recurrent choroidal melanoma after transscleral local resection with diffuse vitreous seeding
TRANSCRIPT

CASE REPORT
Recurrent choroidal melanoma after transscleral localresection with diffuse vitreous seeding
Pedro Gonzalez & Ewan G. Kemp & Fiona Roberts
Received: 25 May 2009 /Revised: 15 October 2009 /Accepted: 19 November 2009 /Published online: 3 February 2010# Springer-Verlag 2010
AbstractBackground Choroidal melanoma usually spreads system-ically via the vascular system or extraocularly throughchannels in the sclera. Intraocular spread through vitreousseeding is uncommon.Methods We present two patients in whom melanomarecurred following transscleral local resection and widespreadfine patchy pigmentation of the retina was identified grossly.The eyes were submitted for histological examination.Results In one case there was recurrent melanoma in thesurgical coloboma with diffuse vitreous seeding and a pre-retinal membrane composed of tumour cells. Tumour cellswere also identified in the anterior chamber. In the secondcase there was no tumour in the coloboma although twosmall satellite choroidal nodules were identified. Tumourcells were also present in the vitreous and covering thesurface of the retina.Conclusions We described two cases of recurrent choroidalmelanoma following transscleral local resection withvitreous seeding. Intraocular seeding following local resec-tion is uncommon. There are several potential mechanismsfor this although it seems likely that in these cases loss ofthe retinal barrier assisted in the intraocular spread of thesetumours.
Keywords Choroidal melanoma . Intraocular spread .
Vitreous seeding
Introduction
Transscleral local resection of primary choroidal melanoma(TSLR) is performed on selected cases as an alternative toenucleation or proton beam therapy and if the tumourthickness is excessive for plaque radiotherapy alone.Tumour recurrence, at the margins of the surgical colobomahas been reported in 3–32% of cases usually as a masslesion [1–4]. Diffuse intraocular spread and vitreousseeding are rare.
Methods
We report two cases where following local resection therewas clinical suggestion of tumour recurrence in thecoloboma and in addition diffuse patchy pigmentation ofthe retina thought to represent seeding of the tumourthroughout the eye.
Results
Case 1
A 46-year-old female presented with a choroidal mass. Shehad a 6-month history of visual disturbance in the right eye.Examination was normal except for an elevated, pigmentedlesion in the right posterior pole (Fig. 1a). Ultrasonic B-
P. Gonzalez : E. G. Kemp : F. RobertsTennent Institute of Ophthalmology, Western Infirmary,Glasgow G11 6NT, UK
F. Roberts (*)Department of Pathology,Glasgow, UKe-mail: [email protected]
Graefes Arch Clin Exp Ophthalmol (2010) 248:741–746DOI 10.1007/s00417-009-1261-9

scan showed a solid mass 3 mm in height and with a basaldiameter of 14 mm at the largest point, consistent withchoroidal melanoma. Local resection of the tumour wasperformed under hypotensive general anaesthesia. Trans-illumination and direct examination allowed identificationof tumour position and dimensions and a corresponding
scleral flap was fashioned. The tumour and underlyingchoroid was removed en-bloc after haemostasis wasachieved with diathermy. Histology confirmed malignantmelanoma of spindle B cell type extending to excisionmargins. Bruch′s membrane was intact overlying thetumour.
Eight weeks later a pigmented area was identified at thenasal edge of the coloboma (Fig. 1b). This tumourrecurrence was treated with an argon laser, which wasrepeated at 1, 2, and 7 years later for clinical evidence oftumour recurrence (Fig. 1c). Further recurrence wasidentified at 23 years after initial surgery and was treatedby plaque radiotherapy. Six months later, the patientpresented urgently with raised intraocular pressure. Clini-cally, this was considered to be neovascular glaucoma withangle closure. Despite maximal medical treatment, the eyebecame painful and enucleation was performed.
The enucleation specimen showed a pigmented masssituated in the centre of the coloboma (Fig. 2a). Throughoutthe posterior segment there was fine patchy pigmentation ofthe retina (Fig. 2a). Histology confirmed malignant mela-noma arising in the coloboma, which was of spindle celltype. The tumour had an irregular surface and small groupsof epithelioid cells were identified ‘seeding’ from thesurface into the vitreous cavity resulting in widespreadintraocular spread (Fig. 2b, c). Tumour cells were also seenwithin a neovascular membrane on the surface of the retina.The posterior vitreous face was detached and ruptured withspread of tumour cells onto the surface of the ciliaryprocesses, iris, cornea, and trabecular meshwork (Fig. 2d).In addition, there was a neovascular membrane on theanterior iris surface and angle closure on the nasal side.
At the time of enucleation, the patient was found to haveultrasound evidence of metastases in the liver and spleen.She received palliative chemotherapy for this and thesplenic mass had shown some reduction in size at her lastfollow-up 2 years later.
Case 2
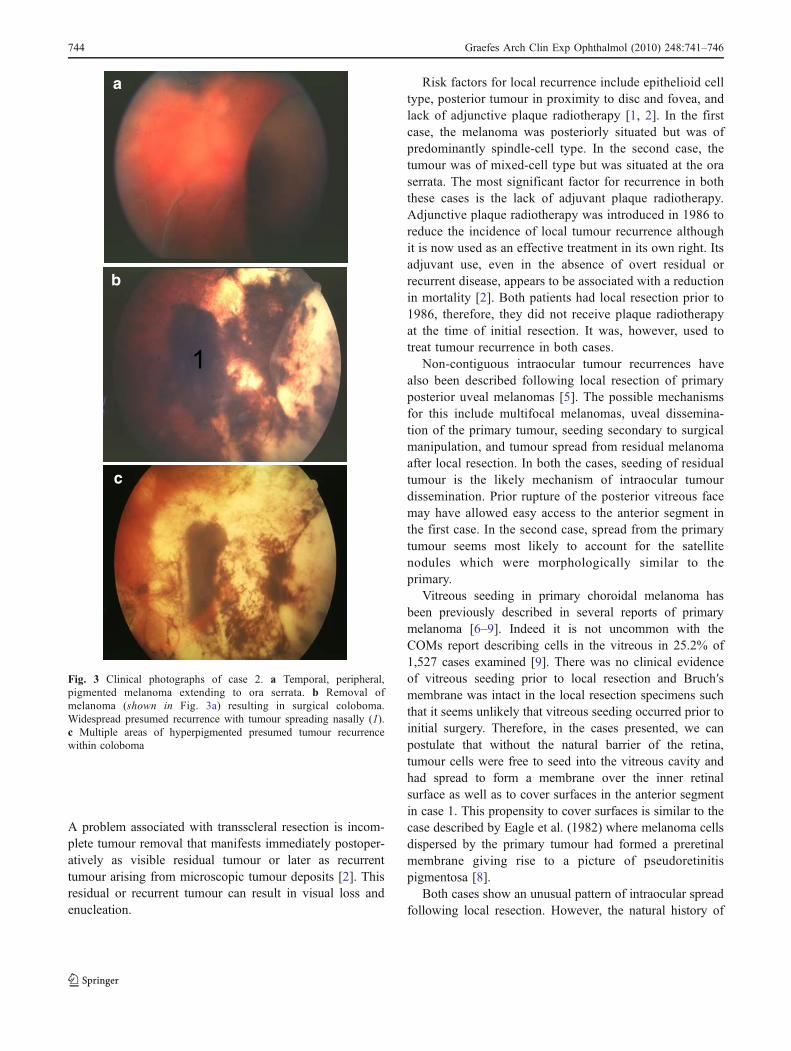
A 52-year-old female presented with a 6-month history offloaters. Examination showed an elevated pigmented lesionin the temporal aspect of the left eye extending to the oraserrata (Fig. 3a). She was otherwise fit and well. Thisappearance was consistent with a diagnosis of choroidalmelanoma with a largest basal diameter of 14 mm. Localresection of the tumour was performed as described for case1. Histology confirmed a malignant melanoma of mixedepithelioid and spindle B cell type, which appearedcompletely excised with clear excision margins. Bruch′s
a
c
b
12
3
Fig. 1 Clinical photographs of case 1. a Domed pigmented choroidalmelanoma arising nasal to the optic disc. b Removal of melanoma(shown in Fig. 1a) resulting in surgical coloboma. Pigmented tumourrecurrence seen at nasal edge (arrow). c Seven years after initial localresection showing surgical coloboma (1) and laser retinopexy (2) witha small area of presumed tumour recurrence at interface (3)
742 Graefes Arch Clin Exp Ophthalmol (2010) 248:741–746

membrane was intact overlying the tumour. The tumourrecurred 2 years later at the edge of the surgical colobomaand was treated with ruthenium plaque radiotherapy(Fig. 3b). Two years later, there was further tumourrecurrence at the coloboma edge that was treated withkrypton laser. A further 2 years later, there were widespreadintra-retinal pigmentary changes considered to be clinicalevidence of tumour recurrence and enucleation was thenperformed (Fig. 3c).
The enucleation specimen showed a 15-mm-diameter whitesurgical coloboma with a heavily pigmented area at theposterior margin (Fig. 4a, b), which on histology was aproliferation of retinal pigment epithelium (RPE). However,there were two small satellite nodules of tumour within the
choroid situated superiorly and some distance from thesurgical coloboma (Fig. 4c). There was fine mottled pigmen-tation on the inner surface of the retina (Fig. 4a) that histologyshowed was a layer of tumour cells covering the surface of theretina as well as within the vitreous cavity (Fig. 4d).
At the time of enucleation, the patient was found to haveliver metastases and she died from metastatic disease6 years after the initial diagnosis.
Discussion
TSLR was first introduced in 1966 and is one alternative toenucleation for the treatment of some uveal melanomas [2].
a b
c d
tc
m
h
Fig. 2 Enucleation specimen from case 1. a Enucleation specimenfrom case 1 showing a pale brown tumour mass (t) with an irregularsurface situated in the surgical coloboma (c) on the temporal side.There is diffuse irregular pigmentation of the retina (arrows). b Theedge of the recurrent tumour mass from case 1 showing theirregularity of the tumour surface with no overlying retina and smallclusters of tumour cells “dropping off” the surface (arrows). (H&E,
magnification x40). c The vitreous from case 1 that was detached andlying anteriorly within the posterior segment contains viable tumourcells (arrows) as well as melanophages (m) and focal haemorrhage (h).(H&E, magnification x200). d Posterior surface of the iris from case 1showing clusters of tumour cells (arrows) in relation to the posteriorpigment epithelium. (H&E, magnification x200)
Graefes Arch Clin Exp Ophthalmol (2010) 248:741–746 743
A problem associated with transscleral resection is incom-plete tumour removal that manifests immediately postoper-atively as visible residual tumour or later as recurrenttumour arising from microscopic tumour deposits [2]. Thisresidual or recurrent tumour can result in visual loss andenucleation.
Risk factors for local recurrence include epithelioid celltype, posterior tumour in proximity to disc and fovea, andlack of adjunctive plaque radiotherapy [1, 2]. In the firstcase, the melanoma was posteriorly situated but was ofpredominantly spindle-cell type. In the second case, thetumour was of mixed-cell type but was situated at the oraserrata. The most significant factor for recurrence in boththese cases is the lack of adjuvant plaque radiotherapy.Adjunctive plaque radiotherapy was introduced in 1986 toreduce the incidence of local tumour recurrence althoughit is now used as an effective treatment in its own right. Itsadjuvant use, even in the absence of overt residual orrecurrent disease, appears to be associated with a reductionin mortality [2]. Both patients had local resection prior to1986, therefore, they did not receive plaque radiotherapyat the time of initial resection. It was, however, used totreat tumour recurrence in both cases.
Non-contiguous intraocular tumour recurrences havealso been described following local resection of primaryposterior uveal melanomas [5]. The possible mechanismsfor this include multifocal melanomas, uveal dissemina-tion of the primary tumour, seeding secondary to surgicalmanipulation, and tumour spread from residual melanomaafter local resection. In both the cases, seeding of residualtumour is the likely mechanism of intraocular tumourdissemination. Prior rupture of the posterior vitreous facemay have allowed easy access to the anterior segment inthe first case. In the second case, spread from the primarytumour seems most likely to account for the satellitenodules which were morphologically similar to theprimary.
Vitreous seeding in primary choroidal melanoma hasbeen previously described in several reports of primarymelanoma [6–9]. Indeed it is not uncommon with theCOMs report describing cells in the vitreous in 25.2% of1,527 cases examined [9]. There was no clinical evidenceof vitreous seeding prior to local resection and Bruch′smembrane was intact in the local resection specimens suchthat it seems unlikely that vitreous seeding occurred prior toinitial surgery. Therefore, in the cases presented, we canpostulate that without the natural barrier of the retina,tumour cells were free to seed into the vitreous cavity andhad spread to form a membrane over the inner retinalsurface as well as to cover surfaces in the anterior segmentin case 1. This propensity to cover surfaces is similar to thecase described by Eagle et al. (1982) where melanoma cellsdispersed by the primary tumour had formed a preretinalmembrane giving rise to a picture of pseudoretinitispigmentosa [8].
Both cases show an unusual pattern of intraocular spreadfollowing local resection. However, the natural history of
a
b
c
1
Fig. 3 Clinical photographs of case 2. a Temporal, peripheral,pigmented melanoma extending to ora serrata. b Removal ofmelanoma (shown in Fig. 3a) resulting in surgical coloboma.Widespread presumed recurrence with tumour spreading nasally (1).c Multiple areas of hyperpigmented presumed tumour recurrencewithin coloboma
744 Graefes Arch Clin Exp Ophthalmol (2010) 248:741–746

their tumours is quite different. The second patient developedmetastases and died 6 years after the primary diagnosis. Thefirst patient is still alive 27 years after initial diagnosis,despite the development of splenic and hepatic metastases2 years ago for which she has received palliative chemother-apy. Distant spread following local resection has beenreported to be associated with large basal tumour diameter,mixed/epithelioid cell type and monosomy 3 on cytogeneticanalysis. Both of our cases had a large basal diameter, but theinitial tumour in case 1 was pure spindle-cell type. Unfortu-nately, attempts to perform fluorescent in situ hybridisationfor chromosome 3 on this archival material failed.
In summary, we present two cases that provide aninteresting historical prospective on the treatment ofchoroidal melanoma. Both had previously been treated bylocal resection and had recurred with vitreous seeding,which was not evident at the time of surgery. In both of ourcases, there were several tumour recurrences and it seemslikely that the loss of the retinal barrier assisted in theintraocular spread of these tumours.
Acknowledgements We wish to acknowledge the contribution ofour friend and colleague Dr. Fiona Dolan in drafting and researchingthis manuscript. Sadly, she died before the manuscript could becompleted. All surgery and pathology was carried out in Glasgow. Thelocal resection surgery for cases 1 and 2 was undertaken by ProfessorW. Foulds. The enucleation for case 2 was undertaken by Professor B.Damato. The macro photographs and original histology of the localresection for cases 1 and 2 and the enucleation for case 2 wereundertaken by Professor W.R. Lee.
References
1. Char DH, Miller T, Crawford JB (2001) Uveal tumour resection. BrJ Ophthalmol 85:1213–1219
2. Damato BE, Paul J, Foulds WS (1996) Risk factors for residual andrecurrent uveal melanoma after trans-scleral local resection. Br JOphthalmol 80:102–108
3. Shields JA, Shields CL, Shah P et al (1991) Partial lamellarsclerouvectomy for ciliary body and choroidal tumors. Ophthalmol98:971–983
4. Augsburger JJ, Lauritzen K, Garnel JW et al (1990) Matched groupstudy of surgical resection versus cobalt-60 plaque radiotherapy for
d
ba
c
Fig. 4 Enucleation specimen from case 2. a Enucleation specimenfrom case 2 showing heavy pigmentation within the surgicalcoloboma (arrows). b. Closer view of the posterior pole of case 2showing diffuse pigmentation of the retinal. The surgical coloboma istowards the left-hand side of the picture (arrows). c. Satellite nodule
of malignant melanoma from case 2. The tumour is heavily pigmented(H&E, magnification x 200). d Retina from case 2 showing layer ofheavily pigmented tumour cells covering the inner surface (arrows)(H&E, magnification x100)
Graefes Arch Clin Exp Ophthalmol (2010) 248:741–746 745

primary choroidal or ciliary body melanoma. Ophthalmic Surg21:682–688
5. Kim JW, Damato BE (2002) Noncontiguous tumour recurrence ofposterior uveal melanoma after transscleral local resection. ArchOphthalmol 120:1659–1664
6. Dunn WJ, Lambert M, Kincaid MC, Dieckert JP, Shore JW (1988)Choroidal malignant melanoma with early vitreous seeding. Retina8:188–192
7. Spencer WH (1975) Optic nerve extension of intraocular neo-plasms. Am J Ophthalmol 80:465–471
8. Eagle RC, Shields JA (1982) Pseudoretinitis pigmentosa secondaryto preretinal malignant melanoma cells. Retina 2:51–55
9. Group Collaborative Ocular Melanoma Study (1998) Histopatho-logic characteristics of uveal melanomas in eyes enucleated fromthe collaborative ocular melanoma study COMS report no. 6. Am JOphthalmol 125:745–766
746 Graefes Arch Clin Exp Ophthalmol (2010) 248:741–746