rationale for vegfr-targeted therapy in rcc - kca 2013 - … · 2014-05-14 · – rcc recurs in...
TRANSCRIPT

Rationale for VEGFR-targeted Therapy in RCC
Tim Eisen
EIKCS, Budapest, May 2013

Tim Eisen - Disclosures
Company Research
Support
Advisory Board Trial
Management
Group
Honoraria
Astra Zeneca + + +
Astellas + +
Aveo + + +
Bayer + + + +
GSK + + + +
Immatics +
Pfizer + + +
Roche + +

We need effective therapies in the adjuvant setting
– RCC recurs in ~20–60% of patients post-nephrectomy,1,2
– Incidence and time to recurrence depend on risk score 2,3
– Median time to recurrence
5–9 months in patients with pTxN+ tumours3
35–38 months in patients with pT1 tumours3
Adjuvant therapy: a key unmet need
0.9
27
39
64
2
70
7
0
10
20
30
40
50
60
70
80
pT1 pT2 pT3 pTxN+
Tumour type pre-nephrectomy*
Pro
po
rtio
n o
f p
atie
nts
wit
h r
ecurr
ence
(%
)
1. Lam JS et al. Curr Urol Rep 2005;6:7–18;
2. Eisen T et al. Eur Urol Suppl 2007;6:492–8; 3. Kassouf W et al. Can Urol Assoc J 2009;3:73–6.
*Kassouf et al reported data from multiple studies; within each tumour
type, each bar represents a different study

Metastases-free survival after resection
Leibovich BC et al. Cancer 2003;97:1663–71.

Angiogenesis is one of many steps
leading to metastasis……
Fidler & Ellis, Nature Medicine (2000)

Angiogenesis – Key Pathways
•Tumour growth requires angiogenesis
•Interacting network of signals
•Positive & negative regulators
•Signals from various cell types
•Signals to various cell types
•Endothelial cells proliferate, migrate &
form new vessels
•Pericytes stabilise vasculature
Ferrara & Kerbel, Nature 2005
Poorly understood VEGFR inhibitor effects
Direct effect on tumour
Immunomodulation
– Inflammation
– Tumour immunity
“Off target” effects of small molecules

Lessons from colorectal cancer
Results have been reported for two Phase III trials of adjuvant
bevacizumab in colorectal cancer:
Neither study met its primary endpoint
However are there still lessons that we can learn?
NSABP C-081
• mFOLFOX6
• mFOLFOX6 + bevacizumab
Bevacizumab administered 1 year
AVANT2
• FOLFOX4
• FOLFOX4 + bevacizumab
• XELOX + bevacizumab
Bevacizumab administered 48 wks
1. Allegra CJ et al. J Clin Oncol 2011, De Gramont A et al. Lancet Oncol 2012; .

AVANT – study design
Primary endpoint: DFS
Secondary endpoints: OS, safety De Gramont A et al. Lancet Oncology 2012.
Resected colon
cancer
(high-risk stage II
and stage III)
(n=3450)
FOLFOX4
(24 weeks)
FOLFOX4
(24 weeks)
Bevacizumab 5 mg/kg q2w with chemotherapy and 7.5
mg/kg q3w monotherapy
(48 weeks)
XELOX4
(24 weeks)
Bevacizumab 7.5 mg/kg q3w
(48 weeks)

Disease-free survival in AVANT
Disease-free survival
at 1 year
Disease-free survival
at 3 years
0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
Favours
bevacizumab addition
Favours
chemo only
Favours
bevacizumab addition
Favours
chemo only
FOLFOX4 + bevacizumab
XELOX + bevacizumab
De Gramont A et al. Lancet Oncol 2012.

Post-operative bevacizumab in
ovarian/peritoneal/fallopian tube cancer
Primary endpoint: Progression-free survival
Secondary endpoints: Overall survival, safety, QoL
+ Placebo
+ Bevacizumab (15 mg/kg)
Inclusion criteria:
• Patients with epithelial ovarian,
primary peritoneal or fallopian tube
cancer
• Disease stage after debulking surgery:
Stage III optimal or suboptimal;
Stage IV
• Less than 1–12 weeks since debulking
surgery
• No prior chemotherapy
RA
ND
OM
IZE
1:1
:1
+ Bevacizumab (15 mg/kg)
N = 1873
Placebo
Bevacizumab (15 mg/kg)
Placebo
Cytotoxic therapy
(6 cycles) Maintenance
therapy
(16 cycles) Carboplatin AUC 6
+ paclitaxel 175 mg/m2
Burger RA et al. J Clin Oncol 2010;28:abstract LBA1. QoL, quality of life.

Key findings in ovarian/peritoneal/fallopian
tube cancer
Three-arm Phase III study of 1st-line systemic therapy after debulking surgery in
advanced epithelial ovarian cancer, primary peritoneal cancer, or fallopian tube cancer
– Regimen 1: Standard chemotherapy + placebo, then maintenance placebo
– Regimen 2: Standard chemotherapy + Bev, then maintenance placebo
– Regimen 3. Standard chemotherapy + Bev, then maintenance Bev
0
0.2
0.4
0.6
0.8
1.0
1.2
Significantly lower risk of
1st progression/death in patients with
maintenance bevacizumab (regimen 3 vs
regimen 1;
p < 0.0001)
Trend toward lower risk of 1st
progression/death with regimen 2 vs
regimen 1
Favours add-on bevacizumab Favours standard therapy
Burger RA et al. J Clin Oncol 2010;28.
Hazard ratio
Bev, bevacizumab

...but there are limitations to cross-study
and cross-tumour comparisons
Biology can vary considerably between tumour types
Outcome with one particular agent may not indicate outcome
with a different agent
CRC and ovarian cancer studies added bevacizumab to existing
adjuvant regimen
– In RCC, there is no approved adjuvant regimen; studies are
evaluating antiangiogenic agents as monotherapy
Adjuvant data in RCC are urgently needed and eagerly awaited!

Many questions to consider…
Do we need to inhibit VEGFR as potently in micrometastases as
strongly as in macrometastases?
Is long-term low dose VEGFR inhibition the way to go?
Novel immunotherapeutic options
Other modalities
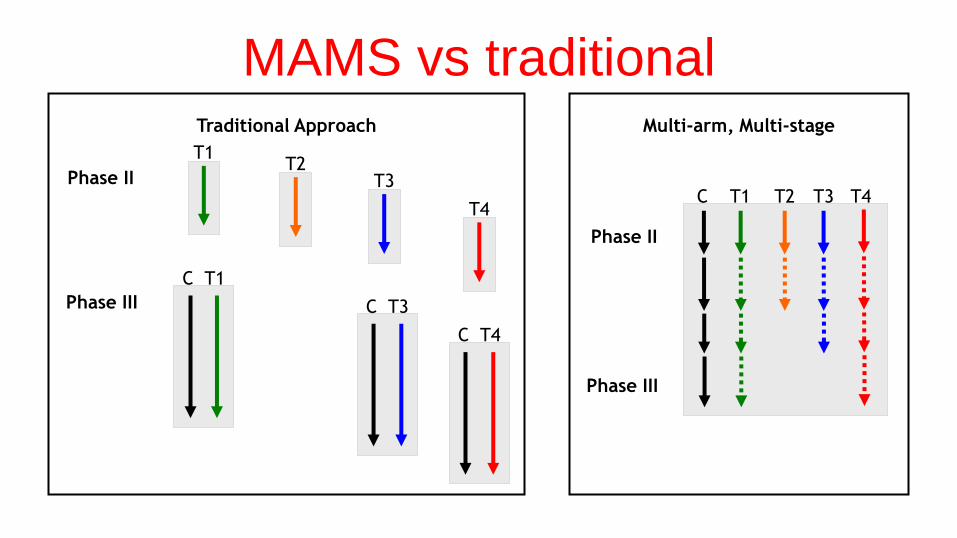
MAMS vs traditional
Traditional Approach
Phase II
Phase III
T1
C T1
T2 T3
C T3
T4
C T4
Multi-arm, Multi-stage
T2 T3 T1 C T4
Phase II
Phase III