questions of ethics: neonatal screening for prenatal alcohol exposure joey gareri hbsc. division of...
TRANSCRIPT

Questions of Ethics:Neonatal Screening for
Prenatal Alcohol Exposure
Joey Gareri HBSc.Division of Clinical Pharmacology and Toxicology
Hospital for Sick Children, TorontoDepartment of Pharmacology
University of Toronto
Dr. Gideon Koren MD, FRCPC
INTRODUCTION Challenges of Diagnosis
Full blown FAS (severe neurodevelopmental delay) Indinstinct philtrum Intrauterine growth retardationShort palpebral fissures
Less apparent forms of FASD, such as Alcohol Related Neurodevelopmental Disorder (ARND) are difficult to diagnose
ARND is associated with non-pathognomonic features Confirmed maternal drinking history in pregnancy
required for diagnosis Delayed diagnosis and intervention further increases the
risk of secondary disabilities
INTRODUCTIONDiagnostic Tools
Questionnaires T-ACE TWEAK
Biomarkers Liver enzymes Ethyl glucuronide
Fatty Acid Ethyl Esters (FAEE)
INTRODUCTIONThe Questions of Ethics
Analysis of the Ethical Aspects of the Screen(Hermerin et al., 1999) Purpose Informed Consent Access to Information Cost Effectiveness
Assessment of the Quality of the Screening Method(Loeber et al., 1999) Coverage Sample Quality Demographic Data Collected Epidemiological Evaluation Proposed Follow-up
INTRODUCTIONNeonatal Screening for Fetal Alcohol Exposure
PROS
maximize diagnosis/intervention across socioeconomic lines
opportunity to initiate therapy at earliest possible time in development (improved prognosis for outcome)
avoids marginalization of high-risk women (as opposed to targeted screening)
birth provides a window of opportunity in engaging high-risk women
optimal intervention timing for behaviour changes in mother
address potential alcohol withdrawal in the neonate
can provide adoptive parents with valuable background information
enormous research potential in engaging an elusive study population
CONS
potential labeling/stigmatization of mother and child
potential for conflict due to perceived or potential implications of a positive test
low disease specificity associated with alcohol exposure (<60% unaffected)
not diagnostic for specific treatment intensive follow-up required, high
cost
can potentially decrease the likelihood of adoption for exposed infants
The Questions of Ethics
Analysis of the Ethical Aspects of the Screen
Purpose Informed Consent Access to Information Cost Effectiveness
Assessment of the Quality of the Screening Method Coverage Sample Quality Demographic Data Collected Epidemiological Evaluation Proposed Follow-up
PURPOSE…Prevalence
Drinking in pregnancy About 50% of women of reproductive age admitted to drinking
regularly (CDC 2002, Health Canada 2002)
Use of alcohol in pregnancy ranges from 3.5% to 9.9% (CDC 2004)
Rates of binge (>5 drinks/ occasion) and frequent (>7 drinks/ week) drinking ~3% (CDC 1997 & 2002)
Prevalence of heavy drinking in pregnancy (>14 drinks/ week) is about 0.1% to 0.3% (CDC 1997 & 2002)
FASD in the general neonatal population FASD ~1% (9.1/1000 live births)
Compare currently screened disorders… phenylketonuria: 1/15,000 congenital hypothyroidism: 1/4,000
Full-blown FAS ~0.1% (0.3-1.5/1000 live births)
PURPOSE…Health Outcomes
CHILD In FAS, the primary neurological insult results in severe mental
retardation In FASD, the primary neurological insult results in a complex pattern of
behavioral or cognitive abnormalities 95% incidence of mental health problems* 50-70% incidence of substance addiction*
ADDICTED MOTHER 78% incidence of depression** 30% incidence of eating disorders** 25% incidence of suicidal thinking**
*statistics provided by FASworld Canada
**statistics provided by Breaking The Cycle 1995-2000 Evaluation Report
PURPOSE…Social Outcomes
CHILD Secondary Disabilities resulting from alcohol-induced damage :
60% incidence of “disrupted school experience” and “trouble with the law”*
55% incidence of institutionalization/incarceration* 70-82% incidence of unemployment/ dependent living* 50% incidence of inappropriate or promiscuous sexual behaviour*
ADDICTED MOTHER 93% incidence of unemployment** 60% incidence of current partner abuse** 50% incidence of recent partner abuse** 96% income <$15,000/yr CAD** 23% incidence of homelessness**
*statistics provided by FASworld Canada
**statistics provided by Breaking The Cycle 1995-2000 Evaluation Report
The Questions of Ethics
Analysis of the Ethical Aspects of the Screen Purpose
Informed Consent Access to Information Cost Effectiveness
Assessment of the Quality of the Screening Method Coverage Sample Quality Demographic Data Collected Epidemiological Evaluation Proposed Follow-up
INFORMED CONSENT...Required
PROS Potential to facilitate
follow-up engagement Addresses legal
concerns Provides mothers with
choice improve retention
CONS Potential to alienate
target population
INFORMED CONSENT…Not Required
PROS Maximum coverage
CONS Uncertain legality
(mother vs. child) Potential conflict on
follow-up engagement Increased danger to
child

The Questions of Ethics
Analysis of the Ethical Aspects of the Screen Purpose Informed Consent Access to Information Cost Effectiveness
Assessment of the Quality of the Screening Method
CoverageSample QualityEpidemiological Evaluation Proposed Follow-up
The BiomarkerMECONIUM baby’s first bowel movements (i.e. first few stools)
A matrix unique to the developing fetus that is already commonly used in neonatal drug screening Superior to blood and urine
Discarded material Collection is easy and non-invasive Wide window of opportunity
Accumulation from 13th week gestation until birth
FATTY ACID ETHYL ESTERS Ethanol metabolites present in both maternal and fetal tissues
(Bearer et al. 1992)
Cohort studies in drinking and non-drinking women showed accumulation of FAEE in the meconium of neonates exposed to alcohol with some evidence of overlap (Mac et al. 1994; Bearer et al. 1996, 1997, 1999, 2003; Klein et al. 1999)
Do not cross the placenta, thus indicating FAEE in meconium are the result of ONLY fetal metabolism of ethanol (Chan et al., 2004)
Positive cut-off = 2.0 nmol total FAEE/g meconium (ethyl palmitate, palmitoleate, stearate, oleate, linoleate, linolenate, and arachidonate (Chan et al., 2003)
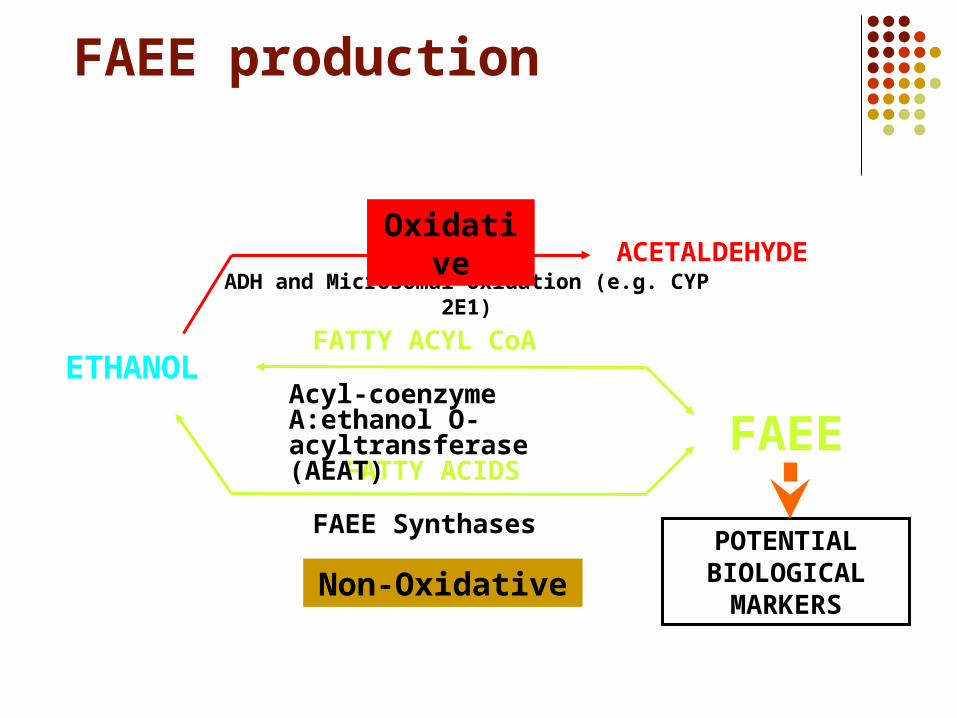
FAEE production
ETHANOL
ADH and Microsomal Oxidation (e.g. CYP 2E1)ACETALDEHYDE
FAEE Synthases
FAEE
Non-Oxidative
FATTY ACIDS
Oxidative
Acyl-coenzyme A:ethanol O-acyltransferase (AEAT)
FATTY ACYL CoA
POTENTIALBIOLOGICAL
MARKERS
Quality Assessment…
COVERAGE Preliminary analysis of our ongoing regional prevalence study
demonstrates a coverage rate of 87.07%.
EPIDEMIOLOGICAL EVALUATION Sensitivity/Specificity
Baseline study carried out in a population of 183 non-drinkers, 17 social drinkers (~2 dks/month), and 6 confirmed heavy drinkers (>14 dks/wk, >5 dks/occasion) yielded a sensitivity of 100% and a specificity of 98.4% *note: the FAEE test cannot detect exposure to mild/social drinking levels of alcohol
Predictive Value This has not yet been determined at this stage of development of the FAEE
test Maximum efficacy of the FAEE test would theoretically provide a predictive
value of 40%. For reasons unknown, 60% of the children born to heavy-drinkers are not alcohol-affected
Quality Assessment…
SAMPLE QUALITY Assessment of sample quality is relatively simple and objective
Issues of sample quality Non-sufficient quantity (<0.5 grams) Feces; can be determined by odour, texture, colour, and
chromatographic character
Ideally the designated biomarker would be used
in conjunction with an accepted questionnaire such
as the T-ACE or TWEAK
The Questions of Ethics
Analysis of the Ethical Aspects of the Screen Purpose Informed Consent Access to Information Cost Effectiveness
Assessment of the Quality of the Screening Method Coverage Sample Quality Epidemiological Evaluation
Proposed Follow-up
PROPOSED FOLLOW-UP… PRELIMINARY ASSESSMENT
There must be a preliminary assessment to determine whether or not social services will be involved; i.e. determine whether the child is in immediate danger
The preliminary assessment must be carried out by a health care worker as this is primarily a health-care issue Public Health Nurse
a PHN is likely the ideal liaison to carry out the initial assessment Currently PHN visits are voluntary
ENGAGEMENT If mother is deemed to require intervention, she must then be
engaged into an easily accessible, “one-stop”, integrated treatment program Outreach worker Family doctor
Monitoring of the child’s development should involve co-ordination with the pediatrician

PROPOSED FOLLOW-UP… CHILD (diagnostic)
18 months; post-natal growth retardation, microcephaly, craniofacial assessment, Bayley’s test (“developmental adequacy”)
3½-4 years; speech delay, fine motor skills, cognitive assertion
CHILD (therapeutic) Treatment initiated before 6 years of age is maximally
effective Enriched learning environments can be very beneficial early
in development Treatment may vary with the specific needs of the affected
individual; i.e. attention deficit, speech, cognitive therapy… e.g. SCREAMS model of intervention*
Structure, Cues, Role models, Environment, Attitude, Medication, Supervision
PROPOSED FOLLOW-UP… MOTHER
Multi-faceted intervention strategy addressing addiction, mental health, social support, family functioning, self-efficacy, and general well-being via… Home visits/intensive case management
Involves all members of family and includes positive action of male partner
Motivational interviewing Enables free choice and change through a process of self-
actualizations This intervention strategy has had proven results when
implemented in several locations across North America
PROPOSED FOLLOW-UP…
MOTHER One-stop-shop approach
Addiction counselling Child development services Health/Medical/Psychiatric care Parenting support services Basic needs services

FOLLOW-UP…Model Integrated Programs
Breaking the Cycle (Toronto, Ontario) Improved developmental scores in children Lower rates of apprehension by social services
Sheway (Vancouver, British Columbia) 1993-1998
50% reduction apprehension by social services over first five years 20% increase in babies with healthy birth weights. And 61 per cent more women were connected to a midwife or doctor
by the time they delivered their babies.
Four-State FAS consortium (North Dakota, South Dakota, Montana, Minnesota)
Preliminary results show statistically significant improvement in 14/16 areas of therapy
FOLLOW-UP…Barriers/Gaps in Treatment
Adult FASD assessment Culture gaps between aboriginal women and
primary health care providers Affordable Housing Greater income security/social assistance Significant partnership between all involved
professionals (MDs, PHNs, outreach workers, etc.)
The Questions of Ethics
Analysis of the Ethical Aspects of the Screen Purpose Informed Consent
Access to Information Cost Effectiveness
Assessment of the Quality of the Screening Method Coverage Sample Quality Epidemiological Evaluation Proposed Follow-up
ACCESS TO INFORMATION…Necessary
Diagnosis and follow up Agencies responsible for follow-up and/or post-natal
medical care require knowledge of a positive result Pediatrician/Family Doctor Public Health Nurse Social Services (if involved) Adoption Agencies/Adoptive Parents
ACCESS TO INFORMATIONBeneficial
Research purposes Access to population data for an elusive study population
Birth weight, Head circumference, Body length, Gestational age, Maternal age, Gravida and Para status
Research Ethics Boards Charged with maintenance of ethical standards in all research
undertakings
Individual data Would require consent under guidance of REBs Potential to isolate susceptible genotypes
60% alcohol-exposed neonates unaffected FAS mothers significantly more likely to produce subsequent FAS
children
Prevention by InterventionNEONATAL INTERVENTION CANNOT PREVENT PRIMARY ALCOHOL-INDUCED DAMAGE
Mothers of alcohol-affected children are significantly more likely to produce subsequent alcohol affected children
Substance-addicted women have an 85% incidence of multiple pregnancies (average = 4) and 25% incidence of child apprehension by social services
EARLY MATERNAL INTERVENTION (e.g. 1st pregnancy) can potentially prevent future cases of FASD
In FASD 50-70% incidence of substance addiction 50% incidence of inappropriate or promiscuous sexual
behaviour FASD INTERVENTION is capable of alleviating
secondary disabilities which perpetuate FASD
The Questions of Ethics
Analysis of the Ethical Aspects of the Screen Purpose Informed Consent Access to Information
Cost Effectiveness
Assessment of the Quality of the Screening Method Coverage Sample Quality Epidemiological Evaluation Proposed Follow-up

COST EFFECTIVENESS
PREVENTION Reduced disease prevalence in the future can potentially
off-set the immediate costs of implementing a mother/child support system.
The lifetime cost of FASD per affected individual has been estimated to be as high as $1,400,000.00 (USD)*
Potential long-term savings in the justice system; FASD prevalence in corrections has been estimated at rates of 25% up to 50%*. Treatment could significantly reduce burden in the criminal justice system
COST EFFECTIVENESS Questionnaire-based… cheaper
Underreporting is common due to embarrassment, guilt, and fear of punitive action
Not specific to gestational alcohol consumption
Biomarkers… objective (upon sufficient validation) Maternal biomarkers for alcohol consumption
Traditional markers of alcoholism (e.g. HAA, CDT, MCV, GGT)
Not specific to gestational alcohol consumption FAEE
Not fully validated Specific to gestational alcohol consumption
THANK YOUAcknowledgements
Canadian Institute for Health ResearchDaphne Chan
Julia Klein Dr. Irena NulmanDr. Joanne Rovet
Dr. Cindy Woodland Margaret LeslieGina DeMarchiNerina Chiodo