rationale for adding a non invasive robotic radiosurgery ... di muzio...rationale for adding a non...
TRANSCRIPT

Rationale for adding a non invasive robotic radiosurgery system in a multi-platform radiotherapy department
Prof. N. Di Muzio, M.D.
Director of Radiotherapy Department
San Raffaele Scientific Institute, Milan, Italy
AERO ACADEMY, May 8, 2017

Disclosure & Disclaimer
• An honorarium is provided by Accuray for this presentation
• The views expressed in this presentation are those of the presenters and do not necessarily reflect the views or policies of Accuray Incorporated or its subsidiaries. No official endorsement by Accuray Incorporated or any of its subsidiaries of any vendor, products or services contained in this presentation is intended or should be inferred.

San Raffaele Scientific Institute RadiationTherapy Department
• 1st TomoTherapy®
System in Europeinstalled in 2004(substituted in 2013with Tomotherapy H)
• 2nd TomoTherapy®
System installed in 2007
• 3rd TomoTherapy®
System installed in 2012
Simulator : “ Varian Acuity”
CT simulator : “GE Hi Speed”
Rapid Arc “Clinac iX” Varian
Gamma knife “ Perfexion”
TomoTherapy “Hi-Art® II System”
TomoHD™ System
TomoH™ System
CyberKnife®
System

STEREOTACTIC BODY RT
RADIOABLATIVE RT
SIMULTANEOUS INTEGRATED BOOST
ADAPTIVE RT
HIGH TECHNOLOGY
OPTIMAL SPARING NORMALTISSUE
HIGH DOSE DELIVERED
OPTIMAL TUMOR CONTROL
New patients/year : 2000

IGRTIMAGING
Reduction of safety margins
Precise localizationof the tumor and/or target volume and sensitive structures
Reduce the uncertainty ofmicroscopic extension
Reduce the uncertainty in the set-up, identify and reduce organ motion
REDUCTION of COLLATERAL DAMAGEto OARs
INCREASE of RADIATION DOSE and DOSE per FRACTION
High selectivity in radiation doseadministration
IMPROVEMENT IN LOCAL CONTROL

How does the CyberKnife® System fit with the main diseases treated in
our department?
1) Prostate Cancer2) CNS malignancies3) Breast Cancer4) Metastases5) ADAPTIVE RT Rectal Cancer

Prostate cancer Cozzarini C, Fiorino C, Deantoni C, et al. Higher-than-expected Severe (Grade 3-4)
late Urinary Toxicity After Postprostatectomy Hypofractionated Radiotherapy: ASingle institution analysis of 1176 Patients. European Urology 2014; 66: 1024-1030
Cozzarini C, Noris Chiorda B, Sini C, et al. Hematologic Toxicity in Patients Treatedwith Postprostatectomy Whole –Pelvis Irradiation with Different Intensity ModulatedRadiation Therapy Techniques is Not Negligible and Is Prolonged: Preliminary Resultsof a Longitudinal, Observational Study. International Journal of Radiation Oncology,Biology, Physics 2016; 95(2): 690-5.
Fodor A, Berardi G, Fiorino C, et al. Toxicity and efficacy of salvage carbon 11-cholinepositron emission tomography/computed tomography-guided radiation therapy inpatients with lymph node recurrence of prostate cancer. British Journal of UrologyInternational 2017; 119(3): 406-413.
Di Muzio NG, Fodor A, Noris Chiorda B, et al. Moderate Hypofractionation withSimultaneous Integrated Boost in Prostate Cancer: Long-term Results of a Phase I-IIStudy. Clinical Oncology (R Coll Radiol) 2016; 28(8): 490-500.

RTOG 5y TOXICITY LAST FOLLOW UP TOXICITY
GU: G 2-4: 20.2 %(± 2.8)GU: G 3-4: 5.9% (± 1.7)
GU: G 2-4: (7.1%)GU: G3-4: (1.9%)
GI: G 2-3: 17.0% (± 2.7)GI: G 3: 6.3% (± 1.7)
GI: G 2-3: (5.2%)GI: G 3: (1.9%)
Di Muzio et al, Clin Oncol 2016

“Extremely hypofractionated image-guided IMRT/SBRT regimens (6.5 Gy per fraction or greater)are an emerging treatment modality with single institutional and pooled reports of similarefficacy and toxicity to conventionally fractionated regimens. They can be considered as analternative to conventionally fractionated regimens at clinics with appropriate technology,physics, and clinical expertise.” (NCCN Guidelines Version 2.2017, Prostate Cancer)
Katz A, et al. Radiation Oncology 2013
King CR, et al. Radiother Oncol 2013
Calculations of the dose distributions in SRS radiotherapy forVMAT and CyberKnife® System techniques shows, that stereotacticradiosurgery of prostate cancer can be carried out on CyberKnife®
System accelerator as well as on the classical accelerator with theuse of VMAT technique
Ślosarek et al Pol J Med Phys Eng 2016Hannan R, Tumati V, Xie X-j, et al. Stereotactic body radiation therapy for low and intermediate risk prostate cancer- Results from a multi-institutional clinical trial. European Journal of Cancer 2016; 59: 142-151

-53,841 IMRT patients & 1,335 SBRT patients with at least 6months of follow-up
-Statistically significant higher GU toxicity at two years with SBRT
-No statistically significant difference in the incidence of fistulasbetween IMRT and SBRT at any point in time
-The majority of symptoms resolved with conservativemanagement
-But…SBRT current techinques may be able to minimize dose toadjacent tissues (prostate targeting) CyberKnife® System
-SBRT preferable for both patients and Institutions (insurers)Yu JB, et al. J Clin Oncol 2014
Halpern JA, et al. Cancer 2016
Median costs $27,145 $17,183 $37,090 $54,706
2) CNS malignancies First Gamma Knife
installed in our institutionin 1993.
Collaboration with theNeurosurgery.
9700 patients treated upto the end of 2016 (2ndEuropean centre afterMarseille).
Leksell Gamma Knife® Perfexion™, version in use

Brain metastases

A 41 year-old woman withmultiple metastases fromlung adenocarcinoma, intreatment with Gefitinib,presented 10 brainmetastases at MRIdiagnosis. Sixteen lesionsidentified on volumetricMRI were treated in March18, 2016. The patient isalive one year later,without brain PD.
A 52 year-old woman withbrain metastases from breastcancer, already treated in2013 with WBRT, presenteda PD in March 2016, with 10metastases at MRI. Atstereotactic MRI 18 lesionswere diagnosed and treatedwith GammaKnife.

Identical clinical results, but CyberKnife®
System better tailored to target thanGK for single brain metastases(Wowra B, et al. J Neurooncol 2009)
-Good CI, as GK for stereotactic radiosurgery of arteriovenous malformations and acousticneuromas-More homogeneous plans, because of inverse planning,-Lower dose spread.(Gevaert T, et al. Radiother Oncol 2013)
Dosimetric comparison for acoustic schwannoma(Dutta D, et al. J Neurooncol 2012)

Lesions close to optic chiasma are not manageable with SRS, but SRT with Gamma knife isnot tolerated by the patients, because of the stereotactic frame, which requiresanesthesia to be positioned, and cannot be worn for more than one day.

Robotic Radiosurgery for the Treatment of Intramedullary SpinalCord Metastases. Garcia R, et al. Cureus 2016
Adler JR. International Congress Series 2002
- Degen JW, et al. CyberKnife stereotactic radiosurgical treatment ofspinal tumors for pain control and quality of life. J Neurosurg: Spine2; 2005
- Gerszten PC, et al. CyberKnife Frameless Stereotacticradiosurgery for Spinal Lesions: Clinical experience in 125 cases.Neurosurgey 2004
- Kufeld M, et al. Radiosurgery of Spinal Meningiomas andSchwanomas. Technology in Cancer Research and treatment 2012
GammaKnife can treat lesions up to C2, thusspinal lesions (meningiomas, schwanomas,metastasis), which need the same precision andthe same reduced margins, can be treated withCyberKnife® System.

3) Breast cancer Our protocol for breast conserving therapy:
whole breast hypofractionated (40 Gy/15 fr)adjuvant radiotherapy with forward plannedintensity modulation (~1500 patients treated).
2.25% local failure at a median follow up of 68months, with low acute (5 G3/442 pts) and latetoxicity (2 G3/442 pts).

PBI good local controlELIOT trial: better than expected results with EBRT in selected low-riskTARGIT A: reduced deaths for other causes ( cardiovascular).
Veronesi U, et al. Lancet Oncol 2013 Vaidya JS, et al. Lancet 2014

3D CRT PBI- Interim Cosmetic Results ( ViciniF, et al. Int J Radiat Oncol Biol Phys 2007
APBI with Mammosite (Wallace M, et al. Int JRadiat Oncol Biol Phys 2010
APBI with HDR BT (Polgar C, et al.Radiother Oncol 2010 )
CK APBI (Obayomi-Davies O, et al. FrontOnc 2016)

All the dosimetric parameters for the target and critical structures met the NSABP B39/RTOG 0413 procol.
With advanced real-time tracking capability, CyberKnife® System should provide better target coverage and spare nearby critical organs for APBI treatment
Xu Q, et al. Medical Physics 2012
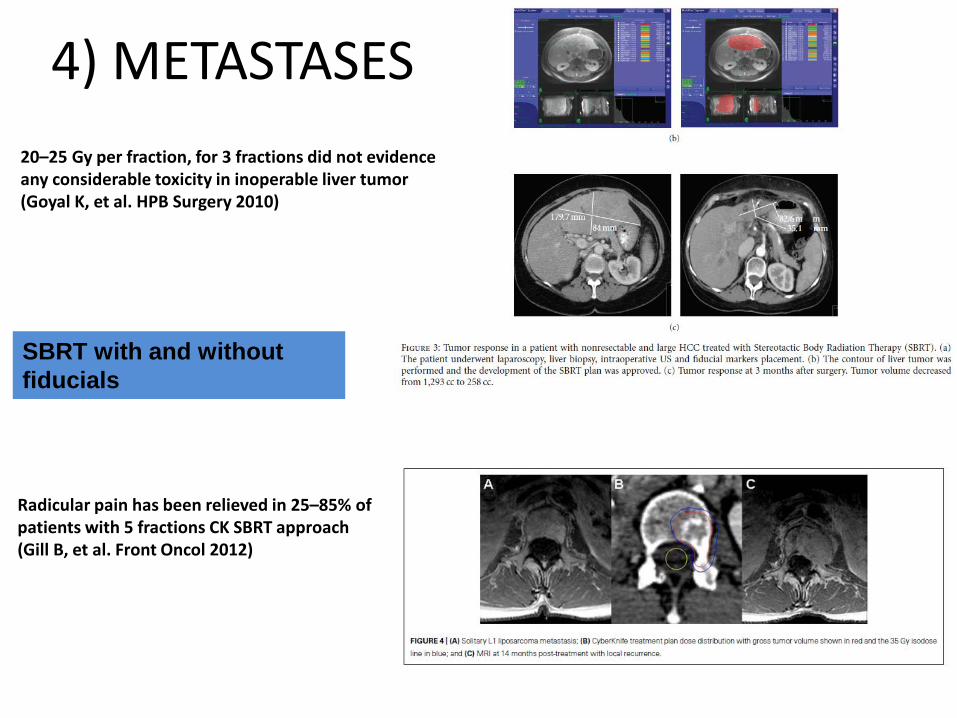
SBRT with and without fiducials
20–25 Gy per fraction, for 3 fractions did not evidence any considerable toxicity in inoperable liver tumor(Goyal K, et al. HPB Surgery 2010)
Radicular pain has been relieved in 25–85% of patients with 5 fractions CK SBRT approach (Gill B, et al. Front Oncol 2012)
4) METASTASES

72 patients not previouslyirradiated in the same areawere treated at pelvic and/orLA lymph nodes at a totaldose of 51.8 Gy/ 28 fr, andwith SIB up to 65.5 Gy(BED 167.73 Gy for α/β 1.5)on + LN
9 re-irradiated patients weretreated without SIB at 50-65.5 Gy/ 25-30 fr.
Prostatic bed was alwaystreated when not previouslyirradiated.
Fodor A et al, BJU International, 2016
91.4% of patients had a PSA reduction 3months after salvage HTT
OS 3 y = 80%, LRFS 3 y= 89.8%, CRFS 3 y=61.8 %
Uni and multivariate analysis showed no impact of ADT on thesepatients!
Prostate Cancer Oligometastases: Picchio M, Berardi G, Fodor A, et al. Eur J Nucl Med Mol Imaging 2014Incerti E, Fodor A, Mapelli P, et al. J Nucl Med 2015Fodor A, Berardi G, Fiorino C, et al. BJU International 2017

• Multi-institutional evaluation of SBRT
• Pts with diagnosis of up to 3 positive LN (73 LN/60 pts), or bone (43 mts/36pts), or visceral (1 lung/1 pts, 1 liver/1 pts) mts at choline (92 pts) or FDGPET/CT (24 pts); 2 pts had bone/LN and visceral mts for a total of 163 mts/119 pts treated with SBRT
• Median PSA at first documented metastases= 4.0 (1.6-8.8)ng/ml, medianinterval from diagnosis to mts: 4.7 (2.7-6.6) years
• DPFS= 21 (15-26) months; LPFS 3 years = 79% for biologically effective dose≤100 Gy and 99 % for >100 Gy; DPFS 3 years= 31%, DPFS 5 years= 15%
Ost P, et al. Progression-free Survival Following Stereotactic BodyRadiotherapy for Oligometastatic Prostate Cancer Treatment-naiveRecurrence: A Multi-institutional Analysis. European Urology 2016

RPM Respiratory Gating™ System
TM : Varian Medical System Gating School Copenhagen
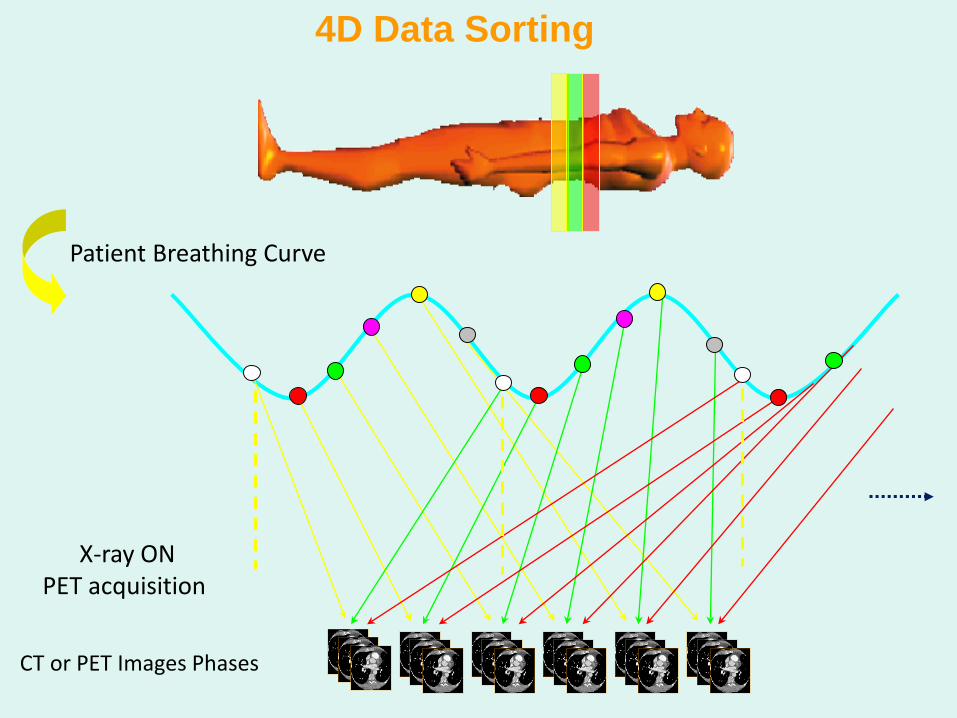
X-ray ONPET acquisition
CT or PET Images Phases
4D Data Sorting
Patient Breathing Curve

Goal:Define the target volume and the volume of space that encompasses tumor motion.

HSR , Milan
4D-PET/CT CONTOURING
exp
insp sum
st
BTV

HSR , Milan
4D-PET/CT CONTOURING
ITV ITV

4D CT
Cine Review
HSR-Milano
ITV

4D CT
Cine Review
HSR-Milano
ITV

Standard Planning
Volume (18.64 cc)
4D-PET/CT
Based Planning
Volume (6.79 cc)
↓ 64%
HSR-Milano
Lung Lesion
CT
PET

28 USA Centers (+ 1 Australian+1Germany)702 Patients: 577 evaluable
Median dose : 50 Gy (range 25/75%48–54) delivered in 3Fr
Median LC for all patients :53 ms nodifference by primary histologic type
Ricco A, et al.Lung metastases treatedwith stereotactic body radiotherapy: theRSSearch ® patient Registry experience.Radiation Oncology 2017

5) Adaptive RT rectal cancer @ San Raffaele: the approach of boosting the shrinking tumour
Background: 2007-2009 moderately Hypo (2.3 Gy/fr, 18 fr, 41.4 Gy + oxaliplatin/5FU). Daily IGRT Tomo; based on LQ-model to be equivalent to bi-fractionation (45Gy, 2.5Gy/day)
Reported results for the first 100 pts: G3 GI:9%; pcR:28%. Compares well with historical experience with bi-fractionation (reduced tox with Tomo)
15Gy
15Gy
30Gy
39.3Gy
15Gy30Gy
30Gy
39.3Gy
15Gy

Adaptive Radiation Therapy: RECTAL CANCER• The rectum was retrospectively contoured on the daily
Megavoltage images (MVCT) of six patients previously treated with TomoTherapy® System. The variations of rectum volume during TomoTherapy® System were examined.
• Rectal volume shows a linear decrease of 58.2 % between the start and end of the treatment (range: 28.6%-75.4%); most of the rectum volume variation was observed in the first half of the treatment with an average reduction of 50%.
• A first estimate of optimized margins for adaptive RT with concomitant boost to the tumour was achieved by expanding the rectal contouring during the initial MVCT s and subsequently during the second half of the treatment with different margins (0.5, 0.7, 1, 1.5, 2 cm).
• In the second half of the treatment, more than 90% (range: 82.4%-100%) of the rectal volume union was contained within a margin of 0.5 cm, while a margin of at least 1 cm is necessary to obtain the same coverage in the first part of the treatment.
• Based on the results of this investigation, a pilot adaptive approach was started in which a concomitant boost is delivered on the last 6 treatment fractions.

DOSE DISTRIBUTION WITH TOMOTHERAPY® SYSTEM
PTV1 PTV2
First phase no boost 100% 2,3Gy/f
Adaptive phase 100% 3Gy/f
ACUTE TOXICITY G1-2 G3
Diarrhoea 25 (50%) 9 (18%)*
Proctitis 27 (54%) 2(4%)
Rectal bleeding 7 (14%) 1 (2%)Cistitis 7 (14%) -Skin erithema 11 (22%) -
*All G3 in the first phase, only in women;No G4 toxicityoccured
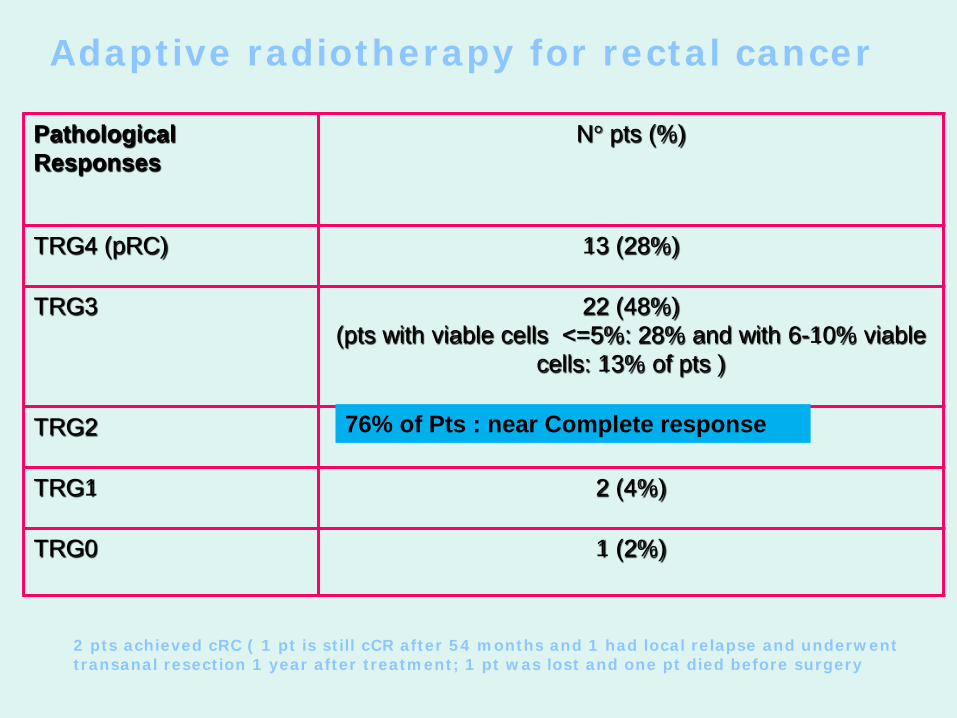
PathologicalResponses
N° pts (%)
TRG4 (pRC) 13 (28%)
TRG3 22 (48%)(pts with viable cells <=5%: 28% and with 6-10% viable
cells: 13% of pts )
TRG2 6 (13%)
TRG1 2 (4%)
TRG0 1 (2%)
Adaptive radiotherapy for rectal cancer
2 pts achieved cRC ( 1 pt is still cCR after 54 months and 1 had local relapse and underwent transanal resection 1 year after treatment; 1 pt was lost and one pt died before surgery
76% of Pts : near Complete response

• Invaluable solution to the treatment of selective tumours/lesions located close to critical structures and/or subject to organ motion
• Salvage of recurrent and metastatic lesions
• Opportunity to treat selective early stage malignancies like the prostate and lung carcinoma
• Management of intractable trigeminal neuralgia.
• Arteriovenous malformation for patients who are not suitable for invasive surgery
• Currently innovative experimental indications for radiosurgery to treat functional disorders like obsessive compulsive disorder (OCD), depression, Parkinson, atrial fibrillation, etc. are underway.
CONCLUSIONS

• Patients today are more informed: I reported to myadministration how many patients asked for thereduction of the radiation treatment duration
Loss of patients (prostate, lung……)
• Economic advantage
In Italy the treatment is not paid per fraction, but as a package ( 7.000 €)
Even though a CyberKnife® System treats less patients per day, more patients/yearwould be treated
How I convinced my administration to buy aCyberKnife® System?