questions for further consideration - basic science ...medu.s3.amazonaws.com/06304726/qfc- basic...
TRANSCRIPT

CLIPP: QUESTIONS FOR FURTHER CONSIDERATION BASIC SCIENCE RESOURCE GUIDES
CLIPP 1: PRENATAL AND NEWBORN VISITS – THOMAS 1-5. Rose has a history of asthma. In her 24th week of pregnancy, she presents with an
asthma exacerbation in moderate respiratory distress. You would typically start her on a short course of oral prednisone as part of her treatment – is it safe to do so during her pregnancy? The FDA has created a rating system for use of drugs in pregnancy – describe this rating system. One month later, Rose presents in premature labor, and the obstetrician suggests treating her with betamethasone – why? (basic science)
CLIPP 2: INFANT WELL CHILD (2, 6 AND 9 MONTHS) - ASIA 2-5. Compare radiation doses of an abdominal CT scan as compared to an abdominal
radiograph (“KUB”). (basic science) CLIPP 3: 3-Year-old well child check - Benjamin 3-4. You are seeing a 2-week-old girl in clinic for routine health maintenance visit. You review
the results of newborn screening: hemoglobin electrophoresis reads FA + hemoglobin Barts. What is Hb Barts? What is this child’s diagnosis? What clinical implications does this diagnosis carry? (basic science)
CLIPP Case 4: 8-YEAR-OLD WELL-CHILD CHECK - JIMMY 4-4. Discuss the indications for lipid screening in children. Which components of a lipid
screen are affected by fasting? (basic science) 4-5. Describe the mechanisms of action of cholestyramine vs. niacin vs. lovastatin vs.
ezetimibe in treating hyperlipidemia (basic science) CLIPP 5: 16-YEAR-OLD GIRL'S HEALTH MAINTENANCE VISIT - BETSY 5-5. Describe the role of vWF in normal clotting. How does desmopressin help control
bleeding in patients with von Willebrand’s disease? (basic science) CLIPP 6: 16-YEAR-OLD BOY'S PRE-PARTICIPATION EVALUATION - MIKE 6-4. A teenage boy passed out at football practice this afternoon. On exam you hear a
systolic murmur. If he has hypertrophic cardiomyopathy, would you expect squatting to make his murmur more or less prominent? Why? What about a Valsalva maneuver? (basic science)
CLIPP 7: NEWBORN WITH RESPIRATORY DISTRESS - ADAM 7-4. Why is the infant of a diabetic mother macrosomic? (basic science) 7-5. Discuss how steroids work to promote fetal lung maturation when given prior to delivery
in cases of premature labor. (basic science)

2
CLIPP Case 8: 6-DAY-OLD WITH JAUNDICE - MEGHAN 8-4. How does phototherapy facilitate excretion of bilirubin? Is this effective for both direct
and indirect hyperbilirubinemia? (basic science) CLIPP Case 9: 2-WEEK-OLD WITH LETHARGY - CRIMSON 9-3. At age 2 months, an infant with congenital hypothyroidism has a markedly elevated TSH.
Parents report adherence to the daily dose of levothyroxine, and your records indicate that the dose is appropriate. What might be the cause of the elevated TSH? (basic science)
CLIPP Case 10: 6-MONTH-OLD WITH A FEVER - HOLLY 10-4. Discuss the differences between how the immune system functions in a 6-month-old
compared to a 6-year-old. How would these differences affect your evaluation and management of patients at different ages? (basic science) Resource Guide Pending
CLIPP CASE 11: 5-YEAR-OLD WITH FEVER AND ADENOPATHY - JASON 11-5. Two children come to the office with fever, sore throat; both have exudative pharyngitis
and positive rapid antigen tests for group A Strep. One patient also has diffuse, rough erythroderma; the other child does not. What accounts for the different clinical manifestation between these two patients? How would you treat each of these patients? (basic science)
CLIPP 12: 10-MONTH-OLD WITH A COUGH - ANNA 12-3. If a child swallows a coin, how can you tell on x-ray whether it is in the trachea or the
esophagus? What are the indications for extracting a foreign body from the GI tract? From the trachea? Describe the locations within the esophagus where foreign bodies are most likely to lodge. (basic science)
12-4. Racemic epinephrine typically provides prompt improvement for patients with croup, while nebulized albuterol typically does not (and may even worsen symptoms) – why? (basic science)
CLIPP 13: 6-YEAR-OLD WITH CHRONIC COUGH - SUNITA No basic science QFC CLIPP Case 14: 18-MONTH-OLD WITH CONGESTION - REBECCA 14-4. A 12-month-old girl is diagnosed with acute otitis media and prescribed amoxicillin
250mg/5mL 1tsp po bid. Two days later she is still intermittently febrile and fussy; repeat exam shows erythematous, bulging TM’s bilaterally. Give at least three possible explanations for this treatment failure. (basic science)
3
CLIPP 15: Two siblings with vomiting–Caleb (age 4 years) and Ben (age 8 weeks) 15-4. A 3-week-old boy with a two-week history of progressive vomiting is found to have
pyloric stenosis on ultrasound. He appears to be 10% dehydrated on exam; admission electrolytes reveal Na 132 / K 4.1/ Cl 89 / HCO3 29 / BUN 14 / creatinine 0.4. Most dehydrated patients are acidotic – why? Why isn’t this patient? (basic science)
CLIPP 16: 7-YEAR-OLD WITH ABDOMINAL PAIN AND VOMITING - ISABELL 16-4. An 8-year-old girl is admitted in DKA. Her initial labs show Na 131 / HCO3 8 / Glucose
780. Is she considered hyponatremic? Two hours later, repeat labs show Na 133 / glucose 450. Is this change in sodium reassuring or worrisome? Why? (basic science)
16-5. After her discharge from the hospital, Isabella’s blood glucose remains under excellent control except after soccer games, when her glucose routinely drops to the 50’s. Why? How would you manage Isabella? (basic science)
CLIPP 17: 3-YEAR-OLD REFUSING TO WALK- EMILY 17-4. Discuss the pathophysiology of septic arthritis and osteomyeltis in children. How is it
different than that seen in adults? (basic science) 17-5. What if Emily presented with a fever to 104 for the previous 4 days, had elevated
inflammatory markers (CRP 5.3 (normal < 0.8; ESR 50 (normal <10)) and you decided she has septic arthritis. What antibiotics would you give her? Explain your rationale for antibiotic choice, including which microbes you are covering and how well antibiotics penetrate into joint spaces and bones. (basic science)
CLIPP 18: 2-WEEK-OLD WITH POOR WEIGHT GAIN - TYLER 18-4. Discuss the effects of prostaglandin E and indications for its use in congenital heart
disease (basic science) 18-5. Describe how to perform a hyperoxia test on a newborn with cyanosis. How does a
response to oxygen affect your differential diagnosis? (basic science) 18-6. How do each of the following affect a patient’s cardiac exam: inhalation vs exhalation?
Lying vs standing? Valsalva maneuver/squatting? (basic science) CLIPP 19: 16-MONTH-OLD WITH A FIRST SEIZURE – IAN 19-3. Suppose that Ian presented with the same symptoms but was afebrile. Discuss the
classification of seizures. Relate the clinical manifestations to your knowledge of neuroanatomy. Describe how the clinical manifestations of the seizures reflect the function of the part of the brain affected (e.g. if someone has a seizure originating in the temporal area, what types of clinical manifestations would you expect?) (basic science)
19-4. Discuss how the commonly used anti-epileptics are metabolized. What types of drug-drug interactions will you need to monitor for? (basic science)
19-5. Compare and contrast different CSF profiles indicating viral vs. bacterial vs. fungal/tuberculous infections of the central nervous system. Review the factors that cause alterations in the CSF during infection for glucose, protein and white blood cell levels. (basic science) Resource Guide/s Pending
4
CLIPP 20: 7-YEAR-OLD WITH HEADACHES – NICHOLAS 20-3. Discuss the mechanisms of pain with headaches due to migraines, tension headaches
and headaches due to trauma. How would you present this information to parents? (basic science)
20-4. Discuss the mechanisms of action for common treatments of migraine headaches in children (basic science)
20-5. Review the pathological findings in common brain tumors seen in children (consider using slides from pathology department to augment this discussion) (basic science)
CLIPP 21: 6-YEAR-OLD BOY WITH BRUISING - ALEX 21-4. Alex underwent a renal biopsy because he continued to have persistent hematuria,
developed proteinuria and some mild hypertension. Describe what you would expect to find on the pathology slides from the renal biopsy. Discuss how these findings explain his ongoing problems. (basic science)
21-5. Discuss the pathophysiology of the different causes of thrombocytopenia in children [ITP, infection associated (viral or bacterial), malignancy, autoimmune disease, genetic disorders]. (basic science)
CLIPP Case 22: 16-YEAR-OLD WITH ABDOMINAL PAIN - MANDY 22-7. Discuss the mechanisms of action for the common antibiotics used when treating STIs.
(basic science) CLIPP 23: 11-YEAR-OLD WITH LETHARGY AND FEVER - SARAH 23-4. Discuss the pathogenesis (how people become ill) with meningococcemia. What
implications does this have on recommendations about immunizations against this organism (students will have to find out how good the vaccine is and how long protection lasts)? (basic science)
CLIPP 24: 2-YEAR-OLD WITH ALTERED MENTAL STATUS - Madelyn 24-3. Discuss the mechanisms for toxicity in tri-cyclic overdose. Discuss the mechanism for
successful alkalinization in ingestions. (basic science) CLIPP 25: 2-MONTH-OLD WITH APNEA - JEREMY 25-4. Discuss the underlying mechanisms/pathophysiology of apnea for the following pediatric
syndromes: obstructive apnea, apnea associated with seizures, apnea associated with infection (e.g. pertussis, RSV) and apnea associated with arrhythmia. (basic science)
CLIPP 26: 9-WEEK-OLD WITH FAILURE TO THRIVE- BOBBY 26-9. Explain the principles underlying various screening and diagnostic tests for cystic
fibrosis, including newborn screening, sweat chloride testing, and genetic testing? (new question added to pool) (basic science)

5
CLIPP 27: 8-YEAR-OLD WITH ABDOMINAL PAIN - JENNY 27-4. As noted in the case, Jenny’s flares become more common at age 12 years. You note
that her Hb is 8.5, MCV 92. What underlying pathophysiology might explain this finding? (basic science)
CLIPP 28: 18-MONTH-OLD WITH WITH DEVELOPMENTAL DELAY - ANTON 28-4. Discuss the neuro-anatomical correlations for the common forms of cerebral palsy.
(basic science) CLIPP 29: INFANT WITH HYPOTONIA - DANIEL 29-4. Describe the embryology of common cardiac defects seen in patients with Down
syndrome. What physical examination finding would you expect with these disorders? (basic science)
29-5. Discuss the different techniques used to confirm chromosomal abnormalities. Review the structure of chromosomes, methods to perform the tests and indications for testing. (basic science)
CLIPP 30: 2-YEAR-OLD WITH SICKLE CELL DISEASE - GERARDO 30-4. Gerardo’s peripheral blood smear shows Howell-Jolly bodies – what does this finding
represent? (basic science) 30-6. How does hydroxyurea help abate the clinical manifestations of sickle cell disease?
(basic science) CLIPP 31: 5-YEAR-OLD WITH PUFFY EYES - KATIE 31-4. Describe the considerations for immunizing a patient who is receiving/recently received
treatment with corticosteroids. (basic science) CLIPP 32: DERM CLINIC No QFC’s have been written for this case
6
MEDICATION SAFETY IN PREGNANCY CLIPP QFC 1-5 – QFC Basic Science Resource Guide
Erin Frank, MD Rose has a history of asthma. In her 24th week of pregnancy, she presents with an asthma exacerbation in moderate respiratory distress. You would typically start her on a short course of oral prednisone as part of her treatment – is it safe to do so during her pregnancy? The FDA has created a rating system for use of drugs in pregnancy – describe this rating system. One month later, Rose presents in premature labor, and the obstetrician suggests treating her with betamethasone – why? Drug Safety in Pregnancy: The FDA has created a rating system to guide medication use during pregnancy. For many medications, few well-controlled studies regarding safety during pregnancy are available. Nonetheless, the FDA ratings are based on the best available data and categorize the risk-benefit ratio for each medication. There are 5 categories: • Category A includes drugs that have been well studied in pregnant women and show no risk
to the fetus during pregnancy. • Category B includes those medications that have been studied in animal models and show
no risk to the fetus. These medications often do not have adequate human trials. • Category C include those medications where animal models have shown some risk to the
fetus however the benefits of use may outweigh the risks to the developing baby in certain women.
• Category D medications have shown risk to the fetus based on studies in humans but again the risks to the fetus and benefits to the woman must be weighed.
• Category X medications have been shown to have significant adverse effects on the fetus including fetal anomalies and should not be used in pregnant women despite any potential benefits.
The effects of each medication vary on its ability to cross the placental barrier and then its effects on the developing fetus. Prednisone, commonly used for treatment of asthma exacerbations, carries a category C classification with the FDA. There are some studies which have shown a slightly increased risk of preterm delivery, pre-eclampsia and small birth weight babies with prednisone during pregnancy. However, in severe asthma the benefit of treating the mother may outweigh the risk to the developing fetus, as the risks of complications from a severe asthma exacerbation pose a greater risk to the fetus (including poor oxygenation and risk of preterm delivery). Betamethasone Therapy in Preterm Labor: The FDA rating system described above deals with the question of fetal safety in the context of medications used for maternal benefit. Medications may also be given to pregnant women explicitly for the purpose of delivering therapy to the fetus.

7
Corticosteroid therapy given to women in premature labor has been shown to improve lung function as well as decrease the risk of intra-ventricular hemorrhage in preterm infant. In several studies, betamethasone has been shown to have the best results with the fewest complications as compared to other glucocorticoids. Betamethasone given to the mother readily crosses the placenta, an obvious prerequisite for fetal therapy. Corticosteroid use, and specifically the use of betamethasone, increases surfactant production in the premature infant’s lungs. This results in improved airway compliance and decreased surface tension within the alveoli. It is also felt to decrease cerebral overcirculation, decreasing the risk of cerebral hemorrhage. Betamethasone is given as an intramuscular injection to women who present in preterm labor, ideally at least 12-24 hours prior to delivery. This allows adequate time to cross the placental blood barrier and have the desired effect within the fetus’s developing lungs. Dosing protocols vary, and additional dosing is controversial, as recurrent dosing may potentially affect fetal growth, hormonal axis and cognitive development. Despite these potential risks, however, the benefit is thought to greatly outweigh the potential risks. References: Dalziel, Robert. "Antenatal Corticosteroids for Accelerating Fetal Lung Maturation for Women at Risk of Preterm Birth (Review)." The Cochrane Library 3 (2006): 1-145.
8
RADIATION WITH COMMON IMAGING MODALITIES CLIPP QFC 2-5 – Basic Science Resource Guide
Erin Frank, MD Compare radiation doses of an abdominal CT scan as compared to an abdominal radiograph (“KUB”). The wide range of imaging modalities at our disposal makes it easier to diagnose various medical conditions than ever before. However, when choosing an imaging technique all possible risks and benefits must be considered. For children who are still growing and developing one of the biggest concerns is the amount of ionizing radiation exposure. Use of ionizing radiation: X-ray radiation falls along the electromagnetic radiation wavelength. X-ray photons used in medical imaging are formed from reactions within linear accelerators or X-ray generators. X-ray radiation involves release of an electron that produces the photon used in imaging. Within the X-ray tubing, a stream of electrons is emitted from the cathode and ultimately reacts with the tubes metal anode. This results in a release of both heat energy and X-rays. These X-rays are streamlined and directed directly at the part of the body being imaged. Ionizing radiation has long been used when imaging the human body. In a traditional radiograph, the part of the body that is of interest to the physician is placed between radiographic film and an X-ray pulse source to obtain the image. The short pulses of x-ray waves penetrate the tissue and continue on to expose to film behind it. Areas that contain a higher density of electrons such as bone absorb much of the radiation while other areas allow complete penetration. Bone contains more calcium and other minerals leading to the increased density of electrons. This is responsible for the varying appearance of different tissues on a plain film. This same principle applies to many sources of radiation imaging. Each tissue within the body absorbs a particular amount of radiation and produces a specific translucency on imaging. This can help identify normal anatomy as well as pathology related to bone and soft tissue. In addition, contrast can be administered when it is necessary to look enhance certain organs (e.g. GI tract, bladder) or evaluate vasculature. Computed Tomography: X-ray computed tomography, or CT scan, utilizes two-dimensional X-ray technology along with computer processing to produce a three-dimensional image of the human body. A series of X-ray images centered around a single axis of rotation are obtained. These images are then processed by the computer’s tomography software to produce a three dimensional image of the patient’s anatomy. These images can then be focused on the area of interest and evaluated in axial, sagittal and coronal planes. In addition, CT scans are able to detect smaller differences in tissue density than any plain radiograph thereby providing more information regarding soft tissue changes. Radiation exposure in Plain Radiographs vs. CT: Typical plain radiographic imaging, such as a single view KUB or Chest Xray, exposes the patient to 0.1 mSv (milli Sievert). In a study such as an abdominal CT scan, the patient receives up to 3-5 mSv of radiation. This increase in radiation dose poses a potential risk for cancer

9
development in exposed patients. Multiple organ systems have been studied to determine their total radiation exposure as well as lifetime risk attributed to this increased radiation exposure. In children there seems to be an increase in overall cancer risk from radiation specific to the body system imaged. In abdominal CT imaging, the highest doses of radiation exposure as well as highest attributable cancer risk occur within the colon. There are potential risks of both solid tumors as well as leukemia following radiation exposure, and some children with a genetic predisposition are more likely to develop oncologic changes from basic imaging techniques. Clinical Correlation: When imaging patients, consideration needs to be given to the risks of radiation exposure weighed against the potential benefits of the study. In children the radiation exposure may have greater lifetime effects. Specific protocols taking into account the patient’s age and size should be implemented for all children undergoing radiographic imaging. Specific techniques to filter the radiation beam and limit number of exposures should be implemented for all patients in the pediatric population. Finally, whenever possible, imaging techniques without significant radiation exposure such as MRI and Ultrasound should be implemented for pediatric patients. References: Alzen G, Benz-Bohm G: Radiation protection in pediatric radiology. Dtsch Arztebl Int 2011; 108(24): 407–14. DOI: 10.3238/arztebl.2011.0407 Feng, Shi-Ting, Martin Wai-Ming Law, Bingsheng Huang, Sherry Ng, Zi-Ping Li, Quan-Fei Meng, and Pek-Lan Khong. "Radiation Dose and Cancer Risk from Pediatric CT Examinations on 64-slice CT: A Phantom Study." European Journal of Radiology 76.2 (2010): E19-23. Rezak, Amy. "Decreased Use of Computed Tomography With a Modified Clinical Scoring System in Diagnosis of Pediatric Acute Appendicitis." Archives of Surgery 146.1 (2011): 64-67.

10
HEMOGLOBIN ELECTROPHORESIS ON NEWBORN SCREENING CLIPP QFC 3-4 – Basic Science Resource Guide
Michael Dell, MD
You are seeing a 2 week old girl in clinic for routine health maintenance visit. You review the results of newborn screening: hemoglobin electrophoresis reads FA + hemoglobin Barts. What is Hb Barts? What is this child’s diagnosis? What clinical implications does this diagnosis carry? The thalassemias are a group of disorders characterized by anemia due to the decreased production of one of the globin chains required for hemoglobin synthesis. These are quantitative abnormalities, unlike qualitative disorders such as sickle cell disease in which abnormal hemoglobin is produced. NORMAL HEMOGLOBIN SYNTHESIS Hemoglobin is synthesized from iron and a tetramer of globin chains. A normal tetramer, in turn, is comprised of two globin chains from the alpha family, encoded on chromosome 16 (including Ɛ and two α genes) and two globin chains from the beta family encoded on chromosome 11 (including ƌ, Ɣ, and ß genes): Embryonic Hb: α2Ɛ2 Fetal Hb (HbF): α2Ɣ2 Adult Hb (HbA): α2ß2 Adult Hb 2 (HbA2): α2ƌ2 HEMOGLOBIN ELECTROPHORESIS Qualitative hemoglobin electrophoresis describes all types of hemoglobin detected in order of descending frequency. Since most adults without an underlying disorder of hemoglobin synthesis have a combination of Hb A and Hb A2, electrophoresis results would read A-A2. Quantitative hemoglobin electrophoresis reports not only the types of hemoglobin detected but the relative amounts of each. Most adults have 95-98% Hb A and 2-3% Hb A2. In ß-thalassemia trait, in which the patient is lacking one of the two normal ß genes, ß chain synthesis is diminished and the relative proportion of HbA2 increases: a quantitative hemoglobin electrophoresis with >5% HbA2 in patient with microcytic anemia confirms a diagnosis of ß-thalassemia trait. In α- thalassemia, however, all forms of hemoglobin are equally affected by a paucity of α chains (see normal Hb synthesis). The relative proportion of hemoglobins reported by quantitative electrophoresis, therefore, will not give any clue toward the diagnosis of α- thalassemia. In newborns, however, underproduction of α chains results in an excess of Ɣ chains (the other globin chain involved in synthesis of HbF). These excess Ɣ chains aggregate into Ɣ4 tetramers, a dysfunctional hemoglobin known as Hb Barts, which may be detected in small amounts on newborn screening tests that include hemoglobin electrophoresis. Once HbF production is down-regulated, typically after 6 months of age, Hb Barts is typically no longer detectable. CLINICAL SIGNIFICANCE Patients lacking both ß genes have ß- thalassemia major, also known as Cooley’s anemia. Anemia is severe, classically with lifelong dependence on transfusions to maintain adequate hemoglobin levels. Patients lacking only one ß gene have ß- thalassemia minor (aka ß thalassemia intermedia), characterized by mild-moderate microcytic anemia. Since normal adults have four α genes, there are more α- thalassemia phenotypes. Absence of all α genes is incompatible with life, resulting in fetal hydrops. Absence of three α genes results in α- thalassemia major, a severe anemia also known as Hb H disease because of the presence

11
of dysfunctional ß4 tetramers (hemoglobin H). Hemoglobin H is typically only detected with this severe paucity of α chains. Absence of two α genes results in α- thalassemia minor/intermedia, characterized by mild-moderate microcytic anemia often confused with iron deficiency. By the time this is detected on routine hemoglobin screening at health maintenance visits between 9-12 months of age, the hemoglobin electrophoresis is no longer useful in diagnosing α- thalassemia. Looking back to the newborn screen and the presence of Hb Barts may be the only definitive evidence of decreased α chain production. Patients missing only one α gene are silent α- thalassemia carriers: the single missing gene does not cause anemia and is of significance only in light of reproductive implications. References Cunningham, MJ. Update on Thalassemia: Clinical Care and Complications. Hematology/Oncology Clinics of North America - 24(1) February 2010. Sankaran, VG and DG Nathan. Thalassemia: An Overview of 50 Years of Clinical Research. Thalassemia: An Overview of 50 Years of Clinical Research. Hematology/Oncology Clinics of North America 24(6) December 2010.

12
HYPERLIPIDEMIA IN CHILDREN CLIPP QFCs 4-4 & 4-5 –Basic Science Resource Guide
Erin Frank, MD Discuss the indications for lipid screening in children. Which components of a lipid screen are affected by fasting? Describe the mechanisms of action of cholestyramine vs. niacin vs. lovastatin vs. ezetimibe in treating hyperlipidemia. LIPID SCREENING Dyslipidemias are a group of conditions with resultant elevations in total cholesterol, low-density lipoproteins (LDL) or triglycerides (TG). They can result from familial inherited conditions or as a result of poor dietary and lifestyle choices. Lipid screening involves evaluation of blood serum levels of total cholesterol as well as the individual components. These include high-density lipoproteins (HDL), low-density lipoproteins (LDL) and very low-density lipoproteins (VLDL). In addition, it includes measurement of serum triglyceride (TG) levels. Recommendations for lipid screening in children and adolescents: New guidelines recommend universal screening between 9-11 years of age irrespective of risk factors. There are no recommendations for screening for dyslipidemia in children under age 2 years. For children 2-8 years or 12-16 years old, screening is indicated only for those with a significant family history of early heart attack, stroke or known coronary blockage or parental history of dyslipidemia. In addition, screening is recommended if the child has high risk medical conditions such as diabetes or hypertension. Universal screening should then resume over age 17. Fasting State: In the non fasting state, there is a transient decrease in both LDL and HDL cholesterol, as well as transient rise in TG concentration depending on the type and amount of food ingested. After eating there is an increase in chylomicrons within the serum which are responsible for these changes. Traditionally, lipid evaluation has been completed in the fasting state. Recent data suggests that the differences found on screening panels between the fasting and non-fasting state are small and not clinically significant. This may make it easier to obtain samples in a greater number of patients. HYPERLIPIDEMIA THERAPY In patients with significant alterations in lipid metabolism, all medication options must be considered. There are multiple classes of lipid-lowering medications, each with different mechanisms of action designed to target specific pathways of lipid metabolism. Cholestyramine: Cholestyramine works as a bile acid sequestrant. It binds bile acid within the intestine, decreasing reabsorption through the enterohepatic circulation. In turn, the body must convert more cholesterol into bile acids, which decreases the circulating hepatic cholesterol supply. The
13
most significant effect of cholestyramine is to decrease low-density lipoprotein (LDL) cholesterol, while triglycerides may be mildly increased. Niacin: Niacin works on adipose tissue to prevent the release of free fatty acids. This results in decreased production of LDL cholesterol. In addition, there is some effect on increasing high-density lipoprotein (HDL) by decreasing the breakdown of HDL cholesterol. Together the overall effect is to reduce triglycerides and LDL as well as increase HDL. Lovastatin (statins): Lovastatin is one of several medications within the statin class, or HMG-CoA reductase inhibitors. These medications block cholesterol synthesis within the cells of the liver. This decreases the amount of cholesterol produced within hepatic cells and leads to up regulation of the LDL receptors. The primary effect of statins is to lower LDL cholesterol, but increases in HDL cholesterol have also been reported. Ezetimibe: Ezetimibe blocks intestinal absorption of cholesterol. It decreases the available cholesterol and plant sterols available to the hepatic cholesterol supply and has been shown to up regulate LDL receptors. This results in a decrease in largely the LDL cholesterol. Recommendations for use of lipid lowering therapy in children: Lipid lowering therapy with the use of medications is not currently recommended in children under age 10 with few exceptions. In children age 10 and older, it is recommended that initial lab values are confirmed with repeat samples and a detailed family history assessment be completed to evaluate risk factors. All children with elevated LDL cholesterol and elevated triglycerides initially should be managed with dietary changes and increased activity if applicable. For children with high-risk histories, co-morbid medical conditions or significantly elevated LDL (>190) despite dietary modifications, pharmacotherapy should be started with a statin as first-line treatment. Persistently elevated triglycerides despite dietary changes should result in addition of fish oil supplements and consideration of niacin therapy based on the level of elevation. Within the patient’s history, details should be obtained including family history of early cardiovascular disease or sudden death. In addition, there are personal risk factors that place the patient at higher risk including smoking, hypertension, and significantly elevated BMI (>97th%). Specific medical conditions including diabetes mellitus, chronic kidney disease, history of heart transplant and history of Kawasaki disease with aneurysm formation are considered significant risk factors, and recommendations currently encourage more aggressive treatment of dyslipidemia in these populations. Evaluating each patient with consideration of their risk factors helps to guide the use of cholesterol lowering medications. Dietary changes remain first line for children of all ages, however these specific risk factors can help guide clinicians in management of cholesterol in more complex patients.

14
References: Haney EM, Huffman LH, Bougastos C, Freeman M, Steiner RD, Nelson ND. Screening and treatment for lipid disorders in children and adolescents: systematic evidence review for the US preventive Services Task Force. Pediatrics. 2007 Jul: 120 (1): e189-214.Review. US Preventative Services Task Force. Screening for lipid disorders in children: US Preventive Services Task Force recommendation statement. Pediatrics. 2007 Jul: 120 (1) e215-9. Kavey, Rae Ellen W., Denise G. Simons-Morton, and Janet M. De Jesus. "Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report." Pediatrics 128 (2011): S1-S44. Print. Steiner, Michael., et. al. "Fasting Might Not Be Necessary Before Lipid Screening: A Nationally Representative Cross-Sectional Study." Pediatrics 128 (2011): 463-70.

15
von WILLEBRAND FACTOR/ TREATMENT OF von WILLEBRAND DISEASE CLIPP QFC 5-5 – QFC Basic Science Resource Guide
Erin Frank, MD Describe the role of von Willebrand Factor (vWF) in normal clotting. How does desmopressin help control bleeding in patients with von Willebrand’s deisease? Normal clotting involves activation of von Willebrand factor and platelet aggregation, with subsequent activation of soluble clotting factors and production of thrombin. Whereas bleeding disorders such as hemophilia are caused by abnormal amount or function of clotting factors, patients with von Willebrand disease have deficiencies in platelet activation and formation of the platelet clot. Von Willebrand Factor: Von Willebrand Factor (vWF) is a large glycoprotein which plays a role in achieving hemostasis. It is produced by the vascular endothelium within the Weibel-Palade bodies. Several monomers of vWF bind together within the golgi apparatus to form much larger vWF mutlimers that are functional within the circulating serum. This multimer binds other proteins such as factor VII and plays a role in platelet aggregation at the site of endothelial injury. Role of vWF in normal Hemostasis: When a blood vessel has been injured, collagen is exposed and vWF binds to this exposed collagen. In addition, this activates the vWF platelet receptor, which in turn binds and activates platelets. vWF acts like the glue holding the platelets together at the site of injury. It binds to platelet glycoprotein 1b receptor when in a complex with glycoprotein IX and V. This occurs during times of rapid flow in small blood vessels. vWF will uncoil in this setting and work to slow platelets. The activation of platelets leads to the release of ADP from storage granules that recruit additional platelets to form a platelet plug; this is the process of platelet aggregation. In addition, vWF is bound to factor VIII in circulation and this is released through the action of thrombin during the clotting cascade.
Von Willebrand Disease (vWD): Von Willebrand disease presents clinically with increased bleeding tendencies. There are several variants of vWD. Some can present with mild manifestations, such as increased nosebleeds or heavy menstrual periods, while other patients present with significant bleeding after surgical intervention or childbirth. Because vWF is an acute phase reactant, stress may increase vWF levels and mitigate bleeding during stress or illness (e.g. appendectomy), while bleeding episodes may be more severe during times of relative wellness (e.g. tooth extraction). Pregnancy also causes elevation of vWF levels (often two to three-fold), and symptoms of bruising and bleeding may decrease during pregnancy (though childbirth itself still represents a significant bleeding threat). FIGURE 1 – Variants of vWD
VARIANT DEFECT INHERITANCE
PHENOTYPE
Type 1 Low levels vWF AD Typically mild Type 2 Qualitatively abnormal vWF
(levels may be normal) AD Variable
Type 3 No vWF (associated low circulating factor VIII)
AR Severe
16
Type 1 vWD - This is a quantitative defect, with low circulating levels of vWF. This accounts for the majority of patients with vWD (approximately 85%). The phenotype is typically mild, including epistaxis, bruising and menorrhagia. Type 1 disease is inherited as an autosomal dominant trait. Type 2 vWD – This is a group of disorders collectively characterized by qualitative abnormalities in vWF.
• Type 2A - vWF multimers are degraded too quickly, leaving only the smallest multimers in circulation. The result is low vWF levels and activity
• Type 2B – vWF has increased affinity for platelets, resulting in overactive platelet binding, increased clearance of vWF and platelets from circulation, and thrombocytopenia [note: the increased vWF-platelet binding may also be due to an abnormal platelet receptor, rather than an abnormal vWF, resulting in so-called “platelet-type” vWD that is phenotypically identical to type 2B vWD]
• Type 2M – unlike type 2B, vWF has decreased affinity for platelets • Type 2N – vWF has decreased affinity for factor VIII. Since factor VIII not bound to vWF
is rapidly cleared from circulation, these patients may act functionally as if they have factor VIII deficiency
Type 3 vWD - These patients have no detectable circulating vWF. As in patients with type 2N, factor VIII unbound to vWF is rapidly cleared, and these patients will have low circulating levels of factor VIII. As a consequence, patients with type 3 vWD can present with severe bleeding. Type 3 disease accounts for only a small percentage of vWD and is inherited in an autosomal recessive fashion. The Use of Desmopressin: Desmopressin (also known as DDAVP) is actually a synthetic version of antidiuretic hormone that can be used to manage mild cases of von Willebrand Disease. DDAVP acts on the Weibel-Palade bodies in the endothelial cells to increase release of stored vWF. This process is mediated by cyclic AMP. DDAVP binds to the V2 receptors on the endothelial cells, which causes a rise in cyclic AMP. The increased cAMP induces vWF secretion from the Weibel-Palade bodies. This increases the amount of circulating vWF in the patient’s blood available for use in platelet activation and aggregation. DDAVP is most effective for patients with type 1 vWD, raising levels of functional vWF. In many type 2 variants, DDAVP will raise levels of vWF but cannot correct the functional abnormality. DDAVP is ineffective in type 3 vWD. References: Bharati, Pavani, and Ram Prashanth. "Von Willebrand Disease: An Overview." Indian Journal of Pharmaceutical Sciences 73 (2011): 7-16. Kaufmann, J., and A. Oksche et al. "Vasopressin-induced Von Willebrand Factor Secretion from Endothelial Cells Involves V2 Receptors and CAMP." Journal of Clinical Investigation 106 (2000): 107-16.

17
HYPERTROPHIC CARDIOMYOPATHY CLIPP QFC 6-4 –Basic Science Resource Guide
Erin Frank, MD A teenage boy passed out at football practice this afternoon. On exam you hear a systolic murmur. If he has hypertrophic cardiomyopathy, would you expect squatting to make his murmur more or less prominent? Why? What about a Valsalva maneuver? Pathophysiology of Hypertrophic Cardiomyopathy Hypertrophic cardiomyopathy (HCM) is characterized by abnormal enlargement of the ventricle, most commonly involving hypertrophy of the ventricular septum. HCM is a consequence of mutations in genes encoding for the constituent proteins of cardiac sarcomeres, such as myosin, dystrophin and troponin. Over 900 such mutations have been described, and these mutations are often transmitted within families in autosomal dominant fashion. The mutations result in areas of fibrosis and disorganization amongst the cardiac muscle fibers called myocardial fiber disarray. This leads to myocardial hypertrophy and thickened cardiomyocytes on histology. This hypertrophied and fibrosed cardiac muscle has poor compliance. During periods of increased cardiac output such as strenuous exercise, the hypertrophied septum may actually obstruct the outflow of blood from the left ventricular outflow tract during systole. In general these patients also have an enlarged and anteriorly misaligned mitral valve that allows the valve to be displaced during systole resulting in mitral regurgitation. The mitral valve leaflet then contributes to obstruction of the left ventricular outflow tract. This is termed dynamic outflow tract obstruction. In addition to altered muscle compliance and contractility, the fibrosis and muscle fiber disorganization seen in HCM is associated with an increased predisposition to arrhythmias. Diagnosis/Physical Exam: The physical exam in a patient with suspected hypertrophic cardiomyopathy should include a very thorough cardiac exam with a focus on murmurs. The murmur typical of HCM is a systolic ejection murmur that intensifies as the blood volume in the left ventricle is decreased. With rise to standing, blood flow to the lower extremities increases and venous blood return to the heart decreases. A valsalva maneuver increases intrathoracic pressure, likewise decreasing systemic venous blood return to the heart. Both standing and valsalva maneuvers, therefore, will increase the intensity of the murmur of HCM. Conversely, squatting drives blood back from the legs to the heart, increasing intracardiac (specifically left ventricular) volume. Increased blood flow from the left ventricle helps to stent open the left ventricular outflow tract and decreases the murmur of HCM. Clinical Correlation: Patients with a concern for HCM need to undergo complete evaluation. They may present with symptoms such as shortness of breath, fainting or fatigue but the majority present after a sudden death or diagnosis of a family member. These patients require close follow up and significant limitation of their physical activity. Beta-blockers are often used in these patients to control heart rate and prevent potential arrhythmias. Careful attention should be paid to adequate hydration, and medications which are known to reduce preload, such a diuretics, should be used with great caution as they may increase obstructive symptoms in a similar manner to the provocative maneuvers described above.

18
References: Prinz, Christian. et al "The Diagnosis and Treatment of Hypertrophic Cardiomyopathy." Deutsches Arzteblatt International 108 (2011): 209-15. Maron, Martin S. et. al "Hypertrophic Cardiomyopathy Is Predominantly a Disease of Left Ventricular Outflow Tract Obstruction." Circulation 114 (2006): 2232-239.

19
GESTATIONAL DIABETES AND MACROSOMIA CLIPP QFC 7-4 – QFC Basic Science Resource Guide
Erin Frank, MD Why is the infant of a diabetic mother macrosomic? Gestational Diabetes: Gestational diabetes is diagnosed when there are elevated blood glucose levels that occur only during pregnancy. In the United States all women are recommended to undergo screening for gestational diabetes during their pregnancy. Some women will have an abnormal oral glucose tolerance test but will have normal blood glucose values during fasting while others will have elevated levels in all states. There is significant variation in treatment from dietary changes to insulin therapy depending on the degree on hyperglycemia.
Gestational diabetes is a result of increased insulin resistance. There is increasing insulin resistance during pregnancy secondary to increasing hormone levels, specifically cortisol and progesterone. In women who develop gestational diabetes, their pancreatic beta cells are not able to increase insulin production adequately to compensate for this resistance. This may be made worse by maternal obesity and increased body fat during pregnancy.
Effect on the Fetus: Serum glucose readily crosses the placenta via the GLUT 3 transporter. In addition, maternal glucose levels in excess of those in the developing fetus promote glucose transport across the placental based on this concentration gradient. If the mother is hyperglycemic, then the fetus is then exposed to higher levels of glucose than otherwise normal. The fetus responds appropriately by increasing insulin production. In addition to controlling fetal blood glucose, these increased insulin levels have a growth stimulating effect and can lead to increased body size, or macrosomia. Insulin has many properties similar to growth hormone and insulin- like growth factors. These are responsible for the increase in fetal size, especially during the later stages of pregnancy. Insulin is not able to cross the placenta with glucose, so it is in fact the fetus’ own endogenous insulin production which promotes the increase in growth. Within the cord blood of fetuses born to women with diabetes, there is dysregulation of insulin like growth factors (IGF). Increased levels of IGF1 and IGFBP3 have been found and these correlate with higher incidence of fetal macrosomia. Clinical Significance and Management: Since the increased growth rate of the fetus is a direct response to increased glucose levels crossing the placenta, treatments are aimed at normalizing maternal blood glucose levels. This will decrease the stimulation to the fetal pancreas and in turn normalize fetal insulin production. Multiple maternal treatment options exist, including dietary restriction, metformin, glyburide and injectable insulin. The choice of which method to use is determine by the level of hyperglycemia in each individual patient. Pregnancies of women with gestational diabetes should be monitored closely. This includes sonograms to evaluate the size of the baby. After delivery, these infants are at higher risk for developing hypoglycemia. The infant’s exposure to maternal hyperglycemia stops as soon as the umbilical cord is clamped, but increased fetal insulin production may persist for hours to

20
days. Infants of diabetic mothers, especially those who are macrosomic, should therefore receive careful blood glucose screening in the newborn nursery. In addition, women with gestational diabetes must be followed after delivery to ensure that their blood glucose has returned to normal. References: Kelly, Len, Laura Evans, and David Messenger. "Controversies around Gestational Diabetes Practical Information for Family Doctors." Canadian Family Physician 51.5 (2005): 688-95. Vambergue, Anne, and Isabelle Fajardy. "Consequences of Gestational and Pregestational Diabetes on Placental Function and Birth Weight." World Journal of Diabetes 2.11 (2011): 196-203.

21
CORTICOSTEROIDS AND FETAL LUNG MATURITY CLIPP QFC 7-5 –Basic Science Resource Guide
Erin Frank, MD Discuss how steroids work to promote fetal lung maturation when given prior to delivery in cases of premature labor. Fetal Lung Development: Initial lung development occurs within the first month after conception. Throughout early pregnancy, the lungs increase in size and the development of the large airways and blood supply develop. It is not until around 25 weeks gestation that early alveoli begin to form. It is of course in these future alveoli that gas exchange will take place. These early alveoli contain type I and II pneumocytes that will ultimately be responsible for surfactant production. The alveoli steadily increase in number during the later stages of pregnancy (weeks 28-35) and their number increases with advancing age. In addition to poor alveolar development, there is a shortage of surfactant within the immature infant’s lung, and the surfactant that is present is less effective. The lamellar bodies, which store surfactant, are not present until around 22 weeks gestation. Fetal surfactant is responsible for decreasing surface tension within the alveoli and preventing collapse during expiration. Inappropriate levels of surfactant lead to atelectasis, ventilation/perfusion mismatch (atelectatic areas are well-perfused but not ventilated) and hypoxia. These lungs also show poor compliance. Other conditions common to the preterm infant including hypoxia, acidosis and hypothermia all reduce the production of surfactant. Effect of Corticosteroids on Fetal Lung Maturity: Antenatal corticosteroid injections, usually in the form of betamethasone, work to stimulate the synthesis of surfactant in fetal lungs. Corticosteroids increase the activity of enzymes needed to produce lipids essential in the production of surfactant. In addition, they have been shown to stimulate development of lung structures, decrease the vascular permeability that can lead to destruction of existing surfactant and induce antioxidant enzymes within the lung. Current evidence suggests that increasing surfactant production is only one small part of the mechanism of action of betamethasone, and it may take several days to see full benefit. Clinical Guidelines: Women presenting with premature labor or premature rupture of membranes between 24 and 34 weeks gestation meet criteria for betamethasone injection. The initial dose is given intramuscularly and repeated within 24-48 hours. The fetus should show increased surfactant development roughly 24 hours after the first dose is administered. Studies have shown a decrease in respiratory distress syndrome as well as intraventricular hemorrhage and periventricular leukomalacia in premature infants receiving antenatal corticosteroids. There is also evidence that antenatal steroid use decreases the risk of postnatal infections and neonatal deaths. From this it is clear that steroids do more for the developing premature fetus than simply increase surfactant production.

22
References: Roberts D, Dalziel S. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database of Systematic Reviews 2006, Issue 3. Art. No.: CD004454. DOI: 10.1002/14651858.CD004454.pub2.
23
PHOTOTHERAPY FOR HYPERBILIRUBINEMIA CLIPP QFC 8-4 –Basic Science Resource Guide
Erin Frank, MD
How does phototherapy facilitate excretion of bilirubin? Is this effective for both direct and indirect hyperbilirubinemia? Bilirubin Metabolism in Infants Bilirubin is the expected byproduct of red blood cell turnover and hemoglobin metabolism. For many reasons, neonatal bilirubin production is higher than that in healthy adults and older children. First, newborns have an increased concentration of red blood cells, with normal hemoglobin levels in term infants ranging from 14-20 g/dL. These red blood cells turn over at a higher rate than in adults and older children, as the life span of fetal red blood cells is about half of adult rbc’s. Bilirubin is a lipid-soluble compound which is transported in the blood to the liver. There it is reversibly conjugated by uridine diphosphoglucuronate glucuronosyltransferase, producing a water soluble compound which can be excreted in the biliary system. Infants have decreased activity of this enzyme, leading to less effective bilirubin conjugation and thus poor excretion of bilirubin. Within the GI tract, some of the bilirubin will be reabsorbed via enterohepatic circulation. The longer the bilirubin remains in the intestines, the greater the chance that conjugated bilirubin will revert to its unconjugated form. Unconjugated bilirubin is highly lipophilic and readily reabsorbed. For these reasons, all neonates are expected to have rising bilirubin levels within the first several days of life. Since these mechanisms are common to all neonates, the process is referred to as physiologic jaundice. Exacerbation of any of these mechanisms may drive bilirubin levels above and beyond expected physiologic levels. Neonates with polycythemia, hemolysis, liver disease, feeding difficulties or intestinal stasis for any reason are at increased risk for heightened severity and prolonged duration of hyperbilirubinemia. Direct vs. Indirect Bilirubin The first step in the evaluation of jaundice in the newborn period is measurement of bilirubin levels, including direct and indirect fractions. Patients with physiologic jaundice always present with an elevated indirect bilirubin but a normal direct bilirubin. Likewise, hemolysis, the most common pathologic reason for neonatal hyperbilirubinemia, increases indirect bilirubin levels only. A small minority of patients will actually develop direct hyperbilirubinemia, defined as direct bilirubin >20% of total or direct bilirubin >2 mg/dL. The disorders that present in this fashion are primarily focused on the liver or obstructive processes affecting biliary flow. Any patient with a direct hyperbilirubinemia must be fully evaluated, as this cannot be contributed to normal newborn physiologic jaundice. Mechanism of Phototherapy Phototherapy works by converting unconjugated bilirubin to a photo-isomer, lumirubin. The energy from the phototherapy is absorbed by the bilirubin leading to structural isomerization. Unlike lipophilic unconjugated bilirubin, lumirubin is non-toxic and easily excreted by the body without the additional step of conjugation in the liver. The lights used in phototherapy are blue because this spectrum of light is most effectively absorbed by the bilirubin.

24
ABSORPTION SPECTRUM OF UNCONJUGATED BILIRUBIN
I UV-‐A I visible I
Phototherapy is not effective at treating elevated direct bilirubin levels. In fact patients with an elevated direct bilirubin may develop bronzing of the skin if exposed to phototherapy. The mechanism of this is not completely understood. Clinical Correlation In newborn infants jaundice is a common problem. While most infants will do well and their jaundice will resolve spontaneously, some infants with excessive hyperbilirubinemia will require treatment to prevent complications such as kernicterus. There are many different phototherapy systems available. The efficacy of any phototherapy is determined by duration of exposure, body surface area exposed and irradiance. Irradiance is influenced by type of light source and the distance from that light source. Commonly used phototherapy systems include daylight, cool white, blue or special blue fluorescent tubes. Of these, the special blue tubes are most effective at producing light in the optimal blue-green spectrum (a common misconception), and the small amount of UV-A light produced is almost entirely absorbed by either the glass wall of the fluorescent tube or the Plexiglas cover of the phototherapy unit.
25
References:
American Academy of Pediatrics, Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004; 114(1):297–316
Maisels, Jeffery, and Anthony F. McDonagh. "Phototherapy for Neonatal Jaundice." New England Journal of Medicine 358.23 (2008): 2522-525 Stokowski, L. "Fundamentals of Phototherapy for Neonatal Jaundice." Advances in Neonatal Care 11.5 (2011): S10-21

26
TREATMENT RESPONSES IN CONGENITAL HYPOTHYROIDISM CLIPP QFC 9-3 - Basic Science Resource Guide
Di Sun, Keith Della Grotta and Adekunle Elegbede At age 2 months an infant with congenital hypothyroidism has a markedly elevated TSH. Parents report adherence to the daily dose of levothyroxine, and your records indicate that the dose is appropriate. What might be the cause of the elevated TSH? NORMAL THYROID DEVELOPMENT AND FUNCTION Thyroid hormone secretion is regulated by the hypothalamus and pituitary gland. The hypothalamus produces thyrotropin releasing hormone (TRH), which stimulates thyrotropes in the anterior pituitary gland to produce thyrotropin stimulating hormone (TSH). TSH promotes thyroid gland growth and secretion of levothyroxine (T4) and liothyronine (T3) both of which are produced by coupling of tyrosine to iodine. Although T4 is the more predominant form secreted from the thyroid gland, >99% of serum T4 is in the inactive protein-bound form attached to thyroid binding globulin (TBG) and other plasma proteins. Within peripheral tissues, T4 is deiodinated to the more active T3, which is the major mediator of thyroid hormone effects. T4 and T3 can also be deiodinated to the inactive forms rT3 and T2. T3 acts via binding nuclear receptors producing a variety of effects. In the neonate, these effects play critical roles in brain maturation, myelination and the establishment of neuronal connections especially in the critical period from birth to the first few months of life. T3 also regulates thyroid function by negative feedback suppression of anterior pituitary TSH secretion. The thyroid gland begins developing by week 3 of gestation. By week 10-12, it is well formed, can synthesize thyroid hormone and has migrated along the thyroglossal duct from its origin in the anterior gut region of endoderm to its endpoint inferior to the thyroid. The pituitary gland is also well formed by week 12. Early secretion of TRH is from the placenta, fetal gut and pancreas. By mid-gestation, the hypothalamic- pituitary axis is mature with hypothalamic secretion of TRH which stimulates TSH secretion from the fetal anterior pituitary. From mid-gestation until birth, TBG synthesis increases. The TSH concentration remains high and the fetal thyroid gland becomes more responsive to TSH. Therefore, thyroid hormone production increases saturating the circulating TBG and progressively increasing serum free T4. The placenta and fetal tissue continue to deactivate T4 and T3 until late gestation (28-32 weeks) when levels of free T3 begin to rise. Within 30 minutes of birth, TSH rapidly increases, stimulated by the low ambient temperature and resulting in a rapid increase in serum T3 and T4. With no concurrent increase in TBG, free T3 and free T4 also increase. Note that the TSH does not cross the placenta and thyroid hormone only crosses in very limited quantities most of which is in the inactive deiodinated form. In fact, the placenta inactivates T4 to rT3 and T3 to T2 via deiodination. CONGENITAL HYPOTHYROIDISM Congenital hypothyroidism (CH) is defined as a deficiency in thyroid hormone at birth and is classified as either primary or secondary according to etiology: Primary congenital hypothyroidism is the most common form of congenital hypothyroidism; etiologies include:
• Thyroid dysgenesis – 85% of primary cases due to a failure of thyroid development: o ectopic thyroid, o thyroid hypoplasia, o athyreosis (absent thyroid)
27
• Thyroid dyshormonogenesis – remaining primary cases due to abnormal thyroid hormone synthesis.
Secondary congenital hypothyroidism is characterized by TSH deficiency, usually caused by problems in the structure or function of the pituitary gland. Endemic cretinism due to iodine deficiency is common in some areas of central Africa with cassava-rich diet that contains cyanate which reduces iodide uptake by the thyroid gland. Unlike other congenital hypothyroid cases, cognitive impairment in these children cannot be prevented with subsequent levothyroxine (LT4) supplementation. CLINICAL SIGNIFICANCE Congenital hypothyroidism is the most common endocrine disorder in neonates and is one of the most common treatable causes of mental retardation. Other associated findings include macrosomia, hypotonia, delayed reflexes, umbilical hernia, macroglossia, persistent jaundice, mottled skin, dysmorphic facies characterized by flattened nasal bridges and hypertelorism, and skeletal abnormalities. However, such features are rarely apparent at birth, meaning that early detection is dependent on the measurement of serum thyroid stimulating hormone (TSH) and/ or thyroid hormone levels shortly after birth. Newborns are screened for hypothyroidism in all 50 states in the U.S. Newborns with abnormal thyroid screens should begin supplementation with levothyroxine as early as possible because delays of as little as 1 week have been shown to result in significantly lower IQ in these individuals. TH-associated CNS development continues until 3 to 4 years of human life. Response to treatment is monitored by following serum TSH and T4 levels. TSH may remain elevated in the setting of a normalized free T4 level for several reasons: • Prolonged half-life of levothyroxine
Levothyroxine has a half-life of up to 1 week. Therefore, it may take several weeks to reach serum steady state concentration and corresponding trough levels of TSH. In fact, normalization of serum TSH has been reported to take 1 to 8 weeks in infants with congenital hypothyroidism after initiation of treatment with levothyroxine.
• Hyperthyrotropinemia
In as much as 40% of infants with congenital hypothyroidism, the serum TSH will remain high even when adequate thyroid hormone supplementation is provided and serum levels of free T4 and T3 are normal. The TSH levels may remain markedly high in months following initiation of treatment, correlating poorly with serum T3 and T4, and may remain relatively high until the peri-pubertal period. The elevated TSH is believed to be due to in utero resetting of the set point for TSH secretion in the anterior pituitary, a condition that has been referred to as “hyperthyrotropinemia”. As such, the anterior pituitary in these individuals is not as sensitive to feedback suppression by T3 or T4. Elevated TSH is also noted to occur in 3% of otherwise normal infants, attributable to a variant high HPT axis set point in the absence of hypothyroidism symptoms.
If the TSH level is high and the T4 level remains low, several other possibilities must be considered: • Under treatment

28
As the patient grows and increases in size and weight, the levothyroxine dose required to maintain a euthyroid state will also increase. If the T4 level was previously normal, an elevated/rising TSH level may indicate the need to increase the dose of levothyroxine.
• Switching to a different formulation of levothyroxine Different generic brands vary in potency. Switching to a new formulation requires dose re-titration. Using a consistent formulation can minimize this risk.
• Inadequate absorption of levothyroxine Levothyroxine absorption in the gut is affected by the patient’s diet. Soy-based formula in particular may interfere with levothyroxine absorption. Medications such as concentrated iron supplements, calcium, aluminium hydroxide, cholestyramine, and sucralfate may also decrease absorption of levothyroxine.
• Noncompliance Although the dosing may appear to be adequate, always confirm instructions for dosing and compliance with these instructions. Personal finances and insurance coverage may interfere with obtaining medication. Illiteracy may interfere with following written instructions. Levothyroxine administration in neonates requires crushing a tablet and dissolving the powder, which can be troublesome for a caregiver. Some parents may try to put the medication in the child’s feeding bottle. If the child does not drink all of the liquid, however, the dose is incompletely administered. Parents should be encouraged to suspend medication in only a few mL of liquid to insure accurate dosing.
References Akcay T, Turan S, Guran T, et al. T4 plus T3 treatment in children with hypothyroidism and inappropriately elevated thyroid-stimulating hormone despite euthyroidism on T4 treatment. Horm Res Paediatr. 2010;73(2):108–114. Bernal, Juan. “Thyroid Hormones and Brain Development.” Vitamins and Hormones. 2005; 71: 95-115. Fagman, Henrik and Mikael Nilsson. “Morphogenesis of the thyroid gland.” Mollec and Cell Endocrin. 2010; 323: 35-54. Fisher DA. Rudolph's Pediatrics 22nd ed. United States: McGraw-Hill Education, 2011. Fisher DA, Schoen EJ, La Franchi S, et al. The hypothalamic-pituitary-thyroid negative feedback control axis in children with treated congenital hypothyroidism. J. Clin. Endocrinol. Metab. 2000;85(8):2722–2727. Grüters A and Krude H. Detection and treatment of congenital hypothyroidism. Nat Rev Endocrinol. 8(2) October 2011. MacGillivray, MH. “Congenital Hypothyroidism.” Pediatric Endocrinology: Mechanisms, Manifestations, and Management. Ed. Pescovitz and Eugster. Philadelphia: Lippincott Williams & Wilkins, 2004. 490-504. Print.

29
Rastogi MV, LaFranchi SH. Congenital hypothyroidism. Orphanet J Rare Dis. 2010;5:17. Rose SR, Brown RS. Update of Newborn Screening and Therapy for Congenital Hypothyroidism. Pediatrics. 2006;117(6):2290–2303. Zimmermann, Michael B. “The role of iodine in human growth and development.” Seminars in Cell and Development Biol. 2011; 22: 645-652.

30
SCARLET FEVER – PATHOPHYSIOLOGY AND TREATMENT CLIPP QFC 11-5 – Basic Science Resource Guide
Erin Frank, MD Two children come to the office with fever, sore throat; both have exudative pharyngitis and positive rapid antigen tests for group A Strep. One patient also has diffuse, rough erythroderma; the other child does not. What accounts for the different clinical manifestations between these two patients? How would you treat each of these patients? Overview of Scarlet Fever:
Scarlet fever is a common complication of infection with Streptococcus pyogenes, or Group A Streptococcus (GAS). It is characterized by a diffuse erythematous rash that is macular and blanching. It often has a ‘sandpaper’ like quality resulting from occlusion of the sweat glands, and some have referred to this combination of keratosis and erythroderma as the appearance of a “sunburned chicken”. The rash begins on the trunk with spread to the extremities, though typically sparing the palms, soles and perioral region. Ultimately there may be fine desquamation, especially of the extremities. Within the skin folds of the body such as the axillary, antecubital and inguinal areas there may be linear erythema highlighting skin folds, known as Pastia’s lines. In addition to the typical findings of exudative pharyngitis, the oral mucosa is often erythematous, and swollen lingual papillae give the tongue a strawberry appearance. GAS Toxin Production GAS produce and release a number of toxins. Some of these, such as Streptolysin S (SLS), Streptolysin O (SLO), DNA-ase, and hyaluronidase are common to all strains of GAS. However, only some strains of GAS produce pyrogenic exotoxins. Streptococcal pyrogenic exotoxins (SPEs) are a family of toxins with the capacity to act as superantigens. Superantigens do not requiring processing by antigen presenting cells. Rather, they stimulate T cells by binding class II MHC molecules directly and nonspecifically. As a consequence, superantigens stimulate a T cell response that is several thousand-fold greater than that stimulated by conventional antigens. resulting in massive release of proinflammatory cytokines.
The systemic symptoms of scarlet fever are caused by a streptococcal pyrogenic exotoxin producing strain of streptococcal bacteria. Over 15 SPE’s have been identified, three of which have been associated with scarlet fever: types A and C, encoded by bacteriophages, and type B, which is encoded on bacterial chromosomes. All of these toxins produce the clinical manifestations of scarlet fever.
Clinical Significance:
There is often a misconception that scarlet fever is related to delayed diagnosis and treatment, but it is related solely to whether the infecting strain is toxin-producing or not. Infection with non-toxin-producing strains of GAS cannot cause scarlet fever. Though most commonly associated with group A Strep pharyngitis, scarlet fever can also occur after infection of the skin or other sites with toxin-producing strains of GAS. Formation of antitoxin antibodies confers immunity

31
only against that specific toxin, such that it is possible for an individual patient to have scarlet fever more than once.
Treatment of GAS pharyngitis is the same regardless of the clinical manifestations of scarlet fever. Treatment with penicillin-based antibiotics has been shown to decrease duration of illness and subsequent rates of rheumatic fever when given within 9 days of the start of illness. Strep pyogenes remains sensitive to penicillin and treatment can include either a single intramuscular dose of penicillin G or a 10-day course of oral therapy with amoxicillin. Additional treatment regimens are available for penicillin allergic patients. References: Bisno, AL, Stevens, DL. Streptococcus pyogenes. In: Principles and Practice of Infectious Diseases, 6th ed, Mandell, GL, Bennett, JE, Dolin, R (Eds), Churchill Livingstone, Philadelphia, PA 2005. p.2362.
Brook, I., and J. E. Dohar. "Management of Group A Beta-hemolytic Streptococcal Pharyngotonsillitis in Children." Journal of Family Practice 55.12 (2006): S1-S11.

32
ESOPHAGEAL AND TRACHEAL FOREIGN BODIES CLIPP QFC 12-3 – QFC Basic Science Resource Guide
Erin Frank, MD If a child swallows a coin, how can you tell on x-ray whether it is in the trachea or the esophagus? What are the indications for extracting a foreign body from the GI tract? From the trachea? Describe the locations within the esophagus where foreign bodies are most likely to lodge. Coins are among the most common foreign body ingestions in the pediatric population. Clinical manifestations vary from life threatening to completely asymptomatic. Determining the location of the coin can guide the clinician in deciding if and when the foreign body should be removed. Foreign body ingestions are most likely to occur in young children (under age 4) but may also be seen in older children with developmental delay. Imaging of radiopaque foreign bodies Coins are easily visualized on standard x-ray imaging because of their radiopaque nature. When obtaining imaging on any child with a suspected foreign body ingestion, recommended imaging includes AP and lateral views of the chest and neck, and possibly the abdomen. The most common locations of symptomatic coin ingestions are the trachea and upper esophagus. Determining esophagus vs. trachea The anatomy of the trachea and esophagus differ greatly from each other and it is these differences that are the basis for using imaging to determine foreign body location. The trachea has multiple cartilaginous C shaped rings that act to keep it patent and open throughout respiration. The opening of the “C” is posterior. A coin in the trachea will typically lie with one edge against the less rigid open portion of the C ring, while the other is wedged against the cartilage. In this orientation, the coin will appear on end in the AP x-ray and in circular profile on the lateral view The esophagus, on the other hand, is composed largely of smooth muscle whose job is to respond to a food bolus with peristalsis and move this bolus along to its destination in the stomach. The esophagus remains relaxed when there is no stimulation from swallowed food or liquids. An ingested coin lodged in the esophagus, on the other hand, will tend to be oriented coronally – that is, on AP x-ray you will visualize the coin as a complete radiopaque circle (figure 1). Conversely, on lateral view the coin will appear as if it is on end. The muscle of the esophagus sits directly against the open end of the C ring of the trachea and this position with the coin oriented in the AP direction represents the path of least resistance for the coin because the ligament connecting the cartilage of the trachea is more rigid than the musculature of the esophagus.

33
Figure 2-‐ coin lodged in esophagus
Anatomic sites for obstruction There are 3 areas of physiologic narrowing in the esophagus at which foreign bodies tend to get stuck: (1) Proximal esophagus (at the thoracic inlet) – this is the most common spot for esophageal foreign bodies to become lodged, because it is the narrowest portion of the esophagus in children. This is also where skeletal transitions to smooth muscle within the esophagus. The cricopharyngeus sling sits at this level and may contribute to the lodging of coins in this location. (2) Mid esophagus (at the level of the aortic arch and carina) - the mid esophagus narrows due to the nearby aortic arch and carina. Carefully inspect the chest x-ray for evidence of a right-sided aortic arch, as this would prompt evaluation for a vascular ring (figure 3)

34
Figure 3 – normal anatomy vs. vascular ring
(3) Distal esophagus (at the gastroesophageal junction) - the junction of the esophagus and stomach is the final location where there is relative narrowing. On chest x-ray you will find the foreign body sitting right over the diaphragm. Indications for removal All tracheal foreign bodies must be removed promptly. Esophageal foreign bodies should be removed from symptomatic patients (e.g. respiratory symptoms, pain, inability to handle oral secretions). Ingestions of sharp objects as well as button batteries (which can often be mistaken for coin ingestions) should occur as soon as this determination is made. These objects are more prone to cause esophageal injury and perforation, and this risk increases with time. Asymptomatic ingestions of low risk objects can be observed for the first 24 hours to monitor for passage into the stomach. If after 24hrs the coin has not moved past the GE junction, then endoscopy should be performed and the foreign body removed. References: Waltzman M. Management of esophageal coins. Pediatric Emerg Care 2006;22:367-373. Dehghani, Navid, and Jeffery P. Ludemann. "Ingested Foreign Bodies in Children: BC Children’s Hospital Emergency Room Protocol." BC Medical Journal 50.5 (2008): 257-62.

35
RACEMIC EPINEPHRINE vs. ALBUTEROL CLIPP QFC 12-4 – Basic Science Resource Guide
Erin Frank, MD Racemic epinephrine typically provides prompt improvement for patients with croup, while nebulized albuterol typically does not (and may even worsen symptoms) – why? Croup (laryngotracheobronchitis) is a viral infection of the glottis and subglottic structures. This leads to increased inflammation and swelling, in turn leading to the typical clinical manifestations including a barky cough and inspiratory stridor. Some children have such significant airway edema that they develop increased work of breathing and tachypnea. Parainfluenza is the leading viral cause of croup, though it can be seen with many other respiratory viral infections. Mechanism of action: Albuterol is a selective beta2-adrenergic receptor agonist. When given by inhalation, it stimulates local beta receptors within lung tissue. Receptor activation leads to increased production of cAMP, which increases activity of protein kinase A. This inhibits phosphorylation of myosin and results in decreased intracellular calcium within the smooth muscle. The result is relaxation of bronchial smooth muscle and bronchodilation. The narrowing of the upper airway in croup, however, is the result of mucosal edema more than smooth muscle constriction (as the upper airway is held open by cartilaginous rings). Albuterol has no direct effect on edema and swelling. Epinephrine is non-specific adrenergic agent. Like albuterol, it has the same beta agonist effect on lower airway bronchodilation. Unlike albuterol, it also activates alpha-adrenergic receptors of the airway. This results in local vasoconstriction that leads to decreased edema within the subglottic structures of the patient’s airways. Racemic epinephrine is provided in nebulized form so it works locally on the receptors in the airway leading to quick and effective delivery and response. Racemic epinephrine does have a short half-life and a short period of response with most of the effect being gone within several hours. Clinical indication: When evaluating a child presenting with “noisy breathing”, it is important to identify the likely source of the noise so as to choose the most effective therapy. Croup is a characterized primarily by symptoms related to upper airway edema and obstruction. Symptoms of upper airway narrowing are typically worst with inspiration and may include retractions, stridor, barking cough and hoarse voice. In contrast, lower airway diseases such as asthma are complicated by bronchoconstriction as well as edema. Though wheezing may be biphasic, it is often heard first and most prominently with exhalation. Because of its non-specific adrenergic action, inhaled racemic epinephrine triggers vasoconstriction in swollen upper airways and decreases swelling, whereas albuterol cannot.

36
References: Bjornson, Candice L., and David W. Johnson. "Croup in the Paediatric Emergency Department." Paediatrics and Child Health 12 (2007): 473-77. Zoorob, R., M. Sidani, and J. Murray. "Croup: an Overview." American Family Physician 83 (2011): 1067-073.

37
TREATMENT FAILURE IN OTITIS MEDIA CLIPP QFC 14 - Basic Science Resource Guide
Carrie Phillipi, MD A 12 month old girl is diagnosed with acute otitis media and prescribed amoxicillin 250mg/5mL 1tsp po bid. Two days later she is still intermittently febrile and fussy; repeat exam shows erythematous, bulging TM’s bilaterally. Give at least three possible explanations for this treatment failure. Acute otitis media (AOM), infection of the middle ear, is the most common condition for which antibacterial agents are prescribed for children in the United States. 50% AOM resolves on its own within 7 days with placebo, leading to efforts to decrease the rates of antibiotic use in the management of AOM. Once a decision has been made to treat with antibiotics, though, amoxicillin is the antibiotic of choice for first-line treatment of otitis media in non-allergic patients. When antibiotics are prescribed for AOM, clinical improvement should be expected within 48 to 72 hours. However, there are many reasons why this antibiotic may be ineffective. An understanding of the microbiology of middle ear infections, antibiotic pharmacodynamics and mechanisms of antibiotic resistance provides insight into treatment failures and helps to dictate second-line therapy when needed. Microbiology of Otitis Media AOM is most frequently preceded by a viral upper respiratory tract infection which leads to eustachian tube inflammation and dysfunction. The resultant negative middle ear pressure draws viruses and bacteria from the nasopharynx into the middle ear cavity. The bacteria most commonly isolated from cultures of middle ear aspirates in patients with AOM include Streptococcus pneumonia (pneumococcus), non-typeable strains of Haemophilus influenzae and Moraxella catarrhalis. In addition, up to 10% of aspirates contain only viral pathogens, and up to 65% contain a combination of viral and bacterial pathogens. Prior to the introduction of the conjugate pneumococcal vaccine (PCV-7) in 2000, Streptococcus pneumonia was the most common bacterial cause of AOM. In the years following the routine use of PCV-7, non-typeable H influenzae became the most frequently isolated middle ear pathogen. Most recently, an increase in the rates of infection with non-PCV7 serotypes of S pneumoniae has essentially equalized the incidence of S pneumoniae and H influenzae in children with AOM. The evolving microbiology of AOM is sure to be influenced by the licensure of the 13-valent pneumococcal conjugate vaccine (PCV-13) directed at curbing these trends in pneumococcal disease. With few exceptions, it is not possible to use clinical clues to predict accurately which bacteria is the causative agent for AOM in a given patient. One such exception is the so-called conjunctivitis-otitis syndrome, with good evidence to suggest that non-typeable H influenza is more common in patients with concomitant AOM and conjunctivitis. Conversely, microbiology clearly influences the clinical course of AOM. In one study, AOM due to S pneumoniae resolved in 19% of children without antibiotic treatment, as compared to 48% of AOM due to H influenzae and 75% of AOM due to M catarrhalis. Pharmacodynamics of Antibiotics Simply stated, the minimum inhibitory concentration (MIC) is the lowest dose of an antimicrobial agent found to suppress the growth of a particular microorganism. Antibiotics function by either time-dependent or dose-dependent mechanisms.

38
For time-dependent antibiotics, such as β-lactam antimicrobials, the important variable is the percent of the dosing interval (%T) during which the antibiotic concentration is above the MIC (often designated as %T > MIC). For amoxicillin, maximal bacterial eradication occurs when concentrations at the tissue site exceed the MIC for approximately 40% of the dosing interval. Other antimicrobial agents utilize dose- or concentration-dependent mechanisms, which are predicated on the concept of a peak concentration/MIC ratio. Here, the peak concentration above the MIC saturates the binding site and is responsible for microbial killing. The best response occurs when the peak concentration exceeds the MIC for the target organism by ten times. Aminoglycosides and fluoroquinolones employ such dose- or concentration-dependent killing. Antimicrobials may also be classified as either bacteriocidal or bacteriostatic based on whether they kill bacteria or merely inhibit their growth, respectively. β-lactam antibiotics are primarily bacteriocidal, inhibiting bacterial cell wall formation by binding to penicillin-binding proteins (PBPs). PBPs are enzymes present on the interior cell wall and are integral to several steps in bacterial cell wall synthesis and homeostasis. PBPs are responsible for strengthening the bacterial cell surface by cross-linking the peptidoglycan matrix and have additional roles in cell division, phage resistance and capsule formation. β-lactam antibiotics access and bind PBPs ultimately causing bacterial cell lysis. Mechanisms of Antibiotic Resistance S. pneumoniae resistance to β-lactams, including amoxicillin, is mediated by mutations in high molecular weight PBPs (types 1 and 2). Alterations in the structure of PBPs result in diminished antibiotic affinity, raising the MIC to both penicillin and cephalosporins. Complicating the problem, genetic changes responsible for altered penicillin binding are affiliated with genes conferring resistance to other antibiotics. High-doses of amoxicillin (80-100 mg/kg/day) are used to overcome this mechanism of resistance and increase the %T > MIC against all S pneumoniae serotypes that are intermediately resistant to penicillin (penicillin MICs, 0.12–1.0 µg/mL), and many but not all highly resistant serotypes (penicillin MICs, ≥2 µg/mL). In the U.S., 83-87% of S pneumoniae isolates are susceptible to these higher doses of amoxicillin. Therefore, “high-dose” amoxicillin (as opposed to standard dosing at 40-50 mg/kg/day) is first line therapy for common bacterial infections in the respiratory tract where S. pneumoniae is a potential pathogen, including otitis media, sinusitis and pneumonia. In contrast, resistance to amoxicillin in H. influenza and M. Catarrhalis is mediated by production of β-lactamase. This mechanism cannot be overcome by simply increasing the dosage of antibiotic, but can be countered by addition of β-lactamase inhibitors such as clavulanate or sulbactam (note that β-lactamase inhibitors have no role in the treatment of infections from S. pneumonia). Current data suggest that 58% to 82% of H influenza isolates are susceptible to amoxicillin, whereas nearly 100% of M catarrhalis are β-lactamase positive and therefore resistant to amoxicillin. Clinical Significance There are several possible explanations for the treatment failure in the scenario above: • The patient’s AOM may be due to a viral etiology and therefore unresponsive to any
antibiotic • An average 12 month old weighs approximately 10kg. A total daily dose of 500mg (250 mg
bid) would be considered standard dosing, whereas high-dose therapy may be more effective against some strains of resistant pneumococcus

39
• Many infections due to H. influenza and nearly all due to M. Catarrhalis will be resistant to amoxicillin. For this reason, AAP practice guidelines recommend that “clinicians should prescribe an antibiotic with additional β-lactamase coverage for AOM when the child has received amoxicillin in the last 30 days or has concurrent purulent conjunctivitis, or has a history of recurrent AOM unresponsive to amoxicillin.
• Lastly, any medication can be difficult for children to take. Inquiring about possible difficulty in adhering to therapy in a non-judgmental manner (e.g. “I find it hard to give my children medicine. How many of the doses do you think you were able to give your child”?) may elucidate another potential source of treatment failure.
References Bradley, JS, et al. Pharmacokinetics, Pharmacodynamics, and Monte Carlo Simulation. Pediatric Infectious Disease Journal 2010; 29(11):1043-1046. Feigin and Cherry, 5th edition, pp. 1216-1218; 1231-33; 2948 Grijalva CG, Nuorti JP, Griffin MR. Antibiotic prescription rates for acute respiratory tract infections in US ambulatory settings. JAMA. 2009;302(7): 758–766 Lieberthal, et al. The Diagnosis and Management of Acute Otitis Media; Clinical Practice Guideline. Pediatrics 2013;131:e964–e999 McCaig LF, Besser RE, Hughes JM. Trends in antimicrobial prescribing rates for children and adolescents. JAMA. 2002;287 (23):3096–3102 Red Book. 2009 Report on the Committee on Infectious Disease, pp. 524-535

40
ACIDOSIS AND ALKALOSIS IN CONTEXT OF VOMITING CLIPP QFC 15-4 - Basic Science Resource Guide
Carrie Phillipi, MD A 3 week old boy with a two-week history of progressive vomiting is found to have pyloric stenosis on ultrasound. He appears to be 10% dehydrated on exam; admission electrolytes reveal Na 132 / K 4.1/ Cl 89 / HCO3 29 / BUN 14 / creatinine 0.4. Most dehydrated patients are acidotic – why? Why isn’t this patient?
The body maintains a pH of 7.4 with minimal variation. Acid-base balance is maintained by:
(1) intracellular and extracellular buffering, (2) regulation of pCO2 by respiratory changes and (3) renal acid excretion
Acidosis occurs when acid builds up in the body or when bicarbonate is lost; acidemia is defined as an arterial pH <7.36. In the setting of acidosis, buffers are utilized and the lungs and kidneys seek to maintain a pH of 7.4 by increasing respiration (thereby decreasing CO2) or by increasing hydrogen ion excretion, respectively.
Acids are capable of donating hydrogen ions (H+) while a base is capable of accepting H+. Bicarbonate (HCO3-) is the body’s most important base or extracellular buffer of H+. When combined, H+ and HCO3- produce water and CO2 as shown in the following equation:
H+ + HCO3- H2CO3 H2O + CO2
Acid-base status is then defined by the Henderson-Hasselbalch equation which describes the relationship between HCO3- and pCO2:
pH = 6.1 + log (HCO3-/ (0.03 x pCO2))
Plasma bicarbonate is regulated by hydrogen ion excretion in the renal tubules. Filtered HCO3- is reabsorbed primarily in the proximal tubule but also in the thick ascending limb. Excreted acid combines with buffers in the lumen of the kidney tubules; increases in H+ secretion therefore cause a rise in serum bicarbonate. When acid is retained, serum bicarbonate falls.
Dehydration with volume depletion typically results in metabolic acidosis, often as a result of lactic acid production in hypoperfused tissues and decreased glomerular filtration resulting in decreased H+ excretion. In patients with diarrhea, acidosis may be exacerbated by bicarbonate loss in stool and ketone production. The most common causes of acidosis in children are shown in Table 1. Note that the most common framework for subdividing causes of acidosis first requires calculation of an anion gap.
Anion Gap = Na+ - (Cl- + HCO3-)
An increased anion gap identifies the presence of excess acid in the form of an “unmeasured anion”, whereas acidosis in the setting of a normal anion gap denotes bicarbonate losses, either from the gastrointestinal tract or from the renal system.
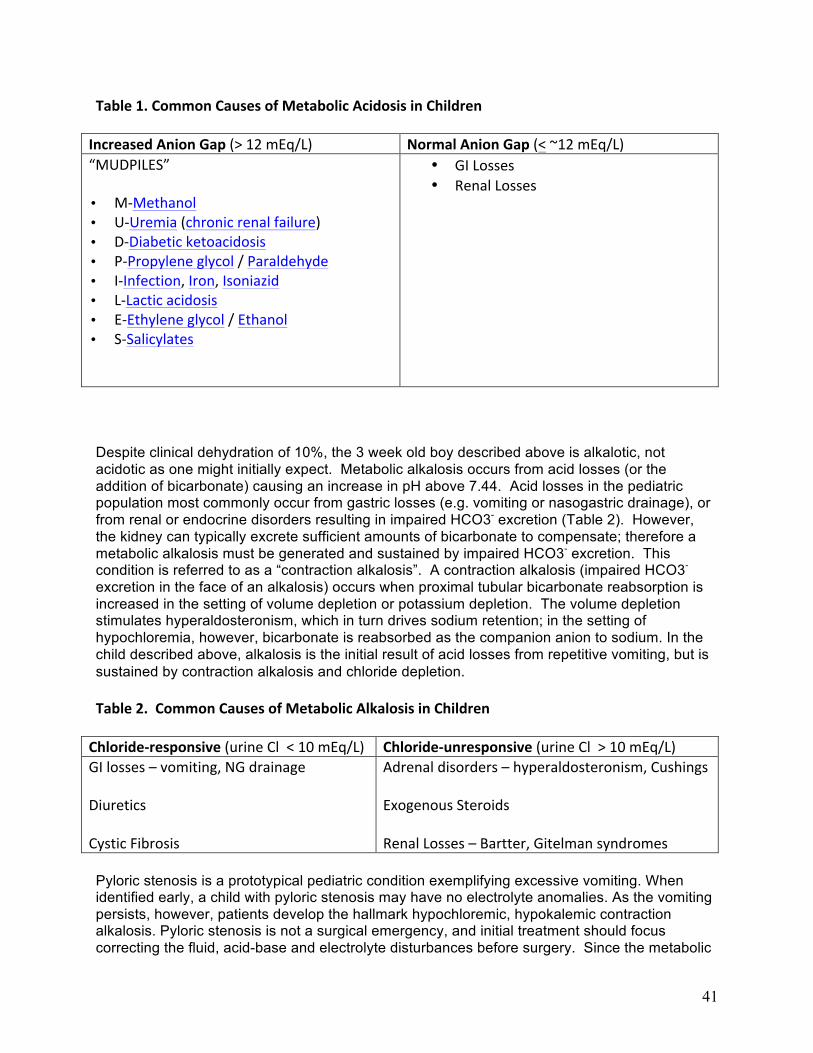
41
Table 1. Common Causes of Metabolic Acidosis in Children
Increased Anion Gap (> 12 mEq/L) Normal Anion Gap (< ~12 mEq/L) “MUDPILES”
• M-‐Methanol • U-‐Uremia (chronic renal failure) • D-‐Diabetic ketoacidosis • P-‐Propylene glycol / Paraldehyde • I-‐Infection, Iron, Isoniazid • L-‐Lactic acidosis • E-‐Ethylene glycol / Ethanol • S-‐Salicylates
• GI Losses • Renal Losses
Despite clinical dehydration of 10%, the 3 week old boy described above is alkalotic, not acidotic as one might initially expect. Metabolic alkalosis occurs from acid losses (or the addition of bicarbonate) causing an increase in pH above 7.44. Acid losses in the pediatric population most commonly occur from gastric losses (e.g. vomiting or nasogastric drainage), or from renal or endocrine disorders resulting in impaired HCO3- excretion (Table 2). However, the kidney can typically excrete sufficient amounts of bicarbonate to compensate; therefore a metabolic alkalosis must be generated and sustained by impaired HCO3- excretion. This condition is referred to as a “contraction alkalosis”. A contraction alkalosis (impaired HCO3- excretion in the face of an alkalosis) occurs when proximal tubular bicarbonate reabsorption is increased in the setting of volume depletion or potassium depletion. The volume depletion stimulates hyperaldosteronism, which in turn drives sodium retention; in the setting of hypochloremia, however, bicarbonate is reabsorbed as the companion anion to sodium. In the child described above, alkalosis is the initial result of acid losses from repetitive vomiting, but is sustained by contraction alkalosis and chloride depletion.
Table 2. Common Causes of Metabolic Alkalosis in Children
Chloride-‐responsive (urine Cl < 10 mEq/L) Chloride-‐unresponsive (urine Cl > 10 mEq/L) GI losses – vomiting, NG drainage
Diuretics
Cystic Fibrosis
Adrenal disorders – hyperaldosteronism, Cushings
Exogenous Steroids
Renal Losses – Bartter, Gitelman syndromes
Pyloric stenosis is a prototypical pediatric condition exemplifying excessive vomiting. When identified early, a child with pyloric stenosis may have no electrolyte anomalies. As the vomiting persists, however, patients develop the hallmark hypochloremic, hypokalemic contraction alkalosis. Pyloric stenosis is not a surgical emergency, and initial treatment should focus correcting the fluid, acid-base and electrolyte disturbances before surgery. Since the metabolic

42
alkalosis is chloride-responsive, IV fluids should contain isotonic sodium and potassium chloride. After initial rehydration, glucose should be added and isotonic fluid therapy should be continued until the serum bicarbonate concentration is less than 30 mEq/dL. The alkalosis must be corrected to prevent potential postoperative apnea which may be associated with anesthesia.
References
Nelson’s Textbook of Pediatrics 13th Edition pp. 1060-1062
Schwaderer, AL and GL Schwartz. Acidosis and Alkalosis. Pediatrics in Review 2004; 25(10): 350-357.

43
EXERCISE AND DIABETES MELLITUS CLIPP QFC 16-5 - Basic Science Resource Guide
Carrie Phillipi, MD After her discharge from the hospital, Isabella’s blood glucose remains under excellent control except after soccer games, when her glucose routinely drops to the 50’s. Why? How would you manage Isabella? Children with diabetes are encouraged to exercise regularly, as physical activity can have many health benefits including lowering blood glucose levels. However, exercise can present challenges for children with diabetes, since muscles are the major consumer of glucose during exercise. After initially depleting their own glucose supplies, muscles become more sensitive to insulin. Muscle cells can even absorb glucose independently of insulin during prolonged exercise. This physiology can be incredibly helpful for prevention and treatment of pre-diabetes and type 2 diabetes with insulin resistance, but can be difficult to manage in type 1 diabetes when a specified dose of insulin must be considered and administered. During periods of exercise, extra calories or lower insulin doses may be needed to prevent hypoglycemia, which can even occur even many hours later. A careful regimen to monitor the effects of exercise on glucose levels should be initiated to determine an optimal insulin regimen. A snack can be eaten before exercise to help prevent hypoglycemia. To treat potential hypoglycemic episodes (blood glucose below 70 mg/dL) , Isabella should have access to glucose in her soccer bag, in the form of glucose tablets or gel, sugar, honey, hard candies, juices or milk. In the event Isabella ingests one of these quick-fix foods, she should recheck her blood glucose in 15 minutes and repeat treatment if it is still too low until her level is above 70 mg/dL. Patients, parents, coaches and even teammates can be taught to recognize symptoms of hypoglycemia such as jitteriness, sweats (though this may be a difficult symptom to interpret during exercise), and decreased alertness. Emergency plans should be reviewed, including what to do when the child’s level of consciousness impairs the ability to ingest quick-fix foods. In such cases, glucose gel can often be placed under the patient’s tongue, where sublingual absorption may restore normal glucose levels. A health care provider can also provide a glucagon injection kit, which will rapidly bring the blood sugar back to normal and help the person regain consciousness. For patients under poor glycemic control with hyperglycemia and ketosis, exercise may need to be avoided as the added stress may worsen metabolic control. References Cooke and Plotnick (2008). Type 1 Diabetes Mellitus in Pediatrics. Pediatrics in Review 29:374-385. National Diabetes Information Clearinghouse (http://diabetes.nih.gov/dm/pubs/hypoglycemia/)

44
PATHOPHYSIOLOGY/TREATMENT OF PEDIATRIC BONE AND JOINT INFECTIONS CLIPP QFC 17-4 & 17-5 – Basic Science Resource Guide
Carrie Phillipi, MD Discuss the pathophysiology of septic arthritis and osteomyelitis in children. How is it different than that seen in adults? What if Emily presented with a fever to 104 for the previous 4 days, had elevated inflammatory markers (CRP 5.3 (normal < 0.8; ESR 50 (normal <10)) and you decided she has septic arthritis. What antibiotics would you give her? Explain your rationale for antibiotic choice, including which microbes you are covering and how well antibiotics penetrate into joint spaces and bones. Osteomyelitis and septic arthritis are two of the more common invasive bacterial infections causing hospitalization and prolonged antibiotic therapy in children. Although bacteria are the most common pathogens, fungi, parasites and other microorganisms can also be responsible for disease. Both infections typically result from hematogenous spread to bone and joint spaces in growing children (acute hematogenous osteomyelitis/septic arthritis from transient bacteremia). The anatomy of the blood vessel supply to the epiphyses of growing bones and the rich blood supply to the joint synovial membrane contributes to the pathophysiology of bone and joint infections seen in children; the majority of cases of de novo osteomyelitis and septic arthritis are seen in the first two decades of life. The most typical sites for osteomyelitis include the metaphyses of long bones such as the tibia, femur and humerus. The metaphyses lie adjacent to the epiphyseal growth plates which are nourished by capillary beds fed by the nutrient branch of the nutrient artery. The capillaries then drain into large and slow draining sinusoidal veins in the bone marrow. Emboli or trauma can lead to vessel occlusion allowing infection to establish at the sites of sluggish blood flow in the sinusoidal veins. Osteomyelitis and septic arthritis may also occur after penetrating trauma or from direct extension, but this is less common. Septic arthritis most commonly presents in joints with an intra-articular metaphysis such as the hip, shoulder, ankle and elbow and may occur in combination with an adjacent osteomyelitis. In all age groups, Staphylococcus aureus is by far the most common organism responsible for osteomyelitis in children. S. aureus has the specific ability to adhere directly to type I collagen in bone fibrils, replicating and giving rise to colonies surrounded by protective glycocalyx. By-products of S. aureus stimulate host inflammatory responses leading to further injury, exudate under pressure and impaired drainage. Focal bone necrosis ensues and the host has limited ability to reabsorb necrotic bone given further compromised sinusoidal drainage. Haemophilus influenzae was a common pathogen before the onset of widespread vaccination in the 1990s and should be considered when immunization is inadequate. Group A Streptococci and Streptococcus pneumoniae may also cause disease, and in neonates Group B Streptococcus must be considered. Children with sickle cell disease may acquire bone and joint infections from Salmonella, but S. aureus is still the most common pathogen in this population. Neisseria gonorrhoeae is a rare cause, but should be considered in sexually active adolescents. Recently, Kingella kingae has been increasingly recognized as a common etiology of bone and joint infection in children, in part due to better detection techniques.
45
After appropriate volume blood cultures have been obtained, Emily’s initial therapy should be directed against S. aureus. In the era of methicillin-resistant S. aureus, Vancomycin or clindamycin (if >90% community isolates are susceptible) should be initiated promptly and empirically. Vancomycin should be initated in all toxic- appearing children. K. kingae is readily sensitive to b-lactam antibiotics and should be considered when initial cultures fail to yield an organism or when response to empiric therapy directed against S. aureus is poor. Septic arthritis can be a surgical emergency and antimicrobial therapy should be administered in concert with surgical washout or needle arthrocentesis. In the absence of prompt intervention, increased intra-articular presuure may compromise blood flow and lead to loss of bone and joint destruction, particularly at the hip or shoulder of infants. . The need for surgical intervention must also be assessed in osteomyelitis. Subperiosteal abscesses, soft tissue abscesses and intramedullary pus should be drained. Antimicrobial penetration of necrotic bone presents a challenge, and high serum levels of antimicrobials may be required to achieve a clinical response. Therapy for osteomyelitis is often continued for 4-6 weeks, requiring placement of a long-term intravenous catheter for prolonged therapy after discharge from initial hospitalization. New data suggest that early transition to oral antimicrobials to complete the the treatment course may be a viable option in some cases of uncomplicated pediatric acute osteomyelitis if a pathogen is identified, a rapid response to therapy occurs, and adherence to oral therapy is likely. In these instances, dosing higher than standard dosing is utilized, and therapeutic drug monitoring may be recommended. As opposed to bone, antibiotic penetration of joint spaces occurs readily and, because of slow efflux from the space, intra-articular concentrations often exceed serum values prior to subsequent dosing. For these reasons, direct injection into the joint space is usually unnecessary. The minimum duration of intravenous antimicrobial therapy for joint infections is generally considered to be three weeks. References Feigin and Cherry, 5th edition, pp. 713-735
Prolonged Intravenous Therapy Versus Early Transition to Oral Antimicrobial Therapy for Acute Osteomyelitis in Children. Pediatrics 2009;123;636
Kingella kingae: An Emerging Pathogen in Young Children. Pediatrics 2011;127;557

46
PROSTAGLANDIN E IN CONGENITAL HEART DISEASE CLIPP QFC 18-4 – Basic Science Resource Guide
Carrie Phillipi, MD
Discuss the effects of prostaglandin E and indications for its use in congenital heart disease. The ductus arteriosus (DA) is an essential fetal structure connecting the pulmonary artery to the aorta. Only a small portion of right ventricular output in the fetus flows through the lungs. The patent ductus ateriosus permits diversion of right ventricular output away from the high-resistance pulmonary circulation and into the aorta. Ductal patency during fetal life is controlled mainly by low fetal oxygen tension and cyclooxygenase-mediated products of arachidonic acid metabolism (specifically prostaglandin E (PGE)). The ductus differs from surrounding vessels in having high concentrations of ductal prostenoid receptors. Locally-produced PGE, as well as circulating PGE from the placenta, stimulates vasodilation of the fetal ductus arteriosis; when fetal oxygen tension rises at birth and placental PGE is no longer circulating and/or is metabolized in the now-functioning lungs, the ductus constricts. As smooth muscle fibers contract, the ductal wall is thickened and shortened with eventual obliteration of the lumen. In the normal newborn, the ductus is functionally closed within 24-48 hours. Fibrosis typically leads to permanent structural closure over the next two to three weeks, leaving the ligamentum arteriosum as the remnant of the ductus arteriosus. Patency beyond the first weeks of life is abnormal and can result in left-right shunting with pulmonary overcirculation later in life.
(Image from http://www.pediatricheartspecialists.com/articles/detail/patent_ductus_arteriosus)
In some forms of congenital heart disease, however, a patent ductus ateriosus may be the only connection between the pulmonary and systemic circulations. Examples of such “ductal-dependent” cardiac lesions include critical aortic stenosis, aortic coarctation and transposition of the great arteries (with an intact ventricular septum). In such cases, infants tend to become severely ill over the first several days of life (rather than at delivery), and maintenance of ductal patency by intravenous administration of exogenous PGE may be life-saving. This therapy may allow for planned repairs of ductal-dependent congenital heart disease. Prior to the use of prostaglandin, reparative efforts for such lesions were often emergencies frequently occurring under desperate conditions.

47
References Schneider, D, and J Moore (2006). Patent Ductus Arteriosus. Circulation 114:1873-1882.

48
HYPEROXIA TESTING CLIPP QFC 18-5 – Basic Science Resource Guide
Carrie Phillipi, MD
Describe how to perform a hyperoxia test on a newborn with cyanosis. How does a response to oxygen affect your differential diagnosis? The hyperoxia test is used to distinguish pulmonary disease from congenital heart disease in a cyanotic newborn. In the presence of cyanotic heart disease, newborns will not usually raise their arterial PaO2 during administration of 100% oxygen. If the PaO2 rises above 150 mmHg with the application of 100% oxygen, an intracardiac shunt can usually be excluded. In contrast, ventilation-perfusion inequalities from pulmonary disease can generally be overcome by oxygen administration. A test approximating the hyperoxia test includes measuring pulse oximetry (rather than PaO2 on blood gas analysis) before and after application of 100% oxygen. Hypoxia from pulmonary pathology is often corrected (or significantly improved) after oxygen administration, whereas a cardiac mixing lesion will be minimally affected. Clinical Significance Since 2011, universal pulse oximetry testing has been recommended as a means for screening all healthy-appearing newborns for critical congenital heart disease. These recommendations target seven cardiac defects which typically include cyanosis as part of the clinical presentation: hypoplastic left heart syndrome; pulmonary atresia; tetralogy of Fallot; total anomalous pulmonary venous return; transposition of the great arteries; tricuspid atresia; and truncus arteriosus.
A healthy newborn in room air should be fully saturated after the first 24 hours of life, with an oxygen saturation of >95% assessed in the right hand and either foot, and <3% difference in SpO2 between the two extremities. SpO2 90-94% in room air, or a difference >3%, is equivocal and should be repeated in one hour; three such results constitutes a failed screen. Any SpO2 <90% in room air is a failed screen. A failed pulse oximetry screen indicates the need for further evaluation and assessment. It is not pathognomonic for heart disease. The hyperoxia test is a quick, readily available test that may help guide prioritization of differential diagnosis following a failed screen. It is not an adequate substitute for an echocardiogram, however, and this test (preferably in consultation with a pediatric cardiologist) should be performed in the absence of findings to explain a neonate’s hypoxemia. References Kemper AR et al. Strategies for Implementing Screening for Critical Congenital Heart Disease. Pediatrics 2011; 128: e1259. Nelson’s Textbook of Pediatrics. 15th Edition. pp. 1311

49
PHYSICAL EXAM MANEUVERS IN EVALUATION OF CARDIAC MURMURS CLIPP QFC 18-6 –Basic Science Resource Guide
Carrie Phillipi, MD How does each of the following affect a patient’s cardiac exam: Inhalation vs. exhalation? Lying vs. standing? Valsalva maneuver/squatting? The cardiac exam involves more than just listening to the heart. A complete heart exam includes inspection, palpation and auscultation across the precordium, evaluation for the presence of hepatosplenomegaly and assessment of peripheral pulses. The cardiac exam changes with respiration. These changes are mainly explained by changes in venous return to the heart. Recall that the first hear sound is caused by the closure of the atrioventricular (mitral and tricuspid) valves, while the second heart sound is caused by closure of the semilunar (aortic and pulmonic) valves. During inhalation, decreased intrathoracic pressure results in increased systemic venous return, increased right-sided heart filling, prolonged right ventricular ejection time. The decreased intrathoracic pressure has the opposite effects on pulmonary venous return, decreasing left-sided heart filling and shortening left ventricular ejection time. The relative delay in pulmonary valve closure, as compared to the aortic valve, produces the so-called “physiologic split S2”. Exhalation increases intrathoracic pressure, limiting systemic venous return to the heart while increasing pulmonary venous return; the temporal gap between closure of the two semilunar valves is diminished, typically eliminating any audible spilt in S2. An atrial septal defect (ASD) negates this physiology, as left-to-right inter-atrial blood flow increases right-sided heart filling irrespective of the respiratory cycle and often produces a “fixed” split S2. By increasing left-sided cardiac filling volumes, exhalation often accentuates left-sided murmurs (especially aortic). Changes in position also alter systemic venous return. Systemic venous return increases with lying and decreases with sitting/standing due to the effects of gravity. Squatting promotes venous return from the legs while increasing peripheral vascular resistance, resulting in increased left ventricular volume; this may decrease the tendency of the mitral valve to prolapse. Squatting may also help to differentiate aortic stenosis from hypertrophic cardiomyopathy: the increased left ventricular volume will increase the murmur of aortic stenosis, while it partially relieves the left ventricular outflow obstruction of hypertrophic cardiomyopathy. Standing produces the opposite effects of squatting. Likewise, the Valsalva maneuver decreases systemic venous return; if maintained for a few seconds, left ventricular volume and output will drop as well. Benign murmurs in childhood therefore are commonly attenuated with maneuvers that decrease cardiac return (e.g. sitting, standing, Valsalva) and intensified by maneuvers (e.g. lying, squatting) or conditions (e.g. fever, exercise, anemia) that increase cardiac output. On occasion, these maneuvers may be therapeutic (and not just diagnostic). “Tet spells” are acute cyanotic episodes seen in children with uncorrected Tetralogy of Fallot (TOF). The spells signify right-to-left shunting leading to decreased pulmonary blood flow. Crying is a common trigger for Tet spells: prolonged exhalation and a Valsalva maneuver combine to increase intrathoracic pressure and decrease cardiac return and pulmonary blood flow. Conversely, squatting decreases blood flow to the legs, increases systemic venous return and increases systemic vascular resistance, thereby directing more cardiac output to the lungs. Care givers may be instructed to raise an infant’s knees to the chest to help relieve Tet spells, and some infants even learn to adopt a knee-chest posture when necessary. Exercise is another common trigger for Tet spells. Exercising muscles require more oxygen delivery, so vascular beds dilate.

50
Peripheral vasodilation results in decreased systemic vascular resistance and promotes systemic blood flow at the expense of pulmonary flow. In addition, exercising muscles extract oxygen from arterial blood with greater efficiency. The blood returning to the heart has lower oxygen content. Squatting allows the oxygen debt accumulated in the muscles to be paid off over a longer period of time, maintaining higher arterial oxygen saturation. Though seen less often since the advent of early surgical correction, older children with unrepaired TOF often learn to squat for symptomatic relief. References Squatting in Fallot's Tetralogy (1968). British Medical Journal p. 470

51
PATHOPHYSIOLOGY AND TREATMENT OF MIGRAINE HEADACHES CLIPP QFC 20-3 & 20-4 – Basic Science Resource Guide
Carrie Phillipi, MD Discuss the mechanisms of pain with headaches due to migraines. Discuss the mechanisms of action for common treatments of migraine headaches in children. Headache (HA) is a frequently encountered chief complaint in pediatric offices as well as a common source of referral to pediatric neurologists. HA can be primary (without identified etiology) or secondary (occurring as sequela of an underlying etiology such as trauma or infection). Fig. 1 -‐ International Classification of Headache Disorders
PRIMARY HEADACHES SECONDARY HEADACHES 1. Migraine 2. Tension-‐type headache (TTH) 3. Cluster headache and other
trigeminal autonomic cephalalgias
4. Other primary headaches
1. Headache attributed to head and/or neck trauma
2. Headache attributed to cranial or cervical vascular disorder
3. Headache attributed to non-‐vascular intracranial disorder
4. Headache attributed to a substance or its withdrawal
5. Headache attributed to infection 6. Headache attributed to disorder of
homoeostasis 7. Headache or facial pain attributed to
disorder of cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, or other facial or cranial structures
8. Headache attributed to psychiatric disorder
Because primary headaches, by definition, lack an identifiable etiology, diagnostic criteria for these headache disorders are clinical and descriptive. Migraine headaches are among the most common primary headache Mechanisms of pain with migraine headaches Both the mechanism of migraines and the etiology of pain from migraine are incompletely understood. However, they are thought to be “trigeminovascular” (or simply neurovascular) in origin, indicating the interplay between activation of the trigeminal complex by the brain, where migraines start, and a “second hit” due to vascular inflammation, mainly in the meninges. This creates a vicious cycle of inflammation/leaky vessels spreading pain signals, pain neurons being stimulated by these chemicals and relaying the pain signal back, which then leads to more inflammation.

52
More specifically, migraines may be initiated by an electrophysiologic event or cortical spreading depression (CSD). Depolarization of neurons and release of constituents from neurons and glia seem to be the candidate event occurring prior to HA onset. This may involve a variety of neuronal transmitters including 5-HT receptor populations and even triggers from the circulation or blood vessel wall. The excitatory amino acid glutamate and NMDA receptors are also thought to be involved, as topical or injected NMDA can trigger CSD. Familial hemiplegic migraine is caused by a gain of function mutation in a calcium channel controlling glutamate release, further implicating its involvement. Pain may be caused by a wave of CSD moving along the cortex releasing potassium, arachidonic acid, hydrogen ions and nitric oxide. This leads to depolarization of the trigeminal afferent loop of the reflex arc, in turn leading to brainstem activation. Parasympathetic efferents and trigeminal activation are proposed to cause resultant vasodilation, and plasma leakage within the dura mater (2). Mechanisms of action for acute treatment of migraine headaches in children. Treatment for migraine HA includes acute and preventive pharmacologic therapy, prevention strategies and bio-behavioral interventions. Two groups of medications have been identified as mainstays of acute pharmacologic therapy: analgesics, including non-steroidal anti-inflammatories (NSAIDs) and acetaminophen, and triptans. Prostaglandins are among the primary mediators of inflammation, pain and fever in the body. The synthesis of prostaglandin H2 (PGH2) takes place in two steps, occurring at spatially separate active sites on the enzyme Prostaglandin H2 synthase: a cyclooxygenase (COX) site and a peroxidase (POX) site: COX POX Arachadonic Hydroperoxide Prostaglandin H2 acid prostaglandin G2 NSAIDs (e.g. ibuprofen, naproxen, aspirin) work by blocking the cyclooxygenase enzymes (COX-1 and COX-2). Though the mechanism of acetaminophen is less well understood, it is also thought to act by inhibiting cyclooxygenase. Unlike NSAIDs, acetaminophen works primarily in the CNS and does not inhibit cyclooxygenase in peripheral tissues and, thus, has no peripheral anti-inflammatory affects. Studies also report data suggesting that acetaminophen selectively blocks a different variant of the COX enzyme, COX-3. Finally, some have speculated that acetaminophen serves as a co-substrate for POX, further inhibiting PG synthesis. Whatever the mechanism, studies have shown that both acetaminophen and NSAIDs are effective when used early in migraine attacks, likely by blocking the cycle of inflammation. Triptans are selective serotonergic agonists with activity on 5-HT1B, 5-HT1D, and 5-HT1F receptors. The vasoconstrictive properties of triptans are mediated by an action on 5-HT1B in arterial smooth muscle. The efficacy of triptans in alleviating pain from migraines is incompletely understood, partly because the pathophysiology of migraine HA is not clearly established. It is unclear whether the mechanism of triptan action is central, peripheral or both. Although triptans are hydrophilic and do not cross the blood brain barrier well, some have hypothesized a central mechanism with disruption of the blood brain barrier during a migraine

53
attack. Triptans are available for children >12 years, especially for severe attacks or if analgesics are ineffective. Prophylactic therapy for migraine HA in children has not been well studied and no high quality randomized controls exist to direct therapy. Agents which are used for prophylaxis include antidepressants (such as amitriptyline), antihypertensives (including propranolol and Ca channel blockers), antihistamines (such as cyproheptadine) and antiepileptic medications (particularly valproate) (3). ------------------------------------------------------------------------------------------------------------------------------ References Lipton, et al. Classification of Primary Headaches. Neurology 2004; 63:427–435
M. Pathophysiology of Headache—Past and Present. Headache 2007; 47 [Suppl 1]:S58-S63.
Léonie Damen, Jacques K.J. Bruijn, Arianne P. Verhagen, Marjolein Y. Berger, Jan Passchier and Bart W Koes. Symptomatic Treatment of Migraine in Children: A Systematic Review of Medication Trials. Pediatrics 2005;116;e295 http://pediatrics.aappublications.org/content/116/2/e295.full.html DOI: 10.1542/peds.2004-2742

54
PATHOLOGY OF COMMON PEDIATRIC BRAIN TUMORS CLIPP QFC 20-5 – Basic Science Resource Guide
Carrie Phillipi, MD Review the pathological findings in common brain tumors seen in children Brain tumors are the most common solid tumor in childhood and can be roughly categorized into (1) glial tumors (gliomas) and (2) nonglial (neuronal) tumors (Table 1). These two groups can be further subclassified by anatomic location and histology. Table 1. Main Histologic Subtypes and Frequency of CNS Tumors in Children
Tumor Type Frequency (%) Gliomas
• Astrocytomas Low-‐grade (pilocytic; diffuse) vs High-‐grade (anaplastic; glioblastomas)
• Ependymomas • Gangliogliomas • Oligodendrogliomas
41.7
10.4 3.2 1.1
Nonglial (neuronal) tumors • Embryonal tumors
(e.g. medulloblastoma, PNET) • Craniopharyngiomas • Pineal tumors • Meningiomas • Others
(e.g. lymphomas, germ cell tumors, metastases)
25.7
4.4 1.3 1.2 11.0
Gliomas comprise the majority of brain tumors in childhood. They are heterogeneous and are named according to the morphologic similarity they share with different lineages of glial cells. Location is classified as supratentorial, brain stem, or cerebellar and is an important predictor of the overall prognosis. The majority of non-glial (neuronal) tumors are embryonal tumors, most importantly medulloblastomas and primitive neuroectodermal tumors (PNET’s). Medulloblastomas and PNET’s are histologically indistinguishable but have different anatomic locations: medulloblastomas are located in the posterior fossa, while PNET’s are supratentorial. Medulloblastoma is the most frequent malignant brain tumor in children. Table 2 details the most notable clinical and histopathologic features of the most common pediatric brain tumors, including pilocytic astrocytomas, high-grade astrocytic tumors, ependymomas, medulloblastomas, and PNETs.

55
Table 2. Clinical and Histopathologic Features of Common Childhood Brain Tumors Tumor Type Clinical Features Histopathology
Pilocytic Astrocytoma
-‐Most common primary brain tumor of childhood (15-‐20% pediatric primary brain tumors) -‐Favorable prognosis; 10-‐year survival rate of 96%. -‐Primarily cerebellar hemispheres, but also hypothalamic/optic pathways, thalamic region, cerebral hemispheres, brain stem, and spinal cord
-‐Non-‐infiltrating tumors; benign appearance with low-‐to-‐moderate cellularity; rare mitoses. -‐Cyst formation -‐Biphasic, ‘‘piloid’’ pattern. -‐Rosenthal fibers and eosinophilic granular bodies/protein droplets
-‐Blood vessels with glomeruloid proliferations
-‐Stain strongly positive for the astrocyte-‐marker glial fibrillary acidic protein (GFAP)
High-‐grade -‐Poor Prognosis
-‐Infiltrating tumors with high cellularity, cellular and nuclear pleomorphism, and mitotic activity

56
Astrocytomas -‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐ -‐ Anaplastic Astrocytoma -‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐ -‐Glioblastoma
-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐ Anaplastic Astrocytoma: Cerebral hemispheres but also deep midline structures of the cerebrum, and occasionally in the posterior fossa, and brain stem. -‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐ Glioblastoma: Combined frontotemporal location is particularly typical
-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐ Anaplastic astrocytoma: -‐Microvascular proliferation by multilayered vessels and necrosis are not allowed by definition. -‐ GFAP positive -‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐ Glioblastoma: -‐microscopically defined by the presence of prominent microvascular proliferation and/or necrosis -‐GFAP expression may be absent
Ependymoma -‐Primarily infratentorial
-‐10% of all pediatric brain tumors; 30% in children younger than 3 years of age
-‐Well-‐circumscribed -‐Perivascular pseudorosettes of glial tumor cells radially arranged around the blood vessels
-‐True ependymal rosettes of tumor cells that form a central lumen on their own
Medulloblastoma -‐Most common malignant childhood brain tumor; 20% to 25% of all primary brain tumors
-‐Densely packed cells with round hyperchromatic nuclei surrounded by a scanty cytoplasm; mitoses frequent

57
in children between 0 and 14 years. -‐ 2 groups: standard risk and high-‐risk patients. -‐Clinical predictors of high-‐risk patients: < 3 years; residual tumor or metastatic disease at diagnosis. -‐ Prognosis further defined by cytogenetics
-‐Neuroblastic (or Homer Wright) rosettes seen in classic histology (one of five histologic variants)
-‐Stain positive for neuronal markers, such as synaptophysin
PNET -‐Poor clinical outcome; poor
response to standard therapies -‐ Exclusively in the cerebrum (i.e. supratentorial); occasionally in the suprasellar region.
-‐Sheets of small round cells; closely related to medulloblastoma from a histological perspective
-‐Undifferentiated neuroepithelial cells -‐Divergent differentiation along neuronal, astrocytic, muscular, or melanocytic lines
Though classic histology for the most important pediatric brain tumors is described here, it should be noted that histologic assessment may be difficult, and molecular cytogenetics play an increasingly important role in establishing diagnoses, defining prognosis and suggesting opportunities for new therapeutic options. References Pfister S, Hartmann C, Korshunov A. Histology and molecular pathology of pediatric brain tumors. J Child Neurol. 2009; 24:1375-1386.
58
RENAL HISTOPATHOLOGY IN HENOCH-SCHONLEIN PURPURA CLIPP QFC 21-4 – Basic Science Resource Guide
Adam Stevenson, MD
Alex underwent a renal biopsy because he developed proteinuria and mild hypertension in addition to continued hematuria. Describe what you would expect to find on the pathology slides from the renal biopsy. Discuss how these findings explain his ongoing problems Henoch-Schönlein Purpura (HSP) is the most common vasculitis in children and is characterized by acute, leukocytoclastic inflammation of small vessels. Reported rates of renal involvement in HSP range from 40-50% and vary with age: approximately 50 percent of older children will develop renal findings, but only 25 percent of children younger than two years. In addition to increased age, the persistence of rash and the development of bloody stools are associated with an increased incidence of renal involvement. It is clear that IgA plays a central role in the pathogenesis of HSP. Of the two subclasses of IgA, IgA1 and IgA2, only IgA1 is involved in HSP. Unlike IgA2, IgA1 contains a hinge region with multiple glycosylation sites, and studies have shown that some patients have decreased glycosylation of IgA1. Such glycosylation defects lead to the presence of galactose-deficient IgA1 (Gd-IgA1), which has a propensity to form high molecular weight complexes with IgG. While all patients with HSP have been found to have circulating IgA1 immune complexes of small molecular mass, only patients with HSP nephritis have been found to have the additional, larger Gd-IgA1-IgG immune complexes. These latter immune complexes appear to be a pivotal factor in the pathogenesis of HSP nephritis. The most common clinical sign of HSP nephritis is microscopic hematuria, with or without low-grade proteinuria, though macroscopic hematuria is not uncommon. In general, patients with microscopic hematuria and trivial proteinuria have an excellent prognosis, and most patients do not undergo renal biopsy. When a biopsy is obtained (typically because of persistent or worsening proteinuria, with or without an abnormal creatinine and hypertension), the histopathology is indistinguishable from IgA nephropathy (Berger's disease). Renal histopathology typically demonstrates mesangial expansion and proliferation with IgA deposition seen on immunofluorescence. Findings may range in severity from minimal change to severe glomerulonephritis. A recent series of biopsy findings showed that cellular crescents were detected in 31% of cases and, when present, typically affected not more than 30% of the glomeruli. Moreover, of the acute glomerular lesions examined, only necrosis and extent of cellular crescents were found to carry a prognostic significance and to correlate with adverse renal outcomes. CLINICAL SIGNIFICANCE While the onset of HSP nephritis may be delayed for weeks to months after appearance of the characteristic rash, those patients who develop renal involvement do so within three months of the onset of rash (most within 4 weeks). Most ultimately recover spontaneously, but urinary abnormalities may persist for months to years. Progression to end-stage renal disease is the most serious potential long-term sequela of HSP, but this is rare (incidence <1%). Late deterioration of renal function (evidenced by rising creatinine and/or hypertension), development of nephrotic syndrome, or >50% of glomeruli with crescents seen on renal biopsy are poor prognostic indicators. Therapy for severe HSP nephritis is the subject of ongoing clinical trials; investigations have focused on potential roles for pulse-dose corticosteroids, cyclophosphamide, azathioprine and cyclosporine, among other treatments.

59
References Lau KK, et al. Pathogenesis of Henoch-Schönlein Purpura Nephritis. Pediatr Nephrol 2010; 25:19-26. Saulsbury FT. Clinical Update: Henoch-Schönlein Purpura. Lancet 2007;369:976–978 Szeto CC. Grading of Acute and Chronic Renal Lesions in Henoch-Schönlein Purpura. Mod Pathol 2001;14(7):635–640

60
DIFFERENTIAL PATHOPHYSIOLOGY OF THROMBOCYTOPENIA CLIPP QFC 21-5 – Basic Science Resource Guide
Adam Stevenson, MD Discuss the pathophysiology of the different causes of thrombocytopenia in children: ITP, infection associated (viral or bacterial), malignancy, autoimmune disease, genetic disorders. Platelets are cell fragments synthesized from bone marrow megakaryocytes. Platelets have key functions, most importantly in primary hemostasis. The bone marrow is stimulated to synthesize platelets by thrombopoietin, which is produced primarily in the liver in response to decreased numbers of bone marrow megakaryocytes or circulating platelets. Circulating platelets survive for approximately 7 to 10 days before being culled from circulation. About one third of total body platelets are transiently sequestered in the spleen at any given time. A normal platelet count is between 140,000 to 450,000/µL with thrombocytopenia defined typically as <100,000/µL. Below 60,000/µL there is a risk of bleeding with significant trauma, and below 20,000/µL spontaneous bleeding can occur. Causes of thrombocytopenia are typically classified by mechanism (see Table 1) and include:
• Decreased production (with or without normal megakaryocytes), • Destruction (both immunologic and non-immunologic), • Dilution, • Sequestration
Table 1: Classification of Thrombocytopenia
Cause Examples of Conditions
Decreased production: w/ diminished or absent megakaryocytes in bone marrow biopsy
Leukemia Aplastic anemia Myelosuppressive drugs Paroxysmal nocturnal hemoglobinuria
Decreased production: w/ normal number of megakaryocytes in bone marrow biopsy
Alcohol-‐induced thrombocytopenia HIV-‐associated thrombocytopenia Myelodysplastic syndromes (some) Vitamin B12 or folate deficiency
Destruction: Immunologic destruction
Idiopathic thrombocytopenic purpura (ITP) Drug-‐induced thrombocytopenia Neonatal alloimmune thrombocytopenia Connective tissue disorders Lymphoproliferative disorders Pregnancy (gestational thrombocytopenia) Heparin induced thrombocytopenia (HIT)
Destruction: Non-‐immunologic destruction
Disseminated intravascular coagulation Sepsis Other viral systemic infections (eg, Cytomegalovirus, hepatitis, Epstein-‐Barr virus) Thrombotic thrombocytopenic purpura Hemolytic-‐uremic syndrome

61
Dilution Massive blood replacement (platelet viability low in stored blood) Extensive crystalloid infusion
Sequestration: Platelet sequestration in enlarged spleen
Cirrhosis with congestive splenomegaly Gaucher's disease Myelofibrosis Kasabach-‐Merritt (sequestration in hemangioma, rather than spleen)
Decreased production with decreased or absent megakaryocytes: Deficiency/absence of megakaryocytes will result in thrombocytopenia. Common causes include conditions such as leukemia and aplastic anemia. Cytotoxic drugs that suppress the bone marrow activity will also result in thrombocytopenia. Decreased production with normal numbers of megakaryocytes: Even if normal numbers of megakaryocytes are found on bone marrow biopsy, they may still be inhibited in their ability to produce platelets. These disorders are relatively rare in children and include alcohol mediated toxicity, HIV, and nutritional deficiencies (vitamin B12, folate). Immune-mediated destruction: Allo- or auto-immune processes may produce antibodies that bind to platelets and mark them for destruction by splenic macrophages. Immune thrombocytopenia (ITP) is one of the most common forms of autoimmune thrombocytopenia and is thought to be due to cross reactivity between viral antigens and platelet antigens. ITP can present in either acute or chronic forms. Neonatal alloimmune thrombocytopenia is caused by maternal antibodies crossing the placenta and interacting with paternal antigens on the neonatal platelets. Many drugs can cause thrombocytopenia through deposition of antibody-drug complexes on the surface of platelets and subsequent complement activation. Though many medications have been associated with thrombocytopenia, common examples include heparin, linezolid, pipercillin, rifampin, sulfa drugs, quinidine, amiodarone, captopril, carbamazepine, ibuprofen, ranitidine, valproate and phenytoin. Non-immune mediated destruction: Destruction from a mechanism other than an antibody/antigen complex is quite common, especially in Disseminated Intravascular Coagulation (DIC), and sepsis. In these disorders, disregulated intravascular coagulation pathways are initiated and perpetuated with resultant consumption of platelets. Thrombotic Thrombocytopenia (TTP) results from the abnormal presence of high molecular weight multimers of von Willebrand protein. These large complexes are thought to trigger platelet aggregation. Similarly, the microangiopathy of Hemolytic Uremic Syndrome causes excessive activation of platelets. In both TTP and HUS, the increased consumption of platelets leads to thrombocytopenia, while thrombosis leads to microvasulature occlusion and end-organ damage. Dilution: Expansion of the blood volume with a relatively platelet free solution will decrease the concentration of platelets in circulation. Large infusion of crystalloids will decrease all indices on a complete blood count including platelets. Large infusion of whole blood or packed red blood cells will cause a relatively delayed dilution, as the low-viability platelets in the donor solution are quickly culled by the spleen.

62
Sequestration: The spleen is able to accommodate a large number of “resting” platelets that can be emergently released by epinephrine. Hence, even though the circulating platelet count is low, thrombocytopenia from sequestration is less likely to cause bleeding than other causes of thrombocytopenia. Increased splenic sequestration is suggested by splenomegaly and caused by any condition that increased the size and/or congestion of the spleen. In Kasabach-Merritt syndrome, large numbers of platelets are sequestered in large cavernous hemangiomas. Unlike splenic sequestration, platelets temporarily sequestered in hemangiomas have a foreshortened lifespan and are not released acutely in response to ephinephrine. References Chu Y. Idiopathic Thrombocytopenic Purpura, Pediatrics in Review Vol. 21 No. 3 March 1, 2000
Neunert C et al., The American Society of Hematology 2011 evidence based practice guideline for immune thrombocytopenia. Blood. 2011 Apr 21;117(16):4190-207. Epub 2011 Feb 16 Stasi R. Pathophysiology and therapeutic options in primary immune thrombocytopenia. Blood Transfus. 2011 Jul;9(3):262-73. doi: 10.2450/2010.0080-10. Epub 2010 Nov 26
63
MECHANISM OF ANTIBIOTIC ACTION IN TREATMENT OF SEXUALLY TRANSMITTED INFECTIONS
CLIPP QFC 22-7 – Basic Science Resource Guide Adam Stevenson, MD
Discuss the mechanisms of action for the common antibiotics used when treating sexually transmitted infections (STI’s). Cephalosporins Cephalosporins belong to the larger Beta-lactam class of antibiotics, along with penicillins and carbepenams. Cephalosporins are bactericidal and, like all beta-lactam antibiotics, disrupt the synthesis of the peptidoglycan layer of bacterial cell walls. The third and final step in the creation of the peptidoglycan layer is normally facilitated by transpeptidases known as penicillin binding proteins (PBPs). PBPs normally bind to the D-Ala-D-Ala end of the peptidoglycan precursors to crosslink the peptidoglycan layers. Beta lactam antibiotics mimic the D-Ala-D-Ala site and competitively inhibit PBP crosslinking. With emerging resistance to fluoroquinolones, only cephalosporins are recommended for the treatment of gonorrhea in the United States. Frequently used cephalosporins include ceftriaxone, cefotaxime and cefoxitin, all of which are available for parenteral use only. Cefixime, an oral 3rd generation cephalosporin, is no longer recommended for use as a first-line regimen in the treatment of uncomplicated gonorrhea in the U.S. due to concerns of resistance (CDC, 2012). Macrolides Macrolide antibiotics have a bacteriostatic mechanism of action as reversible protein synthesis inhibitors. Bacterial ribosomes (70S) are made up of 2 subunits (50S and 30S) containing ribosomal RNA and ribosomal proteins. The 30S subunit binds messenger RNA and begins the ribosomal cycle. The 50S subunit binds transfer RNA and controls elongation. Macrolides bind reversibly to P site on the 50S subunit of the bacterial ribosome and inhibit bacterial protein synthesis by preventing peptidyltransferase from adding the peptidyl attached to tRNA to the next amino acid. This causes dissociation of peptidyl-tRNA from the ribosome, effectively ending bacterial protein synthesis required for bacterial replication. Macrolides such as azithromycin, clarithromycin and erythromycin are recommended as first-line treatment for uncomplicated genital tract infections with Chlamydia trachomatis (though oral macrolide therapy is not sufficient for more invasive infections such as pelvic inflammatory disease). Though azithromycin is effective for uncomplicated gonococcal infections, it should not be used as first-line therapy for gonorrhea due to concerns for rapid development of macrolide resistance. Tetracyclines Like macrolides, tetracyclines inhibit bacterial protein synthesis by binding bacterial ribosomal subunit. Tetracyclines bind the 30S subunit, blocking attachment of tRNA to the A site of the ribosome. The effect is reversible, and thus bacteriostatic. Tetracyclines enter the outer membrane of gram-negative bacteria by passive diffusion through porin channels OmpF and OmpC.
Doxycycline is as effective as azithromycin for the treatment of uncomplicated Chlamydia infections and is first line therapy for treatment of pelvic inflammatory disease (PID). All tetracyclines are contraindicated for patients less than 8 years of age and in pregnant women.

64
Fluoroquinolones The majority of quinolone antibiotics in clinical use are fluoroquinolones, created from the basic quinolone antibiotic group structure in the mid-1980’s by substitution of a fluorine moiety on the standard four quinolone rings. This fluorination expanded the range of activity from typically gram negative to include gram positive activity as well. Fluoroquinolones have a bactericidal effect by interfering with bacterial DNA replication. Fluoroquinolones interact with two bacterial targets, the enzymes DNA gyrase and topoisomerase IV. These enzymes are typically used to introduce the negative superhelical twists in double stranded DNA needed for DNA unwinding and replication. Anti-topoisomerase IV activity is the likely mechanism for activity against Gram-positive bacteria. Activity against DNA gyrase is the mechanism for effectiveness against Gram-negative bacteria. Fluoroquinolones form complexes of these enzymes with DNA, and these complexes block movement of the DNA-replication strands and thus inhibit DNA replication. Clinically important fluoroquinolones include ciprofloaxcain, ofloxacin (ophthalmic use only in U.S.), levofloxacin, gatifloxacin and moxifloxacin. Quinolones are no longer recommended in the United States for the treatment of gonorrhea due to the prevalence of quinolone-resistant strains. However, fluoroqinolones are still widely used worldwide due to their availability and convenience. Metronidazole Metronidazole is the recommended treatment for bacterial vaginosis and trichomoniasis. Metronidazole (α-hydroxyethyl-2-methyl-5-nitroimidazole) is a 5-nitroimidazole, a heterocyclic compound with a nitro group on the fifth position of an imidazole ring. It is derived from the Streptomyces antibiotic azomycin. Metronidazole is a small molecule that enters T. vaginalis via passive diffusion. The drug itself is inactive, but within the hydrogenosomes of T. vaginalis the nitro group is reduced anaerobically to form a cytotoxic nitro radical anion. This nitro radical is hypothesized to bind transiently to DNA, disrupting or breaking the strands and leading to cell death. The nitro radical is thought to target sections of DNA rich in thymine and adenine residues for disruption, since studies have shown that maximal damage is observed in DNA rich in these nucleotides. In vitro, the response of T. vaginalis to metronidazole is rapid. DNA synthesis is inhibited within 30 minutes, and cell death occurs in 5 hours. Anti-virals Genital herpes is one of the most common viral STI’s that is treated with antiviral chemotherapeutics. Three antivirals have been shown to have clinical efficacy in randomized control trials – acyclovir, valacyclovir and famciclovir. Acyclovir (9-[2-hydroxymethyl]guanine) is a nucleoside analog which selectively inhibits the replication of herpes simplex virus. After intracellular uptake, the acyclovir molecule is converted to acyclovir monophosphate by thymidine kinase. Because the thymidine kinase is virally encoded, this step occurs to a significant degree only in infected cells. The monophosphate derivative is further converted to acyclovir triphosphate by cellular enzymes. Acyclovir triphosphate acts directly as an competitive analog to the nucleoside deoxyguanosine triphosphate (dGTP). Incorporation of acyclovir triphosphate into DNA results in chain termination because the absence of a 3' hydroxyl group prevents the attachment of further nucleosides. Valacyclovir and famciclovir have similar mechanisms of action as acyclovir. Valacyclovir is a valine ester pro-drug of acyclovir and has enhanced absorption after oral administration.
65
Famciclovir, a pro-drug of penciclovir, also has high bioavailability but appears somewhat less effective for suppression therapy compares to acyclovir and valacyclovir. References Cudmore SL, Delgaty KL, Hayward-McClelland SF, Petrin DP, and Garber GE. Treatment of Infections Caused by Metronidazole-Resistant Trichomonas vaginalis. Clin Microbiol Rev. 2004 October; 17(4): 783–793. doi: 10.1128/CMR.17.4.783-793.2004
Declerck PJ, De Ranter CJ. In vitro reductive activation of nitroimidazoles. Biochem Pharmacol. 1986 Jan 1; 35(1):59-61. Hooper DC. Mechanisms of action and resistance of older and newer fluoroquinolones. Clin Infect Dis. 2000 Aug;31 Suppl 2:S24-8. Mertz GJ, et al. (Collaborative Famciclovir Genital Herpes Research Group). Oral famciclovir for suppression of recurrent genital herpes simplex virus infection in women: a multicenter, double-blind, placebo-controlled trial. Arch Intern Med 1997; 157:343–49. Salvatore M, Myers BR; Tetracyclines and Chloramphenicol in Mandell: Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 7th ed. 2009 Churchill Livingstone Sexually Transmitted Diseases Treatment Guidelines 2010. MMWR: December 17, 2010 / Vol. 59 / No. RR-12 Vannuffel P, Cocito C. Mechanism of Action of Streptogramins and Macrolides. Drugs 1996:52 Suppl: 1: 20-30 Whitley RJ, Gnann JW Jr. Acyclovir: a decade later. N Engl J Med. 1992;327(11):782. Chapman A, Cammack R, Linstead D, Lloyd D. The generation of metronidazole radicals in hydrogenosomes isolated from Trichomonas vaginalis. J Gen Microbiol. 1985 Sep; 131(9):2141-4. Wolfson JS, Hooper DC. The Fluoroquinolones: Structures, Mechanisms of Action and Resistance, and Spectra of Activity in Vitro. Antimicrobial Agents and Chemotherapy, Oct 1985, 581-586
66
MENINGOCOCCAL DISEASE – PATHOPHYSIOLOGY AND PREVENTION CLIPP QFC 23-4 – Basic Science Resource Guide
Adam Stevenson, MD
Discuss the pathogenesis (how people become ill) with meningococcemia. What implications does this have on recommendations about immunizations against this organism? Microbiology Neisseria meningitidis, or meningococcus, is an aerobic, gram-negative diplococcus, closely related to N. gonorrhoeae. The outer membrane of the meningococcus is surrounded by a polysaccharide capsule that is essential in allowing the bacteria to resist macrophage phagocytosis and complement-mediated lysis. The outer membrane proteins and the capsular polysaccharide make up the main surface antigens of the bacteria. Meningococci are classified based on the structure of the outer polysaccharide capsule. Thirteen antigenically distinct polysaccharide capsules have been discovered. Some meningococcal strains are not typable and do not have a capsule – hence they often exist as asymptomatic nasopharyngeal flora. Almost all invasive disease is caused by one of five serogroups: A, B, C, Y, and W-135. Geographic variation exists; for example, serogroup A is a major cause of disease in sub-Saharan Africa, but is rarely found in the United States. Pathogenesis Meningococcus is transmitted by aerosolized droplet or secretions. The bacteria attach to the mucosal cells of the host nasopharynx and begin to multiply. An antecedent upper respiratory infection may be a contributing factor in acquisition and replication. The incubation period of meningococcal disease is 3 to 4 days, with a range of 2 to 10 days. Once established in the nasopharynx, the organism penetrates the mucosal cells in less than 1% of colonized persons, and enters the bloodstream. Hematogenous spread to multiple organs is common, particularly the skin, joints and meninges. Meningitis is the most common presentation of invasive meningococcal disease, occurring in approximately 50-60% of patients with meningococcal bacteremia. Meningococcal sepsis (bloodstream infection or meningococcemia) without meningitis occurs in 5% to 20% of invasive meningococcal infections. This condition has a significant morbidity that is quite rapid in onset. The case-fatality rate of all invasive meningococcal disease is 9% to 12%, even with appropriate antibiotic therapy. The fatality rate of meningococcemia is up to 40%. Sepsis is characterized by abrupt onset of fever and a petechial or purpuric rash, hypotension, shock, acute adrenal hemorrhage, and multi-organ failure. The virulence of Neisseria meningitidis is 100 times that of other gram-negative organisms, making prompt recognition and treatment essential to prevent significant morbidity and mortality. Less common presentations of meningococcal disease include pneumonia (5% to 15% of cases), arthritis (2%), otitis media (1%), and epiglottitis (less than 1%). Risk factors for the development of meningococcal disease include deficiencies in the terminal common complement pathway and functional or anatomic asplenia. Persons with HIV infection are also at increased risk for meningococcal disease (though not as high as patients with asplenia or complement deficiencies). Certain genetic factors (such as polymorphisms in the genes for mannose-binding lectin and tumor necrosis factor) may also be risk factors.

67
Vaccination Vaccination against meningococcal disease is made difficult by the outer polysaccharide layer. The response to the polysaccharide vaccine is typical of a T-cell independent antigen, with an age-dependent response, and poor immunogenicity in children younger than 2 years of age. Vaccine response is more robust when the epitope is protein derivative. Meningococcal Polysaccharide Vaccine (MSPV) The first monovalent (group C) polysaccharide vaccine was licensed in the United States in 1974. A quadrivalent (A, C, Y, W-135) polysaccharide vaccine was licensed in 1978 (Menomune, sanofi pasteur) Each dose consists of 50 mcg of each of the four purified bacterial capsular polysaccharides. The vaccine contains lactose as a stabilizer. The characteristics of MPSV4 are similar to other polysaccharide vaccines (e.g. pneumococcal polysaccharide). The response to the polysaccharide is typical of a T-cell independent antigen, with an age-dependent response and poor immunogenicity in children younger than 2 years of age. In addition, little boost in antibody titer occurs with repeated doses; the antibody which is produced is relatively low-affinity IgM, and “switching” from IgM to IgG production is poor. A protective level of antibody is usually achieved within 7–10 days of vaccination. Although vaccine-induced protection likely persists in school-aged children and adults for at least three years, the efficacy of the group A vaccine in children younger than 5 years of age may decrease markedly within this period. In one study, efficacy declined from more than 90% to less than 10% three years after vaccination among children who were younger than 4 years of age when vaccinated; efficacy was 67% after three years among children who were older than 4 years of age at vaccination. In healthy adults, antibody levels also decrease over time, but antibodies are detectable as long as 10 years after vaccination. Meningococcal Conjugate Vaccine (MCV) Polysaccharides can be joined, or conjugated, to protein derivatives in order to increase their immunogenicity. A common protein conjugate is the tetanus toxoid protein which is highly immunogenic. Conjugation has been successful in pneuomococcal vaccines as well as meningococcal vaccines. In the meningococcus, reactive aldehyde groups are strategically introduced into the terminal residues of the meningococcal polysaccharides by controlled periodate oxidation. This produces essentially monovalent polysaccharide molecules, which are subsequently covalently linked to tetanus toxoid. Tetanus toxoid conjugates produced high levels of polysaccharide-specific antibodies, above that of pure polysaccharide molecules. Meningococcal conjugate vaccine has been licensed in United Kingdom since 1999 and has had a major impact on the incidence of type C meningococcal disease. A quadrivalent conjugate vaccine was first licensed in the United States in 2005. Two meningococcal conjugate vaccines are now licensed in the United States. Menactra (Sanofi Pasteur) was licensed in 2005. The vaccine contains N. meningiditis serogroups A, C, Y and W-135 capsular polysaccharide antigens conjugated to diphtheria toxoid protein. Menactra was initially approved for use in persons 2 through 55 years of age, though it has subsequently been licensed for use among infants and toddlers aged 9 through 23 months. The approval of Menactra was based on studies that compared the serologic response to a single dose to the response of persons of similar age who received a single dose of meningococcal polysaccharide vaccine. In these studies a similar proportion of recipients achieved at least a fourfold rise in serum bactericidal antibody titer assay following MCV4 as those who received MPSV4. The proportion of recipients in each group that achieved a titer of 1:128 (the titer considered to predict protection) was more than 98% in both groups. Menveo (Novartis) was licensed in the United States in 2010. It, too, is a conjugate vaccine utilizing serogroups A, C, Y and W135. Menveo is also approved for use in persons 2 through 55 years of age.

68
Hib-MenCY-TT (MenHibrix, GlaxoSmithKline) was licensed by FDA in June 2012. Hib-MenCY-TT is approved by the FDA as a 4-dose series for children aged 6 weeks through 18 months. When MCV4 vaccine was licensed in 2005 it was believed that a single dose would provide protection for at least 10 years. Since that time serologic data have become available that show a significant decline in antibody 3 to 5 years after vaccination, although few cases among vaccinated persons have been reported. ACIP believes the serologic data are sufficiently compelling to recommend revaccination for persons at highest risk of meningococcal disease:
- Asplenia or Complement deficiencies: 4 dose primary series if 2-18 months old // 2 dose primary series if 2-55 years old booster doses every 5 years -Adolescents: single dose at 11-12 years old booster dose at 16 years old; if over age 16 years when first dose is given, then no booster is needed unless patient develops risk factor - Foreign travel to/residence in endemic area (e.g. the “meningitis belt” of sub-Saharan Africa): vaccination within three years of travel, then booster every five years if residing in/returning to area
References Cohen AC, et al. Prevention and Control of Meningococcal Disease: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR March 22, 2013 62(RR02);1-22 Conterno LO, da Silva Filho CR, Ruggeberg JU, Heath PT. Conjugate vaccines for preventing meningococcal C meningitis and septicaemia. Cochrane Database Syst Rev. 2011 Jul 6;(7):CD001834. Handbook of Meningococcal Disease: Infection Biology, Vaccination, Clinical edited by Matthias Frosch, Martin C. J. Maiden Jennings HJ and Lugowski C. Immunochemistry of groups A, B, and C meningococcal polysaccharide- tetanus toxoid conjugates. The Journal of Immunology 1981 127(3): 1011-1018 Meningococcal Disease. Epidemiology and Prevention of Vaccine-Preventable Diseases The Pink Book: Course Textbook - 12th Edition (April 2011) Milonovich LM. Meningococcemia: epidemiology, pathophysiology, and management. J Pediatr Health Care. 2007 Mar-Apr;21(2):75-80.

69
TOXICITY AND TREATMENT IN TRICYCLIC OVERDOSE CLIPP QFC 24-3 – Basic Science Resource Guide
Adam Stevenson, MD
Discuss the mechanisms for toxicity in tri-cyclic overdose.
Cyclic antidepressants are named for their 3-ring or 4-ring aromatic (heterocyclic) structure. They are rapidly absorbed in the GI tract and undergo first-pass metabolism in the liver. Conjugates are then renally eliminated. Cyclic antidepressants are very lipophilic and highly protein-bound, leading to large volumes of distribution. They have long elimination half-lives that often exceed 24 hours (e.g. >31-46 hours for amitriptyline). In an overdose, altered pharmacokinetics may prolong elimination and increase toxic effects. Cyclic antidepressants have significant anticholinergic effects that can delay gastric emptying. Additionally, the acidosis that results from respiratory depression and hypotension reduces protein-binding, resulting in higher serum levels of active free drug.
Significant adverse effects are generally seen only with doses greater than 20 mg/kg/d. The toxic effects of cyclic antidepressants are related to the following 4 pharmacologic effects:
• Anticholinergic effects • Direct alpha-adrenergic blockade • Inhibition of norepinephrine and serotonin reuptake in the CNS • Blockade of fast sodium channels in myocardial cells, resulting in quinidine-like
membrane-stabilizing effects
The most serious adverse effects of cyclic antidepressant toxicity are due to CNS effects and cardiovascular instability. Life-threatening cardiovascular complications are due to impaired conduction from fast sodium channel blockade. This decreases the slope of phase zero depolarization, widens the QRS complex, and prolongs the PR and QT intervals. Impaired cardiac conduction may lead to heart block and unstable ventricular arrhythmias or asystole. Cyclic antidepressants have also been shown to directly depress myocardial contractility. However, the profound hypotension seen in serious cyclic antidepressant poisoning is primarily due to vasodilatation from direct alpha-adrenergic blockade.
CNS toxicity is also a serious source of morbidity with tricyclic ingestions. Depressed mental status is generally caused by the antihistamine and anticholinergic properties of cyclic antidepressants, whereas seizures are thought to be due to increased CNS levels of biogenic amines.
Explain the potential benefit of alkalinization in the treatment of toxic tricyclic ingestions.
The use of sodium bicarbonate in tricyclic poisoning has been shown to have beneficial effects. Several mechanisms have been proposed to explain this benefit.
Studies have demonstrated that the plasma protein binding of amitriptyline increases with a more alkaline pH, thus reducing the amount of unbound, pharmacologically-active drug. Alkalinization also reduces the direct effect of acidosis on myocardial contractility.
However, benefit to alkalinization has also been found in the absence of acidosis. Studies on animal models have shown administration of hypertonic sodium chloride to be as effective as

70
sodium bicarbonate in reversing QRS prolongation and hypotension due to tricyclic toxicity. These experiments suggest that increasing the extracellular sodium concentration may be an additional mechanism underlying this therapy, and more recent studies have shown that the effects of increasing the extracellular sodium concentration and of raising the pH are independent and additive.
Finally, urine alkalinization may increase medication excretion from the kidneys. The term urine alkalinization emphasizes that urine pH manipulation, rather than a diuresis, is the prime objective of treatment. The rate of diffusion from the renal tubular lumen back into the blood is decreased when a drug is maximally ionized and increased if the drug is non-ionized. As the ionization of a weak acid is increased in an alkaline environment, manipulation of the urine pH potentially can enhance renal excretion. For each change in urine pH of one unit there is theoretically a 10-fold change in renal clearance. References Kerr, GW, et al. Tricyclic antidepressant overdose: a review. Emerg Med J 2001;18:236-241 doi:10.1136/emj.18.4.236 Proudfoot AT, et al. Position Paper on Urine Alkalinization. Clinical Toxicology, Vol. 42, No. 1, pp. 1–26, 2004 Soghoian S; Chief Editor: Timothy E Corden, MD. Tricyclic Antidepressant Toxicity in Pediatrics. Medscape True BL, Perry PJ, Burns EA. Profound hypoglycemia with the addition of a tricyclic antidepressant to maintenance sulfonylurea therapy. Am J Psychiatry 1987 Nov;144(11):1521.

71
PATHOPHYSIOLOGY OF APNEA IN CHILDREN CLIPP QFC 25-4 – Basic Science Resource Guide
Halana Whitehead and James Campbell Discuss the underlying mechanisms/pathophysiology of apnea for the following pediatric syndromes: obstructive apnea, apnea associated with seizures, apnea associated with infection (e.g. pertussis, RSV) and apnea associated with arrhythmia. Definition & Types of Apnea Apnea is an interruption of respiratory airflow. Pathologic apnea is considered to last 20 seconds or longer, but any respiratory pause associated with physiologic changes (e.g. bradycardia, cyanosis, pallor, and/or loss of tone) is significant. It is important to differentiate this from periodic breathing, a common benign finding in neonates, Apnea can be classified into three main types according to underlying mechanism: (1) central, (2) obstructive, and (3) mixed.
Central apnea results from a lack of respiratory effort. This can be due to the failure of the central respiratory centers to trigger inspiration or the inability of the efferent nerves and muscles to enact central respiratory signals. Clinically, central apnea is characterized by the absence of chest rise or breath sounds during the episode. Risk factors include: - prematurity, -CNS insults (infection, trauma), -intoxication (ethanol, opiates, barbiturates), -respiratory infections in early infancy (see below) Obstructive apnea occurs when respiratory effort is present, but an obstruction in the airway (most often the upper airway) prevents airflow and gas exchange. On exam, chest rise is present, but the patient may be struggling to breathe through an occluded airway. Risk factors include: - excessive upper respiratory secretions, - craniofacial malformations, - hypotonia, - tonsillar/adenoidal hypertrophy, - foreign body aspiration, - intrinsic airway narrowing (subglottic stenosis, laryngo/tracheomalacia)
- airway compression (trauma, mass)
Higher Respiratory Control Centers
(Cortex, Forebrain)
Respiratory Pacemaker (Medulla)
Inspiratory muscle activation
Inspiratory airflow
Intrathoracic volume expansion
Gas exchange
Chemoreceptors
Pulmonary receptors
(J, stretch, irritant)
Obstructive apnea
Central apnea

72
Mixed apnea results from a combination of central and obstructive pathology. In mixed apnea, both decreased respiratory effort and airway obstruction contribute to the interruption of airflow. The apnea associated with gastroesophageal reflux is believed to be of this type. Apnea associated with specific pathologies Apnea associated with seizures: Apnea associated with seizures can occur through several mechanisms depending in part on the seizure type. Generalized tonic-clonic seizures may be associated with laryngeal spasm and tonic contraction of respiratory muscles, causing obstructive apnea. Some seizures may involve the higher respiratory centers, such as those in the limbic system, leading to central apnea. While it is possible to have isolated apnea as the presenting symptom for a seizure, usually apnea of this etiology is accompanied by other signs of seizure such as abnormal limb or eye movements. Apnea associated with infection: Infection can cause apnea through multiple mechanisms depending on the site. CNS infections such as meningitis can directly impact the respiratory centers of the brain leading to central apnea. Septic patients can experience apnea as a result of alterations in oxygen delivery which can prevent both transmission and activation of respiratory signals. It is important to note that apnea may be the first sign of a serious bacterial infection in an infant and should prompt further workup. Upper airway infections, such as epiglottitis or infectious mononucleosis, can cause obstructive apnea through airway occlusion. Respiratory infections, specifically pertussis and respiratory syncytial virus, can precipitate apnea in susceptible patients such as young infants. The mechanism by which RSV causes central apnea in infants remains unclear. Animal studies have implicated respiratory center inhibition caused by overproduction of GABA and substance P and alteration in the sensitivity of laryngeal chemoreceptors for triggering reflex apnea as possible mechanisms. Infants, and especially premature infants, often have diminished responses to hypercapnia, as well as paradoxical responses to hypoxia, resulting in central apnea as opposed to hyperventilation. Infants are also thought to have an exaggerated protective laryngeal reflex, and upper airway secretions may trigger obstructive apnea. The apnea seen in pertussis is likely of a mixed type and is believed to result from laryngeal spasm and vagal hyperstimulation with coughing episodes. Apnea associated with arrhythmia: Arrhythmias are less often associated with apnea than with syncope. Central apnea can be seen in the setting of arrhythmia and results from hypoperfusion of the brain. This is an uncommon cause of apnea in infants, but is more likely in infants with known congenital cardiac anomalies and/or a history of cardiac surgery. In older children, arrhythmias associated with Long QT syndrome and Wolff-Parkinson-White syndrome can cause a sudden drop in cardiac output leading to syncope, apnea and in some cases sudden death. Clinical Significance Children, and especially infants, present to medical attention frequently due to breathing irregularities. Understanding the physiology of breathing, and how it breaks down during illness, can help clinicians target likely diagnoses and focus the evaluations for these patients.
73
References National Institutes of Health Consensus Development Conference on Infantile Apnea and Home Monitoring, Sept 29 to Oct 1, 1986. Pediatrics. 1987;79(2):292. Gillam-Krakauer, M, Carter, BS. Neonatal Hypoxia and Seizures. Pediatrics in Review 2012. 33(9): 387-97 K, Sciot R and Lagae L. Apnea as the sole manifestation of a seizure attributable to meningioangiomatosis of the temporal lobe in an infant. Pediatric Neurology 47 (2012): 144-146. Katz, ES, D'Ambrosio, CM. Pathophysiology of Pediatric Obstructive Sleep Apnea. Proc Am Thorac Soc 2008. 5(2):253-62 Kliegman et al. Nelson Textbook of Pediatrics, 19th ed.
Chapter 95: Respiratory Tract Disorders Chapter 189: Pertussis Chapter 365: Respiratory Pathophysiology and Regulation Chapter 430: Sudden Death
Lindgren et al. Respiratory syncytial virus infection reinforces reflex apnea in young lambs. Pediatric Research. 1992;31(4 Pt 1):381. Matiz, A, Roman, EA. Apnea. Pediatrics in Review 2003. 24(1):32-34 Rocker JA. Pediatric Apnea. Medscape Reference. http://emedicine.medscape.com/article/8000 32 - overview#a0104 Ropper AH and Samuels MA. Adam & Victor’s Principles of Neurology, 9th ed., Chapter 16: Epilepsy and Other Seizure Disorders. Sabogal et al. Effect of respiratory syncytial virus on apnea in weanling rats. Pediatric Research. 2005 Jun; 57(6):819-25. Weinberger, Cockrill and Mandel. Principles of Pulmonary Medicine, 5th ed. (2008), Chapter17: Anatomic and Physiologic Aspects of Neural, Muscular and Chest Wall Interactions with the Lungs. Zhao J, Gonzalez F, Mu D. Apnea of prematurity: from cause to treatment. Eur J Pediatr. 2011; 170(9):1097-105.

74
SCREENING AND DIAGNOSIS FOR CYSTIC FIBROSIS CLIPP QFC 26-9 - Basic Science Resource Guide
Christopher Kim and Kathryn Bowman Explain the principles underlying various screening and diagnostic tests for cystic fibrosis, including newborn screening, sweat chloride testing, and genetic testing. Overview Cystic Fibrosis (CF) is an autosomal recessive condition characterized clinically by progressive lung disease, recurrent sinopulmonary infections, pancreatic insufficiency, nutritional deficiencies, intestinal dysfunction, hepatic disease, and/or male infertility. CF is caused by mutations of the cystic fibrosis transmembrane conductance regulator (CFTR) gene. This gene encodes a cAMP regulated Cl- channel which localizes to the plasma membrane of epithelial cells. The carrier rate for CF in the non-Hispanic white population is approximately 1/25. The many known mutations of the CFTR gene are divided into 5 categories. Class I and II mutations produce abnormal proteins which are degraded before being inserted into the membrane. Class III and IV mutations produce fully mature, yet nonfunctional proteins that are inserted into the plasma membrane. Class V mutations have abnormal splicing, but still produce small amounts of normal protein. This variation in protein function explains the range of clinical severity seen in CF patients. The CFTR chloride channel is present in many organs, including lung, pancreas, skin and the male reproductive tract. While the effect on each tissue is slightly different, disruption of chloride transport affects the passive flow of water across the mucus membranes, leading to thicker secretions and, in turn, organ dysfunction. The diagnosis of CF is established when a patient fulfills two criteria:
1. Risk factors or presentation: phenotypic features, sibling with CF, or positive newborn screen
2. Lab evidence of CFTR: two abnormal sweat chloride tests, detection of two CF-causing mutations, or abnormal nasal potential difference
Newborn Screening While there are several different screening protocols in existence, all begin with measuring immunoreactive tripsinogen (IRT). IRT is a pancreatic enzyme precursor whose concentration is elevated in infants with CF. Levels of IRT are measured from dried blood spots collected between days 1-4 of life. If elevated levels are detected, there are several common protocols for further evaluation. Because normal newborns may have transient increases in IRT, follow-up testing is necessary if the initial IRT level is elevated. Confirmatory tests for an initially elevated IRT may include a repeat IRT or genetic testing (either a DNA assay for ∆F508 or a multiple mutation DNA assay); the exact diagnostic algorithm varies by state. Repeat IRT testing requires a second blood sample, whereas genetic testing can be run on the same sample as the initial screen. Screening is not without its limitations. False negatives can occur when moderately elevated IRT levels fall below the threshold value (varies by state), or if a newborn has an uncommon mutation not included in the confirmatory DNA assay. Newborns with meconium ileus may present with normal or low IRT levels and evade detection from NBS; these patients are usually diagnosed clinically early in life.

75
Genetic Testing The most common CFTR mutation, ∆F508, was discovered in 1989. Since then, over 1900 mutations of the CFTR gene have been discovered, but only a small percentage of these mutations have been clearly proven to cause the CF phenotype. ∆F508 accounts for about 2/3 of mutations in patients with CF, and fewer than 30 mutations account for over 80% of cases. Newborn screening protocols may test either for ∆F508 alone or multiple mutations. The most widely used DNA assay panel was developed by the American College of Medical Genetics (ACMG) and includes 23 of the most common CF mutations. If one or more mutations are found on DNA analysis, the screen is considered positive. However, the great genetic heterogeneity of CF means that inability to detect two CFTR mutations does not necessarily rule out a diagnosis of CF. The American College of Obstetrics and Gynecology (ACOG) recommends that CF testing be offered to all couples planning to conceive. Due to the proportion of mutations not tested for in commercial assays, inability to detect a CFTR mutation in preconception screening does not necessarily rule out CF carrier status. Sweat Chloride Test Any newborn with a positive newborn screen (as well as any for whom there is high clinical suspicion, such as infants with meconium ileus or siblings of CF patients) should undergo sweat chloride testing to confirm or rule out CF. High levels of Cl- in sweat are indicative of CFTR dysfunction. Pilocarpine iontophoresis with quantitative chloride analysis (the “sweat test”) was originally designed by Gibson and Cooke in 1959 and remains the gold standard for CF diagnosis. An electrode pad containing pilocarpine is applied to the patients forearm. A second electrode is applied to the upper arm, and a small current is administered to stimulate sweat secretion. The patient’s arm is cleaned, and sweat is collected for 30 minutes on pre-weighed gauze for analysis. A sweat sample of 75 mg is considered adequate. Testing is often technically difficult in patients under 2 weeks of age or 2 kg body weight, and an inadequate sample collection invalidates the test results. Sweat testing should be performed preferentially at a CF center with extensive experience in the technique. With an adequate sweat collection, levels of sweat chloride greater than 60 mmol/L are diagnostic for CF. Normal sweat contains less than 40 mmol/L in infants older than 6 months, and less than 30 mmol/L in infants under 6 months. For patients whose samples contain intermediate levels of chloride, or if the sample collection is inadequate, repeat sweat chloride testing or multiple mutation DNA testing is indicated. A small proportion of patients with CF have intermediate or normal values of sweat chloride. Presence of clinical features of CF or high clinical suspicion in the presence of a normal sweat chloride test warrants further workup. Clinical Significance The carrier rate for CF in the non-Hispanic white population in the U.S. is approximately 1in 25, correlating with an incidence of 1 in 2500-3500 live births in this population. In 2004, the CDC released a statement which justified the use of newborn screening to detect CF on the grounds that early nutritional supplementation improved long term outcomes. By 2010, newborn screening for CF had become mandatory in all 50 states. Early detection, combined with preventative medical management such as prophylactic antibiotic therapy to minimize the frequency of pulmonary infections and nutritional therapy, in the form of caloric support, vitamin supplementation and exogenous pancreatic enzymes, have significantly decreased morbidity and mortality for CF patients. Average life expectancy for patients with CF has increased from
76
the teens in the 1980’s to the late thirties now, with some CF patients living beyond fifty years of age. References Boucher, R.C., Chapter 259. Cystic Fibrosis, in Harrison's Principles of Internal Medicine, F.A. Longo DL, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, Editor. 2012, McGraw-Hill: New York. De Boeck, K., Wilschanski, M., Castellani, C., Taylor, C., Cuppens, H., Dodge, J., Diagnostic Working Group. (2006). Cystic fibrosis: Terminology and diagnostic algorithms. Thorax, 61(7), 627-635. doi: 10.1136/thx.2005.043539 Farrell, P. M., Rosenstein, B. J., White, T. B., Accurso, F. J., Castellani, C., Cutting, G. R., . . . Cystic Fibrosis Foundation. (2008). Guidelines for diagnosis of cystic fibrosis in newborns through older adults: Cystic fibrosis foundation consensus report. The Journal of Pediatrics, 153(2), S4-S14. doi: 10.1016/j.jpeds.2008.05.005; 10.1016/j.jpeds.2008.05.005 Kleven, D. T., McCudden, C. R., & Willis, M. S. (2008). Cystic fibrosis: Newborn screening in America. MLO: Medical Laboratory Observer, 40(7), 16-8, 22, 24-7. Massie, R.J., et al., Lessons learned from 20 years of newborn screening for cystic fibrosis. Med J Aust, 2012. 196(1): p. 67-70 Robbins, S. L., Kumar, V., & Cotran, R. S.,. (2010). Robbins and Cotran Pathologic Basis of Disease. Philadelphia, PA: Saunders/Elsevier. Sharp, J. K., & Rock, M. J. (2008). Newborn screening for cystic fibrosis. Clinical Reviews in Allergy & Immunology, 35(3), 107-115. doi: 10.1007/s12016-008-8082-1; 10.1007/s12016-008-8082-1 Wagener, J.S., E.T. Zemanick, and M.K. Sontag, Newborn screening for cystic fibrosis. Curr Opin Pediatr, 2012. 24(3): p. 329-35.

77
ANEMIA IN CROHN’S DISEASE CLIPP QFC 27-4 - Basic Science Resource Guide:
Corinne Swearingen and Matthew Foglia
Jenny is a 12-year-old girl with Crohn’s disease. Her flares have recently become more common. At today’s visit you note that her hemoglobin is 8.5. Explain potential underlying causes for Jenny’s anemia. Anemia is quite common in pediatric patients suffering from Crohn’s disease (CD) and other inflammatory bowel disease (IBD), ranging from 40-80% depending on the study population. Pathologic processes associated with the disease or with its treatment can lead to decreased erythrocyte mass in a number of ways. These can be broadly categorized into two basic mechanisms: decreased erythrocyte production and increased erythrocyte damage or loss. ANEMIA ASSOCIATED WITH DECREASED RED CELL PRODUCTION (1) Nutrient Deficiencies One of the hallmarks of Crohn’s disease is diffuse intestinal inflammation with resultant malabsorption of nutrients, including several nutrients which play essential roles in red blood cell production Iron Dietary iron is absorbed primarily by intestinal epithelial cells in the duodenum. Iron is transported across the enterocyte basolateral membrane by ferriportin and into the circulation, where it is transported by transferring to red blood cell precursors in the bone marrow (among other cells). If the body is iron deficient, the liver increases production of transferrin, which can be measured as TIBC. If the body is iron replete, absorbed iron is preferentially stored as ferritin, a protein-iron complex found in highest levels in hepatocytes and in macrophages in the spleen and bone marrow. In addition, the liver produces hepcidin, a negative regulator of iron absorption and mobilization. High hepcidin concentrations turn off both duodenal iron absorption and release of iron from macrophages; low hepcidin concentrations promote iron absorption and heme iron recycling or iron mobilization from macrophages. Iron deficiency is one of the most common causes of anemia in patients with Crohn’s disease. In addition to general malabsorption due to mucosal inflammation, hepcidin levels are increased in response to inflammatory cytokines (see Anemia of Chronic Disease below), further impeding iron absorption and utilization. Finally, intestinal inflammation and injury are associated with both chronic and acute intestinal blood loss. Vitamin B12 Vitamin B12 is absorbed preferentially in the terminal ileum via receptors which recognize B12-intrinsic factor complexes. Though Crohn’s disease may involve any segment of the GI tract from the mouth to the rectum, the small intestine is the most common site of involvement, particularly the distal ileum (approximately one-third of patients have ileitis exclusively). Folate Several immunosuppressive medications used in treatment of Crohn’s disease, including methotrexate and sulfasalazine, interfere with folate metabolism and exacerbate the effects of folate malabsorption.
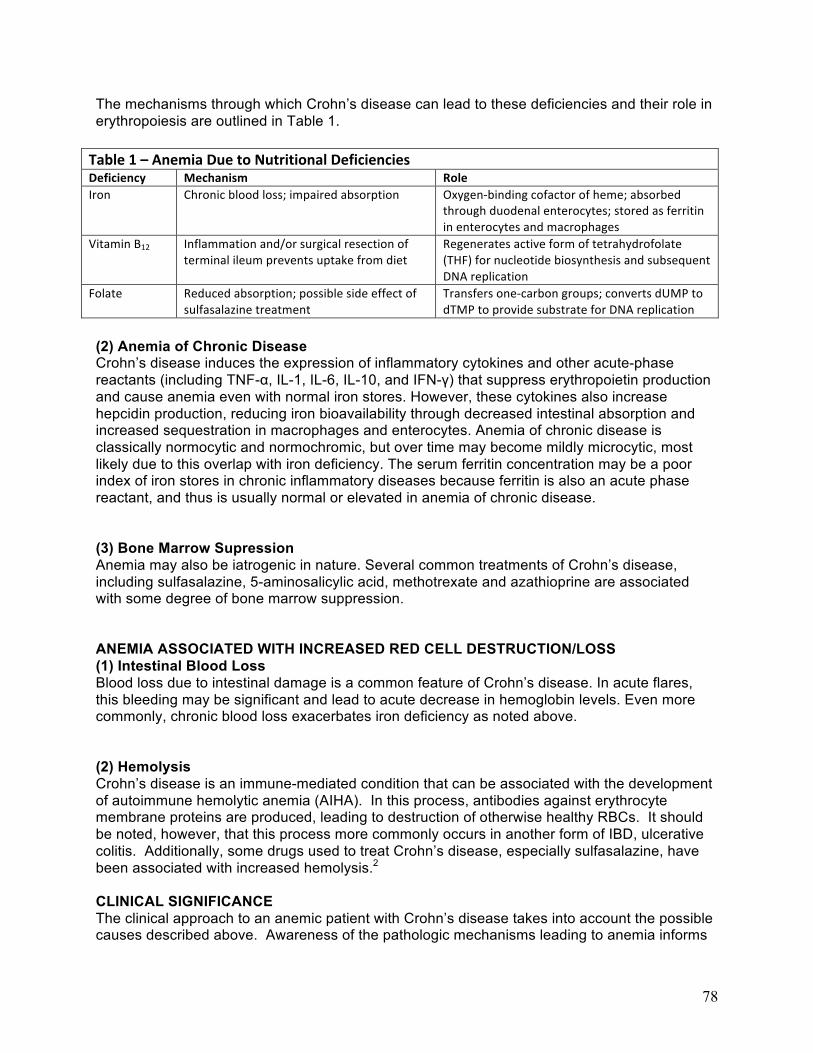
78
The mechanisms through which Crohn’s disease can lead to these deficiencies and their role in erythropoiesis are outlined in Table 1. Table 1 – Anemia Due to Nutritional Deficiencies Deficiency Mechanism Role Iron Chronic blood loss; impaired absorption Oxygen-‐binding cofactor of heme; absorbed
through duodenal enterocytes; stored as ferritin in enterocytes and macrophages
Vitamin B12 Inflammation and/or surgical resection of terminal ileum prevents uptake from diet
Regenerates active form of tetrahydrofolate (THF) for nucleotide biosynthesis and subsequent DNA replication
Folate Reduced absorption; possible side effect of sulfasalazine treatment
Transfers one-‐carbon groups; converts dUMP to dTMP to provide substrate for DNA replication
(2) Anemia of Chronic Disease Crohn’s disease induces the expression of inflammatory cytokines and other acute-phase reactants (including TNF-α, IL-1, IL-6, IL-10, and IFN-γ) that suppress erythropoietin production and cause anemia even with normal iron stores. However, these cytokines also increase hepcidin production, reducing iron bioavailability through decreased intestinal absorption and increased sequestration in macrophages and enterocytes. Anemia of chronic disease is classically normocytic and normochromic, but over time may become mildly microcytic, most likely due to this overlap with iron deficiency. The serum ferritin concentration may be a poor index of iron stores in chronic inflammatory diseases because ferritin is also an acute phase reactant, and thus is usually normal or elevated in anemia of chronic disease. (3) Bone Marrow Supression Anemia may also be iatrogenic in nature. Several common treatments of Crohn’s disease, including sulfasalazine, 5-aminosalicylic acid, methotrexate and azathioprine are associated with some degree of bone marrow suppression. ANEMIA ASSOCIATED WITH INCREASED RED CELL DESTRUCTION/LOSS (1) Intestinal Blood Loss Blood loss due to intestinal damage is a common feature of Crohn’s disease. In acute flares, this bleeding may be significant and lead to acute decrease in hemoglobin levels. Even more commonly, chronic blood loss exacerbates iron deficiency as noted above. (2) Hemolysis Crohn’s disease is an immune-mediated condition that can be associated with the development of autoimmune hemolytic anemia (AIHA). In this process, antibodies against erythrocyte membrane proteins are produced, leading to destruction of otherwise healthy RBCs. It should be noted, however, that this process more commonly occurs in another form of IBD, ulcerative colitis. Additionally, some drugs used to treat Crohn’s disease, especially sulfasalazine, have been associated with increased hemolysis.2
CLINICAL SIGNIFICANCE The clinical approach to an anemic patient with Crohn’s disease takes into account the possible causes described above. Awareness of the pathologic mechanisms leading to anemia informs

79
both the interpretation of diagnostic studies and the appropriate therapy. Differentiating between decreased production and increased destruction/loss is possible using the reticulocyte index, which measures the ability of the bone marrow to produce new erythrocytes. In patients with a poor reticulocyte response, mean corpuscular volume (MCV) distinguishes between microcytic anemia (such as iron-deficiency anemia), macrocytic anemia (commonly B12 or folate deficiency) and normocytic anemia (typically anemia if chronic disease). Serum iron, ferritin, and total iron binding capacity can help further distinguish iron-deficiency anemia from anemia of chronic disease. In patients with a brisk reticulocyte response, hemolysis or acute blood loss must be suspected. AIHA, which may be suspected based on increased lactate dehydrogenase (released from lysed erythrocytes), or serum bilirubin (a breakdown product of hemoglobin), can be confirmed with a Direct Coombs Test, which detects autoantibodies against the patient’s RBCs using an antihuman IgG. The laboratory approach to differentiating causes of anemia is outlined in Table 2. Table 2 – Lab Findings in Anemia Cause of anemia Lab findings LOW RETICULOCYTE COUNT Iron deficiency Decreased MCV / increased TIBC / decreased ferritin, Fe
Anemia of chronic disease Normal MCV (or slight decrease) / normal Fe studies
Folate or B12 deficiency Increased MCV
Bone marrow toxicity Potential suppression of other cell lines
ELEVATED RETICULOCYTE COUNT Acute blood loss Clinical evidence of blood loss / absence of evidence for hemolysis Autoimmune hemolytic anemia Increased LDH, bilirubin / + Coombs test
References Gerasimidis K, McGrogan P, and Edwards CA. The aetiology and impact of malnutrition in paediatric inflammatory bowel disease. J Human Nutrition and Dietetics, May 2011; 24(4):313-326. Gisbert JP and Gomollon F. Common Misconceptions in the Diagnosis and Management of Anemia in Inflammatory Bowel Disease. Am J Gastroenterology, May 2008; 103: 1299-1307. Kumar V, Abbas A, Fausto N, Aster J. Red blood cell and bleeding disorders. In Robbins and Cotran’s Pathologic Basis of Disease.2010;14:639-675.Elsevier Inc. Philadelphia, PA. Wilkins T, Jarvis K, Patel J. Diagnosis and Management of Crohn’s Disease. Am Fam Physician 2011; 84(12):1366-1375.
80
NEUROANATOMY OF CEREBRAL PALSY CLIPP QFC 28-4 - Basic Science Resource Guide
Grace Yau and Rita Schlanger Discuss the neuro-anatomical correlations for the common forms of cerebral palsy Introduction Cerebral palsy (CP) encompasses a heterogeneous constellation of chronic motor abnormalities that result from a non-progressive insult to the developing brain in utero, during birth, or in the perinatal period. The majority of cases can be attributed to prematurity, intrauterine growth retardation, congenital disorders, infection, asphyxia, and/or trauma. Though the neuronal damage occurs early during brain development, clinical manifestations are rarely fully apparent at birth and evolve over time. As cerebral palsy is mostly manifested as a disorder of motor tone, and tone changes with maturation and development of the nervous system, most people would refrain from diagnosing a child with cerebral palsy until after age two. Motor deficits include impaired muscle tone, strength, coordination, posture, and/or movement. While cerebral palsy describes only the motor abnormalities, many patients with CP will have associated neurologic disabilities involving sensation, behavior, cognition, communication and/or seizures. Conversely, many children with developmental delay or neurological abnormalities are labeled with “cerebral palsy” without getting a comprehensive evaluation of their underlying condition. It is very important to do a comprehensive diagnostic evaluation in these children, as “cerebral palsy” really is a descriptive term which encompasses children with abnormal motor tone and motor development from many different etiologies. Neuropathology The nature of an injury to the developing brain is determined by the timing of the injury during development and the type of insult.
In the first 20 weeks of development, congenital abnormalities, infections, and trauma can result in cerebral dysgenesis, including holoprosencephaly, schizencephaly, and polymicrogyria.
Between 26 and 34 weeks of gestation, the germinal matrix and periventricular white matter are so-called “watershed regions”, particularly susceptible to disruption of blood flow .
• Injury to the germinal matrix is manifest acutely as intraventricular hemorrhage. • Periventricular leukomalacia (PVL) describes the delayed neuroanatomical
reorganization after injury to periventricular white matter and is manifest as ventricular enlargement, gliosis of the periventricular regions, and thinning of nearby white matter tracts. Cystic PVL is indicative of more severe injuries and is associated with a poor clinical prognosis.
In the last trimester, cortical, subcortical and deep gray matter lesions, including the thalamus and basal ganglia, are more common. These gray matter lesions may be seen on neuroimaging as:
• porencephaly (which results from arterial ischemic stroke most commonly in the territory of the middle cerebral artery),
• watershed infarcts (often between the anterior and middle cerebral artery territories),
• multicystic encephalomalacia (multifocal strokes that result in a large number of cystic areas),
• abnormal bright signal, especially in the deep gray nuclei.These areas are the most metabolically active and therefore the most susceptible to loss of oxygen at

81
this time. This results in early movement disorders and so called “athetoid cerebral palsy”
Common Forms of Cerebral Palsy Cerebral palsy is traditionally classified as either (1) spastic (pyramidal) or (2) dyskinetic (extrapyramidal) based on the type of motor deficit. Spastic cerebral palsy is the most common form of CP, accounting for 70-80% of all cases. All motor impulses originate in the primary motor cortex. Nerve fibers then travel along the corticospinal tract through the internal capsule, crossing to the other side at the level of the inferior medulla. These upper motor neurons have an inhibitory effect on lower motor neurons through the release of the neurotransmitter GABA at the spinal level. Upper motor neuron lesions result in disinhibition, seen clinically as hyperreflexia, extensor Babinski reflex, hypertonia and persistence of primitive reflexes. Spastic CP is further classified by the distribution of spasticity:
• Spastic diplegia predominantly affects the legs more than the arms and face. The corticospinal tracts leading to the lower extremities run closest to the ventricles, and thus are more prone to injury than those to the upper extremities. Periventricular leukomalacia is the primary lesion seen on neuroimaging and is most commonly seen in premature infants.
• Spastic hemiplegia affects one side of the body (left or right) more than the other. It is due to a unilateral lesion of the upper motor neurons, which may be secondary to a fetal stroke , particularly in the distribution of the middle cerebral artery
• Spastic quadriplegia is the most severe form, affecting all four limbs due to global brain damage. This may be associated with congenital malformations, first trimester infections (such as rubella, CMV) or extensive hypoxic-ischemic encephalopathy. Because of the diffuse nature of the injury, spastic quadriplegia is associated with the highest rates of concomitant neurologic disorders, including mental retardation and seizures.
Dyskinetic cerebral palsy accounts for 15-20% of cases and is primarily due to lesions in deep gray matter, including the basal ganglia and thalamus. The basal ganglia is connected to the cerebral cortex and thalamus and has many functions including voluntary motor control, initiation of movement, and motor coordination. It maintains a delicate balance between excitation and inhibition of motion via multiple neurotransmitters, notably dopamine and GABA. Injury to the basal ganglia may cause extrapyramidal signs including:
• Dystonia - sustained abnormal muscle contraction causing abnormal posturing, grimacing, and drooling.
• Athetosis – involuntary, slow and writhing movements of the limbs. Although intelligence is not typically affected, children may have difficulty speaking because they are unable to coordinate the mouth muscles. Ataxic cerebral palsy is the least common form, occurring in 5-10% of cases. It results from damage to the cerebellum. Children have an unsteady, wide-based gait, difficulty with precise movements, intention tremor, and problems with balance and depth perception; unlike other forms of CP, these patients typically have low muscle tone.

82
Clinical Significance Transcranial ultrasound (possible because of the open fontanel) is quite sensitive for detecting intraventricular hemorrhage without radiation or need for prolonged imaging studies. MRI is a better imaging modality for most other brain abnormalities and detects neuroanatomical defects in 80-90% of children with cerebral palsy. White matter lesions, especially periventricular leukomalacia, are strong predictors of cerebral palsy and often the location of the lesion corresponds with the clinical impairment. Abnormal neuroanatomic findings on MRI can help with diagnosis and characterize the different forms of cerebral palsy. However, neuroimaging is limited in that it cannot determine when the lesion occurred or predict the future neurodevelopment of the child. There are also risks associated with sedation and radiation in children. Neuroanatomic findings also do not accurately predict clinical severity. There are children with cerebral palsy who have normal neuroanatomy and children with brain abnormalities that do not develop neurological impairments. The severity of cerebral palsy is based on scales that assess function and achievement of milestones over time. Cerebral palsy describes a large complex group of disorders. The multiple etiologies and anatomic lesions result in a spectrum of clinical features, comorbidities, quality of life and, ultimately, life expectancy. References McAdams, R. Juul, SE. Cerebral Palsy: Prevalence, Predictability, and Parental Counseling. NEOREVIEWS. 2011; 12(10): e564-e574 Fairhurst, C. Cerebral palsy: the whys and hows. Arch Dis Child EducPract Ed. 2012 Aug; 97(4):122-31. Wilson Jones, M. Morgan, E. Shelton, JE. Thorogood, C. Cerebral Palsy: Introduction and Diagnosis (Part 1). J Pediatr Health Care. 2007;21(3):146-152. Aisen, ML. Kerkovich, D. Mast, J. Mulroy, S. Wren, TA. Kay, RM. Rethlefsen, SA. Cerebral palsy: clinical care and neurological rehabilitation. Lancet Neurol. 2011;10(9):844-52. National Institute of Neurological Disorders and Stroke. Cerebral Palsy: Hope Through Research. NIH Publication No. 10-159. December 2009. IngeborgKrageloh-Mann , Christine Cans. Cerebral palsy update. Brain & Development 2009. 31: 537–544. Michael Johnston, AlexandarHoon. Cerebral palsy. Neuromolecular Medicine 2006. 8: 435-450. Martin Bax, Clare Tydeman, and OlofFlodmark. Clinical and MRI correlates of cerebral palsy: The European Cerebral Palsy Study. JAMA 2006. 296: 1602-1608. Rebecca Folkerth. Neuropathologic substrate of cerebral palsy. Journal of Child Neurology 2005. 20: 940-949.

83
CONGENITAL HEART DISEASE IN DOWN SYNDROME CLIPP QFC 29-4 - Basic Science Resource Guide
Halana Whitehead, Risa Eilbaum, and Thomas Kazecki Describe the embryology of common cardiac defects seen in patients with Down syndrome. What physical examination findings would you expect with these disorders? KEY EVENTS IN CARDIAC EMBRYOLOGY
Cardiac looping: The fetal heart begins as a pair of cardiac tubes which fuse to form a single midline tube by 22 days gestation. As fusion finishes, the primitive heart begins to beat. Next, the heart tube curves rightward and folds to take on a conformation which allows for formation of the chambers of the mature heart. Atrioventricular (AV) Septal Development: Partitioning of the heart tube into four chambers occurs between weeks four and eight of fetal development. Toward the end of week four, a subset of cells in the primordial heart form dorsal and ventral swellings called “endocardial cushions” in the midline between the atria and ventricles (Figure A). The dorsal and ventral cushions eventually fuse with each other to form a septum that divides the primitive atria from the primitive ventricles. On either side of the septum are the left and right AV canals. These canals will eventually become mitral and tricuspid valves, respectively. Ventricular Septal Development: The ventricular septum is made from a muscular component and membranous component. A median ridge in the floor of the primitive ventricle near its apex is the first sign of muscular septal development. The ridge gains height by dilation of the ventricles around it. The interventricular foramen, a connection between both ventricles, is present between the growing septum and the fused endocardial cushions. This closes at week seven when the left and right bulbar ridges fuse with the endocardial cushions to form the membranous component of the septum (Figure B). Development of the aorta and pulmonary arteries: The aorta and its branches develop from the truncus arteriosus, dorsal aortae, aortic arches and the aortic sac. The ascending aorta originates from the fusion of the truncus arteriosus and aortic sac. The mature aortic arch forms from the left fourth embryonic arch and dorsal aortae.

84
The paired dorsal aortae merge to create the descending aorta. The major branches of the aorta develop from the third (brachiocephalic and left common carotid) and right fourth (right subclavian) arches. The right and left sixth aortic arches become the proximal right and left pulmonary arteries, respectively. The ductus arteriosus, which shunts fetal blood from the pulmonary artery to the aorta, originates from the left sixth arch. MOLECULAR BASIS OF DOWN SYNDROME DISEASE Under normal embryologic conditions, phospholipase C increases intracellular calcium concentrations, thereby activating calcineurin A. The elevated levels of calcium stimulate calcineurin A to bind the protein phosphatase PP2B and subsequently dephosphorylate the transcription factor NFAT1. The dephosphorylation of NFAT1 promotes gene expression involved in endocardial cushion development. Current DNA studies suggest that overexpression of the Down Syndrome Critical Regions (DSCR1) gene is involved in the genesis of Down syndrome related cardiac disease. DSCR1 functions by encoding calcipressin 1. Calcipressin1 inhibits calcineurin A by directly binding to it and preventing it from interacting with PP2B, thus interfering with NFAT1 dephosphorylation and endocardial cushion development. COMMON CARDIAC DEFECTS IN DOWN SYNDROME Between 40 and 60% of babies born with Down Syndrome have a congenital heart defect. According to a study done in the UK from 1985-2006, 42% of infants born with Down Syndrome had a cardiovascular anomaly; of these patients, 37% had complete atrioventricular septal defect, 31 % had a ventriculoseptal defect, 15% had an atrial septal defect, 6% had a partial atrioventricular septal defect, 5% tetrology of fallot, and 4% had patent ductus arteriosus. Atrioventricular septal defects: This group of defects results from the incomplete fusion of the endocardial cushions during AV septation which creates an inappropriate communication between the chambers of the heart and interferes with normal valve formation. In the complete form (CAVSD), all four chambers are connected via a common AV valve, ASD and VSD. CAVSD represents more than one-third of the cardiac defects seen in Down syndrome. On exam, an infant with CAVSD may be tachypneic and tachycardic with a narrowly split S2 and a loud P2. A pansystolic murmur may be present at the apex, but can be masked in the newborn period when pulmonary vascular resistance is still high. PAVSD is a less severe form in which there are two distinct AV valves and an ASD, but no VSD. The ASD is typically of the ostium primum type, and is associated with a cleft in the anterior leaflet of the mitral valve. Physical exam in these patients reveals a systolic ejection murmur at the left upper sternal border caused by pulmonic stenosis secondary to pulmonary overcirculation. Mitral regurgitation may also be present. Ventricular septal defects: A VSD results from incomplete ventricular septation and initially leads to a left-to-right shunt. VSDs make up roughly 30% of cardiac defects in Down syndrome patients, with the perimembranous form being the most common in both Down syndrome patients and the general population. Physical findings with a VSD depend on the size of the lesion. Patients with larger lesions may present with tachypnea, tachycardia and other signs of heart failure. A harsh pansystolic murmur most prominent at the left lower sternal border is classically present on auscultation, and the intensity is generally inversely proportional to the size of the VSD.

85
Atrial septal defects: ASDs result from an incomplete atrial septum which allows blood to flow between the atria, initially left to right. The ostium secundum form of ASD is the most common and occurs when the septal tissue that covers the fossa ovale is absent. Isolated ASDs are rarely symptomatic, but may be detected on cardiac exam. The time required to eject the additional blood shunted through the ASD delays closure of the pulmonic valve independent of respiration, leading to a fixed, split S2. This increased blood flow across the pulmonic valve creates turbulence, which can be appreciated as a murmur at the left upper sternal border. Tetralogy of Fallot: Tetralogy of Fallot consists of pulmonary stenosis, right ventricular hypertrophy, a VSD and an overriding aorta. This constellation of defects results from an anterior and superior deviation of the infundibular septum, simultaneously creating a right ventricular outflow tract obstruction and positioning the aorta over the remaining interventricular septum. Since vascular development depends on blood flow, the obstructed pulmonic valve and pulmonary artery never reach full size, which causes shunting of deoxygenated blood into the systemic circulation. Physical findings include cyanosis and tachypnea, with the severity and age of presentation depending primarily on the degree of pulmonary stenosis. A right ventricular heave and a single S2 are commonly present on exam and a systolic murmur may be audible at the left upper sternal border. Patent ductus arteriosus: A PDA occurs when the ductus arteriosus, a physiologic right-to-left fetal shunt, fails to close in response to changes in oxygenation after birth. If the ductus arteriosus remains open, the shunt reverses direction as pulmonary vascular resistance falls. Patients with small PDAs may be asymptomatic. Patients with larger shunts may be tachycardic and tachypneic due to pulmonary overcirculation, which leads to pulmonary hypertension if left uncorrected. A continuous, machinery-like murmur and bounding pulses may be evident on cardiovascular exam.
Additional Resources: Cardiac Embryology Animation - University of Toronto
Congenital Heart Defect Diagrams - Mayo Clinic
References Dennis et al. Recognising heart disease in children with Down syndrome. Archives of disease in childhood: Education and practice edition. 2010 Aug; 95(4):98-104. Irving CA and Chaudhari MP. Cardiovascular abnormalities in Down's syndrome: spectrum, management and survival over 22 years. Archives of disease in childhood. 2012 Apr; 97(4):326-30. Kliegman, Robert M., and Waldo E. Nelson. Chapters 414 and 420. Nelson Textbook of Pediatrics. 19th ed. Philadelphia, Pa. [u.a.: Elsevier Saunders, 2011. N. pag. Web. Macián, Fernando, Cristina López-Rodríguez, and Anjana Rao. "Partners in Transcription: NFAT and AP-1." Oncogene 20.19 (2001): 2476-489.
86
Mann D, Mehta V. Cardiovascular embryology. International Anesthesiology Clinics. 2004; 42(4):15-28. Marino B and Digilio MC. Congenital heart disease and genetic Syndromes: Specific correlation between cardiac phenotype and genotype. Cardiovascular Pathology 9(6) November - December 2000, p. 303-315 Moore, Keith L., and T. V. N. Persaud. "Cardiovascular System." Before We Are Born: Essentials of Embryology and Birth Defects. 8th ed. Philadelphia: Saunders, 2013. N. pag. Web. Suzuki, K., S. Yamaki, and S. Mimori. "Pulmonary Vascular Disease in Down’s Syndrome with Complete Atrioventricular Septal Defect." American Journal of Cardiology 86 (2000): 434-37. Print. Vetter, Victoria. Pediatric Cardiology: The Requisites in Pediatrics , First Edition, February 2006, Chapters 3 & 4- Cyanotic Heart Disease & Acyanotic Congenital Heart Defects
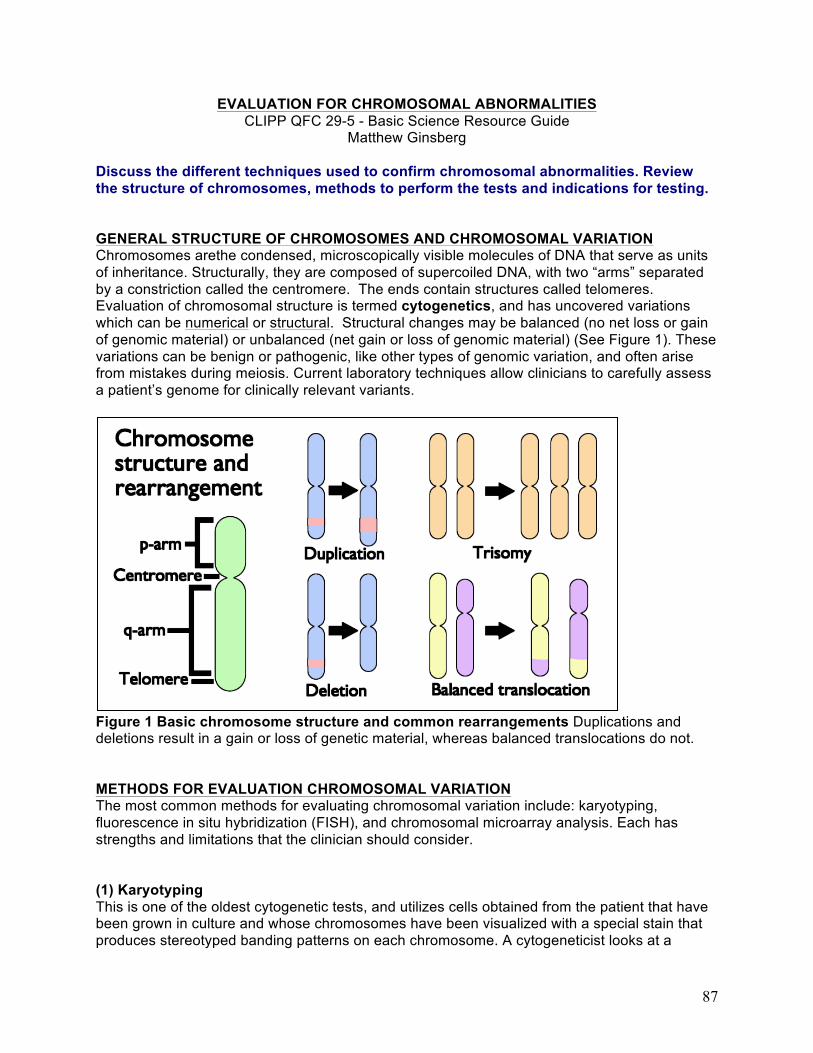
87
EVALUATION FOR CHROMOSOMAL ABNORMALITIES CLIPP QFC 29-5 - Basic Science Resource Guide
Matthew Ginsberg Discuss the different techniques used to confirm chromosomal abnormalities. Review the structure of chromosomes, methods to perform the tests and indications for testing. GENERAL STRUCTURE OF CHROMOSOMES AND CHROMOSOMAL VARIATION Chromosomes arethe condensed, microscopically visible molecules of DNA that serve as units of inheritance. Structurally, they are composed of supercoiled DNA, with two “arms” separated by a constriction called the centromere. The ends contain structures called telomeres. Evaluation of chromosomal structure is termed cytogenetics, and has uncovered variations which can be numerical or structural. Structural changes may be balanced (no net loss or gain of genomic material) or unbalanced (net gain or loss of genomic material) (See Figure 1). These variations can be benign or pathogenic, like other types of genomic variation, and often arise from mistakes during meiosis. Current laboratory techniques allow clinicians to carefully assess a patient’s genome for clinically relevant variants.
Figure 1 Basic chromosome structure and common rearrangements Duplications and deletions result in a gain or loss of genetic material, whereas balanced translocations do not. METHODS FOR EVALUATION CHROMOSOMAL VARIATION The most common methods for evaluating chromosomal variation include: karyotyping, fluorescence in situ hybridization (FISH), and chromosomal microarray analysis. Each has strengths and limitations that the clinician should consider. (1) Karyotyping This is one of the oldest cytogenetic tests, and utilizes cells obtained from the patient that have been grown in culture and whose chromosomes have been visualized with a special stain that produces stereotyped banding patterns on each chromosome. A cytogeneticist looks at a

88
handful of cells under the microscope and searches for large changes in the structure of the chromosomes, extra chromosomes, or missing chromosomes. The main strengths of this study are that it can detect aneuploidies (extra chromosomes and missing chromosomes), inversions and translocations (both balanced and unbalanced); while aneuploidies and unbalanced translocations will also be detected by microarray (see below), karyotyping can detect balanced translocations that may be missed by this technique. In addition, karyotyping is rapid, and it is the least expensive of the techniques. Its main disadvantage is that it has limited resolution; since the cytogenetic bands correspond to millions (perhaps thousands) of bases of DNA, smaller insertions and deletions are not detected. Therefore, this test is most useful for confirming a clinically suspected aneuploidy/polyploidy syndrome (such as trisomy 21) or evaluating for balanced translocations1. (2) FISH (fluorescence in situ hybridization) This test uses different colored fluorescent markers (FISH probes) that hybridize to very specific short sequences on a particular chromosome. These probes are mixed with cells from a patient, and then the probes and chromosomes are visualized with a special microscope. A limited number of probes can be used at the same time, but because they are so specific, they can precisely delineate whether a particular stretch of DNA is missing, duplicated, or on the wrong chromosome. This test is very useful for confirming the results of other chromosomal tests or characterizing the location of duplicated genetic material. However, deletions and duplications that are smaller than the probe size can be missed by FISH analysis, and if two pieces of duplicated DNA are near each other, they may appear as one signal rather than two distinct probes, leading to difficulty detecting this duplication. FISH is an inefficient tool for genome-wide screening1. (3) Chromosomal microarray This test uses a technology that can simultaneously examine many thousands of loci in the genome for chromosomal abnormalities. There are two main types of array that are currently used: oligonucleotide array comparative hybridization (oligoaCGH) and single nucleotide polymorphism (SNP) arrays. Both use a matrix of thousands of “dots” that contain probes for a specific piece of DNA. These tests have a high resolution and can identify microdeletions and microduplications that cannot be seen on karyotyping2. However, these tests take more time, are more expensive, and cannot detect structural abnormalities that do not cause a net imbalance of genomic copy number (i.e. balanced translocations or inversions). Current arrays are also able to detect mosaicism (when there is more than one cytogenetically distinct cell line in a patient).
a) OligoaCGH: A sample of DNA extracted from the patient is chemically labeled and combined with the same amount of total DNA from a control source, also labeled. This mixture is applied to the microarray, where probes bind to DNA at a particular locus. Competitive binding between samples for the probe can be used to identify numerical abnormalities.
b) SNP array: This type of microarray uses probes for SNP sites throughout the genome of
a patient, but does not require control DNA. The SNP array can have higher resolution than oligo arrays, and can detect some phenomena that the oligoaCGH cannot, such as uniparentaldisomies and consanguinity. SNP arrays may detect lower levels of mosaicism than oligo arrays as well.
In the future, whole exome sequencing approaches may replace these methods, since they have the ability to detect most chromosomal abnormalities while also detecting clinically

89
significant sequence variants. (Note: whole exome testing will not detect trinucleotide repeat conditions, won’t necessarily find balanced translocations or inversions, and will not report patented genes). INDICATIONS FOR LABORATORY TESTING OF CHROMOSOMAL VARIATION Chromosomal microarrays are capable of detecting more clinically relevant copy number variants than traditional karyotyping, and they operate at the genome-wide level, so they may be a first-line test for the evaluation of children with unexplained developmental delay/cognitive impairment, autism spectrum disorders, multiple congenital malformations, or the evaluation of apparently balanced translocations on karyotype analysis (since karyotypes may not be capable of detecting small, associated deletions or duplications)1,3,2. Prenatally, arrays may be used when there are fetal anomalies detected on imaging studies, for evaluating the offspring of a parent with an apparently balanced translocation, or if the fetus has an apparently balanced translocation on karyotype. References Tzetis, M., Kitsiou-Tzeli, S., Frysira, H., Xaidara, A. & Kanavakis, E. The clinical utility of
molecular karyotyping using high-resolution array-comparative genomic hybridization. Expert Review of Molecular Diagnostics12, 449–457 (2012).
Manning, M. & Hudgins, L. Array-based technology and recommendations for utilization in
medical genetics practice for detection of chromosomal abnormalities. Genet. Med.12, 742–745 (2010).
D. T. et al. Consensus statement: chromosomal microarray is a first-tier clinical diagnostic test
for individuals with developmental disabilities or congenital anomalies. Am. J. Hum. Genet.86, 749–764 (2010).

90
HOWELL-JOLLY BODIES CLIPP QFC 30-4 – Basic Science Resource Guide
Adam Stevenson, MD Gerardo’s peripheral blood smear shows Howell-Jolly bodies – what does this finding represent on a cellular level? During erythropoiesis in the bone marrow matrix, most red blood cells extrude their nuclei prior to entering the bloodstream. In some cases, though, fragments of non-functional DNA material are retained in the cell and can be seen on routine blood smears. This phenomenon was first noted by William Henry Howell and Justin Marie Jolly in 1890. This retained DNA appears as a basophilic mark on the otherwise eosinophilic erythrocyte on a standard H&E stained blood smear (figure 1). Typically the erythrocyte only retains a single inclusion which appears as a circular dark blue spot. Occasionally, uneven staining of the Howell-Jolly body can be misinterpreted as an intracellular parasite. Figure 1 – Howell-‐Jolly bodies (Giemsa stain)
From DPDx -‐ CDC Parasitology Diagnostic Web Site
These DNA inclusions are normally pitted from the red blood cell by the sinusoidal components of the spleen during erythrocyte circulation, but will persist in individuals with functional hyposplenia or asplenia, such as sickle cell disease. Howell-Jolly bodies may also be seen in patients with severe anemia, though in such patients nucleated red blood cells (figure 2) may also be seen as increased production speeds premature release of cells from the marrow. Figure 2 – Nucleated red blood cells (Giemsa stain)
91
From DPDx -‐ CDC Parasitology Diagnostic Web Site
References DPDx - CDC Parasitology Diagnostic Web Site (http://www.dpd.cdc.gov/dpdx/HTML/ImageLibrary/A-F/Artifacts/body_Artifacts_il9.htm)

92
HXYDROXYUREA THERAPY FOR SICKLE CELL DISEASE CLIPP QFC 30-6 – Basic Science Resource Guide
Adam Stevenson, MD How does hydroxyurea help abate the clinical manifestations of sickle cell disease? Hydroxyurea was first synthesized in 1869 in Germany by Dressler and Stein and was first approved by the FDA in 1967 for the treatment of neoplastic diseases. Hydroxyurea is converted to a free radical nitroxide in vivo, and transported by diffusion into cells where it inactivates the enzyme ribonucleotide reductase. This produces cell death in rapid S phase replication. Prior to its use in patients with sickle cell disease (SCD), hydroxyurea had already been used to decrease the pathologically high red blood cell and platelet counts seen in patients with polycythemia vera. Hydroxyurea was approved by the US Food and Drug Administration (FDA) for the treatment of adults with homozygous (HbSS) sickle cell disease in 1998. It was approved for use in reducing the frequency of painful crises and the need for blood transfusions in adult patients with recurrent moderate-to-severe painful crises (generally at least three during the preceding 12 months). The National Heart, Lung, and Blood Institute issued recommendations in 2002 supporting the use of hydroxyurea for the treatment of children with SCD. Hydroxyurea has multiple beneficial effects that may contribute to its efficacy in SCD. The primary effect seems to be the induction of fetal hemoglobin (HbF) production. This lowers the concentration of Hb S within a red blood cell, resulting in less polymerization of the abnormal hemoglobin. This in turn causes a concomitant increase in total hemoglobin and decrease in hemolysis. However, the mechanisms by which hydroxyurea increases Hb F are unclear. The majority of circulating red blood cells are derived from mature erythroid precursors in the bone marrow; smaller percentages are derived from immature precursors. Gamma (Ɣ) genes, necessary for the production of fetal hemoglobin (α2 Ɣ2), remain more active in these immature precursors. Early studies suggested that hydroxyurea is toxic to the more rapidly dividing late erythroid precursors, which leads to the recruitment of early erythroid precursors with this increased capacity to produce Hb F. Others have suggested that hydroxyurea acts directly on late red blood cell precursors to reprogram them to produce Hb F. It may interrupt the transcription factors that selectively bind to promoter or enhancer regions around the globin genes, thereby altering the ratio of ß and Ɣ gene activity. A recent study has provided evidence for a nitric oxide-derived mechanism for Hb F induction by hydroxyurea. Another study has suggested that it increases Hb F production by inhibiting ribonucleotides. In addition, hydroxyurea may be of benefit in sickle cell disease for reasons unrelated to Hb F production, including its ability to increase the water content of red blood cells. Finally, red blood cell sickling and vaso-occlusion damages vascular endothelium, in turn recruiting platelets and white blood cells. Hydroxyurea reduces white blood cell and platelet counts, which may be beneficial in dampening the cycle of vascular damage, clotting and inflammation. Side Effects As noted above, hydroxyurea is myelosuppressive, and complete blood counts must be monitored regularly in patients on this treatment regimen. Guidelines are available for counts under which hydroxyurea doses must be decreased or held. Hydroxyurea is potentially harmful to the developing fetus, and reproductive counseling is a critical part of treatment for

93
any female patient of child-bearing age. There is empiric concern for increased risk of cancer, specifically leukemia, in patients treated with hydroxyurea. Much of this concern, however, derives from data on treatment of patients with polycythemia vera, a patient population with increased risk of leukemia from their primary disease. It remains unclear what risk, if any, is attributable to hyroxyurea therapy. References Platt OS. Hydroxyurea for the Treatment of Sickle Cell Anemia. N Engl J Med 2008; 358:1362-1369 Segal JB. Hydroxyurea for the Treatment of Sickle Cell Disease AHRQ. Evidence Report/Technology Assessment. Number 165 Strouse JJ. Hydroxyurea for Sickle Cell Disease: A Systematic Review for Efficacy and Toxicity in Children. Pediatrics 2008; 122(6):1332 -1342

94
IMMUNIZATION OF PATIENTS ON CORTICOSTEROID THERAPY CLIPP QFC 31-4 – Basic Science Resource Guide
Adam Stevenson, MD
Describe the considerations for immunizing a patient with nephrotic syndrome who is receiving/recently received treatment with corticosteroids. Corticosteroids are a common treatment for nephrotic syndrome. One proposed mechanism of their effect in nephrotic syndrome is their immunomodulating properties. Corticosteroids prevent interleukin (IL–1 and IL-6) production by macrophages and inhibit all stages of T-cell activation. While this anti-inflammatory effect is useful for the treatment of many disease processes, it can also compromise patients’ immune status. Two main concerns have been raised when vaccinating immunocompromised children: (1) decreased efficacy of the vaccination and (2) safety concerns. Response to both killed vaccines and attenuated, live-virus vaccines may be suboptimal in immunocompromised patients, and response to immunization should be monitored. Theoretical safety concerns related to immunosuppression, however, apply only to live-virus vaccines. The CDC recommends that physician use clinical judgment in determining the level of patient immunosuppression when deciding whether to vaccinate. While the amount of systemically absorbed corticosteroids and the duration of administration needed to suppress the immune system of an otherwise immunocompetent person are not well defined, immunosuppression is directly related to the dose and length of corticosteroid treatment. Hence, specific guidelines have been proposed by the CDC (table 1). Children who are receiving topical corticosteroids, inhaled corticosteroids, physiologic corticosteroid maintenance doses, or systemic dosing less than the equivalent of 2 mg/kg/day of prednisone (or <20 mg/day in patients weighing more than 10 kg) may still receive attenuated live-virus vaccines. Those receiving more than 2 mg/kg/day (or > 20mg) of prednisone for fewer than 14 days may receive attenuated live-virus vaccines as soon as therapy has been discontinued. Those children who have been on corticosteroids for more than 14 days in doses greater than 2 mg/kg/day (either daily or every other day) should not receive attenuated live-virus vaccines for at least 1 month following discontinuation of therapy. Table 1 – Recommendations for live virus vaccines in patients receiving corticosteroid therapy Corticosteroid dosing regimen May receive attenuated live-‐virus vaccines Topical or inhaled corticosteroids Yes Physiologic replacement doses Yes < 2 mg/kg/day (up to 20mg) of prednisone daily Yes ≥ 2 mg/kg/day (up to 20mg) of prednisone x < 14 days Yes, once treatment stopped ≥ 2 mg/kg/day (up to 20mg) of prednisone x > 14 days Wait for 1 month after treatment stopped References Steele, RW. Vaccines and Immunosuppressed Patients. Medscape, 11/08/2001 Immunization in Special Clinical Circumstances. In Red Book: Report of the Committee on Infectious Diseases. 2009