radiological anthropometry of the hand in turner's syndrome
TRANSCRIPT

Radiological Anthropometry of the Hand in Turner's Syndrome
ELIZABETH PARK University of Toronto, Toronto, Ontario, Canada M5S 1Al
K E Y WORDS Turner's syndrome Hand X-ray - Anthropometry
ABSTRACT Metacarpal-phalangeal (M-P) lengths, metacarpal sign, and carpal angle were studied using 142 pairs of hand X-rays from 81 individuals with Turner's syndrome age 6 to 25 years. Left M-P lengths, grouped by bone age, were com- pared with normal female standards and Z-score pattern profiles calculated for each bone age. Differences between Turners and normals in most M-P lengths increased with age, particularly after puberty. Calculation of inter-individual and intra-individual variability yielded good evidence for a M-P pattern profile typical of Turner's syndrome, with increasing growth deficiency from distal to proximal and lateral to medial. The incidence of positive metacarpal sign was 33.8%, with no significant difference between XO and non-XO Turners. It did not appear that M4 ceased growth prematurely, suggesting that short M4 is not the result of early epiphyseal fusion. Carpal angle, reported to be abnormally decreased in Turners, was not found to differ from normal. There was no difference between right and left sides or between XO and non-XO Turners, but carpal angle did decrease sig- nificantly with both decreasing ulnar deviation in positioning of the hand and increasing age. In the latter respect Turners differ from normals who show an increase in carpal angle with age.
Turner's syndrome is a condition of phe- notypic females who lack all or part of an X chromosome (Turner, '38; Ferguson-Smith, '65). The most apparent consequences are short stature (< -2 SD for age and sex), delayed puberty and delayed epiphyseal fusion. The delayed maturation is a conse- quence of the absence of ovaries, and is treated by the cyclical administration of estrogen at the appropriate age. A long list of physical stigmata is associated with the syndrome (Smith, '76), frequently includ- ing certain skeletal abnormalities such as broad chest, cubitus valgus, medial tibia1 exostosis, short fourth metacarpal andlor metatarsal. Less common skeletal abnor- malities of the extremities include abnor- mal angulation of the radius to the carpals, short middle phalanx of the fifth finger, short third to fifth metacarpals and/or metatarsals.
Following the identification of these
skeletal abnormalities there has been an at- tempt to quantify the abnormalities of the hand as seen on X-ray. Archibald et al. ('59) devised the metacarpal sign to evaluate the shortening of the fourth metacarpal in rela- tion to the third and fifth metacarpals (fig. 1). Kosowicz ('65) used a measurement called phalangeal preponderance to dem- onstrate that in Turners the phalanges are disproportionately long relative to the metacarpals. A more precise and com- prehensive method of comparing the rela- tive lengths of the metacarpals and pha- langes to each other and to normal stan- dards is by using pattern profile analysis. This involves expressing each bone length in standard deviation units (Z-scores) based
I The following abbreviations will be used: MI, M2. . . M5 for metacarpals one through five. PPI, PP2 , . . PP5 for proximal phalanges one through five. MP2, MP3. , . MP5 for middle phalanges two through five. DPI, DP2 . . . DP5 for distal phalanges one through five.
&. J. PHYS. ANTHROP., 46: 463-470. 463

464 ELIZABETH PARK
Fig. 1 Hand X-ray of a girl with Turner's syn- drome age 10.8 years (bone age 9.3 years). The metacarpal sign is negative because the line touching the heads of M 5 and M4 does not intersect the head of M3, and the carpal sign is negative because the carpal angle is greater than 117" (141").
on the normal mean for age and sex. When this is done, in Turners, the metacarpals and phalanges are short, but the fourth metacarpal is disproportionately short, and the first proximal phalanx and the second middle phalanx are disproportionately long (Poznanski, '74). Work carried out to date (Poznanski et al., '72) has relied on small samples (<25) and has lumped patients of different ages.
The abnormal angulation of the radius to the carpals is a result of the displacement of the lunate towards the radial epiphysis, so that the proximal edge of the proximal row of carpals presents a more angular configuration than normal (Keats and Burns, '64). The measurement called car-
pal angle was devised to uantify this anomaly (Kosowicz, '65) (fig. 1 7 . The carpal angle of Turners has been reported to be significantly lower than in normal females (Kosowicz, '65; Leszczynski and Kosowicz, '65; Dallapiccola e t al., '72).
Using a large series of Turners, the pres- ent study investigates metacarpal and pha- langeal lengths in greater detail than has previously been done. Metacarpal sign and carpal angle are studied, including cer- tain variables which might influence them. The results of a study of cortical width measurements are reported elsewhere (Park, '77).
MATERIALS AND METHODS
A total of 142 pairs of posterior-anterior hand X-rays were studied. Because some individuals had X-rays taken at more than one age, there were 80 X-rays of 46 XO Turners and 62 X-rays of 35 non-XO Tur- ners (i.e., those with mosaic and/or struc- tural X abnormalities), all Caucasian and between 6 and 25 years of age. The lengths of the five metacarpals and 14 phalanges (left side only) were measured by the author with a dial-reading caliper to the nearest 0.05 mm accordin to the tech- nique outlined by Garn ('70 'i . The 19 bone lengths were grouped by Greulich-Pyle (Greulich and Pyle, '59) bone age, so that individuals of similar biological maturity would be lumped, then compared by t-test with normal Caucasian female standards (Poznanski, '74). Where necessary appro- priate corrections were made for small sample size and heterogeneity of variance. Z-scores were calculated for each individ- ual at each bone age and mean Z-scores then calculated for each bone age. Pattern profiles based on these mean scores were plotted for each bone age.
To test inter-individual variability in pat- tern profile, correlations between every in- dividual and every other individual were calculated as product moment correlations (Pearsonian r) at each bone age. Intra-indi- vidual variability was tested by calculating product moment correlations between the
TURNERS SYNDROME HAND ANTIIROPOMETRY
TABLE 1
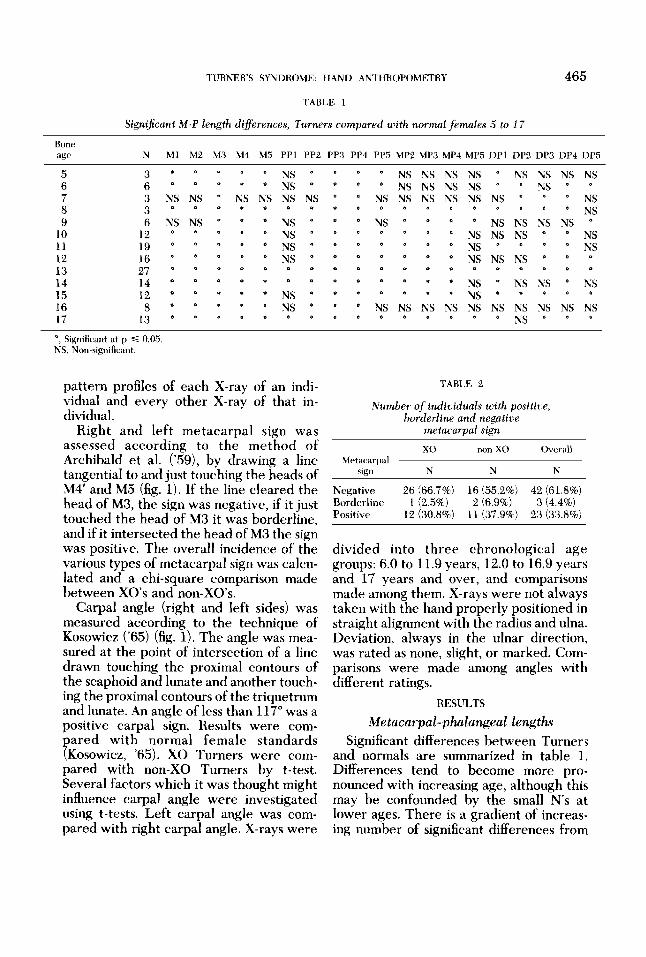
Signijcant M-P length differences, Turnws compared with n o m l females 5 to 17
465
Bone age N hll M2 M3 M4 M5 PP1 PP2 PP3 PP4 PP5 MP2 MP3 MP4 MP5 DP1 DP2 DP3 DP4 DP5
5 6 7 8 9
10 11 12 13 14 15 16 17
3 6 3 3 6
12 19 16 27 14 12 8
13
NS NS NS
NS NS NS NS
*
* 0
NS NS
0
* NS
NS
II
* * (I
NS 0
NS NS NS
*)
*)
0
NS 4
NS NS NS
&
1
*
*
NS &
NS NS NS
*I
(i
(I
di
I)
(I
NS
NS NS NS
II
NS NS NS
NS NS NS *
* NS
NS NS
NS 4
e
0
I)
NS
NS 0
'1
NS NS
NS
NS
NS NS
4
NS NS NS NS * *
LI NS * * NS
* NS * NS
NS NS *
* 0 4
o o *
NS (I NS
NS NS NS o r ) *
* * *
*, Significant at p s 0.05. NS, Non-significant.
pattern profiles of each X-ray of an indi- vidual and every other X-ray of that in- dividual.
Right and left metacarpal sign was assessed according to the method of Archibald et a]. ('59), by drawing a line tangential to and just touching the heads of M4' and M5 (fig. 1). If the line cleared the head of M3, the sign was negative, if it just touched the head of M3 it was borderline, and if it intersected the head of M3 the sign was positive. The overall incidence of the various types of metacarpal sign was calcu- lated and a chi-square comparison made between XO's and non-XO's.
Carpal angle (right and left sides) was measured according to the technique of Kosowicz ('65) (fig. 1). The angle was mea- sured at the point of intersection of a line drawn touching the proximal contours of the scaphoid and lunate and another touch- ing the proximal contours of the triquetrum and lunate. An angle of less than 117" was a positive carpal sign. Results were com- pared with normal female standards (Kosowicz, '65). XO Turners were com- pared with non-XO Turners by t-test. Several factors which it was thought might influence carpal angle were investigated using t-tests. Left carpal angle was com- pared with right carpal angle. X-rays were
TABLE 2
Number of individuals with positive borderline and negative
metacarpal sign
XO non-XO Overall Metacarpal
sign N N N
Negative 26 (66.7%) 16 (55.2%) 42 (61.8%) Borderline 1 (2.5%) 2 (6.9%) 3 (4.4%) Positix 12 (30.8%) 11 (37.9%) 23 (33.8%)
divided into three chronological age groups: 6.0 to 11.9 years, 12.0 to 16.9 years and 17 years and over, and comparisons made among them. X-rays were not always taken with the hand properly positioned in straight alignment with the radius and ulna. Deviation, always in the ulnar direction, was rated as none, slight, or marked. Com- parisons were made among angles with different ratings.
RESULTS
Metacarpal- phalangeal lengths Significant differences between Turners
and normals are summarized in table 1. Differences tend to become more pro- nounced with increasing age, although this may be confounded by the small N's at lower ages. There is a gradient of increas- ing number of significant differences from

466 ELIZABETH PARK
60
50
E E I I- 0 4 0 2 W -1
30.
20.
/ <’- / Ml //- I / ,:. --- - - -
/ /
,’ / / / , / ,
_ _ - - - _ /-x - NORMAL FEMALE
TURNER
6 8 10 12 14 16 18
AGE Fig. 2 Pattern of growth in length of M I , 1.14 and PPl in Turner’s and normal females. M1 stays at
a constant level below normal until falling off at puberty, M4 is always more below normal, with little falling off at puberty; PP1 is only slightly below normal.
distal phalanges through metacarpals. The first proximal phalanx is not significantly different at many of the ages while the other proximal phalanges are significantly different. The lack of significance for age 16 is perhaps explained by the small N at that age.
In general the pattern of growth of the metacarpals and phalanges is similar to that of height growth in Turners, being below normal during childhood, but falling off more noticeably from normal after (bone) age I 2 (fig. 2).
Two representative Z-score pattern profiles, at bone age 13 (N = 27) and bone age 17 (N = 13) are given in figure 3. The patterns at these and other ages exhibit a number of similarities. The metacarpals
and proximal phalanges show greater deviation from normal than the middle and distal phalanges; the metacarpals in turn differ more than the proximal phalanges. Within each of the rows deviation from normal tends to increase from lateral to medial.
The percentage of significant and posi- tive inter-individual pattern profile corre- lations generally varies from 30%-50% at different bone ages; the number of nonsig- nificant correlations is greater than or equal to the number of significant positive correlations at all bone ages. The only sig- nificant negative correlations occur at age 17 and involve only two individuals, one a very atypical Turners (XXp-, 167 cm tallj. Discounting early ages when N’s are very

TURNER'S SYNDROME: HAND ANTHROPOMETHY 467
I 5 1
0- /
-I w a 0
t 5 2 5 1 5
PROXIMAL MIDDLE DISTAL
AGE 13 -_- - AGE 17
-
Fig. 3 Z-score pattern profiles for Turners at bone ages 13 and 17, based on normal female means for age. There are two gradients of increasing size reduction, one from distal to proximal and one from lateral to medial.
small, there is no marked trend for the number of significant correlations to increase or decrease with age. Nor is there any tendency for XO-XO correlations to be greater than non-XO-non-XO correlations, or for either of these to be greater than XO-non-XO correlations.
Correlations of pattern profiles on X-rays of the same individual taken at different points in time show that most of the corre- lations (109 or 93.2%) are significant and positive (r 3 + 0.456); 76 (64.9%) are 2 0.900. No correlations are significant and negative; the eight (6.9%) nonsignificant correlations involved X-rays taken more than five years apart. Correlations values decrease with increasing length of time be- tween X-rays. Overall it appears that there is considerable intra-individual pattern profile constancy, although it was impossi- ble to test the very long term constancy.
Metacarpal sign Positive or borderline metacarpal sign
was present in 38.2% of Turners (table 2 ) . The incidence did not differ between XO's and non-XOs. The left hand was used in these calculations, but the results would not have differed had the right hand been used; of 68 individuals investigated, ten were not bilaterally symmetrical in this re-
TABLE 3
Effect of ulnar deviation on carpal angle
Significant Ulnar dwiation Carpal differences
N arigle (u < 0.05)
rt S.D. None 42 123.8 8.73-
Slight 49 129.6 9.47,
Marked 44 136.7 7.24
O , Significant at p 4 0 05 NS Non significant
spect, five having the left side affected and the right side unaffected and five the reverse.
Carpal angle The mean carpal angle, based on all X-
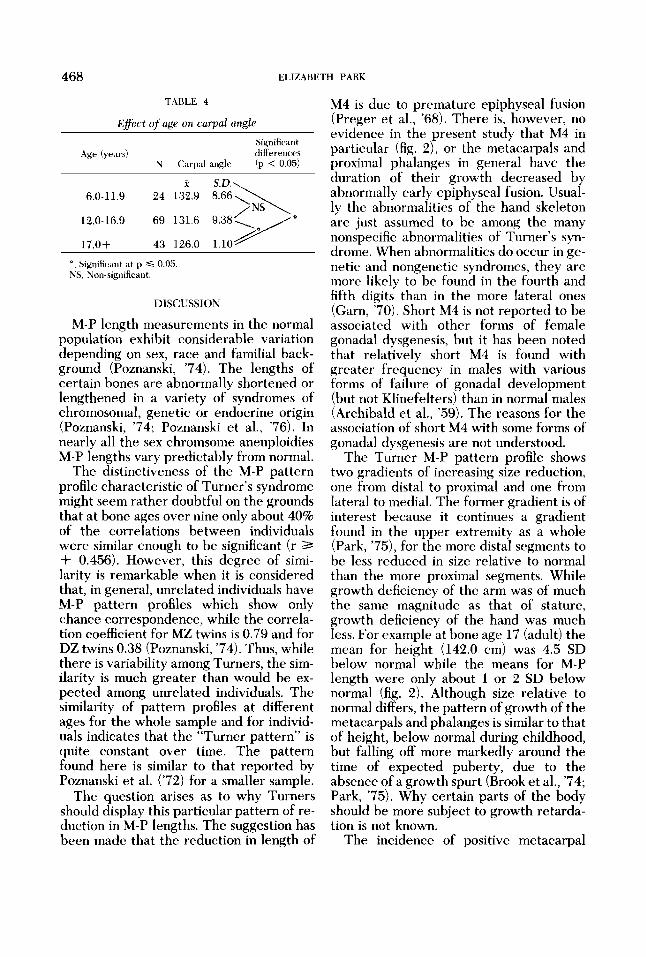
rays, including those with ulnar deviation, was 129.4' .t 9.78", not significantly different from normal females (131.5' I+ 7.2"). Only three of 63 had a positive carpal sign (<117"). XO's and non-XO's did not differ in carpal angle. The difference in carpal angle between right and left sides was not significant. Positioning the hand in marked ulnar deviation significantly in- creased the angle (table 3). With age the angle decreased significantly (table 4).
468 ELIZABETH PARK
TABLE 4
Eflect of uge on carpal angle Significant
.4ge (years) differencry N Carpal angle !p < 0.05)
f S.D.\ 6.0-11.9 24 132.9
12.0-16.9 69 131.6 9.38,
17.0+ 43 126.0 1.10
*, Significant at p 5 0.05 NS, Non-significant.
DISCUSSION
M-P length measurements in the normal population exhibit considerable variation depending on sex, race and familial back- ground (Poznanski, ’74). The lengths of certain bones are abnormally shortened or lengthened in a variety of syndromes of chromosomal, genetic or endocrine origin (Poznanski, ’74; Poznanski et al., ’76). In nearly all the sex chromsome aneuploidies M-P lengths vary predictably from normal.
The distinctiveness of the M-P pattern profile characteristic of Turner’s syndrome might seem rather doubtful on the grounds that at bone ages over nine only about 40% of the correlations between individuals were similar enough to be significant (r 3 + 0.456). However, this degree of simi- larity is remarkable when it is considered that, in general, unrelated individuals have M-P pattern profiles which show only chance correspondence, while the correla- tion coefficient for MZ twins is 0.79 and for DZ twins 0.38 (Poznanski, ’74). Thus, while there is variability among Turners, the sim- ilarity is much greater than would be ex- pected among unrelated individuals. The similarity of pattern profiles at different ages for the whole sample and for individ- uals indicates that the “Turner pattern” is quite constant over time. The pattern found here is similar to that reported by Poznanski et al. (’72) for a smaller sample.
The question arises as to why Turners should display this particular pattern of re- duction in M-P lengths. The suggestion has been made that the reduction in length of
M4 is due to premature epiphyseal fusion (Preger et al., ’68). There is, however, no evidence in the present study that M4 in particular (fig. 2), or the metacarpals and proximal phalanges in general have the duration of their growth decreased by abnormally early epiphyseal fusion. Usual- ly the abnormalities of the hand skeleton are just assumed to be among the many nonspecific abnormalities of Turner’s syn- drome. When abnormalities do occur in ge- netic and nongenetic syndromes, they are more likely to be found in the fourth and fifth digits than in the more lateral ones (Garn, ’70). Short M4 is not reported to be associated with other forms of female gonadal dysgenesis, but it has been noted that relatively short M4 is found with greater frequency in males with various forms of failure of gonadal development (but not Klinefelters) than in normal males (Archibald et al., ’59). The reasons for the association of short 344 with some forms of gonadal dysgenesis are not understood.
The Turner M-P pattern profile shows two gradients of increasing size reduction, one from distal to proximal and one from lateral to medial. The former gradient is of interest because it continues a gradient found in the upper extremity as a whole (Park, ’75), for the more distal segments to be less reduced in size relative to normal than the more proximal segments. While growth deficiency of the arm was of much the same magnitude as that of stature, growth deficiency of the hand was much less. For example at bone age 17 (adult) the mean for height (142.0 em) was 4.5 SD below normal while the means for M-P length were only about 1 or 2 SD below normal (fig. 2). Although size relative to normal differs, the pattern of growth of the metacarpals and phalanges is similar to that of height, below normal during childhood, but falling off more markedly around the time of expected puberty, due to the absence of a growth spurt (Brook et al., ’74; Park, ’75). Why certain parts of the body should be more subject to growth retarda- tion is not known.
The incidence of positive metacarpal

TURNERS SYNDROME: HAND ANTHROPOMETRY 469
sign in the present study (33.8%) is con- siderably lower than frequencies previous- ly reported: 69.7% (Finby and Archibald, '63); 60.0% (Kosowicz, '65); 50.0% (Leszczynski and Kosowicz, '65) ; 77.0% (Preger et a]., '68); 50.0% (Dallapiccola et al.. '72). Why the incidence in other series should be uniformly higher is not clear. It might be the result of bias in the direction of more unusual findings being reported more often than more normal findings. The differences are not likely accounted for by variations in the karyotypic constitutions of the samples, as the frequency of positive metacarpal sign was not found to differ sig- nificantly between XO and non-XO Tur- ners in this series or that of Preger et al. ('68). The fact that the present series is younger than some of the others might be expected to lower the frequency, since it has been reported that there is a tendency for the metacarpal sign to become more positive with increasing age (Preger et al., '68). This seems unlikely, however, be- cause no such trend was noted in the pres- ent series. In the absence of a satisfactory explanation, the low incidence should probably be viewed tentatively as a chance phenomenon.
Decreased carpal angle, a result of increased proximal angulation of the prox- imal row of carpals, is a less extensively re- ported hand anomaly of Turners. In the two original series available for comparison the frequency of positive carpal sign (car- pal angle < 117") was 55% (Kosowicz, '65) and 62% (Leszczynski and Kosowicz, '65). The present study differed considerably, finding no significant difference between Turners and normal females in mean carpal angle, and only 4.8% of individuals with positive carpal sign. Preger et al. ('68) also report a mean carpal angle for 34 Turners of 129", very similar to the normal female mean (131.7"), and Poznanski et al. ('76) found the carpal angle of 28 Turners to be within the normal range (2 = 128O). Since it was determined, in agreement with the findings of Harper et al. ('74) that posi- tioning of the hand in ulnar deviation, and immature bone age were associated with
greater carpal angle, these factors undoub- tedly increased the mean carpal angle in the present series. However, the frequency of positive carpal sign was only 28.6% when X-rays with marked ulnar deviation were excluded, and only 23.3% when X-rays below mature bone age were excluded. Thus, since the frequency of reduced carpal angle appears definitely lower in the present series and at least two others, than in the series originally re- ported, its value as a common feature of Turner's syndrome should be viewed with some skepticism. In addition, if it is to be used, the importance of proper positioning of the hand should be stressed. One finding which may be of importance in the ontogeny of increased angulation of the proximal carpal row in Turners is that, whereas in normals the carpal angle increases with age (Harper et al., '74), in Turners, the carpal angle shows a sig- nificant decrease with increasing maturity.
ACKNOWLEDGMENTS
I would like to thank the Medical Re- search Council of Canada for financial assistance during this research. I am also indebted to Doctor K. 0. McCuaig, Doctor J. D. Bailey and Doctor M. A. Gates for their help.
LITERATURE CITED Archibald, R. M., N. Finhy and F. De Vito 1959 En-
docrine significance of short metacarpals. J. Clin. Endocrinol., 19: 1312-1322.
Brook, C. G. D.; G. Murset, M. Zachmann and A. Prader 1974 Growth in children with 45 XO Turner's syndrome. Arch. Dis. Child., 49: 789-795.
Dallapiccola, B., B. Bagni and G. Pistocci 1972 Der- matoglyphic and skeletal hand abnormalities in Turner's Syndrome - A tentative scoring method. Acta Genet. Med. Gemellol.. 2 7 : 69-79.
Ferguson-Smith, M. A . 1965 Review Article: Karyotype-phenotype correlations in gonadal dysgenesis and their bearing on the pathogenesis of malformations. J. Med. Genet., 2: 142-155.
Finby, N., and R. M. Archibald 1963 Skeletal abnor- malities associated with gonadal dysgenesis. Amer. J. Roentgenol., 89: 1222-1235.
Garn, S. M. 1970 The Earlier Gain and Later Loss of Cortical Bone. Chas. C Thomas, Springfield.
Greulich, W. W., and S. I. Pyle 1959 Radiographic Atlas of Skeletal Development of the Hand and Wrist. Second edition. Stanford Univ. Press, Stan- ford.

470 ELIZABETH PARK
Harper. H. A. S., A. K. Poznanski and S. M. Garn 1974 The carpal angle in American populations. Investig. Radiol., 9: 217-221.
Ktxts, T. E., and T. W. Burns 1964 Radiographic manifestations of gonadal dysgenesis. Radiol. Clin. N. Amer., 2: 297-313.
Kosowicz, J. 1965 The roentgen appearance of the hand and wrist in gonadal dysgenesis. Amer. J. Roentgenol., 93: 354-361.
Leszczynski, S., and J. Kosowicz 1965 Radiological changes in the skeletal system in Turner’s syn- drome. A review of 102 cases. Progress in Radiology, Symposium of the 11 th International Congress of Radiology, Rome, 1965.
Park, E. 1975 An Anthropometric and Radio- graphic Study oP the Development of Individridls with Turner’s Syndrome. Ph.D. thesis, University of Toronto.
1977 Cortical bone measurements in Turner’s syndrome. Am. J. Phys. Anthrop., 46: 455- 462.
Poznanski, A. K. 1974 The Hand in Hadiologic Diagnosis. W. B. Saunders Co., Philadelphia and London.
Poznanski, A. K., S. M. Garn, J. M. Nagy and J. C. Gall, Jr. 1972 Metacarpo-phalangeal pattern profiles in the evaluation of skeletal malformations. Radiol., 104: 1-11.
Poznanski, A. K.: S. M. Garn and H. A. Shaw 1976 The carpal angle in the congenital malformation syndromes. Ann. Radiol., 19: 141-150.
Preger, L., M. B. Howard, L. Steinbach, P. Moskowitz, A. L. Scully and M. B. Goldberg 1968 Roentgen- ographic ahmrmalities in phenotypic females with gonadal dysgenesis. Amer. J. Roentgenol., 104: 899- 910.
Smith, D. W. 1976 Recognizable Patterns of Human Malformation. Second edition. W. B. Saun- ders Co., Philadelphia and London.
Turner, H. H. 1938 A syndrome of infantilism, con- genital webbed neck and cubitus valgus. Endocri- nol., 23: 566-574.