radium -223 treatment of bone metastases in metastatic...
TRANSCRIPT
Radium-223 Treatment of Bone Metastases in Metastatic
Radium-223 Treatment of Bone Metastases in Metastatic
Castration-Resistant Prostate Cancer (mCRPC)
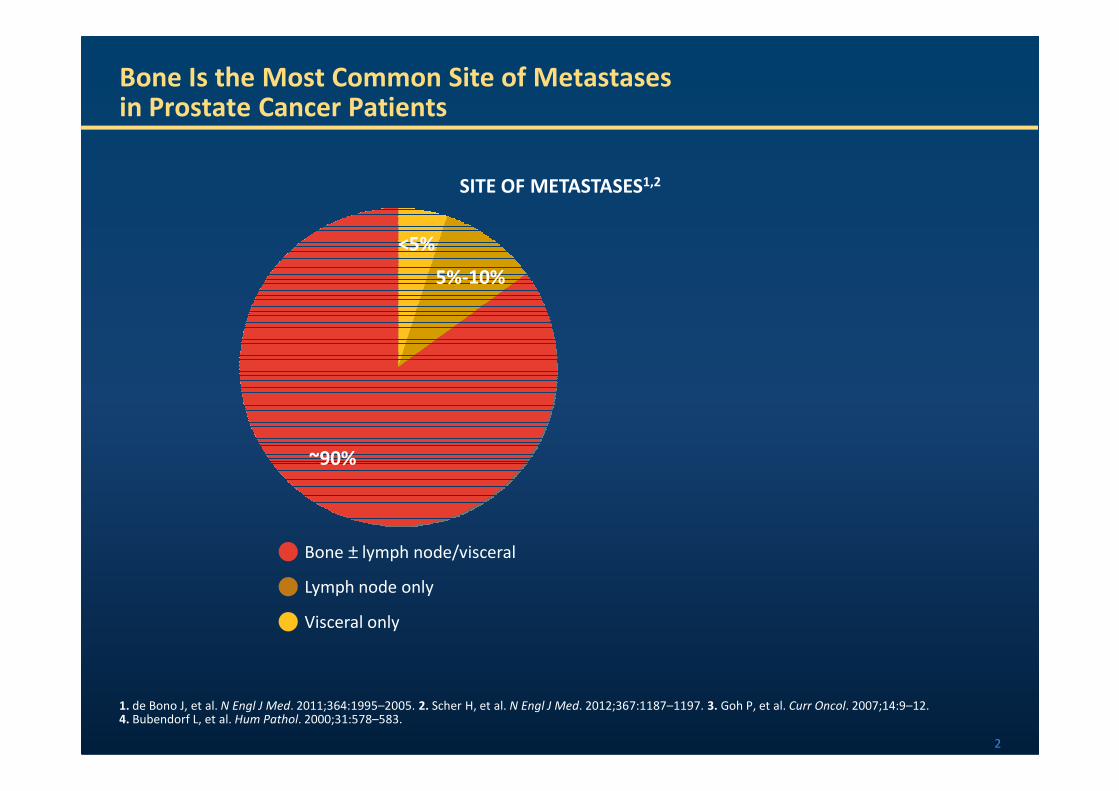
Bone Is the Most Common Site of Metastasesin Prostate Cancer Patients
SITE OF METASTASES1,2
<5%
5%-10%
2
1. de Bono J, et al. N Engl J Med. 2011;364:1995–2005. 2. Scher H, et al. N Engl J Med. 2012;367:1187–1197. 3. Goh P, et al. Curr Oncol. 2007;14:9–12.4. Bubendorf L, et al. Hum Pathol. 2000;31:578–583.
~90%
Bone ± lymph node/visceral
Lymph node only
Visceral only
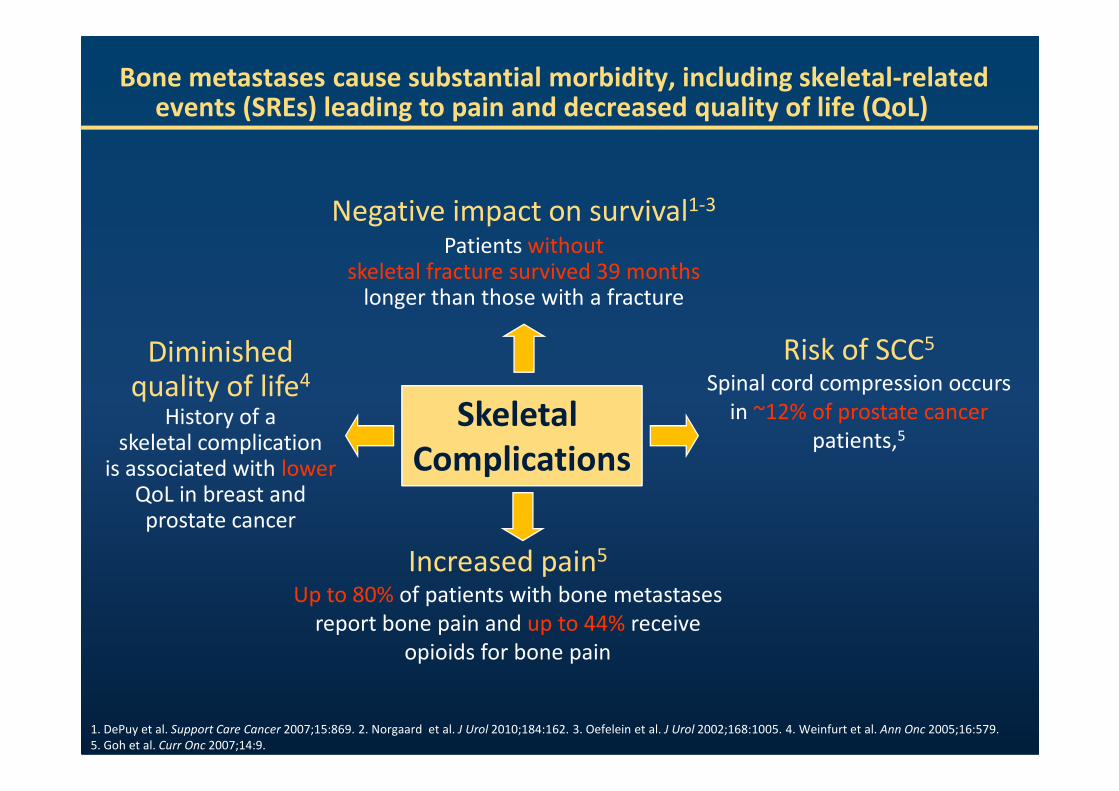
Bone metastases cause substantial morbidity, including skeletal-related events (SREs) leading to pain and decreased quality of life (QoL)
Skeletal
Negative impact on survival1-3
Patients withoutskeletal fracture survived 39 months
longer than those with a fracture
Risk of SCC5
Spinal cord compression occurs
Diminished quality of life4
Skeletal
Complications
Increased pain5
Up to 80% of patients with bone metastases
report bone pain and up to 44% receive
opioids for bone pain
Spinal cord compression occurs
in ~12% of prostate cancer
patients,5
quality of lifeHistory of a
skeletal complication is associated with lower
QoL in breast and prostate cancer
1. DePuy et al. Support Care Cancer 2007;15:869. 2. Norgaard et al. J Urol 2010;184:162. 3. Oefelein et al. J Urol 2002;168:1005. 4. Weinfurt et al. Ann Onc 2005;16:579.
5. Goh et al. Curr Onc 2007;14:9.
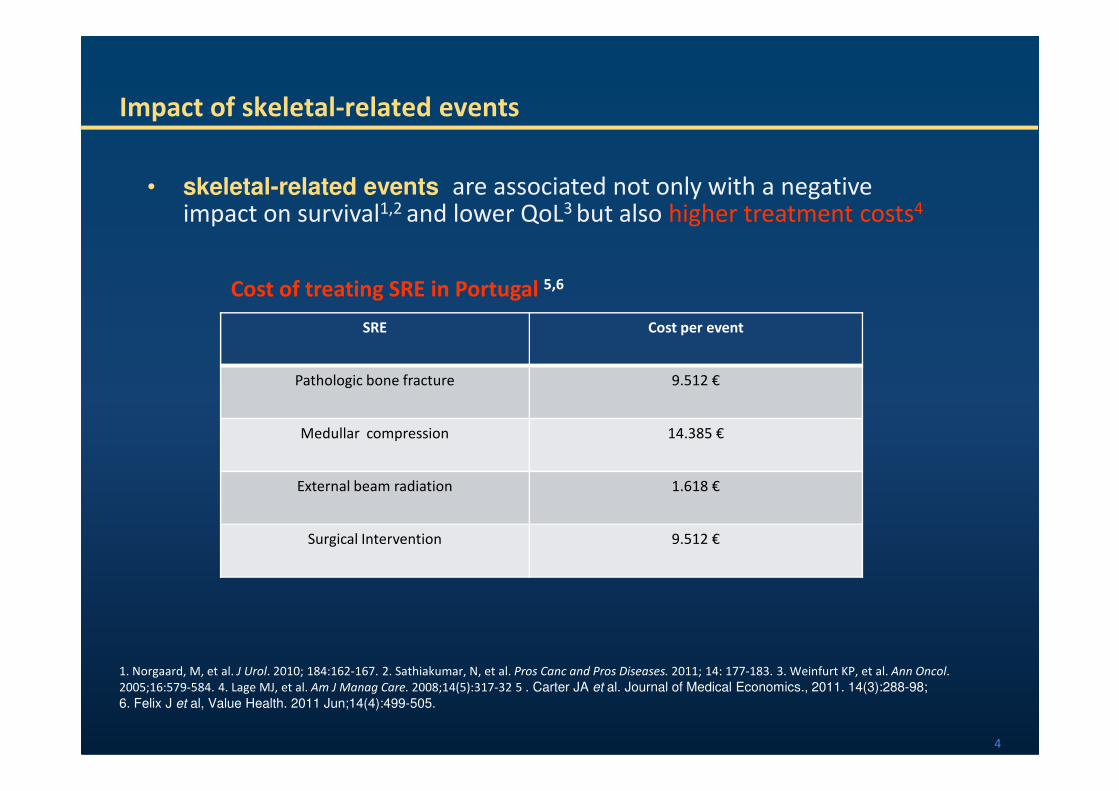
Impact of skeletal-related events
SRE Cost per event
Pathologic bone fracture 9.512 €
• skeletal-related events are associated not only with a negative impact on survival1,2 and lower QoL3 but also higher treatment costs4
Cost of treating SRE in Portugal 5,6
4
1. Norgaard, M, et al. J Urol. 2010; 184:162-167. 2. Sathiakumar, N, et al. Pros Canc and Pros Diseases. 2011; 14: 177-183. 3. Weinfurt KP, et al. Ann Oncol.
2005;16:579-584. 4. Lage MJ, et al. Am J Manag Care. 2008;14(5):317-32 5 . Carter JA et al. Journal of Medical Economics., 2011. 14(3):288-98;
6. Felix J et al, Value Health. 2011 Jun;14(4):499-505.
Medullar compression 14.385 €
External beam radiation 1.618 €
Surgical Intervention 9.512 €

Radium-223 Mechanism of Action
CaCaCa
• Radium and calcium have the same divalent charge
Agency for Toxic Substances and Disease Registry, US Public Health Service. Toxicological profile for radium. (December 1990).
http://www.atsdr.cdc.gov/toxprofiles/tp144.pdf. Accessed March 7, 2014.
RaRaRa
Radium-223Calcium
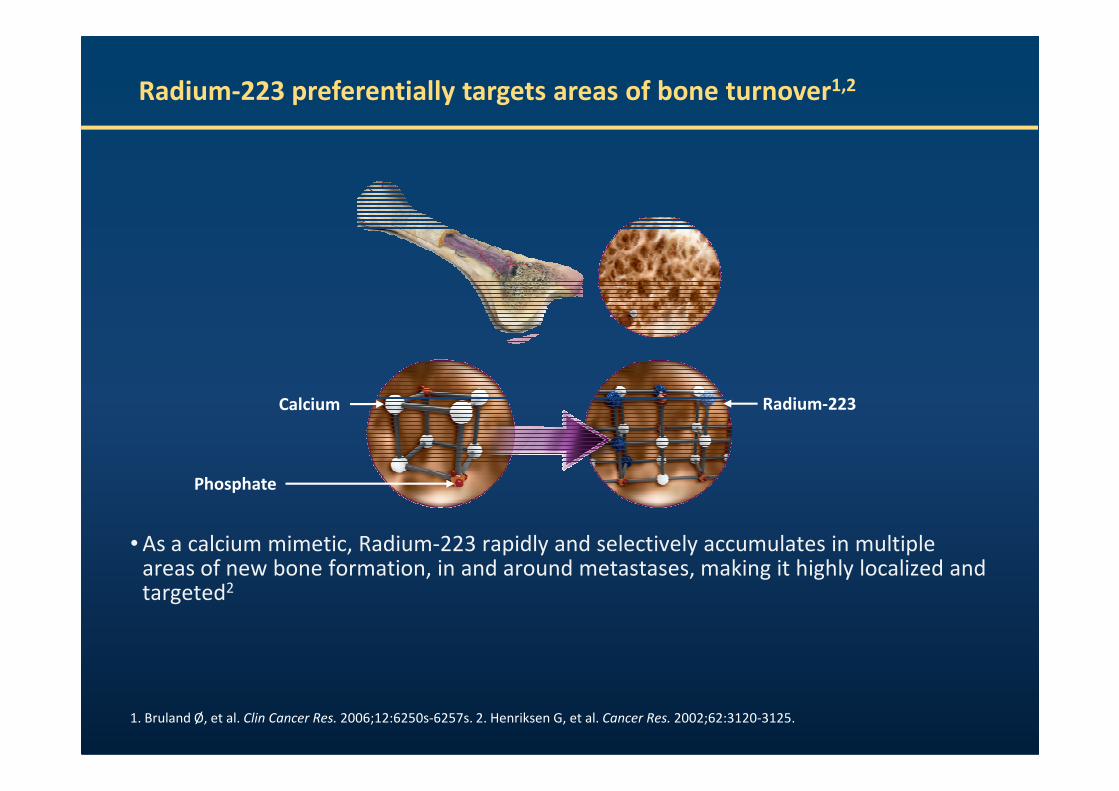
Radium-223 preferentially targets areas of bone turnover1,2
• As a calcium mimetic, Radium-223 rapidly and selectively accumulates in multiple areas of new bone formation, in and around metastases, making it highly localized and targeted2
Radium-223
Phosphate
Calcium
1. Bruland Ø, et al. Clin Cancer Res. 2006;12:6250s-6257s. 2. Henriksen G, et al. Cancer Res. 2002;62:3120-3125.
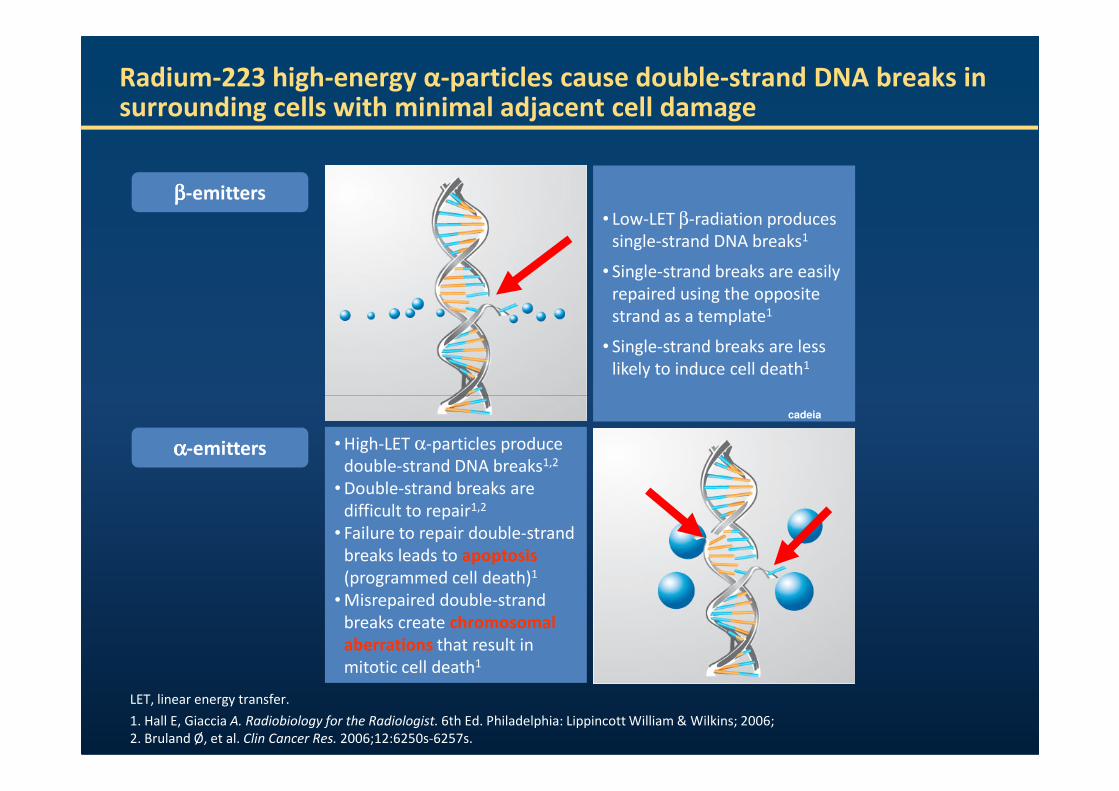
Radium-223 high-energy α-particles cause double-strand DNA breaks in surrounding cells with minimal adjacent cell damage
ββββ-emitters
• Low-LET β-radiation produces
single-strand DNA breaks1
• Single-strand breaks are easily
repaired using the opposite
strand as a template1
• Single-strand breaks are less
likely to induce cell death1
αααα-emitters • High-LET α-particles produce
double-strand DNA breaks1,2
• Double-strand breaks are
difficult to repair1,2
• Failure to repair double-strand
breaks leads to apoptosis
(programmed cell death)1
• Misrepaired double-strand
breaks create chromosomal
aberrations that result in
mitotic cell death1
LET, linear energy transfer.
1. Hall E, Giaccia A. Radiobiology for the Radiologist. 6th Ed. Philadelphia: Lippincott William & Wilkins; 2006;
2. Bruland Ø, et al. Clin Cancer Res. 2006;12:6250s-6257s.
cadeia
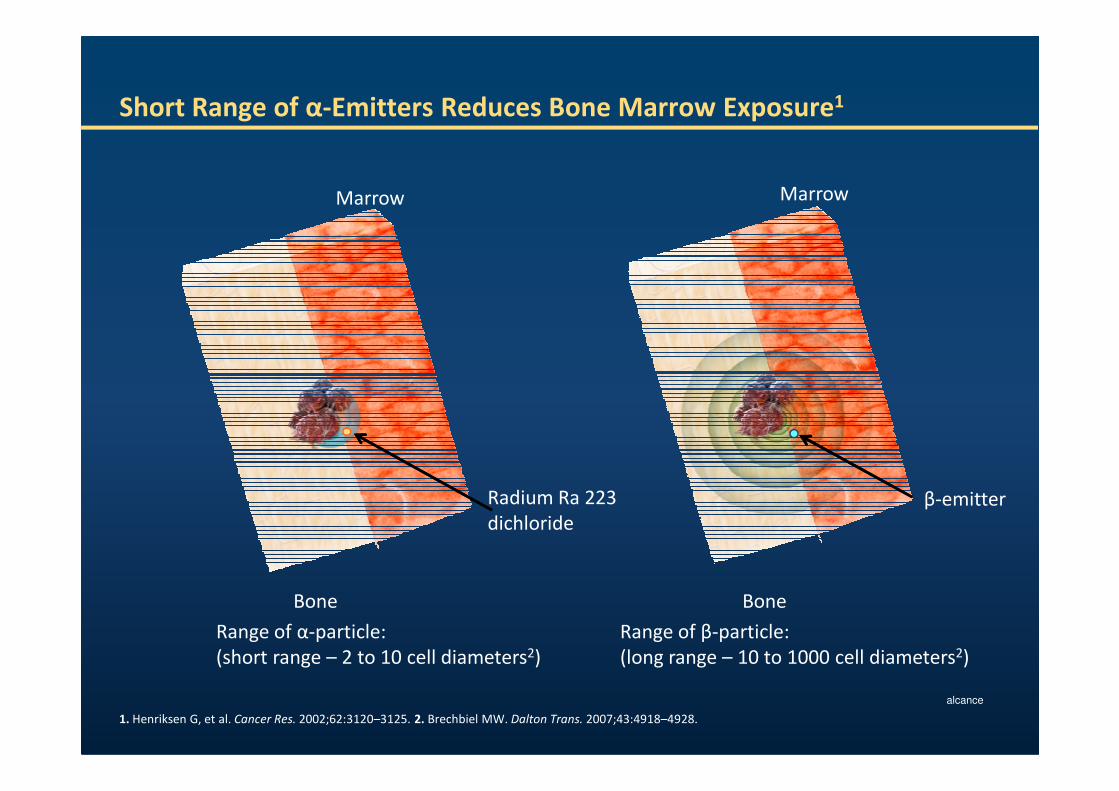
Short Range of α-Emitters Reduces Bone Marrow Exposure1
Marrow Marrow
Bone
Range of α-particle:
(short range – 2 to 10 cell diameters2)
Radium Ra 223
dichloride
Range of β-particle:
(long range – 10 to 1000 cell diameters2)
Bone
β-emitter
1. Henriksen G, et al. Cancer Res. 2002;62:3120–3125. 2. Brechbiel MW. Dalton Trans. 2007;43:4918–4928.
alcance
BiodistributionRadium-223 is rapidly eliminated from the blood and rapidly accumulates in bone
• More than 75% of the activity had left the blood at 15 minutes after injection1
• Radioactivity 4 hours after injection1
– 61% in bone
– 49% in small intestine
– 4% in blood (decreasing to less than 1% at 72 hours)
• Excreted by the small intestine, primarily in feces1
– ~63% of administered radioactivity excreted from the body in ≤7 days
1-Lewington V, et al. Presented at ASCO GU2010. Abstract 216; 2- Xofigo® (radium Ra 223 dichloride) solution for injection Summary of Product
Characteristics (SmPC). Berlin, Germany: Bayer Pharma AG; 2013.
– ~63% of administered radioactivity excreted from the body in ≤7 days
• No dose adjustment is considered necessary in patients with hepatic or renal impairment2
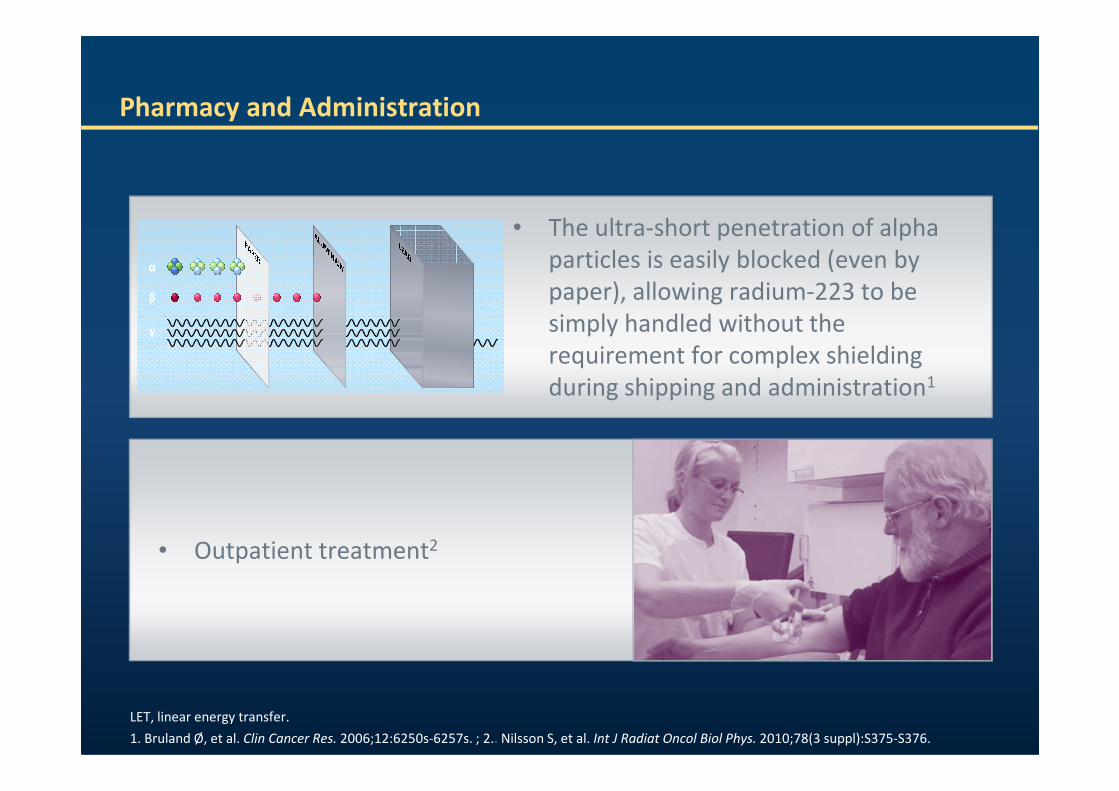
Pharmacy and Administration
• The ultra-short penetration of alpha
particles is easily blocked (even by
paper), allowing radium-223 to be
simply handled without the
requirement for complex shielding
during shipping and administration1
γ
β
α
γ
β
α
LET, linear energy transfer.
1. Bruland Ø, et al. Clin Cancer Res. 2006;12:6250s-6257s. ; 2.. Nilsson S, et al. Int J Radiat Oncol Biol Phys. 2010;78(3 suppl):S375-S376.
during shipping and administration
• Outpatient treatment2
ALSYMPCA STUDY DESIGN

ALSYMPCA: Study Design
(50 kBq/kg IV)
6 injections at 4-week intervals+ best standard of careb
(50 kBq/kg IV)
6 injections at 4-week intervals+ best standard of careb
Placebo (saline)Placebo (saline)
PATIENTS (N=921)
•Confirmed symptomatic CRPC
•≥2 bone metastases
•No known visceral metastases
•Post-docetaxel, unfit for docetaxel, or refused docetaxela
STRATIFICATION
•Total ALP: <220 U/L vs ≥220 U/L
RR 2:1
12
ALP, alkaline phosphatase; ALSYMPCA, ALpharadin in SYMptomatic Prostate CAncer; CRPC, castration-resistant prostate cancer.
a. Unfit for docetaxel includes patients who were ineligible for docetaxel, refused docetaxel, or lived where docetaxel was unavailable.b.Best standard of care defined as a routine standard of care at each center, e.g., local external beam radiation therapy, corticosteroids,
antiandrogens, estrogens (e.g., stilbestrol), estramustine, or ketoconazole.
SOURCE: Parker C, et al. N Engl J Med. 2013;369(3):213–223.
Placebo (saline)6 injections at 4-week intervals
+ best standard of careb
Placebo (saline)6 injections at 4-week intervals
+ best standard of careb
• 136 centers in 19 countries
• Planned follow-up is 3 years
<220 U/L vs ≥220 U/L
•Bisphosphonate use: Yes vs No
•Prior docetaxel: Yes vs No
An updated analysis of efficacy and safety was performed from all 921 enrolled patients when
528 deaths had occurred.
An updated analysis of efficacy and safety was performed from all 921 enrolled patients when
528 deaths had occurred.
> 2 lesões ósseas
No know visceral metástases
Radium-223 Treatment of Bone Metastases in Metastatic Castration-Resistant Prostate Cancer (mCRPC)
Exclusion Criteria
• Chemotherapy in the previous 4 weeks
• Unfavourable condition after chemotherapy
• Previous therapy with Strontium 89 or Sammarium153
• Blood transfusions
• Visceral metastasis
• Spinal cord compression
• (Superscan)
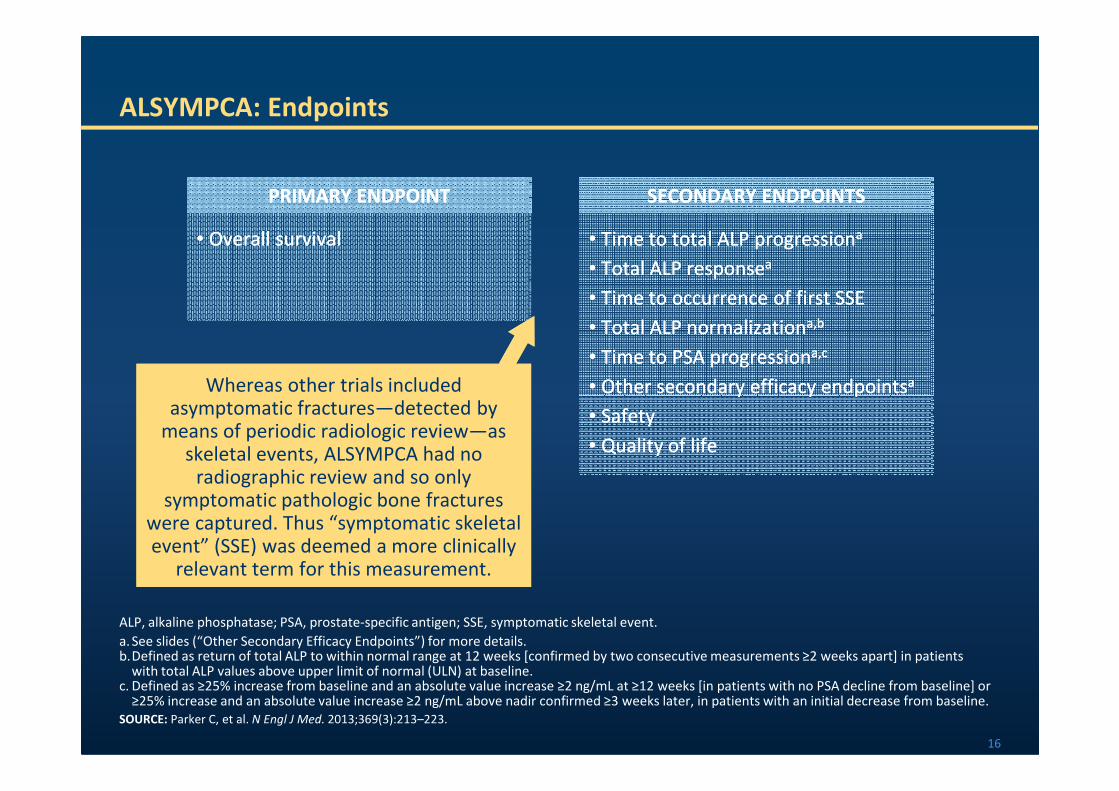
ALSYMPCA: Endpoints
• Overall survival
PRIMARY ENDPOINT
• Overall survival
PRIMARY ENDPOINT
• Time to total ALP progressiona
• Total ALP responsea
• Time to occurrence of first SSE
• Total ALP normalizationa,b
• Time to PSA progressiona,c
• Other secondary efficacy endpointsa
SECONDARY ENDPOINTS
• Time to total ALP progressiona
• Total ALP responsea
• Time to occurrence of first SSE
• Total ALP normalizationa,b
• Time to PSA progressiona,c
• Other secondary efficacy endpointsa
SECONDARY ENDPOINTS
Whereas other trials included asymptomatic fractures—detected by
Whereas other trials included asymptomatic fractures—detected by
16
ALP, alkaline phosphatase; PSA, prostate-specific antigen; SSE, symptomatic skeletal event.
a. See slides (“Other Secondary Efficacy Endpoints”) for more details. b.Defined as return of total ALP to within normal range at 12 weeks [confirmed by two consecutive measurements ≥2 weeks apart] in patients
with total ALP values above upper limit of normal (ULN) at baseline.c. Defined as ≥25% increase from baseline and an absolute value increase ≥2 ng/mL at ≥12 weeks [in patients with no PSA decline from baseline] or
≥25% increase and an absolute value increase ≥2 ng/mL above nadir confirmed ≥3 weeks later, in patients with an initial decrease from baseline.
SOURCE: Parker C, et al. N Engl J Med. 2013;369(3):213–223.
• Other secondary efficacy endpoints
• Safety
• Quality of life
• Other secondary efficacy endpoints
• Safety
• Quality of life
Whereas other trials included asymptomatic fractures—detected by
means of periodic radiologic review—as skeletal events, ALSYMPCA had no
radiographic review and so only symptomatic pathologic bone fractures
were captured. Thus “symptomatic skeletal event” (SSE) was deemed a more clinically
relevant term for this measurement.
Whereas other trials included asymptomatic fractures—detected by
means of periodic radiologic review—as skeletal events, ALSYMPCA had no
radiographic review and so only symptomatic pathologic bone fractures
were captured. Thus “symptomatic skeletal event” (SSE) was deemed a more clinically
relevant term for this measurement.
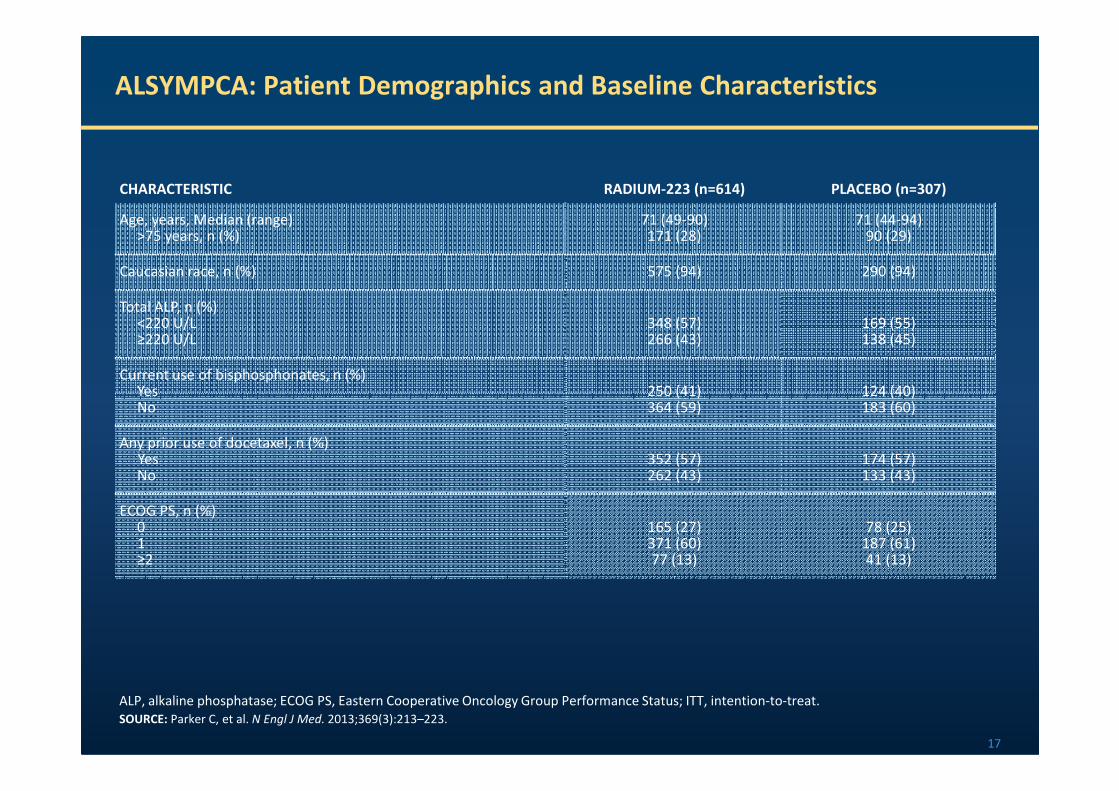
ALSYMPCA: Patient Demographics and Baseline Characteristics
CHARACTERISTIC RADIUM-223 (n=614) PLACEBO (n=307)
Age, years, Median (range)>75 years, n (%)
71 (49-90)171 (28)
71 (44-94)90 (29)
Caucasian race, n (%) 575 (94) 290 (94)
Total ALP, n (%)<220 U/L≥220 U/L
348 (57)266 (43)
169 (55)138 (45)
Current use of bisphosphonates, n (%)Yes 250 (41) 124 (40)
17
ALP, alkaline phosphatase; ECOG PS, Eastern Cooperative Oncology Group Performance Status; ITT, intention-to-treat.
SOURCE: Parker C, et al. N Engl J Med. 2013;369(3):213–223.
YesNo
250 (41)364 (59)
124 (40)183 (60)
Any prior use of docetaxel, n (%)YesNo
352 (57)262 (43)
174 (57)133 (43)
ECOG PS, n (%)01≥2
165 (27)371 (60)77 (13)
78 (25)187 (61)41 (13)
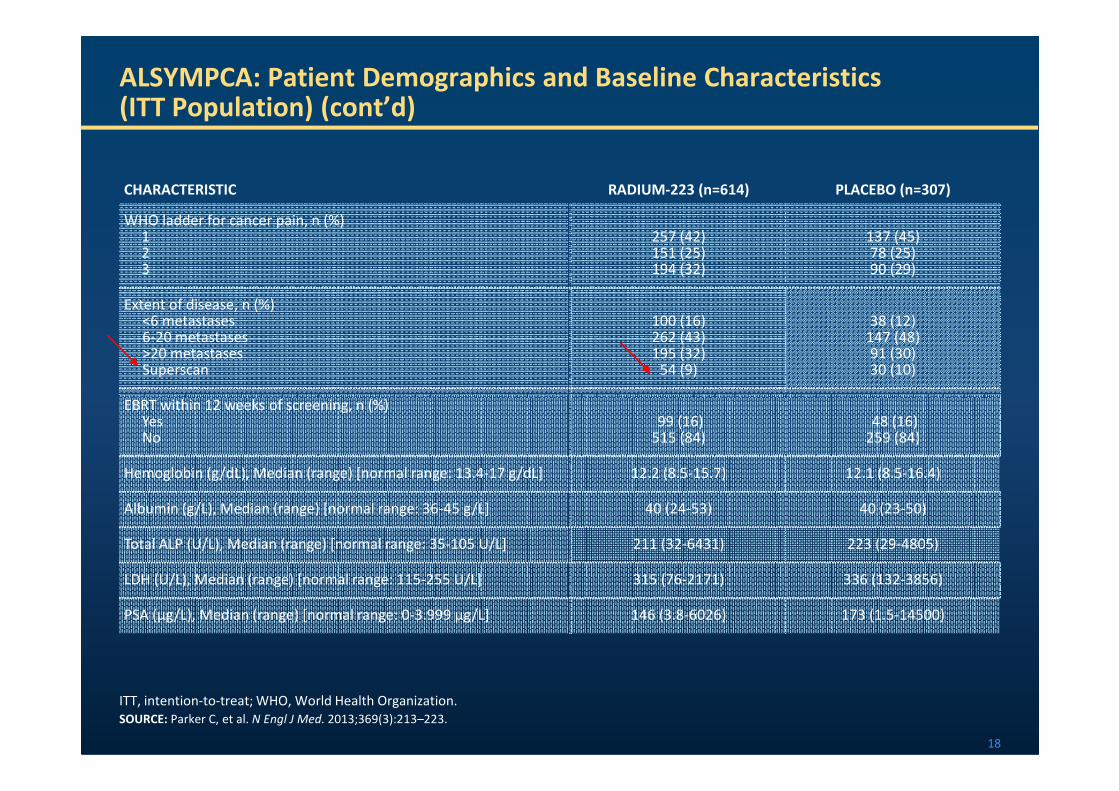
ALSYMPCA: Patient Demographics and Baseline Characteristics(ITT Population) (cont’d)
CHARACTERISTIC RADIUM-223 (n=614) PLACEBO (n=307)
WHO ladder for cancer pain, n (%)123
257 (42)151 (25)194 (32)
137 (45)78 (25)90 (29)
Extent of disease, n (%)<6 metastases6-20 metastases>20 metastasesSuperscan
100 (16)262 (43)195 (32)
54 (9)
38 (12)147 (48)91 (30)30 (10)
EBRT within 12 weeks of screening, n (%)
18
ITT, intention-to-treat; WHO, World Health Organization.
SOURCE: Parker C, et al. N Engl J Med. 2013;369(3):213–223.
EBRT within 12 weeks of screening, n (%)YesNo
99 (16)515 (84)
48 (16)259 (84)
Hemoglobin (g/dL), Median (range) [normal range: 13.4-17 g/dL] 12.2 (8.5-15.7) 12.1 (8.5-16.4)
Albumin (g/L), Median (range) [normal range: 36-45 g/L] 40 (24-53) 40 (23-50)
Total ALP (U/L), Median (range) [normal range: 35-105 U/L] 211 (32-6431) 223 (29-4805)
LDH (U/L), Median (range) [normal range: 115-255 U/L] 315 (76-2171) 336 (132-3856)
PSA (μg/L), Median (range) [normal range: 0-3.999 μg/L] 146 (3.8-6026) 173 (1.5-14500)
ALSYMPCA EFFICACY OUTCOMES
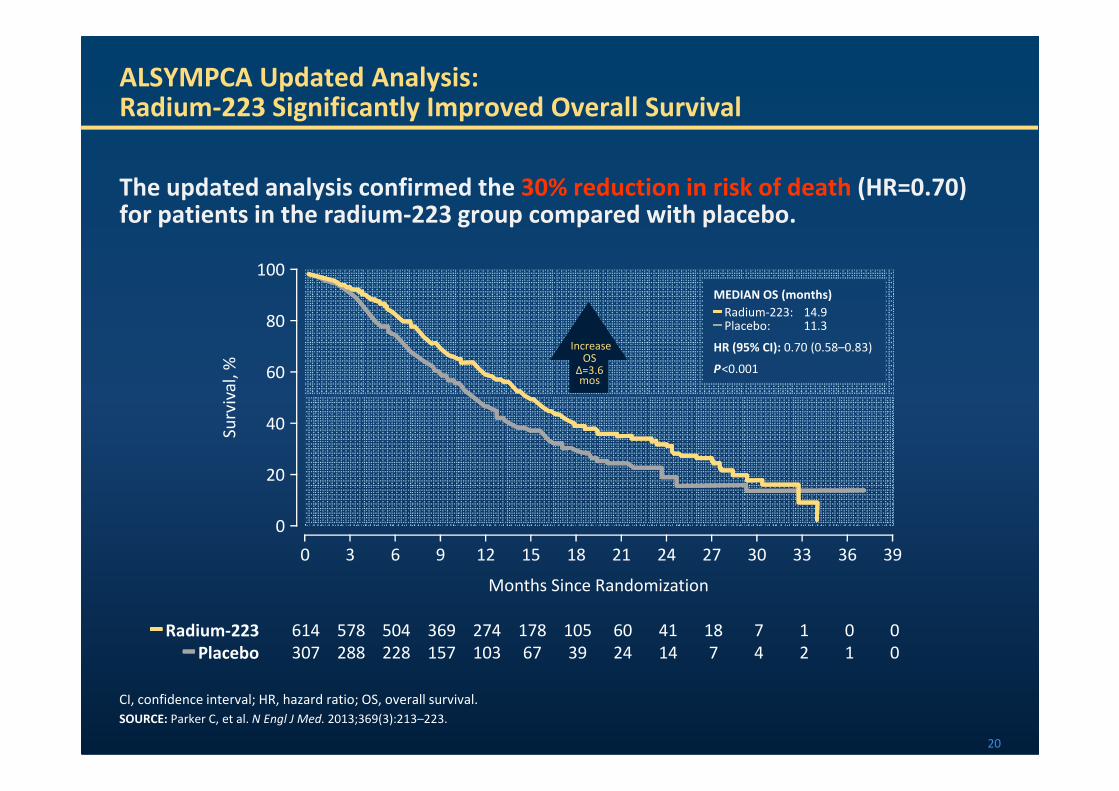
The updated analysis confirmed the 30% reduction in risk of death (HR=0.70) for patients in the radium-223 group compared with placebo.
ALSYMPCA Updated Analysis:Radium-223 Significantly Improved Overall Survival
60
80
100
Su
rviv
al,
%
IncreaseOS
∆=3.6mos
MEDIAN OS (months)━━━━ Radium-223: 14.9━━━━ Placebo: 11.3
HR (95% CI): 0.70 (0.58–0.83)
P<0.001
20
━━━━ Radium-223 614 578 504 369 274 178 105 60 41 18 7 1 0 0
━━━━ Placebo 307 288 228 157 103 67 39 24 14 7 4 2 1 0
CI, confidence interval; HR, hazard ratio; OS, overall survival.
SOURCE: Parker C, et al. N Engl J Med. 2013;369(3):213–223.
20
0
40
Su
rviv
al,
%
Months Since Randomization
0 9 15 24 30 3936332721181263
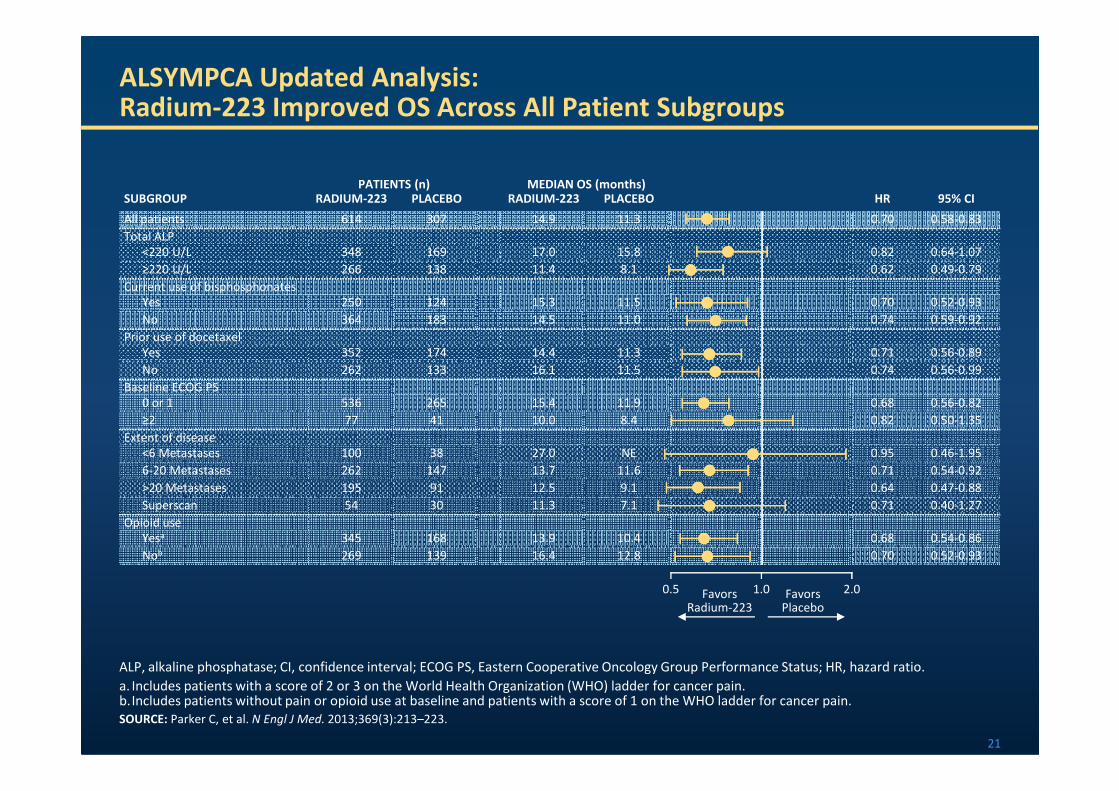
ALSYMPCA Updated Analysis: Radium-223 Improved OS Across All Patient Subgroups
SUBGROUPPATIENTS (n) MEDIAN OS (months)
HR 95% CIRADIUM-223 PLACEBO RADIUM-223 PLACEBO
All patients 614 307 14.9 11.3 0.70 0.58-0.83
Total ALP
<220 U/L 348 169 17.0 15.8 0.82 0.64-1.07
≥220 U/L 266 138 11.4 8.1 0.62 0.49-0.79
Current use of bisphosphonates
Yes 250 124 15.3 11.5 0.70 0.52-0.93
No 364 183 14.5 11.0 0.74 0.59-0.92
Prior use of docetaxel
Yes 352 174 14.4 11.3 0.71 0.56-0.89
No 262 133 16.1 11.5 0.74 0.56-0.99
Baseline ECOG PS
0 or 1 536 265 15.4 11.9 0.68 0.56-0.82
21
0 or 1 536 265 15.4 11.9 0.68 0.56-0.82
≥2 77 41 10.0 8.4 0.82 0.50-1.35
Extent of disease
<6 Metastases 100 38 27.0 NE 0.95 0.46-1.95
6-20 Metastases 262 147 13.7 11.6 0.71 0.54-0.92
>20 Metastases 195 91 12.5 9.1 0.64 0.47-0.88
Superscan 54 30 11.3 7.1 0.71 0.40-1.27
Opioid use
Yesa 345 168 13.9 10.4 0.68 0.54-0.86
Nob 269 139 16.4 12.8 0.70 0.52-0.93
FavorsRadium-223
FavorsPlacebo
ALP, alkaline phosphatase; CI, confidence interval; ECOG PS, Eastern Cooperative Oncology Group Performance Status; HR, hazard ratio.
a. Includes patients with a score of 2 or 3 on the World Health Organization (WHO) ladder for cancer pain. b.Includes patients without pain or opioid use at baseline and patients with a score of 1 on the WHO ladder for cancer pain.
SOURCE: Parker C, et al. N Engl J Med. 2013;369(3):213–223.
0.5 2.01.0
40
60
80
100
Pa
tie
nts
Wit
ho
ut
SS
E,
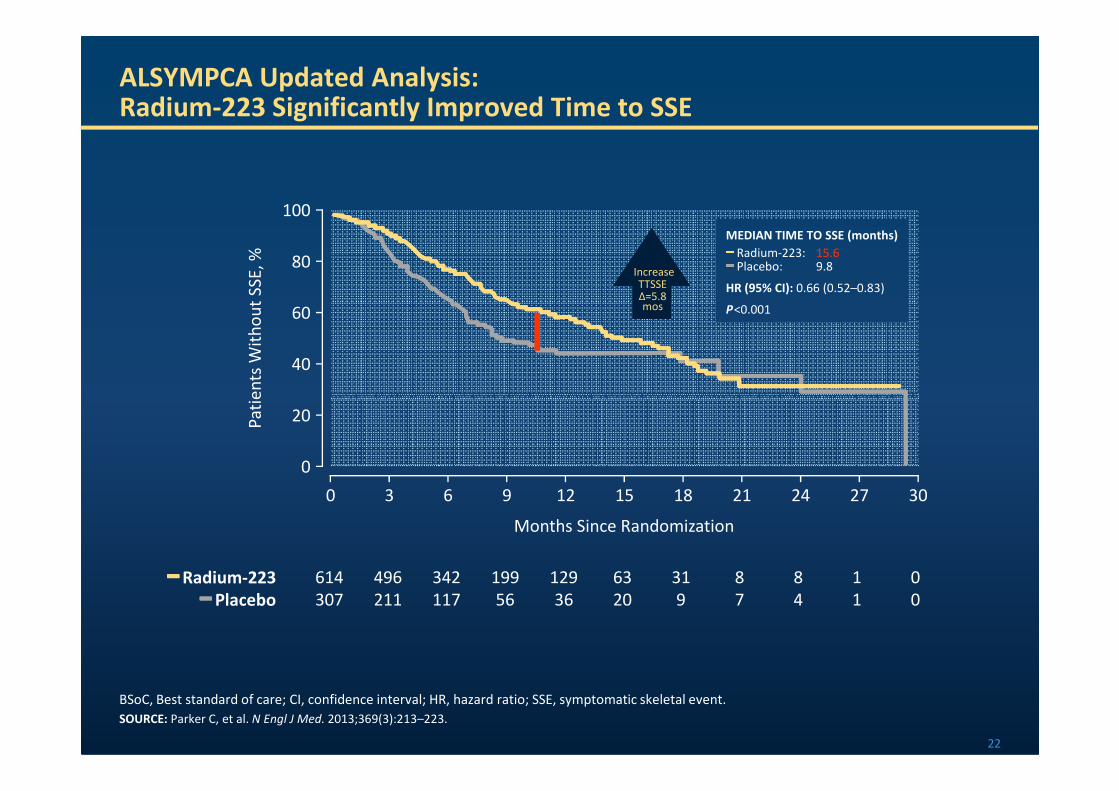
%MEDIAN TIME TO SSE (months)━━━━ Radium-223: 15.6━━━━ Placebo: 9.8
HR (95% CI): 0.66 (0.52–0.83)
P<0.001
ALSYMPCA Updated Analysis: Radium-223 Significantly Improved Time to SSE
IncreaseTTSSE∆=5.8mos
20
0
Pa
tie
nts
Wit
ho
ut
SS
E,
%
Months Since Randomization
0 9 15 24 302721181263
BSoC, Best standard of care; CI, confidence interval; HR, hazard ratio; SSE, symptomatic skeletal event.
SOURCE: Parker C, et al. N Engl J Med. 2013;369(3):213–223.
━━━━ Radium-223 614 496 342 199 129 63 31 8 8 1 0
━━━━ Placebo 307 211 117 56 36 20 9 7 4 1 0
22
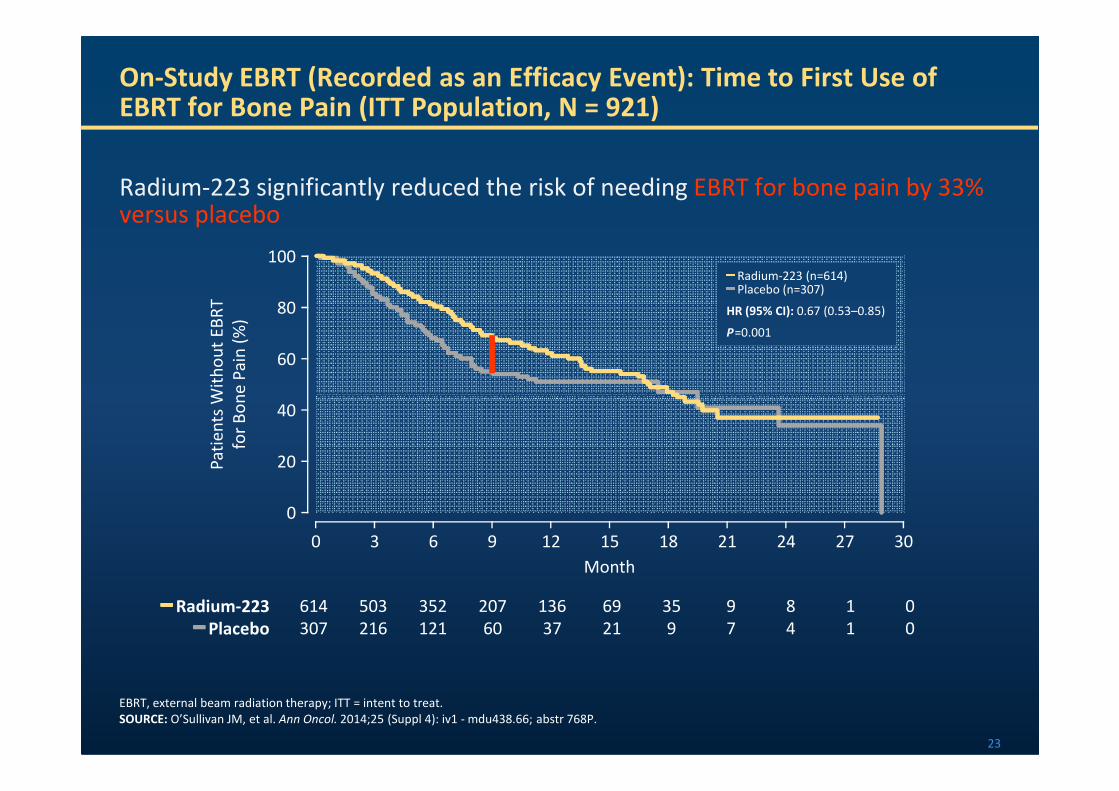
Radium-223 significantly reduced the risk of needing EBRT for bone pain by 33% versus placebo
On-Study EBRT (Recorded as an Efficacy Event): Time to First Use of EBRT for Bone Pain (ITT Population, N = 921)
60
80
100
Pa
tie
nts
Wit
ho
ut
EB
RT
for
Bo
ne
Pa
in (
%)
━━━━ Radium-223 (n=614)━━━━ Placebo (n=307)
HR (95% CI): 0.67 (0.53–0.85)
P=0.001
23
EBRT, external beam radiation therapy; ITT = intent to treat.
SOURCE: O’Sullivan JM, et al. Ann Oncol. 2014;25 (Suppl 4): iv1 - mdu438.66; abstr 768P.
━━━━ Radium-223 614 503 352 207 136 69 35 9 8 1 0
━━━━ Placebo 307 216 121 60 37 21 9 7 4 1 0
20
0
40
Pa
tie
nts
Wit
ho
ut
EB
RT
for
Bo
ne
Pa
in (
%)
Month
0 9 24 30183 21 2715126
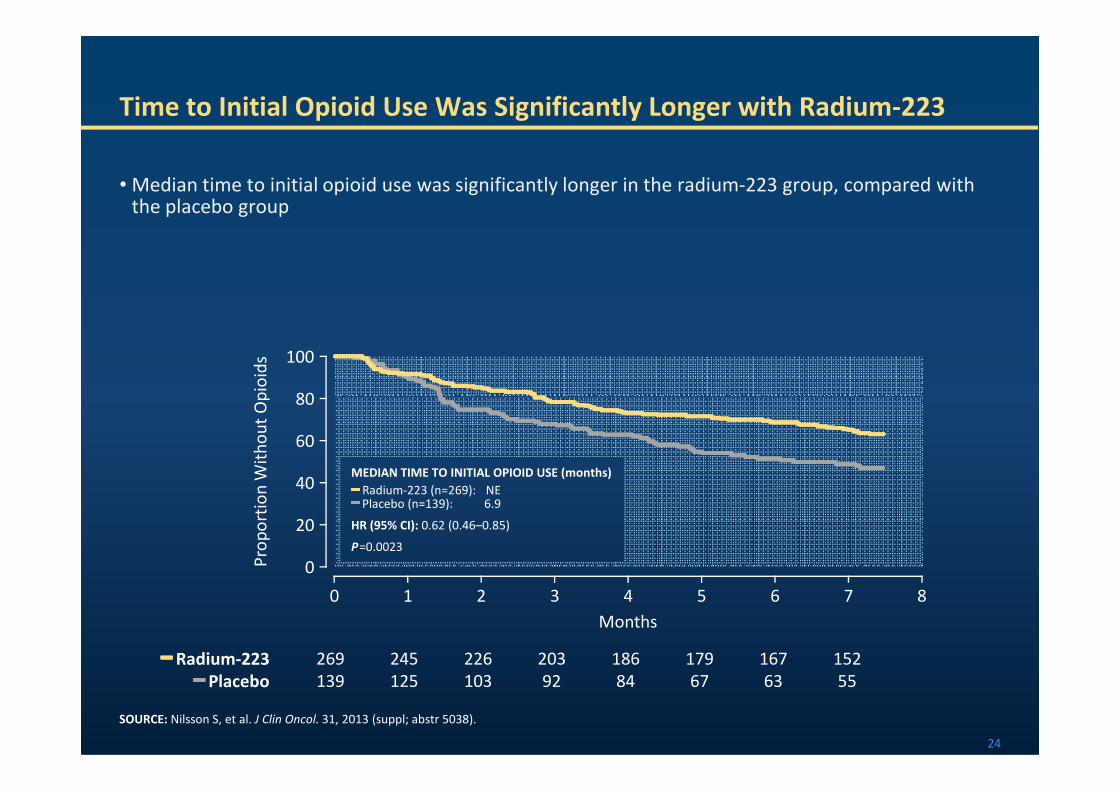
• Median time to initial opioid use was significantly longer in the radium-223 group, compared with the placebo group
Time to Initial Opioid Use Was Significantly Longer with Radium-223
80
100
Pro
po
rtio
n W
ith
ou
t O
pio
ids
24
MEDIAN TIME TO INITIAL OPIOID USE (months)━━━━ Radium-223 (n=269): NE━━━━ Placebo (n=139): 6.9
HR (95% CI): 0.62 (0.46–0.85)
P=0.0023
SOURCE: Nilsson S, et al. J Clin Oncol. 31, 2013 (suppl; abstr 5038).
━━━━ Radium-223 269 245 226 203 186 179 167 152
━━━━ Placebo 139 125 103 92 84 67 63 55
20
0
40
60
80
Pro
po
rtio
n W
ith
ou
t O
pio
ids
Months
0 3 6 875421
ALSYMPCA SAFETY OUTCOMES
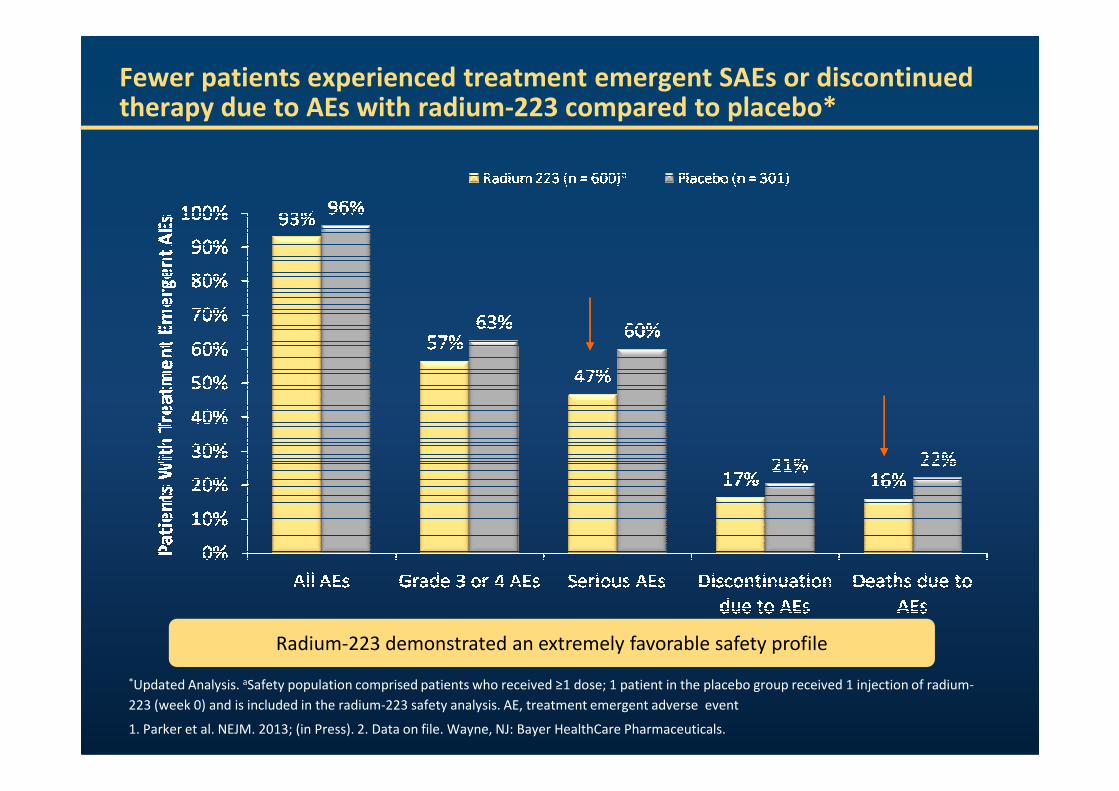
Fewer patients experienced treatment emergent SAEs or discontinued therapy due to AEs with radium-223 compared to placebo*
*Updated Analysis. aSafety population comprised patients who received ≥1 dose; 1 patient in the placebo group received 1 injection of radium-
223 (week 0) and is included in the radium-223 safety analysis. AE, treatment emergent adverse event
1. Parker et al. NEJM. 2013; (in Press). 2. Data on file. Wayne, NJ: Bayer HealthCare Pharmaceuticals.
Radium-223 demonstrated an extremely favorable safety profile
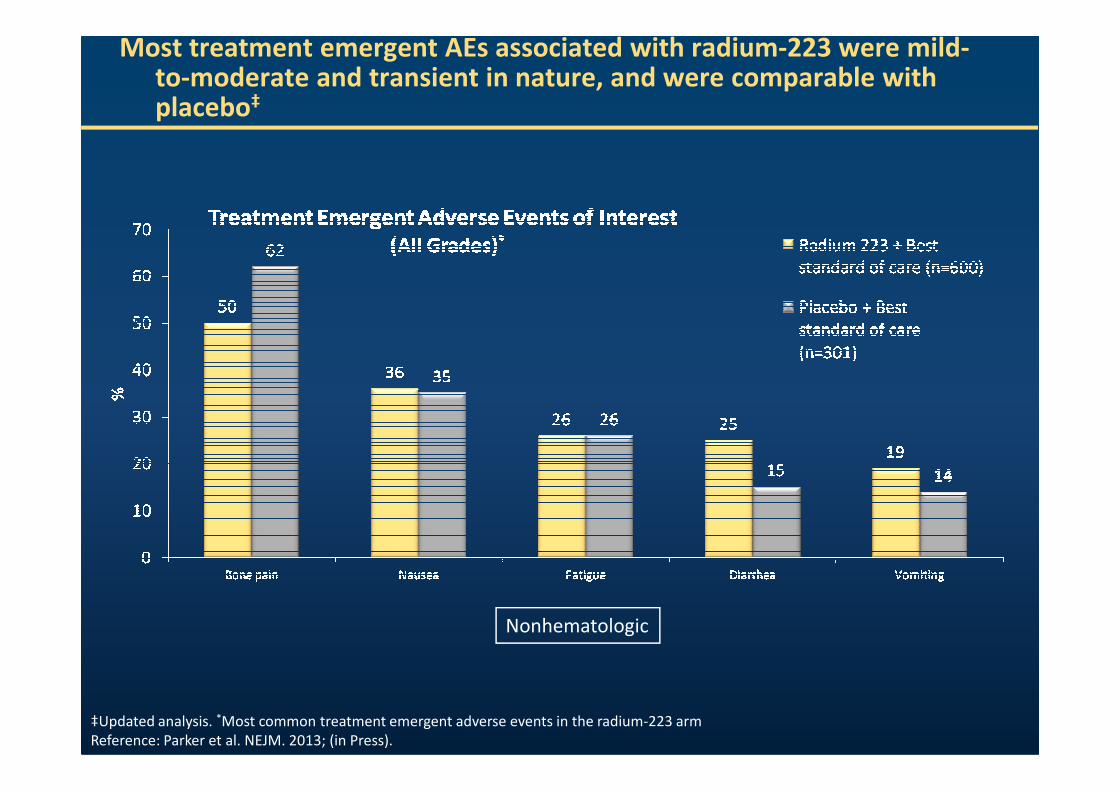
Most treatment emergent AEs associated with radium-223 were mild-to-moderate and transient in nature, and were comparable with placebo‡
Nonhematologic
‡Updated analysis. *Most common treatment emergent adverse events in the radium-223 arm
Reference: Parker et al. NEJM. 2013; (in Press).
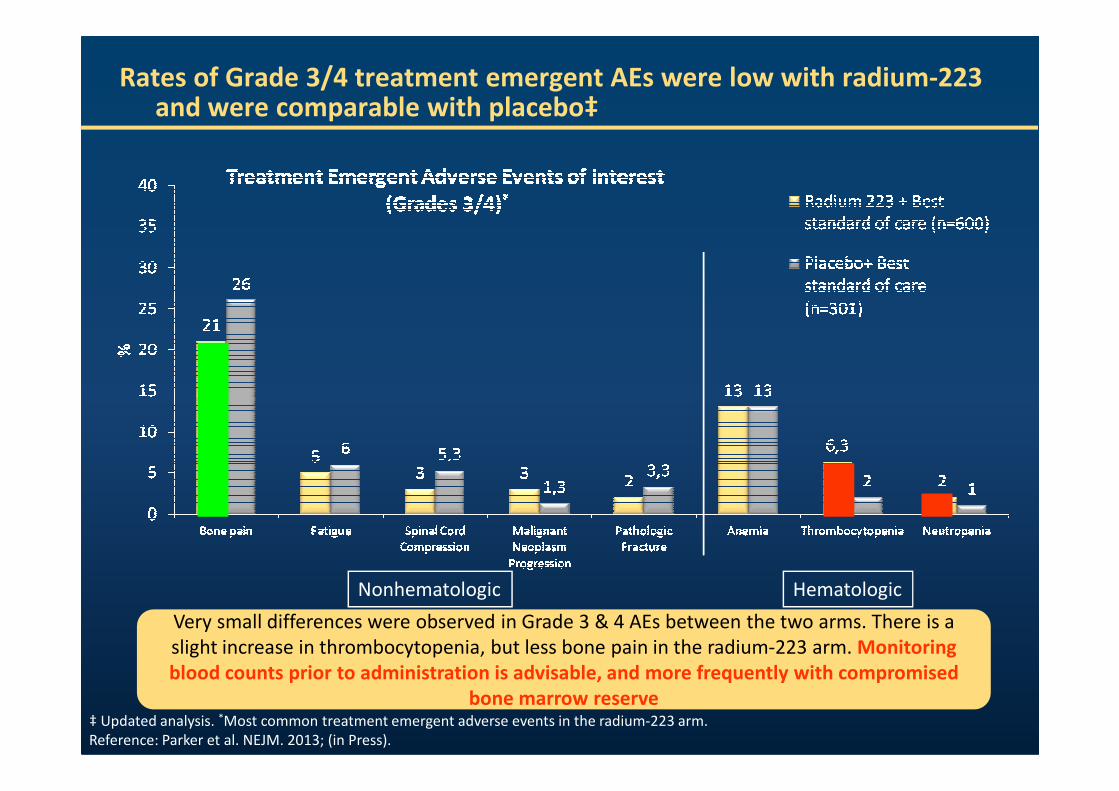
Rates of Grade 3/4 treatment emergent AEs were low with radium-223 and were comparable with placebo‡
Nonhematologic Hematologic
‡ Updated analysis. *Most common treatment emergent adverse events in the radium-223 arm.
Reference: Parker et al. NEJM. 2013; (in Press).
Very small differences were observed in Grade 3 & 4 AEs between the two arms. There is a
slight increase in thrombocytopenia, but less bone pain in the radium-223 arm. Monitoring
blood counts prior to administration is advisable, and more frequently with compromised
bone marrow reserve
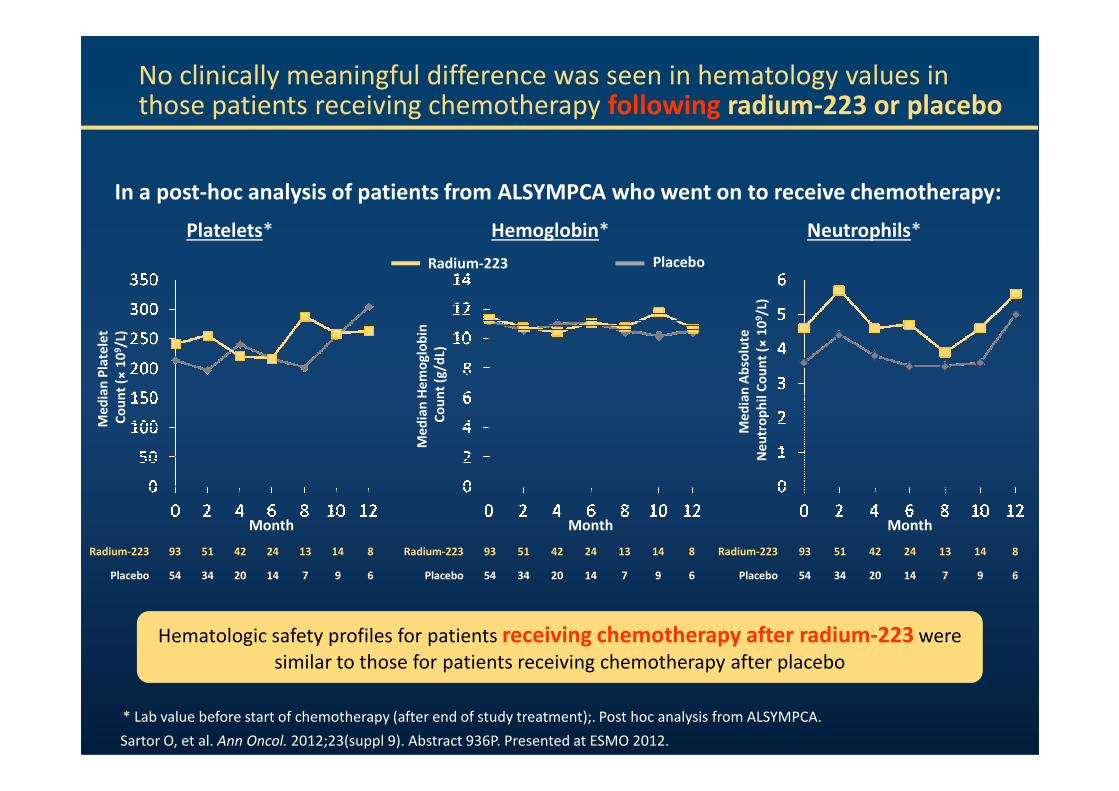
No clinically meaningful difference was seen in hematology values in those patients receiving chemotherapy following radium-223 or placebo
Me
dia
n P
late
let
Co
un
t (×
10
9/L
)
Me
dia
n H
em
og
lob
in
Co
un
t (g
/dL)
Platelets* Hemoglobin*
Radium-223 Placebo
Me
dia
n A
bso
lute
Ne
utr
op
hil
Co
un
t (×
10
9/L
)
Neutrophils*
In a post-hoc analysis of patients from ALSYMPCA who went on to receive chemotherapy:
Month
Me
dia
n P
late
let
Co
un
t (
Radium-223 93 51 42 24 13 14 8
Placebo 54 34 20 14 7 9 6
Me
dia
n H
em
og
lob
in
Co
un
t (g
/dL)
Month
Sartor O, et al. Ann Oncol. 2012;23(suppl 9). Abstract 936P. Presented at ESMO 2012.
* Lab value before start of chemotherapy (after end of study treatment);. Post hoc analysis from ALSYMPCA.
Month
Me
dia
n A
bso
lute
Ne
utr
op
hil
Co
un
t (
Hematologic safety profiles for patients receiving chemotherapy after radium-223 were
similar to those for patients receiving chemotherapy after placebo
Radium-223 93 51 42 24 13 14 8
Placebo 54 34 20 14 7 9 6
Radium-223 93 51 42 24 13 14 8
Placebo 54 34 20 14 7 9 6
Radium-223 Treatment of Bone Metastases in Metastatic Castration-Resistant Prostate Cancer (mCRPC)
• Vogelzang_Prior_Docetaxel_ASCO_2013.pdf
• (Efficacy and Safety of Radium-223 Dichloride in Castration-Resistant Prostate Cancer (CRPC) Patients
• Nos doentes sem quimioterapia prévia a mediana de OS foi 16.1 meses (Ra-223) vs 11.5 meses (Placebo); (HR = 0.745; 95% CI, 0.562-0.987; P = 0.039).
• Nos doentes com quimioterapia prévia a mediana de OS foi 14.4 meses (Ra-223) vs 11.3 meses (Placebo); (HR = 0.710; 95% CI, 0.565-0.891; P = 0.003).
• Globalmente existiu uma baixa incidência de mielosupressão. A incidência de neutropénia e de trombocitopénia foi superior nos doentes com quimioterapia préviavs doentes sem quimioterapia prévia
Conclusions
• In ALSYMPCA, radium-223 significantly prolonged overall survival in patients who had castration-resistant prostate cancer and bone metastases, with a 30% reduction in the risk of death (HR=0.70), as compared with placebo
• In the updated analysis, the median OS was longer by 3.6 months among patients who received radium-223 compared to placebo
•All secondary efficacy endpoints were significant and favored radium-223, including the clinically defined end point of the time to the first SSE
Radium-223 Treatment of Bone Metastases in Metastatic Castration-Resistant Prostate Cancer
(mCRPC) Conclusions
including the clinically defined end point of the time to the first SSE
•Overall QoL remained better in the radium-223 arm
•The overall incidence of AEs (all grade, grade 3/4, SAEs) was consistently lowerin the radium-223 arm than in the placebo group
– The number of patients who discontinued the study drug because of AEs was also lower in the radium-223 group
– No clinically meaningful differences in the frequency of hematologic AEs were observed between the treatment groups
32
SOURCE: Parker C, et al. N Engl J Med. 2013;369(3):213–223.
Radium-223 Treatment of Bone Metastases in Metastatic Castration-Resistant Prostate Cancer (mCRPC)
• Morris_ESMO_2014.pdf
• (Safety of Radium-223 Dichloride With Docetaxel in Patients With Bone Metastases From Castration-Resistant Prostate Cancer: A Phase 1/2a Clinical Trial)
• Estudo de fase I/IIa sobre o tratamento concomitante com rádio-223 e docetaxel
• Rádio-223 + docetaxel é bem tolerado na dose rádio-223 50 kBq/kg cada 6 semanas ו Rádio-223 + docetaxel é bem tolerado na dose rádio-223 50 kBq/kg cada 6 semanas ×5 + docetaxel 60 mg/m2 cada 3 semanas × 10
• Os dados preliminares de segurança sugerem que este regime poderá avançar para uma nova fase de investigação
• Estes dados dizem respeito a uma utilização não aprovada de rádio-223, que apenas está aprovado em monoterapia na dose de 50 kBq/kg cada 4 semanas x 6
Obrigada pela atenção !