queensland university of technology school … · queensland university of technology school of...
TRANSCRIPT

QUEENSLAND UNIVERSITY OF TECHNOLOGY
School of Nursing
Centre for Health Research
“FACTORS INFLUENCING INTERACTION BETWEEN A MOTHER AND HER PREMATURE INFANT”
Leigh Margaret Davis R.M., B.N., (Hons 1st class)

iii
KEYWORDS
Infant, premature or preterm
Depression, postpartum or postnatal
Maternal Stress
Mother-infant interaction
Mother child relations
Neonatal Intensive Care (NICU)

iv ABSTRACT
Significant relationships have been identified between elements of early
parent-infant interactions and later skills or qualities in the child. Generally speaking,
sensitive and responsive interactions between a mother and infant during the first year
of life tend to be linked with improved child developmental outcomes (Barnard, 1996;
Wyly, 1997). Research has examined the influence of infant and family risk factors
on parent-infant interaction. Family risk factors including maternal depression can
reduce a mother’s sensitivity and responsiveness to her infant. Evidence is mounting
that mothers of preterm infants experience higher rates of depression than mothers of
fullterm infants (e.g. Miles et al., 1999). Although all infants may be vulnerable to
the effects of maternal depression, the premature infant is at greater risk due to his/her
decreased responsiveness and increased need for appropriate stimulation (Field,
1995).
The purpose of this study was to examine maternal reports of depressive
symptomatology and associated variables at two time points following a very preterm
birth: at one-month postpartum (Phase 1); and 3 months after infant hospital discharge
(Phase 2). Observational data were collected at Phase 2 to explore whether maternal
depressive symptoms and associated factors influenced maternal-infant interaction.
A two-phase prospective follow-up design involved surveying mothers of very
premature infants (≤ 32weeks) who were admitted to a neonatal intensive care unit
(NICU). Multiple measurements were collected at Phase 1 and Phase 2. Mother-
infant observational data were collected at Phase 2. The subject population comprised
all eligible mothers of very premature infants who were admitted to a 60 bed tertiary
referral NICU of a major metropolitan hospital (n=62).
Mothers completed a survey at Phase 1 and Phase 2. The questionnaire
contained a number of validated instruments measuring depression, stress, social
support and coping. Maternal and infant demographic data were collated from the
hospital records. Observational data were collected and coded using the Nursing
Child Assessment Feeding Scale (Barnard et al., 1989).
Results indicated that 40% of women reported clinically significant depressive
symptomatology at one month postpartum. High maternal stress and low maternal
education and support from nursing staff were major factors explaining depression

v
scores. At Phase 2, 17% of women continued to report clinically significant
depressive symptomatology. Depression at Phase 1 and maternal stress at Phase 2
were important factors explaining Phase 2 depression scores. An exploratory
analysis of the relationship between mother-infant interaction and Phase 1 and Phase
2 variables revealed that the mothers’ coping strategies, both in hospital and at home,
were important factors in explaining mother-infant interaction.
The results support previous findings that many women suffer stress and
depressive symptoms after very premature birth. The results indicate that maternal
depression, at one month postnatally, can be predictive of maternal depression at three
months after infant hospital discharge and that very premature infants are less
responsive interactive partners. These findings highlight possible parenting
difficulties particularly during the first year.
This study has contributed to family centered research by highlighting the
importance of early postnatal experiences to the longer-term psychological health of
mothers and to the mother-infant relationship. Screening mothers of very premature
infants for postpartum depression will enable early identification of symptoms and
appropriate referral for treatment.

vi. TABLE OF CONTENTS
Contents
Page
KEYWORDS
iii
ABSTRACT ……………………………………………………………..
iv
TABLE OF CONTENTS ………………………………………………
vi
LIST OF TABLES ……………………………………………………..
x
LIST OF FIGURES …………………………………………………….
x
STATEMENT OF ORIGINAL AUTHORSHIP ……………………..
xi
DECLARATION OF ENROLMENT …………………………………
xii
ACKNOWLEDGEMENTS ……………………………………………. xiii Chapter One: INTRODUCTION TO THE STUDY 1 Background and significance of the study …………………………. 1 The purpose, objectives, and research questions …………………… 5 The purpose ………………………………………………….. 5 The objectives ……………………………………………….. 6 Research questions ………………………………………… 6 Definition of terms …………………………………………………. 7 Structure of the thesis ……………………………………………… 8 Summary …………………………………………………………… 10 Chapter Two: LITERATURE REVIEW ……………………………..
11
Introduction ………………………………………………………… 11 The Premature Birth Experience …………………………………… 11 Family response to premature birth …………………………. 11 The hospital experience ……………………………………… 14 The medical setting of NICU ……………….………… 14 System of neonatal care delivery ……………………… 16 Communication needs of parents ……………………… 19 Sources of stress ………………………………………. 22 The transition home …………………………………………. 25 Summary ……………………………………………………. 27 The Role of Early Interaction on Development …………………… 28 Parent-infant interaction …………………………………… 28 Parent-preterm infant interaction ……………………… 29 Parent-infant interaction and infant outcome …………. 32 Factors influencing parent-infant interaction ……………….. 33 Maternal depression …………………………………… 35 Social support …………………………………………. 38 Maternal education ……………………………………. 41 Summary ……………………………………………………. 42
Chapter Three: AN HISTORICAL OVERVIEW OF MOTHERS’ INVOLVEMENT IN CARING FOR THEIR PREMATURE INFANTS
vii 43
Abstract …………………………………………………………….. 43 Introduction ………………………………………………………… 45 Purpose of the historical overview ………………………………… 46 Method …………………………………………………………….. 46 Findings ……………………………………………………………. 46 Advances in medical and public health practices …………… 47 Institutionalization and professionalisation of maternal and
infant care …………………………………………………….. 51
The emergence of infant developmental research……………. 56 Discussion …………………………………………………………. 60 Conclusion …………………………………………………………. 61 Chapter Four: THEORETICAL FRAMEWORKS …………………
63
Family adaptation: theories of stress and coping ………………….. 63 Stress ………………………………………………………… 66 Coping ……………………………………………………….. 68 The Resiliency Model ……………………………………….. 69 Historical development …………………………………. 69 Current research applications …………………………… 70 Resiliency model applied to the current study ………….. 71 Stress factor (AA) ………………………………… 73 Family resources (BB) ……………………………. 73 Family coping (PSC) ……………………………… 74 Barnard Child Health Assessment Interaction Theory …………….. 76 Chapter Five: METHOD ………………………………………………
81
Research design ……………………………………………………. 81 Research questions and hypotheses ………………………….. 81 Major variables measured in the study ………………………. 83 Population and sample ………………………………………. 84 Sample size ………………………………………………….. 86 Measures …………………………………………………….. 87 Self-report instruments ………………………………….. 87 Depressive symptomatology ……………………….. 88 Maternal stress ……………………………………… 88 Social support ………………………………………. 89 Coping ……………………………………………… 91 Demographic data ………………………………………. 92 Observational data (Phase 2) …………………………… 92 Nursing Child Assessment Feeding Scale (NCAFS) .. 95 Normative data ……………………………………… 95 Reliability and validity of NCAFS …………………. 96 Procedure for data collection ……………………………………….. 98 Phase 1 ………………………………………………………. 98 Phase 2 ………………………………………………………. 99 Ethical considerations ……………………………………….. 99

Risks to participants ……………………………………..
viii 100
Protection against risks …………………………………. 100 Staff information ………………………………………… 101 Pilot study ………………………………………………………….. 101 Data analysis ………………………………………………………. 103 Summary …………………………………………………………… 105 Chapter Six: THE IMPACT OF VERY PREMATURE BIRTH ON THE PSYCHOLOGICAL HEALTH OF MOTHERS 106 Abstract of the article ………………………………………………. 106 Introduction ………………………………………………………… 107 Stress, coping and premature birth …………………………… 108 Depressive symptoms in mother’s of premature infants …….. 109 Hypothesis …………………………………………………… 110 Subjects and method ……………………………………………….. 110 Instruments …………………………………………………… 110 Demographic data …………………………………………… 112 Procedure ……………………………………………………. 112 Data analysis ………………………………………………………. 112 Results ……………………………………………………………… 112 Conclusions ………………………………………………………… 115 Recommendations ………………………………………………….. 119 Chapter Seven: THE COURSE OF DEPRESSION IN MOTHERS’ OF PREMATURE INFANTS IN HOSPITAL AND AT HOME.
120
Abstract of the article ………………………………………………. 120 Background ………………………………………………………… 120 Purpose of the study ……………………………………………….. 124 Research hypotheses ……………………………………………….. 124 Method ……………………………………………………………… 125 Participants …………………………………………………… 125 Procedure …………………………………………………….. 125 Instruments …………………………………………………… 126 Demographic data …………………………………………… 127 Data analysis ……………………………………………………….. 128 Results ……………………………………………………………… 129 Discussion…………………………………………………………… 131 Recommendations ………………………………………………….. 134 Chapter Eight: MOTHER-INFANT INTERACTION IN PREMATURE INFANTS AT THREE MONTHS AFTER NURSERY DISCHARGE
135
Abstract of the article ………………………………………………. 135 Introduction ………………………………………………………… 136 Method ……………………………………………………………… 138 Self-report data ………………………………………………. 139 Demographic data …………………………………………… 140 Observational data …………………………………………… 141
ix
Results ……………………………………………………………… 141
Discussion ………………………………………………………….. 144 Conclusions ………………………………………………………… 148 Chapter Nine: DISCUSSION AND RECOMMENDATIONS
150
Review of findings …………………………………………………. 151 Phase 1 ……………………………………………………….. 151 Hypothesis 1 …………………………………………….. 151 Phase 2 ……………………………………………………….. 157 Hypothesis 2 …………………………………………….. 159 Hypothesis 3 …………………………………………….. 160 Observational Phase 2 ……………………………………….. 163 Hypothesis 4 …………………………………………….. 163 Hypothesis 5 …………………………………………….. 164 Hypothesis 6 …………………………………………….. 166 Summary of findings ..……………………………………………... 167 Limitations of the study ……………………………………………. 169 Implications for nursing practice …………………………………… 173 Implications for further research …………………………………… 176 Recommendations ………………………………………………….. 178 Conclusion …………………………………………………………. 179 REFERENCES
183
APPENDICIES
Appendix 1 Edinburgh Postnatal Depression Scale ….………………. 218 Appendix 2 The Depression Anxiety and Stress Scale ……………… 220 Appendix 3 Social Support Interview ……..………………………… 222 Appendix 4 The Nurse Parent Support Tool …………………….…... 226 Appendix 5 The Coping Health Inventory for Parents ……………… 228 Appendix 6 Neurobiological Risk Score …………………………….. 233 Appendix 7 Nursing Child Assessment Feeding Scale: Sample items ….. 234 Appendix 8 Mothers Evaluation of Questionnaire ……………………….. 235 Appendix 9 University Human and Research Ethics Approval ……... 236 Appendix 10 Mater Mother’s Hospital Research and Ethics Approval . 237 Appendix 11 Patient Information Sheet ………………………………. 238 Appendix 12 Patient Consent Form …………………………………… 239 Appendix 13 Staff Information Sheet …………………………………. 240

x
LIST OF TABLES Table 5.1
Explanatory variables and measures
84
Table 6.1 Stress, coping and support scores: mean and standard
deviations (n=62) 112
Table 6.2 Logistic Regression Table: Significant variables
associated with the EPDS score 113
Table 7.1 Comparison of means and standard deviations over
time: depression, stress, coping family and nurse support scores (n=52)
128
Table 8.1 Characteristics of the mothers who participated in the
feeding interaction (n=50). 142
Table 8.2 Characteristics of the infants who were involved in
the feeding interaction (n=50) 142
Table 8.3 One Sample T-test and Means, Standard Deviations
of Population Sample (n=50) 143
LIST OF FIGURES Figure 1 An Adaptation of the Resiliency Model 80

xi
Statement of Original Authorship

xii
Declaration of Enrolment

xiii
ACKNOWLEDGEMENTS
This dissertation could not have been possible without the generous support and
guidance of my Principal Supervisor, Professor Helen Edwards. I am particularly
grateful to Helen for reading drafts of this thesis and her encouragement and ability to
challenge and inspire more ideas when I thought all had been said.
I would also like to express my appreciation to my associate supervisor Dr
Judy Wollin. Judy’s enthusiasm and support were essential, and greatly appreciated
throughout this process.
I am also very grateful to my other supervisor, Professor Heather Mohay for
lending me her expertise and knowledge of premature infant development. Her input
and constructive feedback was invaluable.
I wish to thank Harry Bartlett and Stephen Cox for their technical and
statistical assistance. I am also indebted to the mothers and infants who participated
in this study. Without them and their willingness to share their lives, homes and
families, this study would not have been possible.
Special thanks to my colleagues Sam, Gillian, Lorraine, Sandra, Jo, Marion
and others who made this experience such a pleasure.
Finally, I would like to express my thanks and love to my children, Serena and
Jonathan for allowing me to use ‘their’ time as ‘my’ time and to my husband Chris,
who without complaint, allowed me to develop a close relationship with our
computer.
1
CHAPTER ONE
INTRODUCTION TO THE STUDY
Advances in neonatal technology have resulted in declining mortality rates for infants
who are born prematurely. The impact of a premature and often unexpected birth and
the long-term implications for parenting has not been well studied (Miles, Holditch-
Davis, & Shepherd, 1998; Wijnroks, 1999; Wolke, 1998). The way in which each
family will cope and the outcomes of this critical experience both in the short and
long term will vary greatly according to the family and social context in which the
birth occurs. It is therefore important to understand the factors which contribute to
the development of healthy parent-child relationships when an infant is born
prematurely.
Background and significance of the study
Preterm birth accounts for 7.3% of all births in Australia, with approximately 1 in 5
being less than 32 weeks gestation (Day, Sullivan, Ford, & Lancaster, 1997). Over
the past three decades, sophisticated medical management of the premature infant has
forced back the frontiers of viability so that now smaller, sicker and more premature
infants are surviving (Lee et al., 1995; Magill-Evans & Harrison, 1999; Raddish &
Merritt, 1998; Singer et al., 1999). Until 1977, just over half of the infants weighing
between 1,000 and 1,500 grams survived (Hack et al., 1980). During the past two
decades progress in the management of prematurity has resulted in survival rates of
greater than 85% for infants weighing less than 1,500 grams (Richardson, Gray,
Gortmaker et al., 1998). Despite mortality rates decreasing, the incidence of major
handicapping conditions has not changed leading to an increase in the absolute
numbers of children with disabilities (Lorenz et al., 1998).

2
The socio-demographic characteristics of women who give birth to premature
infants has also not improved over time (Gennaro, 1996) with the incidence of
preterm birth generally increased in lower socio-economic groups (McLean, Walters,
& Smith, 1993; Peacock, Bland, & Anderson, 1995). A large number of low birth
weight premature infants are born into poverty with their families experiencing social
and health problems including drug and alcohol use (Kliegman, 1995; Najman,
Williams, Bor, Anderson, & Morrison, 1994), smoking (Kliegman, 1995; McLean et
al., 1993), low maternal education (Elder, 1994; Peacock et al., 1995), domestic
violence (Newberger et al., 1992; Stewart & Cecutti, 1993), stress and major
disruptive life events (Peacock et al., 1995; Wadhwa et al., 1993) poor nutrition and a
lack of adequate health care (Gennaro et al., 1994; Hack et al., 1995). These families
are faced with a double burden: a child with increased health care needs and a family
with limited resources to meet the needs of these special children (Gennaro, 1996).
The birth of a very preterm infant is a critical event in the life of a family and
poses many additional strains that go beyond those expected or experienced by
parenting alone. Essentially, mothers of very premature infants face a daunting task.
They assume the role of parenthood before they or their infant are ready for it. They
do so under highly stressful hospital conditions with only limited opportunities for
normal interaction with their infant. The unfamiliar and highly technological
environment of the neonatal intensive care unit (NICU) and fears for their infant’s
survival and longer term quality of life (Meck, Fowler, Claflin, & Rasmussen, 1995)
may cause additional stress for mothers of these high-risk infants. It might therefore
be anticipated that these mothers are at greater risk for postpartum psychological
distress than mothers of full-term infants (Brooten et al., 1988; Gennaro, 1988;
3
Gennaro, York, & Brooten, 1990) both during infant hospitalisation and after
discharge.
While helping these infants to survive is a commendable accomplishment,
society has been slow to address the informational, emotional, and support needs of
families of very premature infants (Meck et al., 1995). The importance of the role of
parents in the lives of preterm infants and concerns for the developmental outcomes
of these high-risk infants have received increasing attention (Wyly, 1995). When
compared to full-term infants, preterm infants are at an increased risk of disability and
developmental delay including cognitive, language and behavioural deficits
(McCormick, 1993). A number of researchers report that a substantial proportion of
healthy preterm children have developmental concerns in the area of cognitive and
language skills (Censullo, 1994; Cohen et al., 1988; Lukeman & Melvin, 1993). The
factors that influence why some healthy preterm infants do well and others have
developmental delay are not clear. Medical factors alone do not predict
developmental outcomes. Social factors and caregiving processes have been
demonstrated to outweigh medical variables as predictors of cognitive development,
language and school performance (Lee & Barratt, 1993; Liaw & Brooks-Gunn, 1993;
Lukeman & Melvin, 1993) and appear to have a more powerful role in predicting
social and cognitive outcomes among premature infants than term babies (Greenberg
& Crnic, 1988; Schraeder, Heverly, & O'Brien, 1996; Weisglas-Kuperus, Baerts,
Smrkovsky, & Sauer, 1993).
It has been proposed that one possible explanation for the differences in
developmental outcome is the establishment of sub-optimal parent-infant interaction
patterns early in the infant’s life (Sameroff, 1993). The parent-infant relationship and
interaction occurring within that relationship form the initial context in which the

4
infant experiences the world, learns about the environment and how to be a social
partner in a dyadic relationship (Barnard, 1996). Individual differences in the security
of attachment relationships appear to depend on the quality of early interaction
(Bornstein & Lamb, 1992). Developmental research studies have investigated factors
which are predictive of less optimal parent-infant interaction and have reported that
both caregiver and infant variables can disrupt either partner’s responsiveness within
the interaction. Disruption to the interactive relationship is likely to increase the
possibility of maladaptive outcomes occurring between parent and child (Barnard,
1996).
In particular, infant prematurity has been identified as a factor which can place
a strain on the developing parent-infant relationship and make it more vulnerable to
problems. A premature infant can be, behaviourally, a more difficult social partner
and this has the effect of shifting the interactive burden to the mother (Barnard et al.,
1989). Whilst infant prematurity is a recognised risk factor to the interactive
relationship, the presence of psychosocial risk factors in a parent can place the
developing mother-infant relationship in double jeopardy.
Many factors can influence the mother’s responsiveness and interactive skills
including stress, depression, and family resources (Magill-Evans & Harrison, 1999).
Studies have examined the effects of maternal depression on the interactive
relationship and found associations between depression and infant cognitive,
emotional and developmental delay, (Campbell, Cohn, & Meyers, 1995; Field, 1995;
Mayberry & Affonso, 1993; Murray & Cooper, 1997; Singer et al., 1996).
To date, there is limited research which examines the incidence and factors
associated with maternal depression in mothers of very premature infants (≤32
weeks). Furthermore, few studies have attempted to determine if maternal risk
5
factors including maternal depression, measured while the infant is hospitalised and
during the post-discharge period, continue to influence the mother-infant relationship.
Since the quality of the mother-infant relationship is important to the infant’s longer-
term outcome, early identification and intervention with families potentially “at risk”
of maladaptive outcomes will optimise both infant and family outcomes.
This two phase prospective follow-up study utilised theoretical concepts from
the Resiliency Model of Family Adjustment and Adaptation (also called the
Resiliency Model) (McCubbin, Thompson, & McCubbin, 1996) in order to gain a
greater understanding of a family’s response to the birth of a very preterm infant.
This model provided a way of understanding family responses to illness situations and
a framework that can assist in determining whether or not an illness stressor may
cause a family crisis. Family stress research indicates that two families faced with the
same illness stressor can respond in dramatically different ways (McCubbin &
McCubbin, 1993). The family’s adaptational outcome can be examined as a function
of the relationship between characteristics of the infant (degree of prematurity,
birthweight, and neurobiological risk) and the characteristics of the mother
(educational level), and the family’s resources (social support, coping behaviours and
psychological well-being).
The Purpose, Objectives, and Research Questions
The purpose
The purpose of this research was to examine mother-infant interaction at three months
post infant discharge from NICU to determine if a relationship exists between
maternal and infant data collected at one month post preterm birth (Phase 1) and three
months after infant discharge (Phase 2), and maternal-infant interaction at Phase 2.

6
The specific objectives of the study were to:
• Describe infant health status at Phase 1 (P1) and Phase 2 (P2);
• Describe available resources as reported by mothers of very preterm infants at 4
weeks post preterm birth (Phase 1) and at 3 months post infant discharge (Phase
2);
• Examine changes over time, in maternal resources as reported by mothers of very
preterm infants;
• Determine if maternal resources at P2 can be predicted from maternal resources
reported at P1;
• Describe the mother-infant interaction at three months post-infant discharge;
• Determine if maternal resources and infant health status at P1 and P2 are related to
maternal infant interaction at 3 months.
Research questions
In order to achieve the purpose of this study, the following research questions were
examined:
• Which factors are related to mothers’ reports of depressive symptomatology at
P1?
• Is there a relationship between maternal and infant data collected at P1 and
mothers’ reports of depressive symptomatology at P2?
• Is there a relationship between maternal and infant data collected at P2 and
mothers’ reports of depressive symptomatology at P2?
• Is there a difference between the mother and infant interaction scores of the study
population and the normative population?
• Is there a relationship between maternal and infant data collected at P1 and
mother-infant interaction scores at P2?
7
• Is there a relationship between maternal and infant data collected at P2 and
mother-infant interaction scores at P2?
On the basis of these research questions, hypotheses were developed and these will be
described in Chapter 5.
Definition of Terms
In order to clearly understand this study the central terms need to be explained. For
the purpose of this study, the following terms are defined in relation to infancy status:
• Infancy is the period of life between birth and the emergence of language at
approximately 18 months to two years of age (Bornstein & Lamb, 1992)
• Fullterm infant refers to those infants born after 37 completed weeks gestation.
• Preterm or premature infant refers to those infants born before 37 weeks
completed gestation (Enkin, Keirse, Renfrew, & Neilson, 1995).
Since the outcome for the premature baby differs markedly with gestational age, this
broad category has been further divided into:
• Extremely preterm or infants born less than 28 completed weeks gestation;
• Moderately preterm or infants born between 28-32 completed weeks gestation;
• Mildly preterm or infants born between 33-37 completed weeks gestation
(Lancaster, Huang, & Lin, 1996).
The infants who comprised the study sample were extremely and moderately
premature infants, however for the purpose of the study these infants are referred to as
very premature infants or infants born less than 32 weeks completed gestation.

8
Other terms included:
• Maternal resources:
a) a mother’s psychological well-being as measured by maternal self-report
questionnaires;
b) a mother’s perception of available social support from her close family and
nurses as measured by two maternal self-report questionnaires.
c) strategies a mother employs to cope with the crisis of preterm birth as
measured by a self-report coping questionnaire
• Mother-infant interaction:
a) a reciprocal process in which both mother and infant sensitively observes and
adjusts personal behaviour to the other member. Important elements of
mother-infant interaction include the behavioural repertoire of both the infant
and parent, and the reciprocity that develops as both interactive partners
respond and adapt to each other (Barnard & Kelly, 1990).
Structure of the Thesis
This thesis is presented in nine chapters with four of these chapters being in the form
of journal articles which have been submitted for publication to international peer
reviewed journals.
• Chapter 1 provides the background to the research study, the purpose, objectives
and research questions, definition of terms, and the thesis structure.
• Chapter 2 consists of a review of the literature including the impact of premature
birth on the family from the initial hospital experience to the transition home.
This chapter also examines mother-preterm infant interaction and factors which
may influence the mother-infant relationship.
9
• Chapter 3 presents a paper that has been accepted for publication in the Journal of
Advanced Nursing. This paper describes the historical context of a mothers’
involvement in caring for her premature infant. The article concludes with
evidence from behavioural research which emphasises the importance of the
mother–infant relationship in the infant’s developmental outcome.
• Chapter 4 describes the Resiliency Model of Family Stress, Adjustment and
Adaptation (Resiliency Model) (McCubbin & McCubbin, 1993) which was the
theoretical framework for this study. The Resiliency Model provides a way of
understanding how families adapt to unexpected and stressful life events such as
the birth of a very premature infant. The second section of Chapter Four describes
the Barnard Child Health Assessment Interaction Theory (Barnard Model) which
is the theoretical construct upon which the Nursing Child Assessment Feeding
Scale (NCAFS) was developed. The NCAFS was the observational tool used to
code mother-infant interaction in the present study.
• Chapter 5 describes, in detail, the methodology including research design,
outcome and explanatory variables, scientific hypotheses, data collection
procedures, instruments, pilot study, data analysis and ethical considerations.
• Chapter 6 presents a paper that has been submitted to the journal Early Human
Development and is consistent with journal guidelines. This chapter provides the
results and discussion of Phase 1 results.
• Chapter 7 has been submitted as a research paper to the Australian Journal of
Advanced Nursing. This chapter provides the results and discusses the findings
from Phase 2 and is structured according the journal’s guidelines for authors.
10
• Chapter 8 has been submitted to the International Journal of Nursing Practice.
This chapter provides the results and discusses the findings from the observational
component of the study (collected at Phase 2).
• Chapter 9 concludes the thesis by reviewing the findings as reported in chapters
six to eight. The implications of the study’s findings for further research and
recommendations for clinical practice are discussed.
Summary
Evidence clearly supports that the early relationship between a mother and her
preterm infant is linked to infant and childhood developmental outcomes. Unlike
infants born at term, premature infants have been described as more difficult to parent
during the first year and have a greater vulnerability to developmental and
neurological problems. The very difficult transition to parenthood, the stress of infant
hospitalisation and longer-term care may pose many challenges to families who may
have limited resources. These important issues are addressed in the literature review
in Chapter 2.

11
CHAPTER TWO
LITERATURE REVIEW
Perhaps no other critical life cycle event has a more profound meaning to a woman
than the period surrounding pregnancy and birth. The optimal course of pregnancy
encompasses 38 to 42 weeks during which a woman experiences complex physical
and psychological changes (Goldberg & DiVitto, 1995). The period of pregnancy
allows time for parents to prepare for the parenting role, form expectations for the
new infant and actively engage in preparation for infant care. This anticipated event
permits the parents to have some control in planning how the event develops and
takes shape. When this process is interrupted by premature delivery two to three
months before the expected date of birth, a parent’s ability to achieve an optimal
adaptation to parenthood is placed at risk (Mercer, 1990).
The first section in this chapter will discuss how the unique circumstances
surrounding premature birth can negatively influence the mother-infant relationship
and render it more vulnerable to problems. These aspects will be discussed under
three broad headings which include: the family’s response to premature birth, the
hospital experience, and the transition home. The differences in patterns of full-term
and preterm parent-infant interaction and its importance of these interactions to child
developmental outcomes will be discussed in the second section of this chapter. This
is followed by a discussion of some of the psychosocial factors, which have been
shown to influence the early interactive relationship between the mother and infant.
The Premature Birth Experience
Family Response to Premature Birth
For almost all families, the birth of a premature infant and the associated perinatal
problems are experienced as an acute emotional crisis which is characterised by

12
anxiety, grief, denial, depression, stress and for some parents, anger and blame (Allen,
1995; Goldson, 1992). The circumstances surrounding the birth and admission to the
neonatal intensive care (NICU) are thought to have a powerful influence on the
psychological and social adjustment of the parents and to the parent-infant
relationship (Greene, Fox, & Lewis, 1983). In many instances, families have no
warning of a premature or hazardous delivery and parents are typically unprepared for
the birth (Hughes & McCollum, 1994).
In stark contrast to mothers of healthy full-term infants who have unrestricted
access to their infant in the immediate period following birth, mothers of very preterm
infants are deprived of these early experiences because of the acute medical nature of
their infant’s condition. Often these infants are taken immediately after birth to the
NICU to commence life saving treatment before the mother has been able to touch or
see the infant (Easterbrooks, 1988). In some cases infants may have to be transported
to a different hospital where intensive care facilities are available. In this situation,
mothers may not see the baby for the first few days of life.
Separation from their infant has been described as the worst and most painful
aspect of having a baby admitted to NICU (Redshaw, Harris, & Ingram, 1996). Many
parents may experience perinatal grief reaction which often relates to the ‘loss’ of a
full-term pregnancy and the subsequent reward of a healthy ‘normal’ baby
(Wallerstedt & Higgins, 1996). Instead their ‘real’ child is a small, frail and often a
physically unattractive baby who seems to become the possession of a complex array
of NICU staff (Mander, 1994; Sammons & Lewis, 1985).
Linked to the experience of separation from the infant, is the loss of role and
identity as the infant’s parent (Redshaw et al., 1996). Premature birth will require
parents to make adjustment from the parental role which they had hoped to fulfil
13
(Mander, 1994). Protecting and caring for your baby is an essential element in
parenting and yet, many parents are unable to assume this very basic role in the initial
stages of the NICU experience. The NICU staff rather than the mother become the
infant’s primary caregiver (Mander, 1994). Parents have had little time to prepare for
this transition to parenthood and may not even feel like parents because they are
psychologically not ready to end the pregnancy (Sammons & Lewis, 1985). They do
not have a baby that they can care for, and they have no alternative role. A number of
recurring themes compound the stress and inadequacy experienced by these parents.
Uncertainty about their infant’s survival, the inability to feel in control of their
infant’s care, feelings of isolation, difficulties forming attachments and anticipatory
grief can place the parents into disequilibrium (Affleck, Tennen, & Rowe, 1991;
Allen, 1995; Pitts Berns, Geiser, & Levi, 1993).
Feelings of guilt and self-blame are almost inevitable and accompany any
major life loss. Whether or not a basis for guilt can be identified, many parents feel
responsible for their infant’s condition (Allen, 1995; Pitts Berns et al., 1993). This
response of shattered expectations and assumptions has been likened to the reactions
of people who encounter other upsetting and unexpected events such as becoming
seriously ill, the grief of losing a loved one, being the victim of a criminal assault or
surviving a natural disaster (Affleck et al., 1991).
It has been suggested that the key to understanding the family experience of
NICU is to recognise and understand the normal reactions to grief and loss. Parents
have lost their control over the course of labour and delivery and the celebration of
birth with family and friends. Parents have also lost their anticipated fullterm baby
and instead have a fragile baby who is not with them but being cared for by the NICU
14
staff. Their anticipated role as new parents is also lost and replaced by a strange and
difficult form of parenting (Goldberg & DiVitto, 1995).
The next section will discuss the families’ experience and participation in the
NICU while their infant is hospitalised and how the process of care can influence the
evolving parent-infant relationship.
The Hospital Experience
Advances in medical technology have meant that smaller, sicker preterm infants are
being assisted to survive. Whilst this is a major achievement it can mean increased
family stress. Researchers have emphasised that understanding of the nature of this
stress, the coping abilities or resilience of families, and how best to support families is
crucial for professionals providing care to these infants and their families (Affleck et
al., 1991; Berry & Hardman, 1998).
Parents can experience many difficulties when trying to establish meaningful
and positive interactions with their premature infant during hospitalisation (Moehn &
Rossetti, 1996) . In the following discussion these difficulties have been thematically
organised and relate to the medical setting of the NICU, the way in which the system
of neonatal care is organised, the communication needs of parents and sources of
stress.
The Medical Setting of NICU
The pattern of care that often characterises a modern hospital is one of high-turnover,
short-term acute care, focused on medical needs rather than social concerns. Many
NICUs traditionally function within this acute-care medical model, with priority given
to the immediate demands of direct patient care and little time identified to assist
family members in coping with this crisis (Gilkerson, Gorski, & Panitz, 1990). The
NICU environment is strange and unfamiliar to parents, usually crowded with

15
technical equipment and a large number of medical and nursing staff who work as
multiple caretakers and providers of information. The pace of activity, the bright
lights and the noise all violate common beliefs of what a nursery should look like.
Research has shown that when parents see their infant for the first time they
are often shocked by the infant’s small size and distressed by the countless tubes,
wires and machines (Hughes & McCollum, 1994; Miles, 1989; Miles, Funk, &
Kasper, 1992). In one study, mothers described the emotional distancing and the
unreality that accompanied them on their first visit to the NICU (Affleck et al., 1991).
Unable or perhaps unwilling, many parents do not feel immediate affection for their
infant and can face difficulties in becoming emotionally attached to their baby in
hospital (Affleck et al., 1991). Parent’s impressions, feelings, and experiences on that
first visit play a key role in parenting and determining later parent-infant interactions
(Gennaro, 1991; Harrison, 1990).
Parents and family must also face the stress and uncertainty associated with
the severity of their infant’s medical condition and whether the infant will survive or
suffer long term disability (Wereszczak, Miles, & Holditch-Davis, 1997). While
research shows that both parents are distressed by the birth and hospitalisation of a
preterm infant, mothers are likely to report more distress than fathers (Affleck et al.,
1991; Levy-Schiff, Sharir, & Mogilner, 1987; Miles et al., 1992). The intense stress
and anxiety may lead to such difficulties as an inability to establish a satisfying
relationship with the infant, ambivalence toward interacting with the infant, and a
perception of the infant as “different” or “abnormal”(Perehudoff, 1990). Research
indicates that these factors and subsequent difficulties in bonding or attachment may
result in problems coping with the infant after discharge, inadequate parenting, family
breakdown and even child neglect and abuse (Perehudoff, 1990)

16
System of neonatal care delivery
One of the difficulties that NICU staff encounter when dealing with families in
crisis is they typically have received little or no formal training in how to manage
differing family responses to crisis. Neonatal nursing texts and other high-risk
neonatal texts stress the importance of the families psychosocial needs and the critical
importance for nurses to possess assessment skills in order to facilitate family
adaptation to crisis (Best, 1993; Lefrak-Okikawa & Lund, 1993; Pitts Berns et al.,
1993). However, when compared to the volume of text devoted to infant care issues,
information on how to understand and safely support the family during the critical
stages of infant hospitalisation and beyond is given very little attention (Best, 1993;
Lefrak-Okikawa & Lund, 1993; Pitts Berns et al., 1993). This early relationship
between NICU staff and the mother is vitally important because prolonged separation
from the infant causes the mother to become reliant on staff for information and
support. Inadequate understanding and preparation to support families in crisis can
lead to additional distress for parents and staff especially when discrepancies occur
between perceptions and expectations (Able-Boone, Dokecki, & Smith, 1989; Miles,
D'Auria, Hart, Sedlack, & Watral, 1993; Perehudoff, 1990). In the clinical context,
inflexible rules and policies and differing interpretations of these often prevent parent
orientated care from occurring (Redshaw et al., 1996).
There has also been relatively little research investigating how critical care
nurses perceive their role with families (Fox & Jeffrey, 1997). In one study focusing
on nurse practitioners in an adult critical care facility, it was acknowledged that nurses
were in a unique position to facilitate family coping during the stress of critical
illness. However, the likelihood that this would occur was dependent on the extent to
which nurses perceive this to be a legitimate and realistic part of their role (Fox &

17
Jeffrey, 1997). While nurses were supportive, in principle, of fulfilling families’
informational needs, there was less agreement regarding the nurses’ role in
interventions which required them to provide families with emotional support or
counseling. Over half of the nurses were unsure or disagreed that it was realistic for
nurses to support families in addressing their emotional needs (Fox & Jeffrey, 1997).
Similar findings have been reported in the neonatal setting. Even when the
infant has progressed from requiring highly technical intervention and is at a growing
stage (Meck, Fowler, Claflin, & Rasmussen, 1995), nursery activity still functions
from a task-orientated perspective and nursing roles continue to be medically and
technically focused (Beal, Maguire, & Carr, 1996; Fenwick et al., 1999; Griffin,
1990; McGrath & Conliffe-Torres, 1996). A majority of interactions with mothers by
NICU nurses have been reported as primarily instrumental, i.e. the provision of
information about a feeding activity, the infant’s progress or explanations of medical
procedures (Fenwick et al., 1999).
Other studies have investigated neonatal nurses’ perceptions of barriers to
parenting in the NICU and their role with families (Walker, 1997, 1998). It was
found at both a local and national level that a large majority of nurses believe the
barriers to parenting included not only technical equipment but the parents themselves
through their emotional responses such as anxiety, fear, guilt and anger (Walker,
1997, 1998). There was also a general consensus that none of the nursing practices,
policies, or procedures contributed to obstacles confronting parents and nurses
considered that they provided an environment that facilitated parenting and parent
interaction with their infant. Only a small proportion of nurses believed that nurses'
attitudes, policies, procedures and staff turnover could interfere with parents fulfilling
their parental role (Walker, 1997, 1998). In fact nurses have attributed stress directly

18
to parents themselves and the belief that environmental and parental psychological
responses prevent parents from assuming their parental role (Walker, 1997, 1998).
This finding has also been supported in other studies where nursery activity
and interaction seemed to reflect control by staff rather than partnership with parents
(Callery & Smith, 1991; Fenwick et al., 1999). It seems that parents often participate
in a supervised capacity with little opportunity to direct or negotiate care (Fenwick et
al., 1999) and are not encouraged to step outside the established unit guidelines
(Walker, 1997, 1998). These results corroborate with other studies which suggest that
nurses have a limited understanding of potential barriers to parenting, or the
implications of restricting parenting activities and parental involvement with their
infant (Bogden, Brown, & Foster, 1982; Dobbins, Bohling, & Sutphen, 1994).
It appears that parental needs and opportunities for interaction may be met
inconsistently due to the varied perceptions among nurses regarding their
responsibility, coupled with an inadequate preparation of many neonatal nurses to
support the parent-infant relationship. The distinctive role of neonatal nurse
practitioners within the NICU needs further exploration in the light of research
evidence which indicates that parent-health care provider interactions can lay the
foundations for the parents’ satisfactory adjustment to the infant and the situation
(Able-Boone et al., 1989).
It seems to follow then that parents of critically ill preterm infants are not
routinely or systematically assessed to determine their adjustment to the crisis of their
infant’s premature delivery or their ongoing needs. There is also no method currently
employed which could assist nurses to identify those parents who are experiencing or
are likely to experience difficulties (Gennaro, 1996). Family assessment can be
arbitrary and subjective and may not accurately reflect family coping, resources or
19
resilience factors. Each parent brings a different set of experiences and expectations
to the NICU and it is tempting for staff to give most of their time and energy to the
most capable and temperamentally easy parents (Allen, 1995). Parents who need the
most assistance may receive very little and be given less opportunity for parent-infant
interaction (Allen, 1995). Authors have commented that NICU staff appear to have
developed a system for categorising families with some parents being thought to have
potential while others are viewed as difficult or problematic (Allen, 1995). Bogden et
al. (1982) warn that such judgments tend to be made too quickly and are based on
limited information, “short observations”, “limited or no conversation”, and “second-
hand reporting.” This type of labeling is likely to have a negative impact on the
staff’s relationship with parents and families and perhaps indirectly on the parent-
infant relationship.
Communication needs of parents
The ease and the ability of the parents to obtain and understand information about
medical procedures, the feeding of their infant and their own feelings and responses is
a source of situational stress and anxiety for many parents (Bialoskurski, Cox, &
Wiggins, 2002; Meck et al., 1995; Redshaw et al., 1996). Throughout the infant’s
hospitalisation, parents need accurate and timely information about their infant’s
condition. The capacity of parents to retain information, however, may depend on
how this is provided by staff (Meck et al., 1995; Redshaw & Harris, 1995). Families
can only absorb so much information during times of stress and therefore the delivery
of information needs to be paced, relevant and timely (Brunssen & Miles, 1996; Meck
et al., 1995). To begin with, parents have reported feeling overwhelmed by the noise,
exposure to other sick infants, the crowd of health care personnel and seemingly
relentless medical procedures involving their infant (Allen, 1995). As a result,

20
parents have reported feeling disorganised, distraught and unable to concentrate or
process much information (Affleck et al., 1991; Allen, 1995; Redshaw et al., 1996).
It is clearly important to ensure that opportunities are provided for information
to be discussed again and talked through more frequently so that parents can extract
information and clarify misunderstandings when they are ready to hear and
understand. In one study where mothers were interviewed at six weeks post notional
term (i.e 46 weeks), 30% of mothers of very preterm infants had little or no
understanding of the information they had been given during the period of neonatal
intensive care (Calam, Lambrenos, Cox, & Weindling, 1999). It was found that even
in the presence of a good explanation, some mothers used cognitive strategies to
protect themselves from any bad news regarding their infant’s condition in addition to
the difficulty grasping medical information (Calam et al., 1999). It has been
suggested that parents should be told as much as possible using a caring and
empathetic approach (Quine & Pahl, 1987). However, there is a question of who is
authorised to give information to parents. In one study, doctors were generally seen
as the appropriate experts in this role and that generally nurses tended to avoid
answering questions (Quine & Pahl, 1987).
Another obstacle for parents receiving information about their infant is that
many NICUs do not have a well-developed system of primary care so that any
number of health care staff can be responsible for the same infant during the course of
hospitalisation. Parents may have to tell their story over again to each new nurse
assigned to the infant’s care. The presence of multiple information and care givers can
result in parents receiving conflicting and inconsistent information about the infant’s
current condition, changes in condition and long-term outcomes (Bialoskurski et al.,
2002; Pitts Berns et al., 1993). There may also be an incongruence between

21
professional expectations and parental reactions to infant related information (Affleck
& Tennen, 1993; Calam et al., 1999). The professional may feel that they have
provided good information in an appropriate manner, while the parent may recall little
of what has been said, and express anger about the professional involved (Calam et
al., 1999).
Technical information or jargon can also constitute a barrier during
communication between staff and parents (Dobbins et al., 1994; Fenwick et al., 1999;
Plass, 1994). In one study, analysis of observer comments showed that while engaged
in information exchanges with mothers, nurses failed to adequately assess the
mother’s current level of knowledge (Fenwick et al., 1999). Other research findings
have indicated that some nurses tend to deliver information in a didactic fashion,
telling parents rather than communicating with them (Brown & Ritchie, 1990; Callery
& Smith, 1991). These patterns of communication do not result in relationship
building where sharing and negotiation are important elements (Fenwick et al., 1999).
The NICU staff members are a key resource for parents who need information and
support and while in many instances provide a great deal of help they are also often
busy. Parents may not feel able to ask questions or express concerns and can find it
difficult to understand the exact nature of their baby’s problem or medical procedures
and equipment used (Redshaw et al., 1996). Mothers who have more negative
experiences in NICU have reported problems rising from asymmetrical
communication with the nursing staff leading to uncertainty, anxiety and increased
stress (Redshaw & Harris, 1995; Wereszczak et al., 1997). Conflicting instructions
and information, differences between stated policy and actual practice have created
barriers to effective parental involvement in the infant’s care (Hurst, 1993).
22
A recent study (Bialoskurski et al., 2002) asked mothers of premature infants
cared for in NICU to indicate their needs and priorities by completing a questionnaire.
Mothers indicated their need for accurate, reliable and topical information regarding
their infant’s status, the importance of having their questions answered and the need
for regular communication. Mothers identified their need to talk to the same nurse
regularly and with the doctor every day as very important to satisfy their needs
(Bialoskurski et al., 2002).
Sources of stress
Although studies have investigated parental stress related to the sights and sounds
within the NICU, environmental stress has been reported as one of the areas of least
stress to parents (Miles, 1989; Miles, Funk, & Kasper, 1991; Miles et al., 1992).
Research studies have consistently found that changes in the parental role and the
appearance of the infant have been among the highest sources of stress for parents
(Miles, 1989; Miles et al., 1991, 1992). Parental role alterations included physical
separation from their infant, feeling helpless at not being able to protect their infant or
knowing how to help their infant, not being able to hold their infant and even being
afraid to do so (Miles & Holditch-Davis, 1997). Concerns about the infant’s
appearance included the infant’s small size and limp, weak appearance, seeing the
infant in pain or perceiving that the infant looked frightened or sad (Miles &
Holditch-Davis, 1997). Mothers have reported vivid memories of these stress factors
up to three years after the birth (Wereszczak et al., 1997).
The loss of the normal parental role may be compounded by a struggle to
negotiate a caregiving role with neonatal nurses caring for their infant (Miles &
Frauman, 1993). This early relationship between NICU staff and a mother is
important because prolonged separation from the infant causes her to become reliant
23
on the NICU staff for information and support. Staff behaviours and attitudes can
inhibit or encourage parenting skills and on occasions conflict about the parenting role
can arise between parents and staff (Pitts Berns et al., 1993). This situation can
escalate into a struggle for control. Parents may view staff as surrogate parents or the
infant as belonging to staff, since it is the staff who are providing the most care (Pitts
Berns et al., 1993). Mothers and nurses both share a deep concern for the well-being
of the infant, a related sense of responsibility and overlapping roles. However, many
mothers find themselves unequal partners in role negotiations and must learn
strategies to cope with their altered role successfully (Miles & Holditch-Davis, 1997).
Relationships with staff can become a source of stress when discrepancies occur
between perceptions and expectations (Able-Boone et al., 1989; M.S. Miles et al.,
1993; Perehudoff, 1990). To date, there has been relatively little research on the role
of nurses involved with families during times of crisis and the influence that
professional support can have on parental adjustment and long-term adaptational
outcome (O’Brien et al., 1999).
Mothers may also have to deal with extraneous stressors from numerous
sources outside the acute health-care situation (Hughes & McCollum, 1994). These
external stressors may be unknown to NICU personnel but could influence parents’
perceptions and interactions in the NICU (Hughes & McCollum, 1994). Family
research indicates that crises in a family evolve and are resolved over time, and
families are seldom dealing with a single illness-induced crisis (McCubbin &
McCubbin, 1993). Instead families can experience a pile-up of demands and may be
trying to manage stress in other aspects of their lives. The outside stressors which the
family may have to simultaneously cope with could include financial concerns, illness
24
of other family members, or marital stress, all of which can complicate parental
adjustment (Pitts Berns et al., 1993).
In a study by Hughes & McCollum (1994), many parents commented on the
more immediate stressors such as difficulty in arranging child-care for siblings, which
in turn prevented them from visiting their sick infant. Parents in this study reported
that extended family and friends did not understand what they were going through and
they had difficulty explaining what was happening to their infant because of the
acuteness and variability of the situation (Hughes & McCollum, 1994). There seems
to be an unintentional lack of support for vulnerable parents. Family and friends may
not know what to say or how to respond and in some cases do not respond for fear of
worsening the circumstances by saying “the wrong thing” (Mercer, 1990). Clinicians
caring for these vulnerable parents may unconsciously respond to mothers’ healthy
reactions to crisis with avoidance behaviours because they are also uncomfortable and
afraid of saying the wrong thing (Mercer, 1990).
Another stressful transition which all mothers encounter relates to their
infant’s discharge (Brooten et al., 1988). Generally speaking, follow-up services for
preterm LBW infants are fragmentary and episodic and therefore inadequate for
families of ‘at-risk’ infants (Gennaro et al., 1991; Pritchard & Colditz, 2001). Post-
discharge services also vary widely among institutions in terms of which infants are
eligible for care with a great variation in the services that are provided (Gennaro,
1996; Raddish & Merritt, 1998). A number of studies have found that perceiving
little support for their parental role in the NICU, parents did not feel prepared to take
on their parental responsibilities at discharge (Brooten, Gennaro, Knapp, Brown, &
York, 1989; Butts et al., 1988; Kenner & Lott, 1990). The transition home does not
always mean the infants problems are resolved, and introduces new threats to parents’
25
adaptation and coping ability for virtually all parents of preterm infants (Affleck et al.,
1991).
The Transition Home
Although the transition home is often eagerly anticipated, it can be overwhelming for
parents who will assume full responsibility for an infant who for weeks or months has
been regarded as medically fragile (Easterbrooks, 1988; Miles & Holditch-Davis,
1997). While it is beyond the scope of this study to consider long term threats to
parental adaptation, the longer term health and development of medically fragile
infants and uncertainty of the outcome has been reported to be of concern to parents
for some years after discharge (Affleck et al., 1991; McKim, 1993; Wereszczak et al.,
1997).
Some parents have found that the challenges after discharge seemed fewer,
generally less intense, and more easily met than those described by other parents at
discharge. Many mothers recalled the first few months as a satisfying time compared
to what they had faced during their infant’s hospital stay or what they had feared
might happen once they took their infant home (Affleck et al., 1991). However,
unlike parents of fullterm infants, parents of preterm infants may have unique long-
term stress associated with the health and development of a medically fragile infant.
One of the most difficult problems that many parents encounter in the first few
months at home is the infant’s continuing medical problems and dependence on
medical technology (e.g. apnoea monitors, oxygen therapy) (Affleck et al., 1991).
Other issues for parents frequently include the need for medication, poor weight gain,
and recurrent illness and increased number of rehospitalisations (Affleck et al., 1991;
Blackburn, 1995). It has been reported that preterm, very low birthweight infants

26
have rehospitalisation rates that are three to four times higher than those of term
infants (McCormick, Workman-Daniels, Brooks-Gunn, & Peckham, 1993).
Another difficulty may be the exhausting routine of caring for a medically
fragile infant. Mothers have reported important caregiving issues including a lack of
sleep arising from the infant’s unpredictable sleep patterns, frustration over feeding
problems and an inability to soothe the infant’s crying and distress (Affleck et al.,
1991; Hughes, Shults, McGrath, & Medoff-Cooper, 2002). Although these
caregiving issues may be an expected hurdle of early parenthood for all new mothers,
it may be especially challenging to mothers of preterm infants (Hughes et al., 2002).
Preterm infants have been reported to be more difficult to parent than full-term
infants, at least for the first year of life (Gennaro, Tulman, & Fawcett, 1990;
Langkamp, Kim, & Pascoe, 1998). Many preterm infants have behavioural and
temperamental characteristics that render them more difficult and less responsive
interactive partners (Crnic et al., 1983; Field, 1977; Landry et al., 1990).
Parents may also perceive that their infant is fragile and in need of special
protection. Some parents experience considerable anxiety in the first few weeks at
home over whether the baby may still die without warning (Affleck et al., 1991).
Others may engage protective measures such as keeping their infant at home for fear
of exposing them to infection or not leaving their infant in the care of others (Affleck
et al., 1991; Vasquez, 1995). These mothers may find themselves isolated from
family and friends temporarily or for prolonged periods depending on the infant’s
medical needs (Vasquez, 1995).
Other sources of stress reported by some mothers have resulted from conflict
over differing perceptions of infant care held by extended family members and
friends. Contradicting opinions over the infant’s need for special protection can be a

27
subject for debate in many families (Affleck et al., 1991). Tension can arise within
the family over differing perceptions of the infant’s developmental progress. In one
study mothers were distressed that family and friends were unwilling to see the infant
as a “normal child” and unable to understand that it would take longer for the preterm
infant to “catch up” developmentally (Affleck et al., 1991; Gennaro, 1996).
Generally, research studies have not addressed the factors which may affect a
parent’s capacity to adjust their parenting strategies to cope with the nuances of
premature birth and negotiate the many challenges facing the early parent-infant
relationship.
Summary
These very different early experiences for parents mark the beginning of a transition
to parenthood that is uncertain and has been described by some mothers as an
emotional “rollercoaster ride” (Allen, 1995; Eckerman & Oehler, 1992). The preterm
birth experience often occurs as an unanticipated crisis, which occurs before the
parents are physically and psychologically “ready” to begin parenting. The parents
may find that their role is irreversibly altered and early social interaction with their
infant proceeds under very different constraints than for the full-term infant
(Eckerman & Oehler, 1992). These early difficulties may be compounded by a
system of neonatal care which is less prepared and unresponsive to the psychosocial
needs of parents. Parents must not only adjust to the birth and the long-term
implications of prematurity but must learn to adapt to caring for a medically fragile
infant at home.
There is very little information written about the effects of the NICU
hospitalisation on early parental adaptation at home and the influence that these
experiences have on mother-infant interaction. The literature has indicated that
28
medical factors alone do not predict developmental outcome. The way parents
perceive their preterm infant, as well as parent-infant interaction, are important
elements in the longer term developmental outcomes of the premature infant
(Beckwith, 1986; Chapieski & Evankovich, 1997; Crnic & Greenberg, 1987). The
fundamental importance of early parent-infant interaction and its impact on infant
development are reviewed in the next section.
The Role of Early Interaction on Development
Parent-Infant Interaction
During the first year of life, mothers constitute a large proportion of the social
environment of their infants and mediate their experience of the external world (Beck,
1996b). Mothers are a vital source of stimulation in the emotional and cognitive
domains as well as social development for their infants (Beck, 1996b). It has been
argued that early parent-infant interactions are critical to the infant’s development
status and that adaptive parent-interaction provides the foundation of infants’
cognitive, social-emotional and language development and serve as a basis for later
communication with others (Wyly, 1997). Early mother-infant interaction establishes
trust and security and enables an infant to develop healthy emotional ties which are
vital to the attachment process (Wyly, 1995). A positive relationship between
supportive parent-infant interactions and later development has been well documented
(Barnard & Kelly, 1990; Beckwith, 1986; Beckwith & Rodning, 1996; Beckwith,
Rodning, & Cohen, 1992; Crnic, Greenberg, & Slough, 1986). As a result of
successful attachment infants learn about themselves and their environment and ways
to control their environment. Infants and caregivers also learn to adapt to one another
and continually modify their interactions.

29
The ability of the mother to be sensitive and responsive to her infant’s signals
has been proposed as the central feature in interactions which foster development of
optimal or “secure” patterns of attachment and child development (Donovan, Leavitt,
& Walsh, 1998; Wilfong, Saylor, & Elksnin, 1991). Conversely, “insecure”
attachments are thought to develop as a result of a mother’s inconsistent response or
‘insensitivity’ to her infant’s cues (Ainsworth, Blehar, Waters, & Wall, 1978).
Models of mother-infant interaction have been proposed which put forward a
connection between maternal psychological and social factors and sensitivity to infant
behaviour (Teti & Gelfand, 1991). Important variables such as maternal mood, social
support, marital harmony, and infant characteristics or medical condition are
hypothesised to play a role in altering maternal sensitivity and responsiveness which
in turn impacts on the maternal-infant relationship (Donovan et al., 1998). The exact
patterns of influence may vary between groups of infants with different biological risk
conditions. Prematurity has been shown to be a biological risk condition which can
alter mother-infant interactive relationship and findings from a number of studies
have documented interactional patterns which distinguish preterm and full-term
infants (Harrison & Magill-Evans, 1996).
Parent-Preterm Infant Interaction
Differences in interaction between a mother and her preterm infant are evident
shortly after birth. Premature birth thrusts both the infant and parent into new ways of
interaction, perhaps before either is well equipped for the interactions that are
customary after birth. According to Eckerman & Oehler (1992) early postnatal social
interaction is dramatically different for very premature infants and parents in at least
two ways. Firstly, social interaction occurs at a much earlier point in development and
therefore the premature infant is not well prepared to deal with social stimulation

30
typically provided to a fullterm infant. These infants may respond more slowly in a
variable, disorganised, even avoidant manner to stimulation by parents and provide
complex behavioural cues that are less easy for parents to interpret (Eckerman &
Oehler, 1992; Hughes & McCollum, 1994; Pitts Berns et al., 1993). Coupled with
these behavioural differences, the infant’s small, frail appearance may be far from
attractive to parents and may alter the impact of infant behavioural cues (Eckerman &
Oehler, 1992). This can create much anxiety and confusion in parents as they
attempt early interaction with their infant (Hughes & McCollum, 1994; Pitts Berns et
al., 1993). Secondly, social interaction begins not only with an immature infant but
also in many instances, a sick infant, at risk of non-normative neurological
development. As a result of the differences in neural system development there is a
possibility that any two premature infants may differ markedly in their characteristics
as early social partners (Eckerman & Oehler, 1992). Some parents may firmly
establish a rewarding and reciprocal parent-infant interactive experience whilst the
infant is in NICU, for others, the relationship is not reciprocal and instead a frustrating
interactive experience occurs between caregiver and infant (Wyly, 1995).
Even throughout the first year of life, premature infants have been reported to
be less alert, less active and less responsive, initiate interaction less often, to be less
able to provide clear distress signals and to be more easily stressed and overstimulated
than full-term infants (Bakeman & Brown, 1980; Eckerman, Hsu, Molitor, Leung, &
Goldstein, 1999; Eckerman, Oehler, Hannan, & Molitor, 1995). The degree of
prematurity and the severity of neonatal medical problems predict early
developmental delays (Anderson et al., 1996; Landry, Denson, & Swank, 1997).
These developmental problems may further influence interaction (Buka, Lipsitt, &
Tsuang, 1992; Fiese, Poehlmann, Irwin, Gordon, & Curry-Bleggi, 2001). In
31
particular, factors contributing to these differences are likely to be related to the
medical, physiological or neurological vulnerabilities that accompany prematurity.
Neurological factors including intraventricular haemorrhage (IVH) may impose
greater limitations on the repertoire of movements available for use as behavioural
cues (Bigsby, Coster, Lester, & Peucker, 1996; Gorga, Stern, & Ross, 1985).
Mother-infant interactions have been found to be less satisfying for mothers of
premature infants especially where there is neurological dysfunction, than compared
to those between mothers and full-term infants (Bakeman & Brown, 1980; Bigsby et
al., 1996; Greenspan, 1992; Wille, 1991; Yoder, 1987). The stress related to the
infant hospitalisation and the immature and disorganised behaviour of the premature
infant may have an adverse influence on parenting and parent-infant interactions
during the first year of life (Crnic, Ragozin et al., 1983; Field, 1979; Minde,
Whitelaw, Brown, & Fitzhardinge, 1983). Mothers of premature infants may have to
work harder to initiate and maintain interaction than mothers of full-term infants, but
in return receive fewer positive responses from their infant (Harrison, 1990). Some
preterm infants have been reported to make more frequent use of avoidance
behaviours such as gaze aversion or arching in response to social approaches from
mothers who are diligently attempting to connect with their infant (Crnic, Ragozin et
al., 1983; Greenspan, 1992). Infants that become overloaded by environmental
stimuli respond by shutting down and tuning out (Lester, Hoffman, & Brazelton,
1985) and these behaviours have the potential to frustrate caregivers’ attempts at
interaction.
Several reports have shown that mothers appear to be more active in initiating
and maintaining interaction and show a heightened level of stimulation throughout the
first year of an infant’s life (Bakeman & Brown, 1980; Crnic, Ragozin et al., 1983;
32
Field, 1979). Some authors have suggested that the mothers’ behaviour with preterm
infants reflect their efforts to compensate for deficiencies in their infants’ interactional
abilities (Goldberg & DiVitto, 1995; Miles & Holditch-Davis, 1995). However while
mothers of preterm infants can be more active in their interactions they may be also
less sensitive and responsive to their infants (Barnard, Bee, & Hammond, 1984;
Censullo, 1994) and generally provide less appropriate stimulation in early infancy
than mothers of full-term infants (Holditch-Davis & Thoman, 1988). Decreased
maternal responsiveness is of concern as researchers have reported that preterm
infants whose mothers talked to them more during observations at one month of age
had markedly higher Wechsler Intelligence scores at 12 years of age (Sigman, Cohen,
Beckwith, Asarnow, & Parmelee, 1992). Greenberg and Crnic (1988) found that
mothers’ satisfaction with parenting and affect toward the infant when the child was
one month old were predictive of the preterm child’s language development at two
years of age (Greenberg & Crnic, 1988). These studies demonstrate the important
effect of maternal behaviour and affect in interactions upon the development of
preterm children.
Evidence from numerous studies has contributed to the notion that parents of
preterm infants may face unique challenges beyond those expected of parenting a full-
term infant (Goldberg & DiVitto, 1995). Moreover preterm infants are a
heterogeneous group, with considerable variation in medical and neurological
histories. Infants with greater medical and neurobiological risks may be expected to
present a greater challenge to caregivers based on the infant’s behavioural
organisation.
33
Parent-Infant Interaction and Infant Outcome
The importance of early parent-infant interaction is well established. Substantial
research since the 1970s has identified important links between the quality of parent-
infant interactions and child developmental outcomes (Barnard & Kelly, 1990;
Beckwith & Cohen, 1984; Bee et al., 1982; Crnic, Ragozin et al., 1983; Magill-Evans
& Harrison, 1999; Morisset et al., 1990). Significant relationships have been
identified between specific elements of the early parent-infant interaction and later
skills or qualities in the child. Generally speaking, positive interactions during the first
years of life tend to be linked with improved subsequent social, intellectual and
language abilities (Barnard, 1996; Wyly, 1997). Furthermore, maternal
characteristics including dimensions of emotional involvement, warmth, and
sensitivity to infant’s cues have been positively related to accelerations in infant
development (Wyly, 1997). In one preterm sample, maternal sensitivity during play,
that is, following the infant’s cues rather than ignoring or rejecting cues, and
responsiveness and sensitivity were found to be powerful predictors of later language
and social competence (Beckwith & Rodning, 1996). In the same study, the degree to
which mothers spoke responsively when their infants vocalised was associated with
the children’s language ability at three years and social competence at five years of
age (Beckwith & Rodning, 1996).
Through repeated positive interactions with parents, infants become securely
attached to their parents and this has many advantages for an infant’s development.
Securely attached infants view their parents as a security base from which to explore
their environment and this has been found to lead to greater social competence in
toddlerhood (Wyly, 1997). However there are many factors which can influence the
mother-infant interactive relationship.
34
Factors Influencing Parent-Infant Interaction
Prematurity and its associated medical problems have an effect on the infant’s
interactive responsiveness, however the significance of the problem is increased in the
presence of family risk factors. Family variables are also important predictors of
developmental outcomes for preterm infants (Gyler, Dudley, Blinkhorn, & Barnett,
1993; Lee & Barratt, 1993). A growing body of research indicates that biological
and environmental risks interact over time to influence children’s development
(Sameroff, Seifer, Barocas, Zax, & Greenspan, 1987; Spiker, Ferguson, & Brooks-
Gunn, 1993). Research examining the cumulative risk to children’s development has
found that as the number of biological and psychosocial risks increase, cognitive
outcomes decline (Liaw & Brooks-Gunn, 1993; Sameroff, Bartko, Baldwin, Baldwin,
& Seifer, 1998).
Perhaps the most extreme reaction which can result from the accumulation of
biological and environmental risk factors is child abuse or neglect. Infant prematurity
has been identified as a risk factor for later child abuse (Browne, 1997). Maternal
depression as measured by elevated scores on the Edinburgh Postnatal Depression
Scale has also been found to be a powerful predictor of later child abuse potential
(Cadzow, Armstrong, & Fraser, 1999). One study which examined the aetiology of
child abuse in the first year from factors measured soon after birth found that maternal
depression, low maternal education, low social support and the presence of other
dependent children in the home were predictive of reports of child maltreatment
(Kotch et al., 1995). In a later study, it was found that even in those families with
lower levels of maternal depression and/or life event stress, low social support
significantly increased the risk of a maltreatment report by as much as a factor of four
(Kotch, Browne, Dufort, & Winsor, 1999).
35
Therefore the risk factors chosen for the study are factors which have been
shown to post a risk to the parent-infant relationship not only in the child abuse
literature but also from other studies. Maternal variables included maternal
depression, educational level, the perception of social support and coping behaviours.
The infant variables included the degree of prematurity, birthweight, Apgar scores,
length of hospital stay and medical risk status.
Maternal Depression
Research studies have consistently demonstrated that 10-15% of postpartum
women experience depressive symptomatology severe enough to meet the criteria for
a diagnosis of depression (O'Hara & Swain, 1996) with greater than 60 % of these
women having symptom onset within the first four weeks postpartum (American
Psychiatric Association, 1994; Stowe & Nemeroff, 1995). Since these estimates are
derived from full-term populations, the question of whether there is a difference in
rates between full-term and preterm populations has yet to be investigated (O'Brien,
Heron Asay, & McCluskey-Fawcett, 1999). Some authors have suggested that
mothers of premature infants may be at greater risk of psychological distress than
mothers of fullterm infants (Gennaro, 1988; Pederson, Bento, Chance, Evans, & Fox,
1987). In fact there have been a wide variety of estimates of postpartum depression in
mothers of premature infants depending on the instrument used, the timing of
administration and the particular population of premature infants studied. Many
studies have reported depressive symptoms in mothers of premature infants during
infant hospitalisation (Meyer et al., 1995; Miles, Holditch-Davis, Scher, & Schwartz,
2002; Miles, Holditch-Davis, Burchinal, & Nelson, 1999; O'Brien et al., 1999; Singer,
Davillier, Bruening, Hawkins, & Yamashita, 1996; Spear, Leef, Epps, & Locke, 2002;
Younger, Kendell, & Pickler, 1997). Some studies have reported that women who
36
have been depressed initially have continued to be depressed even up to twelve
months post infant discharge (Logsdon & Davis, 1997; Miles, Carlson, & Brunssen,
1999; Thompson, Oehler, & Catlett, 1993). However other studies have reported that
symptoms of depression had subsided by 8-12 months after discharge (Brooten et al.,
1988; Singer et al., 1999). In view of conflicting results, there is a clear need for
more longitudinal studies examining depression in mothers of preterm infants to
determine if the prevalence and predictors of depression differ between mothers of
preterm and full-term infants (Meyer et al., 1995; O'Brien et al., 1999).
In general, research indicates that no single factor can be identified as a cause
of postpartum depression but that it develops as a consequence of a complex interplay
of biological and psychosocial risk factors (Cooper & Murray, 1998; O'Hara, 1997).
A meta-analysis of 44 studies was conducted to determine the magnitude of the
relationship between postpartum depression and predictor variables including a
history of previous depression, social support, life stress, child care stress, and marital
satisfaction (Beck, 1996a). The results indicated that each of these variables had a
moderate effect size, although it was acknowledged that the significant correlations
between the predictor variables and postpartum depression in no way implied
causation (Beck, 1996a).
Women experiencing postpartum depression frequently suffer disabling
symptoms including loss of interest in usually pleasurable activities, fatigue,
difficulties in concentrating or making decisions, anger, over-sensitivity, and sleeping
difficulties (Stowe & Nemeroff, 1995). These symptoms not only significantly
impair a woman's interpersonal functioning (O'Hara, 1997), but also substantially
reduce the pleasure a woman experiences in mothering and interferes with the
development of a positive mother-infant relationship (NICHD, 1999; Stuart &

37
O'Hara, 1995). Studies have found that depressed mothers exhibit less happy, more
dysphoric affect than non-depressed mothers and are often preoccupied and
inattentive toward their children (Gelfand & Teti, 1990; Radke-Yarrow, Zahn-
Waxler, Richardson, Susman, & Martinez, 1994). Depressed mothers are more likely
to behave insensitively with their infants in a hostile intrusive manner or with
detached withdrawal (Radke-Yarrow, 1998; Tronick & Weinberg, 1997). Infants of
depressed mothers have been shown to be more avoidant, discontent, and withdrawn
(Field, 1995). Developmental outcomes for infants of unresponsive, depressed
mothers have been shown to be disturbed in both cognitive and affective domains
(Teti & Gelfand, 1997). If the mother's depression continues, by one year of age the
infant begins to show growth and developmental delays (Field, 1995). If symptoms
of depression become chronic, mothering may be further impaired. A number of
studies have reported that women who were chronically depressed were less positive
with their infants during face-to-face interactions and less sensitive during feeding
and play than women whose depression was only intermittent (Campbell, Cohn, &
Meyers, 1995; Frankel & Harmon, 1996; NICHD, 1999).
The associations between maternal depression and child outcomes are
extremely complex (Cummings & Davies, 1994; Downey & Coyne, 1990). It is
therefore not surprising that research findings have been inconsistent. Not all studies
have found a direct relationship between maternal depression, negative
responsiveness or maternal disengagement (Campbell et al., 1995; Cooper, Murray,
Hooper, & West, 1996; Ruttenberg, 1999; Teti & Gelfand, 1991). The heterogeneity
of depression, including variations in type, severity, chronicity and timing may
contribute to inconsistent findings (Downey & Coyne, 1990). Results may also vary

38
according to whether community samples, clinical samples or high-risk groups were
studied (Lowenstein & Field, 1992; Teti, Gelfand, Messinger, & Isabella, 1995).
As mentioned previously, it is the culmination of biological and psychosocial
risks rather than the presence of one risk factor that poses a threat to the parent-infant
relationship and long term child outcomes (Liaw & Brooks-Gunn, 1993; Sameroff et
al., 1998). However, since many people who are exposed to stressful life events or
chronic stress situations do not develop significant psychiatric impairments, research
interest has shifted to factors such as social support and coping strategies that can
ameliorate the impact of stress and promote resilience in families (Kessler, Price, &
Wortman, 1985)
Social Support
Social support is a term that has been widely used to refer to the mechanisms by
which interpersonal relationships are presumed to protect people from the deleterious
effects of stress (Kessler et al., 1985; Pierce, Sarason, Sarason, Joseph, & Henderson,
1996). Several researchers have pointed to the importance of systems of social and
emotional support which can assist parents to respond to the crisis of preterm birth
(Blackburn & Lowen, 1986; Caflin & Meisels, 1993; Crnic et al., 1986; Hodnett,
1998; Logsdon & Davis, 1998). The influence of stress and social support on an
individual’s physical and psychological well-being has been studied extensively
(Gottlieb, 1981; Gottlieb & Pancer, 1988) and essentially has demonstrated the role of
social support as a coping resource and protective factor during times of stress
(Mueller, 1980; Siegel, 1992).
During the 1980s Crnic and colleagues investigated the influence of a number
of maternal correlates of preterm mother-infant interaction including social support,
life stress and satisfaction with parenting (Crnic et al., 1983a; Crnic et al., 1984; Crnic

39
et al., 1986; Crnic et al., 1983b). The results from these studies found that both
perceived stress and social support significantly predicted maternal attitudes and the
quality of mother-infant interaction at 4 months (Crnic et al., 1983a; Crnic et al.,
1984). Mothers with greater stress were less positive in their attitudes and behaviour
while mothers with greater social support were significantly more positive. In
general, intimate support proved to have the most positive effects. Maternal social
support was also found to have significant effects on infant interactive behaviour
(Crnic et al., 1983a; Crnic et al., 1984). In a later study, Crnic et al. (1986) reported
that stress and support from various sources including professional support were
related to parent and infant outcomes at 8 and 12 months corrected age.
The influence that parents’ social networks have on parenting and subsequent
child development has suggested that support networks have an effect on parenting
attitudes and behaviours which influence, directly and indirectly, child development
(Crnic et al., 1983a). Social support has been identified as a primary mediator of the
impact of stressful events on an individual (Siegel, 1992). Research also suggests that
an individual’s perception of the adequacy of support is more important than the
number of persons who are available in a person’s network. Furthermore social
support may be an individual-difference resource, in that some individuals may
possess greater skills at making use of potential sources of support than others
(Barnard et al., 1988; Siegel, 1992).
The role of social support in families of the ‘high-risk’ infant has been
conceptualised as a moderator variable under conditions of stress. Within this focus,
the infant risk conditions are considered stressors with potentially adverse influences
on the family (Crnic et al., 1983b). A study which focused on the influence of social
networks on mother-infant interaction in a very low birthweight (VLBW) sample
40
found that the density of the social network was related to less maternal sensitivity in
the VLBW group (Zarling, Hirsch, & Landry, 1988). The authors suggested that the
finding of large social networks being more stressful for mothers’ of VLBW infants
reflected the network’s sense of helplessness and confusion over how to be helpful
(Zarling et al., 1988). The stress resulting from such a critical event may cause
parents to distance themselves from people around them or even disengaging from the
baby in order to protect themselves against possible loss (Allen, 1995; Eckerman &
Oehler, 1992). Distancing can occur between parents, their friends, other members of
their family and even the most caring professional (Allen, 1995). Parents have
reported that extended family and friends did not understand what they were going
through and they had difficulty in explaining what was happening to their infant
because of the acuteness and variability of the situation (Hughes & McCollum, 1994).
In this situation, families may not know how to respond and their efforts to support
the mother may be seen as intrusive or inappropriate (Affleck et al., 1991;
Easterbrooks, 1988; Zarling et al., 1988). Other premature infant studies have also
found correlations between social support and the quality of mother-infant interaction
(Feiring, Fox, Jaskir, & Lewis, 1987; Zahr, 1991).
Spousal support has been reported to be significantly related to new mothers’
positive emotional states (Crnic et al., 1983a). Spousal/partner support is frequently
the primary source of support for the mother (Belsky & Vondra, 1989). The
interaction between a mother’s psychological well-being and partner relationship may
be particularly important in the case of premature birth with it’s accompanying stress.
In one study, high levels of spousal support was associated with lower levels of
depression and increased perceptions of family functioning in mothers of premature
infants at six weeks after the infant’s homecoming (O'Brien et al., 1999). However,

41
stressed families with adequate support systems, remain more functional overall and
more effective at facilitating infant development (Crnic et al., 1983).
Maternal Education
Studies have examined other environmental factors including maternal education (less
than twelve years) which can place an infant ‘at risk’ of less optimal infant outcomes
(Sameroff et al., 1998). When examining cumulative risk factors in families of
premature infants, Liaw & Brooks-Gunn (1993) reported in one study that risk factors
occurred more frequently in poor families, and as the number of risks increased, child
IQ decreased. Conversely, children with consistently above-average cognitive scores
were more likely to have Caucasian mothers with higher educational (Liaw & Brooks-
Gunn, 1993).
Other studies have examined the relationship between mother-infant
interaction and other clusters of maternal variables in preterm low birth weight
samples. These variables have included maternal education, socio-economic status,
ethnicity, and depressive symptoms. Maternal education was found to be a significant
predictor of mother-infant interaction at 30 months in a cohort of low birthweight
infant (Spiker et al., 1993) and was significantly related to developmental outcome at
four years (R. J. Thompson, Jr. et al., 1997). Maternal responsiveness and maternal
education have also been shown to significantly predict play maturity in a large cohort
of low birth weight toddlers (Bee et al., 1982; Fewell, Casal, Glick, Wheeden, &
Spiker, 1996). Low maternal education has been associated with less positive
emotion during interaction with preterm children (Leila Beckwith & Rodning, 1996).
It has been suggested that there may be a different interactional dynamic
operating between high and low education families in their response to high levels of
life change or low levels of social support (Bee et al., 1982). Behavioural researchers
42
studying the impact of life change have argued that adults do vary predictably in their
ability to handle high levels of personal stress. In particular, adults with better
personal support systems and more education are thought to be better able to endure
episodes of high life change (Dohrenwend & Dohrenwend, 1978; MacFarlane,
Norman, Streiner, Roy, & Scott, 1980).
Summary
The strong link shown between parent-infant interactions and infant developmental
competence underscores the need to assist parents when interactions are potentially at
risk (Wyly, 1997). Assessment of risk factors in families of premature infants in the
postpartum period offers an important opportunity to intervene as parents have
extensive contact with the medical system and are more likely to be amenable to
intervention. However, little is known about the psychosocial adjustment of parents
during their infant’s hospitilisation and how these experiences, and the family context
in which the birth occurs, influence the early interactive relationship between a
mother and her preterm infant.
It is only within the last 25 years that parents have been allowed to have
contact with their premature infant. The next chapter will briefly review the
historical context of a mothers’ involvement in the care of her premature infant and
how the confluence of research findings finally paved the way for parents and
families to be in closer contact with their premature newborn.

43
CHAPTER THREE
AN HISTORICAL OVERVIEW OF MOTHERS’ INVOLVEMENT IN CARING FOR THEIR PREMATURE INFANTS
The previous chapter provided a review of the literature addressing the crisis nature of
premature birth and how the unique circumstances surrounding the birth can place a
strain on the early mother-infant relationship. The review included evidence of the
fundamental importance of mother-infant interaction to the long-term developmental
outcomes for the preterm infant and factors which may influence that early
relationship. The purpose of this chapter is to provide an historical context to the
development of hospital-based premature infant care and the current trends which
have allowed parents even greater access to their hospitalised infant.
This chapter is presented in the format of a journal article which has been published in the Journal of Advanced Nursing 42 (6) 578-586 .
ABSTRACT
Background
Advances in technology have resulted in increasing survival rates even for extremely
premature infants. While sophisticated medical management is vital to the infant’s
survival, research has found that social factors and care giving processes are important
predictors of the infant’s later outcome. Consequently, evidence is accumulating to
demonstrate the fundamental role of the mother and family to the optimal
developmental outcome of the premature infant.

44
Aim and Method
The aim was to undertake an historical overview of premature infant care practices to
increase neonatal nurse’s knowledge of the crucial role of mothers and families in the
care of their premature infants. Understanding past practice and current trends can
provide neonatal nurses with critical insight which will assist in formulating current
and future care.
Research and historical articles focusing on maternal involvement in preterm infant
care from the development of the incubator to the present time were examined. A
search of the literature between 1960 and 2002 was conducted using MEDLINE,
CINAHL and PSYCLIT. Search terms included premature infant, neonatal intensive
care, history, and maternal care.
Findings
From an analysis of the selected literature, three major themes were identified which
reflect the development of neonatal care. Firstly, over the last century, advances in
medical and public health practice saw the decline in mortality rates for mothers and
infants. Secondly the application of this new knowledge resulted in the
institutionalisation and professionalisation of obstetric and neonatal care which, in
turn, resulted in the isolation of infants from their mothers.
Finally, concurrent advances in infant research emphasised the importance of the
mother–infant relationship to the infant’s developmental outcome resulting in greater
flexibility in hospital practices regarding parental contact with their infant.
Conclusion
As biomedical advances in technology continue to help smaller, sicker premature
infants to survive, neonatal nurses are strategically placed to promote positive

45
outcomes for premature infants and their families through the integration of social
science and behavioural research into nursing practice.
INTRODUCTION
The development of the infant incubator in the late 19th century was credited with
helping to save the lives of premature infants who would have otherwise perished.
During the past 2 decades increasingly sophisticated technology and the medical
management of premature infants has resulted in survival rates of greater than 85%
for infants weighing less than 1,500 grams (Richardson et al., 1998). The general
concept of a limit to viability has been discarded as intense efforts to prolong the lives
of even smaller, sicker infants have escalated (Cone 1985a; Lee et al. 1995; Magill-
Evans & Harrison 1999; Raddish & Merritt 1998; Singer et al. 1999). However while
mortality rates have decreased the proportion of children with major handicapping
conditions has not changed and actual numbers of children with disabilities has
steadily increased (Lorenz et al. 1998). These morbidity concerns and the longer-
term consequences of these developments on the family are less clear. It is possible
that the additional responsibilities and expectations of parenting a very premature
infant may compromise some families competency in basic parenting (Raddish &
Merritt 1998).
A growing body of research evidence points to the fundamental importance of the
mother and family caregiving environment to optimal outcomes for the premature
infant. Neonatal nurses play a pivotal role in facilitating the early mother-infant
relationship. They are the health professionals with whom the mothers and family

46
have the most contact and are ideally placed to promote positive outcomes for mother
and infant by the integration of both biomedical and family developmental research.
PURPOSE OF THE HISTORICAL OVERVIEW The purpose of this historical overview was to provide neonatal nurses with greater
knowledge of past and current practices and the impact of these practices on the
involvement of mothers and families in the care of their premature infants. The
specific aims were to identify historical and research articles that described the
evolution of premature infant care and to examine the influence of the care practices
on maternal involvement.
METHOD
This review examined selected studies and texts from the historical, theoretical and
research literature from 1960 to 2002. These works were identified from the
CINAHL, MEDLINE and PSYCHLIT databases for the selected years. The studies
included described the expansion of premature infant care practices from the
development of the infant incubator to the present time, with a focus on maternal
involvement in infant care. Only articles and texts printed in English were included
and these were identified using key search terms of premature infant, neonatal
intensive care, history, mother-infant interaction, infant outcomes and maternal care.
The method used to analyse selected works consisted of in-depth reading to identify
emerging and consistent themes and the relationship of those themes to the purpose of
the study.
FINDINGS
From the analysis of the selected literature, three distinct phases and associated
themes were identified in the evolution of premature infant care practices. Together
47
these major phases and themes formed the organizing framework for this historical
overview. The first phase began with the development of the incubator in the late
1800s and the emerging theme was the changes and advances which occurred in
medical and public health practices in the first half of the 20th century. The second
phase occurred in the post war era and the theme dominating this period was the
institutionalisation and professionalisation of maternal and infant care. The final
theme, the emergence of infant developmental research and its impact on care
practices also had its beginnings in the post war years.
Advances in Medical and Public Health practices Concerted efforts to rescue infants born prematurely began following the
immeasurable loss of life during the siege of Paris in the Franco-Prussian war of
1870-1871 (Cone 1985b; Silverman 1980). The low birth rate and exceedingly high
infant mortality spurred French physicians to attempt to rebuild a population that had
been decimated by war and famine (Cone 1985b; Desmond 1991). According to
Silverman (1980), England correspondingly saw a steady decline in the birthrate and
the need to preserve the lives of all infants ‘... even the prematurely born…’ was
regarded as important for economic as well as sentimental reasons (Silverman 1980;
p.10).
The infant incubator was developed by a French obstetrician, Tarnier in the 1880s
as a way to preserve the lives of premature infants. In the wake of this development
controversial claims were made by the French that the incubator could lower
premature infant mortality by as much as 50% (Baker 1996). Simple incubators with
glass walls were designed to promote maternal involvement, allowing the mother to
see the infant. Opportunities were also provided for breastfeeding (Baker 1996).
48
Budin, an associate of Tarnier, also advocated the use of an incubator to assist in
providing environmental control for the premature infant. Budin, however, recognised
the practical limits of these activities designed to save premature infants and
acknowledged that infants less than 1,000 grams were seldom able to be saved (Cone
1985a). Budin asked an associate, Couney, to demonstrate the effectiveness of the
incubator at the Berlin Exposition. Since premature infants were not expected to live,
German physicians allowed Couney to care for them until they were ready to go home
(Kennell & Klaus 1976). Couney charged admission fees to the public who wished to
view these infants, although mothers who were not allowed to care for their infants
while in the exhibit, were exempt from paying these fees (Kennell & Klaus 1976).
Couney raised awareness that premature infants could survive and develop as normal
people. In 1901, Couney arrived in the United States for the Pan-American
Exposition in New York where he exhibited Budin’s techniques. An incubator baby
show was staged complete with live premature infants. Unlike his mentor, Budin,
Couney did little to involve the mothers in the care of their infants and it was
documented that he experienced difficulty in persuading mothers to take their
‘survivors’ back after the infants had been on tour (Klaus & Kennell 1993; Goldberg
& DiVitto 1995). Although Couney’s exhibitions were seen as a highly commercial
venture and in dubious taste, he brought recognition of the success of these techniques
in caring for the premature infant who would otherwise have perished (Silverman
1980). Couney’s example became the foundation for many new hospital-based
premature nurseries. The principles of care stressed cleanliness and sterility to the
exclusion of active maternal involvement. The introduction of hospital-based
neonatal care improved infant survival rates but also increased the separation of
49
mothers and their premature infants (Goldberg & DiVitto 1995). In this pre-antibiotic
era, the threat of infection continued to be a significant deterrent to allowing mothers
into the nursery (Kennell & Klaus 1976).
While the scientific understanding of infant pathology increased dramatically
under the leadership of such luminaries as Koop, Lubchenco and Drillen, (Lubchenco
et al. 1963; Drillien 1968; Koop 1993) it was limited and consequently medical
management of this highly vulnerable population was often conducted without the
evidence of formal trials (Oppenheimer 1996). Gradually, unforeseen complications
from infant treatment procedures began to be recognised in the 1940s and 1950s. The
introduction of oxygen therapy in the 1930s was credited with increasing the survival
rates of infants. However, retrolental fibroplasia (an abnormal increase of fibrous
tissue behind the lens of the eye) was described as causing blindness in over 10,000
infants worldwide (Oppenheimer 1996) as a result of excessive concentrations of
oxygen in the incubator (Goldberg & DiVitto 1995; Silverman 1980). Similarly,
antibiotics offered new hope in the prevention of infection in the prematurely born,
but their untested and indiscriminate use meant that some infants were left wholly or
partially deaf (Goldberg & DiVitto 1995) while others suffered kernicterus and often
fatal brain damage (Oppenheimer 1996).
Respiratory distress syndrome was another serious problem and a leading cause of
death in liveborn premature infants in the early fifties (Avery 1992). Initially it was
thought that the cause of respiratory problems in the premature neonates was related
to ‘germs’ with parents as the potential carriers. Consequently, parents were banned
from contact with their infant (Goldberg & DiVitto 1995). In an effort to describe the
pathogenesis of what was to become known as hyaline membrane disease, theories of
50
aspiration were described. It was feared that if an infant were to aspirate any liquid,
respiratory problems could worsen. This belief lead to the introduction of another
untested practice; withholding all food or fluids for up to 4 days (Avery 1992;
Oppenheimer 1996). This practice persisted from the early fifties to the late sixties
and increased the probability of severe acidosis, dehydration, spastic diplegia and
lowered neonatal survival rates (Oppenheimer 1996). Despite the identification in
1949 of hyaline membrane disease (functional immaturity of the lungs) as the primary
cause of these respiratory problems, parents continued to be excluded from contact
with their infants (Goldberg & DiVitto 1995). It was later recognised that much of
what was done for infants with respiratory distress was experimental and never
evaluated as to its efficacy (Avery 1992).
While concern for the high infant mortality rates had been an almost exclusive
focus of policy makers and physicians in public health during the early 1900’s,
concern for women’s health and welfare emerged as infant mortality decreased
(Lewis 1991). Maternal mortality had not improved and a medical investigation of
the complex causes of maternal mortality suggested that the only solution was to
hospitalise women for childbirth (Lewis 1991). The legitimacy of science and the
ideology of professionalism were used as justification for the gradual decline of
midwife attended home births and the rise in the number of hospital births. To some
extent, the move from home to hospital was lead by physicians who persuaded
women that hospitals were the safest places for childbirth (Lewis 1991). In addition,
women’s attitudes to their own health gradually changed including expectations in
relation to childbirth (Beinart 1991). Growing numbers of women from the working
classes began to expect greater professional attendance whether in the form of a

51
doctor or midwife, as well as analgesia during childbirth and a hospital bed in case
something should go wrong (Roberts 1984).
This period was marked by many changes in medical and public health practices
which formalised the provision of hospital based maternal and infant care.
Institutionalisation and professionalisation of maternal and infant care
In the post-war era, changes were being witnessed not only in premature baby care,
but also in maternity hospital practices. Furthermore, a new found interest in the
capacities of young infants emerged and proliferated in the 1950s and 1960s. The
combination of these developments had a positive influence on mothers’ involvement
in the care of their premature infant. The more significant of these changes will now
be discussed.
Post-war changes in premature baby care
According to Silverman, an extraordinary change in attitude toward saving the lives of
premature infants took place in the mid 1950s. To some extent this change was a
delayed reaction to a wave of medical optimism resulting from the huge success of
antibacterial treatments, immunisation programs, and antenatal glucocorticoid drug
therapies in the first fifteen years after World War II (Cone 1985a). Rapid expansion
in the treatment of premature infants was taking place in American nurseries.
Silverman suggested that this expansion was related to affluence and public awareness
of the problem of prematurity in the postwar period (Cone 1985a). Countrywide
statistics cited prematurity as the most frequent cause of death in infancy. America
was in a financial position to direct its attention and resources to deal with public
health issues of national importance (Cone 1985a)

52
In the 1960s, neonatology emerged as a recognised medical specialty (Goldberg &
DiVitto 1995). New techniques for reducing the incidence and severity of the
complications of prematurity were developed. These developments included
techniques for assisted breathing, equipment and pathological tests to detect
physiological problems, new surgical techniques, feeding methods and drugs. Infants
were unwrapped and nursed naked in an incubator, examined more thoroughly and
observed more closely than ever before (Goldberg & DiVitto 1995). Silverman,
suggested that the attack mounted to meet this pubic health problem was similar in
many ways to the all-out strategies that were used to bring about victory in the recent
war, that is, the mobilisation of vast material resources and rapid increases in
technological development (Cone 1985a).
However, despite earlier recognition of the iatrogenic complications, which led to
blindness and deafness in infants, the belief that parents were a source of infection and
should therefore be excluded from the care of the preterm infant persisted (Goldberg
& DiVitto 1995). The prevailing hospital policy in the 1960s and early 1970s was to
permit parents to enter the nursery for the first time only a day or two prior to infant
discharge, if at all (Kennell & Klaus 1976). Handling was considered to be stressful
for the premature infant and affectionate and nurturant handling was kept to a
minimum. The primary human contact for these infants was through invasive medical
procedures (Goldberg & DiVitto 1995). The cost of highly trained staff and
specialised equipment for this small proportion of births forced neonatal intensive
care units (NICU) to be situated in regional medical centres rather than in local
hospitals. The unintended consequence of this change meant further separation of
families and infants due to the fact that infants needed immediate transportation to

53
NICUs for treatment (Goldberg & DiVitto 1995). Mothers would remain in local
hospitals and cling to their infants through photographs and phone conservations with
staff caring for the infant (Plass 1994). Fathers had to divide visiting time between
mother and baby. Restricting contact between parents and term infants was also
practiced but research findings began to challenge these longstanding hospital
practices and increased contact between parents and infant began to be permitted.
These concessions were slowly extended to parents of premature infants, however
when families were able to visit their infant, the impact of the NICU environment and
the presence of highly trained professionals was intimidating to frightened and
anxious parents who often felt overwhelmed, isolated, and insignificant to their
infant’s survival (Goldberg & DiVitto 1995). Throughout the 1960s and early 1970s,
NICU care continued to concentrate on infant survival through temperature control,
nutrition and the maintenance of a sterile environment to prevent infection (Plass
1994). The role of parents and family dynamics were not considered to be within
NICUs ambit.
Some important changes in the direction of maternity and neonatal service
provision occurred in the late 60s and 1970s. A daring experiment was reported from
Stanford University Medical Centre that marked a major transition in neonatal care.
Barnett and colleagues questioned whether parents of premature infants suffered from
severe deprivation due to separation from their infants (Barnett et al. 1970). For the
first time since Budin, mothers were permitted into the NICU soon after birth to
handle and care for their premature infants who were still in incubators (Kennell &
Klaus 1976; Goldberg & DiVitto 1995). To evaluate whether parents would introduce
infection into the premature nurseries, cultures were taken weekly from the umbilicus,

54
skin, and nares of each infant for the entire period their mother was allowed into the
unit incubator (Kennell & Klaus 1976). Infection rates were compared to periods
when parents were not allowed into the nursery and findings clearly did not support
the expected increased occurrence of infection (Barnett et al. 1970).
These data demonstrated conclusively that parental contact was not hazardous for
premature infants and led health professionals to question the traditional policy of
separation. The results led to research investigating the effects of increased contact
between mothers and premature infants. Investigators reported that mothers who
were permitted to enter the nursery showed a greater commitment to their infant, more
confidence in their mothering abilities and increased stimulating and care-taking skills
(Kennell & Klaus 1976). As a result, hospital practices shifted toward allowing and
encouraging parents to visit the NICU to handle and care for their infants (Goldberg
& DiVitto 1995).
Changes in maternity hospital practices.
Despite changes in neonatal care practices, childbirth continued to be viewed as a
medical event, which required expert help. In the early 1970s, the medical model for
childbirth continued to shape the birth experience and almost all expectant women
had their babies delivered in hospital with consultant obstetricians taking over the
ultimate responsibility for childbirth (Wagner 1994). Interventionist obstetric
techniques including induction of labour, intrapartum fetal monitoring, instrumental
deliveries, and caesarean sections reached unprecedented peaks in the 1960s and
1970s (Schwarz 1991). Mothers and infants were kept separate by institutional
barriers: such as, the central nursery, regimented feeding schedules where the infant
55
was brought to the mother every 3-4 hours for feeding then returned to the nursery,
and hygiene regulations (Romito 1986; Wagner 1994).
However, social developments in the late 1960s and 1970s saw changes in the
organisation of maternity care and the rise of ‘maternity pressure groups’, who began
to call into question routine maternity practices and demand change (Romito 1986;
Reiger 2001). Attempts to change the management of birth included reducing the use
of analgesic drugs, allowing women greater freedom of movement and improved
emotional support, which included having their husband/partner present to act as
‘labour coaches’ (Reiger 2001; Wagner 1994). Other consumer groups wanting to
improve breastfeeding rates targeted the traditional practice of separation of mother
and baby and regimented feeding practices (Reiger 2001; Wagner 1994). This rapidly
changing social environment also shaped the political movement towards encouraging
more ‘natural’ birth and feeding. Consumer awareness also increased and there was
an upsurge in the critique of the power of professionals in society (Wagner 1994).
The medical establishment was under attack both from within and without, leading
some medical educators to express a more radical vision of medicine. The social and
preventative role of health care was stressed rather than the traditional emphasis on
curing disease (Reiger 2001). Also emphasised was the client’s need to be more
involved in decision-making about their care rather than merely accepting doctors’
orders (Reiger 2001). In response to pressure from women’s demands for change,
institutions attempted to ‘humanise’ childbirth and provide a more family-centered
approach so that women could exercise more power of choice (Romito 1986).
56
While developments in hospital based obstetric and neonatal care continued to
evolve, research into infant behaviour and development provided new evidence of
the competency of new born infants.
The emergence of infant developmental research.
Renewed interest in the capacities of young infants and later infant development
began to burgeon in the 1950s and 60s. It was argued then that the questions
concerning infancy had been asked before, but because of advanced technology,
researchers believed they had the capacity to measure, enumerate and explore
variables which previously were not able to be explored or even considered (Lewis
1967). Researchers attempted to quantify and make sense of the infant’s apparently
‘haphazard spontaneous and elicited behaviour’ (Wolff 1965). Research findings
demonstrated that the infant was not a passive recipient of a parent’s socialisation but
a ‘highly complex and sophisticated organism’ (Lewis 1967). Through longitudinal
investigations of a variety of infant responses, researchers began to gain a greater
understanding of infant behaviour. Extensive research documented how infants are
capable of organised, spontaneous behaviour from birth (Korner 1964).
It was observed that even in the first postnatal week, infants who cried and were
picked up and soothed would frequently remain in a state of visual alertness. These
brief times of visual alertness when the infant could scan and become acquainted with
the environment were seen by some as the earliest opportunity for infant learning and
perhaps crucial to early development (Korner & Grobstein 1966). Studies attempted
to find a bridge between neonatal behaviour and later infant development (Korner
1964). It was thought that through the study of neonatal behaviour it might be
possible to evaluate an infant’s cognitive and behavioural potential. It was further

57
hypothesised that early behaviour may be an indicator of later vulnerability (Korner
1964).
In the 1950s and 60s, it was widely accepted, that the infant had little or no pattern
vision during the early weeks or months of life because of immaturity of the eye and
brain or the absence of need for visual learning (Fantz 1963). This view was
challenged by direct evidence from studies which showed that infants have reasonably
acute pattern vision, showed greater interest in patterned rather than plain colours,
could differentiate between patterns and showed increased interest in patterns similar
to the human face (Fantz 1963). These discoveries lead to experiments in the late
60s, which observed the repertoire of infant behaviours in response to the human face.
Results indicated that even a very young infant could fixate, smile and vocalise when
presented with an adult face stimulus (Lewis 1967). Studies which investigated the
origin of social responsiveness showed that the infant was aware of a clear
contingency between his/her behaviour and an environmental stimulus (Watson
1973). The key findings were that caregivers have a vital role in initiating and
responding to the infant but that infants also actively contribute to social interactions
(Watson 1973). Prior to these findings the mother was generally seen as the active
partner in the relationship and the infant as the passive recipient of her attention.
As a result of these and other discoveries, the emphasis changed from studies of
individual infant behaviours to examination of the patterns of early social behaviour
and their development within the context of the earliest social relationship – mother-
infant dyadic interaction (Schaffer 1999). This research represented a major
paradigm shift from the ‘unidirectional’ model, which proposed that an infant’s
socialisation was entirely a product of the attitudes and beliefs of parents and what

58
they did as a result of the particular child-rearing practices they adopted (Schaffer
1999). Within this new model, the infant’s developmental progress was seen as being
influenced by biological characteristics including prematurity, as well as the social or
physical environment in which development occurred (Barnard et al. 1988). This
bidirectional approach acknowledged that the infant has an influence on the parent
and therefore there is reciprocity of parent and infant influences (Schaffer 1999)
acting together in a mutually dependent system. The 1970s marked an increase in the
studies of reciprocity and detailed analysis of the structure of parent-infant
interactions (Goldberg & DiVitto 1995) and set in motion studies that would establish
important links between the qualities of early parent-infant interactions and child
development outcomes (Beckwith & Cohen 1984; Bee et al. 1982; Crnic et al. 1983).
At this time, Klaus and Kennell, became interested in the detrimental effects of
separation on parent-infant bonding - the process whereby parents come to feel an
emotional investment in their infant (Klaus & Kennell 1976). A primary motivation
for their interest was the observation during the previous 15 years, that small
premature infants who were sent home intact and thriving would sometimes return to
the emergency rooms, battered by their parents or failing to thrive (Klaus & Kennell
1976). Bonding theory was based on the idea that there was a critical or sensitive
period in the first hours and days after birth when a positive bond can be established
between parent and infant. The consequences of unsuccessful bonding were negative
and long-lasting and included an increased risk of child abuse (Klaus & Kennell
1976). The growing understanding of the importance of early contact stimulated the
rapid acceptance of the bonding theory and the practice of ‘rooming-in’, which
allowed infants to stay with their mothers, and thus provided a most logical and
59
economical way to guarantee sufficient mother contact (Wagner 1994). Subsequent
criticisms of the bonding and sensitive period hypothesis led Klaus and Kennell
(1982) to modify their notion of bonding to encompass the long-term process of the
parent’s developing emotional ties to the child in which the sensitive period is but one
factor. The work of Klaus and Kennell (1976) stimulated much needed changes in
hospital practices surrounding birth. Until then, pregnancy and childbirth had been
treated more as an illness requiring expert medical attention rather than a normal,
healthy and potentially rewarding human experience (Goldberg, 1983).
Other theoretical approaches including ‘attachment theory’; which was rooted in
the concepts advanced by Bowlby (Bowlby 1969) and expanded by Ainsworth
(Ainsworth et al. 1978), emphasised the protective function of the care-giver
providing a ‘secure base’ and the foundation of the structure of an infant’s emotional
ties to parents (Goldberg & DiVitto 1995). Most of the theoretical approaches of this
period emphasised specific aspects of development but, the transactional theory
developed by Sameroff and Chandler (1975) was a more integrative approach
emphasising the ongoing and dynamic aspects of development. Infant and child
development was not seen as the product of a simple cause and effect linear model but
as a complex interplay of mutual influences that operate between child and
environment over time and, which together serve to dissipate or amplify the effects of
earlier developmental insults (Sameroff & Chandler 1975). The differing theoretical
approaches lead to the conclusion that the unique circumstances that surround
premature birth will be challenging for parents and render the parent-infant
relationship more vulnerable to problems than that of full- term infants (Goldberg &
DiVitto 1995).

60
Thus the confluence of ideas arising from each of these three phases had a major
impact on the change in attitudes to the mother’s role in caring for her premature
infant. In seems as though premature care practices have come full circle: from the
early 1900s when parents primarily cared for premature infants if they survived,
through a period of exclusion and isolation of parents and the development of
sophisticated technology, to a gradual return to increasing involvement of parents in
the care of their premature infant (Goldberg & DiVitto 1995).
DISCUSSION
The momentum and ‘never say die’ efforts generated during the postwar era continue
today. Research has continued to demonstrate the fundamental importance of the
mother and family caregiving environment to the developmental outcomes of the
premature infant (Gennaro 1996). Developmental research has expanded the links
between the qualities of the mother-infant interactions and child development
outcomes (Barnard & Kelly 1990; Beckwith & Cohen 1984; Bee et al. 1982; Crnic et
al. 1983; Magill-Evans & Harrison 1999; Morisset et al. 1990). These studies have
been further extended in recent years to show that the infants' experiences not only
influence short term behaviour but actually shape the architecture of the brain, thus
influencing long term behavioural and cognitive outcomes (Shore 1997; Perry 1997).
Research within the NICU has examined practices such as the effects of holding,
cuddling, massage and skin-to-skin contact or ‘kangaroo care’ on even the most
fragile infants (Anderson 1991; Ludington-Hoe et al. 1994; Moran et al. 1999). In
response to data supporting the benefits of affectionate handling, NICUs have
attempted to expand the role of parents by adopting unrestricted visiting and
encouraging parental participation in care. However in a recent national survey to
61
assess the practice of kangaroo care, it was reported that there were major barriers to
its implementation including reluctance by nurses and physicians to initiate or
participate in kangaroo care (Engler et al. 2002). It seems that despite the increasing
amount of literature that emphasises the major role that a mother and family have in
their infant’s long term outcome, nursery activity is generally medically and
technically focused (Beal et al, 1996; Fenwick et al. 1999, 2001; McGrath &
Conliffe-Torres, 1996). There appears to be a gap between neonatal care policies and
practice and the evidence from family and infant research. The neonatal literature
supports that a nurse’s professional responsibility is extended to the family system
(Fenwick et al. 2001). However, it is possible that limitations exist within the current
system of care which may inhibit the ability of neonatal nurses to integrate family
related research evidence into practice.
CONCLUSION
Reviewing historical development in the care of the premature infant can provide
neonatal nurses with critical insight and understanding into how far parent and infant
care has evolved. This knowledge can be used to assist in formulating current and
future care and practice. Many of the early practices to help save premature infants
were experimental and not underpinned by evidence from formal trials and these
untested practices resulted in significant infant morbidity and mortality. These
valuable lessons learned from the past have meant that today, a new practice is
generally not introduced without substantial evidence supporting its benefit.
Perhaps more than ever before policies and practices within the neonatal nurseries
must be supportive of the individual families needs. The neonatal nurse is in a pivotal
position to facilitate the integration of both biomedical and family developmental

62
research in order to develop an evidence based, family centered approach to caring for
a mother and family who have a premature infant.
This chapter has provided an historical review of past practice with a
particular focus on the mother’s involvement in the care of her premature infant.
Despite current trends which have allowed parents greater access to their hospitalised
infant, it seems that to optimise the outcomes for the premature infant, the focus of
care needs to move beyond the infant to incorporate the individual needs of mothers
and families. The next chapter will describe the theoretical frameworks used to
explore a mothers’ adjustment and adaptation to the birth of a very premature infant.

63
CHAPTER FOUR
THEORETICAL FRAMEWORKS
Relevant theories of family adaptation to stressful life circumstances are
reviewed in the first section of this chapter. The theoretical framework chosen to
guide the present study: the Resiliency Model of Family Adjustment and Adaptation
(McCubbin, Thompson, & McCubbin, 1996) is presented.
The Barnard Model which provided the theoretical foundations upon which
the Nursing Child Assessment Feeding Scale (NCAFS) was developed (Barnard et al.,
1989) is described in the second section. The NCAFS is the observational measure
used in second phase of the study to code the video interaction data.
Family Adaptation
Theories of Stress and Coping
Research on how families adapt to critical life events has shifted from a one-person
risk-outcome focus for understanding individual developmental changes, to a more
inclusive dynamic, systems way of thinking where the individual is seen as part of a
larger, systems process of change (Fiese & Sameroff, 1989; Patterson, 1988; Sander,
2000). Several conceptual models have attempted to capture this more dynamic,
systemic view. These models have generally drawn upon three major theoretical
frameworks including the stress and coping theory (Hill, 1949; Lazarus & Folkman,
1984), social-ecological theory (Bronfenbrenner, 1979) and family systems theory
(Minuchin, 1974; Olson, Sprenkle, & Russell, 1979). Of these perspectives, stress
theory as originally described by Hill (Hill, 1949) and developed by Lazarus and his
colleagues (Lazarus & Folkman, 1984) has had the greatest influence on models of
adaptation to childhood illness and disability (Quittner & DiGirolamo, 1998).

64
Several current frameworks developed to examine the family’s adaptation to
childhood illness draw significantly upon stress and coping theory and include the
Resiliency Model of Family Adjustment and Adaptation (Resiliency Model)
(McCubbin et al., 1996), the Varni-Wallander Risk and Resistance model (Varni-
Wallander Model) (Varni & Wallander, 1988), and Thompson’s Transactional Model
(Thompson Model) (Thompson, Gustafson, Hamlett, & Spock, 1992).
Although these models vary in their emphasis, all assume that child illness is
an important stress factor which can lead to compromised mental and physical
outcomes depending on mediating factors including the family’s attribution of
meaning to the event (Patterson, 1988) and the availability of internal and external
resources (McCubbin & McCubbin, 1993). Similar features which appear across
these models are one or more measures of the degree of stress (e.g. severity of illness,
life stress or daily hassles), indicators of potential mediators of stress (e.g. social
support), and outcome measures (e.g. psychosocial adjustment) (Quittner &
DiGirolamo, 1998).
In the Resiliency Model a child’s illness is considered as a crisis event that
places extra stress and demands on the family. The family’s ability to meet these
demands and return to balanced functioning is dependant upon the meaning they
ascribe to the event and available family resources (McCubbin et al., 1996). Similarly
the Varni-Wallander Model (Varni & Wallander, 1988) considers that risk factors
(e.g. disease severity, life stress, hassles) will increase the probability of adjustment
problems (e.g. physical and mental distress). However, these negative effects may be
mediated by resiliency factors such as cognitive appraisals and coping behaviors, and
social-ecological influences (e.g. social support). Lastly the Thompson Model
incorporates many of the same variables as the other two theories, but postulates that
65
different variables may be more or less relevant depending on the childhood illness
being studied (Thompson & Gustafson, 1996). Both the Varni-Wallander and the
Thompson conceptual models have been used to identify risk and resistance factors
that may explain individual differences in adjustment to paediatric chronic illness
including sickle cell disease, cystic fibrosis (Thompson et al., 1992), spina bifida and
paediatric cancer (Varni, Katz, Colegrove, & Dolgin, 1996). These models have been
tested in specific paediatric settings with an emphasis on how children adjust to
chronic illness.
The Resiliency Model is a more generic model which has been applied in
numerous contexts including how families adjust and adapt to unexpected and
stressful events such as the birth of a premature infant (Singer, Davillier, Bruening,
Hawkins, & Yamashita, 1996). The Resiliency Model (McCubbin et al., 1996) was
chosen to inform the present research study as it allows exploration of factors
influencing family members response to the birth of a fragile high risk infant. Other
models have focused largely on the effects of various factors including family
functioning on the outcomes for the child with and without disability or chronic
illness. In circumstances such as the birth of a preterm infant, the developmental
outcome for the infant is unknown, however there is ample evidence that family
variables have a major impact on the long-term outcome. In particular, maternal
depression, as discussed in Chapter Two, can exert a negative influence on an infant’s
long-term developmental outcomes. It is therefore crucial to use a theoretical
framework that facilitates the identification of those factors.
It has been suggested that one of the primary reasons for the proliferation of
these models is the broad finding that even though infant and childhood illnesses can
place families and children at risk for psychosocial disorder, the effect is variable and

66
a majority of families make a successful adaptation (Drotar, 1992). This finding gives
rise to questions such as when and where, and under what conditions are families
most vulnerable to stress?
Stress
Stress research and theory has achieved a high profile worldwide among social and
biological scientists based on abundant evidence that stress is important for our social,
physiological and psychological health (Lazarus, 1999). Although stress is a familiar
concept that is widely used and assessed across a variety of disciplines, the concept of
stress is still poorly defined (Evans, 1998; Siegel, 1992). It has been suggested that
the construct of stress should not be delimited by rigid criteria but should be left as an
umbrella term. Folkman and Lazarus define stress as a relationship between the
person and the environment that is appraised by the person as related to his or her
well-being and in which the person’s resources are taxed or exceeded (Folkman &
Lazarus, 1985). Within this model the presence of an event in a person’s life is not
automatically assumed to be stress provoking. Instead, the individual determines or
appraises whether the event is stressful in relation to his or her resources. Stress is
said to occur when there is a perceived mismatch between the nature of the demand
and the individual’s ability to respond.
It has been noted that treating stress solely as an outside event that happens to
people ignores the important issue that different people may react differently to the
same stressful event (Evans, 1998; Pearlin, 1989). In its most persuasive sense, this
view suggests that if we can measure a pattern of stressful responses within a person
then this should be the sole criterion of whether or not that person has been stressed,
regardless of the nature of the life event (Evans, 1998). From this perspective, an
apparently very positive life event may cause stress, or equally an apparently very

67
negative life event may not (Evans, 1998; Schneewind & Ruppert, 1998; Werner,
1997). It has been argued that this way of defining stress should take priority over
external criteria as most investigations of stress focus on those response variables that
researchers may expect but not necessarily know will produce a certain type of
‘stressful’ effect (Evans, 1998). If a stressful response were not experienced
following exposure to a supposed external source of stress, then the event would not
be viewed as stressful for that particular person. The difficulty of the stress response
approach is that of specifying exactly what constitutes a stressful reaction (Evans,
1998). Therefore the current approach of most modern researchers has been to adopt
an interactionist position. Stress is seen as a transaction between the environment and
the person with emphasis on how the person perceives and copes with the
environmental challenges posed by the event (Evans, 1998).
Since the shift away from identifying associations between risks and outcomes
there has been a greater research focus on factors and processes that contribute to
diversity in response to risks, with some individuals being more vulnerable and some
more resilient in dealing with adversity (Hetherington & Blechman, 1996). As more
dynamic models of the stress process have evolved over the last two decades, research
interest has shifted to environmental factors which may ameliorate stress such as the
interpersonal relationships, social support and coping strategies (Kessler, Price, &
Wortman, 1985; LaMontagne, Johnson, & Hepworth, 1995; Nolan, Grant, & Keady,
1996). This implies that it is not just an event but also how the person or family
involved perceives the event, how great the stress is, and which coping strategies are
available (Nolan et al., 1996; Schneewind & Ruppert, 1998). However, the key factor
appears to be the subjective interpretation of stress events rather than the objective
characteristics that best determine the stress response (Kane & Penrod, 1995). The
68
immediate implications for professionals is to listen to families and explore their
perceptions of the stress event and process of care and how these appear to affect the
family (Nolan et al., 1996).
Coping
The concepts of stress and coping go hand in hand and therefore a discussion of stress
is incomplete without an understanding of how an individual responds in relation to a
stressful experience; that is, an individual’s coping behaviours (Lazarus, 1999; Siegel,
1992). Many recent models of stress view coping as the outcome of a cognitive
process in which a challenge or threat is first of all perceived; the ability to control the
challenge or threat is assessed; and finally, a calculation of the difference between
perception and control is made (Fisher, 1996). Coping therefore refers to the actions
that people undertake on their own behalf as they attempt to lessen or avoid the
impact of life problems (Pearlin & Schooler, 1978). Stress is therefore seen as a
consequence of perceiving a deficit between the demands of the event and personal
resources with which to manage the demands resulting in a sense of uncontrollability
or helplessness (Evans, 1998). In this context the amount of control a person actually
has is unimportant: it is the amount of control that a person believes they have that is
important. This discrepancy allows for an individual to adopt a variety of stress
reducing strategies (Evans, 1998). Additionally, individuals can show diversity in
response to a threatening situation according to how they cognitively appraise it. The
appraisal processes can be seen as ways of controlling and coping with potential
sources of stress (Evans, 1998).
Coping is a key concept for theory and research on adaptation and health and
has been described as a process which changes over time and in accordance with the
situational contexts in which it occurs (Lazarus, 1993). Thus, what a person does to
69
cope depends on the situational context of the event and varies according to the
diverse adaptational requirements of threat and the available resources to meet the
demand (Lazarus, 1993). McCubbin and McCubbin (1993) have defined coping as
the specific efforts by which individuals or families attempt to reduce the effect of a
stressor on the family and to manage the situation. This definition is applied whether
the individual or family achieves “bonadjustment” in other words moves through the
situation with relative ease or if families continue to experience crisis and imbalance
resulting in “maladjustment” (McCubbin et al., 1996).
The Resiliency Model will now be discussed in greater detail including the
historical development, current research applications of the model and the constructs
used in the current study.
The Resiliency Model
Historical development
Family stress theory was developed by Reuben Hill (1949) after war-induced
separation and reunion among families (Hill, 1949). Hill’s ABCX model illustrated
how families experiencing the same stressor event could react and respond differently.
The ABCX model placed emphasis on the stress event (A), family resources (B), and
the family’s interpretation of the stressor (C), which may protect families from
deteriorating into a crisis situation (X). A balance between these factors appeared to
determine a family’s susceptibility to a family crisis (Hill, 1949, 1958). The Double
ABCX model of family adaptation (McCubbin & Patterson, 1983) was developed as
an extension of Hill’s work and is the forerunner of the Resiliency Model. The
Double ABCX model included the cumulative effects of stress and additional
variables that influence adjustment. These variables included the pile up of additional
stressors (AA); new and existing resources (BB); and family perceptions of the

70
situation (CC) and coping strategies (PSC) influencing adjustment. The Resiliency
Model is a substantive revision of the Double ABCX model, and expanded earlier
theories by emphasising family adaptation rather than adjustment, and includ
additional factors such as family type, problem solving capability, and a higher level
of family perception (McCubbin & McCubbin, 1993). The Resiliency Model was
developed to explain why some families are more resilient than others and better able
to adjust and adapt to stress and crises by examining the family system as a unit. The
model considers the family processes of problem-solving, natural strengths and
capabilities, the role of the community, and how the family and community interact to
shape both the individual’s and the family’s response and adaptation to the stressful
situation (McCubbin et al., 1996; McCubbin & McCubbin, 1993).
Current research applications
The Resiliency Model has been used as the guiding theoretical framework for
other studies involving family well-being and adaptation. In particular the model has
been used to guide many studies where nursing assessment and intervention have
been important to alleviate family stress. For example, Curley (1992) based her
nursing intervention framework upon the Double ABCX Model (McCubbin &
Patterson, 1983) when investigating nursing interventions designed to assess and
alleviate parental stress when an child is admitted to the paediatric intensive care
(Curley & Wallace, 1992). In another study, Singer (1996) used the Double ABCX
Model to guide the assessment of social support and distress in mothers after the birth
of a very low birth weight infant (Singer et al., 1996). More recently, Leske (1998)
adopted the Resiliency Model to guide nursing assessment and strategies for
intervention for families in crisis after a member’s critical injury (Leske & Jiricka,
1998). The Resiliency Model has also been used in other studies involving nursing

71
assessment and interventions in a family stress situation (Mays, 1988; Robinson,
1997) and family stress was identified as the most amenable factor for nurse initiated
intervention (Robinson, 1997).
Resiliency Model applied to the current study
Research has shown that two families faced with the same illness stressor can
respond in dramatically different ways (Pearlin, 1989); one family marshals its
members to deal constructively with the demands it faces, whereas another family is
immobilised by the situation and begins to unravel as demands are placed on it (M.A.
McCubbin & McCubbin, 1993). The Resiliency Model provides a way of
understanding family responses to illness. The framework can assist in determining
whether or not an illness stressor may cause a family crisis. In the Resiliency Model,
social support is viewed as one of the primary moderators between stress and
psychological wellbeing. Coping is described as an active process encompassing both
the utilisation of existing family resources and the development of new behaviours
and resources which assist in strengthening the family unit and alleviate the impact of
stressor events (McCubbin et al., 1993).
In its simplest form, the Resiliency Model focuses on the stressor, family
resistance resources, and family member’s appraisals of the stressor event in
predicting adjustment outcome (McCubbin & Patterson, 1983). The Resiliency
Model is best suited to the research that is the focus of this thesis, as the outcome of
interest is a family sub-system variable (i.e. mother-infant interaction). An individual
level theory may be inadequate to explain the variability in outcome where both
individual and family outcome measures are the focus. The constructs and the
underlying assumptions of the Resiliency Model encompass both individual and
family measures.
72
While there are many key concepts proposed in the Resiliency Model only three
of the major constructs were investigated for the purpose of this study, namely the
stress factor (AA), family resources (BB factor) and family problem solving and
coping (PSC factor). Very premature birth represents a life crisis event and families
need to draw upon their existing resources in order to cope with such a stressful event.
Research studies have acknowledged the importance of parents in the lives of their
preterm infants and have begun to focus their attention on the adaptational needs of
parents. These three constructs were chosen because they represent the family’s
strengths and capabilities in responding to a stressful event which will influence a
family’s adaptational outcome.
There are two related but discernible phases within the Resiliency Model that
mark a family crisis, i.e. adjustment and adaptation. Adjustment is intended to denote
the initial response to a crisis event during which minor changes are made as the
family attempts to meet demands utilising existing resources or resistance capabilities.
Outcomes vary from positive adjustment in which established patterns of family
functioning are maintained to maladjustment in which a family crisis exists. In some
crisis situations such as the birth of a premature infant, families may have numerous
and more extensive demands which require substantive changes to the family system
(McCubbin et al., 1996; McCubbin & McCubbin, 1993). In these situations families
will remain in a state of crisis until there are changes made in the family’s pattern of
functioning which can restore harmony and balance (McCubbin et al., 1996). This
change heralds the beginning of the adaptation phase. During the adaptation phase the
family attempts to restore homeostasis or stability by acquiring new resources and
coping behaviours. Family change and adaptation over time is the primary focus of
73
the Resiliency Model and denotes the outcome of family efforts to bring a new level
of balance and functioning to a family crisis situation (McCubbin et al., 1996).
Stress factor (AA)
In the Resiliency Model a stressor is defined as a demand placed on the family that
either produces, or has the potential to produce, a change in the family system
(McCubbin et al., 1996). This change or threat of change can influence all areas of
family life including the marital relationship, the parent-child relationship, the sibling
relationship and the family system (McCubbin et al., 1996). The severity of the
stressor is determined by the degree to which the stressor threatens the stability of the
unit, disrupts family functioning, or places significant demands on the family’s
resources and capabilities (McCubbin, 1990). These demands or stresses to a family
do not remain stagnant, but change over time.
Family resources (BB)
The Resiliency Model defines adaptive resources as both existing resources and
expanded resources that are developed and strengthened in response to the demands
posed by the stressor event (McCubbin et al., 1996). The family’s capability is
defined as the potential the family has available for meeting demands. These include
family resources or what a family has, and coping behaviours or what the family does
(McCubbin et al., 1996). Three potential origins of resources include individual
family members, the family working as a unit, and the community. A resiliency
resource is a characteristic of one of these resources that facilitates adaptation to a
stress or critical event (McCubbin et al., 1996). On an individual level, a person’s
physical, spiritual and emotional health is viewed as a personal resource through
which personal energy is available to meet family demands (McCubbin et al., 1996).
McCubbin and McCubbin (1993) also cite other critical family resources including

74
financial resources, family flexibility, family hardiness, shared spiritual beliefs,
family communication, traditions, celebrations and family routines (McCubbin &
McCubbin, 1993). Community-based resources and supports include the social
network, medical and care-provider, friendship and community based activities
outside the family unit. A family faced with a crisis may access and use these
resources in an attempt to bring the crisis demands under control (McCubbin et al.,
1996). At a broad social level, state and federal government policies that support
families are also viewed as sources of support (McCubbin et al., 1996). Social
support has most often been viewed as one of the primary buffers between stress and
family breakdown. McCubbin and McCubbin (1996) utilise Cobb’s definition of
social support as the most useful in the context of the Resiliency Model when a family
is faced with a crisis situation. Social support is defined as information exchanged at
an interpersonal level that provides (a) emotional support which leads individual
members to believe they are loved and cared for; (b) esteem support leading
individual members to believe they are respected and valued; and (c) network support
leading members to believe that they belong to a network of communication involving
mutual support and mutual understanding (Cobb, 1976). The greater the efficacy of
the family’s support network and quality of affirming social support, the greater the
ease with which the family is able to adapt to the crisis (McCubbin & McCubbin,
1993)
Family coping (PSC)
In the Resiliency Model, family coping refers to specific cognitive and behavioural
efforts by which the individual and family attempt to reduce or manage demands and
utilise available resources to manage a crisis situation (McCubbin et al., 1996).
Specific coping behaviours may be grouped into patterns, such as coping directed at
75
maintaining family integration and cooperation. This particular coping pattern
emerged as important for families who have a chronically ill child (M.A McCubbin,
1984). Coping patterns are conceptualised as more generalised ways of responding
that transcend different kinds of stressful situations rather than a specific coping
behaviour within the context of a multiple pile-up of stress (McCubbin et al., 1996).
McCubbin and McCubbin (1991) noted, although coping has been most often
theoretically linked to individual efforts, family coping may be viewed as coordinated
problem solving behaviour of the whole system which involves complementary
efforts of individual family members who fit together as a synergistic whole
(McCubbin et al., 1996). This creates a balance between demands and resources
while at the same time eliminating stressors and hardships. McCubbin et al. (1996)
have identified four broad headings that characterise the ways in which coping
facilitates adaptation. These include:
• Direct action to eliminate or reduce the number and intensity of demands;
• Direct action to acquire additional resources outside the family;
• Management of tension associated with ongoing strains (a necessary function of
coping because of the inevitable residual family strains resulting from an illness);
• Cognitive appraisal to change the meaning of the situation to make it more
constructive, manageable, and acceptable (McCubbin et al., 1996).
To summarise, coping may be directed at the reduction or elimination of stress,
the acquisition of additional resources, the ongoing management of family system
tension, and shaping the appraisal at both the situational and the cognitive level
(McCubbin et al., 1996).
The present study is diagrammatically shown in Figure One (p. 80). The model
presented has been adapted from the Resiliency Model (McCubbin et al., 1996) to
76
illustrate the major constructs which provide the theoretical framework for the study.
The figure illustrates that a family’s adaptational outcome (XX) can be examined as a
function of the relationship between characteristics of the infant (degree of
prematurity, birthweight, and neurobiological risk) and the characteristics of the
mother (previous history of depression, educational level) (AA), and the family’s
resources (social support, psychological well-being)(BB) and coping behaviours
(PSC). Whether the family is able to move through the crisis situation to achieve
‘bonajustment’ or whether a family continues to experience crisis and imbalance
resulting in ‘maladjustment’ is dependant on the balance between the demands of the
stressor event and the family’s resources to meet those demands.
The Resiliency Model is an appropriate framework to inform the study of the
adjustment and adaptation of mothers and families following very preterm birth. It
provides a way of viewing a mother’s and family efforts over time to adapt to
multiple stressors and attempts to delineate variables that may influence the family’s
ability to achieve adaptation. In the present study, the family’s adaptation was
conceptualised as the mother’s ability to interact with her premature infant after
discharge.
The observational tool used to assess mother-infant interaction in the current
study is underpinned by the Barnard Model which will now be discussed.
Barnard Child Health Assessment Interaction Theory
The theoretical assertions contained within the Barnard Child Health Assessment
Interaction Theory (Baker et al., 1994) have informed and provided the basis for the
Barnard Model. This theory focuses on the importance of identification of problems
as early as possible in an infant’s life (making them more amenable to intervention)

77
and on the critical role of the environment in determining child health outcomes
(Baker et al., 1994; Huber, 1991). A principal feature of the environment is the nature
of interaction between the infant and significant others and the quality of this
interaction that have the potential to influence important areas of cognitive, linguistic
and social development. Both caregiver and infant convey a certain level of style and
skill to their opportunities for mutual interaction. The parent influences the infant and
the infant influences the parent so that both are changed and mutual modification
occurs as the partners become attuned to each other so that interaction becomes
smooth-flowing (Huber, 1991). Since the adaptive processes are easier to modify
than the basic characteristics of either partner, it is this area where assessment and
intervention can be most effective. Barnard also emphasises the fundamental
importance of the nursing profession in providing support to the infant’s caregiver.
The Barnard Model views the parent-infant system as interactive and
influenced by the individual characteristics of each member and the ways in which
they are modified to meet the needs of the system. Modification is defined as
adaptive behaviour (Barnard, Booth, Mitchell, & Telzrow, 1988). The major
constructs of the Barnard Model are based on the assumption that caregivers and
infants have certain responsibilities to maintain interaction. The infant is responsible
for producing clear cues and being responsive to the caregiver. The caregiver is
responsible for responding to the infant’s cues, alleviating the infant’s distress, and
providing opportunities for growth and learning. This interaction results in the infant
and caregiver responding and reacting to each other, and adapting their behaviour to
accommodate or modify the other’s behaviour. Either partner can place the
interaction at risk. An infant’s inability to give clear clues or respond to the caregiver
can interfere with the adaptive process (Barnard, 1996). Infant characteristics such a

78
prematurity can have a detrimental effect on the repertoire of infant behaviours
(Barnard, 1996; Barnard et al., 1988). Likewise a caregiver’s lack of knowledge of
infant behaviour, depression or life stress are examples of conditions which can
influence interaction. Such conditions may cause the caregiver to be less sensitive to
infant cues, unable to alleviate the infant’s distress or unable to provide growth-
fostering situations for the infant (Barnard, 1996; Barnard et al., 1988). In situations
where both caregiver and infant experience such conditions, maladaptive interactions
are more likely to occur. If only one social partner is providing less than optimal
interaction, the other partner can generally support the interaction to maintain
reciprocity (Barnard, 1996).
The Barnard model argues that interaction patterns must contain certain
features which permit infant to receive the quantity and quality of stimulation needed
for optimal development. Firstly, each partner must have a sufficient repertoire of
behaviours such as talking, smiling and movement so that interwoven sequences such
as leading and following are possible and fluid interaction patterns develop (Barnard,
1996). Secondly, the Barnard Model suggests that each partner’s responses must be
subject to one another and as the infant matures, the caregiver must adapt their
behaviour to remain both consistent and contingent in responding to the infant.
Thirdly, the richness of interactive components in terms of positive parental affect and
verbal stimulation, the range of play materials provided and the ability of the child to
become involved with the parent in stimulating activities is also related to cognitive
and social skills. Finally, adaptive patterns between caregiver and infant must change
over time relative to the emerging developmental capabilities of the infant. As
cognitive, motor and social skills develop the infant assumes more interactive
responsibility (Barnard, 1996). This mutuality in parent-infant interaction has been

79
described by others as reciprocity or mutuality (Condon & Sander, 1974; Spiker,
Ferguson, & Brooks-Gunn, 1993) and synchrony (Censullo, Bowler, Lester, &
Brazelton, 1987). It is within this conceptual orientation that the NCAFS tool is used
for documenting parent-infant interaction (Barnard, 1978).
Two theoretical models have been discussed in this chapter and underpinned
the current study. The models selected provided a framework to explore the
adjustment of mothers at 4 weeks following preterm birth and adaptation during the
first three months after infant discharge. The next chapter details information about
the study participants, data collection procedures, research instruments and ethical
considerations.

0
Figure 1. An Adaptation of the Resiliency Model FAMILY CRISIS SITUATION (AA)
FAMILY STRENGTHS & CAPABILITIES (BB)
ADAPTATIONAL OUTCOME (XX)
PHASE 1 PHASE 2
Family Crisis Situation
Family Resources (BB)
Family Resources (BB)
BONADJUSTMENT
Family Coping (PSC)
Family Coping (PSC)
MALADJUSTMENT
Adapted from: McCubbin, H. I., Thompson, A. I., & McCubbin, M. A. (1996). Family assessment: resiliency, coping and adaptation. Inventories for research and practice. Madison: University of Wisconsin Publishers.
Birth of a very premature infant
Maternal stress History of Depression
Family support Nurse support Psychological well being Maternal education
Family support Nurse support Psychological well being
Mother-infant Interaction
Scores
Gestational age Birthweight Apgars
Maternal Coping Strategies
Maternal Coping Strategies
Infant NBRS Infant LOS
Family Crisis
Situation

81
CHAPTER FIVE
METHOD
The research design, research questions and hypotheses, the population,
sample (including sample size calculation), data collection methods and the
instruments used in this study, are described in this chapter. The ethical issues
associated with this study are also discussed.
Research Design
This study was a two-phase prospective follow-up design which involved surveying
mothers of very premature infants (≤ 32weeks) who were admitted to the neonatal
intensive care unit (NICU). The study consisted of multiple measurements collected
at 4 weeks post-partum, Phase 1 (P1), and 12 weeks following infant discharge from
NICU, Phase 2 (P2). In addition, mother-infant observational data were collected
during Phase 2.
Research questions and hypotheses
The purpose of the study was to examine the factors related to maternal depressive
symptomatology at P1 and P2 and to determine whether there is a relationship
between maternal and infant variables collected at both times and mother-infant
interaction observed at P2. To achieve the purpose of this study, the following
primary research questions were examined:
• Which factors are related to mothers’ reports of depressive symptomatology at
P1?
• Is there a relationship between maternal and infant data collected at P1 and
mothers’ reports of depressive symptomatology at P2?

82
• Is there a relationship between maternal and infant data collected at P2 and
mothers’ reports of depressive symptomatology at P2?
• Is there a difference between the mother and infant interaction scores of the study
population and the normative population?
• Is there a relationship between maternal and infant data collected at P1 and
mother-infant interaction scores at P2?
• Is there a relationship between maternal and infant data collected at P2 and
mother-infant interaction scores at P2?
The following scientific hypotheses were developed to examine the research questions
and were expressed as below:
The first hypothesis was tested during Phase 1 (P1) of the study and was stated as:
• Maternal depressive symptomatology at four weeks post premature birth will
be related to a previous history of depression, limited formal education,
limited social support, high levels of stress, limited use of coping strategies
and infants who were at low gestational age and birthweight.
The second and third hypotheses tested data across the two phases of the study and
were stated as:
• Elevated levels of maternal depression at 12 weeks after infant hospital
discharge will be related to a previous history of depression and limited formal
education; limited social support, limited use of coping strategies and high
levels of stress and depressive symptoms during P1; and having infants of low
gestational age, birthweight and apgar scores.

83
• After controlling for P1 depression, elevated levels of depressive symptoms at
P2 will be related to limited social support, limited use of coping strategies,
high levels of stress during P2; and having infants who had long hospital stays
and high medical risk.
The fourth, fifth and sixth hypotheses tested during the observational component of
Phase 2 (P2) of the study and were stated as:
• There will be a difference in feeding interaction scores between the study
sample and the population norms.
• Less optimal mother-infant interactions will be related to: a previous history of
depression and limited formal education; limited support and use of coping
strategies and high levels of stress and depression during P1 and infants who
had lower gestational age, birthweight and apgar scores.
• Less optimal mother-infant interactions will be related to: limited support and
use of coping strategies and high levels of stress and depressive symptoms at
P2, and having infants who had high medical risk and long hospital stays.
Major variables measured in the study
The main outcome variables in this study were maternal depressive symptomatology
measured at P1 and P2, using the Edinburgh Postnatal Depression Scale, and mother-
infant interaction scores measured at P2 using the Nursing Child Assessment Feeding
Scale.
The explanatory variables and measures used to collect these data are shown
in the table 5.1 below. A more detailed description of the measures is included later
in this chapter.

84
Table 5.1: Explanatory variables and measures
Explanatory variables Measure Maternal stress symptoms
Stress Scale of the Depression, Anxiety and Stress Scale (Lovibond & Lovibond, 1995)
Family social support Social Support Interview (SSI) (O’Hara et al., 1982; 1983)
Nurse support Nurse Parent Support Tool (NPST) (Miles, Carlson, & Brunssen, 1999)
Maternal coping strategies Coping Health Inventory for Parents (CHIP) (McCubbin et al., 1983)
Medical Risk Index Neurobiological Risk Score (NBRS) (Brazy, Eckerman, Oehler, Goldstein, & O'Rand, 1991)
Maternal education Maternal self-report
Previous history of depression
Infant Gestational Age
Infant Birthweight
Apgar Scores
Length of hospital stay
All these data were collated from the mother and infant medical records.
Population and Sample
The subject population consisted all eligible mothers of very premature infants who
were admitted to a 60 bed tertiary referral NICU of a major metropolitan hospital.
The expected annual admission rates for infants born less than 32 weeks is
approximately 100 infants.
It was recognised that mothers were initially faced with a very stressful
situation after the premature birth and subsequent admission of their infant to the
NICU. Consequently, at least four weeks was allowed to lapse before mothers were
approached to participate in the study. This timeframe allowed mothers to physically
recover from the birth and adjust to the acuteness of their infant’s situation in addition
to providing time for the infant’s condition to stabilise.

85
It was considered appropriate to administer the Edinburgh Postnatal
Depression Scale (EPDS) at four weeks postpartum if the infant’s medical condition
was stable and the mothers consented to participate in the study. Antenatal depression
occurring in the second and third trimester has been found to be a significant predictor
of postpartum depression (Beck, 1996a). Other studies have also administered the
EPDS at three and four weeks (Da Costa, Larouche, Dritsa, & Brender, 2000;
Yamashita, Yoshida, Nakano, & Tashiro, 2000).
The following inclusion criteria were used:
• Mothers of singleton infants of less than 32 completed weeks of gestation who
were admitted to the NICU;
• Mothers living within a 200 kilometre radius of the participating hospital;
• Mother able to read and converse in English.
The following exclusion criteria identified those who were ineligible for entry to the
study:
• Mothers of multiple births;
• Mothers ≤ 18 years of age;
• Mothers of infants with major congenital anomalies or identifiable syndromes;
• Mothers who lived outside the specified geographical areas;
• Mothers who were unable to read or converse in English.
A total of seventy-two mothers met the eligibility criteria during the
recruitment phase of the study from May 2000 to February 2001. Five mothers (8%)
declined to participate. Three of these mothers had full-time study commitments. The
other two mothers did not cite a reason for non-participation. Another five mothers
(8%) agreed to take part, however for reasons of distance from the hospital and full
time care of other siblings, these mothers were unable to visit their infant within the
86
allocated timeframe. The remaining sixty-two mothers made up the P1 sample. At
P2, all P1 mothers were contacted and of the original 62 mothers, five were unable to
be followed up due to infant rehospitalisation (two) and social issues (three). Four
mothers were not traceable and there was one infant death. The remaining fifty-two
mothers made up the final comparison sample.
The sample consisted of mothers, of whom a majority were born in Australia
(91.9%) and aged between 18-42 with the mean age of 29 years (sd 5.7). Just over
77% (48) had completed secondary or tertiary education. For 55% (34) of mothers
this was their first baby, and for a further 24% (15) who were multiparous, it was their
first premature infant. Sixteen percent (10) reported having had a previous history of
depression. An overwhelming majority of mothers (95%) reported having a
supportive spouse or partner.
The infants’ gestational ages ranged from 24-32 weeks with a mean of 28 weeks (sd
2.4). Birthweight ranged from 513-2002 grams with a mean of 1088 grams (sd 359).
Apgar scores at 1 minute ranged from 1-9 with a mean of 5.75 (sd 2.48) and at 5
minutes they ranged from 1-10 with a mean of 7.71(sd 2.25).
Sample Size
Power calculations to determine an appropriate sample size were based on group
comparisons where the groups were defined based on median splits of the various
explanatory variables (depression, support, and coping scores). Since the major
outcome variable was mother-infant interaction scores, it was expected that the
proportion of ‘responsive interactive’ relationships in the optimal comparison group
would be about 80%. Differences of 30% or greater were defined to be of clinical
interest (ie 80% vs 50% or less in the two comparison groups). This information was
entered into a computerised power analysis program (Erdfelder et al., 1996). A
87
minimum of 45 women per comparison group was required to detect such differences
with 80% power and using a type I error of 5% (two-tailed). Allowing 15% extra for
the proposed multivariate modelling and approximately 20% extra for expected
attrition, a target sample of 130 mothers was set.
From a target sample of 130, a final sample of 90 was statistically possible
however, certain limitations prevented this sample size being achieved. Firstly, the
researcher had access to only one tertiary institution and while the expected
admissions amounted to 100 infants per year, this estimate included multiple birth
infants who were excluded from the current study. The second limitation involved the
limited timeframe in which participants could be recruited. Since the research project
included a follow-up phase, the recruitment phase needed to be limited to 10 months
to ensure that all participants could be followed within the allocated timeframe.
Despite these limitations, the obtained sample size of 62 was consistent with other
research studies which have observed interaction between a mother and her preterm
infant in the first 12 months of life. Such studies have reported similar sample sizes
ranging from 46-52 dyads (Coyl, Roggman, & Newland, 2002; Ruttenberg, Finello, &
Cordeiro, 1997; Wijnroks, 1999; Zahr, 1991).
Measures
Self Report Instruments
Self-report data were collected from the mothers on current stressors, perceptions of
available support and their current emotional well-being. One of the strongest
arguments to be made in favour of the self-report method is that it frequently yields
information that would be difficult to gather by any other means (Polit & Hungler,
1997). Self-report data therefore captures measurable aspects of the phenomenon

88
under investigation and is cost-effective (Polit & Hungler, 1997;(Singleton, Straits, &
Straits, 1993).
Depressive symptomatology: The 10-item Edinburgh Postnatal Depression
Scale (EPDS) (Cox, Holden, & Sagovsky, 1987) is a well-validated and widely used
screening tool for depressive symptoms after childbirth. Each item is scored on a 4-
point scale (0-3), the total score ranging from 0-30. In this study a score of ≥12 was
classified as indicative of significant depressive symptomatology. The EPDS rates
core features of low mood, anhedonia, anxiety and sleep disturbance due to anxiety
(Pritchard & Harris, 1993). Validity coefficients for the postnatal period, as reported
by Cox et al. (1987), were sensitivity 85%, specificity 77%, and a positive predictive
value of 83%. The split-half reliability of the scale was found to be 0.88 and the
standardised alpha-coefficient was 0.87. In the current study, the alpha coefficients
for Phase 1 and Phase 2 were .83 and .91 respectively. The EPDS is shown as
Appendix 1
Maternal stress: The 21 item Depression Anxiety Stress Scales (DASS)
(Lovibond & Lovibond, 1995) was developed in response to the failure of traditional
measures to clearly distinguish between anxiety and depression (Antony et al., 1998).
Factor analytic studies with nonclinical (Lovibond & Lovibond, 1995) and clinical
samples (Brown et al., 1997) have confirmed that the DASS items can be reliably
grouped into three scales: (a) depression, (b) anxiety, and (c) stress. Unlike other
scales, the stress scale of the DASS includes items that measure symptoms such as
tension, irritability, and a tendency to overreact to stressful events (Antony et al.,
1998). The psychometric properties of the 42 item DASS have been addressed in two
published studies (Brown et al., 1997; Lovibond & Lovibond, 1995) and suggest that
the DASS has adequate internal consistency and temporal stability and provides a
89
better separation of the features of anxiety and depression, relative to existing
measures. The alpha coefficient for the stress scale has been reported as .90
(Lovibond & Lovibond, 1995). More recently the psychometric properties of the
DASS have been tested in clinical groups and in a community sample (Antony et al.,
1998). The results have confirmed earlier findings that the DASS distinguished well
between the features of depression, anxiety and stress. In the current study, the alpha
coefficients for Phase 1 and Phase 2 were .95 and .91 respectively. The DASS is
shown as Appendix 2.
Social support: The research study used two measures of social support. The
first self-report measures support provided by social network members (Social
Support Interview) and the second focuses on support provided by the nursing staff
(Nurse Parent Support Tool).
The Social Support Interview (SSI) (O’Hara et al., 1982; 1983) was designed
by O’Hara, a researcher in peri-partum mood disorders, to assess pre-partum and post-
partum social support provided by, and given to, a participant’s spouse/partner,
closest confidant and closest parent. The SSI was initially derived from the Social
Network Interview (Mueller,1980). O’Hara designed the Social Support Interview
(SSI) to be used in his first two studies (O’Hara et al., 1982; 1983). The results of
O’Hara’s early studies indicated that a lack of social support from important members
of a woman’s social network (ie. spouses, confidants and mothers) was clearly related
to post-natal depression. Results also indicated that depressed women had a greater
amount of contact with, and were seeking support from their network members but
were not receiving it. Most of the dissatisfaction related to their spouses and to a
lesser extent their confidants (O’Hara et al., 1982; 1983). In response to the results
from these two studies (O’Hara et al. 1982; 1983) O’Hara slightly modified Mueller’s
90
Social Network Interview to focus more on network utilisation and less on frequency
of contact. He first developed a 10-item SSI (O’Hara et al., 1984) and later adapted
this to a 13-item SSI (O’Hara, 1995), which was used in the current study. The three
sub-scales of the SSI (confidant, parent and spouse/partner) each show adequate
internal consistency with alphas ranging from .77 to .85. (O’Hara, 1990). In the
current study, the alpha coefficients for Phase 1 and Phase 2 respectively, were
confidant .98 and .93; parent .98 and .97; and spouse/partner .95 and .96. The SSI is
shown as Appendix 3.
The Nurse Parent Support Tool (NPST) (Miles et al., 1999a) is designed to
measure maternal perception of nursing support during their child’s hospitalisation.
The 21-item NPST assesses four dimensions of support: (1) supportive
communication and provision of information related to the child’s illness, treatments,
care, and related issues; (2) parental esteem support focused on respecting, enhancing,
and supporting the parental role; (3) emotional support to help mothers cope with
their own emotional responses and needs related to the child’s illness; and (4)
caregiving support involving the quality of care provided to the child. Parents are
asked to rate the amount of nursing support received on a Likert-type rating scale
ranging from “1” almost never to “5” almost always. The scores are summed and
divided by the number of items completed (21). The range of scores is from 1-5 with
the higher scores reflecting a greater amount of perceived support from staff. NPST
scores in the population sample as reported by Miles ranged from 1.38 to 5.00 with a
mean of 4.12 and a standard deviation of .072. Internal consistency has been reported
to have a Cronbach’s alpha 0.95 (Miles, Carlson, & Brunssen, 1999). In the current
study, the alpha coefficients for Phase 1 and Phase 2 were .93 and .95, respectively.
91
The Nurse Parent Support Model (NPSM) which underpins the development
of this research instrument, is derived from Rubin’s nursing theory (Rubin, 1968)
which views the primary goal of nurses as providing a supportive relationship for
patients within the stressful hospital environment (Mercer, 1995). The NPSM was
based on more comprehensive aspects of social support including the many areas of
interpersonal support provided by nurses to patients and families identified by House
(House, 1981). The NPSM does not conceptualise nursing support as similar to or as
a replacement for social support, rather that professional support provided by nurses
to mothers during infant hospitalisation as an essential component of nursing practice
(NPST manual). The NPST is shown as Appendix 4.
Coping: The research study used a coping measure which assessed parents’
appraisal of their coping responses to the management of family life when they had an
infant who was seriously and/or chronically ill.
The Coping Health Inventory for Parents (CHIP) (McCubbin et al., 1983)
consists of a checklist of 45 specific behaviours, which are divided into three
subscales. The first coping subscale measures family integration, cooperation and an
optimistic perception of the situation. This subscale is composed of 19 behaviours
that focus on strengthening family life and relationships and the parents’ perception of
life with a chronically ill child (McCubbin, Thompson, & McCubbin, 1996). The
second coping subscale measures the parents’ effort to maintain social support, self-
esteem and psychological stability. The subscale consists of 18 items which assess
the parents efforts to develop relationships with others, engage in activities which
promote feelings of individual identity and self worth as well as behaviours to manage
psychological tensions and stress (McCubbin et al., 1996). The third coping subscale
focuses attention on the parent’s understanding of the health care situation through

92
efforts to communicate with other parents and the health care team. The subscale
consists of 8 items which are directed at the parents’ relationships with health care
professionals and other parents and includes behaviours to develop a greater
understanding of the illness and managing home care treatments (McCubbin et al.,
1996).
The CHIP asks parents to record on a scale of 0-3, how helpful each behaviour
is in their particular family situation. If a coping behaviour is not used, the parent is
given a choice of, a) I do not cope this way because I chose not to use it, or b) this
coping behaviour is not possible in our family and therefore not applicable to us
(McCubbin et al., 1996). The reliability (Cronbach’s alpha) for the first and second
coping pattern is reported as (.79). The alpha reliability for the third coping pattern is
reported as .71 (McCubbin et al., 1996). In the current study, the alpha coefficients
for Phase 1 and Phase 2 respectively, were coping pattern one .74 and .73; coping
pattern two .87 and .79 and coping pattern three .75 and .57. The CHIP is shown as
Appendix 5.
Demographic Data
The researcher collected the following information from the maternal and
infant hospital records. Maternal demographic data including educational level and
previous history of depression, and infant data on birthweight (grams) gestational age
(weeks) and total length of hospital stay (LOS) and Apgar scores were extracted from
medical records.
The infant’s medical risk was calculated using the Neurobiologic Risk Score
(NBRS) (Brazy et al., 1991). The NBRS was developed in response to the need for
an assessment tool that provides early identification of infants who are at high risk for
neurodevelopmental abnormality. Seven high-risk medical conditions are scored 0,

93
1,2 and 4 and from this score three neurobiological risk groups are identified: Low
risk (0-4), intermediate risk (5-7) and high risk (>8). The researcher and the Director
of Neonatology at the hospital determined the NBRS for infants whose mothers
participated in the study from chart data after infant discharge. The NBRS is shown
as Appendix 6.
Observational Data (Phase 2)
Criticisms of self-report data led to an increased interest in observational measures of
parenting behaviour including both naturalistic and structured techniques (Berlin,
Brooks-Gunn, Spiker, & Zaslow, 1995). One of the major advantages of naturalistic
observational assessments is their ability to capture a broad range of spontaneously
occurring behaviour. Methods for observing parent-infant interactions were first
developed and used by researchers who were concerned with the nature of early social
interaction and its contribution to child development (Wyly, 1997). Research
evidence was accumulating that showed that interactions between parents and infants
were influenced by many factors including the family environment and these in turn
influenced the infant. The primary focus on infants began to shift to a greater focus
on the family incorporating broader-based assessments of the infant, parent, and
environment, including infant social competence and mother-infant interaction (K. I.
Barnard & Kelly, 1990; Meisels & Shonkoff, 1990; Wyly, 1997).
A number of empirically based scales have been developed to assess parent-
infant functioning and to guide intervention. The choice of an assessment procedure
depends on the purpose of assessing the interaction and the specific behaviours to be
measured (Wyly, 1997). A number of assessment scales have been developed to
assess the overall quality of the parent-infant interaction and are principally used for
research in the clinical setting (Wyly, 1997).

94
In view of the study aims a number of mother-infant interaction tools were
considered and evaluated for their suitability to use with infants under six months of
age. The maternal behaviour rating scale (MBRS) (Mahoney, Powell, & Finger, 1986)
was rejected because it was designed to measure quality of maternal interactive
behaviours with one, two and three-year-old infants who had intellectual impairment.
The mother-infant play interaction scale (MIPIS) (Walker & Thompson, 1982)
designed to assess the interactive strategies used by mothers and infants in an
unstructured play situation, was also rejected because the normative data on this scale
was limited to low risk mother-infant dyads (Wyly, 1997). The parent-caregiver
involvement scale (PCIS) (Farren et al., 1987) which rates caregivers’ involvement
during interactive free play with an infant or toddler during a 20-minute live or
videotaped observation was similarly rejected primarily because of its focus on the
caregiver's interactions thus precluding assessment of the development of reciprocal
exchanges between parent and child (K. I. Barnard & Kelly, 1990). The Greenspan-
Lieberman Observation System (GLOS) (Greenspan & Lieberman, 1980) was
designed for assessment of care-giver-infant interaction during a semi-structured play
situation. It was developed as a clinical observational tool used to assess adaptive and
maladaptive parent-interaction in a laboratory setting. However because of its length
and complexity, it has not been used widely furthermore as observations in the present
study were to be made in the home it was considered inappropriate (Wyly, 1997).
The Nursing Child Assessment Feeding Scale (NCAFS) was selected as the
most appropriate interactional tool to use in this study. The NCAFS was designed to
evaluate critical features in parent-child interactions by assessing the ability of the
parent and infant to participate in synchronous mutual interaction (Barnard, 1978a,
1978b, 1978c). The feeding situation is viewed as a familiar activity that provides the

95
most opportunities for interaction between parent and infant. The NCAFS is
specifically designed to be used from birth to three years and has been found to be
useful both to nurses (for whose practice they were originally designed) and a variety
of other health professionals interested in early intervention with infants and young
children (Huber, 1991). The NCAFS has been a frequently used method of assessing
maternal infant interactions and has been used extensively in clinical practice in
populations of premature and very low birthweight infants (Alfasi & et al., 1985;
Farel, Freeman, Keenan, & Huber, 1991; Harrison & Magill-Evans, 1996; Huber,
1991; Magill-Evans & Harrison, 1999; Roman et al., 1995; Slater, Naqvi, Andrew, &
Haynes, 1987; Tesh & Holditch-Davis, 1997). The NCAFS coding system identifies
in a systematic and quantitative way, the behaviours and events which arise within the
observational setting.
NCAFS. The feeding scale (NCAFS) contains four subscales which measure
parent behaviours and include sensitivity to cues, response to distress, social-
emotional growth fostering, and cognitive growth fostering. Two subscales measure
infant behaviours including clarity of cues and responsiveness to the parent (Huber,
1991). A total of 76 individual items are observed and scored as present or absent
during a feeding time (Huber, 1991). All items are binary (yes or no) and scores
obtained from NCAFS coding include a caregiver score and an infant score which are
added together to give a total feeding score. The total amount of time taken to collect
video-data for NCAFS coding depends on the length of feeding time (Huber, 1991).
Sample items from the NCAFS are found in Appendix 7.
Normative data. Nurses participating in the NCAST project in 1979 collected
normative data for the NCAFS from mother-infant pairs whom they observed. In this
project trainees were required to observe five different “normal” families and achieve
96
a minimum of 85% agreement with a partner on both feeding and teaching scales. A
total of 845 feeding scales and 922 teaching scales represent these agreements
(Barnard et al., 1989). The sample consisted of mother-infant dyads from 19 cities in
the western United States. Mothers were primarily white, married and with an average
education level of 13 years or more. Infants ranged from 1-31 months at the time of
the feeding observations. Maternal scores were consistently related to the amount of
education the mother had received. The greater the number of years of education, the
higher the average scores on the maternal subscale. In situations where the mother
was unmarried, dyad scores were lower (Barnard et al., 1989).
Reliability and validity of NCAFS. The ability to achieve an interobserver
reliability of 85% is built in to the certification process required to code the NCAFS
scale (Barnard et al., 1989). The 85% interobserver reliability must be achieved with
a partner on at least five cases using the NCAFS scale. Barnard et al. (1989) reported
that this level is readily achieved by most observers (Barnard et al., 1989). In the
current study a trained NCAST coder was used to code the interaction data. Internal
consistency for both scales has been calculated for subscale and total scores (Barnard
et al., 1989).
The internal consistency reliabilities for the feeding scale items using the
Cronbach alphas are reported as follows: total parent score .83, total infant score .73,
and the combined total score .86. In the current study, the alpha coefficients were as
follows: the total parent score .94, total infant score .82 and the combined total score
.95 (Barnard et al. 1989). Some of the subscales do not display such strong internal
consistency, however the high total score is evidence that the entire interactive
process is being assessed (Foss, Hirose, & Barnard, 1999).
97
Concurrent, predictive, and construct validity of the NCAFS has been
investigated (Barnard et al., 1989). Empirical findings have been summarised by
Barnard et al. (1989) to support their assertion that four major characteristics are
fundamental to the parent-child interaction system. The authors suggest that low
interaction scores represent an immediate inability to express a repertoire of abilities
and not a lack of interactive behaviours. Various conditions of the mother and infant
such as depression, prematurity or apathy result in low levels of performance on
factors being measured rather than an inability to respond. This assertion is supported
by data, which suggest that infant prematurity and low maternal education and
depression, and other high risk factors are associated with low scores on the NCAFS
instrument (Barnard, Bee, & Hammond, 1984; Barnard, Booth, Mitchell, & Telzrow,
1988).
It is emphasised that NCAFS scales were not designed to measure the entire
range of interactive behaviours available for observation, and this can be a limitation
to the variety of purposes for which the NCAFS is appropriate. Another limitation of
the NCAFS scales concerns its use as a research tool. As a research tool, the NCAFS
scales lack standardisation data on populations other than healthy, mostly white, low-
risk, middle class mother-infant dyads (Huber, 1991). It has been argued that further
short-term test-retest reliability data would be useful, however the authors recommend
two administrations of the NCAFS scales before a decision is made that an
interactional problem exists in the mother-infant dyad (Barnard, Osofsky, Beckwith,
Hammond, & et al., 1996).
The NCAFS tool was chosen as the assessment tool of choice in the present
study because as a clinical tool observations can be made in almost any setting. The
time required to administer the NCAFS is very short and it is administered during a

98
routine feeding time that would occur whether an observer was present or not. Unlike
observational tools which require administration in a laboratory or where significant
amounts of time are needed for naturalistic observations, the NCAFS provides
minimal disruption to a mother and infant’s normal routine (Huber, 1991).
Procedure for data collection
Phase One
Phase One consisted of an initial survey at four weeks after the infant’s birth. This
survey provided the first psychosocial assessment of mothers of NICU infants. In
consultation with the Nurse Practice Coordinator, the researcher collated a list of
eligible participants from the unit admission data. The researcher liaised with the
NICU social worker to seek assistance for any participant who requested further
support and counselling.
Four weeks after their infant’s admission, mothers were approached by the
researcher during a nursery visit and invited to participate in the study. Completion of
the questionnaire occurred outside the NICU in a quiet area at an appropriate and at a
time convenient to the participant. A participant information statement and consent
form was given to those mothers who were willing to participate. The information
sheet also included an explanation of the Phase 2 data collection process. Participants
were advised that giving written consent and completing the questionnaire indicated
their consent to participate in the Phase 2 follow up. Additionally, participants were
advised that written consent would also allow the researcher to access their hospital
charts for additional information and forward appropriate results (ie high depression
scores) to the Neonatal Nurse Practice Coordinator for referral.
In approaching subjects for consent, the researcher did not coerce subjects and
emphasised that participation was voluntary. Potential participants were given one

99
week to consider their decision to participate in the study. Before written consent was
obtained the researcher requested verbal confirmation of the mother’s understanding
of the extent of their involvement in the study.
Phase Two
At 12 weeks following infant discharge, the researcher contacted the Phase 1
participants and requested permission to visit them in their home. Phase 2 data
collection occurred in the participant’s home, which was a familiar and non-
threatening environment. The mothers were asked to complete the Phase 1
questionnaire again. In order to observe mother-infant interaction the researcher
video-recorded the mother and infant during a feeding session in a place where the
mother indicated that she usually fed her infant.
A small digital video camera with a built in microphone was positioned at the
furthest distance from the observational setting as possible in order the minimise the
effect on maternal care behaviours. The mother was asked to feed her infant as usual
and to indicate to the researcher when she had finished the feeding. After the camera
had been set up and checked and the recording commenced, the researcher sat in a
position away from the feeding situation, and not directly observing the mother-infant
dyad. Every care was taken to ensure that a camera was positioned as unobtrusively
as possible to ensure that interactions occurred in as natural a setting as possible. Two
qualified NCAFS coders independently coded video-data. The dyads were given an
identification number and only the investigator could link to their names and
questionnaire data.
Ethical Considerations
While two tertiary referral centres were approached for ethical clearance to conduct
this research project, a number of barriers prevented the researcher from continuing to

100
seek permission from one recruiting centre. These issues related to the reconstitution
of the ethics committee and cancellation of two of the quarterly ethic’s committee
meetings resulting in significant delays to the approval process. Since the research
project was limited by time constraints, it was decided to abandon further approaches
for ethical clearance. Ethical approval to conduct this research project was obtained
from the University Human and Research Ethics Committee (Appendix 9) and from
the Mater Mother’s Hospital (Appendix 10). A copy of the patient information sheet
and consent form are attached as Appendix 11 and Appendix 12 respectively.
Risks to participants. In relation to the survey data collection, it was
acknowledged that there were potential risks to participants that included the
possibility of feeling uncomfortable and anxious about some questions. Also
participants may have feared being under investigation or that they could be identified
in some way by their responses. Additionally, it is possible that participants may have
felt uncomfortable as they were identified on tape. Other possible concerns included
how the tapes were used or whether the tapes could be lost. In acknowledging these
potential risks to participants, the next section outlines how the researcher
endeavoured to minimise these potential risks.
Protection against risks. Participants understood that participation was
voluntary and if at any time they decided not to continue participating in the study,
then they were free to withdraw without further comment, penalty or alteration to
mother and infant care. Videotaping occurred in the participant’s own home and in a
observational setting that was made to be as natural and unobtrusive as possible.
Copies of the tapes were posted to all participants.
While it is recognised that anonymity was not possible, as participants were
visually identified on tape, the participant was informed of steps that were to be taken

101
to ensure confidentiality. Videotapes were not used for any purpose other than for
coding to answer the research hypotheses. Copies of videotaped interaction were
given an identification number, coded by independent coders and returned directly to
the researcher where tapes were securely stored in a locked cabinet. Only the
principal researcher was able to link participant details to the identification number on
the video-data. Videotapes will be kept securely by the principal researcher for five
years and then destroyed in accordance with NH&MRC guidelines. Data were
analysed and stored on a secure network drive and back-up disks kept in a locked
filing cabinet. Finally, no information about the project will be published in any form
that will allow any individual to be recognised.
Staff Information. Staff working in the NICU were given information about
the project through inservice presentations and a staff information sheet which was
included in the infant’s chart (see Appendix 13). The proposal was presented to the
staff of the Growth and Development Research team who were responsible for
monitoring the development of graduates from the NICU at the participating hospital.
Pilot Study
The survey instruments were piloted with an independent sample of 10 mothers of
preterm, VLBW infants admitted to NICU. Mothers were asked to comment on the
appropriateness of the questions in content and length and on whether videotaping a
feeding interaction would be acceptable. A copy of the evaluation form used by
mothers is attached as Appendix 8. In consultation with the neonatal staff, the first
ten eligible mothers (n=10) were approached at approximately four weeks after their
infant’s admission to the neonatal nurseries and invited to participate in the study.
The purpose of the pilot study was to determine the ease, clarity and acceptability of
the survey instrument to participants. After providing information about the purpose

102
of the pilot study, all mothers who were approached agreed to participate by
completing a survey questionnaire and an evaluation questionnaire.
The evaluation questionnaire consisted of seven questions. Participants were
asked in general whether the survey questions were easy to understand. Responses
indicated that 80% (n=8) of participants found the questions easy to understand while
20% (n=2) reported some difficulty. However the researcher was present while
participants completed the survey questionnaire and this enabled immediate
clarification of any perceived difficulties.
Participants were also asked to indicate whether they found the survey
questions easy to answer. Responses indicate that all participants reported that the
questions were very easy or mostly easy to answer. In relation to the length of the
survey questionnaire participants were asked how long it took them to complete the
questionnaire. Ninety percent (n=9) responded that the questionnaire was not too
long to complete while 10% (n=1) thought it was long but did not find it a problem.
In addition, the researcher noted the time it took each participant to complete the
questionnaire. Eighty percent (n=8) of participants took less than thirty minutes to
complete the questionnaire while 20% (n=2) took up to forty minutes.
The final three questions asked participants to rate how accurately sections of
the questionnaire measured how they were feeling, the support available to them and
ways in which they have been coping. Responses indicate that 90% (n=9) percent of
participants thought the measures of psychological well-being expressed how they
were feeling while 10% (n=1) reported mostly. In relation to perceived social
support, 60% (n=6) of participants reported that the questions reflected support
available to them while 40% (n=4) indicated mostly. Finally participants were asked
if questions in the coping questionnaire measured ways in which they have been

103
coping. Eighty percent (n=8) of participants answered yes, while 20% (n=2)
indicated mostly. Therefore, based on the available data there were no major
concerns identified by participants in relation to the survey questionnaire or the
amount of time it took to complete. Therefore no modification was made to the
survey questionnaire for the main study.
Likewise, the video procedure using the NCAFS techniques was piloted by the
researcher and coded by a trained NCAFS coder. Preterm parent volunteers were
sought through the Preterm Infant Parents Association (PIPA) to participate in
piloting the NCAFS technique. There were two trained NCAFS coders in Brisbane
who agreed to code the video-data for this study. The purpose of the pilot study was
to determine the ease and acceptability of the questionnaire to participants and to
ensure that video-data were collected in such a way that it was amenable to coding
using the NCAFS technique. The results from this study were forwarded to the ethics
committee for final approval before the main study commenced.
Data Analysis
The data were entered into SPSS for Windows Release 10 and prepared for analysis.
Raw data were checked for errors by examining frequencies for each variable, and by
using the Explore procedure in SPSS for Windows. No missing values were found in
the data that were returned.
In order to analyse the self-report data, logistic regression analyses were
performed to determine whether Phase 1 maternal self-report results could predict
Phase 1 maternal depressive symptomatology. This was repeated for Phase 2
maternal self-report data and Phase 2 maternal depressive symptoms. Finally, the
Phase 1 maternal self-report results including depressive symptomatology were used
to determine if any Phase 1 variables could predict Phase 2 depression. Results from

104
the analyses were compared to determine the best predictive model. A comparison of
self-report data between Phase 1 and Phase 2 data using repeated measures analyses
(specifically doubly multivariate repeated measures analysis of variance) were
performed to compare the differences between maternal self-report at Phase 1 and
Phase 2.
Since the analysis of the self-report data involved identifying those variables
which could predict whether a mother would be depressed or not at Phase 1 and Phase
2, binary logistic regression was considered the most appropriate statistical test.
There are few assumptions of logistic regression and the three assumptions that were
tested in the current study were: 1) there were no autocorrelations; 2) no correlation
between the error and independent variables; and 3) an absence of perfect
multicollinearity between the predictor variables (Tabachnick & Fidell, 1996).
Inspection of intercorrelations among the predictor variables revealed some moderate
to strong correlations, although none were strong enough to make multicollinearity a
concern. Examination of standard errors of the logistic regression models, which were
all of an expected magnitude, suggested that multicollinearity due to linear
combinations of independent variables was not a concern. Logistic regression has no
assumptions about the distribution of the predictor variables and these predictors can
be any mix of continuous, discrete and dichotomous variables (Tabachnick & Fidell,
1996). In the current study the predictor variables were a mix of both categorical and
continuous variables.
The assumption for testing hypotheses about the differences in means between
two samples using Student’s t-tests and for conducting multiple regression is that “the
observations are random samples from normal distributions with the same variance”
105
(Norušis, 1993, p. 260). The normality of the data were investigated using histograms
and q-q plots, and found to be satisfactory. Any deviations from the normal curve
were therefore considered to be random.
Summary
The methodology used in the study has been described in this chapter. The
results of the study are presented in the following three chapters which have been
submitted to international journals for publication. Findings from Phase One of the
current study are presented in the next chapter.
106
CHAPTER SIX
THE IMPACT OF VERY PREMATURE BIRTH ON THE PSYCHOLOGICAL HEALTH OF MOTHERS
The results from Phase One of the current study which tested the first hypothesis
examining associations between a range of maternal and infant variables and self-
reported depressive symptomatology are presented in this chapter.
This chapter is presented in the format of a journal article which has been
published in Early Human Development 73, 61-70.
Abstract of the Article
Background
The birth of a very premature infant is a critical event in the life of a family and
studies have shown that mothers of these infants are at greater risk of psychological
distress than mothers of fullterm infants.
Study Design
A total population study of mothers of preterm infants born at less than 32 weeks
gestation at a tertiary referral hospital.
Subjects and Methods
Sixty-two mothers of very preterm infants (<32 weeks) participated in the present
study which examines correlates of maternal depressive symptomatology at one
month following very premature birth. Information was obtained from structured
questionnaires completed by mothers at one month after infant admission to neonatal
intensive care.
107
Results
Forty percent of the mothers reported significant depressive symptoms on the
Edinburgh Postpartum Depression Scale. Logistic regression analysis indicated that
high maternal stress resulted in an increased likelihood of depressive symptoms (OR
1.15, CI 1.04-1.26, p <0.01). Higher levels of maternal education (p<0.05), and
increased perception of support from nursing staff (OR 1.06, CI .88-1.00, p<0.05),
resulted in decreased likelihood of depressive symptoms.
Conclusions
The birth and subsequent hospitalisation of a very premature infant evokes
considerable psychological distress in mothers. These results have implications for
policy development in order to enhance family centred care in the neonatal intensive
care.
1. Introduction
Research studies have consistently demonstrated that 10-15% of postpartum women
experience depressive symptomatology severe enough to meet the criteria for a
diagnosis of depression (O'Hara & Swain, 1996) with greater than 60 % of these
women having symptom onset within the first six weeks postpartum (Stowe &
Nemeroff, 1995). Women experiencing postpartum depression suffer disabling
symptoms including loss of interest in usually pleasurable activities, fatigue,
difficulties in concentrating or making decisions, anger, over-sensitivity, and sleeping
difficulties (O'Hara & Swain, 1996).
The aetiology of postpartum depression is unclear and no single causative
factor has been isolated. However findings have consistently suggested that the major
factors contributing to the development of postpartum depression are primarily of a
psychosocial nature (Cooper & Murray, 1998; O'Hara, 1997). In particular, lack of

108
social support (Bernazzani et al., 1997), previous history of depression (Bernazzani et
al., 1997; O'Hara & Swain, 1996), marital conflict (O'Hara et al., 1991) and stressful
life events (Areias et al., 1996; Paykel et al., 1996) have been found to significantly
increase the risk of postpartum depression. In addition, a mother’s level of education
has been implicated as a possible risk factor in more recent studies (Gurel & Gurel,
2000; Johnstone et al., 2001). While the prevalence of postpartum depression has
been well studied in fullterm infant populations there is a paucity of research
investigating the differing experience of postpartum depression in mothers of
premature infants.
1.1 Stress, Coping and Premature Birth
Despite more open access to intensive care units and improved communication,
recent studies have indicated that mothers of premature infants are likely to
experience significant levels of stress (Brooten et al., 1988; Thompson, Oehler, &
Catlett, 1993). The unfamiliar and highly technological environment of the neonatal
intensive care unit (NICU), can take time to adjust to, however the physical aspects of
the unit have generally not been shown to be stressful for parents (Brunssen & Miles,
1996; Miles, 1989; Raeside, 1997). Evidence suggests that some of the greatest
sources of stress for parents include the appearance of a fragile, sick infant (Lindsay
et al., 1992; Raeside, 1997), fears for their infant’s survival (Meck et al., 1995),
alteration of their parental role, and the separation from their infant brought about by
hospitalisation (Hughes et al., 1994; Moehn & Rossetti, 1996; Shields-Poe & Pinelli,
1997).
The stress and uncertainty surrounding premature birth increases the need for
support, at least temporarily, while mothers struggle to cope with problems arising
from early birth (Easterbrooks, 1988). Many studies on family stress have examined
109
the different coping mechanisms which parents of premature infants use to moderate
their levels of stress. Perceived and actual availability of social support has been
found to influence a mother’s coping efforts (Lau & Morse, 2001). Supportive social
networks and being able to rely on a spouse or parent for help have been related to
less maternal depression and greater parenting competence (Gowen et al. 1989)
1.2 Depressive Symptoms in Mothers of Premature Infants.
There have been a wide variety of estimates of postpartum depression in mothers of
premature infants depending on the instrument used, the timing of administration and
the particular population of premature infants studied. Estimates of between 28%
(Meyer et al., 1995) and 70% of mothers of premature infants (Younger et al., 1997)
have been reported as having clinically significant degrees of psychological distress.
In a more recent longitudinal study, it was reported that at time of hospital discharge
and 12 months later, 45% and 36% (respectively) of mothers of medically fragile
infants reported scores which indicated a risk for depression (Miles et al., 1999).
Maternal depression is of concern not only because of its disabling effects on a
woman herself but also because it has been associated with infant cognitive,
emotional and developmental delay (Field, 1995; Murray & Cooper, 1997).
Although all infants may be vulnerable to the effects of maternal depression, the
premature infant is at greater risk due to his/her decreased responsiveness and
increased need for stimulation (Field, 1995).
Currently, there is little research that attempts to examine the variables that
correlate with depressive symptoms in mothers of very premature infants. The
purpose of this study was to identify factors associated with maternal depressive
symptomatology at approximately one-month post very premature birth.

110
1.4 Hypothesis
The hypothesis to be tested was that maternal depressive symptomatology at one
month post premature birth will be related to a previous history of depression, limited
formal education, limited social support, high levels of stress, limited use of coping
strategies and infants who were of low gestational age, birthweight and apgar scores.
2. Subjects and Method
All mothers of singleton premature infants born at less than 32 weeks gestation,
without congenital anomalies and cared for for at least three weeks in the neonatal
nurseries of a local tertiary referral hospital between May 2000 and February 2001
were eligible for inclusion. Mothers were required to be able to read and converse in
English and live within a 200km radius of the participating hospital.
Seventy-two mothers met the criteria during the recruitment phase of the study
and sixty-two mothers made up the final sample.
2.1 Instruments
The survey questionnaire booklet contained a number of previously validated
research instruments.
2.1.1 Edinburgh Postpartum Depression Scale (EPDS)
The 10-item Edinburgh Postpartum Depression Scale (EPDS) (Cox, Holden, &
Sagovsky, 1987) is a well-validated and widely used screening tool for depression
after childbirth. The EPDS is not diagnostic for depression, but gives an estimate of
psychological disturbance and alerts health care professionals that further assessment
may be required. Scores range from 0-30. A cut-off of 12 has been used in a number
of other studies investigating postpartum depression (Appleby et al., 1997) and was
also adopted for the present study.

111
2.1.2 Stress Scale of the Depression Anxiety and Stress Scale (DASS)
The 21 item Depression Anxiety Stress Scales (DASS) (Lovibond & Lovibond,
1995) was developed in response to the failure of traditional measures to clearly
distinguish between stress, anxiety and depression (Antony, Bieling, Cox, Enns, &
Swinson, 1998). The stress scale consists of 7 items with each scored on a 4-point
scale (0-3) with higher scores indicating higher level of stress.
2.1.3 Social Support Interview (SSI)
The SSI was designed by O’Hara, to assess pre-partum and post-partum social
network support (O'Hara, Rehm, & Campbell, 1983). The SSI rates support available
on a five-point scale for each identified sources of support (spouse, parent and
confidant). Summing across the questions gives a total support score ranging from 0 –
135. A high score reflects a high level of perceived support.
2.1.4 The Nurse Parent Support Tool (NPST)
The Nurse Parent Support Tool (NPST) (Miles, J. Carlson, & S Brunssen, 1999) is
designed to measure a mother’s perception of nursing support during her infant’s
hospitalisation. The perceived amount of nursing support received is rated on a
Likert-type rating scale. The range of scores is from 1-5 with the higher scores
reflecting a greater amount of perceived support from staff.
2.1.5 Coping Health Inventory for Parents (CHIP)
The Coping Health Inventory for Parents (CHIP) (McCubbin et al., 1983) is a
coping measure used to assess parents’ appraisal of their coping responses when their
infant is seriously ill. The CHIP consists of a checklist of 45 specific behaviours.
The CHIP asks parents to record on a scale of 0-3, how helpful each behaviour is in
their particular family situation. Summing across the questions gives a total support
score with higher scores indicating greater satisfaction with coping behaviours.

112
2.2 Demographic data
Maternal demographic data were collected and included education and a previous
history of depression. Infant data included apgar scores, birthweight (grams) and
gestational age (weeks).
2.3 Procedure
Recruiting commenced once university and hospital ethical clearance had been
granted. Mothers were invited to participate in the study during a nursery visit at
approximately one month after infant admission to the neonatal nurseries. This
timeframe was decided upon to allow time for the mother to physically recover from
childbirth, and become familiar with the nursery environment and for the infant’s
medical condition to stabilise. Information about the study was provided to mothers
in the parents’ lounge and written informed consent was obtained. Mothers were then
asked to complete the questionnaires listed above which had been compiled into a
single booklet. Demographic data on previous history of maternal depression and
infant birth history were collated from hospital records.
3. Data Analysis
In preparation for data analysis, bivariate associations were examined using Chi
square, t-tests and Mann Whitney for non-normally distributed variables. Only those
variables with significant associations with the dependent variable were entered into
the final logistic model. Multivariable logistic regression analysis was carried out to
examine the association between maternal depressive symptomatology and a range of
variables examined in the study.
4. Results
The majority of mothers in the sample were born in Australia (91.9%). The mother’s
ages ranged from 18-42 with the mean age of 29 years (sd 5.7). Just over 77% (48)

113
had completed secondary or tertiary education. For 55% (34) of mothers this was
their first baby, and for a further 24% (15) who were multiparous it was their first
premature infant. Sixteen percent (10) reported having had a previous history of
depression. An overwhelming majority of mothers (95%) reported having a
supportive spouse or partner.
Infant gestational age ranged from 24-32 weeks with a mean of 28 weeks (sd
2.4). Birthweight ranged from 513-2002 grams with a mean of 1088 grams (sd 359).
Apgar scores at 1 minute ranged from 1-9 with a mean of 5.75 (sd 2.48) and at 5
minutes they ranged from 1-10 with a mean of 7.71(sd 2.25).
The means and standard deviations of the major variables are presented in
Table 1. In general, the participants were mildly to moderately stressed, were
somewhat satisfied with their coping efforts and reported receiving high levels of
support from the nursing staff.
Table 6.1: Stress, coping and support scores: mean and standard deviations (n=62) Variable Mean (SD) Range Total possible score Total stress score
15 (9.06)
0-40
40
Total coping score
81 (18.44)
35-122
135
Nurse support
4.15 (.58)
2-5
5
Initial bivariate associations revealed that family social support scores, previous
history of depression, infant birthweight and apgar scores were not statistically
associated with the EPDS scores. Maternal stress scores, education, nurse support
scores, the infant’s gestational age were associated with the EPDS scores and were
used in the logistic regression model.

114
Scores on the EPDS ranged from 1-22, and 40.3% (25) of mothers scored ≥ 12
on the Edinburgh Postpartum Depression Scale. Overall, the logistic regression
model was significant χ2 36.271(7), (p <0.001). These results are presented in
Table 2.
Table 6.2: Logistic Regression Table : Significant variables associated with EPDS score a
Variables
% depressed
Adjusted OR 95% CI
P Value
Total stress score 40 1.15 (1.040-1.259) .006 Total nurse support score
40
1.064 (.883-1.00)
.050
Maternal Education .046 • Primary/Some
Secondary
17.5 Referent
• Completed Secondary
14.5
.058 (.006-.556)
.014
• Tertiary 8 .094 (.008-1.042) .054 a (n = 62) The relationship between maternal stress and depressive symptomatology reached
statistical significance such that a one point increase in stress score increased the risk
of depression by 14 percent. The relationship between a mothers’ perception of
support provided by nursing staff and depressive symptomatology also reached
statistical significance, so as nursing support decreased by a point, the risk of
depression increased by 6 percent.
Depressive symptomatology was also associated with educational status. The
risk of depressive symptoms was significantly higher in mothers who had completed
primary and some secondary education compared to those mothers completing
secondary education. There was a similar trend for mothers who had completed
primary and some secondary education compared to tertiary educated mothers but this
did not reach statistical significance. No significant difference was found between the
115
prevalence of depression and those mothers completing secondary education and
tertiary educated mothers (p=.598). Neither gestational age of the infant nor maternal
coping scores were statistically significant when entered into the final logistic model.
5. Conclusions
The percentage of mothers reporting depressive symptomatology in this sample of
mothers of very premature infants is higher than the population norms (40% vs 10-
15%). This was not unexpected given that families were in the acute phase of their
infants’ hospitalisation and were still coming to terms with the disappointment of the
early birth, the ongoing day to day medical crises and the possibility that their infant
may have continuing health and/or developmental problems. The result is similar to
other studies which have demonstrated that mothers of premature infants suffer
significant depressive symptomatology in the postpartum period while their infant is
in hospital (Logsdon & Davis, 1997; Miles et al., 1999c).
The primary purpose of the study was to test the hypothesis that certain
maternal demographic and psychosocial variables, as well as infant variables, are
associated with maternal depressive symptoms at one-month post premature birth.
The hypothesis was partially supported in that maternal education; stress symptoms
and perceptions of nurse support were significantly correlated with depressive
symptoms. However, family social support, coping behaviours and infant factors
were not associated with depressive symptoms.
The most significant variable associated with depressive symptomatology was
maternal stress symptoms. It has been well established that mothers of premature
infants assume the role of parenthood under highly stressful hospital conditions before
they or their infant are ready for it. Separated from their fragile infants, unable to feel
part of their care, and fearing for their survival, with only limited opportunities to

116
interact, it is not surprising that mothers operating under these stressful conditions
reported symptoms of depression.
While concurrent life stressors were not measured in this study, parents may
also experience stress relating to other contexts outside the NICU. Nursery staff may
be unaware of these outside stressors, which nevertheless may influence parents’
perceptions and interactions on the unit (Hughes & McCollum, 1994). During the
data collection interview, many mothers reported significant concurrent life stressors
including bereavement, financial and work concerns which may have contributed to a
mother’s depressive symptoms. In future studies, a formal assessment of external
sources of life stressors could be included to provide a clearer picture of maternal
distress.
As hypothesised, a mother’s level of education was related to depressive
symptoms. Mothers who had not completed secondary education were more likely to
be depressed compared to those who had completed secondary or tertiary education.
Those mothers with a lower level of education may have fewer resources that enable
them to ask questions or establish effective patterns of communication in the face of
high-risk birth and NICU hospitalisation. In addition, these mothers may have lower
expectations of support and information or may have felt overwhelmed or intimidated
within the acute care setting. Mothers with a lower level of education may also have
limited financial resources with which to travel to and from hospital or to care for a
sick infant at home creating additional stress. Maternal education has been linked to
depression in mothers of full-term infants (Gurel & Gurel, 2000; Johnstone et al.,
2001).
Perception of support provided by nurses was also significantly associated
with depressive symptoms. Results indicated that as perception of nurse support
117
decreased a mother’s depressive symptoms increased. The means and standard
deviations for the NPST reported in the study (Table 2) are comparable to those
reported by Miles in a validation study where a mean of 4.12 and SD 0.72 were
reported (Miles et al., 1999a). These high scores suggest that neonatal nurses were
perceived to provide a high level of support and are an important resource for
mothers. Other studies have also reported high satisfaction with the support provided
by the primary nurse caring for the infant (Affleck et al., 1991; Miles et al., 1996). It
is also possible that mothers were unwilling to be critical of nurses at this stage of
their infant’s hospitalisation as they are still very dependant upon them for their
infant’s care. Also whether the presence of depressive symptoms caused mothers to
perceive less support from nurses or whether less nursing support contributed to
maternal depression is not clear. Mothers may not have been able to obtain the
support they needed, as it can be difficult to establish lines of communication with
nursery staff. Families encounter a complex array of caretakers during the course of
hospitalisation (Affleck et al., 1991; Redshaw et al., 1996). Parents may have to tell
their story again and again to each new nurse assigned to the infant’s care. In this
environment, a mother may not be able to develop a trusting relationship with her
infant’s care-giver or feel safe to talk about other issues which concern her.
Family social support was not associated with EPDS scores and was therefore
not used in the final model. Since the majority of participants (97%) reported having
a supportive spouse/partner whom they could rely upon for material help and
emotional support it is possible that this high level of close family support buffered
against the negative responses to their infant’s NICU hospitalisation. This finding is
similar to other studies which have found the baby’s father as a vital source of support
(Affleck et al., 1991; Miles et al., 1996). The coping strategies adopted by mothers
118
were also not related to their depressive symptoms. McCubbin and McCubbin (1993)
have defined coping as the specific efforts by which individuals or families attempt to
reduce the effect of a stressor on the family and to manage the situation. Seeking
social support and communicating with others during infant hospitalisation were
specific coping strategies described by mothers in other studies (Affleck et al., 1991;
Crnic et al., 1984; Hughes et al., 1994). Since mothers in this study reported
moderately high levels of spousal support, this support may have enhanced coping
efforts.
Other variables, which showed no association with depressive symptoms,
were a previous history of depression and measures of infant status. A previous
history of depression has been shown to be a risk factor for postpartum depression in
other studies (Bernazzani et al., 1997). The lack of association with the EPDS in the
present study could be due to the relatively small number of mothers who reported
previous depressive episodes (10 out of 62 subjects). The buffering effect of the high
levels of nurse and family support reported by the participants may also have been
protective. The hypothesis that mothers with smaller, sicker infants would be at
greater risk for depressive symptoms was not conclusively supported and may have
been because the infants were all very preterm and represented a fairly homogenous
group. Very few studies have examined factors associated with maternal distress
during infant hospitalisation and the results of the present study may have been
influenced by a number of factors. Most mothers were reasonably well educated and
felt supported by their partner and family and infants were all very preterm. Further
research with a larger and more heterogenous sample would increase the likelihood of
detecting effects which are truly present.

119
The results need to be interpreted within the limitations of the study, including
the sample size, reliance on self-report data and the correlational nature of the study
which does not permit any causative links to be identified.
Recommendations Findings from this study indicate that the birth of a very premature infant evokes
considerable psychological distress in mothers. Given the high percentage of
depressive symptomatology identified in this study it is recommended that mothers of
very preterm infants be routinely screened for postpartum depression. Once
identified, postpartum depression is amenable to treatment, which can alleviate
months of suffering for mothers and reduce potentially adverse outcomes for the
mother and infant. The neonatal period affords a crucial opportunity to identify
mothers who are most at risk of postpartum depression.
The findings reported in this paper also have implications for nursing, medical
and other health care professionals working in the NICU. Researchers have
emphasised that understanding of the nature of stress, the coping abilities or resilience
of families, and how best to support families is vital for professionals providing
services to these infants and their families (Affleck et al., 1991; Berry & Hardman,
1998). Other investigators have suggested that the psychosocial adjustment in both
parents, but in particular mothers should be assessed and counselling to reduce their
distress should be provided (Doering, Dracup, & Moser, 1999). Interventions which
aim to identify and reduce maternal stress and depression need to be developed not
only to promote family stability but also to provide long-term benefits to the infant’s
development.

120
CHAPTER SEVEN
THE COURSE OF DEPRESSION IN MOTHERS’ OF PREMATURE INFANTS IN HOSPITAL AND AT HOME
The results from Phase One and Phase Two of the current study are presented in this
chapter. This phase of the study tested the second and third hypotheses which
examined the association between maternal depressive symptoms at Phase 2 and
maternal and infant variables from both Phase One and Phase Two.
This chapter is presented in the format of a journal article which has been
published in the Australian Journal of Advanced Nursing , 21 (2) 20-27..
Abstract of the Article
The risk of continuing depression in mothers of very premature infants after discharge
has not been studied in any depth. This study compared reports of maternal
depressive symptomatology at one month after infant birth (Phase 1) and three months
following infant hospital discharge (Phase 2). Fifty-two mothers completed the
Edinburgh Postnatal Depression Scale at these two points in time.
Results indicate that the percentage of mothers who reported high levels of
depressive symptoms significantly decreased between Phase 1 and Phase 2. Logistic
regression analysis indicated that depression scores at Phase 1 and maternal stress at
Phase 2 were important factors in explaining depression scores at Phase 2.
Background
In Australia, premature birth accounts for 7.3% of all births with approximately 1 in 5
of these being less than 32 weeks gestation (Day et al., 1997). Over the past three
decades, significant advances in the medical management of critically ill premature
infants have resulted in unprecedented rates of survival of small premature infants
especially those of extremely low birth weight (<1000grams) (Lee et al., 1995;

121
Raddish & Merritt, 1998; Vohr & Msall, 1997). These medically fragile infants can
spend weeks and months separated from their parents receiving life saving treatment
in the neonatal nurseries.
While the infant’s hospitalisation is stressful for mothers, the transition home
does not always mean the infant’s problems are resolved and such circumstances
introduce new challenges to parents’ adaptation and coping ability (Affleck et al.,
1991). Going home with their baby is often eagerly anticipated but can be stressful
for parents who will assume full responsibility for an infant who for weeks or months
has been regarded as medically fragile and in the care of experts (Easterbrooks, 1988;
Miles & Holditch-Davis, 1997). A number of studies have found that parents feel ill
equipped to assume full responsibility for their infant at discharge (Brooten et al.,
1989; Kenner & Lott, 1990). In the weeks following discharge parents continue to
feel anxious about infant care issues, how to recognise infant illness, understanding
growth and development and fearing for their infant whom they still view as sick
(Brooten et al., 1989; Kenner & Lott, 1990). In many cases parents must give care to
a sick infant whose needs are beyond the needs of a normally developing infant
(Patterson et al., 1994; Sterling et al., 1996). It has also been reported that premature
infants are more difficult to parent than full-term infants, at least for the first year of
life, as they tend to be less adaptable, less predictable, and fussier than their term
counterparts, probably due to neurological immaturity (Gennaro et al., 1990;
Gottwald & Thurman, 1990). These aspects of the infant’s behaviour and atypical
infant responses may affect parent-infant interaction and complicate the developing
relationship (Harrison & Magill-Evans, 1996).
Together, these difficulties can create additional stress that can lead to
depression (Mercer, 1990) and mothers’ of these infants have been shown to be at

122
greater risk of psychological distress than mothers of term infants (Gennaro, 1988;
Pederson et al., 1987). However there have been few studies into the extent to which
depressive symptomatology continues for mothers after infant discharge. Studies
have found initially high levels of maternal psychological distress in the neonatal
period subsided by 8-12 months after discharge (Brooten et al., 1988; Singer et al.,
1999; Thompson et al., 1993). However women with premature infants have been
shown to demonstrate evidence of depression prior to infant discharge and at one
month after discharge (Logsdon & Davis, 1997). In another study of maternal
depression, 33% of mothers of infants in NICU showed high levels of psychological
distress, three to five weeks after infant admission and a further 41% were
significantly distressed at 6 months (corrected for prematurity) (Thompson et al.,
1993). Miles (1999) also reported elevated but comparable rates of depression at the
time of hospital discharge (42%) and 12 months later (36%).
There has been little consensus regarding which mothers of very premature
infants are most at risk and which maternal or infant characteristics best predict
maternal depressive symptoms (Meyer et al., 1995). Some studies have found that the
severity of the infant’s illness has been related to increased rates of depression
(Bennett & Slade, 1991; Blumberg, 1980; Locke et al., 1997) but others have not
(Gennaro et al., 1990; O'Brien et al., 1999; Spear et al., 2002; Thompson et al., 1993).
In general, research indicates that postpartum depression develops as a consequence
of a complex interplay of biological and psychosocial risk factors (Cooper & Murray,
1998; O'Hara, 1997). Studies have also drawn attention to protective factors that
reduce the risk of depression developing (Affleck et al., 1991). Social support
research has established many links between supportive elements within family
relationships and individual outcomes including psychological distress or coping with

123
stressful life events (Pierce et al., 1996). Researchers have found that the stress
buffering role of social support was related to improved psychological adjustment in
mother’s of premature infants (Affleck et al., 1991) and that parents who have
effective social networks are better adjusted and interact in more optimal ways with
their child (Dunst et al., 1986). Researchers are now examining both risk and
resiliency factors in relation to postpartum depression.
Theoretical models have attempted to provide ways to understand how
families adapt to differing stages of childhood illness including the birth and transition
home of a very premature infant. The Resiliency Model of Family Stress, Adjustment
and Adaptation (McCubbin, Thompson, & McCubbin, 1996) suggests that two related
but discernible phases mark a family crisis: namely adjustment and adaptation.
Adjustment is described as the family’s initial response to a crisis event during which
the family attempts to meet demands utilising existing resources or resistance
capabilities (McCubbin & McCubbin, 1993). The adaptation phase describes the
outcome of the family’s efforts to bring about a new level of functioning in response
to a family crisis situation (McCubbin & McCubbin, 1993). During the adaptation
phase the family attempts to restore family stability by acquiring new resources and
coping behaviours. Families who are able to marshal their resources may respond
with resiliency and adaptive functioning. A family’s coping behaviours consist of
cognitive and behavioural efforts to manage psychological stress (Lazarus, 1993).
Family change and adaptation over time is the primary focus of the Resiliency Model
and denotes the outcome of family efforts to bring a new level of balance, harmony,
coherence, and functioning to a family crisis situation (McCubbin et al., 1996). The
Resiliency Model attempts to delineate post-crisis variables that may influence the

124
family’s ability to achieve adaptation, including critical psychological, social and
coping factors that may affect adaptation.
In this study, the adjustment phase or Phase 1 (P1) denoted the period at one
month after infant admission to neonatal intensive care (NICU) while the mothers of
very premature infants were in the process of adjusting to the crisis of premature
birth. Those mothers who agreed to participate at P1 also gave consent for the
researcher to visit them three months after their infant had been discharged home.
This time was considered as the adaptation phase or Phase 2 (P2) when mothers had
time to adapt to the practical and emotional effects of caring for their very premature
infant.
Purpose of the study
This paper reports the second phase in a two-phase study investigating variables
associated with maternal reports of depressive symptomatology at 3 months after the
infant was discharged from hospital (Phase 2). The results of the first phase (P1) are
the subject of another paper, but generally indicated that many mothers suffered
considerable psychological distress while their infant was hospitalised. The purpose
of the second phase of the study was to visit these mothers again at three months after
infant hospital discharge to compare maternal depressive symptomatology and factors
that influence depressive symptoms across time. Specifically, the study aimed to
determine if critical psychosocial and demographic factors measured at P1 and P2 are
associated with depressive symptoms at P2.
Research Hypotheses
• Elevated levels of maternal depression at three months after infant hospital
discharge will be related to a previous history of depression and limited formal

125
education; limited social support (from family and/or nursing staff), limited
use of coping strategies and high levels of stress and depressive symptoms
during P1; and having infants of low gestational age, birthweight and apgar
scores.
• After controlling for P1 depression, elevated levels of depressive symptoms at
P2 will be related to limited social support, limited use of coping strategies,
high levels of stress during P2 and having infants who had long hospital stays
and high medical risk.
Method
Participants
All mothers of singleton premature infants born at less than 32 weeks gestation,
without congenital anomalies and cared for at least three weeks in the neonatal
nurseries of a local tertiary referral hospital were eligible to participate in the study.
Mothers were required to be able to read and converse in English and live within a
200km radius of the participating hospital.
Procedure
The institutional and university ethics committees approved the follow-up protocol.
Sixty-two mothers participated in the first phase of the study by completing a survey
questionnaire at one month after infant admission to the neonatal nurseries. In giving
informed consent, participants gave the researcher permission to visit them in their
homes at three months after infant discharge from hospital.
At Phase 2, all of the Phase 1 mothers were contacted. Of the original 62
mothers, five were unable to be followed up due to infant rehospitalisation (two) and
social issues (three). Four mothers were not traceable and there was one infant death.
Fifty-two mothers made up the final comparison sample.

126
Instruments
Mothers completed a survey questionnaire which contained a number of previously
validated research instruments drawing upon the concepts contained within the
Resiliency Model. This model focuses on the stress response (depression and stress
measures), resources a family has (ie support) and what a family does in response to a
stressful event (ie coping behaviours). The questionnaires which were included are
described below.
Edinburgh postpartum depression scale (EPDS)
The 10-item Edinburgh Postpartum Depression Scale (EPDS) (Cox, Holden, &
Sagovsky, 1987) is a well-validated and widely used screening tool for depression
after childbirth. Each item is scored on a 4-point scale (0-3), the minimum and
maximum total score ranging from 0-30, respectively. In this study a score of 12 and
above was used as a cut-off for depressive symptomatology.
Stress scale of the depression, anxiety and stress scale (DASS)
The stress scale of Depression Anxiety Stress Scales (DASS) (Lovibond & Lovibond,
1995) contains 7 questions each scored on a 4-point scale (0-3), and a minimum and
maximum total score ranging from 0-40. Higher scores indicate higher levels of
stress.
Social support interview (SSI)
The SSI was designed to assess post-partum social support provided by, and given to,
a participant’s spouse/partner, closest confidant and closest parent (O’Hara et al.,
1982; 1983). The SSI asks the participant to give a rating from no person available
(0) and never to always (1-5), for each identified sources of support (spouse, parent
and confidant). Summing across the questions give a total support score ranging from
0 – 135. A high score reflects a high level of perceived support.

127
The nurse parent support tool (NPST)
The Nurse Parent Support Tool (NPST) (Miles, Carlson, & Brunssen, 1999) is
designed to measure a mother’s perception of nursing support during their infant’s
hospitalisation. Parents are asked to rate the amount of nursing support received on a
Likert-type rating scale ranging from “1” almost never to “5” almost always. The
scores are summed and divided by the number of items completed (21). The range of
scores is from 1-5 with the higher scores reflecting a greater amount of perceived
support from staff.
Coping health inventory for parents (CHIP)
The Coping Health Inventory for Parents (CHIP) (McCubbin et al., 1983) is a coping
measure used to assess parents’ appraisal of their coping responses when their infant
is seriously ill. The CHIP consists of a checklist of 45 specific behaviours. The CHIP
asks parents to record on a scale of 0-3, how helpful each behaviour is in their
particular family situation. Summing across the questions gives a total support score
with higher scores indicating greater satisfaction with coping behaviours.
Demographic Data
The principal researcher collected the following information from the maternal and
infant hospital records.
Neurobiological risk score (NBRS)
The infant Neurobiologic Risk Score (NBRS) (Brazy, Eckerman, Oehler, Goldstein,
& O'Rand, 1991) was developed in response to the need for an assessment tool that
provides early identification of infants who are at high risk for neurodevelopmental
abnormality. The seven-item NBRS instrument uses a progression of scores (ie
0,1,2,4) to assess the presence, duration and severity of a medical event. Three
neurobiological risk groups are identified: Low risk (0-4), intermediate risk (5-7) and

128
high risk (>8). The principal researcher and the director of neonatology determined
the NBRS for participants from chart data after infant discharge.
Maternal demographic data including education and a previous history of
depression were collected. Infant data included birthweight (grams) gestational age
(weeks) and total length of hospital stay (LOS).
Data Analysis
An independent samples t-test was performed to compare the mean EPDS scores
between those who continued in the study and those who were lost through attrition.
Results indicated that the differences in the means were not significant (p = 0.477).
Also there was a difference in the timing of administration of the P2 questionnaire due
to the differing lengths of infant hospitalisation. In order to test if there was a
relationship between length of time to follow-up and P2 depression scores the
correlation between the two variables was examined. Results indicated there was not
a significant association between the length of time to follow-up and P2 depression
scores (r=.148, p=.136).
To test for significant changes in total scores of the four explanatory variables
across the two phases, a doubly multivariate analysis of variance was conducted. The
multivariate result was significant (F (df = 5,47) = 7.38, p < 0.001; power = .998; eta2
= .44). Inspection of the univariate results indicated that at phase two mothers
reported lower stress scores (F = 7.23 (df =1,51), p <0.05 ; power = .75; eta2 = .124),
and higher coping scores (F = 12.24 (df = 1,51), p <0.001; power = .929; eta2 =.194).
The results indicated that for social support and nurse support there was no change
over time, although the latter approached significance (p = 0.052). The means and
standard deviations are presented in Table 3.
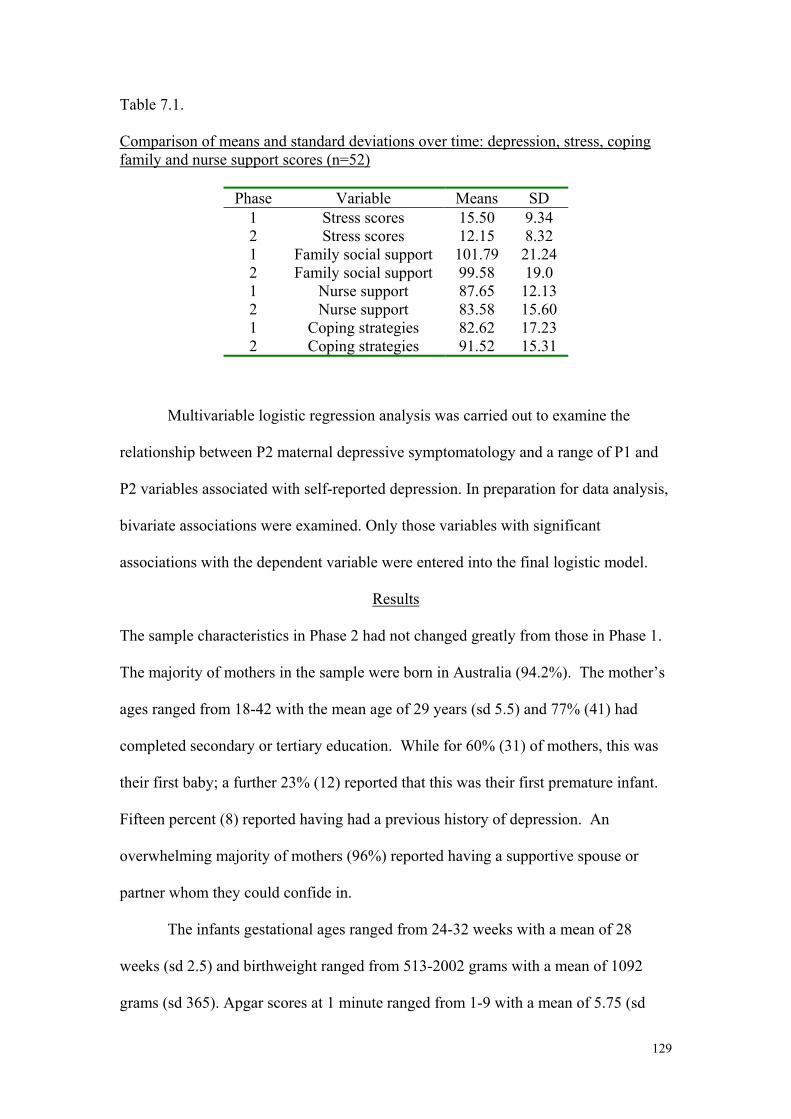
129
Table 7.1. Comparison of means and standard deviations over time: depression, stress, coping family and nurse support scores (n=52)
Phase Variable Means SD 1 Stress scores 15.50 9.34 2 Stress scores 12.15 8.32 1 Family social support 101.79 21.24 2 Family social support 99.58 19.0 1 Nurse support 87.65 12.13 2 Nurse support 83.58 15.60 1 Coping strategies 82.62 17.23 2 Coping strategies 91.52 15.31
Multivariable logistic regression analysis was carried out to examine the
relationship between P2 maternal depressive symptomatology and a range of P1 and
P2 variables associated with self-reported depression. In preparation for data analysis,
bivariate associations were examined. Only those variables with significant
associations with the dependent variable were entered into the final logistic model.
Results
The sample characteristics in Phase 2 had not changed greatly from those in Phase 1.
The majority of mothers in the sample were born in Australia (94.2%). The mother’s
ages ranged from 18-42 with the mean age of 29 years (sd 5.5) and 77% (41) had
completed secondary or tertiary education. While for 60% (31) of mothers, this was
their first baby; a further 23% (12) reported that this was their first premature infant.
Fifteen percent (8) reported having had a previous history of depression. An
overwhelming majority of mothers (96%) reported having a supportive spouse or
partner whom they could confide in.
The infants gestational ages ranged from 24-32 weeks with a mean of 28
weeks (sd 2.5) and birthweight ranged from 513-2002 grams with a mean of 1092
grams (sd 365). Apgar scores at 1 minute ranged from 1-9 with a mean of 5.75 (sd

130
2.48) and apgar scores at 5 minutes ranged from 1-10 with a mean of 7.71(sd 2.25).
Infants were hospitalised between 26-179 days with a mean of 70 days (sd 30).
Neurobiological Risk Scores ranged from 0-15 with a mean of 2.7 (sd 3). A vast
majority of infants 81% (42) fell within the range of low risk for developmental delay
while 9.6% (5) were at intermediate risk and a further 9.6% (5) were categorised at
high risk for developmental delay.
During P1 just over 40% (25/62) of mothers scored significant depressive
symptomatology however this number decreased to 17% (9/52) at P2 a level similar
to the population prevalence of 10-15% (O'Hara & Swain, 1996). However of the
mothers who suffered significant depressive symptoms at P2, all but one had been
depressed at P1.
A separate paired samples t-test was conducted to formally test the
significance of the change in the EPDS scores between P1 and P2. Results showed
strong evidence for a drop in EPDS scores across time (p=0.001) ( P1= 10.54 to P2=
7.33) indicating that mothers depressive symptomatology did improve between the
two time points. At P2, scores on the EPDS ranged from 1-25 (Mean 7.3 SD 5.29).
Just over 17% (9) of the mothers scored > 12 on the Edinburgh Postpartum
Depression Scale, the threshold indicating probable depression (Cox, Holden, &
Sagovsky, 1987).
Initial bivariate associations of the P1 variables from the first hypothesis
revealed that maternal socio-demographic and infant demographic were not
statistically associated with the P2 depression scores. Only P1 depression scores were
associated with P2 depression. To test the first hypothesis, a logistic regression
examined the relationship between P1 depressive symptomatology and P2 depression
scores. The logistic regression model was significant χ2 12.93 (3), (p <0.001).
131
Depression scores reported while the infant was in hospital was significant (p<0.05)
so that mothers who were depressed at P1 were 28% more likely to be depressed at P2
(OR 1.28, CI = 1.02-1.59).
Bivariate associations with the P2 variables from the second hypothesis
showed that maternal socio-demographic and infant hospital stay and morbidity risk
were also not significantly associated with P2 depression scores. Only P2 stress
scores were associated with P2 depression. Therefore only P1 depression scores and
P2 stress scores were used in the final logistic regression model to examine the
hypotheses of interest. After controlling for P1 depression scores a second logistic
regression was conducted to examine the relationship between P2 depression and
variables reported at P2. The logistic regression model was significant χ2 20.99 (4),
(p<0.001). The mother’s stress score was significant (p<0.049) indicating that as the
mother’s stress increased the risk of depression also increased by 17 percent (OR
1.17 CI = 1.00-1.35).
Discussion
The purpose of the study was to compare maternal reports of depressive symptoms
across time and to test two hypotheses that certain maternal demographic,
psychosocial and infant variables measured at P1 and P2 are associated with maternal
depressive symptoms at P2.
It seems that maternal reports depressive symptomatology decreased
significantly at three months after infant discharge. This finding is consistent with
previous work that showed that mothers experienced less psychological distress in the
months after discharge (Brooten et al., 1988; Singer et al., 1999). However, the
findings are not consistent with other studies that found elevated rates of maternal
depressive symptoms after discharge (Miles, Holditch-Davis, Burchinal, & Nelson,

132
1999; Thompson et al., 1993). It seems that evidence of continuing depression in
mothers of very premature infants remains inconclusive.
The association between premature birth and postpartum depression has been
reported in terms of women experiencing an adverse life stressor (Kumar & Robson,
1984), or having an infant in NICU for an extended period (Gennaro 1988). However,
the results from the current study can be interpreted in light of evidence suggesting
that no one factor can be implicated as a ‘cause’ for postpartum depression; that it is a
result of the complex interaction between biological and psychosocial risk factors
(Cooper & Murray, 1998; O'Hara, 1997). This suggests the birth of a very premature
infant may not pose a threat to family adaptation in the presence of adequate family
resiliency resources. The Resiliency Model examines the adaptational outcome as a
function of the relationship between characteristics of the infant (degree of
prematurity, birthweight, and neurobiological risk) and the characteristics of the
mother (educational level) and the family’s resources (social support and coping).
The study’s sample was generally well resourced with a majority of women living
with a supportive spouse or partner, having 12 years education or more, and infants
who were at low risk for neurodevelopmental abnormality. It appeared that many
mothers in the study had resolved their initial shock and by 3 months had adapted to
the realities of caring for their premature infant as evidenced by the decrease in
depression scores over time.
Nevertheless, the incidence of depression in this study is similar to the
population prevalence and unlike mothers of full-term infants who experience shorter
hospital stays, mothers of very premature infants remain in constant contact with the
health care system until their infant is discharged. The neonatal period provides an
ideal opportunity to screen for those women who may be most at risk. This provides

133
an opportunity for staff to identify the mothers’ depressive symptomatology and
ensure support systems are in place to reduce it continuation especially following
discharge from hospital. The disabling symptoms of postpartum depression create a
disruption in family life when exceptional demands are being placed on a woman
caring for a vulnerable infant (Holden, 1994). In particular, the very premature infant
is more vulnerable to the adverse effects of continued maternal depression due to
his/her decreased responsiveness and increased need for appropriate stimulation
(Field, 1995). In order to prevent the development of more serious symptoms, it is
crucial to identify and treat women with postpartum depression as early as possible
(Beck, 1998).
The first hypothesis was partially supported in that depression scores reported
at one month after infant admission to hospital were significantly associated with
depressive symptoms at 3 months post-discharge. There is a need for psychosocial
and family services to be incorporated into neonatal follow-up services to evaluate
maternal depression and adaptation since some studies have reported severe
symptoms of psychological distress in mothers of high risk premature infants at two
years (Singer et al., 1999). Referral for treatment may prevent the development of
more serious symptoms that can have deleterious effects to the mother, family and
infant.
The second hypothesis was also partially supported in that maternal reports of
stress once at home with the infant were associated with depressive symptoms. While
stress may be a result of many influences including the unique health care needs of an
infant who may be temperamentally more difficult (Gennaro, 1996), mothers were
seen relatively early in the neonatal period when all young infants require substantial
care giving efforts. However maternal stress and depression, through their impact on

134
the quality of parenting and the caregiving environment, can have deleterious effects
on parent-infant interaction, as well as the cognitive, emotional, and social
developmental outcome of the infant (Sameroff & Fiese, 1990). The effect of the
other P2 variables including support and coping was not linked to P2 depression.
Since the majority of mothers scored below the cut off for depression this result may
reflect successful adaptive functioning when families are no longer in a state of crisis.
Other infant outcome variables including length of hospital stay and
neurobiological risk were also not associated with P2 depressive symptoms.
Although some studies have suggested that mothers whose infants were hospitalised
longer may have a greater chance for physical and emotional recuperation than those
with shorter stays (Brooten et al., 1988; Tulman & Fawcett, 1988), the length of
hospital stay did not influence maternal depression in this study. Also the severity of
the infant’s illness was not associated with depression, a finding supported by some
studies (Gennaro, York et al., 1990; Thompson et al., 1993) but not by others (Bennett
& Slade, 1991; Blumberg, 1980).
Results of the study need to be considered with caution due to the relatively
small sample size; future studies would require a larger sample size to increase the
study’s power to detect effects, which are truly present. Results need to be
interpreted within the limitations of the study, in particular the reliance on self-report
data and the correlational nature of the study.
Recommendations
The findings have implications for health care policy given that the increased survival
of very premature infants with neurodevelopmental abnormalities may lead to an
intolerable family burden for those families with the least resources (McCormick,
1997; Raddish & Merritt, 1998). Findings from this study support the need for more

135
longitudinal studies focusing on maternal stress and depressive symptoms in mothers’
of very premature infants and the factors that place a woman at continuing risk of
depression. Once identified, postpartum depression is amenable to treatment. Early
identification and intervention will promote family stability and enhance the long-
term development of infants who are at both biological and psychosocial risk.
Developing and practising preventive measures is cost-effective as well as humane
and the importance of allocating scarce health care resources to prevention rather than
treatment is increasingly acknowledged (Holden, 1994).

135
CHAPTER EIGHT
MOTHER-INFANT INTERACTION IN PREMATURE INFANTS AT THREE MONTHS AFTER NURSERY DISCHARGE
The findings from the exploratory phase of this study which tested the fourth, fifth and
sixth hypotheses are presented in Chapter Eight. These hypotheses examined the
differences in interaction scores between the present study’s sample and the population
norms as well as the relationship between Phase 1 and Phase 2 maternal and infant
variables and mother-infant interaction.
This chapter is presented according the format required for journal articles
which was accepted for publication in the International Journal of Nursing Practice 9,
374-381.
ABSTRACT
Both the immature and disorganised behaviour of the premature infant and
psychosocial or socio-economic factors which adversely affect a mother’s
responsiveness to her premature infant can jeopardise the mother-infant relationship.
At three months after infant hospital discharge, the interactions of fifty
premature infants (≤ 32wks) and their mothers were videotaped and coded using the
Nursing Child Assessment Feeding Scale (NCAFS). The relationship between data
derived from the feeding interaction and maternal psychosocial and infant perinatal
variables collected at one month after birth and at three months after discharge from
hospital were examined. Results showed that the mothers’ use of coping strategies
both in hospital and at home were important factors in explaining mother-infant
interaction.

136
INTRODUCTION
Although there have been some contradictory findings, a substantial number of
studies have documented interactional patterns which distinguish preterm and full-
term infants (Harrison & Magill-Evans, 1996). Preterm infants have been reported to
initiate interaction less often, provide fewer distinct cues to their caregiver, to be less
attentive and to show less positive affect (Barnard et al., 1984; Goldberg & DiVitto,
1995). Interactions have been found to be less mutually satisfying for mothers and
premature infants than for mothers and full-term infants (Bakeman & Brown, 1980;
Wille, 1991). The stress associated with the infant's hospitalisation and the immature
and disorganised behaviour of the premature infant might contribute to parenting
difficulties during the first year of life (Minde et al., 1983). Mothers may have to
work harder to initiate and maintain interaction than mothers of full-term infants, and
in return receive fewer positive responses from their infant (Harrison, 1990). Several
studies have reported that mothers of preterm infants are more active in initiating and
maintaining interactions and engage in increased amounts of stimulation throughout
the first year (Bakeman & Brown, 1980; Crnic et al., 1983; Field, 1979). This
heightened level of maternal behaviour may reflect their efforts to compensate for
deficiencies in their preterm infants’ interactional abilities (Goldberg & DiVitto,
1995; Miles & Holditch-Davis, 1995).
During the first year after birth, the mother constitutes a major part of the
infant’s social environment (Beck, 1996). The presence of risk factors which can
negatively affect the mother’s availability as an interactive partner, in addition to the
biological risk conferred by infant prematurity, can place the developing parent-infant
relationship in what has been described as ‘double jeopardy’ (Beckwith, 1988;
Escalona, 1982; Parker et al., 1988).

137
Numerous studies have examined the influences of psychosocial factors,
including the quality of the marital relationship, maternal education, (Belsky et al.,
1991; Gerner, 1999; Spiker et al., 1993) maternal stress, depression (Carter et al.,
2001; Coyl et al., 2002; Teti et al., 1995; Wijnroks, 1999)and social support (Crnic et
al., 1984; Feiring et al., 1987) on mother-infant interactions. Both research and theory
suggest that these contextual factors are interrelated and together influence maternal
sensitivity and responsiveness to the infant (Belsky et al., 1995). Thus important links
have been established between the quality of the social environment of the premature
infant and child development outcomes (Barnard & Kelly, 1990; Beckwith & Cohen,
1984; Bee et al., 1982; Crnic et al., 1983; Magill-Evans & Harrison, 1999; Morisset et
al., 1990). Generally speaking, positive interactions during the first years of life tend
to be linked with improved subsequent intellectual and language abilities (Barnard,
1996; Barnard et al., 1988).
Researchers have suggested although it may be difficult to alter
socioeconomic or psychosocial variables, parent-infant interaction may be amenable
to change (Barnard, 1996; Koniak-Griffin et al., 1992). Some interventions have been
shown to improve the quality of mother-infant interactions especially in high-risk
dyads (Barnard et al., 1988; Kang et al., 1995; Koniak-Griffin et al., 1992).
Increasing a parent’s sensitivity and responsiveness during frequently occurring
interactions, such as at feeding times, can positively influence the infant’s
responsiveness and enhance the parent-infant relationship (Barnard, 1995). Although
the importance of the early environment to later developmental outcome has been
acknowledged, less is known about which aspects of the environment are the most
salient. Detailed examination of factors which can influence interactions between a
mother and her premature infant is therefore warranted.

138
The purpose of this study was to examine the interaction between mothers and
their preterm infants during a feeding situation and to identify possible factors which
may influence this interaction. The research hypotheses were:
1. There would be a difference in feeding interaction scores between the study
sample and population norms.
2. Less optimal mother-infant interactions would be related to maternal history of
depression, limited formal education, limited support and use of coping
strategies, high levels of stress and depression, measured at P1 and infants
who had low gestational age, birthweight and apgar scores.
3. Less optimal mother-infant interactions would be related to limited support,
high levels of stress and depression, limited use of coping strategies measured
at P2 and infants who were at high medical risk and experienced longer
hospital stays.
METHOD
Data were collected at two points in time. At one month after infant admission
to the neonatal nursery (Phase 1), a mothers’ report of social support, stress,
depressive symptomatology, coping strategies, previous history of depression and
educational level as well as the infants’ gestational age, birthweight and apgar scores
were collected. At three months after infant hospital discharge (Phase 2), mothers’
again reported on social support, stress, depressive symptomatology and coping
strategies and data on the infants’ length of hospitalisation and medical risk were
collected. Mothers who agreed to participate completed a survey questionnaire at
both times and gave consent to a 20 minute videotaped feeding interaction with their
infant at Phase 2. These data were examined to determine if a relationship existed

139
between maternal psychosocial and infant perinatal variables collected at Phase 1 (P1)
and Phase 2 (P2) and mother-infant interaction.
This two-phase prospective follow-up study surveyed all mothers of singleton
premature infants born at less than 32 weeks gestation, without congenital anomalies
and cared for in the neonatal intensive care (NICU) of a local tertiary referral hospital
for at least three weeks. Mothers were required to be able to read and converse in
English and live within a 200km radius of the participating hospital. Sixty-two
mothers participated at P1 and fifty-two mothers participated at P2. Videotapes from
fifty dyads were available for analysis.
Self report data
At P1 and P2 mothers completed a questionnaire which contained the following five
scales.
• The Social Support Interview is designed to assess post-partum social support
(O'Hara, Rehm, & Campbell, 1982, 1983). The SSI asks the participant to
give a rating from no person available (0) and never to always (1-5), for each
potential sources of support (spouse, parent and confidant). Summing across
the questions give a total support score ranging from 0 – 135. A high score
reflects a high level of perceived support.
• The Nurse Parent Support Tool (NPST) (Miles, Carlson, & Brunssen, 1999) is
designed to measure a mother’s perception of nursing support that they have
received during their infant’s hospitalisation. Parents are asked to rate the
amount of nursing support received on a rating scale ranging from “1” almost
never to “5” almost always; higher scores reflecting a greater amount of
perceived support from staff. At P2 participants were asked to reflect on the

140
support they had received when their infant was in hospital in completing the
questionnaire.
• The stress scale of the Depression Anxiety and Stress Scale (DASS)
(Lovibond & Lovibond, 1995) contains 7 questions each scored on a 4-point
scale (0-3), with a total score ranging from 0-21. Higher scores indicate
higher levels of stress.
• The Edinburgh Postpartum Depression Scale (EPDS)(Cox, Holden, &
Sagovsky, 1987) is a well-validated and widely used screening tool for
depression after childbirth. In this study a score of ≥12 was classified as
indicative of depressive symptomatology.
• The Coping Health Inventory for Parents (CHIP) (McCubbin et al., 1983) is a
coping measure used to assess parents’ appraisal of their coping responses
when their infant is seriously ill. The CHIP asks parents to record on a scale
of 0-3, how helpful each of the 45 specific behaviours are in their particular
family situation. Summing across the questions gives a total coping score
from which the three subscales scores are derived. Higher scores indicate
greater satisfaction with coping behaviours.
Demographic data
Maternal demographic data included education and recorded history of
depression and infant data included birthweight (grams), gestational age (weeks) and
total length of hospital stay (LOS).
The infant Neurobiologic Risk Score (NBRS) (Brazy, Eckerman, Oehler,
Goldstein, & O'Rand, 1991) aims to provide early identification of infants who are at
high risk for neurodevelopmental abnormality. Seven high-risk medical conditions are
scored and from this score three neurobiological risk groups are identified: Low risk

141
(0-4), intermediate risk (5-7) and high risk (>8). The principal researcher and the
Director of Neonatology determined the NBRS for participants from the medical
records after infant discharge.
Observational data
The Nursing Child Assessment Feeding Scale (NCAFS) (Barnard, 1978) is a well
validated and frequently used method of assessing maternal infant interactions and has
been used extensively in clinical practice in populations of preterm and very low
birthweight infants during the first year of life (Alfasi & et al., 1985; Farel, Freeman,
Keenan, & Huber, 1991; Harrison & Magill-Evans, 1996; Huber, 1991; Magill-Evans
& Harrison, 1999; Roman et al., 1995; Slater, Naqvi, Andrew, & Haynes, 1987; Tesh
& Holditch-Davis, 1997). During a feeding interaction, the mother’s score is based
on being sensitive to the infant’s cues, alleviating the infant’s distress, and fostering
cognitive and social-emotional development. The infant's score is based on the ability
to provide clear clues and respond to the caregiver’s actions (Barnard, 1996). Mother
and infant scores are combined to give a total score. All 76 items on the NCAFS are
binary (yes/no). The total amount of time taken for the administration of the NCAFS
depends on the length of feeding time (Huber, 1991). A certified NCAFS coder who
had no prior knowledge of the participants, coded the videotaped interaction.
The relevant ethics committees approved the study protocol. Videotapes and
questionnaires were numerically coded to protect patient confidentiality.
RESULTS
The study sample was generally well resourced with a majority of women living with
a supportive spouse or partner, having 12 years education or more, and infants who
were at low risk for neurodevelopmental abnormality. (See Tables 8.1 & 8.2)
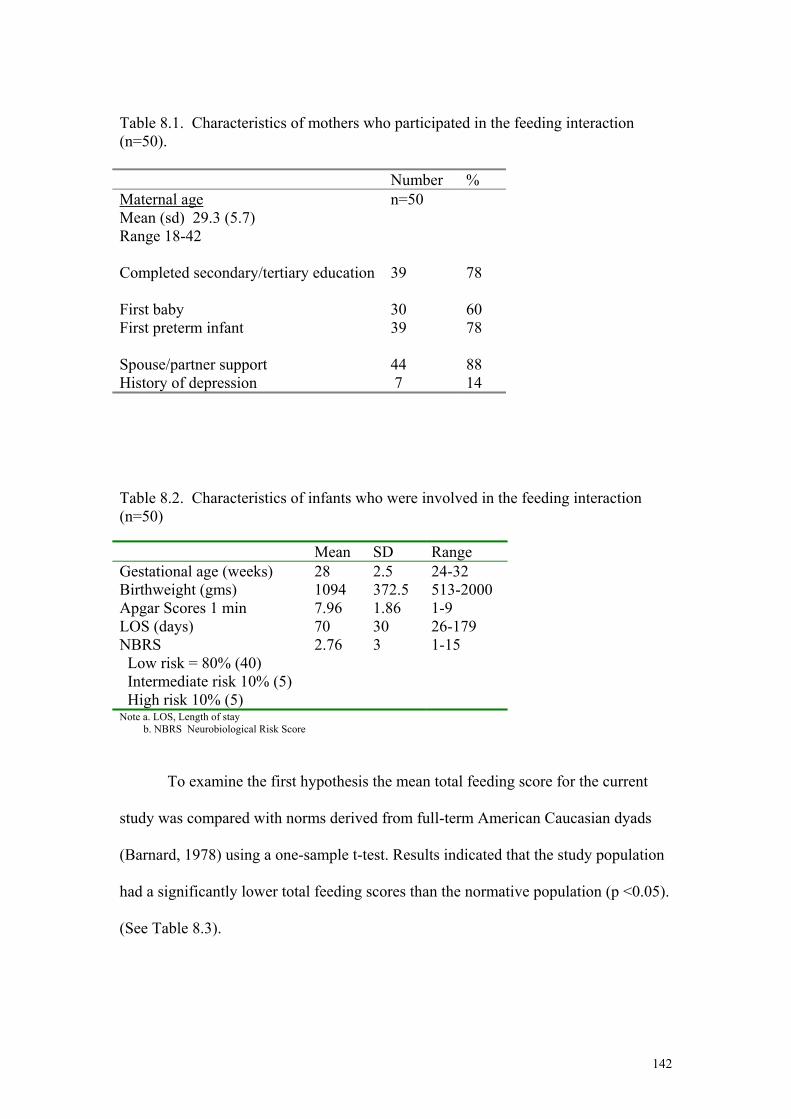
142
Table 8.1. Characteristics of mothers who participated in the feeding interaction (n=50). Number % Maternal age Mean (sd) 29.3 (5.7) Range 18-42
n=50
Completed secondary/tertiary education
39
78
First baby
30
60
First preterm infant 39 78 Spouse/partner support
44
88
History of depression 7 14 Table 8.2. Characteristics of infants who were involved in the feeding interaction (n=50) Mean SD Range Gestational age (weeks) 28 2.5 24-32 Birthweight (gms) 1094 372.5 513-2000 Apgar Scores 1 min 7.96 1.86 1-9 LOS (days) 70 30 26-179 NBRS 2.76 3 1-15 Low risk = 80% (40) Intermediate risk 10% (5) High risk 10% (5) Note a. LOS, Length of stay b. NBRS Neurobiological Risk Score
To examine the first hypothesis the mean total feeding score for the current
study was compared with norms derived from full-term American Caucasian dyads
(Barnard, 1978) using a one-sample t-test. Results indicated that the study population
had a significantly lower total feeding scores than the normative population (p <0.05).
(See Table 8.3).

143
Table 8.3 One Sample T-test and Means, Standard Deviations of Sample (n=50)
Total Scores Mean Std. Dev. t-test p
Total feeding score 61.02 8.58 -2.69 .010 Caregiver total score 42.20 5.37 -1.448 .154 Infant total score 18.82 3.77 -4.073 .000
Infant Subscale Scores
Clarity of Cues 12.50 2.03 -1.496 .141 Responsiveness to Caregiver 6.32 2.13 -5.769 .000
A one-sample t-test was also conducted to examine the two scales, which
comprise the total feeding score, ie the total caregiver and total infant scores (See
Table 8.3). No differences were found between the population means and the mean
caregiver scores for the study mothers however, the study infants had significantly
lower total infant scores than the normative population (p < .001). (See Table 8.3). Of
the two subscales comprising the total infant scores the “responsiveness to caregiver”
score was significantly lower than the population mean but the “clarity of cues” was
not. The study confirmed results from other studies which have indicated that preterm
infants can be less responsive social partners posing a risk to the formation of the
parent-infant relationship (Barnard et al., 1984; Goldberg & DiVitto, 1995).
To examine the second hypothesis, bivariate associations (using Chi square, t-test
and Mann Whitney U test) were conducted between total feeding scores, total
caregiver and total infant scores and all the P1 variables i.e. previous history of
depression, education, nursing and family support, stress, coping, depression scores
and infant gestational age, birthweight and apgar scores. The only significant
correlation was found between infant total scores and the mother’s coping behaviours
at P1 (r= .308, p = 0.029), indicating that there was an association between mothers
who coped better while the infant was in hospital and those who had more responsive

144
infants at three months after infant discharge from hospital. Bivariate associations
were also examined between the P1 coping subscale scores and total feeding and no
significant associations were found.
To examine the third hypothesis, bivariate associations were conducted between
the total feeding score, total caregiver and total infant scores and all P2 variables. No
statistically significant correlations were found between the predictor variables and
total feeding scores. However, there was a trend towards significance between
mothers’ coping behaviours at P2 and total feeding scores (r=.267, p=0.061). To
further examine this trend, the coping scale was divided into its three subscales and
bivariate associations were conducted between the coping subscales and total feeding
scores. The results showed a significant correlation between coping subscale 1 and
total feeding scores (r=.384, p<0.01). This subscale measures family integration,
cooperation and an optimistic definition of the situation and indicates that mothers
who utilised this coping pattern displayed higher feeding scores.
DISCUSSION
The purpose of the study was to test three hypotheses concerning the differences
between the study and population feeding scores and the relationships between
maternal demographic, psychosocial variables and infant variables and mother-infant
interaction at P2. There was some support for the proposal that there would be
differences between the study sample and the normative population. No differences
found between the caregiver feeding scores and the scale norms. This finding is not
surprising as the sample characteristics were similar to the normative population who
consisted of married American Caucasian mothers with an average education level of
13 years or more (Barnard et al., 1989).

145
However a significant difference was found between infant total scores, in
particular the subscale of responsiveness to caregiver. This finding is not unexpected
as the normative sample consisted of full-term infants and prematurity has been
identified as a risk factor associated with low scores on the NCAFS instrument
(Barnard, Booth et al., 1988). These results confirm that premature infants are less
responsive social partners and can have a diminished ability to provide to the parent
cues that promote proximity and contact (Barratt, Roach, & Leavitt, 1992; Goldberg
& DiVitto, 1995). Therefore the responsiveness and skill of the parent may be
particularly important to foster optimal interactions which influence the infant’s
development. One study found that preterm infants whose caregivers had high scores
on responsive, reciprocal, and autonomy-promoting care had improved developmental
scores from 9 months to 5 years. Those caregivers with low scores had a decrease in
performance (Cohen & Parmelee, 1983).
There was only limited support for the proposal that there would be a
relationship between mother-infant interaction scores and P1 variables. The only
significant correlation was maternal coping and infant feeding scores indicating that
mothers who coped better while the infant was in hospital had more responsive infants
at three months after infant discharge. Coping efforts have been described as active or
passive strategies and behaviours designed to maintain or strengthen the family as a
whole, and that serve to protect the family from stressful situations such the birth of a
very premature infant (McCubbin, Thompson, & McCubbin, 1996). It has been
suggested that effective coping strategies remove the source of stress or impact
perceptions of coping ability, while ineffective coping strategies alienate sources of
support, lead to negative self-perceptions and fail to relieve the problem (Wills,
Blechman, & McNamara, 1996). The hospitalisation of an infant brings mothers into

146
frequent contact with nursing staff and other health care professionals whose efforts to
reduce maternal stress and reinforce coping strategies can only promote family
stability, and therefore enhance the infant’s responsiveness and mother-infant
relationship after hospital discharge(McCubbin et al., 1983).
The expected relationship between the P1 variables of educational level,
history of depression, social support, stress and depression, and infants of low
gestational age, birthweight and apgar scores and P2 interaction scores was not found.
Previous studies have shown that maternal education to be a significant predictor of
interaction ratings (Gerner, 1999; Spiker et al., 1993). The fact that this was not
found in the present study was probably due to the fact that almost 80% of
participants had completed at least 12 years of education. Hence unlike studies from
other centres only very few mothers had low levels of education and therefore a
relatively small range in the levels of education achieved by mothers in the present
study.
It is also not surprising that family support was not linked to interactive scores
as at both phases a vast majority of participants reported having a spouse/partner as
well as a friend in whom they could confide and 80% reported having a supportive
mother or father. Researchers have found that parents who have effective social
networks are better adjusted and interact in more optimal ways with their child (Dunst
et al., 1986). In particular, a woman’s satisfaction with the intimate support provided
by her spouse/partner has been shown to have a positive effect on the quality of
mother-infant interaction (Crnic et al., 1984). Some authors have suggested that
through the provision of emotional support, fathers may enable a mother to be a
responsive caregiver to their infant (Magill-Evans & Harrison, 2001).
147
The levels of stress and depression experienced by these mothers while their
infant was in hospital (P1) were also not associated with interaction scores. In other
studies, mothers’ rating of stress in the infant’s 1st year was a significant predictor of
child adjustment at 4 ½ years (Abidin & McGaughey, 1992) and a significant
predictor of preterm children’s socioemotional functioning at 8 years (Magyary et al.,
1992). Likewise maternal depression through its impact on maternal interpersonal
functioning, has been shown to disrupt normal mother-infant engagements and, as a
consequence, impair infant developmental progress (Murray & Cooper, 1997;
NICHD, 1999). However while many of these mothers reported stress and depressive
symptoms during P1, these symptoms did not significantly affect interaction scores at
P2.
There was also very limited support for the expected relationship between P2
variables and P2 interaction scores. The only significant association related to coping
behaviours in that mothers’ who utilised coping strategies directed at maintaining
family integration and cooperation while maintaining a positive outlook on life
displayed higher total feeding scores. This particular coping pattern has also been
found to be important in families who have a chronically ill child (McCubbin, 1984).
The utilisation of effective coping strategies and behaviours is one positive way in
which parents can manage the stress associated with premature birth.
The results also indicated that increased maternal coping was significantly
correlated with lower stress and depression scores as was nursing and family support.
Even though reports of nursing support at P2 were retrospective, mothers had time to
reappraise their hospital experience which was still vividly recalled by all participants.
This finding suggests that nursing and family support may act as a buffer against
maternal stress and depression, enhancing maternal coping efforts.

148
In keeping with findings from other studies the preterm infants in the present
study were generally less responsive than the normative population, although most
were at low risk for developmental delay. However, none of the infant variables were
associated with interaction scores. In a study of fullterm infants at two months of age
infant variables were found to affect quality of the infant’s engagements with the
mother, but to have little effect on the mother’s interactive style (Murray & Cooper,
1997). It has been suggested that mothers’ of preterm infants adopt a compensatory
parenting style in which they adjust their interactions to the infants’ capacity to
respond (Eizirik et al., 1994; Miles & Holditch-Davis, 1995). These compensatory
efforts however sometimes became less successful as the infant got older and the
feeding situation became more demanding (Gerner, 1999). Since mothers in the
present study were seen relatively early in the post-discharge period, the cumulative
strains of parenting a premature infant may not have been evident. Dramatic changes
occur in the infant’s developmental capacities in the first six months of life which
influence both infant behaviour and the behaviour of the caregiving adults (Zeanah et
al., 1997). It may be more important to assess mother-infant interaction later in
development when difficulties may begin to emerge.
CONCLUSIONS
While the infants in this study were shown to be less responsive social partners, the
detrimental effects of adverse psychosocial factors on early mother-infant interaction
were not supported. The reason for this finding may be due to the homogeneity of the
sample and few identified risk factors. Future studies would require a larger and more
diverse sample in order to compare differences between groups.
The results have implications for neonatal nurses who have a pivotal role in
facilitating the early mother-infant relationship while the infant is hospitalised.

149
Nursing efforts to help mothers to cope more effectively during their infant’s
hospitalisation, can promote positive outcomes and result in long- lasting benefits to
the mother-infant relationship even after infant discharge.
150
CHAPTER NINE
DISCUSSION
The general aim of this study was to explore the influence of selected maternal and
infant variables on early mother-infant interaction. The study was undertaken to
increase understanding and knowledge of the factors which promote or inhibit the
development of the early mother-infant relationship in a sample of mothers of very
preterm infants. A specific aim was to examine maternal psychological distress and
correlates of that distress after the birth of a very premature infant and compare
maternal variables across time in hospital and once the infant was discharged home.
Further specific aims were to observe mother-infant interaction during a feeding time
after infant discharge to assess the impact of maternal depression, stress and
associated factors on early mother-infant interaction patterns.
The study contributes to the family stress and coping literature in several
ways. While previous literature has identified that premature birth is a critical event
in the life of a family (Meck et al., 1995; Thompson et al., 1993), little research has
explored specific risk factors in this population. Maternal depressive symptomatology
is one psychosocial risk factor that has been shown to affect how well a woman can
function as well as exerting an influence on mother-infant interaction (Carter et al.,
2001; Coyl et al., 2002; Teti et al., 1995). This study examined this risk across time
and its link to factors which contribute to maternal psychological distress.
More importantly this study investigated whether mother-infant interaction
could be predicted from maternal and infant variables across time. Although the
importance of the early environment to later child developmental outcomes has been
acknowledged (Beckwith, 1984; Crnic et al., 1983; Magill-Evans & Harrison, 1999;
151
Morisset et al., 1990) there is less known about which aspects of the environment are
associated with optimal infant outcomes.
The study was guided by McCubbin’s transactional theory of stress and
coping, otherwise known as the Resiliency Model of Family Stress, Adjustment and
Adaptation (Resiliency Model), (McCubbin, Thompson, & McCubbin, 1996). The
Resiliency Model provides a way of viewing family efforts to adapt to multiple
stressors through the use of various family resources as elements for a coping process
aimed at achieving family balance. This model has proven usefulness in guiding
nursing assessment in family stress situations (Mays, 1988; Robinson, 1997) and was
a constructive framework for exploring the links between the variety of maternal and
infant variables and mother-infant interaction.
This chapter begins with a review of the major findings from the study. The
findings from both Phase 1 and Phase 2 will be reviewed separately, followed by
findings from the observational component of the study. The main conclusions,
together with the theoretical and practical implications of the study are discussed.
Recommendations from the study will be proposed.
Review of Findings
Phase 1
Phase 1 of this study as reported in Chapter 6, explored maternal psychosocial risk
factors at one month following very premature birth and tested the first hypothesis
which stated:
Hypothesis 1. Maternal depressive symptomatology at one month post
premature birth will be related to a previous history of depression, limited formal
education, limited social support, high levels of stress, limited use of coping strategies
and infants who were at low gestational age and birthweight.

152
The birth of a very premature infant is a critical event in the life of a family
(Brooten et al., 1988; Gennaro, 1988; Thompson et al., 1993) and the circumstances
surrounding pregnancy and birth may constitute major risk factors for the
development of postpartum depression. Researchers have suggested that mothers of
preterm infants may be at greater risk of psychological distress than mothers of
fullterm infants (Gennaro, 1988; Pederson et al., 1987). It was therefore hypothesised
that there would be a relationship between mother’s reports of high levels of
depressive symptoms and a number of maternal and infant risk factors. At one month
after birth, sixty-two mothers completed a structured questionnaire including
measures of social support, nurse support, depression, stress, and coping behaviours.
Just over 40% (25/62) of mothers scored > 12 on the Edinburgh Postnatal
Depression Scale, a cut-off used in the present study to indicate the presence of
depressive symptomatology. These results support findings from other studies which
have shown that many mothers of critically ill premature infants suffer depressive
symptoms in the neonatal period (Logsdon & Davis, 1997; Meyer et al., 1995; Miles
et al., 1999c; Younger et al., 1997). While the percentage of mothers reporting
depressive symptoms is higher than the population norms (40%vs 10-15%)(O'Hara &
Swain, 1996) it was not an unexpected result as mothers were in the acute phase of
their infants’ hospitalisation. It is possible that they were still coming to terms with
the disappointment of the early mothering, the ongoing day-to-day medical crises and
the possibility that their infant may have continuing health and/or developmental
problems. Much of the previous research has surveyed mothers either shortly after
admission to the neonatal intensive care unit (NICU) or prior to infant discharge,
which are periods that have been identified as particularly stressful for mothers.
However, in the current study mothers were given time to physically recover from the
153
birth process and surveyed after they had become accustomed to the nursery
environment and their infant’s medical condition had stabilised. It seems that despite
more open access to intensive care units, improved communication and greater
parental participation in infant care, the findings from the current study confirm that
even after a period of adjustment mothers continue to experience distress and
depressive symptoms.
The primary purpose of this phase was to determine which variables were
related to depressive symptoms. The hypothesis was partially supported and there
were three variables that were significantly associated with a mother’s report of
depressive symptomatology. The most significant of these variables was maternal
stress (p < 0.01), followed by maternal education (p < 0.05) and perceptions of
support from nursing staff (p = 0.05).
The technological environment of the NICU and the presence of highly
trained professionals can be stressful and overwhelming for any new parent. In this
study, mothers who reported higher levels of stress were more likely to report higher
levels of depression. Women who experience both symptoms of stress and depression
may find it particularly difficult to establish a satisfying relationship with their infant.
It has been suggested that some of the greatest sources of stress for parents include the
appearance of a fragile, sick infant (Lindsay et al., 1992; Raeside, 1997), fears for
their infant’s survival (Meck et al., 1995), alteration of their parental role and the
separation from their infant brought about by hospitalisation (Hughes et al., 1994;
Moehn & Rossetti, 1996; Shields-Poe & Pinelli, 1997). Stress can also arise from
numerous contexts outside the NICU.
Research has also shown that family crises develop and are resolved over time
and that families are seldom dealing with a single stressor event. McCubbin proposes
154
that researchers and clinicians often interpret family behaviour as a response to a
single stressor event rather than taking into account that families are often
experiencing a ‘pile-up’ of demands (McCubbin et al., 1996). Stress arising from
other life circumstances including unresolved family strains, financial difficulties and
illness can exacerbate the family stress response. Many of the mothers in this study
reported other concurrent life stressors including bereavement, financial and work
related concerns. Therefore future studies could include an assessment of other
stressors to provide a clearer picture of the precipitators of maternal distress.
A mothers’ level of education was also significant in explaining depressive
symptomatology at four weeks postpartum. Women who had completed less than 10
years of education were more likely to be depressed when compared to those
completing secondary or tertiary education. As discussed in Chapter 2, the neonatal
nursery can be a very difficult environment in which to establish effective
communication. Those mothers with a lower level of education may have fewer
resources that enable them to ask questions or establish effective patterns of
communication in the face of high-risk birth and NICU hospitalisation. In addition,
these mothers may have lower expectations of support and information or may have
felt overwhelmed or intimidated within the acute care setting. Even in the presence of
an adequate explanation mothers with fewer educational resources may have
difficulties interpreting the infant care situation, or may not know what questions to
ask. It is also possible that these mothers have limited financial resources with which
to travel to and from hospital or to care for a sick infant at home, creating additional
stress. Mothers with limited formal education who are experiencing elevated
depressive symptoms may require closer monitoring of their adjustment during their
infant’s hospitalisation.
155
Finally, how mothers perceived support received from the nursing staff was
also related to depressive symptoms. Higher reports of nurse support were related to
lower levels of depressive symptoms. Previous research documents the valuable role
of the neonatal nurse in providing information and teaching to mothers of medically
fragile infants. The interpersonal environment created by the nursing staff during an
infant’s hospitalisation defines a large part of the reality for mothers and families
(Miles et al., 1999b). Nurses are the health care professionals with whom the mothers
have most communication. They frequently control contact and interaction with
medically fragile infants and are important sources of information (Brown & Ritchie,
1990; Miles & Frauman, 1993). Therefore the responses of nurses can be critical to
how parents cope with the infant’s illness and hospitalisation and with ongoing health
problems after discharge (Miles et al., 1999b). What is not clear from the study is
whether the presence of depressive symptoms caused mothers to perceive less support
from nurses or whether less nursing support contributed to maternal depression.
Much of the previous research into the role of nursing support is based on
narrative accounts and clinical observations from the health care providers
perspective. There has been a paucity of research which attempts to measure nursing
support and relates it to maternal and infant outcomes in the short and longer term.
The findings from the current study underscore the important role of nursing support
to the psychological wellbeing of mothers of very premature infants. The neonatal
period provides an ideal opportunity to develop an understanding of the impact of
very premature birth on mothers and families. However, there are currently barriers
within the system of neonatal care which impede the ability of nurses to create an
interpersonal environment where professional support can be maximised. These
barriers have been discussed in Chapter 2.

156
Nursing support may be especially important for families of very preterm
infants especially while an infant is hospitalised. One study found that some mothers
of preterm infants rated social support or satisfaction of their social needs as a high
priority in the achievement of their own well-being (Bialoskurski et al., 2002). The
authors suggest that the social circumstances for these mothers may be less than
adequate and therefore their social needs must be met, before their concern for their
infant’s well-being. In this study, perceived support from nursing staff worked as a
family resource factor (Bialoskurski et al., 2002). In another recent study, it was
found that mothers who believed they had positive family-centred relationships with
health care providers in the NICU were more satisfied with the care received and
reported higher levels of psychological well-being (Van Riper, 2001). Further
research into the relationship between maternal well-being and satisfaction with
health care provider role is warranted.
The variables that were not associated with mother’s depressive symptoms
during infant hospitalisation included: family support; coping strategies; previous
history of depression; and measures of infant status (birthweight and gestational age).
A majority of mothers in this study not only reported having a supportive
spouse/partner in whom they could rely on for material help and emotional support
but also high levels of close family support. In one study, mothers who reported
receiving high levels of support from their partner believed that premature birth was
associated with less change in the family and family functioning (O'Brien et al.,1999).
This finding is similar to other studies which have found the baby’s father as a vital
source of support (Affleck et al., 1991; Miles et al., 1996). Spousal support has been
reported to be significantly related to new mothers’ positive emotional states (Crnic et
al., 1983).
157
There were also relatively small numbers of mothers who reported a previous
episode of postpartum depression (10/62) which may explain the lack of association
with mothers’ earlier depressive symptoms. The degree of prematurity and
birthweight of the infants were also unrelated to maternal depressive symptoms. All
infants in the study were born at less than 32 weeks gestation, so they were a fairly
homogenous group. Other maternal variables including age and parity could have
been examined as it might be expected that younger mothers having their first baby
could be more stressed or depressed and cope less effectively than older, more
experienced mothers. Additionally, a previous history of depression may have
predisposed mothers to score more highly on all of the assessment scales. However,
due to the small sample size and the majority of mothers being primiparas with mean
age of 28 and only 16% who had a previous history of depression, this analysis was
not possible.
Phase 2
The results from the second phase of the study are discussed in Chapter 7.
Ten mothers who participated at Phase 1 were lost through attrition and the remaining
fifty-two mothers were visited in their homes at three months after their infant was
discharged home. These mothers were asked to complete the same questionnaire they
had completed at Phase 1.
The study firstly compared the levels of depression across time and found that
the majority of mothers were less depressed once at home with their infant. This
finding supports results from some studies (Brooten et al., 1988; Singer et al., 1999)
but not others where depressive symptoms in mothers of preterm infants have
continued to be elevated after infant discharge (Miles et al., 1999c; O'Brien et al.,
1999; Thompson et al., 1993). In the present study, just over 15% of the sample

158
(8/52) was depressed at both phases of the study and one mother who was not
depressed at Phase 1 became depressed at Phase 2. There appears to be little
consensus in the literature about the course of depressive symptoms in mothers of
premature infants and which factors are related to that distress.
This study also compared levels of stress, coping and family support over time
and found that once at home with their infant, mothers generally reported less stress,
increased coping strategies and continued high levels of family support. It is
generally agreed that postpartum depression does not develop as a result of one risk
factor (eg stressful life event such as preterm birth) but as a consequence of a complex
interplay of biological and psychosocial risk factors (Cooper & Murray, 1998;
O'Hara, 1997). Two known factors which increase a woman’s vulnerability to
postpartum depression following full-term birth include a poor marital relationship
(Hickey et al., 1997; McGill et al., 1995; Zelkowitz & Milet, 1995) and a lack of
perceived social support from her partner and parents (Campbell et al., 1992; O'Hara
et al., 1983; Watson et al., 1984). Since the majority of mothers in the present study
reported having a supportive partner and high levels of family support, these factors
may have provided protection for the mothers’ psychological wellbeing. Studies in
preterm populations have found that women who reported higher levels of partner and
family support also reported lower symptoms of depression (O'Brien et al., 1999;
Thompson et al., 1993). However one study suggested that a mothers’ report of
depression was lowest immediately after infant discharge suggesting a ‘honeymoon’
period (O'Brien et al., 1999). The infant’s homecoming relieves the stress associated
with travel to hospital and coping with an unfamiliar hospital environment. The
reality of caring for a medically fragile infant at home brings a different kind of stress
that is not immediately apparent. The authors suggested that professionals may need
159
to keep in contact with family over several months to obtain an accurate picture of a
families ability to cope with the full range of stresses associated with caring for a
premature infant (O'Brien et al., 1999).
The primary purpose of the Phase 2 follow-up was to test the second and third
hypotheses. The second hypothesis explored the possibility of being able to predict
depressive symptomatology at Phase 2 from variables measured at Phase 1. The third
hypothesis examined the relationship between maternal and infant variables measured
at Phase 2 and Phase 2 depressive symptomatology. The results of these hypotheses
will be discussed separately. The second hypothesis stated that:
Hypothesis 2: Elevated levels of maternal depression at three months after
infant hospital discharge will be related to a previous history of depression and
limited formal education; limited social support (from family and/or nursing staff);
limited use of coping strategies and high levels of stress and depressive symptoms
during P1; and having infants of low gestational age, birthweight and apgar scores.
This hypothesis was not generally supported. Apart from Phase 1 depressive
symptoms, all other Phase 1 variables were not significantly related to depressive
symptoms at Phase 2. These results are not totally unexpected as a previous history of
depression, social support, coping and infant gestational age, birthweight and apgar
scores were not related to Phase 1 depressive symptoms. The possible reasons for the
lack of associations have been discussed previously.
However the variables of maternal stress, education and perceptions of nursing
support which were previously significant in explaining depression scores at 4 weeks
postpartum did not continue to be related to Phase 2 depression. This may have been
due to the finding that there were significantly fewer mothers who reported depressive
symptoms at Phase 2. Once at home with their infants, women generally described

160
being well supported by family and friends and were no longer having to cope with
the various stressors related to the infant’s hospitalisation.
Depression scores at Phase 1 were related to Phase 2 depression. This finding
is supported by results from another study that found that depression at a four week
infant follow-up appointment was significantly related to depression reported by
mothers during infant hospitalisation (Logsdon & Davis, 1997). Early identification
may assist in preventing the depressive episode from continuing with the use of timely
and appropriate therapeutic interventions (Field, 1998) while the infant is still
hospitalised. Unlike mothers of full-term infants who have short hospital stays, there
are more opportunities to screen mothers of preterm infants for postpartum
depression. These mothers remain in constant contact with the health care system
until their infant is discharged. For some families with extremely premature infants
(≤ 28 weeks) this period may be as long as three to four months. Considering the
profound impact that continuing depression has on the woman and the mother-infant
relationship, it is important to recognise and treat symptoms before they become more
serious. However follow-up services are generally not offered to families but to
infants only. Even then, these follow-up services for infants are often fragmentary
and episodic (Gennaro et al., 1991) and based strictly on infant medical criteria.
Hypothesis 3: After controlling for P1 depression, elevated levels of
depressive symptoms at P2 will be related to limited social support, limited use of
coping strategies, high levels of stress during P2 and having infants who had long
hospital stays and high medical risk.
The third hypothesis was also not generally supported. Apart from Phase 2
stress, all other Phase 2 variables were not significantly related to depressive
symptoms at Phase 2. The results showed that mothers consistently reported high

161
levels of support at both times and increased satisfaction with coping strategies at
Phase 2. It is therefore not surprising that these variables were not significant.
Interestingly, the infant’s prematurity characteristics and neurobiological risk
score were not associated with the mother’s depressive symptoms at either phase.
Other studies have also found that family dynamics are more important in the initial
stages of adaptation at home than the degree of prematurity or birthweight (O'Brien et
al., 1999; Thompson et al., 1993). It has been suggested that the lack of clear and
direct links between the degree of infant illness and measures of family adaptation
may be attributable to a number of factors. Firstly the measures of the severity of
illness are not tied to specific tasks and demands to which families must respond (e.g.
oxygen needs or treatment regimes) and therefore may not adequately reflect the
extent of daily stress experienced by families (Drotar, 1992; Quittner et al., 1992).
Secondly, a family’s perception of illness severity compared to objective medical
indicators have shown different relationships to psychological distress (Quittner &
DiGirolamo, 1998). Some authors have suggested that objective criteria may be less
important than personal perceptions of illness which may mediate adjustment (Drotar
& Bush, 1985). The notion that an individual’s perceptions of the stressor event is
strongly related to psychological distress is one of the central tenants of stress and
coping theory (Lazarus & Folkman, 1984).
Although the infants in the present study were all born very prematurely, the
majority had few serious medical complications and were at low risk of
developmental delay. This may have resulted in fewer infant care demands once at
home. This finding that infant illness status was not related to maternal depression
supports results from other studies (Gennaro et al., 1990; O'Brien et al., 1999; Spear et

162
al., 2002; Thompson et al., 1993) but not from others (Bennett & Slade, 1991;
Blumberg, 1980).
Maternal stress scores at Phase 2 were significant in predicting Phase 2
depressive symptoms. While the infant’s hospitalisation is stressful for mothers, the
transition home does not always mean the infant’s problems are resolved but may
introduce new challenges to parents’ adaptation and coping ability (Affleck et al.,
1991). Going home with their baby is often eagerly anticipated but can be stressful
for parents who will assume full responsibility for an infant who for weeks or months
has been regarded as medically fragile and in the care of experts (Easterbrooks, 1988;
Miles & Holditch-Davis, 1997). In the weeks following discharge parents continue
to feel anxious about infant care issues, how to recognise infant illness, understanding
growth and development and fearing for their infant whom they still view as sick
(Brooten et al., 1989; Kenner & Lott, 1990). In many cases parents must give care to
a sick infant whose needs are beyond the needs of a normally developing infant
(Patterson et al., 1994; Sterling et al., 1996). In addition, many premature infants
have behavioural and temperamental characteristics that make them less responsive
and more difficult to parent in the first year (Goldberg & DiVitto, 1995). In one
study, mothers reported stress arising from conflict over differing perceptions of
infant care and developmental progress held by extended family members and friends
(Affleck et al., 1991).
It has been reported that for mothers of very low birth weight, premature
infants, elevated maternal stress levels can continue in the longer term, for up to four
years after birth (Singer et al., 1999; Wereszczak et al., 1997), even for well-educated
nuclear families (Cronin et al., 1995).

163
Observational Study
The results from the Phase 2 observational component of the study are
reported in Chapter 8. Researchers have acknowledged that parent and infant
characteristics are both important to the formation of relationships (Sameroff, 1993)
and that mother-infant relationships develop in a reciprocal, bi-directional manner
over time (Sameroff & Fiese, 2000). This exploratory study examined the
relationship between Phase 1 and Phase 2 maternal and infant variables on mother-
infant interaction at Phase 2. Based on the findings of previous investigations it was
expected that the additional stress of maternal depression coupled with the difficulty
in caring for a premature infant could exaggerate interaction difficulties.
Fifty-one mothers out of fifty-two agreed to be videotaped with their infant
during a feeding time using the Nursing Child Assessment Feeding Scale (NCAFS)
(Barnard et al., 1989). One mother declined videotaping and one of the videotapes
was unable to be coded due to the poor sound quality. Fifty videotaped feeding
interactions comprised the observational sample.
The primary purpose of the observational component at Phase 2 was to test the
fourth, fifth and sixth hypotheses. The fourth hypothesis examined the differences in
the feeding scores between the current study sample and population norms. The fifth
and sixth hypotheses examined the relationship between maternal and infant variables
at Phase 1 and Phase 2 and mother-infant interaction scores.
Hypothesis 4: There will be a difference in feeding interaction scores between
the study sample and population norms.
The results demonstrated some support for this hypothesis. There was no
significant difference found between the caregiver interaction scores for the study

164
sample and the population norms. This may have been because the characteristics of
the mothers in the study closely resembled the population norms as described by
Barnard (Barnard et al., 1989). However there was a significant difference found
between infant interaction scores. This finding was not surprising since the
population norms were calculated from fullterm infants and the study sample was
very preterm infants. The results do confirm that preterm infants can be less
responsive social partners (Eckerman et al., 1999; Goldberg & DiVitto, 1995) and
therefore the burden of interaction shifts to the mother. The mother’s sensitivity and
responsiveness may be particularly important for the preterm infant, to foster optimal
interactions which contribute to the infant’s long-term development. Factors that may
adversely affect a mother’s ability to be sensitive and responsive to her infant, such as
maternal depression, can pose a threat to the mother-infant relationship and infant
developmental outcomes (Eckerman et al., 1999; Field, 1982; Goldberg & DiVitto,
1995). The final two hypotheses tested the relationship between Phase 1 and Phase 2
maternal and infant risk factors and mother-infant interaction.
Hypothesis 5: Less optimal mother-infant interactions will be related to: a
previous history of depression and limited formal education; limited support and
use of coping strategies and high levels of stress and depression during P1 and
infants who had lower gestational age, birthweight and apgar scores.
The results confirmed very limited support for the proposal that there would
be a relationship between mother-infant interaction scores and Phase 1 variables.
While there were no significant correlations among the coping subscales, there was a
significant correlation between total coping scores and infant feeding scores. This
result indicated that mothers who coped better while the infant was in hospital had
more responsive infants at three months after infant discharge. Coping strategies are
165
designed to maintain or strengthen the family as a whole and serve to protect the
family from stressful situations such the birth of a very premature infant (McCubbin
et al., 1996). Neonatal nurses have frequent contact with mothers of hospitalised
premature infants. Therefore nursing efforts which are aimed to reduce maternal
stress and reinforce coping strategies can not only promote family stability, but also
enhance the infant’s responsiveness and mother-infant relationship after hospital
discharge (McCubbin et al., 1983).
The expected relationship between the Phase 1 variables of educational level,
history of depression, social support, stress and depression, and infants of low
gestational age, birthweight and apgar scores and Phase 2 interaction scores was not
demonstrated in this research. While maternal education has been shown to
significantly predict interaction ratings in other studies (Gerner, 1999; Spiker et al.,
1993), there was a relatively small range in the levels of education, with a majority of
participants having had 12 years of education or more.
Similarly, study mothers generally reported high levels of spousal, family and
nurse support. Researchers have found that parents who have effective social
networks are better adjusted and interact in more optimal ways with their child (Dunst
et al., 1986). In particular, a woman’s satisfaction with the intimate support provided
by her spouse/partner has been shown to have a positive effect on the quality of
mother-infant interaction (Crnic et al., 1984). Some authors have suggested that
through the provision of emotional support, fathers may enable a mother to be a
responsive caregiver to their infant (Magill-Evans & Harrison, 2001).
The levels of stress and depression experienced by these mothers while their
infant was in hospital (P1) were also not associated with interaction scores. Stress and
depression can adversely impact maternal interpersonal functioning and disrupt
166
normal mother-infant engagements (Murray & Cooper, 1997; NICHD, 1999).
However while many of these mothers reported stress and depressive symptoms
during P1, these symptoms did not significantly influence interaction scores at P2. A
possible reason for this finding is that depressive symptoms did not persist over time
for many mothers. In addition a majority of mothers reported being well supported by
their spouse/partner, close family and nursing staff both during the infant’s hospital
stay and at home. It has been reported that there is no single cause in the development
of postpartum depression (such as exposure to a critical life event) but that it develops
as a consequence of a complex interplay of biological and psychosocial risk factors
(Cooper & Murray, 1998; O'Hara, 1997). Limited social support and marital stress
have been identified as two risk factors in the development and persistence of
postpartum depression (Beck, 1996). These risk factors were not present for a
majority of mothers in the current study.
Hypothesis 6: Less optimal mother-infant interactions will be related to: limited
support and use of coping strategies and high levels of stress and depressive
symptoms at P2, and having infants who had high medical risk and long hospital
stays.
The results indicated limited support for the hypothesis of a relationship
between Phase 2 variables and mother-infant interaction. The expected relationship
between interaction scores and mothers who reported limited support, stress and
depression at Phase 2 with infants who were hospitalised longer and at high-risk of
developmental delay was not found. This lack of association can be explained by the
results demonstrated that generally, mothers who reported high levels of social
support were generally less stressed or depressed and had infants’ who were at a low
risk for developmental delay.

167
As with the results from the previous hypothesis, there was a similar trend
with P2 maternal coping strategies and while the total scores approached statistical
significance, one of the coping subscales was significantly related to total feeding
scores. This subscale measured coping strategies directed at maintaining family
integration and cooperation while maintaining positive outlook on life. Mothers who
reported greater use of coping strategies displayed higher total feeding scores.
Strengthening or reinforcing parental coping has been suggested as a viable target for
health care professionals who are seeking to facilitate family adaptation to stress
(McCubbin et al., 1983).
Summary of Findings
Overall, the findings indicate that after a period of adjustment, even the most well
resourced mothers may suffer stress and depressive symptoms during their premature
infants’ hospitalisation. These results may not be unexpected as mothers continue to
adjust to the reality of their infant’s medical crisis. However, the finding that mothers
who experience stress, have the least education, and who perceive low levels of
nursing support were more likely to be depressed, has clear implications for nursing
practice. These implications will be discussed later in the chapter.
Once at home with their infants, mothers reported being less depressed
although the percentage of mothers who reported depressive symptoms was similar to
the population prevalence of postnatal depression. The finding that all except one of
these mothers were also depressed at Phase 1 is clinically significant. The potential
for being able to predict post-discharge depressive symptoms from depressive
symptoms occurring during the infants hospital stay raises the issue of screening
mothers early in the neonatal period. Once identified, postpartum depression is
amenable to treatment, which can alleviate months of suffering for mothers and
168
reduce potentially adverse outcomes for the mother, family and infant. The neonatal
period affords a crucial opportunity to identify mothers who are most at risk of
postpartum depression while they have extended postpartum contact with the health
care system.
The observational component of the study confirmed that premature infants
are less responsive social partners and so the burden of maintaining the interactive
relationship is shifted to the mother. Many factors can adversely affect a mother’s
responsiveness to her infant and therefore jeopardise the mother-infant relationship.
This exploratory study examined the influence of maternal depression and other
factors measured during Phase 1 and Phase 2 on mother-infant interaction scores.
Findings indicated that mothers who positively appraised their coping efforts while
their infant was hospitalised had more responsive infants at three months. Once at
home, mothers who used coping strategies directed at maintaining family integration
while maintaining a positive outlook on life displayed higher total feeding scores.
Nursing efforts to help mothers cope more effectively during their infant’s
hospitalisation, can promote positive outcomes and result in long- lasting benefits to
the mother-infant relationship even after infant discharge.
The negative influence of maternal depression on mother-infant interaction
was not conclusively demonstrated in this study. This finding may be due to the
relatively small numbers of women who were depressed (9 out of 50 subjects at Phase
2). A larger, more diverse sample would increase the likelihood of detecting effects
that are truly present. In addition, the majority of mothers were reasonably well
educated, felt supported by their partner and family and had infants who were at low
risk for developmental delay. Research on how risk factors affect infant development
suggests that the transmission of risk is neither specific nor linear. Multiple risks

169
from different domains (e.g. biological., psychological., or social) may occur
simultaneously and may in turn be exacerbated or ameliorated by the infant’s family
system (Seifer, 1995). Thus, the total number of risk conditions affecting an infant
may be more predictive of various outcomes than exposure to any single risk factor
(Sameroff et al., 1998; Weisglas-Kuperus et al., 1993; Zeanah et al., 1997).
Limitations of the Study
A number of limitations reduce the generalisability of the findings in the
current study. The study was conducted from a consecutive sample of mothers and
infants from one neonatal tertiary referral centre in a major metropolitan area. It has
been reported that large numbers of premature infants are born into poverty with
accompanying social and health problems (Gennaro, 1996). However, the mothers in
the study were generally well educated, and felt supported by their spouse/partner and
family. The sample selection also excluded non-English speaking mothers, those
who were less than 18 years of age and mother’s of multiple births and infants’ with
congenital anomalies. Therefore, the characteristics of the mothers in this study
sample may not adequately represent the total population of mothers of very
premature infants.
In addition, a majority of infants in the study were assessed as being at low
risk of developmental abnormalities. The literature documents that very premature
infants are at a higher risk of major handicapping conditions which has lead to an
increase in the absolute numbers of children with disabilities (Lorenz et al., 1998).
Other studies have documented differences in feeding interactions and outcome for
premature infants with and without medical risk factors. It was reported that mothers
of infants with risk factors were more likely to report clinically significant symptoms
of depression (Singer et al., 1996, 1997). The characteristics of the infants in the

170
study may therefore not adequately represent the total population of very premature
infants which also limits the generalisablity of the findings.
While sample size for the major outcome variable of Phase 2, mother-infant
interaction, did not reach the target sample of 90, other research studies which have
observed interaction between a mother and her preterm infant in the first 12 months of
life have reported similar sample sizes ranging from 46-52 dyads (Coyl et al., 2002;
Ruttenberg et al., 1997; Wijnroks, 1999; Zahr, 1991). Therefore, with respect to
sample size, it was considered appropriate to compare findings from this study to
other studies of mother-infant dyads. Nevertheless the potential for Type II error is
greater when the sample size is less than that the number originally required to show a
statistically significant effect. Therefore this study was limited by the small sample
size and the low power to detect a statistically significant relationship between the
variables.
Another limitation included the study’s reliance on self-report data and the
correlational nature of the study which does not permit any causative links to be
identified. In particular, the EPDS is a self-report questionnaire that gives an estimate
of psychological disturbance, not a definitive diagnosis of depression. The diagnostic
psychiatric interview using the DSM IV criteria is the generally accepted gold
standard for the definition and diagnosis of a case of major depression (Cox et al.
1987; Boyce et al. 1993). The use of questionnaires to define ‘cases’ is clearly a crude
method and an inadequate substitute for a clinical interview. However the EPDS has
been demonstrated to be a valid indicator of cases of major depression (Cooper &
Murray, 1995; Cox et al., 1987). Although lacking the rigour of a clinical diagnosis,
self-report measures can be an economical and effective way of tracking dysphoria in
171
large samples of postnatal women. Future studies need to include a diagnostic
interview using the DSM IV criteria to confirm a diagnosis of depression.
Information relating to a history of depression was collected from the
woman’s pregnancy health record. However the study was limited because women
are not routinely screened antenatally for symptoms of depression and therefore no
baseline data was available to give an indication of a woman’s psychological
wellbeing prior to their infant’s birth. Although a majority of the study participants
were primiparas (55%), the researcher did not establish whether participants were
currently receiving treatment for depression at Phase 1. Understanding the mothers’
treatment status may have influenced the interpretation of both Phase 1 and Phase 2
findings.
In addition, the researcher referred all mothers with scores > 12 on the
Edinburgh Postnatal Depression scale to the NICU social worker. The researcher did
not return to ask the social worker about any support or counselling interventions that
may have been offered to the mother or ask mothers at Phase 2 if they had received
treatment for depression. Therefore the study was not able to examine the influence
of these interventions on P2 depressive symptomatology and the significant reduction
in the percentage of mothers reporting significant depressive symptomatology at P2.
McCubbin (1993) has suggested that families are seldom dealing with a single
illness-induced crisis but can experience a pile-up of demands and may be trying to
manage stress in other aspects of their lives. These other life stressors may also exert
an influence on mother-infant interaction. The Family Inventory of Life Events
(FILE) (McCubbin et al., 1996) is a 71-item questionnaire which assesses other life
stressors experienced by families. This family stress index was not included in the
study because of concerns about the length of time it would take mothers to complete

172
the questionnaire. Therefore the results are limited to the contribution of the selected
variables chosen for the study (i.e. symptoms of stress and depression, perceptions of
support, satisfaction with coping strategies and objective measures of infant status).
It is also acknowledged that the study was not able to include the spouse or
other family members but explored family adaptation to very premature birth through
the mother’s perception only. Fathers also contribute to infant development both
directly through caregiving and indirectly through the provision of practical and
emotional support to the infant’s mother. Some studies have suggested that
non-depressed fathers may buffer the effects of maternal depression on infant
interaction through the provision of optimal stimulation (Field, 1998; Hossain et al.,
1994). Future studies need to consider the contribution of fathers and other close
family members to infant developmental outcomes.
Another limit to the generalisability of findings is that the interaction data are
based on one single feeding interaction at three months after infant discharge. Since
this was relatively early in the post-discharge period, the cumulative strains of
parenting a premature infant may not have been evident. Dramatic changes occur in
the infant’s developmental capacities in the first six months of life which influence
both infant behaviour and the behaviour of the caregiving adults (Zeanah et al., 1997).
In one study, differences were found in a feeding interaction at 6 months of age, but
not at 3 months, between fullterm and preterm infants. These results indicated that
mothers of preterm infants related more poorly to their infants (Gerner, 1999). These
findings suggest that difficulties with preterm infants and interaction may emerge over
time and it may be important to assess interaction later in development. However, the
current study was limited by the restricted timeframe in which interaction assessments
could be made.
173
While the limitations of the study are acknowledged, they do not detract from
the significance of the findings and the implications for practice and research.
Implications for Nursing Practice
The greatest value of this study is in the potential ability of the results to be used in
clinical services and intervention programs provided to mothers of very preterm
infants. It has been suggested that the major goal for neonatal nursing is the
promotion of parental involvement in the care of the infant (Hurst, 1993) and the
provision of quality care to facilitate maternal and infant well-being (Bialoskurski et
al., 2002). It has also been suggested that nurses have a major role in helping to
reduce maternal distress (Holditch-Davis & Miles, 2000) and that psychosocial
assessment would help to identify mothers who may require intense counseling to
help reduce their distress (Doering et al., 1999; Heimer & Staffen, 1998).
The findings from the current study indicated that a high percentage of
mothers reported depressive symptomatology at one month postnatally. Diagnostic
criteria for postpartum depression include onset of symptoms within four weeks
postpartum (American Psychological Association, 1994) although gradual onset of
symptoms can mean that it is not easily distinguishable from the fatigue and
emotional lability experienced by most mothers in the first days and weeks after the
birth (Holden, 1994). In particular, stress, anxiety and depressive symptoms may be
seen as an expected response when an infant is born very premature and therefore
may not be understood in terms of a possible mood disorder.
While it is clear that not all women will go on to develop postnatal depression,
it can be difficult to diagnose and requires an expert understanding of the risk factors,
symptoms and presentation of the disorder. Research has shown that women tend not
to seek help for their depression (MacLennan et al., 1996) and despite frequent

174
contacts with health care providers, nearly half of the women suffering postpartum
depression are not identified by their clinicians (Hearn et al., 1998). Evidence is
mounting that mothers’ of premature infants experience higher rates of postpartum
depression than mothers of fullterm infants (e.g. Younger et al., 1997). Neonatal
nurses have a unique relationship with mother’s of preterm infants and are ideally
placed to identify symptoms though screening and the provision of appropriate
referral and support. The availability of reliable screening tools such as the
Edinburgh Postnatal Depression Scale (EPDS) (Cox et al., 1987) will assist nurses in
the recognition of mothers in need of referral to a mental health professional.
However, in a study exploring mothers with postnatal depression, perceptions of
nurses caring for those mothers revealed that an essential component of caring was
nurses having sufficient knowledge about this mood disorder to make a quick, correct
working diagnosis and to make appropriate referrals (Beck, 1995).
The immediate, impromptu availability of emotional and practical nursing
support seems to be especially important in the neonatal context where mothers will
spend many hours over an extended period in close proximity to nursing staff.
Neonatal nurses are the health professionals with whom the mothers and family have
the most contact and nursing support may be critical to a mother’s emotional well-
being. This support provided by nurses may be even more important to a mother
while her infant is hospitalised, as family and friends may also have difficulty
adjusting to the acute care situation and may feel helpless and unsure of their roles.
Perceived and actual availability of support can also influence mothers’ coping
efforts by reducing the impact of stress to a manageable level (Lau & Morse, 2001;
McCubbin et al., 1996). Studies have reported that one of the ways in which parents
cope with the stress of NICU hospitalisation is by seeking information about their

175
infant’s progress from nursing and medical staff which helps by reducing the
uncertainty (Hughes et al., 1994; Seideman et al., 1997). Coping is not a static
process but dynamic one that is constantly changing (Lau & Morse, 2001). Stress and
depressive symptoms can also impair a mother’s concentration, cognitive processing
and retention of information (O’Hara, 1996), so that it is important for nurses to
ensure that opportunities are provided for information to be discussed again and
talked through more frequently so that parents can extract information and clarify
misunderstandings when they are ready to hear and understand. This may be
particularly important for mothers with low education, who may not know what
questions to ask or be reluctant to voice their concerns. To do this effectively, nurses
must be attuned to the individual differences in mothers’ perceptions of events and
coping styles. Nurses can assist mothers to develop appropriate and useful coping
skills which can reduce highly negative emotions to manageable levels. The benefits
to the mother can be immediate through the reduction of stress and depressive
symptoms and longer term through improved mother-infant interaction after
discharge. Additionally, the very preterm infant is a less responsive social partner
during mother-infant interactions. Nurses can provide timely interventions to prevent
inappropriate mother-infant interaction and assist mothers to understand their infant’s
cues and unique attributes.
In the light of evidence that emphasises the fundamental role of the mother to
the optimal developmental outcome of the premature infant, it is imperative that the
role of the neonatal nurse moves beyond the infant to incorporate care of both the
mother and infant. Further research is needed into the unique role of neonatal nurses
involved with families during times of crisis and the influence that nursing support
has on a mother’s coping efforts and adaptational outcome.

176
Implications for Further Research
The present study was conducted in a setting where a majority of mothers
were well educated and supported and had infants who were at low risk of
developmental delay. Since the incidence of preterm birth is higher in lower socio-
economic groups where large numbers of premature infants are born into poverty with
the accompanying health and social problems (Gennaro, 1996), further investigation
is required into the needs of these mothers in NICU and beyond. The majority of
infants in the study did not experience significant medical complications which would
place them at high risk of developmental delay. Future studies need to include equal
numbers of infants with and without medical risk factors to investigate the importance
of medical complications to a mother’s psychological adjustment and to compare the
differences in interaction between groups.
It is also acknowledged that fathers have an equally important role not only to
the developmental outcomes for premature infants but through supporting mothers
caring for their infants. To date, there has been limited investigation into the effects
of very premature birth on fathers, although studies have reported that both mothers
and fathers are equally distressed by differing aspects of the infant’s hospitalisation
(Hughes & McCollum, 1994; Miles, Funk, & Kasper, 1992). Since there appears to
be no uniform response, consideration needs to be given to the specific needs of both
mothers and fathers and the family as a whole when trying to help parents cope with
the NICU experience. The burden of care may also be greater in other at-risk groups
including non-English speaking and adolescent mothers, and mothers of multiple
births or with infants who have congenital anomalies. Therefore longitudinal studies
using larger and more diverse samples including mothers and fathers and infants at
risk would enable examination of parent-infant interaction over the course of the
177
developing relationship. These studies would also need to consider the influence of
other variables such as concurrent life events which may also influence a mother’s
responsiveness to her premature infant.
The findings also indicate that well resourced mothers can suffer stress and
depressive symptoms even after their infant’s medical condition has stabilised. This
highlights the crisis nature of very premature birth which may precipitate the
development of postnatal depression in vulnerable women. According to the
population prevalence, it is safe to assume that at least 10-15% of mothers of very
premature infants will experience an episode of postnatal depression. While
screening tools such as the EPDS are valuable to give an estimate of psychological
disturbance, these tools do not provide a definitive diagnosis of depression. Future
studies need to consider establishing a definitive diagnosis of depression through a
diagnostic interview with a psychologist or psychiatrist.
One of the most critical steps in early detection, support, and referral of this
devastating disorder is identifying reliable predictors of postpartum depression. In the
current study risk factors included stress, low education and nursing support.
Researchers have developed inventories of predictors of postpartum depression (Beck,
2002; Cooper et al., 1996). The recently revised Postpartum Depression Predictors
Inventory (PDPI) (Beck, 1998, 2002), can be used as a screening tool in a guided
interview format with a clinician to help evaluate the pre-existing risks for postpartum
depression. Future research is needed to establish the value of utilizing these
inventories in clinical practice to identify mothers at risk. Once identified, these
individual vulnerabilities or risk factors may be amenable to change and benefit from
psychosocial intervention.

178
Very few studies have targeted interventions which are individualised
according to the needs of the family. One such study testing an individualised
family-based intervention during hospitalisation and transition home reported a
reduction in maternal stress and depression and improved mother-infant interactions
in the experimental group (Meyer et al. 1994). Therefore, interventions that
specifically aim to reduce the negative effects of postpartum maternal stress and
depressive symptoms in mothers of very preterm infants need to be developed and
incorporated into practice.
Since infant prematurity and the neurobiological risk score were not related to
a mother’s depressive symptoms or interactive scores, future studies may need to
incorporate measures of a mother’s perception of her infant’s illness rather than
relying on purely objective measures of the infant’s medical condition. As previously
discussed, objective measures of infant illness are not tied to specific tasks and
demands to which families must respond and therefore may not adequately reflect the
extent of daily stress experienced by families (Drotar, 1992; Quittner et al., 1992).
Recommendations
In order to enhance clinical practice and extend further study into families and their
very premature infants, several recommendations are proposed as follows:
1. Future longitudinal studies using a larger and more diverse sample of parents
and infants which focus on parental stress, coping and depressive symptoms
and the impact of these factors on dyadic interaction patterns. These studies
need to also consider the influence of other important factors (e.g. life events
and parental perceptions of the infant’s illness);
2. Future studies to develop and test interventions to reduce maternal stress and
depression and encourage effective maternal coping to be incorporated into

179
neonatal nursing practice, in addition to exploration of the unique role of the
neonatal nurse to maternal well-being and the mother-infant relationship;
3. Introduction of universal screening for postpartum depression in NICU as part
of routine family assessment, followed by a clinical interview to confirm
suspected cases and regular monitoring, treatment and referral as appropriate;
4. Introduction of a system of primary care for neonatal nursing to promote
continuity of care and support between nurses and mothers which can enable
nurses to encourage responsive mother-infant interaction patterns and to assist
mothers to understand and interpret their infant’s behaviour;
5. Education and training for neonatal nurses is required to increase nurses’
knowledge and understanding of postpartum depression and the benefits of
screening and intervention and to enhance neonatal nurses’ counselling skills;
6. Advanced neonatal nursing courses to provide a greater emphasis on maternal
and family responses to the crisis of premature birth.
Conclusion
In this research project, the interaction between a mother and her very
premature infant was examined at three months after infant discharge from NICU to
determine if a relationship existed between maternal and infant data collected at one
month post preterm birth (Phase 1) and three months after infant discharge (Phase 2),
and maternal-infant interaction.
The first research question addressed the factors which were related to
maternal depressive symptomatology at Phase1. The results indicated that mothers
who experienced high levels of stress, who had less than 10 years of education and
perceived low levels of nursing support were more likely to suffer depressive
symptoms at Phase 1.

180
The second research question addressed the relationship between maternal and
infant factors collected at Phase 1 and maternal depressive symptomatology at Phase
2. Depressive symptoms at Phase 1 were significantly related Phase 2 depressive
symptoms.
The third research question addressed the relationship between Phase 2
factors and Phase 2 depressive symptoms. The findings indicated that mothers who
experienced stress once they were at home with their infant were more likely to suffer
depressive symptomatology at Phase 2.
The fourth research question looked for differences between mother-infant
interaction scores between the study sample and the normative population and found
that the very premature infants in the study were less responsive and had statistically
significant lower interaction scores when compared to the population norms.
The fifth research question addressed the relationship between mother-infant
interaction scores and the maternal and infant data collected at P1. A statistically
significant correlation (<0.05) was found between mothers’ coping strategies and
infant feeding scores. Mothers who coped better while their infant was in hospital had
more responsive infants at three months after infant discharge.
The final research question addressed the relationship between mother-infant
interaction scores and the maternal and infant data collected at P2 and found a
statistically significant correlation (p<0.01) between a specific coping subscale and
total feeding scores. Mothers who coped using strategies directed at maintaining
family integration while maintaining a positive outlook on life displayed more
positive feeding interactions with their infant.
This study has demonstrated that the birth and the events surrounding very
premature birth is highly stressful for many mothers, even in the presence of

181
supportive family relationships. The current study also confirmed that stress is
directly related to depressive symptomatology and therefore mothers of very preterm
infants are likely to experience higher rates of postpartum depression. Moreover, the
study established that neonatal nursing staff are not only an important source of
support for mothers but that this support is essential to a mother’s psychological well-
being while their infant is hospitalised. In particular, those mothers who are stressed
with fewer years of education may need additional assistance and support from nurses
as they try to adjust to becoming parents under particularly stressful hospital
situations. Findings also indicated that adaptational processes during the NICU
experience (e.g., coping strategies) might influence the developing mother-infant
interaction after discharge. The very preterm infants in the study were found to be
significantly less responsive during mother-infant interaction when compared to the
full-term population norms. Nursing efforts directed to reduce maternal stress and
depressive symptoms and to assist mothers to cope more effectively while the infant is
hospitalised are likely to enhance the mother-infant relationship after discharge.
Finally, the rates of depressive symptomatology in mothers after discharge were
similar to the population prevalence of depression. One of the most compelling
reasons to screen for depression amongst mothers of very preterm infants is that early
identification and treatment of postpartum depression can result in a shorter duration
of the depressive episode and reduce the likelihood of adverse outcomes for both the
infant and family.
This study has contributed to family centered research by highlighting the
importance of early postnatal experiences to the longer-term psychological health of
mothers and to the mother-infant relationship. Neonatal nurses have a vital role in
improving the quality of care and outcomes for mothers and infants who are cared for

182
in NICUs. The findings of the study provide evidence fundamental to contemporary
neonatal nursing practice.

183
REFERENCES Abidin, R., C., J., & McGaughey, M. (1992). The relationship of early family
variables to children's subsequent behavioral adjustment. Journal of Clinical Child Psychology, 21, 61-69
. Able-Boone, H., Dokecki, P. R., & Smith, M. S. (1989). Parent and health care
provider communication and decision making in the intensive care nursery. Children's Health Care, 18(3), 133-141
Affleck, G., & Tennen, H. (1993). Cognitive adaptation to adversity: insights from
parents of medically fragile infants. In A. P. Turnbull & J. M. Patterson & S. K. Behr & D. L. Murphy & J. G. Marquis & M. J. Blue-Banning (Eds.), Cognitive coping, families, and disability. (pp. 135-150). Baltimore: Paul H. Brookes Publishing Co.
Affleck, G., Tennen, H., & Rowe, J. (1991). Infants in crisis: how parents cope with
newborn intensive care and its aftermath. New York: Springer-Verlag New York Inc.
Affleck, G., Tennen, H., Rowe, J., & Higgins, P. (1990). Mothers' remembrances of
newborn intensive care: a predictive study. Journal of Pediatric Psychology, 15(1), 67-81.
Affleck, G., Tennen, H., Rowe, J., Roscher, B., & Walker, L. (1989). Effects of
formal support on mothers' adaption to the hospital-to-home transition of high-risk infants: the benefits and costs of helping. Child Development, 60, 488-501.
Ainsworth, M. D. S., Blehar, M., Waters, E., & Wall, S. (1978). Patterns of
attachment : a psychological study of the strange situation. Hillsdale, N.J: Lawrence Erlbaum Associates.
Alfasi, G., & et al. (1985). Mother-infant feeding interactions in preterm and full-term
infants. Infant Behavior and Development, 8(2), 167-180. Allen, J. (1995). Family reactions to premature birth. In W. V. Wyly (Ed.), Preterm
infants and their families (pp. 171-191). San Diego: Singular Publishing Group.
American Psychiatric Association (1994). Diagnostic and statistical manual of mental
disorders (DSM IV) (Vol. 4th edition). Washington DC: American Psychiatric Association.
Anderson, A. E., Wildin, S. R., Woodside, M., Swank, P. R., Smith, K. E., Denson, S.
E., Miller, c. L., Butler, I. J., & Landry, S. H. (1996). Severity of medical and neurologic complications as a determinant of neurodevelopmental outcome at 6 and 12 months in very low birth weight infants. Journal of Child Neurology, 11, 215-219.

184
Anderson, G. C. (1991). Current knowledge about skin-to-skin (kangaroo) care for preterm infants. Journal of Perinatology, 1, 216-226.
Antony, M., Bieling, P., Cox, B., Enns, M., & Swinson, R. (1998). Psychometric
properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychological Assessment, 10(2), 176-181.
Appleby, L., Gregoire, A., Platz, C., Prince, M., & Kumar, R. (1994). Screening
women for high risk of postnatal depression. Journal of Psychosomatic Research, 38(6), 539-545.
Areias, M. E., Kumar, R., Barros, H., & Figueiredo, E. (1996). Correlates of postnatal
depression in mothers and fathers. British Journal of Psychiatry, 169(1), 36-41.
Astbury, J., Brown, S., Lumley, J., & Small, R. (1994). Birth events, birth experiences
and social differences in postnatal depression. Australian Journal of Public Health, 18(2), 176-184.
Avery, M. (1992). A 50-year overview of perinatal medicine. Early Human
Development, 29, 43-50. Bakeman, R., & Brown, J. V. (1980). Early interaction: Consequences for social and
mental development at three years. Child Development, 51, 437-447. Baker, J. K., Borchers, D. A., Cochran, D. T., Kaltofen, K., Orcutt, N., Peacock, J. A.,
Terry, E. G., Wesolowski, C. A., & Yeager, L. A. (1994). Kathryn E. Barnard. In A. Marriner-Tomey (Ed.), Nursing theorists and their work (3rd ed., pp. 406-422). St. Louis: Mosby.
Baker, J. P. (1996). The machine in the nursery: incubator technology and the origins
of newborn intensive care. Baltimore: The Johns Hopkins University Press. Barnard, K., Osofsky, J., Beckwith, L., Hammond, M., & et al. (1996). A
collaborative effort to study mother-child interaction in three risk groups: Social risk mother, adolescent mother, preterm infant. Infant Mental Health Journal, 17(4), 293-301.
Barnard, K. E. (1978a). NCAST: Nursing child assessment satellite training: learning
resource manual. Seattle: University of Washington. Barnard, K. E. (1978b). Nursing child assessment feeding scale. Seattle: University of
Washington. Barnard, K. E. (1995). NCAST feeding and teaching scales: meaning and utilization.
NCAST National News, pp. Vol 11. No 13.

185
Barnard, K. E. (1996). Influencing parent-child interactions for children at risk. In M. J. Guralnick (Ed.), The effectiveness of early intervention: second generation research (pp. 249-268): Paul Brookes Publishing.
Barnard, K. E., Bee, H. L., & Hammond, M. A. (1984). Developmental changes in
maternal interactions with term and preterm infants. Infant Behavior and Development, 7(1), 101-113.
Barnard, K. E., Booth, C. L., Mitchell, S. K., & Telzrow, R. W. (1988). Newborn
nursing models: a test of early intervention to high-risk infants and families. In E. D. Hibbs (Ed.), Children and families: studies in prevention and intervention (pp. 63-81). Madison: International Universities Press, Inc.
Barnard, K. E., Hammond, M. A., Booth, C. I., Bee, H. I., Mitchell, S. K., & Spieker,
S. J. (1989). Measurement and meaning of parent-child interaction. In D. Keating (Ed.), Applied developmental psychology (Vol. 3, pp. 39-79). California: Academic Press.
Barnard, K. E., Magyary, D., Sumner, G., Booth, C. L., Mitchell, S. K., & Spieker, S.
(1988). Prevention of parenting alterations for women with low social support. Psychiatry, 51(3), 248-253.
Barnard, K. E., Snyder, C., & Spietz, A. (1984). Supportive measures for high-risk
infants and families. Birth Defects: Original Article Series, 20(5), 291-329. Barnard, K. I., & Kelly, J. F. (1990). Assessment of parent-child interaction. In J. P.
Shonkoff (Ed.), Handbook of early childhood intervention (pp. 278-302). Cambridge: Cambridge University Press.
Barnett, C., Leiderman, P., Grobstein, R., & Klaus, M. (1970). Neonatal separation:
the maternal side of interactional deprivation. Pediatrics, 45, 197-205. Beal, J. A., Maguire, A., & Carr, R. (1996). Neonatal nurse practitioners: identity as
advanced practice nurses. JOGNN - Journal of Obstetric, Gynecologic, & Neonatal Nursing, 25(5), 401-406.
Beck, A. T., Steer, R. A., Ball, R., & Ranieri, W. (1996). Comparison of beck
depression inventories -IA and -II in psychiatric outpatients. Journal of Personality Assessment, 67(3), 588-597.
Beck, C. T. (1995). Perceptions of nurses' caring by mothers experiencing postpartum
depression. JOGNN - Journal of Obstetric, Gynecologic, & Neonatal Nursing, 24(9), 819-825.
Beck, C. T. (1996a). A meta-analysis of predictors of postpartum depression. Nursing
Research, 45(5), 297-303. Beck, C. T. (1996b). Postpartum depressed mothers' experiences interacting with their
children. Nursing Research, 45(2), 98-104.

186
Beck, C. T. (1998). A review of research instruments for use during the postpartum period. MCN, American Journal of Maternal Child Nursing, 23(5), 254-261.
Beck, C. T., & Gable, R. K. (2001). Comparative analysis of the performance of the
Postpartum Depression Screening Scale with two other depression instruments. Nursing Research, 50(4), 242-250.
Beck, C. T. (1998). A checklist to identify women at risk for developing postpartum
depression. JOGNN Journal of Obstetric, Gynecologic, & Neonatal Nursing, 27(1), 39-46.
Beck, C. T. (2002). Revision of the Postpartum Depression Predictors Inventory.
JOGNN Journal of Obstetric, Gynecologic, & Neonatal Nursing, 31, 394-402. Beckwith, L. (1984). Parent interaction with their preterm infants and later mental
development. Early Child Development and Care, 16(1-2), 27-40. Beckwith, L. (1986). Parent interaction with their preterm infants and later mental
development. In A. S. Honig (Ed.), Risk factors in infancy. Special aspects of education (Vol. 7, pp. 27-40). London: Gordon and Breach Science Publishers.
Beckwith, L. (1988). Intervention with disadvantaged parents of sick preterm infants.
Psychiatry, 51(3), 242-247. Beckwith, L., & Cohen, S. E. (1984). Home environment and cognitive competence
in preterm children during the first 5 years. In A. W. Gottfried (Ed.), Home environment and early cognitive development : longitudinal research. (pp. 235-271). New York: Academic Press.
Beckwith, L., & Rodning, C. (1992). Evaluating effects of intervention with parents
of preterm infants. In M. D. Sigman (Ed.), The psychological development of low-birthweight children (Vol. 6, pp. 389-410). New Jersey: Ablex Publishing Corporation.
Beckwith, L., & Rodning, C. (1996). Dyadic processes between mothers and preterm
infants: development at ages 2 to 5 years. Infant Mental Health Journal, 17(4), 322-333.
Beckwith, L., Rodning, C., & Cohen, S. (1992). Preterm children at early adolescence
and continuity and discontinuity in maternal responsiveness from infancy. Child Development, 63(5), 1198-1208.
Bee, H. L., Barnard, K. E., Eyres, S. J., Gray, C. A., Hammond, M. A., Spietz, A. L.,
Snyder, C., & Clark, B. (1982). Prediction of IQ and language skill from perinatal status, child performance, family characteristics, and mother-infant interaction. Child Development, 53(5), 1134-1156.
Belsky, J. (1981). Early human experience: a family perspective. Developmental
Psychology, 17, 3-23.
187
Belsky, J., Fish, M., & Isabella, R. A. (1991). Continuity and discontinuity in infant
negative and positive emotionality: Family antecedents and attachment consequences. Developmental Psychology, 27, 421-431.
Belsky, J., Rosenberger, K., & Crnic, K. (1995). The origins of attachment security.
"Classical" and contextual determinates. In J. Kerr (Ed.), Attachment theory. Social, developmental, and clinical perspectives. (pp. 153-184). New Jersy: The Analytic Press.
Belsky, J., & Vondra, J. (1989). Lessons from child abuse: the determinates of
parenting. In V. Carlson (Ed.), Child maltreatment: Theory and research on the causes and consequences of child abuse and neglect. (pp. 153-202). New York: Cambridge University Press.
Bennett, D. E., & Slade, P. (1991). Infants born at risk: Consequences for maternal
post-partum adjustment. British Journal of Medical Psychology, 64(2), 159-172.
Berlin, I. J., Brooks-Gunn, J., Spiker, D., & Zaslow, M. J. (1995). Examining
observational measures of emotional support and cognitive stimulation in black and white mothers of preschoolers. Journal of Family Issues, 16, 664-686.
Bernazzani, O., Saucier, J. F., David, H., & Borgeat, F. (1997). Psychosocial
predictors of depressive symptomatology level in postpartum women. Journal of Affective Disorders, 46(1), 39-49.
Berry, J. O., & Hardman, M. L. (1998). Lifespan perspectives on the family and
disability. Boston: Allyn and Bacon. Best, M. A. (1993). The family in crisis. In J. Deacon (Ed.), Core curriculum for
neonatal intensive care nursing (pp. 537-547). Philadelphia: W.B. Saunders Company.
Bialoskurski, M., Cox, C. L., & Wiggins, R. D. (2002). The relationship between
maternal needs and priorities in a neonatal intensive care environment. Journal of Advanced Nursing, 37(1), 62-69.
Bigsby, R., Coster, W., Lester, B. M., & Peucker, M. R. (1996). Motor behavioral
cues of term and preterm infants at 3 months. Infant Behavior & Development, 19, 295-307.
Blackburn, S. (1995). Problems of preterm infants after discharge. Journal of
Obstetric, Gynecologic and Neonatal Nursing, 24(1), 43-49. Blackburn, S., & Lowen, L. (1986). Impact of an infant's premature birth on the
grandparents and parents. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 15(2), 173-178.
188
Blumberg, N. (1980). Effects of neonatal risk, maternal attitude and congitive style on early postpartum adjustment. Journal of Abnormal Psychology, 89, 139-150.
Bogden, R., Brown, M., & Foster, S. (1982). Be honest but not cruel: staff-patient
communication on a neonatal unit. Human Organization, 41, 6-16. Bornstein, M. H., & Lamb, M. E. (1992). Development in infancy: an introduction
(Third edition ed.). New York: McGraw-Hill, Inc. Boss, P. (1988). Family stress management. California: Sage. Bowlby, J. (1969). Attachment and loss, Attachment (Vol. 1). New York: Basic
Books. Bowlby, J. (1971). Attachment (Vol. 1). Harmondsworth: Penguin. Bowlby, J. (1973). Attachment and loss: Seperation, anxiety and anger. (Vol. 2). New
York: Basic Books. Boyce, P. M., & Stubbs, J. M. (1994). The importance of postnatal depression.
Medical Journal of Australia, 161(8), 471-472. Boyce, P. M., Stubbs, J. M., & Todd, A. (1993). The edinburgh postnatal depression
scale: validation for an Australian sample. Australian and New Zealand Journal of Psychiatry, 27, 472-476.
Bracht, M., Ardal, F., Bot, A., & Cheng, C. M. (1998). Initiation and maintenance of a
hospital-based parent group for parents of premature infants: key factors for success. Neonatal Network - Journal of Neonatal Nursing, 17(3), 33-37.
Brazy, J., Eckerman, C., Oehler, J., Goldstein, R., & O'Rand, A. M. (1991). Nursery
neurobiologic risk score: important factors in predicting outcome in very low birth weight infants. Journal of Pediatrics, 118, 783-792.
Brody, E. M. (1995). Prospects for family caregiving: response to change, continuity
and diversity. In J. D. Penrod (Ed.), Family caregiving in an ageing society. California: Sage.
Bronfenbrenner, U. (1979). The ecology of human development. Cambridge: Harvard
University Press. Brooten, D., Gennaro, S., Brown, L. P., Butts, P., Gibbons, A. L., Bakewell-Sachs, S.,
& Kumar, S. P. (1988). Anxiety, depression, and hostility in mothers of preterm infants. Nursing Research, 37(4), 213-216.
Brooten, D., Gennaro, S., Knapp, H., Brown, L., & York, R. (1989). Clinical
specialist pre- and postdischarge teaching of parents of very low birth weight infants. JOGNN - Journal of Obstetric, Gynecologic, & Neonatal Nursing, 18(4), 316-322.

189
Brown, J., & Ritchie, J. A. (1989). Nurses' perceptions of their relationships with parents of hospitalized children. Maternal-Child Nursing Journal, 18(2), 79-96.
Brown, J., & Ritchie, J. A. (1990). Nurses' perceptions of parent and nurse roles in
caring for hospitalized children. Children's Health Care, 19(1), 28-36. Browne, K. (1997). Predicting and preventing child maltreatment. In K. Browne & M.
Herbert (Eds.), Preventing Family Violence (pp. 111-137). New York: Wiley. Brunssen, S. H., & Miles, M. S. (1996). Sources of environmental stress experienced
by mothers of hospitalized medically fragile infants. Neonatal Network - Journal of Neonatal Nursing, 15(3), 88-89.
Buka, S. L., Lipsitt, L. P., & Tsuang, M. T. (1992). Emotional and behavioral
development of low-birthweight infants. In M. D. Sigman (Ed.), The psychological development of low-birthweight children (Vol. 6). New Jersey: Ablex Publishing Corporation.
Butts, P. A., Brooten, D., Brown, L., Bakewell-Sachs, S., Gibbons, A., Finkler, S.,
Kumar, S., & Delivoria-Papadapoulos, M. (1988). Concerns of parents of low birthweight infants following hospital discharge: a report of parent-initiated telephone calls. Neonatal Network - Journal of Neonatal Nursing, 7(2), 37-42.
Cadzow, S. P., Armstrong, K. L., & Fraser, J. A. (1999). Stressed parents with infants:
reassessing physical abuse risk factors. Child Abuse & Neglect, 23(9), 1-9 Caflin, C. J., & Meisels, S. J. (1993). Assessment of the impact of very low
birthweight infants on families. In N. J. Anastasiow & S. Harel (Eds.), At-Risk infants: interventions, families, and research. (pp. 57-79). Baltimore: Paul H. Brookes Publishing Co.
Calam, R., Lambrenos, K., Cox, A., & Weindling, A. (1999). Maternal appraisal of
information given around the time of preterm delivery. Journal of Reproductive and Infant Psychology, 17, 267-280.
Callery, P., & Smith, L. (1991). A study of role negotiation between nurses and the
parents of hospitalised children. Journal of Advanced Nursing, 16, 772-781. Campbell, S. B., Cohen, J. F., Flanagan, C., Popper, S., & Meyers, T. (1992). Course
and correlates of postpartum depression during the transition to parenthood. Development and Psychopathology, 4, 29-47.
Campbell, S. B., Cohn, J. F., & Meyers, T. (1995). Depression in first-time mothers:
Mothernfant interaction and depression chronicity. Developmental Psychology, 31(3), 349-357.

190
Carter, A. S., Garrity-Rokous, F. E., Chazan-Cohen, R., Little, C., & Briggs-Gowan, M. J. (2001). Maternal depression and comorbidity: Predicting early parenting, attachment security, and toddler social-emotional problems and competencies. Journal of the American Academy of Child & Adolescent Psychiatry, 40(1), 18-26.
Catlett, A. T., Miles, M. S., & Holditch-Davis, D. (1994). Maternal perception of
illness severity in premature infants. Neonatal Network - Journal of Neonatal Nursing, 13(2), 45-49.
Censullo, M. (1994). Developmental delay in healthy premature infants at age two
years: implications for early intervention. Journal of Developmental & Behavioral Pediatrics, 15(2), 99-104.
Censullo, M., Bowler, R., Lester, B., & Brazelton, T. B. (1987). An instrument for the
measurement of infant-adult synchrony. Nursing Research, 36, 244-248. Chapieski, M. L., & Evankovich, K. D. (1997). Behavioral effects of prematurity.
Seminars in Perinatology, 21(3), 221-239. Cobb, S. (1976). Social support as a moderator of life stress. Psychosomatic
Medicine, 38, 300-314. Cogill, S. R., Caplan, H. L., Alexandra, H., Robson, K. M., & Kumar, R. (1986).
Impact of maternal postnatal depression on cognitive development of young children. British Medical Journal Clinical Research Ed., 292(6529), 1165-1167.
Cohen, S. E., Parmelee, A. H., Sigman, M., & Beckwith, L. (1988). Antecedents of
school problems in children born preterm. Journal of Pediatric Psychology, 13(4), 493-507.
Cohn, J. F., Campbell, S. B., Matias, R., & Hopkins, J. (1990). Face-to-face
interactions of postpartum depressed and nondepressed mother-infant pairs at 2 months. Developmental Psychology, 26(1), 15-23.
Cohn, J. F., Matias, R., Tronick, E. Z., Connell, D., & Lyons-Ruth, K. (1986). Face-
to-face interactions of depressed mothers and their infants. New Directions for Child Development(34), 31-45.
Condon, W. S., & Sander, L. W. (1974). Neonate movement is synchronized with
adult speech: Interactional participation and language acquisition Method of micro-analysis of sound films of behavior. Science, 183(4120), 99-101.
Cone, T. E. (1985a). Forward by Silverman W.A., History of the care and feeding of
the premature infant (pp. vii-viii). Boston: Little, Brown and Company. Cone, T. E. (1985b). History of the care and feeding of the premature infant. Boston:
Little, Brown and Company.

191
Cooper, P. J., Campbell, E. A., Day, A., Kennerley, H., & Bond, A. (1988). Non-psychotic psychiatric disorder after childbirth. A prospective study of prevalence, incidence, course and nature [see comments]. British Journal of Psychiatry, 152, 799-806.
Cooper, P. J., & Murray, L. (1995). Course and recurrence of postnatal depression.
Evidence for the specificity of the diagnostic concept. British Journal of Psychiatry, 166(2), 191-195.
Cooper, P. J., & Murray, L. (1998). Postnatal depression. British Medical Journal,
316, 1884-1886. Cooper, P. J., Murray, L., Hooper, R., & West, A. (1996). The development and
validation of a predictive index for postpartum depression. Psychological Medicine, 26, 627-634.
Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Detection of postnatal depression.
Development of the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry, 150, 782-786.
Coyl, D. D., Roggman, L. A., & Newland, L. A. (2002). Stress, maternal depression,
and negative mother-infant interactions in relation to infant attachment. Infant Mental Health Journal, 23(1-2), 145-163.
Crnic, K. A., & Greenberg, M. T. (1987). Transactional relationships between
perceived family style, risk status, and mother-child interactions in two-year-olds. Journal of Pediatric Psychology, 12(3), 343-362.
Crnic, K. A., Greenberg, M. T., Ragozin, A. S., Robinson, N. M., & Basham, R. B.
(1983a). Effects of stress and social support on mothers and premature and full-term infants. Child Development, 54(1), 209-217.
Crnic, K. A., Greenberg, M. T., Robinson, N. M., & Ragozin, A. S. (1984). Maternal
stress and social support: Effects on the mother-infant relationship from birth to eighteen months. American Journal of Orthopsychiatry, 54(2), 224-235.
Crnic, K. A., Greenberg, M. T., & Slough, N. M. (1986). Early stress and social
support influences on mothers' and high-risk infants' functioning in late infancy. Infant Mental Health Journal, 7(1), 19-33.
Crnic, K. A., Ragozin, A. S., Greenberg, M. T., Robinson, N. M., & Basham, R. B.
(1983b). Social interaction and developmental competence of preterm and full-term infants during the first year of life. Child Development, 54(5), 1199-1210.
Cronin, C. M., Shapiro, C. R., Casiro, O. G., & Cheang, M. S. (1995). The impact of
very low-birth-weight infants on the family is long lasting. Archives Pediatric Adolescent Medicine, 149, 151-158.

192
Cummings, E. M., & Cicchetti, D. (1990). Towards a transactional model of relations between attachment and depression. In E. M. Cummings (Ed.), Attachment in the preschool years: Theory, research and intervention. Chicago: University of Chicago Press.
Cummings, E. M., & Davies, P. T. (1994). Maternal depression and child
development. Journal of Child Psychology and Psychiatry., 35, 73-112. Curley, M. A. Q., & Wallace, J. (1992). Effects of the nursing mutual participation
model of care on parental stress in the pediatric intensive care unit -- a replication. Journal of Pediatric Nursing: Nursing Care of Children & Families, 7(6), 377-385.
Cutrona, C., & Troutman, B. (1986). Social support, infant temperament, and
parenting self-efficacy: a mediational model of postpartum depression. Child Development, 57, 1507-1518.
Day, P., Sullivan, E. A., Ford, J., & Lancaster, P. (1997). Australia's mothers and
babies (9). Sydney: Australian Institute of Health and Welfare National Perinatal Statistics Unit.
DeMier, R. L., Hynan, M. T., Hatfield, R. F., Varner, M. W., Harris, H. B., &
Manniello, R. L. (2000). A measurement model of perinatal stressors: identifying risk for postnatal emotional distress in mothers of high-risk infants. Journal of Clinical Psychology, 56(1), 89-100.
Dennis, C. L., & Kavanagh, J.Psychological interventions for preventing postpartum
depression [Update Software]. Issue 4, 2001. The Cochrane Library: Update Software. Retrieved, from the World Wide Web:
Desmond, M. M. (1991). A review of newborn medicine in america: european past
and guiding ideology. American Journal of Perinatology, 8(5), 308-321. Dobbins, N., Bohling, C., & Sutphen, J. (1994). Partners in growth: implementing
family centred changes in the neonatal intensive care unit. Children's Health Care, 32(2), 115-126.
Doering, L. V., Dracup, K., & Moser, D. (1999). Comparison of psychosocial
adjustment of mothers and fathers of high-risk infants in the neonatal intensive care unit. Journal of Perinatology, 19(2), 132-137.
Dohrenwend, B. S., & Dohrenwend, B. P. (1978). Overview and prospects: some
issues in research on stressful life events. Journal of Nervous & Mental Disease, 166, 7-15.
Donovan, W. L., Leavitt, L. A., & Walsh, R. O. (1998). Conflict and depression
predict maternal sensitivity to infant cries. Infant Behavior and Development, 21(3), 505-517.

193
Downey, G., & Coyne, J. C. (1990). Children of depressed parents: an integrative review. Psychological Bulletin, 108, 50-76.
Drillien, C. M. (1968). Classification of newborn infants by weight and gestation.
Developmental Medicine & Child Neurology., 10(5), 667-670. Drotar, D. (1992). Integrating theory and practice in psychological intervention with
families of children with chronic illness. In T. J. Akamatsu & S. E. Stephens & S. E. Hobfall & J. H. Crowther (Eds.), Family Health Psychology (pp. 172-192). Washington, DC: Hemisphere Publishing.
Drotar, D., & Bush, M. (1985). Mental health issues and services. In N. Hobbs & J. H.
Perrin (Eds.), Issues in the care of children with chronic illness. (pp. 514-550). San Franscisco: Jossey-Bass.
Dunst, C. J., Trivette, C., & Deal, A. (1988). Enabling and empowering parents.
Cambridge, MA: Brookline Books. Dunst, C. J., Trivette, C. M., & Cross, A. H. (1986). Roles and support networks of
mothers of handicapped children. In R. R. Fewell & P. F. Vadasy (Eds.), Families of handicapped children: needs and supports across the life span. Texas: Pro-ed.
Easterbrooks, M. A. (1988). Effects of infant risk status on the transition to
parenthood. In G. Y. Michaels & W. A. Goldberg (Eds.), The transition to parenthood: current theory and research (pp. 176-208). Cambridge: Cambridge University Press.
Eckerman, C. O., Hsu, H. C., Molitor, A., Leung, E. H., & Goldstein, R. F. (1999).
Infant arousal in an en-face exchange with a new partner: effects of prematurity and perinatal biological risk. Developmental Psychology, 35, 282-293.
Eckerman, C. O., & Oehler, J. M. (1992). Very-low-birthweight newborns and
parents as early social partners. In S. L. Friedman & M. D. Sigman (Eds.), The psychological development of low-birthweight children (Vol. 6, pp. 91-123). New Jersey: Ablex Publishing Corporation.
Eckerman, C. O., Oehler, J. M., Hannan, T. E., & Molitor, A. (1995). The
development prior to term age of very prematurely born newborns' responsiveness in en face exchanges. Infant Behavior & Development, 18(283-297).
Edwards, K. A., & Allen, M. E. (1988). Nursing management of the human response
to premature birth experience. Neonatal Network, 6, 82-86. Eizirik, L., Bohlin, G., & Hagekull, B. (1994). Interaction between mother and pre-
term infant at 34 weeks post-conceptional age. Early Development & Parenting, 3, 171-180.

194
Elder, M. G. (1994). New perspectives for the effective treatment of preterm labour - an international concensus. Research and Clinical Forums., 16(3), 189-194.
England, S. J., Ballard, C., & George, S. (1994). Chronicity in postnatal depression.
European Journal of Psychiatry, 8, 93-96. Engler, A. J., Ludington-Hoe, S. M., Cusson, R. M., Adams, R., Bahnsen, M.,
Brambaugh, E., et al. (2002). Kangaroo care: national survey of practice, knowledge, barriers, and perceptions. MCN, American Journal of Maternal Child Nursing, 27(3), 145-153.
Enkin, M., Keirse, M. J., Renfrew, M., & Neilson, J. (1995). A guide to effective care
in pregnancy and childbirth (2nd ed.). Oxford: Oxford University Press. Erdfelder, E., Faul, F., & Buchner, A. (1996). GPOWER: A general power analysis program. Behavior Research Methods, Instruments, & Computers, 28, 1-11. Escalona, S. K. (1982). Babies at double hazard: early development of infants at
biologic and social risk. Pediatrics, 70(5), 670-676. Evans, P. (1998). Stress and coping. In M. Pitts & K. Phillips (Eds.), The psychology
of health (Vol. 2nd edition, pp. 48-66). London: Routledge. Fantz, R. L. (1963). Pattern vision in newborn infants. Science, 140, 296-297. Farel, A. M., Freeman, V. A., Keenan, N. L., & Huber, C. J. (1991). Interaction
between high-risk infants and their mothers: the NCAST as an assessment tool. Research in Nursing & Health, 14(2), 109-118.
Farren, D. C., Kasari, C., Yoder, P., Harber, L., Huntington, G. S., & Comfort-Smith,
M. (1987). Rating mother-child interactions in handicapped and at-risk infants. In T. Tamir (Ed.), Stimulation and intervention in infant development. London: Freund Publishing House.
Feiring, C., Fox, N. A., Jaskir, J., & Lewis, M. (1987). The relation between social
support, infant risk status and mother-infant interaction. Developmental Psychology, 23(3), 400-405.
Fenwick, J., Barclay, L., & Schmied, V. (1999). Activities and interactions in level II
nurseries: a report of an ethnographic study. Journal of Perinatal & Neonatal Nursing, 13(1), 53-65.
Fewell, R. R., Casal, S. G., Glick, M. P., Wheeden, C. A., & Spiker, D. (1996).
Maternal education and maternal responsiveness as predictors of play competence in low birth weight, premature infants: a preliminary report. Journal of Developmental & Behavioral Pediatrics, 17(2), 100-104.

195
Field, T. (1995). Infants of depressed mothers. Infant Behavior and Development, 18(1), 1-13.
Field, T. (1998). Maternal depression effects on infants and early interventions.
Preventive Medicine: An International Devoted to Practice and Theory, 27(2), 200-203.
Field, T., & et al. (1985). Pregnancy problems, postpartum depression, and early
mothernfant interactions. Developmental Psychology, 21(6), 1152-1156. Field, T. M. (1977). Effects of early separation, interactive deficits, and experimental
manipulations on infant-mother face-to-face interaction. Child Development, 48(3), 763-771.
Field, T. M. (1979). Interaction patterns of pre-term and term infants. In Field & S.
Sostek & S. Goldberg & H. H. Shuman (Eds.), Infants born at risk (pp. 333-356). New York: Spectrum.
Field, T. M. (1982). Affective displays of high risk infants during early interactions.
In A. Fogel (Ed.), Emotion and early interaction (pp. 101-126). Hillsdale, N.J.: Lawrence Erlbaum Associates.
Fiese, B. H., Poehlmann, J., Irwin, M., Gordon, M., & Curry-Bleggi, E. (2001). A
pediatric screening instrument to detect problematic infant-parent interactions: Initial reliability and validity in a sample of high and low risk infants. Infant Mental Health Journal, 22, 463-478.
Fiese, B. H., & Sameroff, A. J. (1989). Family context in pediatric psychology: a
transactional perspective. Journal of Pediatric Psychology, 14(2), 293-314. Fisher, S. (1996). Life stress, personal control and the risk of disease. In C. Cooper
(Ed.), Handbook of stress, medicine and health. London: CRC Press. Folkman, S., & Lazarus, R. S. (1985). If it changes it must be a process: a study of
emotion and coping during three stages of a college examination. Journal of Personality and Social Psychology, 48, 150-170.
Foss, L. A., Hirose, T., & Barnard, K. E. (1999). Relationship of three types of parent-
child interaction in depressed and non-depressed mothers and their children's mental development at 13 months. Nursing and Health Sciences, 1, 211-219.
Fox, S., & Jeffrey, J. (1997). The role of the nurse with families of patients in ICU:
the nurses' perspective. Canadian Journal of Cardiovascular Nursing, 8(1), 17-23.
Frankel, K. A., & Harmon, R. J. (1996). Depressed mothers: They don't always look
as bad as they feel. Journal of the American Academy of Child & Adolescent Psychiatry, 35, 289-293.

196
Garcia Coll, C. T., Halpern, L. F., Vohr, B. R., Seifer, R., & et al. (1992). Stability and correlates of change of early temperament in preterm and full-term infants. Infant Behavior & Development, 15(2), 137-153.
Gelfand, D. M., & Teti, D. M. (1990). The effects of maternal depression on children.
Clinical Psychology Review, 10(3), 329-353. Gennaro, S. (1988). Postpartal anxiety and depression in mothers of term and preterm
infants. Nursing Research, 37(2), 82-85. Gennaro, S. (1991). Facilitating parenting of the neonatal intensive care graduate.
Journal of Perinatal and Neonatal Nursing, 4, 55-61. Gennaro, S. (1996). Family response to the low birth weight infant. Nursing Clinics of
North America, 31(2), 341-350. Gennaro, S., Brooten, D., & Bakewell-Sachs, S. (1991). Postdischarge services for
low-birth-weight infants. JOGNN - Journal of Obstetric, Gynecologic, & Neonatal Nursing, 20(1), 29-36.
Gennaro, S., Tulman, L., & Fawcett, J. (1990). Temperament in preterm and full-term
infants at three and six months of age. Merrill-Palmer Quarterly, 36, 201-215. Gennaro, S., York, R., & Brooten, D. (1990). Anxiety and depression in mothers of
low birthweight and very low birthweight infants: birth through 5 months. Issues in Comprehensive Pediatric Nursing, 13(2), 97-109.
Gennaro, S., York, R., Brown, L., Stringer, M., & Brooten, D. (1994). A
sociodemographic comparison of families of very low-birthweight infants: 1982-1991. Public Health Nursing, 11(3), 168-173.
Gerner, E. M. (1999). Emotional interaction in a group of preterm infants at 3 and 6
months of corrected age. Infant & Child Development, 8(3), 117-128. Gilkerson, L., Gorski, P. A., & Panitz, P. (1990). Hospital-based intervention for
preterm infants and their families. In S. J. Meisels & J. P. Shonkoff (Eds.), Handbook of early childhood intervention (pp. 445-468). Cambridge: Cambridge University Press.
Goldberg, S., & DiVitto, B. (1995). Parenting children born preterm. In M. H. E.
Bornstein (Ed.), Handbook of Parenting - Children and Parenting (Vol. 1, pp. 209-231). Hove, UK: Lawrence Erlbaum Associates.
Goldson, E. (1992). The neonatal intensive care unit: premature infants and parents.
Infants & Young Children, 4(3), 31-42. Gorga, D., Stern, F. M., & Ross, G. (1985). Trends in neuromotor behavior of preterm
and fullterm infants in the first year of life: A preliminary report. Developmental Medicine and Child Neurology, 27, 756-766.
197
Gotlib, I. H., Whiffen, V. E., Wallace, P. M., & Mount, J. H. (1991). Prospective investigation of postpartum depression: Factors involved in onset and recovery. Journal of Abnormal Psychology, 100(2), 122-132.
Gottwald, S. R., & Thurman, S. K. (1990). Parent-infant interaction in neonatal
intensive care units: implications for research and service delivery. Infants & Young Children, 2(3), 1-9.
Graveley, E. A., & Littlefield, J. H. (1992). A cost-effectiveness analysis of three
staffing models for the delivery of low-risk prenatal care. American Journal of Public Health, 82(2), 180-184.
Greenberg, M. T., & Crnic, K. A. (1988). Longitudinal predictors of developmental
status and social interaction in premature and full-term infants at age two. Child Development, 59(3), 554-570.
Greene, J. G., Fox, N. A., & Lewis, M. (1983). The relationship between neonatal
characteristics and three-month mother-infant interaction in high-risk infants. Child Development, 54(5), 1286-1296.
Greenspan, S. (1992). Infancy and early childhood: The practice of clinical
assessment and intervention with emotional and developmental challenges. Madison: International Universities Press.
Greenspan, S., & Lieberman, A. (1980). Infants, mothers and their interactions: a
quantitative clinical approach to developmental assessment., The Course of Life: Psychoanalytic Contributions Toward Understanding Personality Development (Vol. 1). Washington: U.S. Government Printing Office.
Griffin, T. (1990). Nurse barriers to parenting in the special care nursery. Journal of
Perinatal & Neonatal Nursing, 4(2), 56-67. Gurel, S., & Gurel, H. (2000). The evaluation of determinants of early postpartum low
mood: the importance of parity and inter-pregnancy interval. European Journal of Obstetrics, Gynecology, & Reproductive Biology, 91(1), 21-24.
Gyler, L., Dudley, M., Blinkhorn, S., & Barnett, B. (1993). The relationship between
psychosocial factors and developmental outcome for very low and extremely low birthweight infants: a review. Australian & New Zealand Journal of Psychiatry., 27(1), 62-73.
Hack, M., Merkatz, I. R., Jones, P. K., & Fanaroff, A. A. (1980). Changing trends of
neonatal and postneonatal deaths in very-low-birth-weight infants. American Journal of Obstetrics & Gynecology, 137(7), 797-800.
Hack, M., Wright, L. L., Shankaran, S., Tyson, J. E., Horbar, J. D., Bauer, C. R., et al.
(1995). Very-low-birth-weight outcomes of the National Institute of Child Health and Human Development Neonatal Network, November 1989 to October 1990. American Journal of Obstetrics & Gynecology, 172(2 Pt 1), 457-464.

198
Hall-Johnson, S. H. (1986). Nursing assessment and strategies for the family at risk:
high-risk parenting. Philadelphia: Lippincott, J.B. Harrison, H. (1993). The principles for family-centered neonatal care. Pediatrics,
92(5), 643-650. Harrison, M. J. (1990). A comparison of parental interactions with term and preterm
infants. Research in Nursing & Health, 13(3), 173-179. Harrison, M. J., & Magill-Evans, J. (1996). Mother and father interactions over the
first year with term and preterm infants. Research in Nursing & Health, 19(6), 451-459.
Hearn, G., Iliff, A., Jones, I., Kirby, A., Ormiston, P., et al. (1998). Postnatal
depression in the community. British Journal of General Practice, 48, 1064-1066.
Heimer, C. A., & Staffen, L. R. (1998). For the sake of the children: the social
organization of responsibility in the hospital and the home. Chicago: The University of Chicago Press.
Hetherington, E. M., & Blechman, E. A. (1996). Introduction and overview. In E. M.
Heatherington & E. A. Blechman (Eds.), Stress, coping, and resiliency in children and families. New Jersey: Lawrence Erlbaum Associates, Publishers.
Hickey, A. R., Boyce, P. M., Ellwood, D., & Morris-Yates, A. D. (1997). Early
discharge and risk for postnatal depression [see comments]. Medical Journal of Australia, 167(5), 244-247.
Hill, R. (1949). Families under stress. New York: Harper & Row. Hill, R. (1958). Social stresses on the family. Social Casework, 37, 139-150. Hodnett, E. D. (1998, 25-11-97). Support from caregivers during at-risk pregnancy
[full text electronic database]. The Cochrane Database of Systematic Reviews published by Update Software for the Cochrane collaboration. Retrieved 13-5-99, 1999, from the World Wide Web:
Holden, J. M. (1994). Can non-psychotic depression be prevented? In J. Cox & J.
Holden (Eds.), Perinatal psychiatry: use and misuse of the edinburgh postnatal depression scale (pp. 54-81). London: Gaskell.
Holditch-Davis, D., & Miles, M. S. (2000). Mothers' stories about their experiences in
the neonatal intensive care unit. Neonatal Network Journal of Neonatal Nursing, 19(3), 13-21.
Holditch-Davis, D. H., & Thoman, E. B. (1988). The early social environment of
premature and fullterm infants. Early Human Development, 17(2-3), 221-232.

199
Hossain, Z., Field, T. M., Gonzalez, J., Malphurs, J., & et al. (1994). Infants of
"depressed" mothers interact better with their nondepressed fathers. Infant Mental Health Journal, 15(4), 348-357.
House, J. S. (1981). Work stress and social support. Reading, MA.: Addison-Wesley. Huber, C. J. (1991). Documenting quality of parent-child interaction: use of the
NCAST scales. Infants & Young Children, 4(2), 63-75. Hughes, M., McCollum, J., Seftel, D., & Sanchez, G. (1994). How parents cope with
the experience of neonatal intensive care. Childrens Health Care, 23, 1-14. Hughes, M. A., & McCollum, J. (1994). Neonatal intensive care: mothers' and fathers'
perceptions of what is stressful. Journal of Early Intervention, 18(3), 258-268. Hughes, M. B., Shults, J., McGrath, J., & Medoff-Cooper, B. (2002). Temperament
characteristics of premature infants in the first year of life. Journal of Developmental and Behavioral Pediatrics, 23(6), 430-436
Hurst, I. (1993). Facilitating parental involvement through documentation. Journal of
Perinatal and Neonatal Nursing, September, 80-90. Johnstone, S. J., Boyce, P. M., Hickey, A. R., Morris-Yatees, A. D., & Harris, M. G.
(2001). Obstetric risk factors for postnatal depression in urban and rural community samples. Australian & New Zealand Journal of Psychiatry, 35(1), 69-74.
Kane, R. A., & Penrod, J. D. (1995). Family caregiving in an aging society: policy
perspectives. California: Sage. Kang, R., Barnard, K., Hammond, M., Oshio, S., Spencer, C., Thibodeaux, B., &
Williams, J. (1995). Preterm infant follow-up project: a multi-site field experiment of hospital and home intervention programs for mothers and preterm infants. Public Health Nursing, 12(3), 171-180.
Kendall-Tackett, K. A., & Kaufman Kantor, G. (1993). Postpartum depression: a
comprehensive approach for nurses. California: Sage Publications. Kennell, J. H., & Klaus, M. H. (1976). Caring for parents of a premature or sick
infant. In M. H. Klaus & J. H. Kennell (Eds.), Maternal-infant bonding: the impact or early separation or loss on family development (pp. 99-166). Saint Louis: C.V. Mosby Company.
Kenner, C., & Lott, J. W. (1990). Parent transition after discharge from the NICU.
Neonatal Network, 9, 31-38. Kessler, R. C., Price, R. H., & Wortman, C. B. (1985). Social factors in
psychopathology: stress, social support, and coping processes. Annual Review of Psychology, 36, 531-572.

200
Klaus, M. H., & Kennell, J. H. (1976). Maternal-infant bonding. St. Louis: Mosby. Klaus, M. H., & Kennell, J. H. (1993). Care of the parents. In M. H. Klaus & A. A.
Fanaroff (Eds.), Care of the high-risk neonate (Vol. Fourth Edition, pp. 189-211). Philadelphia: W.B. Saunders Company.
Kliegman, R. M. (1995). Neonatal technology, perinatal survival, social
consequences, and the perinatal paradox. American Journal of Public Health, 85, 909-913.
Koniak-Griffin, D., Verzemnieks, I., & Cahill, D. (1992). Using videotape instruction
and feedback to improve adolescents' mothering behaviors. Journal of Adolescent Health, 13, 570-575.
Kotch, J. B., Browne, D. C., Dufort, V., & Winsor, J. (1999). Predicting child
maltreatment in the first 4 years of life from characteristics assessed in the neonatal period. Child Abuse & Neglect, 23(4), 305-319.
Kotch, J. B., Browne, D. C., Ringwalt, C. L., Stewart, P. W., Ruina, E., Holt, K., et al.
(1995). Risk of child abuse or neglect in a cohort of low-income children. Child Abuse & Neglect, 19, 1115-1130.
Koop, C. E. (1993). Pediatric surgery: the long road to recognition. Pediatrics, 92(4),
618-621. Korner, A. F. (1964). An approach to the study of the influence of primary endowment
factors on later development. New York: International Universities Press, Inc. Korner, A. F., & Grobstein, R. (1966). Visual alertness as related to soothing in
neonates: implications for maternal stimulation and early deprivation. Child Development, 37, 867-876.
Kumar, R., & Robson, K. M. (1984). A prospective study of emotional disorders in
childbearing women. British Journal of Psychiatry, 144, 35-47. LaMontagne, L. L., Johnson, B. D., & Hepworth, J. T. (1995). Evolution of parental
stress and coping processes: a framework for critical care practice. Journal of Pediatric Nursing, 10(4), 212-218.
Lancaster, P., Huang, J., & Lin, M. (1996). Australia's mothers and babies . (No.
Perinatal Statistics Series No. 3). Sydney: AIHW National Perinatal Statistics Unit.
Landry, S. H., Chapieski, M. L., Richardson, M. A., Palmer, J., & Hall, S. (1990). The
social competence of children born prematurely: effects of medical complications and parent behaviors. Child Development, 61(5), 1605-1616.

201
Landry, S. H., Denson, S. E., & Swank, P. R. (1997). Effects of medical risk and socioeconomic status on the rate of change in cognitive and social development for low birth weight children. Journal of Clinical and Experimental Neuropsychology, 19, 261-274.
Langkamp, D. L., Kim, Y., & Pascoe, J. M. (1998). Temperament of preterm infants
at 4 months of age: Maternal ratings and perceptions. Journal of Developmental and Behavioral Pediatrics, 19, 391-395.
Lau, R., & Morse, C. A. (2001). Parents' coping in the neonatal intensive care unit: a
theoretical framework. Journal of Psychosomatic Obstetrics & Gynecology, 22(1), 41-47.
Lazarus, R. S. (1993). Coping theory and research: past, present, and future.
Psychosmoatic Medicine, 55, 234-247. Lazarus, R. S. (1999). Stress and emotion: a new synthesis. London: Springer
Publishing Company Inc. Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York:
Springer. Lee, H., & Barratt, M. S. (1993). Cognitive development of preterm low birth weight
children at 5 to 8 years old. Journal of Developmental & Behavioral Pediatrics, 14(4), 242-249.
Lee, K. S., Kim, B. I., Khoshnood, B., Hsieh, H. L., Chen, T. J., Herschel, M., &
Mittendorf, R. (1995). Outcome of very low birth weight infants in industrialized countries: 1947-1987. American Journal of Epidemiology, 141(12), 1188-1193.
Lefrak-Okikawa, L., & Lund, C. H. (1993). Nursing practice in the neonatal intensive
care unit. In M. H. Klaus & A. A. Fanaroff (Eds.), Care of the high-risk neonate (pp. 212-227). Philadelphia: W.B. Saunders Company.
Leske, J. S., & Jiricka, M. K. (1998). Impact of family demands and family strengths
and capabilities on family well-being and adaptation after critical injury. American Journal of Critical Care, 7(5), 383-392.
Lester, B. M., Hoffman, J., & Brazelton, T. B. (1985). The rhythmic structure of
mother infant interaction in term and preterm infants. Child Development, 56(1), 15-27.
Levy, V., & Kline, P. (1994). Perinatal depression: a factor analysis. British Journal
of Midwifery, 2(4), 154-159. Levy-Schiff, R., Sharir, H., & Mogilner, M. (1987). Mother and father preterm infant
relationship in the hospital preterm nursery. Child Development, 60, 93-102.
202
Lewis, J. (1991). Mothers and maternity policies in the twentieth century. In J. Garcia & R. Kilpartick & M. Richards (Eds.), The politics of maternity care (pp. 15-29). Oxford: Clarendon Press.
Lewis, M. (1967). The meaning of a response or why researchers in infant behavior
should be oriental metaphysicians. Merril-Palmer Quarterly, 13, 7-18. Liaw, F., & Brooks-Gunn, J. (1993). Patterns of low-birth-weight children's cognitive
development. Developmental Psychology, 29, 1024-1035. Lindsay, J. K., Roman, L. A., De Wys, M., Eager, M., Levick, J., & Quinn, M.
(1992). Creative caring in the nicu: parent-to-parent support. Neonatal Network, 12(4), 37-44.
Locke, R., Baumgart, S., Locke, K., Goodstein, M., Thies, C., & Greenspan, J.
(1997). Effect of maternal depression on premature infant health during initial hospitalization. Journal of the American Osteopathic Association, 97(3), 145-149.
Logsdon, M. C., & Davis, D. W. (1997). Predictors of depression in mothers of
preterm infants. Journal of Social Behavior & Personality, 12(1), 73-83. Logsdon, M. C., & Davis, D. W. (1998). Guiding mothers of high-risk infants in
obtaining social support. MCN, American Journal of Maternal Child Nursing, 23(4), 195-199.
Lorenz, J. M., Wooliever, D. E., Jetton, J. R., & Paneth, N. (1998). A quantitative
review of mortality and developmental disability in extremely premature newborns. Archives of Pediatrics & Adolescent Medicine, 152(5), 425-435.
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional
states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research & Therapy, 33(3), 335-343.
Lowenstein, M. K., & Field, T. (1992). Maternal depression effects on infants.
Analise Psicologica, 10(1), 63-69. Lubchenco, L. O., Hansman, C., Dressler, M., & Boyd, E. (1963). Intrauterine growth
as estimated from liveborn birth-weight data at 24-42 weeks of gestation. Pediatrics, 32, 793-800.
Ludington-Hoe, S. M., Thompson, C., Swinth, J., Hadeed, A. J., & Anderson, G. C.
(1994). Kangaroo care: research results, and practice implications and guidelines... findings of two research projects. Neonatal Network - Journal of Neonatal Nursing, 13(1), 19-27.
Lukeman, D., & Melvin, D. (1993). Annotation: the preterm infant: psychological
issues in childhood. Journal of Child Psychology and Psychiatry, 34, 837-849.

203
MacFarlane, A. H., Norman, G. R., Streiner, D. L., Roy, R., & Scott, D. J. (1980). A longitudinal study of the influence of psychosocial environment on health status: a preliminary report. Journal Of Health and Social Behavior, 21, 124-133.
MacLennan, A., Wilson, D., & Taylor, A. (1996). The self-reported prevalence of
postnatal depression. Australian & New Zealand Journal of Obstetrics & Gynaecology, 36, 313.
Magill-Evans, J., & Harrison, M. J. (1999). Parent-child interactions and development
of toddlers born preterm. Western Journal of Nursing Research, 21(3), 292-312.
Magill-Evans, J., & Harrison, M. J. (2001). Parent-child interactions, parenting stress,
and developmental outcomes at 4 years. Children's Health Care, 30(2), 135-150.
Magyary, D., Brandt, P. A., Hammond, M., & Barnard, K. (1992). School age follow-
up of the development of preterm infants: infant and family predictors. In S. L. Friedman & M. D. Sigman (Eds.), The psychological development of low-birthweight children (Vol. 6). New Jersey: Ablex Publishing Corporation.
Mahoney, G., Powell, C., & Finger, I. (1986). The maternal behavior rating scale.
Topics in Early Childhood Special Education, 6, 44-56. Mander, R. (1994). Loss and bereavement in childbearing. Oxford: Blackwell
Scientific Publications. Marks, M. N., Wieck, A., & Checkley, S. A. (1992). Contribution of psychological
and social factors to psychotic and non-psychotic relapse after childbirth in women with previous histories of affective disorder. Journal of Affective Disorders, 29, 253-264.
Mayberry, L. J., & Affonso, D. D. (1993). Infant temperament and postpartum
depression: a review. Health Care for Women International, 14(2), 201-211. Mays, R. M. (1988). Family stress and adaptation. Nurse Practitioner, 13(8), 52, 54,
56. McCarthy, D. (1972). Manual for the mccarthy scales of children's abilities. New
York: Psychological Corporation. McCormick, M. (1985). The contribution of low birth weight to infant mortality and
childhood morbidity. New England Journal of Medicine, 312, 82-90. McCormick, M. C. (1992). Advances in neonatal intensive care technology and their
possible impact on the development of low-birthweight infants. In S. L. Friedman & M. D. Sigman (Eds.), The psychological development of low-birthweight children (Vol. 6, pp. 37-60). New Jersey: Ablex Publishing Corporation.

204
McCormick, M. C. (1993). Has the prevalence of handicapped infants increased with
improved survival of the very low birth weight infant? Clinics in Perinatology, 20(1), 263-277.
McCormick, M. C. (1997). The outcomes of very low birth weight infants: are we
asking the right questions? Pediatrics, 99(6), 869-876. McCubbin, H. I., McCubbin, M. A., Patterson, J., Cauble, A. E., Wilson, L., &
Warwick, W. (1983). CHIP Coping health inventory for parents: An assessment of parental coping patterns in the care of the chronically ill child. Journal of Marriage and the Family, 45, 359-370.
McCubbin, H. I., & Patterson, J. M. (1983). The family stress process: the double
abcx model of adjustment and adaption. In H. I. McCubbin & M. B. Sussman & J. M. Patterson (Eds.), Social stress and the family: advances and developments in family stress theory and research (pp. 7-37). New York: The Haworth Press.
McCubbin, H., & Patterson, J. (1983). Family transitions: adaptation to stress. In H.
McCubbin & C. Figley (Eds.), Stress and the family: Coping with normative transitions (Vol. 1, pp. 5-25). New York: Brunner/Mazel.
McCubbin, H. I., Thompson, A. I., & McCubbin, M. A. (1996). Family assessment:
resiliency, coping and adaptation. Inventories for research and practice. Madison: University of Wisconsin Publishers.
McCubbin, M. A. (1984). Nursing assessment of parental coping with cystic fibrosis.
Western Journal of Nursing Research, 6(4), 407-421. McCubbin, M. A. (1990). The typology model of adjustment and adaptation: a family
stress model. Guidance and Counseling, 5, 6-22. McCubbin, M. A., & McCubbin, H. I. (1993). Families coping with illness: the
resiliency model of family stress, adjustment, and adaptation. In C. B. Danielson & B. Hamel-Bissell & P. Winstead-Fry (Eds.), Families health and illness: perspectives on coping and intervention. St. Louis: Mosby.
McGill, H., Burrows, V. L., Holland, L. A., Langer, H. J., & Sweet, M. A. (1995).
Postnatal depression: a Christchurch study. New Zealand Medical Journal, 108(999), 162-165.
McGrath, J. M., & Conliffe-Torres, S. (1996). Integrating family-centered
developmental assessment and intervention into routine care in the neonatal intensive care unit. Nursing Clinics of North America, 31(2), 367-386.
McGrath, M. M., Sullivan, M. C., & Seifer, R. (1998). Maternal interaction patterns
and preschool competence in high-risk children. Nursing Research, 47(6), 309-317.

205
McKim, E. M. (1993a). The difficult first week at home with a premature infant. Public Health Nursing, 10(2), 89-96.
McKim, E. M. (1993b). The information and support needs of mothers of premature
infants. Journal of Pediatric Nursing: Nursing Care of Children & Families, 8(4), 233-244.
McLean, M., Walters, W. A., & Smith, R. (1993). Prediction and early diagnosis of
preterm labor: a critical review. Obstetrics & Gynecology Survey, 48, 209-225. Mebert, C. J. (1991). Variability in the transition to parenthood experience. In K.
Pillemer & K. McCartney (Eds.), Parent-child relations throughout life (pp. 43-57). New Jersey: Lawrence Erlbaum Associates, Publishers.
Meck, N. E., Fowler, S. A., Claflin, K., & Rasmussen, L. B. (1995). Mothers'
perceptions of their nicu experience 1 and 7 months after discharge. Journal of Early Intervention, 19(3), 288-301.
Meisels, S. J., & Shonkoff, J. P. (1990). Handbook of early childhood intervention.
New York: Cambridge University Press. Mercer, R. T. (1990). Parents at risk. New York: Springer Publishing Company. Mercer, R. T. (1995). Becoming a mother: Research on maternal identity from Rubin
to the present. New York: Springer. Meyer, E. C., Garcia Coll, C. T., Lester, B. M., Boukydis, C. F., McDonough, S. M.,
& Oh, W. (1994). Family-based intervention improves maternal psychological well-being and feeding interaction of preterm infants. Pediatrics, 93(2), 241-246.
Meyer, E. C., Garcia Coll, C. T., Seifer, R., Ramos, A., Kilis, E., & Oh, W. (1995).
Psychological distress in mothers of preterm infants. Journal of Developmental & Behavioral Pediatrics, 16(6), 412-417.
Miles, M. S. (1989). Parents of critically ill premature infants: sources of stress.
Critical Care Nursing Quarterly, 12(3), 69-74. Miles, M. S., Carlson, J., & Brunssen, S. (1999a). The nurse parent support tool.
Journal of Pediatric Nursing, 14(1), 44-50. Miles, M. S., Carlson, J., & Brunssen, S. (1999b). The Nurse Parent Support Tool
Manual [http://www.unc.edu/depts/crci/instruments/npst/npstman.pdf]. Retrieved 21.8.02, 2002, from the World Wide Web:
Miles, M. S., Carlson, J., & Funk, S. G. (1996). Sources of support reported by
mothers and fathers of infants hospitalized in a neonatal intensive care unit. Neonatal Network - Journal of Neonatal Nursing, 15(3), 45-52.
206
Miles, M. S., D'Auria, J. P., Hart, E. M., Sedlack, D. A., & Watral, M. A. (1993). Parental role alterations experienced by mothers of children with a life-threatening chronic illness. In S. G. Funk & E. M. Tornquist & M. T. Champagne & R. A. Wiese (Eds.), Key aspects of caring for the chronically ill: hospital and home (pp. 281-289). New York: Springer Publishing Company Inc.
Miles, M. S., & Frauman, A. C. (1993). Nurses' and parents' negotiation of caregiving
roles for medically fragile infants: barriers and bridges. In S. G. Funk & E. M. Tornquist & M. T. Champagne & R. A. Wiese (Eds.), Key aspects of caring for the chronically ill: hospital and home. (pp. 239-270). New York: Springer Publishing Company.
Miles, M. S., Funk, S. G., & Kasper, M. A. (1991). The neonatal intensive care unit
environment: sources of stress for parents. AACN Clinical Issues in Critical Care Nursing, 2(2), 346-354.
Miles, M. S., Funk, S. G., & Kasper, M. A. (1992). The stress response of mothers
and fathers of preterm infants. Research in Nursing & Health, 15(4), 261-269. Miles, M. S., & Holditch-Davis, D. (1995). Compensatory parenting: how mothers
describe parenting their 3-year-old, prematurely born children. Journal of Pediatric Nursing: Nursing Care of Children & Families, 10(4), 243-253.
Miles, M. S., & Holditch-Davis, D. (1997). Parenting the prematurely born child:
pathways of influence. Seminars in Perinatology, 21(3), 254-266. Miles, M. S., Holditch-Davis, D., Scher, M., & Schwartz, T. (2002). A longitudinal
study of depressive symptoms in mothers of prematurely-born-infants. Paper presented at the The 13th Biennial International Conference on Infant Studies, Toronto, Canada.
Miles, M. S., Holditch-Davis, D. H., Burchinal, P., & Nelson, D. (1999c). Distress
and growth outcomes in mothers of medically fragile infants. Nursing Research, 48(3), 129-140.
Minde, K., Whitelaw, A., Brown, J., & Fitzhardinge, P. (1983). Effect of neonatal
complications in premature infants on early parent infant interactions. Developmental Medicine and Child Neurology, 25(6), 763-777.
Minuchin, S. (1974). Families and family therapy. Cambridge: Harvard University
Press. Moehn, D. G., & Rossetti, L. (1996). The effects of neonatal intensive care on
parental emotions and attachment. Infant-Toddler Intervention: the Transdisciplinary Journal, 6(3), 229-246.
207
Moran, M., Radzyminski, S. G., Higgins, K. R., Dowling, D. A., Miller, M. J., & Anderson, G. C. (1999). Maternal kangaroo (skin-to-skin) care in the NICU beginning 4 hours postbirth. MCN, American Journal of Maternal Child Nursing, 24(2), 74-79.
Morisset, C. E., Barnard, K. E., Greenberg, M. T., Booth, C. L., & Spieker, S. J.
(1990). Environmental influences on early language development: the context of social risk. Development and Psychopathology, 2, 127-149.
Mueller, D. P. (1980). Social networks: a promising direction for research on the
relationship of social environment to psychiatric disorder. Social Science and Medicine, 14A, 147-161.
Murray, L., & Cooper, P. J. (1997). Postpartum depression and child development.
New York: The Guilford Press. Murray, L., & Cooper, P. J. (1997). The role of infant and maternal factors in
postpartum depression, mother-infant interactions and infant outcome. In P. J. Cooper (Ed.), Postpartum Depression and Child Development (pp. 111-135). New York: The Guilford Press.
Najman, J., Williams, G., Bor, W., Anderson, M., & Morrison, J. (1994). Obsterrical
outcomes of aboriginal pregnancies at a major urban hospital. Australian Jounal of Public Health, 18, 185-189.
Newberger, E. H., Barkin, S. I., Leiberman, E. S., McCormick, M. C., Yllo, K., Gary,
L., et al. (1992). Abuse of pregnant women and adverse birth outcome: current knowledge and implications for practice. Journal of the American Medical Association, 267, 2370-2372.
NICHD, (1999). Chronicity of maternal depressive symptoms, maternal sensitivity,
and child functioning at 36 months. Developmental Psychology, 35(5), 1297-1310.
Nolan, M., Grant, G., & Keady, J. (1996). Understanding family care: a
multidimensional model of caring and coping. Buckingham: Open University Press.
O'Brien, M., Heron Asay, J., & McCluskey-Fawcett, K. (1999). Family functioning
and maternal depression following premature birth. Journal of Reproductive and Infant Psychology, 17(2), 176-188.
O'Hara, M. W. (1997). The nature of postpartum depressive disorders. O'Hara, M. W. (1997). The nature of postpartum depressive disorders. In P. cooper
(Ed.), Postpartum depression and child development (pp. 3-31). New York: Guilford.
208
O'Hara, M. W., Neunaber, D. J., & Zekoski, E. M. (1984). Prospective study of postpartum depression: prevalence, course, and predictive factors. Journal of Abnormal Psychology, 93(2), 158-171.
O'Hara, M. W., Rehm, L. P., & Campbell, S. B. (1982). Predicting depressive
symptomatology: cognitive-behavioral models and postpartum depression. Journal of Abnormal Psychology, 91(6), 457-461.
O'Hara, M. W., Rehm, L. P., & Campbell, S. B. (1983). Postpartum depression. A
role for social network and life stress variables. Journal of Nervous & Mental Disease, 171(6), 336-341.
O'Hara, M. W., Schlechte, J. A., Lewis, D. A., & Varner, M. W. (1991). Controlled prospective study of postpartum mood disorders: psychological, environmental, and hormonal variables. Journal of Abnormal Psychology, 100(1), 63-73.
O'Hara, M. W., & Swain, A. M. (1996). Rates and risk of postpartum depression-A
meta-analysis. O'Hara, M. W., Zekoski, E. M., Philipps, L. H., & Wright, E. J. (1990). Controlled
prospective study of postpartum mood disorders: comparison of childbearing and nonchildbearing women. Journal of Abnormal Psychology, 99(1), 3-15.
Olson, D. H., Sprenkle, D., & Russell, C. (1979). Circumplex model of marital and
family systems 1 : Cohesion and adaptability dimensions, family types and clinical application. Family Process, 18, 3-28.
Oppenheimer, G. M. (1996). Prematurity as a public health problem: US policy from
the 1920's to the 1960's. American Journal of Public Health, 86(6), 870-878. Parker, S., Greer, S., & Zuckerman, B. (1988). Double jeopardy: The impact of
poverty on early child development. Pediatric Clinics of North America, 35(6), 1227-1240.
Patterson, J. M. (1988). Families experiencing stress. Family Systems Medicine, 8,
421-434. Patterson, J. M. (1993). The role of family meanings in adaptation to chronic illness
and disability. In A. P. Turnbull & J. M. Patterson & S. K. Behr & D. L. Murphy & J. G. Marquis & M. J. Blue-Banning (Eds.), Cognitive coping, families and disability. Baltimore: Paul H. Brookes.
Patterson, J. M., Jernell, J., Leonard, B. J., & Titus, J. C. (1994). Caring for medically
fragile children at home: the parent-professional relationship. Journal of Pediatric Nursing: Nursing Care of Children & Families, 9(2), 98-106.
Patterson, J. M., & McCubbin, H. I. (1983). Chronic illness: family stress and coping.
In C. R. Figley & H. I. McCubbin (Eds.), Stress and the family (Vol. II: Coping with catastrophe, pp. 21-36). New York: Brunner/Mazel Publishers.
209
Paykel, E., Cooper, Z., Ramana, R., & Hayhurst, H. (1996). Life events, social support and marital relationships in the outcome of severe depression. Psychological Medicine, 26(1), 121-133.
Peacock, J. L., Bland, J. M., & Anderson, H. R. (1995). Preterm delivery: effects of
socioeconomic factors, psychological stress, smoking, alcohol, and caffiene. British Medical Journal, 311, 531-536.
Pearlin, L. I. (1989). The sociological study of stress. Journal of Health and Social
Behavior, 30, 241-256. Pearlin, L. I., & Schooler, C. (1978). The structure of coping. Journal of Health and
Social Behavior, 19, 2-21. Pederson, D. R., Bento, S., Chance, G. W., Evans, B., & Fox, A. M. (1987). Maternal
emotional responses to preterm birth. American Journal of Orthopsychiatry, 57(1), 15-21.
Perehudoff, B. (1990). Parents' perceptions of environmental stressors in the special
care nursery. Neonatal Network - Journal of Neonatal Nursing, 9(2), 39-44. Perry, B. D. (1997). Incubated in terror: neurodevelopmental factors in the "cycle of
violence." In J. D. Osofsky (Ed.), Children in a violent society (pp. pp. 124-149). New York: The Guilford Press.
Pierce, G. R., Sarason, B. R., Sarason, I. G., Joseph, H. J., & Henderson, C. A. (1996).
Conceptualizing and assissing social support in the context of the family. In G. R. Pierce & B. R. Sarason & I. G. Sarason (Eds.), Handbook of Social Support and the Family (pp. 3-42). New York: Plenum Press.
Pitts Berns, S., Geiser, R., & Levi, L. (1993). The changing family unit. In C. Kenner
& A. Brueggemeyer & L. Gunderson (Eds.), Comprehensive neonatal nursing: a physiologic perspective (pp. 69-79). Philadelphia: W.B. Saunders Company.
Plass, K. M. (1994). The evolution of parental roles in the nicu. Neonatal Network,
13(6), 31-33. Prichard, M., & Colditz, P. (2001). Optimising health outcomes for children at high
risk of neurodevelopmental disability in queensland. Herston, Brisbane: Perinatal Research Centre, Royal Women's Hospital Health Service District.
Quine, L., & Pahl, J. (1987). First diagnosis of severe handicap: a study of parental
reactions. Developmental Medicine & Child Neurology., 29, 232-242. Quine, L., & Pahl, J. (1991). Stress and coping in mothers caring for a child with
severe learning difficuties: a test of lazarus' transactional model of coping. Journal of Community and Applied Social Psychology, 1, 57-70.

210
Quittner, A. L., & DiGirolamo, A. M. (1998). Family adaptation to childhood disability and illness. In R. T. Ammerman & J. V. Campo (Eds.), Handbook of Pediatric Psychology and Psychiatry (Vol. 1, pp. 70-102). Boston: Allyn and Bacon.
Quittner, A. L., DiGirolamo, A. M., Michel, M., & Eigen, H. (1992). Parental
response to cysitc fibrosis: a contextual analysis of the diagnosis phase. Journal of Pediatric Psychology, 17, 683-704.
Raddish, M., & Merritt, T. A. (1998). Early discharge of premature infants. A critical
analysis. Clinics in Perinatology, 25(2), 499-520. Radke-Yarrow, M., Zahn-Waxler, C., Richardson, D., Susman, A., & Martinez, P.
(1994). Caring behavior in children of clinically depressed and well mothers. Child Development, 65, 1405-1414.
Radke-Yarrow, M. (1998). Children of depressed mothers: from early childhood to
maturity. New York: Cambridge University Press. Raeside, L. (1997). Perceptions of environmental stressors in the neonatal unit. British
Journal of Nursing, 6(16), 914-923. Redshaw, M., & Harris, A. (1995). Maternal perception of neonatal care. Acta
Paediatrica, 84, 593-598. Redshaw, M., Harris, A., & Ingram, J. (1994). A home from home? Regard for
parents in policy and practice in neonatal care. Child Health, 2, 79-86. Redshaw, M. E., Harris, A., & Ingram, J. C. (1996). Delivering neonatal care. The
neonatal unit as a working environment: A survey of neonatal unit nursing. Norwich: HMSO Publications Centre.
Reiger, K. M. (2001). Our bodies, our babies: the forgotten women's movement.
Melbourne: Melbourne University Press. Reighard, F. T., & Evans, M. L. (1995). Use of the Edinburgh Postnatal Depression
Scale in a southern, rural population in the United States. Progress in Neuro Psychopharmacology & Biological Psychiatry, 19(7), 1219-1224.
Rice, P. L. (1992). Stress and health (2nd ed.). California: Brooks/Cole Publishing
Company. Richardson, D. K., Gray, J. E., Gortmaker, S. L., Goldmann, D. A., Pursley, D. M., &
McCormick, M. C. (1998). Declining severity adjusted mortality: evidence of improving neonatal intensive care. Pediatrics, 102(4), 893-899.
Robinson, D. L. (1997). Family stress theory: implications for family health. Journal
of the American Academy of Nurse Practictioners, 9(1), 17-23.

211
Roman, L. A., Lindsay, J. K., Boger, R. P., DeWys, M., Beaumont, E. J., Jones, A. S., & Haas, B. (1995). Parent-to-parent support initiated in the neonatal intensive care unit. Research in Nursing & Health, 18(5).
Romito, P. (1986). The humanizing of childbirth: the response of medical institutions
to women's demand for change. Midwifery, 2, 135-140. Rubin, R. (1968). A theory of clinical nursing. Nursing Research, 17(210-212). Ruttenberg, W. B. (1999). Low income Latina mothers and their preterm, very low
birthweight infants: The impact of early mother-infant interactions on subsequent infant development and the caregiving environment. Dissertation Abstracts International: Section B: the Sciences & Engineering, 59(11-B), 6095.
Sameroff, A. J. (1993). Models of development and developmental risk. In C. Zeanah
(Ed.), Handbook of infant mental health (pp. 3-13). New York: Guilford. Sameroff, A. J., Bartko, W. T., Baldwin, A., Baldwin, C., & Seifer, R. (1998). Family
and social influences on the development of child competence. In M. Lewis & C. Feiring (Eds.), Families, risk, and competence (pp. 161-185). New Jersey: Lawrence Erlbaum Associates, Publishers.
Sameroff, A. J., & Chandler, M. J. (1975). Reproductive risk and the continuum of
caretaking casualty. In F. D. Horowitz (Ed.), Review of child development research (Vol. 4). Chicago: University of Chicago Press.
Sameroff, A. J., & Fiese, B. H. (1990). Transactional regulation and early
intervention. In S. J. Meisels & J. P. Shonkoff (Eds.), Handbook of early childhood intervention (pp. 119-302). Cambridge: Cambridge University Press.
Sameroff, A. J., & Fiese, B. H. (2000). Models of development and developmental
risk. (2nd ed.). New York: Guilford Press. Sameroff, A. J., Seifer, R., Barocas, R., Zax, M., & Greenspan, S. (1987). Intelligence
quotient scores of 4-year-old children: social-environmental risk factors. Pediatrics, 79(3), 343-350.
Sammons, W. A., & Lewis, J. M. (1985). Premature babies: a different beginning.
Missouri: The C.V. Mosby Company. Sander, L. W. (2000). Where are we going in the field of infant mental health? Infant
Mental Health Journal, 21(1-2), 5-20. Saunders, A. N. (1994). Changing nurses' attitudes toward parenting in the NICU.
Pediatric Nursing, 20(4), 392-394.

212
Schaffer, H. R. (1999). Understanding socialization: from unidirectional to bidirectional conceptions. In M. Bennett (Ed.), Developmental Psychology: Achievements and Prospects (pp. 272-288). Philadelphia: Psychology Press.
Schneewind, K. A., & Ruppert, S. (1998). Personality and family development. New
Jersey: Lawrence Erlbaum Associates, Publishers. Schraeder, B. D., Heverly, M. A., & O'Brien, C. (1996). The influence of early
biological risk and the home environment on nine-year outcome of very low birth weight. Canadian Journal of Nursing Research, 28(4), 79-95.
Schwarz, E. W. (1991). The engineering of childbirth: a new obstetric programme as
reflected in british obstetric textbooks. In J. Garcia & R. Kilpartick & M. Richards (Eds.), The Politics of Maternity Care: Services for Childbearing Women in Twentieth-Century Britian (pp. 47-60). Oxford: Clarendon Press.
Seideman, R. Y., Watson, M. A., & Corff, K. E. (1997). Parent stress and coping in
NICU and PICU. Journal of Pediatric Nursing, 12, 169-177. Seifer, R. (1995). Perils and pitfalls of high-risk research. Developmental Psychology,
31, 420-424. Shields-Poe, D., & Pinelli, J. (1997). Variables associated with parental stress in
neonatal intensive care units. Neonatal Network - Journal of Neonatal Nursing, 16(1), 29-37.
Shore, R. (1997). Rethinking the brain: new insights into early development. New
York: Families and Work Institute. Siegel, L. J. (1992). Conceptual and general issues: Overview. In A. M. La Greca &
L. J. Siegel & J. L. Wallander & C. E. Walker (Eds.), Stress and Coping in Child Health. New York: Guilford Press.
Sigman, M., Cohen, S. E., Beckwith, L., Asarnow, R., & Parmelee, A. H. (1992). The
prediction of cognitive abilities at 8 and 12 years of age from neonatal assessments of preterm infants. In S. L. Friedman & M. D. Sigman (Eds.), Annual advances in applied developmental psychology: the psychological development of low-birthweight children (Vol. 6, pp. 299-314). New Jersey: Ablex.
Silverman, W. A. (1980). Retrolental fibroplasia: a modern parable. New York:
Grune & Stratton. Singer, L. T., Davillier, M., Bruening, P., Hawkins, S., & Yamashita, T. S. (1996).
Social support, psychological distress, and parenting strains in mothers of very low birthweight infants. Family Relations, 45, 343-350.

213
Singer, L. T., Davillier, M., Preuss, L., Szekely, L., Hawkins, S., Yamashita, T., & Baley, J. (1996). Feeding interactions in infants with very low birth weight and bronchopulmonary dysplasia. Journal of Developmental & Behavioral Pediatrics, 17(2), 69-76.
Singer, L. T., Salvator, A., Guo, S., Collin, M., Lilien, L., & Baley, J. (1999).
Maternal psychological distress and parenting stress after the birth of a very low-birth-weight infant. Journal of the American Medical Association, 281(9), 799-805.
Singleton, R., Straits, C., & Straits, M. (1993). Approaches to social research. New
York: Oxford University Press. Slater, M. A., Naqvi, M., Andrew, L., & Haynes, K. (1987). Neurodevelopment of
monitored versus nonmonitored very low birthweight infants: the importance of family influences. Journal of Developmental and Behavioral Pediatrics, 8(5), 278-285.
Small, R., Astbury, J., Brown, S., & Lumley, J. (1994). Depression after childbirth.
Does social context matter? [see comments]. Medical Journal of Australia, 161(8), 473-477.
Spear, M. L., Leef, K., Epps, S., & Locke, R. (2002). Family reactions during infants'
hospitalization in the neonatal intensive care unit. American Journal of Perinatology, 19(4), 205-213.
Spiker, D., Ferguson, J., & Brooks-Gunn, J. (1993). Enhancing maternal interactive
behavior and child social competence in low birth weight, premature infants. Child Development, 64(3), 754-768.
Stamp, G. E., & Crowther, C. A. (1994). Postnatal depression: a South Australian
prospective survey. Australian & New Zealand Journal of Obstetrics & Gynaecology, 34(2), 164-167.
Stewart, D. E., & Cecutti, A. (1993). Physical abuse in pregnancy. Canadian Medical
Association Journal, 149, 1257-1263. Stein, A., Gath, D. H., Bucher, J., Bond, A., Day, A., & Cooper, P. J. (1991). The
relationship between post-natal depression and mother-child interaction. British Journal of Psychiatry, 158, 46-52.
Sterling, Y. M., Jones, L. C., Johnson, D. H., & Bowen, M. R. (1996). Parents'
resources and home management of the care of chronically ill infants. Journal of the Society of Pediatric Nurses, 1(3), 103-109.
Stowe, Z. N., & Nemeroff, C. B. (1995). Women at risk for postpartum-onset major
depression. American Journal of Obstetrics and Gynaecology, 173, 639-645.

214
Stuart, S., & O'Hara, M. W. (1995). Treatment of postpartum depression with interpersonal psychotherapy.
Tabachnick, B. G., & Fidell, L. S. (1996). Using Multivariate Statistics. New York:
HarperCollins College Publishers. Tesh, E. M., & Holditch-Davis, D. (1997). HOME inventory and NCATS: relation to
mother and child behaviors during naturalistic observations. Research in Nursing and Health, 20, 295-307.
Teti, D. M., & Gelfand, D. M. (1991). Behavioral competence among mothers of
infants in the first year: The mediational role of maternal self-efficacy. Child Development, 62(5), 918-929.
Teti, D. M., & Gelfand, D. M. (1997). Maternal cognitions as mediators of child
outcomes in the context of postpartum depression. In L. Murray & P. Cooper (Eds.), Postpartum depression and child development. (pp. 136-164). New York: The Guilford Press.
Teti, D. M., Gelfand, D. M., Messinger, D. S., & Isabella, R. (1995). Maternal
depression and the quality of early attachment: An examination of infants, preschoolers, and their mothers. Developmental Psychology, 31(3), 364-376
. Thompson, E. H., Jr., Futterman, A. M., Gallagher-Thompson, D., Rose, J. M., &
Lovett, S. B. (1993). Social support and caregiving burden in family caregivers of frail elders. Journal of Gerontology, 48(5), S245-254.
Thompson, R. J., & Gustafson, K. E. (1996). Adaptation to chronic childhood illness.
Washington DC: American Psychological Association. Thompson, R. J., Gustafson, K. E., Hamlett, K. W., & Spock, A. (1992). Stress,
coping, and family functioning in the psychological adjustment of mothers of children and adolescents with cystic fibrosis. Journal of Pediatric Psychology, 17, 705-724.
Thompson, R. J., Jr., Gustafson, K. E., Oehler, J. M., Catlett, A. T., Brazy, J. E., &
Goldstein, R. F. (1997). Developmental outcome of very low birth weight infants at four years of age as a function of biological risk and psychosocial risk. Journal of Developmental & Behavioral Pediatrics, 18(2), 91-96.
Thompson, R. J., Oehler, J. M., & Catlett, A. T. (1993). Maternal psychological
adjustment to the birth of an infant weighing 1,500 grams or less. Infant Behavior and Development, 16(4), 471-485.
Tulman, L., & Fawcett, J. (1988). Return of functional ability after childbirth. Nursing
Research, 37(2), 77-81. Van Riper, M. (2001). Issues in neonatal care. Family-provider relationships and
well-being in families with preterm infants in the NICU. Heart & Lung: Journal of Acute & Critical Care, 30(1), 74-84.
215
Varni, J. W., Katz, E. R., Colegrove, J. R., & Dolgin, M. (1996). Family functioning
predictors of adjustment of children with newly diagnosed cancer: A prospective analysis. Journal of Child Psychology and Psychiatry, 37(321-328).
Varni, J. W., & Wallander, J. L. (1988). Pediatric chronic disabilities: Hemophilia and
spina bifida as examples. In D. K. Routh (Ed.), Handbook of pediatric psychology (pp. 190-221). New York: Guilford Press.
Vasquez, E. (1995). Creating paths: living with a very-low-birth-weight infant.
JOGNN - Journal of Obstetric, Gynecologic, & Neonatal Nursing, 24(7), 619-624.
Vohr, B. R., & Msall, M. E. (1997). Neuropsychological and functional outcomes of
very low birth weight infants. Seminars in Perinatology, 21(3), 202-220. Wadhwa, P. D., Sandman, C. A., Porto, M., Dunkel-Schetter, C., & Garite, T. J.
(1993). The association between perinatal stress and infant birth weight and gestational age at birth: a prospective investigation. American Journal of Obstetrics and Gynecology, 169, 858-865.
Wagner, M. (1994). Pursuing the birth machine: the search for appropriate birth
technology. Camperdown: Ace Graphics. Walker, L. O., & Thompson, E. T. (1982). Mother infant play interaction scale. In S.
Smith-Humenick (Ed.), Analysis of Current Assessment Strategies on the Health Care of Young Children and Childbearing Families. Norwalk CT: Appleton-Century Crofts.
Walker, S. B. (1997). Neonatal nurses' views on the barriers to parenting in the
intensive care nursery -- a pilot study. Australian Critical Care, 10(1), 13-16. Walker, S. B. (1998). Neonatal nurses' views on the barriers to parenting in the
intensive care nursery. Australian Critical Care, 11(3), 86-91. Wallerstedt, C., & Higgins, P. (1996). Facilitating perinatal grieving between the
mother and the father. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 25(5), 389-394.
Watson, J. P., Elliott, S. A., Rugg, A. J., & Brough, D. I. (1984). Psychiatric disorder
in pregnancy and the first postnatal year. British Journal of Psychiatry, 144, 453-462.
Watson, J. S. (1973). Smiling, cooing, and "the game". In L. J. Stone & H. T. Smith &
L. B. Murphy (Eds.), The Competent Infant: Research and Commentary (pp. 1087-1096). New York: Basic Books.

216
Webster, J., Linnane, J., Dibley, L., Starrenburg, S., Roberts, J., & Hinson, J. (1997). The impact of screening for risk factors associated with postnatal depression. Journal of Qualitative Clinical Practice, 17, 65-71.
Weisglas-Kuperus, N., Baerts, W., Smrkovsky, M., & Sauer, P. J. J. (1993). Effects of
biological and social factors on the cognitive development of very low birth weight children. Pediatrics, 92(5), 658-665.
Wereszczak, J., Miles, M. S., & Holditch-Davis, D. (1997). Maternal recall of the
neonatal intensive care unit. Neonatal Network - Journal of Neonatal Nursing, 16(4), 33-40.
Werner, E. E. (1997). Vulnerable but invincible: high-risk children from birth to
adulthood. Acta Paediatrica. Supplement, 422, 103-105. Whiffen, V. E., & Gotlib, I. H. (1989). Infants of postpartum depressed mothers:
Temperament and cognitive status. Journal of Abnormal Psychology, 98(3), 274-279.
Wijnroks, L. (1999). Maternal recollected anxiety and mother-infant interaction in
preterm infants. Infant Mental Health Journal, 20(4), 393-409. Wilfong, E. W., Saylor, C., & Elksnin, N. (1991). Influences on responsiveness:
Interactions between mothers and their premature infants. Infant Mental Health Journal, 12(1), 31-40.
Wille, D. E. (1991). Relation of preterm birth with quality of infant-mother
attachment at one year. Infant Behavior and Development, 14(2), 227-240. Willis. (1989). Medical dominance : the division of labour in Australian health care
(2nd ed.). Sydney: Allen & Unwin. Wills, T. A., Blechman, E. A., & McNamara, G. (1996). Family support, coping and
competence. In E. M. Hetherington & E. Blechman (Eds.), Stress, coping, and resiliency in children and families (pp. 107-133). New Jersey: Lawrence Erlbaum Associates, Publishers.
Wolff, P. H. (1965). The development of attention in young infants. Annals of the
New York Academy of Sciences, 118, 815-830. Wyly, M. V. (1995a). Family-centered care in the NICU. In M. V. Wyly (Ed.),
Premature infants and their families. Developmental interventions (pp. 225-253). San Diego: Singular Publishing Group, Inc.
Wyly, M. V. (1995b). Parent-preterm infant interactions. In M. V. Wyly (Ed.),
Premature infants and their families: developmental interventions (pp. 145-169). San Diego: Singular Publishing Group, Inc.
Wyly, M. V. (1997). Infant Assessment. Colorado: Westview Press.

217
Yoder, P. J. (1987). Relationship between degree of infant handicap and clarity of infant cues. American Journal of Mental Deficiency, 91, 639-641.
Younger, J. B., Kendell, M. J., & Pickler, R. H. (1997). Mastery of stress in mothers
of preterm infants. Journal of the Society of Pediatric Nurses, 2(1), 29-35. Zahr, L. (1991). Correlates of mother-infant interaction in premature infants from low
socioeconomic backgrounds. Pediatric Nursing, 17(3), 259-264. Zarling, C. L., Hirsch, B. J., & Landry, S. (1988). Maternal social networks and
mother-infant interactions in full-term and very low birthweight, preterm infants. Child Development, 59(1), 178-185.
Zeanah, C. H., Boris, N. W., & Larrieu, J. A. (1997). Infant development and
developmental risk: a review of the past 10 years. Journal of the American Academy of Child & Adolescent Psychiatry, 36(2), 165-178.
Zelkowitz, P., & Milet, T. H. (1995). Screening for post-partum depression in a
community sample. Canadian Journal of Psychiatry - Revue Canadienne de Psychiatrie, 40(2), 80-86.