radionuclide studies and radioiodine therapies for thyroid diseases
TRANSCRIPT

In vivo Thyroid function Tests &
Radioiodine Therapy
Jiraporn Sriprapaporn, M.D. Division of Nuclear Medicine Department of Radiology Siriraj Hospital
THYROID_MD4_JIRAPORN_July 2015

Outlines
In-vivo Thyroid Function Tests
RAIU
Thyroid scan
I-131 total body scan
Radioiodine Therapy
Hyperthyroidism
Thyroid Cancer
THYROID_MD4_JIRAPORN_July 2015

I. In-vivo Thyroid Function Tests
RAIU
Thyroid scan
I-131 total body scan
II. Hyperthyroidism
III. Thyroid Cancer
THYROID Outlines
Hypothalamic-pituitary-thyroid axis THYROID_MD4_JIRAPORN_July 2015

ROUTINE:
1. Begin with clinical history and physical examination.
2. In-vitro TFT (LAB)
If satisfied Definite Diagnosis Treatment
If not, What are you going to do?
Diagnosis of thyroid disorders
THYROID_MD4_JIRAPORN_July 2015

In-vitro TFT is equivocal.
In-vitro TFT does not get along with the clinical
context.
In-vitro TFT does not provide the information
needed.
When to perform in-vivo TFT?
THYROID_MD4_JIRAPORN_July 2015

Indications :
Confirm hyperthyroidism in case questionable serum TFT
DDx hyperthyroidism VS thyroiditis
Calculate RAI Rx dose for hyperthyroidism
Radiotracer : I-131 10 µCi, oral
Patient preparation :
Withdraw anti-thyroid drug for 1 wk.
Withdraw thyroid hormone at least 2 wk.
Avoid factors producing iodine overload :
• No prior contrast study 4-6 wk.
• No amiodarone, betadine, KI
Fasting ~ 2 hr.
Radioactive Iodine Uptake (RAIU)
THYROID_MD4_JIRAPORN_July 2015
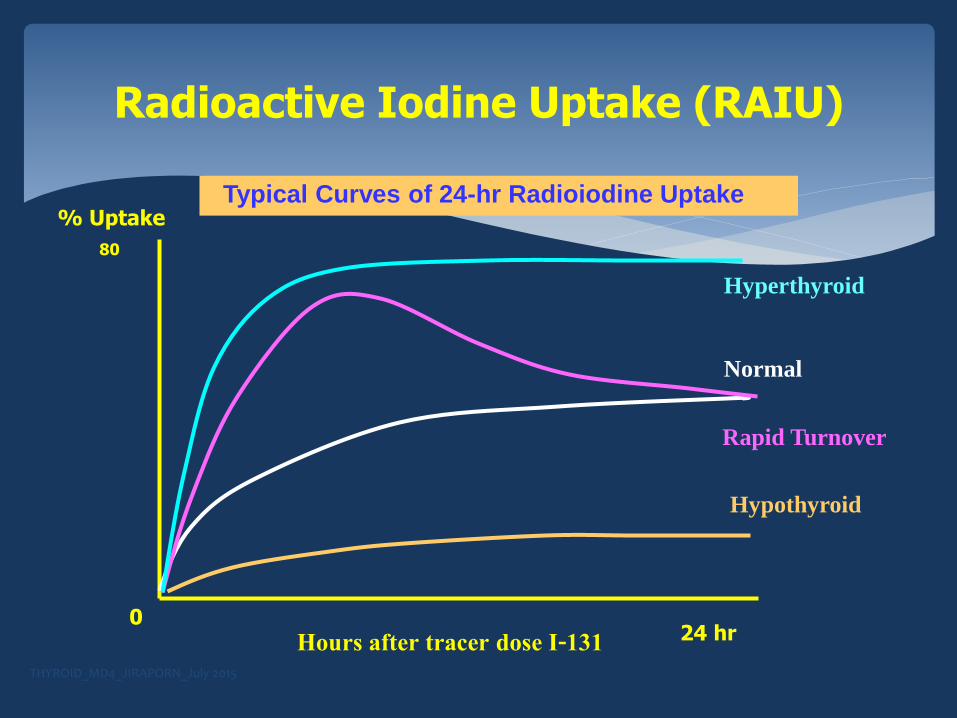
Radioactive Iodine Uptake (RAIU)
Hypothyroid
Typical Curves of 24-hr Radioiodine Uptake
Normal
Hyperthyroid
Hours after tracer dose I-131 24 hr
% Uptake
80
0
Rapid Turnover
THYROID_MD4_JIRAPORN_July 2015

Normal: 15%-45% (Siriraj)
Increased uptake :
Hyperthyroidism
Iodine deficiency/ starvation
Others: early Hashimoto’s thyroiditis, rebound effect after discontinuing
antithyroid drugs, hypoalbuminemia (pregnancy, CKD, lithium, hCG)
Decreased uptake - 4 mechanisms
Block trapping : Iodine overload, exogenous iodine (thyrotoxicosis
factitia), endogenous iodine (struma ovarii)
Block organification : PTU, MMI
Parenchymal destruction : Subacute thyroiditis
Hypothyroidism : post-Sx, post RAI Rx, other causes
RAIU: Interpretation
THYROID_MD4_JIRAPORN_July 2015

Radiopharmaceuticals: Tc-99m & Iodine isotopes
Mechanism : iodine is more specific than Tc-99m
Indications for thyroid scan: ATA guideline
Tc-99m vs radioiodine
Patient Preparation
Imaging Techniques
Image Interpretation
THYROID_MD4_JIRAPORN_July 2015
Thyroid Scan

Radionuclides I-123 I-131 Tc-99m pertechnetate
Decay Electron capture Beta-minus decay Isomeric transition
T ½ 13 hrs. 8 days 6 hrs.
Energy keV 159 364 140
Radiation emitted only & β only
Localization by Active transport: Trapping & Organification
Active transport: T & Org Active transport: Trapping only
Administration Oral Oral IV
Dose 100-400 µCi 50-100 µCi 2 mCi
Imaging Time 3-4 hr. and/or 24 hr. 24 hr. 20 min.
Strength
-Test both trapping & organification -Pure gamma ray -No beta ray
-Test both trapping & organification -Substernal goiter
-Pure gamma ray -Rapid result, Low radiation
Weakness -Cyclotron produced not widely available
-Beta ray -Slow result
-Test only trapping function
Thyroid Scan: Radionuclides

ATA Guideline 2009:Thyroid Nodule
Thyroid nodule TSH
Low TSH Thyroid scan to
R/O toxic adenoma
Not low U/S –FNA to R/O
thyroid malignancy
If FNA suggests or
suspicious for malignancy
Surgery
ATA: American Thyroid Association
Cooper et al. THYROID 2009 THYROID_MD4_JIRAPORN_July 2015
Evaluate cause of hyperthyroidism in case presenting with a palpable thyroid nodule (suspected toxic adenoma)
Evaluate function of thyroid nodule in euthyroid patients : solitary or dominant thyroid nodule (suspected cold nodule or to R/O thyroid cancer)
Evaluate anatomy & location of thyroid gland: neonatal hypothyroidism, suspected ectopic thyroid
Tc-99m thyroid scan Indications
THYROID_MD4_JIRAPORN_July 2015

Evaluate substernal mass or mediastinal mass to
R/O substernal goiter
Planning for I-131 treatment : Differentiated
thyroid cancer (DTC). I-131 total body scan is
preferred.
I-131 thyroid scan Indications
THYROID_MD4_JIRAPORN_July 2015

Thyroid Scan: Techniques
Tc-99m thyroid scan
For routine use !!
2 mCi TcO4- IV injected
Imaging at 20 mins later
I-131 thyroid scan
For special purposes
60-100 uCi I-131 orally given
Imaging at 24 hr. later
Withdraw T4 at least 2 wks before thyroid scan
THYROID_MD4_JIRAPORN_July 2015

Normal Thyroid Scan
X Tc-99m I-123
THYROID_MD4_JIRAPORN_July 2015

Ectopic Thyroid
Lingual thyroid
X
THYROID_MD4_JIRAPORN_July 2015

Thyroid Nodules: Incidence of CA
Solitary thyroid nodule : 15-20%
Multinodular goiter :5%
Hot nodule: < 1%
REF: The Requisites, 4th edition, 2014 THYROID_MD4_JIRAPORN_July 2015

Solitary Cold Nodule
THYROID_MD4_JIRAPORN_July 2015

Multinodular Goiter
THYROID_MD4_JIRAPORN_July 2015

Hot Nodule
S
Autonomous nodule
THYROID_MD4_JIRAPORN_July 2015
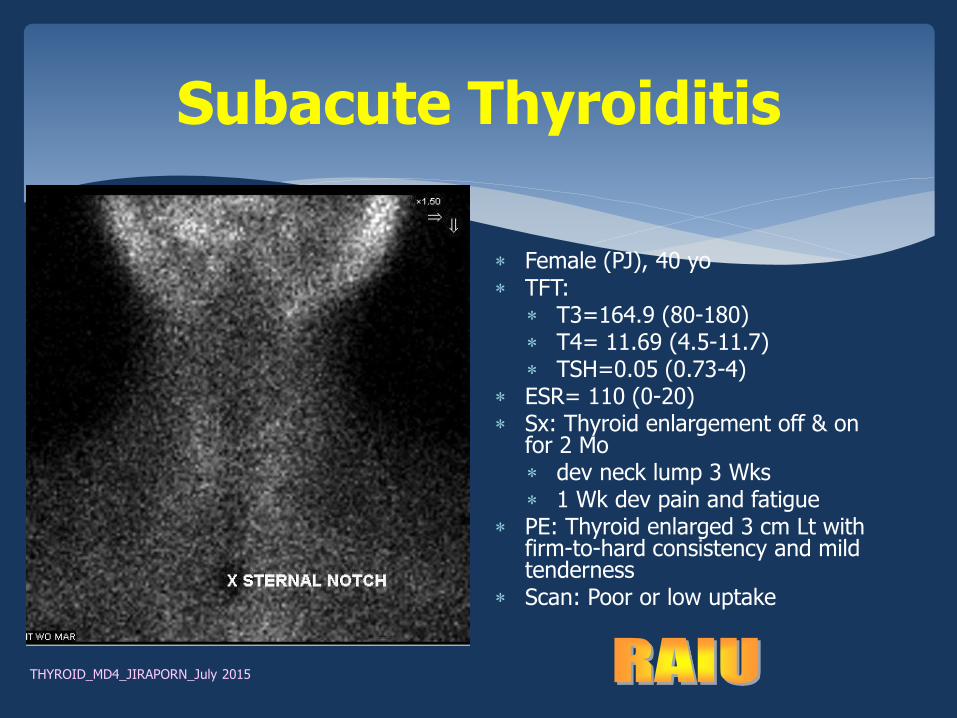
Subacute Thyroiditis
Female (PJ), 40 yo TFT:
T3=164.9 (80-180) T4= 11.69 (4.5-11.7) TSH=0.05 (0.73-4)
ESR= 110 (0-20) Sx: Thyroid enlargement off & on
for 2 Mo dev neck lump 3 Wks 1 Wk dev pain and fatigue
PE: Thyroid enlarged 3 cm Lt with firm-to-hard consistency and mild tenderness
Scan: Poor or low uptake
THYROID_MD4_JIRAPORN_July 2015

Solitary Thyroid Nodules
F:M = 4:1 but % CA in M > F
Cold nodules: Incidence of CA upto 20%
Warm nodules: 4%
Hot nodules: < 1%
THYROID_MD4_JIRAPORN_July 2015

Indication: Differentiated thyroid cancer (DTC)
Evaluate residual thyroid tissue
Evaluate functioning metastasis
Evaluate treatment response
Patient preparation
Thyroid hormone withdrawal for 4 weeks TSH > 30 mIU/L
Low-iodine diet 1-2 weeks.
I-131 whole/total body scan
THYROID_MD4_JIRAPORN_July 2015
Technique
Diagnostic WBS/TBS
I-131 5 mCi oral
Imaging at 48-72 hr. later
Post-therapeutic WBS/TBS
- I-131 100-200 mCi oral for treatment
Imaging 3-7 days later
I-131 whole/total body scan
THYROID_MD4_JIRAPORN_July 2015

Normal : Physiologic uptake -thyroid tissue,
salivary glands, nasal mucosa, oropharynx, GI
tract, liver, urinary bladder, choroid plexus
Abnormal : tumor recurrence, metastasis (I-131
avid)
Interpretation
THYROID_MD4_JIRAPORN_July 2015

Negative I-131 TBS
Post total thyroidectomy and I-131 ablation
C = Colon
B = Urinary bladder
Thyroid bed
Bladder B
C
THYROID_MD4_JIRAPORN_July 2015

Intense uptake at thyroid bed residual thyroid
tissue or thyroid remnant.
Physiologic I-131 distribution
PostRx I-131 TBS
THYROID_MD4_JIRAPORN_July 2015

RxTBS: Multiple foci of uptake in the left thyroid bed, lungs, right humerus, ribs, acetabulum, and femurs
Follicular thyroid carcinoma with multiple bone metastases
Anterior Posterior
THYROID_MD4_JIRAPORN_July 2015

FTC PO & multiple RAI Rx with distant metastases
KW 27-2-2012
THYROID_MD4_JIRAPORN_July 2015

Planar RxTBS:
Thyroid remnant uptake
Faint uptake at right
upper medistinum
SPECT/CT:
A small Rt paratracheal
node with I-131 uptake
RxTBS in a thyroidectomized PTC Patient: SPECT/CT confirmed nodal met.
Sriprapaporn J, JMAT 2015
THYROID_MD4_JIRAPORN_July 2015

A 65-y-old woman with thyroidectomized PTC
Planar 131I imaging detected only 1 focus of radioiodine uptake, corresponding to residue in thyroglossal tract (arrow).
SPECT/CT image fusion (C) confirmed residue (arrow) but also showed 1 radioiodine-avid LN metastasis (arrow, D) in right submandibular region.
Diagnosis was confirmed at surgery to be PTC lymph node metastasis.
SPECT/CT confirm thyroglossal duct remnant & revealed Rt submandibular LN metas.
Spanu A, JNM 2009 THYROID_MD4_JIRAPORN_July 2015

I. In-vivo Thyroid Function Tests
RAIU
Thyroid scan
I-131 total body scan
II. Hyperthyroidism
III. Thyroid Cancer
Contents
THYROID_MD4_JIRAPORN_July 2015

Terminology:
Thyrotoxicosis = increased thyroid hormones in the circulation, any causes.
Hyperthyroidism = Increased production of thyroid hormones
Cause of hyperthyroidism
Graves’ disease (diffuse toxic goiter)
Toxic multinodular goiter (Toxic MNG or Plummer’s disease)
Toxic adenoma (solitary autonomous nodule)
II. Hyperthyroidism
THYROID_MD4_JIRAPORN_July 2015

1. Medical treatment
2. Surgical treatment
3. Radioiodine treatment
4. Combined medical & RAI Rx **
Choices of Rx Hyperthyroidism
THYROID_MD4_JIRAPORN_July 2015

Antithyroid drugs Surgery I-131
Indication
1. Children, teenagers
2. Pregnant women
3. Not severe symptoms
4. Thyroid is not much
enlarged.
1. Marked thyroid enlargement with compressive symptoms ex. dysphagia, airways obstruction
2. Suspected coexisting thyroid cancer
3. Not respond to medical Rx & C/I for I-131 treatment
1. Severe A/E of ATD 2. Failed medical Rx 3. Relapse after medical Rx or
surgery 4. Poor compliance 5. Elderly 6. U/D eg. CAD, CHF
ขอ้ด ี
1. Available 2. Low cost
1. Rapid result 2. Immediate reduction of gland
size 3. High remission rate
1. Total cost is not high. 2. Painless 3. Gradual reduction of gland
size 4. Low side effect 5. High remission rate
ขอ้เสยี
1. Long-term administration
2. Low remission rate 3. Adverse drug effects:
fever, rash pruritus, arthralgia, hepatitis, agranulocytosis
1. High cost 2. Painful, needs hospitalization 3. May be impossible in cases
with lots of comorbid conditions.
4. Possible surgical complications eg. recurrent laryngeal n. injury
1. Radiation exposure 2. C/I pregnancy, lactating
women, small children 3. Slow action (few wks.) 4. Chance to develop
permanent hypothyroidism & needs long-life thyroid hormone replacement
Treatment options
THYROID_MD4_JIRAPORN_July 2015

Medical Treatment of Hyperthyroidism
Titrate the antithyroid drug dose every 4 weeks until thyroid
functions normalize.
Remission rate is ~ 60 % when therapy is continued for 2 years [15]
and the drug can be discontinued.
Notably, half of the patients who go into remission have a
recurrence of hyperthyroidism within the following year.
Nodular forms of hyperthyroidism (toxic MNG and toxic
adenoma) are permanent conditions and will not go into
remission. RAI Rx or surgery
eMedicine.com
15: Harper MB, Mayeaux EJ Jr. Thyroid disease. In: Taylor RB. Family medicine: principles and practice. 6th ed. New York: Springer, 2003:1042–52.
THYROID_MD4_JIRAPORN_July 2015

Radioactive Iodine Therapy
Radioactive iodine therapy [7] is the most common treatment for hyperthyroidism in adults in the United States.
Although the effect is less rapid than it is in antithyroid medication or thyroidectomy, it is effective and safe and does not require hospitalization.
eMedicine.com THYROID_MD4_JIRAPORN_July 2015

RAI Treatment for
Hyperthyroidism
RAI is widely used for > 70 yrs., since early 1940s
No evidence of increased risk to develop malignancies
I-131 solution vs capsule
I-131 solution is less expensive than I-131 capsule
No patient isolation/admission is necessary but precaution is
advised.
Need birth control for women in reproductive life during the
course of RAI treatment !!
THYROID_MD4_JIRAPORN_July 2015

RAI Treatment for Hyperthyroidism: Indications
Failed medical/surgical treatment-relapse
Serious adverse effects of antithyroid drugs: drug allergy,
agranulocytosis
Progressive enlargement of thyroid gland during medical therapy
Inconvenience for frequent contact
Poor compliance of medications
Poor socioeconomic problems
Presence of serious associated medical illness eg. heart failure THYROID_MD4_JIRAPORN_July 2015

RAI Rx for Hyperthyroidism: Contraindications
Pregnant
Lactating
Precaution: Severe hyperthyroidism
THYROID_MD4_JIRAPORN_July 2015

I-131 Dose Calculation
Dose determination - formula below
Gland size, % uptake, dose of I-131 /gram thyroid tissue
Other factors
Severity of hyperthyroidism
Types of hyperthyroidism: nodular* vs diffuse
Other clinical parameters
RAI Dose = [Thyroid mass (g) x 80-200 uCi/gm]/% uptake
THYROID_MD4_JIRAPORN_July 2015

RAI Rx Guideline for Hyperthyroidism
Stop antithyroid drugs for 5-7 days
24 hr. I-131 uptake
I-131 Rx dose according to calculation.
Combined medical Rx in severe thyrotoxic pts.
Peak result of RAI Rx needs about 3-4 months.
Long term F/U, monthly after 1st RAI Rx & reevaluate before reRx.
Repeat RAI Rx: usually 3-6 mo interval if still hyper.
Thyroid H. replacement if permanent hypothyroidism is developed.
THYROID_MD4_JIRAPORN_July 2015

Seem very low-nausea/vomiting is not common.
No increase in cancer incidence
Not cause infertility; mostly related to hyper- or hypothyroid conditions.
Sisson JC, et al. (2011). Radiation safety in the treatment of patients
with thyroid diseases by radioiodine 131I: Practice recommendations of the American Thyroid Association. From the American Thyroid Association Taskforce on Radioiodine Safety. Thyroid, 21(4): 335–346.
Side Effects of RAI Rx for Hyperthyroidism
THYROID_MD4_JIRAPORN_July 2015

I. In-vivo Thyroid Function Tests
RAIU
Thyroid scan
I-131 total body scan
II. Hyperthyroidism
III. Thyroid Cancer
Thyroid
THYROID_MD4_JIRAPORN_July 2015

Classification of thyroid cancer
Well-differentiated thyroid cancer:
Derived from follicular cells uptake iodine ***
Papillary thyroid cancer (PTC) or mixed papillary-follicular,
Follicular (FTC), Hurthle cell carcinoma (variant of FTC)
Medullary carcinoma
Derived from C-cells does not uptake iodine
Undifferentiated or anaplastic thyroid cancer
III. Thyroid cancer
THYROID_MD4_JIRAPORN_July 2015
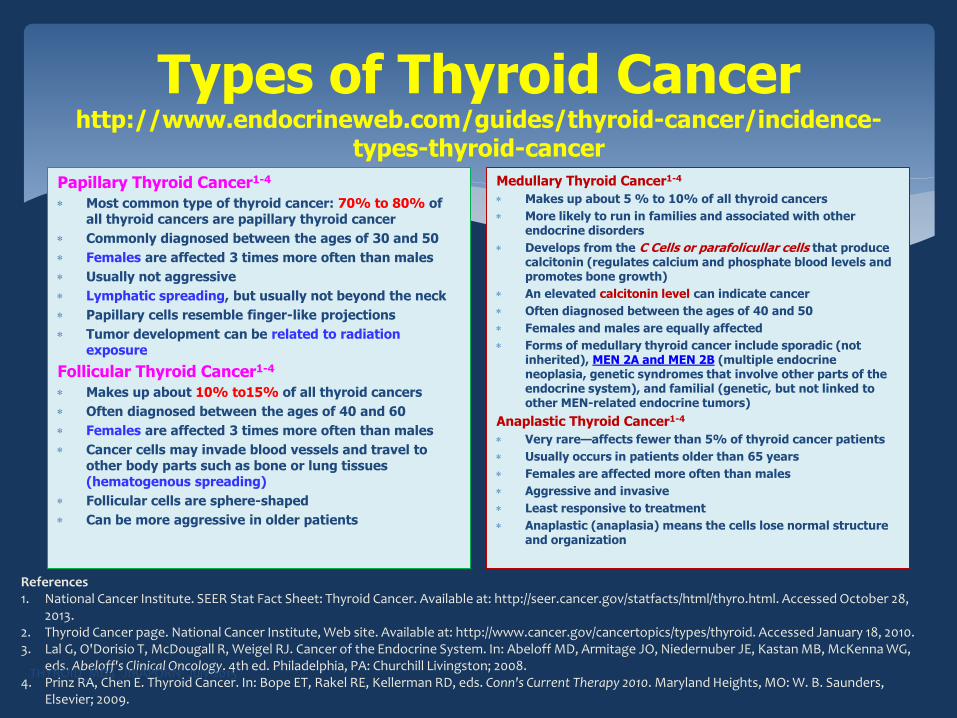
Types of Thyroid Cancer http://www.endocrineweb.com/guides/thyroid-cancer/incidence-
types-thyroid-cancer
Papillary Thyroid Cancer1-4
Most common type of thyroid cancer: 70% to 80% of all thyroid cancers are papillary thyroid cancer
Commonly diagnosed between the ages of 30 and 50
Females are affected 3 times more often than males
Usually not aggressive
Lymphatic spreading, but usually not beyond the neck
Papillary cells resemble finger-like projections
Tumor development can be related to radiation exposure
Follicular Thyroid Cancer1-4
Makes up about 10% to15% of all thyroid cancers
Often diagnosed between the ages of 40 and 60
Females are affected 3 times more often than males
Cancer cells may invade blood vessels and travel to other body parts such as bone or lung tissues (hematogenous spreading)
Follicular cells are sphere-shaped
Can be more aggressive in older patients
Medullary Thyroid Cancer1-4
Makes up about 5 % to 10% of all thyroid cancers
More likely to run in families and associated with other endocrine disorders
Develops from the C Cells or parafolicullar cells that produce calcitonin (regulates calcium and phosphate blood levels and promotes bone growth)
An elevated calcitonin level can indicate cancer
Often diagnosed between the ages of 40 and 50
Females and males are equally affected
Forms of medullary thyroid cancer include sporadic (not inherited), MEN 2A and MEN 2B (multiple endocrine neoplasia, genetic syndromes that involve other parts of the endocrine system), and familial (genetic, but not linked to other MEN-related endocrine tumors)
Anaplastic Thyroid Cancer1-4
Very rare—affects fewer than 5% of thyroid cancer patients
Usually occurs in patients older than 65 years
Females are affected more often than males
Aggressive and invasive
Least responsive to treatment
Anaplastic (anaplasia) means the cells lose normal structure and organization
References 1. National Cancer Institute. SEER Stat Fact Sheet: Thyroid Cancer. Available at: http://seer.cancer.gov/statfacts/html/thyro.html. Accessed October 28,
2013. 2. Thyroid Cancer page. National Cancer Institute, Web site. Available at: http://www.cancer.gov/cancertopics/types/thyroid. Accessed January 18, 2010. 3. Lal G, O'Dorisio T, McDougall R, Weigel RJ. Cancer of the Endocrine System. In: Abeloff MD, Armitage JO, Niedernuber JE, Kastan MB, McKenna WG,
eds. Abeloff's Clinical Oncology. 4th ed. Philadelphia, PA: Churchill Livingston; 2008. 4. Prinz RA, Chen E. Thyroid Cancer. In: Bope ET, Rakel RE, Kellerman RD, eds. Conn's Current Therapy 2010. Maryland Heights, MO: W. B. Saunders,
Elsevier; 2009.
THYROID_MD4_JIRAPORN_July 2015

Objectives:
Remnant ablation : To ablate thyroid remnant
facilitate detection of recurrent disease and tumor staging
Adjuvant therapy : To destroy suspected, but unproven metastasis
RAI therapy : To treat known persistent disease
I-131 treatment Targeted Therapy
THYROID_MD4_JIRAPORN_July 2015

Primary tumor (T)
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor is found
T1 Tumor size ≤ 2 cm in greatest dimension and is limited to the thyroid
T1a Tumor ≤ 1 cm, limited to the thyroid
T1b Tumor > 1 cm but ≤ 2 cm in greatest dimension, limited to the thyroid
T2 Tumor size > 2 cm but ≤ 4 cm, limited to the thyroid.
T3
Tumor size >4 cm, limited to the thyroid or any tumor with minimal extrathyroidal extension (eg, extension to sternothyroid muscle or perithyroid soft tissues)
T4a
Moderately advanced disease; tumor of any size extending beyond the thyroid capsule to invade subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve
T4b Very advanced disease; tumor invades prevertebral fascia or encases carotid artery or mediastinal vessel
THYROID_MD4_JIRAPORN_July 2015
2010, 7th ed AJCC TNM Classification System for Differentiated Thyroid Carcinoma
Regional lymph nodes (N)
Regional lymph nodes are the central compartment, lateral cervical, and upper mediastinal lymph nodes:
NX Regional nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Regional lymph node metastasis
N1a Metastases to level VI (pretracheal, paratracheal, and prelaryngeal/Delphian lymph nodes)
N1b Metastases to unilateral, bilateral, or contralateral cervical (levels I, II, III, IV, or V) or retropharyngeal or superior mediastinal lymph nodes (level VII)
Distant metastasis (M)
M0 No distant metastasis is found
M1 Distant metastasis is present
http://emedicine.medscape.com/article/2006643-overview Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, et al. AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer-Verlag; 2010.

THYROID_MD4_JIRAPORN_July 2015
Staging of Differentiated Thyroid Carcinoma
Papillary and follicular thyroid cancer (age < 45y):
Stage T N M
I Any T Any N M0
II Any T Any N M1
Papillary and follicular; differentiated (age ≥ 45y):
Stage T N M
I T1 N0 M0
II T2 N0 M0
III T3 N0 M0
IVA T1-3 N1a M0
T4a N1b M0
IVB T4b Any N M0
IVC Any T Any N M1

Table 1. ATA Strata for Recurrence Risk11
Risk Stratum Characteristics Risk for PD or recurrence (Tuttle RM 2010)
Low
•No local or distant metastases •All macroscopic tumor has been resected •No tumor invasion of locoregional tissues or structures •No aggressive histology (e.g., tall cell, insular, columnar cell carcinoma) or vascular invasion •If 131I is given, there is no uptake outside the thyroid bed on the first RxWBS
3 %
Intermediate
•Microscopic invasion of tumor into the perithyroidal soft tissues at initial surgery •Cervical lymph node metastases or 131I uptake outside the thyroid bed on the RxWBS done after thyroid remnant ablation •Tumor with aggressive histology or vascular invasion
21 %
High
•Macroscopic tumor invasion •Incomplete tumor resection •Distant metastases •Thyroglobulinemia out of proportion to what is seen on the RxWBS
68 %
11. 2009 ATA GUIDELINE http://online.liebertpub.com/doi/full/10.1089/thy.2009.0110 12. Tuttle RM, Tala H, Shah J, Leboeuf R, Ghossein R, Gonen M, Brokhin M, Omry G, Fagin JA, Shaha A. Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid. 2010; 20:1341-1349.
THYROID_MD4_JIRAPORN_July 2015

THYROID_MD4_JIRAPORN_July 2015
Management of DTC
SURGERY
RADIOIODINE Rx
HORMONAL Rx
Long-term Follow-up

Near-total or Total thyroidectomy
Cervical LN dissection for gross nodal enlargement
Lobectomy with isthmectomy: micropapillary CA,
unifocal, low-risk, no CLN metastasis followed by
TSH suppression (Result of treatment ~ Total
thyroidectomy with I-131 ablation)
Management of DTC:Surgery
THYROID_MD4_JIRAPORN_July 2015
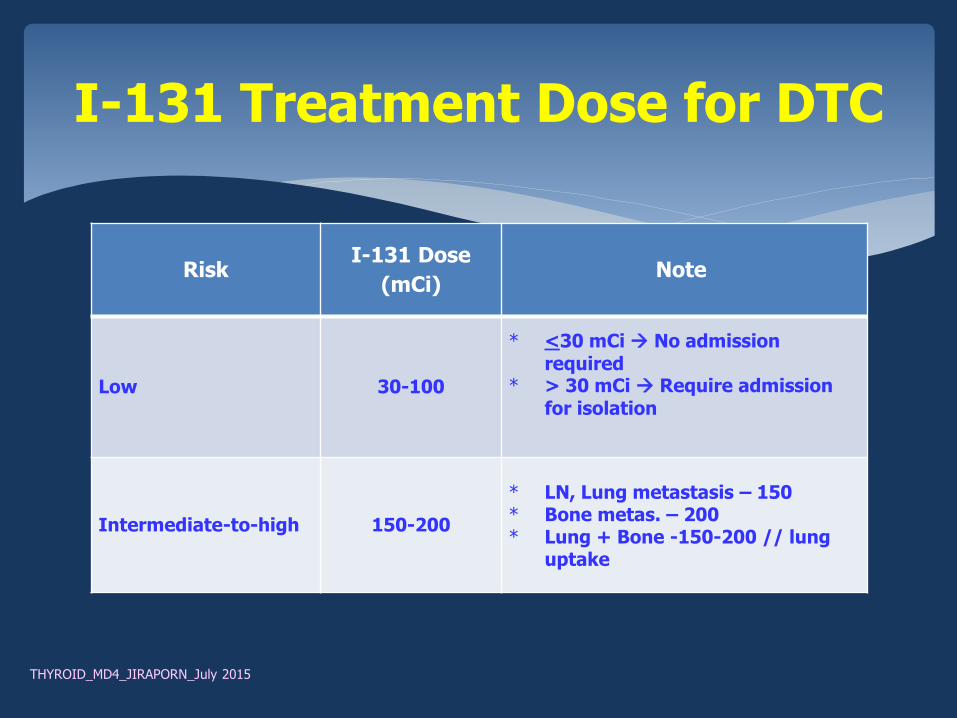
Risk I-131 Dose
(mCi) Note
Low 30-100
* <30 mCi No admission required
* > 30 mCi Require admission for isolation
Intermediate-to-high 150-200
* LN, Lung metastasis – 150 * Bone metas. – 200 * Lung + Bone -150-200 // lung
uptake
I-131 Treatment Dose for DTC
THYROID_MD4_JIRAPORN_July 2015

1. Surgery, Not start thyroid hormone
2. Patho = DTC, planned for RAI Rx
3. 1-2 weeks: Tc-99m thyroid scan & 24-hr I-131 uptake to assess residual thyroid remnant
4. PO 4 weeks wo thyroid hormone medication, TSH > 30 mU/L : RAI Rx
5. Follow up with T4 (FT4), TSH, Tg, & TgAb, Tot calcium; CXR U/S, CT, PET/CT (as necessary)
6. Diagnostic TBS at 6-12 months after RAI Rx to see Rx response.
7. If DxTBS +ve another RAI Rx
Steps of Management of DTC
Tg = Tumor marker of DTC. Tg is most reliable when the Pt had total thyroidectomy followed by I-131 ablation. (no thyroid remnant) & no TgAb

Patient preparation: withdraw thyroxine for 4 weeks before RAI Rx
Low iodine-containing diet intake for 1-2 Wks.
Admission for patient isolation for 2-3 days.
On admission, prepare sour candies or fruits, etc to reduce I-131 retention in the salivary glands to reduce radiation
sialoadenitis.
Encourage water intake & frequent voiding after Rx esp. in the first few days to reduce radiation to bladder wall.
Laxatives in case with constipation to reduce radiation to
the bowel wall.
Avoid radioactivity contamination to the body and the room
RAI Treatment Procedure for DTC:
THYROID_MD4_JIRAPORN_July 2015

Thyroid Cancer with Lung Metastasis
PTC s/p total thyroidectomy
I-131 TBS (5 mCi): Thyroid remnant
& bilateral lung metastases
Tg = 65 ng/ml
CXR: Negative
Rx: RAI 150 mCi
THYROID_MD4_JIRAPORN_July 2015

Thyroid Cancer with Lung Metas. After one session of RAI treatment
ANT POST ANT POST
THYROID_MD4_JIRAPORN_July 2015

Negative physical examination
Negative DxTBS
Low stimulated Tg level, < 2
Negative neck U/S
Remission Criteria
THYROID_MD4_JIRAPORN_July 2015

Status/ TSH level (mIU/L)
Not Remission Remission
Low risk DTC 0.1-0.5 0.3-2
Non-low risk DTC < 0.1 0.1-0.5
Level of TSH recommended
NR: Thyroid hormone Rx = Suppressive dose Reference range of TSH : 0.27-4.20 mIU/L
THYROID_MD4_JIRAPORN_July 2015

Complications of RAI Treatment for DTC
Early complications
Acute radiation sickness: nausea/vomiting
Radiation thyroiditis
Acute sialoadenitis
Pain, hemorrhage & swelling in the metastases
Transient BM suppression
Late complications
Pulmonary fibrosis
Permanent BM suppression
Secondary primary malignancies: bone, GI cancer, colorectal, and salivary gland cancers, (// high accumulation dose) and leukemia.
Impaired male fertility [18832945] THYROID_MD4_JIRAPORN_July 2015
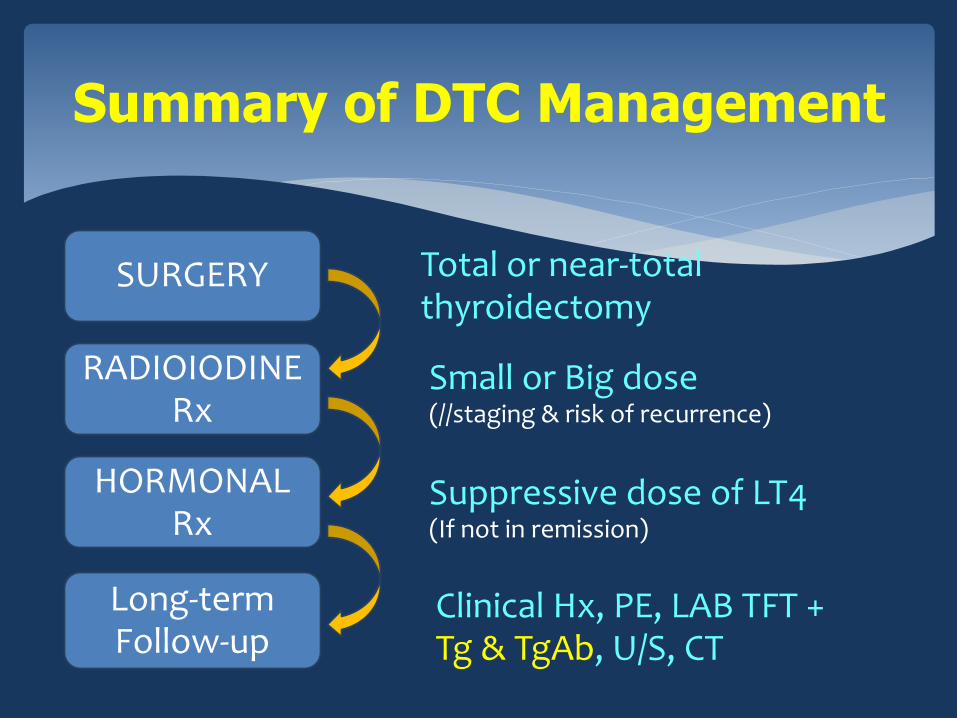
Summary of DTC Management
Total or near-total thyroidectomy
Suppressive dose of LT4 (If not in remission)
Small or Big dose (//staging & risk of recurrence)
Clinical Hx, PE, LAB TFT + Tg & TgAb, U/S, CT
SURGERY
RADIOIODINE Rx
HORMONAL Rx
Long-term Follow-up