rapidly progressive cognitive impairment without delirium
TRANSCRIPT
Rapidly Progressive CognitiveImpairment Without Delirium
Diagnostic Challenges from the MemoryClinic
Dr Andrew Tarbuck (FRCPsych)Dr Yasir Hameed (MRCPsych)North Central DCLL TeamJulian Hospital. Norwich.May 2015

Objectives
Describe three clinical cases
Rapidly progressive dementia or cognitivedecline
List differential diagnosis
Explain rational diagnostic approach

The Skills Required for Old AgePsychiatrists

DementiaComplexityLaterLife
Dang! . . .Now wherewas I going?
Superman in his later years
Case 1: Rapid Descent

63 years old lady lives with husband
Referred urgently by GP in February 2014 due toincreasing confusion, poor memory and various othersymptoms
She had a fall 10 days ago and everything becameworse
Disoriented in her own home (unable to work out howto get out through a door)
Unusual experiences, auditory hallucination,misidentification of family, rooms and furniture

Speech incoherent and vague
Sleeping 18 hours a day
Unsteady on her feet, rapid decline in mobilityand self care
Fluctuating presentation
No fever. No alcohol or drug misuse.

Psychosocial stressors evident: Grandsondiagnosed with leukaemia before Christmas.
She lost her mother, two friends over a courseof two years
New onset of panic attacks with anxietysymptoms (hyperventilation) and perceptualdistortions (feeling that the room/walls/peopleclosing on her)
Headaches and burning sensation over herbody

GP examination: Conscious, but disoriented toperson, place and time. Cranial nerves andperipheral nerves intact. GP COG 3/9. She wasable to draw a clock and put arms on.
Her appetite fine (she eats everything we put infront of her)
Husband is unable to cope. Her son anddaughter visiting regularly.
Further informationPast Psych Hx: Overdose in 1970s in context of
relationship breakdown. None since.
Past Med Hx: ME since 1987 and IBS. On Amitriptyline25 mg nocte for years.
Family Hx: Brother died from complications of alcoholdependence. Daughter under Ix by neurologist for ?Peripheral neuropathy.
Personal Hx: Lives with husband. Daughter livesnearby. Son lives in Essex (paramedic).

What is your differential diagnosis?
Over next few weeksCT scan 2.3.14 and bloods: NAD.
CRHT brief involvement then referred to DIST. Mirtazapinestarted. Amitriptyline stopped.
Consultant Psychiatrist’s review on 24.3.14: she was inwheelchair, disoriented, non psychotic. Unable to completedetailed cognitive assessment. Neurological exam revealedataxic gait, with choreoathetoid movements of both upperlimbs, poor coordination, but normal tone and reflexes.
Recommended urgent admission to NNUH.

NNUH admission 24.3.15
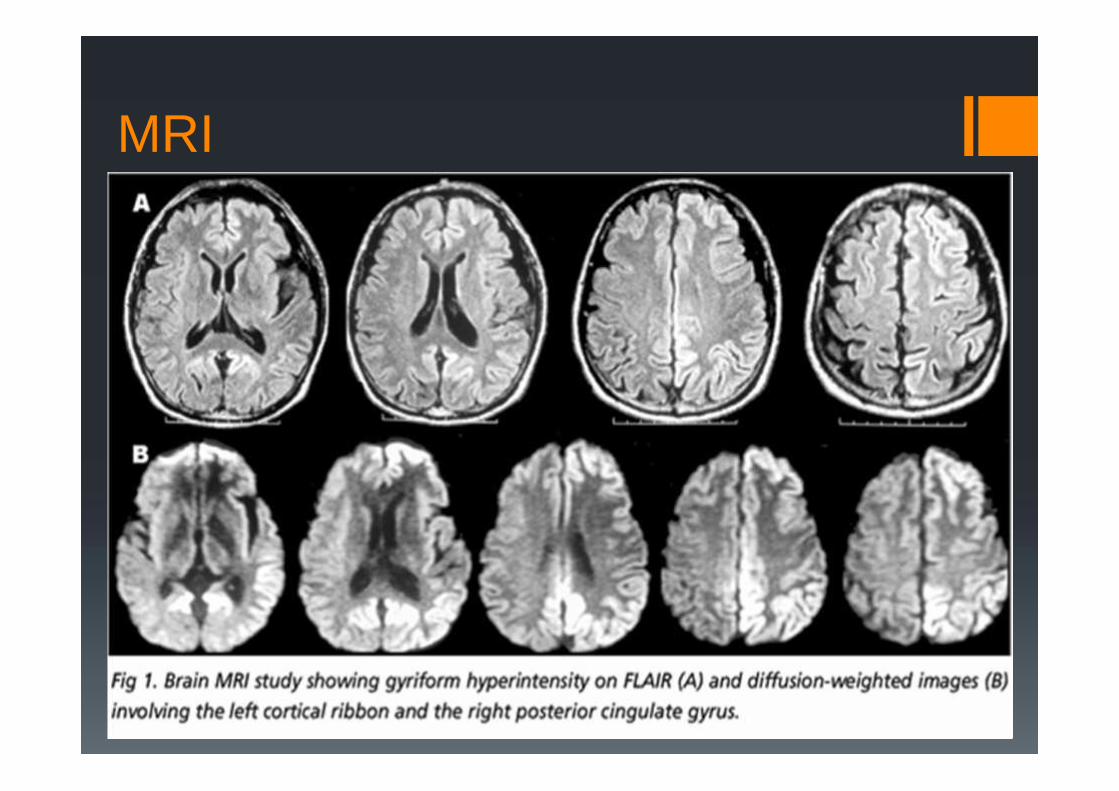
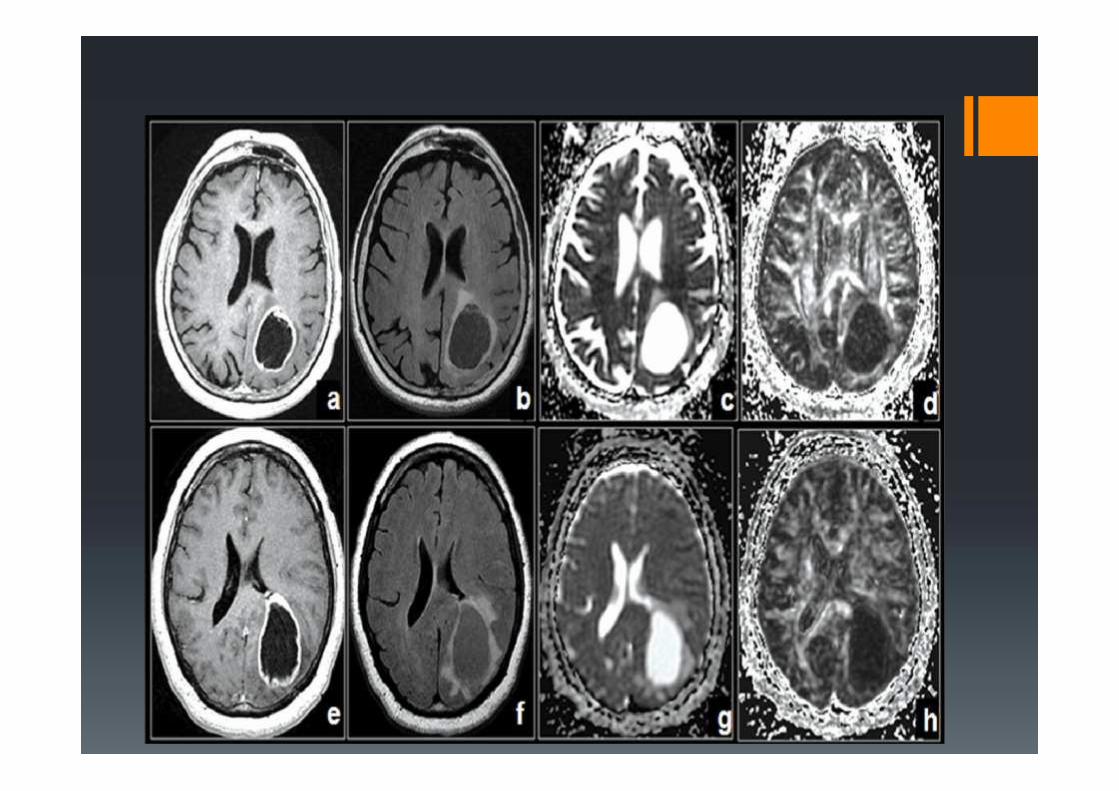
MRI 26.3.14: Extensive bilateral asymmetricalcortical restricted diffusion with mild associatedhigh signal on T2 and FLAIR images. Sparing ofsubcortical regions. Small old lacunar infarction inLt caudate nucleus. Mild small vessel disease.Mild cerebral atrophy.
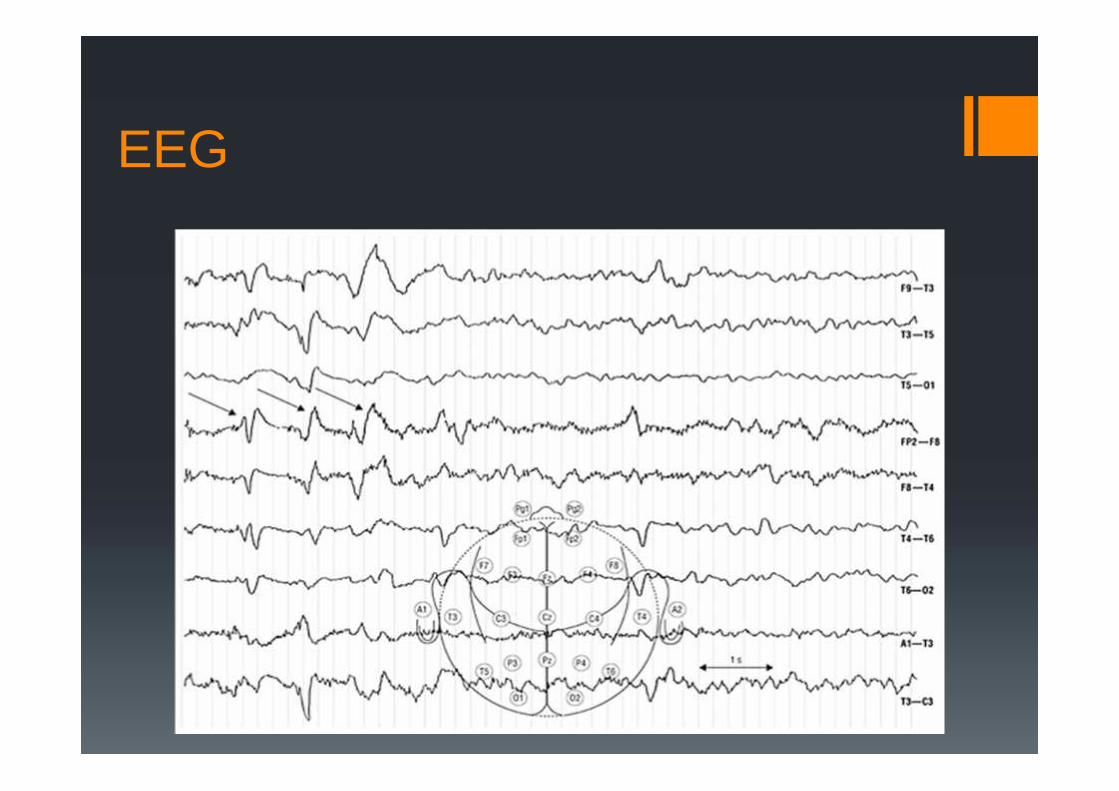
EEG: diffusely low, nonspecific changessuggestive of neurodegenerative disease.
MRI
EEG

Outcome
Patient passed away on 21.4.14.
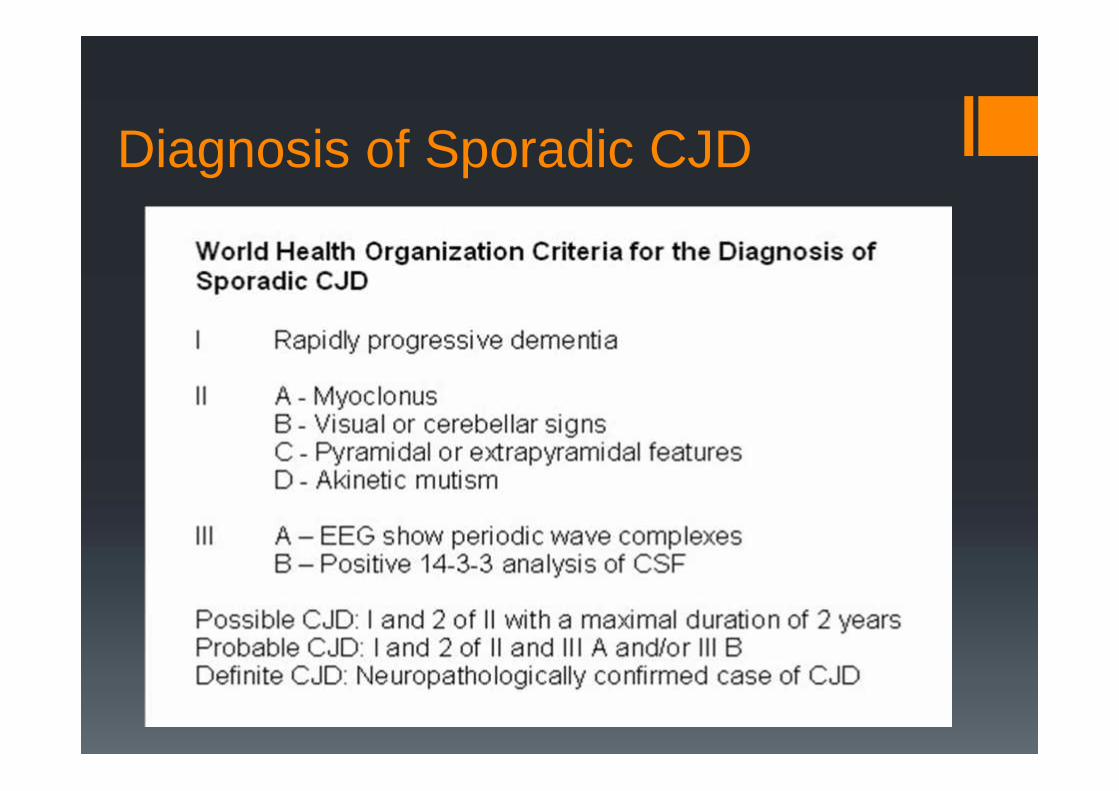
Diagnosis of Sporadic CJD

Other types of CJDVariant CJD: First reported in 1996 in UK. Transmission of
BSE infection from Cattle to human. Compared to sCJD: Ageonset is younger, longer duration of illness (1 year or more),initial presentation is psychiatric then neurological. Tonsillarbiopsy is used to show abnormal protein.
Familial (Genetic) CJD: Caused by an inherited abnormalgene (a mutation in the human prion protein gene, PRNP).Positive family history and genetic testing can confirm thediagnosis.

Case 2: Bewilderment
79 years old man
Referred in April 2014 with 4 weeks history of interruptedsleep, tearful.
Bewildered with poor memory
Frontal headache
GP COG 1/9 (scored 9/9 in November 2013)
GP started citalopram, he didn’t take it.
No obvious neurological or physical sign
Past Med Hx of bladder stones, BPH, AAA surveillance, AFand cardiac stent. On warfarin.
Psychiatric assessment He had severe ear infection and UTI in March
Rapid deterioration from this point
Reports of visual hallucinations. Right sided inattention (bumping intowalls and doorways) with right left disorientation.
Unsteady on his legs
Episodes of urinary incontinence
Reduced motivation and poor self care. Labile mood.
Word finding difficulty and using wrong words (says “water” when hewant to go to the toilet). Non fluent dysphasia.
Cognitive assessment: disoriented, severecognitive impairment. Nominal dysphasia (unableeven to name pen or watch). Poorcomprehension. Unable to score any points onformal cognitive testing.
Any suggestions for diagnosis?

Differential diagnosis
CVA with subsequent progression (possiblybleeding)Intracerebral abscess resulting from his recentear infectionSubdural haematoma (although no history ofrecent falls or head injuries)Some other space occupying lesion

MRI 06 May 2014Solitary 4.2 x 3.4 cm centrally heterogeneousmass in the left pareito-occipital region. Localmass effect with effacement of the leftposterior horn of the lateral ventricle. Mildsmall vessel disease.
Conclusion: Glioblastoma of left parieto-occipital and to a lesser extent, temporallobe.
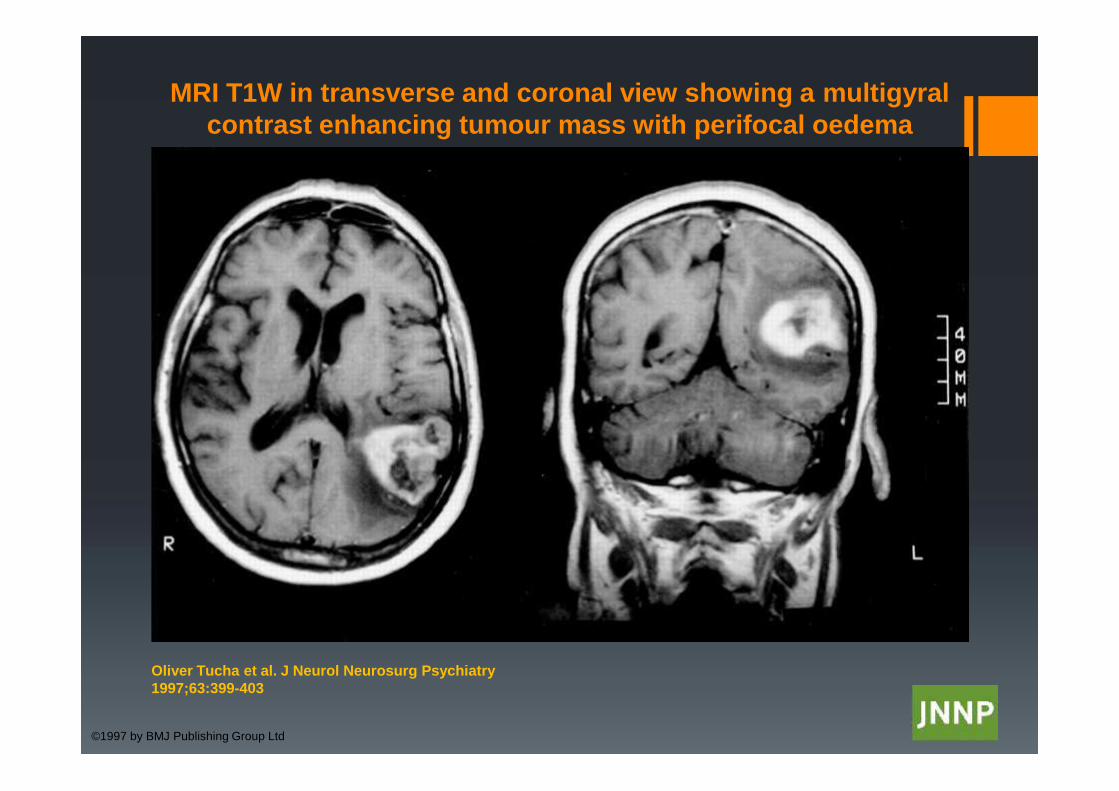
MRI T1W in transverse and coronal view showing a multigyralcontrast enhancing tumour mass with perifocal oedema
Oliver Tucha et al. J Neurol Neurosurg Psychiatry1997;63:399-403
©1997 by BMJ Publishing Group Ltd

Outcome
Patient passed away on 26.07.2014

Glioblastoma
The most common and most aggressive type ofprimary brain cancer.
Current treatment include maximal surgicalresection followed by concurrent radio andchemotherapy.
The prognosis is poor, with median survival ofabout14 months.
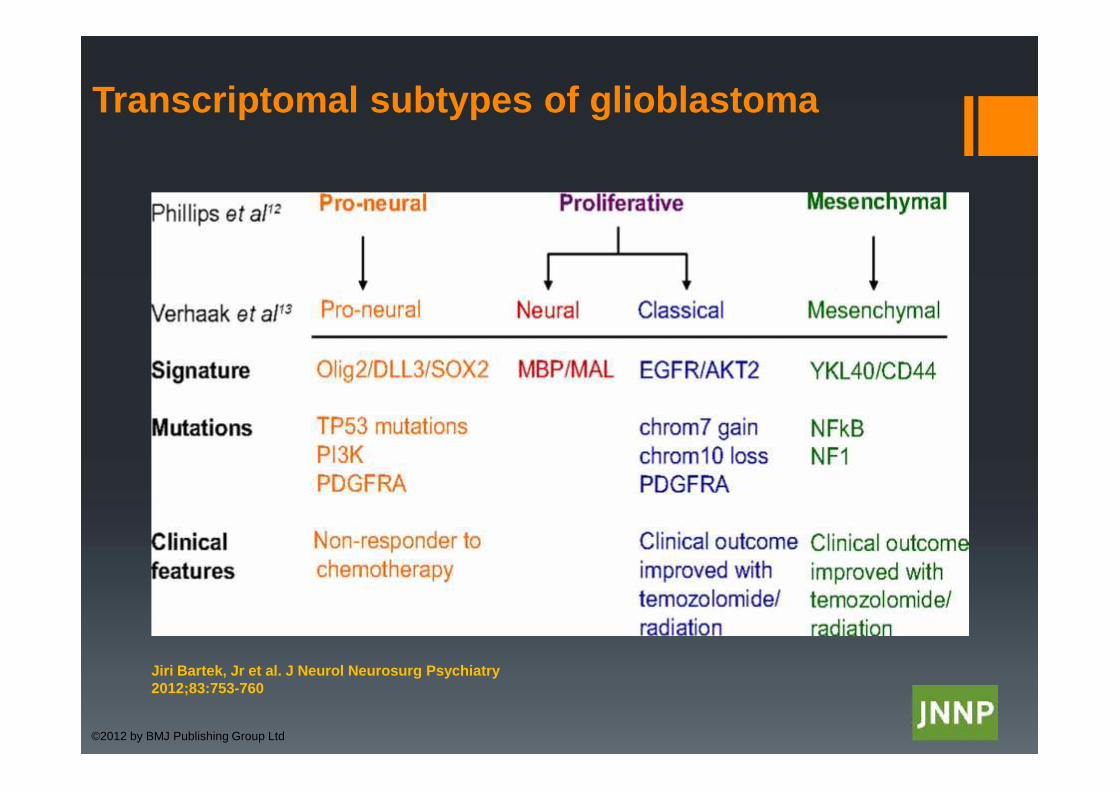
Transcriptomal subtypes of glioblastoma
Jiri Bartek, Jr et al. J Neurol Neurosurg Psychiatry2012;83:753-760
©2012 by BMJ Publishing Group Ltd
Gerstmann syndrome
Finger agnosiaRight-left disorientationAgraphiaAcalculia
Dominant hemisphere lesions affectingthe angular gyrus
Case 3: Talking to ghosts
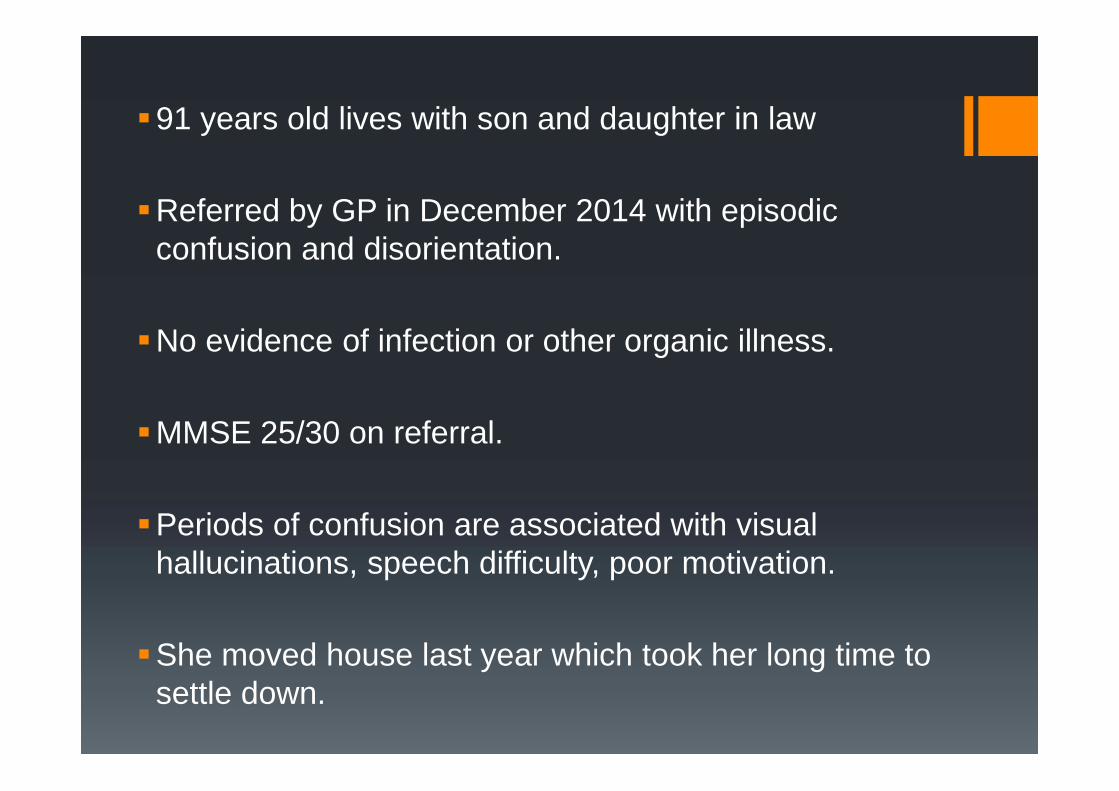
91 years old lives with son and daughter in law
Referred by GP in December 2014 with episodicconfusion and disorientation.
No evidence of infection or other organic illness.
MMSE 25/30 on referral.
Periods of confusion are associated with visualhallucinations, speech difficulty, poor motivation.
She moved house last year which took her long time tosettle down.

Reports of gradual decline in mobility and one report offall, no head injury.
ADLs gradually worsened, poor control of hands’movement.
Reports of interrupted sleep, and she may have fallenout of bed repeatedly.
GP started Escitalopram with no effect.
No family history of note.

Psychiatric assessmentMood was flat, but not depressed.Monotonous slow speechNot psychoticLimited insight.
Cognitive assessment: MMSE 25/30 with difficulty in shortterm recall, writing a sentence and copying a diagram. Shewas unable to draw a clock.



DaT Scan
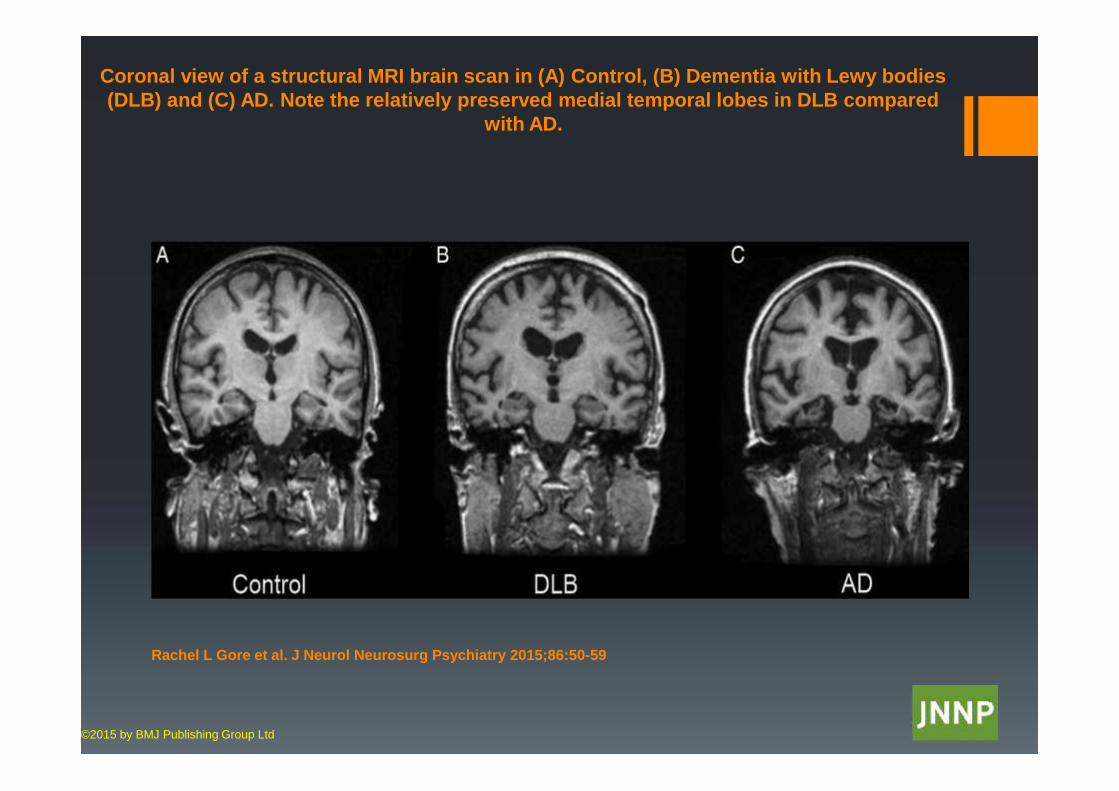
Coronal view of a structural MRI brain scan in (A) Control, (B) Dementia with Lewy bodies(DLB) and (C) AD. Note the relatively preserved medial temporal lobes in DLB compared
with AD.
Rachel L Gore et al. J Neurol Neurosurg Psychiatry 2015;86:50-59
©2015 by BMJ Publishing Group Ltd

Neurology Assessment
Tremor both upper limbs, more in left hand.
No significant bradykinesia.
Shuffling gait with no arm swing on either side.
Cog wheel rigidity with re-enforcement.
Neurologist agreed on dopamine replacement therapy.
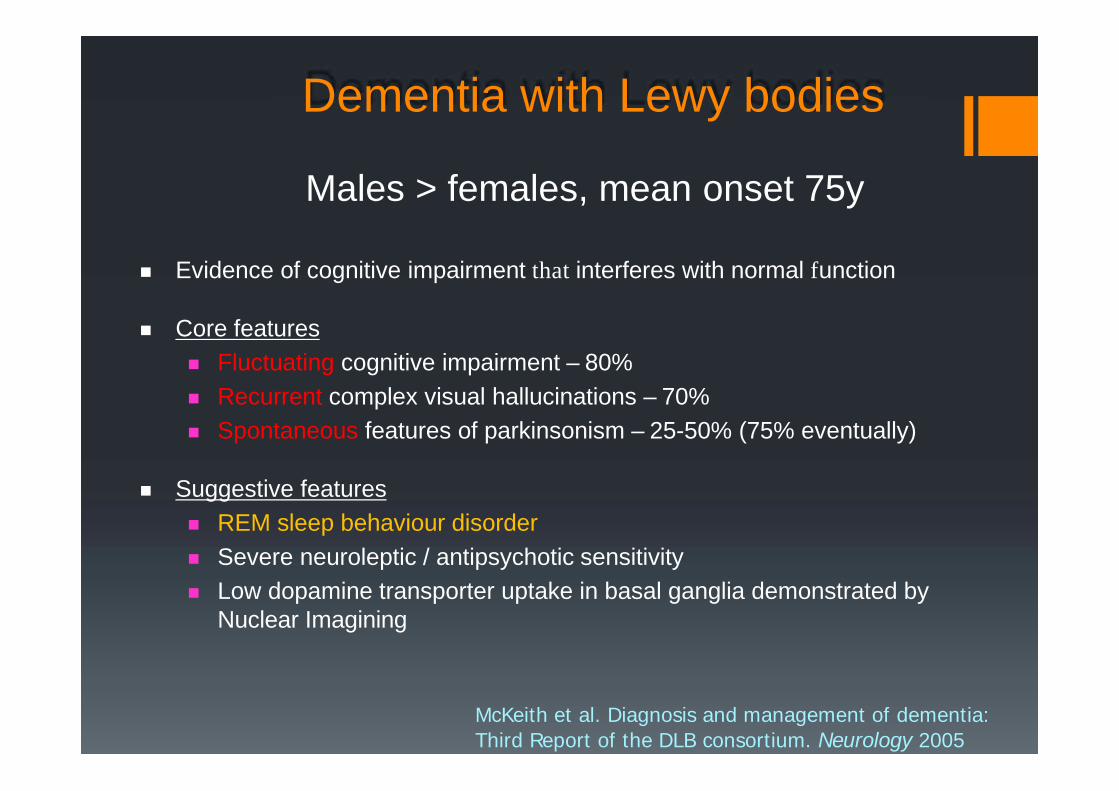
Dementia with Lewy bodies
McKeith et al. Diagnosis and management of dementia:Third Report of the DLB consortium. Neurology 2005
Evidence of cognitive impairment that interferes with normal function
Core features Fluctuating cognitive impairment – 80% Recurrent complex visual hallucinations – 70% Spontaneous features of parkinsonism – 25-50% (75% eventually)
Suggestive features REM sleep behaviour disorder Severe neuroleptic / antipsychotic sensitivity Low dopamine transporter uptake in basal ganglia demonstrated by
Nuclear Imagining
Males > females, mean onset 75y

Supportive features Falls and syncope Unexplained loss of consciousness Autonomic dysfunction Hallucinations in other modalities Systematised delusions Depression Preserved medial temporal lobe structures on CT/MRI Generalised low uptake on HMPOA SPECT/PET perfusion/metabolism
scan with reduced occipital activity Prominent slow wave activity on EEG with temporal lobe transient sharp
waves
Dementia with Lewy bodies
McKeith et al. Diagnosis and management of dementia:Third Report of the DLB consortium. Neurology 2005
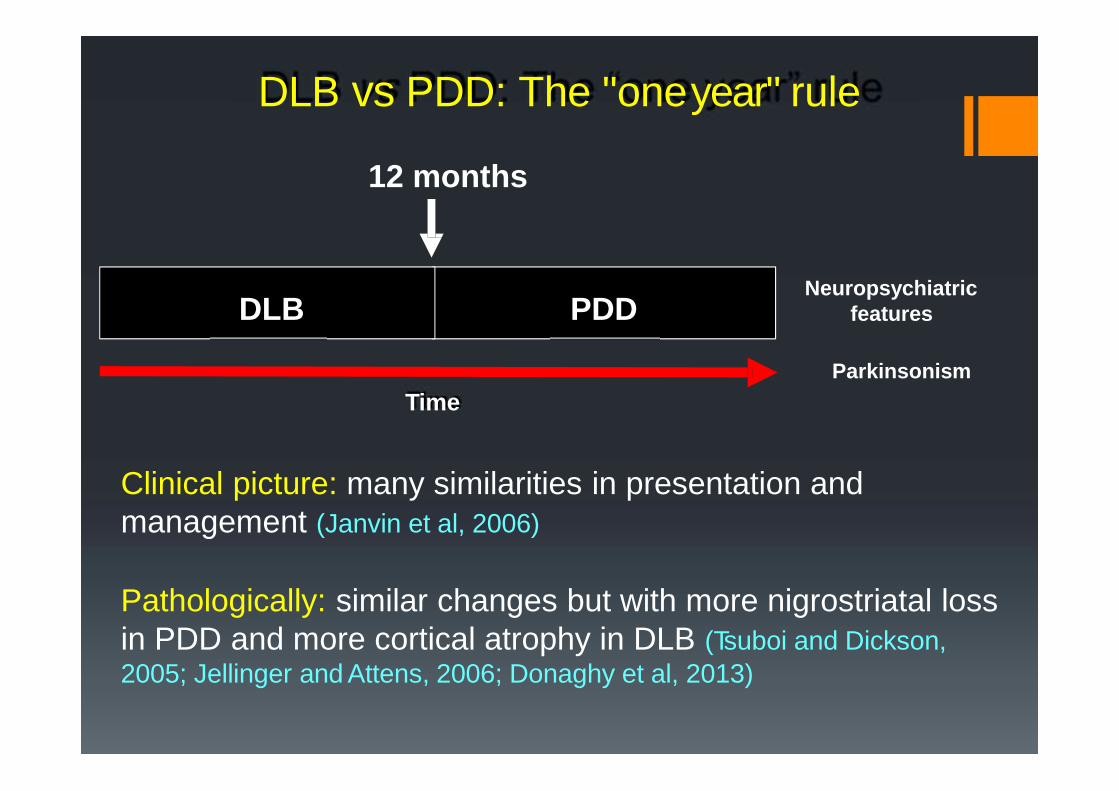
DLB vs PDD: The "oneyear" rule
12 months
ParkinsonismTime
Clinical picture: many similarities in presentation andmanagement (Janvin et al, 2006)
Pathologically: similar changes but with more nigrostriatal lossin PDD and more cortical atrophy in DLB (Tsuboi and Dickson,2005; Jellinger and Attens, 2006; Donaghy et al, 2013)
PDDDLBNeuropsychiatric
features

Difficulty in diagnosis of LBDDifficulty in assessment of fluctuating course
Failure to ask about supportive features (especially REMBehavioural Sleep Disorder, occurs in 50-80%)
Poor or no cognitive assessment
Atypical presentations are common
Underuse of the possible diagnosis of LBD and underuseof biomarkers
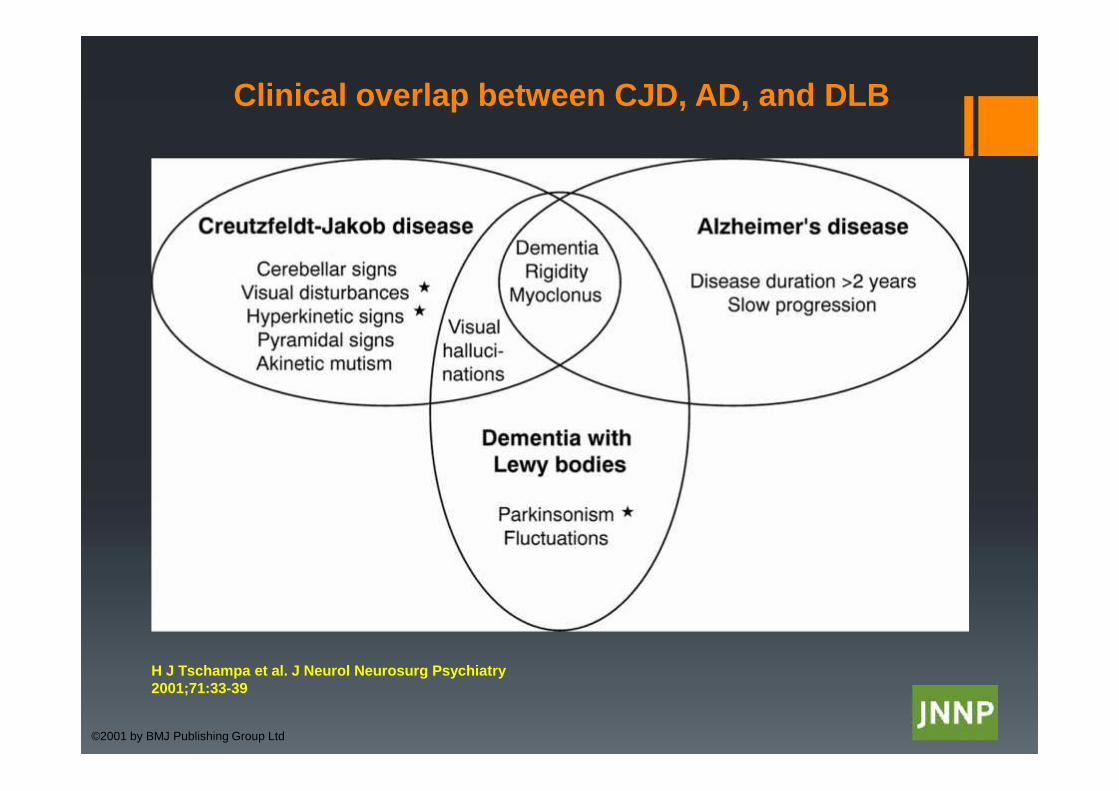
Clinical overlap between CJD, AD, and DLB
H J Tschampa et al. J Neurol Neurosurg Psychiatry2001;71:33-39
©2001 by BMJ Publishing Group Ltd
Robin Williams’ silent suffering
