radiotherapy awareness event
TRANSCRIPT

Radiotherapy
Weston Park Hospital
Helen Simpson
Trainee Consultant Radiographer
Oct 2019

What is Radiotherapy
Radiotherapy is the use of x-rays and electro-magnetic radiation to treat disease.
Major modality in the management of cancer alongside surgery and
chemotherapy 40% of cured patients have received RT as part of treatment At WPH 4000 new patients treated 6500 patient attendances Energy much higher than when used to diagnose illness
Diagnostic – up to 150 kV Radiotherapy – up to 10 mV

The Origins of Radiotherapy
X-rays were discovered by Roentgen in 1895
The development of the x-ray tube rapidly led to clinical applications, first as a diagnostic tool and later for therapy

The Origins of Radiotherapy
In 1898 Marie and Pierre Curie discovered Radium and Polonium
This resulted in the use of radioactive materials for cancer treatment

First Radiotherapy Treatment
Emil Grubbe 1875 – 1960 First to use X-rays for treatment of Cancer 1896 Treated patient with recurrent carcinoma of
the Breast Due to radiation exposure himself had 90 operations to remove cancers

Radiotherapy: then and now
Late 1940’s 2018
We can use radiotherapy with the aim to:
Cure the cancer (radical radiotherapy)
Reduce Risk of recurrence (Adjuvant)
Control symptoms caused by the cancer to improve quality of life (palliative radiotherapy)
Aim of Radiotherapy
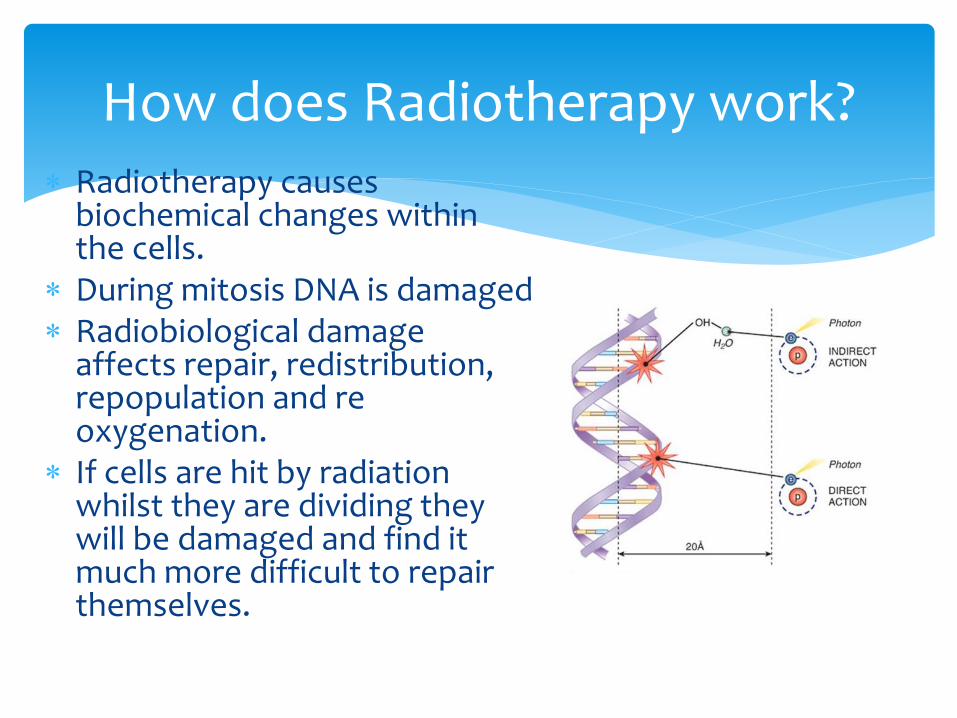
How does Radiotherapy work? Radiotherapy causes
biochemical changes within the cells.
During mitosis DNA is damaged Radiobiological damage
affects repair, redistribution, repopulation and re oxygenation.
If cells are hit by radiation whilst they are dividing they will be damaged and find it much more difficult to repair themselves.

How does Radiotherapy work?
Cancer cells multiply and divide much more quickly than normal cells
Normal cells in the treatment area are also affected by the x-rays but they recover quickly
Deliver enough radiation to kill the cancer cells whilst allowing normal cells to repair themselves


Breast Radiotherapy

Radiotherapy is a standard treatment option for most women following WLE with invasive breast cancer Post-mastectomy radiotherapy is given to node-positive (macro metastases) invasive breast cancer or involved resection margins. Radiotherapy is also given for intermediate and high grade DCIS ( Ductal Carcinoma in Situ). Adjuvant – kills residual microscopic disease after surgery and/or chemotherapy to reduce the risk of local regional recurrences. Nodal Radiotherapy – 4 or more positive lymph nodes or 1-3 with poor prognostic factors Radiotherapy after neo- adjuvant chemotherapy and surgery
Breast Radiotherapy

Localisation
Radiotherapy planning scan in the treatment position
CT scanner provides cross sectional image slices to enable visualisation of the target area to be irradiated – size shape volume
Patient marking - tattooing
Different to a diagnostic scanner – larger aperture couch top identical to treatment units
Radiotherapy Planning
Radiotherapy Scanner

Essential for accurate reproducibility
Usually 3 max
Permanent
Tattooing

Pre- treatment pathway
CT scan appointment
Consented for RT
Dr approves fields
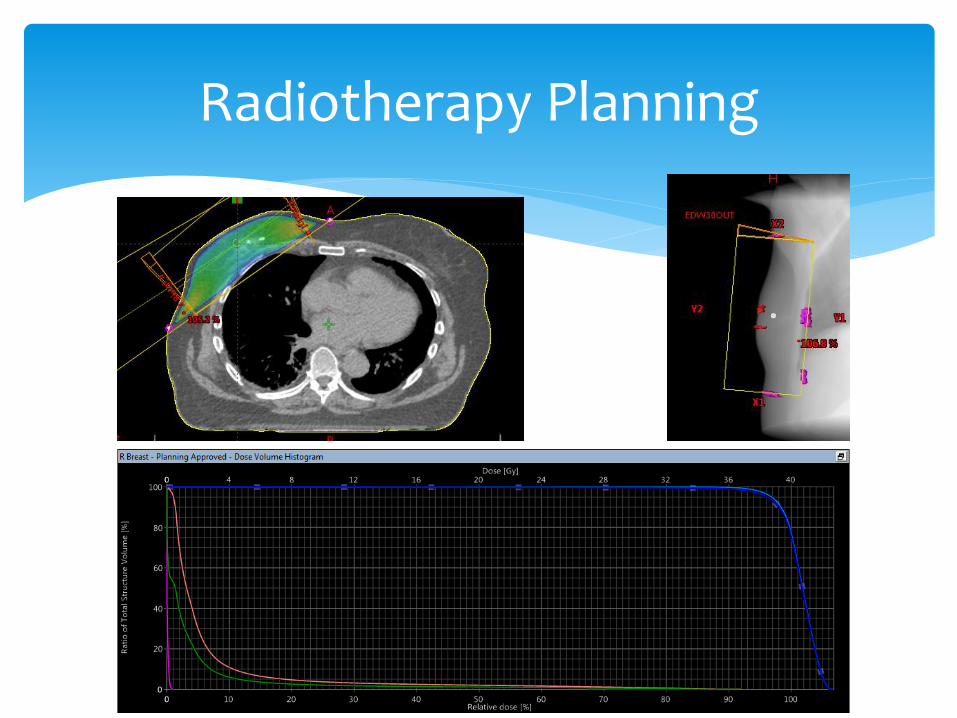
placement outlines PTV & organs at risk
A computerised plan produced
represents dose distribution through the
volume
Plan checked by physicists &
Doctor prescribes dose
Treatment inputted and prepared on
computer system
Radiotherapy begins
Radiographers place radiation
fields on CT
From CT scan to treatment
takes 7-10days

Radiotherapy Planning
Radiotherapy Planning

External beam Radiotherapy
Treatment machines are called Linear Accelerators
High energy x-rays
6-10 Mv

Breast Radiotherapy Treatment
Tangents – glancing fields

Daily treatment
Monday to Friday
15 daily treatments to the breast tissue +/- nodes
If having a boost to the tumour bed additional 8 treatments
Usually treated on same linear accelerator
Team of 4 Radiographers
Do not feel anything, see anything

Deep Inspiration Breath hold
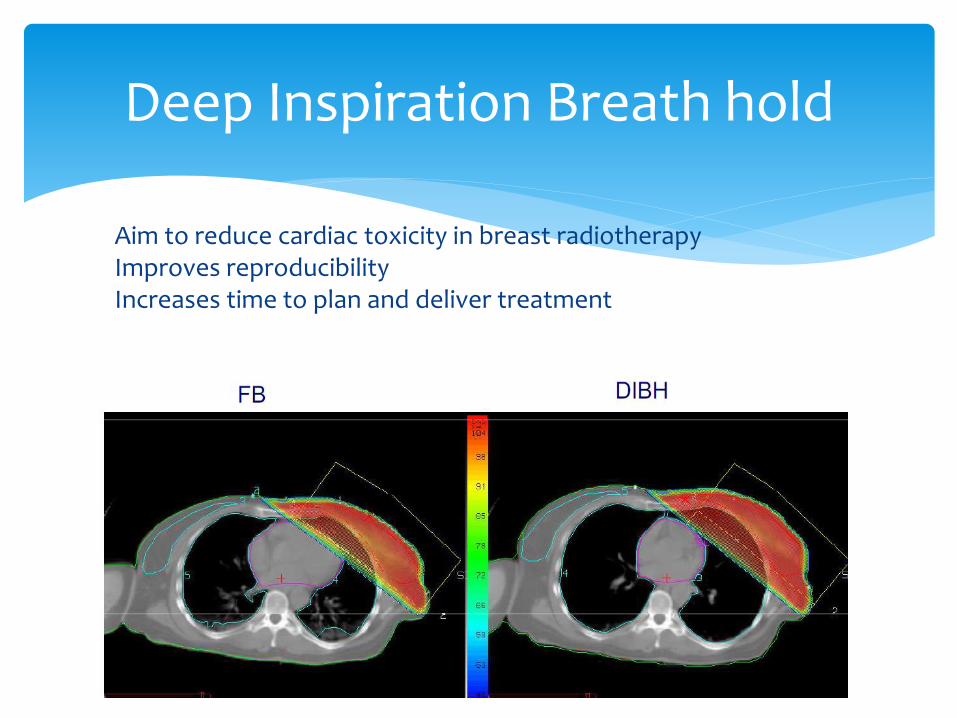
Deep Inspiration Breath hold
Aim to reduce cardiac toxicity in breast radiotherapy Improves reproducibility Increases time to plan and deliver treatment
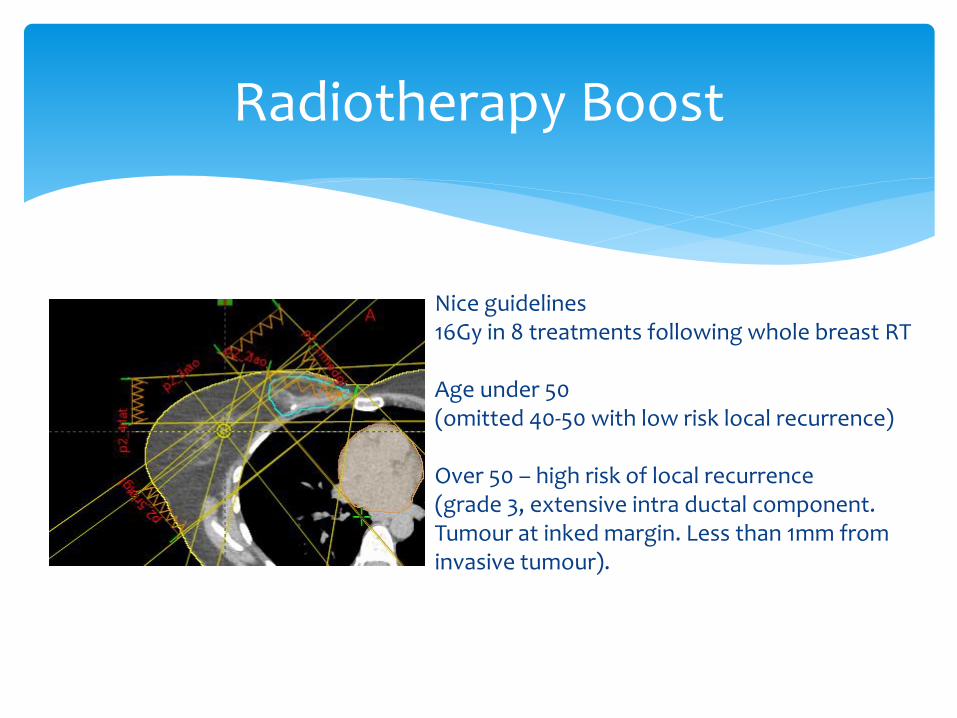
Radiotherapy Boost
Nice guidelines 16Gy in 8 treatments following whole breast RT Age under 50 (omitted 40-50 with low risk local recurrence) Over 50 – high risk of local recurrence (grade 3, extensive intra ductal component. Tumour at inked margin. Less than 1mm from invasive tumour).

Radiotherapy Boost

Implants

Seroma’s
Affect the external contour of the patient Dose implications Delay to start radiotherapy Implications of repeated drainage
Radiotherapy to Nodes
Supraclavicular Fossa 4 or more involved axillary lymph nodes 1 to 3 positive lymph nodes if other poor prognostic factors (for example, T3 and/or grade 3) and good performance status Axilla/SCF As an alternative to Axillary Node Dissection (AND) after positive Sentinel Node Biopsy (not for micro metastasis) Not routinely after AND, unless high risk of axillary recurrence Internal Mammary Chain Involved internal mammary node Consider in high risk node-positive (macro metastases) T4 N2-3 N1 with medial/central location

Radiotherapy to Nodes

Intensity Modulated Radiotherapy
Conform (shape) the beam around the treatment area using Multileaf Collimators (MLCs).
IMRT

IGRT(Image guided radiotherapy)
Modern Radiotherapy Linear Accelerators have integral imaging facilities that allow us to image the patients ‘real time’ whilst they are in the treatment position and before we deliver any treatment. At the treatment console we can compare the planning images directly with those captured by the LA to optimise treatment accuracy.

Side effects of Radiotherapy Skin reaction – Radiation Dermatitis. Only in area treated – 10-14days after first exposure (the time
it takes for the damage to the basal layer of the skin to migrate to the skin surface).
Activation of the inflammatory response Dependent on area treated Build up as treatment progresses peak reaction 7-10
days after treatment finishes (time taken for basal cells damaged to reach the skin surface)
erythema Dry/ moist desquamation – when basal layer
can’t produce enough new cells Hair loss if any in treated area fatigue
Breast reactions
Non perfumed moisturising cream e.g. E45, diprobase, aveeno, aloe vera – from before radiotherapy begins.
1% hydrocortisone cream - to itchy skin BD
Flamazine / intrasite gel – moist desquamation
Medication for Side effects

Toxicity
Acute Radiation Toxicity – Rarely life threatening Rapidly proliferating tissues Reversible Dose limiting in some contexts
Late Radiation Toxicity - Can be severe but well understood due to long history Slow/ non-proliferating tissues Irreversible Nearly always dose limiting
Factors affecting Skin effects
Intrinsic factors Age – older skin slower epidermal cycle Nutrition - undernourished Smoking/Alcohol – decrease capillary blood flow impairs healing Co-morbidities – diabetes and steroids UV exposure/ ethnic origin – BME patient Obesity – extra skin folds Infection – bacterial or fungal can slow healing
Extrinsic factors Radiotherapy – dose, size, bolus Energy of radiotherapy – higher doses less damage (skin sparing effect) Radio sensitises - some chemotherapy cisplatin, 5-Fu Chemical / thermal / mechanical – metal in creams, irritants, extremes of temperature hot water bottles , ice packs, clothes that rub.

Long terms side effects
Skin pigmentation changes within the treated area Telangiectasia – thread veins Breast oedema Breast shrinkage Nodal areas Arm lymphoedema Shoulder stiffness Rare Lung fibrosis Rib fractures Cardiac damage Second cancer Implants – capsule formation, rupture, fat necrosis.

Evidence for future practice in radiotherapy and influence cancer treatment regimes
Improves patient choice
Improving survival and quality of life of our patients
Changes in practice- we are where we are today due to previous research
Radiotherapy Research Why is it important?

Radiotherapy Research
WPH completed the feasibility study 2019 – next will be multi centre study

Future Breast Radiotherapy

Radiotherapy Team
Consultant Clinical Oncologists Consultant Radiographer ACP Specialist Radiographer Radiographers Planning Technicians Physicists Information and support Radiographers

Radiotherapy open evenings- monthly
Information booklets
Photo books in DGH’s
Open evenings for all health care professionals
Radiotherapy awareness events
Initiatives to Improve the Radiotherapy Journey
Information and Support during Radiotherapy
On treatment review
All patients monitored on a daily basis by Radiographers on treatment machine
All patients having 5 or more treatments are reviewed weekly.
Review can be by member of the medical team or by specially trained radiographers- ACP.
Radiographers can give certain medication under a PGD, or as independent prescribers.

Thank you