysmography was used on the index fingers of both hands to determine digital pressures. The apparatus used was the VasoGuard Nicolet, 8MHz (Scimed Ltd, Bristol, UK), and digital pressures obtained by wrapping an inflatable cuff around the proximal phalanx of the index finger and positioning a sensor on the palmar side of the distal phalanx. The ratio of finger pressure to systolic blood pressure was the digital brachial index (DBI). In the 14 patients studied, the mean DBI was 0.6; a range of 0.44-1.08 indicates that even high DBIs may correspond with steal. The authors suggested that photoplethysmography may be the only assessment technique with diagnostic potential for steal in hemodialysis, with DBI=0.6 reported as the cut-off point, 100% sensitivity, and 63-76% specificity.
Stress (detection)Summary: Digital plethysmography appears to detect some (but not all) forms of hemodynamic stress. This use needs to be further validated before implementation in clinical settings.
Evidence: Linder et al. conducted a screening trial to test noninvasive detection of hemodynamic stress of exercise using photoplethysmographic techniques145. Under the hypothesis that cardiac stress induces detectable changes in blood flow, 11 healthy subjects performed the Bruce Protocol treadmill test low frequency. Photoplethysmographs were measured by pulse oximeter. Low frequency waves (f=0.05-0.2 Hz) were detected in blood flow in the forehead and ear, but not in the finger. Digital plethysmography may not be a reliable technique for detecting exercise-induced hemodynamic stress to the vasculature.
Huiku et al. conducted a diagnostic trial using finger photoplethysmography and ECG to assess surgical stress during general anesthesia268. The technique was developed in 60 female patients and validated in 12 female patients who had elective surgery with general anesthesia (propofol-remifentanil target controlled). Waveforms were collected during anesthesia and extracted offline; stimulus intensity and remifentanil concentration were used to estimate total surgical stress (TSS). These data were used to develop a surgical stress index (SSI), which was computed as a combination of normalized heart beat interval (HBI[norm]) and plethysmographic pulse wave amplitude (PPGA[norm]) using the equation SSI=100-(0.7*PPGA[norm]+0.3*HBI[norm]). The SSI was validated in 12 patients before and during surgery. SSI increased at the incision, and the elevation was sustained throughout surgery. The rise in SSI was also inversely proportional to remifentanil concentration. These results suggest that SSI responds to surgical stimuli and anesthesia; however, this technique requires further validation before its use during surgery or anesthesia.
Vascular reconstruction (operative decision aid)Summary: Digital plethysmography is a valuable perioperative decision aid in vascular reconstruction surgeries, and has been used since at least the 1950s to monitor surgery of degenerative arterial disease148. Although it remains unclear whether it should be used as a sole operative aid, it is a useful adjunct to clinical evaluation.
Evidence: Rodriguez et al. conducted a retrospective case series to validate the use of Doppler ultrasound and digital plethysmography to non-invasively determine whether a radial artery is suitable for harvest for coronary artery bypass grafting (CABG)149. Retrospective analysis was performed on 346 arms of 187 patients undergoing CABG. Radial arteries were excluded from harvest for anatomical abnormalities (<2mm in size, diffuse calcifications) and insufficient perfusion during radial artery perfusion (>40% reduction on digital pressure, non-reversal of radial artery flow, or minimal increase in ulnar velocity). In 187 patients, 94 arms were excluded from harvest for anatomical abnormalities (1.5%), diffuse calcifications (8.7%), congenital anomalies (2.3%), or radial artery occlusion (0.3%). Digital plethysmography detected non-reversal of flow (7.3%), abnormal digital pressure (5.5%), and inappropriate ulnar velocity increases (1.7%). Of 116 radial
28
arteries harvested, there were no incidences of hand ischemia, and none of the patients required hand rehabilitation. These results suggest that digital plethysmography is a valuable tool to determine the suitability of a radial artery for CABG.
Rothkopf et al. reviewed case reports of ulnar artery aneurysms to evaluate the success of microvascular reconstruction150. In ten cases of ulnar artery aneurysm in nine male patients from 1978 to 1988, intraoperative digital plethysmography was useful in determining the necessity for microvascular reconstruction.
Critical illness (cardiac monitoring)Summary: Although the noninvasive nature of digital plethysmography makes it an attractive method for monitoring cardiac parameters in critically ill patients, its potential inaccuracy in hemodynamically unstable patients may preclude its use as a sole hemodynamic monitoring device in critical care.
Evidence: Stover et al. conducted a diagnostic trial to compare noninvasive digital plethysmography with the standard invasive cardiac monitoring system in critical care79. Ten critically ill patients were continuously monitored using the Nexfin HD system, which noninvasively monitors blood pressure and cardiac output based on pulsatile unloading of finger arterial walls via an inflatable finger cuff. Measurements were simultaneously obtained using standard invasive arterial catheters. Mean arterial pressures of the two methods had a correlation coefficient r=0.67 with -2mmHg bias and two standard deviations±16mmHg. Cardiac output measures had a correlation of r=0.83 with 0.23/min bias, two standard deviations of +/-2.1/min, and 29% error rate. While the noninvasive plethysmographic technique may improve the safety of cardiac monitoring, it was not as reliable as the standard invasive technique and is thus far not recommended for critical care.
Preeclampsia (blood pressure monitoring)Summary: Although the noninvasive nature of digital plethysmography makes it an attractive method for monitoring blood pressure in preeclamptic pregnant women, its potential inaccuracy may preclude its use as a sole hemodynamic monitoring device in these patients.
Evidence: Elvan-Taşpinar conducted a comparative, case-controlled diagnostic trial to compare the Finometer™ and the previously validated SpaceLabs 90207 with standard auscultatory blood pressure measurements during pregnancy76. The study was conducted on 123 pregnant women (54 normotensive, 31 preeclamptic, and 38 hypertensive women). Guidelines from the British Hypertension Society (BHS) and Association for the Advancement of Medical Instrumentation (AAMI) were followed for independent validation of the Finometer™. Automated readings were made using the Finometer™ and the SpaceLabs 90207; the results were compared to auscultatory blood pressure measurements, and analyzed using Bland-Altman plots, BHS grades, mean pressure differences and 95% limits of agreement. BHS grades were used to rate the Finometer™ for all women (grades C/D), as well as for normotensive (C/B), preeclamptic (D/D), and hypertensive (D/D) women). The Finometer™ only met AAMI criteria for diastolic blood pressure for normotensive pregnant women. The SpaceLabs monitor grades were consistent with an earlier validation study. These results do not support using the Finometer™ for determining absolute blood pressures in pregnant women, particularly preeclamptic or hypertensive pregnant women.
Formulary: Brands used in clinical trails/third-party testingProducts/supplies/equipment of particular brands used in statistically significant trials:
2300 Finapres® digital noninvasive blood pressure monitor (Ohmeda, Englewood, CO, USA; TNO Biomedical Instrumentation, Amsterdam, Netherlands) (66;212;241); Digimatic® 2000 plethysmograph (Medimatic)137; EndoPat finger plethysmograph (Itamar)96; Finometer™ (Finapres® Measurement Systems (FMS), Arnhem, Netherlands) (209;212;269;270) with Beatscope® software for deriving the stroke volume from the blood pressure waveform76,271; Masimo SET® Rad-9® and Novametrix Oxypleth® oximeters with photoplethysmographic phase characteristics61; Nexfin HD (BMEYE B.V, Amsterdam, Netherlands)79; PulseTrace PCA 2™ (Micro Medical)65; Portapres® (TNO-BMI, Amsterdam)214,272; Pulse Trace System™ digital photoplethysmograph (Micro Medical Ltd., Gillingham, Kent, UK)65,102,152; SpaceLabs photoplethysmographic probe76,273; VasoGuard Nicolet finger plethysmograph, 8MHz (Scimed Ltd, Bristol, UK)142; WatchPAT100 (Itamar Medical; Caesarea, Israel)95,246-252.

29
Synonyms/Common Names/Related TermsAccelerated plethysmography (APG), air plethysmography, arterial blood oxygen saturation (SaO2), autonomous nervous responses, baroreflex sensitivity (BRS), Beatscope®, beat-to-beat blood pressure, Beer-Lambert pulse oximetry model, bilateral photoplethysmography, cardiac autonomic nervous modulation, Digimatic®, digital arterial blood flow, digital arteritis, digital photo-plethysmograph analyzer (DPA), digital photoplethysmography (D-PPG), digital plethysmography (DPG), digital pneumatic plethysmography (DPP), digital pressure index (DPI), digital pulse contour analysis, digital pulse plethysmography, digital volume pulse (DVP), dual-channel photoplethysmography, DVP-derived stiffness index (SI[DVP]), electrocardiographic-triggered venous-occlusion plethysmograph, EndoPat, Finapres®, finger arterial pressure, finger photoplethysmography (FPPG), finger plethysmography, finger reactive hyperemia, finger volume plethysmography, fingertip blood flow measured by mercury strain gauge plethysmography with venous occlusion, finger-to-toe distance, Finometer™, functional PPG (fPPG), green light photoplethysmography, infrared finger plethysmography, infrared light transmitted through a fingertip (LTF), infra-red photo plethysmography, light plethysmography, light reflection rheography, light reflex plethysmography of the finger, light transmission plethysmography, Masimo SET® Rad-9, maximal digital pulse, mercury gauge method of digital plethysmography, mercury strain gauge plethysmography, modern infrared photosensors (IPs), multi-channel photoplethysmography, Nexfin HD, noncontact simultaneous dual wavelength photoplethysmography, Novametrix Oxypleth®, optoelectronic plethysmography, oximeter with photoplethysmographic phase characteristics, PCA 2, Penaz method, peripheral arterial tone (PAT), peripheral arterial tonometry (PAT), photocell plethysmography, photo-electric plethysmography (PHELP), photoelectric plethysmography, photoplethysmograph finger probe, photoplethysmography (PPG), photoplethysmography toe pulse measurement, piezoelectric finger plethysmography, planimetric photoplethysmography, plethysmogram, plethysmograph (PTG), plethysmographic finger blood pressure measurement device, Portapres®, pulse oximetric finger plethysmography, pulse oximetry, Pulse Trace, pulse transit time (PTT), pulse wave analysis, pulse wave transit time (PWTT), pulse wave velocity (PWV), qualitative digital plethysmography, reflected infrared light photoplethysmography, R-wave-gated photo-plethysmography (RWPP), second derivative of the finger photoplethysmogram (SDPTG), servo-controlled infrared finger plethysmography, servo-plethysmomanometry, SpaceLabs, strain gauge plethysmography, toe-finger time delay change, vascular reactivity, vascular transit time (VTT), VasoGuard Nicolet, venous occlusion plethysmography, venous plethysmography, WatchPAT100.
Not included in this reviewAbsolute transmitted light plethysmography for assessing dental pulp health1; acoustic plethysmography for measuring specific airway resistance2; air displacement plethysmography for assessing body composition3-5) air displacement plethysmography to estimate lung volume6air plethysmography to measure venous outflow in the limbs7; air pressure chest wall plethysmography to measure heart rate and chest wall motion8; ambulatory inductive plethysmography to evaluate respiratory function9; automated respiratory inductive plethysmography, a measure of breathing10; barometric whole body plethysmography (BWBP) to assess airflow11; body plethysmography in respiratory analysis12-14; clitoral photoplethysmography for measuring sexual arousal in women15; computed strain-gauge plethysmography (CSGP) used to screen for deep venous thrombosis (DVT)16-18; constant volume plethysmography, a respiratory test19; ear plethysmography20; electric field plethysmography (EFPG) to measure respiration and cardiac activity21 esophageal photoplethysmography22; flowmetric plethysmography for measuring airway inflammation23forearm plethysmography24,25; genital plethysmography; hybrid computed tomography (CT) and single photon emission CT (SPECT/CT-) plethysmography used to measure bone and soft tissue blood flow26 impedance plethysmography, used to assess distal veins (often in the legs) and for diagnosing deep vein thrombosis7 ; inductance (or inductive) plethysmography, used to measure bloating and abdominal girth in irritable bowel syndrome (IBS)27 and to measure volume-targeted ventilation for leak compensation28 ; infrared plethysmography performed on non-digital body parts, such as in measuring blood volume pulse (BVP) biofeedback therapy29; labial photoplethysmography for measuring sexual responses in women30; limb (e.g., forearm, calf) plethysmography; lung plethysmography; micro-plethysmography to measure small volume displacement in the airway3; optoelectronic plethysmography (OEP) to assess chest wall surface motion32; oximeter plethysmography in estimating airway obstruction33; penile plethysmography, which is used in phallometry as an objective measure of sexual response and used controversially to assess erectile response in sex offenders34-37; portable respiratory inductive plethysmography (RIP), a noninvasive method to monitor breathing patterns38; pulse oximeter plethysmography for measuring respiratory parameters39; pulse-volume plethysmography to measure penile bloodflow40 ; remote ambient light

30
photo-plethysmography for measuring vascular skin lesions and remotely sensing vital signs41; respiratory inductance plethysmography (RIP) for measuring respiratory parameters42 , speaking43 , and chest wall motion44 ; respiratory inductive plethysmography for respiratory monitoring45; serial impedance plethysmography for diagnosing acute deep vein thrombosis in the limbs46; strain gauge plethysmography of the limbs7; transabdominal photoplethysmography to measure fetal heart rate47; vaginal photoplethysmography, which is used to measure sexual arousal in women48; venous congestion plethysmography of the limbs49; venous occlusion plethysmography of the limbs (e.g., calf, leg, forearm)50-53; whole body air displacement plethysmography (ADP) for measuring body volume and composition54,55; whole body plethysmography for measuring respiratory parameters56,57.
Author InformationAttribution/MONOGRAPH Currency
Last Updated: 11/20/09.
This information was compiled and reviewed by Dr. Steven M. Helschien. Authors/Editors: Wendy Chao, PhD (Natural Standard Research Collaboration); Catherine Ulbricht, PharmD (Massachusetts General Hospital).
Blinded Peer-Review: Natural Standard Editorial Board.
Bibliography1 Kakino S, Takagi Y, Takatani S. Absolute transmitted light plethysmography for assessment of dental pulp vitality through quantification of pulp chamber hematocrit by a
three-layer model. J Biomed Opt 2008 Sep;13(5):054023.2 Reynolds JS, Johnson VJ, Frazer DG. Unrestrained acoustic plethysmograph for measuring specific airway resistance in mice. J Appl Physiol 2008 Aug;105(2):711-7.3 Fields DA, Goran MI, McCrory MA. Body-composition assessment via air-displacement plethysmography in adults and children: a review. Am J Clin Nutr 2002
Mar;75(3):453-67.4 Fields DA, Hunter GR. Monitoring body fat in the elderly: application of air-displacement plethysmography. Curr Opin Clin Nutr Metab Care 2004 Jan;7(1):11-4.5 Buchholz AC, Majchrzak KM, Chen KY, Shankar SM, Buchowski MS. Use of air displacement plethysmography in the determination of percentage of fat mass in african
american children. Pediatr Res 2004 Jul;56(1):47-54.6 Higgins PB, Silva AM, Sardinha LB, Hull HR, Goran MI, Gower BA, et al. Validity of new child-specific thoracic gas volume prediction equations for air-displacement
plethysmography. BMC Pediatr 2006;6:18.7 Locker T, Goodacre S, Sampson F, Webster A, Sutton AJ. Meta-analysis of plethysmography and rheography in the diagnosis of deep vein thrombosis. Emerg Med J 2006
Aug;23(8):630-5.8 Perring S, Jones E. Simultaneous measurement of instantaneous heart rate and chest wall plethysmography in short-term, metronome guided heart rate variability studies:
suitability for assessment of autonomic dysfunction. Physiol Meas 2003 Aug;24(3):745-51.9 Grossman P, Spoerle M, Wilhelm FH. Reliability of respiratory tidal volume estimation by means of ambulatory inductive plethysmography. Biomed Sci Instrum 2006;42:193-
8.10 Brown KA, Aoude AA, Galiana HL, Kearney RE. Automated respiratory inductive plethysmography to evaluate breathing in infants at risk for postoperative apnea. Can J
Anaesth 2008 Nov;55(11):739-47.11 Hirt RA, Vondrakova K, de Arespacochaga AG, Gutl A, van den Hoven R. Effects of cadmium chloride inhalation on airflow limitation to histamine, carbachol and adenosine
5’-monophosphate assessed by barometric whole body plethysmography in healthy dogs. Vet J 2007 Jan;173(1):62-72.12 Badier M, Guillot C, Dubus JC. Bronchial challenge with carbachol in 3-6-year-old children: body plethysmography assessments. Pediatr Pulmonol 1999 Feb;27(2):117-23.13 Olaguibel JM, Alvarez-Puebla MJ, Anda M, Gomez B, Garcia BE, Tabar AI, et al. Comparative analysis of the bronchodilator response measured by impulse oscillometry
(IOS), spirometry and body plethysmography in asthmatic children. J Investig Allergol Clin Immunol 2005;15(2):102-6.14 Schlesinger AE, White DK, Mallory GB, Hildeboldt CF, Huddleston CB. Estimation of total lung capacity from chest radiography and chest CT in children: comparison with
body plethysmography. AJR Am J Roentgenol 1995 Jul;165(1):151-4.15 Gerritsen J, van der Made F, Bloemers J, van HD, Kleiverda G, Everaerd W, et al. The clitoral photoplethysmograph: a new way of assessing genital arousal in women. J Sex Med
2009 Jun;6(6):1678-87.16 Goddard AJ, Chakraverty S, Wright J. Computer assisted strain-gauge plethysmography is a practical method of excluding deep venous thrombosis. Clin Radiol 2001
Jan;56(1):30-4.17 Flanagan DE, Creasy T, Thomas P, Cavan D, Armitage M. Computer-assisted venous occlusion plethysmography in the diagnosis of acute deep venous thrombosis. QJM 2000
May;93(5):277-82.18 Pazzagli M, Mazzantini D, Desideri M, Palla A. Computerized impedance plethysmography in the diagnosis of delayed deep vein thrombosis after total hip replacement.
Monaldi Arch Chest Dis 2000 Apr;55(2):106-9.19 Singh D, Tal-Singer R, Faiferman I, Lasenby S, Henderson A, Wessels D, et al. Plethysmography and impulse oscillometry assessment of tiotropium and ipratropium bromide;
a randomized, double-blind, placebo-controlled, cross-over study in healthy subjects. Br J Clin Pharmacol 2006 Apr;61(4):398-404.20 Awad AA, Ghobashy MA, Ouda W, Stout RG, Silverman DG, Shelley KH. Different responses of ear and finger pulse oximeter wave form to cold pressor test. Anesth Analg
2001 Jun;92(6):1483-6.21 Ruhsam C, Pfutzner H, Nopp P, Nakesch H, Frais-Kolbl H, Marktl W. Time-frequency spectral analysis of electric field plethysmography signals. Med Prog Technol
1995;21(1):17-28.22 Kyriacou PA, Moye AR, Gregg A, Choi DM, Langford RM, Jones DP. A system for investigating oesophageal photoplethysmographic signals in anaesthetised patients. Med
Biol Eng Comput 1999 Sep;37(5):639-43.23 Nolen-Walston RD, Kuehn H, Boston RC, Mazan MR, Wilkins PA, Bruns S, et al. Reproducibility of airway responsiveness in horses using flowmetric plethysmography and
histamine bronchoprovocation. J Vet Intern Med 2009 May;23(3):631-5.24 Lenders J, Janssen GJ, Smits P, Thien T. Role of the wrist cuff in forearm plethysmography. Clin Sci (Lond) 1991 May;80(5):413-7.

31
25 Quinn RJ. Wrist cuffs for forearm plethysmography. Ir J Med Sci 1967 Oct;6(502):465-71.26 Dayan L, Keidar Z, Israel O, Milloul V, Sachs J, Jacob G. SPECT/CT-plethysmography--non-invasive quantitation of bone and soft tissue blood flow. J Orthop Surg Res
2008;3:36.27 Reilly BP, Bolton MP, Lewis MJ, Houghton LA, Whorwell PJ. A device for 24 hour ambulatory monitoring of abdominal girth using inductive plethysmography. Physiol Meas
2002 Nov;23(4):661-70.28 Andrieu MC, Quentin C, Orlikowski D, Desmarais G, Isabey D, Louis B, et al. Inductive plethysmography to control volume-targeted ventilation for leak compensation.
Intensive Care Med 2008 Jun;34(6):1150-5.29 Speckenbach U, Gerber WD. Reliability of infrared plethysmography in BVP biofeedback therapy and the relevance for clinical application. Appl Psychophysiol Biofeedback
1999 Dec;24(4):261-5.30 Prause N, Cerny J, Janssen E. The labial photoplethysmograph: a new instrument for assessing genital hemodynamic changes in women. J Sex Med 2005 Jan;2(1):58-65.31 Tiddens HA, Holland WP, de VJ, de JJ. The micro-plethysmograph: a new device to measure small volume displacements by isolated human airway segments. J Pharmacol
Toxicol Methods 1998 Jul;40(1):13-20.32 Dellaca’ RL, Ventura ML, Zannin E, Natile M, Pedotti A, Tagliabue P. Measurement of total and compartmental lung volume changes in newborns by optoelectronic
plethysmography. Pediatr Res 2010 Jan;67(1):11-6.33 Arnold DH, Spiro DM, Desmond RA, Hagood JS. Estimation of airway obstruction using oximeter plethysmograph waveform data. Respir Res 2005;6:65.34 Danjou P, Lacomblez L, Warot D, Puech AJ. Assessment of erectogenic drugs by numeric plethysmography. J Pharmacol Methods 1989 Mar;21(1):61-9.35 Simon WT, Schouten PG. Plethysmography in the assessment and treatment of sexual deviance: an overview. Arch Sex Behav 1991 Feb;20(1):75-91.36 Simon WT, Schouten PG. The plethysmograph reconsidered: comments on Barker and Howell. Bull Am Acad Psychiatry Law 1993;21(4):505-12.37 Barker JG, Howell RJ. The plethysmograph: a review of recent literature. Bull Am Acad Psychiatry Law 1992;20(1):13-25.38 Brullmann G, Fritsch K, Thurnheer R, Bloch KE. Respiratory monitoring by inductive plethysmography in unrestrained subjects using position sensor-adjusted calibration.
Respiration 2010;79(2):112-20.39 Wertheim D, Olden C, Savage E, Seddon P. Extracting respiratory data from pulse oximeter plethysmogram traces in newborn infants. Arch Dis Child Fetal Neonatal Ed 2009
Jul;94(4):F301-F303.40 Lavoisier P, Barbe R, Gally M. Validation of a continuous penile blood-flow measurement by pulse-volume-plethysmography. Int J Impot Res 2002 Apr;14(2):116-20.41 Verkruysse W, Svaasand LO, Nelson JS. Remote plethysmographic imaging using ambient light. Opt Express 2008 Dec 22;16(26):21434-45.42 Brooks LJ, DiFiore JM, Martin RJ. Assessment of tidal volume over time in preterm infants using respiratory inductance plethysmography, The CHIME Study Group.
Collaborative Home Infant Monitoring Evaluation. Pediatr Pulmonol 1997 Jun;23(6):429-33.43 Wilhelm FH, Handke EM, Roth WT. Detection of speaking with a new respiratory inductive plethysmography system. Biomed Sci Instrum 2003;39:136-41.44 Warren RH, Horan SM, Robertson PK. Chest wall motion in preterm infants using respiratory inductive plethysmography. Eur Respir J 1997 Oct;10(10):2295-300.45 Zhang Z, Bi Y, Yu M, Wu T, Li R. [Detecting sleep apnea/hypopnea events with a wearable respiratory inductive plethysmograph system]. Sheng Wu Yi Xue Gong Cheng Xue
Za Zhi 2008 Apr;25(2):318-22.46 Heijboer H, Buller HR, Lensing AW, Turpie AG, Colly LP, ten Cate JW. A comparison of real-time compression ultrasonography with impedance plethysmography for the
diagnosis of deep-vein thrombosis in symptomatic outpatients. N Engl J Med 1993 Nov 4;329(19):1365-9.47 Gan KB, Zahedi E, Mohd Ali MA. Transabdominal fetal heart rate detection using NIR photopleythysmography: instrumentation and clinical results. IEEE Trans Biomed Eng
2009 Aug;56(8):2075-82.48 Laan E, van Driel EM, van Lunsen RH. Genital responsiveness in healthy women with and without sexual arousal disorder. J Sex Med 2008 Jun;5(6):1424-35.49 Bauer A, Bruegger D, Gamble J, Christ F. Influence of different cuff inflation protocols on capillary filtration capacity in human calves -- a congestion plethysmography study. J
Physiol 2002 Sep 15;543(Pt 3):1025-31.50 Chuah SS, Woolfson PI, Pullan BR, Lewis PS. Plethysmography without venous occlusion for measuring forearm blood flow: comparison with venous occlusive method. Clin
Physiol Funct Imaging 2004 Sep;24(5):296-303.51 Groothuis JT, van VL, Kooijman M, Hopman MT. Venous cuff pressures from 30 mmHg to diastolic pressure are recommended to measure arterial inflow by
plethysmography. J Appl Physiol 2003 Jul;95(1):342-7.52 Kooijman M, Poelkens F, Rongen GA, Smits P, Hopman MT. Leg blood flow measurements using venous occlusion plethysmography during head-up tilt. Clin Auton Res 2007
Apr;17(2):106-11.53 Leslie SJ, Attina T, Hultsch E, Bolscher L, Grossman M, Denvir MA, et al. Comparison of two plethysmography systems in assessment of forearm blood flow. J Appl Physiol
2004 May;96(5):1794-9.54 Dewit O, Fuller NJ, Fewtrell MS, Elia M, Wells JC. Whole body air displacement plethysmography compared with hydrodensitometry for body composition analysis. Arch Dis
Child 2000 Feb;82(2):159-64.55 Lee SY, Gallagher D. Assessment methods in human body composition. Curr Opin Clin Nutr Metab Care 2008 Sep;11(5):566-72.56 Carry PY, Baconnier P, Eberhard A, Cotte P, Benchetrit G. Evaluation of respiratory inductive plethysmography: accuracy for analysis of respiratory waveforms. Chest 1997
Apr;111(4):910-5.57 Vilozni D, Efrati O, Hakim F, Adler A, Livnat G, Bentur L. FRC measurements using body plethysmography in young children. Pediatr Pulmonol 2009 Sep;44(9):885-91.58 American College of Cardiology Cardiovascular Technology Assessment Committee. Heart rate variability for risk stratification of life-threatening arrhythmias. J Am Coll
Cardiol 1993 Sep;22(3):948-50.59 Parati G, Di RM, Ulian L, Santucciu C, Girard A, Elghozi JL, et al. Clinical relevance blood pressure variability. J Hypertens Suppl 1998 Aug;16(3):S25-S33.60 Thayer JF, Yamamoto SS, Brosschot JF. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int J Cardiol 2010 May
28;141(2):122-31.61 Foo JY, Wilson SJ, Dakin C, Williams G, Harris MA, Cooper D. Variability in time delay between two models of pulse oximeters for deriving the photoplethysmographic
signals. Physiol Meas 2005 Aug;26(4):531-44.62 Hartmann B, Bassenge E. [Noninvasive, continuous measurement of finger artery pressure with the servo-plethysmo-manometer Finapres]. Herz 1989 Aug;14(4):251-9.63 Alty SR, Angarita-Jaimes N, Millasseau SC, Chowienczyk PJ. Predicting arterial stiffness from the digital volume pulse waveform. IEEE Trans Biomed Eng 2007
Dec;54(12):2268-75.64 Kim EJ, Park CG, Park JS, Suh SY, Choi CU, Kim JW, et al. Relationship between blood pressure parameters and pulse wave velocity in normotensive and hypertensive subjects:
invasive study. J Hum Hypertens 2007 Feb;21(2):141-8.65 Gunarathne A, Patel JV, Hughes EA, Lip GY. Measurement of stiffness index by digital volume pulse analysis technique: clinical utility in cardiovascular disease risk
stratification. Am J Hypertens 2008 Aug;21(8):866-72.66 Fuhrman TM, Reilley TE, Pippin WD. Comparison of digital blood pressure, plethysmography, and the modified Allen’s test as means of evaluating the collateral circulation to
the hand. Anaesthesia 1992 Nov;47(11):959-61.67 Naghavi M, Falk E, Hecht HS, Jamieson MJ, Kaul S, Berman D, et al. From vulnerable plaque to vulnerable patient--Part III: Executive summary of the Screening for Heart
Attack Prevention and Education (SHAPE) Task Force report. Am J Cardiol 2006 Jul 17;98(2A):2H-15H.68 Dennis MJ. Plethysmography: the new wave in haemodynamic monitoring--a review of clinical applications. Aust Crit Care 2000 Mar;13(1):14-20.69 Shelley KH. Photoplethysmography: beyond the calculation of arterial oxygen saturation and heart rate. Anesth Analg 2007 Dec;105(6 Suppl):S31-6, tables.70 Kreibig SD, Wilhelm FH, Roth WT, Gross JJ. Cardiovascular, electrodermal, and respiratory response patterns to fear- and sadness-inducing films. Psychophysiology 2007
Sep;44(5):787-806.

32
71 Deegan BM, O’Connor M, Lyons D, OLaighin G. Development and evaluation of new blood pressure and heart rate signal analysis techniques to assess orthostatic hypotension and its subtypes. Physiol Meas 2007 Nov;28(11):N87-102.
72 van der Velde N, van den Meiracker AH, Stricker BH, van der Cammen TJ. Measuring orthostatic hypotension with the Finometer device: is a blood pressure drop of one heartbeat clinically relevant? Blood Press Monit 2007 Jun;12(3):167-71.
73 Herdenstam CG. Digital plethysmography in psoriasis. Acta Derm Venereol 1959;39(1):41-6.74 Zahedi E, Jaafar R, Ali MA, Mohamed AL, Maskon O. Finger photoplethysmogram pulse amplitude changes induced by flow-mediated dilation. Physiol Meas 2008
May;29(5):625-37.75 Chemla D, Teboul JL, Richard C. Noninvasive assessment of arterial pressure. Curr Opin Crit Care 2008 Jun;14(3):317-21.76 Elvan-Taspinar A, Uiterkamp LA, Sikkema JM, Bots ML, Koomans HA, Bruinse HW, et al. Validation and use of the Finometer for blood pressure measurement in normal,
hypertensive and pre-eclamptic pregnancy. J Hypertens 2003 Nov;21(11):2053-60.77 Akkermans J, Diepeveen M, Ganzevoort W, van Montfrans GA, Westerhof BE, Wolf H. Continuous non-invasive blood pressure monitoring, a validation study of Nexfin in a
pregnant population. Hypertens Pregnancy 2009 May;28(2):230-42.78 Smith SM, Potter JF, Samani NJ, Sammons EL, Rathbone WE, Bentley S, et al. Are baroreflex events detected by invasive and non-invasive techniques coincident? Clin Physiol
Funct Imaging 2008 Jul;28(4):262-9.79 Stover JF, Stocker R, Lenherr R, Neff TA, Cottini SR, Zoller B, et al. Noninvasive cardiac output and blood pressure monitoring cannot replace an invasive monitoring system
in critically ill patients. BMC Anesthesiol 2009;9:6.80 Maestri R, Pinna GD, Robbi E, Capomolla S, La Rovere MT. Noninvasive measurement of blood pressure variability: accuracy of the Finometer monitor and comparison with
the Finapres device. Physiol Meas 2005 Dec;26(6):1125-36.81 Foo JY, Lim CS. Pulse transit time as an indirect marker for variations in cardiovascular related reactivity. Technol Health Care 2006;14(2):97-108.82 Naschitz JE, Bezobchuk S, Mussafia-Priselac R, Sundick S, Dreyfuss D, Khorshidi I, et al. Pulse transit time by R-wave-gated infrared photoplethysmography: review of the
literature and personal experience. J Clin Monit Comput 2004 Dec;18(5-6):333-42.83 Takazawa K, Tanaka N, Fujita M, Matsuoka O, Saiki T, Aikawa M, et al. Assessment of vasoactive agents and vascular aging by the second derivative of photoplethysmogram
waveform. Hypertension 1998 Aug;32(2):365-70.84 Tardy Y, Meister JJ, Perret F, Brunner HR, Arditi M. Non-invasive estimate of the mechanical properties of peripheral arteries from ultrasonic and photoplethysmographic
measurements. Clin Phys Physiol Meas 1991 Feb;12(1):39-54.85 Penaz J. Photoelectric measurement of blood pressure, volume and flow in the finger. Digest of the 10th International Conference on Medical, and Biological Engineering.
Dresden: International Federation for Medical and Biological Engineering; 1973. p. 904.86 Nilsson L, Goscinski T, Kalman S, Lindberg LG, Johansson A. Combined photoplethysmographic monitoring of respiration rate and pulse: a comparison between different
measurement sites in spontaneously breathing subjects. Acta Anaesthesiol Scand 2007 Oct;51(9):1250-7.87 Eberhardt RT, Raffetto JD. Chronic venous insufficiency. Circulation 2005 May 10;111(18):2398-409.88 Fronek A. Photoplethysmography in the diagnosis of venous disease. Dermatol Surg 1995 Jan;21(1):64-6.89 Maeda Y, Sekine M, Tamura T, Moriya A, Suzuki T, Kameyama K. Comparison of reflected green light and infrared photoplethysmography. Conf Proc IEEE Eng Med Biol Soc
2008;2008:2270-2.90 de Wilde RB, Schreuder JJ, van den Berg PC, Jansen JR. An evaluation of cardiac output by five arterial pulse contour techniques during cardiac surgery. Anaesthesia 2007
Aug;62(8):760-8.91 Michaux B, Vanhoutte JJ, Jaffrin MY, Fontenier G. Calibration-free mercury strain-gauge plethysmograph. Med Biol Eng Comput 1979 Jul;17(4):539-42.92 Eagan CJ. The physics of the mercury strain gauge and of its use in digital plethysmography. Tech Note Arct Aeromed Lab (US ) 1961 Feb;60-17:1-14.93 Chen YT, Chiayg CY, Wang MC, Tsai WC, Wu HT, Liu CC. Serial changes of pulse wave velocity and correlations with hemodynamic parameters during general anesthesia.
Acta Anaesthesiol Taiwan 2006 Dec;44(4):193-8.94 Silke B, McAuley D. Accuracy and precision of blood pressure determination with the Finapres: an overview using re-sampling statistics. J Hum Hypertens 1998 Jun;12(6):403-9.95 Schnall RP, Shlitner A, Sheffy J, Kedar R, Lavie P. Periodic, profound peripheral vasoconstriction--a new marker of obstructive sleep apnea. Sleep 1999 Nov 1;22(7):939-46.96 Faizi AK, Kornmo DW, Agewall S. Evaluation of endothelial function using finger plethysmography. Clin Physiol Funct Imaging 2009 Sep;29(5):372-5.97 Sharif-Kashani B, Behzadnia N, Shahabi P. Comparing results of digital photoplethysmography in two groups of chronic obstructive pulmonary disease patients with and
without high pulmonary artery pressure. Phlebology 2008;23(3):125-9.98 Kura N, Fujikawa T, Tochikubo O. New finger-occlusion plethysmograph for estimating peripheral blood flow and vascular resistance. Circ J 2008 Aug;72(8):1329-35.99 Matoba T, Ohkita Y, Chiba M, Toshima H. Noninvasive assessment of the autonomic nervous tone in angina pectoris: an application of digital plethysmography with auditory
stimuli. Angiology 1983 Feb;34(2):127-36.100 Kawase H, Maeda M, Horai T, Wada H, Kitajima Y, Seishima M. [Significance of the cardiovascular function tests in patients with collagen diseases, especially for SSc
(systemic scleroderma)]. Rinsho Byori 2004 May;52(5):401-5.101 Millasseau SC, Kelly RP, Ritter JM, Chowienczyk PJ. Determination of age-related increases in large artery stiffness by digital pulse contour analysis. Clin Sci (Lond) 2002
Oct;103(4):371-7.102 Salvi P, Magnani E, Valbusa F, Agnoletti D, Alecu C, Joly L, et al. Comparative study of methodologies for pulse wave velocity estimation. J Hum Hypertens 2008
Oct;22(10):669-77.103 Chen JY, Tsai WC, Wu MS, Hsu CH, Lin CC, Wu HT, et al. Novel Compliance Index derived from digital volume pulse associated with risk factors and exercise capacity in
patients undergoing treadmill exercise tests. J Hypertens 2007 Sep;25(9):1894-9.104 Tsai WC, Chen JY, Wang MC, Wu HT, Chi CK, Chen YK, et al. Association of risk factors with increased pulse wave velocity detected by a novel method using dual-channel
photoplethysmography. Am J Hypertens 2005 Aug;18(8):1118-22.105 Otsuka T, Kawada T, Katsumata M, Ibuki C, Kusama Y. Independent determinants of second derivative of the finger photoplethysmogram among various cardiovascular risk
factors in middle-aged men. Hypertens Res 2007 Dec;30(12):1211-8.106 Hashimoto J, Watabe D, Kimura A, Takahashi H, Ohkubo T, Totsune K, et al. Determinants of the second derivative of the finger photoplethysmogram and brachial-ankle
pulse-wave velocity: the Ohasama study. Am J Hypertens 2005 Apr;18(4 Pt 1):477-85.107 Kogure D, Iwamoto T, Takasaki M. [Aging and ultrasonographic findings of carotid atherosclerosis]. Nippon Ronen Igakkai Zasshi 1997 Jul;34(7):560-8.108 Takada H, Washino K, Harrell JS, Iwata H. Acceleration plethysmography to evaluate aging effect in cardiovascular system. Using new criteria of four wave patterns. Med Prog
Technol 1996;21(4):205-10.109 Kim DW, Kim SW, Kim SC, Nam KC, Kang ES, Im JJ. Detection of diabetic neuropathy using blood volume ratio of finger and toe by PPG. Conf Proc IEEE Eng Med Biol Soc
2007;2007:2211-4.110 Kim SW, Kim SC, Nam KC, Kang ES, Im JJ, Kim DW. A new method of screening for diabetic neuropathy using laser Doppler and photoplethysmography. Med Biol Eng
Comput 2008 Jan;46(1):61-7.111 Jaryal AK, Selvaraj N, Santhosh J, Anand S, Deepak KK. Monitoring of cardiovascular reactivity to cold stress using digital volume pulse characteristics in health and diabetes.
J Clin Monit Comput 2009 Apr;23(2):123-30.112 Rakower SR, Shahgoli S, Wong SL. Doppler ultrasound and digital plethysmography to determine the need for sympathetic blockade after frostbite. J Trauma 1978
Oct;18(10):713-8.113 Middleton PM, Chan GS, O’Lone E, Steel E, Carroll R, Celler BG, et al. Changes in left ventricular ejection time and pulse transit time derived from finger
photoplethysmogram and electrocardiogram during moderate haemorrhage. Clin Physiol Funct Imaging 2009 May;29(3):163-9.

33
114 Middleton PM, Chan GS, O’Lone E, Steel E, Carroll R, Celler BG, et al. Spectral analysis of finger photoplethysmographic waveform variability in a model of mild to moderate haemorrhage. J Clin Monit Comput 2008 Oct;22(5):343-53.
115 Ubbink DT. Toe blood pressure measurements in patients suspected of leg ischaemia: a new laser Doppler device compared with photoplethysmography. Eur J Vasc Endovasc Surg 2004 Jun;27(6):629-34.
116 Carter SA, Tate RB. The relationship of the transcutaneous oxygen tension, pulse waves and systolic pressures to the risk for limb amputation in patients with peripheral arterial disease and skin ulcers or gangrene. Int Angiol 2006 Mar;25(1):67-72.
117 Sadiq S, Chithriki M. Arterial pressure measurements using infrared photosensors: comparison with CW Doppler. Clin Physiol 2001 Jan;21(1):129-32.118 Whiteley MS, Fox AD, Horrocks M. Photoplethysmography can replace hand-held Doppler in the measurement of ankle/brachial indices. Ann R Coll Surg Engl 1998
Mar;80(2):96-8.119 Sharif-Kashani B, Behzadnia N, Shahabi P, Sadr M. Screening for deep vein thrombosis in asymptomatic high-risk patients: a comparison between digital
photoplethysmography and venous ultrasonography. Angiology 2009 Jun;60(3):301-7.120 Khandanpour N, Armon MP, Jennings B, Clark A, Meyer FJ. Photoplethysmography, an easy and accurate method for measuring ankle brachial pressure index: can
photoplethysmography replace Doppler? Vasc Endovascular Surg 2009 Dec;43(6):578-82.121 Allen J, Overbeck K, Nath AF, Murray A, Stansby G. A prospective comparison of bilateral photoplethysmography versus the ankle-brachial pressure index for detecting and
quantifying lower limb peripheral arterial disease. J Vasc Surg 2008 Apr;47(4):794-802.122 Alnaeb ME, Crabtree VP, Boutin A, Mikhailidis DP, Seifalian AM, Hamilton G. Prospective assessment of lower-extremity peripheral arterial disease in diabetic patients using
a novel automated optical device. Angiology 2007 Oct;58(5):579-85.123 Erts R, Spigulis J, Kukulis I, Ozols M. Bilateral photoplethysmography studies of the leg arterial stenosis. Physiol Meas 2005 Oct;26(5):865-74.124 Allen J, Oates CP, Lees TA, Murray A. Photoplethysmography detection of lower limb peripheral arterial occlusive disease: a comparison of pulse timing, amplitude and shape
characteristics. Physiol Meas 2005 Oct;26(5):811-21.125 Planchon B, de FP, Dupas B, Grolleau JY. [Value of digital plethysmography in the positive diagnosis and prognostic evaluation of digital arteriopathies]. J Mal Vasc
1987;12(2):123-6.126 Schapira D, Nahir AM, Hadad N. Interferon-induced Raynaud’s syndrome. Semin Arthritis Rheum 2002 Dec;32(3):157-62.127 Wouda AA. Raynaud’s phenomenon. Photoelectric plethysmography of the fingers of persons with and without Raynaud’s phenomenon during cooling and warming up. Acta
Med Scand 1977;201(6):519-23.128 Zweifler AJ, Trinkaus P. Occlusive digital artery disease in patients with Raynaud’s phenomenon. Am J Med 1984 Dec;77(6):995-1001.129 Samueloff S, Miday R, Wasserman D, Behrens V, Hornung R, Asburry W, et al. A peripheral vascular insufficiency test using photocell plethysmography. J Occup Med 1981
Sep;23(9):643-6.130 Suichies HE, Aarnoudse JG, Wouda AA, Jentink HW, de Mul FF, Greve J. Digital blood flow in cooled and contralateral finger in patients with Raynaud’s phenomenon.
Comparative measurements between photoelectrical plethysmography and laser Doppler flowmetry. Angiology 1992 Feb;43(2):134-41.131 Dyszkiewicz A, Tendera M. Vibration syndrome diagnosis using a cooling test verified by computerized photoplethysmography. Physiol Meas 2006 Apr;27(4):353-69.132 Pistorius MA, Briant C, Planchon B. [Determination of reference temperatures for a cold test in digital plethysmography]. J Mal Vasc 1994;19(3):195-8.133 de Faucal P., Planchon B, Boudard D, Peltier P, Barrier J, Grolleau JY. [Finger plethysmography for studying the blood rheological and hemodynamic components of an
acrosyndrome]. J Mal Vasc 1986;11(4):356-61.134 Planchon B, de FP, Essboui S, Grolleau JY. A quantitative test for measuring reactivity to cold by the digital plethysmograph technique: application to 66 control subjects and
65 patients with Raynaud’s phenomenon. Angiology 1986 Jun;37(6):433-9.135 Martinez S, Lozano P, Pallares L, Julia J, Artigues I, Plaza A, et al. [Usefulness of photoplethysmography and indexes of digital pressure in Raynaud phenomenon]. Med Clin
(Barc ) 1999 Sep 25;113(9):327-30.136 Lindsell CJ, Griffin MJ. Finger systolic blood pressures: effects of cold provocation on the reference finger. Cent Eur J Public Health 1995;3 Suppl:45-8.137 Nasu Y, Kurozawa Y, Fujiwara Y, Honma H, Yanai T, Kido K, et al. Multicenter study on finger systolic blood pressure test for diagnosis of vibration-induced white finger. Int
Arch Occup Environ Health 2008 Apr;81(5):639-44.138 Thompson A, House R, Manno M. Assessment of the hand-arm vibration syndrome: thermometry, plethysmography and the Stockholm Workshop Scale. Occup Med (Lond)
2007 Oct;57(7):512-7.139 Thompson A, House R, Manno M. The sensitivity and specificity of thermometry and plethysmography in the assessment of hand-arm vibration syndrome. Occup Med
(Lond) 2008 May;58(3):181-6.140 Miyashita K, Morioka I, Luo WZ, Gowa Y, Takeda S, Kasamatsu T, et al. Age-related evaluation of peripheral circulation of workers with vibration exposure. Cent Eur J Public
Health 1995;3 Suppl:22-6.141 Sollinger D, Mohaupt MG, Wilhelm A, Uehlinger D, Frey FJ, Eisenberger U. Arterial stiffness assessed by digital volume pulse correlates with comorbidity in patients with
ESRD. Am J Kidney Dis 2006 Sep;48(3):456-63.142 van Hoek F., Scheltinga MR, Kouwenberg I, Moret KE, Beerenhout CH, Tordoir JH. Steal in hemodialysis patients depends on type of vascular access. Eur J Vasc Endovasc
Surg 2006 Dec;32(6):710-7.143 Bresler M, Sheffy K, Pillar G, Preiszler M, Herscovici S. Differentiating between light and deep sleep stages using an ambulatory device based on peripheral arterial tonometry.
Physiol Meas 2008 May;29(5):571-84.144 Grote L, Zou D, Kraiczi H, Hedner J. Finger plethysmography--a method for monitoring finger blood flow during sleep disordered breathing. Respir Physiol Neurobiol 2003
Jul 16;136(2-3):141-52.145 Linder SP, Wendelken S, Clayman J, Steiner PR. Noninvasive detection of the hemodynamic stress of exercise using the photoplethysmogram. J Clin Monit Comput 2008
Aug;22(4):269-78.146 Dyszkiewicz A, Kucharz EJ. [Photoplethysmographic evaluation of microcirculation in patients with overt and latent hyperthyroidism or hypothyroidism]. Pol Arch Med
Wewn 2000 Jul;104(1):339-43.147 Dyszkiewicz A. Finger cooling test and psychometric analysis in thyroid auxiliary diagnostics. Acta Bioeng Biomech 2007;9(2):61-8.148 Evans IL, Crawford ES, DeBakey ME. Digital plethysmography in evaluation of surgery of degenerative arterial disease. Surg Forum 1957;8:438-42.149 Rodriguez E, Ormont ML, Lambert EH, Needleman L, Halpern EJ, Diehl JT, et al. The role of preoperative radial artery ultrasound and digital plethysmography prior to
coronary artery bypass grafting. Eur J Cardiothorac Surg 2001 Feb;19(2):135-9.150 Rothkopf DM, Bryan DJ, Cuadros CL, May JW, Jr. Surgical management of ulnar artery aneurysms. J Hand Surg Am 1990 Nov;15(6):891-7.151 Heath ME, Downey JA. The cold face test (diving reflex) in clinical autonomic assessment: methodological considerations and repeatability of responses. Clin Sci (Lond) 1990
Feb;78(2):139-47.152 Arioz DT, Saglam H, Demirel R, Koken G, Cosar E, Sahin FK, et al. Arterial stiffness and dipper/nondipper blood pressure status in women with preeclampsia. Adv Ther 2008
Sep;25(9):925-34.153 Winkelmann BR, Matheis G, Kleist P, Potter S, Wohltmann D, Kaltenbach M. Discordance of anti-ischemic and hemodynamic effects of captopril in stable coronary artery
disease. Coron Artery Dis 1994 Oct;5(10):829-44.154 Duprez D, Clement DL. Vasodilator effects of enalapril in patients with arterial hypertension. Acta Cardiol 1986;41(5):359-64.155 Inglessis N, Nussberger J, Hagmann M, Hiesse-Provost O, Insuasty J, Reid J, et al. Comparison of the angiotensin II antagonist UP269-6 with the angiotensin converting
enzyme inhibitor enalapril in normotensive volunteers challenged with angiotensin I. J Cardiovasc Pharmacol 1995 Jun;25(6):986-93.
34
156 Payne RA, Symeonides CN, Webb DJ, Maxwell SR. Pulse transit time measured from the ECG: an unreliable marker of beat-to-beat blood pressure. J Appl Physiol 2006 Jan;100(1):136-41.
157 Talke PO, Caldwell JE, Richardson CA, Heier T. The effects of clonidine on human digital vasculature. Anesth Analg 2000 Oct;91(4):793-7.158 Dixon RM, Meire HB, Leigh C, Posner J, Rolan PE. Evaluation of non-invasive techniques to assess vasoconstriction in healthy volunteers using methoxamine as a probe drug.
Cephalalgia 1996 Nov;16(7):507-17.159 Nieminen T, Tammela TL, Koobi T, Kahonen M. The effects of tamsulosin and sildenafil in separate and combined regimens on detailed hemodynamics in patients with
benign prostatic enlargement. J Urol 2006 Dec;176(6 Pt 1):2551-6.160 Clement DL, Duprez D, De PN. Effect of indoramin on finger circulation in patients with Raynaud disease. J Cardiovasc Pharmacol 1986;8 Suppl 2:S84-S87.161 Talke P, Lobo E, Brown R. Systemically administered alpha2-agonist-induced peripheral vasoconstriction in humans. Anesthesiology 2003 Jul;99(1):65-70.162 Babchenko A, Davidson E, Adler D, Ginosar Y, Kurz V, Nitzan M. Increase in pulse transit time to the foot after epidural anaesthesia treatment. Med Biol Eng Comput 2000
Nov;38(6):674-9.163 Ginosar Y, Weiniger CF, Kurz V, Babchenko A, Nitzan M, Davidson E. Sympathectomy-mediated vasodilatation: a randomized concentration ranging study of epidural
bupivacaine. Can J Anaesth 2009 Mar;56(3):213-21.164 Klemsdal TO, Moan A, Kjeldsen SE. Effects of selective angiotensin II type 1 receptor blockade with losartan on arterial compliance in patients with mild essential
hypertension. Blood Press 1999;8(4):214-9.165 Chern CM, Hsu HY, Hu HH, Chen YY, Hsu LC, Chao AC. Effects of atenolol and losartan on baroreflex sensitivity and heart rate variability in uncomplicated essential
hypertension. J Cardiovasc Pharmacol 2006 Feb;47(2):169-74.166 Jablonka DH, Awad AA, Stout RG, Silverman DG, Shelley KH. Comparing the effect of arginine vasopressin on ear and finger photoplethysmography. J Clin Anesth 2008
Mar;20(2):90-3.167 Motomiya T. [Pyridinolcarbamate treatment of atherosclerosis obliterans analysed by toe plethysmography]. Nippon Naika Gakkai Zasshi 1970 Feb 10;59(2):117-25.168 Brecht T. Effects of misoprostol on human circulation. Prostaglandins 1987;33 Suppl:51-60.169 Fischer M, Reinhold B, Falck H, Torok M, Alexander K. Topical nitroglycerin ointment in Raynaud’s phenomenon. Z Kardiol 1985 May;74(5):298-302.170 van der Veur E, ten Berge BS, Wouda AA, Wesseling H. Effects of atenolol, labetalol and propranolol on the peripheral circulation in hypertensive patients without obstructive
vascular disease. Eur J Clin Pharmacol 1985;28(2):131-4.171 Arosio E, De MS, Prior M, Zannoni M, Lechi A. Effects of nebivolol and atenolol on small arteries and microcirculatory endothelium-dependent dilation in hypertensive
patients undergoing isometric stress. J Hypertens 2002 Sep;20(9):1793-7.172 Muller M, Isenschmid M, Buhrer M, Bircher J. [Automatic finger plethysmography as a human pharmacologic research tool. A methodologic study]. Arzneimittelforschung
1984;34(6):702-6.173 Brotzu G, Falchi S, Mannu B, Montisci R, Petruzzo P, Staico R. The importance of presynaptic beta receptors in Raynaud’s disease. J Vasc Surg 1989 Jun;9(6):767-71.174 Vayssairat M, Corvol P, Mathieu JF, Bonin M, Housset E. [Hemodynamic study, under hot and cold conditions, of the digital artery in arterial hypertension and the effects of
cardioselective and non-cardioselective beta blocker treatment]. J Mal Vasc 1986;11(3):223-8.175 Duprez D, De BT, De PN, Hermans L, De BM, Clement DL. Effects of isradipine on peripheral hemodynamic reflex responses in mild-to-moderate essential hypertension. Am
J Hypertens 1991 Feb;4(2 Pt 2):194S-6S.176 Kallenberg CG, Wouda AA, Meems L, Wesseling H. Once daily felodipine in patients with primary Raynaud’s phenomenon. Eur J Clin Pharmacol 1991;40(3):313-5.177 Finch MB, Copeland S, Passmore AP, Johnston GD. A double-blind cross-over study of nifedipine retard in patients with Raynaud’s phenomenon. Clin Rheumatol 1988
Sep;7(3):359-65.178 Van Osta A, Moraine JJ, Melot C, Mairbaurl H, Maggiorini M, Naeije R. Effects of high altitude exposure on cerebral hemodynamics in normal subjects. Stroke 2005
Mar;36(3):557-60.179 Murray A, Drummond GB, Dodds S, Marshall L. Low-frequency changes in finger volume in patients after surgery, related to respiration and venous pressure. Eur J
Anaesthesiol 2009 Jan;26(1):9-16.180 Johnstone M. The effects of sedation on the digital plethysmogram. A radiotelemetric study of haloperidol. Anaesthesia 1967 Jan;22(1):3-15.181 Arneklo-Nobin B, Elmer O, Akesson A. Effect of long-term ketanserin treatment on 5-HT levels, platelet aggregation and peripheral circulation in patients with Raynaud’s
phenomenon. A double-blind, placebo-controlled cross-over study. Int Angiol 1988 Jan;7(1):19-25.182 Schelling JL, West R. [Measurement of peripheral vasodilation by digital plethysmography in clinical tests of hyperemia & of the effects of certain vasodilative drugs.]. Schweiz
Med Wochenschr 1958 Dec 6;88(49):1233-6.183 Wesseling H, den Heeten A., Wouda AA. Sublingual and oral isoxsuprine in patients with Raynaud’s phenomenon. Eur J Clin Pharmacol 1981;20(5):329-33.184 Millasseau SC, Kelly RP, Ritter JM, Chowienczyk PJ. The vascular impact of aging and vasoactive drugs: comparison of two digital volume pulse measurements. Am J
Hypertens 2003 Jun;16(6):467-72.185 Slanar O, Aubrecht J, Perlik F. Noninvasive evaluation of portal-systemic shunting by glyceryl trinitrate. Physiol Res 2002;51(4):413-6.186 Klemsdal TO, Mundal HH, Bredesen JE, Gjesdal K. Transdermal nitroglycerin: clinical and pharmacokinetic consequences of renewing the patch and the application site. Eur
J Clin Pharmacol 1997;52(5):379-81.187 Stengele E, Winkler F, Trenk D, Jahnchen E, Petersen J, Roskamm H. Digital pulse plethysmography as a non-invasive method for predicting drug-induced changes in left
ventricular preload. Eur J Clin Pharmacol 1996;50(4):279-82.188 de Mey C., Erb K, Zimmermann T, Mutschler H, Blume H, Belz GG. Clinical pharmacological equivalence of a novel FCH-free GTN spray with low ethanol content vs a
FCH-containing GTN spray. Eur J Clin Pharmacol 1995;47(5):437-43.189 Wagner G. Selected issues from an overview on nicorandil: tolerance, duration of action, and long-term efficacy. J Cardiovasc Pharmacol 1992;20 Suppl 3:S86-S92.190 Huber T, Merz PG, Harder S. [Biologic availability and hemodynamic actions following administration of sublingual glycerol trinitrate. A new delivery system].
Arzneimittelforschung 1991 Jul;41(7):715-8.191 Migliacci R, Busti G, Flamini F, Marini M, Santucci C, Nenci GG, et al. Effect of glyceryl trinitrate on distensibility of peripheral muscular arteries in humans is not mediated
by prostaglandins. Cardiovasc Res 1991 Aug;25(8):692-9.192 Erb KA, de MC, Wolf GK, Kroll M, Belz GG. [Evaluation of pharmacodynamic equivalence of glycerol trinitrate-containing sprays for oral administration with or without
chlorofluorocarbons ]. Arzneimittelforschung 1991 May;41(5):484-8.193 Bass A, Walden R, Hirshberg A, Schneiderman J. Pharmacokinetic activity of nitrites evaluated by digital pulse volume recording. J Cardiovasc Surg (Torino) 1989
May;30(3):395-7.194 Lund F. Digital pulse plethysmography (DPG) in studies of the hemodynamic response to nitrates--a survey of recording methods and principles of analysis. Acta Pharmacol
Toxicol (Copenh) 1986;59 Suppl 6:79-96.195 Coppock JS, Hardman JM, Bacon PA, Woods KL, Kendall MJ. Objective relief of vasospasm by glyceryl trinitrate in secondary Raynaud’s phenomenon. Postgrad Med J 1986
Jan;62(723):15-8.196 Isenschmid M, Muller M, Buhrer M, Vorkauf H, Bircher J. Absolute bioavailability of glyceryl trinitrate from a transdermal system, assessed by digital plethysmography. Int J
Clin Pharmacol Ther Toxicol 1985 Jul;23(7):345-51.197 Porchet H, Bircher J. Noninvasive assessment of portal-systemic shunting: evaluation of a method to investigate systemic availability of oral glyceryl trinitrate by digital
plethysmography. Gastroenterology 1982 Apr;82(4):629-37.198 Hannemann RE, Erb RJ, Stoltman WP, Bronson EC, Williams EJ, Long RA, et al. Digital plethysmography for assessing erythrityl tetranitrate bioavailability. Clin Pharmacol
Ther 1981 Jan;29(1):35-9.
35
199 Tucker AT, Pearson RM, Cooke ED, Benjamin N. Effect of nitric-oxide-generating system on microcirculatory blood flow in skin of patients with severe Raynaud’s syndrome: a randomised trial. Lancet 1999 Nov 13;354(9191):1670-5.
200 Piatti P, Fragasso G, Monti LD, Setola E, Lucotti P, Fermo I, et al. Acute intravenous L-arginine infusion decreases endothelin-1 levels and improves endothelial function in patients with angina pectoris and normal coronary arteriograms: correlation with asymmetric dimethylarginine levels. Circulation 2003 Jan 28;107(3):429-36.
201 Schutte AE, Huisman HW, van Rooyen JM, Oosthuizen W, Jerling JC. Sensitivity of the Finometer device in detecting acute and medium-term changes in cardiovascular function. Blood Press Monit 2003 Oct;8(5):195-201.
202 Williams C, Kingwell BA, Burke K, McPherson J, Dart AM. Folic acid supplementation for 3 wk reduces pulse pressure and large artery stiffness independent of MTHFR genotype. Am J Clin Nutr 2005 Jul;82(1):26-31.
203 Milkowski A, Garg HK, Coughlin JR, Bryan NS. Nutritional epidemiology in the context of nitric oxide biology: a risk-benefit evaluation for dietary nitrite and nitrate. Nitric Oxide 2010 Feb 15;22(2):110-9.
204 Arneklo-Nobin B, Edvinsson L, Eklof B, Haffajee D, Owman C, Thylen U. Analysis of vasospasm in hand arteries by in vitro pharmacology, hand angiography and finger plethysmography. Gen Pharmacol 1983;14(1):65-7.
205 Collins KJ, Exton-Smith AN, James MH, Oliver DJ. Functional changes in autonomic nervous responses with ageing. Age Ageing 1980 Feb;9(1):17-24.206 Chauveau M. [What information can digital plethysmography provide in acrosyndromes?]. Phlebologie 1987 Apr;40(2):431-40.207 Aldrich TK, Moosikasuwan M, Shah SD, Deshpande KS. Length-normalized pulse photoplethysmography: a noninvasive method to measure blood hemoglobin. Ann Biomed
Eng 2002 Nov;30(10):1291-8.208 Eeftinck Schattenkerk DW, van Lieshout JJ, van den Meiracker AH, Wesseling KR, Blanc S, Wieling W, et al. Nexfin noninvasive continuous blood pressure validated against
Riva-Rocci/Korotkoff. Am J Hypertens 2009 Apr;22(4):378-83.209 Schutte AE, Huisman HW, van Rooyen JM, Malan NT, Schutte R. Validation of the Finometer device for measurement of blood pressure in black women. J Hum Hypertens
2004 Feb;18(2):79-84.210 Ahlund C, Pettersson K, Lind L. Pulse wave analysis on fingertip arterial pressure: effects of age, gender and stressors on reflected waves and their relation to brachial and
femoral artery blood flow. Clin Physiol Funct Imaging 2008 Mar;28(2):86-95.211 Guelen I, Westerhof BE, Van Der Sar GL, van Montfrans GA, Kiemeneij F, Wesseling KH, et al. Validation of brachial artery pressure reconstruction from finger arterial
pressure. J Hypertens 2008 Jul;26(7):1321-7.212 Guelen I, Westerhof BE, Van Der Sar GL, van Montfrans GA, Kiemeneij F, Wesseling KH, et al. Finometer, finger pressure measurements with the possibility to reconstruct
brachial pressure. Blood Press Monit 2003 Feb;8(1):27-30.213 Azabji KM, Lador F, Licker M, Moia C, Tam E, Capelli C, et al. Cardiac output by Modelflow method from intra-arterial and fingertip pulse pressure profiles. Clin Sci (Lond)
2004 Apr;106(4):365-9.214 Hsu HY, Chao AC, Chen YT, Wong WJ, Chern CM, Hsu LC, et al. Comparison of critical closing pressures extracted from carotid tonometry and finger plethysmography.
Cerebrovasc Dis 2005;19(6):369-75.215 Chirife R, Pigott VM, Spodick DH. Measurement of the left ventricular ejection time by digital plethysmography. Am Heart J 1971 Aug;82(2):222-7.216 Whinnett ZI, Davies JE, Willson K, Chow AW, Foale RA, Davies DW, et al. Determination of optimal atrioventricular delay for cardiac resynchronization therapy using acute
non-invasive blood pressure. Europace 2006 May;8(5):358-66.217 Coffman JD, Rasmussen HM. Effects of beta-adrenoreceptor-blocking drugs in patients with Raynaud’s phenomenon. Circulation 1985 Sep;72(3):466-70.218 Finch MB, Dawson J, Johnston GD. The peripheral vascular effects of nifedipine in Raynaud’s syndrome associated with scleroderma: a double blind crossover study. Clin
Rheumatol 1986 Dec;5(4):493-8.219 Clement DL. Peripheral action of spironolactone: plethysmographic studies. Am J Cardiol 1990 Jun 19;65(23):12K-3K.220 Clement DL. Effect of spironolactone on systemic blood pressure, limb blood flow and response to sympathetic stimulation in hypertensive patients. Eur J Clin Pharmacol
1982;21(4):263-7.221 Bonnemeier H, Richardt G, Potratz J, Wiegand UK, Brandes A, Kluge N, et al. Circadian profile of cardiac autonomic nervous modulation in healthy subjects: differing effects
of aging and gender on heart rate variability. J Cardiovasc Electrophysiol 2003 Aug;14(8):791-9.222 Agelink MW, Malessa R, Baumann B, Majewski T, Akila F, Zeit T, et al. Standardized tests of heart rate variability: normal ranges obtained from 309 healthy humans, and
effects of age, gender, and heart rate. Clin Auton Res 2001 Apr;11(2):99-108.223 Laitinen T, Niskanen L, Geelen G, Lansimies E, Hartikainen J. Age dependency of cardiovascular autonomic responses to head-up tilt in healthy subjects. J Appl Physiol 2004
Jun;96(6):2333-40.224 Piccirillo G, Fimognari FL, Viola E, Marigliano V. Age-adjusted normal confidence intervals for heart rate variability in healthy subjects during head-up tilt. Int J Cardiol 1995
Jun 30;50(2):117-24.225 Gautschy B, Weidmann P, Gnadinger MP. Autonomic function tests as related to age and gender in normal man. Klin Wochenschr 1986 Jun 2;64(11):499-505.226 O’Brien IA, O’Hare P, Corrall RJ. Heart rate variability in healthy subjects: effect of age and the derivation of normal ranges for tests of autonomic function. Br Heart J 1986
Apr;55(4):348-54.227 Pfeifer MA, Weinberg CR, Cook D, Best JD, Reenan A, Halter JB. Differential changes of autonomic nervous system function with age in man. Am J Med 1983 Aug;75(2):249-
58.228 Shimazu T, Tamura N, Shimazu K. [Aging of the autonomic nervous system]. Nippon Rinsho 2005 Jun;63(6):973-7.229 Sherebrin MH, Sherebrin RZ. Frequency analysis of the peripheral pulse wave detected in the finger with a photoplethysmograph. IEEE Trans Biomed Eng 1990
Mar;37(3):313-7.230 Selvaraj N, Jaryal A, Santhosh J, Deepak KK, Anand S. Assessment of heart rate variability derived from finger-tip photoplethysmography as compared to electrocardiography.
J Med Eng Technol 2008 Nov;32(6):479-84.231 Giardino ND, Lehrer PM, Edelberg R. Comparison of finger plethysmograph to ECG in the measurement of heart rate variability. Psychophysiology 2002 Mar;39(2):246-53.232 Theorell T, Edhag O, Fagrell B. Non-invasive methods for evaluating the importance of heart rate and atrial activity in cardiac pacing. Results of ballistocardiography and
digital plethysmography studies in six patients with heart block. Acta Med Scand 1978;203(6):497-502.233 Butter C, Stellbrink C, Belalcazar A, Villalta D, Schlegl M, Sinha A, et al. Cardiac resynchronization therapy optimization by finger plethysmography. Heart Rhythm 2004
Nov;1(5):568-75.234 Abe M, Yoshizawa M, Sugita N, Tanaka A, Chiba S, Yambe T, et al. A method for evaluating effects of visually-induced motion sickness using ICA for photoplethysmography.
Conf Proc IEEE Eng Med Biol Soc 2008;2008:4591-4.235 Matoba T, Kusumoto H, Omura H, Kotorii T, Kuwahara H. Digital plethysmographic responses to auditory stimuli in patients with vibration disease. Tohoku J Exp Med 1975
Apr;115(4):385-92.236 Gladdish S, Manawadu D, Banya W, Cameron J, Bulpitt CJ, Rajkumar C. Repeatability of non-invasive measurement of intracerebral pulse wave velocity using transcranial
Doppler. Clin Sci (Lond) 2005 May;108(5):433-9.237 Loukogeorgakis S, Dawson R, Phillips N, Martyn CN, Greenwald SE. Validation of a device to measure arterial pulse wave velocity by a photoplethysmographic method.
Physiol Meas 2002 Aug;23(3):581-96.238 Selvaraj N, Jaryal AK, Santhosh J, Anand S, Deepak KK. Monitoring of reactive hyperemia using photoplethysmographic pulse amplitude and transit time. J Clin Monit
Comput 2009 Oct;23(5):315-22.239 von Mollendorff E, Neugebauer G. Digital pulse plethysmography--a tool for investigating vasoactive substances. Methods Find Exp Clin Pharmacol 1985 Sep;7(9):501-10.
36
240 Bogert LW, van Lieshout JJ. Non-invasive pulsatile arterial pressure and stroke volume changes from the human finger. Exp Physiol 2005 Jul;90(4):437-46.241 Imholz BP, Wieling W, van Montfrans GA, Wesseling KH. Fifteen years experience with finger arterial pressure monitoring: assessment of the technology. Cardiovasc Res 1998
Jun;38(3):605-16.242 Hirschl MM, Woisetschlager C, Waldenhofer U, Herkner H, Bur A. Finapres vs portapres. J Hum Hypertens 1999 Dec;13(12):899.243 Becker F. Exploration of arterial function with noninvasive technics. Results in chronic arterial occlusive disease of the lower limbs according to Leriche and Fontaine
classification. Int Angiol 1985 Jul;4(3):311-22.244 Maisonneuve H, Planchon B, de FP, Mussini JM, Patra P. [Vascular manifestation of thoracic outlet syndrome. Prospective study of 104 patients]. J Mal Vasc 1991;16(3):220-5.245 Laroche GP, Theriault G. [Validity of plethysmography and the digital temperature recovery test in the diagnosis of primary and occupational Raynaud’s phenomenon]. Clin
Invest Med 1987 Mar;10(2):96-102.246 Pang KP, Gourin CG, Terris DJ. A comparison of polysomnography and the WatchPAT in the diagnosis of obstructive sleep apnea. Otolaryngol Head Neck Surg 2007
Oct;137(4):665-8.247 Herscovici S, Pe’er A, Papyan S, Lavie P. Detecting REM sleep from the finger: an automatic REM sleep algorithm based on peripheral arterial tone (PAT) and actigraphy.
Physiol Meas 2007 Feb;28(2):129-40.248 Zou D, Grote L, Peker Y, Lindblad U, Hedner J. Validation a portable monitoring device for sleep apnea diagnosis in a population based cohort using synchronized home
polysomnography. Sleep 2006 Mar 1;29(3):367-74.249 Hedner J, Pillar G, Pittman SD, Zou D, Grote L, White DP. A novel adaptive wrist actigraphy algorithm for sleep-wake assessment in sleep apnea patients. Sleep 2004 Dec
15;27(8):1560-6.250 Pittman SD, Ayas NT, MacDonald MM, Malhotra A, Fogel RB, White DP. Using a wrist-worn device based on peripheral arterial tonometry to diagnose obstructive sleep
apnea: in-laboratory and ambulatory validation. Sleep 2004 Aug 1;27(5):923-33.251 Ayas NT, Pittman S, MacDonald M, White DP. Assessment of a wrist-worn device in the detection of obstructive sleep apnea. Sleep Med 2003 Sep;4(5):435-42.252 Bar A, Pillar G, Dvir I, Sheffy J, Schnall RP, Lavie P. Evaluation of a portable device based on peripheral arterial tone for unattended home sleep studies. Chest 2003
Mar;123(3):695-703.253 Karthik S, Pal GK, Nanda N, Hamide A, Bobby Z, Amudharaj D, et al. Sympathovagal imbalance in thyroid dysfunctions in females: correlation with thyroid profile, heart rate
and blood pressure. Indian J Physiol Pharmacol 2009 Jul;53(3):243-52.254 Chen JL, Chiu HW, Tseng YJ, Chu WC. Hyperthyroidism is characterized by both increased sympathetic and decreased vagal modulation of heart rate: evidence from spectral
analysis of heart rate variability. Clin Endocrinol (Oxf) 2006 Jun;64(6):611-6.255 Casu M, Cappi C, Patrone V, Repetto E, Giusti M, Minuto F, et al. Sympatho-vagal control of heart rate variability in patients treated with suppressive doses of L-thyroxine for
thyroid cancer. Eur J Endocrinol 2005 Jun;152(6):819-24.256 Cacciatori V, Bellavere F, Pezzarossa A, Dellera A, Gemma ML, Thomaseth K, et al. Power spectral analysis of heart rate in hyperthyroidism. J Clin Endocrinol Metab 1996
Aug;81(8):2828-35.257 Cacciatori V, Gemma ML, Bellavere F, Castello R, De Gregori ME, Zoppini G, et al. Power spectral analysis of heart rate in hypothyroidism. Eur J Endocrinol 2000
Sep;143(3):327-33.258 Barczynski M, Tabor S, Thor P. [Evaluation of autonomic nervous system function with heart rate variability analysis in patients with hyperthyroidism and during
euthyroidism after pharmacologic and surgical treatment]. Folia Med Cracov 1997;38(3-4):27-35.259 Shuvy M, Arbelle JE, Grosbard A, Katz A. A simple test of one minute heart rate variability during deep breathing for evaluation of sympatovagal imbalance in
hyperthyroidism. Isr Med Assoc J 2008 Aug;10(8-9):603-6.260 Dagre AG, Lekakis JP, Papaioannou TG, Papamichael CM, Koutras DA, Stamatelopoulos SF, et al. Arterial stiffness is increased in subjects with hypothyroidism. Int J Cardiol
2005 Aug 3;103(1):1-6.261 Dagre AG, Lekakis JP, Protogerou AD, Douridas GN, Papaioannou TG, Tryfonopoulos DJ, et al. Abnormal endothelial function in female patients with hypothyroidism and
borderline thyroid function. Int J Cardiol 2007 Jan 18;114(3):332-8.262 Napoli R, Biondi B, Guardasole V, Matarazzo M, Pardo F, Angelini V, et al. Impact of hyperthyroidism and its correction on vascular reactivity in humans. Circulation 2001
Dec 18;104(25):3076-80.263 Napoli R, Guardasole V, Angelini V, Zarra E, Terracciano D, D’Anna C, et al. Acute effects of triiodothyronine on endothelial function in human subjects. J Clin Endocrinol
Metab 2007 Jan;92(1):250-4.264 Napoli R, Biondi B, Guardasole V, D’Anna C, De SA, Pirozzi C, et al. Enhancement of vascular endothelial function by recombinant human thyrotropin. J Clin Endocrinol
Metab 2008 May;93(5):1959-63.265 Napoli R, Guardasole V, Zarra E, D’Anna C, De SA, Lupoli GA, et al. Impaired endothelial- and nonendothelial-mediated vasodilation in patients with acute or chronic
hypothyroidism. Clin Endocrinol (Oxf) 2010 Jan;72(1):107-11.266 Taddei S, Caraccio N, Virdis A, Dardano A, Versari D, Ghiadoni L, et al. Impaired endothelium-dependent vasodilatation in subclinical hypothyroidism: beneficial effect of
levothyroxine therapy. J Clin Endocrinol Metab 2003 Aug;88(8):3731-7.267 Dimitriadis G, Mitrou P, Lambadiari V, Boutati E, Maratou E, Panagiotakos DB, et al. Insulin action in adipose tissue and muscle in hypothyroidism. J Clin Endocrinol Metab
2006 Dec;91(12):4930-7.268 Huiku M, Uutela K, van GM, Korhonen I, Kymalainen M, Merilainen P, et al. Assessment of surgical stress during general anaesthesia. Br J Anaesth 2007 Apr;98(4):447-55.269 Krediet CT, Wilde AA, Halliwill JR, Wieling W. Syncope during exercise, documented with continuous blood pressure monitoring during ergometer testing. Clin Auton Res
2005 Feb;15(1):59-62.270 Yiallourou SR, Walker AM, Horne RS. Effects of sleeping position on development of infant cardiovascular control. Arch Dis Child 2008 Oct;93(10):868-72.271 Leonetti P, Audat F, Girard A, Laude D, Lefrere F, Elghozi JL. Stroke volume monitored by modeling flow from finger arterial pressure waves mirrors blood volume withdrawn
by phlebotomy. Clin Auton Res 2004 Jun;14(3):176-81.272 Fahrenberg J, Foerster F, Muller W. Non-invasive estimations of ventricular ejection time and stroke volume: comparison of impedance cardiography and the Portapres 2. J
Med Eng Technol 1997 Jan;21(1):15-22.273 Blanc VF, Haig M, Troli M, Sauve B. Computerized photo-plethysmography of the finger. Can J Anaesth 1993 Mar;40(3):271-8.