ready, set, goal - review of optometry
TRANSCRIPT
Women In OptometryWomen In Optometry
Dedicated to the interests of women ODs
September 2011
SUPPLEMENT TO
GOAL!Dr. Janelle Davison is making plans to succeed in practice
Ready,Set,
WO3Q11:WO 2Q08-SK 8/23/11 10:09 PM Page 1

The American Optometric Foundation has announcedthe recipients of the 2011 Vistakon Award ofExcellence in Contact Lens Patient Care, which rec-ognizes outstanding fourth-year student clinicianswho have demonstrated excellent overall knowledge
of the contact lens field plus skillful, considerate and pro-fessional care of contact lens patients during their opto-metric education. Several women were recipients, includingStephanie Ratermann, OD; Lauren Evonne Quaine, OD;Yin-Yin Aung, OD; Natalie Cathy Pham, OD; BrittanyNelson, OD; Lindsey Beth Barouh, OD; Veronica Woi, OD;Katherine Paulsen, OD; Dana Beth Pollack, OD; SheilaKarst Morris, OD; Pam Satjawatcharaphong, OD; KatieWicks, OD; and Tanya Marie Polonenko, OD. Each winnerwill receive a $1,000 award and a personalized plaque com-memorating her accomplishment.
The American Optometric Foun-dation and VISTAKON®, Division ofJohnson & Johnson Vision Care, Inc.,announced the recipients of several2011 residency awards. ChristenKenrick, OD, of New England College ofOptometry, and Lindsay A. Sicks, OD,
of NortheasternState UniversityOklahoma College ofOptometry, receivedthe Dr. George W.Mertz Contact LensResidency Awards.Jenelle L. Mallios,OD, and Yos M.Priestley, OD, bothof the New EnglandCollege of Optometry,
received the Dr. Terrance IngrahamPediatric Optometry Residency Awards.Each will receive $4,000 toward her grad-uate education that includes a $750 travel fellowship toattend the Annual Meeting of the American Academy ofOptometry in Boston, October 12-15.
The Fresh Start of Fall
There’s something refreshing about the fall. Theair is crisp. School playgrounds are filled with
activity. There’s some sense of urgency to accomplishtasks before the days grow cold.
This issue of Women In Optometry seems filled with the promise of freshstarts, too. Members of the class of 2011 are settling in as practitioners, resi-dents or in other roles. These young ODs bring their clinical training and enthu-siasm into the profession—and it is impressive. Just look at our feature on thetop graduates.
Other stories, too, examine the energy of young ODs. Our cover story with Dr.Janelle Davison and another with Dr. Amie Gisbert show how these young womenare cultivating practices that are sure to make an impact in their communities.
That’s not the only way to make an impact, however. Our story with Dr.Katherine Mastrota, who serves as a director of a specialty referral center, providesan example of how the dialogue and cooperation between ODs and other eye careprofessionals can work. It’s all about relationships, an angle explored in our storywith Dr. Wanda Tort, Dr. Ana Maria Pico and Dr. Maria Gorbea, who not only developedtheir partnership relationship but also are shifting the way Puerto Ricans perceiveprimary care optometry.
Be sure to read the results from our latest survey on the continuing integrationof medical services into optometric practices. It shows that the vast majority ofwomen routinely treat certain medical conditions, primarily dry eye, ocular allergiesand ocular infections. But it also shows significant interest in treating or managingpatients with conditions such as glaucoma and age-related macular degeneration.
It’s an exciting time of year and an exciting time for the profession. Enjoy thesplendor.
Marjolijn Bijlefeld, Director of Custom PublicationsPractice Advancement Associates
Comments on Women In Optometry can be sent to [email protected] or fax 540-242-3438
SEPTEMBER 2011
Women In Optometry is published quarterly by the Professional Publications Groupof Jobson Medical Information, publisher of Review of Optometry,Review of Cornea & Contact Lenses and Review of Ophthalmology.
Sponsors:Allergan • CIBA VISION • Marchon
Review of Optometry • The Vision Care InstituteAddress advertising inquiries to Scott Tobin, advertising production
manager, Jobson Professional Publications Group,11 Campus Blvd., Suite 100, Newtown Square, PA 19073, at
[email protected] or call 610-492-1011.
Naheed Ahmad, ODRoswell, Ga.
Louise Sclafani, OD,FAAOChicago, Ill.
Charlotte Tlachac,OD, FAAOAlameda, Calif.
WO Advisory Panel
Ann M. Hoscheit, ODGastonia, N.C.
Elise Brisco, OD,FAAOLos Angeles, Calif.
Kimberly K.Friedman, ODMoorestown, N.J.
Shout Out
Women In Optometry September 2011
Marjolijn Bijlefeld
Page 3
Publisher:Executive Editor:
Director of Custom Publications, Practice Advancement Associates:Associate Editor:Creative Director:Graphic Designer:
Al GrecoRoger Mummert Marjolijn Bijlefeld Maggie Biunno Stephanie Kloos DonoghueBarbara W. Gallois
Awards and Kudos
WO
Dr. Sicks
Dr. Mallios
Dr. Priestley
WO3Q11:WO 2Q08-SK 8/23/11 10:09 PM Page 3

ow many patients needing refrac-tive correction in your practicewould like to wear contact lensesif given the opportunity? Ifyour response is that many
would, there might be a disconnectbetween the services your practicedelivers and patient desires. In theaverage independent practice, only30 percent of eye exams performedare contact lens exams.
The Management and BusinessAcademy™ (MBA) and First PracticeAcademy™ (FPA) detailed practiceprofiles point out the huge oppor-tunity that exists in convertingsome of those spectacle exampatients into contact lens patients.
Concrete strategies to increasingyour contact lens fits and contact
lens-related revenue are outlined and discussed in greater detail inthe MBA publication, Best Practices of Contact Lens Management 2011.
Stop waiting for patients to ask for contact lenses. Look atthe results of the Enhancing the Approach to Selecting Eyewear(EASE) study, which set out to determine the effect of applyingcontact lenses to patients prior to sending them into the opticaldispensary to select frames. Eighty-five percent of the testpatients thought that wearing contact lenses was helpful whilechoosing frames, and test patients spent an average of 32 per-cent more on eyeglasses than control patients. Furthermore, 33percent of test patients purchased contact lenses within threemonths, compared to 13 percent of control patients.1
Here are additional best prac-tices to converting eyeglasses-onlypatients to contact lens exams.
1. Encourage all eyeglasseswearers about to enter high schoolto try contact lenses. Surveys showthat interest in trying contact lensesis higher among teenagers than inany other age group. Every teeneyeglasses wearer should be offereda free trial of contact lenses.
2. Ask every patient wearing eyeglasses only: “Are theretimes when you would rather not wear eyeglasses?” People engagedin outdoor or athletic activities might be interested in part-timecontact lens wear. Many early presbyopes could be great candidatesfor multifocal contact lenses. Others who want to look their bestfor special occasions will also respond positively to this question.
3. Elicit interest in contact lenses on medical historyand lifestyle questionnaires. Also, ask if patients ever worecontact lenses previously. This question will open the door to adiscussion on improvements in comfort, optics and conven-ience that might make their former complaints moot.
4. Present end benefits, not technical lens features.Focus on the life-enhancing end benefits, not on technical fea-tures of contact lenses.
5. Preface each recommendation with the phrase, “I rec-ommend.” This wording has much greater impact and professionalcredibility than weaker phrases such as, “Could I make a sugges-tion” or “You might want to think about...” or “One option is...”Prefacing recommendations with the word “I” (”I would like youto...”) conveys personal interest in the patient’s welfare.
6. Offer daily disposable trial lenses to eyeglassespatients as they select frames. EASE study participants suggesttelling patients who are offered a free contact lens trial duringframes selection that there is no obligation to buy contact lensesand that the lenses are offered solely as a convenience.
The bottom line is that contact lens patients yield higherannual revenues and profits to a practice (see chart above).
MBA Offers SupportDownload a copy of the Best Practices of Contact Lens
Management 2011 report from mba-ce.com. The 32-page publica-tion provides guidance on many facets of contact lens manage-ment, including how to track key metrics, reduce transaction costs,develop a sound pricing strategy and improve the product mix.
Beverly Korfin, MBA, is senior manager of marketing opera-tions for CIBA VISION®.
1Atkins et al. Enhancing the approach to selecting eyewear (EASE): A multi-centre, practice-based study into the effect of applying contact lenses prior to spectacle dispensing. ContactLens and Anterior Eye. 2009;32(3)103-107.
By Beverly Korfin, MBA
It’s Your Businessalso appears on the web site ofWomen of Vision.Check it out atwovonline.org.
Sponsored by CIBA VISION®
It’s Your Business
2011-07-0963
The Contact Lens Correlation
H Annual Revenue and Profit fromSoft Lens and Eyeglasses-Only Patients
Annual per patientGross revenue Gross profit
Soft lens patientsSoft lens purchases $110.00 $51.70Exam revenue1 $83.75 $83.75Eyeglasses purchases2 $70.24 $42.84Total $263.99 $178.29
Eyeglasses-only patientsEyeglasses purchases3 $93.93 $57.29Exam revenue4 $41.40 $41.40Total $135.33 $98.69
1Average interval 18 months2Assumes 80% ever purchase eyeglasses; average interval 34 months, average purchase = $1993Average interval between purchases: 29 months; average purchase = $2274Average interval 26 months5Average gross profit margin = 61%
Sources: Practice Advancement Associates estimates based on industry audits, VisionWatch, contactlens industry audits, ABB CONCISE Soft Lens Retail Price Monitor, MBA Practice Profile benchmarks
5
5
Complete Eye Exams Performed in Optometric Practice
58% 30%
New practicesEstablished practices
12%
Source: MBA and FPA Practice Profile, 2010
“Healthy eye”exams
Contact lensexams
Eyeglass exams
58% 30%
12%
WO3Q11:WO 2Q08-SK 8/23/11 10:10 PM Page 4

Page 5CLASS ACTS
essica R. Czerny, OD, of Williamsburg, Mich., was hon-ored as the valedictorian of theclass of 2011 at the MichiganCollege of Optometry. Dr. Czernyand her husband graduatedtogether, and they were looking
for jobs in the same town. Dr. Czerny wouldlike to find a private practice with anemphasis in pediatrics/vision therapy.
Amy Buchanan, OD,of Kingsport, Tenn.,was named valedicto-rian at Inter American University ofPuerto Rico School of Optometry. Dr.Buchanan is completing a residency atMount Home VA Medical Center inJohnson City, Tenn.
Brandy DanielleJohnson, OD, and Iris
Maureen Miller, OD, were the New EnglandCollege of Optometry’s two valedictorians
this year. Dr. Johnson,of Red Deer, Alberta,Canada, and her hus-band moved toAtlanta, where sheplans to start hercareer, participate inoverseas optometric missions and eventu-ally return to Canada to start an independ-ent practice. Dr. Miller, of Watford City,N.D., started work in Warwick, R.I., at anOD/MD practice,
which is affiliated with Brown Universityand Life Span Hospital.
Northeastern State University College ofOptometry’s top-ranked graduate wasJessica Leigh Lucas, OD, of Plano, Texas.Following graduation, Dr. Lucas began
working in a privatepractice in Norman,Okla.
Cheryl Marie Baker, OD, of ClintonTownship, Mich., was valedictorian of hergraduating class at Nova SoutheasternUniversity College of Optometry. Dr. Bakerwas seeking a position in the Denver metroarea.
Stacy Diane Kessler, OD, of WestBloomfield, Mich., graduated at the top of her class at The OhioState University College of Optometry. Dr. Kessler is completing a
J residency program at the Louis StokesCleveland VA Medical Center in NortheastOhio.
Pacific UniversityCollege of Optometry’s2011 valedictorianwas Gina MarieSilvers, OD, ofSartell, Minn. Dr.Silvers was looking
for an independent/group practice settingin the Pacific Northwest.
Dana Webster, OD, of Elizabethtown, Pa.,graduated as valedictorian of her class at thePennsylvania College of Optometry at SalusUniversity. Dr. Webster is completing a resi-dency at EyeCare Professionals, P.C., inHamilton Square, N.J., affiliated with theSouthern College of Optometry, and she willfocus on vision therapy, rehabilitative optom-etry and pediatrics.
Shora Mobin Ansari,OD, of Yorba Linda, Calif., graduated asvaledictorian at Southern California Collegeof Optometry. Dr. Ansari plans to join a pri-vate practice in the Orange County area.
Southern College ofOptometry had twotop graduates: HeidiHunt Herring, OD, ofKnoxville, Tenn., and Nicole Kosciuk, OD,of Arlington Heights, Ill. Dr. Herring movedto East Tennessee to practice with herfather, John Hunt, OD, a 1984 SCO gradu-ate, and her husband, Ben Herring, OD, a2010 SCO graduate. Dr. Kosciuk started anocular disease/low vision residency at theJesse Brown VA Medical Center in Chicago.
State University ofNew York StateCollege of Optometry’s2011 valedictorianwas Nikki A. Yee,OD, of Miami, Fla. Dr.Yee is completing aresidency in primaryeye care and low
vision rehabilitation at the VA West Haven,Conn.
The class of 2011 has entered the workforce, ready to make its mark.These 18 women graduated as valedictorians or with the highest GPAin their graduating classes. Congratulations to all the graduates.
Continued on page 6
Dr. Czerny
Dr. Buchanan
Dr. Johnson
Dr. Miller
Dr. Lucas
Dr. Baker
Dr. Kessler
Dr. Silvers
Dr. Webster
Dr. Ansari
Dr. Hunt Herring
Dr. Kosciuk
Dr. Yee
Women In Optometry September 2011Gra
duat
ion
© D
alla
seve
ntsin
c |
Dre
amsti
me.
com
WO3Q11:WO 2Q08-SK 8/23/11 10:12 PM Page 5

Page 6
OD, of Indiana University School of Optometry; Lauren Nelson,OD, of University of Houston College of Optometry; and AmandaPowers, OD, of New England College of Optometry. WO
Vision Monday’s “Most Influential Women in Optical”
special report recognizes leaders in the optical industry,and for the past six years, VM has also praised recentgraduates who stood out in their optometry schoolclasses. The graduates mentioned in VM’s “Class of 2011
Special Report” were selected by their schools for a number ofreasons, including their academic achievement, awards and schol-arships, research, volunteer work and participation in professionalorganizations.
WO congratulates these recent grads for being selected forthis recognition: Sarah Brehm, OD, of Nova SoutheasternUniversity College of Optometry; Jessica Carson, OD, ofUniversity of Missouri–St. Louis College of Optometry; KellyChajka, OD, of SUNY College of Optometry; Carla Gilbertson, OD,of Michigan College of Optometry; Britta Hansen, OD, of Schoolof Optometry, University of California–Berkeley; Brigitte Keener,OD, of Southern College of Optometry; Melissa Liepins, OD, ofIllinois College of Optometry; L.A. Lossing, OD, of Ohio StateUniversity College of Optometry; Jessica Lucas, OD, of NorthernState University Oklahoma’s College of Optometry; Kacie Monroe,
RecentGraduates
in the Spotlight
Gra
duat
ion
© D
alla
seve
ntsin
c |
Dre
amsti
me.
com
Continued from page 5
University of Alabama at BirminghamSchool of Optometry’s top graduate wasSheila Karst Morris, OD, of Wallace, Idaho.Dr. Morris is completing an ocular diseaseresidency at Omni Eye Services of Atlanta.
Stephanie Burns, OD,received the honor ofthe Beta Sigma Kappa(BSK) Silver Medal atthe University ofCalifornia, Berkeley,School of Optometry.Dr. Burns, of DuBois,Pa., is interested inpracticing in a privateor group practice inthe Seattle area.
Lauren Rinando Nelson, OD, of Beaumont,Texas, graduated from the University ofHouston College of Optometry with a 4.0GPA. Dr. Nelson plans to return to and work
in a practice in her hometown.
More Brainpower
Several men graduated at the top of their class, as well, some sharing the titlewith a female classmate.
Nicholas Lillie, OD, Illinois College of OptometryAnthony VanAlstine, OD, Indiana College of OptometryKelvin Kiu Wing So, OD, Pacific University College of OptometryMatthew Patrick McGuigan, OD, Pennsylvania College of Optometry at Salus UniversityGuillaume Lafleur, OD, University of Montreal School of Optometry
Women In Optometry September 2011
Jessica “Jessie” A. Carson, OD, of St.Louis, Mo., was the University of Missouri–St. Louis, College of Optometry’s top grad-uate. She is completing aresidency at Fayetteville, Ark.
University of WaterlooSchool of Optometry’s vale-dictorian was BreanneFacey, OD, of Waterdown,Ontario. Dr. Facey begins hercareer in the Burlington,
Ontario area, with a focus on pediatrics andvision therapy.
Dr. Morris
Dr. Burns
Dr. Nelson
Dr. Carson
Dr. Facey
CLASS ACTS
WO
Dr. Brehm Dr. Carson Dr. Chajka Dr. Gilbertson
Dr. Hansen Dr. Keener Dr. Liepins Dr. Lossing
Dr. Lucas Dr. Monroe Dr. Nelson Dr. Powers
WO3Q11:WO 2Q08-SK 8/23/11 10:14 PM Page 6
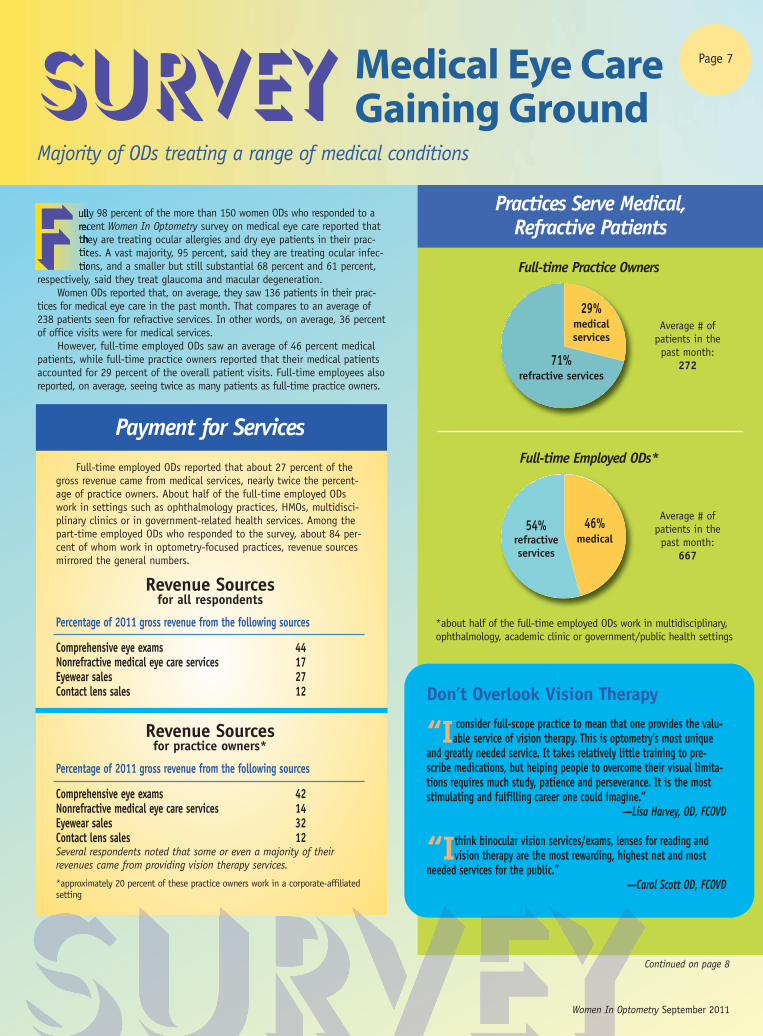
Practices Serve Medical,Refractive Patients
Full-time Practice Owners
Page 7
Survey Medical Eye CareGaining Ground
Majority of ODs treating a range of medical conditions
Don’t Overlook Vision Therapy
“I consider full-scope practice to mean that one provides the valu-able service of vision therapy. This is optometry’s most unique
and greatly needed service. It takes relatively little training to pre-scribe medications, but helping people to overcome their visual limita-tions requires much study, patience and perseverance. It is the moststimulating and fulfilling career one could imagine.”
—Lisa Harvey, OD, FCOVD
“Ithink binocular vision services/exams, lenses for reading andvision therapy are the most rewarding, highest net and most
needed services for the public.”—Carol Scott OD, FCOVD
ully 98 percent of the more than 150 women ODs who responded to arecent Women In Optometry survey on medical eye care reported thatthey are treating ocular allergies and dry eye patients in their prac-tices. A vast majority, 95 percent, said they are treating ocular infec-tions, and a smaller but still substantial 68 percent and 61 percent,
respectively, said they treat glaucoma and macular degeneration.Women ODs reported that, on average, they saw 136 patients in their prac-
tices for medical eye care in the past month. That compares to an average of238 patients seen for refractive services. In other words, on average, 36 percentof office visits were for medical services.
However, full-time employed ODs saw an average of 46 percent medicalpatients, while full-time practice owners reported that their medical patientsaccounted for 29 percent of the overall patient visits. Full-time employees alsoreported, on average, seeing twice as many patients as full-time practice owners.
F
Full-time Employed ODs*
29%medicalservices
71% refractive services
54%refractiveservices
46% medical
Continued on page 8
Women In Optometry September 2011
Payment for ServicesFull-time employed ODs reported that about 27 percent of the
gross revenue came from medical services, nearly twice the percent-age of practice owners. About half of the full-time employed ODswork in settings such as ophthalmology practices, HMOs, multidisci-plinary clinics or in government-related health services. Among thepart-time employed ODs who responded to the survey, about 84 per-cent of whom work in optometry-focused practices, revenue sourcesmirrored the general numbers.
Revenue Sourcesfor all respondents
Percentage of 2011 gross revenue from the following sources
Comprehensive eye exams 44Nonrefractive medical eye care services 17Eyewear sales 27Contact lens sales 12
Revenue Sourcesfor practice owners*
Percentage of 2011 gross revenue from the following sources
Comprehensive eye exams 42Nonrefractive medical eye care services 14Eyewear sales 32Contact lens sales 12Several respondents noted that some or even a majority of their revenues came from providing vision therapy services.
*approximately 20 percent of these practice owners work in a corporate-affiliatedsetting
Average # ofpatients in thepast month:
272
Average # ofpatients in thepast month:
667
*about half of the full-time employed ODs work in multidisciplinary,ophthalmology, academic clinic or government/public health settings
WO3Q11:WO 2Q08-SK 8/23/11 10:16 PM Page 7

Page 8
Four-Year Shift
“Due to managed care reducing reimbursement for comprehensiveexams and diagnostic tests, my gross receipts are 45 percent
services and 55 percent optical sales. In 2007, my gross was 65 percentservices and 35 percent optical sales. I am reducing my cost-of-goodssold in order to increase profits in optical sales. I must do this to com-pensate for the decrease in insurance reimbursements forservices.”
—2003 graduate and practice owner
Asmaller percentage of men responded to the WO survey, but thosewho did respond generally say that they treat medical conditions at
a higher rate and are more comfortable with the coding and billingissues. Significantly, a much higher percentage of men who respondedfeel that medical eye care is financially lucrative, disagreeing completelyor somewhat with the statement that medical services yield less revenueper hour (45 percent of men compared to 31 percent of women).
The Men’s View
SurveyContinued from page 7
WO
Women In Optometry September 2011
A Complex Business
As one young practice owner, a 2005 graduate, wrote, “I want tostart billing more medical, but it is so hard to get started, get on theright panels and bill things correctly. Most current classes are veryexpensive, and it’s hard to get good one-on-one time with the instruc-tor. I wish there was a peer group or something like that to help.”
More than one-third of the women who responded seemed toagree with her that the business of medical billing and coding pushesthem outside of their comfort zone.
I am uncomfortable with the complexity of medical billing and coding.
Others, like Tamara Hill-Bennett, OD, of Philadelphia, say it’s anessential business skill. “Understanding the complexity of billing isan area where we as practitioners are lacking. I am of the mindset asa practice owner that it is important for me to understand the billingprocess to ensure that my staff is billing properly, as well as that Iam filling out the superbill correctly. At the end of the day, becausewe rely on the insurance companies to pay us, so we have to educateourselves with this process.”
23%
15%
28%13%
21%
Practice Owners(full and part time)
Employed ODs(full and part time)
16%
23%
18% 18%
25%
Fulfilling but Not Always Financially Rewarding
Women ODs reported that they generally found providing medicaleye care to be the most fulfilling and stimulating aspect of theirpractice. Several women who provide vision therapy services specifi-cally mentioned the professional and personal fulfillment derived fromtheir work.
I find medical eye care to be the most fulfilling and stimulating aspect of my practice.
I believe medical eye care services yield less revenue per hour thando prescribing and dispensing corrective devices.
32%
40%
8%5%
15%
23%
47%
9%7%
14%
Practice Owners(full and part time)
46%
28%
11%1%
14%
Employed ODs(full and part time)
Overall
Overall
13%
28%20%
11%
28%
Look at the difference, however,between ODs who are practice own-ers compared to employed ODs.Employed ODs seem to enjoy med-ical eye care to a greater degree.
However, women are divided intheir opinions on the remunerativevalue of providing these services.
As one practice owner wrote,“Reimbursement for medical eye careis quite low since the insurancecompanies usually reimburse lessthan 20 percent of our office visitcharge. Getting about $15 for treat-ing a red eye doesn’t really go veryfar financially.”
The Future of Medical Eye Care
Within 20 years, medical eye care is likely to be the dominant source ofrevenue of independent ODs.
Women ODs seem to agree that medicaleye care will gain as a source of revenuefor independent ODs.
14%
37%
16%5%
28%
Pie Key
Agree Agree Neither agree Disagree Disagree completely somewhat nor disagree somewhat completely
See pie key at bottom of page. See pie key atbottom of page.
WO3Q11:WO 2Q08-SK 8/23/11 10:17 PM Page 8
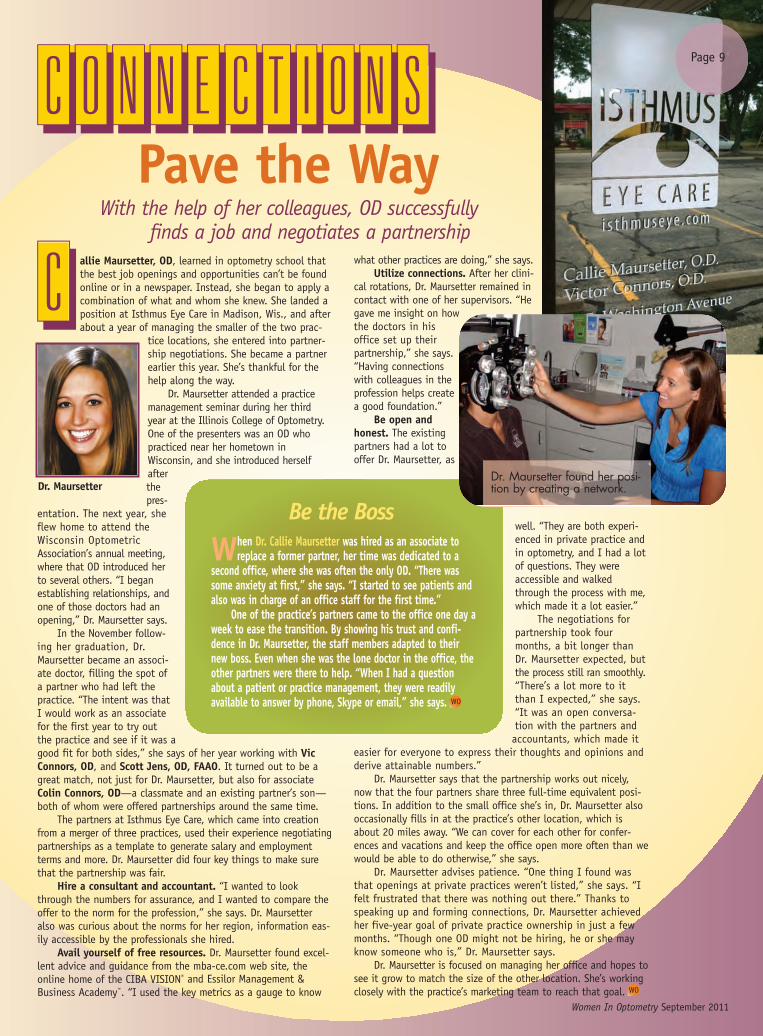
Pave the WayWith the help of her colleagues, OD successfully
finds a job and negotiates a partnershipallie Maursetter, OD, learned in optometry school thatthe best job openings and opportunities can’t be foundonline or in a newspaper. Instead, she began to apply acombination of what and whom she knew. She landed aposition at Isthmus Eye Care in Madison, Wis., and afterabout a year of managing the smaller of the two prac-
tice locations, she entered into partner-ship negotiations. She became a partnerearlier this year. She’s thankful for thehelp along the way.
Dr. Maursetter attended a practicemanagement seminar during her thirdyear at the Illinois College of Optometry.One of the presenters was an OD whopracticed near her hometown inWisconsin, and she introduced herselfafterthepres-
entation. The next year, sheflew home to attend theWisconsin OptometricAssociation’s annual meeting,where that OD introduced herto several others. “I beganestablishing relationships, andone of those doctors had anopening,” Dr. Maursetter says.
In the November follow-ing her graduation, Dr.Maursetter became an associ-ate doctor, filling the spot ofa partner who had left thepractice. “The intent was thatI would work as an associatefor the first year to try outthe practice and see if it was agood fit for both sides,” she says of her year working with VicConnors, OD, and Scott Jens, OD, FAAO. It turned out to be agreat match, not just for Dr. Maursetter, but also for associateColin Connors, OD—a classmate and an existing partner’s son—both of whom were offered partnerships around the same time.
The partners at Isthmus Eye Care, which came into creationfrom a merger of three practices, used their experience negotiatingpartnerships as a template to generate salary and employmentterms and more. Dr. Maursetter did four key things to make surethat the partnership was fair.
Hire a consultant and accountant. “I wanted to lookthrough the numbers for assurance, and I wanted to compare theoffer to the norm for the profession,” she says. Dr. Maursetteralso was curious about the norms for her region, information eas-ily accessible by the professionals she hired.
Avail yourself of free resources. Dr. Maursetter found excel-lent advice and guidance from the mba-ce.com web site, theonline home of the CIBA VISION® and Essilor Management &Business Academy™. “I used the key metrics as a gauge to know
what other practices are doing,” she says.Utilize connections. After her clini-
cal rotations, Dr. Maursetter remained incontact with one of her supervisors. “Hegave me insight on howthe doctors in hisoffice set up theirpartnership,” she says.“Having connectionswith colleagues in theprofession helps createa good foundation.”
Be open andhonest. The existingpartners had a lot tooffer Dr. Maursetter, as
well. “They are both experi-enced in private practice andin optometry, and I had a lotof questions. They wereaccessible and walkedthrough the process with me,which made it a lot easier.”
The negotiations forpartnership took fourmonths, a bit longer thanDr. Maursetter expected, butthe process still ran smoothly.“There’s a lot more to itthan I expected,” she says.“It was an open conversa-tion with the partners andaccountants, which made it
easier for everyone to express their thoughts and opinions andderive attainable numbers.”
Dr. Maursetter says that the partnership works out nicely,now that the four partners share three full-time equivalent posi-tions. In addition to the small office she’s in, Dr. Maursetter alsooccasionally fills in at the practice’s other location, which isabout 20 miles away. “We can cover for each other for confer-ences and vacations and keep the office open more often than wewould be able to do otherwise,” she says.
Dr. Maursetter advises patience. “One thing I found wasthat openings at private practices weren’t listed,” she says. “Ifelt frustrated that there was nothing out there.” Thanks tospeaking up and forming connections, Dr. Maursetter achievedher five-year goal of private practice ownership in just a fewmonths. “Though one OD might not be hiring, he or she mayknow someone who is,” Dr. Maursetter says.
Dr. Maursetter is focused on managing her office and hopes tosee it grow to match the size of the other location. She’s workingclosely with the practice’s marketing team to reach that goal.
Dr. Maursetter
When Dr. Callie Maursetter was hired as an associate toreplace a former partner, her time was dedicated to a
second office, where she was often the only OD. “There wassome anxiety at first,” she says. “I started to see patients andalso was in charge of an office staff for the first time.”
One of the practice’s partners came to the office one day aweek to ease the transition. By showing his trust and confi-dence in Dr. Maursetter, the staff members adapted to theirnew boss. Even when she was the lone doctor in the office, theother partners were there to help. “When I had a questionabout a patient or practice management, they were readilyavailable to answer by phone, Skype or email,” she says.
Be the Boss
Women In Optometry September 2011
Page 9
Dr. Maursetter found her posi-tion by creating a network.
WO
WO
CONNECTIONS
C
WO3Q11:WO 2Q08-SK 8/23/11 10:17 PM Page 9

that she would see a positive cash flow after four months of busi-ness, but it took an extra three months. She admits her projec-tions may have been overzealous, but she is pleased she saw apositive cash flow within the first year. “The first year is rough nomatter what, with ups and downs,” she says. “Have thick skin,
think outside the box and makechanges as needed to keepthings chugging along.”
For example, to encouragesales, she has developed eyewearpackages that won’t break thebank. Patients are also morecomfortable with the value of apackage designed for their needsrather than having to select froma variety of add-on options.“Most people are more conserva-tive, so we’ve rearranged how wesell,” she says.
For the first year, shefocused on a marketing plan toget patients in the door. Now,
she has added goals of optimiz-ing revenue per patient and cre-ating a high level of service to
ensure patient loyalty. The practice also recently was awarded abid as one of three Cobb County Schools vision consultants for the2011-2012 school year. The practice has a well-liked Facebookpage, and she’s created a practice Twitter account. “I’m the driverof my practice,” she says. “But no matter how good of a doctoryou are, if you can’t find a reliable and trusting staff, you willhave turnover and may even lose patients.” Dr. Davison has keptthat in mind during the past year, along with these other keypoints that have contributed to her business success.
Analyze insurance plans. To get patients in the door, Dr.Davison started out on as many insurance panels as possible. Now, ayear after opening, she is reviewing the relationships. She analyzeseach plan on a number of factors: How many patients come in as aresult of this plan? What is the profit or loss on reimbursement forbasic services? Are there opportunities to leverage the plan forhigher per patient revenue? If she finds plans that are not beneficialto the practice, she won’t renew her participation.
Spend marketing money wisely. Dr. Davison tries to deter-mine the referral source for each patient and monitors the results.The practice has invested in several forms of marketing: directmail, circulars, building a professional web site, search engineoptimization and more. “Most of our patients come from insuranceweb sites and referrals, so we know where to put our dollars,” shesays. Knowing these statistics allows Dr. Davison to cut back onprint advertising to dedicate money, time and effort to moreeffective ideas.
Create an incentive program. One of those ideas was to start apatient incentive program. Dr. Davison customizes this program peri-odically to make it most effective. She provides patients with businesscards to pass along to friends or family members. The patient’s nameis written on the card, and when a new patient turns in one of those
Cover StoryPage 10
Women In Optometry September 2011
Before she even graduated from the PennsylvaniaCollege of Optometry in 2006, Janelle Davison,OD, had mapped out her future. Her goal was toopen her own practice within the next five years.“I knew I would have bills and student loans, but
after talking with colleagues, Idecided it was better to do itsooner than later,” she says. Asa young entrepreneur, she’dhave plenty of time to developand build a practice into thebusiness of her dreams.
The opportunity arose soonerthan expected. After working fora corporate optometry officeand doing other fill-in/contractwork, Dr. Davison opened thedoors to Brilliant Eyes VisionCenter in Marietta, Ga., in June2010. “From June 2010 to July2011, our number of patientstripled,” Dr. Davison says.
When the pace slowed in thespring, she didn’t panic. From herjob experience prior to openingthe practice and from discussions with colleagues, she realized herbusiness wasn’t failing but was following predictable trends. “Peopledon’t always think about eye exams in April or May with graduationand prom on their minds,” she says. “Our bumps in the road havematched the busy and slow seasons of optometry, so we are headedin a positive direction.”
When she started planning her practice, her business projec-tions included a better economic environment. In fact, she hoped
Ready, GOALSet,For a planner by nature, setting goals and analyzing the progress come naturally
Dr. Davison has been growing her practice since it openedin mid-2010.
Dr. Davison conducts an InfantSee exam.
WO3Q11:WO 2Q08-SK 8/23/11 10:18 PM Page 10

cards, the referring patient gets $35 credit towards an optical pur-chase for eyeglasses or a year’s supply of contact lenses. The discountis not combined with insurance purchases, but it does help withsecond-pair sales, especially for sunglasses. Potential referring doctorsin the area, even dentists, chiropractors and more, receive packets ofinformation explaining how optometry can play a vital part in mon-itoring diabetes and hypertension. Also, patients whose purchasestotal more than $500 receive a special Starbucks gift card.
Keep a current web site. Dr. Davison’s initial goal for her website was very basic—almost an electronic Yellow Pages-type displayad. Having basic practice information and her photo are importantelements when patients look for a doctor. She uses Internet searchesherself when she needs to locate a doctor. “I like to know who I willbe seeing and read about that person,” she says. “If there’s no website, I’m already questioning whether the doctor will be up to date.”
But that was just a starting point. She quickly added otherimportant features, such as a contact lens ordering section, morepatient education materials and links to her social media sites. HerFacebook site was up and running even before her practice, and Dr.Davison’s fan base multiplies rapidly: her goal in the beginning ofthis summer was to reach 500 fans by August. She had already dou-bled that expectation a month earlier. She has linked informativevideos to her web site and other web-based account pages. “Peoplelooking at your site want it to be interactive and informative,” Dr.Davison says. “I want them to see that our office is progressive andtechnologically current.”
Add a contact lens technician. Dr. Davison was determined toconvert more of her eyeglasses-only patients into contact lenswearers. She discovered that her single technician was more com-fortable in the optical dispensary than in the contact lens area. As aresult, optical sales were going strong, but the technician didn’t fol-low through with a proactive contact lens message. Dr. Davisonadded a contact lens technician to the practice several months ago,and this staff member is responsible for keeping trial lenses organ-ized, insertion and removal instructions and providing patients infor-mation on the lenses, rebates and special offers on annual supplypurchases. The strategy has paid off. Since making the change, con-tact lens exams have nearly doubled, and it’s rare to see a contactlens patient leaving the office without an annual supply. “My new
Women In Optometry September 2011
WO
Page 11
Dr. Davison crafted asophisticated look to her
reception area and dispensary.
! Goals Going Forward
Dr. Janelle Davison is as much a planner now as she was when she firstbegan developing her practice-acquisition goals. Here’s what is on the
short-term goal list.
Goal: Double contact lens revenue and one-year supply capture rate bythe beginning of 2012.
Plan: Offer instant savings per box with an annual supply of contactlenses, in addition to manufacturers’ rebates; provide free shipping forannual supplies to the patient’s home or office for added convenience andto lower the in-office transaction costs; and fit technologically advancedcontact lenses, including hybrid contact lenses for astigmatism.
Goal: Improve and increase medical model implementation, medicaloffice visits and billing from current 22 percent of practice revenue to 32-37 percent range by early 2012.
Plan: Dr. Davison has implemented a “community eye health expertprogram.” Through the program, she makes presentations at communitygatherings and association meetings to discuss the importance of preven-tive eye care and what role optometry can play in preventive care.
Goal: Increase patient exams per day from current average of 5-6exams per day to 8-10 exams per day.
Plan: Dr. Davison is exploring marketing ideas to draw in new patients,asking patients for their referrals and encouraging her office staff to fillin empty spaces in the appointment book. On her busiest day, she saw 16patients, so she and the staff know they can accommodate more.
Goal: Keep office technology up to date.
Plan: Plot equipment acquisition, do the research and analyze the man-ufacturers’ ROI scenarios. The next major acquisition for Dr. Davison likelywill be an optical coherence tomography unit by mid-2012.
technician helps close the gap,” Dr. Davison says. “With two peopleproviding the education, we can do a better job at promoting con-tact lenses and annual supplies.”
Nancy Barajas, the new contact lenstechnician, has increased profitabilityby improving the focus on contact lenses.
WO
WO3Q11:WO 2Q08-SK 8/23/11 10:19 PM Page 11

Make Yourself Known inCommunity and Profession
Seek Opportunities to Expand Skills
By Ann Madden, OD, Elkhart, Ind.My husband is a businessman, not an OD,
so his perspective is quite different from mine. For mywhole career, I’ve worked either as an employed doctor or anindependent contractor. On my own, I might have poured allmy focus into patient care—but his advice has been to differ-entiate myself by adding value to the practices where I’veworked and seek out opportunities to expand my skills.
When you contribute to the practice in ways beyond deliv-ering stellar patient care, you also contribute to your own career.That point was driven home to me recently when I decided tochange my employment situation. I had taken on a significantpractice management role with my previous employer, particu-larly in leading the drive to electronic medical records. I becameinvolved with my local professional society, serving as the vicepresident. I’ve taught at THE VISION CARE INSTITUTE,participated with the professional affairs consulting team forVISTAKON®, a Division of JJVCI, and worked with optometryschool students.
When the time came to seek a different job, I had severalexcellent options. It took a businessman to remind me thatwhile patient care is my first duty, finding ways to secure myown future by discovering and adding to my business skills isalso critically important.
Create a Network
By Janelle Routhier, OD, FAAO, Jacksonville, Fla.One of my mentors, an educator, provided
me with this simple but effective advice to helpme find a position in academia or industry: keep
showing up. “People will remember you, and you’ll create anetwork,” he said. He was right. I began attending every pro-fessional meeting that my schedule would allow. I soughtopportunities to attend professional events. There are somemeetings I have attended so routinely that now my colleaguesnotice when I’m not there.
The strategy works well if you have a reason to be at these
events. My entrée for most professional meetings was an aca-demic poster. I’d stand next to my poster, which provided mean opportunity to discuss the findings or theories with inter-ested passersby. Those poster sessions allowed me the chanceto build my network through the one-on-one discussions.
I also sought the chance to make the most of my atten-dance at these events by scheduling a meeting time with anesteemed colleague whom I knew would be attending. I’d con-tact that person ahead of time, asking for a brief meetingbecause I was interested in some aspect of that person’s ideas,interests or educational achievements. Most of these col-leagues have made the time for me.
The advice helped me in more ways than one. I gainedperspective, experience and confidence—along with a networkof people who knew my name and work. I feel that combina-tion was my advantage when I came on board at VISTAKON®
as manager in the medical affairs department. In fact, it’s goodadvice wherever you are in your career.
Keep Track of Your Goals
By Gina Wesley, OD, MS, FAAO, Medina, Minn.I knew I wanted to start my own, inde-
pendent practice, and soon after my 2006 gradu-ation from The Ohio State University School ofOptometry, I had that opportunity. I relied heavily on the fol-lowing pieces of advice.
Be the CEO of your practice. Weigh every practicedecision with an eye toward how it will help you build a solid,productive business. Measure the effectiveness of yourprocesses, analyze the return on investment of equipment,make sure your employees understand your goals and worktogether as a team.
Develop your own style. There’s no single formula forrunning a successful practice. The way that other ODs managetheir business or handle their clinical duties may not be the bestway for you. Think about what meets your needs and those ofyour patients. Listen to others and learn from their successes—or even their shortcomings. Then go with your own flow.
Market continually. Marketing is not a bad word; it’s anessential component to growing a practice. It’s also more involvedthan simply sending out postcards or occasional emails to yourpatients. Marketing is a grassroots approach that covers everycontact your patient has with your practice. The way your staffanswers the telephone, the first impression a patient receiveson entering the door and the education seminars you hold inthe community are all components that affect your currentand potential patients’ impressions. Make each occasion clearand memorable, and that will go farther than any mailer.
THE VISION CARE INSTITUTE™, LLC, Alumni Roundtable
These three optometrists, each of whom attended THE VISION CARE INSTITUTE™,share the best pieces of advice they’ve received in their careers.
© 2011
WO3Q11:WO 2Q08-SK 8/23/11 10:20 PM Page 12

form of optometry:“Asking which is better,one or two, all day everyday, seven days a week. So youhave to mix it up a little andkeep it interesting,” Dr. McNamarasays. In addition to U.S. forces,she examines detainees, retirees,contractors and NATO soldiers.And every couple of weeks, theteam packs up its equipment,loads it on a helicopter and isflown to remote forward-operatingbases to provide quality eye carewith an emphasis on vision readi-ness and combat eye protection.
Before deploying toAfghanistan, Dr. McNamara alsoperformed military humanitarianmissions in Bulgaria, Cambodiaand Kosovo and has been sta-tioned at 12 different locationsthroughout the U.S. andGermany. The military lifestylecan be tough on a family. “Mydaughter, Ashley, attended 13different schools before she grad-uated,” she says, and her son,Ethan, is currently staying withhis grandparents in North
Carolina. “Militarydeployments, schoolingand missions arealways disruptive tofamily life, so it helpsto have good friendsand a supportive familywho are willing tohelp.” Although shemisses her children,she reports that the124th optometry teamhas great unit cohe-sion. “The CampPhoenix optometryclinic has a great workenvironment, the patients are appreciative, and I havedeveloped lasting friendships with the people withwhom I’m deployed.”
Dr. McNamara has a sense of humor, even whileacknowledging the risks of her role. Unlike a humanitarianmission, ODs who have been deployed “pack a weapon;have to beg, borrow and steal to get equipment; takeoccasional Blackhawk rides; and have to work through afew rude interruptions from incoming mortars,” she says.“Being part of a deployed optometry team puts every-thing in perspective and reminds me of why I joined themilitary; it’s a fun and rewarding profession.”
U.S. Army Lt. Col. Debra McNamara, OD, who is the124th Medical Detachment optometry team leader,18th MEDCOM from Fort Shafter, Hawaii, shares a com-mon goal with many optometrists: to provide eye carethat enhances the patient’s career and lifestyle needs.
Beyond that key similarity, however, Dr. McNamara’s role is a farcry from most community-based OD practices. Her setting andenvironment constantly change, and her patients face extremevisual tasks far more demanding than computer use.
Dr. McNamara has been deployed since May to Afghanistan,where she provides initial diagnosis and management of eye injurieson the battlefield and detects, diagnoses, treats and manages oculardisorders, injuries, disease and visual dysfunctions in U.S. fightingforces. “Providing eye care while deployed requires the same clinicalskill set used in any optometry clinic, with the addition of a specificfocus on maintaining combat-readiness,” she says. She’s beencaring for patients with glaucoma, macular edema, keratoconus andtrauma, as well as a number of recurrent erosions due to the dry cli-mate and severe conditions. Dr. McNamara works without specializeddiagnostic equipment, such as a visual field machine, topography orocular coherence tomography unit, so she utilizes the military EMRto review patients’ previous military eye exams and research previ-ous diagnostic testing to assist with diagnoses.
Her team is comprised of two optometrists, two optical fabrica-tion specialists and two medic/optometry technicians. “The 124thoptometry team is modular, scalable and flexible enough to providefar-forward optometry support to the area of operation and providesassembly, repair and fabrication of spectacles and optical inserts forprotective masks and ballistic eye protection,” Dr. McNamara says.
But so much of what she does comes back to the simplest
Women In Optometry September 2011
Page 13
WO
Dr. Debra McNamara started college on basketball and volleyballscholarships, then enlisted in the Army halfway through as a
military intelligence electronic warfare signals intelligence analyst.Optometry was not even a consideration as she was sent to the DefenseLanguage Institute to learn German in Monterey, Calif., in 1988.
In 1992, Dr. McNamara used her GI Bill and volleyball scholarship toget a biology degree when a friend, Dave Gibson, now an OD in NorthCarolina, encouraged her to go to optometry school, too. He accompa-nied her to a career planning center, helped her apply and schedule herremaining prerequisites. “He even found a flyer on the military’s HealthProfessional Scholarship Program (HPSP),” she says. “Life presented afork in the road; I was ready for a change, and before I knew what hadhappened, I had a new career path.”
She drove cross-country to Pacific University College of Optometry(PUCO) in August 1994, nine months pregnant, with her mother anddaughter, then 4. “I showed up at PUCO with ankles the size of water-melons, I couldn’t fit behind the school desks and then 20 days intooptometry school, Ethan was born.” The staff at PUCO was very supportive,and with help from a determined friend, her PUCO classmates and a gen-erous four-year Army HPSP scholarship, Dr. McNamara was on her way.
The first Serbian/Albanian combinedhealth engagement
A Fork in the Road
Dr. Debra McNamara is keenly interested intraumatic brain injury (TBI) and post-
trauma vision syndrome (PTVS). Her optometryschool professors “hammered home the impor-tance of binocular function and how it pertainsto sensory integration and vestibular function.Having a strong binocular vision backgroundhas turned out to be an important clinical assetto have as a military optometrist,” she says.
“There are so many soldiers who have suf-fered TBI but have still not been diagnosed ortreated for their PTVS. There is a real need forODs who are interested in vision therapy andwho enjoy the sense of camaraderie that devel-ops when you collaborate with a team of occu-pational therapists, physical therapists, neurol-ogists, psychologists, physicians, audiologists,nurse case managers and other health careproviders to improve the lives of soldiers.”
Vision for Her Future
Military OD committed to the eye healthof troops now and in the future
WO
AfghanistanOn the Ground
in
WO
WO3Q11:WO 2Q08-SK 8/23/11 10:22 PM Page 13

Page 14
Women In Optometry September 2011
Why should patients choosePearland Professional Vision?Amie Gisbert, OD, of Pearland,Texas, believes her new practicewill evoke love at first sight.
The Houston area is saturated with ODs, soshe’s focusing on the fine details that will
keep patients returning. “Wedon’t have money for all ofthe latest equipment yet,but there are still ways tocreate the wow factor forthe patient,” she says.
Create Your DesiredAtmosphere
The down economyworked in her favor while shewas looking for the perfectpractice location. She founda building, vacant since itsconstruction two years ear-lier, at a great price with anadded bonus: a uniqueoctagonal-shaped area per-fect for a chic dispensary.
Construction began inlate May 2011, and Dr.Gisbert let her husbandRamon Gisbert, an archi-tectural intern, get creativewith the design. A localconstruction company thatspecializes in optometryoffices, HM GeneralContractors, brought the
vision to life.The office opened in August. “I envision
it being like a retail center: clean and artsy,”
she says. With enticing, exciting window andshelving displays, passersby will want to stopin often, Dr. Gisbert hopes. “Retail stores hirepeople specifically to design seasonal dis-plays, and I think that if we want to be moresuccessful in optical sales, we should spendmore time thinking about what makes ourmerchandise ‘pop’ and how patients perceivethe office.”
The two windows next to the entrancewill change once or twice a year and will bedecorated with posters, eyeglasses arrangedon pedestals, a display of brand names car-ried and more. Themed displays will rotateevery few months in the window nook thatfaces the street.
Inside, Dr. Gisbert has fused her favoriteelements of contemporary and traditionalstyles. Permanent parts of the office—walls,cabinets, countertops—are neutral shades ofbeige and brown. The flooring consists ofvinyl that looks like dark wood and darkbrown/black carpet, and the dispensingtables are custom-made with countertop tilesthat look like metal strands woven together.“The color comes from all the decor, fixtures,furniture and displays which are more tradi-tional,” Dr. Gisbert says. The octagon-shapedceiling is outlined in light fixtures illuminat-ing the opticaldispensarybelow.
Kids passa weatheredplank thatsays, “Eye-EyeMatey,” into apirate roomwhere they canfeel like they’veboarded theJolly Roger. “Itwill be a funplace for thekids to relaxand watchmovies andplay with toyswhile their par-ents are touringthe optical or getting exams,” Dr. Gisbert says.
She equipped one of her three exam lanesfor the practice opening and has room for twomore. TV monitors make the exam process more
interactive. “Patients will be able to see every-thing that I’m seeing through the slit lamp,”Dr. Gisbert says.
Bring in PatientsIn the months before opening, Dr. Gisbert
made sure that the new practice would createa buzz in the community. Her husbanddesigned her web site, practice logo and allcustom displays. She posted photos of theconstruction in progress on her web site andFacebook page for her growing fan base.
The giant sign outside will increase prac-tice visibility and was put up as the con-struction progressed. Dr. Gisbert also plans toinvest in direct mail, which she will cus-
tomize for certainhousehold incomesand age groups. Shewill link videos toher web site,Facebook and onYouTube to educateand explain herservices and special-ties, such as ortho-keratology, whichnot many doctors inthe area offer.
She’s planningher grand openingand other activi-ties, such as a spe-cial day for momsand daughters tobrowse the office
and enjoy manicuresand pedicures. She will continue to workas a relief doctor two days a week untilher practice builds up enough patientvolume.
Now or Never
Dr. Amie Gisbert knew that in a still-recoveringeconomy, she could fall into a routine and put
off opening her own practice. Feeling more confi-dent clinically, and tired after two years of a longcommute, she was encouraged to start. “Now is theperfect time,” she says. “I live in Pearland, and I’mexcited to get more involved in our community.”
To manage the complex process of opening apractice cold, Dr. Gisbert and a friend, who is alsoopening a practice, developed a two-page, detailedlist to guide them through the steps it takes toopen a new practice cold. Find it on facebook.com/womagazine.
OD focuses on the details to perfect the patient experience
WO
WO
Dr. Gisbert nextto Kid’s Corner
The new building had been vacant for two years.
Before and afterconstruction
Standing out from the Start
WO3Q11:WO 2Q08-SK 8/23/11 10:23 PM Page 14

Practice set the tone for a different delivery for optometry services in Puerto Rico
Page 15Three ODs Lead the Way
wenty-five years ago, the profes-sional landscape in Puerto Rico wasquite different. Wanda Tort, OD,completed her studies in the InterAmerican University
of Puerto Rico School ofOptometry’s first graduatingclass, ready to break the moldin which optometric servicesplayed a distant second role tooptical dispensing.
She met two like-mindedpractitioners, both cliniciansworking with the school: AnaMaria Pico, OD; and MariaGorbea, OD. Dr. Tort beganobserving Dr. Pico in her visiontherapy clinic on Saturdays andwas assisting in the clinic byher senior year. The trio’s com-mon goals brought themtogether. “We wanted to bedoctors with a professionaloffice instead of a focus onoptical services,” Dr. Tort says.
With that philosophy andtheir mixed interests andexpertise, they opened the doors to their full-scope behavioral practice. Dr. Tort and Dr. Picofocus their time on children and vision therapy,while Dr. Gorbea sees adults, adapts contactlenses and specializes in low vision rehabilita-tion. Dr. Tort also adapts prosthetic eyes, aspecialty skill that she learned because shebelieved it could benefit their patient base.
It took some time for patients to adjust tothe new dynamic. To generate buzz, the doctorsconducted school screenings and sent letters toschool psychologists and other affiliated healthcare providers. They also introduced anotherunique aspect to eye care: a timely appoint-ment book. Dr. Tort explains that most eye carebusiness in Puerto Rico is generated by walk-ins. Even when patients do have appointments,the time slot may have been reserved for morethan one person. So it is still a first-come, first-served basis. “We have always worked on thedot and on the hour,” she says.
The doctors wrote articles for the localnewspapers to explain the new direction oftheir practice, and little by little, the referralsstarted rolling in. Referrals came through wordof mouth by satisfied patients, as well as frompsychologists, occupational therapists, physicaltherapists, pediatricians, neurologists andmore. “It’s the people who know what we aredoing and how we run our practice who spreadthe word,” Dr. Tort says.
Last year, as the practice approached its
low vision services, and we don’t want anyonetripping,” Dr. Tort says.
Another focus of the renovations includedthe vision therapy room. Previously, most
equipment in the room wasvisible even when it wasn’tbeing used. “Autistic childrenand those with other specialneeds can become overstimu-lated when they see all ofthat,” Dr. Tort says. The reno-vations included expandedcloset space and cabinets, sothat each piece of equipmentis covered or closed behind adoor now. “The room is clean,white and has no distrac-tions.”
The recent remodelingreinforces the message to thecommunity that Dr. Tort, Dr.Gorbea and Dr. Pico are thereto stay. “I’d still be practicingeven if I won the lottery,” Dr.Tort says, laughing. “I don’t seemyself doing anything else
because I really enjoy what wedo.” In fact, Dr. Tort hopes that she can expandthe vision therapy portion of the practice in thecoming years—they have the demand and space,but not the time—by adding another therapistto the staff. And in another five years, the doc-tors hope to add an associate doctor. “Eventually,we would want someone to take over the prac-tice that took a long time to build.”
quarter-century milestone, the doctors decidedit was time for an office facelift. “We wantedto make the office more comfortable for bothour staff and our patients. We expanded and
reorganized our secretarial area and changedour waiting room,” Dr. Tort says. Because ofthe heavy pediatric volume, the doctors agreedthat kids in the reception area needed theirown space. The creation of a low wall allowsparents to keep an eye on their children, buttoys and games no longer take over the entirespace. “We also have an older population for
T
(l-r): Dr. Pico, Dr. Tort and Dr. Gorbea found a new model of practice thathas been working for them for 25 years.
WO
Women In Optometry September 2011
Women of Vision Meeting Honors LeadersA recent Women of Visionluncheon honored (l-r):Dr. Dori Carlson as thefirst woman president ofthe American OptometricAssociation and Dr. KarlaZadnik, president of theAmerican Academy ofOptometry. This is thefirst time both organiza-tions have been led bywomen at the same time.They were joined by Dr.Mary Anne Murphy, thenew chair of Optometry Giving Sight in the U.S., and Dr. Tone Garaas-Maurdalen ofNorway, the first woman president of the World Council of Optometry. The four joined in onthe free-flowing luncheon and discussion as well as commenting on the various aspects ofwomen in leadership within their organizations. WO
WO3Q11:WO 2Q08-SK 8/23/11 10:24 PM Page 15

Page 16
Dr. Le, Dr. Lillie & Dr. SchafersSeveral womenoptometristsreceived theInnovator in CareAward from theannual feature inCorporateOptometry Reportsnewsletter.Congratulationsto these corporate-affiliated ODs, including Tanya Le, OD, of Target Opticalin Yorkville, Ill.; Julie Lillie, OD, of Sterling VisionCare in Jamestown, N.Y.;and Emma Schafers, OD, of US Vision in Des Peres, Mo.
Womenin theNEWS
When Laura Windsor, OD, FAAO, the AmericanOptometric Association’s (AOA) 2011 Young Optometristof the Year, hears her colleagues talking about theirunease with implementing electronic health records(EHR), she feels their pain. She’s not facing the same
scramble as her colleagues who are just starting to move away frompaper-based records, though. She made that switch six years ago inher four Indiana low-vision clinics. But she knows that in their hasteto get on board—in order to receive reimbursements and ultimatelyavoid penalties—they are more likely to make mistakes.
That’s where her experience could be most helpful, she says. “Inmy practice, I think in the beginning we did a lot of things thewrong way,” she admits. So she approached the Indiana OptometricAssociation (IOA) last year, offering assistance in producing a manualto guide others through EHR implementation. Dr. Windsor, who is alsothe IOA’s vice president for its East Central Optometric Society and onthe IOA’s EHR task force, penned the 70-page manual with two otherODs. It covers the selection of an EHR system, as well as strategiesfor implementation and helping the staff and doctors adapt to thesystem. The manual was distributed to IOA members and is availablefor purchase by nonmembers.
When Dr. Windsor startedwith EHR in her three clin-ics—in Hartford City,Indianapolis and FortWayne, Ind.—she pur-chased tablets for enteringthe data. “It was the worstmistake we’ve ever made,”she says, adding that theyspent thousands of dol-lars when $500 laptopswould have worked muchbetter. Instead of givingup, she and the staffpersevered. “I like tobe realistic. It is notgoing to be greatfrom the first day.And it’s going toslow you downbefore it speedsyou up,” she says.However, shequickly encour-ages colleaguesthat it isworthwhile. “I
Women In Optometry June 2011Continued on page 17
Dr. Lyons
Stephanie Lyons, OD, of Chicago, Ill., was theonly optometrist in the entire city to be nomi-nated by Chicago Parents readers as one ofChicago’s Favorite Kids’ Docs.
AOA’s Young OD of the Year is committed t
Doctor Leverages Her Experience to
Help Others Ease into EHR
Barbara Horn, OD, of Washington, Mich., was elected to the AmericanOptometric Association’s (AOA) Board of Trustees. With her election,this is the first time four women are serving on the AOA Board ofTrustees together. She joins newly elected AOA President Dori Carlson,OD, FAAO, of Park River, N.D.; Hilary Hawthorne, OD, of Los Angeles,Calif.; and Andrea Thau, OD, FAAO, of New York, N.Y.
Dr. Horn Dr. Carlson Dr. ThauDr. Hawthorne
Dr. Horn, Dr. Carlson, Dr. Hawthorne & Dr. Thau
Recognitions
Several women were recognized in theVision Monday and Review of OptometricBusinesss 2011 Optical BusinessInnovator Awards in June. (A) SusanKeene, OD, of Marion Va., and (B)Laurie Sorrenson, OD, of Austin Texas,were both featured in the BusinessManagement section. Awarded for theirContact Lens Dispensing were (C) TaraPeterson, OD, of Littleton, Colo., and
(D) Nancy Wojcik, OD, of Arlington Heights, Ill. Also honored were (E) KathleenAndersen, OD, of Rancho Santa Margarita, Calif., for the Patient Experience, and(F) Jennifer Brady Cook, OD, of Lutz, Fla., for Optical Dispensing.
Dr. Le Dr. Lillie Dr. Schafers
A B C
D E F
Earning the AOA Young OD of theYear award was a bright spot in a dif-ficult year for Dr. Laura Windsor andher husband, Jeff Whetzel. Theirdaughter, Lauren Victoria WindsorWhetzel, just 6, passed away unex-pectedly following complicationsafter tonsil surgery in February.The family has established Tori’sButterfly Garden Foundation to sup-port fine arts, gardening and natureeducation in their county and sendspink “Live Life Like Tori” braceletsto those who make donations. Learnmore at torisbutterflygarden.org.
Healing throughAction
WO3Q11:WO 2Q08-SK 8/23/11 10:25 PM Page 16

Women in the NEWSContinued from page 16
Page 17
Women In Optometry September 2011
couldn’t livewithout it.” A sys-
tem of electronicrecords has increased
her practice’s organizationand ability to access informa-
tion to an exceptional degree. Sheenjoys the added bonus of being able to access her system from anylocation with Internet access.
Dr. Windsor uses her technological skills in other ways as well.She’s has been theIOA’s web masterin the past andhas developed herown practice website to the pointwhere it containsextensive educa-tional informationon low vision andneuro-optometricconditions, as wellas treatments. Oneyeassociates.com,visitors can readabout low visionconditions andsystems, watchvideos andmovies that Dr.Windsor has
co-produced,find out about her services and much more. The web site hasdrawn new patients from near and far, including countries suchas Venezuela, Mexico, China, Canada, France, New Zealand,Greece and Malta. Despite her practice being “in the Indianacornfields,” these patients are happy to make the tripbecause they do not have the care to help them in theirhome countries.
Dr. Windsor has gained increasing audiences throughwriting and lecturing across country. She often focuses ontopics such as low vision and specialized conditions likeachromatopsia. For the past 10 years, she and severalother Indiana ODs have held an annual lecture on third-party billing and insurance. Dr. Windsor is co-writer andeditor of the 350+-page manual for the sections shecovers, including diagnostic procedures, supplementaltesting, EHR, e-prescribing, OSHA and the rules andregulations of billing.
Dr. AndersenHeartSmart Technologies EyeCare Division hosted a dinnerfor Kathleen Andersen, OD, andher staff, of Rancho SantaMargarita, Calif., to celebrate Dr.Andersen being in private prac-tice for 20 years. CEO BlaineUng presented Dr. Andersen witha plaque of her story in WO.
Dr. RobertsonKatie E. Robertson, OD, of Springfield, Mo., was thefirst recipient of the American Optometric Society’sDr. Harvey Yamamoto Award.
Dr. FranklinShannon Franklin, OD, of Crozet Eye CareOptometrists in Charlottesville, Va., has beennamed to serve on the national InfantSEE® com-mittee, a program of Optometry Cares–TheAmerican Optometric Association Foundation.
Dr. Laura Windsor followed in her father’sfootsteps and joined him in practice.
Richard Windsor, OD, FAAO, also specialized inlow vision, and his passion for the specialtymade her realize that she wanted to focus onthese services, too. Her father was awarded theOptometrist of the Year award from theAmerican Optometric Association (AOA) in1999. She is grateful to be the recipient of theAOA’s Young Optometrist of the Year recogni-tion this year. “It’s a great honor and privilegeto be acknowledged for my work in low vision,my lecturing and my writing,” she says. WO
Dr. Geist & Dr. WeissTwo of the Nebraska OptometricAssociation’s (NOA) past presidentsare leading respected regionaloptometric associations. Teri Geist,OD, of Omaha, is president of theNorth Central States OptometricCouncil, and Ellen Weiss, OD, also
of Omaha, leads the Heart of America Contact Lens Society. The overlapof their tenures has led to the first time NOA has had two members insuch prominent roles simultaneously.
Inherited Interest
WO
d to her community and her profession
Dr. Geist Dr. Weiss
Vision Monday RecognitionsVision Monday recognizes several women ODs in its 2011 Most InfluentialWomen In Optical feature. In the Executive Suite category, VM notices the
work of (A) Dori Carlson, OD, FAAO,of Park River, N.D. Four ODs wererecognized in the Rising Stars sec-tion: (B) Carla Mack, OD, FAAO,director, global medical affairs atBausch + Lomb in Rochester, N.Y.;(C) LaSheta P. David, OD, owner of
Invision Family Eyecare in Concord, N.C.; (D)Jennifer M. Smith, OD, FCOVD, vice president/co-owner, Draisin Vision Group in Charleston, S.C.;(E) Jeanette Carbone Varanelli, OD, FAAO, chiefof optometry at John D. Dingell VA Medical Center,Department of Veterans Affairs in Detroit, Mich.
A B C
D E
WO3Q11:WO 2Q08-SK 8/23/11 10:25 PM Page 17

Dr. Mastrota managesthe daily patient flow,making sure the spe-cialist has the supportfrom optometrists,optometry residents andstudents and technicalstaff to handle the 80-90 patients scheduledto see the specialist.
Each day presents aunique lineup. One day,the center sees only ocu-loplastic surgery patients; the next it mightbe all retinal patients or glaucoma patients.Typically, Dr. Mastrota and the front officestaff have one day a week where no specialistis on the schedule. On those days, she sched-ules post-operative patients and handles on-call requests for ODs who ask her to covertheir emergencies while they’re on vacation.
“I thought when I first came to Omnithat my biggest challenge would be thepatient care since it was at a different levelfrom what I had been doing day-to-day,”she recalls. “I wondered whether I had theclinical skills. But the greater challenge hasbeen staff management and developing apolitical sensitivity to the different ODs andMDs.” For example, she’s had to learn tocontrol her tendency to micromanage proj-ects and people. “It doesn’t really matter ifthe pages are lined up exactly so in thetwo-hole punch,” she says, laughing. “Butit does matter to remember how differentdoctors have different philosophies about
For a short time, Katherine Mastrota,MS, OD, FAAO, “was very close toopening my own practice,” sherecalls. But a succession of opportu-nities led her in another direction,
ultimately to where she is now—the centerdirector of Omni EyeSurgery New York. Inher role of caring forprimarily other ODs’patients, she keepsthe primary care ODs’role firmly in mind.
That attitudehas earned her a lotof respect from hercolleagues who sendtheir patients toOmni for specialty
care. Dr. Mastrota is the center director forthe New York City Omni center; there are fouraffiliated centers in New Jersey. Specialistscycle through the five Omni locations, pro-viding surgery or follow-up care as needed.
Page 18
That’s Her Paddle
Wondering whether Dr. Katherine Mastrota isconnected to the Mastrota Meibomian Gland
Paddle? She is the designer of the tool to gentlyand effectively express meibum from the meibo-mian glands. WO
Dr. Mastrota
disease management, keep their preferredprocesses in mind and help the clinic daysprogress as seamlessly as possible.”
Since Omni neither provides primary eyecare nor dispenses contact lenses or eye-glasses, optometrists in the region feel con-fident that their patients will be sent backto them. “We will not prescribe eyeglassesor contact lenses, as that care is renderedby our referring optometrists. We are verystrict about that policy,” Dr. Mastrota says,noting that she has spent years at this cen-ter and previously at the Jofe Eye Institutecultivating OD-referral relationships. “Nopatient is truly our own,” she adds. Only ahandful of patients—many of whom arenative New Yorkers who don’t drive—call thecenter directly for care. She’ll provide anyurgent care needed and then refer them toan easily accessible OD in the area for con-tinued care.
Dr. Mastrota says that being meticulousabout returning patients to their primary careOD is critical to improving care overall.“When ODs send a cataract patient to anophthalmologist and that patient doesn’treturn to the practice, that is discouraging tothe referring ODs,” she says. “The result couldbe that ODs tend to want to hold onto theirpatients, during which time the cataractbecomes more dense and vision declines,compromising patient safety and quality oflife.” She believes that since Omni’s referringODs can send patients there with completeconfidence that those patients will be back,intervention can occur sooner.
In fact, the wide range of options avail-able to optometrists is what intrigues herabout the profession. “Not only are there somany modes of practice, but if you want todo pathology or vision therapy or contactlenses, you can find a place to provide thatservice.” That flexibility may be one reasonoptometry is drawing so many women.
PPDoctor coordinates specialty care for patientswhile keeping OD colleagues in mind
Protecting the Referral Relationship
Dr. Mastrota counsels patients preparing for surgery or avisit to the specialist. Then she wants them to return totheir primary eye care provider.
Women In Optometry September 2011
WO
Impact of High-Tech Classrooms Worries Parents
Parents have some concern about theeffects of the evolving technology intoday’s classrooms, according to theAmerican Optometric Association's(AOA) 2011 American Eye-Q® survey.
“Today's classroom technology is extremely visual,making it critical for students to maintainexcellent eye health,” says James Sheedy,OD, PhD, an AOA technology and vision expert.“Binocular vision, focusing abilities as well asnearsightedness and farsightedness should bechecked by an eye doctor yearly, particularly asstudents head back to school.” The increasinguse of 3D imagery in the classroom may proveproblematic for those who experience headaches,
nausea or have problems with binocular vision.Students can help avoid computer vision
syndrome by practicing the 20-20-20 rule:Take a 20-second break at least every 20minutes of focused viewing, and view some-thing 20 feet away. Studies show that peopleneed to rest their eyes to keep them moist.Plus, staring off into the distance helps theeyes from locking into a close-up position.The AOA further recommends that studentstake a 15-minute break for every two hoursspent on computers or other digital devices.
For more information on 3D vision, or todownload a copy of 3D in the Classroom–AnAOA Report, visit 3deyehealth.org. WO
WO3Q11:WO 2Q08-SK 8/23/11 10:27 PM Page 18

Women In Optometry September 2011
Page 19
Change ignites a reaction and discussion.That’s surely been the case with topics suchas optometric board certification and thepush for comprehensive eye examinations forall the nation’s children. Although there is
tugging from all directions, this give-and-take is sim-ply an evolution. It’s pushing optometry forward. Wecan’t be stuck in our ways, and we must realize thatchange is good.
Even I wasn’t always gung-ho about change. Asone of six women in my optometry school class, Iimagined myself moving into a stable career, settlingdown in a small town with an underserved populationand taking care of the community in my own private practice.Instead, I haven’t seen a traditional patient in nearly 20 years. That’snot to say I wasn’t busy; my work weeks often averaged 50-80 hours.But I saw a greater need outside of the traditional setting.
While clinical care in a traditional practice setting is a greatcareer and the foundation of the profession of optometry, it’s not theonly venue or choice. For example, in my career, I have developedchildren’s vision programs and worked in mobile vision clinics onfreezing winter days and under the scorching summer sun as a publichealth officer with the Indian Health Service. That federal program isresponsible for providing health care to Native American and AlaskanNative peoples. I helped establish primary eye care clinics in rural
Appalachia at a time when the mining industry reducedits support of health care for miners and their families. Ialso developed comprehensive primary care, quality assur-ance diabetes programs funded through the Centers forDisease Control and Prevention for high-risk populations. My mother’s professional work with early stages of what
became HeadStart programs prompted my own fascination with childdevelopment. I was fortunate to encounter the late John Streff, OD,DOS, FCOVD, FAAO, a committed educator ahead of his time with hisappreciation for the visual processing system.
My career has brought me into contact with others who changedthe course of my life. An adjunct faculty position lead to a role asdirector of off-campus clinical programs at Southern California Collegeof Optometry. That experience served me well when I was a practicumcoordinator for a newly developed Masters of Public Health program
that I helped shepherd through to accreditation at theRobert C. Byrd Health Sciences Center. The energy,motivation and dedication of students are inspiring.
My career may seem complicated. It has becomea far cry from the 9-to-5 day that I once sought whenfirst considering the profession of optometry as acareer choice. Now I balance the demands and oppor-tunities of related work: consulting, working on dis-semination plans for Healthy People 2020, reviewingfederal grant applications, serving on state andnational boards and advisory panels and attendingmeetings such as the National Rural Health AssociationAnnual Meeting or the American Public HealthAssociation’s first midyear meeting. Looking back,each of the places I stopped along my career’s jour-ney could have been a lifelong pursuit on its own.
But I’ve adjusted my plans and changed courseaccordingly when and where there was a need. Not
everyone embraces change. I didn’t settle into the practice I onceenvisioned, but I have had other opportunities to help practitionersin rural areas better serve their patients. I’ve been able to see andcultivate interests and excitement among students. I’ve been able toadvocate for underserved minority populations and the elderly. Theseopportunities were available to me because I was willing to chal-lenge myself and to embrace change.
The idea of change can be intimidating, but don’t let it overpoweryou. It’s important to face it and move forward for the future ofour profession. Optometry is changing, and so are the people in it.
Dr. Bowyer coordinates her many roles from Morgantown, W.V.
PinkInkPinkInk
Dr. Bowyer
WO
There Is Powerin ChangeBy Norma K. Bowyer, OD, MS, MPH, FAAO
Sponsors of Women In Optometry
WO3Q11:WO 2Q08-SK 8/23/11 10:28 PM Page 19