r2 diagnosis and management of menstrual disordersll
TRANSCRIPT
Management of menstrual disorders
Under supervision ofDr O. BenGharbia
MRCGP, MD, MSc SciBy Dr. Amir M Hanafi
PGY2

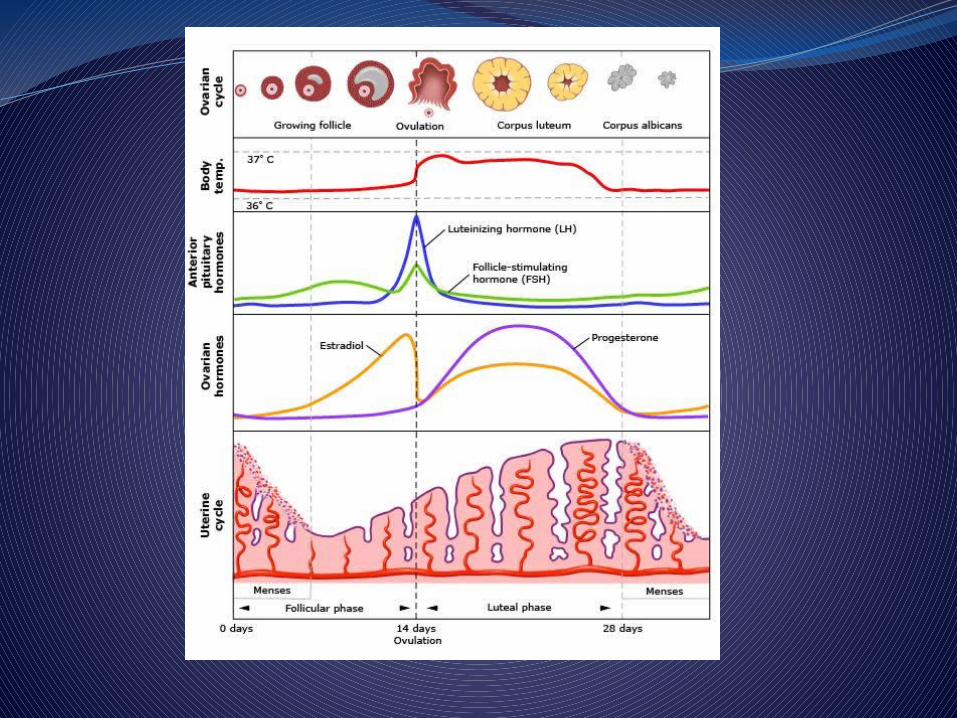
ObjectivesTo review menstrual physiologyTo know how to manage a case of MenorrhagiaTo know how to manage a case of
DysmenorrheaTo know how to manage a case of Amenorrhea

TerminologyDysfunctional uterine bleeding — excessive
noncyclic endometrial bleeding unrelated to anatomical lesions, usually anovulatory bleeding.
Menorrhagia —It is technically defined as blood loss greater than 80 mL per cycle and/or menstrual periods lasting longer than seven days
Metrorrhagia — light bleeding from the uterus at irregular intervals.

Terminology (contd.)Intermenstrual bleeding — occurs
between mensesPolymenorrhea — regular bleeding that
occurs at an interval less than 24 days.Premenstrual spotting — light bleeding
preceding regular menses.

Terminology (contd. 2)Amenorrhea — absence of bleeding for at
least three usual cycle lengths. Oligomenorrhea — bleeding that occurs at
an interval greater than 35 days or less than 9 cycles per year.
Dysmenorrhea — Primary dysmenorrhea refers to recurrent, crampy lower abdominal pain that occurs during menstruation in the absence of pelvic pathology.

Case 1. MenorrhagiaA 43-year-old , got 2 children, LMP 21 days ago, presents with heavy menstrual bleeding. In the last 6 months there has been a change with menses coming every 25-32 days, lasting 7-10 days and associated with cramps not relieved by ibuprofen, passing clots. Prior to 6 months ago her cycles came every 28-30 days, lasted for 6 days, and were associated with cramps that were relieved by ibuprofen.
Conti, case 1She denies dizziness, but complains
of feeling weak and fatigued. Her weight has not changed in the
last year. She denies any bleeding disorders
or reproductive cancers in the family.
She takes no daily medications and has no other medical problems.
She is divorced , non smoker and works as a teacher.

Conti, case 1On examination; BP=130/88; P= 100; Ht=158 cm’; Wt=68 kg .
She appears pale. No (hirsuitism, acne,ecchymosis/ purpura,
thyroid, galactorrhea) Pelvic exam shows normal vulva, vagina and
cervix: normal size, not tender, mobile uterus; non-tender adnexae without palpable masses.
What are the parameters of a normal menstrual cycle?

The parameters of a normal menstrual cycle
• Interval 21-35 days (Mean: 28 days)• Duration: 2-7 days (Mean: 5 days)• Volume: <80ml (Mean 35 ml)• Composition: Non-clotting blood, endometrial
debris

The possible etiologies could cause this patient’s bleeding?PALM-COEIN is an acronym that was
published in 2011 by the International Federation of Gynecology and Obstetrics at 2011.
Was created for the purpose of establishing a universally accepted nomenclature to describe uterine bleeding abnormalities
The possible etiologies could cause this patient’s bleeding• PALM-Structure Causes
Polyp Adenomyosis Leiomyoma Malignancy and Hyperplasia
COEIN-Non-structural Causes Coagulopathy Ovulatory Dysfunction
Endometrial Iatrogenic
Not Yet Classified
What are the appropriate lab tests that should be ordered in this patient?
• CBC, TSH, Prolactin• Pregnancy Test• Endometrial Biopsy• Pelvic Ultrasound
Results of investigationLabs show Hgb: 9 gr/100 dl., HCT: 27%, HCG:
negative, , TSH and Prolactin are within normal limits.
Pelvic Ultrasound: heterogeneous myometrium, endometrial lining 1.4cm with, normal ovaries.
Endometrial biopsy: normal secretory endometrium.
What further tests would you order based on the following results?

Further tests would you order?
Fluid-enhanced sonohysterogram
HysterosalpingogramDiagnostic hysteroscopy
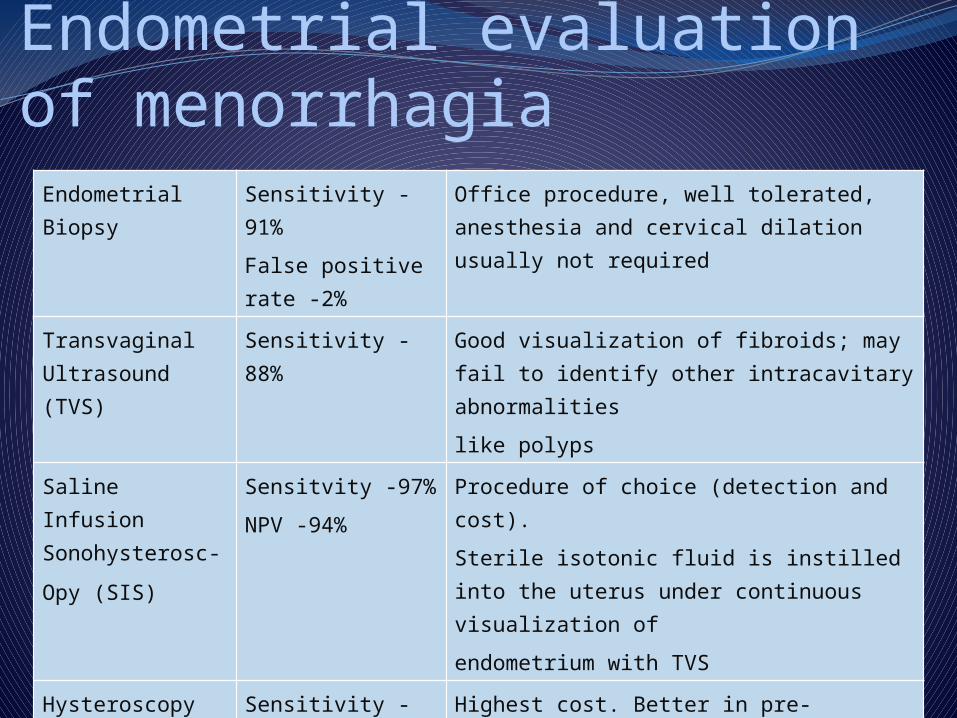
Endometrial evaluation of menorrhagia
Endometrial Biopsy
Sensitivity -91%
False positive rate -2%
Office procedure, well tolerated, anesthesia and cervical dilation usually not required
Transvaginal Ultrasound (TVS)
Sensitivity -88% Good visualization of fibroids; may fail to identify other intracavitary abnormalities
like polyps
Saline Infusion Sonohysterosc-
Opy (SIS)
Sensitvity -97%
NPV -94%
Procedure of choice (detection and cost).
Sterile isotonic fluid is instilled into the uterus under continuous visualization of
endometrium with TVS
Hysteroscopy Sensitivity -100% Highest cost. Better in pre-menopausal women. Does not reduce hysterectomy rate even without intra cavitary path. Used as gold standard for other procedures
How can you tell if this patient is having ovulatory cycles?History consistent with ovulatory cycles
(regular, presence of cycle) Timed (luteal phase) endometrial biopsy- is it
secretory? LH surge kits (ovulation prediction kits)
detect LH surge in urine which follows LH surge in serum but occurs before ovulation
Basal body temperature chart with small temperature increase (0.5 degrees) after ovulation
Day 21 serum progesterone level.
Menorrhagia, medical management
NSAID’s, 30% 1st line, 5 days, decrease prostaglandins
Anti fibrinolyltic (transamine) 50% decrease in blood flow)
OCP’s, esp. if contraception desired, up to 60% dec. supp. HP axis
Oral continous progestins (day 5 to 26), most prescribed,
Levonorgestrel IUD (Mirena), High satisfaction rate
GnRH agonists, Inhibit FSH and LH release– hypogonadism, bone
Conjugated estrogens for acute bleedingDanazol, androgenic steroid, amenorrhea in 4-6
weeks, androgenic side effectsOther treatments as indicated e.g. DDAVP for
coagulation defectsCombination can be used
Menorrhagia, surgical management
Surgical
Ablation
Myomectomy
Hysterect-omy
? D & C
polypectomy

Menorrhagia, management summaryTailor treatment to individual
patient.Consider patients age, coexisting
medical diseases, FH, desire for fertility, cost of rx and adverse effects
Surgical management reserved for organic causes (e.g fibroids) or when medical management fails to alleviate symptoms

Case 2; dysmenorrheaA 14-year-old female comes to the clinic,
complaining of severe dysmenorrhea (painful periods) for the past six months. She began menstruating 10 months ago with her first two periods occurring about 2 months apart without pain or any other symptoms.
Since then, she menstruates every 28 days and also notices nausea, diarrhea and headaches during her periods. The pain has gotten so bad for 3 days each month that she often misses school.

Case 2 conti,She is involved in sports and after
school programs, and you think it is unlikely that she is pretending to have dysmenorrhea to get out of school. She denies use of drugs . She says that she gets partial relief by using 2-3 ibuprofen , two or three times a day during her period.
The review of systems, past medical history and social history are noncontributory. The patient’s mother has endometriosis.
Physical exam: The patient’s general and systemic
examination were unremarkable . Pelvic exam not done, a rectal exam
showing a normal size non-tender uterus, which is mobile and anteflexed. There are no nodules on the back of the uterus, and there are no adnexal masses or tenderness.
Laboratory: Urinalysis is negative for blood, nitrites
and leukocytes.
Discussion QuestionsWhat is the differential diagnosis
and most likely diagnosis?What additional evaluation is
needed?How would you manage the possible
diagnoses ?
What is the differential diagnosis and most likely diagnosis?Primary dysmenorrhea is most likely; based on the
onset of pain and associated systemic symptoms, as well as the partial response to NSAIDs
• Secondary dysmenorrhea with underlying endometriosis is less likely; based on the normal physical examination, and the short interval since menarche.
The patient may have an increased risk of endometriosis due to her mother’s history. Most causes of secondary dysmenorrhea increase with age such as structural abnormalities ( i.e. leiomyomata, polyps).
What additional evaluation is needed?A careful history is all that is needed in most
cases of primary dysmenorrhea. No additional evaluation is needed for the
presumptive diagnosis of primary dysmenorrhea.
• However, if appropriate treatment fails to relieve symptoms within 3 months, pelvic exam and additional evaluation (such as ultrasound, hysteroscopy or laparoscopy) is needed to rule out a secondary cause such as endometriosis.

How would you manage the diagnoses of primary dysmenorrhea?NSAIDs are first line treatmentCombination hormonal contraceptives (pills, or
patch) or progesterone-only contraceptive (progesterone injection or implant) provide effective contraception and improve symptoms of dysmenorrhea.
NSAIDs are prostaglandin-synthetase inhibitors, While hormonal contraceptives inhibit ovulation
and progesterone stimulation of prostaglandin production.
Within three months of starting hormonal contraceptives, 90% of women experience improvement.
Case 3; Amenorrhea A 26-year-old seen at clinic complaining of no periods for 9 months. She got 2 children, ages are 5 and 3 years. She breastfed her youngest for 1 year, menses returned right after she stopped, and were monthly and normal until 9 months ago.She is not using any contraception or any other medication. She feels very fatigued, has frequent headaches and has had trouble losing weight. She has no history of abnormal Paps or STI’s. She is married and works from home as a computer consultant.
Examination BP= 120/80, P= 64, Ht=164cm , Wt= 61 kg . She appears tired but in no distress.Breasts show scant bilateral milky white
discharge with manual stimulation. Breast exam reveals no masses, dimpling or retraction.
Examination otherwise normal, including pelvic exam.
HCG is negative.
Discussion Questions:1. Does this patient have primary amenorrhea,
secondary amenorrhea or oligomenorrhea? 2. What is the differential diagnosis for this
disorder? 3. What additional studies are needed? 4. Consider that this patient has a prolactin
level of above 130. The test when repeated with the patient fasting is 100. What is your next step? (normal range <22)
5. If the patient had a withdraw bleed to a progestational challenge and a normal TSH and prolactin, what would be the most likely diagnosis, and what is first line treatment, and long term concern if untreated.
Does this patient have primary or secondary amenorrhea, or oligomenorrhea?Primary amenorrhea definition: no
period age 14 without secondary sex characteristics, age 16 with secondary sex characteristics.
Secondary amenorrhea definition: 6 months of amenorrhea after a history of normal menses.
Oligomenorrhea: menstrual interval >35 days but less than 6 months.

What is the differential diagnosis for this disorder? Pregnancy Hypothalamic--‐Pituitary Dysfunction�
(Pituitary adenoma, sever Hypothyroidism, Medications, brain tumor, chronic illness, excessive exercise & stress,)
Ovarian Dysfunction (Premature ovarian failure)
Genital Outflow Tract AbnormalitiesAnovulation (Polycystic ovarian
syndrome& Thyroid dysfunction)

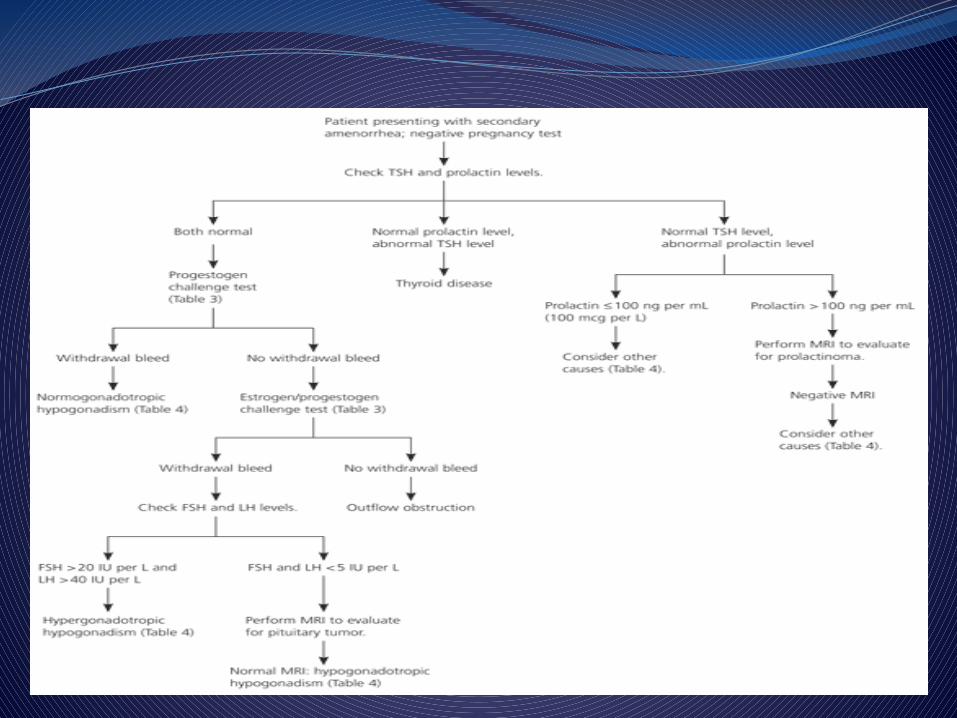
What additional studies are needed?CBC, pregnancy test, TSH, prolactin level, FSH,
Progesterone challenge can distinguish anovulation hypogondism versus a low estrogen or pituitary/hypothalamic etiology.

Results Prolactin 12 ng/ml (normal range <22) &
TSH 1.2 uIU/ml (normal range: 0.4-4.0)• Progestin challenge is negative
consistent with hypogonadism. • Next step in hypogonadism is FSH 80
uIU/ml. Consistent with premature ovarian
insufficiency (POI) Treat POI with HRT; replace estrogen in
order to protect against osteoporosis (and progestin to protect the uterus
Consider that this patient has a prolactin level of above 130. when repeated with the patient fasting is 100. What is your next step?
Males: 2 - 18 ng/mLNonpregnant females: 2 - 29 ng/mLPregnant women: 10 - 209 ng/mL
Pituitary MRITreat with dopamine agonist like bromocriptine or surgical option.
If the patient had a withdraw bleed to a progestational challenge and a normal TSH and prolactin, what would be the most likely diagnosis, first line treatment, and long term concern if untreated?

Polycystic ovarian syndrome• If not wanting to conceive, COCP are best first line treatment. If wanting to conceive, ovulation induction with clomiphene citrate.• Long term the patient is at risk for endometrial hyperplasia / uterine cancer if not treated with progestins regularly. Patient is also at increased risk of diabetes and high cholesterol.

Thank you
Case 4; postmenopausal bleeding
A 66 year-old nulliparous women who underwent menopause at 55 years complains of a 2- week history of vaginal bleeding
Prior to menopause she had irregular menses. She denies the use of oestrogen replacement therapy
her medical history is significant for diabetes mellitus & hypertension controlled with an oral hypoglycaemic & antihypertensive agent.

On examination;84 kg weight, height 158cmBP 150/90 mmHg and temp 37.1 cThe heart and lung exam are normal The
abdomen is obese and no masses are palpated
the external genitalia appear normal The uterus normal size with out adnexal
masses
Discussion QuestionsWhat is the next step?
Perform an endometrial biopsy
What is your concern ?Concern ; Endometrial Cancer
What is the risk factor for endometrial cancer?
She undergoes endometrial sampling , and is diagnosed with endometrial cancer
Which of the following is a risk factor for endometrial cancer ?
a risk factor for endometrial cancer ? endogenous risk factors
increasing age obesity and physical inactivity low parity or infertility diabetes mellitus hypertension early menarche and late menopause polycystic ovarian syndrome family history lynch syndrome (hereditary nonpolyposis colorectal cancer) oestrogen secreting tumours (granulosa or thecal cell tumours of ovary) history of breast cancer immunodeficiency
exogenous risk factors unopposed oestrogen only hormone replacement therapy tamoxifen therapy dietary factors previous radiotherapy
Thank You