quality of life in patients after resection of pt3 lateral ... · quality of life in patients after...
TRANSCRIPT

Canis et al. - Quality of life after tongue reconstruction
Quality of life in patients after resection of pT3 lateral tongue carcinoma:
microvascular reconstruction vs. primary closure
Martin Canis, M.D.1, Bernhard G. Weiss1, Friedrich Ihler, M.D.1,
Eva Hummers-Pradier, M.D.2, Christoph Matthias, M.D.1, Hendrik A. Wolff, M.D.3
1 Department of Otorhinolaryngology, Head and Neck Surgery, University of Göttingen,
Germany
2 Department of General Practice/Family Medicine, University of Göttingen, Germany
3 Department of Radiation Oncology, University of Göttingen, Germany
short title: Quality of life after tongue reconstruction
Corresponding author: Prof. Martin Canis, MD
University of Göttingen
Dept. of Otorhinolaryngology, Head & Neck Surgery
Robert-Koch-Str. 40
Germany, 37075 Göttingen
Phone: +49-551-39-8971
Fax: +49-551-3922809
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article as an‘Accepted Article’, doi: 10.1002/hed.23862

Canis et al. - Quality of life after tongue reconstruction
-2/17-
Abstract
Background: Controversy exists regarding the functional advantages of free-flap reconstruc-
tion after partial glossectomy as compared to primary closure.
Methods: Forty patients were included in this retrospective study after resection of a pT3
lateral tongue carcinoma. Twenty patients received a free forearm flap and 20 patients had a
primary closure. All patients had adjuvant chemoradiation, were free of disease at least 1
year after therapy and completed the German versions of the EORTC questionnaires QLQ-
C30 and QLQ-H&N35.
Results: Mean time between surgery and quality of life assessment was 16.2 ± 3.4 months.
The average resection was 41.60 % (reconstruction) of the oral tongue, and 39.1 % (primary
closure). After reconstruction, patients had significantly (p>0.05) fewer problems with the
swallowing, speech and social eating subdomains of the EORTC QLQ-H&N35. All other
items showed no significant differences.
Conclusion:
Our preliminary results suggest that free flaps might be useful when treating pT3 tongue can-
cer.

Canis et al. - Quality of life after tongue reconstruction
-3/17-
Introduction
The relevance of health-related quality of life (HRQOL) has undergone a quantum shift since
the beginning of the 21st century. According to the World Health Organization (WHO),
HRQOL is the quality of life relative to one’s health or disease status and intended to be a
major concern of policymakers, researchers, and health care practitioners (1). Once regarded
as a secondary outcome measure occasionally useful in addition to biological and clinical
markers of disease, a major change has occurred within the last years with HRQOL issues
now being at the forefront of public health policies. Head and neck squamous cell carcinoma
(HNSCC) severely affect patients’ health and well-being: While surgical treatment and radio-
therapy improve the prognosis with regard to survival, they frequently result in impaired basic
and social activities of daily life, and can be disfiguring (2). Therefore, assessing the impact of
HNSCC therapy on HRQOL is of utmost importance not only for the individual patient, but
also to guide future therapeutic strategies. After resection of large tongue carcinomas, pres-
ervation and restoration of speech and swallowing function is one of the most important pri-
mary considerations with regard to long-term HRQOL (3). However, decision-making in terms
of reconstructive surgery is challenging for both surgeon and patient since an individual pre-
diction of postoperative function is hardly possible. Major factors that affect postoperative
function and HRQOL depend on tumour stage and site, the extent of tissue resection and the
type of reconstruction (4-5). For patients presenting with carcinoma of the lateral tongue, post-
operative swallowing and speech performance is mostly affected by the extent of tissue loss,
with function decreasing with an increasing percentage of resection (6). For tissue resection,
primary closure (7), local flaps (8), pedicled flaps (9) or microvascular free tissue transfer (10) has
been propagated and published. However, there is no evidence proving the functional advan-
tages of any one method over the others in terms of HRQOL (11).
For therapeutic decision-making in patients with pT3 tongue carcinoma we investigated
speech and swallowing-related quality of life after partial glossectomy, microvascular tongue
reconstruction or primary closure of the defect and adjuvant chemoradiation. We compared

Canis et al. - Quality of life after tongue reconstruction
-4/17-
patients who had undergone primary closure vs. those who had received free forearm flap
reconstruction at least 1 year earlier. The present study was exploratory and findings were
regarded as preliminary. .
Patients and methods
Patients
The study was carried out as a retrospective chart analysis between January 2009 and July
2012 and approved by the Institutional review board (reference number 19/11/13An). All pro-
cedures were conducted in one single tertiary centre by 2 experienced surgeons. A total of
40 consecutive patients with previously untreated locally advanced squamous cell carcinoma
of the tongue and pT3, cN0-2, cM0 disease were treated with curative intent at the Depart-
ment for Otorhinolaryngology – Head and Neck Surgery of the Göttingen University Medical
Center. All tumours were staged according to the current classification of the Union for Inter-
national Cancer Control (UICC) and the American Joint Committee on Cancer (AJCC) (12).
Inclusion criteria were: pT3 tongue carcinoma, primary tumour resection, alive and disease-
free at least 1 year after surgery. We included 20 consecutive patients after resection of a
pT3 lateral tongue carcinoma and microvascular reconstruction and 20 consecutive patients
after resection of a pT3 carcinoma of the lateral tongue and primary closure of the defect.
Exclusion criteria for this study were: non-squamous cell carcinomas, simultaneously second
primary tumour, simultaneous distant metastases, cN3 neck disease.
Treatment of primary tumours
Preoperative examination consisted of microscopic and rigid or flexible endoscopic examina-
tion of the oral cavity, the oro-/hypopharynx and the larynx on the alert patient, followed by
ultrasonography of the neck for lymph node evaluation and local staging. Computed tomo-

Canis et al. - Quality of life after tongue reconstruction
-5/17-
graphy (CT) or magnetic resonance imaging (MRI) of the neck was undertaken unless the
patient presented with satisfactory imaging performed at the referring hospital. Further stan-
dard preoperative investigations included a CT scan of the chest and ultrasonography of the
abdomen.
At the beginning of the planned surgery under general anaesthesia a panendoscopy was
performed to exclude any second primary tumour in the upper aero-digestive tract prior to
tumour resection. Enoral laser microsurgery was undertaken with the CO2-laser in continuous
superpulse mode. Resection was performed using the technique previously described by
Steiner and Ambrosch (13). Histopathological examination of the resection margins proved to
be a complete (R0) resection. In patients undergoing a reconstruction procedure, tissue de-
fects were reconstructed by a free radial forearm transplant whereas in control patients the
defects were closed by suture. No patient declined to participate in this study. .
Adjuvant chemoradiotherapy
Adjuvant chemoradiotherapy was performed in all patients. In all cases, intensity modulated
external-beam radiotherapy was given five times per week with daily concomitant Cisplati-
num-based chemotherapy. The primary tumour and all lymph nodes areas with histopa-
thologically proven invasion of the capsule were treated daily with 2.08Gy up to a cumulative
dose of 62.4Gy. Histopathologically diseased lymph nodes without invasion of the capsule
received 1.92Gy daily up to a cumulative dose of 57.6Gy. On both sides of the neck, includ-
ing the supraclavicular region, all lymph node areas without proven invasion were covered
with 1.8Gy daily up to a cumulative dose of 54Gy.
Evaluation of HRQOL

Canis et al. - Quality of life after tongue reconstruction
-6/17-
All patients completed the German versions of the European Organization for Research and
Treatment of Cancer (EORTC) Core Quality of Life Questionnaire (QLQ-C30) (14) and the
EORTC Head and Neck Life Questionnaire (QLQ-H&N35) (15). The QLQ-C30 questionnaire is
widely used in conjunction with the QLQ-H&N35 to assess health-related quality of life in
clinical studies of head and neck cancer patients and has demonstrated adequate psycho-
metric properties. Patients were surveyed at least 12 months after completion of all therapeu-
tic procedures. The EORTC QLQ-C30 consists of a global health status/global QOL scale, 5
functional scales, and symptom or single-item scales. The H&N35 contains 18 symptom or
single-item scales. High values for the functional and general QOL scales indicate high func-
tionality and QOL, whereas high values in the symptom scales indicate strong symptoms or
impairment. Value differences of 10 are usually considered clinically relevant. (15)
Statistical methods
Statistical analyses were carried out by SigmaPlot 2004 for Windows Version 9.01 (Systat
Software, Chicago, IL, USA). To detect significant differences between groups with free flap
and primary closure, the student T-test was used to compare measurements if the data was
normally distributed as assessed by Shapiro-Wilk normality test. If no normal distribution was
found, Mann-Whitney rank sum test was used instead. For categorical variables, Chi-square
test or Fisher's exact test were performed. Throughout all tests, a p-value of α < 0.05 was
considered to be statistically significant.
Results
Patients and HRQOL scores
We included 20 patients after resection of a pT3 lateral tongue carcinoma and microvascular
reconstruction. Patient´s characteristics are shown in Table 1. Mean follow up since comple-
tion of all treatment was 18.7 ± 5.2 months, 17.2 ± 4.6 months within the reconstruction group
and 19.8 ± 6.6 months within the primary closure group. Postoperative N categories of both

Canis et al. - Quality of life after tongue reconstruction
-7/17-
groups are given in Table 1. The mean time between surgery and HRQOL assessment was
16.2 ± 3.4 months, 17.8 ± 6.5 in the reconstruction group and 15.9 ± 4.4 in the primary clo-
sure group. The average resection volume in the reconstruction group was 26.7 ± 9.9 cm3,
within the primary closure group 25.0 ± 8.4 cm3. This comprises an average 41.60 % reduc-
tion of the entire tongue volume (16) in the reconstruction group, and 39.1 % in the primary
closure group.
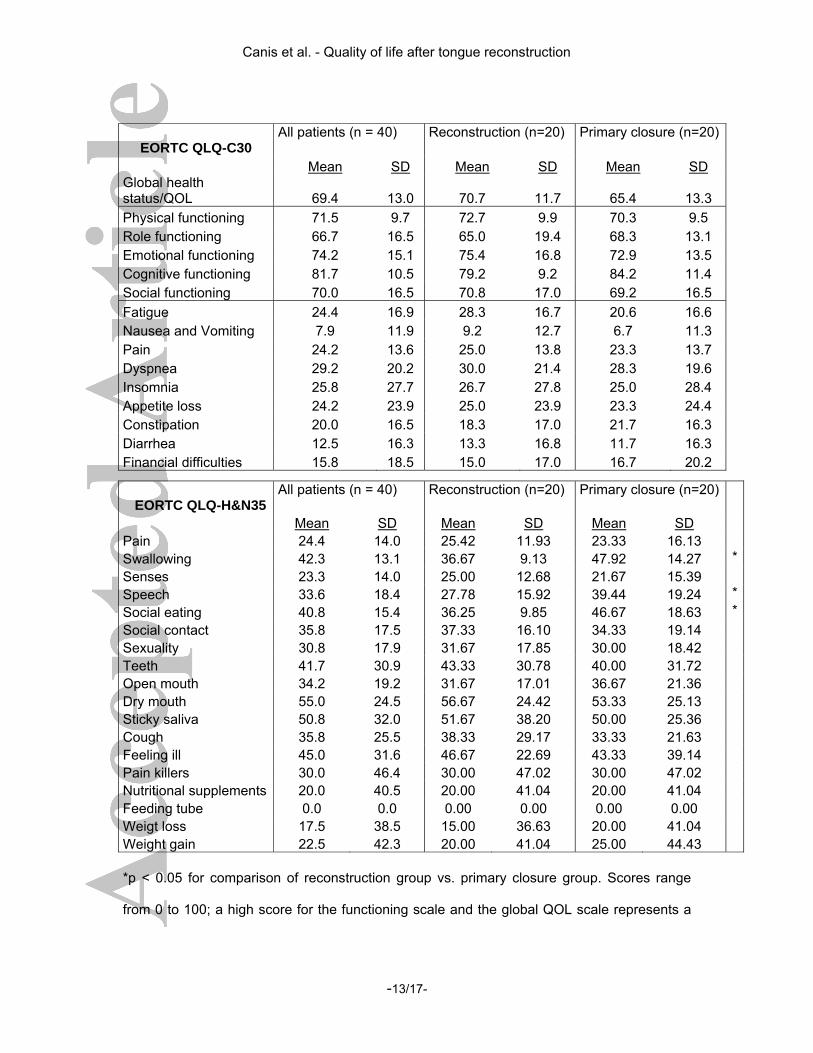
The EORTC QLQ-C30 and the EORTC QLQ-H&N35 scales and items are shown in Table 2.
Mean values of QoL questionnaires after reconstruction and primary closure are also shown
in Figure 1 and Figure 2. After reconstruction with free radialis forearm flaps, patients had
significantly (p < 0.05) less difficulty (on 3 of 33 scales) within the swallowing, speech and
social eating subdomain of the EORTC QLQ-H&N35 compared to patients after primary clo-
sure.
The 3 scales (swallowing, speech, and social eating) that differed significantly between the
groups also showed clinically meaningful mean differences (greater than 10 points), favoring
the reconstruction group. . All other items within the EORTC QLQ-C30 and the EORTC QLQ-
H&N35 questionnaires showed no statistically significant or clinical relevant differences.
Postoperative complications and functional results
Within the reconstruction group one patient experienced partial necrosis of the free flap and
needed revision of the venous anastomosis under general anaesthesia; one patient had
postoperative bleeding of the donor site requiring revision under plexus anaesthesia. Ten
patients needed a temporary tracheotomy due to swelling. Their tracheostoma was closed
before chemoradiotherapy in 6 cases and after chemoradiotherapy in 4 cases. Within the
primary closure group 1 patient developed cervical hematoma after neck dissection and 1
patient experienced postoperative bleeding in the oral cavity. Temporary tracheostomy was
needed in 2 patients due to swelling that were closed after adjuvant treatment. Both had to
be managed in the operating room. Two patients needed a temporary tracheotomy post-

Canis et al. - Quality of life after tongue reconstruction
-8/17-
operatively due to swelling of the tongue with dyspnoea. In both groups, no patient died due
to bleeding, aspiration and/or airway obstruction.
Postoperatively, all patients needed nasogastric feeding tubes for a mean duration of 14.3
days, range 7 to 36 days in the reconstruction group and 11.7 days, range 5 to 28 days in the
primary closure group. In each group, 1 patient required a temporary gastrostomy tube due
to impaired swallowing function After a gradual improvement these were removed 4 months
later in the reconstruction group and after 8 months after primary closure. Nasogastric feed-
ing tubes and gastrostomy tubes were removed only when the patients were able to eat a
normal diet without any clinical and radiologic signs of aspiration.
Discussion
Partial glossectomy has a vast influence on a patient’s HRQOL since swallowing and speech
performance is mostly affected by the extent of tissue loss (4-5). Moreover, scaring of the
tongue can tie the tongue down to the remaining floor of the mouth, thereby further decreas-
ing function (17). Therefore, numerous authors have proposed reconstruction of soft tissue
after partial glossectomy in order to maintain mobility of the remaining tongue (18). Recon-
struction enables the surgeon to achieve oncologic safety due to wider tumour resection
while minimizing voids and allowing for better speech and mastication. Many types of free
and pedicled flaps have been described for tongue reconstruction including free radial fore-
arm (10, 19) and antero-lateral tigh flaps (20) or pedicled supraclavicular artery island (21) and
myocutaneous pectoralis major flap (9). On the other hand, some authors recommend recon-
struction of the tongue by free flap only in cases where the void is larger than 50 % of the
tongue (10). Therefore, it is still not clear if free-flap reconstruction improves HRQOL, and
there is considerable debate about functional advantages of free-flap reconstruction, as
compared with pedicled flaps or primary closure.
In HRQOL investigations, the time of evaluation is a crucial factor and studies have demon-
strated some variability within the first 12 months after treatment (22). Some studies (23-24) sug-

Canis et al. - Quality of life after tongue reconstruction
-9/17-
gested some stability of scores one year after treatment, however others suggested variabil-
ity over the course of long-term follow-up.(25). HRQOL can be reliably surveyed as a long-
term outcome quality indicator in disease-free head and neck cancer patients. Different stud-
ies (3, 26) investigated HRQOL combining a general questionnaire with a disease specific in-
strument. Within the present study we used the same approach with a general questionnaire
applicable to all cancer patients: the EORTC QLQ-C30, as well as specific questionnaire: the
EORTC QLQ-H&N35. The EORTC QLQ-H&N35 is designed for use in association with the
EORTC QLQ-C30 questionnaire by patients with head and neck cancer regardless of the
tumour site, stage, or treatment regimen.
The radial forearm flap continues to be the workhorse in reconstruction of substantial de-
fects in the oral cavity (18). It is a thin, soft tissue transplant with consistent anatomy, however
variable in size and shape. Further advantages are large-caliber vessels for microvascular
anastomosis and low donor site morbidity. The results of Brown et al. (27) support the use of
free flaps for glossectomies larger than one-quarter of the tongue in order to prevent scarring
and contracture of the resection site. Hartl et al. (11) investigated correlations between
HRQOL and the extent of surgical resection in patients who had undergone free-flap tongue
reconstruction after resection of T4a tongue carcinoma. Using the EORTC H&N35 question-
naire, the authors demonstrated that the volume of resection is a major predictor of swallow-
ing- and aspiration related quality of life following tongue resection and free-flap reconstruc-
tion. However, reconstruction did not seem to palliate effects of soft-tissue loss especially in
tongue base resection. In our study significantly better scores in the EORTC H&N35 swallow-
ing, speech and social eating subdomains were found after free flap reconstruction. The dif-
ference may be due to the necessity of extended resections of the base of the tongue, as all
patients studied by Hartl et al. (11) had been diagnosed pT4a tongue carcinoma following a
near total tongue resection. However, in the Hartl et al. study, no direct comparison was
made to patients without any reconstructive measures, an option that might have been asso-
ciated with even worse HRQOL.

Canis et al. - Quality of life after tongue reconstruction
-10/17-
McConnel et al. (7) found that primary closure resulted in better speech and swallowing
than did regional or free-flap reconstruction, comparing equivalent tumour sites and resection
volumes. The authors concluded that soft tissue reconstruction, resulting in an amotile seg-
ment, may impair the driving force of the remaining tongue. In contradiction, the preliminary
results of present study may suggest that free-flap reconstruction enables improved func-
tional outcome as measured by the swallowing, speech and social eating subdomains of the
EORTC H&N35 questionnaire. These 3 scales differed significantly between the groups and
were also the only scales that showed improvements in a clinically meaningful way with value
differences larger than 10 points. The difference between studies might be explained by the
larger resections in our study (median reduction of the oral tongue by 41.60 % and 39.1 %)
compared to a reduction of 10 to 20 % of the oral tongue in the publication of McConnel et al.
(7). Even though we did not find better overall HRQOL according to the EORTC QLQ-C30
questionnaire, our findings imply that tongue reconstruction with free flaps may be beneficial
in the treatment of tongue cancer of patients whose tumour resection exceeds 30 – 40% of
the entire oral tongue. In cases with a resection of less than 20 - 30%, primary closure might
be equivalent to reconstruction (or even better, considering the publication of McConnel et al.
(7)) in terms of HRQOL and thus the treatment of choice. However, due to the non-
randomized design, the small sample of patients, the exploratory nature of the analyses and
the absence of objective speech or swallowing assessments all conclusions are preliminary
and have to be proven by further investigations.
Conclusion
Controversy still exists regarding the functional advantages of free-flap reconstruction after
partial glossectomy as compared to primary closure. Even though we did not find better
overall HRQOL within the EORTC QLQ-C30 questionnaire, one year after resection of about
40% of the oral tongue patients had significantly better outcomes in the swallowing, speech

Canis et al. - Quality of life after tongue reconstruction
-11/17-
and social eating subdomains of the EORTC QLQ-H&N35 questionnaire after reconstruction
with a free forearm flap compared to primary closure. These findings suggest that tongue
reconstruction with free flaps might be useful when treating pT3 tongue cancer. Due to the
preliminary character of the findings future research must proof if reconstruction of tongue
defects is beneficial for the functional outcome of patients with pT3 lateral tongue cancer.

Canis et al. - Quality of life after tongue reconstruction
-12/17-
Tables
Sample characteristics
*: Fisher's exact test; †: Mann-Whitney rank sum test; ‡: Chi-square test.
Table 1: Sample characteristics
Reconstruction
(n=20) Primary closure
(n=20) p-value
Sex
male n = 18 90% n = 17 85%
female n = 2 10% n = 3 5% 1.000*
Age [years]
median 56 58 0.401†
range 23 - 81 33 - 81
Time from diagnosis until surgery [months]
median 0.3 0.4 0.732†
range 0.1 – 1.2 0.2 – 0.9 Resection volume
[cm3]
mean 26.7 25.0 0.839†
SD 14.6 9.9
Neck Dissection
Level I-III 20 100% 20 100%
Level IV 13 65% 11 55% 0.871‡
Level V 9 45% 10 50%
Level I-V 4 20% 5 25%
Marital Status
Single 6 30% 4 20% 0.715‡
Married 14 70% 16 80%
Habit
Cigarette smoking 16 80% 18 90% 0.661‡
Alcohol 8 40% 9 45% 1.000‡
pN
0 0 0% 0 0% 0.884‡
1 3 15% 4 20%
2a 6 30% 4 20%
2b 7 35% 7 35%
Canis et al. - Quality of life after tongue reconstruction
-13/17-
EORTC QLQ-C30 All patients (n = 40)
Reconstruction (n=20)
Primary closure (n=20)
Mean SD Mean SD Mean SD Global health status/QOL 69.4 13.0 70.7 11.7 65.4 13.3 Physical functioning 71.5 9.7 72.7 9.9 70.3 9.5 Role functioning 66.7 16.5 65.0 19.4 68.3 13.1 Emotional functioning 74.2 15.1 75.4 16.8 72.9 13.5 Cognitive functioning 81.7 10.5 79.2 9.2 84.2 11.4 Social functioning 70.0 16.5 70.8 17.0 69.2 16.5 Fatigue 24.4 16.9 28.3 16.7 20.6 16.6 Nausea and Vomiting 7.9 11.9 9.2 12.7 6.7 11.3 Pain 24.2 13.6 25.0 13.8 23.3 13.7 Dyspnea 29.2 20.2 30.0 21.4 28.3 19.6 Insomnia 25.8 27.7 26.7 27.8 25.0 28.4 Appetite loss 24.2 23.9 25.0 23.9 23.3 24.4 Constipation 20.0 16.5 18.3 17.0 21.7 16.3 Diarrhea 12.5 16.3 13.3 16.8 11.7 16.3 Financial difficulties 15.8 18.5 15.0 17.0 16.7 20.2
*p < 0.05 for comparison of reconstruction group vs. primary closure group. Scores range
from 0 to 100; a high score for the functioning scale and the global QOL scale represents a
EORTC QLQ-H&N35 All patients (n = 40)
Reconstruction (n=20)
Primary closure (n=20)
Mean SD Mean SD Mean SD Pain 24.4 14.0 25.42 11.93 23.33 16.13 Swallowing 42.3 13.1 36.67 9.13 47.92 14.27 *Senses 23.3 14.0 25.00 12.68 21.67 15.39 Speech 33.6 18.4 27.78 15.92 39.44 19.24 *Social eating 40.8 15.4 36.25 9.85 46.67 18.63 *Social contact 35.8 17.5 37.33 16.10 34.33 19.14 Sexuality 30.8 17.9 31.67 17.85 30.00 18.42 Teeth 41.7 30.9 43.33 30.78 40.00 31.72 Open mouth 34.2 19.2 31.67 17.01 36.67 21.36 Dry mouth 55.0 24.5 56.67 24.42 53.33 25.13 Sticky saliva 50.8 32.0 51.67 38.20 50.00 25.36 Cough 35.8 25.5 38.33 29.17 33.33 21.63 Feeling ill 45.0 31.6 46.67 22.69 43.33 39.14 Pain killers 30.0 46.4 30.00 47.02 30.00 47.02 Nutritional supplements 20.0 40.5 20.00 41.04 20.00 41.04 Feeding tube 0.0 0.0 0.00 0.00 0.00 0.00 Weigt loss 17.5 38.5 15.00 36.63 20.00 41.04 Weight gain 22.5 42.3 20.00 41.04 25.00 44.43

Canis et al. - Quality of life after tongue reconstruction
-14/17-
better level of functioning, whereas a high score for a symptom scale or a single-item scale
represents a high level of symptoms or problems.
Table 2: Results of the EORTC QLQ-C30 and the EORTC QLQ-H&N35 quality of life ques-
tionnaires.
Legends
Figure 1: Mean values of EORTC C30 questionnaire after reconstruction and primary clo-
sure.
Figure 2: Mean values of EORTC HN35 questionnaire after reconstruction and primary clo-
sure. *p < 0.05 for comparison of reconstruction group vs. primary closure group
References
1. Bakas T, McLennon SM, Carpenter JS, et al. Systematic review of health-related
quality of life models. Health Qual Life Outcomes 2012;10:134.
2. So WK, Chan RJ, Chan DN, et al. Quality-of-life among head and neck cancer
survivors at one year after treatment--a systematic review. Eur J Cancer 2012;48(15):2391-
408.
3. Pierre CS, Dassonville O, Chamorey E, et al. Long-term quality of life and its
predictive factors after oncologic surgery and microvascular reconstruction in patients with
oral or oropharyngeal cancer. Eur Arch Otorhinolaryngol 2013.
4. McConnel FM, Logemann JA, Rademaker AW, et al. Surgical variables affecting
postoperative swallowing efficiency in oral cancer patients: a pilot study. Laryngoscope
1994;104(1 Pt 1):87-90.

Canis et al. - Quality of life after tongue reconstruction
-15/17-
5. Colangelo LA, Logemann JA, Pauloski BR, Pelzer JR, Rademaker AW. T stage and
functional outcome in oral and oropharyngeal cancer patients. Head Neck 1996;18(3):259-
68.
6. Borggreven PA, Aaronson NK, Verdonck-de Leeuw IM, et al. Quality of life after
surgical treatment for oral and oropharyngeal cancer: a prospective longitudinal assessment
of patients reconstructed by a microvascular flap. Oral Oncol 2007;43(10):1034-42.
7. McConnel FM, Pauloski BR, Logemann JA, et al. Functional results of primary closure
vs flaps in oropharyngeal reconstruction: a prospective study of speech and swallowing. Arch
Otolaryngol Head Neck Surg 1998;124(6):625-30.
8. Ye W, Hu J, Zhu H, Zhang Z. Tongue reconstruction with tongue base island
advancement flap. J Craniofac Surg 2013;24(3):996-8.
9. Fang QG, Shi S, Zhang X, Li ZN, Liu FY, Sun CF. Assessment of the quality of life of
patients with oral cancer after pectoralis major myocutaneous flap reconstruction with a focus
on speech. J Oral Maxillofac Surg 2013;71(11):2004 e1-5.
10. Urken ML, Moscoso JF, Lawson W, Biller HF. A systematic approach to functional
reconstruction of the oral cavity following partial and total glossectomy. Arch Otolaryngol
Head Neck Surg 1994;120(6):589-601.
11. Hartl DM, Dauchy S, Escande C, Bretagne E, Janot F, Kolb F. Quality of life after
free-flap tongue reconstruction. J Laryngol Otol 2009;123(5):550-4.
12. Sobin LH, Compton CC. TNM seventh edition: what's new, what's changed:
communication from the International Union Against Cancer and the American Joint
Committee on Cancer. Cancer 2010;116(22):5336-9.
13. Steiner W, Ambrosch P. Endoscopic Laser Surgery of the Upper Aerodigestive Tract.
Stuttgart, Germany: Thieme, 100-104 2000.
14. Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for
Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in
international clinical trials in oncology. J Natl Cancer Inst 1993;85(5):365-76.
Canis et al. - Quality of life after tongue reconstruction
-16/17-
15. Mehanna HM, Morton RP. Patients' views on the utility of quality of life questionnaires
in head and neck cancer: a randomised trial. Clin Otolaryngol 2006;31(4):310-6.
16. Humbert IA, Reeder SB, Porcaro EJ, Kays SA, Brittain JH, Robbins J. Simultaneous
estimation of tongue volume and fat fraction using IDEAL-FSE. J Magn Reson Imaging
2008;28(2):504-8.
17. McConnel FM, Teichgraeber JF, Adler RK. A comparison of three methods of oral
reconstruction. Arch Otolaryngol Head Neck Surg 1987;113(5):496-500.
18. Bokhari WA, Wang SJ. Tongue reconstruction: recent advances. Curr Opin
Otolaryngol Head Neck Surg 2007;15(4):202-7.
19. Salibian AH, Allison GR, Armstrong WB, et al. Functional hemitongue reconstruction
with the microvascular ulnar forearm flap. Plast Reconstr Surg 1999;104(3):654-60.
20. Longo B, Ferri G, Fiorillo A, Rubino C, Santanelli F. Bilobed perforator free flaps for
combined hemitongue and floor-of-the-mouth defects. J Plast Reconstr Aesthet Surg
2013;66(11):1464-9.
21. Chen WL, Zhang DM, Yang ZH, Wang YY, Fan S. Functional hemitongue
reconstruction using innervated supraclavicular fasciocutaneous island flaps with the cervical
plexus and reinnervated supraclavicular fasciocutaneous island flaps with neurorrhaphy of
the cervical plexus and lingual nerve. Head Neck 2013.
22. Ronis DL, Duffy SA, Fowler KE, Khan MJ, Terrell JE. Changes in quality of life over 1
year in patients with head and neck cancer. Arch Otolaryngol Head Neck Surg
2008;134(3):241-8.
23. Rogers SN, Hannah L, Lowe D, Magennis P. Quality of life 5-10 years after primary
surgery for oral and oro-pharyngeal cancer. J Craniomaxillofac Surg 1999;27(3):187-91.
24. Bozec A, Poissonnet G, Chamorey E, et al. Free-flap head and neck reconstruction
and quality of life: a 2-year prospective study. Laryngoscope 2008;118(5):874-80.

Canis et al. - Quality of life after tongue reconstruction
-17/17-
25. Verdonck-de Leeuw IM, Buffart LM, Heymans MW, et al. The course of health-related
quality of life in head and neck cancer patients treated with chemoradiation: A prospective
cohort study. Radiother Oncol 2014;110(3):422-8.
26. Ciuman R, Mohr C, Kroger K, Dost P. The forearm flap: assessment of functional and
aesthetic outcomes and quality of life. Am J Otolaryngol 2007;28(6):367-74.
27. Brown JS, Rogers SN, Lowe D. A comparison of tongue and soft palate squamous
cell carcinoma treated by primary surgery in terms of survival and quality of life outcomes. Int
J Oral Maxillofac Surg 2006;35(3):208-14.

Mean values of EORTC C30 questionnaire after reconstruction and primary closure.
254x190mm (96 x 96 DPI)
Page 18 of 19
John Wiley & Sons, Inc.
Head & Neck

Mean values of EORTC HN35 questionnaire after reconstruction and primary closure. *p < 0.05 for comparison of reconstruction group vs. primary closure group
254x190mm (96 x 96 DPI)
Page 19 of 19
John Wiley & Sons, Inc.
Head & Neck